
Submitted:
20 August 2025
Posted:
21 August 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background/Objectives: Blood is often the first organ to show changes during local or systemic infection, but common definitions of sepsis rarely include CBC findings in risk assessment tools. Infection remains the main cause of sepsis, which Sepsis-3 defines as life-threatening organ dysfunction from a dysregulated immune response. Changes in circulating monocytes—such as altered MDW and increased inflammation—can be seen in sepsis and SARS-COV-2. This study evaluates MDW as a blood marker for detecting infections and compares it with traditional markers for risk stratification. Methods: From December 2021 to December 2023, 608 adults with suspected infection or sepsis were enrolled at San Donato Hospital's Emergency Department in Arezzo. All patients were admitted and monitored in assigned wards, with destination, history, clinical, and lab data collected during their stay and follow-up. Results: Monocyte Distribution Width (MDW) detects bloodstream infection with high efficacy (sensitivity 92%, specificity 85%, and negative predictive value 95% at ER admission). MDW also stratifies risk for infections that may progress to sepsis—including urinary, respiratory, post-surgical, and wound infections—with sensitivity, specificity, and negative predictive value around 70–72%. Conclusions: Blood is usually the first organ to show changes during infection, with blood cell morphology and CBC parameters affected by bacterial, viral, or fungal pathogens. Techniques like flow cytometry and impedance measurements provide Cell Population Data (CPD), such as MDW, which support diagnostic algorithms for infection or sepsis. CPDs are well-suited for AI analysis, and the extensive information from CBCs should be integrated into both diagnosis and treatment.
Keywords:
monocyte distribution width
; MDW
; complete blood count
; bloodstream infections
; cell population data
; SARS-CoV-2
; procalcitonin
; infection disease
; sepsis
Introduction
Numerous studies indicate that changes in specific blood cell populations, as detected by Complete Blood Count (CBC), may be relevant in infections, particularly when sepsis is suspected [1,2]. Blood is typically the first organ affected and altered in response to both local and systemic infection. However, various definitions and documentation concerning sepsis or infection have not included these CBC findings in study or report, and no related parameters have been incorporated into algorithms or scoring systems for risk stratification.
In both recent and older publications addressing sepsis, the primary cause is consistently identified as infection by an external agent. Notably, The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) recommends: "Sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection." From this definition, it can be inferred that, starting from the initial infection, various systems and organs are progressively affected by this syndrome, with the resultant impairments constituting sequelae that can lead to severe consequences, including death. Sepsis, induced by infection, represents a significant public health issue. The definitions of sepsis and septic shock were updated in January 2016 with the objective of identifying patients at higher risk of adverse outcomes, particularly those requiring intensive care unit (ICU) treatment or having a high risk of mortality [3,4].
Previously, a sepsis diagnosis necessitated the presence of infection along with two or more systemic inflammatory response syndrome (SIRS) criteria; when accompanied by organ dysfunction, this was termed 'severe sepsis'. The updated definition no longer considers the presence of infection and SIRS sufficient for a sepsis diagnosis. Instead, sepsis now requires an infection plus organ dysfunction, indicated by an acute change in Sequential Organ Failure Assessment (SOFA) score of two points or more. Thus, what was previously termed 'severe sepsis' is now classified as 'sepsis,' with the new definition providing specific criteria for identifying qualifying organ dysfunction for the first time. The most severe form of sepsis is septic shock, characterized by circulatory failure in patients with sepsis, where circulatory, cellular, and metabolic abnormalities are associated with an increased risk of death [5,6,7].
Bloodstream infections (BSIs) remain a major type of infection and represent a critical medical challenge with significant morbidity and mortality rates . The pathogenesis of these infections involves complex microbiological and immunological mechanisms, typically initiated by the translocation of pathogenic microorganisms from localized infection sites, such as the lungs, urinary tract, skin or catheter, into the bloodstream [8,9,10,11,12].
BSIs account for at least of 40% of acquired (community or hospital) sepsis and septic shock cases, and approximately 20% of ICU-acquired cases. In critically ill patients, BSI can be imported (documented at ICU admission) or acquired in the ICU, occurring in approximately 25% and 75% of cases, respectively. These infections are invariably associated with poor outcomes, especially when there is a delay in adequate antimicrobial therapy and source control.
Overall, ICU-acquired BSIs occur in 5-7% of admissions, corresponding to an average of 6-10 episodes per 1,000 patient-days. Key risk factors for ICU-acquired BSIs include high severity indices at admission, prolonged ICU stay, immunosuppression, liver disease, surgical admission, and the need for invasive devices or procedures. The EUROBACT-1 international study reported that ICU-acquired BSIs primarily resulted from catheter-related infections (21%), nosocomial pneumonia (21%), and intra-abdominal infections (12%); notably, no definitive source was identified for 24% of episodes [13].
Monocyte Distribution Width (MDW) assesses the variation in monocyte size within the bloodstream and has been introduced as a diagnostic tool for sepsis in Emergency Departments and Intensive Care Units. MDW is valued for its rapid response to pathogenic stimuli and its accessibility via routine blood testing [14,15,16,17,18,19,20]. Infection induces functional changes in circulating monocytes, which are reflected by alterations in MDW, monocyte anisocytosis, and heightened inflammation or cytokine storms observed in conditions such as sepsis and Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-COV-2). Monitoring MDW in patients admitted with sepsis, including those with SARS-COV-2, throughout their hospitalization may provide prognostic insights regarding potential adverse outcomes [21,22]. Numerous studies have described the efficacy of MDW in detecting bacterial, fungal, and viral infections [23,24,25]. If validated, MDW could serve as a reliable parameter for risk stratification and for monitoring infection progression and tissue damage in emergency room and ICU settings, particularly among vulnerable patient groups. This study investigates the effectiveness of MDW as a blood marker for identifying localized or systemic infections as part of risk stratification and compares its performance to traditional markers. The aim is to enhance early detection of infections to prevent the onset of sepsis and septic shock.
Material and Method
Patient Enrolment
Patients with clinical presentations of suspected infection or sepsis were enrolled in the Emergency Department of San Donato Hospital in Arezzo between December 2021 and December 2023. Six hundred and eight patients over the age of 18 were included in the study. All 608 patients were admitted to the Emergency Department and followed up in the assigned wards.
Destination, history, clinical, and laboratory data were collected for all enrolled patients during their admission to the Emergency Department and during follow-up in the inpatient wards. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the local ethics committee (Prot. No. 14911 Arezzo MDW_SEPSI 28/06/2021).
Laboratory Parameters
Upon admission to the Emergency Department, patients underwent a comprehensive series of tests, including procalcitonin (PCT), C-reactive protein (CRP), monocyte distribution width (MDW), complete blood count (CBC) with differential white blood cell count, estimated glomerular filtration rate (eGFR, CKD-EPI), creatinine, urea, sodium, potassium, glucose, total protein, lactate dehydrogenase (LDH), aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin, and a nasopharyngeal swab for SARS-CoV-2 diagnosis via RT-PCR. Clinical chemistry tests used serum samples analysed with the Cobas 8000 (Roche Diagnostic). CBC, differential WBC count, and MDW were measured from whole blood with K2EDTA using the UniCel DxH 900 (Beckman Coulter) within 2 hours. Blood, urine cultures, and other microbiological tests were routinely performed in at-risk patients to monitor for infections.
Statistical Analysis
Microsoft Excel, MedCalc 23.024 version (MedCalc LTD), and SPSS 20.0 (IBM) software were used for data collection, storage, and statistical analysis. The Kolmogorov–Smirnov test was applied to assess the normality of the distribution of the data. Quantitative variables are presented as mean and standard deviation (SD), while categorical variables are presented as absolute and relative frequencies. Group differences were analyzed using the parametric T-test for continuous variables and the nonparametric Mann–Whitney U test for categorical variables. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive and negative likelihood ratios (LR+ and LR-, respectively), and the area under the curve (AUC) of the ROC analysis were calculated.
Results
Six hundred and eight subjects were enrolled (235 female and 373 male), with a mean ±SD age of 70.9 ±13.9 years. The principal characteristics of the enrolled patients, divided by gender are shown in Table 1; there were no significant differences except for creatinine, GFR and all CBC parameters (except MPV).
Among 608 subjects, 196 had no infection, 134 tested positive via blood culture, and 235 had localized infections (urine, wound, or respiratory). An additional 43 severe SARS-COV-2 cases were grouped with the blood culture positives.
Table 2 summarizes group characteristics and compares variables across these populations. Age, leukocytes and neutrophils did not show statistically significant differences between the three groups; while PCT, MDW and PCR were statistically different between all groups.
Notably, age, leukocytes, and neutrophils did not exhibit statistically significant differences among the three groups. However, PCT, MDW, and PCR demonstrated statistically significant differences across all groups. Patients with bloodstream-positive infections and those with localized infections showed statistically significant differences from the non-infected group in PCT, PCR, MDW, as well as erythrocytes, haemoglobin, and haematocrit. Moreover, patients with bloodstream-positive infections also exhibited statistically significant differences compared to non-infected patients or those with localized infections in lymphocytes, basophils, monocytes, and platelets counts. Lastly, eosinophils and MPV presented statistically significant differences when comparing subjects with localized infections to non-infected individuals and those with bloodstream-positive infections (slight significance), and non-infected individuals to those with localized infections, respectively.
Table 3 and Figure 1 present the results obtained from the ROC analysis. Specifically, Figure 1 illustrate the AUC for each parameter (MDW, PCT, and PCR), representing diagnostic efficacy across groups with different types of infections. MDW, identified as the most effective parameter, detects both localized and widespread infections, regardless of whether they are viral, bacterial, or fungal in nature. This is followed by PCT and PCR in terms of effectiveness. Table 3 summarizes the performance values, highlighting the significant statistical differences between them.
The Youden index (Table 4) identifies the most effective cutoffs in terms of sensitivity, specificity, predictivity, and likelihood ratio.
Discussion
Multiple lines of evidence now conclusively demonstrate that sepsis results from the host’s response to infection, which is intended to eliminate invading pathogens. Consequently, clinical outcomes in sepsis are influenced not only by the pathogenicity and viability of the infectious agents—which can directly cause tissue damage—but also, and perhaps more significantly, by the host’s immune response. This response, if excessive, may lead to unintended organ and tissue injury, as potent immune effectors may affect both microbial invaders and the host’s own tissues indiscriminately [23].
However, some researchers suggest that the actual incidence of sepsis may be overestimated in numerous studies. Notably, a significant proportion of patients enrolled in clinical sepsis trials might lack probable or confirmed infection, which could diminish the statistical power of these studies to demonstrate the efficacy of specific treatments. Furthermore, the initial clinical diagnosis of sepsis often correlates poorly with infection when assessed using rigorous diagnostic criteria [26,27].
Now, lack a precise definition of the dysregulated host response and a diagnostic test to confirm its presence. Moreover, we have limited ability to confirm or characterize infection in real time. Up to one third of patients who have been treated for presumed bacterial sepsis had a non-infectious illness in hindsight. Even among patients with sepsis, the cause of the infection is not determined in up to one third of cases [28].
BSIs are a common type of infection and present a medical challenge associated with measurable morbidity and mortality rates [9,10,11,12].
The development of these infections involves microbiological and immunological mechanisms, typically beginning with the movement of pathogenic microorganisms from localized sites—such as the lungs, urinary tract, skin, or catheter—into the bloodstream. Various microbial organisms, including Gram-positive and Gram-negative bacteria and certain fungal species, can cause these infections. Management involves timely source control and selection of antimicrobial agents based on individual risk factors and local resistance patterns [29]. Antimicrobial stewardship is important for guiding appropriate antibiotic use, covering both the choice of agent and duration of treatment. Optimizing antibiotic duration for BSIs is a key aspect, as both prolonged and insufficient therapy can lead to adverse outcomes [30,31,32,33].
The primary finding of this study is the capacity of the Monocyte Distribution Width (MDW) to detect BSI with a high degree of efficacy: sensitivity, specificity, and negative predictive value were 92%, 85%, and 95%, respectively, upon emergency room admission. Additionally, MDW demonstrates utility in stratifying infection risk for localised infectious outbreaks that may progress to sepsis (such as urinary tract, respiratory tract, post-surgical cases, and wound infections), yielding sensitivity, specificity, and negative predictive value of 70%, 72%, and 72%, respectively. Although performance in these scenarios is lower compared to bloodstream infections, it remains significant, particularly given the marker's ability to track infection progression. These findings endorse MDW as a valuable tool for early microbiological investigation and for effective prevention of complications leading to sepsis and septic shock. Addictionaly, MDW exhibits progressive values corresponding to the severity of pathology, demonstrating marked increases from localized infection through BSI, sepsis or septic shock, and ultimately to mortality. These findings support those reported by other researchers who have investigated this marker [19,23,25].
Furthermore, results corroborate the progressive response of monocytes to histones, as demonstrated by time- and dose-dependent increases in MDW [34]. Notably, significant changes were observed even at the lowest histone concentration (50 μg/mL) within 30 minutes. This indicates that histones have an immediate and pronounced effect on circulating monocytes, primarily influencing cell morphology, such as volume, cytoplasmic granularity, vacuolization, and nuclear structure which are reflected in changes to the MDW parameter, without altering monocyte count [35,36].
As noted in the introduction, numerous studies have demonstrated that alterations in specific blood cell populations, as identified by CBC, may hold clinical significance in the context of infections, especially when sepsis is suspected [1,2]. Blood is typically the first organ affected and altered in response to both local and systemic infection.
The morphology of blood cells changes in response to the presence of bacterial, viral, or fungal pathogens, and CBC parameters are also affected during infectious processes or by the release of histones into the circulation. Recent studies have quantified the relationship between circulating histones and the degree of monocyte response. These changes are recorded by various analytical methods, such as flow cytometry or impedance measurements, and represented as positional coordinates in three-dimensional space. Advances in technology have enabled haematology analysers to provide Cell Population Data (CPD), which quantifies both morphological (volume, granularity, and complexity) and functional characteristics of blood cells. CPDs can be produced using technologies like VCS (Volume, Conductivity, Light Scatter) and fluorescence flow cytometry. Some CPDs serve as new markers (e.g., MDW, Monocyte Distribution Width), while others are incorporated into diagnostic and prognostic algorithms for sepsis. Although CPDs yield valuable information, further research is needed to clarify their clinical significance and contribution, not only in sepsis but also in other medical conditions. Their accessible nature allows them to be effectively processed with mathematical models, including those utilized in artificial intelligence for pattern recognition.
Author Contributions
Study conception and design: AO, ML; Acquisition of data: AO, ML, SM, CA; Analysis and interpretation of data: AO, ML, GC, EMP, DT, and SM; Drafting of manuscript: AO, Critical revision of manuscript: All authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received external funding by Beckman Coulter.
Institutional Review Board Statement
The study addendum was approved by the local ethics committee (Prot. No. 14911 Arezzo MDW_SEPSI 28/06/2021), Written or oral informed consent was obtained from the participants or their families.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| MDW | Monocyte distribution width; |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus-2; |
| AUC | Area under the curve; |
| ICU | Intensive care unit; |
| K2EDTA | Ethylenediaminetetraacetic acid-K2; |
| CRP | C-reactive protein; |
| PCT | Procalcitonin; |
| ROC | Receiver operating characteristic; |
| CBC | Complete Blood Count; |
| SOFA | Sequential Organ Failure Assessment; |
| CPD | Cell Population Data; |
| BSI | Bloodstream infections; |
References
- Farkas JD. The complete blood count to diagnose septic shock. J Thorac Dis. 2020 Feb;12(Suppl 1):S16-S21. [CrossRef]
- Lorubbio M. and Ognibene A. Il contributo dell’esame emocromocitometrico nella diagnosi di infezione e sepsi Biochimica Clinica, 48 (4) 381-383 - 2024.
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):801-10. [CrossRef]
- Manu Shankar-Hari 1 , Gary S Phillips 2 , Mitchell L Levy 3 , Christopher W Seymour 4 , Vincent X Liu 5 , Clifford S Deutschman 6 , Derek C Angus 7 , Gordon D Rubenfeld 8 , Mervyn Singer 9 ; Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) Sepsis Definitions Task Force JAMA . 2016 Feb 23;315(8):775-87.
- Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, Rubenfeld G, Kahn JM, Shankar-Hari M, Singer M, Deutschman CS, Escobar GJ, Angus DC. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):762-74. Erratum in: JAMA. 2016 May 24-31;315(20):2237. https://doi.org/10.1001/jama.2016.0288. [CrossRef]
- Markwart R, Saito H, Harder T, Tomczyk S, Cassini A, Fleischmann-Struzek C, Reichert F, Eckmanns T, Allegranzi B. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020 Aug;46(8):1536-1551. [CrossRef]
- Cecconi M, Evans L, Levy M, Rhodes A. Sepsis and septic shock. Lancet. 2018 Jul 7;392(10141):75-87.
- Evans T. Diagnosis and management of sepsis. Clin Med (Lond). 2018 Mar;18(2):146-149.
- Naghavi M, Vollset SE, Ikuta KS, et al. Global burden of bacterial antimicrobial resistance 1990-2021: a systematic analysis with forecasts to 2050. Lancet 2024;404:1199–226. [CrossRef]
- Verway M, Brown KA, Marchand-Austin A, et al. Prevalence and mortality associated with bloodstream organisms: a population-wide retrospective cohort study. J Clin Microbiol 2022;60(4) . [CrossRef]
- Hassoun-Kheir N, Guedes M, Ngo Nsoga MT, et al. A systematic review on the excess health risk of antibiotic-resistant bloodstream infections for six key pathogens in Europe. S14-s25 Clin Microbiol Infect 2024;30(1). [CrossRef]
- Allel K, Stone J, Undurraga EA, et al. The impact of inpatient bloodstream infections caused by antibiotic-resistant bacteria in low- and middle-income countries: A systematic review and meta-analysis. PLoS Med 2023;20:21 . [CrossRef]
- Tabah A, Koulenti D, Laupland K, Misset B, Valles J, Bruzzi de Carvalho F, Paiva JA, Cakar N, Ma X, Eggimann P, Antonelli M, Bonten MJ, Csomos A, Krueger WA, Mikstacki A, Lipman J, Depuydt P, Vesin A, Garrouste-Orgeas M, Zahar JR, Blot S, Carlet J, Brun-Buisson C, Martin C, Rello J, Dimopoulos G, Timsit JF. Characteristics and determinants of outcome of hospital-acquired bloodstream infections in intensive care units: the EUROBACT International Cohort Study. Intensive Care Med. 2012 Dec;38(12):1930-45. [CrossRef]
- Crouser ED, Parrillo JE, Seymour CW, et al. Monocyte distribution width: a novel indicator of sepsis-2 and sepsis-3 in high-risk emergency department patients. Crit Care Med 2019;47:1018–25. [CrossRef]
- Crouser ED, Parrillo JE, Martin GS, et al. Monocyte distribution width enhances early sepsis detection in the emergency department beyond SIRS and qSOFA. J Intens Care 2020;8:33. [CrossRef]
- Polilli E, Sozio F, Frattari A, et al. Comparison of monocyte distribution width (MDW) and procalcitonin for early recognition of sepsis. PLoS ONE 2020;15: . [CrossRef]
- Agnello L, Ciaccio AM, Del Ben F, Lo Sasso B, Biundo G, Giglia A, Giglio RV, Cortegiani A, Gambino CM, Ciaccio M. Monocyte distribution width (MDW) kinetic for monitoring sepsis in intensive care unit. Diagnosis (Berl). 2024 Apr 22;11(4):422-429. [CrossRef]
- Agnello L, Ciaccio AM, Vidali M, Cortegiani A, Biundo G, Gambino CM, Scazzone C, Lo Sasso B, Ciaccio M. Monocyte distribution width (MDW) in sepsis. Clin Chim Acta. 2023 Aug 1;548:117511. [CrossRef]
- Ognibene A, Lorubbio M, Montemerani S, Tacconi D, Saracini A, Fabbroni S, Parisio EM, Zanobetti M, Mandò M, D'Urso A. Monocyte distribution width and the fighting action to neutralize sepsis (FANS) score for sepsis prediction in emergency department. Clin Chim Acta. 2022 Sep 1;534:65-70. [CrossRef]
- Campagner A, Agnello L, Carobene A, Padoan A, Del Ben F, Locatelli M, Plebani M, Ognibene A, Lorubbio M, De Vecchi E, Cortegiani A, Piva E, Poz D, Curcio F, Cabitza F, Ciaccio M. Complete Blood Count and Monocyte Distribution Width-Based Machine Learning Algorithms for Sepsis Detection: Multicentric Development and External Validation Study. J Med Internet Res. 2025 Feb 26;27:e55492. [CrossRef]
- Ognibene A, Lorubbio M, Magliocca P, Tripodo E, Vaggelli G, Iannelli G, Feri M, Scala R, Tartaglia AP, Galano A, Pancrazzi A, Tacconi D. Elevated monocyte distribution width in COVID-19 patients: The contribution of the novel sepsis indicator. Clin Chim Acta. 2020 Oct;509:22-24. [CrossRef]
- Lorubbio M, Tacconi D, Iannelli G, Feri M, Scala R, Montemerani S, Mandò M, Ognibene A. The role of Monocyte Distribution Width (MDW) in the prognosis and monitoring of COVID-19 patients. Clin Biochem. 2022 May;103:29-31. [CrossRef]
- Malinovska A, Hernried B, Lin A, Badaki-Makun O, Fenstermacher K, Ervin AM, Ehrhardt S, Levin S, Hinson JS. Monocyte Distribution Width as a Diagnostic Marker for Infection: A Systematic Review and Meta-analysis. Chest. 2023 Jul;164(1):101-113.
- Huang YH, Chen CJ, Shao SC, Li CH, Hsiao CH, Niu KY, Yen CC. Comparison of the Diagnostic Accuracies of Monocyte Distribution Width, Procalcitonin, and C-Reactive Protein for Sepsis: A Systematic Review and Meta-Analysis. Crit Care Med. 2023 May 1;51(5):e106-e114. [CrossRef]
- Cusinato M, Sivayoham N, Planche T. Sensitivity and specificity of monocyte distribution width (MDW) in detecting patients with infection and sepsis in patients on sepsis pathway in the emergency department. Infection. 2023 Jun;51(3):715-727. [CrossRef]
- Reinhart K, Bauer M, Riedemann NC, Hartog CS. New approaches to sepsis: molecular diagnostics and biomarkers. Clin Microbiol Rev. 2012 Oct;25(4):609-34. [CrossRef]
- Klein Klouwenberg PM, Cremer OL, van Vught LA, Ong DS, Frencken JF, Schultz MJ, Bonten MJ, van der Poll T. Likelihood of infection in patients with presumed sepsis at the time of intensive care unit admission: a cohort study. Crit Care. 2015 Sep 7;19(1):319. [CrossRef]
- Marshall JC. Why have clinical trials in sepsis failed? Trends Mol Med 2014; 20:195–203.
- Meyer NJ, Prescott HC. Sepsis and Septic Shock. N Engl J Med. 2024 Dec 5;391(22):2133-2146.
- Gibbs AAM, Laupland KB, Edwards F, et al. Trends in Enterobacterales bloodstream infections in children. Pediatrics 2024;154. [CrossRef]
- C.J. Murray, K.S. Ikuta, F. Sharara, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis Lancet, 399 (2022) . [CrossRef]
- U. Okomo, E.N.K. Akpalu, K. Le Doare, et al. Aetiology of invasive bacterial infection and antimicrobial resistance in neonates in sub-Saharan Africa: a systematic review and meta-analysis in line with the STROBE-NI reporting guidelines Lancet Infect Dis, 19 (2019), pp. 1219-1234 . [CrossRef]
- L.Y. Leung, H.L. Huang, K.K. Hung, et al. Door-to-antibiotic time and mortality in patients with sepsis: Systematic review and meta-analysis Eur J Intern Med, 129 (2024), pp. 48-61. [CrossRef]
- Ligi D, Lo Sasso B, Della Franca C, Giglio RV, Agnello L, Ciaccio M, Mannello F. Monocyte distribution width alterations and cytokine storm are modulated by circulating histones. Clin Chem Lab Med. 2023 Feb 28;61(8):1525-1535. [CrossRef]
- Ligi D, Giglio RV, Henry BM, Lippi G, Ciaccio M, Plebani M, Mannello F. What is the impact of circulating histones in COVID-19: a systematic review. Clin Chem Lab Med. 2022 Jul 19;60(10):1506-1517. [CrossRef]
- Ligi D, Lo Sasso B, Giglio RV, Maniscalco R, DellaFranca C, Agnello L, et al. Circulating histones contribute to monocyte and MDW alterations as common mediators in classical and COVID-19 sepsis. Crit Care 2022;26:260. [CrossRef]
Figure 1.
ROC analysis: Graphic A, B, C and D showed AUCs of MDW (blue line), PCT (orange line) and PCR (green line), for overall infection, BSIs, BSIs excluded SARS-COV-2 and localized infection respectively.
Figure 1.
ROC analysis: Graphic A, B, C and D showed AUCs of MDW (blue line), PCT (orange line) and PCR (green line), for overall infection, BSIs, BSIs excluded SARS-COV-2 and localized infection respectively.
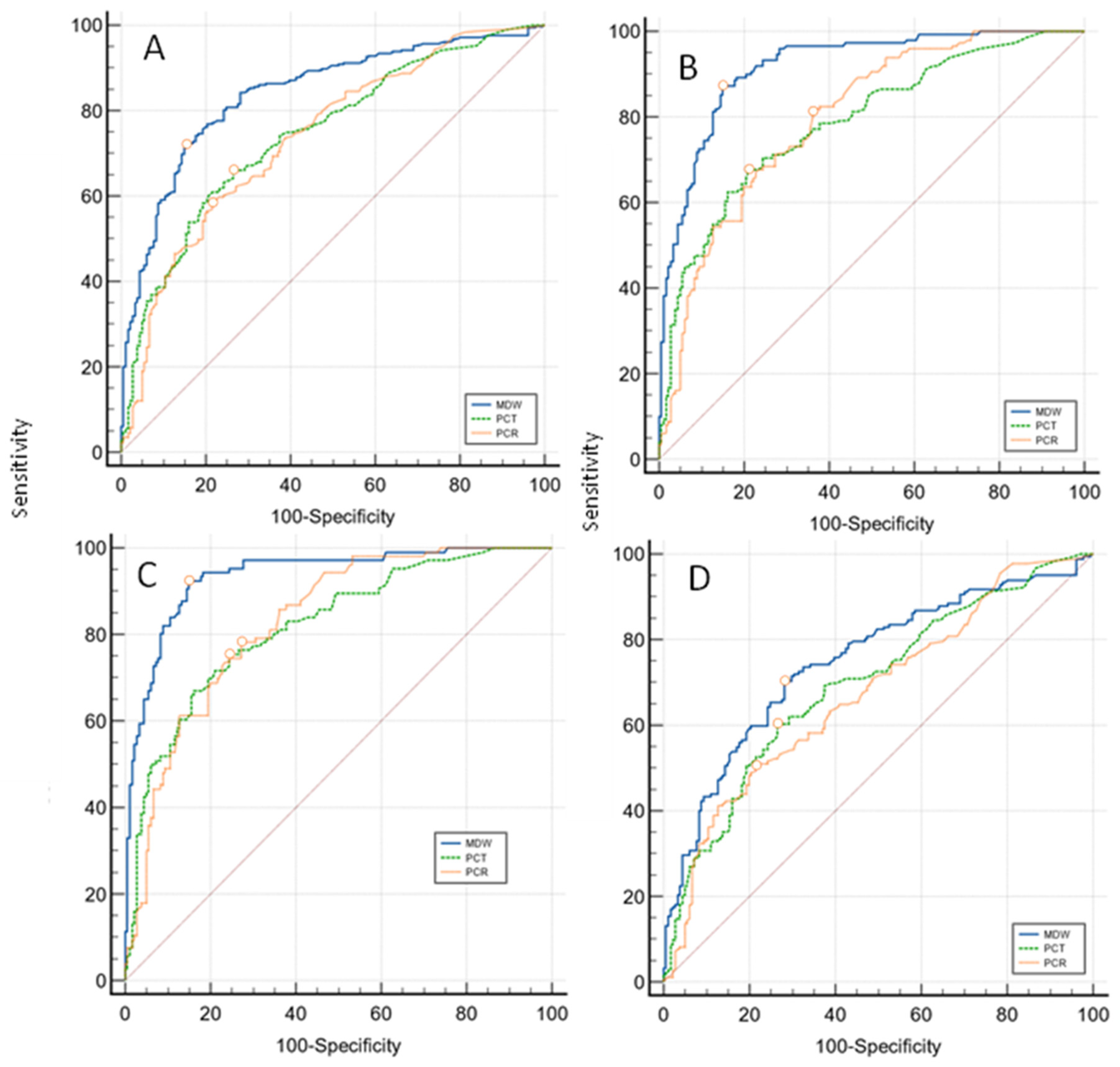
Figure 2.
MDW distribution in survivors and not-survivors.
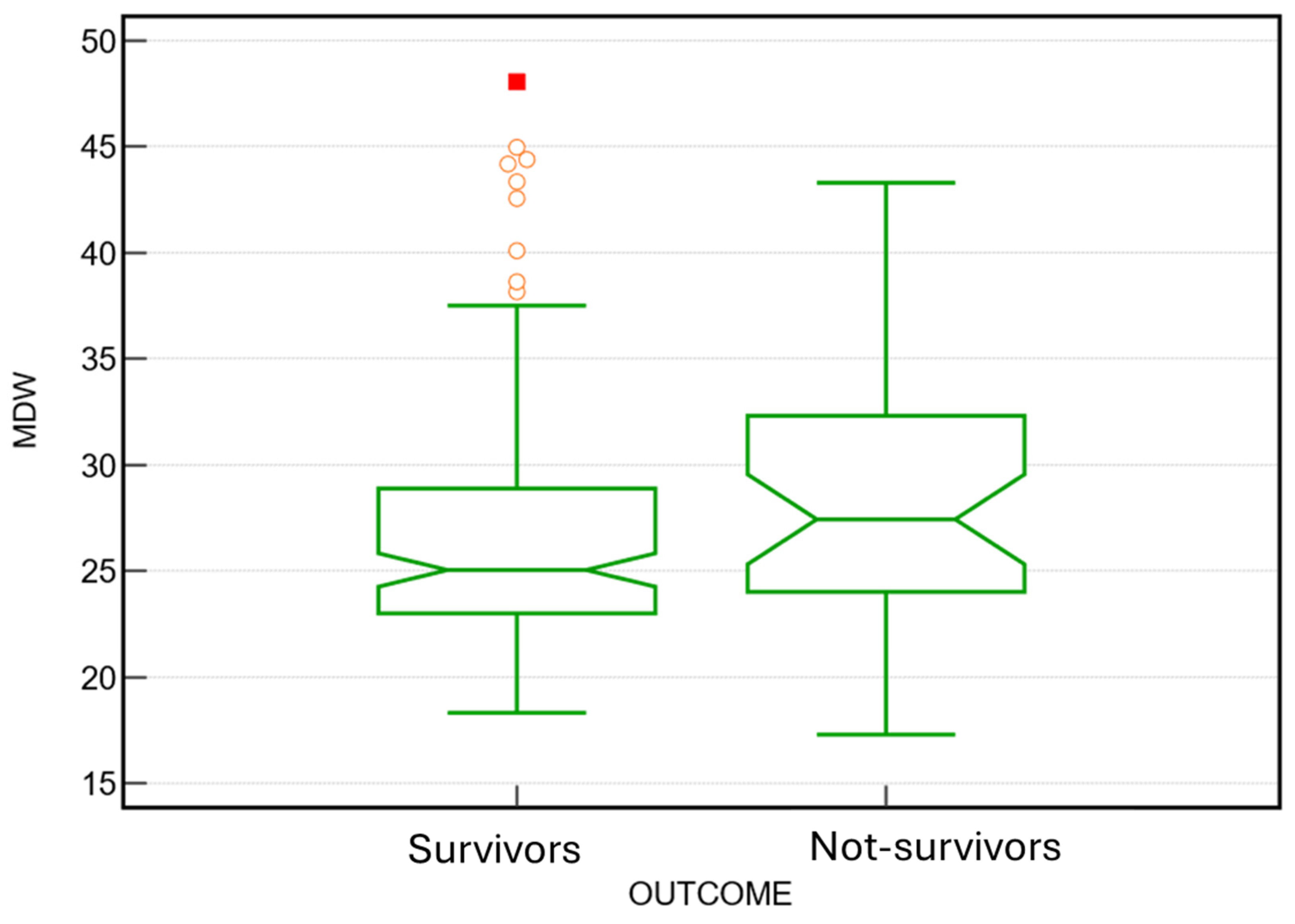

Table 1.
Characteristics of Study Subjects.
| Patient’s characteristics | |||||||
| All [N. 608] | Female [N. 235] | Male [N. 373] | |||||
| Variables | Mean | ±SD | Mean | ±SD | Mean | ±SD | P value |
| Age (years) | 70,9 | ±13,87 | 72,46 | ±12,87 | 70,02 | ±14,39 | NS |
| GFR_CKD_EPI (mL/min/1,73) | 58,04 | ±29,60 | 54,08 | ±29,41 | 60,60 | ±29,48 | <0,05 |
| Creatinine (mg/dL) | 1,57 | ±1,42 | 1,46 | ±1,25 | 1,64 | ±1,52 | <0,05 |
| Total Bilirubin (mg/dL) | 1,09 | ±2,19 | 1,10 | ±2,37 | 1,09 | ±2,07 | NS |
| Procalcitonin (PCT) (ng/mL) | 12,7 | ±39,22 | 11,08 | ±35,27 | 13,82 | ±41,57 | NS |
| Reactive C protein (PCR) (mg/dL) | 11,4 | ±9,98 | 11,32 | ±9,89 | 11,44 | ±10,06 | NS |
| MDW | 23,7 | ±6,5 | 23,77 | ±5,85 | 23,60 | ±6,95 | NS |
| WBC (109/L) | 12,91 | ±8,46 | 14,06 | ±8,02 | 12,19 | ±8,65 | <0,05 |
| RBC (1012/L) | 3,72 | ±0,775 | 3,63 | ±0,72 | 3,78 | ±0,80 | <0,05 |
| Haemoglobin (g/dL) | 11,0 | ±2,2 | 10,57 | ±1,88 | 11,27 | ±2,27 | <0,05 |
| Neutrophiles (109/L) | 10,8 | ±6,98 | 11,86 | ±7,38 | 10,14 | ±6,63 | <0,05 |
| Lymphocytes (109/L) | 1,09 | ±1,67 | 1,18 | ±1,81 | 1,035 | ±1,57 | <0,05 |
| Basophiles (109/L) | 0,023 | ±0,04 | 0,03 | ±0,043 | 0,02 | ±0,029 | <0,05 |
| Eosinophiles (109/L) | 0,07 | ±0,25 | 0,103 | ±0,37 | 0,047 | ±0,114 | <0,05 |
| Platelets (109/L) | 207,4 | ±114,3 | 225,6 | ±121,6 | 196,1 | ±108,2 | <0,05 |
| MPV (fL) | 9,8 | ±1,60 | 9,985 | ±1,63 | 9,74 | ±1,57 | NS |
| Monocytes (109/L) | 0,93 | ±4,01 | 0,86 | ±1,27 | 0,97 | ±5,02 | <0,05 |
Table 2.
Patient characteristics by infection type.
| Infection | |||||||||
| No infection [# 196] | BSIs [# 177] |
Localized infection [# 235] |
No infection vs BSIs | No infection vs Localized infection | BSIs vs Localized infection |
||||
| Mean | SD | Mean | SD | Mean | SD | P | P | P | |
| Age (years) | 69,38 | 15,46 | 72,44 | 11,88 | 71,17 | 13,77 | NS | NS | NS |
| Creatinine (mg/dL) | 1,28 | 1,15 | 1,70 | 1,39 | 1,70 | 1,60 | 0,0001 | 0,0024 | NS |
| MDW | 19,44 | 3,49 | 27,10 | 5,93 | 24,60 | 7,04 | <0,0001 | <0,0001 | 0,0002 |
| PCT (ng/mL) | 3,11 | 15,32 | 24,74 | 57,14 | 11,31 | 32,96 | <0,0001 | 0,002 | 0,0033 |
| PCR (mg/dL) | 6,48 | 7,63 | 15,60 | 10,33 | 12,12 | 9,73 | <0,0001 | <0,0001 | 0,0006 |
| Erythrocytes (1012/L) | 3,93 | 0,75 | 3,62 | 0,74 | 3,62 | 0,78 | <0,0001 | <0,0001 | NS |
| Haemoglobin (g/dL) | 11,63 | 2,06 | 10,77 | 2,05 | 10,65 | 2,20 | <0,0001 | <0,0001 | NS |
| Haematocrit (%) | 35,04 | 6,40 | 32,50 | 6,50 | 32,19 | 6,66 | <0,0001 | <0,0001 | NS |
| Leukocytes (109/L) | 12,11 | 4,80 | 13,65 | 11,67 | 13,03 | 7,92 | NS | NS | NS |
| Neutrophils (109/L) | 10,03 | 4,38 | 11,27 | 8,43 | 11,10 | 7,49 | NS | NS | NS |
| Lymphocytes (109/L) | 1,22 | 1,92 | 1,08 | 2,20 | 0,99 | 0,69 | <0,0001 | NS | NS |
| Basophil (109/L) | 0,02 | 0,03 | 0,02 | 0,04 | 0,03 | 0,04 | 0,0242 | NS | NS |
| Eosinophils (109/L) | 0,05 | 0,10 | 0,04 | 0,10 | 0,11 | 0,38 | NS | 0,0276 | 0,0329 |
| Monocytes (109/L) | 0,81 | 0,54 | 1,21 | 7,28 | 0,82 | 1,21 | <0,0001 | NS | NS |
| Platelets (109/L) | 217,75 | 92,59 | 189,21 | 111,19 | 211,82 | 131,12 | 0,0002 | NS | NS |
| MPV (fL) | 9,52 | 1,439 | 9,83 | 1,74 | 10,11 | 1,57 | NS | 0,0001 | NS |
Table 3.
ROC analysis results for commonly used parameters in patients by infection cluster type Criterion values and coordinates of the ROC curve [Show].
Table 3.
ROC analysis results for commonly used parameters in patients by infection cluster type Criterion values and coordinates of the ROC curve [Show].
| Overall infections 412 vs No infection 196 Sample size 608 | ||||||
| Variable | AUC | SE | 95% CI | Difference between areas |
95% CI |
Significance level |
| MDW | 0,840 | 0,0173 | 0,808 to 0,869 | 0,095 (MDW vs PCT) | 0,0542 to 0,135 | P < 0,0001 |
| PCT | 0,746 | 0,0213 | 0,708 to 0,781 | 0,103 (MDW vs PCR) | 0,0628 to 0,143 | P < 0,0001 |
| PCR | 0,737 | 0,0222 | 0,699 to 0,773 | 0,00825 (PCR vs PCT) | -0,0363 to 0,0528 | P = NS |
| Localized infections 235 vs No infection 196 Sample size 431 | ||||||
| MDW | 0,748 | 0,0258 | 0,700 to 0,792 | 0,0533 (MDW vs PCT) | -0,001 to 0,108 | P = NS |
| PCT | 0,695 | 0,0275 | 0,645 to 0,742 | 0,0737 (MDW vs PCR) | 0,0230 to 0,124 | P = 0,0044 |
| PCR | 0,675 | 0,0280 | 0,624 to 0,723 | 0,0203 (PCR vs PCT) | -0,0368 to 0,0774 | P = NS |
| BSIs 177 vs No infection 196 Sample size 373 | ||||||
| MDW | 0,918 | 0,0150 | 0,883 to 0,945 | 0,13 (MDW vs PCT) | 0,0842 to 0,176 | P < 0,0001 |
| PCT | 0,788 | 0,0251 | 0,740 to 0,831 | 0,12 (MDW vs PCR) | 0,0758 to 0,164 | P < 0,0001 |
| PCR | 0,798 | 0,0240 | 0,751 to 0,840 | 0,010 (PCR vs PCT) | -0,0405 to 0,0612 | P = NS |
| BSIs, SARS-COV-2 excluded 134 vs No infection 196 Sample size 330 | ||||||
| MDW | 0,936 | 0,0148 | 0,901 to 0,961 | 0,118 (MDW vs PCT) | 0,0706 to 0,164 | P < 0,0001 |
| PCT | 0,818 | 0,0258 | 0,769 to 0,861 | 0,107 (MDW vs PCR) | 0,0624 to 0,151 | P < 0,0001 |
| PCR | 0,829 | 0,0238 | 0,781 to 0,871 | 0,011 (PCR vs PCT) | -0,0404 to 0,0622 | P = NS |
Table 4.
MDW and the cutoff efficiency (Youden statistic) to diagnostics infection.
| MDW Criterion | Sensitivity | 95% CI | Specificity | 95% CI | +LR | 95% CI | -LR | 95% CI | +PV | -PV | |
| Overall infections | >20,43 | 72,45 | 65,6 - 78,6 | 84,15 | 80,2 - 87,5 | 3,05 | 2,42 - 3,85 | 0,22 | 0,17 - 0,28 | 86,5 | 68,6 |
| BSIs | >21,96 | 86,84 | 80,4 - 91,8 | 85,05 | 79,2 - 89,8 | 5,81 | 4,13 - 8,17 | 0,15 | 0,10 - 0,23 | 82 | 89,2 |
| Localised infections | >20,43 | 70,37 | 63,3 - 76,8 | 72,45 | 65,6 - 78,6 | 2,55 | 2,00 - 3,26 | 0,41 | 0,32 - 0,52 | 71,1 | 71,7 |
| BSIs excluded COVID19 | >21,96 | 91,59 | 84,6 - 96,1 | 85,05 | 79,2 - 89,8 | 6,13 | 4,36 - 8,61 | 0,099 | 0,053 - 0,19 | 77,2 | 94,8 |
Table 5.
Infection marker in survivors e not-survivors’ patients.
| Parameters | Outcome | N | Mean | ±SD. | SE | P value |
| MDW | not-survivors | 110 | 25,51 | 6,19 | 0,59 |
0.001 |
| survivors | 498 | 23,26 | 6,55 | 0,29 | ||
| PCT | not-survivors | 110 | 13,9 | 38,07 | 3,65 |
NS |
| survivors | 498 | 12,5 | 39,51 | 1,81 | ||
| PCR | not-survivors | 110 | 12,8 | 9,48 | 0,91 |
NS |
| survivors | 498 | 11,08 | 10,07 | 0,46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



