Submitted:
30 July 2025
Posted:
01 August 2025
You are already at the latest version
Abstract
The built environment is one of the determinants of health as it acts as a promoter of healthy lifestyles. This research is dealing with the investigation of design solutions to promote healthy and active aging in socio-health care facilities for primary care in Italy. This is a three year research which aims at developing Design Guidelines of waiting space in Casa della Comunità (House of the Community, a new model of territorial primary care facility in Italy) to promote good health for all people. According to these goals, the research mixed different research methods in three main phases: background research, starting from literature review to define a Theoretical Framework; data collection and field research, dealing with technical analysis of international best practices, perceptive analysis through interviews and questionnaires to the staff, patients and caregivers of the socio-health care facilities, in order to define spatial requirements for waiting spaces; results, developing tools and design solutions of health-promotive waiting spaces (Design Guidelines and two applications in virtual reality pilot and in a physical one in Florence, Italy). In this contribution, we focus on the background and field research phase, describing the process leading to the definition of spatial requirements for Casa della Comunità’s waiting spaces.
Keywords:
health promotion
; active design
; healthy and active ageing
; sensory design
; waiting spaces
; primary care
1. Introduction
The Italian health reform DM 77/2022 [1] is promoting the spread of local socio-healthcare facilities on the National territory to support well-being and health promotion in communities. The House of the Community (Case della Comunità - CdC) is a new model of primary care facility [2] with the aim of treatment, prevention and health promotion, focusing on chronic diseases and continuous care for elderly. It is a physical place where people should be welcomed to have access to health and social knowledge and assistance. For this reason, the configuration of spaces and the characters of the environment are very important, aiming at promoting comfort, wellbeing and inclusion.
It is now consolidated in the scientific literature that the built environment influences public health as it acts as a promoter of healthy lifestyles [3]: doing physical activity, having a healthy diet, being involved in positive social interactions. Healthy lifestyles help to prevent chronic diseases (such as cardiovascular diseases, diabetes, some types of cancer) and physical and cognitive decline [4]. Thus, actions aimed at supporting fragility and combating loneliness also benefit from the design of a healthy and inclusive built environment.
Waiting spaces can have a specific and crucial role in this field, using the time of waiting to involve people in the interaction with the space to promote health and the social community. Despite a growing understanding of the importance of the built environment for health, there remains limited research on how specific architectural features of waiting spaces impact well-being in the context of primary care and no evidence about design of Case della Comunità.
For this reason, this research, part of Age-it project1 for active and healthy ageing, deals with the study of waiting spaces of local socio-health care facilities for primary care (CdC), proposing sensory waiting environments which promote health: reducing stress before the healthcare interventions and favouring relations with professionals; supporting physical and mental wellbeing and rehabilitation, by psychological support and physical activity; favouring the prevention of chronic diseases and healthy life styles. Moreover, in this period of rapid demographic changes and increasing demands on healthcare systems, rethinking waiting environments is not only a matter of comfort, but also a question of public health and social sustainability.
2. Materials and Methods
The research has been led in three years by three main phases, as summarised in the diagram in Figure 1: background research, data collection and field research, results and application (tools and solutions).
Each phase has generated the next one: the background research was the basis for the definition of a Theoretical Framework, a tool to lead the data collection and the field research phase (technical and perceptive analysis); the field research phase generated case studies sheets and space and perceptive requirements, which have represented the basis for the development of Design Guidelines.
The Design Guidelines are the main result of the research, presenting strategies and solutions to design CdC’s waiting spaces; these have then been applied in two pilots:
- a virtual model of a sensory waiting space, built in collaboration with STIIMA CNR (Intelligent Industrial Technologies and Systems for Advanced Manufacturing, Italian national research council), IRCCS INRCA (Innovative Models for Ageing Care and Technology) and UNICATT (Catholic University of the Sacred Heart);
- a physical pilot by the renovation of waiting spaces of the existent CdC Le Piagge in Florence (the construction is now in progress, inauguration previewed for next October).
These two pilots are going to be validated in the next year and feedback will be used for a final revision of the Design Guidelines, to verify the efficacy of this tool as a support to design for professionals.
The development of the Design Guidelines [5] and the results of the two pilots will be presented in other specific publications.
2.1. Background Research and Theoretical Framework
As presented in the introduction, the research aims at supporting the design process of waiting spaces to: i) reduce patients and caregivers/visitors’ stress, in particular during the waiting time, in the phase preceding the healthcare service; ii) support people’s psychological comfort; iii) promote healthy and active aging and prevention of chronic diseases (Figure 2).
These main goals refer to three fundamental groups of theories (Figure 2) from scientific literature which represent the main principles of the research.
The first group of theories refers to the concept that the built environment has an impact on people’s health by altering stress levels. Del Nord, 2006 [6] dedicates one chapter to “the stress and the stressors in the hospital” [7] referring to the factors of the physical dimension of the space which contribute to alter people’s stress to improve the healthcare experience and affect their health. It refers to four specific dimensions of the environment at the building scale which can have an impact on stress/health:
- Stimulation, refers to creating a balance in between sensory stimuli. Overwhelming (e.g., noises, strong lights, etc.) causes stress in people; at the same time, a low stimulation causes sensory deprivation and boredom;
- Coherence, refers to configuring comprehensible and clear building layout to avoid stress;
- Affordance, refers to the ability of an environment to induce the right behaviours and functions/activities;
- Control, refers to the ability of a person to modify the environment to adapt it to the person’s specific needs.
In another chapter “the environment and the perceptive-sensory factors” [8] it suggests operative indications for the design project to make the environment a healing resource to satisfy the physical and psychosocial needs of all the users and contribute positively in healthcare outcomes and caregiving.
In between these salutogenic properties of the environment, the second group of theories refers to those characters of the environment that allow patients, caregivers/visitors and the staff to have “restoration” [9,10,11,12] (by colours, nature, art, etc.) and “coping” [13] stress conditions. “Restoration” refers to the process of recovering cognitive and emotional energies by the interaction with the environment. The restoration process can occur when a person is observing or experiencing nature or art to generate wellbeing and influence human health [14]. The concept of “coping” deals with what a person does (from a cognitive, emotional and behavioural point of view) to face a critical condition. Research has well demonstrated that the environment has an important role in the process of stress/coping. The ability to control the environment and the development of social relations are two main resources of coping [13].
Finally, the third group of theories refer to the concept that the Casa della Comunità has health promotion as the main mission. For this reason, the design of this facility should be based on to the theories of health-promotive architecture [15] and health promoting buildings [16], interpreting the concept of health promotion [17] through the built environment, e.g., active design [18], promotion of physical activity, Healthy Buildings approach [19], etc.
Starting from these groups of theories and following the Requirement Classes of the Building System (UNI 8289:1981), this research focuses on the Wellbeing and Usability classes, also according to the Guidelines for the Humanization of Healthcare Spaces [20]:
- Psycho-emotional well-being and the needs of: privacy, concentration, social interaction, continuity with the home environment, mental disengagement (positive distraction and restoration), psychological support, control, information and involvement;
- Environmental well-being, i.e., the conditions that guarantee physical and sensorial well-being: acoustic, thermo-hygrometric, visual, olfactory, and tactile well-being;
- Usability, i.e., the set of conditions that allow the use of spaces, furnishings and equipment in adequate conditions. More specifically, we analyse the layout and configuration of spaces to favour.
Starting from these fundamentals, we were able to define a Theoretical Framework as an operative tool for the technical analysis phase, leading the collection and the analysis of best practices, led by five main criteria (see Section 2.2.2.), to be able to define spatial requirements for health-promotive waiting spaces.
This Theoretical Framework is based on three main areas of investigation: i) Territorial primary care and CdC, ii) Waiting Areas, iii) Sensory Design.
First of all, we were looking at territorial primary care facilities, such Case della Comunità/Case della Salute, but it was not easy to find similar examples as it represents a new model of healthcare facility. For this reason, we were also looking at Primary Care facilities and Community Centres to identify existing design solutions in waiting spaces for health promotion according to the idea of age-friendly and healthy cities, promoted by WHO - World Health Organisation [21]. Moreover we decided to expand this research, looking at good examples (best practices) of waiting rooms in healthcare facilities for outpatient departments, medical and healthcare centres, also looking at rules and guidelines for welcome spaces, such as Health Building Notes (UK) [22]. Finally, we explore the field of Sensory Design, collecting sensory solutions found in welcome and waiting spaces of both, outpatient departments and primary care facilities. Again, there was a lack of similar experiences, so we decided to spread the research in other contexts, in which sensory environments are commonly used, such as children’s hospitals, geriatric facilities, physiotherapy, etc. to collect effective solutions to be applied to CdC settings.
2.2. Technical Analysis: Case Studies
We identified a gap in literature regarding guidelines for the design of CdC and promoting health through waiting spaces. Starting from Case-based design [23] theory, the authors analysed relevant European case studies to deduct innovative solutions to be applied in the design of waiting spaces in the primary care context and fill the gaps through the application of significant technical-design solutions in this specific context:
- identification of invariants that are common in case studies (welcome and waiting spaces of various types of social and healthcare facilities, e.g., hospital, clinic, health centre, etc.) and can be translated into input for the project;
- innovative ideas related to other contexts or different users, to be reinterpreted and applied to the project. To explore innovation, Sensory Design was identified as an adequate approach to both provide comfort and promote health in waiting spaces, dealing with relaxing, welcoming and customizable environments for different users by the integration of digital technologies.
2.2.1. Selection Criteria
For the first and the second area of investigation, best practices were chosen in between healthcare buildings with innovative design solutions and characters in at least two or three categories described in Section 2.2.2, so much so that they could be defined as “Best Practices”. In particular, they were selected in between hospitals with an outpatient department, outpatient clinics, health houses or local primary care facilities that were presenting interesting or innovative solutions for welcome and waiting spaces. European buildings were selected in order to evaluate examples close in size and in the social and cultural context, designed and built since the 2000s. Specialized healthcare facilities were excluded, such as emergency departments, cancer centres, paediatric hospitals, dental clinics etc. as they would represent different solutions for requirements and context. The research was carried out through literature review and online search engines on dedicated portals (e.g., google, archdaily, healthcare design, pinterest, architect magazine, architecture for health, dezeen, etc.), by some keywords: hospital AND outpatient AND waiting spaces; european AND hospital AND outpatient AND waiting spaces; (different countries) hospital AND outpatient AND waiting spaces; outpatient department AND elderly; house of community; community hospital; community centre; primary care; medical centre; healthcare architecture AND waiting spaces; healthcare architecture AND elderly.
For the third area, the authors collected Sensory Design examples in European healthcare facilities, built since 2010 by the criteria presented in Bellini and Setola, 2024 [24].
In total 37 case studies were selected: 20 for the first area, as summarized in Table 1, and 17 for the sensory area [24].
By the technical analysis, case studies were summarised in 37 Case Studies Sheets which were showing the contribution of each best practice in the categories defined by the Theoretical Framework to highlight the best solutions in designing waiting spaces to be applied to the CdC’s context.
2.2.2. Observation Criteria
Aiming at the research objectives, case studies of the first area of investigation were analysed on the basis of five categories (Figure 4):
- Efficacy of layout configuration: solutions to configure welcome and waiting areas to optimise the use and quality of healthcare environments. In this category, the authors evaluated the type of spaces, their position and relation with the healthcare services, their integration and connection with the entrance, the configuration of the distribution areas and public spaces, the clarity and comprehensibility of the routes;
- Environmental Comfort, Control, Familiarity and Affordance: the effective use of colours and materials to promote comfort and a sense of familiarity, recognizability and sense of welcoming. The authors analysed design solutions for light (natural and artificial), ventilation and all the aspects that impact on the environmental well-being; furnishing solutions to promote the sense of welcoming and homing; the ability of control by the patients/caregivers/visitors; the affordance capabilities of the proposed furnishings;
- Restoration, Sensory Stimulation: strategies for support and recovery through art, nature or other regenerative elements; the variety of sensory stimulations and the possible regulation of stimuli;
- Sociality Promotion: promotion of a functional mix and design solutions to foster relationships and a sense of community;
- Active and Healthy Aging: strategies and design solutions to promote active design (e.g., through the use of stairs), healthy food, Healthy Buildings construction, etc.
As regards the Sensory Design area of investigation, the following analysis criteria were followed (Figure 5):
- Space Models: Designing the building according to a multisensory approach; Sensory equipment diffused in public spaces; Sensory atrium or sensory waiting spaces; Snoezelen rooms; Portable sensory equipment;
- Relaxation Strategies: specific elements of the project which represent targeted solutions to reduce stress, promote psychological comfort and support restoration;
- Movement Promotion: solutions to favour the interaction between the person and the space (or the object) and encourage movement and physical activity, according with the idea of active and healthy waiting time;
- Technology Integration: devices and automation technologies which promote the control of space by the person, the regulation of sensory stimuli, and the interaction between the person and the environment. The authors also analysed the integration of these elements into the environment by the architectural project.
2.3. Perceptive Analysis: Co-Design
A semi-structured interview model was submitted to the healthcare professionals (40 persons among doctors, nurses, management and administration) of the relevant healthcare facilities in order to collect data on the use and perception of the waiting spaces. The interviews were submitted in INRCA facilities in Ancona, Casa della Comunità Le Piagge (Florence), Casa della Comunità Morgagni (Florence), Department of Multidimensional Medicine of Florence.
Then, a semi-structured interview model has been submitted to patients (41 persons) and caregivers (26 persons), at the same facilities where the interviews with healthcare professionals were carried out, getting qualitative results to be integrated in the Design Guidelines.
The interviews were posing questions about three main topics: the spatial configuration; the presence of sensory elements that could improve relaxation or mental distraction (e.g., music, projections, coloured lights, etc.) and the health promotion (e.g., having information on health, doing physical activity, etc.).
During the interviews, respondent pictures of different waiting rooms (Table 2) selected in the technical analysis were shown to people to support questions about the space and favour the discussion.
After the interviews, a questionnaire model has also been submitted to patients and caregivers, which will provide more quantitative data on specific questions about the waiting spaces configuration.
Perceptive requirements are the result of the co-design analysis and will be described in another publication, related to this specific topic.
2.4. Mixing Methods
The Theoretical Framework was used to select and analyse case studies. The results of the technical analysis were represented by spatial models and environmental characters identified as invariants in designing waiting rooms and points of innovation to be applied in the primary care context of CdC. These aspects were discussed in the co-design phase, by showing pictures of best practices selected (Table 2) and discussing the results of technical analysis with users. Moreover, both the results of technical and perceptive analysis were summarised by the five categories of the Theoretical Framework, defining spatial requirements for designing health-promotive waiting spaces (Figure 6) and then to develop Design Guidelines.
3. Results and Discussion
According to the aim of this paper, in this section we present the results of the definition of space requirements for active and healthy waiting space.
Space requirements represent the result of both, technical and perceptive analysis, mixing indications derived by the study of best practices and qualitative responses to the interviews, related to the point of view of patients, caregivers and staff regarding waiting spaces’ models of the technical phase.
3.1. Space Requirements
3.1.1. Efficacy of Layout Configuration
According to the different layouts of the healthcare facilities analysed, we identified 8 different models of waiting spaces based on the configuration layouts (Table 3).
Waiting areas can be placed directly in the atrium (M01), articulated by spaces with different seats oriented to favour social relations, but also to guarantee privacy, depending on different needs (referring for example to case studies a12, a13 in Table 1). This area can also be characterized by colours (a12, a16), art or nature, to favour comprehension and recognizability.
Waiting area can be along “the street” (M02), which runs longitudinally through the whole healthcare facility, recreating differentiated waiting corners along the route, like small sitting points. Nature can have an important role in this area, such as creating “green rooms” through flower beds with tall vegetation that divides the spaces (a2), or using flower beds with lower spread plants (a10); as well as art that can be spread along the path, such as artworks, sculptures, lighting systems (a8, a14) or large multi-level walls (a14, a18). Sociality can be supported by furniture, such as seats oriented to look at each other or around a table to encourage relationships; as well as games or art along the route (a10, a14, a17) to share the experience and favour the dialogue. The street can be on a single level, double or triple volume, overlooking the other floors through galleries and raised connections (a8, a17, a18, a20), also creating larger areas of interaction such as a central big square (a18, a20) or smaller ones at the various floors, creating a connection by stairs or slides that lead from one floor to another (a14).
Another recurring typology is represented by waiting spaces built around patios or courtyards (M03), which are suitable to be green (a1, a5, a6, a7, a9, a14, a15), to maintain continuous contact with nature and encourage distraction during the waiting time. Courtyards can be accessible (M04) or not. They can have different shapes and sizes: as an example, long and rectangular spaces allow natural but indirect, non-dazzling light to be given inside, and can provide seats along the openings (a5, a9) in order to maintain a relationship with nature even if not going outside; smaller and more contained spaces, with the same dimensional relationship between waiting and green space, can let the outside in interior spaces and expands the space up (a19), also thanks to big transparent glass openings. When accessible, they can be places to stop and relax on seats in a structured greenery (a7, a14) or in a wild and more natural context (a1, a6); they can have covered spaces to install artworks (a8) or doing different activities, such as yoga, children’s playing, etc. (a15). Green courtyards can represent the core of the structure, also having a function linked to health promotion, physical and mental support activities and sociality (a6, a15).
A different model can be represented by a well-defined waiting space, such as a separate waiting room (M05), independent from the other areas of the healthcare facility, while maintaining visual contact and access control of the relevant healthcare services/spaces. For example, this typology involves the placement of several rooms in different areas of the building, close to the healthcare services/spaces, completely separated and facing outwards to maintain the relationship with the context and the surrounding landscape (a11, a16). These waiting areas can be highlighted by colour to facilitate recognisability, both from inside and outside (a16). They can be closed and contained, to favour privacy and relaxation, supported also by dim light (a11) or other sensory elements. Otherwise, the separation of the space can be less strong, creating a filter (M06), such as glass walls (a13), wooden slats (a13), or a semi-transparent perforated surface (a4), which can let light filter through and maintain the visual relationship with the different areas, also favouring the relationship with other users and the visibility of the entrances to the outpatient area, reducing stress.
The last typology is represented by “the corner” (M07), some waiting points within a larger space, placed along the path or around the courtyards, identified by colour, seating elements (a2, a12, a17) or artworks (a15); as well as niches/pods open in corridors or other public spaces, built into the walls or with an independent structure, identified by colours or materials (a12); as well as furniture to create a point of rest, such as armchairs with higher backrests and sides, placed around the head to promote privacy (a12, a14, a17).
The model M08 is very common in the existing healthcare buildings, but it should be avoided in new designs because of some critical issues such as the lack of privacy, the passage of people, the noise, the lack of space, the difficulty in relating with other people. Anyway, in the Design Guidelines we decided to analyse this model as we are also referring to refurbishment of existing buildings.
The definition of the 8 spatial models (Table 3) was an important result of the technical analysis which represented the basis of discussion in the interviews with the staff, to understand their opinion about the impact of configuration on people’s perception of the waiting experience in the different models. The staff itself expresses the importance of “the organization of spaces to enhance the perceived quality of the facility and consequently of the healthcare service, as well as reducing stress and fostering relationships of patients/caregivers with the staff”. A clear and comprehensible layout is therefore very important in the design.
The most debated point, which determines the different layouts of waiting spaces, concerns the view of the door of the healthcare service from the waiting area: on the one hand, seeing the door allows for monitoring and can therefore reassure the patient, for example, that they won’t miss their turn; on the other hand, it can generate anxiety since they are never able to distract themselves and relax, maintaining a constant state of stress. It is perhaps more important to know you are in the right place (and therefore provide appropriate information, both through spatial layouts and signage), to know that one of the staff will call you, or at least to have access to call systems for the visit/exam. In this sense, the waiting room can also be a completely separate room, which has the advantage of being a private place where patients/caregivers can relax and distract themselves.
It’s highly recommended to have a secluded area away from the main corridors to promote calm and privacy during waiting, while avoiding waiting directly in the corridors, as “it’s a transit point and therefore one can see various health, pathological, and social situations,” which can generate anxiety. This also promotes privacy, not looking at the doors during waiting and ensuring visual and acoustic privacy.
The configuration of waiting spaces should be as varied as possible to meet the different needs of users. For example, some people prefer seclusion (such as a seating area in an alcove), while others prefer a shared space where they can more easily pass the time, talk, and interact with others. The waiting area should foster relationships between patients or caregivers, for example by having a connected coffee or tea area, which promotes greater conviviality. Open large space is also suitable for people with dementia or Parkinson, where they can move freely and in safety. In any case, it is important to be able to find privacy in an open space, to recreate a sort of intimacy between the caregiver and the patient, to have the opportunity to read, for example, and to distract oneself, reducing the feeling of waiting time.
Outdoor waiting is a very interesting model, but it is affected by weather conditions, so at least some coverage is required, and obviously it cannot be the only waiting area. It’s beneficial to have space for walking while waiting, to “promote active aging,” or an area dedicated to “sensory stimulation”. “This could also be a corridor/greenhouse with plants inside”. In any case, it’s important that the green area be adjacent to the waiting room to maintain a connection.
Greenery can also be imagined within waiting areas, to “mentally escape and thus think less about what patients are about to do” and to create “privacy” between seats. However, it’s important to have big windows to allow proper oxygenation, that there be no flowers, which can cause allergies and infections, and that maintenance and cleaning are guaranteed. The sight of greenery already positively influences the waiting experience.
We discussed the same topics with patients and caregivers.
Regarding the layout, we discussed with users first of all the importance of seeing the door. This is a rather controversial topic, with the majority saying they are indifferent or, on the contrary, prefer not to see it, but with a small difference. Caregivers show a similar result, with the majority being indifferent or preferring not to see the door. People who ask to see the door are linked to the anxiety of “not seeing what’s happening,” or “losing their turn,” checking they “didn’t make a mistake,” or “making the visit seem closer”; in general, a sense of control. Many say that if they can’t see the door, a display or call support is necessary. However, the situation is different for caregivers who prefer to maintain eye contact to ensure they can intervene if needed. Those who prefer not to see the door are often linked to a situation of anxiety or distress caused by constantly seeing the door and constantly waiting for the other person to come out before it’s their turn; furthermore, not seeing the door makes it easier to distract oneself in a positive way, for example by “looking at a beautiful view”.
According to this idea, the use of a filter between the waiting area and the outpatient doors seems to be an effective solution. This allows for monitoring, but also ensures a more private waiting experience. On the other hand, the filter used should be pleasant and not too restrictive, like “sticks” or a “barbed wire fence,” which makes the area feel “like a prison”.
Many, however, report the importance of waiting in a large, open space. For this reason, many users dislike a separate waiting room, as it often feels small and cramped. This can be addressed by a large window overlooking the outside, which is always appreciated for its view, natural light, and connection to the outside world. Those who prefer to see the door view will obviously find a separate room unpopular, especially if it’s far from the outpatient area, but this problem can be addressed for many with a display or call system. The problem of small spaces is often associated with the potential for crowding, which is considered very negative. Anyway, there are some who prefer this model because it’s separate, quieter, and more secluded.
The connection with the outdoors, and in particular the view of greenery, is greatly appreciated by virtually all users. In this sense, many of them would gladly wait outside to “get some fresh air,” especially if there are many people and it’s hot, and to pass the time: “It’s more distracting, you can look around,” “you can completely disconnect from the inside.” Here, too, clearly, displays and call devices are necessary. Many prefer a situation where the outdoor space is adjacent to the waiting room, to maintain visual control. Finally, many report the problem of waiting outside in adverse weather conditions, such as rain, cold in winter, or hot in summer. They suggest adding seating, activity equipment, children’s games, fountains, social spaces, or connected services such as a cafeteria outside. The advantages of waiting outside for those with children were also highlighted, as it allows for easier entertainment during the wait.
3.1.2. Environmental Comfort, Control, Familiarity and Affordance
The quality of light (natural and artificial) and ventilation are the basis of the design of a healthcare facility that creates comfort for the patient. Natural ventilation can be favoured by the use of courtyards and patios, but also through openings on the ceiling, for example in pitched roofs (a7). Acoustic is also the basis of the comfort of healthcare buildings. For example, it should be favoured the use of acoustic false ceilings in waiting areas where noises and reverberation can occur (a5, a11).
The design of spaces, openings and facade can be different according to solar orientation to promote comfort and energy saving (a5, a6, a11, a16). The use of large openings or transparent glass surfaces, even on the roof, should be favoured, especially in public areas (a1, a2, a4 , a10, a12, a13, a14, a15, a16, a17) to promote natural light and relation with the landscape. The system of shading for the façade can regulate the amount of incoming light and avoid glare and overheating phenomena (a5). There can also be an internal filter to regulate natural light and allow visibility, favouring comfort and privacy (a4). Moreover, the indirect light entering from internal green courtyards allows light to spread in a more comfortable way (a8, a9, a14).
Artificial lighting also plays an important role in the quality and comfort of the internal spaces of healthcare facilities. Lighting fixtures that are not dazzling and give a warm, welcoming and familiar atmosphere are to be favoured, guaranteeing a bright, comfortable and welcoming environment in any weather condition (a8, a13, a17). They can also be elements that, integrated into the artworks, favour interaction and navigation (a8).
The choice of colours and materials can also help spread light in a warm and welcoming way (a15), such as the use of wood, whereby the light is reflected and acquires a warm tone that offers softer contrasts ( A15). The use of warm and neutral colours should be encouraged (a3, a5, a8, a12, a16), which, together with the use of natural materials, can inspire a sense of familiarity (a8). Colours can liven up the environment and give a bright and positive tone, especially at the entrance and along the paths (a12, a16), promoting the idea of a welcoming and friendly place. For example, the use of yellow can promote a sense of positivity (a12, a16); the use of green and other natural shades can create a warm, bright and welcoming atmosphere (a17); cold colours are more functional for staff spaces, to create a stimulating and attractive work environment (a17). Then, the use of colour can also promote recognisability, comprehension and navigation. The use of wood is suitable (a1, a4, a5, a6, a7, a13, a14) to promote warmth, welcoming, familiarity and the sense of belonging to the territory, favouring the use of local and natural materials (a5, a6, a7). It also reminds of external nature and provides a positive associative effect, evoking positive memories, calm and well-being (a15). Then, it can be used in flooring also to identify waiting areas, to differentiate and highlight them compared to the paths, and to make them more domestic and comfortable (a14). Moreover, it can be used on the facade, reflecting from the outside of the building the desire to provide the city with a healthy and environmentally friendly building (a7) and creating a warm character also on the outside, encouraging people to enter (a15). The use of local materials is also valid for the use of stone and the integration with the surrounding context, therefore favouring identity and recognisability (a11). The same type of integration can also be favoured by the size of the building and its volumes, integrating with the surrounding urban landscape, while making itself recognizable through the use of materials and colours (a18, a19). In fact, the use of different materials on the façade completely changes the appearance from the outside and the relationship between the interior and the surrounding landscape (urban and natural), choosing to differ or to create a dialogue with the context (a19).
The familiarity of spaces, as well as their usability, are also favoured by the furniture. Various waiting possibilities with different types of seating are suitable to favour relations and facilitate control by users, facing outwards to encourage the relationship with nature. Sofas, chairs with tables (low or high), soft seats, armchairs, coloured or wooden chairs, promote familiarity, comfort and privacy (a1, a8, a11, a12, a14, a15, a18, a19, a20). Furniture can also promote identity and attachment with the community, using iconic and local products (a4). The involvement of citizens in the design, as well as for the furniture, can also be encouraged for iconic elements, such as patterns reproduced on the internal and external coverings of the building (a15). Another important role of furniture is to reduce the imbalance that may exist between patient and doctor, for example by the use of curved elements, such as round tables, in which everyone can sit at the same level (a13, a15). Finally, some accessories, such as lockers (a1), can improve user comfort.
According to the staff, brightness in a waiting room positively impacts the waiting experience, especially with regard to mental health. Natural light is preferred where possible, or artificial lighting that is well-diffused and not overwhelming (for example, avoid flickering neon lights). In addition to lighting, openings are very important to ensure natural ventilation, especially when waiting rooms are crowded, and a view of the outside (see next section).
Colours greatly help enliven the environment and make it more aesthetically pleasing. Some colours are ideal for relaxation, such as light blue, while others can create anxiety; in any case, light, not too bright colours, such as red, are preferred. Colours reminiscent of traditional healthcare and institutional environments, such as light green or white, should be avoided. It is suitable to use the same colours for walls and doors.
Materials are very important. For example, wood is a natural, warm, and welcoming material that can be very beneficial in waiting areas. “Curbed lines are also transmitting the same feelings of calm and welcoming”.
These spaces should also convey a sense of cleanliness and order, with linear furnishings. Comfortable sofas or armchairs are preferred for both seating comfort and conviviality. They evoke the idea of a more informal and familiar environment, where, for example, “you could also have a table with magazines to distract yourself while waiting.” The ergonomics of the seats should also be considered to facilitate standing, especially for elderly patients or those with mobility issues. As an example, it is important to have seats with armrests.
However, hygiene, health, and safety standards must always be respected.
According to patients and caregivers, a significant portion of users prefer a familiar environment, through the use of natural materials such as wood and a more homey style of furnishings. Wood, in particular, is appreciated by most people because it “provides warmth,” is “more welcoming, and less cold.” On the other hand, we did not expect a significant percentage (more than half) of people to be so concerned about hygiene and therefore, for this reason, less inclined to use more domestic fabrics or furnishings. They prefer a functional environment, easy to clean, and that “gives a sense of health,” reflecting the function of this space.
Regarding colours, users prefer soft, pastel, bright, and vibrant colours, but not too strong. Almost all users reject white, except for a few who prefer it above all else, as it “gives a sense of cleanliness” and “makes the space seem more open.” In general, blue is highly appreciated because it “relaxes,” “reminds one of the sky,” “of water,” or “of the sea.” Green is also highly appreciated, and some prefer yellow, but only if it’s not too strong, although many say they don’t like it.
Regarding lighting, natural light is preferred by virtually all users, as it “reminds one of being outdoors,” “is more vital and joyful,” and allows one to “maintain a connection with the environment and the passing of time,” except for a few who appreciate the use of coloured lights. As for artificial lighting, soft, not-too-bright, warm, “relaxing” lights are preferred, reproducing outdoor light or modulated at different times of the day.
They don’t like bare spaces, but they also don’t like messy, chaotic spaces that are overcrowded. A modern, linear furnishing style is often appreciated because it’s clean and tidy, but it shouldn’t be too cold. Some prefer single, unpadded chairs, as mentioned, but many instead point to the benefits of using sofas because they’re more comfortable and, above all, more convivial, as they foster social interaction.
3.1.3. Restoration, Sensory Stimulation
Most studies place nature as the major source of restoration, together with art and sensory elements.
The relationship with nature can be promoted in healthcare facilities, both inside and outside. Inside the building, nature can enter the spaces with internal greenery, which makes the space more lively, familiar, healthy and therapeutic (a2, a10), as well as creating a filter through the tallest vegetation, as if they were real “green rooms” (a2). Then, it can be an indirect visual relationship with the surrounding landscape (a1, a6, a11, a14, a15), of green patios and courtyards (a5, a9, a19), or of the sky itself (a19), through glass openings in the waiting and connecting spaces. When it is possible, it is suitable if green courtyards are accessible (a1, a5, a6, a7, a9, a14, a15), allowing a direct relationship with nature, more or less structured, with rest and interaction areas, or spaces equipped for various activities, such as yoga, or children’s playing (a15). This concept can be extended to the entire structure, creating a symbiosis between interior and exterior, in a variety of essences and colours, based on the seasons (a6), through larger and smaller courtyards or green terraces hanging in the volumes (a3, a14, a15, a18), and roof gardens (a6, a18). The design of green courtyards can also be associated with specific functions of the structure (atrium, bar, staff, children, etc.), extending their use outside, and be connected to different sensory stimuli, for example based on the 4 elements earth, air, fire and water (a15). The arrangement of the external greenery is important, both from the point of view of welcoming and involvement of citizens. Greenery at the entrance (a4, a12) or around the building (a17, a20) allows to create both a link and a filter with the urban context, and can be freely used by citizens (a15). It can be equipped with paths and seats (a4), work arts or other elements to encourage interaction and sensory experiences (a12), or connections with other functions such as the café or the waiting area (a18).
On the other hand, nature can also be transmitted through art, recreated in different artworks, colours and materials (a8), in graphics and illustrations (a14) or as a pattern that recurs throughout the building, also creating a link with the territory and promoting a sense of identity and belonging (a15).
The illustrations can become an integral part of the architecture, completely invested by art (a14, a17). Otherwise the colours can liven up the space, make it less institutional, and favour sensory stimulation (a19, a20). Art can be reproduced in artworks, paintings or sculptures, which invite interaction with the space and positive distraction; facilitate navigation, in focal points of the building such as the entrance or reception, in the waiting rooms or in the paths (a8, a10, a12, a15, a17); create a connection with the city (a3), with sculptures (a10) or street art outside. It is favourable to use artworks by local artists (a12), even creating exhibitions that change (a18), and open after closing the healthcare facility to favour visits and knowledge of the structure by new groups of citizens (a15).
Sensory perception can also be encouraged by dim and coloured lighting, and music, for example by placing a piano (a2) or diffusing sounds and music in the public area. Finally intimate spaces, such as sensory rooms, are suitable to favour relaxation, containment, and sensory rebalancing (a11).
According to the staff, it’s important to create a comfortable, welcoming, intimate, and safe waiting area where people can relax, allowing time to pass without worrying about when their turn will come. “If you feel more relaxed, you’re also a little more cooperative, perhaps more willing to talk and able to clarify, for example, symptoms.” It should be a sort of “decompression room.” “A quiet and serene environment, with comfortable seating, paintings or murals on the walls, succulents (which require no maintenance), and soft lighting.” The idea of “being able to involve local young people in creating the mural and have it donated to seniors, to foster the idea of multigenerationalism and the feeling of belonging”, is interesting. Colour, art, and greenery are all good in all their forms. Green elements keep people active and promote mental health. Even the pathways could be imagined as “tree-lined paths, with a view of greenery in the background, which can convey a message of greater tranquillity and health promotion.”
Projections of landscapes and natural scenery, video screens, or touch screens can distract and relax, refocusing attention elsewhere, as can background music. The music should be “low, non-disturbing (for example, loud sounds can create discomfort in people with dementia or make some people nervous), calm, and possibly instrumental, even better if you can choose based on your preferences,” or “sounds of nature, especially water,” “wind, rain, and animals.” Even objects that can be played and interacted with manually, such as a large chess set, are desirable.
In any case, “whether it’s a game, entertainment, music, or a connection... the important thing is not to feel like you’ve wasted the time you spent waiting.”
“A sensory preparation room can be ideal,” “a relaxing, meditative place where you can be alone, even with and for those accompanying you.” “A place where you can stay for an hour and not feel the need to do anything else, a warm, natural, familiar environment, darkened with curtains,” “illuminated by chromotherapy,” with “video projections for distraction,” “comfortable seating, waterfalls and sounds,” with “water, which also provides a sense of coolness.” Such a space “can also improve pain tolerance,” for example, in the case of invasive tests, “can feel better in case of bad news by the doctor”, “in case of fragility” and for “people with cognitive or behavioural diseases”. In general, a dedicated and “possibly isolated” space is preferred, as it is quieter and more intimate, offering greater privacy; however, some prefer the idea of having sensory elements in a larger waiting room, where they can continue to interact with others, or use a sensory alcove overlooking the waiting area, so as to still be able to isolate themselves somewhat.
As for the staff, art is appreciated by almost all patients/caregivers, as it “distracts”—especially if you’re alone—”stimulates curiosity,” “makes you stop and look,” “makes time pass,” “relaxes and calms,” and “provides a sense of beauty.” Only a few say it “isn’t interesting” or “not relevant,” but no one makes negative comments about it or disdains it.
Nature and the view outside are universally appreciated by all users, as it “is relaxing,” “provides calm,” “openness” and a “sense of respite,” conveys “the idea of being outside,” and allows you to “watch time pass.” Some did, however, mention the importance of seeing the outside, but without having a completely transparent glass wall overlooking the waiting area. This is likely also linked to the cultural context, where it is uncommon to have completely open glass facades.
More controversial is the issue of having greenery within the waiting area; the majority of users appreciate it, but some are concerned about the potential for allergies, the presence of insects, and the potential for dirt caused by plants. Above all, they are concerned about the possibility of inadequate maintenance, which could result in the plants becoming damaged or drying out. This can be addressed by choosing plants that are hypoallergenic, highly durable, and require little maintenance, or by using preserved plants.
For the same reason, although most people prefer real natural elements, some prefer the artificial view of nature, such as through screens or video projections, which “allow your imagination to travel.”
This raises the topic of sensory spaces, which are appreciated by almost all patients, and the majority of caregivers, because they “relax,” “calm,” “relieve anxiety,” “help you sleep,” “distract you, and stop you from thinking.” Many have never experienced a sensory space, so the results may be partially affected by a lack of knowledge. Some refer to the use of this space not only during the wait, but also after the appointment, or for activities such as those of psychologists, or for specific pathologies and vulnerable users.
They also question whether they can truly relax in such a context. For this reason, the majority prefer a separate space, since it is isolated and “makes you feel more at peace,” and more than one person can use it at a time. For the same reason, the sensory pod is less appreciated. Some also raise the issue of hygiene, having to use it promiscuously. Those who generally prefer to isolate themselves appreciate it, as they can remain in the waiting room, yet still be isolated and have an individual experience. In this sense, for example, it can be useful for breastfeeding.
Screens and projections that reproduce natural scenarios are appreciated by almost all users, preferably with background music, as it “distracts and takes you away from your thoughts,” or “travel scenarios that let your imagination soar.”
Music is also appreciated by everyone, but it’s important that it be soft and light, just a background. Some people prefer to be able to choose it; otherwise, relaxing music, classical or instrumental, is generally preferred, along with the sounds of nature, especially water, “like a waterfall, ideally real.”
3.1.4. Sociality Promotion
A mix of functions and a connection with the surrounding territorial and social context should be encouraged. For example, placing healthcare facilities in buildings that also have a residential function (a3, a10), or more public functions such as an atelier/carpentry shop (a3), a gallery to exhibit the work of local artists, a space where local groups meet and a base for neighbourhood initiatives (a18), an area for firefighters (a12), a gym, physiotherapy services, a library (a18), spaces for children (a10) or consultants for family (a18), outdoor spaces also used by citizens, green areas (a3, a4, a10, a12) or market areas (a4), or the urban square itself (a4, a13). Otherwise, another strategy is to connect to functions already existing in the area, such as cafes, or sports facilities (a5), a contemporary art museum, or an arena for outdoor events (a9). In this sense also the choice to locate the structure in a central position in the city (a10) or well connected by public transport, for example by placing itself near the train station (a10).
The public atrium, the street and the courtyards are the point of greatest connection, encouraging meeting and exchange between the different users of the facility and creating a real public space that can be considered similar to a street or a town square (a2, a8, a10, a14, a17, a18, a20), also accompanied by public services and functions such as café, hairdresser (a2), etc.
It is important to create permeability between internal spaces and through paths, to guarantee visibility and favour relations. It can be provided by the use of transparent walls (a19); filters created with wooden slats (a11, a13) or grilled surfaces (a4); walkways, balconies and views of the double volume of the street (a2, a10, a11, a14, a17, a18, a20); corners or seats along the route that foster relationships during stops and passages (a12, a15). Even outside, permeable paths that promote circulation in the form of tunnels, elevated roads where residents meet, children play, plants grow, etc. (a3, are favourable for developing sociality. Finally, the relationship between inside and outside can promote permeability, for example by opening and making the central distribution axis transparent, as if it were an urban road (a4).
Likewise, patios and courtyards are a valid strategy not only to maintain the relationship with the greenery, but also to foster relationships between people, both if they are accessible, creating relaxation and leisure spaces where it is easier to meet and relate with other users (a6, a7, a15), and if they are not, placing waiting areas around the open spaces to promote continuous visibility and permeability (a1 , a5, a9, a19). Internal courtyards can also be enriched by artworks to improve distraction and restoration (a8), and encourage socialization (a2), also organising various activities, such as yoga or games for children (a15). This concept can be extended in the common spaces of the hospital organising various information and awareness-raising activities, distracting and regenerative ones, reading, physical activity, or workshops (a6).
Furniture represent another social strategy, through the use of different seating possibilities to favour usability for different types of users, oriented in various directions, with tables or low tables (a1, a2, a4, a6, a11, a12, a14, a17, a18, a20), to freely choose whether to have privacy or relationships with others. Tables, chairs and workstations with electrical sockets or for public use (a6) can also allow working while waiting (a2). Dedicated staff areas also allow to strengthen the relationship between professionals, especially if characterized by furnishings and materials that encourage familiarity and informality (a17, a18, a20).
In general, according to the staff, it’s very positive to have a convivial environment, “a fertile intergenerational space,” “useful for both patients and caregivers,” since “talking with others allows them to share and discuss their problems and find comfort,” “distraction, reduce tension,” and “support, especially if they are without a caregiver.” For example, “it can be helpful to bring together young people with diabetes, with the aim of getting them to know each other and better accept the situation.” Similarly, sharing is very important for pregnant women, as well as for the elderly, who “often suffer from loneliness and need to talk about their illnesses, grandchildren, etc.” However, it’s important that the waiting room isn’t overcrowded and that “one patient’s anxiety can be transmitted to another.” It could be interesting to have a “living room as a waiting space, where people can feel comfortable, looking outside and talking with other people”.
The majority of patients and caregivers say it’s very important to connect with others while waiting, “especially if you’re alone,” because “seeing people reduces anxiety,” “keeping others company,” “allowing you to hear about other experiences,” and “taking your mind off what you have to do.” Open spaces are best suited for this, as they allow you to choose whether or not to engage in this interaction and “not necessarily find yourself face-to-face.” In any case, it’s important to ensure acoustic comfort, reducing the noise from people talking, “which can be very annoying.” It’s also important to provide “a space for privacy,” depending on the moment and the person’s mood. A pod is a “cozy space” where you can “seclude and isolate yourself.” However, it’s appreciated by only a few patients and less than half of caregivers, as it’s considered “too closed off,” making them feel “excluded and isolated.” Some people expressed their willingness to use the pod for breastfeeding.
3.1.5. Active and Healthy Ageing
Health can be promoted by information panels (a15) or screens, as well as by activities, such as courses. The promotion of physical activity is also important, through spaces dedicated to fitness (a6), green courtyards (a6) and active and social spaces in which to encourage movement.
According to the active design approach, stairs should be highlighted, such as by a scenic shape or a central position (a4, a6, a14, a15, a20), or even through the colour (a8), materials (a4, a11) or lights (a4, a8), encouraging their use; connecting elements can also include games such as a slide (a14). On the contrary, elevators can be positioned in a secondary area compared to the centrality of the staircase (a4, a11).
Slow and green mobility should be favoured through the study of viability (a12), the provision of slow traffic areas (a1), bicycle parking near the entrance (a20), guarded and covered (a3), reducing car parking spaces (a3), charging points for electric vehicles and foldable bicycle (a18), access to public transport (a3).
Healthy food and potable free water should be provided. To promote healthy behaviours, spaces dedicated to awareness-raising of healthy eating (a6) can be provided, also through an educational kitchen where families can learn to cook healthy meals (a15), or a city market with local products (a4).
The staff like very much the idea of promoting health during waiting; the main goal should be “improve patient/caregiver’s knowledge about health and make them feel relaxed after waiting”.
All staff expressed interest in the idea of “information points” where patients could “know where to go,” obtain information on the “needs of seniors,” or generally promote healthy lifestyles, in various forms: video seemed the most suitable solution, through a projection, a monitor, or a touchscreen, which could also be interacted with; posters or “something large on the walls”; and pamphlets and brochures, which could also be “picked up and taken home.” Most, however, preferred something shared over individual tablets. Informing could “be useful for distracting, shifting attention, and passing the time.” It is important to provide information “on nutrition, exercise, and social engagement”; on “prevention, such as smoking cessation, or the promotion of specific diets, which, for example, reduce vascular risk, including by providing recipes”; “education for expectant mothers”; “on gender-sensitive medicine for young people, including by organizing peer training or meetings with the public”; on “other patients’ experiences, through video stories, which can provide reassurance, particularly for young diabetics, to facilitate acceptance of the disease”; “on interventions to be performed or on specific pathologies, such as in-depth analysis, again through videos, of anatomy, since many things are often taken for granted when talking to the patient”; “on how to use the devices”; “on local itineraries that can be taken for patients with mobility difficulties to encourage walks, for example in the woods, which reduce behavioural disturbances.” “Having this information in a quiet, peaceful, and intimate setting is certainly more beneficial.” It would also be interesting if “they could watch these videos both before and after healthcare services, even at home, to prepare or, on the contrary, get suggestions for continuing the treatment.” Language should be simple, and explanations should be “with cartoon-like illustrations” or presented “in a fun, entertaining, and interactive way.”
Similarly, interaction and play can engage people and encourage them to exercise. The idea of “going outside and engaging in physical activity” is particularly positive, combining exercise with the opportunity to “see plants and stimulate the senses,” such as “a walk along a tree-lined avenue,” or a “wellness trail,” even with covered areas. This would be ideal, especially for diabetic patients.
We also discussed the opportunity of using passive training equipment, such as seating elements which make people stay in a position in order to activate the muscles and restore their motor function. As an example, we were showing a picture of MyActiveBench by the Italian company (Metalco s.r.l.) [26], a “standing” seat for correct posture and active muscle tone, specifically designed and conceived for “fast recovery” moments. Anyway, passive training equipment has been less successful, as the staff appear concerned about the safety of using the devices independently, imagining elderly patients and/or patients with mobility issues. However, some are very interested in the idea and have proposed using these devices for caregivers, suggesting including an educational message on how to use them. They are considered more suitable for use in a dedicated physical activity area, especially outdoors, in the area adjacent to the waiting room.
The staff was also divided on the idea of self-testing (physical and cognitive): an interactive screen/projection aiming at making people do individual tests such as getting up from a chair, walking, lifting weights, bending and stretching, etc. [26] to understand their healthy and active ageing level and a dedicated cognitive training interface to experiment their neuro skills. The staff think self-testing can be very useful for some patients (e.g., diabetics), on the other hand there is concern about doing the tests independently, due to the patient’s interpretation of the results and the worry and anxiety it may generate. Some of the tests considered useful, especially thinking about healthy and active aging, are represented by “the test of balance, the analysis of movement, the speed of walking, the memory test”.
The majority of patients and caregivers were interested in having access to information about health promotion. They preferred screens/video projections as a means of communication because they were more immediate and engaging, offering brief, “commercial-like” information, since people don’t read, and shared, thus fostering greater relations. They also referred to multiple shared screens, but not individual tablets that would perform the same function as a phone.
Among patients, those who responded that they preferred not to have this information cited concerns and anxiety about the procedure, preferring to distract themselves while waiting and escape from their current state. Some also preferred to receive this information from the doctor, as it was targeted and “safe.”
Those who proposed using paper-based support instead referred to the possibility of taking the information home for further study at a later time.
The majority of patients reported they would not use passive training equipment, while almost the half of caregivers said they would; this result may also be attributed to the age of the interviewees. In general, several patients stated “they want to be comfortable” while waiting and doing physical activity at home or in the gym, or at most outside, even being intimidated by the idea of doing so in front of other people. Some said they “prefer the idea of a walk rather than sitting in a position like this, as they need to release their anxiety.” Many reported that they do not consider these devices suitable for the elderly.
Regarding movement, the majority of patients and caregivers said they would enjoy playing and interacting with various devices “to pass the time.” Some also enjoyed light physical activity. This is certainly considered beneficial for children. Again, reference is made to the embarrassment of doing these activities in front of others, so they would be happy with a dedicated or screened area.
Finally, regarding the idea of being able to perform self-tests (physical and cognitive), more than half of patients and the majority of caregivers are in favour of using these devices. Many are concerned that they are not interpreted by a professional and therefore do not constitute “serious and reliable information,” “based on a doctor’s instructions.”
4. Conclusions
This contribution presents a portion of a three-year research project dealing with waiting spaces to promote good health for all people in the social community.
We were focusing on the background and field research phases, describing how we used these methods to define spatial requirements for active and healthy waiting spaces in Casa della Comunità, a new model of territorial socio-healthcare facility in Italy. Technical and perceptive analysis were mixed to improve results about defining space requirements. The technical analysis was based on the selection and study of international case studies of waiting spaces of primary care facilities and led by the five categories of the Theoretical Framework: i) Efficacy of layout configuration; ii) Environmental Comfort, Control, Familiarity and Affordance; iii) Restoration, Sensory Stimulation; iv) Sociality Promotion; v) Active and Healthy Aging. These categories represent the main principles for active and healthy waiting spaces in a Casa della Comunità. The technical analysis was useful to learn from best practices invariants which can be translated into input for the project according to these categories. As an example, one of the first results of this analysis has been the definition of 8 models of layout for waiting spaces. These layout models and the case studies’ invariants analysed were used as a basis of discussion in the perceptive analysis, leading interviews to the staff, patients and caregivers by iconic pictures to improve the comprehension of their needs during waiting. Mixing methods, it has been possible to clarify people’s preferences about different spatial models, such as waiting in an open space, in a separate room, or directly outside, expressing advantages and disadvantages of each model; characters of the environment to be used as drivers for designing waiting spaces, such as colours, materials, lights, or furniture they prefer; activities people will like to do during waiting time, such as relaxing, chatting, reading, playing, walking around or doing physical activity; interests people have about health and its promotion, such as improving knowledge in this field, testing their physical and mental level of ageing, etc.
As a result of these two phases, spatial requirements have been summarized according to the five categories, defining different spatial models and environmental characters to be developed in the Design Guidelines of health-promotive waiting spaces in Casa della Comunità. Design Guidelines will be an effective tool for professionals in order to design healthy and active environments able to keep all people in good health in a new model of healthcare facility which actually presents no evidence about optimal design. One of the greatest originalities of this contribution is represented by the introduction of the concept of “active waiting time” and “widespread health promotion in waiting spaces” which were appreciated by all users (staff, patients, caregivers) as an opportunity of improving knowledge about health, promoting better lifestyles and increasing social cohesion.
This study highlights how thoughtfully designed waiting spaces in healthcare facilities can actively support well-being and healthy aging. As we move forward, such research will become even more relevant: our environments are not just backgrounds, indeed, they shape experiences, emotions, and health outcomes. Future studies in this field will likely explore new ways to blend technology, nature, and inclusivity, making everyday places healthier and more responsive to people’s needs. The emphasis on inclusivity in healthcare design ensures that all individuals feel included and valued, contributing to the creation of welcoming, empowering, and health-promoting environments for all. The continued development of research on health-promoting built environments is crucial for creating spaces that promote active living, inclusivity, and well-being, thereby directly addressing contemporary health challenges and advancing sustainable healthcare models.
Supplementary Materials
This paper was developed within the project funded by Next Generation EU -“Age-It - Ageing well in an ageing society” project (PE0000015), National Recovery and Resilience Plan (NRRP) - PE8 - Mission 4, C2, Intervention 1.3”. The views and opinions expressed are only those of the authors and do not necessarily reflect those of the European Union or the European Commission. Neither the European Union nor the European Commission can be held responsible for them. This contribution represents one of the results of the research project “Sensory design for spaces in social and health care facilities for healthy and active ageing”, led in Spoke 9 - Advanced Gerontechnologies for active and healthy ageing, Task 1.2 - Design strategies to improve active/healthy ageing in primary healthcare facilities.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, E.B and N.S.; methodology, E.B and N.S.; investigation, E.B. and L.R.; data curation, E.B., V.R. and L.R.; writing—original draft preparation, E.B.; writing—review and editing, E.B and N.S.; visualization, E.B.; supervision, N.S.; funding acquisition, N.S. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
| 1 | Next Generation EU -“Age-It - Ageing well in an ageing society” project (PE0000015), National Recovery and Resilience Plan (NRRP) - PE8 - Mission 4, C2, Intervention 1.3 |
References
- Ministero della Salute. DECRETO 23 maggio 2022, n. 77. Regolamento recante la definizione di modelli e standard per lo sviluppo dell’assistenza territoriale nel Servizio sanitario nazionale, GU Serie Generale n.144 del 22-06-2022.
- Brambilla, M.; Maciocco, G. Dalle Case della Salute alle Case della Comunità. La sfida del PNRR per la sanità territoriale; Carocci editore: Roma, Italy, 2022.
- Jackson, R.J.; Kochtitzky, C. Creating a Healthy Environment: The Impact of the Built Environment on Public Health. Monograph Series; Sprawl Watch Clearinghouse: Washington DC, US 2001; pp. 1–19.
- Rao, M.; Prasad, S.; Tissera, H.; Adshead, F. The built environment and health. The Lancet 2007, vol. 370, n. 9593, pp. 1111-1113.
- Bellini, E.; Setola, N. Active and healthy Case della Comunità: Design Guidelines as a tool to design waiting spaces, Sustainability 2025, 17, (under review).
- Del Nord, R. Lo Stress ambientale nel progetto dell’ospedale pediatrico. Indirizzi tecnici e suggestioni architettoniche; Motta Architettura: Milano, Italy, 2006.
- Del Nord, R. Lo stress e gli stressori in ospedale. In Lo Stress ambientale nel progetto dell’ospedale pediatrico. Indirizzi tecnici e suggestioni architettoniche; Del Nord, R., Eds.; Motta Architettura: Milano, Italy, 2006; pp. 60-79.
- Del Nord, R. L’ambiente e i fattori percettivo-sensoriali. in Lo Stress ambientale nel progetto dell’ospedale pediatrico. Indirizzi tecnici e suggestioni architettoniche; Del Nord, R., Eds.; Motta Architettura: Milano, Italy, 2006; pp.102-149.
- Von den Bosch, M. Oxford Textbook of Nature and Public Health: The role of nature in improving the health of a population; Oxford University Press: Oxford, UK, 2018.
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, US, 1989.
- Ulrich, R. View through a Window May Influence Recovery from Surgery. Science 1984, 224(4647), pp. 420-421. [CrossRef]
- Ulrich, R.; Simons, R.; Losito, B.; Fiorito, E.; Miles, M.; Zelson, M. Stress recovery during exposure to natural and urban environments. Journal of Environmental Psychology 1991, 11 (3), pp. 201-230. [CrossRef]
- Evans, G.W.; McCoy, J.M. When buildings don’t work: The role of architecture in human health. Journal of Environmental Psychology 1998, 18(1), 85–94. [CrossRef]
- Setola, N.; Bellini, E.; Marcheschi, E. Santa Maria Nuova come studio di caso in una ricerca evidence-based. in AI-Care. Arte, Identità e Cura. Gli spazi pubblici dell’ospedale di Santa Maria Nuova; Diana, E., Geddes, M., Setola, N., Eds.; Edizioni Polistampa: Firenze; Biblioteca di Storia e Medicina, Quaderni/7, 2019; pp. 67-100.
- Verderber, S. Innovations in Hospital Architecture; Routledge: New York, 2010.
- HPH. Global HPH Strategy 2021-2025, Hamburg, 2020.
- Golembiewski, R.T. Salutogenic architecture in healthcare settings. In The Handbook of Salutogenesis; Mittelmark, M., Eds.; Springer International Publishing: Cham, 2017; pp. 267-276.
- SSport England. Active Design: Planning for health and wellbeing through sport and physical activity, 2015. Available online: https://www.sportengland.org/guidance-and-support/facilities-and-planning/design-and-cost-guidance/active-design (accessed on 24th July 2025).
- Allen, J.; Bernstein, A.; Cao, X.; Eitland, E.S.; Flanigan, S.; Gokhale, M.; Goodman, J.M.; Klager, S.; Klingensmith, L.; Laurent, J.G.C.; et al. Building Evidence for Health. The 9 Foundations of a Healthy Building; Harvard T.H. Chan School of Public Health: Boston, MA, USA, 2017, pp. 1-36.
- Del Nord, R. Peretti, G. L’umanizzazione degli spazi di cura. Linee guida; Ministero della Salute, Tesis: Firenze, Italy, 2012.
- World Health Organization. National programmes for age-friendly cities and communities: a guide; World Health Organization: Geneva, 2023.
- NHS, England. Technical standards and guidance (health building notes/health technical memoranda documents) (HBN 00-01, 00-04, 08-02, 10-02, 11-01, 12). Available online: https://www.england.nhs.uk/estates/health-building-notes/ (accessed on 24th July 2025).
- Zambelli M. La conoscenza per il progetto. Il case-based reasoning nell’architettura e nel design; Firenze University Press, Firenze, 2022.
- Bellini, E.; Setola, N. Sensory Design in healthcare welcome spaces for active and healthy aging. In Effects of Design on Health and Wellbeing; Verma, I.; Arpiainen, L., Eds.; IOS Press: Amsterdam; Studies in Health and Information Technology book (HTI) series, 2024; pp. 165-182.
- Bertiato, F.; Bellini, E.; Setola, N.; KALI project: a new concept for health promotion within waiting rooms. In Ambient Assisted Living. ForItAAL 2024. Lecture Notes in Bioengineering; Fiorini, L., Sorrentino, A., Siciliano, P., Cavallo, F., Eds.; Springer: Cham, 2024, pp. 30-50.
Figure 1.
Diagram of the three-year research process. In red the section described in this paper.
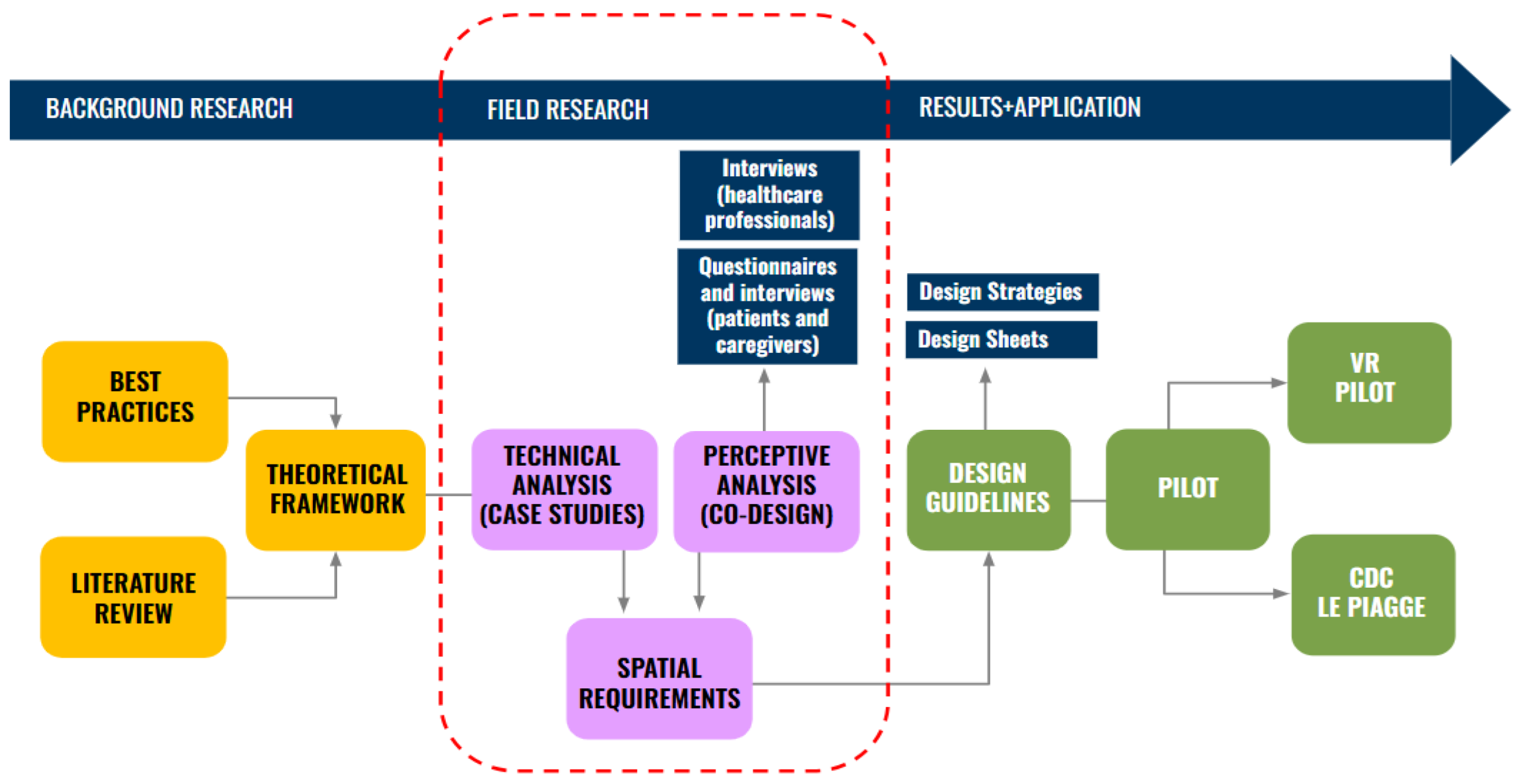
Figure 2.
Diagram of the fundamentals of the research.
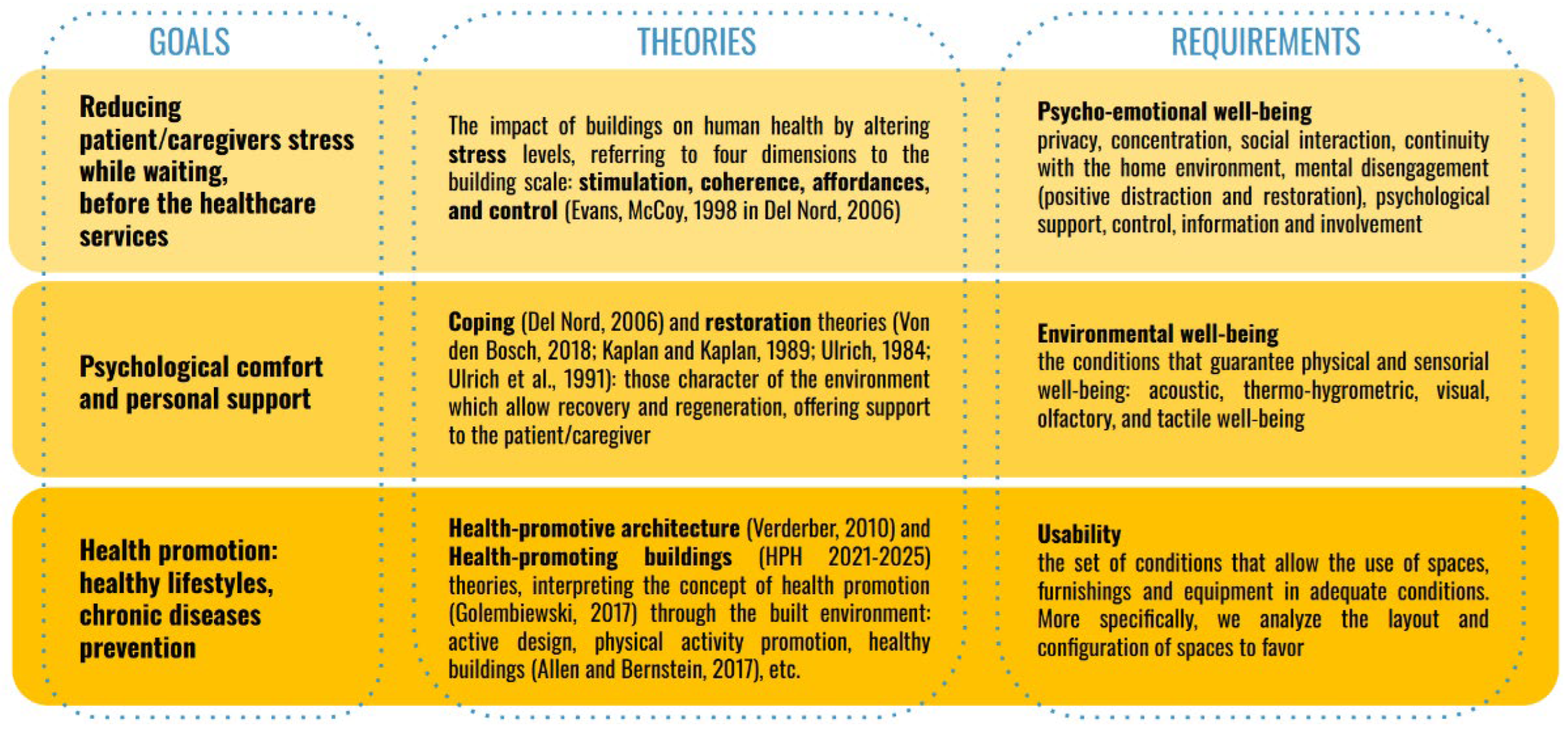
Figure 3.
Diagram of the Theoretical Framework.
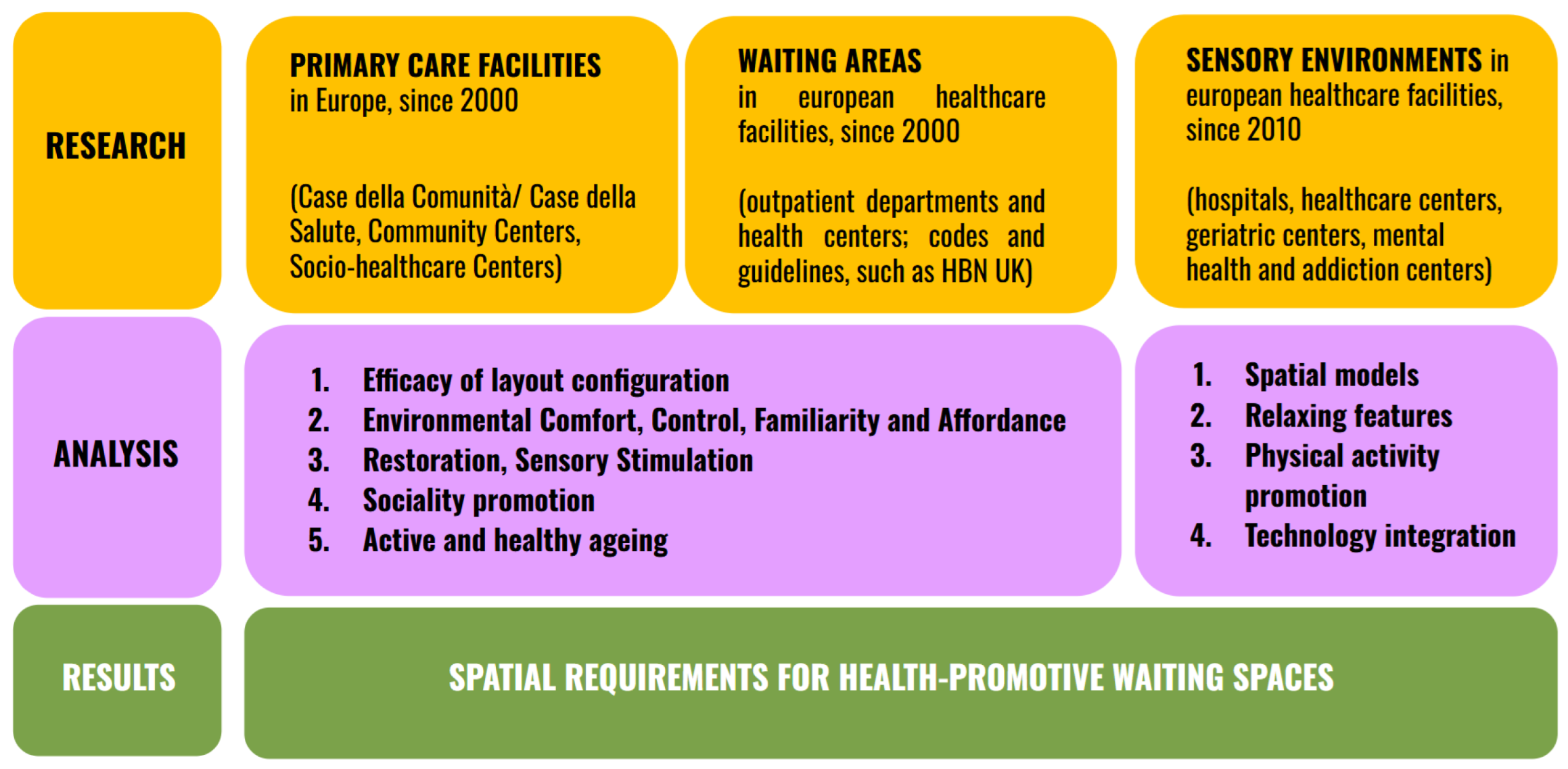
Figure 4.
Case Study Sheet a06.

Figure 5.
Case Study Sheet b07.
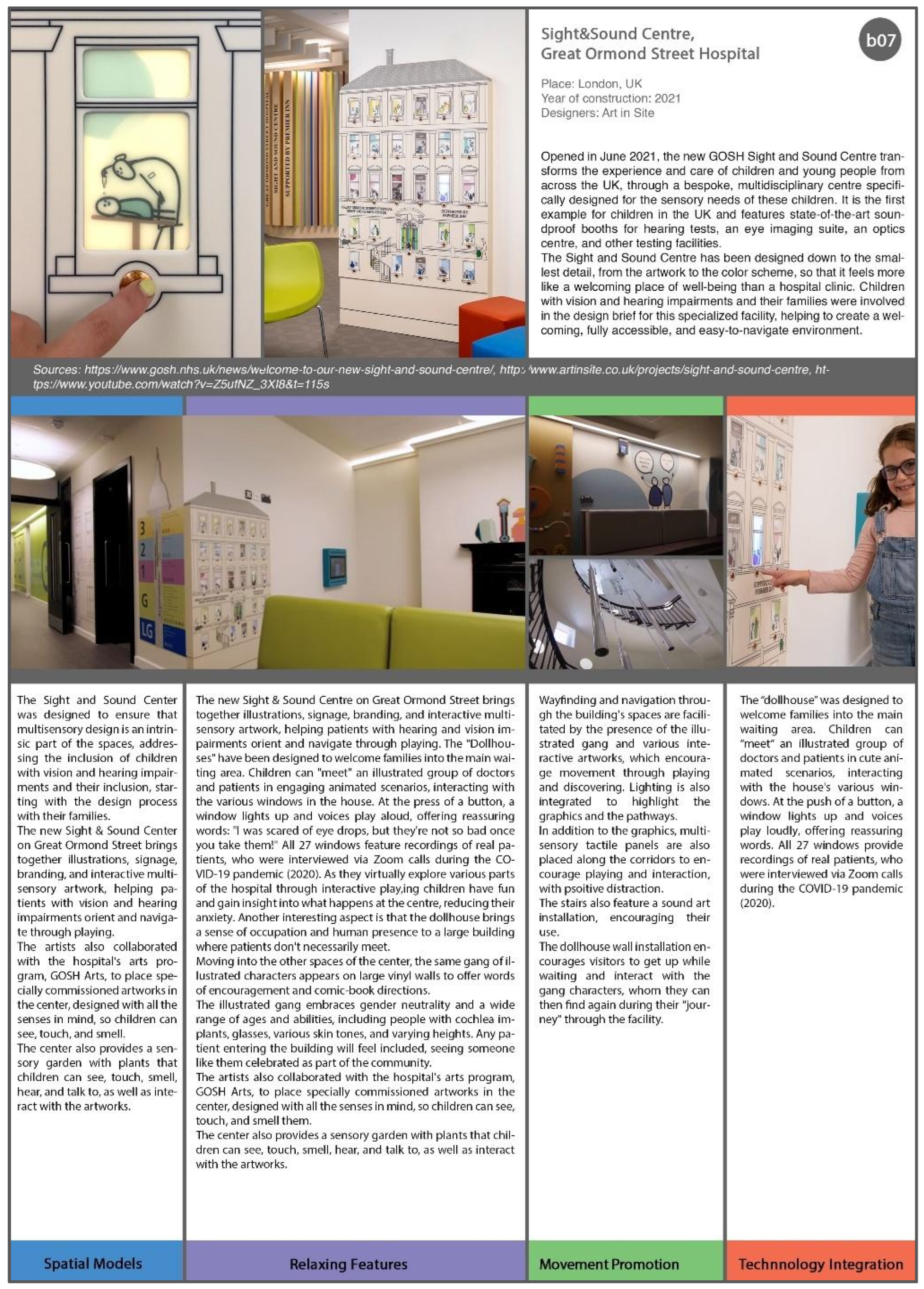
Figure 6.
Diagram about the process of mixing research methods.
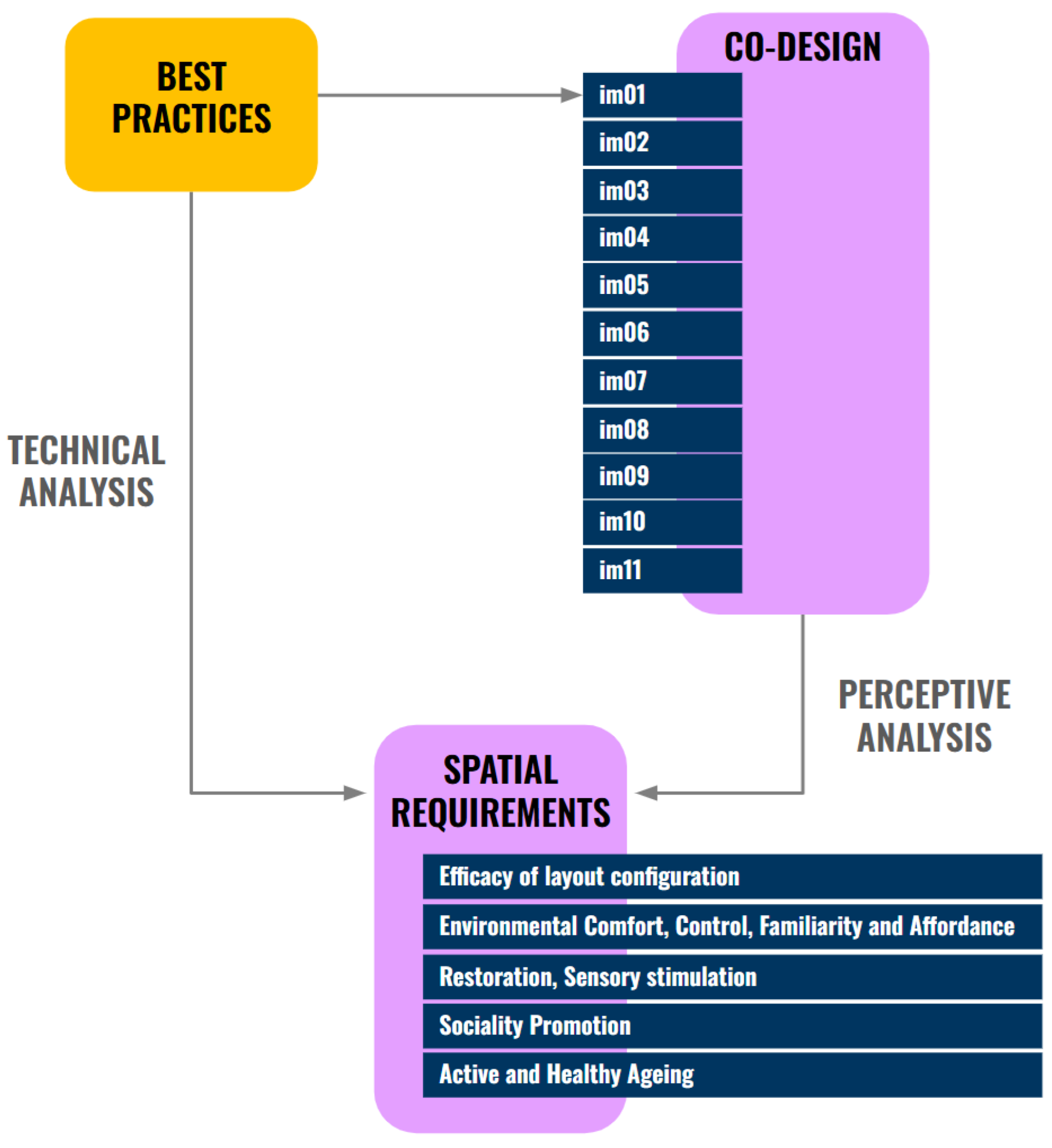

Table 1.
Case studies analysed in the technical analysis phase: waiting spaces of European healthcare facilities, built since the 2000s.
Table 1.
Case studies analysed in the technical analysis phase: waiting spaces of European healthcare facilities, built since the 2000s.
| Case study | Place | Year | Designer | Area (mq) | |
|---|---|---|---|---|---|
| a1 |
Tergooi Medical Centre https://www.archdaily.com/1001687/tergooi-medical-center-wiegerinck |
Hilversum, The Netherlands | 2023 | Wiegerinck | 55.000 |
| a2 | Dijklander Hospital https://www.archdaily.com/995948/dijlander-hospital-revitalization-bureau-ira-koers-and-plus-studio-roelof-mulder?ad_medium=gallery |
Purmerend, The Netherlands | 2022 | Studio Roelof Mulder, Ira Koers | 1.780 |
| a3 |
Bijgaardehof Co-Housing and Healthcare Centre https://www.archdaily.com/988277/bijgaardehof-co-housing-and-healthcare-center-bogdan-and-van-broeck |
Ghent, Belgium | 2022 | Bogdan & Van Broeck | 9.375 |
| a4 | Health Municipal Clinic in Liffol-Le-Grand https://www.archdaily.com/1006257/health-municipal-clinic-in-liffol-le-grand-studiolada |
Liffol-Le-Grand, France | 2021 | Studiolada | 615 |
| a5 | CAP Riells i Viabrea https://archello.com/project/cap-riells-i-viabrea |
Riells i Viabrea, Spain | 2021 | Comas-pont Arquitectes | 566 |
| a6 | Steno Diabetes Center Copenhagen https://www.archdaily.com/1006085/steno-diabetes-center-copenhagen-vilhelm-lauritzen-architects-plus-mikkelsen-architects-plus-sted |
Copenhagen, Denmark | 2021 | Vilhelm Lauritzen Arch. + Mikkelsen Arch. + STED | 18.200 |
| a7 |
Taverny Medical Centre https://www.archdaily.com/932080/taverny-medical-center-maaj-architectes |
Taverny, France | 2020 | Maaj Architectes | 1.095 |
| a8 | Hospital Nova https://www.theplan.it/architettura/hospital-nova-l-ospedale-del-futuro-che-pensa-fuori-dagli-schemi |
Jyvaskyla, Finland | 2020 | JKMM Architects | 116.000 |
| a9 | Health Centre at Gibraleón https://www.archdaily.com/956493/health-center-at-gibraleon-javier-terrados-estudio-de-arquitectura |
Gibraleon, Spain | 2020 | Javier Terrados Estudio de Arquitectura | |
| a10 | Lindesberg health centre https://whitearkitekter.com/project/lindesberg-health-centre/ |
Lindesberg, Sweden | 2020 | White Architects | |
| a11 | Health Municipal Clinic In Audun-Le-Roman https://www.archdaily.com/1000868/health-municipal-clinic-in-audun-le-roman-studiolada |
Audun-Le-Roman, France | 2019 | Studiolada | |
| a12 | The Jean Bishop Care Centre https://www.archdaily.com/909641/the-jean-bishop-integrated-care-centre-medical-architecture |
Kingston upon Hull, UK | 2018 | Medical Architecture | 2.761 |
| a13 | Luz Saúde Vila Real Hospital https://www.archdaily.com.br/br/945349/hospital-luz-saude-vila-real-openbook-architecture?ad_medium=gallery |
Villa Real, Portugal | 2018 | OPENBOOK Architecture | 6.800 |
| a14 | Zaans Medical Centre https://www.archdaily.com/874330/zaans-medical-centre-mecanoo |
Zaandam, The Netherlands | 2016 | Mecanoo | 38.500 |
| a15 | Närsjukhus in Angered https://www.sweco.se/projekt/angereds-narsjukhus/ |
Gothenburg, Sweden | 2015 | ||
| a16 | Porreres Medical Centre https://www.archdaily.com/189622/porreres-medical-center-maca-estudio |
Porreres, Majorca, Spain | 2011 | MACA Estudio | 900 |
| a17 | Orbis (now Zuyderland) Medical Centre https://dezwartehond.nl/en/projecten/orbis-zuyderland-medisch-centrum/ |
Sittard-Gele, The Netherlands | 2010 | De Zwarte Hond | 73.850 |
| a18 | Kentish Town Health Centre https://modulo.net/it/realizzazioni/kentish-town-health-centre |
London, UK |
2009 | Allford Hall Monaghan Morris | |
| a19 | Centros Municipales de Salud https://www.archdaily.cl/cl/02-208005/3-centros-municipales-de-salud-en-madrid-san-blas-usera-villaverde-estudio-entresitio |
Madrid, Spain | 2008-10 | Estudio Entresitio | 5.430 |
| a20 | Heart of Hounslow Polyclinic https://commercialpropertyphotography.com/health-care/heart-of-hounslow-medical-practice/ |
London, UK |
2007 | Penoyre & Prasad (now Perkins&Will) | 8.800 |
Table 2.
List of images used to discuss with patients and caregivers during the interviews.
| Case study | Typology of space | Web Sources | |
|---|---|---|---|
| im01 | Zaans Medical Centre |
Waiting area near the medical rooms. This is an example of a waiting space where people can see the doors of the medical room during waiting time. Colours are vivid, artworks are present on the walls and the furniture is coloured, modern and homey. |
https://www.archdaily.com/874330/zaans-medical-centre-mecanoo/594ce485b22e38e9290004a9-zaans-medical-centre-mecanoo-photo?next_project=no |
| im02 | Luz Saúde Vila Real Hospital | Waiting room filtered by a timber frame screen. The colours of the room are warm and the lights are soft. | https://www.inap2.com/kr-sq/gallery/gallery_e951861bd33b87c365b190e678d03048/ |
| im03 | Porreres Medical Centre | Waiting room on the first floor. It is an example of the model “waiting in a separate room”. All the walls of the room are yellow, the seats are simple and at the end of the room there is a big window looking outside in an urban context. | https://www.archdaily.com/189622/porreres-medical-center-maca-estudio/5016efad28ba0d235b00053b-porreres-medical-center-maca-estudio-photo |
| im04 | Tergooi Medical Centre | Waiting room next to a green courtyard. It is a good example of favouring relations by comfortable and homey furniture. Sofas are oriented in different directions to let people look at each other or outside at nature. The walls are white and clean. | https://www.archdaily.com/1001687/tergooi-medical-center-wiegerinck/6475318820e8d30376dd6c9e-tergooi-medical-center-wiegerinck-photo |
| im05 | Tergooi Medical Centre | Waiting pod integrated in a wall of a corridor. Walls are white and the pod is highlighted by the orange colour. While sitting it is possible to look outside by the windows on the opposite wall. |
https://www.archdaily.com/1001687/tergooi-medical-center-wiegerinck/647531883d39be5bd4fa41e0-tergooi-medical-center-wiegerinck-photo |
| im06 | Health Municipal Clinic in Liffol-Le-Grand | Waiting room on the second floor. The walls are white and the room is filtered by a timber screen which filters the big amount of natural light. As seats, the typical “Liffol chairs” are used, which are a symbol for the local culture. | https://www.archdaily.com/1006257/health-municipal-clinic-in-liffol-le-grand-studiolada/64f0b142bbf563583c72ac19-health-municipal-clinic-in-liffol-le-grand-studiolada-photo |
| im07 | Zaans Medical Centre | Waiting area on the first floor. It is an open space, connected with openings to different floors. All the walls are characterized by big art illustrations. Furniture is homey, coloured and oriented to make people interact. | https://www.oneclub.org/awards/adcawards/-award/27298/zaans-medical-centre-healing-environment/ |
| im08 | Steno Diabetes Centre Copenhagen | Waiting area along the glazing wall, looking at the green courtyard. | https://www.archdaily.com/1006085/steno-diabetes-center-copenhagen-vilhelm-lauritzen-architects-plus-mikkelsen-architects-plus-sted/64ed052452867b5c9aedc962-steno-diabetes-center-copenhagen-vilhelm-lauritzen-architects-plus-mikkelsen-architects-plus-sted-photo |
| im09 | Dijklander Hospital | Waiting area in the street of the hospital. Plants and greenery are growing around the seats, creating some green rooms where people can wait. | https://www.archdaily.com/995948/dijlander-hospital-revitalization-bureau-ira-koers-and-plus-studio-roelof-mulder/63dd1e07e8dab046150a93c5-dijlander-hospital-revitalization-bureau-ira-koers-and-plus-studio-roelof-mulder-photo |
| im10 | Zaans Medical Centre | Waiting area around the green courtyard. The big glazing wall creates a direct connection between the interior and the exterior. | https://www.archdaily.com/874330/zaans-medical-centre-mecanoo/594ce8a8b22e3898a7000814-zaans-medical-centre-mecanoo-image?next_project=no |
| im11 | Taverny Medical Centre | Waiting area in the green courtyard. It explores the idea of waiting outside. | https://www.archdaily.com/932080/taverny-medical-center-maaj-architectes/5e211fc03312fd970e0003cf-taverny-medical-center-maaj-architectes-photo |
Table 3.
Models of waiting spaces layouts derived from the analysis of case studies. The red represents the waiting spaces, the yellow the corridors/connections, the blue the outpatient area.
Table 3.
Models of waiting spaces layouts derived from the analysis of case studies. The red represents the waiting spaces, the yellow the corridors/connections, the blue the outpatient area.
| Model | Diagram of the spatial model | |
|---|---|---|
| M01 | waiting in the main hall |  |
| M02 | waiting in the main street |  |
| M03 | waiting around the courtyards |  |
| M04 | waiting in the courtyards |  |
| M05 | waiting in a separate room |  |
| M06 | waiting room in front of the outpatient area |  |
| M07 | waiting corners |  |
| M08 | waiting in the corridor |  |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



