
Submitted:
26 August 2025
Posted:
01 September 2025
You are already at the latest version
Abstract
Background: The relationship between alcohol consumption and arterial stiffness parameters remains unclear. This study aimed to analyze the association between alcohol consumption and arterial stiffness in young Spanish adults. Methods: A cross-sectional descriptive study was conducted, involving 501 participants (222 men and 279 women), aged 18–34 years, who were free from cardiovascular disease and recruited from the urban population of Salamanca. Arterial stiffness was assessed using the cardio-ankle vascular index (CAVI) and brachial-ankle pulse wave velocity (ba-PWV) with the Vasera VS-2000® device, and carotid-femoral pulse wave velocity (cf-PWV) with the Sphygmocor System®. Alcohol consumption was assessed using a standardized questionnaire and quantified in grams per week, then categorized into sex-specific tertiles. Results: The mean age was 26.5 years, higher in men. Mean values of vascular function parameters were: CAVI 6.13±0.75 (no sex differences), cf-PWV 5.60±1.29 m/s, and ba-PWV 10.80±1.01 m/s (both higher in men). Overall, systolic blood pressure, pulse pressure, and waist circumference were higher among individuals with greater alcohol consumption. Men in tertile 2 and women in tertile 3 reported less physical activity. In multinomial regression analysis, using tertile 1 as reference, a positive association was observed for ba-PWV with moderate alcohol consumption (β = 0.78, 95% CI: 0.63–0.98). Conclusions: Alcohol consumption was positively associated with ba-PWV, but not with cf-PWV or CAVI.
Keywords:
alcohol consumption
; vascular stiffness
; young adults
1. Introduction
Alcohol consumption among adults aged 18–34 years is highly prevalent worldwide [1], in the European Union [2], and in Spain [3], with rates approaching 90%. During adolescence and early adulthood, alcohol use is widely normalized as a social activity, and episodes of drunkenness are often integrated into these interactions [4].
Arterial stiffness is strongly linked to aging, and accelerated stiffening is considered a marker of early vascular aging [5]. Noninvasive measures of arterial stiffness, such as carotid-femoral pulse wave velocity (cf-PWV), brachial-ankle pulse wave velocity (ba-PWV), and the cardio-ankle vascular index (CAVI), provide an integrated view of vascular health and are independent predictors of cardiovascular disease and all-cause mortality [6,7,8,9].
Several studies have reported that alcohol intake is associated with increased arterial stiffness [10,11,12,13], higher blood pressure [14,15,16,17], hypertriglyceridemia, and a greater incidence of type 2 diabetes [18]. Conversely, other studies suggest that moderate alcohol consumption, without binge-drinking episodes, may reduce the risk of coronary heart disease compared with abstinence [14,19], although some report no benefit [20,21,22]. There is general agreement that heavy alcohol intake is linked to increased cardiovascular risk and mortality [12,14,19,21], describing a J-shaped relationship between alcohol consumption, cardiovascular disease, and arterial stiffness [19,23,24,25]. These effects appear more pronounced in women [14,21]. It has also been suggested that the apparent benefits of low-to-moderate consumption may reflect confounding by healthier lifestyle habits among light drinkers [26]. Importantly, potential benefits of alcohol have only been demonstrated in epidemiological studies [14,21], without accounting for confounding factors such as age, ethnicity, sex, beverage type, or drinking pattern [19].
In summary, previous research suggests that heavy alcohol intake is a risk factor for increased arterial stiffness [10,11,12,13,23,24,25], even in adolescents [27]. Binge drinking also worsens arterial stiffness in young adults [28]. Consumption above 14 units per week shows a positive linear relationship with arterial stiffness, even among individuals under 50 years [13,29]. Some studies show that stiffness decreases within the first hour after alcohol ingestion [30,31], while chronic low-to-moderate consumption may reduce stiffness [25,32].
Taken together, these findings indicate that the relationship between alcohol consumption and arterial stiffness, when assessed with comprehensive vascular measures, remains unclear in young adults. Therefore, the primary objective of this study was to examine the association between alcohol consumption and arterial stiffness across the vascular tree in young Spanish adults.
2. Materials and Methods
2.1. Study Design
This study was part of the EVA-Adic project, whose protocol has been previously published [33]. The EVA-Adic study was a descriptive observational study conducted by the Primary Care Research Unit of Salamanca (APISAL) and registered at ClinicalTrials.gov (identifier: NCT05819840).
2.2. Study Population
A total of 501 individuals aged 18–34 years from the urban health area of Salamanca were selected by simple random sampling, using the individual health card database from urban primary care centers. Inclusion criteria were age between 18 and 34 years and residence in the urban health area. Exclusion criteria were terminal illness, inability to attend the research unit for assessments, or failure to provide written informed consent.
2.3. Variables and Measurement Instruments
All measurements and tests were performed within a period of less than 8 days by a team of previously trained investigators following standardized procedures. The quality of the measurements was monitored by an independent researcher.
2.3.1. Sociodemographic Variables and Personal History
At baseline, age and sex were recorded.
2.3.2. Lifestyle Factors
Alcohol Consumption. Alcohol intake was assessed using a structured questionnaire, which recorded the amount of alcohol consumed during the previous 7 days in grams per week. Alcohol use was further evaluated with the Alcohol Use Disorders Identification Test (AUDIT), which classifies consumption into low risk (0–7 points), medium risk (8–15 points), high risk (16–19 points), and dependence (≥20 points) [34]. The categories of abstainers, low risk, intermediate risk, and high risk were defined according to the criteria of the Spanish Ministry of Health [35]. Alcohol consumption was categorized into sex-specific tertiles.
Adherence to the Mediterranean Diet. Adherence to the Mediterranean diet was assessed with the Mediterranean Diet Adherence Screener (MEDAS), which has been validated in the Spanish population [36].
Tobacco: Smoking status was assessed using the standardized four-item questionnaire from the WHO MONICA study [37]. In addition, the number of years of smoking was recorded.
Physical Activity: Physical activity was assessed using the International Physical Activity Questionnaire-Short Form (IPAQ-SF) [38]. This questionnaire includes 7 items on the type and duration of physical activity performed during the past 7 days. The total result was expressed in metabolic equivalents of task per minute per week (MET-min/week).
2.3.3. Arterial Stiffness
Arterial stiffness was evaluated through carotid–femoral pulse wave velocity (cf-PWV), brachial–ankle pulse wave velocity (ba-PWV), and cardio–ankle vascular index (CAVI).
cf-PWV was measured using the SphygmoCor® device (AtCor Medical Pty Ltd., West Ryde, Australia) with participants in the supine position. The pulse wave at the carotid and femoral sites was obtained by estimating the delay relative to the R-wave of the ECG, and cf-PWV was calculated. Distance was measured with a measuring tape from the sternal notch to the carotid and femoral sensors [39].
ba-PWV and CAVI were measured with the VaSera VS-2000® device (Fukuda Denshi Co., Ltd., Tokyo, Japan). Electrodes were placed on the arms and legs, and a phonocardiographic sensor was positioned in the second intercostal space. Measurements were obtained while the participant remained silent and still. CAVI was calculated using the following equation: stiffness parameter β = 2ρ × 1/(SBP − DBP) × ln(SBP/DBP) × PWV, where ρ is blood density and PWV is measured between the aortic valve and the ankle. Measurements were considered valid after three cardiac cycles [40]. ba-PWV was calculated using the following equation: ba-PWV = (0.5934 × height (cm) + 14.4724)/tba, where tba is the time interval between the brachial and ankle pulse waves [41,42].
2.3.4. Cardiovascular Risk Factors
Laboratory Variables: Venous blood samples were obtained between 8:00 and 9:00 a.m. after an overnight fast and abstention from alcohol, tobacco, or caffeine for at least 12 hours. Samples were collected at APISAL and analyzed for glucose, total cholesterol, HDL cholesterol, LDL cholesterol, and triglycerides, following standardized laboratory procedures.
Blood Pressure: was measured three times consecutively using a validated sphygmomanometer (Omron M10-IT®, Omron Healthcare, Kyoto, Japan). Measurements were taken on the dominant arm with the participant seated after resting for at least 5 minutes, using an appropriately sized cuff. The procedure followed the recommendations of the European Society of Hypertension (ESH) [43]. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were recorded, and pulse pressure (PP) was calculated as SBP minus DBP.
2.3.5. Anthropometric Variables
Height was measured in centimeters using a calibrated stadiometer (Seca 222, Medical Scale® and Measurement Systems, Birmingham, UK), with the participant barefoot, standing upright against the wall, and at full inspiration. Waist circumference was measured with a flexible measuring tape, positioned parallel to the floor above the iliac crests, at the end of expiration, with the participant standing upright and without clothing. These procedures followed the recommendations of the Spanish Society for the Study of Obesity (SEEDO) [44]. Weight was measured in kilograms using the InBody 230® analyzer (Biospace), following the manufacturer’s instructions. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m²) [45].
2.4. Statistical Analysis
Differences between means of variables with two categories were analyzed using the Student’s t-test or the Mann–Whitney U test, as appropriate. For variables with more than two categories, analysis of variance (ANOVA) was applied, followed by the DMS post hoc test. Analysis of covariance (ANCOVA) was performed to adjust for potential confounding variables. The relationship between alcohol consumption and arterial stiffness was analyzed using multinomial logistic regression. The dependent variable was alcohol consumption categorized into tertiles, with the lowest tertile as the reference. Independent variables included cf-PWV, ba-PWV, and CAVI. Covariates included age (years), sex (male = 1; female = 0), mean Mediterranean diet adherence score, total physical activity (MET-min/week), pulse pressure (mmHg), LDL cholesterol (mg/dL), waist circumference (cm), and fasting plasma glucose (mg/dL). Statistical analyses were performed using SPSS for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). A p-value < 0.05 was considered statistically significant. The statistician was blinded to clinical data. All analyses were conducted both overall and stratified by sex.
2.6. Ethical Considerations
The study protocol was approved by the Ethics Committee for Research with Medicines of the Health Area of Salamanca on 10 July 2021 (Ref. PI 2021 088671048) and on 24 July 2023 (Ref. PI 2023 071332). The study was conducted in accordance with the Declaration of Helsinki [46] and WHO recommendations. Data confidentiality was ensured according to the Spanish Law 3/2018 on Personal Data Protection and Guarantee of Digital Rights and the European General Data Protection Regulation (EU) 2016/679. Written informed consent was obtained from all participants prior to inclusion, after they had been informed about the examinations and questionnaires involved in the study.
3. Results
3.1. Participant Characteristics
The main characteristics of the study participants are presented overall and stratified by sex in Table 1. More women than men were included (279 vs. 222, p < 0.05). Men reported higher alcohol and tobacco consumption and performed more physical activity than women. Women had higher Mediterranean diet adherence scores than men. Men exhibited higher levels of LDL cholesterol, HDL cholesterol, triglycerides, blood pressure, and obesity-related parameters compared to women.
The characteristics of participants according to alcohol consumption tertiles are presented in Table 2. Participants in the third tertile exhibited higher SBP, PP, and waist circumference.
The characteristics of men according to alcohol consumption tertiles are shown in Table 3. Men in tertile 2 performed less physical activity.
The characteristics of women according to alcohol consumption tertiles are shown in Table 4. Women in tertile 3 performed less physical activity.
3.2. Arterial Stiffness According to Alcohol Consumption Tertiles
Figure 1 shows the marginal means adjusted for age, Mediterranean diet adherence score, and physical activity according to alcohol consumption, overall and by sex, for cf-PWV (p = 0.81), ba-PWV (p = 0.075), and CAVI (p = 0.450), with no significant differences observed.
3.3. Risk Drinking According to AUDIT
Figure 2 shows the classification of the study population based on AUDIT results. Most participants were classified as low risk (87.82%; 82.88% in men and 97.75% in women). High-risk drinking was observed in 0.80% of the population (0.90% in men and 0.70% in women).
3.4. Association Between Alcohol Consumption and Arterial Stiffness
The correlation between alcohol consumption (g/week) and cf-PWV was Rho = 0.081 (p = 0.490), with ba-PWV Rho = 0.090 (p = 0.060), and with CAVI Rho = 0.082 (p = 0.641).
Results of the multinomial regression analysis are shown in Figure 3. For each 1 cm increase in cf-PWV, the β coefficient for belonging to the moderate consumption group vs. abstainer/low consumption was 0.99 (95% CI: 0.82–1.19) and for excessive consumption 0.90 (95% CI: 0.74–1.10). For each 1 cm increase in ba-PWV, the β coefficient for moderate vs. abstainer/low consumption was 0.78 (95% CI: 0.63–0.98) and for excessive consumption 0.78 (95% CI: 0.61–1.02). For each 1-unit increase in CAVI, the β coefficient for moderate vs. abstainer/low consumption was 1.17 (95% CI: 0.84–1.61) and for excessive consumption 1.13 (95% CI: 0.78–1.62).
4. Discussion
This study provides new insights into the relationship between alcohol consumption and arterial stiffness (measured by cf-PWV, ba-PWV, and CAVI) in adults aged 18–34 years. In this population, we found that moderate alcohol consumption was associated with lower ba-PWV values compared to abstainers, suggesting a potential protective effect of moderate alcohol intake.
4.1. Arterial Stiffness Values
The ba-PWV values observed in our study are similar to those reported in Japanese populations by Nishiwaki et al., 2025 (10.70 m/s) [47] and Nakao et al. (11.13 m/s) [48], as well as in the Thai population by Jaruchart et al., 2016 (10.77 m/s) [49]. In contrast, Yufu et al. reported higher averages in a Japanese cohort (12.01 m/s) [50], consistent with the Asian average reported by Yiming et al., 2017 (12.0 m/s) [51]. Lower averages have been reported in two populations: Baier et al. in a German cohort (9.3 m/s) and Satish et al. in an Indian cohort (9.94 m/s) [52]. The cf-PWV values in our study are comparable to those reported in India by Satish et al., 2021 (5.8 m/s) [52]. For European populations, the mean values are lower than reference values published in 2010 for individuals under 30 years (6.2 m/s) and 30–39 years (6.5 m/s). More recent European studies, such as Agbaje et al. for the UK (6.12 m/s) [54] and Baier et al. for Germany (7.3 m/s) [55], also report higher cf-PWV values than those found in our study. In the Americas, Diaz et al. found higher values in Argentina (6.1 m/s) [56], as did studies in the United States [57,58,59]. Regarding CAVI, Nishiwaki et al. [60] reported lower values (5.8) in men aged 18–21, while Russian populations aged 18–28 show similar values (5.87) [61]. Conversely, higher CAVI values have been observed in Mongolia (6.5) [62], while Chinese cohorts show similar values to ours (6.4) [63], although other authors have reported higher means (6.7) [64]. In the United States, values similar to ours have been reported in this age range [65]. Differences among studies may be due to small sample sizes, differing age ranges within “young adults,” sampling methods, or real regional differences, such as lower cardiovascular risk in Spain and Mediterranean countries compared to other regions.
Sex-specific analysis in our study showed lower ba-PWV and cf-PWV values in women compared to men. Similar differences have been reported in Korean populations by Cho et al. [66], and in European [67], UK [54], and US [58] populations. In contrast, CAVI values were higher in men in our study, although the difference was not significant. Comparable findings have been reported in Japanese [68,69] and Korean [70] populations. Namekata et al. observed significant sex differences in CAVI, but their cohort included adults aged 20–70 years [69].
4.2. Alcohol Consumption and Arterial Stiffness
Numerous studies have explored the relationship between alcohol intake and arterial stiffness, showing that excessive alcohol consumption is associated with higher cf-PWV [12], ba-PWV [29], and CAVI [23]. The EVA study, conducted in Spanish adults aged 35–75 years, reported a J-shaped association between alcohol and cf-PWV [23], consistent with findings in the UK population [12]. J-shaped curves between ba-PWV and alcohol intake have also been observed in Korean [71] and Japanese [32,72] cohorts. While high alcohol intake has been linked to increased arterial stiffness in adolescents [27], few studies have focused on individuals aged 18–35. Our study observed a U-shaped relationship between alcohol intake and ba-PWV, though the results were not statistically significant. Increased cf-PWV associated with alcohol intake has been reported in American populations aged 18–30 [28,57], whereas Canadian cohorts did not show such differences [17]. No previous studies have assessed CAVI in relation to alcohol consumption in this age group. The EVA study, which used CAVI in an older adult population, found a U-shaped association with alcohol [23]. In our younger cohort, we observed an inverted U-shaped relationship between alcohol consumption and CAVI.
Acute alcohol intake can transiently reduce arterial stiffness within 60 minutes of consuming a minimal dose of 3.3 mL/kg body weight [31], in both general and younger populations (<35 years) [73]. However, the long-term effect of alcohol on arterial stiffness remains controversial, as these changes may involve structural, functional, or combined vascular alterations [74]. Potential mechanisms for improved arterial elasticity include increased HDL cholesterol, reduced LDL oxidation [75], decreased platelet aggregation and fibrogenesis, enhanced fibrinolysis, and improved insulin sensitivity [76]. These findings may have implications for the early identification of modifiable lifestyle factors related to vascular aging in young adults. Further studies are needed to deepen the understanding of this relationship.
4.3. Limitations and Strengths
This study presents the following limitations: Causality cannot be established due to the observational nature of the study. Given the relatively small sample size and the predominance of female participants, comparisons between sexes should be interpreted with caution. The selected population was from an urban setting, which limits the generalizability of the results to other populations. Alcohol consumption, smoking status, adherence to the Mediterranean diet, and physical activity were assessed using self-reported questionnaires, and the group classified as non-drinkers did not distinguish between lifetime abstainers and former drinkers.
The strengths of this study include: It is the first study to focus on the relationship between alcohol consumption and vascular parameters in individuals aged 18 to 34 years. Multiple measures of arterial stiffness were used, and the researchers collecting data on the study variables were trained and followed a standardized protocol.
5. Conclusion
Alcohol consumption was positively associated with ba-PWV but not with cf-PWV or CAVI.
Author Contributions
Writing—Review & Editing, A.V-P, L.G-S, M. M.G-M and MA.G.-M.; Supervision, All Authors. Writing—Original Draft Preparation, A.V-P, L.G-S, M. M.G-M; Investigation, A.V-P, S.V-G, C. L-S S.G-M.; and S.G-S. All authors have read and agreed to the published version of the manuscript.
Funding
This study has been funded by the Spanish Ministry of Science and Innovation, Instituto de Salud Carlos III (ISCIII). RD21/0016/0010 (Network for Research on Chronicity, Primary Care, and Health Promotion (RICAPPS) is funded by the European Union-Next Generation EU, Facility for Recovery and Resilience (MRR). The government of Castilla y León also collaborated with the funding of this study through the research projects (Government of Castilla y León (GRS2707/C/2023; GRS 2500/B/22) and the Institute for Biomedical Research of Salamanca (IBSAL) (IBYE22/00003; IBYAP23_0002) also collaborated with the funding of this study through the research projects. He also received funding from the Spanish Society of Family and Community Medicine (semFYC) after winning the Isabel Fernández 2023 doctoral thesis grant.
EVA-Adic Investigators Group The members of the EVA-Adic Group are
Manuel A. Gómez Marcos, Luis García-Ortiz, Emiliano Rodríguez-Sánchez, Cristina Lugones-Sánchez, Olaya Tamayo-Morales, Susana González-Sánchez, Leticia Gómez-Sánchez, Sara M. Vicente-Gabriel, Alberto Vicente-Prieto, Sandra Conde-Martín, Marta Gómez-Sánchez, Elena Navarro Matias, Carmen Patino-Alonso, José A. Maderuelo-Fernández, Angela de Cabo-Laso, Benigna Sanchez-Salgado, and Laura Fernandez-Matas.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting the findings of this study are available on ZENODO under the DOI. https://doi.org/10.5281/zenodo.16910594.
Acknowledgments
We would like to thank all members of the EVA-Adic. We would also like to thank the patient advisers who collaborated with the study investigators.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| cf-PWV | carotid–femoral pulse wave velocity |
| ba-PWV | brachial–ankle pulse wave velocity |
| CAVI | cardio-ankle vascular index |
| AUDIT | Alcohol Use Disorders Identification TEST |
| MEDAS | Mediterranean Diet Adherence Screener |
| IPAQ-SF | International Physical Activity Questionnaire-Short Form |
| METs-min/week | metabolic equivalent of task |
| SBP | systolic blood pressure |
| DBP | diastolic blood pressure |
| PP | pulse pressure |
| BMI | body mass index |
References
- World Health Organization. Global status report on alcohol and health and treatment of substance use disorders; 2024.
- European Union Drugs Agency. Prevalence of drug use, Alcohol, Lifetime prevalence, Young adults (15-34). Available online: https://www.euda.europa.eu/data/stats2024/gps_en#displayTable:GPS-128 (accessed on 01/12/2024).
- Observatorio Español de las Drogas y las Adicciones. Informe 2024. Alcohol, tabaco y drogas ilegales en España. 2024, 1-74.
- Seaman., P.; Ikegwuonu, T. Drinking to belong. Understanding young adults’ alcohol use within social networks; Joseph Rowntree Foundation: Glasgow, 2010; pp. 1–56. [Google Scholar]
- Boutouyrie, P.; Chowienczyk, P.; Humphrey, J.D.; Mitchell, G.F. Arterial Stiffness and Cardiovascular Risk in Hypertension. Circulation Research 2021, 128, 864–886. [Google Scholar] [CrossRef] [PubMed]
- Yue, X.; Chen, L.; Shi, Y.; Suo, Y.; Liao, S.; Cheang, I.; Gao, R.; Zhu, X.; Zhou, Y.; Yao, W.; et al. Comparison of arterial stiffness indices measured by pulse wave velocity and pulse wave analysis for predicting cardiovascular and all-cause mortality in a Chinese population. Hypertension Research 2024, 47, 767–777. [Google Scholar] [CrossRef]
- Kim, H.L.; Kim, S.H. Pulse Wave Velocity in Atherosclerosis. Front Cardiovasc Med 2019, 6, 41. [Google Scholar] [CrossRef]
- Back, M.; Topouchian, J.; Labat, C.; Gautier, S.; Blacher, J.; Cwynar, M.; de la Sierra, A.; Pall, D.; Duarte, K.; Fantin, F.; et al. Cardio-ankle vascular index for predicting cardiovascular morbimortality and determinants for its progression in the prospective advanced approach to arterial stiffness (TRIPLE-A-Stiffness) study. EBioMedicine 2024, 103, 105107. [Google Scholar] [CrossRef]
- Stone, K.; Fryer, S.; McDonnell, B.J.; Meyer, M.L.; Faulkner, J.; Agharazii, M.; Fortier, C.; Pugh, C.J.A.; Paterson, C.; Zieff, G.; et al. Aortic-Femoral Stiffness Gradient and Cardiovascular Risk in Older Adults. Hypertension 2024, 81. [Google Scholar] [CrossRef]
- Hwang, C.L.; Muchira, J.; Hibner, B.A.; Phillips, S.A.; Piano, M.R. Alcohol Consumption: A New Risk Factor for Arterial Stiffness? Cardiovascular Toxicology 2022, 22, 236–245. [Google Scholar] [CrossRef]
- Cypiene, A.; Gimzauskaite, S.; Rinkuniene, E.; Jasiunas, E.; Laucevicius, A.; Ryliskyte, L.; Badariene, J. Effect of Alcohol Consumption Habits on Early Arterial Aging in Subjects with Metabolic Syndrome and Elevated Serum Uric Acid. Nutrients 2023, 15, 1–12. [Google Scholar] [CrossRef]
- O'Neill, D.; Britton, A.; Brunner, E.J.; Bell, S. Twenty-Five-Year Alcohol Consumption Trajectories and Their Association With Arterial Aging: A Prospective Cohort Study. Journal of American Heart Association 2017, 6, e005288. [Google Scholar] [CrossRef]
- Schutte, R.; Zhang, J.; Kiran, M.; Ball, G. Alcohol and arterial stiffness in middle-aged and older adults: Cross-sectional evidence from the UK Biobank study. Alcohol Clinical & Experimental Research 2024, 48, 1915–1922. [Google Scholar] [CrossRef]
- Piano, M.R. Alcohol’s Effects on the Cardiovascular System. Alcohol Research 2017, 38, 219–241. [Google Scholar]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Back, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. European Heart Journal 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Tasnim, S.; Tang, C.; Musini, V.M.; Wright, J.M. Effect of alcohol on blood pressure. Cochrane Database Syst Rev 2020, 7, CD012787. [Google Scholar] [CrossRef]
- Yu, A.; Cooke, A.B.; Scheffler, P.; Doonan, R.J.; Daskalopoulou, S.S. Alcohol Exerts a Shifted U-Shaped Effect on Central Blood Pressure in Young Adults. Journal of General Internal Medicine 2021, 36, 2975–2981. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Sola, J. Cardiovascular risks and benefits of moderate and heavy alcohol consumption. Nature Reviews Cardiology 2015, 12, 576–587. [Google Scholar] [CrossRef] [PubMed]
- Goel, S.; Sharma, A.; Garg, A. Effect of Alcohol Consumption on Cardiovascular Health. Current Cardiology Report 2018, 20, 19. [Google Scholar] [CrossRef]
- Stockwll, T.; Zhao, J.; Panwar, S.; Roemer, A.; Naimi, T.; Chikritzhs, T. Do “Moderate” Drinkers Have Reduced Mortality Risk? A Systematic Review and Meta-Analysis ofAlcohol Consumption and All-Cause Mortality. Journal of studies on alcohol and drugs 2016, 77, 185–198. [Google Scholar] [CrossRef]
- Zhao, J.; Stockwell, T.; Naimi, T.; Churchill, S.; Clay, J.; Sherk, A. Association Between Daily Alcohol Intake and Risk of All-Cause Mortality: A Systematic Review and Meta-analyses. JAMA Network Open 2023, 6, e236185. [Google Scholar] [CrossRef]
- GBD Alcohol Collaborators. Alcohol use and burden for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef]
- Gonzalez-Sanchez, J.; Garcia-Ortiz, L.; Rodriguez-Sanchez, E.; Maderuelo-Fernandez, J.A.; Tamayo-Morales, O.; Lugones-Sanchez, C.; Recio-Rodriguez, J.I.; Gomez-Marcos, M.A.; Investigators, E.V.A. The Relationship Between Alcohol Consumption With Vascular Structure and Arterial Stiffness in the Spanish Population: EVA Study. Alcoholism Clinical and Experimental Research 2020, 44, 1816–1824. [Google Scholar] [CrossRef]
- Arroyo-Romero, S.; Gomez-Sanchez, L.; Suarez-Moreno, N.; Navarro-Caceres, A.; Dominguez-Martin, A.; Lugones-Sanchez, C.; Tamayo-Morales, O.; Gonzalez-Sanchez, S.; Castro-Rivero, A.B.; Gomez-Sanchez, M.; et al. Relationship Between Alcohol Consumption and Vascular Structure and Arterial Stiffness in Adults Diagnosed with Persistent COVID: BioICOPER Study. Nutrients 2025, 17, 1–17. [Google Scholar] [CrossRef]
- Del Giorno, R.; Maddalena, A.; Bassetti, S.; Gabutti, L. Association between Alcohol Intake and Arterial Stiffness in Healthy Adults: A Systematic Review. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Biddinger, K.J.; Emdin, C.A.; Haas, M.E.; Wang, M.; Hindy, G.; Ellinor, P.T.; Kathiresan, S.; Khera, A.V.; Aragam, K.G. Association of Habitual Alcohol Intake With Risk of Cardiovascular Disease. JAMA Netw Open 2022, 5, e223849. [Google Scholar] [CrossRef]
- Charakida, M.; Georgiopoulos, G.; Dangardt, F.; Chiesa, S.T.; Hughes, A.D.; Rapala, A.; Davey Smith, G.; Lawlor, D.; Finer, N.; Deanfield, J.E. Early vascular damage from smoking and alcohol in teenage years: the ALSPAC study. European Heart Journal 2019, 40, 345–353. [Google Scholar] [CrossRef]
- Hwang, C.L.; Piano, M.R.; Thur, L.A.; Peters, T.A.; da Silva, A.L.G.; Phillips, S.A. The effects of repeated binge drinking on arterial stiffness and urinary norepinephrine levels in young adults. J Hypertens 2020, 38, 111–117. [Google Scholar] [CrossRef]
- Shiina, K.; Takahashi, T.; Nakano, H.; Fujii, M.; Iwasaki, Y.; Matsumoto, C.; Yamashina, A.; Chikamori, T.; Tomiyama, H. Longitudinal Associations between Alcohol Intake and Arterial Stiffness, Pressure Wave Reflection, and Inflammation. Journal of Atherosclerosis and Thrombosis 2023, 30, 192–202. [Google Scholar] [CrossRef]
- Nishiwaki, M.; Yamaguchi, T.; Nishida, R.; Matsumoto, N. Dose of Alcohol From Beer Required for Acute Reduction in Arterial Stiffness. Front Physiol 2020, 11, 1033. [Google Scholar] [CrossRef]
- Nishiwaki, M.; Kora, N.; Matsumoto, N. Ingesting a small amount of beer reduces arterial stiffness in healthy humans. Physiological Reports 2017, 5, e13381. [Google Scholar] [CrossRef]
- Sasaki, S.; Yoshioka, E.; Saijo, Y.; Kita, T.; Okada, E.; Tamakoshi, A.; Kishi, R. Relation between alcohol consumption and arterial stiffness: A cross-sectional study of middle-aged Japanese women and men. Alcohol 2013, 47, 643–649. [Google Scholar] [CrossRef]
- Vicente-Gabriel, S.; Lugones-Sanchez, C.; Tamayo-Morales, O.; Vicente Prieto, A.; Gonzalez-Sanchez, S.; Conde Martin, S.; Gomez-Sanchez, M.; Rodriguez-Sanchez, E.; Garcia-Ortiz, L.; Gomez-Sanchez, L.; et al. Relationship between addictions and obesity, physical activity and vascular aging in young adults (EVA-Adic study): a research protocol of a cross-sectional study. Front Public Health 2024, 12, 1–12. [Google Scholar] [CrossRef]
- Montero, S.Á.; Casado, P.G.; Cruz, C.l.T.d.l.; Fernandez, F.B. Papel del test AUDIT (Alcohol Use Disorders Identification Test) para la detección de consumo excesivo de alcohol en atención primaria. Revista de Medicina Familiar y Comunitaria 2001, 11, 553–557. [Google Scholar] [CrossRef]
- Ministerio de Sanidad Gobierno de España. Límites de Consumo de Bajo Riesgo de Alcohol Actualización del riesgo relacionado con los niveles de consumo de alcohol, el patrón de consumo y el tipo de bebida Parte 1. Actualización de los límites de consumo de bajo riesgo de alcohol. 2020, 24-25.
- Schröder, H.; Fito, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvado, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing mediterranean diet adherence among older spanish men and women. The Journal of Nutrition Nutritional Epidemiology 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Tunstall-Pedoe, H. The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. Journal of Clinical Epidemiology 1988, 41, 105–114. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. International Journal of Behavioral Nutrition and Physical Activity 2011, 8, 1–11. [Google Scholar] [CrossRef]
- Fortier, C.; Agharazii, M. Arterial Stiffness Gradient. Pulse (Basel) 2016, 3, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Shirai, K.; Hiruta, N.; Song, M.; Kurosu, T.; Suzuki, J.; Tomaru, T.; Miyashita, Y.; Saiki, A.; Takahashi, M.; Suzuki, K.; et al. Cardio-Ankle Vascular Index (CAVI) as a Novel Indicator of Arterial Stiffness: Theory, Evidence and Perspectives. Journal of Atherosclerosis and Thrombosis 2011, 18, 924–938. [Google Scholar] [CrossRef] [PubMed]
- Yamashina, A.; Tomiyama, H.; Takeda, K.; Tsuda, H.; Arai, T.; Hirose, K.; Koji, Y.; Hori, S.; Yamato, Y. Validity, Reproducibility, and Clinical Significance of Noninvasive Brachial-Ankle Pulse Wave Velocity Measurement. Hypertens Research 2002, 25, 359–364. [Google Scholar] [CrossRef]
- Kawai. T; Ohishi. M; Onishi. M; Ito. N; Takeya. Y; Maekawa. Y; Rakugi. H. Cut-Off Value of Brachial-Ankle Pulse Wave Velocity to Predict Cardiovascular Disease in Hypertensive Patients: A Cohort Study. Journal of Atherosclerosis and Thrombosis 2013, 20, 391–400. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. European Heart Journal 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Rubio, M.A.; Barbany, M.; Moreno, B. Consenso SEEDO 2007 para la evaluación del sobrepeso y la obesidad y el establecimiento de criterios de intervención terapéutica. Medicina Clínica 2007, 128, 184–196. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and overweight. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 02-01-2025).
- Association, W.M. World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Participants. JAMA 2025, 333, 71–74. [Google Scholar] [CrossRef]
- Nishiwaki, M.; Kume, D.; Matsumoto, N. Investigations of segmental arterial stiffness in a cross-sectional study on young adult male trained swimmers, cyclists, and non-trained men. Physiological Reports 2025, 13, e70186. [Google Scholar] [CrossRef]
- Nakao, M.; Nomura, K.; Karita, K.; Nishikitani, M.; Yano, E. Relationship between Brachial-Ankle Pulse Wave Velocity and Heart Rate Variability in Young Japanese Men. Hypertension Research 2004, 27, 925–931. [Google Scholar] [CrossRef]
- Jaruchart, T.; Suwanwela, N.C.; Tanaka, H.; Suksom, D. Arterial stiffness is associated with age-related differences in cerebrovascular conductance. Exp Gerontol 2016, 73, 59–64. [Google Scholar] [CrossRef]
- Yufu, K.; Takahashi, N.; Hara, M.; Saikawa, T.; Yoshimatsu, H. Measurement of the brachial-ankle pulse wave velocity and flow-mediated dilatation in young, healthy smokers. Hypertension Research 2007, 30, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Yiming, G.; Zhou, X.; Lv, W.; Peng, Y.; Zhang, W.; Cheng, X.; Li, Y.; Xing, Q.; Zhang, J.; Zhou, Q.; et al. Reference values of brachial-ankle pulse wave velocity according to age and blood pressure in a central Asia population. PLoS One 2017, 12, e0171737. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.G.; Arakeri, S.; Khode, V. Association of Low BMI with Aortic Stiffness in Young Healthy Individuals. Current Hypertension Reviews 2021, 17, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Boutouyrie, P.; Vermeersch, S.J. Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: 'establishing normal and reference values'. European Heart Journal 2010, 31, 2338–2350. [Google Scholar] [CrossRef]
- Agbaje, A.O.; Barmi, S.; Sansum, K.M.; Baynard, T.; Barker, A.R.; Tuomainen, T.P. Temporal longitudinal associations of carotid-femoral pulse wave velocity and carotid intima-media thickness with resting heart rate and inflammation in youth. Journal of Applied Physiology 2023, 134, 657–666. [Google Scholar] [CrossRef]
- Baier, D.; Teren, A.; Wirkner, K.; Loeffler, M.; Scholz, M. Parameters of pulse wave velocity: determinants and reference values assessed in the population-based study LIFE-Adult. Clinical Research in Cardiology 2018, 107, 1050–1061. [Google Scholar] [CrossRef]
- Diaz, A.; Zocalo, Y.; Bia, D.; Wray, S.; Fischer, E.C. Reference intervals and percentiles for carotid-femoral pulse wave velocity in a healthy population aged between 9 and 87 years. The Journal of Clinical Hypertension 2018, 20, 659–671. [Google Scholar] [CrossRef]
- Tisdel, D.M.; Gadberry, J.J.; Burke, S.L.; Carlini, N.A.; Fleenor, B.S.; Campbell, M.S. Dietary fat and alcohol in the prediction of indices of vascular health among young adults. Nutrition 2021, 84, 111120. [Google Scholar] [CrossRef]
- Perdomo, S.J.; Moody, A.M.; McCoy, S.M.; Barinas-Mitchell, E.; Jakicic, J.M.; Gibbs, B.B. Effects on carotid-femoral pulse wave velocity 24 h post exercise in young healthy adults. Hypertens Res 2016, 39, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.J.; Lee, P.Y.; Chuang, Y.H.; Huang, C.C. Measurement of local pulse wave velocity for carotid artery by using an ultrasound-based method. Ultrasonics 2020, 102, 106064. [Google Scholar] [CrossRef] [PubMed]
- Nishiwaki, M.; Takahara, K.; Matsumoto, N. Arterial stiffness in young adult swimmers. European Journal of Applied Physiology 2017, 117, 131–138. [Google Scholar] [CrossRef]
- Sorokin, A.; Kotani, K.; Bushueva, O.; Taniguchi, N.; Lazarenko, V. The cardio-ankle vascular index and ankle-brachial index in young russians. Journal of Atherosclerosis and Thrombosis 2015, 22, 211–218. [Google Scholar] [CrossRef]
- Uurtuya, S.; Taniguchi, N.; Kotani, K.; Yamada, T.; Kawano, M.; Khurelbaatar, N.; Itoh, K.; Lkhagvasuren, T. Comparative study of the cardio-ankle vascular index and ankle-brachial index between young Japanese and Mongolian subjects. Hypertension Research 2009, 32, 140–144. [Google Scholar] [CrossRef]
- Zhou, Z.; Hou, L.; Cui, M.; Mourot, L.; Zhu, W. Acute effects of low-volume intermittent versus higher-volume continuous exercise on arterial stiffness in healthy young men. Scientific Reports 2022, 12, 1749. [Google Scholar] [CrossRef]
- Zheng, L.; Zhang, X.; Zhu, W.; Chen, X.; Wu, H.; Yan, S. Acute effects of moderate-intensity continuous and accumulated exercise on arterial stiffness in healthy young men. European Journal of Applied Physiology 2015, 115, 177–185. [Google Scholar] [CrossRef]
- Huck, C.J.; Bronas, U.G.; Williamson, E.B.; Draheim, C.C.; Duprez, D.A.; Dengel, D.R. Noninvasive measurements of arterial stiffness: repeatability and interrelationships with endothelial function and arterial morphology measures. Vascular Health and Risk Management 2007, 3, 343–349. [Google Scholar]
- Cho, J.; Baek, H.J. A Comparative Study of Brachial-Ankle Pulse Wave Velocity and Heart-Finger Pulse Wave Velocity in Korean Adults. Sensors (Basel) 2020, 20. [Google Scholar] [CrossRef]
- Azizzadeh, M.; Karimi, A.; Breyer-Kohansal, R.; Hartl, S.; Breyer, M.K.; Gross, C.; Boutouyrie, P.; Bruno, R.M.; Hametner, B.; Wassertheurer, S.; et al. Reference equations for pulse wave velocity, augmentation index, amplitude of forward and backward wave in a European general adult population. Scientific Reports 2024, 14, 23151. [Google Scholar] [CrossRef] [PubMed]
- Yagura, C.; Takamura, N.; Kadota, K.; Nagazumi, T.; Morishita, Y.; Nakazato, M.; Maeda, T.; Kusano, Y.; Abe, Y.; Aoyagi, K. Evaluation of cardiovascular risk factors and related clinical markers in healthy young Japanese adults. Clinical Chemistry and Laboratory Medicine 2007, 45, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Namekata, T.; Suzuki, K.; Ishizuka, N.; Shirai, K. Establishing baseline criteria of cardio-ankle vascular index as a new indicator of arteriosclerosis: a cross-sectional study. BMC Cardiovasc Disord 2011, 11, 51. [Google Scholar] [CrossRef]
- Su-Yeon, C.; Byung-Hee, O.; Bae Park, J.; Dong-Ju, C.; Moo-Yong, R.; Sungha, P. Age-associated increase in arterial stiffness measured according to the cardio-ankle vascular index without blood pressure changes in healthy adults. Journal of Atherosclerosis and Thrombosis 2013, 20, 911–923. [Google Scholar]
- Moon, J.; Hwang, I.C.; Kim, K.K.; Kang, W.C.; Cha, J.Y.; Moon, Y.A. Casual alcohol consumption is associated with less subclinical cardiovascular organ damage in Koreans: a cross-sectional study. BMC Public Health 2018, 18, 1091. [Google Scholar] [CrossRef]
- Uemura, H.; Katsuura-Kamano, S.; Yamaguchi, M.; Arisawa, K. Relationships of elevated levels of serum hepatic enzymes and alcohol intake with arterial stiffness in men. Atherosclerosis 2015, 238, 83–88. [Google Scholar] [CrossRef]
- Karatzi, K.; Rontoyanni, V.G.; Protogerou, A.D.; Georgoulia, A.; Xenos, K.; Chrysou, J.; Sfikakis, P.P.; Sidossis, L.S. Acute effects of beer on endothelial function and hemodynamics: a single-blind, crossover study in healthy volunteers. Nutrition 2013, 29, 1122–1126. [Google Scholar] [CrossRef]
- Tanaka, H.; Safar, M.E. Influence of lifestyle modification on arterial stiffness and wave reflections. American Journal of Hypertension 2005, 18, 137–144. [Google Scholar] [CrossRef]
- Castaldo, L.; Narvaez, A.; Izzo, L.; Graziani, G.; Gaspari, A.; Minno, G.D.; Ritieni, A. Red Wine Consumption and Cardiovascular Health. Molecules 2019, 24. [Google Scholar] [CrossRef]
- Hines, L.M.; Rimm, E.B. Moderate alcohol consumption and coronary heart disease: a review. Postgraduate Medical Journal 2001, 77, 747–752. [Google Scholar] [CrossRef]
Figure 1.
Marginal means of arterial stiffness parameters. Overall and sex-stratified marginal means according to alcohol consumption, adjusted for age, physical activity, and Mediterranean diet adherence. (a): cf-PWV; (b): ba-PWV; (c): CAVI.
Figure 1.
Marginal means of arterial stiffness parameters. Overall and sex-stratified marginal means according to alcohol consumption, adjusted for age, physical activity, and Mediterranean diet adherence. (a): cf-PWV; (b): ba-PWV; (c): CAVI.
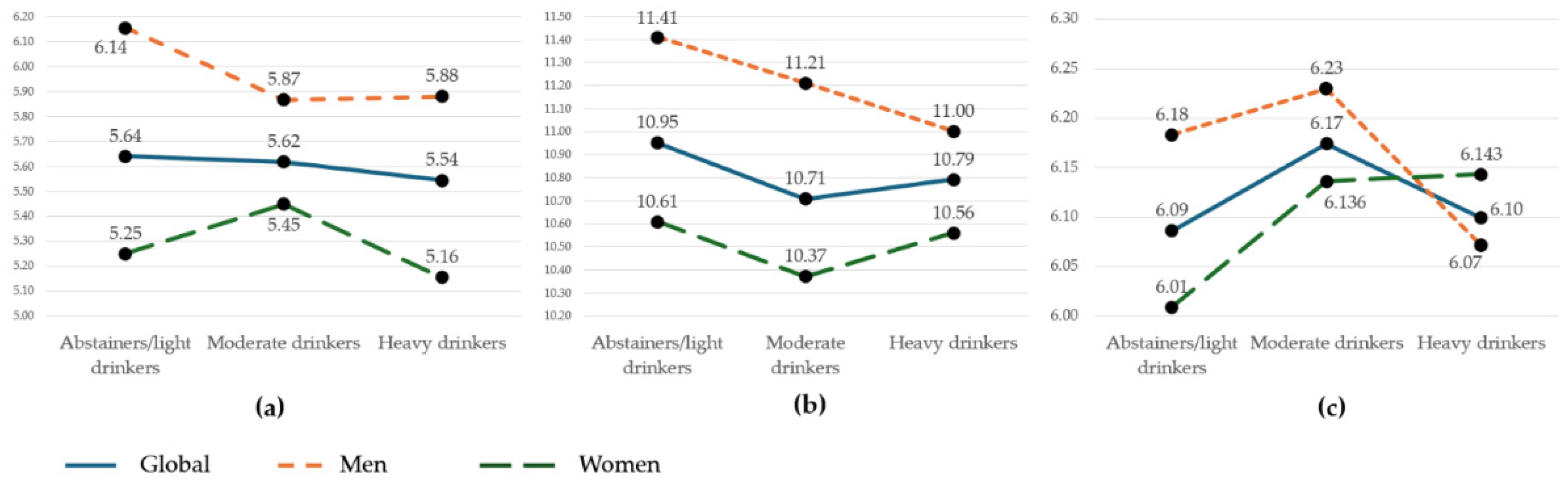
Figure 2.
AUDIT results. Graphs show the total population according to alcohol consumption risk: overall (a), men (b), and women (c).
Figure 2.
AUDIT results. Graphs show the total population according to alcohol consumption risk: overall (a), men (b), and women (c).
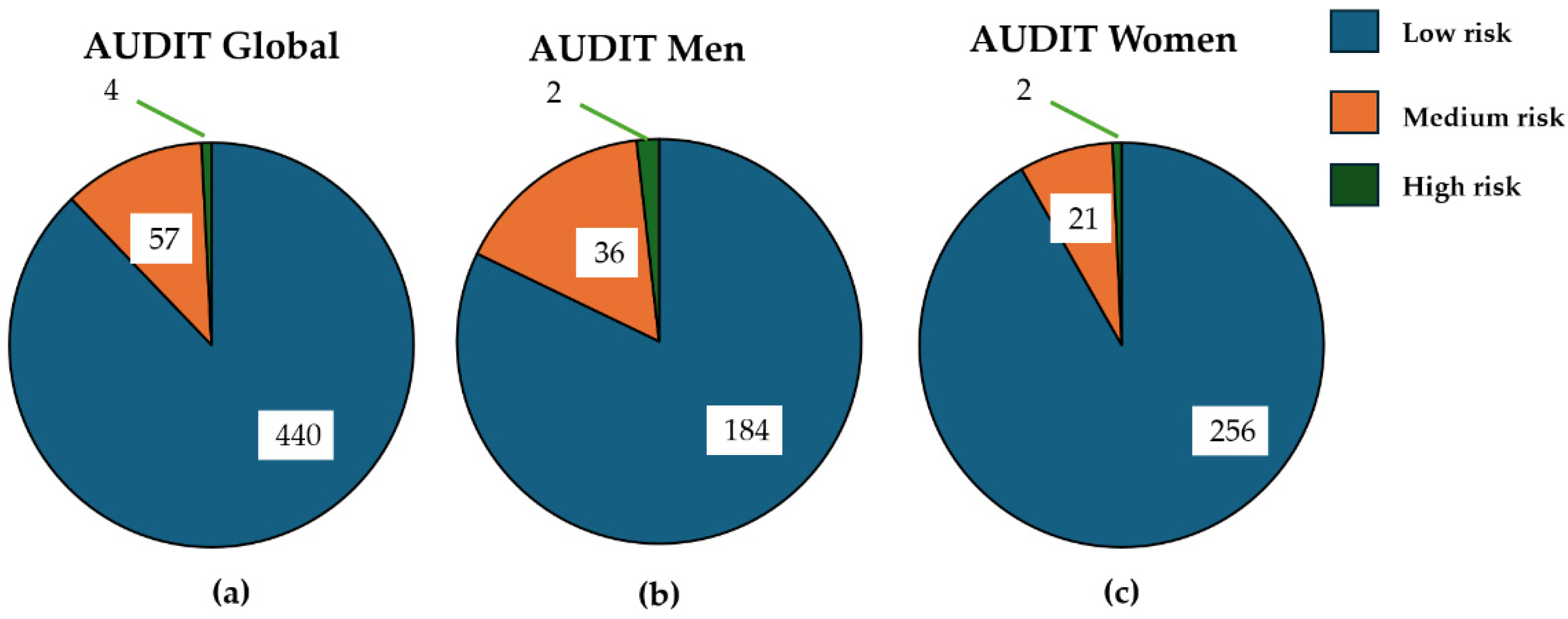
Figure 3.
Association between alcohol consumption and arterial stiffness measurements. Multinomial regression analysis using alcohol consumption as the dependent variable and cf-PWV, ba-PWV, and CAVI as independent variables. Adjusted for age, sex, Mediterranean diet adherence, physical activity, pulse pressure, fasting glucose, LDL cholesterol, and waist circumference. cf-PWV: carotid–femoral pulse wave velocity; ba-PWV: brachial–ankle pulse wave velocity; CAVI: cardio-ankle vascular index. *p < 0.05.
Figure 3.
Association between alcohol consumption and arterial stiffness measurements. Multinomial regression analysis using alcohol consumption as the dependent variable and cf-PWV, ba-PWV, and CAVI as independent variables. Adjusted for age, sex, Mediterranean diet adherence, physical activity, pulse pressure, fasting glucose, LDL cholesterol, and waist circumference. cf-PWV: carotid–femoral pulse wave velocity; ba-PWV: brachial–ankle pulse wave velocity; CAVI: cardio-ankle vascular index. *p < 0.05.
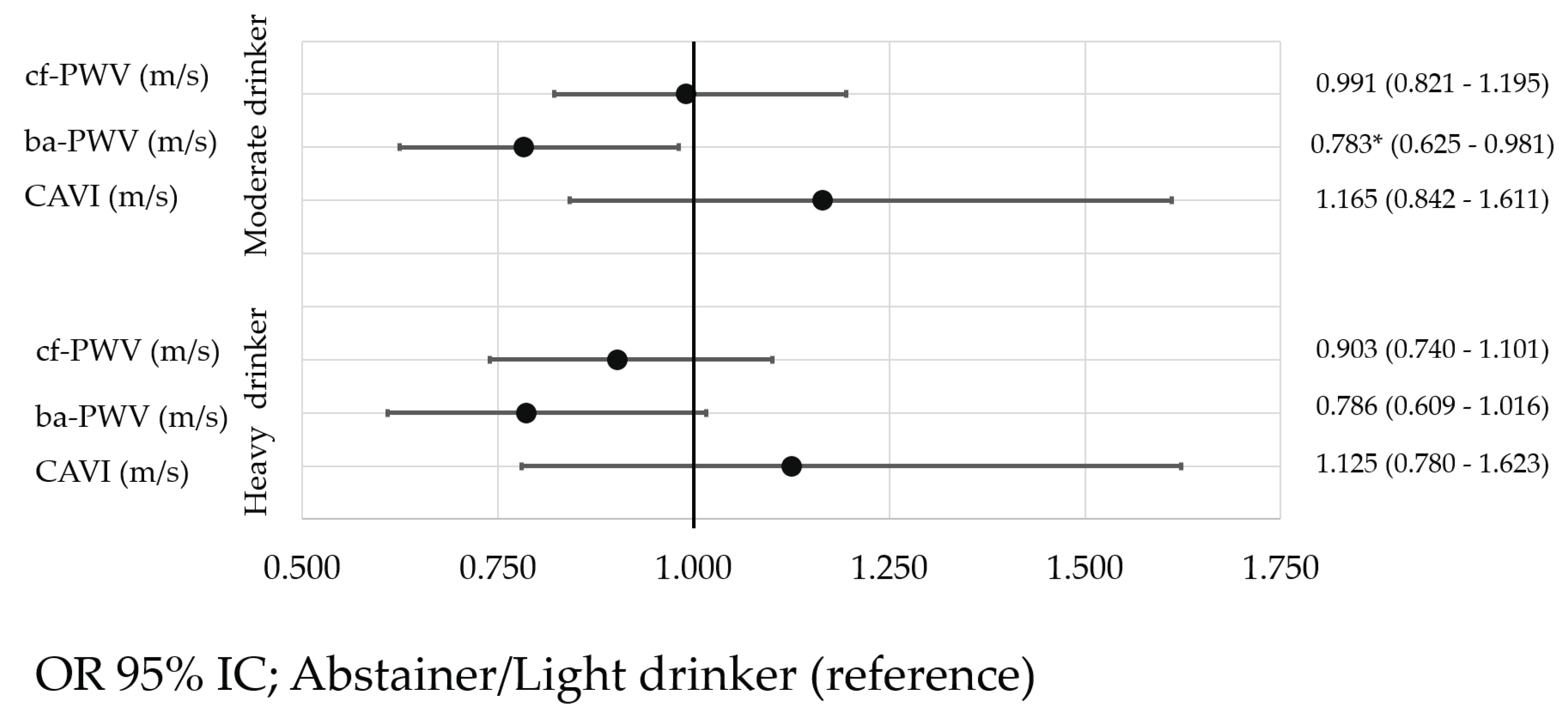

Table 1.
General characteristics of participants, overall and by sex.
| . | Global (n = 501) | Men (n=222) | Women (n=279) | ||||
|---|---|---|---|---|---|---|---|
| Mean o n | DS o % | Mean o n | DS o % | Mean o n | DS o % | p-Value | |
| Age (years) | 26.58 | 4.40 | 27.04 | 4.41 | 26.22 | 4.37 | 0.040 |
| Lifestyle | |||||||
| Alcohol (g/week) | 48.80 | 73.59 | 61.54 | 91.14 | 38.66 | 53.90 | < 0.001 |
| Smokers. n (%) | 70 | 14.0 | 28 | 12.61 | 42 | 15.05 | 0.434 |
| Cigarettes/day | 9.05 | 7.31 | 10.56 | 7.39 | 7.92 | 7.10 | 0.042 |
| MD (total score) | 7.44 | 2.01 | 6.96 | 2.06 | 7.81 | 1.88 | < 0.001 |
| METS/min/week | 2651 | 2490 | 3159 | 3130 | 2248 | 1730 | < 0.001 |
| Risk factors | |||||||
| Total cholesterol (mg/dL) | 170.16 | 28.66 | 170.98 | 29.77 | 169.52 | 27.79 | 0.573 |
| LDL (mg/dL) | 96.13 | 25.97 | 101.83 | 28.47 | 91.50 | 22.78 | < 0.001 |
| HDL (mg/dL) | 58.30 | 12.85 | 52.20 | 10.84 | 63.12 | 12.26 | < 0.001 |
| Triglycerides (mg/dL) | 83.11 | 44.24 | 95.55 | 55.70 | 73.19 | 28.80 | < 0.001 |
| Glucose (mg/dL) | 81.10 | 12.43 | 82.35 | 16.20 | 80.09 | 8.18 | 0.044 |
| SBP (mmHg) | 110.94 | 11.56 | 118.61 | 10.29 | 104.84 | 8.46 | < 0.001 |
| DBP (mmHg) | 68.08 | 7.78 | 70.15 | 8.11 | 66.44 | 7.11 | < 0.001 |
| PP (mmHg) | 42.86 | 8.45 | 48.47 | 7.90 | 38.39 | 5.81 | < 0.001 |
| BMI (kg/m2) | 24.04 | 3.80 | 25.30 | 3.65 | 23.03 | 3.63 | < 0.001 |
| Waist circumference (cm) | 79.39 | 11.50 | 85.23 | 10.58 | 74.74 | 9.99 | < 0.001 |
| Arterial stiffness | |||||||
| CAVI | 6.13 | 0.75 | 6.16 | 0.75 | 6.10 | 0.74 | 0.341 |
| cf-PWV (m/s) | 5.60 | 1.29 | 5.95 | 1.18 | 5.33 | 1.30 | < 0.001 |
| ba-PWV (m/s) | 10.80 | 1.01 | 11.20 | 1.05 | 10.48 | 0.84 | < 0.001 |
Continuous variables are expressed as mean ± standard deviation, and categorical variables as numbers and percentages. MD: Mediterranean diet; MET: metabolic equivalent of task; SBP: systolic blood pressure; DBP: diastolic blood pressure; PP: pulse pressure; BMI: body mass index; CAVI: cardio-ankle vascular index; cf-PWV: carotid–femoral pulse wave velocity; ba-PWV: brachial–ankle pulse wave velocity; p value: differences between men and women.
Table 2.
Participant characteristics according to alcohol consumption tertiles.
| . | Abstainers/light drinkers (1st tertile) (n = 142) |
Moderate drinkers (2nd tertile) (n=226) |
Heavy drinkers (3rd tertile) (n=133) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean o n | DS o % | Mean o n | DS o % | Mean o n | DS o % | p Value | |||
| Age (years) | 26.39 | 4.65 | 26.84 | 4.35 | 26.35 | 4.22 | 0.505 | ||
| Lifestyle | |||||||||
| Smokers. n (%) | 30 | (21.12) | 48 | (21.23) | 50 | (37.59) | |||
| Cigarettes/day | 10.37 | 7.26 | 9.06 | 7.17 | 8.26 | 7.51 | 0.463 | ||
| MD (total score) | 7.50 | 1.98 | 7.57 | 1.95 | 7.14 | 2.11 | 0.135 | ||
| METS/min/week | 3002.10 | 2706 | 2459 | 1802 | 2604 | 3151 | 0.121 | ||
| Risk factors | |||||||||
| Total cholesterol (mg/dL) | 171.11 | 30.89 | 170.70 | 28.62 | 168.22 | 26.25 | 0.660 | ||
| LDL (mg/dL) | 97.30 | 28.47 | 97.33 | 25.12 | 92.77 | 24.41 | 0.235 | ||
| HDL (mg/dL) | 57.51 | 12.54 | 58.85 | 12.90 | 58.20 | 13.14 | 0.621 | ||
| Triglycerides (mg/dL) | 86.51 | 43.92 | 78.82 | 43.36 | 86.85 | 45.74 | 0.143 | ||
| Glucose (mg/dL) | 82.25 | 15.51 | 79.91 | 8.47 | 81.89 | 14.22 | 0.149 | ||
| SBP (mmHg) | 111.26 | 12.30 | 109.64 | 11.41 | 112.82 | 10.77 | 0.039 | ||
| DBP (mmHg) | 68.68 | 7.99 | 67.73 | 7.72 | 68.05 | 7.67 | 0.526 | ||
| PP (mmHg) | 42.58 | 9.12 | 41.91 | 7.86 | 44.77 | 8.43 | 0.007 | ||
| BMI (kg/m2) | 24.08 | 4.28 | 23.72 | 3.82 | 24.53 | 3.16 | 0.149 | ||
| Waist circumference (cm) | 78.97 | 12.27 | 78.38 | 11.41 | 81.55 | 10.55 | 0.037 | ||
| Arterial stiffness | |||||||||
| CAVI | 6.08 | 0.85 | 6.18 | 0.73 | 6.09 | 0.66 | 0.315 | ||
| cf-PWV (m/s) | 5.63 | 1.19 | 5.62 | 1.01 | 5.55 | 1.74 | 0.839 | ||
| ba-PWV (m/s) | 10.95 | 1.07 | 10.71 | 0.97 | 10.80 | 0.98 | 0.076 | ||
Values are expressed as mean ± standard deviation for continuous variables and as numbers and percentages for categorical variables. MD: Mediterranean diet; MET: metabolic equivalent of task; SBP: systolic blood pressure; DBP: diastolic blood pressure; PP: pulse pressure; BMI: body mass index; CAVI: cardio-ankle vascular index; cf-PWV: carotid–femoral pulse wave velocity; ba-PWV: brachial–ankle pulse wave velocity; p value: differences between consumption groups.
Table 3.
Characteristics of men according to alcohol consumption tertiles.
| . | Abstainers/light drinkers (1st tertile) (n = 61) |
Moderate drinkers (2nd tertile) (n=88) |
Heavy drinkers (3rd tertile) (n=73) |
||||
|---|---|---|---|---|---|---|---|
| Mean o n | DS o % | Mean o n | DS o % | Mean o n | DS o % | p Value | |
| Age (years) | 26.03 | 4.92 | 27.74 | 4.25 | 27.03 | 4.03 | 0.067 |
| Lifestyle | |||||||
| Smokers. n (%) | 11 | (18.03) | 21 | (23.86) | 23 | (31.51) | |
| Cigarettes/day | 11.27 | 7.23 | 10.43 | 8.61 | 10.35 | 6.52 | 0.940 |
| MD (total score) | 7.20 | 1.91 | 7.00 | 2.19 | 6.73 | 2.03 | 0.413 |
| METS/min/week | 4011 | 3423 | 2704 | 1883 | 2996 | 3890 | 0.037 |
| Risk factors | |||||||
| Total cholesterol (mg/dL) | 167.92 | 33.45 | 175.10 | 29.62 | 168.49 | 26.22 | 0.244 |
| LDL (mg/dL) | 99.74 | 31.32 | 106.62 | 28.37 | 97.77 | 25.40 | 0.120 |
| HDL (mg/dL) | 51.87 | 11.57 | 52.78 | 11.68 | 51.77 | 9.12 | 0.813 |
| Triglycerides (mg/dL) | 94.15 | 53.17 | 94.57 | 59.16 | 97.97 | 54.08 | 0.906 |
| Glucose (mg/dL) | 83.72 | 21.96 | 80.10 | 8.03 | 83.94 | 17.79 | 0.244 |
| SBP (mmHg) | 118.94 | 11.83 | 118.73 | 9.86 | 118.21 | 9.52 | 0.911 |
| DBP (mmHg) | 70.05 | 8.27 | 70.93 | 8.11 | 69.29 | 7.98 | 0.442 |
| PP (mmHg) | 48.89 | 8.67 | 47.80 | 7.42 | 48.92 | 7.83 | 0.596 |
| BMI (kg/m2) | 24.92 | 3.92 | 25.59 | 3.96 | 25.25 | 2.97 | 0.542 |
| Waist circumference (cm) | 83.20 | 11.46 | 86.19 | 10.57 | 85.76 | 9.72 | 0.209 |
| Arterial stiffness | |||||||
| CAVI | 6.14 | 0.89 | 6.26 | 0.71 | 6.07 | 0.65 | 0.260 |
| cf-PWV (m/s) | 6.10 | 1.32 | 5.91 | 1.06 | 5.88 | 1.22 | 0.528 |
| ba-PWV (m/s) | 11.38 | 1.08 | 11.22 | 1.05 | 11.01 | 1.02 | 0.118 |
Values are expressed as mean ± standard deviation for continuous variables and as numbers and percentages for categorical variables. MD: Mediterranean diet; MET: metabolic equivalent of task; SBP: systolic blood pressure; DBP: diastolic blood pressure; PP: pulse pressure; BMI: body mass index; CAVI: cardio-ankle vascular index; cf-PWV: carotid–femoral pulse wave velocity; ba-PWV: brachial–ankle pulse wave velocity; p value: differences between consumption groups.
Table 4.
Characteristics of women according to alcohol consumption tertiles.
| . | Abstainers/light drinkers (1st tertile) (n = 81) |
Moderate drinkers (2nd tertile) (n=138 |
Heavy drinkers (3rd tertile) (n=60) |
||||
|---|---|---|---|---|---|---|---|
| Mean o n | DS o % | Mean o n | DS o % | Mean o n | DS o % | p-Value | |
| Age (years) | 26.67 | 4.46 | 26.26 | 4.33 | 25.53 | 4.33 | 0.312 |
| Lifestyle | |||||||
| Smokers. n (%) | 19 | 31.14 | 27 | 30.68 | 27 | 36.99 | |
| Cigarettes/day | 9.84 | 7.42 | 8.00 | 5.76 | 6.48 | 7.95 | 0.289 |
| MD (total score) | 7.73 | 2.01 | 7.93 | 1.70 | 7.65 | 2.11 | 0.553 |
| METS/min/week | 2242.38 | 1661.20 | 2302.70 | 1737.95 | 2128.19 | 1824.36 | 0.809 |
| Risk factors | |||||||
| Total cholesterol (mg/dL) | 173.54 | 28.78 | 167.89 | 27.71 | 167.90 | 26.50 | 0.310 |
| LDL (mg/dL) | 95.41 | 26.12 | 91.31 | 20.75 | 86.54 | 21.77 | 0.080 |
| HDL (mg/dL) | 61.81 | 11.55 | 62.68 | 12.17 | 65.93 | 13.12 | 0.123 |
| Triglycerides (mg/dL) | 80.69 | 34.52 | 68.70 | 24.37 | 73.47 | 28.11 | 0.012 |
| Glucose (mg/dL) | 81.13 | 7.58 | 79.78 | 8.76 | 79.43 | 7.54 | 0.395 |
| SBP (mmHg) | 105.47 | 9.09 | 103.84 | 8.08 | 106.26 | 8.32 | 0.133 |
| DBP (mmHg) | 67.64 | 7.66 | 65.70 | 6.73 | 66.53 | 7.06 | 0.147 |
| PP (mmHg) | 37.83 | 6.07 | 38.15 | 5.47 | 39.73 | 6.09 | 0.124 |
| BMI (kg/m2) | 23.45 | 4.44 | 22.52 | 3.20 | 23.65 | 3.19 | 0.063 |
| Waist circumference (cm) | 75.78 | 11.96 | 73.41 | 8.88 | 76.42 | 9.22 | 0.081 |
| Arterial stiffness | |||||||
| CAVI | 6.03 | 0.82 | 6.14 | 0.73 | 6.11 | 0.67 | 0.582 |
| cf-PWV (m/s) | 5.27 | 0.95 | 5.44 | 0.94 | 5.14 | 2.16 | 0.295 |
| ba-PWV (m/s) | 10.62 | 0.94 | 10.37 | 0.75 | 10.54 | 0.88 | 0.092 |
Values are expressed as mean ± standard deviation for continuous variables and as numbers and percentages for categorical variables. MD: Mediterranean diet; MET: metabolic equivalent of task; SBP: systolic blood pressure; DBP: diastolic blood pressure; PP: pulse pressure; BMI: body mass index; CAVI: cardio-ankle vascular index; cf-PWV: carotid–femoral pulse wave velocity; ba-PWV: brachial–ankle pulse wave velocity; p value: differences between consumption groups.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



