
Submitted:
30 July 2025
Posted:
31 July 2025
You are already at the latest version
Abstract
Vocal production requires coordinated control of respiratory, laryngeal, and autonomic sys-tems. In individuals with high vocal demand, this physiological load may influence autonomic regulation, even without voice disorders. This scoping review mapped current evidence on the relationship between voice production and autonomic nervous system (ANS) activity in adults, focusing on studies assessing concurrently both systems. A systematic search was conducted in PubMed, Scopus, Web of Science, Embase, and CINAHL (2010–2025) following PRISMA-ScR guidelines. Eligible studies included adults performing structured vocal tasks with concurrent autonomic measurements. Data were extracted and synthesized descriptively. Fif-teen studies met inclusion criteria. Most involved healthy adults with high vocal demand; some included participants with subclinical or functional voice traits. Vocal tasks ranged from singing and sustained phonation to speech under cognitive or emotional load. Autonomic measures included heart rate (HR), heart rate variability (HRV), electrodermal activity (EDA), blood pressure (BP), among others. Four thematic trends emerged: autonomic synchroniza-tion during group vocalization; modulation of autonomic tone by vocal rhythm and structure; voice–ANS interplay under stress; and physiological coupling in hyperfunctional vocal behav-iours. Review findings confirm that vocal activity can shape autonomic function, supporting integration of autonomic markers into experimental and clinical voice research.
Keywords:
Voice production
; Voice use
; Vocal tasks
; Singing
; Vocal load
; Functional voice disorders
; Autonomic nervous system
; Heart rate variability
; Electrodermal activity
; Stress response
1. Introduction
Vocal production requires precise coordination among the respiratory, laryngeal, and supralaryngeal systems, regulated by somatic and vegetative mechanisms. This function, essential for both spoken and sung communication, involves fine motor control, aerodynamic stability, and continuous biomechanical adjustments to sustain efficient phonation [1,2].
These physiological demands increase substantially in individuals who use their voice intensively or professionally. In such high vocal load contexts; including singers, teachers, actors, and wind instrument players; functional overload may occur even in the absence of structural pathology, potentially leading to reduced vocal endurance, instability, or changes in voice quality. Several studies have documented this phenomenon across different populations. Among singing students, there is a high prevalence of laryngeal discomfort and potentially harmful vocal behaviours [3]. In teachers, functional vocal complaints have been associated with reduced heart rate variability [4]. Endoscopic assessments in professional singers without self-reported symptoms have revealed unexpectedly high rates of laryngeal abnormalities, while similar findings have been reported in pre-professional musical theater students and wind instrument players suggesting subclinical vocal strain or chronic biomechanical stress [5,6,7].
The physiological strain experienced by individuals with high vocal demands raises critical questions about the role of involuntary regulatory systems in sustaining vocal function. While phonation is driven by voluntary neuromuscular control, its efficiency depends on a range of automatic physiological processes governed by the autonomic nervous system (ANS). This system continuously modulates key parameters—including heart rate (HR), blood pressure (BP), pulmonary ventilation, and subglottal pressure—that collectively support the biomechanical foundations of voice production [8,9]. Through the dynamic interplay of its sympathetic and parasympathetic branches, the ANS enables rapid physiological adjustments that maintain internal stability under varying behavioural demands [10].
In this context, the analysis of vagal and sympathetic control through indicators such as respiratory sinus arrhythmia (RSA), heart rate variability (HRV), electrodermal activity (EDA), or blood pressure variability (BPV) has increasingly been used to explore autonomic involvement during vocal tasks with varying cognitive, emotional, or communicative demands [11,12]. These physiological adjustments are thought to reflect the functional integration of central autonomic networks during activities that require sustained motor coordination, such as prolonged vocal production. Along these lines, sympathetic activation could induce changes in intrinsic laryngeal muscle activity during a silent speech-preparation task, without active phonation or functional voice assessment [13]. Similarly, different autonomic responses in singing students during live performances were reported, based on cognitive performance levels [14].
Moreover, many studies assessing acoustic or autonomic parameters do so independently, without simultaneous vocal monitoring or correlation between variables [4,14]. Even in recent investigations involving detailed vocal analysis under stress conditions, autonomic engagement is inferred from the vocal task design, but not directly measured, limiting the ability to capture the physiological interplay between vocalization and autonomic regulation [15]. There is still no clear consensus on how the ANS influences vocal production or how to assess its involvement effectively. This conceptual and methodological fragmentation has hindered the development of robust explanatory models that frame voice as a complex motor behaviour modulated by the ANS.
To address this gap, the present scoping review aims to map the current scientific evidence on the interplay between vocal production and ANS modulation in adults, focusing exclusively on studies that assess both systems simultaneously and in a correlated manner. By describing the populations studied, the vocal and autonomic parameters measured, and the experimental designs employed, this review seeks to contribute to a more integrated understanding of the phenomenon. It also provides a foundation for future research on voice and ANS and for the development of evidence-informed voice-related clinical applications.
2. Materials and Methods
2.1. Methodological Framework and Objectives
This scoping review was conducted in accordance with the PRISMA Extension for Scoping Reviews (PRISMA-ScR) guidelines and following the methodological recommendations of the Joanna Briggs Institute (JBI), which provide a standardized framework for mapping the breadth and nature of evidence across a defined field of study. The review protocol was prospectively registered on the Open Science Framework (OSF) and is publicly available at https://doi.org/10.17605/OSF.IO/AXS8F.
The review systematically mapped the scientific literature on the modulation of the ANS during spoken and sung voice production in adult populations. Emphasis was placed on adult populations engaged in structured vocal activity - primarily healthy individuals with high vocal demands, such as opera singers, amateur and professional choristers, music students, and performing artists. While some studies included individuals with subclinical or self-reported voice difficulties, the majority focused on non-pathological voice users, enabling the exploration of autonomic modulation under various vocal demands and ecological or experimental conditions.
Specifically, the review aimed to: 1) identify the autonomic and cardiovascular parameters most frequently assessed during voice-related tasks (e.g., HRV, EDA, blood pressure), 2) examine the methodological approaches used to investigate voice–ANS interactions in both clinical and experimental settings 3) highlight key knowledge gaps and propose future directions for research at the intersection of voice science, physiology, and autonomic regulation.
2.2. Inclusion Criteria and Conceptual Scope
Eligibility criteria were defined using the Population–Concept–Context (PCC) framework and were further refined during full-text screening based on specific methodological thresholds.
Population (P)
Studies were eligible if they included adults (≥18 years) who met at least one of the following criteria:
- Demonstrated high vocal demand, such as singers, actors, choir members, teachers, or performing arts students, provided they actively engaged in structured vocal tasks within experimental or ecological settings.
- Presented with functional dysphonia (either clinically diagnosed or subclinical), when accompanied by monitored vocal activity and relevant physiological measurements.
Excluded groups comprised:
- Individuals with chronic cardiovascular conditions (e.g., heart failure), due to the risk of confounding autonomic responses unrelated to vocal activity.
- Studies in which participants did not perform vocalizations, or where voice was used solely as a stimulus (e.g., to elicit stress) without acoustic or physiological analysis.
Concept (C)
Eligible studies assessed autonomic or cardiovascular responses during voice production. Accepted measures included:
- Direct autonomic indices: such as HR, HRV, RSA, EDA, BPV, baroreflex sensitivity.
- Indirect markers: such as salivary cortisol, when clearly associated with autonomic regulation and when voice production was a central element of the protocol.
- Excluded studies that reported only general physiological data alone (e.g., HR, respiratory rate) without autonomic interpretation or without a functional analysis of vocal performance.
Context (C)
Eligible contexts included:
- Ecological settings such as live performances, oral examinations, or rehearsals.
- Controlled experimental protocols involving structured vocal tasks, provided that both vocal behaviour and autonomic activity were objectively measured and jointly interpreted.
Studies were excluded if vocalization was unmonitored or used merely as a generic physical task, without any direct interpretation of voice–ANS interaction.
Only peer-reviewed journal articles published between January 2010 and April 2025 were considered, as the consistent use of objective autonomic measures in voice research (e.g., HRV, EDA, subglottic pressure) became more widespread and methodologically standardized during the past decade. Eligible studies had to be written in English. These limits were established to ensure methodological quality, accessibility of content, and relevance to current scientific standards in voice research and autonomic physiology.
In all cases, studies were required to report objective physiological recordings. In studies assessing multiple outcomes, only those explicitly linking vocal activity with autonomic nervous system responses were extracted and analysed. Vocal tasks embedded within broader experimental paradigms—such as those involving cognitive load, emotional processing, or stress—were included only when the voice–ANS relationship was clearly integrated into the study’s analytical framework.
2.3. Search Strategy and Study Selection Process
The literature search was conducted across five major biomedical databases: PubMed, Scopus, Web of Science, Embase, and CINAHL. The search strategy was developed in alignment with the predefined inclusion criteria and conceptually structured around the PCC model. Key terms were derived from each component and combined using Boolean operators, then adapted to the syntax and filtering options specific to each database. A list of representative keywords organized according to the PCC framework is provided in Table 1.
Initial screening of titles and abstracts was carried out directly within the database interfaces. Records deemed potentially relevant were exported to Mendeley Reference Manager, where duplicates were identified and removed. The remaining unique records were organized in Excel spreadsheets for full-text eligibility assessment. The search process was conducted between March and May 2025. As a quality control measure, reference lists of included studies were manually reviewed to verify completeness, although no additional eligible articles were retrieved through this process.
Study selection was performed independently by two reviewers following a structured two-phase process: (1) screening of titles and abstracts and (2) full-text review based on predefined eligibility criteria. Discrepancies were resolved through discussion, and a third reviewer was consulted when necessary.
2.4. Data Extraction and Variables Collected
Once the final set of studies was confirmed, relevant data were extracted by one reviewer using a predefined format tailored to the aims of this review. The structure and categories of this charting tool were agreed upon by the research team. The extracted information was subsequently cross-checked by a second reviewer to ensure accuracy and consistency. No automated extraction tools were used, and no contact with original authors was required. The following variables were collected from each included study:
- Bibliographic information: authors and year of publication.
- Study design: methodological classification (e.g., experimental, cross-sectional, observational, longitudinal).
- Study population: number of participants, demographic characteristics (e.g., age, sex), and vocal profile (e.g., singers, teachers, individuals with functional voice disorders).
- Study objective: main aim or hypothesis related to the relationship between vocal production and autonomic regulation.
- Autonomic and physiological variables: HR, HRV [root mean square of successive differences (RMSSD), standard deviation of normal-to-normal intervals (SDNN), low-frequency power (LF), high-frequency power (HF), percentage of successive R–R intervals between normal heartbeats (NN intervals) that differ by more than 50 ms (pNN50), and standard deviation of successive differences (SDSD)]; BPV; pulse pressure (PP); blood pressure (BP); pulse volume amplitude (PVA); systolic blood pressure (SBP); diastolic blood pressure (DBP); mean pressure (MP); RSA; skin conductance response (SCR) or EDA; salivary cortisol; respiration rate.
A subset of studies also reported additional derived indices from physiological signals, including measures of physiological coupling and synchrony, such as time–frequency coherence (TFC), cross-frequency coupling (CFC), partial time–frequency coherence (pTFC), absolute coupling index (ACI), phase synchronization index (PSI), Integrative Coupling Index (ICI), or Granger Causality (GC); as well as geometric measures of HRV, including triangular index (TRI) and triangular interpolation of NN interval histogram (TINN).
- Vocal task and context: type of vocalization (e.g., sustained phonation, singing, reading aloud, polyphonic ensemble singing, speech under cognitive load), and whether the task was performed in an ecological or experimental setting.
- Main findings: outcomes related to changes in autonomic markers, voice parameters, or significant correlations reported by the original authors.
- Voice–ANS interplay: how each study described or interpreted the interaction between vocal behaviour and autonomic modulation, whether correlative, functional, or physiological.
All information was extracted directly from the primary sources. Only objective data explicitly reported in the original studies were included, and the charted content was limited to descriptive elements such as population characteristics, vocal tasks, physiological variables, and reported outcomes relevant to the voice–ANS interaction. No critical appraisal of the included studies was conducted.
The extracted data were summarized using a structured descriptive approach. Each study was handled individually and reported in a uniform narrative format based on the predefined variables. This process facilitated the identification of recurring patterns through a descriptive synthesis, without quantitative comparison across studies.
3. Results
3.1. Identification and Selection of Studies
A total of 6097 records were identified through searches in five electronic databases: PubMed (n = 1953), Scopus (n = 2678), Web of Science (n = 1441), Embase (n = 22), and CINAHL (n = 3). After applying automatic filters for publication year, language, and population within each platform, 5703 records were excluded. The remaining 394 citations were screened by title and abstract, leading to the exclusion of 338 records that did not meet the eligibility criteria.
The remaining 56 citations were exported to Mendeley Reference Manager, where 23 duplicates were identified and removed. A total of 33 full-text articles were assessed for eligibility. Eighteen studies were excluded for the following reasons: no voice–ANS relationship (n = 11), ineligible population (n = 2), preliminary or non–peer-reviewed publication status (n = 2), or lack of active vocalization (n = 3).
This resulted in a final sample of 15 included studies. Three of the full-text articles initially retained were later excluded during the data charting phase, as they did not provide analysable evidence linking vocal activity with autonomic function. The complete selection process is illustrated in the PRISMA 2020 flow diagram (Figure 1).
3.2. Characteristics and Results of Included Studies
This scoping review includes 15 studies published between 2011 and 2024, that examine the relationship between vocal activity and ANS modulation in adult populations. Most involved healthy individuals with high vocal demands—such as singers, actors, or performing arts students—while others assessed autonomic responses during vocal tasks under cognitive or emotional load.
Table 2 summarizes the main characteristics, autonomic variables, and reported outcomes of each included study. To complement the tabulated data, a descriptive summary of each study is provided below. Results are presented in chronological order and refer exclusively to outcomes explicitly reported in the original publications that are relevant to the objectives of this review.

Table 2.
Overview of the studies included in the scoping review on the relationship between voice production and autonomic nervous system function.
Table 2.
Overview of the studies included in the scoping review on the relationship between voice production and autonomic nervous system function.
| No. | First author (Year) | Study design | Study population | Study objective | Autonomic variables measured | Vocal context | Main findings | Voice–ANS interplay |
|---|---|---|---|---|---|---|---|---|
| 1 | Müller & Lindenberger (2011) [16] |
Controlled observational within-subject | n = 12 (11 singers + 1 conductor); adult choir members (Germany) | To examine how choral singing influences interpersonal synchronization of autonomic and respiratory signals, comparing unison with multipart vocal conditions. | HRV synchrony (PSI, ACI, ICI, GC), respiration (PSI, ACI, ICI, GC) | Unison singing, part singing, and canon with eyes open and closed | Respiration and HRV synchronization increased during singing (> 0.15 Hz), strongest in unison (η² = 0.83; 0.59); GC showed conductor influence (p < .0001). | Increased synchronization of respiration and HRV was observed during choral singing, particularly during unison performance. |
| 2 | Bermúdez de Alvear et al. (2013) [17] |
Controlled experimental | n = 14 healthy adults (7 men, 7 women) without known vocal or cardiovascular conditions (Spain) | To determine whether voice F₀ correlates with heart rate and blood pressure during autonomic challenge. | HR, SP, DP, MP | Sustained /æ/ phonation (5 s) duringbaseline and three autonomic tasks: handgrip, cold pressor and arithmetic. | Phonation increased HR and MBP across conditions, with ΔHR exceeding MBP changes. F₀ correlated with HR during phonation (r = .290; p < .001), but not with BP. Mental arithmetic triggered the highest HR and F₀ rise (~13 Hz). | Coupling between F₀ and HR was observed during phonation, with the strongest responses under cognitive load. |
| 3 | Vickhoff et al. (2013) [18] | Controlled experimental | n = 11; healthy 18-year-olds with choral experience (Sweden) | To characterize the autonomic response to vocal tasks with varying respiratory and rhythmic structures. |
HRV (RMSSD, coherence), RSA, HR, SC, temperature | Humming, hymn singing, mantra singing (0.1 Hz) | Mantra: ↑RMSSD (p < 0.01), highest HRV coherence; Hymn: ↑RMSSD (p < 0.05), moderate coherence; Humming: no group synchrony; SC and temp: no change. | HRV coherence and RMSSD increased during structured vocalization at 0.1 Hz, particularly with mantras and hymns, no changes observed with humming. |
| 4 | Pisanski et al. (2016) [19] |
Controlled experimental | n = 34; female undergraduate psychology students (United Kingdom) | To assess whether individual cortisol reactivity predicts changes in voice pitch during academic oral exam stress. | Salivary cortisol | Spontaneous and read speech (oral exam context) | ↑Mean and min F₀ under stress in both tasks (p = .014/.034); cortisol ↑ (+74%) predicted F₀ only under stress (rs = .46/.45); no effect on max F₀ or SD. | Increases in voice pitch during stress were associated with elevated cortisol levels, as observed in both vocal tasks. |
| 5 | MacPherson et al. (2017) [20] | Controlled experimental within-subject | n = 16; healthy young adults (USA) | To analyse the effects of cognitive load during speech on autonomic arousal and vocal acoustics. | SCR, PVA, PP | Oral reading of Stroop stimuli (congruent vs. incongruent conditions) | Cognitive load during speech increased sympathetic arousal (↑SCR, p = .001) and altered voice quality (↑CPP, p = .050; ↓L/H ratio, p = .004) | Changes in voice quality and increased sympathetic arousal were both observed during speech under cognitive stress. |
| 6 | Bernardi et al. (2017) [21] | Controlled crossover experimental | n = 20 healthy adults; no vocal training (Canada) | To examine the cardiorespiratory effects of song singing and toning and clarify whether observed changes stem from vocalization itself or the associated breathing pattern. | HRV (SDNN, LF, HF), HR | Singing of familiar slow songs (Western style) and improvised vocalization of free vowel sounds (toning) | Toning increased HRV (SDNN: p < .001, η²ₚ = 0.70) and LF power (p < .001, η²ₚ = 0.48), while reducing HF power (p < .001, η²ₚ = 0.57), compared to singing. Heart rate rose in both tasks (p = .002, η²ₚ = 0.41). Toning also induced a spontaneous breathing rhythm. | Toning was associated with a spontaneous 0.1 Hz respiratory pattern and enhanced HRV. |
| 7 | Müller et al. (2019) [22] |
Controlled within-subject experimental | n = 12; adults amateur choir members (Germany) |
To characterize the changes in network topology induced by choral singing and their association with HR and HRV as measures of autonomic activity. | HR, HRV (SDNN, RMSSD, LF/HF) | Canon singing in unison (Cun); canon singing in three parts with eyes open (Ceo) and closed (Cec) | In Cun, HR and LF/HF decreased with stronger CFC input and output (r = –0.799; r = –0.667). In Ceo, LF/HF decreased with CFC input (r = –0.576) | Unison singing was associated with increased global connectivity; multipart singing showed greater cardiorespiratory coupling. |
| 8 | Ciccarelli et al. (2019) [23] | Longitudinal observational (ambulatory) | n = 14 adults with NPVH(USA) | To characterize SCR–f₀ SD coupling in patients with NPVH during daily voice use. | EDA (SCR) | Ambulatory speech in daily life | Significant SCR– F₀ SD correlations (p < .05) were predominantly observed at a 2-minute lag in NPVH group. | Sympathetic activity (SCR) and F₀ variability were temporally aligned in NPVH participants during daily voice use. |
| 9 | Ruiz-Blais et al. (2020) [24] | Controlled experimental (within-subjects) | n = 18; non-expert singers (United Kingdom) | To determine whether vocal tasks induce HRV synchrony in non-experts, and if this coupling exceeds the effects of respiration. | HR, RMSSD; HRV inter-dyad coherence (TFC, pTFC) | Synchronized short, synchronized long, and asynchronous short notes. | ↑HRV TFC and RMSSD during long-note vocalizations (p = 0.0039 and p = 0.0002); ↑pTFC (p = 0.0078) after controlling for RSA; no HR change. | Long-note vocalizations increase HRV coherence alongside RSA. |
| 10 | Tanzmeister et al. (2022) [25] | Randomizedcontrolled experimental | n = 101; healthy amateur singers aged 18–44 (Austria) |
To evaluate if paced singing at 0.1 Hz enhances cardiovascular regulation and reduces stress reactivity. |
HR, LF-/HF-HRV, SBP, DBP | Paced singing at 0.1 Hz vs. Spontaneous singing | Paced singing (0.1 Hz): ↑LF-HRV (p < .001, d = 1.66); ↑HR (p < .001, d = 1.23); ↑SBP (p < .001, d = 1.48); no change in HF-HRV. | 0.1 Hz singing increases LF-HRV and sympathetic output. |
| 11 | Lange et al. (2022) [26] |
Experimental within-subject | n = 9; healthy adult professional singers and a male conductor (Germany) |
To test the impact of physical contact on cardiorespiratory synchronization during ensemble singing. | HRV (PSI, ACI, ICI), respiration (PSI, ACI, ICI) | Ensemble singing with and without physical contact | Singing ↑HRV synchronization (PSI η² = 0.568, p = .019); Touch vs. no touch: ↑respiration synchronization with touch (PSI η² = 0.539, p = .024); no touch effect on HRV. | Singing increased HRV synchrony, and physical contact was associated with greater respiratory synchronization. |
| 12 | Abur et al. (2023) [27] |
Prospective observational | n = 12 (6 males, 6 females) healthy older adults (68–78 years of age) (USA) | To assess the impact of cognitive load on autonomic activation and voice acoustics during structured speech tasks. | PVA, PP, SCR | Reading Stroop sentences aloud (congruent vs incongruent conditions) | During vocal tasks under cognitive load, SCR amplitude increased (p < .001) and pulse volume amplitude decreased (p = .025). No significant changes were observed in acoustic measures (CPP, L/H ratio, f₀). | Sympathetic activation was observed during speech under cognitive load, with no significant changes in vocal acoustic parameters. |
| 13 | Szkiełkowska et al. (2023) [28] | Cross-sectional observational | n = 81; 27 operas singers and 54 controls; healthy, no voice complaints (Poland) | To assess whether SEMG and ANS parameters can detect early signs of hyperfunctional dysphonia. | HRV, BVP, EDA | Sustained /æ/ phonation and glissando |
↑SEMG amplitude in subHD (SUB, max = 254 mV, and SCM, max = 201 mV); ↑HRV, ↓BVP, ↑EDA (only in singers) | SubHD shows increased laryngeal tension and altered ANS signals; patterns differed by vocal training. |
| 14 | Scherbaum & Müller (2023) [29] |
Observational study (with experimental component) | n = 3 professional male singers (Georgia) | To investigate heart rate variability synchronization during polyphonic singing. | HRV (RMSSD) | Polyphonic ensemble singing (Georgian tradition) | Two singers (top and middle voices) showed synchronized HRV patterns during singing; bass voice showed less variability and no clear synchrony. | HRV synchronization was observed during the performance of complex traditional polyphony, particularly in the most dynamically active vocal parts. |
| 15 | Kranodębska et al. (2024) [30] | Cross-sectional observational | n = 50 adults: 26 operas singers and 24 controls; all vocally healthy (Poland) | To explore the association between vocal muscle activity and autonomic responses during vocal and non-vocal tasks under emotional load. | HRV (RMSSD, SDNN, SDSD, pNN50, TRI, TINN), HR, EDA, BVP | Free phonation and glissando | Free phonation and glissando, performed under emotional load, in the full sample, showed significant correlations (p < .05) between SUB and CT amplitudes and HRV (SDNN, RMSSD, pNN50, TRI), EDA (entropy, GSR/min) and BVP. | Emotional vocal tasks revealed concurrent modulation of HRV, EDA, and BVP alongside laryngeal muscle activation (CT, SUB). |
Note. Abbreviations and variable labels are reported as in the original studies and are listed approximately in order of appearance within the table: HRV = heart rate variability; PSI = phase synchronization index; ACI = absolute coupling index; ICI = integrative coupling index; GC = Granger causality; HR = heart rate; SP/SBP = systolic blood pressure; DP/DBP = diastolic blood pressure; MBP = mean pressure; F₀ = fundamental frecuency; RMSSD = root mean square of successive differences; RSA = respiratory sinus arrhythmia; SC = skin conductance; f₀ SD = standard deviation of fundamental frequency; SCR = skin conductance response; PVA = pulse volume amplitude; PP = pulse pressure; L/H ratio = the low/high spectral ratio; SDNN = standard deviation of NN intervals; LF = low-frequency power; HF = high-frequency power; CFC = cross-frequency coupling; EDA = electrodermal activity; NPVH = non-phonotraumatic vocal hyperfunction; TFC = time–frequency coherence; pTFC = partial time–frequency coherence; CPP = cepstral peak prominence; BVP = blood volume pulse; SEMG = surface electromyography; subHD = subclinical hyperfunctional dysphonia; CT = cricothyroid; SUB = submental; SCM = sternocleidomastoid; SDSD = standard deviation of successive differences; pNN50 = percentage of adjacent NN intervals differing by more than 50 ms; TRI = triangular index; TINN = triangular interpolation of NN interval histogram; n = number of participants; p = level of statistical significance (typically p ≤ 0.05); r = correlation coefficient (strength and direction of association between variables); Δ = difference or change; η² = eta squared (effect size); η²ₚ = partial eta squared (effect size); ↑ = increase; ↓ = decrease.
In a controlled within-subject observational study with 12 adults, Müller and Lindenberger (2011) assessed HRV and respiration during unison, multipart, and canon singing (eyes open and closed). Synchronization was evaluated using PSI, ACI, ICI and GC. PSI values for respiration (F = 326.4, p < .0001, η² = 0.83) and HRV (F = 92.8, p < .0001, η² = 0.59) were significantly higher during singing, particularly in unison performances. Strongest coupling occurred above 0.15 Hz. GC analysis confirmed a significant conductor-to-choir influence (p < .0001) [16].
To investigate correlations between voice fundamental frequency (F₀) and cardiovascular parameters in response to autonomic challenges, Bermúdez de Alvear et al. (2013) designed a controlled experimental study involving 14 healthy adults. Participants produced sustained /æ/ phonation during baseline and three stress tasks (handgrip, cold pressor, and mental arithmetic). HR and SBP, DBP, MP were recorded continuously. Phonation increased HR and BP across all conditions, with ΔHR consistently exceeding pressure changes. F₀ significantly correlated with HR during phonation (r = .290, p < .001), but not with BP. Mental arithmetic induced the highest HR and F₀ increase (~13 Hz) [17].
Using a controlled experimental design, Vickhoff et al. (2013) explored autonomic responses to vocal tasks with varying rhythmic structure in a sample of 11 participants with choral experience. Tasks included free humming, hymn singing, and mantra singing paced at 0.1 Hz. Autonomic variables included HRV (RMSSD coherence), RSA, HR, skin conductance (SC), and temperature. Mantra singing produced the highest vagal activation, with significantly increased RMSSD (p < 0.01) and strong inter-subject HRV coherence at 0.1 Hz. Hymn singing also increased RMSSD (p < 0.05), but with lower coherence. Humming showed no group synchrony; SC and temperature remained unchanged [18].
The association between cortisol reactivity and vocal pitch during academic oral exam stress was explored by Pisanski et al. (2016) in a controlled experimental study involving 34 female psychology students. Participants completed baseline and stress phases involving spontaneous and read speech. Salivary cortisol levels increased by 74% under stress, and this rise significantly predicted mean F₀ in both spontaneous (rs = .46) and read speech (rs = .45) produced under stress. Both mean F₀ (p = .014) and minimum F₀ (p = .034) increased during the stress condition, with no changes in the maximum or variability of F₀ [19].
A controlled within-subject design was employed to evaluate autonomic and vocal changes in 16 healthy adults during cognitive stress, as reported by MacPherson et al. (2017). Participants read congruent and incongruent Stroop stimuli aloud while SCR, PVA, and PP were recorded. Voice quality was assessed using cepstral peak prominence (CPP) and the low/high spectral ratio (L/H ratio). The incongruent condition increased sympathetic arousal (SCR, p = .001), reduced L/H ratio (p = .004), and showed a trend toward increased CPP (p = .050). Both autonomic and vocal parameters changed during speech under cognitive load, although no significant associations were found between them [20].
To compare the autonomic responses elicited by different types of vocalizations, Bernardi et al. (2017) conducted a controlled crossover experimental study with 20 healthy adults without vocal training. HR and HRV—including the SDNN, LF, and HF—were measured. Toning increased SDNN (p < .001, η²ₚ = 0.70) and LF power (p < .001, η²ₚ = 0.48), and decreased HF power (p < .001, η²ₚ = 0.57), in comparison with singing. HR rose in both tasks (p = .002, η²ₚ = 0.41), with no between-condition differences. Toning also induced a spontaneous breathing rhythm near 0.1 Hz [21].
Evidence from a within-subject study with 12 adult choir members highlights the evaluation of autonomic responses and physiological coupling during choral singing, as conducted by Müller et al. (2019). Participants sang a canon under three conditions: unison (Cun), three-part with eyes open (Ceo), and with eyes closed (Cec). HR and HRV (SDNN, RMSSD, LF/HF) were recorded, and CFC was used to quantify synchrony across vocal, respiratory, and cardiac rhythms. In Cun, HR was negatively correlated with CFC input strength (r = –0.799, p = .001), and LF/HF with CFC output (r = –0.667, p = .016). In Ceo, LF/HF was also negatively correlated with CFC input strength (r = –0.576, p = .049) [22].
A longitudinal observational design was used by Ciccarelli et al. (2019) to examine the relationship between sympathetic activation and voice variability during daily speech in individuals diagnosed with non-phonotraumatic vocal hyperfunction (NPVH). EDA was measured using SCR, and the standard deviation of fundamental frequency (f₀ SD) was calculated from ambulatory voice recordings. Significant SCR–f₀ SD correlations (p < .05) were predominantly observed at a 2-minute lag in the NPVH group [23].
Ruiz-Blais et al. (2020) implemented a within-subject experimental study with 18 non-expert singers in dyads to evaluate HRV synchrony during vocal tasks and its relation to respiration. Participants performed synchronized short notes, asynchronous short notes, and synchronized long-note vocalizations. Autonomic measures included HR, RMSSD, and HRV inter-dyad coherence using TFC to assess overall synchrony, and partial TFC (pTFC) to isolate effects beyond RSA. Long-note vocalizations significantly increased RMSSD (p = 0.0002), TFC (p = 0.0039), and pTFC (p = 0.0078). The pTFC increase remained significant after controlling for RSA. No changes in HR were observed [24].
The physiological effects of paced vocalization at 0.1 Hz versus spontaneous singing were examined in a randomized controlled trial involving 101 healthy amateur singers, as described by Tanzmeister et al. (2022). The study assessed autonomic parameters including HR, LF-/HF-HRV, and systolic/diastolic blood pressure (SBP/DBP). Paced singing significantly increased LF-HRV (p < 0.001, d = 1.66), HR (p < 0.001, d = 1.23), and SBP (p < 0.001, d = 1.48), with no significant effect on HF-HRV [25].
The effects of ensemble singing on cardiorespiratory synchronization were investigated in a within-subject experimental study with 9 professional singers, as detailed in Lange et al. (2022). HRV and respiration were recorded and analysed using PSI, ACI and ICI. Singing significantly increased HRV synchrony (PSI η² = 0.568, p = .019). Physical contact did not affect HRV coupling but led to a significant increase in respiratory synchronization (PSI η² = 0.539, p = .024) [26].
In a prospective observational study, Abur et al. (2023) assessed autonomic and vocal responses in 12 older adults (68–78 years) during speech tasks with varying cognitive demand. Participants performed aloud reading of Stroop-type sentences in congruent (low load) and incongruent (high load) conditions. Autonomic variables included SCR, PVA, and PP, as indicators of sympathetic nervous system activity. SCR increased significantly (p < .001) and PVA decreased (p = .025) during high-load vocal conditions. No significant changes were found in acoustic parameters (CPP, L/H ratio, f₀) [27].
Electrophysiological and autonomic measures were explored as potential markers of subclinical hyperfunctional dysphonia (subHD) in 81 adults without vocal complaints (27 singers, 54 non-singers), as presented in Szkiełkowska et al. (2023). Participants underwent laryngeal exams, surface electromyography (SEMG) of neck muscles, and autonomic assessment (HRV, BVP, EDA) using Empatica E4 during sustained /æ/ phonation and glissando. SubHD was identified in 26 cases, who showed increased SEMG amplitudes [submental (SUB) max = 254 mV; sternocleidomastoid (SCM) max = 201 mV], higher HRV, reduced BVP, and elevated EDA (in singers only) during vocal tasks [28].
In an observational study incorporating experimental elements, Scherbaum & Müller (2023) investigated HRV synchronization during polyphonic singing in 3 professional male performers. HRV (RMSSD) was monitored via finger pulse sensors while participants performed the Georgian song Chven Mshvidoba. The top and middle voice singers exhibited closely aligned HRV patterns, particularly during dynamic vocal segments. In contrast, the bass singer showed lower HRV variability and lacked synchrony [29].
In a recent study, Krasnodębska et al. (2024) examined associations between vocal muscle activation and autonomic responses during emotionally loaded tasks in a cross-sectional observational design involving 50 vocally healthy adults (26 opera singers, 24 non-singers). Participants performed free phonation and glissando, while surface EMG recorded activity from SUB, cricothyroid (CT), and SCM muscles. Simultaneously, HRV (RMSSD, SDNN, SDSD, pNN50, TINN), HR, EDA (entropy, GSR/min), and BVP were monitored. Significant correlations (p < .05) were found between SUB and CT amplitudes and autonomic markers (HRV, EDA, BVP) during both free phonation and glissando, with no associations observed for the SCM [30].
4. Discussion
The studies included in this scoping review consistently show that structured vocal tasks are associated with detectable changes in autonomic parameters, particularly HRV, EDA, and BVP. These responses were observed across various contexts, including sustained phonation, group singing, and vocal tasks involving emotional or cognitive load, with variations depending on task characteristics and participant profiles. One of the most recurrent findings is the occurrence of physiological synchronization among individuals during collective vocalization, suggesting autonomic coordination through shared respiratory and cardiac rhythms. Additionally, several studies indicate that rhythm, temporal regularity, and vocal continuity influence cardiorespiratory dynamics, reinforcing the regulatory potential of slow and repetitive vocalization. The interaction between autonomic activity and the emotional or cognitive demands of speech has also been highlighted, pointing to a bidirectional relationship between physiological arousal and vocal production. Finally, studies focusing on clinical and subclinical populations reveal an association between laryngeal muscle activity and autonomic indicators, supporting the integration of physiological measures in the assessment of functional or effort-related dysphonia. Considered as a whole, these findings support the active involvement of the autonomic nervous system in vocal behaviour and its relevance in both clinical and experimental contexts.
4.1. Autonomic Synchronization During Group Vocalization
Group singing has been shown to enhance physiological synchronization, as demonstrated in the study by Müller and Lindenberger (2011), which reported increased coupling in both respiratory and cardiac rhythms, measured through PSI and ACI—particularly during unison performance. The effect was amplified at frequencies above 0.15 Hz, suggesting a strong connection between rhythmic vocal output and autonomic entrainment. These results support the hypothesis that choral singing promotes autonomic synchrony through coordinated modulation of respiratory patterns and HRV [16]. Expanding on this, Müller et al. (2019) used CFC analyses to show that unison singing was associated with reduced sympathetic activity, while multipart singing was linked to parasympathetic engagement, indicating differential autonomic modulation depending on the vocal coordination style [22].
Following a similar approach, Ruiz-Blais et al. (2020) observed a significant increase in HRV coherence between dyads of non-expert singers during synchronized sustained vocalizations, especially when producing long sustained notes. This coupling persisted after accounting for respiratory effects using pTFC, supporting the presence of specific interpersonal autonomic modulation during shared vocalization [24]. Similarly, Lange et al. (2022) demonstrated that group singing increases HRV synchrony compared to rest, and that physical contact between performers further enhances respiratory coordination without modifying cardiac coupling [26].
Scherbaum and Müller (2023) observed HRV synchronization between the top and middle vocal parts during traditional Georgian polyphony, most clearly during dynamically expressive passages [29]. In contrast, the lower voice, characterized by greater vocal stability, showed no such synchrony, suggesting that vocal variability may play a key role in eliciting shared physiological responses. Although primarily focused on vocal structure, Vickhoff et al. (2013) also documented inter-subject HRV coherence during mantra singing at 0.1 Hz, reinforcing the notion that rhythmically structured vocalization supports interpersonal autonomic alignment [18].
Overall, the findings confirm that group vocal tasks—particularly those involving rhythmic structure, unison performance, or synchronized emission of long notes—induce autonomic synchronization between participants, as evidenced by HRV and respiratory coherence. This synchronization entails differential modulation of sympathetic and parasympathetic tone depending on the type of vocal coordination involved. Supporting this conclusion, highly localized respiratory and HRV synchrony among choir singers has been demonstrated using advanced signal decomposition techniques, including intersubject correlation (ISC) and normalized intersubject phase synchrony (N-IPS) algorithms. Although their analysis focused on physiological coupling without direct assessment of vocal parameters, their results reinforce the notion that collective vocal engagement promotes interpersonal autonomic synchrony through tightly coordinated respiratory and cardiac rhythms [31].
4.2. Autonomic Modulation by Type and Structure of Vocalization
Two studies reported that vocalizations near 0.1 Hz enhance vagal tone, although their approaches differed: while Vickhoff et al. (2013) used highly structured mantra chanting to demonstrate increased RMSSD and HRV coherence between individuals, Bernardi et al. (2017) showed that even unstructured toning could spontaneously induce slow breathing and elevate SDNN and LF-HRV. This suggests that vocal rhythm, whether trained or spontaneous, can entrain autonomic regulation through respiratory pathways [18,21].
In contrast, Tanzmeister et al. (2022) found that paced singing at 0.1 Hz increased LF-HRV but also elevated HR and BP, reflecting a mixed autonomic response. Unlike the previous studies, this protocol employed explicit pacing and likely introduced greater cognitive demand, potentially leading to sympathetic co-activation despite respiratory deceleration [25].
Additional evidence is provided by Ruiz-Blais et al. (2020), who showed that synchronized long-note vocalizations enhanced HRV coherence and increased pTFC beyond what could be explained by RSA alone. This indicates that vocal continuity, not just respiratory rate, contributes significantly to interpersonal autonomic coupling [24].
These results indicate that rhythmically structured vocalizations performed at slow tempos (~0.1 Hz) can modulate both sympathetic and parasympathetic activity. The extent of this modulation appears to depend on vocal continuity, task complexity, and the depth of respiratory involvement. This interpretation is supported by studies on paced breathing and resonance frequency: enhanced vagal activity has been observed when breathing is paired with rhythmic motor patterns at 0.1 Hz and resonance breathing has been shown to entrain autonomic rhythms through central-peripheral synchronization. Although non-vocal, these findings reinforce the physiological plausibility of slow, structured vocalization as a driver of autonomic regulation, mainly parasympathetic [32,33].
4.3. Autonomic Responses to Emotional and Cognitive Vocal Demands
An initial association between fundamental frequency (F₀) and HR during speech was described by Orlikoff and Baken [34]. In line with this, Bermúdez de Alvear et al. (2013) identified a similar relationship under mental effort, suggesting that cardiac autonomic modulation may shape laryngeal control [17]. This view is further supported by findings from Pisanski et al. (2016), who showed that increases in voice pitch under real-life stress were associated with elevated cortisol, indicating hypothalamic–pituitary–adrenal (HPA) axis involvement in vocal modulation [19].
Evidence from MacPherson et al. (2017) revealed alterations in voice quality during emotionally valenced speech, consistent with increased sympathetic activity [20]. Similarly, Krasnodębska et al. (2024) demonstrated specific coupling between autonomic indices (HRV, EDA, BVP) and laryngeal muscle activation (CT and SUB), highlighting the physiological demand of emotionally expressive vocalization [30].
Conversely, Abur et al. (2023) observed a dissociation between sympathetic activation and vocal acoustics during speech under cognitive load in older adults, though the extent to which age contributed to this finding remains unclear [27].
Together, these studies reveal that emotional and cognitive vocal tasks can elicit varying degrees of autonomic–vocal interaction, with some contexts promoting close physiological integration, while others show potential dissociation, likely shaped by task characteristics and individual factors. Although not included in the final review set, recent studies offer complementary evidence supporting the impact of emotionally demanding performance on autonomic regulation. Acoustic shifts under stress have been observed, underscoring vocal sensitivity to emotional load even in the absence of direct autonomic recordings [15]. Additionally, significant changes in autonomic function have been reported during live piano performance in professional musicians, including increased HR and BP, elevated sympathetic activity, and reduced baroreceptor sensitivity, suggesting that performance-related stress elicits robust autonomic responses comparable to those observed in voice-related tasks [35].
4.4. Vocal Effort, Functional Dysphonia, and Autonomic Signatures
Ciccarelli et al. (2019) found a significant association between sympathetic activation (as measured by SCR) and increased f₀ SD during daily speech in individuals with NPVH. The observed coupling emerged with a temporal lag, suggesting a delayed but specific autonomic influence on voice variability [23].
Extending this line of evidence to a subclinical population, Szkiełkowska et al. (2023) studied individuals with signs of hyperfunctional dysphonia and found that affected participants exhibited elevated SUB and SCM muscle activation during phonation, as well as autonomic alterations—namely, increased HRV and EDA and reduced BVP. These patterns were particularly notable in trained singers, highlighting how vocal training may shape the interaction between muscle tension and autonomic regulation [28].
Supporting this perspective, Krasnodębska et al. (2024) observed consistent correlations between laryngeal muscle activity (CT and SUB) and multiple autonomic markers (HRV, EDA, BVP) during emotionally loaded vocal tasks, reinforcing the role of vocal effort in autonomic engagement. In contrast, no such associations were found for the SCM muscle, pointing to functional specificity within the vocal tract [30].
Among the reviewed studies, there is consistent support for a link between vocal effort and autonomic reactivity, with evidence of specific coupling between laryngeal muscle activity and autonomic markers. While most studies employed experimental protocols with surface electromyography and direct autonomic recordings, one additional study provide complementary clinical insight by identifying reduced parasympathetic activity—reflected in lower RMSSD and pNN50—in teachers reporting functional voice disorders. These individuals also presented neurovegetative symptoms linked to vocal fatigue, underscoring how autonomic imbalance may manifest in occupational voice users even in the absence of overt structural pathology [4]. Taken together, the findings suggest that integrating autonomic assessment in voice evaluation could help detect early dysfunction and refine diagnostic criteria in functional and subclinical dysphonia.
5. Limitations
Although this scoping review was designed with a rigorous methodological framework, certain limitations should be acknowledged. In line with PRISMA-ScR guidelines, no formal critical appraisal of the included studies was conducted, as the primary aim was to map existing evidence rather than assess study quality. Nonetheless, the inclusion of studies with heterogeneous designs and small sample sizes may influence the consistency of reported associations. Additionally, gray literature and unpublished sources were excluded, which may have limited the retrieval of other relevant findings. The wide variability in vocal tasks, autonomic parameters, and methodological approaches across studies posed challenges for direct comparisons; however, this heterogeneity was mitigated through thematic synthesis in the discussion. Despite these factors, the review provides a structured and meaningful overview of current knowledge on the interplay between voice and the autonomic nervous system.
6. Conclusions and Future Directions
This scoping review systematically mapped the current evidence on the relationship between voice production and ANS interactions in adult populations. The studies demonstrate that vocal activity, particularly when structured, emotionally loaded, or cognitively demanding, can elicit measurable changes in autonomic markers such as HR, BP, HRV, EDA, and BVP. These physiological responses vary according to the type of vocal task, the context in which it is performed, and the functional vocal profile of the participants.
Four thematic trends emerged from the literature: (1) group vocalization tasks can induce autonomic synchronization between participants, (2) slow-paced and rhythmically structured vocalizations modulate sympathetic and parasympathetic tone via respiratory coupling, (3) emotional and cognitive vocal challenges reveal context-dependent voice–ANS interplay, and (4) hyperfunctional voice profiles are consistently associated with altered autonomic regulation.
Despite methodological heterogeneity, the findings converge on the notion that the ANS is actively engaged during vocal behaviour and may contribute to the regulation, adaptation, and potential dysfunction of voice production. These insights underscore the relevance of incorporating autonomic assessment into voice research and clinical voice evaluation.
Future studies should focus on standardizing physiological protocols, expanding research to clinical populations with functional dysphonia, and further exploring the bidirectional relationship between vocal effort and autonomic modulation. Progress may also result from the incorporation of structured and comparative vocal tasks, which could help delineate the physiological patterns associated with distinct vocal profiles. Integrating objective autonomic measures into voice assessment represents a promising approach for improving early detection of dysfunction, refining functional diagnoses, and guiding more personalized interventions in both clinical and occupational contexts.
Author Contributions
Conceptualization, C.M.-L. and L.C.-F.; Methodology, C.M.-L., L.C.-F. and M.G.-G.; Investigation, C.M.-L., L.C.-F. and M.G.-G.; Data curation, M.G.-G.; Writing—original draft preparation, C.M.-L.; Writing—review and editing, M.G.-G., M.S.D.-M. and M.V.L.-G.; Supervision, M.V.L.-G. and M.S.D.-M. All authors contributed substantially to the development of this scoping review: Carmen Morales-Luque (C.M.-L.), predoctoral researcher (FPU program, Spanish Ministry of Science), coordinated the design and implementation of the methodological protocol, participated in the screening and data extraction process, and led the writing of the original draft. She also refined the inclusion criteria and guided the organization of results and discussion. Laura Carrillo-Franco (L.C.-F.), predoctoral researcher (PIF program, UMA), collaborated in the conceptual and methodological development of the review, assisted in study selection and data analysis, and contributed to the interpretation of findings. Marta González-García (M.G.-G.), lecturer in Nursing at the University of Málaga, supported methodological design and contributed clinical insight during the evidence synthesis. She was also responsible for curating and verifying extracted data and participated in the critical review of the manuscript. Manuel Víctor López-González (M.V.L.-G.) and Marc Stefan Dawid-Milner jointly supervised the review process, contributed to the refinement of the discussion and structure, and ensured scientific and editorial accuracy.
Funding
This study was supported by a program grant Junta de Andalucía, Groups nº CTS-156. Open access publication was funded by the University of Málaga / CBUA.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| HRV | Heart Rate Variability |
| PSI | Phase Synchronization Index |
| ACI | Absolute Coupling Index |
| ICI | Integrative Coupling Index |
| GC | Granger Causality |
| HR | Heart Rate |
| BP | Blood Pressure |
| MP | Mean Pressure |
| F₀ | Fundamental Frequency |
| RMSSD | Root Mean Square of Successive Differences |
| RSA | Respiratory Sinus Arrhythmia |
| SC | Skin Conductance |
| f₀ SD | Standard Deviation of Fundamental Frequency |
| SCR | Skin Conductance Response |
| PVA | Pulse Volume Amplitude |
| PP | Pulse Pressure |
| L/H ratio | Low/High Spectral Ratio |
| SDNN | Standard Deviation of NN Intervals |
| LF | Low-Frequency Power |
| HF | High-Frequency Power |
| CFC | Cross-Frequency Coupling |
| EDA | Electrodermal Activity |
| NPVH | Non-Phonotraumatic Vocal Hyperfunction |
| TFC | Time–Frequency Coherence |
| pTFC | Partial Time–Frequency Coherence |
| SBP | Systolic Blood Pressure |
| DBP | Diastolic Blood Pressure |
| CPP | Cepstral Peak Prominence |
| BVP | Blood Volume Pulse |
| SEMG | Surface Electromyography |
| subHD | Subclinical Hyperfunctional Dysphonia |
| CT | Cricothyroid |
| SUB | Submental |
| SCM | Sternocleidomastoid |
| SDSD | Standard Deviation of Successive Differences |
| pNN50 | Percentage of Adjacent NN Intervals Differing by More Than 50 ms |
| TRI | Triangular Index |
| TINN | Triangular Interpolation of NN Interval Histogram |
References
- Chhetri, D.K.; Neubauer, J.; Sofer, E.; Berry, D.A. Influence and interactions of laryngeal adductors and cricothyroid muscles on fundamental frequency and glottal posture control. J. Acoust. Soc. Am. 2014, 135, 2052–2064. [Google Scholar] [CrossRef]
- Lã,, F. M.B.; Gill, B.P. Physiology and its impact on the performance of singing. In The Oxford Handbook of Singing, Welch, G., Howard, D.M., Nix, J., Eds.; Oxford University Press: Oxford, UK, 2015; pp. 66–84. [Google Scholar] [CrossRef]
- Achey, M.A.; He, M.Z.; Akst, L.M. Vocal hygiene habits and vocal handicap among conservatory students of classical singing. J. Voice 2016, 30, 192–197. [Google Scholar] [CrossRef]
- Cardoso, R.; Meneses, R.F.; Lumini-Oliveira, J.; Pestana, P. Associations between teachers’ autonomic dysfunction and voice complaints. J. Voice 2021, 35, 843–851. [Google Scholar] [CrossRef]
- Castelblanco, L.; Habib, M.; Stein, D.J.; de Quadros, A.; Cohen, S.M.; Noordzij, J.P. Singing voice handicap and videostrobolaryngoscopy in healthy professional singers. J. Voice 2014, 28, 608–613. [Google Scholar] [CrossRef]
- D’haeseleer, E.; Claeys, S.; Meerschman, I.; Bettens, K.; Degeest, S.; Dijckmans, C.; et al. Vocal characteristics and laryngoscopic findings in future musical theater performers. J. Voice 2017, 31, 462–469. [Google Scholar] [CrossRef] [PubMed]
- El-Demerdash, A.M.; Hafez, N.G.; Tanyous, H.N.; Rezk, K.M.; Shadi, M.S. Screening of voice and vocal tract changes in professional wind instrument players. Eur. Arch. Otorhinolaryngol. 2024, 281, 4903–4911. [Google Scholar] [CrossRef] [PubMed]
- Wehrwein, E.A.; Orer, H.S.; Barman, S.M. Overview of the anatomy, physiology, and pharmacology of the autonomic nervous system. Compr. Physiol. 2016, 6, 1239–1278. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, C.H. Basics of autonomic nervous system function. In Low, P.A.; Benarroch, E.E. Handb. Clin. Neurol., Ed.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 407–418. [Google Scholar] [CrossRef]
- Benarroch, E.E. Physiology and pathophysiology of the autonomic nervous system. Continuum (Minneap. Minn.) 2020, 26, 12–24. [Google Scholar] [CrossRef]
- Grossman, P.; Taylor, E.W. Toward understanding respiratory sinus arrhythmia: Relations to cardiac vagal tone, evolution and biobehavioral functions. Biol. Psychol. 2007, 74, 263–285. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Helou, L.B.; Jennings, J.R.; Rosen, C.A.; Wang, W.; Verdolini Abbott, K. Intrinsic laryngeal muscle response to a public speech preparation stressor: Personality and autonomic predictors. J. Speech Lang. Hear. Res. 2020, 63, 2940–2951. [Google Scholar] [CrossRef]
- Motamed Yeganeh, N.; McKee, T.; Werker, J.F.; Hermiston, N.; Boyd, L.A.; Cui, A.-X. Opera trainees’ cognitive functioning is associated with physiological stress during performance. Musicae Sci. 2024, 28, 365–374. [Google Scholar] [CrossRef]
- Dahl, K.L.; Stepp, C.E. Effects of cognitive stress on voice acoustics in individuals with hyperfunctional voice disorders. Am. J. Speech Lang. Pathol. 2023, 32, 264–274. [Google Scholar] [CrossRef]
- Müller, V.; Lindenberger, U. Cardiac and respiratory patterns synchronize between persons during choir singing. PLoS ONE 2011, 6(9), e24893. [Google Scholar] [CrossRef]
- Bermúdez de Alvear, R.M.; Barón-López, F.J.; Alguacil, M.D.; Dawid-Milner, M.S. Interactions between voice fundamental frequency and cardiovascular parameters. Preliminary results and physiological mechanisms. Logoped Phoniatr Vocol 2013, 38(1), 52–58. [Google Scholar] [CrossRef] [PubMed]
- Vickhoff, B.; Malmgren, H.; Åström, R.; Nyberg, G.; Ekström, S.-R.; Engwall, M.; et al. Music structure determines heart rate variability of singers. Front Psychol 2013, 4, 334. [Google Scholar] [CrossRef] [PubMed]
- Pisanski, K.; Nowak, J.; Sorokowski, P. Individual differences in cortisol stress response predict increases in voice pitch during exam stress. Physiol Behav 2016, 163, 234–238. [Google Scholar] [CrossRef]
- MacPherson, M.K.; Abur, D.; Stepp, C.E. Acoustic measures of voice and physiologic measures of autonomic arousal during speech as a function of cognitive load. J Voice 2017, 31(4), 504.e1–504.e9. [Google Scholar] [CrossRef]
- Bernardi, N.F.; Snow, S.; Peretz, I.; Orozco Perez, H.D.; Sabet-Kassouf, N.; Lehmann, A. Cardiorespiratory optimization during improvised singing and toning. Sci Rep 2017, 7, 8113. [Google Scholar] [CrossRef]
- Müller, V.; Delius, J.A.M.; Lindenberger, U. Hyper-frequency network topology changes during choral singing. Front Physiol 2019, 10, 207. [Google Scholar] [CrossRef] [PubMed]
- Ciccarelli, G.; Mehta, D.; Ortiz, A.; Van Stan, J.; Toles, L.; Marks, K.; et al. Correlating an ambulatory voice measure to electrodermal activity in patients with vocal hyperfunction. Proc Int Conf Wearable Implant Body Sens Netw 2019, 1–5. [Google Scholar] [CrossRef]
- Ruiz-Blais, S.; Orini, M.; Chew, E. Heart rate variability synchronizes when non-experts vocalize together. Front Physiol 2020, 11, 7–62. [Google Scholar] [CrossRef] [PubMed]
- Tanzmeister, S.; Rominger, C.; Weber, B.; Tatschl, J.M.; Schwerdtfeger, A.R. Singing at 0.1Hz as a resonance frequency intervention to reduce cardiovascular stress reactivity? Front Psychiatry 2022, 13, 876344. [Google Scholar] [CrossRef] [PubMed]
- Lange, E.B.; Omigie, D.; Trenado, C.; Müller, V.; Wald-Fuhrmann, M.; Merrill, J. Intouch: Cardiac and respiratory patterns synchronize during ensemble singing with physical contact. Front Hum Neurosci 2022, 16, 928563. [Google Scholar] [CrossRef]
- Abur, D.; MacPherson, M.K.; Shembel, A.C.; Stepp, C.E. Acoustic measures of voice and physiologic measures of autonomic arousal during speech as a function of cognitive load in older adults. J Voice 2023, 37(2), 194–202. [Google Scholar] [CrossRef] [PubMed]
- Szkiełkowska, A.; Krasnodębska, P.; Mitas, A.; Bugdol, M.; Romaniszyn-Kania, P.; Pollak, A. Electrophysiological predictors of hyperfunctional dysphonia. Acta Otolaryngol 2023, 143(1), 56–63. [Google Scholar] [CrossRef]
- Scherbaum, F.; Müller, M. From intonation adjustments to synchronization of heart rate variability: Singer interaction in traditional Georgian vocal music. Musicologist 2023, 7(2), 155–177. [Google Scholar] [CrossRef]
- Krasnodębska, P.; Szkiełkowska, A.; Pollak, A.; Romaniszyn-Kania, P.; Bugdol, M.N.; Bugdol, M.D.; et al. Analysis of the relationship between emotion intensity and electrophysiology parameters during a voice examination of opera singers. Int J Occup Med Environ Health 2024, 1, 84–97. [Google Scholar] [CrossRef]
- Hemakom, A.; Powezka, K.; Goverdovsky, V.; Jaffer, U.; Mandic, D.P. Quantifying team cooperation through intrinsic multi-scale measures: respiratory and cardiac synchronization in choir singers and surgical teams. R. Soc. Open Sci. 2017, 4, 170853. [Google Scholar] [CrossRef]
- Chin, M.S.; Kales, S.N. Understanding mind-body disciplines: A pilot study of paced breathing and dynamic muscle contraction on autonomic nervous system reactivity. Stress Health 2019, 35, 542–548. [Google Scholar] [CrossRef]
- Schwerdtfeger, A.R.; Schwarz, G.; Pfurtscheller, K.; Thayer, J.F.; Jarczok, M.N.; Pfurtscheller, G. Heart rate variability (HRV): From brain death to resonance breathing at 6 breaths per minute. Clin. Neurophysiol. 2020, 131, 676–693. [Google Scholar] [CrossRef] [PubMed]
- Orlikoff, R.F.; Baken, R.J. The effect of the heartbeat on vocal fundamental frequency perturbation. J. Speech Hear. Res. 1989, 32, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Gutiérrez, J.Á.; de Rojas Leal, C.; López-González, M.V.; Chao-Écija, A.; Dawid-Milner, M.S. Impact of music performance anxiety on cardiovascular blood pressure responses, autonomic tone and baroreceptor sensitivity to a western classical music piano-concert. Front. Neurosci. 2023, 17, 1213117. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA 2020 flow diagram of study selection.
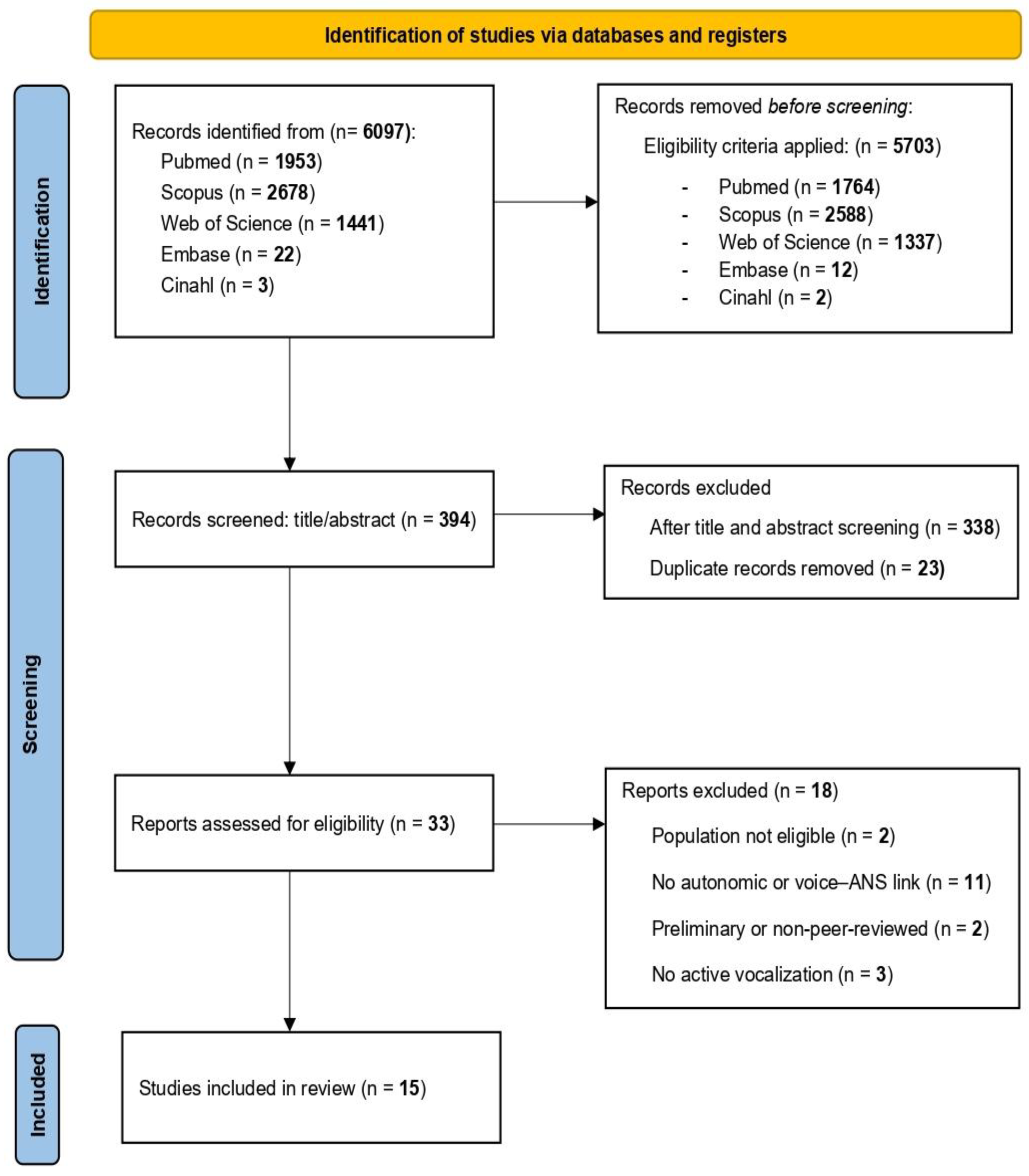
Table 1.
Keywords used in the search strategy, organized by PCC component.
| PCC | Keywords |
|---|---|
| (P) | "Professional Voice Users", "Teachers", "Singers", "Voice Disorders", "Functional Dysphonia", "Muscle Tension Dysphonia", "Vocal Hyperfunction" |
| (C) | "Voice", "Singing", “Voice production”, “Vocal effort”, “Autonomic Nervous System", "Autonomic Dysfunction", "Autonomic Regulation", "Sympathetic Nervous System", "Parasympathetic Nervous System", "Heart Rate Variability", "HRV", "Heart Rate", "Heartbeat", "Blood Pressure", "Stress Response" |
| (C) | “Structured vocal tasks”, "Singing Ensemble", “Singing performance”, “Spoken tasks under stress”, “Cognitive-emotional vocal conditions”, “Experimental voice protocols” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



