Submitted:
28 August 2025
Posted:
29 August 2025
You are already at the latest version
Abstract
Background: Preterm birth (PTB) is a major cause of neonatal morbidity and mortality worldwide. Inflammatory cytokines, especially IL-6, play a pivotal role in PTB pathogene-sis. Lactoferrin (LF), an iron-binding glycoprotein, possesses antimicrobial and immuno-modulatory properties that may reduce PTB risk. This narrative review aims to synthesize evidence on LF supplementation effects on inflammation, cytokine modulation, biochem-ical markers, and obstetric outcomes linked to PTB. Methods: Eight clinical studies from Italy involving 728 pregnant women at risk of PTB were analyzed. LF was administered orally, vaginally, or both, with varying dosages and durations. Outcomes included in-flammatory markers (IL-6, prostaglandins), cervical and uterine parameters, oxidative stress biomarkers, and clinical endpoints such as PTB rates and neonatal intensive care unit (NICU) admissions. Results: LF supplementation consistently reduced cervi-co-vaginal and serum IL-6 levels (e.g., p ≤ 0.005), decreased prostaglandin concentrations (p < 0.01), and improved cervical length (p < 0.0001) while lowering uterine contraction frequency (p = 0.05). Oxidative stress markers significantly improved (p < 0.0001). Clini-cally, LF-treated groups exhibited reduced PTB incidence (25.0% vs 44.6%; p = 0.02), high-er gestational age at delivery (37.7 ± 3.2 vs 35.9 ± 4.1 weeks; p = 0.01), and fewer NICU ad-missions (8.3% vs 21.5%; p = 0.05). Immunological profiles indicated decreased pro-inflammatory cytokines and increased immune-regulatory factors in amniotic fluid.
Conclusions: LF demonstrates a multifaceted immunomodulatory effect that mitigates in-flammation and improves obstetric and neonatal outcomes associated with PTB risk. These findings support LF’s potential as a preventive intervention against PTB, high-lighting the need for further large-scale randomized trials.
Keywords:
lactoferrin
; preterm birth
; inflammation
; cytokines
; pregnancy outcomes
1. Introduction
Preterm birth is defined by the World Health Organization (WHO) as all births occurring before 37 completed weeks of gestation or fewer than 259 days since the first day of a woman’s last menstrual period [1] . The estimated global prevalence of preterm birth in 2020 was 9.9%, corresponding to approximately 13.4 million live preterm births [2]. Of the 5.3 million deaths in children under five years worldwide recorded in 2019, 17.7% approximately 0.94 million were attributed to complications of preterm birth, making it the leading cause of child mortality globally [3]. Although numerous socio-demographic, nutritional, medical, obstetric, and environmental factors have been associated with an increased risk of spontaneous preterm birth, its etiology remains only partially understood [4]. Inflammatory cytokines are considered key mediators in the pathogenesis of preterm birth, with infections frequently ascending through the uterine cervix. Preterm labor and delivery have been linked to elevated levels of IL-6, IL-8, and IL-10 in the amniotic fluid. In particular, a marked increase in IL-6 concentration appears to represent a significant marker of intrauterine infection that triggers preterm delivery [5]. Moreover, in over 30% of cases, preterm premature rupture of membranes (PROM) and subsequent preterm delivery are associated with bacterial infection of the amniotic fluid (amnionitis) and elevated concentrations of inflammatory cytokines such as IL-6 and IL-8 [6]. The risk of preterm birth has also been shown to correlate positively with increased levels of hsCRP, IL-10, IL-6, TNF-α, total cholesterol, triglycerides, and HDL (all P<0.05) [7]. Notably, elevated IL-6 concentrations in amniotic fluid have been associated with intra-amniotic inflammation even in the absence of overt clinical signs, highlighting the need for more accurate diagnostic and therapeutic strategies [8]. Lactoferrin (LF) is an approximately 80 kDa glycoprotein found in human milk, where it constitutes 10–15% of total protein content, and in various mucosal secretions such as saliva and intestinal fluids [9] . It has demonstrated significant potential in mitigating oxidative stress across multiple biological systems [10,11]. Specifically, lactoferrin has been shown to attenuate the pro-inflammatory response of neonatal monocyte-derived macrophages. Treatment with human lactoferrin on LPS-activated neonatal macrophages, isolated from heparinized cord and peripheral blood, resulted in a reduced production of cytokines including TNF, IL-1β, IL-6, IL-8, and IL-10. Furthermore, lactoferrin decreased the expression of activation markers and phagocytic capacity in these macrophages. Taken together, lactoferrin may represent a promising candidate for improving adverse pregnancy outcomes not only due to its antimicrobial properties but also through its ability to modulate immune cell function and reduce inflammation [12]. In addition, lactoferrin supplementation has been studied in various clinical and physiological contexts for its ability to modulate systemic inflammation and support immune function. Clinical studies involving diverse populations—including healthy individuals, patients with type 2 diabetes, and pregnant women with iron deficiency anemia (IDA)—have shown significant reductions in IL-6 and TNF-α levels following lactoferrin supplementation [13]. Although two systematic reviews have examined the clinical efficacy of lactoferrin in the prevention of preterm birth [14], these works addressed the topic within a broader scope, including various domains such as iron metabolism regulation in IDA, antimicrobial and immunomodulatory properties, and obstetric outcomes in at-risk populations—namely, preterm birth incidence and neonatal intensive care unit admission. However, to date, there is no narrative synthesis specifically addressing the role of lactoferrin in modulating inflammatory mechanisms associated with the risk of preterm birth.
The purpose of this narrative review is to summarize the available literature on the potential effects of lactoferrin supplementation on inflammation regulation, cytokine profile modulation, and other biochemical markers and clinical obstetric outcomes associated with the risk of preterm birth.
2. Materials and Methods
This article was conceived as a structured narrative review aimed at synthesizing and critically evaluating the current literature on the role of lactoferrin in modulating inflammatory mechanisms associated with preterm birth risk. Although not a strict systematic review, the methodology adhered to rigorous principles inspired by PRISMA guidelines to enhance clarity, transparency, and reproducibility.
2.1. Search Strategy
The literature search was conducted across three main electronic databases: PubMed, Embase, and Web of Science, with no restrictions on publication date, covering all available studies up to the date of the search. Eligible studies were required to investigate the effect of lactoferrin administration either bovine or recombinant human on inflammatory markers, oxidative stress, or obstetric outcomes in pregnant women at risk of preterm birth, including those undergoing mid-trimester genetic amniocentesis. The search was restricted to articles published in English or Italian in peer-reviewed journals. In collaboration with an expert librarian, a comprehensive search strategy was developed using a combination of free-text terms and Medical Subject Headings (MeSH), including: “lactoferrin,” “preterm birth,” “preterm delivery,” “inflammation,” “cytokines,” “oxidative stress”. Additionally, the reference lists of relevant reviews and included studies were manually screened to identify further eligible publications.
2.2. Inclusion Criteria
Based on the Population–Intervention–Comparison–Outcome (PICO) framework, the inclusion criteria were defined as follows: i) pregnant women at risk of preterm birth, including those undergoing mid-trimester genetic amniocentesis. Inflammatory profiles detected at the time of amniocentesis have been shown to independently predict adverse outcomes such as preterm premature rupture of membranes [15]. ii) Intervention: the administration of lactoferrin, either bovine (bLf) or recombinant human lactoferrin (rhLf), through oral or vaginal means as a preventive or therapeutic approach to modulate inflammatory processes during pregnancy. iii) Comparison: studies including control groups with no treatment, placebo, or alternative treatments. iv). Outcomes: the modulation of inflammatory markers (e.g., IL-6, TNF-α, PGE2), oxidative stress biomarkers, biochemical indicators in amniotic fluid or cervicovaginal secretions; obstetric parameters such as cervical length, preterm birth rates, gestational age at delivery, and neonatal outcomes (e.g., NICU admission, birth weight).
2.3. Exclusion Criteria
The exclusion criteria for this review were as follows: i) studies not involving pregnant women at risk of preterm birth, such as studies on non-pregnant populations, postpartum women, or experimental laboratory models (in vitro or animal studies); ii) studies assessing substances or interventions other than lactoferrin, or studies in which lactoferrin was administered in combination with other investigational treatments, making it impossible to isolate its effects; iii) articles not providing original research data, including case report, review articles, meta-analyses, editorials, commentaries, and conference abstracts.
2.4. Study Selection and Data Extraction
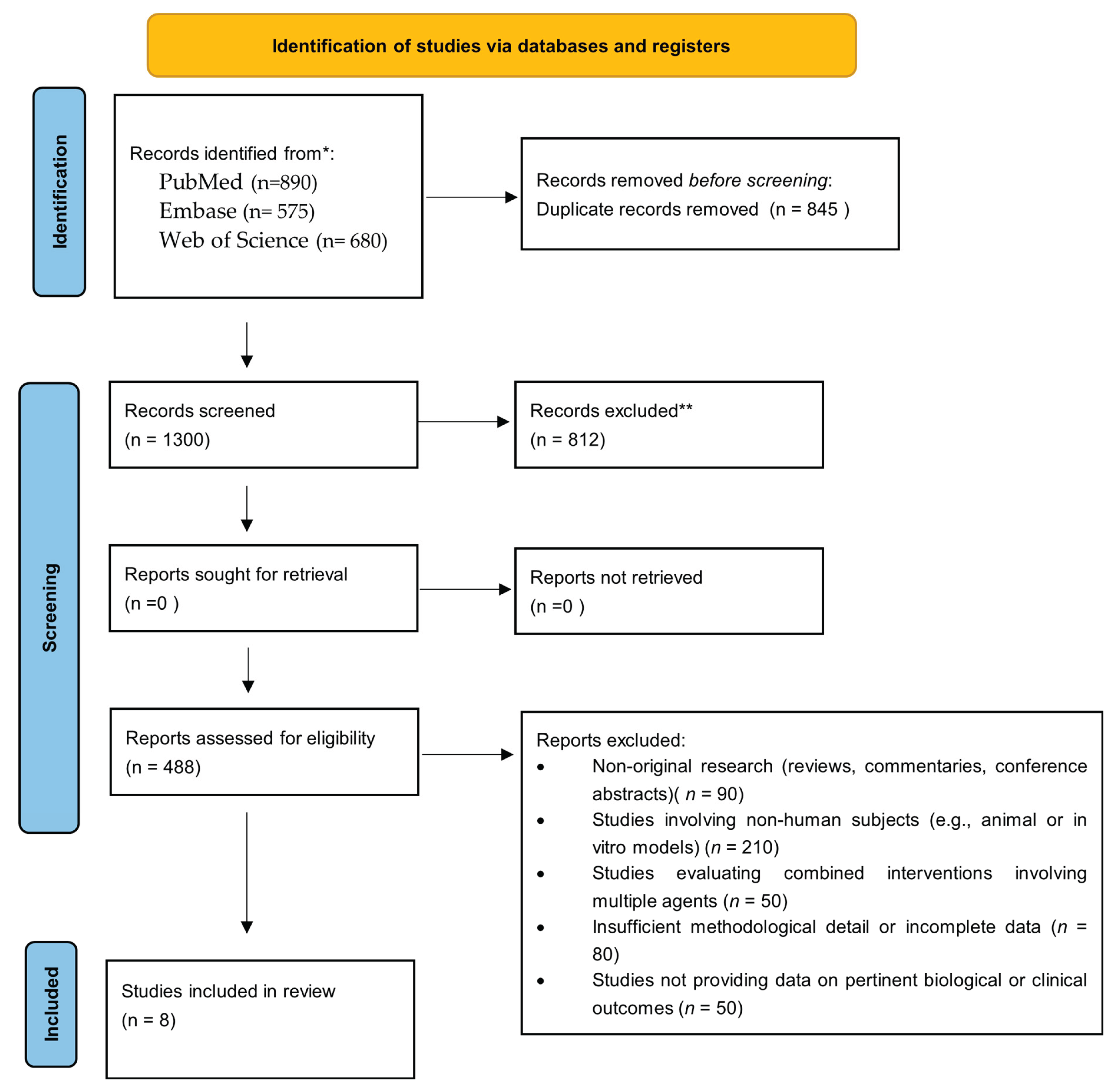
A total of 2140 records were identified through database searches (PubMed, Embase, Web of Science). After removing duplicates, 1300 abstracts were screened for eligibility by two independent reviewers (S.E.M. and A.M.) using the Rayyan platform. Studies were excluded mainly due to non-original research, irrelevant populations or interventions, and combined treatments preventing isolation of lactoferrin’s effects. Full-text articles were then assessed for eligibility, with discrepancies resolved by discussion referring to predefined inclusion criteria. Consequently, 8 articles met the inclusion criteria and were included in the final qualitative synthesis. The PRISMA-inspired flow diagram of study selection is shown in Figure 1.
3. Results
This review summarizes data from eight clinical studies conducted in Italy, including a total of 728 pregnant women (see Table 1, Supplementary Material). The studies used different formulations of lactoferrin, including recombinant human lactoferrin (rhLf; e.g., Lattoferrina® by AG-pharma) and bovine lactoferrin (bLf; e.g., Lattoglobina® by Grunenthal and Difesan® by Progine Farmaceutici). Lactoferrin was administered orally (one study), vaginally (six studies), or via a combination of oral and vaginal routes (one study). The clinical outcomes examined cover multiple pathophysiological and clinical aspects related to the risk of preterm birth. For clarity, the findings are organized into five main thematic areas: (3.1) inflammatory markers, (3.2) cervical and uterine parameters, (3.3) biochemical biomarkers and oxidative stress, (3.4) obstetric and neonatal clinical outcomes, and (3.5) immunological profile of the amniotic fluid.
3.1. Inflammatory Markers
Several studies have consistently reported a significant reduction in IL-6 levels following lactoferrin administration. Giunta et al. [16] observed a marked decrease in cervico-vaginal IL-6 after 10 days of oral recombinant human lactoferrin (rhLf) treatment (1,834 ± 0.4 pg/mL vs. 3,466 ± 1.8 pg/mL; p = 0.005), an effect that was notably maintained at 30 days (p = 0.05). Similarly, Paesano et al.[17] confirmed a significant reduction in both serum IL-6 at delivery (p = 0.0001) and cervico-vaginal IL-6 after 4 weeks (p = 0.0001) in women treated with a combination of oral and vaginal bovine lactoferrin (bLf). In alignment with these findings, Locci et al. (2013) reported a substantial decrease in cervico-vaginal IL-6 levels in women treated with vaginal bLf for 21 days (5.823 pg/mg vs. 80.82 pg/mg; p < 0.0001). Vesce et al. [18] documented a significant reduction in amniotic IL-6 in patients who received lactoferrin 4 hours prior to amniocentesis (242.3 ± 163.5 pg/mL vs. 1,084.1 ± 1,458.3 pg/mL; p = 0.03). With regard to prostaglandins, Paesano et al. (2012) reported a significant decrease in cervico-vaginal PGF2α levels (p = 0.0001), whereas Trentini et al. [19] found notably lower PGE2 concentrations in the treatment group (3.8 vs. 5.3 pg/mg creatinine; p < 0.01).
3.2. Cervical and Uterine Parameters
Several studies have evaluated both morphological and functional parameters, including cervical length, uterine contraction frequency, and alterations in vaginal flora (AVF). Locci et al. [20] reported a significant increase in cervical length after 21 days of vaginal bLf treatment (37.6 mm [34.8–43.0] vs. 21.38 mm [20.0–23.5]; p < 0.0001), along with a corresponding reduction in the frequency of uterine contractions (>6 every 30 minutes: 9% vs. 20.3%; p = 0.05). An inverse correlation between IL-6 levels and cervical length was consistently identified in both groups (treated and control), with a correlation coefficient of r = –0.81 in the lactoferrin group (p < 0.0001). Giunta et al. [16] additionally reported a significant reduction in the prevalence of AVF in the rhLf-treated group (from 71% to 15% over 30 days; p = 0.0007), while no significant differences were observed in the incidence of funneling, which was absent in both groups.
3.3. Biochemical Biomarkers and Oxidative Stress
Trentini et al. [19] assessed the amniotic expression of matrix metalloproteinases (MMPs) and their inhibitors, observing a significant reduction in MMP-9 (p < 0.005) and TIMP-1 (p < 0.001), alongside a marked increase in MMP-2 (p < 0.0001). Consequently, the MMP-2/TIMP-2 ratio significantly increased in the vaginal bLf-treated group (p < 0.0001). Subsequently, Trentini et al. [21] investigated oxidative stress markers, demonstrating a significant reduction in TBARS levels (p < 0.0001 at 4 hours; p < 0.05 at 12 hours), a marked decrease in the oxidative stress index (OSI; p < 0.0001), and a 35% increase in total antioxidant capacity (TAS) compared to controls (p < 0.0001).
3.4. Obstetric and Neonatal Clinical Outcomes
Giunta et al. [16] reported that all patients in both the rhLf and control (ferrous sulfate) groups successfully delivered beyond 37 weeks of gestation. Complementing these findings, Miranda et al. [22] observed a significantly lower rate of preterm birth (<37 weeks) in women treated with vaginal bLf (25.0%) compared to controls (44.6%; p = 0.02). Moreover, the mean gestational age was significantly higher in the treatment group (37.7 ± 3.2 vs. 35.9 ± 4.1 weeks; p = 0.01), and there was a notable reduction in hospitalizations due to threatened preterm labor (45.0% vs. 70.8%; p = 0.04) as well as a lower rate of neonatal intensive care unit (NICU) admissions (8.3% vs. 21.5%; p = 0.05). No significant differences were found regarding chorioamnionitis, preterm premature rupture of membranes (PPROM) before 34 weeks, or neonatal birthweight.
3.5. Amniotic Immunological Profile
The study by Maritati et al. [23] investigated the impact of vaginal bLf administration on the cytokine profile of amniotic fluid. Significant reductions in various pro-inflammatory cytokines were observed, including IL-9, TNF-α, IP-10, IFN-γ, IL-1α, IL-15, and MCP-3 (p < 0.05–0.001). Conversely, there were significant increases in cytokines and growth factors associated with immune regulation and tissue repair, such as IL-17, FGF-basic, GM-CSF, G-CSF, MCP-1, and SDF-1α (p < 0.001). These findings strongly suggest an immunomodulatory effect of lactoferrin at the amniotic level, which may confer protection against intrauterine inflammation.
4. Discussion
This narrative review has highlighted consistent evidence supporting the use of lactoferrin (LF), in both its bovine (bLF) and recombinant human (rhLF) forms, as an immunomodulatory, anti-inflammatory, and antimicrobial molecule in the prevention of adverse obstetric outcomes particularly preterm birth and preterm premature rupture of membranes (PPROM). The data analyzed are consistent with the known pathophysiological mechanisms underlying inflammation-mediated preterm labor. It is well established that infection/inflammation-associated PPROM is initiated by the upregulation of pro-inflammatory cytokines, which in turn modulate the expression of matrix metalloproteinases (MMPs) in amniochorionic cells [24,25,26,27]. In this regard, intra-amniotic infection or inflammation detected at the time of amniocentesis has been shown to be significantly and independently associated with subsequent PPROM in women with intact membranes and preterm labor [28]. This supports the inclusion of studies involving women undergoing amniocentesis in the present review, as these cohorts provide a direct window into inflammatory mechanisms that precede and predict adverse obstetric outcomes. At the fetal level, systemic cytokine responses—characterized by elevated plasma IL-6 levels >11 pg/mL have been associated with imminent onset of spontaneous labor in patients with PPROM [29]. This provides robust evidence for the active role of pro-inflammatory cytokines in triggering preterm birth, as demonstrated by the elevation of fetal IL-6 preceding (rather than following) the clinical onset of labor [6]. These observations align with the findings of our studies, which reported a significant reduction in IL-6 levels at the serum, amniotic, and cervico-vaginal levels following LF administration, suggesting a potential early interruption of the inflammatory cascade. Furthermore, LF-induced cytokine modulation has also been documented at the amniotic level, where significant decreases in TNF-α, IFN-γ, IL-1α, and MCP-3 were observed, alongside increases in anti-inflammatory and growth-promoting mediators such as IL-17, GM-CSF, and SDF-1α [23]. These findings suggest a rebalancing effect on the intrauterine immune microenvironment. In parallel, LF appears to exert a favorable influence on the downstream proteolytic cascade of inflammation by modulating the expression and activity of MMPs key enzymes involved in collagen degradation and the progressive weakening of the amniochorionic membranes. Specifically, MMP-9 levels and MMP-9:TIMP ratios have been shown to be significantly higher in preterm births compared to term pregnancies (P < 0.001), while TIMP-1 and TIMP-2 levels were significantly lower (P = 0.002 and P < 0.001, respectively), with mean reductions of 11% for TIMP-1 and 22% for TIMP-2 [30]. Additionally, comparisons of placental mRNA expression levels of MMP-1, -2, and -9 between term and preterm labor revealed significantly elevated expression in the latter group, indicating a molecular environment more conducive to premature membrane rupture [31]. Consistently, Trentini et al. [19] reported a significant reduction in MMP-9 levels following intravaginal administration of bLF, along with selective regulation of other relevant enzymes and inhibitors. Beyond its anti-inflammatory and anti-proteolytic effects, lactoferrin has also been associated with improvements in cervical and uterine parameters, indirectly contributing to pregnancy stabilization [17]. Notably, bLF administration has been shown to significantly increase cervical length, reduce uterine contraction frequency, and produce an inverse correlation between IL-6 levels and cervical length [20] all factors supporting LF’s potential utility in mitigating the risk of preterm labor. Oxidative stress, often elevated in inflammatory pregnancy conditions, also appears to improve in response to LF. Trentini et al. [21] reported reductions in TBARS, an increase in total antioxidant capacity (TAS), and a decrease in the oxidative stress index (OSI) following intravaginal bLF administration. Similar findings were observed by Rascon-Cruz et al. [32], who identified LF as a promising systemic antioxidant agent for conditions characterized by oxidative stress, including cardiovascular, neurodegenerative, and oncological disorders. In particular, LF significantly reduced plasma hydrogen peroxide levels in dexamethasone-induced hypertensive animal models when administered at a dose of 400 mg/kg/day, while preserving cellular viability and function. Clinically, these effects translate into lower rates of preterm birth, increased gestational age at delivery, reduced hospital admissions for preterm labor, and fewer neonatal intensive care unit (NICU) admissions [16,22]. Moreover, a comparative study by Pino et al.[33] provided valuable insights into the dose–response relationship of vaginal lactoferrin in the treatment of bacterial vaginosis a condition associated with chronic inflammation and increased risk of preterm birth. Women treated with 200 mg/day for 10 days experienced more marked and sustained improvements in vaginal microbiota than those receiving 100 mg/day. In the 200 mg group, 92.8% achieved a Nugent score <7 at treatment completion, and 85.7% achieved a score ≤3 (indicative of normal flora), with stability maintained even two weeks after discontinuation. These findings support a dose-dependent effect of LF in restoring vaginal eubiosis, suggesting that the 200 mg/day dosage may be preferable in clinical settings requiring a stronger antimicrobial and immunomodulatory response [34]. Consistently, Otsuki et al. [35] observed that rhLF’s antibacterial and anti-cytokine effects occur primarily in mucus producing cervical epithelial cells, which may play a key role in facilitating LF’s adherence to bacteria and limiting their proliferation. Under these conditions, LF inhibited E. coli growth, LPS-induced cytokine production, and macrophage activation likely via enhanced NO production rather than a simple opsonization effect. Systemic administration data are also promising. A four-month follow-up of pregnant women revealed that daily oral LF at a dose of 100 mg twice daily significantly reduced the incidence of asymptomatic bacteriuria (7.5% vs. 30.1%; p < 0.00001) and acute cystitis (0.9% vs. 9.6%; p < 0.00001), while increasing the proportion of negative urine cultures (47% vs. 15.1%; p < 0.00001), thereby confirming LF’s efficacy as a multifactorial preventive strategy. Furthermore, it is important to note that no meta-analysis was performed in this review because of the substantial heterogeneity in study designs, populations, lactoferrin formulations, dosages, and clinical endpoints, which precluded quantitative synthesis. Finally, timing of administration also appears to influence LF efficacy. A study by Rosa et al. [36] demonstrated that oral intake of cbLF before meals resulted in greater reductions in serum IL-6 and improved hematological parameters, likely due to the fact that gastric protease activity during meals may partially degrade the molecule and impair its bioavailability. This finding emphasizes that, in addition to dose and route of administration, timing is a critical factor affecting LF’s therapeutic effectiveness.
5. Limits
This narrative review is subject to several limitations. First, all included studies were conducted in Italy, limiting the generalizability of findings to other healthcare systems and socio-cultural contexts, highlighting the need for multicenter and international studies to confirm these results in broader populations. International evidence remains scarce and is mostly limited to case reports or small-scale experimental studies. Second, the majority of the studies were open-label clinical trials, often with small sample sizes, limited follow-up, and absence of placebo control or blinding, which increases the risk of performance and detection bias. Third, heterogeneity in study design, populations, lactoferrin formulations (bovine vs. recombinant), dosages, and clinical endpoints prevents direct comparison and precludes meta-analytic synthesis. Furthermore, the overall methodological quality of the included studies varied, and none were multicenter trials, thus limiting the external validity and reproducibility of the findings. Finally, although some studies reported positive effects, the lack of high-quality randomized controlled trials (RCTs) with rigorous methodology and adequate power highlights the need for further robust investigations before drawing definitive conclusions.
6. Conclusions
The findings of this review indicate that lactoferrin supplementation, administered via oral and/or vaginal routes, exerts a multifaceted modulatory effect on inflammatory processes, biochemical markers, and immunological profiles associated with preterm birth risk. Notably, lactoferrin consistently reduced pro-inflammatory cytokines such as IL-6 across various biological compartments and improved cervical and uterine parameters related to pregnancy maintenance. Additionally, lactoferrin influenced key proteolytic enzymes and oxidative stress markers, potentially contributing to the stabilization of fetal membranes. Clinically, supplementation was associated with extended gestational duration, decreased rates of preterm labor, and reduced neonatal intensive care admissions. These results support the therapeutic potential of lactoferrin in mitigating mecanisms involved in inflammation underlying preterm birth. However, further large-scale, multicenter, and international randomized controlled trials are needed to confirm these findings and better define optimal dosage, route of administration, and timing of supplementation.
Author Contributions
The following statements should be used: Conceptualization, A.M. and S.El.; methodology, S.El.; validation, P.M; B.M..; writing—original draft preparation A.M; S.El; writing—review and editing, A.M; S.El; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AF | Amniotic Fluid |
| bLF | bovine lactoferrin |
| BV | bacterial vaginosis |
| ID | Iron deficiency |
| IDA | iron deficiency anemia |
| LF | lactoferrin |
| LPS | Lipopolysaccharide |
| MMP | matrix metalloproteinase |
| NICU | Neonatal Intensive Care Unit |
| OSI | Oxidative Stress Index |
| OSI | oxidative stress index |
| OxS | Oxidative Stress |
| PGE2 | Prostaglandin E2 |
| PTB | prevention of preterm birth |
| PTD | preterm delivery |
| PTL | Threatened Preterm Labor |
| rhLf | recombinant human lactoferrin |
| TAS | Total Antioxidant Status |
| TIMP | Tissue inhibitor of metalloproteinase |
References
- WHO Recommendations for Care of the Preterm or Low Birth Weight Infant, 1st ed. Geneva: World Health Organization, 2022.
- World Health Organization, ‘Born too soon: the global action report on preterm birth’, p. 112, 2012, Accessed: Jul. 22, 2025. [Online]. Available: https://iris.who.int/handle/10665/44864.
- V. C. Ward et al., ‘Overview of the Global and US Burden of Preterm Birth’, Clin. Perinatol., vol. 51, no. 2, pp. 301–311, Jun. 2024. [CrossRef]
- J. P. Vogel, S. Chawanpaiboon, A.-B. Moller, K. Watananirun, M. Bonet, and P. Lumbiganon, ‘The global epidemiology of preterm birth’, Best Pract. Res. Clin. Obstet. Gynaecol., vol. 52, pp. 3–12, Oct. 2018. [CrossRef]
- T. Karampitsakos et al., ‘The Impact of Amniotic Fluid Interleukin-6, Interleukin-8, and Metalloproteinase-9 on Preterm Labor: A Narrative Review’, Biomedicines, vol. 13, no. 1, p. 118, Jan. 2025. [CrossRef]
- R. Romero, J. Espinoza, L. F. Gonçalves, J. P. Kusanovic, L. Friel, and S. Hassan, ‘The role of inflammation and infection in preterm birth’, Semin. Reprod. Med., vol. 25, no. 1, pp. 21–39, Jan. 2007. [CrossRef]
- L. Hu et al., ‘Relationship between gastrointestinal disturbances, blood lipid levels, inflammatory markers, and preterm birth’, J. Obstet. Gynaecol., vol. 45, no. 1, Dec. 2025. [CrossRef]
- M. Vajrychova et al., ‘Quantification of intra-amniotic inflammation in late preterm prelabour rupture of membranes’, Sci. Rep., vol. 15, p. 14814, Apr. 2025. [CrossRef]
- S. Jin and P. M. Kang, ‘A Systematic Review on Advances in Management of Oxidative Stress-Associated Cardiovascular Diseases’, Antioxidants, vol. 13, no. 8, p. 923, Jul. 2024. [CrossRef]
- J. K. Actor, S.-A. Hwang, and M. L. Kruzel, ‘Lactoferrin as a natural immune modulator’, Curr. Pharm. Des., vol. 15, no. 17, pp. 1956–1973, 2009. [CrossRef]
- D. Legrand, ‘Overview of Lactoferrin as a Natural Immune Modulator’, J. Pediatr., vol. 173 Suppl, pp. S10-15, Jun. 2016. [CrossRef]
- J. A. Talbert, J. Lu, S. K. Spicer, R. E. Moore, S. D. Townsend, and J. A. Gaddy, ‘Ameliorating adverse perinatal outcomes with Lactoferrin: An intriguing chemotherapeutic intervention’, Bioorg. Med. Chem., vol. 74, p. 117037, Nov. 2022. [CrossRef]
- B. S. Berthon, L. M. Williams, E. J. Williams, and L. G. Wood, ‘Effect of Lactoferrin Supplementation on Inflammation, Immune Function, and Prevention of Respiratory Tract Infections in Humans: A Systematic Review and Meta-analysis’, Adv. Nutr., vol. 13, no. 5, pp. 1799–1819, Apr. 2022. [CrossRef]
- A. D’Amico et al., ‘Role of lactoferrin in preventing preterm birth and pregnancy complications: a systematic review and meta-analysis’, Minerva Obstet. Gynecol., vol. 75, no. 3, pp. 273–278, Jun. 2023. [CrossRef]
- S. Y. Lee, K. H. Park, E. H. Jeong, K. J. Oh, A. Ryu, and A. Kim, ‘Intra-Amniotic Infection/Inflammation as a Risk Factor for Subsequent Ruptured Membranes after Clinically Indicated Amniocentesis in Preterm Labor’, J. Korean Med. Sci., vol. 28, no. 8, p. 1226, 2013. [CrossRef]
- G. Giunta, L. Giuffrida, K. Mangano, P. Fagone, and A. Cianci, ‘Influence of lactoferrin in preventing preterm delivery: a pilot study’, Mol. Med. Rep., vol. 5, no. 1, pp. 162–166, Jan. 2012. [CrossRef]
- R. Paesano, M. Pietropaoli, F. Berlutti, and P. Valenti, ‘Bovine lactoferrin in preventing preterm delivery associated with sterile inflammation’, Biochem. Cell Biol. Biochim. Biol. Cell., vol. 90, no. 3, pp. 468–475, Jun. 2012. [CrossRef]
- F. Vesce et al., ‘Vaginal lactoferrin administration before genetic amniocentesis decreases amniotic interleukin-6 levels’, Gynecol. Obstet. Invest., vol. 77, no. 4, pp. 245–249, 2014. [CrossRef]
- A. Trentini et al., ‘Vaginal Lactoferrin Modulates PGE2, MMP-9, MMP-2, and TIMP-1 Amniotic Fluid Concentrations’, Mediators Inflamm., vol. 2016, p. 3648719, 2016. [CrossRef]
- M. Locci et al., ‘Vaginal lactoferrin in asymptomatic patients at low risk for pre-term labour for shortened cervix: cervical length and interleukin-6 changes’, J. Obstet. Gynaecol. J. Inst. Obstet. Gynaecol., vol. 33, no. 2, pp. 144–148, Feb. 2013. [CrossRef]
- A. Trentini et al., ‘Vaginal Lactoferrin Administration Decreases Oxidative Stress in the Amniotic Fluid of Pregnant Women: An Open-Label Randomized Pilot Study’, Front. Med., vol. 7, Sep. 2020. [CrossRef]
- M. Miranda et al., ‘Vaginal lactoferrin in prevention of preterm birth in women with bacterial vaginosis’, J. Matern.-Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet., vol. 34, no. 22, pp. 3704–3708, Nov. 2021. [CrossRef]
- M. Maritati et al., ‘Influence of vaginal lactoferrin administration on amniotic fluid cytokines and its role against inflammatory complications of pregnancy’, J. Inflamm. Lond. Engl., vol. 14, p. 5, 2017. [CrossRef]
- D. Kumar et al., ‘Proinflammatory cytokines found in amniotic fluid induce collagen remodeling, apoptosis, and biophysical weakening of cultured human fetal membranes’, Biol. Reprod., vol. 74, no. 1, pp. 29–34, Jan. 2006. [CrossRef]
- R. Menon and S. J. Fortunato, ‘Infection and the role of inflammation in preterm premature rupture of the membranes’, Best Pract. Res. Clin. Obstet. Gynaecol., vol. 21, no. 3, pp. 467–478, Jun. 2007. [CrossRef]
- S.-S. Shim et al., ‘Clinical significance of intra-amniotic inflammation in patients with preterm premature rupture of membranes’, Am. J. Obstet. Gynecol., vol. 191, no. 4, pp. 1339–1345, Oct. 2004. [CrossRef]
- F. Vadillo-Ortega and G. Estrada-Gutiérrez, ‘Role of matrix metalloproteinases in preterm labour’, BJOG Int. J. Obstet. Gynaecol., vol. 112 Suppl 1, pp. 19–22, Mar. 2005. [CrossRef]
- S. Y. Lee, K. H. Park, E. H. Jeong, K. J. Oh, A. Ryu, and A. Kim, ‘Intra-amniotic infection/inflammation as a risk factor for subsequent ruptured membranes after clinically indicated amniocentesis in preterm labor’, J. Korean Med. Sci., vol. 28, no. 8, pp. 1226–1232, Aug. 2013. [CrossRef]
- R. Romero et al., ‘A fetal systemic inflammatory response is followed by the spontaneous onset of preterm parturition’, Am. J. Obstet. Gynecol., vol. 179, no. 1, pp. 186–193, Jul. 1998. [CrossRef]
- I. Tency et al., ‘Imbalances between Matrix Metalloproteinases (MMPs) and Tissue Inhibitor of Metalloproteinases (TIMPs) in Maternal Serum during Preterm Labor’, PLoS ONE, vol. 7, no. 11, p. e49042, Nov. 2012. [CrossRef]
- D. Sundrani, A. Narang, S. Mehendale, S. Joshi, and P. Chavan-Gautam, ‘Investigating the expression of MMPs and TIMPs in preterm placenta and role of CpG methylation in regulating MMP-9 expression’, IUBMB Life, vol. 69, no. 12, pp. 985–993, Dec. 2017. [CrossRef]
- Q. Rascón-Cruz et al., ‘Antioxidant Potential of Lactoferrin and Its Protective Effect on Health: An Overview’, Int. J. Mol. Sci., vol. 26, no. 1, p. 125, Dec. 2024. [CrossRef]
- A. Pino, G. Giunta, C. L. Randazzo, S. Caruso, C. Caggia, and A. Cianci, ‘Bacterial biota of women with bacterial vaginosis treated with lactoferrin: an open prospective randomized trial’, Microb. Ecol. Health Dis., vol. 28, no. 1, p. 1357417, Jan. 2017. [CrossRef]
- J. Artym, M. Zimecki, and M. L. Kruzel, ‘Lactoferrin for Prevention and Treatment of Anemia and Inflammation in Pregnant Women: A Comprehensive Review’, Biomedicines, vol. 9, no. 8, p. 898, Jul. 2021. [CrossRef]
- K. Otsuki, T. Nishi, T. Kondo, and K. Okubo, ‘Review, role of lactoferrin in preventing preterm delivery’, Biometals Int. J. Role Met. Ions Biol. Biochem. Med., vol. 36, no. 3, pp. 521–530, Jun. 2023. [CrossRef]
- L. Rosa, A. Cutone, M. S. Lepanto, R. Paesano, and P. Valenti, ‘Lactoferrin: A Natural Glycoprotein Involved in Iron and Inflammatory Homeostasis’, Int. J. Mol. Sci., vol. 18, no. 9, p. 1985, Sep. 2017. [CrossRef]
Figure 1.
PRISMA-Inspired Flowchart Representing the Study Selection Process.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



