Submitted:
29 August 2025
Posted:
29 August 2025
You are already at the latest version
Abstract
Corticobasal syndrome (CBS) is an uncommon neurodegenerative syndrome, with a prevalence of only a few thousand patients in the U.S. Symptoms include alien hand syndrome, rigidity, myoclonus, weakness (often asymmetric), dysarthria, aphasia, dementia, and dysphagia, among others. There is no known cause or effective treatment for CBS. The underlying neuropathology associated with CBS includes corticobasal degeneration (CBD), Alzheimer’s disease, progressive supranuclear palsy, Creutzfeldt-Jakob disease, vascular disease, and frontotemporal lobar degeneration. Here we report a patient with CBS who had had exposure to burn pits, was found to harbor high levels of multiple toxins, and responded to a personalized, precision medicine protocol that included detoxification, hormone optimization, brain training, hyperbaric oxygen, and diet and lifestyle enhancement. Her symptoms abated, her MoCA score increased from 21/30 to 28/30, her electrophysiological studies normalized with marked improvement in quantitative EEG, and her MRI volumetrics improved. This case study suggests the possibility that more extensive toxin evaluations in patients with CBS may be revealing, and that personalized treatment directed at identified potential drivers such as organic toxins may offer the potential for symptom improvement in a disease for which no treatment has previously shown efficacy. The results also suggest the need for a proof-of-concept clinical trial for patients with CBS.
Keywords:
extrapyramidal
; neurotoxin
; precision medicine
; dementia
; neurodegeneration
; functional medicine
Introduction
Neurodegenerative diseases such as Alzheimer’s, ALS, Lewy body disease, frontotemporal dementia, progressive supranuclear palsy, and corticobasal degeneration are terminal illnesses in dire need of more efficacious treatments. Recent results in patients with Alzheimer’s disease, both anecdotal and clinical trial, offer hope that personalized, precision medicine approaches and more extensive evaluation testing may identify and address key drivers of the neurodegenerative process, leading to significant, sustained clinical improvement [1,2,3,4].
Corticobasal syndrome (CBS) is an uncommon neurodegenerative syndrome, with a prevalence of approximately one in 100,000 in the United States. As its name implies, symptoms reflect both cortical neuronal degeneration and basal ganglia involvement. Thus motor symptoms similar to those of Parkinson’s disease, such as rigidity, bradykinesia, weakness, postural instability, dysarthria, and tremor may occur, along with others such as dystonia; and cortical symptoms such as dementia, aphasia, alien hand syndrome, myoclonus, and apraxias. The onset of CBS is typically in the 50-70 year-old age range, and it is a progressive and terminal disease, with death occurring in six to eight years after diagnosis [5].
The neuropathology of CBS may reveal any of several different pathologies. Corticobasal degeneration [6] is the most common neuropathology in patients with CBS, and it is a four-repeat tauopathy that features pathognomonic astrocytic plaques, circumscribed cortical atrophy with spongiosis and ballooned neurons in a widespread distribution that includes cortical grey and white matter, basal ganglia, diencephalon, and rostral brainstem.
In patients with CBS without the neuropathology of corticobasal degeneration, other pathological entities such as Alzheimer’s disease, progressive supranuclear palsy, Creutzfeldt-Jakob disease, vascular disease, or frontotemporal lobar degeneration may be present.
The majority of cases of CBS are sporadic, but some are associated with mutations in tau. Other mutations associated with CBS, such as c9ORF72 and PRNP, are associated with alternative pathologies such as frontotemporal lobar degeneration or Creutzfeldt-Jakob disease.
The cause(s) of CBS is unknown, and to date no treatment has been shown to reverse the inexorable decline.
Here we describe a patient with CBS who suffered from a high burden of multiple toxicants, and responded to a personalized, precision medicine protocol that included detoxification, hormone optimization, hyperbaric oxygen, brain training, and diet and lifestyle enhancement. These findings suggest that more extensive toxin evaluations should be considered in patients with CBS, and that personalized treatment directed at the identified potential drivers of neurodegeneration such as organic toxins and/or mitochondrial toxins may offer the potential for symptom improvement in a disease for which no treatment has previously shown efficacy.
Case Description
A 59-year-old retired Marine presented with right upper extremity weakness and progressive memory loss.
She was deployed in the Iraq Gulf war in 1990, where she experienced exposure to oilfield fires. After those exposures she had persistent throat and nasal congestion as well as persistent migraines. She was deployed again in Iraq in 2000 where she had significant exposure to burn pits.
In 2013, she experienced a left-hand tremor and had an EMG done, which was read as negative. She had a total hysterectomy and bilateral salpingo-oophorectomy that year without hormone replacement. In 2015, she started to develop aphasia and word finding difficulty. She made changes to her diet in 2019 with the help of an integrative health coach, which led to elimination of her migraines and reduction in word-finding problems.
In 2022 she went to the Veterans Administration clinic for evaluation. Brain MRI showed generalized volume loss with greater focal right parietal loss than left. She had an amyloid PET scan that showed amyloid plaque in the temporal, parietal, and frontal regions. The differential diagnosis from the radiologist was corticobasal degeneration versus Alzheimer’s. She was told by the VA neurologist that she had corticobasal syndrome and that there were no effective treatments for her care. She commented that “the visit sent me into a deep depression.”
She presented to the author (CT) for evaluation in 2023. At that time, her neurological examination was notable for left upper extremity rigidity, tremors, myoclonus, and hyperreflexia. Her Montreal Cognitive Assessment (MoCA) score was 21/30. Her ApoE genotype was found to be 3/3. A NeuroQuant volumetric MRI showed significant right-sided atrophy, with parietal lobe volume at the 1st percentile, occipital lobe volume at the 1st percentile, and temporal lobe volume at the 5th percentile with sparing of the right hippocampus (72nd percentile). Laboratory evaluation revealed a homocysteine of 12.5 mcmol/L, and multiple elevated chemicals including glyphosate, 4-hydroxyanisole (4-HA), phenylglyoxylic acid (PGO), and monoethyl phthalate (MEP), which were all 3 to 4 times higher than the 95th percentile.
She was begun on a precision medicine protocol that included a plant-rich (6-9 cups of vegetables a day) mildly ketogenic diet, daily exercise, sleep hygiene, brain training, detoxification, and supplementation. Other treatments included bioidentical hormone replacement, Cytomel for low triiodothyronine, occupational and physical therapy, thiamine injections, and hyperbaric oxygen at 2.0 atmospheres for 60 sessions.
Detoxification consisted of the plant rich diet and sauna 3-4 times / week. In addition, she had foundational hepatic detoxification and drainage using the Pekana Naturheilmittel kit, which included Apo-hepat to promote liver and gallbladder function, Itires to enhance lymphatic drainage, and Renelix to support renal and urological excretion. Upon establishing tolerance, the protocol was expanded to include GI Detox (Biocidin Botanicals), a binder designed to sequester gastrointestinal toxins and support enterohepatic elimination, as well as Tri-Fortify oral glutathione (Researched Nutritionals) to enhance endogenous antioxidant capacity and phase II detoxification. By the third month, XenoProtX (Xymogen) and Phosphatidylcholine (BodyBio) were introduced to further support both phase I and phase II hepatic detoxification and to provide additional micronutrient and phospholipid support for hepatocyte membrane integrity and xenobiotic metabolism.
After 6 months of treatment her MOCA had improved to a 28/30, she reported improved awareness of her left hand, and whereas she had had no significant voluntary, coordinated left hand function on presentation, she improved to the point that she could stack quarters and pennies with her left hand.
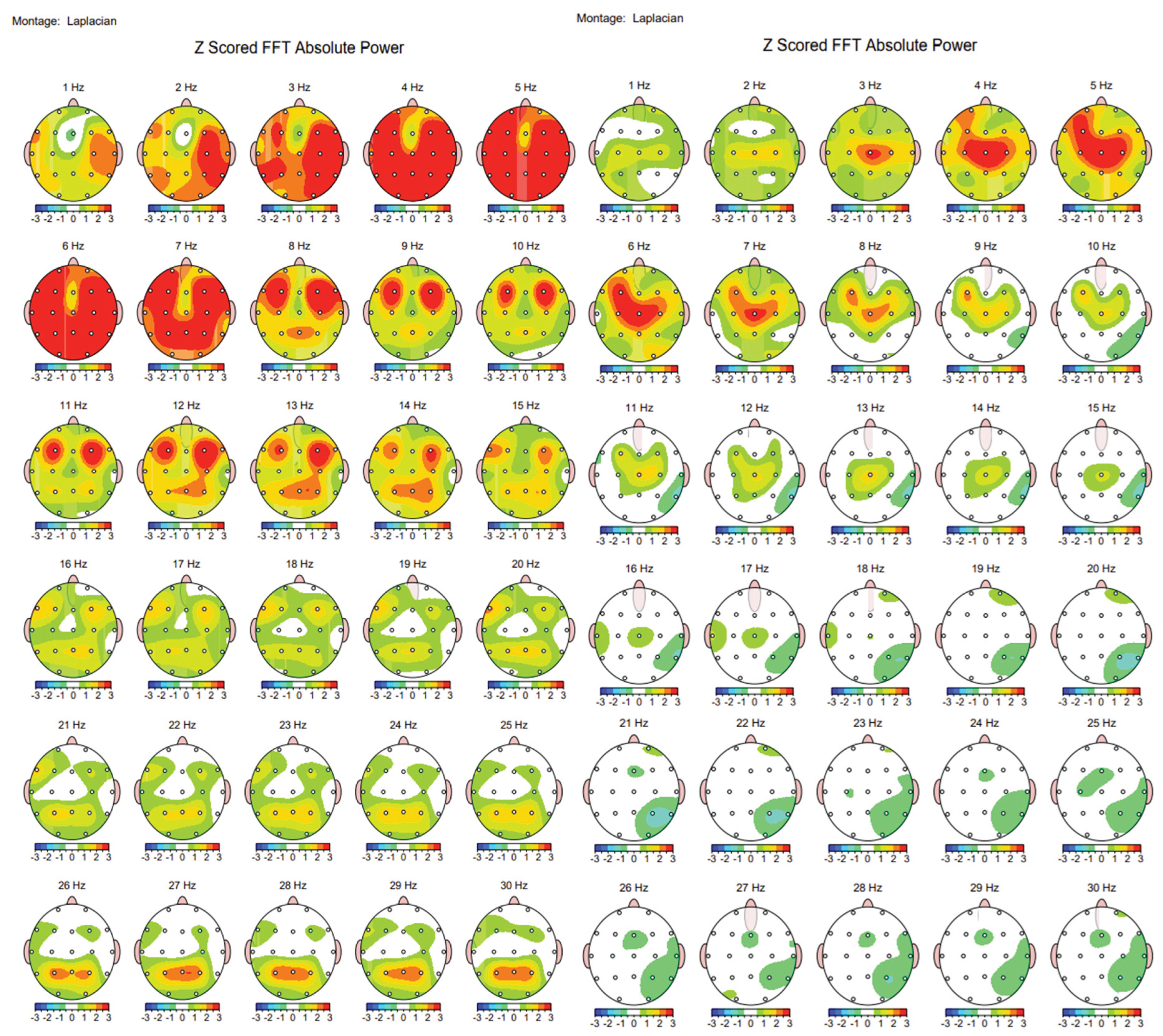
Electrophysiological studies also demonstrated marked improvement: quantitative EEG showed improvements at both 5 Hz and 7 Hz (Figure 1), with a nearly complete loss of abnormalities.
A follow-up NeuroQuant after 12 months of treatment showed the following changes from 12 months earlier: cortical grey matter 43rd percentile (up from 21st), cerebral white matter 52nd (down from 94th), temporal lobe 39th (29th), parietal lobe 3rd (2nd), Frontal lobe 93rd (68th), occipital lobe 6th (4th). There were more modest changes in the right sided regions: right temporal lobe 7th (5th), right parietal lobe 1st (1st), right occipital lobe 1st (1st), and right frontal lobe 78th (52nd) .
As of the end of 2024, she continues to do well.
Discussion
Neurodegenerative diseases have been terminal illnesses, in dire need of more efficacious therapeutics. However, the causes of these diseases have in most cases been elusive and attempts to treat the pathology—such as the use of anti-amyloid antibodies in Alzheimer’s disease —have not led to sustained improvements in symptoms.
The patient described here had symptoms that fit well with the diagnosis of CBS. Her positive amyloid PET scan demonstrated that she has Alzheimer’s disease, although it does not exclude the possibility that she may also have the neuropathology of corticobasal degeneration. Alzheimer’s disease neuropathology is the second most common pathology associated with CBS.
Determining the major mechanistic drivers of the degenerative process in each patient would represent a potentially impactful advance, and a key part of this determination is to demonstrate improvement in patients in whom these putative drivers are targeted. Documenting cases such as the one reported here should lead ultimately to the recognition of patterns that would then allow clinical trials.
The response of this patient, with improved symptoms, MoCA score, electrophysiology, and MRI volumetrics, suggests that at least some parameter(s) that was targeted played a role in the pathophysiological process.
One of the potential contributors to neurodegeneration in this patient is her borderline hyperhomocysteinemia; however, simply normalizing homocysteine has not been shown to exert the marked effects on cognition that were documented here. In contrast, the many toxicants associated with burn pits—particulates, polycyclic aromatic hydrocarbons, volatile organic compounds, dioxins, petroleum and lubricant products, plastics, rubber, wood, food waste, heavy metals, and others—have been linked to pulmonary toxicity, hepatic toxicity, renal toxicity, and cancers, among other effects. Is it possible that this patient’s burn pit exposure contributed to her CBS?
Although the many chemicals assessed during the patient’s evaluation may not have included the key toxicants driving the patient’s neurodegeneration, the chemicals that were identified as being 3-4-fold more than the 95th percentile level included glyphosate, 4-hydroxyanisole (4-HA), phenylglyoxylic acid (PGO), and monoethyl phthalate (MEP).
Glyphosate is an herbicide and antibiotic, a synthetic amino acid derivative that blocks the shikimate pathway in plants and has the potential to alter the gut microbiome [7]. It has been implicated in autism spectrum disorder and Parkinson’s disease, among other disease states [8]. CBS is considered a “Parkinson’s plus” syndrome, which raises the question of whether the high level of glyphosate in this patient may have contributed to the neurodegenerative process.
4-hydroxyanisole is a preservative, but it may be converted into a toxic oxidant in the presence of tyrosinase, which is present in melanocytes and at low levels in cells that produce neuromelanin, such as dopaminergic neurons [9].
Phenylglyoxylic acid is a toxic metabolite of styrene [10], and exposure may occur through exposure to styrofoam or plastics. Effects of phenylglyoxylic acid include reductions in serotonin and norepinephrine, while the effects on dopamine include increases in the cerebellum, hippocampus, pons, and in the brain as a whole.
Monoethyl phthalate exposure may occur from exposure to plastics, insect repellants, or rocket propellant. MEP is an endocrine disruptive toxin that may also affect fetal development and create respiratory irritation. MEP may exert neurotoxicity, reducing acetylcholine, compromising the blood-brain barrier, and creating inflammation [11].
The role that each of these toxins may have played in the patient’s CBS is unknown, but given the positive response to a protocol that included detoxification, and the extensive evidence that some toxicants are associated with neurodegeneration (e.g., paraquat, trichloroethylene, and methylphenyltetrahydropyridine, among many others), it is possible that any or all of the toxicants to which this patient was exposed played a role in her development of CBS.
In an effort to improve outcomes for patients with CBS, it may be helpful to extend evaluations to include organic toxicants such as those identified here, and to include as a therapeutic option a personalized, precision medicine protocol that is targeted to the identified potential contributors. As data accumulate, emerging patterns of exposures and other potential contributors may point the way to a clinical trial centered on the likely contributors to CBS in each patient.
Acknowledgment
We are grateful to Paul Conrady and Hyperbarics for Heros (hyperbaricsforheros.org) that provided HBOT therapy to our patient free of charge in acknowledgement of her service to her country. This organization has provided these services for multiple veterans, setting a fine example that should be followed.
References
- Bredesen, D.E.; Sharlin, K.; Jenkins, D.; Okuno, M.; Youngberg, W.; Cohen, S.H.; Stefanko, A.; Brown, R.L.; Chung, H.; Chwa, W.J.; Jarrett, M.; Hathaway, A.; Toups, K.; Wilkinson, J.; Mellington, M.; Henneberg, A. Reversal of cognitive decline: 100 patients. Journal of Alzheimer's Disease & Parkinsonism 2018, 8, 450. [Google Scholar] [CrossRef]
- Toups, K.; Hathaway, A.; Gordon, D.; Chung, H.; Raji, C.; Boyd, A.; Hill, B.D.; Hausman-Cohen, S.; Attarha, M.; Chwa, W.J.; Jarrett, M.; Bredesen, D.E. Precision medicine approach to Alzheimer's disease: Successful pilot project. Journal of Alzheimer's Disease 2022, 88, 1411–1421. [Google Scholar] [CrossRef] [PubMed]
- Sandison, H.; Callan, N.G.L.; Rao, R.V.; Phipps, J.; Bradley, R. Observed improvement in cognition during a personalized lifestyle intervention in people with cognitive decline. Journal of Alzheimer's Disease 2023, 94, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Bredesen, D.E.; Ross, M.K.; Ross, S. Sustained cognitive improvement in Alzheimer's disease patients following a precision medicine protocol: Case series. Biomedicines 2024, 12, 1776. [Google Scholar] [CrossRef] [PubMed]
- Mayo Clinic Staff. (2023, December 22). Corticobasal degeneration (corticobasal syndrome) - Symptoms and causes. Mayo Clinic. Retrieved from https://www.mayoclinic.org/diseases-conditions/corticobasal-degeneration/symptoms-causes/syc-20354767.
- Kouri, N.; Whitwell, J.L.; Josephs, K.A.; Rademakers, R.; Dickson, D.W. Corticobasal degeneration: a pathologically distinct 4R tauopathy. Nature Reviews Neurology 2011, 7, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Walsh, L.; Hill, C.; Ross, R.P. Impact of glyphosate (Roundup™) on the composition and functionality of the gut microbiome. Gut Microbes 2023, 15, 2263935. [Google Scholar] [CrossRef] [PubMed]
- Caballero, M.; Amiri, S.; Denney, J.T.; Monsivais, P.; Hystad, P.; Amram, O. Estimated residential exposure to agricultural chemicals and premature mortality by Parkinson's disease in Washington State. International Journal of Environmental Research and Public Health 2018, 15, 2885. [Google Scholar] [CrossRef] [PubMed]
- Swanson, J.F.; Kunkle, G.A.; Stepien, R.L. Cytotoxicity of 4-hydroxyanisole and tyrosinase activity in variant cell lines of B16 melanoma. Pigment Cell Research 1989, 2, 525–530. [Google Scholar] [CrossRef]
- Terre'Blanche, G.; Heyer, N.; Bergh, J.J.; Mienie, L.J.; van der Schyf, C.J.; Harvey, B.H. The styrene metabolite, phenylglyoxylic acid, induces striatal-motor toxicity in the rat: influence of dose escalation/reduction over time. Neurotoxicity Research 2011, 20, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Huo, W.-B.; Deng, J.-Y.; Tang, Q.-P.; Wang, J.-X.; Liao, Y.-L.; Gou, D.; Pei, D.-S. Neurotoxicity and the potential molecular mechanisms of mono-2-ethylhexyl phthalic acid (MEHP) in zebrafish. Ecotoxicology and Environmental Safety 2023, 265, 115516. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
QEEG Laplacian at baseline 2022 and 12 months later.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



