
Submitted:
06 August 2025
Posted:
07 August 2025
You are already at the latest version
Abstract
Background/Objectives: Human epidermal growth factor receptor 2 (HER2) inhibitors have significantly improved the prognosis of patients with HER2-positive breast cancer. Currently, HER2 inhibitors, including tyrosine kinase inhibitors targeting HER2 and other HER family members, as well as antibody–drug conjugates, have been developed and are in clinical use. Each of these agents has distinct mechanisms of action and adverse event profiles. In treatment models such as therapy for HER2-positive breast cancer, in which multiple agents with HER2-inhibitory activity are used sequentially or in combination, a comprehensive understanding of the adverse events associated with each drug is beneficial. However, investigations into overall adverse event trends remain limited. Therefore, this study aimed to conduct a comprehensive analysis of the characteristic adverse events associated with HER2 inhibitors. Methods: Using the Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) database, we performed cluster analysis and principal component analysis (PCA) based on the reporting odds ratios of key adverse events associated with HER2 inhibitors approved for breast cancer treatment. Results: Cluster analysis revealed a strong correlation between monoclonal antibody drugs and hair-related adverse events. PCA indicated that the first component reflects the adverse event occurrence risk, the second differentiates between monoclonal antibodies and tyrosine kinase inhibitors, and the third may serve as an indicator distinguishing molecular targeted agents from antibody–drug conjugates. Conclusions: Analysis of FAERS data enabled comprehensive visualization of the real-world adverse event profiles of individual HER2 inhibitors. These findings are expected to enhance our understanding of safety profiles, support informed drug selection, and contribute to the development of improved adverse event management strategies.
Keywords:
HER2 inhibitors
; adverse event profile
; molecular targeted therapy
; breast cancer
; FAERS database
; principal component analysis
; cluster analysis
; monoclonal antibody
; antibody–drug conjugate
; tyrosine kinase inhibitor
1. Introduction
Human epidermal growth factor receptor 2 (HER2) is a membrane-bound receptor-type tyrosine kinase encoded by the ERBB2 gene. It belongs to the HER family, which comprises HER1, HER2, HER3, and HER4 [1]. In healthy cells, HER2 receptors are involved in signal transduction processes like cell proliferation and differentiation. However, preclinical studies suggest that HER2 protein overexpression is associated with enhanced tumor cell proliferation and increased metastatic potential, indicating a possible involvement in malignancy. HER2 overexpression is observed in various cancers, particularly breast [2] and gastric cancers [3], with an expression rate of 10%–35% in breast cancer patients [2]. Shortened disease-free survival, increased recurrence rates, and significantly reduced overall survival have been reported in this population, indicating poor prognosis [4].
Following the development of trastuzumab [5,6,7], recently, molecular targeted agents directed against HER2 and other HER family receptors have been developed and introduced into clinical practice. Agents inhibiting HER2 activity provide markedly improved outcomes for patients with HER2-positive breast cancer and play an essential role in treatment strategies. Whereas these agents all inhibit HER2 activity, certain drugs also target other members of the EGFR family, resulting in diverse mechanisms of action and safety profiles. In treating HER2-positive breast cancer, targeted therapy is recommended using HER2 inhibitors combined with chemotherapy regardless of disease stage [8], with well-established efficacy [5,6,7,9,10,11,12,13,14]. In treatment models where several HER2-targeted agents are administered sequentially, a comprehensive understanding of the associated adverse events is vital for optimal side effect management. Therefore, a holistic understanding of the safety profiles of HER2 inhibitors is needed.
Representative adverse events reported for HER2 inhibitors include cardiotoxicity and infusion reactions from monoclonal antibodies (mAbs) like trastuzumab [6,15]; thrombocytopenia from antibody–drug conjugates (ADCs) like trastuzumab emtansine (T-DM1) [16]; interstitial lung disease (ILD) associated with trastuzumab deruxtecan (T-DXd) [11]; and diarrhea from tyrosine kinase inhibitors (TKIs) like neratinib [14]. However, comprehensive investigations remain limited on the overall adverse events associated with these agents.
To holistically evaluate the adverse events associated with HER2 inhibitors, we examined large-scale spontaneous reporting systems (SRS) data. SRS are valuable data sources for post-marketing safety surveillance, enabling the detection of rare side effects that may not emerge during clinical trials. The Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS), maintained by the United States FDA, contains a multinational dataset. Its large volume of reports allows for highly accurate statistical analyses, contributing to a more precise understanding of adverse event trends.
Among the signal detection and evaluation methods applicable to SRS data, volcano plot analysis provides comprehensive visual insights. Volcano plots are constructed using the logarithm of the reporting odds ratio (lnROR) and the negative log of the p-value from Fisher’s exact test (−log(p-value)), and they are well-suited for observing one-to-many relationships between a specific drug and multiple adverse events. However, simultaneously capturing relationships among multiple drugs and numerous adverse events requires analytical strategies that either group drugs or events before analysis. Therefore, to assess these complex relationships, we applied data mining methodologies such as cluster analysis [17] and principal component analysis (PCA) [18], which can handle the high dimensionality and sparsity of SRS data.
The objective of this study was to comprehensively evaluate the major adverse events related to HER2 inhibitors approved for breast cancer using the FAERS database, employing cluster analysis and PCA. Our findings are expected to enhance our understanding of adverse event occurrence patterns and safety profiles, informing optimal drug selection and improving adverse event management.
2. Results
2.1. Construction of the Analytical Data Table
We created a combined data table by merging the FAERS drug information (DRUG) table, which comprises 18,321,080 rows, and the adverse event information (REAC) table, which comprises 18,328,666 rows. Duplicate entries were removed during the table construction process. A flowchart illustrating the table construction process is presented in Figure 1.
2.2. Number of Reports
Table 1 presents the number of adverse events reported for the nine HER2 inhibitors included in the FAERS database.
2.3. Frequently Reported Adverse Events
Sixty-three adverse events with >1,500 reported cases linked to the examined HER2 inhibitors were identified. After excluding two preferred terms (“no adverse event” and “off-label use”), 61 adverse event categories were extracted and are displayed in Table S1. This table includes the adverse event term, the number of reports, ROR, 95% confidence interval, p-value, and the four-cell layout of the 2 × 2 contingency table used for ROR calculation. The cells are defined as follows: (a) adverse event with the target drug, (b) no adverse event with the target drug, (c) adverse event with a non-target drug, and (d) no adverse event with a non-target drug. This arrangement enables quantitative estimation of the association strength between each drug and adverse event via the ROR. Among these, diarrhea was most frequently reported, followed by nausea and fatigue. Adverse events with notably high ROR values (ROR [95% CI]) included: hair disorders, 39.93 [37.68–42.32]; metastases to the central nervous system, 38.96 [37.03–40.99]; decreased ejection fraction, 35.47 [33.87–37.15]; and cardiotoxicity, 34.46 [32.33–36.72]. These adverse events were estimated to exhibit relatively strong associations with the HER2-targeting agents.
2.4. Hierarchical Cluster Analysis
Hierarchical cluster analysis (Ward’s method) was conducted on the nine HER2 inhibitors based on the lnROR values and adverse events identified in Section 2.3. This analysis classified the drugs into three clusters (Figure 2): cluster A (lapatinib, neratinib, tucatinib, and T-DM1); cluster B (pyrotinib and T-DXd); and cluster C (trastuzumab, pertuzumab, and margetuximab). Similarly, hierarchical cluster analysis was performed on the 61 adverse events, identifying eight distinct clusters (Figure 2): cluster 1 (including abdominal pain, urinary tract infection, and pneumonia); cluster 2 (including anxiety, pain, arthralgia, and back pain); cluster 3 (anemia, decreased white blood cell count, and decreased platelet count); cluster 4 (including asthenia, decreased weight, and fatigue); cluster 5 (hair color changes, abnormal hair texture, hair disorders, and madarosis); cluster 6 (infusion-related reactions and ILD); cluster 7 (myelosuppression); and cluster 8 (including metastatic breast cancer, metastases to the central nervous system, and decreased ejection fraction).
2.5. PCAs
The PCA results are shown in Figure 3. The contribution rates of the first, second, and third principal components were 59.8%, 18.2%, and 8.03%, respectively. Principal component 1 demonstrated a positive correlation with the lnROR values calculated by collectively evaluating the target drugs as a single group of HER2 inhibitors (R2 = 0.655, p < 0.0001; see Figure 4). Principal component 2 was positively correlated with lapatinib (r = 0.450), neratinib (r = 0.464), and tucatinib (r = 0.667), whereas it exhibited negative correlations with pertuzumab (r = −0.542), trastuzumab (r = −0.567), and margetuximab (r = −0.367). Principal component 3 was positively correlated with neratinib (r = 0.521) and negatively correlated with T-DXd (r = −0.440) and T-DM1 (r = −0.325).
The correlation coefficient (r) represents the value from the PCA loading matrix. It is a quantitative indicator of the relationship between each drug and the respective principal component.
3. Discussion
3.1. Number of Adverse Event Reports Related to HER2 Inhibitors
Among the HER2 inhibitors analyzed, mAbs had the highest number of reported adverse events, followed by TKIs and ADCs, as shown in Table 1. Notably, trastuzumab had the highest number of reports, which may be attributed to its long-standing clinical use.
Of the top 61 adverse events selected for cluster analysis and PCA, diarrhea was the most frequent, followed by nausea and fatigue (Table S1). Previous studies also identified nausea and fatigue as common adverse events associated with HER2 inhibitors [19]. Diarrhea was predominantly reported with HER2 TKIs [19,20].
In a previous study [19], adverse events such as a decreased ejection fraction and cardiac failure were among the top 10 reported for trastuzumab. These were ranked 19th and 60th, respectively, in the current analysis. Similarly, at rank 38, thrombocytopenia, frequently reported with T-DM1, appeared as platelet count decreased, whereas ILD, a serious clinical concern with T-DXd, was ranked 40th. These findings suggest that the adverse events identified by report frequency were appropriately selected for inclusion in the analysis.
3.2. Classification of HER2 Inhibitors Based on Hierarchical Clustering Analysis
Cluster analysis is a data mining technique that groups data based on similarities. Hierarchical clustering organizes data into nested clusters and generates dendrograms for visual representation.
In this study, Ward’s method was used to perform hierarchical clustering analysis on the nine HER2 inhibitors based on lnROR values calculated for 61 adverse event terms extracted in Section 4 (Materials and Methods). This analysis classified the drugs into three distinct clusters (Figure 2). Notably, aside from the ADCs, the TKIs and mAbs were separated early in the clustering process.
Cluster A included lapatinib, neratinib, tucatinib, and T-DM1, with most agents being TKIs. This cluster exhibited strong associations with adverse events, including fatigue, vomiting, and dehydration. Diarrhea—the most frequently reported adverse event—was associated with multiple drugs in this cluster. Diarrhea is a well-known common adverse event of TKIs [20] that can lead to substantial fluid and electrolyte loss, which may induce dehydration. Notably, all agents in cluster A, except T-DM1, showed poor associations with infusion-related reactions and myelosuppression, possibly due to their oral administration and the selective targeting of HER2, which has low expression in hematopoietic cells [21].
Cluster B included pyrotinib and T-DXd. Compared to the other clusters, these agents showed relatively poor associations with central nervous system-related adverse events like anxiety and pain. However, both drugs showed similar associations with metastatic breast cancer and central nervous system metastases, suggesting that despite differing mechanisms, they may share common influences on disease metastasis. The limited associations with anxiety and pain imply a potentially lower impact on patients’ quality of life (QoL), which may be clinically advantageous.
Pyrotinib, an irreversible TKI targeting EGFR, HER2, and HER4, was approved in 2018 in China and is widely used as a second-line therapy for HER2-positive metastatic breast cancer, especially in developing countries lacking access to innovative ADCs such as T-DM1 and T-DXd [22]. Systematic reviews and meta-analyses have confirmed its efficacy, including benefits for patients with brain metastases [23]. Likewise, T-DXd shows significantly improved progression-free survival in HER2-positive breast cancer patients with brain metastases [24].
Cluster C consisted exclusively of mAbs: trastuzumab, pertuzumab, and margetuximab. This cluster was strongly associated with hair-related adverse events, including hair color changes, hair disorders, abnormal hair texture, and madarosis. Drug-related side effects, hormonal changes, and immune responses commonly induce these symptoms. Chemotherapy and immunosuppressants disrupt hair growth cycles, leading to hair loss. In standard HER2-positive breast cancer therapy, mAbs are often used together with alopecia-inducing cytotoxic agents like anthracyclines and taxanes [25,26].
Hair that regrows after chemotherapy may differ in color, texture, thickness, or wave pattern from the patient’s original hair [27]. Pigment changes are thought to result from oxidative damage, including impaired melanin transport from follicular keratinocytes and melanocyte and melanocyte stem cell apoptosis [28]. Alterations in hair structure may also reflect changes in hair shaft keratin and asymmetric follicular growth [29,30]. Whereas a systematic review reported that approximately 15% of molecular targeted agents are associated with alopecia [31], careful interpretation is warranted to determine whether these mAbs directly cause hair-related adverse events. The involvement of concomitant cytotoxic or targeted therapies on these adverse effects cannot be excluded.
Although the precise causes of hair-related adverse events could not be established in this study, cluster analysis enabled the visualization of adverse event patterns that may not be fully explained by theoretical mechanisms, providing real-world insights into the safety profiles of HER2 inhibitors.
3.3. Classification of Adverse Events Based on Clustering Analysis
The adverse events were classified into eight distinct clusters (Figure 2):
- Cluster 1: abdominal pain, alopecia, cardiac failure, chills, cough, death, dyspnea, general physical health deterioration, malaise, pneumonia, pyrexia, and urinary tract infection
This cluster comprises adverse events related to systemic health deterioration (e.g., general physical health deterioration, malaise, and death), infectious symptoms (e.g., pneumonia, urinary tract infections, cough, and pyrexia), and administration-related side effects (e.g., chills and cardiac failure). As visually suggested by the heatmap in Figure 2, chills and alopecia were relatively strongly associated with mAbs.
Chills are a hallmark of infusion-related reactions, particularly during the initial administration. A strong association signal was observed with margetuximab, a chimeric anti-HER2 monoclonal antibody featuring an engineered Fc domain optimized to enhance immune activation [32,33]. In a Phase III trial combining margetuximab with chemotherapy, the overall incidence of infusion-related reactions (any grade) was 13.3%, ranking it among the top 15 most frequent adverse events [34]. Within cluster 6, which includes infusion-related reactions, margetuximab showed a notable signal, suggesting that the chills reported with margetuximab may primarily originate from infusion-related reactions.
Alopecia also showed a notable association with mAbs, as observed in Figure 2; two hypotheses could explain this observation. First, mAbs targeting HER2 may directly affect hair follicles. However, clinical trials and basic research have not yet elucidated the causal mechanism [35]. Second, synergistic effects and confounding influences from concomitant medications must be considered. As previously discussed, molecular targeted agents are frequently administered in combination with other cytotoxic chemotherapeutic drugs. Therefore, the alopecia signal is unlikely to reflect the effects of mAbs alone and is more likely influenced by co-administered agents. In summary, whereas these findings suggest the potential involvement of mAbs in alopecia, they cannot be interpreted as evidence for a direct causal relationship. Although HER2 receptor inhibition may impact the hair follicles pharmacologically, the widespread use of combination therapies necessitates careful consideration of drug–drug interactions and confounding factors. To clarify these relationships, further investigation is needed.
- Cluster 2: anxiety, arthralgia, back pain, dizziness, drug ineffective, erythema, headache, hypoaesthesia, myalgia, pain, pain in extremity, paresthesia, pruritus, and rash
This cluster primarily includes neurological and sensory symptoms, which were poorly associated with the HER2 inhibitors. This may reflect the limited expression of HER2 in the nervous system and the restrictive nature of the blood–brain barrier (BBB).
Due to their high molecular weight, mAbs poorly penetrate the BBB, resulting in limited CNS activity. Conversely, TKIs are low-molecular-weight compounds that are thought to cross the BBB more readily than high-molecular-weight agents such as trastuzumab [36,37,38,39]. However, TKIs also showed low neurological impact, possibly due to their selectivity for HER2-overexpressing tumor cells, thereby preserving normal neuronal function.
ADCs share pharmacokinetic properties with trastuzumab, like slow clearance and limited distribution volume, primarily remaining confined to plasma [40]. Nonetheless, emerging evidence suggests that some ADCs have intracranial effects. Their CNS delivery mechanisms are under active investigation [41,42,43].
Taken together, these findings suggest that HER2 inhibitors may have favorable CNS safety profiles, which could be a crucial consideration in therapeutic decision-making.
- Cluster 3: anemia, febrile neutropenia, neutropenia, decreased platelet count, pleural effusion, thrombocytopenia, decreased white blood cell count
This cluster includes adverse events commonly associated with myelosuppression and immunosuppression, typically resulting from cytotoxic chemotherapy. TKIs aside from pyrotinib (i.e., lapatinib, tucatinib, neratinib) showed weak associations with hematological toxicity, supporting the idea that TKIs generally carry a lower risk of causing bone marrow suppression.
- Cluster 4: asthenia, constipation, decreased appetite, dehydration, diarrhea, epistaxis, fatigue, malignant neoplasm progression, nausea, stomatitis, vomiting, and decreased weight
This cluster encompasses gastrointestinal dysfunction, nutritional decline, and general systemic deterioration. Unlike cluster 3, TKIs such as lapatinib, tucatinib, and neratinib showed stronger correlations with these events.
Diarrhea was associated with all TKIs, including pyrotinib, which irreversibly inhibits HER family members. Phase II/III trials have reported a high incidence of diarrhea (83% for pyrotinib [44]; 97% for neratinib [14]). This toxicity is likely mediated by EGFR inhibition in the gastrointestinal tract, which disrupts mucosal integrity [20]. Severe diarrhea may lead to fluid and electrolyte loss, contributing to dehydration and nutritional decline. Dose escalation and prophylactic antidiarrheal measures can reduce its severity [45].
- Cluster 5: hair color changes, hair disorders, abnormal hair texture, and madarosis
This cluster exclusively comprises hair-related adverse events, with strong associations to mAbs, as discussed in Section 3.2. These events may reflect post-chemotherapy hair regeneration, immunological effects, or indirect pharmacologic consequences.
- Cluster 6: infusion-related reactions and ILD
These events were more prevalent with intravenously administered agents, such as trastuzumab, pertuzumab, margetuximab, T-DXd, and T-DM1.
ILD was especially associated with T-DXd and is a known adverse event with a reported high frequency [11,46]. Our analysis confirmed the strong positive signal with T-DXd, whereas neratinib exhibited a strong negative correlation. These trends are consistent with prior studies evaluating ILD in cancer therapies [47].
- Cluster 7: Myelosuppression
This cluster consisted solely of myelosuppression, a condition commonly observed in chemotherapy, particularly when cytotoxic agents impair hematopoietic stem cells in the bone marrow, thereby suppressing blood cell production. In our analysis, myelosuppression was associated with ADCs and mAbs. Among TKIs, pyrotinib showed a strong positive association, whereas other TKIs exhibited negative correlations.
TKIs carry a relatively low risk of bone marrow suppression; however, certain TKIs—such as imatinib [48], nilotinib [49], and dasatinib [50], used in chronic myeloid leukemia treatment—present hematologic toxicity. These findings suggest that pyrotinib has a unique pharmacological mechanism and safety profile distinct from that of conventional TKIs.
As noted previously, pyrotinib is often an alternative to ADCs, and this must be taken into consideration. Therefore, further investigation is necessary to elucidate the underlying causes of myelosuppression and comprehensively assess pyrotinib’s safety profile.
- Cluster 8: breast cancer metastatic, cardiotoxicity, disease progression, decreased ejection fraction, hypokalemia, metastases to the central nervous system, mucosal inflammation, peripheral neuropathy, and palmar–plantar erythrodysesthesia syndrome
In contrast to cluster 2, cluster 8 exhibited strong associations with adverse events across the examined agents. This cluster likely represents adverse events specifically associated with HER2-targeted therapies.
In HER2-positive breast cancer, central nervous system metastases occur in up to 50% of patients [51,52], and this phenomenon is frequently encountered in clinical practice. In our analysis, central nervous system metastases showed strong associations with all examined HER2-targeted agents. Drugs with HER2-inhibitory activity, including mAbs, ADCs, and TKIs, have been associated with cardiotoxicity, likely due to HER2 expression in cardiac myocytes [6,15,16,53,54]. Moreover, these drugs are frequently administered in conjunction with other cardiotoxic therapies, like anthracyclines and radiotherapy, which may further exacerbate cardiac risks.
In this analysis, decreased ejection fraction was associated with all HER2 inhibitors except pyrotinib, whereas cardiotoxicity showed only a weak correlation with neratinib. Notably, many clinical trials exclude patients with pre-existing cardiac abnormalities, suggesting that the incidence of cardiotoxicity may be underestimated. However, this study utilized the FAERS database to analyze a broader and more diverse patient population, allowing adverse event patterns to be reflected under real-world medical conditions. Given the risk of cardiac issues during HER2-targeted therapy, the FDA has recommended baseline cardiac screening and at intervals throughout treatment [55].
Palmar–plantar erythrodysesthesia syndrome, also known as hand–foot syndrome (HFS), was associated with all agents except T-DXd. HFS is commonly induced by fluoropyrimidine agents such as capecitabine [56]. In a clinical trial in patients with residual HER2-negative invasive breast cancer evaluating adjuvant capecitabine following preoperative chemotherapy, the incidence of HFS in the capecitabine arm was as high as 73.4% [57]. Many HER2 inhibitors associated with HFS are commonly administered with capecitabine [12,13,14,23,34,37,38,39,58]. These findings underscore the importance of accounting for the influence of combination therapies involving capecitabine.
Taken together with the results of cluster analysis, PCA further elucidated the detailed adverse events associated with molecularly targeted drugs that have HER2-inhibitory activity.
3.4. PCA
PCA is a dimensionality reduction technique used to enhance interpretability by expressing a dataset with multiple variables as a smaller number of components, while minimizing information loss. In this study, PCA was used to evaluate the relationships between each adverse event (Preferred Terms) and HER2-targeted drugs.
Principal component 1 was positively correlated with lnROR (Figure 4). This component represents the risk of developing adverse events likely to be induced by HER2 inhibitors.
Principal component 2 showed positive correlations with TKIs like lapatinib (r = 0.450), neratinib (r = 0.464), and tucatinib (r = 0.667), while demonstrating negative correlations with mAbs including pertuzumab (r = −0.542), trastuzumab (r = −0.567), and margetuximab (r = −0.367). Thus, principal component 2 may reflect differences in the mechanisms of action of these drugs. Specifically, intracellular HER2 tyrosine kinase inhibition is plotted toward the positive axis, whereas extracellular HER2-targeted antibody effects are plotted toward the negative axis.
This analysis was conducted by log-transforming the RORs to approximate a normal distribution, followed by evaluating their relationship with HER2 inhibitors via PCA. The observation that adverse event reporting patterns are expressed in principal component 2 based on differences in mechanisms of action suggests that the high selectivity of molecular targeted agents is strongly reflected in their adverse event profiles.
ADCs, including T-DXd and T-DM1, have hybrid mechanisms combining HER2 targeting via the antibody portion with cytotoxic payload delivery through linkers. Due to these unique characteristics, ADCs have a neutral position, neither fully aligned with low-molecular-weight TKIs (positive axis), which directly inhibit intracellular signaling, nor with mAbs (negative axis), which act through immune-mediated receptor targeting.
Although pyrotinib is classified as a TKI, it has multiple associations with adverse events typically observed with cytotoxic chemotherapeutic agents, such as bone marrow suppression (Figure 2 and Figure 3). This may differ from that of other TKIs, resulting in a neutral position in the PCA.
Principal component 3 was positively correlated with neratinib (r = 0.521) and negatively correlated with T-DXd (r = −0.440) and T-DM1 (r = −0.325). In the plot, the positive axis was associated with adverse events involving localized tissues such as skin and mucosa. Conversely, the negative axis captured adverse events commonly reported for ADCs, including decreased platelet count and ILD (Figure 4). This suggests that principal component 3 may distinguish adverse event profiles between pure molecular targeted agents and ADCs.
Off-target toxicity, which refers to toxic effects unrelated to the antibody’s target molecule and often constitutes dose-limiting toxicities [59], is a key issue in ADC safety assessments. The cytotoxic payloads used in ADCs are generally highly potent and often too toxic to be used as standalone drugs [60]. ADCs are designed with linkers that stabilize the payload in serum and promote rapid clearance outside the tumor [61,62]. The target-dependent mechanisms of ADCs enhance tissue selectivity and cytotoxic efficacy toward cancer cells during drug action, while simultaneously reducing, but not eliminating, the systemic toxicity associated with the cytotoxic payload.
Off-target toxicity may result from premature linker cleavage [63] or unintended ADC uptake into non-target cells [64]. Thrombocytopenia observed with T-DM1may occur via Fc receptor-mediated uptake into megakaryocytes, followed by payload-induced cellular injury, as demonstrated in in vitro studies [64].
T-DXd is composed of trastuzumab conjugated via a cleavable tetrapeptide linker to a topoisomerase I inhibitor payload [61,65]. As previously described, the most serious adverse event associated with T-DXd is ILD through an undetermined mechanism. ILD with T-DXd may result from off-target toxicity following payload release or immune-mediated lung injury involving macrophage activation [66]. Preclinical studies in monkeys revealed that T-DXd is preferentially localized in macrophages rather than pulmonary epithelial cells [67].
Our observations suggest that adverse events associated with ADCs may be related to off-target effects. Cytotoxic adverse events induced by the payload are observed as negative loadings in principal component 3, implying that this axis represents toxicity specific to molecularly targeted agents.
Based on the structure of principal components 1 through 3, we can summarize the tendencies of drugs and their corresponding adverse events. TKIs, such as neratinib and lapatinib, showed strong associations with diarrhea, whereas mAbs, like trastuzumab and pertuzumab, were significantly associated with hair-related adverse events. To the best of our knowledge, this is the first report in the literature to extract adverse event profiles using cluster analysis and PCA applied to SRS data.
While ADCs such as T-DM1 and T-DXd have structurally incorporated monoclonal antibodies, their pharmacological activity is primarily driven by their payload. The payload may induce adverse events like decreased platelet count and ILD, which are distinct from adverse events specific to non-ADC molecular targeted agents (e.g., trastuzumab and neratinib). Thus, PCA successfully demonstrated differences in adverse events based on drug characteristics (Figure 3c,d). Through this comprehensive evaluation, each principal component captured clinically relevant, drug-specific adverse event profiles, providing valuable insights to predict side effects and formulate management strategies during treatment selection.
3.5. Limitations
This study has several limitations. First, because the FAERS database is based on spontaneous reports, it may be subject to reporting bias and contain incomplete or inaccurate information. The number of reports can vary depending on the reporter’s interest level, and not all adverse events are consistently documented. Mild adverse events may be underreported, whereas severe events are more likely to be frequently captured. Furthermore, the total number of patients receiving HER2 inhibitors is unknown, which precludes an accurate estimation of the true incidence of adverse events. Therefore, our results indicate associations between drugs and adverse events but do not directly demonstrate causality. To establish causal relationships, more rigorous approaches, including randomized controlled trials or large-scale observational studies, are required.
Moreover, confounding factors, including underlying disease, concomitant medications, and treatment duration, were not included in this analysis but may impact adverse event occurrence. Thus, any interpretation of the results must account for both qualitative and quantitative limitations inherent to SRS.
Moreover, given that the ROR calculation process is susceptible to substantial bias, direct comparisons between numerical values are constrained. Accordingly, our study was conducted based on the hypothesis that limiting the analysis to the top 10% of adverse events by report frequency may ensure reliability in ROR-based comparisons.
Despite these limitations, our analysis successfully captured the real-world patterns of adverse event manifestation during clinical use—for example, the association between hair-related adverse events and monoclonal antibodies identified through cluster analysis. Additionally, PCA enabled us to estimate latent components that may influence the adverse events associated with HER2 inhibitors.
4. Materials and Methods
4.1. Data Table Construction
To perform a comprehensive analysis of adverse events associated with HER2 inhibitors, we utilized the FAERS database, which covers cases reported from January 2004 to September 2024 (as of the October 2024 release) [68]. FAERS comprises seven data tables: Demographic (DEMO), DRUG, REAC, Outcome (OUTC), Report Sources (RPSR), Indication (INDI), and Therapy (THER). Data curation, including coding, mapping, and cleaning, was conducted by ArkMS Inc. (https://www.arkms.co.jp/, accessed 13 June 2025). For this analysis, we constructed an integrated analysis table by joining the DRUG and REAC tables using the Primary ID. The DRUG table classified the reported drugs into four categories: primary suspected drug, secondary suspect drug, concomitant drugs, and interactions. For this study, we extracted drugs reported as primary or secondary suspect drugs.
This study was based on anonymized data obtained from a publicly accessible database; therefore, the Ethics Committee of Meiji Pharmaceutical University waived the requirement for ethical approval and informed consent.
4.2. Terminology for Adverse Events and Targeted Drugs
The Medical Dictionary for Regulatory Activities (MedDRA) is an international medical terminology developed by the International Conference on Harmonization of Drug Regulations (ICH) to promote the global sharing of regulatory information on medical products for human use. MedDRA follows a five-level hierarchical structure consisting of System Organ Class (SOC), High Level Group Terms (HLGT), High Level Terms (HLT), Preferred Terms (PT), and Lowest Level Terms (LLT). In this study, adverse events were coded using the (PT of MedDRA version 27.1. HER2-targeted agents approved for the treatment of breast cancer were included in this analysis.
4.3. Relationship Between HER2 Inhibitors and Adverse Events
We used the ROR, its 95% confidence interval, and the p-value derived from Fisher’s exact test to assess the relationship between HER2 inhibitors and adverse events. When the contingency tables contained zero cells, the ROR calculation was not feasible, and the estimation became unstable. To correct for potential bias, we applied the Haldane–Anscombe correction by adding 0.5 to each cell value [69].
We constructed 2 × 2 contingency tables to investigate the associations between HER2 inhibitors and all reported adverse events (Figure 5). Based on these tables, RORs were calculated to estimate the strength of associations. Subsequently, the ROR values and Fisher’s exact test were used to evaluate the statistical significance of adverse events associated with HER2 inhibitors.
4.4. Construction of the Data Matrix for Clustering and PCA
To investigate the associations between HER2 inhibitors and adverse events, we used the natural logarithm of the ROR (lnROR) as a quantitative indicator. A data matrix of lnROR values was constructed for adverse events frequently reported with HER2 inhibitors. Adverse events selected for analysis were those with >1,500 reports, which covered approximately the top 10% in frequency among all HER2 inhibitors. Nine agents were included: TKIs (lapatinib, neratinib, tucatinib, pyrotinib); mAbs (trastuzumab, pertuzumab, margetuximab); and ADCs (T-DM1, T-DXd). The resulting lnROR matrix was incorporated into Table S1.
4.5. Hierarchical Clustering Analysis
To classify the adverse events associated with HER2 inhibitors, hierarchical clustering analysis (Ward’s method) was performed based on the lnROR matrix constructed in Section 4.4. The number of clusters was determined by examining the distance graph and identifying the inflection point where the slope sharply increased, which was considered optimal.
4.6. PCA
PCA was conducted using the lnROR matrix described in Section 4.4, with the analysis based on a correlation coefficient matrix.
To evaluate the multivariate relationships between HER2 inhibitors and adverse events, the HER2-targeted drugs were treated as a unified group. The group-wise lnROR values were utilized to assess correlations with principal components. Specifically, lnROR values across 61 adverse events were plotted against the principal components, and regression lines were fitted to visually examine the relationship between adverse event trends and each component (Figure 4).
Furthermore, correlation coefficients (r) derived from the PCA loading matrix were used to quantify the relationship between each drug and its respective principal components.
4.7. Statistical Analysis
The database processing, cluster analysis, and PCA were performed using JMP Pro 18.2 (SAS Institute Inc., Cary, NC, USA). To construct the 2 × 2 contingency tables, calculate RORs (Figure 1), derive 95% confidence intervals, and conduct Fisher’s exact tests, we utilized the Python environment with the pandas and SciPy packages. All statistical significance thresholds were set at p < 0.05.
5. Conclusions
In this study, we performed a comprehensive evaluation of adverse events associated with HER2 inhibitors using data mining techniques such as clustering analysis and PCA. The results demonstrated a strong correlation between mAbs and hair-related adverse events. Furthermore, PCA revealed that principal component 2 effectively distinguished between mAbs and TKIs, whereas principal component 3 differentiated between the adverse event profiles of pure molecular targeted agents and ADCs.
These findings enable a visual understanding of the adverse event trends linked to each HER2 inhibitor used during the treatment of HER2-positive breast cancer. The comprehensive visualization of drug-specific adverse event features in real-world settings may facilitate intuitive grasp and practical handling of these agents by medical professionals. Additionally, examining real-world safety profiles for individual drugs may promote intuitive comprehension among medical professionals when handling these agents in clinical practice. Additionally, similar adverse event patterns across different agents may encourage shared strategies in side effect management, contributing to improved strategic planning. Ultimately, these insights are expected to facilitate treatment approach optimization focusing on QoL enhancement and improve both drug selection and adverse event management.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Supplementary Table 1. Statistical summary of the top 61 adverse events associated with HER2 inhibitors based on reporting odds ratios (RORs)
Author Contributions
Conceptualization, Y.U.; Methodology, Y.U.; Software, Y.U.; Validation, A.Y. and Y.U.; Formal Analysis, A.Y. and Y.U.; Investigation, A.Y. and Y.U.; Resources, A.Y. and Y.U.; Data Curation, A.Y. and Y.U.; Writing—Original Draft Preparation, A.Y. and Y.U.; Writing—Review & Editing, A.Y. and Y.U.; Visualization, A.Y. and Y.U.; Supervision, A.Y. and Y.U.; Project Administration, Y.U.; Funding Acquisition, Y.U. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially funded by the Grants-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Science (JSPS), grant number 22K06707.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article and Supplementary Materials.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| FDA | Food and Drug Administration |
| ILD | Interstitial lung disease |
| JSPS | Japan Society for the Promotion of Science |
| PCA | Principal component analysis |
| QoL | Quality of life |
| ROR | Reporting odds ratios |
| SRS | Spontaneous reporting systems |
| mAb | Monoclonal antibodies |
| ADC | Antibody-drug conjugates |
| TKI | Tyrosine kinase inhibitors |
References
- Coussens, L.; Yang-Feng, T.L.; Liao, Y.C.; Chen, E.; Gray, A.; McGrath, J.; Seeburg, P.H.; Libermann, T.A.; Schlessinger, J.; Francke, U.; et al. Tyrosine kinase receptor with extensive homology to EGF receptor shares chromosomal location with neu oncogene. Science 1985, 230, 1132–1139. [Google Scholar] [CrossRef]
- Schechter, A.L.; Stern, D.F.; Vaidyanathan, L.; Decker, S.J.; Drebin, J.A.; Greene, M.I.; Weinberg, R.A. The neu oncogene: an erb-B-related gene encoding a 185,000-Mr tumour antigen. Nature 1984, 312, 513–516. [Google Scholar] [CrossRef]
- Gravalos, C.; Jimeno, A. HER2 in gastric cancer: a new prognostic factor and a novel therapeutic target. Ann. Oncol. 2008, 19, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Cameron, D.; Piccart-Gebhart, M.J.; Gelber, R.D.; Procter, M.; Goldhirsch, A.; de Azambuja, E.; Castro, G., Jr.; Untch, M.; Smith, I.; Gianni, L.; et al. 11 years’ follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive early breast cancer: final analysis of the HERceptin Adjuvant (HERA) trial. Lancet 2017, 389, 1195–1205. [Google Scholar] [CrossRef]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.; Jackisch, C.; et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef] [PubMed]
- Joensuu, H.; Kellokumpu-Lehtinen, P.L.; Bono, P.; Alanko, T.; Kataja, V.; Asola, R.; Utriainen, T.; Kokko, R.; Hemminki, A.; Tarkkanen, M.; et al. Adjuvant docetaxel or vinorelbine with or without trastuzumab for breast cancer. N. Engl. J. Med. 2006, 354, 809–820. [Google Scholar] [CrossRef]
- Giordano, S.H.; Franzoi, M.A.B.; Temin, S.; Anders, C.K.; Chandarlapaty, S.; Crews, J.R.; Kirshner, J.J.; Krop, I.E.; Lin, N.U.; Morikawa, A.; et al. Systemic therapy for advanced human epidermal growth factor receptor 2-positive breast cancer: ASCO guideline update. J. Clin. Oncol. 2022, 40, 2612–2635. [Google Scholar] [CrossRef]
- Gianni, L.; Pienkowski, T.; Im, Y.H.; Roman, L.; Tseng, L.M.; Liu, M.C.; Lluch, A.; Staroslawska, E.; de la Haba-Rodriguez, J.; Im, S.A.; et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Huang, C.S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef]
- Hurvitz, S.A.; Hegg, R.; Chung, W.P.; Im, S.A.; Jacot, W.; Ganju, V.; Chiu, J.W.Y.; Xu, B.; Hamilton, E.; Madhusudan, S.; et al. Trastuzumab deruxtecan versus trastuzumab emtansine in patients with HER2-positive metastatic breast cancer: Updated results from DESTINY-Breast03, a randomised, open-label, phase 3 trial. Lancet 2023, 401, 105–117. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Schwedler, K.; Schmidt, M.; Barinoff, J.; Mundhenke, C.; Cufer, T.; Maartense, E.; de Jongh, F.E.; Baumann, K.H.; Bischoff, J.; et al. Trastuzumab beyond progression: Overall survival analysis of the GBG 26/BIG 3-05 phase III study in HER2-positive breast cancer. Eur. J. Cancer 2011, 47, 2273–2281. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Mueller, V.; Borges, V.; Hamilton, E.; Hurvitz, S.; Loi, S.; Murthy, R.; Okines, A.; Paplomata, E.; Cameron, D.; et al. Corrigendum to “Tucatinib versus placebo added to trastuzumab and capecitabine for patients with pretreated HER2-positive metastatic breast cancer with and without brain metastases (HER2CLIMB): Final overall survival analysis. ” Ann. Oncol. 2023, 34, 630. [Google Scholar] [CrossRef] [PubMed]
- Saura, C.; Oliveira, M.; Feng, Y.H.; Dai, M.S.; Chen, S.W.; Hurvitz, S.A.; Kim, S.B.; Moy, B.; Delaloge, S.; Gradishar, W.; et al. Neratinib plus capecitabine versus lapatinib plus capecitabine in HER2-positive metastatic breast cancer previously treated with ≥2 HER2-directed regimens: Phase III NALA trial. J. Clin. Oncol. 2020, 38, 3138–3149. [Google Scholar] [CrossRef]
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef]
- Harpaz, R.; Perez, H.; Chase, H.S.; Rabadan, R.; Hripcsak, G.; Friedman, C. Biclustering of adverse drug events in the FDA’s spontaneous reporting system. Clin. Pharmacol. Ther. 2011, 89, 243–250. [Google Scholar] [CrossRef]
- Hamazaki, R.; Uesawa, Y. Characterization of antineoplastic agents inducing taste and smell disorders using the FAERS database. Pharmaceuticals 2024, 17, 1116. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.; Chen, J.; Duan, L.; Wang, F.; Lai, H.; Mo, Z.; Zhu, W. Comparing the difference of adverse events with HER2 inhibitors: A study of the FDA adverse event reporting system (FAERS). Front. Pharmacol. 2024, 15, 1288362. [Google Scholar] [CrossRef]
- Schlam, I.; Swain, S.M. HER2-positive breast cancer and tyrosine kinase inhibitors: The time is now. NPJ Breast Cancer 2021, 7, 56. [Google Scholar] [CrossRef]
- Press, M.F.; Cordon-Cardo, C.; Slamon, D.J. Expression of the HER-2/neu proto-oncogene in normal human adult and fetal tissues. Oncogene 1990, 5, 953–962. [Google Scholar]
- Hu, W.; Yang, J.; Zhang, Z.; Xu, D.; Li, N. Pyrotinib for HER2-positive metastatic breast cancer: A systematic review and meta-analysis. Transl. Cancer Res. 2023, 12, 247–256. [Google Scholar] [CrossRef]
- Yang, Z.; Meng, J.; Mei, X.; Mo, M.; Xiao, Q.; Han, X.; Zhang, L.; Shi, W.; Chen, X.; Ma, J.; et al. Brain radiotherapy with pyrotinib and capecitabine in patients with ERBB2-positive advanced breast cancer and brain metastases: A nonrandomized phase 2 trial. JAMA Oncol. 2024, 10, 335–341. [Google Scholar] [CrossRef]
- Hurvitz, S.A.; Kim, S.B.; Chung, W.P.; Im, S.A.; Park, Y.H.; Hegg, R.; Kim, M.H.; Tseng, L.M.; Petry, V.; Chung, C.F.; et al. Trastuzumab deruxtecan versus trastuzumab emtansine in HER2-positive metastatic breast cancer patients with brain metastases from the randomized DESTINY-Breast03 trial. ESMO Open 2024, 9, 102924. [Google Scholar] [CrossRef]
- Baselga, J.; Cortés, J.; Kim, S.B.; Im, S.A.; Hegg, R.; Im, Y.H.; Roman, L.; Pedrini, J.L.; Pienkowski, T.; Knott, A.; et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N. Engl. J. Med. 2012, 366, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.R.; Im, S.A.; Mattar, A.; Colomer, R.; Stroyakovskii, D.; Nowecki, Z.; De Laurentiis, M.; Pierga, J.Y.; Jung, K.H.; Schem, C.; et al. Fixed-dose combination of pertuzumab and trastuzumab for subcutaneous injection plus chemotherapy in HER2-positive early breast cancer (FeDeriCa): A randomised, open-label, multicentre, non-inferiority, phase 3 study. Lancet Oncol. 2021, 22, 85–97. [Google Scholar] [CrossRef]
- Fairlamb, D.J. Hair changes following cytotoxic drug induced alopecia. Postgrad. Med. J. 1988, 64, 907. [Google Scholar] [CrossRef] [PubMed]
- Tobin, D.J.; Hagen, E.; Botchkarev, V.A.; Paus, R. Do hair bulb melanocytes undergo apoptosis during hair follicle regression (catagen)? J. Investig. Dermatol. 1998, 111, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Westgate, G.E.; Ginger, R.S.; Green, M.R. The biology and genetics of curly hair. Exp. Dermatol. 2017, 26, 483–490. [Google Scholar] [CrossRef]
- Bernard, B.A. The hair follicle enigma. Exp. Dermatol. 2017, 26, 472–477. [Google Scholar] [CrossRef]
- Belum, V.R.; Marulanda, K.; Ensslin, C.; Gorcey, L.; Parikh, T.; Wu, S.; Busam, K.J.; Gerber, P.A.; Lacouture, M.E. Alopecia in patients treated with molecularly targeted anticancer therapies. Ann. Oncol. 2015, 26, 2496–2502. [Google Scholar] [CrossRef]
- Nordstrom, J.L.; Gorlatov, S.; Zhang, W.; Yang, Y.; Huang, L.; Burke, S.; Li, H.; Ciccarone, V.; Zhang, T.; Stavenhagen, J.; et al. Anti-tumor activity and toxicokinetics analysis of MGAH22, an anti-HER2 monoclonal antibody with enhanced Fcγ receptor binding properties. Breast Cancer Res. 2011, 13, R123. [Google Scholar] [CrossRef]
- Stavenhagen, J.B.; Gorlatov, S.; Tuaillon, N.; Rankin, C.T.; Li, H.; Burke, S.; Huang, L.; Vijh, S.; Johnson, S.; Bonvini, E.; et al. Fc optimization of therapeutic antibodies enhances their ability to kill tumor cells in vitro and controls tumor expansion in vivo via low-affinity activating Fcγ receptors. Cancer Res. 2007, 67, 8882–8890. [Google Scholar] [CrossRef]
- Rugo, H.S.; Im, S.A.; Cardoso, F.; Cortés, J.; Curigliano, G.; Musolino, A.; Pegram, M.D.; Wright, G.S.; Saura, C.; Escrivá-de-Romaní, S.; et al. Efficacy of margetuximab vs trastuzumab in patients with pretreated ERBB2-positive advanced breast cancer: A phase 3 randomized clinical trial. JAMA Oncol. 2021, 7, 573–584. [Google Scholar] [CrossRef]
- Menopause Hair Care: Understanding the Changes and Solutions. Available online: https://restorehairguide.com/does-herceptin-cause-hair-loss-unraveling-the-connection/ (accessed on 14 June 2025).
- Lin, N.U.; Diéras, V.; Paul, D.; Lossignol, D.; Christodoulou, C.; Stemmler, H.J.; Roché, H.; Liu, M.C.; Greil, R.; Ciruelos, E.; et al. Multicenter phase II study of lapatinib in patients with brain metastases from HER2-positive breast cancer. Clin. Cancer Res. 2009, 15, 1452–1459. [Google Scholar] [CrossRef]
- Bachelot, T.; Romieu, G.; Campone, M.; Diéras, V.; Cropet, C.; Dalenc, F.; Jimenez, M.; Le Rhun, E.; Pierga, J.Y.; Gonçalves, A.; et al. Lapatinib plus capecitabine in patients with previously untreated brain metastases from HER2-positive metastatic breast cancer (LANDSCAPE): A single-group phase 2 study. Lancet Oncol. 2013, 14, 64–71. [Google Scholar] [CrossRef]
- Freedman, R.A.; Gelman, R.S.; Anders, C.K.; Melisko, M.E.; Parsons, H.A.; Cropp, A.M.; Silvestri, K.; Cotter, C.M.; Componeschi, K.P.; Marte, J.M.; et al. TBCRC 022: A phase II trial of neratinib and capecitabine for patients with human epidermal growth factor receptor 2-positive breast cancer and brain metastases. J. Clin. Oncol. 2019, 37, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.U.; Borges, V.; Anders, C.; Murthy, R.K.; Paplomata, E.; Hamilton, E.; Hurvitz, S.; Loi, S.; Okines, A.; Abramson, V.; et al. Intracranial efficacy and survival with tucatinib plus trastuzumab and capecitabine for previously treated HER2-positive breast cancer with brain metastases in the HER2CLIMB trial. J. Clin. Oncol. 2020, 38, 2610–2619. [Google Scholar] [CrossRef]
- Yin, O.; Xiong, Y.; Endo, S.; Yoshihara, K.; Garimella, T.; AbuTarif, M.; Wada, R.; LaCreta, F. Population pharmacokinetics of trastuzumab deruxtecan in patients with HER2-positive breast cancer and other solid tumors. Clin. Pharmacol. Ther. 2021, 109, 1314–1325. [Google Scholar] [CrossRef] [PubMed]
- Venur, V.A.; Leone, J.P. Targeted therapies for brain metastases from breast cancer. Int. J. Mol. Sci. 2016, 17, 1543. [Google Scholar] [CrossRef] [PubMed]
- Mair, M.J.; Bartsch, R.; Le Rhun, E.; Berghoff, A.S.; Brastianos, P.K.; Cortes, J.; Gan, H.K.; Lin, N.U.; Lassman, A.B.; Wen, P.Y.; et al. Understanding the activity of antibody–drug conjugates in primary and secondary brain tumours. Nat. Rev. Clin. Oncol. 2023, 20, 372–389. [Google Scholar] [CrossRef]
- Askoxylakis, V.; Ferraro, G.B.; Kodack, D.P.; Badeaux, M.; Shankaraiah, R.C.; Seano, G.; Kloepper, J.; Vardam, T.; Martin, J.D.; Naxerova, K.; et al. Preclinical efficacy of ado-trastuzumab emtansine in the brain microenvironment. J. Natl. Cancer Inst. 2015, 108, djv313. [Google Scholar] [CrossRef]
- Ma, F.; Ouyang, Q.; Li, W.; Jiang, Z.; Tong, Z.; Liu, Y.; Li, H.; Yu, S.; Feng, J.; Wang, S.; et al. Pyrotinib or lapatinib combined with capecitabine in HER2-positive metastatic breast cancer with prior taxanes, anthracyclines, and/or trastuzumab: A randomized, phase II study. J. Clin. Oncol. 2019, 37, 2610–2619. [Google Scholar] [CrossRef]
- Barcenas, C.H.; Hurvitz, S.A.; Di Palma, J.A.; Bose, R.; Chien, A.J.; Iannotti, N.; Marx, G.; Brufsky, A.; Litvak, A.; Ibrahim, E.; et al. Improved tolerability of neratinib in patients with HER2-positive early-stage breast cancer: The CONTROL trial. Ann. Oncol. 2020, 31, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Rugo, H.S.; Bianchini, G.; Cortes, J.; Henning, J.W.; Untch, M. Optimizing treatment management of trastuzumab deruxtecan in clinical practice of breast cancer. ESMO Open 2022, 7, 100553. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Li, Y.; Zhu, C.; Dong, Q.; Zhang, Y.; Liu, Z.; Ren, D.; Zhao, F.; Zhao, J. Disproportionality analysis of interstitial lung disease associated with novel antineoplastic agents during breast cancer treatment: A pharmacovigilance study. EClinicalMedicine 2025, 82, 103160. [Google Scholar] [CrossRef] [PubMed]
- Saglio, G.; Kim, D.W.; Issaragrisil, S.; le Coutre, P.; Etienne, G.; Lobo, C.; Pasquini, R.; Clark, R.E.; Hochhaus, A.; Hughes, T.P.; et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N. Engl. J. Med. 2010, 362, 2251–2259. [Google Scholar] [CrossRef]
- Hughes, T.P.; Munhoz, E.; Salvino, M.A.; Ong, T.C.; Elhaddad, A.; Shortt, J.; Quach, H.; Pavlovsky, C.; Louw, V.J.; Shih, L.Y.; et al. Nilotinib dose-optimization in newly diagnosed chronic myeloid leukaemia in chronic phase: final results from ENESTxtnd. Br. J. Haematol. 2017, 179, 219–228. [Google Scholar] [CrossRef]
- Aguilera, D.G.; Tsimberidou, A.M. Dasatinib in chronic myeloid leukemia: A review. Ther. Clin. Risk Manag. 2009, 5, 281–289. [Google Scholar] [CrossRef]
- Bendell, J.C.; Domchek, S.M.; Burstein, H.J.; Harris, L.; Younger, J.; Kuter, I.; Bunnell, C.; Rue, M.; Gelman, R.; Winer, E. Central nervous system metastases in women who receive trastuzumab-based therapy for metastatic breast carcinoma. Cancer 2003, 97, 2972–2977. [Google Scholar] [CrossRef]
- Lai, R.; Dang, C.T.; Malkin, M.G.; Abrey, L.E. The risk of central nervous system metastases after trastuzumab therapy in patients with breast carcinoma. Cancer 2004, 101, 810–816. [Google Scholar] [CrossRef]
- Romond, E.H.; Perez, E.A.; Bryant, J.; Suman, V.J.; Geyer, C.E., Jr.; Davidson, N.E.; Tan-Chiu, E.; Martino, S.; Paik, S.; Kaufman, P.A.; et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N. Engl. J. Med. 2005, 353, 1673–1684. [Google Scholar] [CrossRef]
- Swain, S.M.; Baselga, J.; Kim, S.B.; Ro, J.; Semiglazov, V.; Campone, M.; Ciruelos, E.; Ferrero, J.M.; Schneeweiss, A.; Heeson, S.; et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N. Engl. J. Med. 2015, 372, 724–734. [Google Scholar] [CrossRef]
- Cardiotoxicity: An Unexpected Consequence of HER2-Targeted Therapies. Available online: https://www.acc.org/latest-in-cardiology/articles/2016/06/06/09/32/cardiotoxicity (accessed on 14 June 2025).
- Kwakman, J.J.M.; Elshot, Y.S.; Punt, C.J.A.; Koopman, M. Management of cytotoxic chemotherapy-induced hand-foot syndrome. Oncol. Rev. 2020, 14, 442. [Google Scholar] [CrossRef]
- Masuda, N.; Lee, S.J.; Ohtani, S.; Im, Y.H.; Lee, E.S.; Yokota, I.; Kuroi, K.; Im, S.A.; Park, B.W.; Kim, S.B.; et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Sassoon, I.; Blanc, V. Antibody–drug conjugate (ADC) clinical pipeline: A review. Methods Mol. Biol. 2013, 1045, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Manabe, S. Development and current status of antibody–drug conjugate (ADC). Drug Deliv. Syst. 2019, 34, 10–21. [Google Scholar] [CrossRef]
- Ogitani, Y.; Aida, T.; Hagihara, K.; Yamaguchi, J.; Ishii, C.; Harada, N.; Soma, M.; Okamoto, H.; Oitate, M.; Arakawa, S.; et al. DS-8201a, a novel HER2-targeting ADC with a novel DNA topoisomerase I inhibitor, demonstrates a promising antitumor efficacy with differentiation from T-DM1. Clin. Cancer Res. 2016, 22, 5097–5108. [Google Scholar] [CrossRef]
- Nakada, T.; Sugihara, K.; Jikoh, T.; Abe, Y.; Agatsuma, T. The latest research and development into the antibody–drug conjugate, [fam-] trastuzumab deruxtecan (DS-8201a), for HER2 cancer therapy. Chem. Pharm. Bull. (Tokyo) 2019, 67, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Doronina, S.O.; Toki, B.E.; Torgov, M.Y.; Mendelsohn, B.A.; Cerveny, C.G.; Chace, D.F.; DeBlanc, R.L.; Gearing, R.P.; Bovee, T.D.; Siegall, C.B.; et al. Development of potent monoclonal antibody auristatin conjugates for cancer therapy. Nat. Biotechnol. 2003, 21, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Uppal, H.; Doudement, E.; Mahapatra, K.; Darbonne, W.C.; Bumbaca, D.; Shen, B.Q.; Du, X.; Saad, O.; Bowles, K.; Olsen, S.; et al. Potential mechanisms for thrombocytopenia development with trastuzumab emtansine (T-DM1). Clin. Cancer Res. 2015, 21, 123–133. [Google Scholar] [CrossRef]
- Doi, T.; Shitara, K.; Naito, Y.; Shimomura, A.; Fujiwara, Y.; Yonemori, K.; Shimizu, C.; Shimoi, T.; Kuboki, Y.; Matsubara, N.; et al. Safety, pharmacokinetics, and antitumour activity of trastuzumab deruxtecan (DS-8201), a HER2-targeting antibody–drug conjugate, in patients with advanced breast and gastric or gastro-oesophageal tumours: A phase 1 dose-escalation study. Lancet Oncol. 2017, 18, 1512–1522. [Google Scholar] [CrossRef]
- von Arx, C.; De Placido, P.; Caltavituro, A.; Di Rienzo, R.; Buonaiuto, R.; De Laurentiis, M.; Arpino, G.; Puglisi, F.; Giuliano, M.; Del Mastro, L. The evolving therapeutic landscape of trastuzumab–drug conjugates: Future perspectives beyond HER2-positive breast cancer. Cancer Treat. Rev. 2023, 113, 102500. [Google Scholar] [CrossRef]
- Kumagai, K.; Aida, T.; Tsuchiya, Y.; Kishino, Y.; Kai, K.; Mori, K. Interstitial pneumonitis related to trastuzumab deruxtecan, a human epidermal growth factor receptor 2-targeting Ab–drug conjugate, in monkeys. Cancer Sci. 2020, 111, 4636–4645. [Google Scholar] [CrossRef] [PubMed]
- FDA Adverse Event Reporting System (FAERS). Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-adverse-event-reporting-system-faers (accessed on 12 June 2025).
- Lawson, R. Small sample confidence intervals for the odds ratio. Commun. Stat. Simul. Comput. 2004, 33, 1095–1113. [Google Scholar] [CrossRef]
Figure 1.
Flowchart for data analysis table construction. The reporting odds ratios (ROR)-calculator generated the data analysis table and the lnROR matrix. The data analysis table is used to examine adverse event reports, calculate p-values, and report RORs and 95% confidence intervals for drugs and adverse reactions. The lnROR matrix was used for hierarchical clustering and PCA.
Figure 1.
Flowchart for data analysis table construction. The reporting odds ratios (ROR)-calculator generated the data analysis table and the lnROR matrix. The data analysis table is used to examine adverse event reports, calculate p-values, and report RORs and 95% confidence intervals for drugs and adverse reactions. The lnROR matrix was used for hierarchical clustering and PCA.
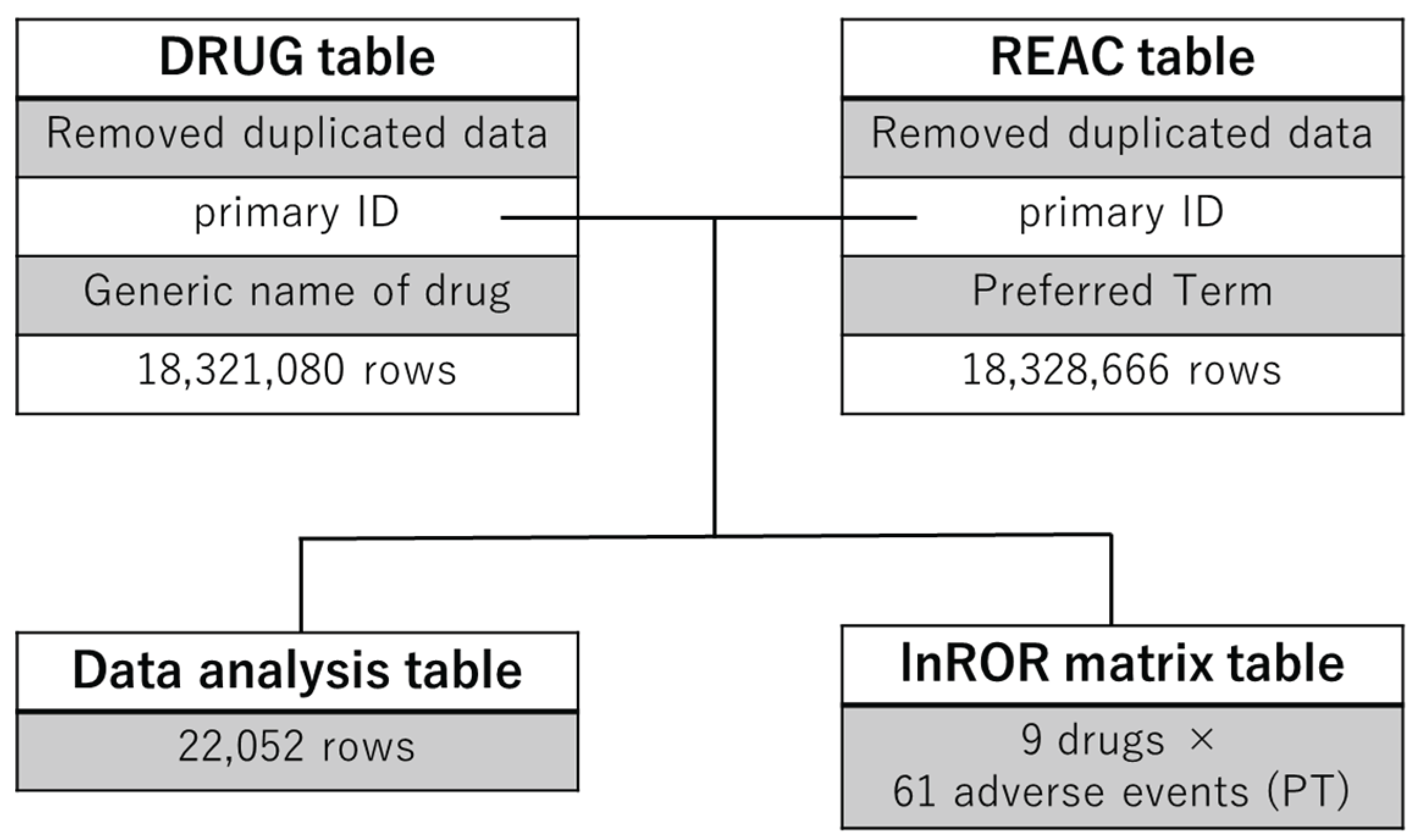
Figure 2.
Hierarchical clustering analysis. This figure illustrates the relationship between nine drugs (three mAbs, two ADCs, and four TKIs) and the top 61 adverse events. In the colormap, red indicates a positive correlation, whereas blue represents a negative correlation.
Figure 2.
Hierarchical clustering analysis. This figure illustrates the relationship between nine drugs (three mAbs, two ADCs, and four TKIs) and the top 61 adverse events. In the colormap, red indicates a positive correlation, whereas blue represents a negative correlation.
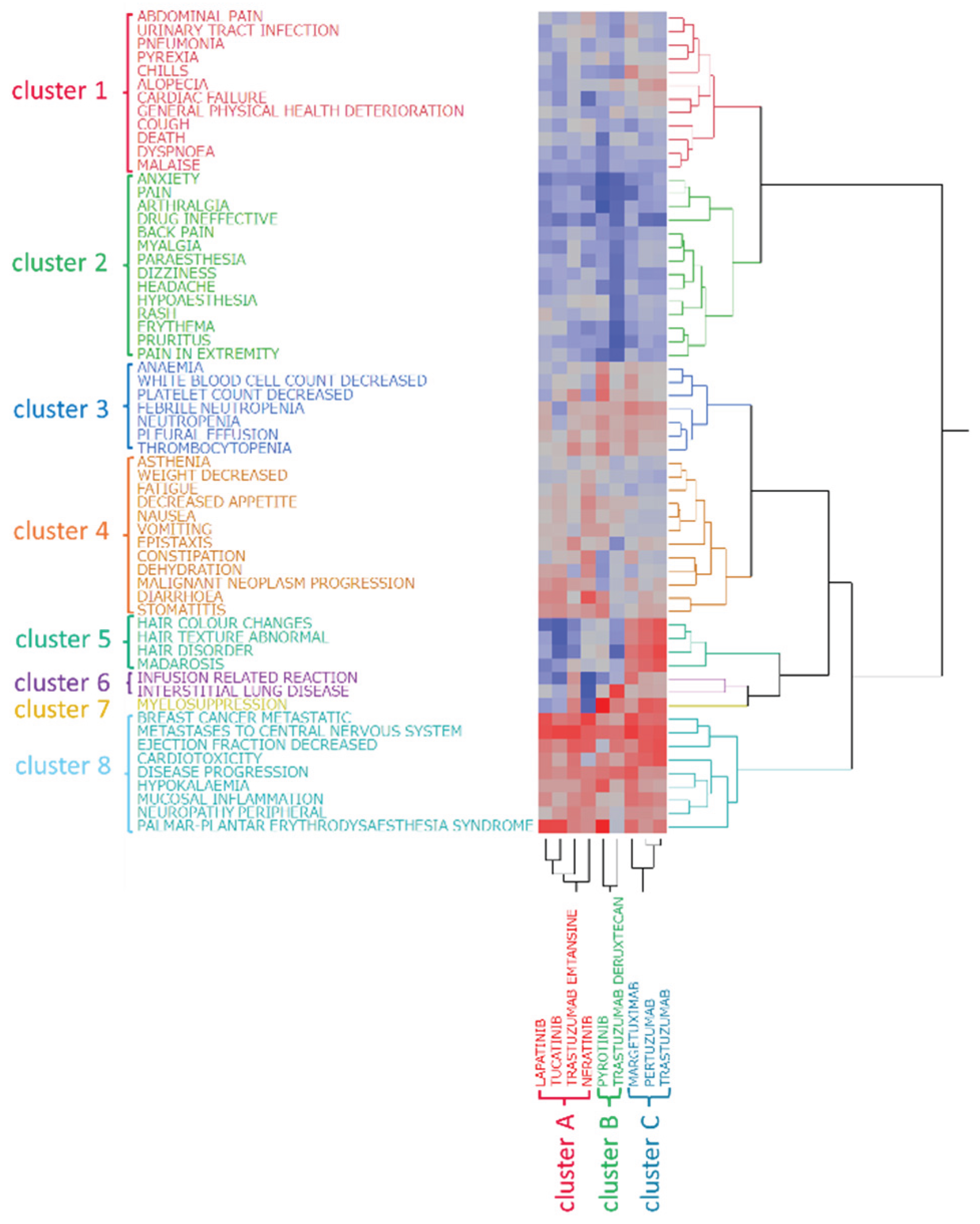
Figure 3.
PCA of the evaluated drugs and major adverse events. The loading plots (a and c) show the relationships between the drugs and principal components, with each vector representing a drug. The score plots (b and d) illustrate the relationships between adverse events and the principal components, with each dot representing an adverse event. Plots are color-coded by the common logarithm of the number of reports (a).
Figure 3.
PCA of the evaluated drugs and major adverse events. The loading plots (a and c) show the relationships between the drugs and principal components, with each vector representing a drug. The score plots (b and d) illustrate the relationships between adverse events and the principal components, with each dot representing an adverse event. Plots are color-coded by the common logarithm of the number of reports (a).
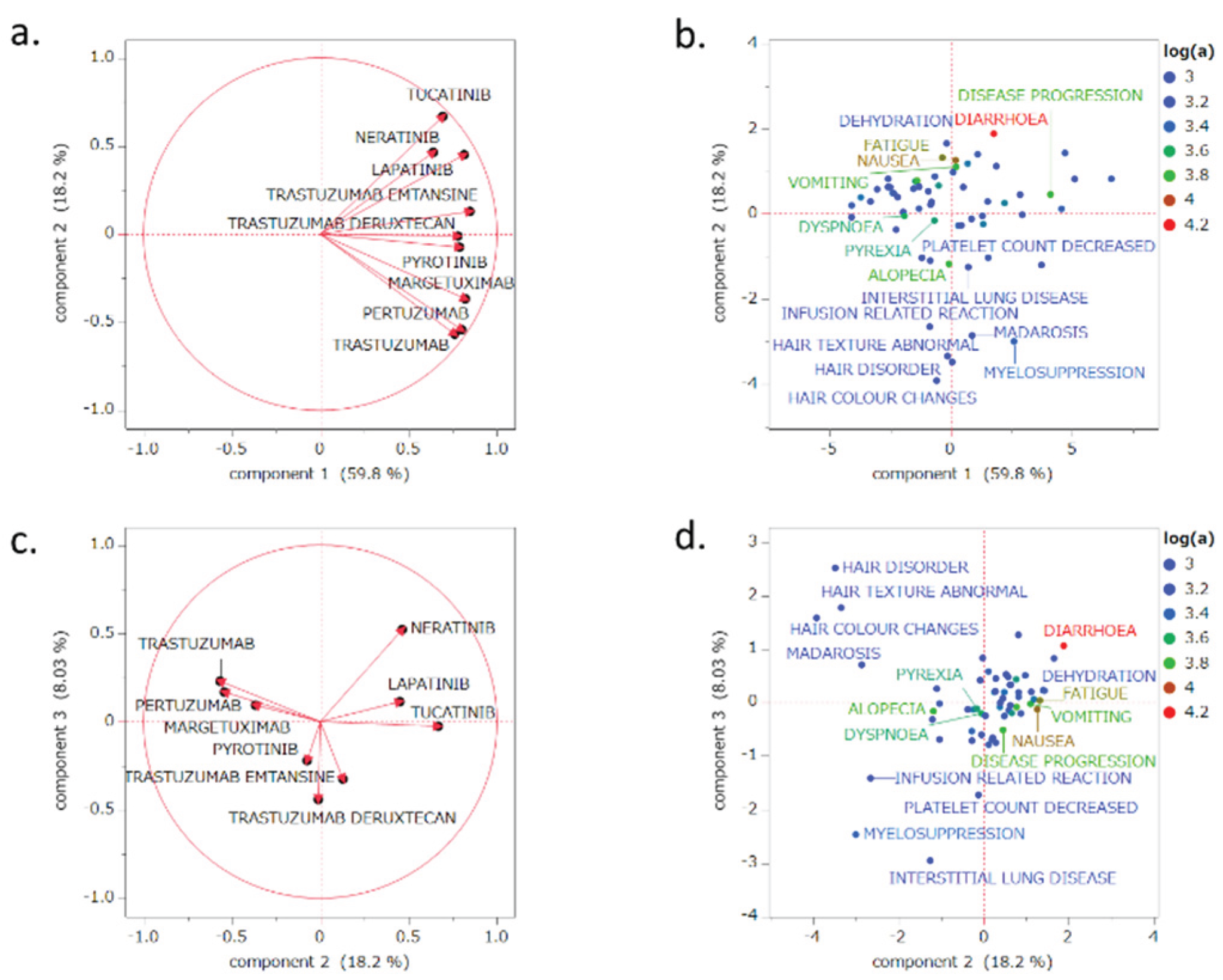
Figure 4.
Scatter plot of principal component 1 and the natural log-transformed reporting odds ratio (lnROR). We evaluated the correlation between principal component 1 and lnROR, which was derived by applying a natural logarithmic transformation to the ROR calculated from all analyzed drugs treated as a single group of HER2 inhibitors. The drugs were plotted, and a least squares regression line was fitted to the data.
Figure 4.
Scatter plot of principal component 1 and the natural log-transformed reporting odds ratio (lnROR). We evaluated the correlation between principal component 1 and lnROR, which was derived by applying a natural logarithmic transformation to the ROR calculated from all analyzed drugs treated as a single group of HER2 inhibitors. The drugs were plotted, and a least squares regression line was fitted to the data.
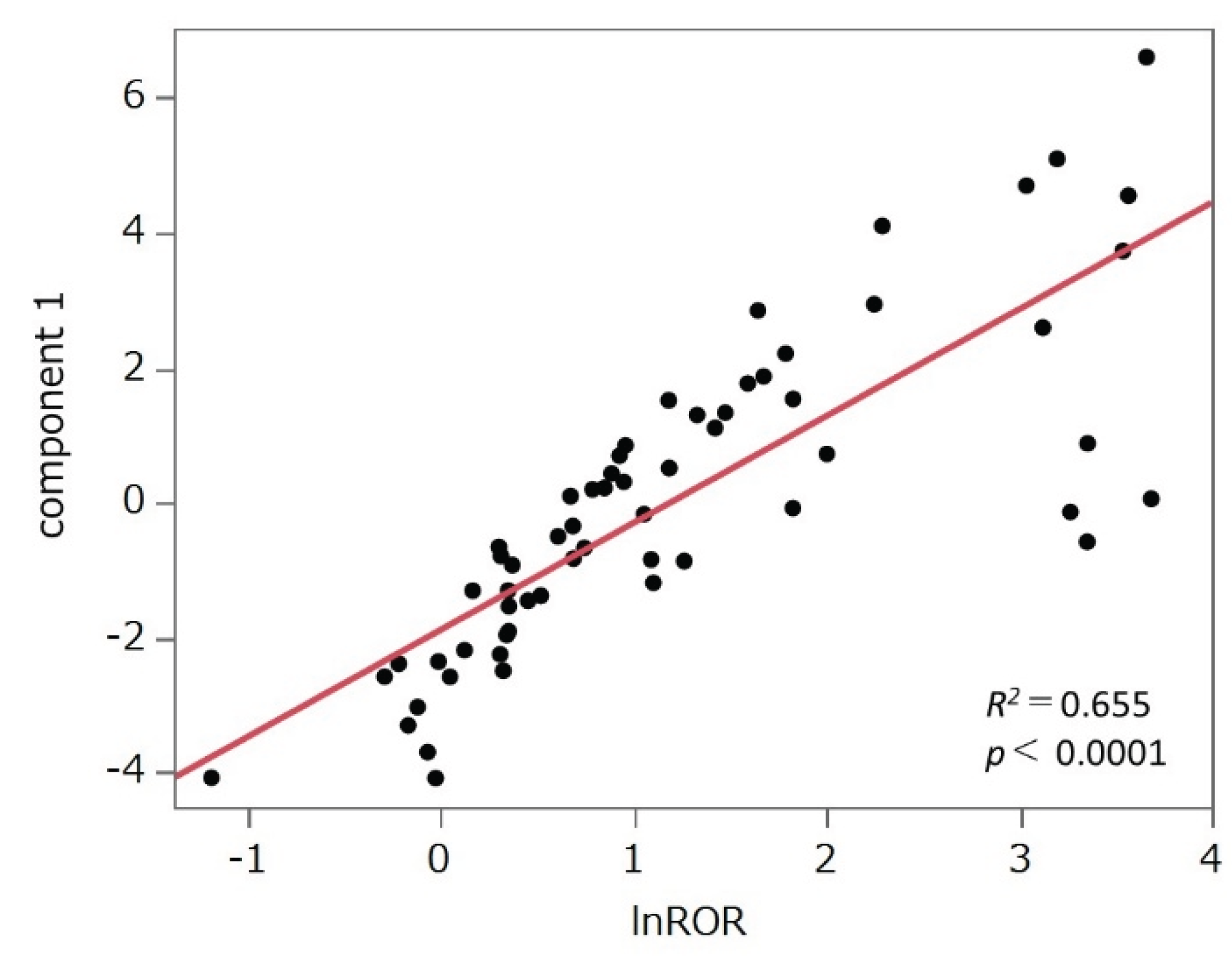
Figure 5.
Cross-tabulation and formula used to calculate ROR for disproportionality analysis.
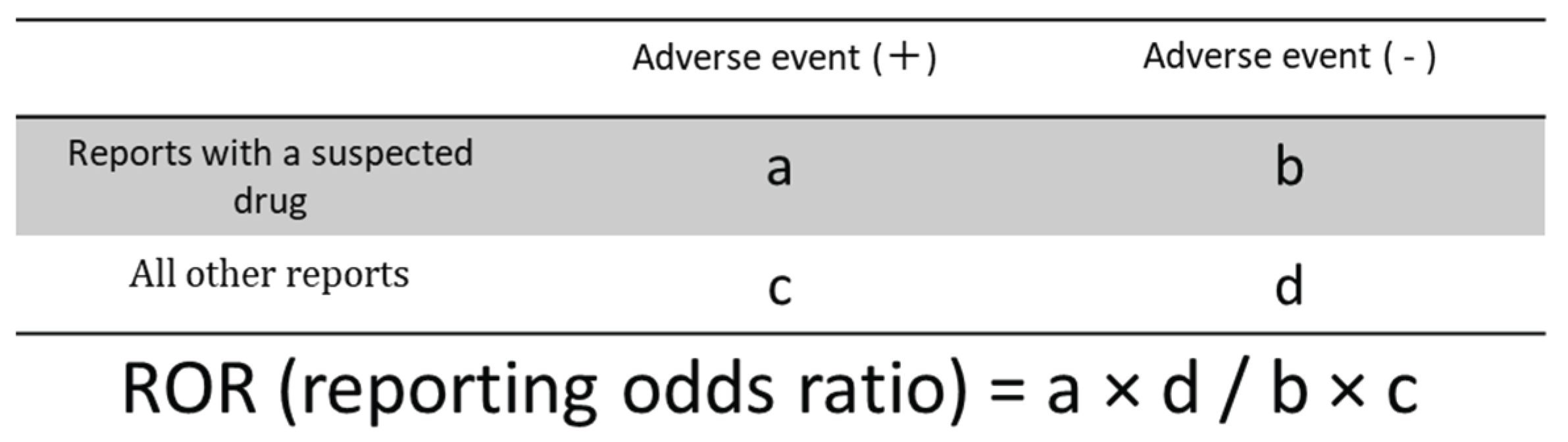

Table 1.
Number of reported adverse events.
| Drug | Number of cases |
|---|---|
| Monoclonal antibodies (mAbs) | 94,516 |
| Trastuzumab | 67,765 |
| Pertuzumab | 26,692 |
| Margetuximab | 59 |
| Antibody-drug conjugates (ADCs) | 13,381 |
| Trastuzumab emtansine (T-DM1) | 7,897 |
| Trastuzumab deruxtecan (T-DXd) | 5,484 |
| Tyrosine kinase inhibitors (TKIs) | 23,967 |
| Lapatinib | 16,073 |
| Tucatinib | 5,402 |
| Neratinib | 2,162 |
| Pyrotinib | 330 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



