
Submitted:
06 August 2025
Posted:
07 August 2025
You are already at the latest version
Abstract
Background: H-type sacral fragility fractures are commonly deemed biomechanically unstable and often treated with spinopelvic fixation (SPF). However, elderly osteoporotic patients may benefit from less invasive approaches. Methods: A retrospective cohort of 51 elderly patients with CT-confirmed H-type sacral fractures underwent navigated transsacral bar (TSB) fixation. Radiographic stability and clinical outcomes were evaluated at 3 months. Results: No revision surgeries or implant failures were observed. Most patients regained mobility at discharge. TSB alone provided adequate stabilization, challenging the necessity of routine SPF in this demographic. Conclusion: Navigated TSB fixation offers a stable, less invasive alternative to SPF for selected osteoporotic sacral fractures
Keywords:
sacral fractures
; fragility fractures
; osteoporosis
; transsacral bar
; spinopelvic fixation
; elderly
; computer navigation
1. Introduction
Osteoporotic sacral insufficiency fractures (SIFs) are an increasingly recognized and clinically relevant entity, largely driven by global demographic shifts toward an aging population. In Germany and other industrialized nations, the incidence of pelvic fragility fractures in individuals over 65 years has risen sharply over the past two decades, reflecting both the growing elderly demographic and improved detection through advanced imaging modalities [1,2]. These fractures result from diminished bone mineral density and deterioration of trabecular microarchitecture, rendering the sacrum susceptible to failure under minimal or even physiological loading conditions. Although often the result of low-energy trauma, such as a fall from standing height, they may also occur atraumatically during routine activities.
Pain-related immobility is the most common clinical presentation, leading to a cascade of secondary complications including physical deconditioning, venous thromboembolism, muscle wasting, and loss of independence. In the frail elderly, such complications are not merely inconvenient but can directly influence long-term morbidity and mortality [3].
While non-displaced or minimally displaced fractures can often be managed conservatively with analgesia, osteoporosis therapy, and early mobilization, more complex fracture morphologies — particularly the so-called H-type or Honda sign configuration — present a more formidable challenge [4]. These fractures, characterized by bilateral vertical components intersected by a horizontal fracture through the sacral ala and body, are biomechanically reminiscent of vertically unstable pelvic injuries encountered in high-energy trauma [5]. Consequently, spinopelvic fixation (SPF), combining sacroiliac fixation with multisegmental lumbopelvic constructs, has become widely adopted as the “gold standard” for restoring stability and enabling early mobilization in such cases.
However, the wholesale application of high-energy trauma treatment principles to elderly patients with osteoporotic bone warrants critical reconsideration. In contrast to younger trauma patients, elderly individuals frequently retain substantial sacroiliac ligament integrity, and their overall biomechanical loading is significantly reduced due to lower activity levels [6]. Recent biomechanical studies have demonstrated that ligamentous structures can provide considerable residual stability even when fracture lines appear to completely traverse the sacrum [9]. This raises the question of whether all H-type fractures in elderly, low-demand patients truly require the most rigid and invasive fixation constructs available.
Technological advances in intraoperative imaging and navigation have paved the way for alternative strategies that balance biomechanical stability with surgical invasiveness. Among these, navigated transsacral bar (TSB) fixation has gained attention. Originally developed for high-energy pelvic trauma, TSB fixation involves placing a solid bar across the sacrum from ilium to ilium, engaging cortical bone on both sides to achieve bicortical purchase [8]. When guided by modern computer navigation, this technique allows for precise implant positioning with minimal soft-tissue disruption. In theory, this approach offers sufficient stability for osteoporotic H-type fractures while avoiding the extended operative times, greater blood loss, and higher complication rates associated with SPF in this population [9].
Despite promising biomechanical and early clinical data, the literature on TSB fixation for osteoporotic sacral fractures remains sparse. More importantly, there is a lack of dedicated studies examining navigated TSB fixation as a standalone approach in elderly patients with H-type sacral fractures — a group that stands to benefit most from reduced surgical morbidity.
The present study addresses this gap by evaluating the radiographic and clinical outcomes of elderly patients with osteoporotic H-type fractures treated exclusively with navigated TSB fixation. By focusing on this specific population, we aim to challenge the prevailing assumption that fracture morphology alone dictates the need for SPF, and to assess whether a targeted, less invasive fixation strategy can achieve comparable — or superior — outcomes in terms of stability, pain relief, and functional recovery. Our findings may support a paradigm shift toward more nuanced, patient-specific decision-making in the surgical management of sacral fragility fractures.
2. Materials and Methods
2.1. Study Design and Ethical Considerations
This was a single-center retrospective cohort analysis conducted at a tertiary academic spine and trauma center. The study was approved by the Ethics Committee of the Medical Association of Hessen (Reference Number: 2022-2899-zvBO) and conducted in accordance with the Declaration of Helsinki and Good Clinical Practice (GCP) guidelines. All participants provided written informed consent for treatment and use of anonymized data for research purposes.
2.2. Patient Selection
Patients ≥65 years with CT-confirmed osteoporotic H-type sacral fractures treated between January 2022 and January 2025 with navigated transsacral bar (TSB) fixation were eligible. Osteoporotic etiology was confirmed by clinical history, imaging findings, and, where available, bone mineral density testing.
Exclusion criteria included:
High-energy trauma mechanism
Pathological fractures due to metastatic disease, infection, or prior radiation therapy
Prior pelvic fixation
Incomplete imaging data or insufficient follow-up
Fracture Classification and Surgical Indications
Fractures were classified using both the Fragility Fractures of the Pelvis (FFP) classification system, which emphasizes biomechanical and clinical factors, and the Osteoporotic Fractures (OF) Pelvis classification.
Fragility Fractures of the Pelvis (FFP) Classification:
The Fragility Fractures of the Pelvis (FFP) classification, introduced by Rommens and Hofmann in 2013, is a morphology-based system specifically designed for low-energy pelvic fractures in elderly patients with osteoporosis. It categorizes injuries into four main types of increasing mechanical instability:
FFP Type I – Isolated anterior pelvic ring fracture: stable; typically managed non-operatively.
FFP Type II – Non-displaced posterior ring fracture: includes sacral ala fractures without displacement, with or without anterior ring involvement; generally stable and amenable to conservative treatment.
FFP Type III – Unilateral displaced posterior ring fracture: rotationally unstable; usually requires surgical stabilization.
FFP Type IV – Bilateral posterior ring involvement: most unstable form; may present as bilateral sacral fractures, H-type fractures, or spinopelvic dissociation; surgical fixation strongly indicated.
This classification focuses primarily on fracture morphology and mechanical stability. In our study, all patients had FFP Type III or IV injuries, reflecting high mechanical instability and the need for surgical intervention.
Osteoporotic Fractures (OF) Pelvis Classification:
The OF Pelvis classification is a novel, treatment-oriented scoring system designed to guide the management of osteoporotic pelvic fractures. It extends the principles of the established OF spine classification to the pelvic ring and integrates fracture morphology with key patient-related parameters. It differentiates five grades:
OF 1 – Minor fragility injury without structural instability: typically isolated anterior pelvic ring fractures (e.g., pubic ramus) without posterior ring involvement; stable and managed non-operatively.
OF 2 – Stable posterior ring involvement: non-displaced posterior pelvic ring fractures (e.g., sacral ala insufficiency fracture) with preserved weight-bearing capacity; generally suitable for conservative management.
OF 3 – Unstable unilateral posterior ring involvement: displaced unilateral posterior pelvic ring fractures or sacral fractures compromising load transfer; surgical stabilization often indicated if pain limits mobilization.
OF 4 – Bilateral posterior ring instability: bilateral posterior pelvic ring fractures, frequently including H-type sacral fractures, indicating high mechanical instability; surgical fixation usually recommended.
OF 5 – Spinopelvic dissociation: complete separation of the spinal column from the pelvis, typically due to high sacral fracture lines; urgent surgical fixation indicated.
In addition to morphology, the OF Pelvis Score incorporates pain severity, neurological deficits, baseline mobility, comorbidities, and frailty to produce a cumulative score. In this study, surgical fixation was generally performed for OF Grades 3–5 when the total score exceeded 8 points, indicating mechanical and functional instability. Classification and scoring were performed in consensus by two fellowship-trained orthopedic trauma surgeons.
2.3. Surgical Technique
All procedures were performed in a hybrid operating theatre using computer-assisted navigation (Brainlab, Munich, Germany) in combination with intraoperative CT imaging (AIRO, Stryker, USA). Patients were positioned supine on a radiolucent operating table and underwent 360° sterile draping to allow unrestricted intraoperative imaging and surgical access. After sterile preparation, an intraoperative CT scan was acquired and automatically registered to the navigation system, providing real-time 3D anatomical data for trajectory planning.
The optimal implant pathway was planned on the navigation workstation to safely traverse the sacrum while avoiding the sacral foramina and engaging the densest available cortical bone, particularly along the anterior sacral border.
Through small bilateral skin incisions (approximately 2–3 cm) over the posterior superior iliac spine, navigated guidewires were advanced percutaneously across the sacrum under continuous navigational guidance. A solid transsacral bar (7.5 mm diameter, titanium or stainless steel) was inserted from ilium to contralateral ilium with confirmed bicortical purchase. The bar was secured on the contralateral side with a counter washer screw, allowing controlled compression across the fracture and preventing distraction. In all cases, supplementary short sacroiliac screws were placed to enhance rotational stability.
2.4. Data Collection and Variables
Demographic variables (age, sex), mechanism of injury (e.g., fall from standing height), and comorbidities were recorded. Fracture morphology was assessed for the presence of H-type configuration—defined by bilateral vertical fracture lines intersected by a transverse component—as well as any comminution, which may influence mechanical stability.
Preoperative imaging included high-resolution computed tomography (CT) for fracture delineation and magnetic resonance imaging (MRI) when sacral edema or occult fractures were suspected. Operative data encompassed total surgical duration and intraoperative complications. Postoperative variables included hospital length of stay and discharge mobility status, categorized as walker-assisted, crutch-assisted, or independent.
2.5. Postoperative Care and Rehabilitation
All patients were mobilized within 24–48 hours postoperatively under physiotherapy supervision. Partial weight-bearing with a walker or crutches was advised for 4–6 weeks, progressing to full weight-bearing as tolerated. Standard thromboprophylaxis was administered until adequate mobility was regained.
2.6. Follow-Up Protocol and Radiological Assessment
Follow-up occurred at 3 and 12 months postoperatively, including clinical evaluation, pain assessment (0–10 numeric rating scale), and radiographic evaluation. Stability was defined as absence of implant migration, loosening, or new fracture displacement. CT scans were performed selectively if pain recurred or instability was suspected.
2.7. Statistical Analysis
Descriptive statistics were performed using IBM SPSS Statistics version 29 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as means ± standard deviation (SD), while categorical data were presented as frequencies and percentages. Due to the exploratory nature of the study, no inferential statistical comparisons were made at this stage.
3. Results
A retrospective analysis was conducted on 51 patients treated for pelvic fractures at our institution in the year 2022. This cohort comprised comprehensive clinical, demographic, radiographic, operative, and early follow-up data. Data completeness was high, with minor gaps in follow-up variables such as pain scores and implant loosening status.
3.1. Patient Demographics and Baseline Characteristics
The patient cohort was predominantly female (n = 45; 88.2%), reflecting the gender distribution commonly associated with osteoporotic pelvic fractures in older populations. The mean age at the time of treatment was 77.4 years (SD: 6.5 years; range: 66–88), consistent with a geriatric population vulnerable to fragility fractures. Traumatic injury was identified as the precipitating event in 26 patients (51.0%), while the remaining 25 patients (49.0%) sustained fractures in the absence of identifiable trauma, suggestive of insufficiency mechanisms.
3.2. Fracture Classification and Radiographic Findings
Fractures were classified using the Fragility Fracture of the Pelvis (FFP) system. FFP Type 4 fractures, indicating the most complex and unstable injury pattern with bilateral posterior involvement, were the most prevalent, observed in 35 patients (68.6%). Types 2 and 3 were less common, while Type 1 fractures were absent. Notably, posterior pelvic ring fractures were overwhelmingly bilateral (n = 47; 92.2%), underscoring the severity of instability in this population.
Anterior pelvic ring fractures were absent in 27 patients (52.9%), unilaterally present in 15 (29.4%), and bilateral in 9 (17.6%). A comminuted fracture zone, which may increase surgical complexity and affect healing, was documented in 19 patients (37.3%). Additionally, H-shaped sacral fractures and sacral involvement in the lateral and median zones were common radiographic features, frequently requiring advanced fixation strategies.
3.3. Surgical Management and Hospital Course
All patients underwent surgical treatment, with operative techniques and implants tailored to fracture morphology. The most common therapeutic approach involved a combination of transsacral bar with two short sacroiliac screws as a security against rotation.
After excluding patients who underwent additional surgical procedures, the mean operative time was approximately 70.3 minutes, with a range of 41 to 110 minutes. The average postoperative hospitalization was 9.2 days (range: 5–14 days), aligning with expectations for elderly surgical patients undergoing pelvic stabilization.
3.4. Postoperative Mobility and Rehabilitation
Mobility status at discharge was recorded for all patients. The majority were discharged using a rollator walker (n = 33; 64.7%), indicative of moderate functional recovery. Other assistive devices included Crutches and high walker. No patients were discharged ambulatory without aids, highlighting the lasting impact of pelvic fractures on mobility.
3.5. Follow-Up Pain and Implant Integrity
Postoperative pain was assessed at both 3-month and 12-month intervals. At 3 months, pain scores were available for 46 patients, with a mean value of 1.9 on a 10-point numeric rating scale, suggesting generally favorable early outcomes. By 12 months, pain data were available for 35 patients. A substantial proportion (n = 19; 54.3%) reported complete pain resolution (score = 0), and only a minority (n = 2) reported persistent moderate pain levels (score ≥ 5).
Importantly, radiographic assessment for implant loosening revealed no cases of loosening among the 51 patients with evaluable follow-up data, indicating high biomechanical integrity of the fixation constructs employed.
Figure 1.
Two Clinical Examples: CT images on the left illustrate a displaced pelvic fracture with a comminuted zone in the lateral mass and an anterior angulation in the sagittal plane. The accompanying X-ray shows fixation using two transsacral bars (TSB). Follow-up CT images on the right, taken six months postoperatively, demonstrate satisfactory fracture consolidation.
Figure 1.
Two Clinical Examples: CT images on the left illustrate a displaced pelvic fracture with a comminuted zone in the lateral mass and an anterior angulation in the sagittal plane. The accompanying X-ray shows fixation using two transsacral bars (TSB). Follow-up CT images on the right, taken six months postoperatively, demonstrate satisfactory fracture consolidation.
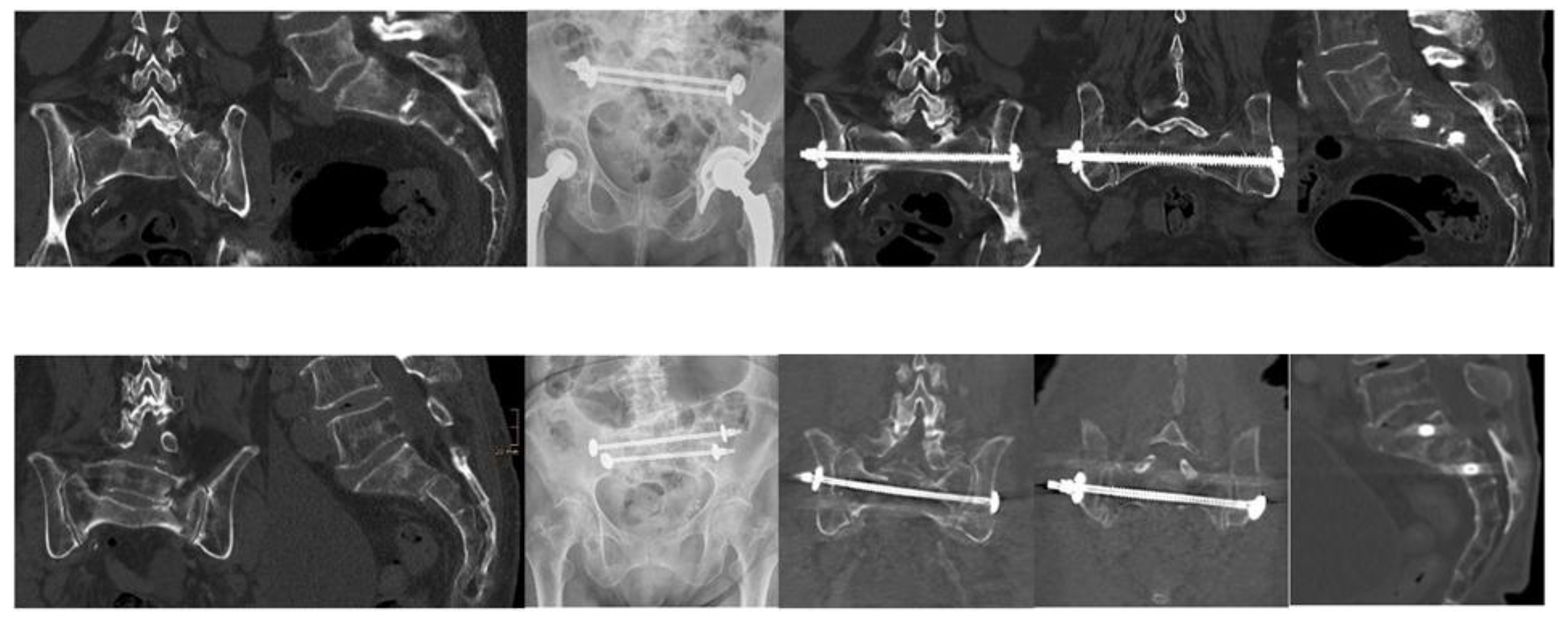
Figure 2.
Overview of Pelvic Fracture Morphology and Classifications, Including H-Fractures, Comminution, FFP, and OF Typing.
Figure 2.
Overview of Pelvic Fracture Morphology and Classifications, Including H-Fractures, Comminution, FFP, and OF Typing.
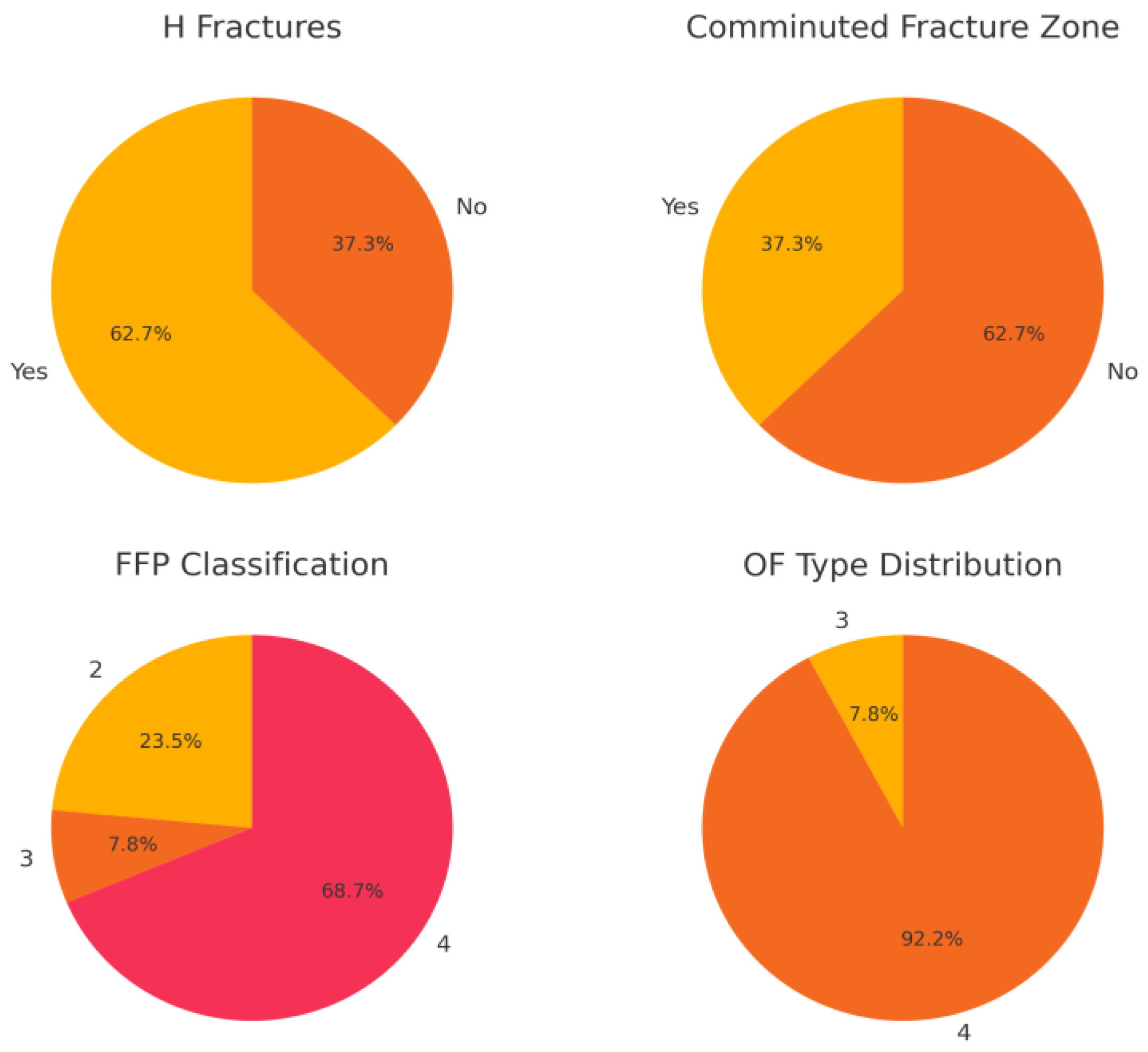

Table 1.
Baseline Characteristics of the Study Population.
| Parameter | Value |
| Demographics Age, median (range) Female, % Male, % |
|
| 77.4 (66-88) years 88.2 11.8 | |
| Fracture Classification FFP Type 4, % FFP Type 2, % FFP Type 3, % OF Type 4, % OF Type 3, % Comminuted zone, % H-type Fractures, % |
|
| 68.7 23.5 7.8 92 8 37.25 62.7 | |
| Operation time, median (range) Hospital stay, median (range) Loosening rate, % |
70.3 minutes (41-110) |
| 9.2 days (5-14)0 | |
| Mobilty and Pain Walker at discharge, % High Walker at discharge Crutches at discharge Bedridden No walking aids Pain level at 3 months, mean (0-10) Pain level at 12 months, mean (0-10) |
64.71 11.76 19.61 1.96 1.96 1.9 1.96 1.09 |
4. Discussion
This study provides new clinical evidence challenging the long-standing assumption that H-type sacral fragility fractures—characterized by bilateral vertical and transverse fracture components—necessarily require spinopelvic fixation (SPF) to ensure mechanical stability [9]. In our cohort of elderly patients with osteoporotic bone quality, navigated transsacral bar (TSB) fixation alone was sufficient to achieve stable fixation, with no cases of implant failure, secondary dislocation, or need for revision surgery over the follow-up period.
These findings support a potential paradigm shift in the surgical management of sacral fragility fractures in older adults. Unlike high-energy trauma patients, elderly individuals typically sustain these fractures under low-stress loading conditions and often retain intact posterior pelvic ligamentous structures. Biomechanical studies have shown that the sacroiliac and posterior ligament complexes remain functional in many osteoporotic fractures, even when fracture lines extend across the sacrum [9]. This residual ligamentous stability reduces the demand placed on the fixation construct. Consequently, applying high-energy trauma principles—such as routinely using long multisegmental spinopelvic constructs—may represent overtreatment for many elderly patients, exposing them to greater operative morbidity, longer hospitalizations, and prolonged rehabilitation without a proven mechanical or functional benefit.
4.1. Advantages of TSB Fixation
Transsacral fixation—particularly when performed under computer navigation—offers several inherent advantages in this patient population. It maintains mobility at adjacent lumbar segments, preserves soft tissue integrity, reduces operative exposure, and allows for shorter anesthesia duration. The minimally invasive approach is associated with less intraoperative blood loss and lower infection risk, which is especially relevant in elderly, frail patients with multiple comorbidities. Furthermore, the use of a counter washer screw to secure the bar on the contralateral ilium permits controlled fracture compression and prevents distraction, potentially enhancing stability and promoting union.
By using navigation-guided trajectories, the surgeon can consistently achieve optimal cortical purchase while avoiding neurovascular structures—a key factor given the narrow bony corridors of the sacrum in elderly patients. This may partly explain the absence of implant loosening or migration in our series. Our results suggest that, in appropriately selected cases, TSB fixation is not only a less invasive option but also a biomechanically sound method of stabilizing H-type fractures in osteoporotic bone.
4.2. Reconsidering Morphology-Driven Decision-Making
Traditionally, fracture morphology—particularly the presence of an H-type configuration—has been viewed as a proxy for instability, leading to the automatic recommendation for SPF. However, our findings, in line with recent reports [4,7,8], indicate that morphology alone is insufficient as a surgical indication. Instead, surgical decision-making should be multifactorial, incorporating:
The integrity of ligamentous structures on MRI or CT
Patient frailty and comorbidity burden
Baseline mobility and functional goals
Pain severity and tolerance of conservative management
Such an approach avoids overtreatment while still ensuring mechanical stability and functional recovery.
4.3. Comparison to Literature
When compared with contemporary surgical series for fragility fractures of the pelvis (FFP), our results are favorable across key outcomes.
In a cohort of 85 elderly patients treated with trans-sacral bar osteosynthesis, Wagner et al. reported a one-year mortality rate of 9.6% and an operative revision rate of 15%. Most patients regained ambulatory function by follow-up, although some required walking aids [8].
In a prospective comparison of bisegmental transsacral stabilization (BTS) and spinopelvic fixation (SPF), Mendel et al. found that BTS procedures had a mean operative time of 72 ± 23 minutes, whereas SPF procedures averaged 94 ± 27 minutes. Both groups had median hospital stays of 8–9 days [4].
In our cohort, navigated TSB fixation achieved no implant failures, no revision surgeries, a mean operative time of 77.4 minutes, and a median hospital stay of 9.2 days. These results compare favorably with previously published series, with operative efficiency and hospital stays similar to or better than other minimally invasive strategies.
4.4. Health-Economic Considerations
Although this study did not include a formal cost analysis, the shorter operative time, lower complication rates, and reduced hospital stay associated with TSB fixation are likely to translate into lower overall healthcare costs. Avoidance of revision surgery and fewer readmissions due to wound or implant-related complications also contribute to potential cost savings—an important consideration in the treatment of an increasingly prevalent condition in aging societies.
4.5. Limitations
The primary limitations of this study include its retrospective design, modest sample size, and relatively short follow-up period. Functional outcomes were assessed indirectly, without standardized quality-of-life measures such as the EQ-5D or Oswestry Disability Index. In addition, the absence of a directly matched SPF control group limits the strength of comparative statements. Nonetheless, the uniformity of favorable radiographic and clinical outcomes, combined with the absence of mechanical failures, strengthens the case for TSB fixation as a viable alternative to SPF in this context.
4.6. Future Directions
Future research should focus on prospective, multicenter trials comparing TSB and SPF in elderly patients with H-type sacral fractures, ideally including standardized functional and quality-of-life measures. Long-term follow-up is needed to assess implant survival, late-onset loosening, and sustained functional independence. Biomechanical studies exploring hybrid constructs (TSB plus cement augmentation) and their potential benefits in severely osteoporotic bone would also be valuable. Finally, cost-effectiveness analyses will be important to guide surgical strategy in the face of rising healthcare demands in aging populations.
5. Conclusions
This study provides compelling early evidence that navigated transsacral bar fixation alone may offer a viable and less invasive alternative to spinopelvic fixation for osteoporotic H-type sacral fractures in elderly patients. These findings support a more tailored, physiology-based surgical approach, and warrant further investigation to refine indications and optimize outcomes in this vulnerable population.
Author Contributions
Conceptualization: Martin Naisan, Marcus Richter, Philipp Hartung; Methodology: Martin Naisan, Felix Schmitz, Yazan Noufal; Formal analysis: Felix Schmitz, Yama Afghanyar; Investigation: Martin Naisan, Yazan Noufal, Matthias Fröhlich; Data curation: Martin Naisan; Writing—original draft preparation: Martin Naisan; Writing—review and editing: Philipp Drees, Marcus Richter, Matthias Fröhlich, Philipp Hartung; Supervision: Marcus Richter, Philipp Drees, Philipp Hartung; Project administration: Martin Naisan. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval was obtained from the Ethics Committee of the Medical Association of Hessen (Reference Number: 2022-2899-zvBO). All participants provided written informed consent for treatment and the use of anonymized data for research purposes. The study adhered to the principles of the Declaration of Helsinki and was conducted in accordance with Good Clinical Practice (GCP) guidelines.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study. The study was conducted in accordance with the Declaration of Helsinki and approved by the institutional ethics committee, with all patient data anonymized prior to analysis.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Abbreviations
The following abbreviations are used in this manuscript:
| SPF | Spinopelvic Fixation |
| TSB | Transsacral Bar |
| SIFs | Osteoporotic Sacral Insufficiency Fractures |
| FFP | Fragility Fractures of Pelvis |
| OF | Osteoporotic Fractures |
References
- Rommens PM, Hofmann A. Comprehensive classification of fragility fractures of the pelvic ring: recommendations for surgical treatment. Injury. 2013;44(12):1733-1744. [CrossRef]
- Höch A, Pieroh P, Henkelmann R, Josten C, Böhme J. Outcome and 2-year survival rate in elderly patients with lateral compression fractures of the pelvis. Geriatr Orthop Surg Rehabil. 2017;8(1):3-9. [CrossRef]
- Nuber S, Schubert A, Fürmetz J, Pflug A, Böcker W, Kammerlander C, Böcker W, Nüchtern JV. Midterm follow-up of elderly patients with fragility fractures of the pelvis: a prospective cohort study comparing operative and non-operative treatment according to a therapeutic algorithm. Injury. 2022;53(2):496-505. [CrossRef]
- Mendel T, Schenk P, Ullrich BW, Hofmann GO, Goehre F, Schwan S, Schütz T, Arand C. Mid-term outcome of bilateral fragility fractures of the sacrum after bisegmental transsacral stabilization versus spinopelvic fixation: a prospective study of two minimally invasive fixation constructs. Bone Joint J. 2021;103-B(3):462-468. [CrossRef]
- Gänsslen A, Hüfner T, Krettek C. Percutaneous iliosacral screw fixation of unstable pelvic injuries by conventional fluoroscopy. Oper Orthop Traumatol. 2006;18(3):225-244. [CrossRef]
- Rommens PM, Boudissa M, Krämer S, Kisilak M, Hofmann A, Wagner D. Operative treatment of fragility fractures of the pelvis: a critical analysis of 140 patients. Eur J Trauma Emerg Surg. 2022;48(4):2881-2896. [CrossRef]
- Eckardt H, Egger A, Hasler RM, Zech CJ, Vach W, Suhm N, Morgenstern M, Saxer F. Good functional outcome in patients suffering fragility fractures of the pelvis treated with percutaneous screw stabilisation: assessment of complications and factors influencing failure. Injury. 2017;48(12):2717-2723. [CrossRef]
- Wagner D, Kisilak M, Porcheron G, Krämer S, Mehling I, Hofmann A, Rommens PM. Trans-sacral bar osteosynthesis provides low mortality and high mobility in patients with fragility fractures of the pelvis. Sci Rep. 2021;11(1):14201. [CrossRef]
- Peng Y, Zhang G, Zhang S, Ji X, Li J, Du C, Zhao W, Zhang L. Biomechanical study of transsacral-transiliac screw fixation versus lumbopelvic fixation and bilateral triangular fixation for “H”- and “U”-type sacrum fractures with traumatic spondylopelvic dissociation: a finite element analysis study. J Orthop Surg Res. 2021;16(1):428. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



