Submitted:
04 September 2025
Posted:
05 September 2025
You are already at the latest version
Abstract
Gait and postural symmetry are fundamental aspects of motor control, with particular relevance for rehabilitation and pediatric development. Asymmetries in plantar loading and balance regulation may reflect normal maturation or early signs of dysfunction. This pilot study aimed to assess plantar pressure distribution and postural stability in healthy pediatric subjects using baropodometric and stabilometric analyses. A single participant (male, 8 years old) with normal motor development underwent static and dynamic baropodometric tests and stabilometric evaluations under both eyes-open and eyes-closed conditions. Static analysis showed a slight predominance of left-foot loading (51%) and a posterior support tendency, while dynamic gait assessment revealed a longer stance duration on the left side and greater propulsion forces on the right. Stabilometric tests demonstrated increased sway and a Romberg index >2.0 in visual deprivation, confirming strong reliance on vision for balance control. These findings indicate that functional asymmetries can be detected even in healthy children and highlight the feasibility of baropodometric and stabilometric tools as objective measures. This pilot study provides preliminary evidence supporting their application in developmental assessment, rehabilitation monitoring, and preventive care in pediatric populations.
Keywords:
gait symmetry
; pediatric biomechanics
; rehabilitation
; baropodometry
; stabilometry
; motor recovery
; postural control
; plantar pressure
; balance assessment
1. Introduction
Symmetry and asymmetry in gait and postural control are fundamental aspects of biomechanics, rehabilitation, and motor recovery. Balanced plantar pressure distribution and stable postural sway represent efficient motor strategies, whereas asymmetries may denote compensatory mechanisms, musculoskeletal dysfunctions, or neuromotor impairments [1,2,3].
Recent studies have emphasized the role of objective methods, such as baropodometry and stabilometry, in evaluating motor symmetry. Doshi et al. [4] showed that wearable inertial sensors can differentiate gait and postural features in populations at risk of falls. Baropodometric methods have been applied in hemiparesis [1], multiple sclerosis [5], low back pain [2], and scoliosis [3], whereas stabilometry is frequently used to quantify center of pressure (CoP) oscillations and postural sway [14,17]. Pediatric studies have confirmed that plantar loading and postural strategies differ significantly from those of adults, reflecting ongoing maturation [9,10,11,16,29].
Baropodometric and stabilometric analyses represent two of the most widely used noninvasive techniques for quantifying gait and postural control. Baropodometry refers to the assessment of plantar pressure distribution during the static stance and dynamic gait. This method provides detailed information on weight-bearing patterns, foot loading symmetry, propulsion forces, and gait phases [1,9,10]. Clinically, baropodometry has been used to monitor alterations in plantar support in patients with hemiparesis [1], multiple sclerosis [5], and scoliosis [3] as well as to evaluate the relationship between foot type and postural control in children [9]. In rehabilitation, it is often used to track the evolution of motor recovery and guide interventions aimed at redistributing plantar loads [2,8,20].
In contrast, stabilometry focuses on the analysis of center of pressure (CoP) oscillations when an individual stands on a force or pressure platform. It quantifies postural sway using parameters such as path length, ellipse area, and sway velocity, thereby reflecting sensory integration and balance control strategies [14,17]. Stabilometric evaluation has proven useful in detecting increased visual dependence in children [29], monitoring motor recovery after musculoskeletal injuries [31], and assessing proprioceptive training effects [7,25]. Its sensitivity to changes in visual, vestibular, or proprioceptive inputs makes it particularly relevant in pediatric populations, where balance control is still developing [10,16].
Taken together, baropodometry and stabilometry provide a complementary view of motor function; while the former captures plantar loading and gait mechanics, the latter reflects postural regulation and sensory integration. Their integration allows for a more holistic evaluation of symmetry and asymmetry in human movement, with applications ranging from sports sciences to preventive pediatric care and clinical rehabilitation [6,13,18].
Within Symmetry, multiple studies have addressed gait and postural asymmetries. Monteiro-Rodrigues et al. [6] identified plantar pressure asymmetries in healthy adults, whereas Shibata and Yoshida [7] demonstrated that targeted mobilization improved stability under visual deprivation. Other studies have explored gait symmetry after trauma [31], plantar pressure indices in musculoskeletal disorders [20,23], and computational analyses of plantar loading [17,18]. Furthermore, recent pediatric studies have highlighted asymmetries in gait with prostheses [8], foot type differences [9], and the impact of high-intensity training on neurodivergent children [13].
Despite these advances, no study has systematically applied baropodometric or stabilometric methods to quantify symmetry in healthy children. Pediatric literature outside of Symmetry highlights that children often exhibit posterior loading, increased sway, and visual dependence for balance [10,11,16,25,26]. These asymmetries diminish with age but may persist or become maladaptive in conditions such as idiopathic toe walking [27], developmental coordination disorder [28], or neuromuscular disease [27,29]. Thus, establishing normative pediatric data is essential.
In this context, we formulated several working hypotheses to guide the pilot investigation. We expected that the analyses would reveal subtle but measurable asymmetries, even in healthy pediatric subjects, and that these methods would prove feasible for application in preventive and rehabilitation-oriented pediatric assessments.
HW1: Baropodometric analysis will reveal subtle asymmetries in plantar load distribution, even in healthy pediatric subjects.
HW2: Stabilometric testing indicates increased postural sway and a higher Romberg index under visual deprivation, reflecting children’s developmental reliance on vision for balance control.
HW3: The combined use of baropodometric and stabilometric methods will demonstrate feasibility as complementary tools for early screening and preventive assessment of gait and postural asymmetries in pediatric populations.
The present pilot study aimed to evaluate gait and postural symmetry in a healthy pediatric subject using baropodometric and stabilometric analyses. By documenting subtle asymmetries, this study contributes to the understanding of developmental motor control and offers perspectives for early rehabilitation monitoring.
2. Materials and Methods
To explore these working hypotheses (HW1–HW3), this pilot study employed a baropodometric platform and stabilometric system to quantify plantar pressure distribution and postural sway in healthy pediatric subjects. The experimental design was structured to capture both static and dynamic load patterns, as well as balance control under visual and non-visual conditions.
2.1. Participants
The study involved a single healthy pediatric participant (male, 8 years old) with no history of neuromotor or orthopedic disorders and exhibiting normal motor development. Participation was voluntary, and written informed consent was obtained from the parents prior to enrollment. The experimental protocol adhered to the principles of the Declaration of Helsinki and was conducted in a private rehabilitation clinic in Bucharest, where participants were regularly engaged in a preventive motor activity program.
2.2. Measurement Instruments
Evaluation was performed using a baropodometric platform (FreeMed®, Sensor Medica, Guidonia, Italy) and a computerized stabilometric system (FreeMed® Stabilometry Module, Sensor Medica, Italy), capable of recording plantar pressure distribution and center of pressure (CoP) oscillations in real time.
Baropodometric analysis included:
- Static test: assessment of plantar load distribution between the left and right foot, and between the forefoot and rearfoot.
- Dynamic test: Analysis of successive footprints during gait, including stance and propulsion phases.
Stabilometric analysis included:
- Romberg test (eyes open and closed) was used to evaluate postural control and visual dependence.
- Computation of the sway ellipse area and CoP trajectory (path length and area) as indicators of balance stability.
2.3. Experimental Protocol
The participant performed all trials barefoot, with the arms relaxed alongside the body:
- Static analysis: upright stance for 30 s while focusing on a fixed visual target at the eye level.
- Dynamic analysis: walking across the platform at a self-selected pace, repeated three times; mean values were used.
- Stabilometric analysis (Romberg test): bipodal stance for 30 s with eyes open, followed by 30 s with eyes closed.
All trials were automatically recorded and processed using proprietary software.
2.4. Parameters Analyzed
- Plantar load distribution: % load on the left vs. right foot; % load on the forefoot vs. rearfoot.
- Dynamic gait parameters: step length (cm), contact time (ms), and peak propulsion pressure (kPa).
- Stabilometric parameters:
- 1. CoP sway area (mm²) and path length (mm)
- 2. Anteroposterior and mediolateral oscillations (mm)
- Romberg index (ratio of eyes closed to eyes open).

Table 1.
Parameters analyzed in baropodometric and stabilometric assessments.
| Category | Parameter | Unit | Description |
| Static plantar pressure | Left vs. right load distribution | % | Relative distribution of plantar load between left and right foot |
| Static plantar pressure | Forefoot vs. rearfoot load distribution | % | Relative distribution of plantar load between forefoot and rearfoot |
| Dynamic gait | Step length | cm | Distance between two successive steps |
| Dynamic gait | Contact time | ms | Duration of foot–ground contact |
| Dynamic gait | Peak propulsion pressure | kPa | Maximum plantar pressure generated during propulsion |
| Stabilometry | CoP sway area | mm² | Area covered by center of pressure oscillations |
| Stabilometry | CoP path length | mm | Total length of the CoP trajectory during test |
| Stabilometry | Romberg index | ratio (eyes closed/open) | Ratio of postural stability with eyes closed vs. eyes open |
3. Results
The results are presented in relation to the working hypotheses formulated in the introduction.
- HW1 (Baropodometric analysis): Static plantar pressure distribution indicated a slight left–right asymmetry, with a predominance of left-foot loading (51%) compared to the right (49%), and a posterior tendency with greater rearfoot support (62%). Dynamic analysis confirmed this pattern, with the left side contributing to a longer stance duration, while the right side generated higher propulsion forces. These findings support HW1 by demonstrating detectable asymmetries, even in a healthy subject.
- HW2 (Stabilometric analysis): Stabilometric testing revealed increased postural sway under visual deprivation, with a larger sway ellipse area and a Romberg index exceeding 2.0. These results are consistent with those of HW2, indicating that children exhibit a strong reliance on vision to maintain balance.
- HW3 (Combined feasibility): Together, the baropodometric and stabilometric results demonstrate the feasibility of integrating these complementary methods for symmetry and asymmetry assessment in pediatric populations, supporting HW3.
3.1. Static Baropodometric Analysis
The static baropodometric assessment revealed an overall balanced distribution of plantar loads, with a slight predominance in the left foot (51%) compared to the right foot (49%). Analysis of the anterior–posterior distribution showed that the rearfoot supported the majority of the load (62%), while the forefoot accounted for 38%. These findings indicate a mild asymmetry characterized by a posterior loading tendency, which may reflect the developmental features of pediatric posture. The detailed values are presented in Table 1, and the distribution of plantar loads between the left and right feet is graphically represented in Figure 1.
Table 1.
Static baropodometric data. Distribution of plantar load between left and right foot, and between forefoot and rearfoot.
Table 1.
Static baropodometric data. Distribution of plantar load between left and right foot, and between forefoot and rearfoot.
| Foot | Load (%) | Forefoot (%) | Rearfoot (%) |
|---|---|---|---|
| Left | 51 | 37 | 63 |
| Right | 49 | 39 | 61 |
3.2. Dynamic Baropodometric Analysis
During the dynamic assessment of gait, successive footprints demonstrated consistent sequencing; however, subtle asymmetries were observed between the two limbs. The left foot exhibited a slightly longer step length (52 cm vs. 50 cm) and a longer stance duration (0.72 s vs. 0.68 s), suggesting its role in contributing to overall stability. In contrast, the right foot generated higher peak propulsion forces (240 N vs. 220 N), reflecting a greater contribution to the forward progression. These complementary asymmetries illustrate a functional differentiation between stability and propulsion during gait, which has been described as a characteristic of pediatric motor development. The specific values are summarized in Table 2, and the comparison of step length, stance duration, and propulsion forces between the left and right sides is illustrated in Figure 2.
3.3. Stabilometric Analysis
The stabilometric evaluation highlighted an increase in postural sway when the visual input was removed. With eyes open, the center of pressure (CoP) path length was 210 mm, and the sway ellipse area was 180 mm², values that remained within the expected range for a stable stance, although mediolateral oscillations were evident. With eyes closed, both parameters increased markedly (340 mm for path length and 320 mm² for ellipse area), indicating reduced postural stability in the absence of visual guidance. The Romberg index exceeded 2.0, confirming a strong reliance on visual input for balance control, which is consistent with the pediatric postural strategies described in the literature. The corresponding stabilometric values are reported in Table 3, and the differences between the eyes-open and eyes-closed conditions are depicted in Figure 3.
In summary, the static analysis revealed a mild left–right asymmetry in plantar loading, with the left foot supporting 51% of body weight compared to 49% on the right, and a predominance of rearfoot loading (62%) relative to the forefoot (38%) (Table 1, Figure 1). This posterior loading strategy is commonly described in children, as the maturation of gait is associated with the progressive redistribution of plantar pressures toward a more balanced forefoot–rearfoot pattern. Previous pediatric studies have shown that younger children exhibit greater variability and asymmetry in static support, which tends to decrease with age as motor control improves.
Dynamic assessment further highlighted subtle gait asymmetries (Table 2 and Figure 2). The left foot demonstrated a slightly longer step length (52 cm vs. 50 cm) and stance duration (0.72 s vs. 0.68 s), suggesting a stabilizing role, whereas the right foot exhibited higher peak propulsion forces (240 N vs. 220 N), reflecting a greater contribution to forward progression. Such side-specific differences are consistent with developmental gait patterns, where one limb often provides stability, while the contralateral limb contributes more to propulsion. Pediatric gait literature describes these asymmetries as part of a transitional process toward a mature, more symmetrical gait pattern typically reached in late childhood.
Stabilometric evaluation confirmed increased postural sway under visual deprivation (Table 3, Figure 3). With eyes open, the CoP path length was 210 mm and the sway ellipse area was 180 mm²; with eyes closed, these values increased to 340 mm and 320 mm², respectively. The Romberg index exceeded 2.0, indicating a strong dependence on visual input for balance control. This finding is in line with prior research showing that children rely more heavily on visual cues for maintaining postural stability, as proprioceptive and vestibular integration remains less efficient than in adults. Pediatric stabilometric studies have consistently reported larger sway amplitudes and higher Romberg indices, suggesting that balance control mechanisms are still maturing throughout early and middle childhood.
Taken together, these results demonstrate that even in healthy pediatric subjects, objective baropodometric and stabilometric analyses can identify functional asymmetries and developmental characteristics of gait and posture. The combination of mild plantar asymmetry, complementary gait dynamics, and visual dependence for balance illustrates typical variability in pediatric motor control. Supported by both numerical data (Table 1, Table 2 and Table 3) and graphical representations (Figure 1, Figure 2 and Figure 3), these findings emphasize the feasibility of detecting relevant asymmetries in pediatric populations and highlight the potential role of these tools in rehabilitation and developmental monitoring.
4. Discussion
This pilot study examined gait and postural symmetry in a healthy pediatric subject, guided by three working hypotheses (HW1–HW3). The discussion is therefore organized around these hypotheses, emphasizing the consistency of the findings with the existing literature and their relevance for pediatric assessment and rehabilitation. The results demonstrated subtle but measurable asymmetries in plantar pressure distribution, gait parameters, and postural control. These observations suggest that asymmetry in childhood should not be regarded solely as a pathological marker, but may also reflect normal developmental variability in motor strategies.
4.1. HW1 – Baropodometric Analysis and Plantar Load Asymmetries
Static analysis revealed a slight predominance of left-foot loading and posterior distribution of plantar pressure. This pattern is consistent with the findings of Monteiro-Rodrigues et al. [6], who reported rearfoot dominance in adults, and with pediatric studies demonstrating posterior support strategies during growth [9,10]. Dynamic analysis further emphasized the complementary roles of the limbs: the left foot primarily contributed to stability, whereas the right foot generated greater propulsion forces. Similar asymmetric contributions have been described in both healthy children [12,16] and pathological contexts, such as idiopathic toe walking [27]. These results support HW1 by showing that baropodometry can detect subtle but measurable asymmetries, even in children without clinical pathology. While such asymmetries may represent adaptive mechanisms facilitating motor development, their persistence could predispose to musculoskeletal imbalance, underscoring the preventive value of baropodometric assessments in pediatric populations.
4.2. HW2 – Stabilometric Analysis and Visual Dependence in Postural Control
Stabilometric assessment revealed strong reliance on visual input, with enlarged sway areas and a Romberg index greater than 2.0 under eyes-closed conditions. These results confirm HW2 and are in line with previous studies showing that children rely more heavily on vision to maintain balance than adults [25,29]. Shibata and Yoshida [7] similarly reported that targeted rehabilitation could reduce postural instability under visual deprivation, supporting the importance of sensory training in balance development. Further evidence from VR-based postural control interventions [28] and EMG-based gait analyses [12] highlights the role of multimodal sensory integration in pediatric motor control. Moreover, exaggerated visual dependence has been observed in children with developmental coordination disorders or neuromuscular impairments [27,28], suggesting that stabilometry is a valuable diagnostic and monitoring tool in both healthy and clinical populations.
4.3. HW3 – Combined Feasibility of Baropodometric and Stabilometric Assessment
The integration of baropodometric and stabilometric findings provides strong support for HW3, demonstrating the feasibility of these complementary methods in pediatric evaluation. Baropodometry offers detailed information on plantar load distribution, gait phases, and propulsion, whereas stabilometry captures postural sway and sensory reliance. Together, they provide a holistic picture of motor function and symmetry, aligning with prior work that has emphasized the need for multimodal assessment in rehabilitation and sports science [2,6,18]. In the pediatric context, this combined approach has significant potential for early screening, preventive interventions, and individualized rehabilitation strategies, particularly for children with orthopedic or neuromotor vulnerabilities. By highlighting both functional asymmetries and sensory integration patterns, this methodology contributes to a more comprehensive understanding of motor development and its clinical application.
4.4. Clinical Implications
Although the participant was healthy, the findings were clinically significant. Baropodometry and stabilometry have been validated in hemiparetic [1], MS [5], and scoliosis populations [3]. Extending their application to pediatric practice may help detect early asymmetries and monitor rehabilitation effects. Foot type differences [9], prosthesis use [8], and pathological gait conditions [27,28] all demonstrate the value of plantar pressure analysis in guiding interventions.
Additionally, reliability studies have confirmed that baropodometric measures are valid for children aged 4–12 years [26], supporting the feasibility of their integration in pediatric care.
4.5. Gait and Postural Symmetry Assessment in Pediatric Prevention and Rehabilitation
The assessment of gait and postural symmetry is not only of scientific relevance but also of clinical and preventive importance. In children, asymmetries may initially appear as functional adaptations during growth; however, if not identified early, they can predispose children to postural deviations, musculoskeletal imbalances, or inefficient motor patterns [9,10,29]. Baropodometric and stabilometric analyses, by providing objective and quantifiable data, enable clinicians to detect such deviations at a subclinical stage before they evolve into overt pathology.
From a preventive perspective, integrating these methods into routine pediatric evaluations may support the identification of children at risk of developing postural or gait abnormalities, such as flatfoot, idiopathic toe walking, or balance deficits associated with poor sensory integration [11,16,27]. Early detection can guide targeted interventions, including proprioceptive training, corrective exercise, and adapted motor activity programs in schools or community health initiatives [2,25,28].
From a rehabilitation perspective, these tools have the advantage of objectively monitoring treatment progress. They can quantify changes in plantar load redistribution, improvements in balance control, and reductions in asymmetry following interventions such as manual therapy, perceptive rehabilitation, or VR-based balance training [5,7,13,28]. For pediatric populations recovering from orthopedic injuries or neuromotor disorders, baropodometric and stabilometric assessments offer outcome measures and motivational feedback to both families and therapists.
Ultimately, combining prevention and rehabilitation approaches based on gait and postural symmetry analyses may contribute to promoting healthier motor development trajectories, reducing long-term risks, and enhancing children’s quality of life.
4.6. Future Research Directions
Although this pilot study demonstrated the feasibility of detecting functional asymmetries in a healthy pediatric subject, its single-case design represents an obvious limitation. Therefore, future research should prioritize larger age-stratified cohorts to establish normative datasets of plantar pressure distribution and stabilometric indices across different stages of development. Such reference values are essential for distinguishing normal developmental variability from pathological asymmetries.
Comparative studies between healthy children and those with neuromotor or orthopedic conditions, such as idiopathic toe walking, developmental coordination disorder, or neuromuscular diseases, would further clarify whether the observed asymmetries are adaptive or maladaptive. Longitudinal designs could provide valuable insights into how gait and postural symmetry evolve over time and whether specific asymmetries predict later motor impairments or postural deficits.
In parallel, future studies should examine the effectiveness of targeted rehabilitation programs, such as proprioceptive training, sensorimotor stimulation, or VR-based therapies, in reducing maladaptive asymmetries and enhancing balance control. Combining baropodometric and stabilometric analyses with advanced technologies, including wearable sensors, machine learning algorithms, and real-time biofeedback systems, may offer new opportunities for continuous monitoring and personalized intervention. Moreover, integrating these approaches into school or preventive health programs could support the early identification of children at risk of developing motor dysfunction.
Ultimately, interdisciplinary collaboration between clinicians, biomechanists, engineers, and educators is essential to expand the scope of research from single-case pilot studies to comprehensive frameworks that address both fundamental developmental processes and applied rehabilitation strategies.
These findings reinforce the idea that functional asymmetries are integral to motor development. Distinguishing developmental variability from maladaptive asymmetry is essential for timely rehabilitation. By extending the scope of symmetry to pediatric populations, this study emphasizes the importance of early screening and objective monitoring of gait and postural symmetry.
5. Conclusions
This pilot study demonstrated that baropodometric and stabilometric analyses can successfully identify subtle functional asymmetries in gait and postural control, even in healthy pediatric subjects. Static plantar loading revealed a mild left–right imbalance with posterior predominance, dynamic testing highlighted differentiated roles of the limbs in stability and propulsion, and stabilometric measures confirmed strong reliance on visual input for balance. Together, these findings support the feasibility and clinical potential of symmetry assessment tools in pediatric populations.
Although limited by its single-case design, this study provides a methodological framework and preliminary evidence that may inform larger investigations. Establishing normative pediatric data, comparing healthy and pathological groups, and integrating advanced monitoring technologies are essential for advancing research in this area. Beyond its scientific contribution, the present study underscores the relevance of symmetry assessment in rehabilitation and preventive care, highlighting its potential to guide early intervention and promote optimal motor development in children.
The results support HW1 by demonstrating detectable plantar load asymmetries, HW2 by confirming visual dependence in postural control, and HW3 by validating the combined feasibility of baropodometric and stabilometric assessments as complementary tools for pediatric evaluation.
Author Contributions
“Conceptualization, methodology, validation, formal analysis, investigation, data curation, writing—original draft preparation, writing—review and editing, visualization, supervision: Teodora Dominteanu, Amelia Elena Stan and Andreea Voinea. All authors have read and agreed to the published version of the manuscript.”
Funding
“This research received no external funding”.
Data Availability Statement
”No new data were created or analyzed in this study. Data sharing is not applicable to this article”.
Acknowledgments
”During the preparation of this manuscript, the authors used ChatGPT (OpenAI, San Francisco, CA, USA) and Paperpal (Cactus Communications, Mumbai, India) for English translation, grammar improvement, and proofreading support. The authors have carefully reviewed and edited the output, and take full responsibility for the content of this publication”.
Conflicts of Interest
“The authors declare no conflicts of interest.”
Abbreviations
The following abbreviations are used in this manuscript:
| CoP | Center of Pressure |
References
- De Menezes, L.T.; Barbosa, P.H.F.A.; Costa, A.S.; Mundim, A.C.; Ramos, G.C.; Paz, C.C.S.C.; Martins, E.F. Baropodometric technology used to analyze types of weight-bearing during hemiparetic upright position. Fisioter. em Mov. 2012, 25(3), 583–594.
- Paolucci, T.; Fusco, A.; Iosa, M.; Grasso, M.R.; Spadini, E.; Paolucci, S.; Saraceni, V.M.; Morone, G. The efficacy of a perceptive rehabilitation on postural control in patients with chronic nonspecific low back pain. Clin. Rehabil. 2012, 26(4), 335–345.
- Marin, L.; Kawczyński, A.; Carnevale Pellino, V.; Febbi, M.; Silvestri, D.; Pedrotti, L.; Lovecchio, N.; Vandoni, M. Displacement of centre of pressure during rehabilitation exercise in adolescent idiopathic scoliosis patients. J. Clin. Med. 2021, 10, 2837. [CrossRef]
- Doshi, K.B.; Moon, S.H.; Whitaker, M.D.; Lockhart, T.E. Assessment of gait and posture characteristics using a smartphone wearable system for persons with osteoporosis with and without falls. Sci. Rep. 2023, 13, 538. [CrossRef]
- Maden, T.K.; Bayramlar, K.Y.; Yakut, Y. The effect of cervical mobilization on balance and static plantar loading distribution in patients with multiple sclerosis: A randomized crossover study. Neurosciences 2022, 27(1), 31–39. [CrossRef]
- Monteiro-Rodrigues, L.; Nuno, S.L.; Granja, T.; Florindo, M.E.; Gregório, J.; Atalaia, T. Perfusion, stance and plantar pressure asymmetries in the absence of disease—A pilot study. Symmetry 2022, 14, 441. [CrossRef]
- Shibata, D.; Yoshida, Y. Self-Mobilization Exercise Program Improved Postural Stability in the Anterior-Posterior Direction with Eyes Closed. Symmetry 2023, 15, 1321. [CrossRef]
- Glowinski, S.; et al. Gait analysis with an upper limb prosthesis in a child: Influence on plantar pressures and gait symmetry. J. Clin. Med. 2025, 14, 2245. [CrossRef]
- Molina-García, C.; Álvarez-Salvago, F.; Pujol-Fuentes, C.; López-del-Amo-Lorente, A.; Ramos-Petersen, L.; Martínez-Sebastián, C.; Martínez-Amat, A.; Jiménez-García, J.D.; De Diego-Moreno, M. Influence of foot type on physical characteristics, laxity, strength and baropodometry in children aged 5–10 years. Appl. Sci. 2024, 14, 8578. [CrossRef]
- Mocanu, G.; et al. Analysis of the influence of age stages on static plantar pressure indicators using a baropodometric platform. Appl. Sci. 2021, 11, 7320. [CrossRef]
- Kojić, M.; et al. The relationship between foot status and motor status in preschool-aged children. Healthcare 2021, 9, 936. [CrossRef]
- Daunoravičienė, K.; et al. EMG-based analysis of gait symmetry in healthy children. Sensors 2021, 21, 5983. [CrossRef]
- Chernik, N.D.; Young, M.W.; Jacobson, R.N.; Kantounis, S.J.; Lynch, S.K.; Virga, J.Q.; Cannata, M.J. Effects of high-intensity training on gait symmetry and locomotor performance in neurodivergent children: A pilot study. Symmetry 2025, 17, 1073. [CrossRef]
- Fullin, A.; Caravaggi, P.; Picerno, P.; Mosca, M.; Caravelli, S.; De Luca, A.; Lucariello, A.; De Blasiis, P. Variability of postural stability and plantar pressure parameters in healthy subjects evaluated by a novel pressure plate. Int. J. Environ. Res. Public Health 2022, 19, 2913. [CrossRef]
- Abou Ghaida, H.; et al. Effect of sensor size, number, and position on center of pressure measurements. Sensors 2023, 23, 4848. [CrossRef]
- Liu, W.; et al. Biomechanical characteristics of typically developing toddlers. Children 2022, 9, 406. [CrossRef]
- Serrato-Pedrosa, J.A.; et al. Biomechanical evaluation of plantar pressure distribution in soft tissue during standing. Appl. Sci. 2024, 14, 1650. [CrossRef]
- Taborri, J.; et al. Machine learning for postural stability prediction using baropodometric features. Sensors 2024, 24, 3646. [CrossRef]
- Loukovitis, A.; et al. Test–retest reliability of PODOSmart® gait analysis insoles. Sensors 2021, 21, 7532. [CrossRef]
- Babović, S.S.; et al. Labeling of baropodometric analysis data using computer vision: Evaluation of foot progression angle. Medicina 2023, 59, 840. [CrossRef]
- Fan, Y.; Fan, Y.; Li, Z.; Lv, C.; Luo, D. Natural gaits of the non-pathological flat foot and high-arched foot. arXiv 2010, arXiv:1012.3816.
- Patwari, M.; Chazistergos, P.; Sundar, L.; Chockalingam, N.; Ramachandran, A.; Naemi, R. Comparison of plantar soft tissue strainability distribution and homogeneity between ulcerated and non-ulcerated patients using strain elastography. arXiv 2022, arXiv:2203.14629.
- Serrato-Pedrosa, J.A.; et al. Numerical analysis of plantar pressure points during gait using finite element modeling. Symmetry 2024, 6, 32. [CrossRef]
- Wang, Y.; Zhang, P.; Chen, G.; Jiang, T.; Zou, Y. Comparison of the asymmetries in foot posture, gait and plantar pressure between patients with unilateral and bilateral knee osteoarthritis. Sci. Rep. 2024, 14, 26761. [CrossRef]
- Sánchez-Rodríguez, R.; et al. Computerized baropodometry in young individuals: plantar pressure and postural load distribution. Life 2025, 15, 1354. [CrossRef]
- Bermejo-Franco, A.; et al. Reliability of plantar pressure and stabilometric measures in children aged 4–12 years: Analysis by baropodometry. J. Orthop. Sports Phys. Ther. 2022, 52, 215–224.
- Ploegmakers, J.J.W.; et al. Postural oscillation in children with Charcot-Marie-Tooth disease: A stabilometric study. PLoS ONE 2018, 13, e0204949. [CrossRef]
- Carcreff, L.; et al. Postural control in children with developmental coordination disorder assessed with virtual reality. Biomedicines 2023, 11, 176. [CrossRef]
- Butterfield, S.A.; et al. Development of postural control from late childhood to adolescence: A longitudinal stabilometric analysis. Neurosci. Lett. 2021, 756, 135948. [CrossRef]
- Trojaniello, D.; et al. IMU-based long-term gait monitoring in children with foot pain: A feasibility study. Sci. Rep. 2025, 15, 91374. [CrossRef]
- Shulman, D.; et al. Gait symmetry after pilon fractures: A biomechanical assessment. Symmetry 2021, 13, 349. [CrossRef]
Figure 1.
Static load distribution. Percentage of plantar load between the left and right foot, as measured in the static baropodometric test.
Figure 1.
Static load distribution. Percentage of plantar load between the left and right foot, as measured in the static baropodometric test.
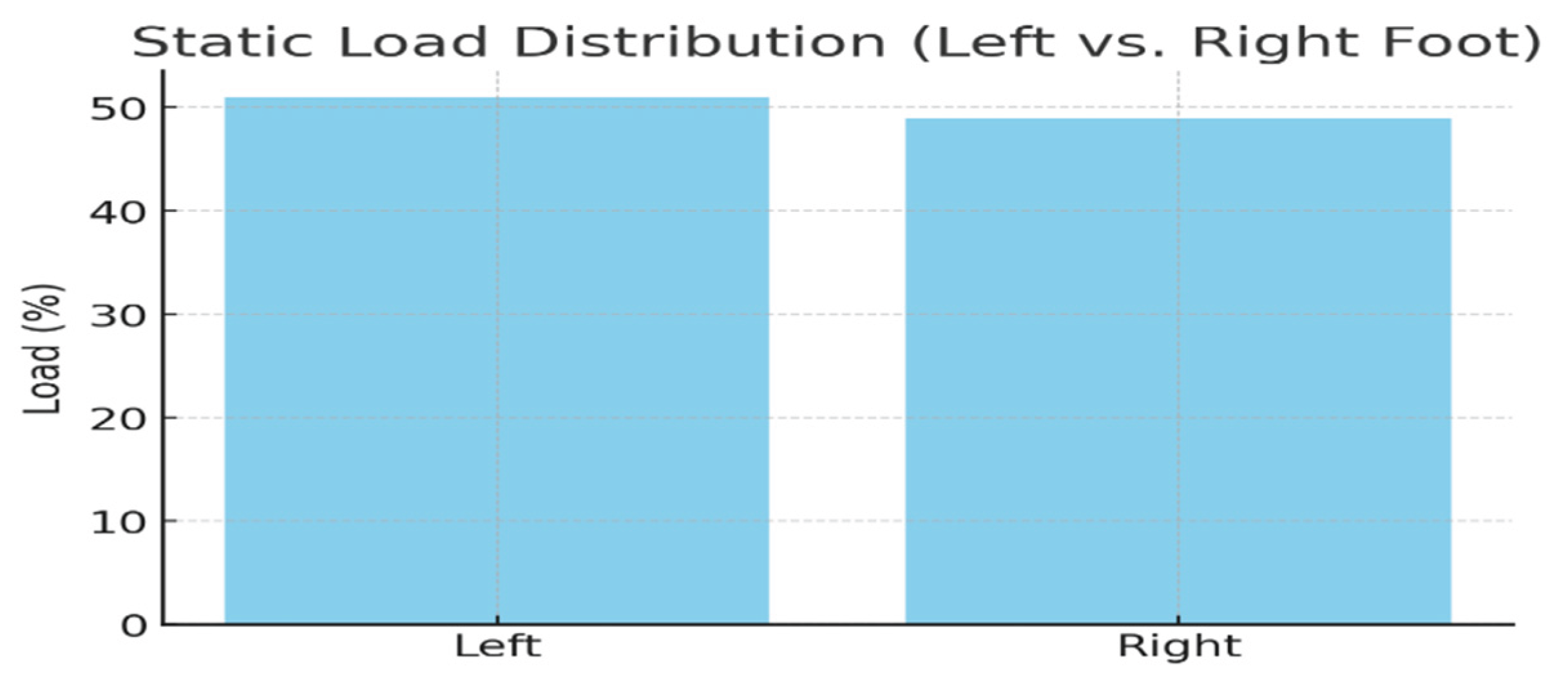
Figure 2.
Dynamic gait parameters. Comparison of step length, stance duration, and peak propulsion force between the left and right foot.
Figure 2.
Dynamic gait parameters. Comparison of step length, stance duration, and peak propulsion force between the left and right foot.
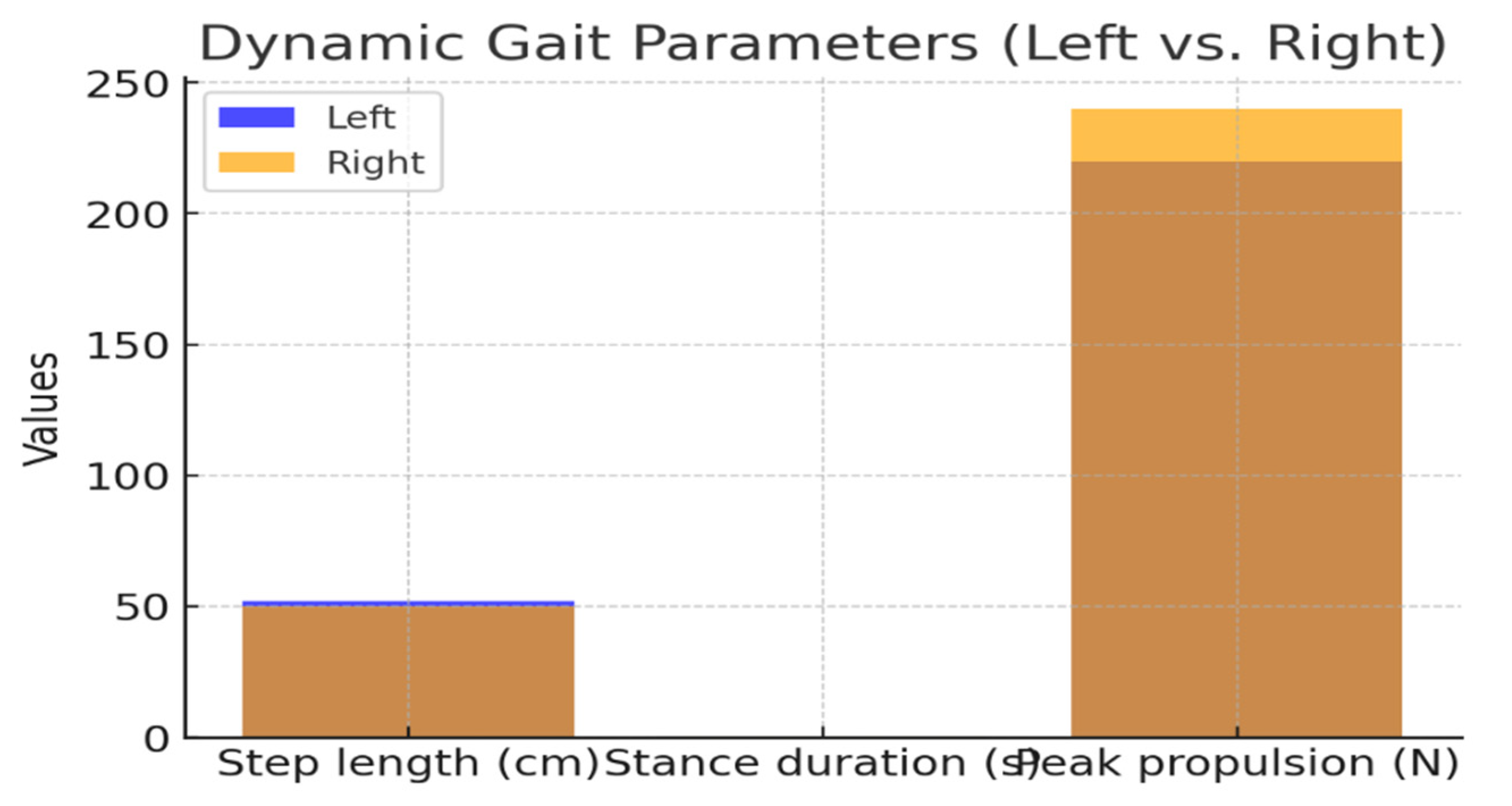
Figure 3.
Stabilometric results. Center of pressure (CoP) trajectory length and sway ellipse area under eyes-open and eyes-closed conditions.
Figure 3.
Stabilometric results. Center of pressure (CoP) trajectory length and sway ellipse area under eyes-open and eyes-closed conditions.
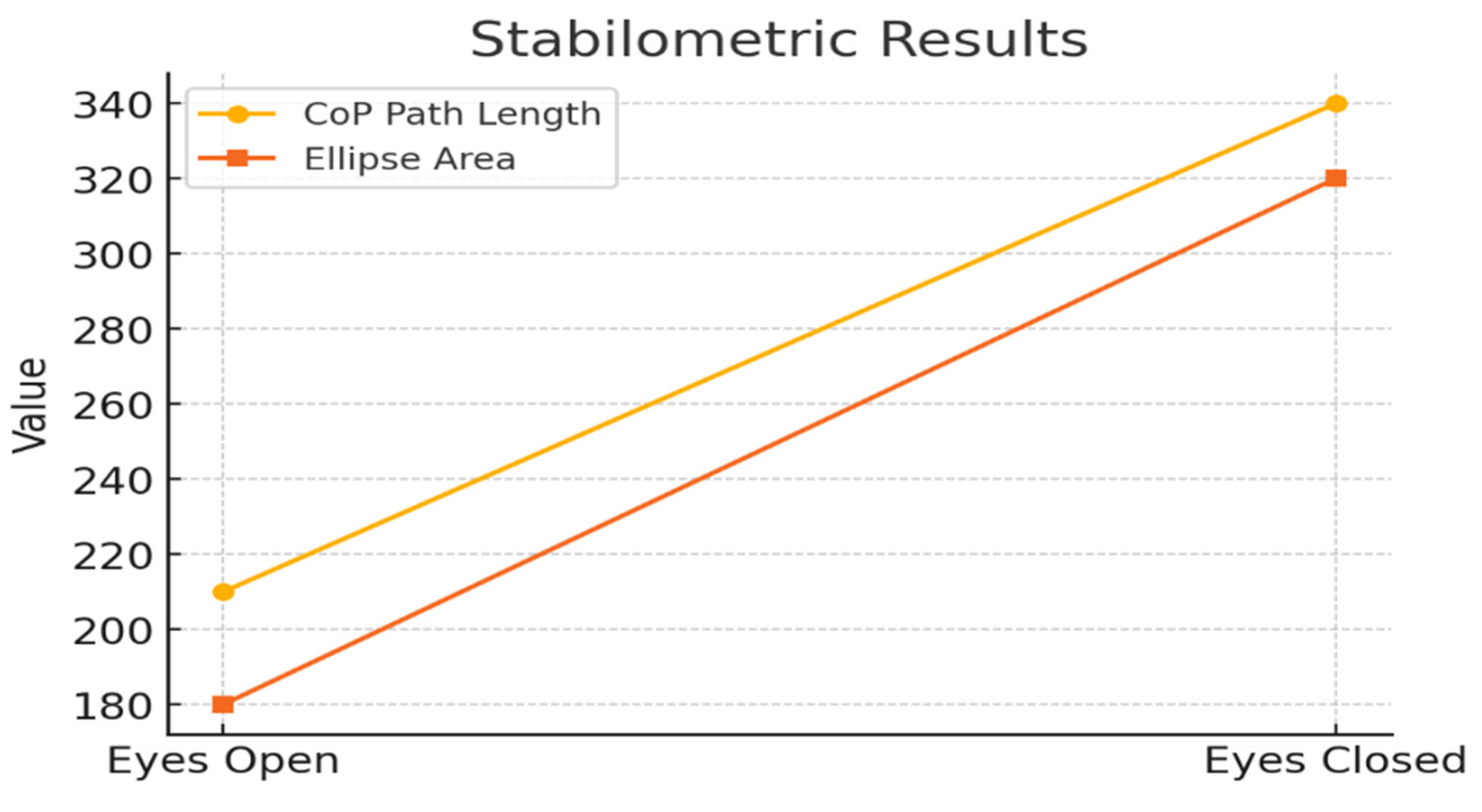
Table 2.
Dynamic gait data. Comparison of step length, stance duration, and propulsion force between the left and right foot.
Table 2.
Dynamic gait data. Comparison of step length, stance duration, and propulsion force between the left and right foot.
| Parameter | Left Foot | Right Foot |
|---|---|---|
| Step length (cm) | 52 | 50 |
| Stance duration (s) | 0.72 | 0.68 |
| Peak propulsion (N) | 220 | 240 |
Table 3.
Stabilometric data. Center of pressure (CoP) trajectory, ellipse area, and Romberg index under eyes-open and eyes-closed conditions.
Table 3.
Stabilometric data. Center of pressure (CoP) trajectory, ellipse area, and Romberg index under eyes-open and eyes-closed conditions.
| Condition | CoP Path Length (mm) | Ellipse Area (mm²) | Romberg Index |
| Eyes Open | 210 | 180 | 1.0 |
| Eyes Closed | 340 | 320 | 2.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



