Submitted:
04 September 2025
Posted:
05 September 2025
You are already at the latest version
Abstract
Purpose: To explore the prognostic potential of gross tumor volume (GTV)–based delta-radiomic features from CT simulation scans in patients with locally advanced unresectable vulvar cancer. Methods: A total of 21 patients (between 2019–2024) undergoing definitive radiotherapy were included, with baseline and post–phase-I (after 25 fractions) CT simulation scans analyzed. Radiomic features (n = 107) were extracted from GTVs using PyRadiomics, and delta features were calculated as the relative change between scans. A multi-step selection pipeline (univariable Cox screening (p < 0.10), correlation filtering and Lasso-Cox) was applied for each endpoint: local control (LC), regional control, distant metastasis–free survival, progression-free survival, and overall survival (OS). Model discrimination was assessed via 500-iteration bootstrapped concordance index (C-index), and calibration was plotted at 24 months. Results: Median follow-up was 50.0 months. The 2-year LC and OS rates were 56.2% and 55.9%, respectively. Final multivariable models retained a sole texture Δ feature for LC (HR = 2.62, 95% CI = 1.05–6.52, p = 0.039; C-index = 0.748) and six Δ features for OS (C-index = 0.864). No features were retained for other endpoints. For LC, increased run-length non-uniformity after phase I predicted poorer control. For OS, increased texture/shape complexity predicted worse survival, whereas increased uniformity predicted better survival. Conclusion: CT-based delta-radiomic features, particularly shape and texture metrics, may predict LC and OS in unresectable vulvar cancer. Despite the small sample size, these findings highlight the potential for delta-radiomics as a noninvasive biomarker for risk stratification. Validation in larger cohorts and exploring potential in adaptive radiotherapy are warranted.
Keywords:
vulvar cancer
; delta-radiomics
; radiomics
; CT simulation
; gross tumor volume (GTV)
; prognosis and risk stratification
; local control
; overall survival
; adaptive radiotherapy
1. Introduction
Vulvar cancer is a rare but increasingly diagnosed gynecological cancer, accounting for nearly 5% of all gynecologic malignancies [1,2]. Squamous cell carcinoma accounts for 95% of cases [3]. It is considered a significant clinical challenge, especially in its advanced stages. The management of locally advanced unresectable vulvar cancer usually involves definitive chemoradiation [4]. However, outcomes remain poor, underscoring the need for improved prognostic tools [5,6,7].
Locoregional rather than distant failures account for most treatment relapses in vulvar cancer, carrying substantial morbidity and offer limited salvage options [8,9]. Distant metastases are uncommon and typically occur only after locoregional relapse [8]. Patients who experience locoregional or distant recurrence have markedly poorer survival rates [10].
Radiomics, the high-throughput extraction of quantitative data from medical images, has become a valuable approach for describing tumor heterogeneity and predicting clinical outcomes. Radiomic features extraction from computed tomography (CT) images has become increasingly known as a non-invasive biomarker that have the potential to help in cancer prognostics [11,12]. CT simulation scans are routinely obtained for all radiotherapy patients and thus represent a readily available source of segmented images, with data that can help predict response to treatment, prognosis and treatment-related toxicities [13,14,15]. In March, 2025, Xiao et al. constructed a model combining CT-based radiomic features and clinical indices can predict overall survival (OS) in cervical cancer patients treated with intensity-modulated radiotherapy (IMRT) and concurrent chemotherapy [16].
Another extension of this work is “delta-radiomics,” which assesses changes in radiomic features over the course of therapy [17]. In cervical cancer, delta-radiomics has shown promising results in predicting intermediate and high-risk pathological factors in patients receiving neoadjuvant therapy [18], and may even outperform FIGO stage and MRI-assessed maximum tumor diameter in prognostication of locally advanced cervical cancer treated with chemoradiotherapy [19].
Despite the huge advancements in the field of radiomics and delta-radiomics, the application of delta-radiomics in vulvar cancer remains underexplored. Given the ability of delta-radiomics to identify treatment-related changes and predict clinical outcomes, examining its utility in vulvar cancer could provide valuable insights. The present study aims to evaluate the prognostic potential of delta-radiomic features extracted from CT simulation images in patients with locally advanced unresectable vulvar cancer, focusing on their association with local control (LC), regional control (RC), distant metastasis-free survival (DMFS), progression-free survival (PFS), and OS.
2. Methods
2.1. Patients
In this study, we retrospectively reviewed the records of patients with histologically confirmed, locally advanced, unresectable vulvar squamous cell carcinoma treated at our institution between January 2019 and December 2024. Unresectable disease was defined as primary tumors not amenable to complete surgical excision without unacceptable morbidity, based on multidisciplinary team assessment. Inclusion criteria included: (i) availability of baseline CT simulation scans acquired before the start of definitive radiotherapy and a second CT simulation scan acquired after the first phase of treatment (25 fractions), (ii) gross tumor volume (GTV) of the primary vulvar tumor contoured by the treating radiation oncologist on both scans, and (iii) complete clinical and follow-up data for the study endpoints. Patients with incomplete imaging, inadequate ROI segmentation, or missing follow-up information were excluded. A minimum follow-up duration of 3 months was required. Demographic, clinical, and treatment-related variables were retrieved from electronic medical records, including age at diagnosis, performance status, FIGO stage, radiotherapy dose and technique, concurrent chemotherapy administration, and follow-up duration.
2.2. Treatment, CT Acquisition Parameters and Segmentation
All patients received definitive radiotherapy in two phases. Phase I consisted of 45 Gy delivered in 25 daily fractions, five fractions per week. Field of radiotherapy included the primary vulvar tumor and inguino-pelvic lymph nodes. Phase II subsequently brought the total dose to 60–66 Gy over 30–33 fractions, with a field encompassing the primary vulvar tumor, and involved lymph nodes were included to the maximum tolerable dose. Concurrent chemotherapy consisted of cisplatin at dose of 40mg/mm2, administered weekly [20].
All patients underwent CT simulation in the supine position, with straight-leg position. As contrast-enhanced CT is not routinely used in simulation for definitive radiotherapy, all included images were acquired without contrast. Scans were acquired using Philips Brilliance Big Bore CT (85-cm bore) with a 3-mm slice thickness, axial slices, extending from at least the L2 vertebral level to below the perineum. Baseline CT simulation scans were obtained within two weeks prior to the start of radiotherapy, and post–phase I scans were performed after completion of 25 fractions, prior to initiating the second phase of treatment. Contouring and planning were done using the Pinnacle3 16.2 (Philips Medical System) treatment planning system [21]. All imaging data were stored in DICOM format and retrieved from the institutional radiotherapy planning system for subsequent processing and radiomic feature extraction.
2.3. Radiomic Feature Extraction
Radiomic features were extracted from CT simulation images acquired before and after the first phase of definitive radiotherapy; first scan is before starting radiotherapy, and second scan is after 25 fractions. The pipeline was implemented in Python using open-source libraries including PyRadiomics [22], SimpleITK, pydicom, and rt_utils.
2.4. DICOM Image and RT Structure Acquisition
CT simulation data were retrieved in DICOM format. For each patient, the CT series was read using SimpleITK’s ImageSeriesReader, which reconstructs the three-dimensional image volume. The resulting CT image was saved as a NIfTI file. In parallel, the corresponding RT structure set (RTSTRUCT) was accessed using pydicom. The ROI corresponding to the gross tumor volume (GTV) of the primary vulvar tumor contoured by treating radiation oncologist was then selected for feature extraction.
2.5. ROI Mask Generation
The RTSTRUCT file was combined with the CT DICOM series using the RTStructBuilder from the rt_utils package. The builder generated a binary mask. Given that the default output shape of the mask was (width, height, slices), the mask array was transposed to ensure correct spatial interpretation by SimpleITK. This transposed binary mask was then converted into a SimpleITK image and its spatial metadata was aligned with that of the CT image. The resulting ROI mask was saved in NIfTI format.
2.6. Radiomic Feature Extraction
Radiomic feature extraction was performed using PyRadiomics. The saved CT image and corresponding ROI mask were loaded as SimpleITK images. A default PyRadiomics feature extractor was instantiated, and 107 quantitative features (including first-order statistics, shape, and texture features based on gray-level co-occurrence, run-length, size-zone, and neighboring gray tone difference matrices) were extracted. This entire pipeline was repeated for both baseline and post-25-fraction CT scans for each patient, thereby enabling a delta-radiomic analysis to evaluate changes in features with respect to survival outcomes.
2.7. Calculation of Delta-Radiomics
Delta-radiomic features, or Δ features, were computed to capture the intra-treatment variation in imaging features. The formula used was:
Where and are the radiomic features from the baseline and post-phase-I scans, respectively.
To ensure comparability across features with different scales, a z-score normalization was applied to the Δ features (Δ features). This transformation rescales the data to have a mean of zero and a standard deviation of one.
2.8. Feature Selection for Survival Outcomes
To select delta-radiomic features for prediction of outcomes, we first performed univariable Cox proportional-hazards regression for each Δ feature against each of the 5 endpoints (LC, RC, DMFS, PFS, and OS), retaining only those with a two-sided p-value < 0.10. Next, we computed pairwise Pearson correlations among the retained features and eliminated one member of any pair with |r| > 0.90, dropping the feature with the weaker univariable association. This step reduces redundant features and combat collinearity. The yielded set of Δ features was then fed into a Lasso-penalized Cox model (L1 regularization) with penalty strength λ chosen via five-fold cross-validated concordance index maximization. Δ features with non-zero coefficients at the optimal λ were deemed robust predictors. Finally, Lasso-selected Δ features were entered into an unpenalized Cox model and a bidirectional stepwise selection based on Akaike’s Information Criterion (AIC) was done. The complete workflow of image processing and radiomics analysis is illustrated in Figure 1.
2.9. Statistical Analysis
Patients’ characteristics were reported as medians, interquartile ranges (IQR), counts and percentages. Median follow-up was calculated using reverse Kaplan-Meier method. Rates of each survival endpoint of LC, RC, DMFS, PFS and OS, were reported as median, 2-year and 4-year rates. Results of significant univariate Cox proportional hazards regression were reported in the supplementary material. For multivariable analysis, proportional-hazards assumptions were assessed using Schoenfeld residuals (all global and covariate-specific tests should be p > 0.05). For covariates showing evidence of violation, time-varying effects were modeled by adding covariate–log(time) interaction terms, and the stepwise selection procedure was repeated with hierarchical retention of main effects. Multicollinearity was assessed by calculating variance inflation factors (all VIFs should be < 5). Results of the final cox model after feature selection were reported in terms of hazard ratios (HR) and CI for each Δ feature, along with the 500-iteration bootstrapped C-index. Calibration plots were provided as supplementary material. A p-value < 0.05 was deemed significant. All statistical analyses were performed using Python version 3.11.13.
3. Results
3.1. Patient Characteristics
Twenty-one patients with locally advanced unresectable vulvar cancer were included. Table 1 shows patients’ characteristics and treatment specifics. The median age at diagnosis was 57.0 years (range: 37–79 years; IQR: 17.0). All patients were treated with definitive radiotherapy. Radiotherapy was planned via volumetric modulated arc therapy (VMAT) in all patients. The total vulvar radiotherapy dose had a median of 65.0 Gy (IQR: 2.6), while the median dose of first phase of radiotherapy in Gy was 45.0 (IQR: 5.4). Only one patient did not receive concurrent chemotherapy with radiotherapy.
3.2. Treatment Outcomes
After a median follow-up of 50.0 months (IQR 10.7–59.0), median LC was not reached, with the 2-year rate of 56.2% (95% CI 29.0–76.5). RC median was also not reached, with 2-year rate being 65.7% (95% CI 33.6–85.1). Median DMFS was 20.0 months (95% CI 11.3–71.0), and the 2-year rate was 44.3% (95% CI 19.3–66.8). Median PFS was 10.0 months (95% CI 8.0–67.0), and the 2-year PFS rate was 36.1% (95% CI 13.7–59.3). Notably, most or all of the events counted by these four endpoints occurred before 2 years, as evident in Table 2. Median OS was 28.0 months (95% CI 16.2–71.0), and the 2-year was 55.9% (95% CI 28.4–76.4). Survival curves are illustrated in Figure 2.
3.3. Univariable Analyses and Feature Selection
On univariable cox regression, several significant Δ features were yielded for each endpoint, and those with a p value of < 0.1 are reported in Supplementary Table 1, along with Kaplan-Meier curves for those with a p value of < 0.5 (Supplementary figures 1-4; none had a p value of < 0.5 for RC).
All Δ features with a p value of < 0.1 were included in the pairwise Pearson correlations (Supplementary Table 2). After excluding redundant Δ features, a Lasso-penalized Cox model was run for each endpoint. At this step, only LC and OS retained any Δ features; no features survived selection for RC, DMFS, or PFS. Selected Δ features that were included in the multivariable analyses are illustrated in Table 3. Supplementary Table 3 shows the temporal changes in Δ features retained in final models.
3.4. Multivariable Analyses and Internal Validation
After AIC-based bidirectional stepwise selection, the final multivariable Cox model for LC only retained the Δ RLNU_norm with a coefficient of 0.962 (HR: 2.62, 95% CI: 1.05–6.52; p = 0.039, Table 4). This translates into more than doubling of the hazard of local recurrence for each one–standard-deviation increase in Δ RLNU_norm. the 500-iteration bootstrap yielded a mean C-index of 0.748 (95% CI 0.506–0.987, Figure 3).
For OS, time-varying effects were incorporated in the final multivariable Cox proportional hazards model to address violations of the proportional hazards assumption identified in initial testing. Bidirectional stepwise selection retained six Δ features (Table 4). Among these, Δ DiffAvg, Δ SVR, Δ DiffVar, and Δ GLNU_norm were statistically significant (p < 0.05); greater increases in texture or contrast (DiffVar, SVR) seem to portend worse survival, whereas larger increases in uniformity metrics (DiffAvg, GLNU_norm) predicter better survival. All retained variables satisfied the proportional hazards assumption in the final model. The bootstrap-corrected C-index for the OS model was 0.864 (95% CI 0.633–0.973, Figure 3). Calibration plots are illustrated in supplementary Figure 5.
4. Discussion
This hypothesis-generating study is the first to provide proof-of-concept that CT GTV-based delta-radiomics may serve as a non-invasive biomarker in patients with locally advanced unresectable vulvar cancer. Using a rigorous feature selection pipeline, including univariable Cox screening, correlation filtering, Cox-Lasso regularization, and AIC-based selection, several features were nominated to predict LC and OS, with no features retained for RC, DMFS and PFS. This likely reflects the source of the features, the GTV, and highlights the fact that predictors of the more common failure pattern, local failure, are likely to predict worse OS in our group of patients.
Such dimensionality reduction is of paramount importance in radiomics studies, where multiple testing can lead to falsely significant findings [23]. Although multiple significant Δ features on univariable cox analyses were yielded (Supplementary Table 1), none were retained after our multi-step feature selection process, as described in results.
Our multivariable Cox model for LC identified one significant feature, RLNU_norm. This texture-based metric captures how uniform the run lengths (i.e., sequences of the same gray level) are in the GTV [22]. Each one unit increase in the RLNU_norm is associated with a 2.6-fold higher hazard of local recurrence (Table 4); the more run-length heterogeneity the tumor becomes after first phase of radiotherapy, the worse its LC is expected to be. For OS, the model retained six Δ features, of which four were significant, indicating that increased uniformity (e.g., in Δ GLNU_norm and Δ DiffAvg) predicted better survival, while increased heterogeneity or complexity (Δ SVR and Δ DiffVar) predicted worse outcomes.
Our multivariable model for OS had a 500-iteration bootstrap C-index of 0.87 (95 % CI 0.61–0.97), indicating a strong discrimination, despite the limited sample size and only 9 captured events. Such findings suggest a promising role of radiomics and delta-radiomics for vulvar cancer prognostication and risk-stratification.
Our findings suggest that residual tumors exhibiting more irregular shapes and higher texture heterogeneity during radiotherapy may reflect treatment resistance and portend worse outcomes. Increasing SVR, a shape feature, reflects the increasing tumor surface complexity relative to volume during treatment. This change can be attributed to the development of infiltrative growth patterns, spiculated borders resulting from radiation-induced fibrosis (or the persistence of aggressive tumor clones), and a necrotic core that leaves uneven tumor surfaces [24].
It has been shown that in carcinoma, metastatic potential is acquired through early molecular changes such as epithelial-to-mesenchymal transformation, orchestrated by the tumor microenvironment and stromal interactions [25]. Whether this heterogeneity in radiomic features reflects the molecular diversity of tumor clones remains a question for future translational studies. Another mystery to be unfolded is whether using subregional segmentation instead of whole GTV as the region of interest to extract radiomic features would capture the well-known intra-tumoral heterogeneity, which may help sharpen the performance of radiomics [26].
We chose to focus on unresectable vulvar cancer because prognostic markers are less well established in this setting. In such cases, tumor-derived radiomic features may represent an important source of prognostic information, whereas in post-surgical scenarios, numerous other determinants, such as pathological findings, margin status, and treatment-related factors, are readily available and have been validated to play a substantial role in outcome prediction [27].
Prior delta-radiomic studies in cervical cancer have demonstrated prognostic value for response to treatment and survival outcomes [16,18,19]. However, vulvar cancer has been underrepresented in radiomics research, with a single study that used 18F-FDG PET/CT-based radiomics to correlate with tumor biology and predict prognosis. Our study addresses this gap and suggests that even in rare cancers, quantitative imaging biomarkers can be developed using standardized pipelines. Moreover, our findings align with prior evidence suggesting that local control, more than distant failure, remains the main challenge in locally advanced vulvar cancer, and potentially determines outcomes in vulvar cancer [7,10,28], thus justifying the focus on GTV-derived features.
CT simulation scans are routinely obtained in radiotherapy planning, and our reliance on these widely available images enhances clinical applicability. Such scans are usually contoured by experienced radiation oncologists according to established contouring guidelines [29]. While MRI and PET/CT may offer more detailed soft-tissue characterization or metabolic data [19,30], their availability, cost, and variability in segmentation limit generalizability. A model based solely on Δ features from segmented CT scans could be integrated into existing workflows with minimal disruption, across different socioeconomic settings. Moreover, results on delta-radiomic features raise the potential for adaptive radiotherapy, where patients with unfavorable delta-radiomic profiles could be flagged early for treatment modifications [31,32]. In fact, prior clinical observations in vulvar cancer indicate that more than half of patients require adaptive replanning during definitive radiotherapy, particularly those with large baseline tumor volumes [33].
Limitations
Our study has several limitations. First, its single-center, retrospective design, small sample size and the lack of external validation reduce its statistical power, and increase the risk of overfitting, all of which may limit the generalizability and reproducibility of the findings. Also, the small sample size hindered the calculation of distant control analysis, as some studies report this event in as few as 5.1% of the cases only [8]. Nonetheless, our limited sample size reflects the rarity of unresectable vulvar cancer. Such obstacle was mitigated by using a multi-step feature selection pipeline with internal bootstrapping and calibration to ensure robustness and reduce overfitting. Accordingly, our results should be interpreted as exploratory, but they provide a rationale for larger multi-institutional validation. Future multi-institutional collaboration will be essential for external validation.
Another limitation is the potential subjectivity in ROI contouring, which may affect reproducibility. This reflects the complexity of available consensuses for vulvar cancer contouring, which are difficult to be prescriptive for every patient scenario, especially in the locally advanced unresectable setting [34,35].
FIGO staging was not included in the final model to avoid overloading the analysis with predictors given the small sample size. Moreover, staging variability was minimal in our cohort, as nearly all patients had stage III–IV disease.
Although contrast-enhanced CT could potentially enhance the prognostic performance of radiomic models, it is not routinely used in simulation for vulvar cancer radiotherapy. Also, feature extraction from contrast-enhanced CT scans introduces potential variability and may not be reproducible across institutions. Using non-enhanced images is more translatable to standard clinical workflows and is safer in patients with kidney impairment.
5. Conclusions
In this study, we demonstrate that CT-based delta-radiomic features, particularly shape and texture metrics, hold a potential prognostic value in locally advanced unresectable vulvar cancer. These features capture intra-treatment changes in tumor morphology and heterogeneity that correlate with LC and OS, potentially offering earlier and more objective risk stratification than conventional methods. While our single-center experience provides foundational evidence for delta-radiomics in this rare malignancy, larger multi-institutional studies are needed to validate these findings. Such noninvasive biomarkers provide hope to guide personalized therapeutic strategies. Future work should integrate radiomics with histopathological and genomic data to elucidate the biological underpinnings of these imaging phenotypes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Acknowledgments
We would like to thank Mohammad Atari for his expert guidance and support with statistical methodology and analyses.
Ethics Approval
This retrospective study data was approved by the Institutional Review Board (IRB) (25 KHCC 028) on 3 September 2025.
References
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA: A Cancer J. Clin. 2025, 75, 10–45. [CrossRef]
- Buttmann-Schweiger, N.; Klug, S.J.; Luyten, A.; Holleczek, B.; Heitz, F.; du Bois, A.; Kraywinkel, K.; Grce, M. Incidence Patterns and Temporal Trends of Invasive Nonmelanotic Vulvar Tumors in Germany 1999-2011. A Population-Based Cancer Registry Analysis. PLOS ONE 2015, 10, e0128073. [CrossRef]
- Alkatout, I.; Schubert, M.; Garbrecht, N.; Weigel, M.T.; Jonat, W.; Mundhenke, C.; Günther, V. Vulvar cancer: epidemiology, clinical presentation, and management options. Int. J. Women’s Health 2015, 7, 305–313. [CrossRef]
- Abu-Rustum, N.R.; Yashar, C.M.; Arend, R.; Barber, E.; Bradley, K.; Brooks, R.; Campos, S.M.; Chino, J.; Chon, H.S.; Crispens, M.A.; et al. Vulvar Cancer, Version 3.2024, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2024, 22, 117–135. [CrossRef]
- Rao, Y.J.; Chin, R.-I.; Hui, C.; Mutch, D.G.; Powell, M.A.; Schwarz, J.K.; Grigsby, P.W.; Markovina, S. Improved survival with definitive chemoradiation compared to definitive radiation alone in squamous cell carcinoma of the vulva: A review of the National Cancer Database. Gynecol. Oncol. 2017, 146, 572–579. [CrossRef]
- Macchia, G.; Lancellotta, V.; Ferioli, M.; Casà, C.; Pezzulla, D.; Pappalardi, B.; Laliscia, C.; Ippolito, E.; Di Muzio, J.; Huscher, A.; et al. Definitive chemoradiation in vulvar squamous cell carcinoma: outcome and toxicity from an observational multicenter Italian study on vulvar cancer (OLDLADY 1.1). La Radiol. medica 2023, 129, 152–159. [CrossRef]
- Kim Y, Kim JY, Kim JY, Lee NK, Kim JH, Kim YB, et al. Treatment outcomes of curative radiotherapy in patients with vulvar cancer: results of the retrospective KROG 1203 study. Radiat Oncol J [Internet]. 2015 Sep 1 [cited 2025 Aug 7];33(3):198. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4607573/.
- Prieske K, Haeringer N, Grimm D, Trillsch F, Eulenburg C, Burandt E, et al. Patterns of distant metastases in vulvar cancer. Gynecol Oncol [Internet]. 2016 Sep 1 [cited 2025 Aug 7];142(3):427–34. Available from: https://www.gynecologiconcology-online.net/action/showFullText?pii=S0090825816308782.
- Salom, E.M.; Penalver, M. Recurrent vulvar cancer. Curr. Treat. Options Oncol. 2002, 3, 143–153. [CrossRef]
- Zach, D.; Åvall-Lundqvist, E.; Falconer, H.; Hellman, K.; Johansson, H.; Rådestad, A.F. Patterns of recurrence and survival in vulvar cancer: A nationwide population-based study. Gynecol. Oncol. 2021, 161, 748–754. [CrossRef]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [CrossRef]
- Manganaro, L.; Nicolino, G.M.; Dolciami, M.; Martorana, F.; Stathis, A.; Colombo, I.; Rizzo, S. Radiomics in cervical and endometrial cancer. Br. J. Radiol. 2021, 94, 20201314. [CrossRef]
- Zhou, C.; Hou, L.; Tang, X.; Liu, C.; Meng, Y.; Jia, H.; Yang, H.; Zhou, S. CT-based radiomics nomogram may predict who can benefit from adaptive radiotherapy in patients with local advanced-NSCLC patients. Radiother. Oncol. 2023, 183, 109637. [CrossRef]
- Kasai, A.; Miyoshi, J.; Sato, Y.; Okamoto, K.; Miyamoto, H.; Kawanaka, T.; Tonoiso, C.; Harada, M.; Goto, M.; Yoshida, T.; et al. A novel CT-based radiomics model for predicting response and prognosis of chemoradiotherapy in esophageal squamous cell carcinoma. Sci. Rep. 2024, 14, 1–10. [CrossRef]
- Nafchi, E.R.; Fadavi, P.; Amiri, S.; Cheraghi, S.; Garousi, M.; Nabavi, M.; Daneshi, I.; Gomar, M.; Molaie, M.; Nouraeinejad, A. Radiomics model based on computed tomography images for prediction of radiation-induced optic neuropathy following radiotherapy of brain and head and neck tumors. Heliyon 2024, 11, e41409. [CrossRef]
- Xiao, L.; Wang, Y.; Shi, X.; Pang, H.; Li, Y. Computed tomography–based radiomics modeling to predict patient overall survival in cervical cancer with intensity-modulated radiotherapy combined with concurrent chemotherapy. J. Int. Med Res. 2025, 53. [CrossRef]
- Shur, J.D.; Doran, S.J.; Kumar, S.; ap Dafydd, D.; Downey, K.; O’cOnnor, J.P.B.; Papanikolaou, N.; Messiou, C.; Koh, D.-M.; Orton, M.R. Radiomics in Oncology: A Practical Guide. RadioGraphics 2021, 41, 1717–1732. [CrossRef]
- Wu, R.-R.; Zhou, Y.-M.; Xie, X.-Y.; Chen, J.-Y.; Quan, K.-R.; Wei, Y.-T.; Xia, X.-Y.; Chen, W.-J. Delta radiomics analysis for prediction of intermediary- and high-risk factors for patients with locally advanced cervical cancer receiving neoadjuvant therapy. Sci. Rep. 2023, 13, 1–8. [CrossRef]
- Wagner-Larsen, K.S.; Lura, N.; Gulati, A.; Ryste, S.; Hodneland, E.; Fasmer, K.E.; Woie, K.; Bertelsen, B.I.; Salvesen, Ø.; Halle, M.K.; et al. MRI delta radiomics during chemoradiotherapy for prognostication in locally advanced cervical cancer. BMC Cancer 2025, 25, 1–15. [CrossRef]
- Reade, C.J.; Eiriksson, L.R.; Mackay, H. Systemic therapy in squamous cell carcinoma of the vulva: Current status and future directions. Gynecol. Oncol. 2014, 132, 780–789. [CrossRef]
- Xia P, Murray E. 3D treatment planning system—Pinnacle system. Med Dosim [Internet]. 2018 Jun 1 [cited 2025 Aug 8];43(2):118–28. Available from: https://pubmed.ncbi.nlm.nih.gov/29580933/.
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [CrossRef]
- Limkin, E.J.; Sun, R.; Dercle, L.; Zacharaki, E.I.; Robert, C.; Reuzé, S.; Schernberg, A.; Paragios, N.; Deutsch, E.; Ferté, C. Promises and challenges for the implementation of computational medical imaging (radiomics) in oncology. Ann. Oncol. 2017, 28, 1191–1206. [CrossRef]
- Vallières, M.; Kay-Rivest, E.; Perrin, L.J.; Liem, X.; Furstoss, C.; Aerts, H.J.W.L.; Khaouam, N.; Nguyen-Tan, P.F.; Wang, C.-S.; Sultanem, K.; et al. Radiomics strategies for risk assessment of tumour failure in head-and-neck cancer. Sci. Rep. 2017, 7, 1–14. [CrossRef]
- Atiya, H.I.; Gorecki, G.; Garcia, G.L.; Frisbie, L.G.; Baruwal, R.; Coffman, L. Stromal-Modulated Epithelial-to-Mesenchymal Transition in Cancer Cells. Biomolecules 2023, 13, 1604. [CrossRef]
- Zhang, L.; Wang, Y.; Peng, Z.; Weng, Y.; Fang, Z.; Xiao, F.; Zhang, C.; Fan, Z.; Huang, K.; Zhu, Y.; et al. The progress of multimodal imaging combination and subregion based radiomics research of cancers. Int. J. Biol. Sci. 2022, 18, 3458–3469. [CrossRef]
- Nooij, L.; Brand, F.; Gaarenstroom, K.; Creutzberg, C.; de Hullu, J.; van Poelgeest, M. Risk factors and treatment for recurrent vulvar squamous cell carcinoma. Crit. Rev. Oncol. 2016, 106, 1–13. [CrossRef]
- Woelber, L.; Eulenburg, C.; Kosse, J.; Neuser, P.; Heiss, C.; Hantschmann, P.; Mallmann, P.; Tanner, B.; Pfisterer, J.; Jückstock, J.; et al. Predicting the course of disease in recurrent vulvar cancer – A subset analysis of the AGO-CaRE-1 study. Gynecol. Oncol. 2019, 154, 571–576. [CrossRef]
- Gaffney, D.K.; King, B.; Viswanathan, A.N.; Barkati, M.; Beriwal, S.; Eifel, P.; Erickson, B.; Fyles, A.; Goulart, J.; Harkenrider, M.; et al. Consensus Recommendations for Radiation Therapy Contouring and Treatment of Vulvar Carcinoma. Int. J. Radiat. Oncol. 2016, 95, 1191–1200. [CrossRef]
- Collarino, A.; Garganese, G.; Fragomeni, S.M.; Arias-Bouda, L.M.P.; Ieria, F.P.; Boellaard, R.; Rufini, V.; de Geus-Oei, L.-F.; Scambia, G.; Olmos, R.A.V.; et al. Radiomics in Vulvar Cancer: First Clinical Experience Using18F-FDG PET/CT Images. J. Nucl. Med. 2018, 60, 199–206. [CrossRef]
- Ger, R.B.; Wei, L.; El Naqa, I.; Wang, J. The Promise and Future of Radiomics for Personalized Radiotherapy Dosing and Adaptation. Semin. Radiat. Oncol. 2023, 33, 252–261. [CrossRef]
- Tanaka, S.; Kadoya, N.; Sugai, Y.; Umeda, M.; Ishizawa, M.; Katsuta, Y.; Ito, K.; Takeda, K.; Jingu, K. A deep learning-based radiomics approach to predict head and neck tumor regression for adaptive radiotherapy. Sci. Rep. 2022, 12, 1–13. [CrossRef]
- Abuhijla, F.; Salah, S.; Al-Hussaini, M.; Mohamed, I.; Jaradat, I.; Dayyat, A.; Almasri, H.; Allozi, A.; Arjan, A.; Almousa, A.; et al. Factors influencing the use of adaptive radiation therapy in vulvar carcinoma. Rep. Pr. Oncol. Radiother. 2020, 25, 709–713. [CrossRef]
- Gaffney DK, King B, Viswanathan AN, Barkati M, Beriwal S, Eifel P, et al. No Title. 2016 Jul 15 [cited 2025 Aug 8];95(4). Available from: https://pubmed.ncbi.nlm.nih.gov/27130794/.
- Oonk, M.H.; Planchamp, F.; Baldwin, P.; Mahner, S.; Mirza, M.R.; Fischerová, D.; Creutzberg, C.L.; Guillot, E.; Garganese, G.; Lax, S.; et al. European Society of Gynaecological Oncology Guidelines for the Management of Patients with Vulvar Cancer - Update 2023. Int. J. Gynecol. Cancer 2023, 33, 1023–1043. [CrossRef]
Figure 1.
Radiomics analysis workflow. Radiomic features were extracted from gross tumor volume (GTV) masks delineated on pre- and mid-radiotherapy CT simulation scans. Delta features (Δ features) were calculated and Z-normalized. Feature selection was performed sequentially using univariable Cox proportional hazards screening, correlation filtering, and Cox–LASSO regularization, to identify predictors of local control (LC), regional control (RC), distant metastasis–free survival (DMFS), progression-free survival (PFS), and overall survival (OS). Several features were retained for LC and OS prediction, with no features retained for RC, DMFS, or PFS. Final models were developed using multivariable Cox regression with Akaike Information Criterion (AIC)-based stepwise selection, and their performance was evaluated using 500-iteration bootstrap concordance index (C-index) estimation, calibration curves, and Kaplan–Meier survival analysis.
Figure 1.
Radiomics analysis workflow. Radiomic features were extracted from gross tumor volume (GTV) masks delineated on pre- and mid-radiotherapy CT simulation scans. Delta features (Δ features) were calculated and Z-normalized. Feature selection was performed sequentially using univariable Cox proportional hazards screening, correlation filtering, and Cox–LASSO regularization, to identify predictors of local control (LC), regional control (RC), distant metastasis–free survival (DMFS), progression-free survival (PFS), and overall survival (OS). Several features were retained for LC and OS prediction, with no features retained for RC, DMFS, or PFS. Final models were developed using multivariable Cox regression with Akaike Information Criterion (AIC)-based stepwise selection, and their performance was evaluated using 500-iteration bootstrap concordance index (C-index) estimation, calibration curves, and Kaplan–Meier survival analysis.
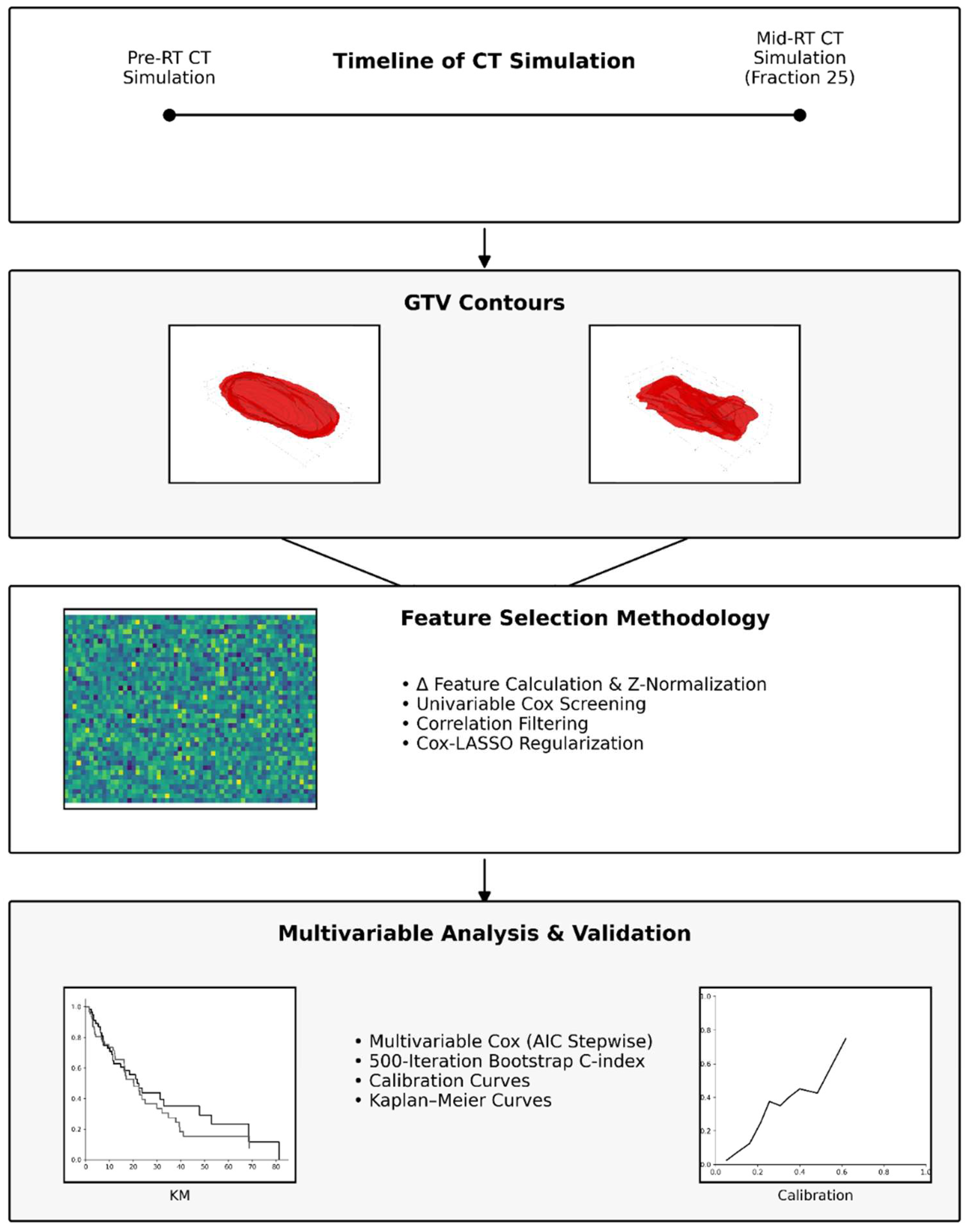
Figure 2.
Kaplan–Meier curves for local control (LC), regional control (RC), distant metastasis–free survival (DMFS), progression–free survival (PFS), and overall survival (OS) in the study cohort.
Figure 2.
Kaplan–Meier curves for local control (LC), regional control (RC), distant metastasis–free survival (DMFS), progression–free survival (PFS), and overall survival (OS) in the study cohort.
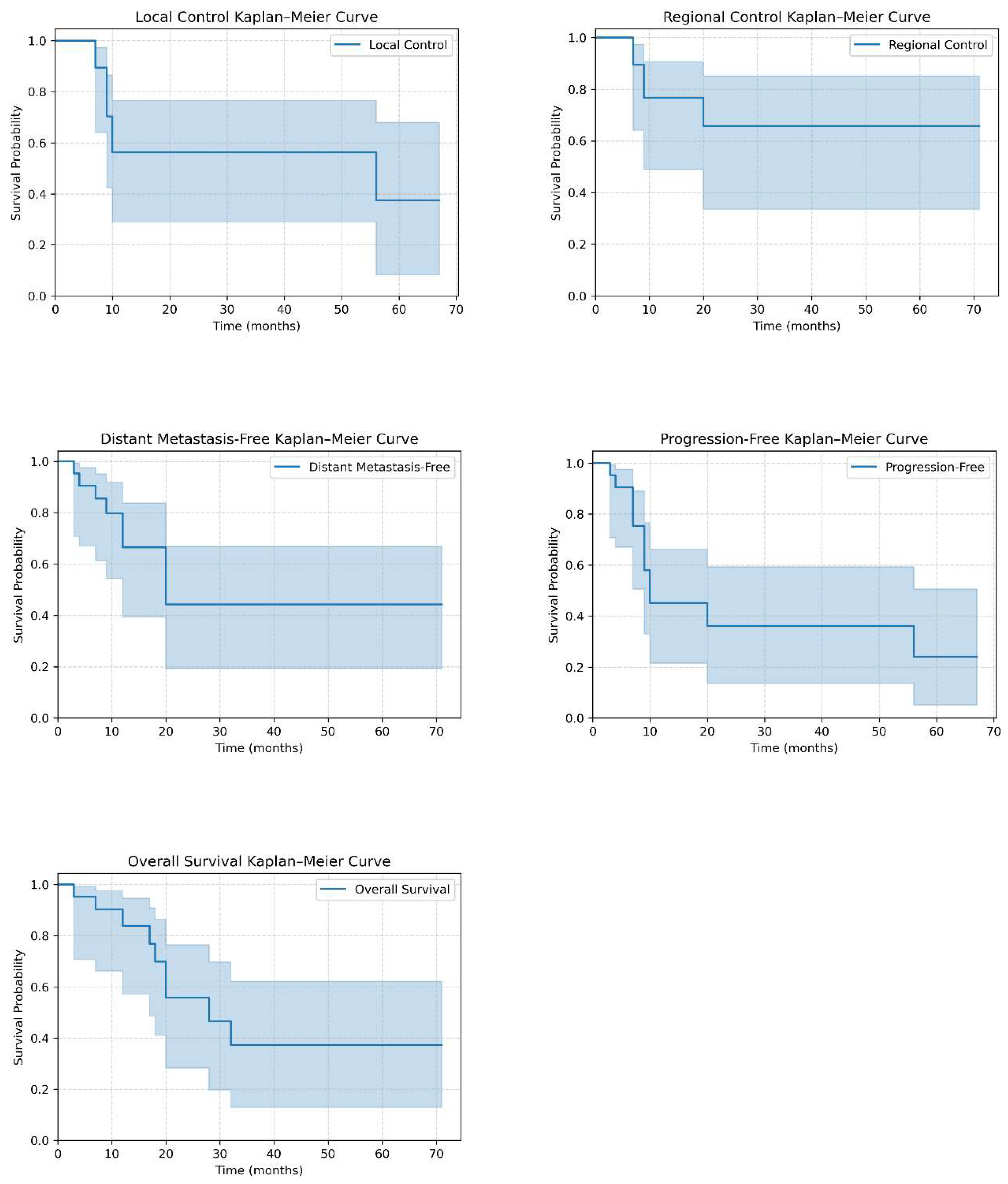
Figure 3.
Bootstrapped concordance index (C-index) for the final multivariable Cox models predicting local control (LC) and overall survival (OS). The LC model retained only ΔRLNU_norm (C-index = 0.751), while the OS model retained six Δ features (C-index = 0.896).
Figure 3.
Bootstrapped concordance index (C-index) for the final multivariable Cox models predicting local control (LC) and overall survival (OS). The LC model retained only ΔRLNU_norm (C-index = 0.751), while the OS model retained six Δ features (C-index = 0.896).
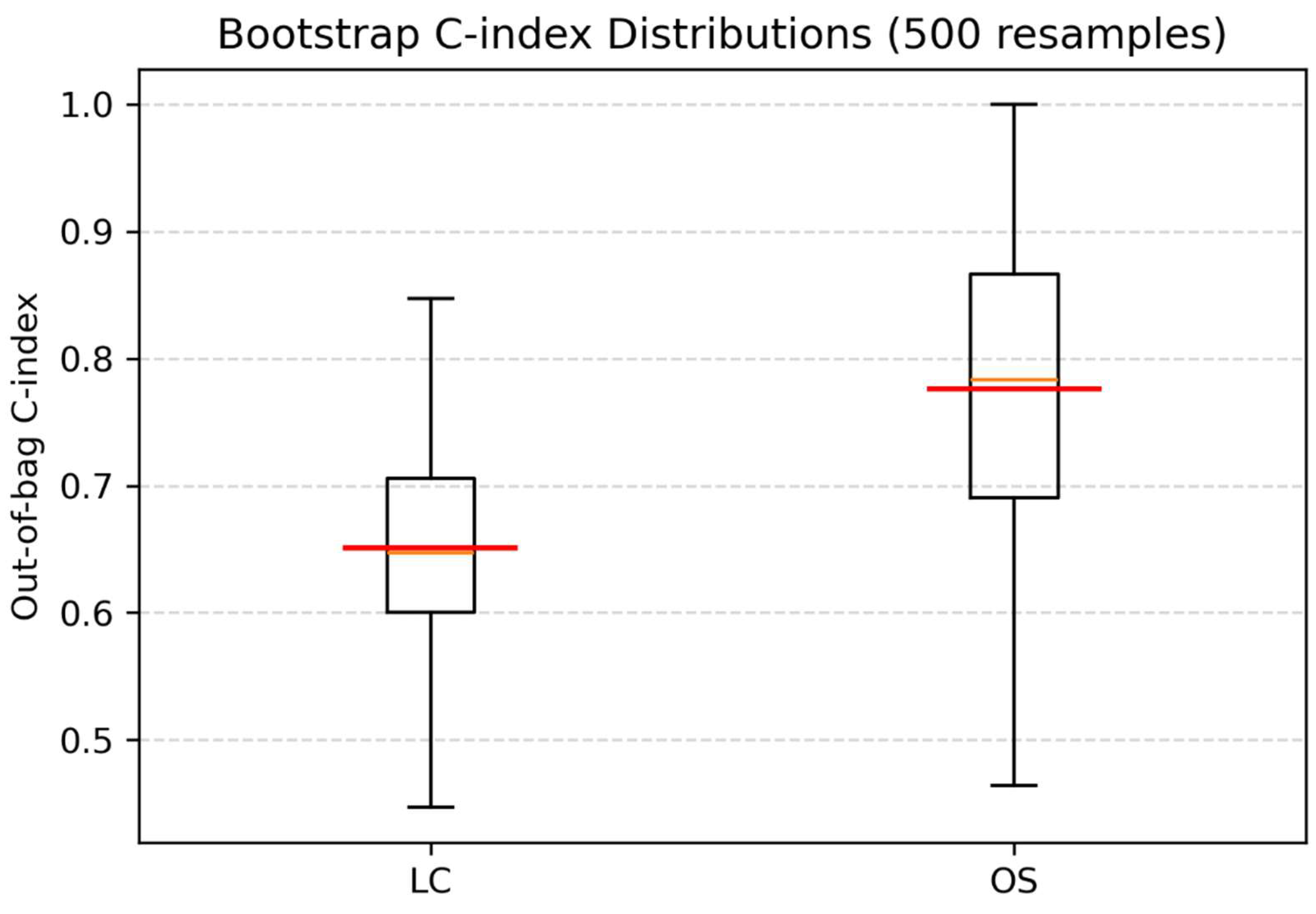

Table 1.
Patients and Disease Characteristics and Treatment Specifics (n = 21).
| Variable | Median | IQR | |||
| Age at diagnosis (years) | 57 | 17 | |||
| Total vulvar dose (Gy) | 65 | 2.6 | |||
| External-beam Radiotherapy dose in Gy | 45 | 5.4 | |||
| External-beam Radiotherapy number of fractions | 25 | 3 | |||
| Nodal dose (Gy) | 63 | 12 | |||
| EBRT Time (days) | 54 | 10 | |||
| Chemotherapy cycles | 5 | 1 | |||
| Variable | Category | Count | Percentage (%) | ||
| Grade | 1 | 1 | 4.8 | ||
| 2 | 15 | 71.4 | |||
| 3 | 4 | 19 | |||
| Missing | 1 | 4.8 | |||
| HPV Categories | Not associated | 12 | 57.1 | ||
| HPV-associated | 7 | 33.3 | |||
| Missing | 2 | 9.5 | |||
| FIGO Stage | II | 1 | 4.8 | ||
| IIIA | 1 | 4.8 | |||
| IIIB | 7 | 33.3 | |||
| IIIC | 1 | 4.8 | |||
| IVA | 2 | 9.5 | |||
| IVB | 6 | 28.6 | |||
| Missing | 3 | 14.3 | |||
| Concurrent Chemotherapy | Yes | 20 | 95.2 | ||
| No | 1 | 4.8 | |||
Table 2.
Treatment outcomes.
| Endpoint | Events (n) | Total (n) | Event rate (%) | Events ≤24 months (n) | ≤24 months (%) |
| Local Control | 8 | 21 | 38.1 | 7 | 87.5 |
| Regional Control | 5 | 21 | 23.8 | 5 | 100.0 |
| Distant Metastasis–Free | 9 | 21 | 42.9 | 9 | 100.0 |
| Progression–Free | 12 | 21 | 57.1 | 11 | 91.7 |
| Overall Survival | 9 | 21 | 42.9 | 7 | 77.8 |
Table 3.
Feature selection results for study endpoints.
| Endpoint | Selected Δ features |
| LC | GLCM Inverse Difference Moment (IDM) |
| GLRLM Run Length Non-Uniformity Normalized (RLNU_norm) | |
| GLRLM Run Percentage (RP) | |
| First-order Entropy | |
| GLCM Difference Entropy (DiffEnt) | |
| GLCM Cluster Prominence (ClusProm) | |
| RC | none retained |
| DMFS | none retained |
| PFS | none retained |
| OS | GLCM Difference Average (DiffAvg) |
| Shape Surface-Volume Ratio (SVR) | |
| GLCM Difference Variance (DiffVar) | |
| GLDM Large Dependence Low Gray-Level Emphasis (LDLGLE) | |
| GLSZM Size Zone Non-Uniformity (SZNU) | |
| GLSZM Gray-Level Non-Uniformity Normalized (GLNU_norm) | |
| GLSZM Zone Entropy (ZoneEnt) | |
| GLSZM Gray-Level Variance (GLVar) | |
| First-order Energy |
LC, Local Control; RC, Regional Control; DMFS, Distant Metastasis-Free Survival; PFS, Progression-Free Survival; OS, Overall Survival; GLCM, Gray-Level Co-occurrence Matrix; GLRLM, Gray-Level Run-Length Matrix; GLSZM, Gray-Level Size-Zone Matrix; GLDM, Gray-Level Dependence Matrix; First-order, features derived from the voxel intensity histogram without spatial context.
Table 4.
Multivariable Cox model with AIC-based bidirectional stepwise selection for LC and OS.
| Multivariable Cox model for LC (retaining one variable) | ||||
| Δ Feature | Coef | HR | 95% CI | p-value |
| GLRLM Run-Length Non-Uniformity Normalized (RLNU_norm) | 0.9625 | 2.618 | [1.05, 6.52] | 0.0388 |
| Multivariable Cox model for OS (time-varying) | ||||
| Feature | Coef | HR | 95% CI | p-value |
| GLCM Difference Average (DiffAvg) | –9.0097 | 0.00012 | [3×10−8, 0.48] | 0.0327 |
| Shape Surface-Volume Ratio (SVR) | 5.7666 | 319.45 | [1.74, 5.9×104] | 0.0302 |
| GLCM Difference Variance (DiffVar) | 5.7931 | 328.02 | [1.33, 8.1×104] | 0.0393 |
| GLDM Large Dependence Low Gray-Level Emphasis (LDLGLE) | –8.3732 | 0.00023 | [1×10−8, 5.28] | 0.1021 |
| GLSZM Gray-Level Non-Uniformity Normalized (GLNU_norm) | –9.2533 | 0.00010 | [3×10−8, 0.33] | 0.0259 |
| First-order Energy | –1.6158 | 0.1987 | [0.03, 1.22] | 0.0807 |
LC, Local Control; OS, Overall Survival; GLCM, Gray-Level Co-occurrence Matrix; GLRLM, Gray-Level Run-Length Matrix; GLSZM, Gray-Level Size-Zone Matrix; GLDM, Gray-Level Dependence Matrix; First-order, features derived from the voxel intensity histogram without spatial context.
Table 4.
Multivariable Cox model with AIC-based bidirectional stepwise selection for LC and OS.
| Multivariable Cox model for LC (retaining one variable) | ||||
| Δ Feature | Coef | HR | 95% CI | p-value |
| GLRLM Run-Length Non-Uniformity Normalized (RLNU_norm) | 0.9625 | 2.618 | [1.05, 6.52] | 0.0388 |
| Multivariable Cox model for OS (time-varying) | ||||
| Feature | Coef | HR | 95% CI | p-value |
| GLCM Difference Average (DiffAvg) | –9.0097 | 0.00012 | [3×10−8, 0.48] | 0.0327 |
| Shape Surface-Volume Ratio (SVR) | 5.7666 | 319.45 | [1.74, 5.9×104] | 0.0302 |
| GLCM Difference Variance (DiffVar) | 5.7931 | 328.02 | [1.33, 8.1×104] | 0.0393 |
| GLDM Large Dependence Low Gray-Level Emphasis (LDLGLE) | –8.3732 | 0.00023 | [1×10−8, 5.28] | 0.1021 |
| GLSZM Gray-Level Non-Uniformity Normalized (GLNU_norm) | –9.2533 | 0.00010 | [3×10−8, 0.33] | 0.0259 |
| First-order Energy | –1.6158 | 0.1987 | [0.03, 1.22] | 0.0807 |
LC, Local Control; OS, Overall Survival; GLCM, Gray-Level Co-occurrence Matrix; GLRLM, Gray-Level Run-Length Matrix; GLSZM, Gray-Level Size-Zone Matrix; GLDM, Gray-Level Dependence Matrix; First-order, features derived from the voxel intensity histogram without spatial context.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



