Submitted:
28 July 2025
Posted:
29 July 2025
You are already at the latest version
Abstract
Gunshot injuries are challenging conditions because of the unique characteristics of the wounding agents producing soft tissue damage that may be compounded by the formation of an expanding temporary cavity (cavitation). Variations in the ballistic performance leading to higher energy transfer by the projectile, including bullet tumbling, deformation and fragmentation, cause increased soft tissue injury and may also lead to more extensive bone comminution compromising local blood supply. Once life-threatening injuries have been excluded or properly addressed, the emergency management of localized trauma from bullets and shotgun pellets may be complicated due to progressive tissue necrosis within the zone of injury. Additionally, the risk of infection should be tackled especially in high energy bone injuries. War experience suggests a baseline separation between wounds with limited tissue destruction which can routinely be managed as simple penetrating injuries and those resulting from high energy transfer to the tissues involving a substantial amount of necrotic elements surrounding the wound channel which call for a more aggressive surgical approach. A further justification for such a distinction is the need for antibiotic therapy, which varies according to most studies depending on the wounding mechanism, the nature of the wound and the extent of tissue injury. The emergency physician should also be aware of the possibility of “bizarre” bullet paths resulting in occult injuries of important anatomic structures.
Keywords:
gunshot wounds
; wound ballistics
; penetrating trauma
; shotgun injuries
; vascular injuries
; assault rifles
1. Introduction
The greater availability of firearms in modern societies has resulted in increased frequency of gunshot injuries and deaths among civilians, due to suicide attempts, assaults and unintentional discharge of guns [1]. Whereas most self-inflicted injuries of this type result in death and only few wounded arrive in hospital emergency departments alive, more victims of firearm-related violence in general suffer nonfatal injuries than die [2]. Firearm injuries remain challenging because of the unique characteristics of the wounding agents and the resultant trauma which may involve unpredictable wound tracks and additional collateral damage due to the phenomenon of cavitation leading to progressive tissue necrosis, especially with high energy injuries. Such injuries are seen in mass shooting incidents against civilians by lone actors and terrorist groups using military-type rifles [3,4].
Effective management of gunshot injuries in the emergency department requires an understanding of the behavior of bullets and other types of projectiles (e.g., fragments, shotgun pellets) in the human body to support the diagnostic process and the interpretation of imaging studies [5,6]. Moreover, certain aspects of the initial management of these injuries, such as the benefit for antibiotic prophylaxis and the removal of retained projectiles, have to be addressed according to the currently best available evidence [7].
2. Wound Ballistics
The term wound ballistics refers to the subset of terminal ballistics (the study of the effects of a projectile within the target) which examines the behavior of and the damage caused by penetrating projectiles in human and animal tissue and certain tissue simulants [8,9]. Gunshot wounds are produced by bullets, which by means of their velocity perforate skin and deeper tissues acting as kinetic energy penetrators. Whereas gunshot wounds are usually classified under penetrating trauma, their mechanism involves features of both blunt and penetrating injury [5,10,11].
Projectiles from firearms are commonly separated according to their velocity at the point of exit from the barrel of the gun (muzzle velocity) into two main categories. High-velocity projectiles include rifle bullets and experimental projectiles exceeding velocities of 600-760 m/s (fragments from explosive devices also fall into this category) [12,13,14] whereas handgun bullets travel at or below the speed of the sound in air (340 m/s), thus considered low-velocity projectiles. A third category comprises projectiles with medium velocities, such as those from Magnum handgun cartridges, between 400 m/s and 450 m/s [12].
An important categorization of bullets related to their construction, which corresponds to distinctly different ballistic behavior within the target, is between expanding and nonexpanding ones [15,16]. Expanding bullets include solid lead bullets (used exclusively with handguns), copper-plated lead bullets, and semi-jacketed bullets with an open tip available in soft-point and hollow-point types. Designed expanding bullets intend to maximize the tissue damage with a greater amount of energy transferred [15,16], in the case of hunting ammunition (typically soft-point rifle bullets) with the aim to effectively kill the game [15,17]. Full metal-jacketed (FMJ) projectiles are nonexpanding, typically consisting of a soft lead core encased in a jacket made of harder metal, such as cupronickel, which completely covers the tip but usually leaves the base of the bullet open [18] (Figure 1). Since the ban on expanding (“Dum-Dum”) bullets imposed for military use by the Third Declaration of the 1899 Hague Convention, on the grounds of avoiding unnecessary suffering [19], the FMJ construction became the standard for military small arms ammunition. Assault rifles, which are the modern type of military rifle, use bullets with smaller cartridges containing less propellant compared to full-powered military rifle cartridges previously used, as it was found that the latter didn’t offer a significant tactical advantage in typical infantry battle conditions. However, there have been recent reports for use of illegal ammunition with expanding bullets in the war of Ukraine [20,21]. Modern designs of military bullets contain various components of steel with or without a lead core.
2.1. Dynamics of Penetrating Projectiles
High-velocity bullets are capable of completely perforating the human body [15,17] whereas low-velocity ones may or may not exit the body depending on the anatomic areas they pass through. A projectile that comes to rest within the body has obviously delivered all of its available energy to the tissues [18]. The importance of the projectile velocity in the wounding process can be deduced from the kinetic energy formula K=1/2mv2, which states that the kinetic energy K associated with the motion of an object is proportional to its mass m but the dominant determinant is its velocity v as the latter enters the equation raised to the second power [14,22]. The energy transferred to the object by the force that accelerates it (the firing of the gun in the case of a projectile launched from a firearm) can also be transferred from the moving object once a decelerating force applies on it [23]. Theoretically, the kinetic energy of a projectile penetrating tissue is the energy available for transfer via a retarding force (drag) due to tissue resistance acting against the projectile motion. However, it remains controversial to which extent the kinetic energy formula can convey the tissue damage produced during the projectile-tissue interaction [8,24]. Specifically, this formula does not reflect the increased tissue damage from tumbling projectiles [25].
Projectiles with the same kinetic energy at impact but different masses and velocities behave differently in the same type of tissue, creating different wound morphologies [8]. This has been shown in gelatin (used as an ideal skeletal muscle simulant) [26], where the penetration depth is usually less for the projectile that is smaller and faster compared to the heavier, slower one [27]. Whereas the letter causes mainly crushing and disruption of the material that contacts, the lighter, faster sphere dissipates most of its kinetic energy by propelling tissue sideways resulting in the formation of a temporary cavity (cavitation) [26].
Military rifle bullets penetrate tissue initially with the longitudinal axis of the bullet close to its line of trajectory (i.e., at stable flight) [28] creating a wound channel with roughly the same diameter as the projectile, termed the narrow channel [29,30]. After a distance that varies depending on the bullet design, the bullet becomes destabilized because of the action of the retarding force. Since the latter tends to concentrate on the bullet’s forepart, it generates an overturning moment which prompts the bullet to yaw [31]. Yaw is the deviation of the bullet’s longitudinal axis from its line of trajectory [18]. Since modern rifle bullets have a streamlined (“spitzer”) shape, any such change in their orientation can only increase their presented area which also increases the magnitude of the retarding force by a positive feedback mechanism [31] (Figure 2).
A tendency to yaw, which is a feature of military rifle bullets, while already existing in air, is effectively counteracted there by the gyroscopic stabilization of the spin (imparted to the bullet by the rifling of the bore of the gun). In tissue, however, this stabilization is rapidly overcome because of the higher density of the medium and the enormous retarding forces [18,27]. Consequently, tumbling (rapid yaw) of the bullet appears as a result of which the diameter of the wound channel increases until it becomes maximum once the bullet travels sideways (at 90 degrees of yaw). At this point, the bullet strikes tissue with its whole length thus maximizing the damage produced [27] while the amount of energy transferred to tissue also reaches its maximum [14,18,32]. Such a bullet will eventually turn base-forward, which, of course, implies a sufficient length of the wound channel [18,27].
Expanding projectiles sustain deformation (mushrooming) of their nose under the pressure of the impact. This provides shoulder stabilization to the projectile preventing yaw and tumbling [30]. An expanding bullet, which mushrooms within 2 to 4 cm after penetration (i.e., without formation of a narrow channel) [30], may increase the wound diameter by 2.5 times. As a result, the surface area of the tissue that sustains direct damage from crushing and tearing by the projectile frontal area theoretically increases approximately 6.25 times [27]. However, this increase in wound diameter becomes clinically significant only with rifle bullets [18].
Bullet fragmentation is common as a result of bone impact while it also occurs with expanding rifle bullets containing a lead core as they penetrate soft tissue [18,33,34]. A different pattern of breakup, also without a bone hit, affects military rifle bullets with a lead core. Above a certain velocity, approximately at 600 m/s, the extreme bending and compressive stresses encountered while the tumbling bullet moves sideways within soft tissue cause flattening of the jacket [30]. At still higher velocities, the bullet may even fracture, usually at the cannelure (the circumferential crimp on the jacket around which the cartridge case holds firmly the bullet in the unused ammunition) releasing metallic fragments within soft tissue [27]. This results in a snowstorm appearance of the wound in plain radiographs [18].
Depending on range and velocity, fragmentation is a common characteristic of the 5.56 mm bullet used in the M16 assault rifle; it is seen both with the projectile fired from the original M-193 cartridge which was developed for the Vietnam-era M16A1 rifle, and the NATO-standardized SS109/M-855 cartridge of the M16A2 rifle [18,27]. This small-caliber bullet essentially relies on fragmentation to bring about its excessive destructive effect on tissue creating large wounds, as a result of which there have been press releases and medical reports falsely claiming that because of its high muzzle velocity (exceeding 900 m/s) it blows up in the body [18]. However, fragmentation of this bullet does not occur consistently since it is velocity-dependent requiring a penetration velocity above 760 m/s [35]. In addition, it entails tumbling of the bullet which requires a sufficient width of tissue while in borderline cases pre-impact yaw has a critical role in reducing the length of the narrow channel and precipitating early tumbling [30,36].
2.2. Pathophysiology of Bullet Wounds and Cavitation Injuries
The nature and severity of bullet injuries depends primarily on anatomic factors related to the shot placement and the bullet trajectory [37,38,39] and the functional effects resulting from the anatomic structures and organs disrupted [40,41] (Figure 3). Projectile characteristics, some of them inherent (mass, contour and construction) and other developing during the passage from the gun barrel (velocity, stability), also play a role as wounding factors [27]. According to some experts [27], the caliber of the projectile, i.e., its diameter (expressed either as fraction of an inch or in millimeters), is not an important determinant of the wounding effect. However, a relationship of larger bullet calibers with morbidity and mortality in gunshot victims has been reported [42,43].
The most common cause of death in victims of shooting incidents is hemorrhage [10,44,45]. Gunshot wounds to the head may be compatible with survival depending on the bullet trajectory [8,40], although in case of involvement of the brainstem, death ensues instantaneously [45]. A recent review of combat injuries in view of the war in Ukraine published in German, identified severe traumatic brain injury (TBI) and hemorrhage from injuries to the chest and abdomen as the main causes of primary mortality whereas secondary mortality after surgical intervention resulted from injuries to the trunk, neck and TBI [46]. Among civilians, gunshot wounds to the head and neck are the most serious representing more than half of the fatal cases [43].
Two basic components of tissue damage have been recognized in bullet wounds [14,27,29,47]: the permanent wound channel which is the area of overt tissue destruction after the bullet has exited the body or come to rest within it, and the temporary cavity that forms in the wake of the bullet invisible to the naked eye. Ballistic trauma from low-velocity projectiles (e.g., handguns) almost exclusively involves the direct mechanism of crushing and laceration. As a result, in order to cause significant injury to a structure, a handgun bullet must penetrate that structure. High-velocity bullets possess enough energy to cause additional damage through cavitation and possibly secondary injury due to bullet fragmentation [18,28].
Cavitation occurs as the bullet track expands with its walls thrust outwards, at velocities that reach up to one tenth that of the projectile from the deposition of its kinetic energy (Figure 4). The cavity created by this phenomenon involves massive tissue displacement increasing in size several times the projectile diameter within milliseconds after the projectile has left the body [48,49]. In sufficiently elastic tissue, the cavity after some undulation collapses undergoing a violent implosion, thus demonstrating both its temporary character and the highly dynamic nature of this phenomenon [32,36,48].
The degree of tissue damage from cavitation depends on the type and properties of the tissue(s) perforated by the bullet [18]. These properties also affect the projectile-tissue interaction which has a central role in the wounding process [48]. Cavity expansion results in tensile injury [36,50], consisting in a stretch mechanism of the temporary cavity [8]. In solid inelastic parenchymatous organs, such as the liver, this mechanism causes extensive disruption [14,48,51]. Significant lesser damage occurs to the lungs, because of the compliance and low density of the lung parenchyma [14,51,52], often presenting as extensive pulmonary contusion in radiographs [5]. Skeletal muscle is believed to undergo mostly reversible injury from the stretch mechanism due to its elasticity [26]. Indirect injury to internal organs, lying at a distance of several cm from the path of the projectile, can occur from the pressure waves associated with cavitation, often referred to as “blast injury” [53,54,55].
In head injuries, formation of a temporary cavity is an important cause of the ensuing pathology since even low-velocity FMJ handgun bullets create a significant cavitation effect. Pressure waves reaching 644 kPa in experimental head models are most likely associated with the collapse of the temporary cavity [56]. Remote effects of cavitation commonly manifest as indirect fractures of the thin orbital plates and the cranial base [30]. A zone of destruction of brain tissue around the wound channel extends up to 18 mm, which when affecting the brain stem can account for the onset of respiratory arrest leading to death [57]. Military rifle bullets penetrating the head produce extreme pressures amplified due the unyielding brain case, which exceed 2760 kPa resulting in explosive fractures of the calvarium from within [29].
2.3. High Energy Injuries
High energy bullet wounds are characterized by tissue damage extending peripheral to the wound track as a result of the temporary cavity formation following penetration by a high-velocity projectile [58]. The size of the temporary cavity is directly related to the projectile energy transferred to the tissue [18]. Clinically significant cavitation is a predominant manifestation of high energy transfer resulting in a “zone of injury”, often extensive, surrounding the wound channel [22]. Due to the extensive rupture of small blood vessels from the stretching effect of the expanding temporary cavity, the zone of injury has the appearance of bruised discolored muscle [29]. Within this zone, a pattern of progressive necrosis is encountered, which is not obvious during the initial examination [59,60,61]. This evolving process has been reported in experimental animals too, sometimes even after formal debridement [62,63,64], Extensive endothelial trauma affecting the microcirculation beyond the limits of obvious tissue damage, which is proportional to the energy transferred, appears to be a critical event in the underlying pathology [48,65,66].
In the absence of gross infection or vascular impairment, whether muscle necrosis occurs other than at a microscopic level, has been a matter of debate [28]. The different response of muscle to cavitation in various experimental studies may be related to the animal species used [58] and the underlying patterns of involvement of vascular territories in the muscle tissue [67]. The temporary cavity also creates a strong suction effect forcing air and debris to enter the wound [68]. The wound demonstrating a large amount of dead and ischemic non-viable tissue contaminated with foreign material represents the unique pathology of the high energy gunshot injury [29].
Assault rifle bullets possess significant less kinetic energy than those from full-powered military cartridges (e.g., 1693 Joules for the 5.56 mm NATO vs. 3272 Joules for the full-powered 7.62 mm NATO). However, assault rifle bullets are particularly effective in energy transfer because of their tendency for tumbling and possibly fragmentation during tissue penetration, and also because of a greater degree of cavitation injury due to the large temporary cavities they create (Figure 5).
As a result, gunshot wounds from high-velocity projectiles have a longer wound track potentially penetrating through multiple anatomic parts, with a wider zone of injury around it, compared to wounds produced by lower velocity bullets [69]. A deforming or disintegrating bullet from a powerful handgun is also capable of producing high energy effects to the wound with a large temporary cavity [58,70]; a large handgun bullet may produce a similar effect because of a bone hit (Figure 6).
A large exit wound is always a sign of high energy transfer [15,58]. In the case of a non-deforming military-type rifle bullet, it results from expansion of a large temporary cavity near the point of exit associated with bullet tumbling or breakup, or expulsion of bone fragments acting as secondary projectiles [35,64,71,72]. This is more likely to occur with wounds of the torso involving a long wound track [73]. However, a small exit hole from a tumbling bullet that has eventually turned 180 degrees leaving the body base-forward may conceal extensive injury in a deeper layer from high energy transfer [28,29].
Bullet fragmentation in soft tissue can be regarded as the most extreme manifestation of high energy transfer by high-velocity projectiles, consistently associated with greater tissue destruction [72,74]. The fragments created from a high-velocity bullet often have not sufficient energy to exit the target [21,75]. The resultant tissue damage involves a combination effect with cavitation, as the fragments create secondary wound channels extending radially from the main wound track, and the subsequent stretch mechanism causes more extensive disruption of this damaged tissue than what would be expected by this mechanism alone [33,75].
Gunshot wounds of the extremities are often complicated with vascular trauma. The latter may be an indirect injury as a result of the temporary cavity [76]. A large temporary cavity can cause arterial trauma or compartment syndrome, resulting in ischemic necrosis and infection [25,77]. Gunshot injuries sustained in combat have shown an increased rate of vascular injury [78], amounting to 26% and 33% in the wars in Iraq and Afghanistan respectively [79]. When compared to the much lower rates of vascular injury reported among civilian cases (commonly resulting from low-velocity projectiles), which is less than 10% [60,80], these figures suggest a link between vascular damage and cavitation in the context of high energy trauma. The mechanism of injury most commonly involves stretching of the vessel wall resulting in intimal tears and thrombosis; however, avulsive vascular injuries may also occur [81]. Neurologic deficits of different degree may also be encountered in extremity wounds, either indirectly from the severe stretch produced by cavitation or from direct laceration or contusion by the projectile [82,83].
2.4. Shotgun Injuries
Shotguns are smooth-bored (nonrifled) long-rifle firearms, which fire either multiple pellets collectively known as the shot or a single projectile (slug). Pellets are separated by size into two general categories, birdshot (of smaller diameter used for birds and small game) and buckshot (for large game) [84]. Lead pellets have an upper limit of velocity, approximately 420 m/s, above which collisions between individual pellets cause deformation whereas for steel pellets this is not a limiting factor and higher velocities can be attained [18]. In many areas, including the European union and the United States, lead shot has been banned for game hunting in wetlands because of lead poisoning of waterbirds [84]. Upon discharge, the pellet spread (“pattern”) attains a conical shape [77] and the wad, usually a plastic insert isolating the shot from the propellant within the shotgun cartridge, is also expelled from the muzzle [18,84]. As a result, the firing range from muzzle to target is the primary determinant of the wound morphology [18,85]; it affects not only the number of pellets that hit the target but also the density of the shot pattern.
Within close distances (<3 m), the pellets are still bunched together acting as a single projectile, with their initial velocity virtually unchanged [27]. At such range, the shotgun is a formidable weapon [18] and the resultant wound involves massive tissue destruction [75,85,86,87]. Up to a certain point, the size of the wound increases with range [8]. The wound appearance is determined by the gauge (caliber) of the shotgun and the choke, a constriction of the barrel at the muzzle which controls the diameter of the shot pattern. The gauge influences the density of the pattern, depending on which the wound either consists in a single large cavity or contains multiple wound channels from individual pellets. The size of the wound, however, is affected by the diameter of the pattern, which is governed by the degree of choke [88]. With increasing distances within a range of 1-3 m, the wound margins appear increasingly more scalloped and ragged, reflecting the gradual divergence of pellets at the periphery of the shot, until smaller wounds from individual pellets congregate surrounding the main wound of entry [9,18]. The wad can also reach the target over relatively short distances, and within approximately 2 m, for as long as the whole shot enters the body through a single wound, the wad should be expected to be found within the wound as radiolucent foreign body [9,88]; however, it does not participate in wounding beyond distances of 5-7 m [84]. Because of the unfavorable ballistic shape of pellets, their velocity drops rapidly [18] and beyond 6 m, due to the resultant loss in their kinetic energy, they tend to cause limited tissue damage [87].
Shotgun slugs have muzzle velocities ranging approximately between 400 and 560 m/s. They are heavy projectiles made of lead or copper alloys, which within their effective range of 100 m produce extensive internal injury, demonstrating extreme shocking effect, due to rapid delivery of their kinetic energy to the target. Energy transfer to the wound is achieved because of the blunt shape of the slug associated with marked cavitation and the tendency of lead slugs to flatten or breakup [10,89]. By contrast, cavitation has no significant role in injuries from shotgun pellets [18].
2.5. Bone Injuries
Bone is significantly denser and harder than the surrounding soft tissue, also demonstrating very limited elasticity. These characteristics result in greater amounts of energy transfer following bone hit by a projectile, which sustains early destabilization with temporary cavity formation and possibly breakup [8,58]. The bone at high impact velocities (>551 m/s) demonstrates behavior of a brittle material [90,91]. Depending on the velocity of the projectile, provided that its energy suffices for complete perforation of bone, the energy transfer initially results in drill-hole fractures demonstrating a conoidal defect with the exit hole larger than the entry (beveling), while at higher velocities greater bone fragmentation occurs as radiating fractures appear propagating outwards from the point of impact [91,92]. Fractures of long bones of the extremities from low-velocity bullets demonstrate rather typical fracture lines, such as divot fractures of the cortex, drill-hole fractures in the metaphyseal area, and the so-called butterfly and double butterfly fractures of the diaphysis, with various degrees of fragmentation around the exit hole [93,94]. Diaphyseal gunshot wounding of the human femur by a 9 mm FMJ bullet at an impact velocity of 360 m/s has been shown to produce a similar ballistic fracture pattern with a round entry hole surrounded by radiating and concentric fractures lines resulting in comminution and frequently a square exit bone defect [95].
Bone comminution by projectiles smaller in diameter than the bone is mainly produced by the hydrodynamic phenomena associated with cavitation within the bone marrow [30,95]. Rifle bullets as well as those from larger and more powerful handguns, which are capable of higher energy transfer, tend to produce fractures of an explosive character with severe comminution, as a result of the temporary cavity they induce [70]. The diameter of the projectile is more important than its mass regarding the bone damage produced at higher velocities, because of the greater energy transfer and the associated temporary cavity resulting from the presented area of larger projectiles [96]. Because of the associated soft tissue damage and disruption of the blood supply, these fractures are often complicated with infection, delayed union or nonunion [27].
Indirect fractures, i.e., without physical contact of the fracture site with the projectile, can be seen in high energy injuries due to the pressure wave from cavitation. These fractures, which can occur probably within a distance of 3 cm from the projectile trajectory, characteristically are linear or have a wedged shape. This is caused as the expansion of the temporary cavity bends the bone beyond its tensile strength, which results in tension failure of the cortex on the opposite side [97].
2.6. Infectious Potential of Gunshot Wounds
Bacterial colonization of gunshot wounds mainly occurs from the skin flora and clothing. The bullet transports microorganisms and textile fibers into the tissue while the suction effect of the temporary cavity causes additional contamination [30,98,99]. Debris is also present on the bullet surface, which is not self-sterilized from the temperature developing during its passage through the barrel [8,30]. Abdominal wounds may become heavily contaminated by spillage of fecal content and colonic injuries are associated with increased incidence of infectious complications [100] which are more common in high energy gunshot wounds [101]. As a result, gunshot wounds are considered prone to infection, with wound infection rates around 15%, whereas high energy wounds appear to carry a greater risk because of the large amount of devitalized tissue present [7].
3. Initial Evaluation of Gunshot Injuries
In case of a gunshot incident, information that should be sought from emergency medicine service (EMS) providers includes the victim’s approximate position at the time of wounding, which can help in assessment of the bullet trajectory, and the distance of shooting, particularly in the case of a shotgun wound. Any available information about the weapon type (handgun, rifle, or shotgun) and caliber can also be helpful for the initial appraisal of the character of the wound, its extent and length [22].
3.1. General Principles
Evaluation and initial management of patients with gunshot injuries should generally follow the Advanced Trauma Life Support (ATLS) guidelines [102,103]. Since most preventable deaths from penetrating injuries are due to exsanguinating hemorrhage, the traditional mnemonic acronym of initial trauma assessment A-B-C-D-E (Airway, Breathing, Circulation, Disability, Exposure) has been modified for gunshot victims as C-A-B (Circulation, Airway, Breathing) [75,104,105,106]. This paradigm shift reflects the priority currently given to the early control of catastrophic hemorrhage in exsanguinating penetrating trauma [107,108], along with attempts to restore impaired or failing vital functions [41]. The priority placed on hemorrhage control applies both in the prehospital setting and in the Emergency Department (ED), despite the potentially different techniques employed in each case [109]. For severe bleeding involving the limbs, prehospital proper application of arterial tourniquet is recommended [75,105,106]. Subsequently, hemodynamically stable patients may proceed with diagnostic imaging for triage of the severity of gunshot injuries whereas hypotensive patients require immediate surgical intervention [55,110,111].
Gunshot wounds to the head carry a high mortality rate and their treatment requires consultation with a neurosurgeon following stabilization of the patient [41,77]. These injuries are characterized by additional damage due to bone fragments in-driven from the entry site. Low-velocity bullets penetrating the head occasionally ricochet intracranially [112,113], whereas rifle bullets cause extensive brain injury to the brain because of the large amount of energy transferred via cavitation [112,114,115], which may also affect the cerebral vasculature [116].
In chest injuries, consultation with a trauma surgeon is required and tube thoracostomy should be instituted with a low diagnostic threshold [41,77]. Triage of life-threatening chest injuries should prioritize patients with airway compromise, pericardial tamponade, tension pneumothorax, and massive hemothorax, all of which can be rapidly fatal thus necessitating immediate action without delay for confirmatory investigations [52,117]. Based on autopsy reports, tension pneumothorax appears to be a common cause of potentially preventable death among fatalities in mass shooting incidents [118]. Therefore, both emergency physicians and EMS pesronnel should quickly assess gunshot victims for possible pneumothorax, which is amenable to pleural decompression through needle or tube thoracostomy [75,105].
Abdominal gunshot wounds usually require exploratory laparotomy, even when the wounded presents with stable vital signs, because of the possibility of extensive intra-abdominal damage secondary to cavitation [75,77,119,120]. Early recognition of vascular injury is crucial, greatly facilitated by the increasing use of computed tomographic angiography (CTA) [121]. Thoracic wounds, particularly those below the fourth rib, or abdominal wounds, especially by high-velocity projectiles, should raise suspicion of thoracoabdominal injury traversing the diaphragm [50,75,122,123].
Gunshot wounds to the extremities, in addition to fracture of long bones, may cause neurovascular injury [13,75,77,103]. Simple gunshot fractures can be treated conservatively, whereas those involving high energy transfer need operational management with external fixation for fracture stabilization, especially in lower extremity fractures [124,125]. Antibiotics are generally recommended despite lack of evidence supporting their routine administration for gunshot fractures [7,103,125,126].
3.2. Trajectory Analysis and Imaging
As with all types of penetrating trauma, identification of internal organs at risk from the course of the penetrating projectile is imperative in order to avoid missing injury to a critical structure that may lead to rapid decompensation of the patient [127]. Radiographic assessment is essential for determining the bullet path and the organs and anatomic formations affected, and for locating any retained bullet or fragments [87]. Trajectory delineation can be accomplished using radiopaque pointers of skin wounds, such as paperclips or BBs (these can cause confusion in cases with shotgun pellet injuries) before obtaining a plain X-ray or a computed tomography (CT) scan. The line connecting markers of paired (entry-exit) wounds or the marker of a penetrating (entry) wound with a retained bullet (in the case of an uneven number of markers), indicates the anatomic structures lying in the bullet path that should be assumed to be injured [5,119,127]. While correct matching of entry and exit wounds is obviously important, as is description and documentation of each one in detail, speculation about which is which based on inspection should be avoided [75,77] unless there is unequivocal evidence from gunpowder deposits or muzzle imprint indicating the entrance side [22,128] (Figure 6a).
Plain radiographs are usually the initial or sole imaging study used for the assessment of gunshot wounds [5]. Localization of a retained bullet should be made by obtaining two orthogonal views [5,27,129] a principle established during the Greco-Turkish war of 1897 [130], when radiographic investigation of bullet wounds was employed for the first time near the frontline [131]. CT is useful for detection and localization of bullets, especially the scout CT images which provide a better overview of the wounded part [5]. When radiographic trajectory analysis cannot locate a bullet within the estimated area of wounding and there is no exit wound, migration of the bullet should be considered and additional radiographs are required [27]. Ultrasound or fluoroscopy can be used to detect the current location of such a bullet, a necessary precaution when surgical removal is planned [7].
Bullet migration occurs either by gravity or by embolization through the venous or arterial bloodstream. Bullets within serous cavities, such as the pleural and peritoneal cavities, or in the subarachnoid space can move to a dependent location because of gravity [7,27,132]. Anecdotal cases of bullet fragments in the head migrating as early as 36 hours post-injury have been attributed to the difference between the respective specific gravities of metal and brain facilitated by the presence of damaged cerebral tissue in proximity to the bullet [133]. Bullet migration by the force of gravity through uninjured brain tissue has also been reported [134].
The bullet path may not be straight with projectiles travelling at lower velocities, which are more likely to be deflected off bony surfaces or strong facial layers [5,22,27]. The wound trajectory is primarily influenced by the posture of the victim and an an unusual bodily position at the moment of shooting can result in a strange or “inexplicable” erratic projectile path [28,38]. In mass shootings and terrorist attacks, there is penetration of multiple targets by single projectiles, with ricochet and bullet disintegration [44].
There are three clinical scenarios in which accurate delineation of the bullet trajectory is of critical importance. In head injuries, while the level of consciousness, estimated by the Glascow Coma Scale (GCS) score on admission, clinically remains a reliable predictor of long-term outcome, the wound trajectory, demonstrated in head CT scan, is the strongest prognostic factor of survival [114,135]. Deep bihemispheric and transventricular trajectories as well as those demonstrating multilobar or posterior fossa involvement are associated with high mortality rates [115,136,137,138].
Assessment of bullet trajectory is also important in neck wounds, because of the associated risk of vascular, neurologic and upper aerodigestive tract injury [38,127,139,140], with additional damage potentially caused by cavitation [141]. Traditionally, anatomical division of the neck into three zones (I-III, from the chest up) has been used to determine the decision for surgical exploration in hemodynamically stable patients based on the level of the entry wound and the estimated possibility of involvement of deeper structures [142]. However, bullet trajectories are difficult to assess clinically, even within the limited anatomical boundaries of the neck, whereas nearly half of gunshot wounds to the neck extend to multiple zones [143]. Currently, the availability of CTA has allowed a more selective approach to these patients, in the absence of hard signs of vascular trauma, such as expanding hematoma, absent carotid pulse and carotid bruit, which mandate exploration regardless of the zone of injury [140]. Other indications for surgery (with immediate airway control) include signs of obvious or imminent airway compromise (e.g., stridor), massive subcutaneous emphysema, as well as positive diagnostic studies for laryngotracheal or esophageal injury [140,141,144].
The third clinical situation necessitating determination of the wound trajectory is a possible transmediastinal chest wound. A trajectory through the mediastinum should be suspected when there is an exit wound in the thoracic cavity opposite to the entry wound, when the bullet is found located in the thorax on the opposite side from its point of entry or in close proximity to the mediastinal space, or when the patient has sustained multiple gunshot wounds to the chest [145]. The possibility of cardiac injury should also be considered in cases with precordial or epigastric entry wounds [38]. Patients with such injuries who arrive at the emergency department (ED) pulseless or progress to cardiac arrest are candidates for resuscitative ED thoracotomy [52,145,146,147]. Hemodynamically stable patients require evaluation of the vital structures contained in the mediastinum (heart, aorta, trachea as well as esophagus) [77] and CTA of the chest is the imaging study of choice for the diagnosis of a transmediastinal bullet wound in these patients [145].
Shotgun wounds do not contain a single wound track that can be visualized on CT scans and surgically explored. Thus, they represent especially challenging situations during the initial management [36]. Because of the presence of multiple pellets in the wound, they are often complicated with numerous potential sites of vascular injury, which requires CTA for proper diagnosis. Embolization of small pellets through venous channels to the heart or causing occlusion of an artery is a serious complication that may occur as a delayed effect of these injuries [148].
3.3. Vascular Injury of the Extremities
Investigation of suspected vascular trauma is an integral part of the management of gunshot wounds in the extremities since vascular injuries often pose life- or limb-threatening conditions [13,149]. “Hard signs” providing strong evidence of vascular injury which necessitates immediate surgical exploration include active hemorrhage, expanding or pulsating hematoma, loss of distal pulses, and palpable thrill or audible bruit [103,144,150,151,152,153]. However, in patients with multilevel trauma to an extremity, e.g., from multiple gunshot wounds or shotgun injury, making uncertain the exact location of the vascular damage, diagnostic imaging may be required prior to surgery [151,152].
In the absence of hard signs, a history of significant hemorrhage, proximity of the injury site to major vessels, bruising or small stable hematoma, diminished distal pulses, and the presence of neurologic deficit (from injury to an anatomical related nerve) represent soft signs of possible vascular injury [103,151]. These prompt vascular workup, usually by means of arterial pressure indices (API)—with the exception of hemodynamically unstable patients who should also be transported to the operating room [151,153]. CTA, which is currently the gold standard for imaging of extremity vascular injury [148,152,154], can usually be reserved for patients with a pathologic API measurement (<0.9) [151,153,155,156]. When no other signs of vascular injury are detected, a history of high energy trauma represents an independent indication for investigation [151].
An updated approach [157] suggested clinical evaluation of extremity vascular injury on the basis of hemorrhagic and ischemic presenting signs. Hemorrhagic signs (active/history of significant hemorrhage, systemic hypotension, pulsatile mass/palpable thrill in proximity to the injury site, expanding hematoma) usually predominate in penetrating trauma and their presence may indicate a potentially life-threatening hemorrhage; ischemic signs (diminished pulse, abnormal API, cool limb, pallor or impaired motor or sensory nerve function distal to the injury site) more likely appear from blunt trauma suggesting more extensive vascular pathology [157,158]. Vascular injury presenting with ischemic signs may be the result of cavitation. Patients with ischemic signs can also benefit from CTA, as it is critical for preoperative planning [159].
3.4. Debridement of Soft Tissue Gunshot Wounds
Soft tissue gunshot wounds produced by conventional low-velocity bullets and those from high-velocity ones limited to the narrow channel may be considered “low energy” injuries and treated conservatively as they are amenable to simple wound excision and irrigation [147,160,161]. These wounds are characterized by entry and exit holes smaller than 1 cm, connected by a short, narrow channel-type wound track, without any appreciable internal cavity or evidence of bullet fragmentation [160]. In the absence of fracture, the risk of wound infection appears to be low in these injuries [147], although administration of prophylactic antibiotics is generally recommended [161]. Tetanus prophylaxis is given as indicated [147].
High energy injuries require debridement and antibiotic coverage because of the extensive contamination along the wound track and the subsequent necrosis. In view of this necrotic tendency, surgical exploration and debridement may be planned as a serial procedure repeated every 24-48 hours until the wound bed appears healthy [161,162] or performed in one stage with the aim to remove all necrotic and ischemic non-viable muscle tissue at once sparing operating time and resources when these are limited [163]. Traditionally, intraoperative estimation of muscle tissue viability is empirically based on the “4 C’s” classic criteria of color, consistency, contractility, and capillary bleeding [124,160]. These indicators used by inexperienced clinicians may lead to unnecessary excision of potentially survivable tissue as they have been reported to correlate poorly with the microscopic appearance of excised muscle [164]. It should be noted, however, that necrotic muscle fibers my appear “normal” by light microscopy several days post-injury due to the delayed phagocytic response as a result of devascularization [165].
3.5. Removal of Retained Projectiles
Removal of asymptomatic retained bullets should not be attempted routinely, except in cases of direct accessibility, because wound exploration may cause further injury and result in significant blood loss. It is indicated when the bullet is located within or near a joint [5,7,124,147], or when there is concern about migration and damage to a nearby neurovascular structure [147]. Although the risk of lead poisoning is generally low, rarely this condition may result in chronic symptoms from various systems, such as anemia and neuropathy [5]. Bullets within a fracture site should preferably be removed as lead projectiles have been shown to inhibit ossification and their presence may result in nonunion [103].
4. Conclusions
A knowledge of wound ballistics provides a platform for understanding of the unique wounding mechanisms of penetrating projectiles, particularly the high-velocity ones. These are important considerations during interpretation of imaging data with clinical findings, since the presentation and the initial appearance of the wound usually do not reveal the full extent of the damage in deep structures. Identification of high energy gunshot injuries should also be supported by a background in ballistic characteristics of these wounds and their destructive potential, with clinical implications in cases involving vital organs or the vasculature. Recognition of the energy transfer effects in soft tissue wounds allows stratification of patients regarding the need for wound exploration and possibly more extensive or repeated debridement, and also the inherent risk for infectious complications. Wound ballistics, however, do not substitute for sound clinical judgement about cases that may be treated non-surgically or as outpatients on a selective basis and more serious injuries requiring life-preserving operations and extensive orthopedic procedures.
Author Contributions
Conceptualization, P.K.S., G.V., C.B., A.N. and G.M.; literature search: P.K.S., C.B., A.N., C.P. and S.S.; ballistic data curation: P.K.S. and N.E.T.; writing𑁋original draft preparation: P.K.S., C.B. and E.S.; writing𑁋review and editing: P.K.S., A.N., C.P., N.E.T., E.S., S.A. and D.G.; figure preparation: P.K.S., G.V., N.E.T. and S.A. All authors have read and agreed to the published version of the manuscript.
Funding
No external funding.
Acknowledgments
The first author wishes to thank Ms. Małgorzata (Gosia) Warmiñska-Marczak for kindly providing an inspection copy of the Textbook of Adult Emergency Medicine, Fifth edition, Elsevier, 2020, and a digital copy of the chapter on Hunting and fishing injuries of Auerbach’s Wilderness Medicine, Seventh edition, Elsevier, 2017.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Johns Hopkins Bloomberg School of Public Health. Firearm Violence in the United States. Available online: https://publichealth.jhu.edu/center-for-gun-violence-solutions/research-reports/gun-violence-in-the-united-states#:~:text=Evidence%20consistently%20shows%20that%20access%20to%20firearms%20increases%20the%20risk%20of%20suicide.&text=Access%20to%20a%20firearm%20in,suicide%20more%20than%20three%2Dfold.&text=Firearms%20are%20dangerous%20when%20someone,most%20lethal%20suicide%20attempt%20method (accessed on 1 July 2025).
- Centers for Disease Control and Prevention. Fast Facts: Firearm Injury and Death. July 5, 2024. Available online: https://www.cdc.gov/firearm-violence/data-research/facts-stats/index.html (accessed on 1 July 2025).
- Rozenfeld, M.; Givon, A.; Rivkind, A.; Bala, M.; Peleg, K.; Israeli Trauma Group (ITG). New trends in terrorism-related injury mechanisms: Is there a difference in injury severity? Ann Emerg Med 2019, 74, 697–705. [CrossRef]
- Binkley, J.M.; Kemp, K.M. Mobilization of resources and emergency response on the national scale. Surg Clin North Am 2022, 102, 169–180. [CrossRef]
- Ditkofsky, N.; Nair, J.R.; Frank, Y.; Mathur, S.; Nanda, B.; Moreland, R.; Rotman, J.A. Understanding ballistic injuries. Radiol Clin North Am 2023, 61, 119–128. [CrossRef]
- Ferreira, C.; Correia, M. Surgical frontiers in war zones: perspectives and challenges of a humanitarian surgeon in conflict environments. Trauma Surg Acute Care Open 2024, 9, e001234. [CrossRef]
- Baum, G.R.; Baum, J.T.; Hayward, D.; MacKay, B.J. Gunshot wounds: ballistics, pathology, and treatment recommendations, with a focus on retained bullets. Orthop Res Rev 2022, 14, 293–317. [CrossRef]
- Karger, B. Forensic ballistics: injuries from gunshots, explosives and arrows. In Handbook of Forensic Medicine, 2nd ed.; Madea, B., Ed.; Wiley: Chichester, West Sussex, UK, 2022; Volume 2, pp. 459–503. [CrossRef]
- Dries, D.J. Guns, bullets, and wounds. Air Med J 2023, 42, 80–85. [CrossRef]
- Stefanopoulos, P.K.; Tsiatis, N.E.; Herbstein, J.A. Gunshot wounds. In Encyclopedia of Forensic Sciences, 3rd ed.; Houck, M.M., Ed.; Elsevier: Oxford, UK, 2023, Volume 3, pp. 75–98. [CrossRef]
- dos Santos, L.M.P.; da Cunha, M.R.; Reis C.H.B.; Buchaim, D.V.; da Rosa, A.P.B.; Tempest, L.M.; da Cruz, J.A.P.; Buchaim, R.L.; Issa, J.P.M. The use of human surrogates in anatomical modeling for gunshot wounds simulations: an overview about “how to do” experimental terminal ballistics. Front Bioeng Biotechnol 2025, 13, 1536423. [CrossRef]
- Ragsdale, B.D. Gunshot wounds: a historical perspective. Mil Med 1984, 149, 301–315. [CrossRef]
- Bartlett, C.; Monier, B.; Wright, M.; Lesiak, A. Gunshot wounds to the extremity. In Encyclopedia of Trauma Care; Papadakos, P.J., Gestring, M.L., Eds.; Springer: Heidelberg, Germany, 2015; pp. 703–707. [CrossRef]
- Rhee, P.M.; Moore, E.E.; Joseph, B.; Tang, A.; Pandit, V.; Vercruysse, G. Gunshot wounds: A review of ballistics, bullets, weapons, and myths. J Trauma Acute Care Surg 2016, 80, 853–867. [CrossRef]
- DeMuth, W.E., Jr. Bullet velocity and design as determinants of wounding capability: an experimental study. J Trauma 1966, 6, 222–232.
- Bruner, D.; Gustafson, C.G.; Visintainer, C. Ballistic injuries in the emergency department. Emerg Med Pract 2011, 13, 1–32.
- Ommundsen, H.; Robinson, E.H. Rifles and Ammunition; Cassell: London, UK, 1915; Chapter 10: Sporting Rifle Ammunition, pp. 179–185.
- DiMaio, V.J.M. Gunshot Wounds: Practical Aspects of Firearms, Ballistics, and Forensic Techniques, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2016, ISBN 978-1-4987-2569-9.
- Kneubuehl, B.P. Wound ballistics and international agreements. In Wound Ballistics: Basics and Applications, 2nd ed.; Kneubuehl, B.P., Ed.; Springer: Berlin, Germany, 2022; pp. 337–358. [CrossRef]
- Anatoliyovych, I.L.; Yuriyovych, O.U.; Valentynovych, O.H. Surgical treatment features of liver gunshot wound with a dumdum bullet (expanding bullet). Int J Emerg Med 2022, 15, 57. [CrossRef]
- Gumeniuk, K.; Lurin, I.A.; Tsema, I.; Malynovska, L.; Gorobeiko, M.; Dinets, A. Gunshot injury to the colon by expanding bullets in combat patients wounded in hybrid period of the Russian-Ukrainian war during 2014-2020. BMC Surg 2023, 23, 23. [CrossRef]
- Bledsoe, B.E. Mechanism of injury. In Bledsoe’s Paramedic Care: Principles & Practice, 6th ed.; Bledsoe, B.E., Porter, R.S., Cherry, R.A., Eds.; Pearson: Upper Saddle River, New Jersey, USA, 2023; Volume 2, pp. 1757–1793, ISBN 978-013-691459-4.
- Walker, J. Halliday & Resnick Fundamentals of Physics, 12th ed.; Wiley: Hoboken, NJ, USA, 2022; Volume 1, Chapter 7: Kinetic energy and work, pp. 156–185, ISBN 978-1-119-80115-3.
- McAninch, J.W.; Santucci, R.A. Renal and ureteral trauma. In Campbell-Walsh Urology, 9th ed.; Kavoussi, L.R.; Novick, A.C.; Partin, A.W.; Peters, C.A., Eds.; Saunders: Philadelphia, PA, USA, 2007; Volume 2, pp. 1274–1292, ISBN 978-0-7216-0798-5.
- Burkhalter, W.E. Orthopedic Surgery in Vietnam; Office of the Surgeon General: Washington DC, USA, 1994.
- Fackler, M.L. Wound ballistics. A review of common misconceptions. JAMA 1988, 259, 2730–2736. [CrossRef]
- Hollerman, J.J.; Fackler, M.L. Wound ballistics. In Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed.; Tintinalli J.E., Ed.; McGraw-Hill: New York, NY, USA, 2011; pp. e38–e43, ISBN 978-0-07-148480-0.
- Mendelson, J.A. The relationship between mechanisms of wounding and principles of treatment of missile wounds. J Trauma 1991, 31, 1181–1202. [CrossRef]
- Owen-Smith, M.S. High-velocity and military gunshot wounds. In Management of Gunshot Wounds; Ordog, G.J., Ed.; Elsevier: New York, NY, USA, 1988; pp. 61–94, ISBN 0-444-01246-X.
- Kneubuehl, B.P. General wound ballistics. In Wound Ballistics: Basics and Applications, 2nd ed.; Kneubuehl, B.P., Ed.; Springer: Berlin, Germany, 2022; pp. 87–163. [CrossRef]
- Kneubuehl, B.P. Ballistics: Theory and Practice (Translated from the German language edition by Rawcliffe, S.); Springer: Berlin, Germany, 2024; Chapter 2: Physical basics, p. 34. [CrossRef]
- Janzon, B. Projectile-material interactions: simulants. In Scientific Foundations of Trauma; Cooper, G.J., Dudley, H.A.F., Gann, D.S., Little, R.A., Maynard, R.L., Eds.; Butterworth Heinemann: Oxford, UK, 1997; pp. 26–36, ISBN 0 7506 1585 0.
- Fackler, M.L.; Surinchak, J.S.; Malinowski, J.A.; Bowen, R.E. Bullet fragmentation: a major cause of tissue disruption. J Trauma 1984,24, 35-39.
- Berlin, R.H.; Janzon, B.; Lidén, E.; Nordström, G.; Schantz, B.; Seeman, T.; Westling, F. Terminal behaviour of deforming bullets. J Trauma 1988, 28, S58-S62. [CrossRef]
- Fackler, M.L. Wounding patterns of military rifle bullets. Int Defense Rev 1989, 22, 159–165.
- Stefanopoulos, P.K.; Mikros, G.; Pinialidis, D.E.; Oikonomakis, I.N.; Tsiatis, N.E.; Janzon, B. Wound ballistics of military rifle bullets: An update on controversial issues and associated misconceptions. J Trauma Acute Care Surg 2019, 87, 690–698. [CrossRef]
- MacPherson, D. Bullet Penetration: Modelling the Dynamics and the Incapacitation Resulting from Wound Trauma; Ballistic publications: El Segundo, CA, USA, 2005; Chapter 4: Incapacitation of bullet wounds, p. 52, ISBN 0-9643577-1-2.
- Reginelli, A.; Russo, A.; Maresca, D.; Martiniello, C.; Cappabianca, S.; Brunese, L. Imaging assessment of gunshot wounds. Semin Ultrasound CT MR 2015, 36, 57–57. [CrossRef]
- Altheimer, I.; Schaible, L.M.; Klofas, J.; Comeau, M. Victim characteristics, situational factors, and the lethality of urban gun violence. J Interpers Violence 2019,34, 1633-1656. [CrossRef]
- Moritz, A.R. The Pathology of Trauma, 2nd ed.; Lea & Febiger: Philadelphia, USA, 1954; p. 64.
- Riddez, L. Wounds of war in the civilian sector: principles of treatment and pitfalls to avoid. Eur J Trauma Emerg Surg 2014, 40, 461–468. [CrossRef]
- Ordog, G.J.; Prakash, A. Civilian gunshot wounds: determinants of injury. In Management of Gunshot Wounds; Ordog, G.J., Ed.; Elsevier: New York, NY, USA, 1988; pp. 157–165, ISBN 0-444-01246-X.
- Braga, A.A.; Cook, P.J. The association of firearm caliber with likelihood of death from gunshot injury in criminal assaults. JAMA Netw Open 2018, 1, e180833. [CrossRef]
- Tracqui, A.; Deguette, C., Delabarde, T.; Delannoy, Y.; Plu, I; Sec, I.; Hamza, L.; Taccoen, M.; Ludes, B. An overview of forensic operations performed following the terrorist attacks on November 13, 2015, in Paris. Forensic Sci Res 2020, 5, 202–207. [CrossRef]
- Spitz, W.U.; Diaz, F.J. Spitz and Fisher’s Medicolegal investigation of Death: Guidelines for the Application of Pathology to Crime Investigation, 5th ed.; Charles C. Thomas, Springfield, IL, USA, 2020; Chapter 8: Injury by gunfire, pp. 313–403, ISBN 9780398093129.
- Witzenhausen, M.; Brill, S.; Schmidt, R.; Beltzer, C. Aktuelle Mortalität von Kriegsverletzungen—eine narrative Übersichtsarbeit. Chirurgie, 2024, 95, 546–554. [CrossRef]
- DeMuth, W.E., Jr.; Smith, J.M. High-velocity bullet wounds of muscle and bone: the basis of rational early treatment. J Trauma 1966, 6, 744–755. [CrossRef]
- Amato, J.L.; Billy, L.J.; Lawson, N.S.; Rich, N.M. High velocity missile injury. An experimental study of the retentive forces of tissue. Am J Surg 1974, 127, 454–459. [CrossRef]
- Wen, Y.; Xu, C.; Jin, Y.; Batra, R.C. Rifle bullet penetration into ballistic gelatin. J Mech Behav Biomed Mater 2017, 67, 40–50. [CrossRef]
- Stefanopoulos, P.K.; Koutsouvela, D.G.; Panagiotopoulou, O.; Herbstein, J.; Tsiatis, N.; Mikros, G.; Pinialidis, D.E.; Salemis, N.S. Biomechanics of gunshot injuries and applications to wound ballistics research. In Forensic Analysis of Gunshot Residue, 3D-Printed Firearms, and Gunshot Injuries: Current Research and Future Perspectives; Cizdziel, J., Black, O., Eds.; Nova Science: New York, NY, USA, 2019; pp. 121–165, ISBN 978-1-53614-882-4.
- Fackler, M.L.; Surinchak, J.S.; Malinowski, J.A.; Bowen, R.E. Wounding potential of the Russian AK-74 assault rifle. J Trauma 1984, 24, 263–266. [CrossRef]
- Khandar, S.J.; Johnson, S.B.; Calhoon, J.H. Overview of thoracic trauma in the United States. Thorac Surg Clin 2007, 17, 1–9. [CrossRef]
- Karademir, K.; Gunhan, M.; Can, C. Effects of blast injury on kidneys in abdominal gunshot wounds. Urology 2006, 68, 1160–1163. [CrossRef]
- Owers, C.; Garner, J. Intra-abdominal injury from extra-peritoneal ballistic trauma. Injury, 2014, 45, 655–658. [CrossRef]
- Chai, L.F.; Nahass, M.M.; Iacono, S.A.; Grover, K.; Shan, Y.; Ferraro, J.; Ikegami, H.; Hanna, J.S. Delayed cardiac tamponade secondary to blast injury from gunshot wound. Trauma Case Rep 2023, 47, 100914. [CrossRef]
- Zhang, J.; Yoganandan, N.; Pintar, F.A.; Gennarelli, T.A. Temporal cavity and pressure distribution in a brain simulant following ballistic penetration. J Neurotrauma 2005, 22, 1335–1347. [CrossRef]
- Oehmichen, M.; Meissner, C.; König, H.G.; Gehl, H.B. Gunshot injuries to the head and brain caused by low-velocity handguns and rifles: A review. Forensic Sci Int 2004, 146, 111–120. [CrossRef]
- Janzon, B.; Hull, J.B.; Ryan, J.M. Projectile-material interactions: soft tissue and bone. In Scientific Foundations of Trauma; Cooper, G.J., Dudley, H.A.F., Gann, D.S., Little, R.A., Maynard, R.L., Eds.; Butterworth Heinemann: Oxford, UK, 1997; pp. 37–52, ISBN 0 7506 1585 0.
- Myerson, M.S.; Sammarco, V.J. Penetrating and lacerating injuries of the foot. Foot Ankle Clin 1999, 4, 647–672.
- Shin, E.H.; Sabino, J.M.; Nanos, G.P., III; Valerio, I.L. Ballistic trauma: Lessons learned from Iraq and Afghanistan. Semin Plast Surg 2015, 29, 10–19. [CrossRef]
- Adams M.H.; Gaviria, M.; Sabbag, C.M. Military ballistic injuries of the upper extremity. Hand Clin 2025, 41, 269–280. [CrossRef]
- Dahlgren, B.; Berlin, R.; Janzon, B.; Nordström, G.; Nylöf, U.; Rybeck, B.; Schantz, B.; Seeman, T. The extent of muscle tissue damage following missile trauma one six and twelve hours after the infliction of trauma, studied by the current method of debridement. Acta Chir Scand Suppl 1979, 489, 137–144.
- Wang, Z.G.; Feng, J.X.; Liu, Y.Q. Pathomorphological observations of gunshot wounds. Acta Chir Scand Suppl 1982, 508, 185–195.
- Fackler, M.L.; Breteau, J.P.; Courbil, L.J.; Taxit, R.; Glas, J.; Fievet, J.P. Open wound drainage versus wound excision in treating the modern assault rifle wound. Surgery 1989, 105, 576–584.
- Popov, V.A.; Vorob’ev, V.V.; Pitenin, I.Y. Microcirculatory changes in tissues surrounding a gunshot wounds. Bull Exp Biol Med 1990, 109, 437–441. [CrossRef]
- Vuong, P.N.; Berry, C. The Pathology of Vessels; Springer: Berlin, Germany, 2002; Chapter 6: Vascular trauma, pp. 119–137. [CrossRef]
- Le Gros Clark, W.E.; Blomfield, L.B. The efficiency of intramuscular anastomoses, with observations on the regeneration of devascularized muscle. J Anat 1945, 79, 15–32.
- Grosse Perdekamp, M.; Kneubuehl, B.P.; Serr, A.; Vennemann, B.; Pollak, S. Gunshot-related transport of micro-organisms from the skin of the entrance region into the bullet path. Int J Legal Med 2006, 120, 257–264. [CrossRef]
- Watson, J.D.B.; Tai, N.R.M.; Martin, M.J. Military vascular injuries; considerations and techniques. In Vascular Injury: Endovascular and Open Surgical Management; DuBose, J.J.; Teixeira, P.G., Rajani, R.R., Eds.; McGraw-Hill: New York, NY, USA, 2023; pp. 273–284. ISBN 978-1-26-426983-9.
- Ragsdale, B.D.; Josselson, A. Experimental gunshot fractures. J Trauma 1988, 28, S109–S115. [CrossRef]
- Wang, Z.G.; Qian, C.W.; Zhan, D.C.; Shi, T.Z.; Tang, C.G. Pathological changes of gunshot wounds at various intervals after wounding. Acta Chir Scand Suppl 1982, 508, 197–210.
- Penn-Barwell, J.G.; Sargeant, I.D.; Severe Lower Extremity Combat Trauma (SeLECT) Study Group. Gun-shot injuries in UK military casualties—Features associated with wound severity. Injury 2016, 47, 1067–1071. [CrossRef]
- Manta, A.M.; Petrasso, P.E.Y.; Tomassini, L.; Piras, G.N.; De Maio, A.; Cappelletti, S.; Straccamore, M.; Siodambro, C.; De Simone, S.; Peonim, V.; et al. The wounding potential of assault rifles: analysis of the dimensions of entrance and exit wounds and comparison with conventional handguns. A multicentric study. Forensic Sci Med Pathol 2024, 20, 896–909. [CrossRef]
- Jorgensen, J.J.; Naess, P.A.; Gaarder, C. Injuries caused by fragmenting rifle ammunition. Injury 2016, 47, 1951–1954. [CrossRef]
- Sanders, M.J.; McKenna, K.D. Sander’s Paramedic Textbook, 6th ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2025; ISBN 9781284264791.
- Ng, E.; Choong, A.M.T.L. External iliac artery injury secondary to indirect pressure wave effect from gunshot wound. Chin J Traumatol 2016, 19, 134–135. [CrossRef]
- Sanchez, L.D.; Ketterer, A.R. Gunshot attacks: mass casualties. In Ciottone’s Disaster Medicine, 3rd ed.; Ciottone, G.R., Ed.; Elsevier: Philadelphia, PA, USA, 2024; pp. 904–906. [CrossRef]
- Rasmussen, T.E.; Stannard, A. Injury to extremities. In Fischer’s Mastery of Surgery, 6th ed.; Fischer, J.E., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; pp. 2495–2504, ISBN 978-1-60831-740-0.
- White, J.M.; Stannard, A.; Burkhardt, G.E.; Eastridge, B.J.; Blackbourne, L.H.; Rasmussen, T.E. The epidemiology of vascular injury in the wars in Iraq and Afghanistan. Ann Surg 2011, 25, 1184–1189. [CrossRef]
- Tarkunde, Y.R.; Clohisy, C.J.; Calfee, R.P.; Halverson, S.J.; Wall, L.B. Firearm injuries to the wrist and hand in children and adults: an epidemiologic study. Hand (N Y) 2023,18, 575-581. [CrossRef]
- Rich, N.M.; Spencer, F.C. Vascular Trauma; Saunders: Philadelphia, PA, USA, 1978; Chapter 3: Experimental arterial trauma, pp. 44–60, ISBN 0-7216-7580-8.
- Straszewski, A.J.; Schultz, K.; Dickherber, J.L.; Dahm, J.S.; Wolf, J.M.; Strelzow, J.A. Gunshot-related upper extremity nerve injuries at a level 1 trauma center. J Hand Surg Am 2022, 47, 88.e1-88.e6. [CrossRef]
- McQuillan, T.J., 3rd; Zelenski, N.A. Ballistic injuries of the brachial plexus. Hand Clin 2025, 41, 351–359. [CrossRef]
- Otten, E.J. Hunting and fishing injuries. In Auerbach’s Wilderness Medicine, 7th ed.; Auerbach, P.S., Cushing, T.A.; Harris, N.S., Eds.; Elsevier: Philadelphia, PA, USA, 2017; Volume 1, pp. 549–563, ISBN 978-0-323-35942-9.
- Schmidt, A.; Wise, K.; Kelly, B. The physics of trauma. In PHTLS Prehospital Trauma Life Support, 10th ed.; Pollak, A.N., Ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2023; pp. 103–147, ISBN 9781284264746.
- Glezer, J.A.; Minard, G.; Croce, M.A.; Fabian, T.C.; Kudsk, K.A. Shotgun wounds to the abdomen. Am Surg 1993, 59, 129–132.
- Cestero, R.; Plurad, D.; Demetriades, D. Ballistics. In Color Atlas of Emergency Trauma, 3rd ed.; Demetriades, D., Chudnofsky C.R., Benjamin, E.R., Eds.; Cambridge University Press: Cambridge, UK, 2021; pp. 247–262. [CrossRef]
- Breitenecker, R. Shotgun wound patterns. Am J Clin Pathol 1969, 52, 258–269. [CrossRef]
- Gestring, M.L.; Geller, E.R.; Akkad, N.; Bongiovanni, P.J. Shotgun slug injuries: case report and literature review. J Trauma 1996, 40, 650–653. [CrossRef]
- Zhu, F.; Saif, T.; Presley, BR.; Yang, K.H. The mechanical behaviour of biological tissues at high strain rates. In Military Injury Biomechanics: The Cause and Prevention of impact Injuries; Franklyn, M., Vee Sin Lee, P., Eds.; CRC Press: Boca Raton, FL, USA, 2017; pp. 103–118, ISBN 978-1-4987-4282-5.
- Caister, A.J.; Carr, D.J.; Campbell, P.D.; Brock, F.; Breeze, J. The ballistic performance of bone when impacted by fragments. Int J Legal Med, 2020, 134, 1387–1393. [CrossRef]
- Pandey, P. K.; Joshi, Y.K.; Ganpule, S.G. Review of interaction of bullets and fragments with skin-bone-muscle parenchyma. ASME J of Medical Diagnostics 2025, 8, 040801. [CrossRef]
- Smith, H.W.; Wheatley, K.K. Biomechanics of femur fractures secondary to gunshot wounds. J Trauma 1984, 24, 970–977. [CrossRef]
- Rose, S.C.; Fujisaki, K.; Moore, E.E. Incomplete fractures associated with penetrating trauma: etiology, appearance and natural history. J Trauma 1988, 28, 106–109. [CrossRef]
- Schwab, N.; Jordana, X.; Monreal, J.; Garrido, X.; Soler, J.; Vega, M.; Brillas, P.; Galtés, I. Ballistic long bone fracture pattern: an experimental study. Int J Legal Med 2024, 138, 1685–1700. [CrossRef]
- Harger, J.H.; Huelke, D.F. Femoral fractures produced by projectiles𑁋the effects of mass and diameter on target damage. J Biomech 1970, 3, 487–493. [CrossRef]
- Kieser, D.C.; Carr, D.J.; Leclair, S.C.J.; Horsfall, I.; Theis, J.C.; Swain, M.V.; Kieser, J.A. Gunshot induced indirect femoral fracture: mechanism of injury and fracture morphology. J R Army Med Corps 2013, 159, 294–299. [CrossRef]
- Tian, H.M.; Huang, M.J.; Liu, Y.Q.; Wang, Z.G. Primary bacterial contamination of wound track. Acta Chir Scand Suppl 1982, 508, 265–269.
- Hinz, B.J.; Muci-Küchler, K.H.; Smith, P.M. Distribution of bacterial in simplified surrogate extremities shot with small caliber projectiles. In Proceedings of the ASME 2013 International Mechanical Engineering Congress and Exposition (IMECE2013). Volume 3A: Biomedical and Biotechnology Engineering. San Diego, CA, USA, 15-21 November 2013; pp. 1–11. [CrossRef]
- Lazovic, R.; Radojevic, N.; Curovic, I. Performance of primary repair on colon injuries sustained from low- versus high-energy projectiles. J Forensic Leg Med 2016, 39, 125–129. [CrossRef]
- Jones, R.C. Surgical infections in trauma. In Infectious Diseases, 2nd ed.; Gorbach, S.L.; Bartlett, J.G.; Blacklow, N.R., Eds.; Saunders: Philadelphia, PA, USA, 1998; pp. 927–932, ISBN 0-7216-6119-X.
- Stewart, R.M. ATLS® Advanced Trauma Life Support® Student Course Manual, 10th ed.; American College of Surgeons: Chicago, IL, USA, 2018, ISBN 78-0-9968262-3-5.
- Lin, J.S.; Rhee, P.C. Wrist and forearm fractures from ballistic injuries. Hand Clin 2025, 41, 313–322. [CrossRef]
- Penn-Barwell, J.G.; Bennett, P.M.; Heil, K.M. Firearms, ballistics and gunshot wounds. In Trauma Care Manual, 3rd ed.; Greaves, I., Porter, K., Garner, J., Eds.; CRC Press: Boca Raton, FL, USA, 2022; pp. 372–385. [CrossRef]
- Pilbery, R.; Lethbridge, K. Ambulance Care Practice, 2nd ed.; Class Professional Publishing: Bridgwater, Somerset, UK, 2023 (reprint); Chapter 17: Trauma, pp. 311–371, ISBN 9-781859-598542.
- Ferrada, P.; Duschesne, J.; Piehl, M. Prioritizing circulation over airway in trauma patients with exsanguinating injuries: What you need to know. J Trauma Acute Care Surg 2025, online ahead of print. [CrossRef]
- Kuckelman, J.; Derickson, M.; Long, W.B.; Martin, M.J. MASCAL management from Baghdad to Boston: Top ten lessons learned from modern military and civilian MASCAL events. Curr Trauma Rep 2018, 4, 138–148. [CrossRef]
- Ferrada, P.; Dissanaike, S. Circulation first for the rapidly bleeding trauma patient𑁋It is time to reconsider the ABCs of trauma care. JAMA Surg 2023, 158, 884–885. [CrossRef]
- Gangidine, M.M.; Sorensen, D.M. Penetrating extremity trauma: Part I. Trauma Reports 2019, 20, 1–11.
- Martin, M.J.; Beekley, A.C.; Eckert, M.J. Front Line Surgery: A Practical Approach, 2nd ed.; Springer: Cham, Switzerland, 2017; Top Ten Combat Trauma Lessons, p. xxiii, ISBN 978-3-319-56780-8.
- Bohan, P.M.K.; Leonard, J.M.; Kaplan, L.J. A ‘Direct to operating room’ approach improves critically injured patient outcomes. Curr Opin Crit Care 2025, 31, online ahead of print. [CrossRef]
- Kim, P.E.; Go, J.L.; Zee, C.-S. Radiographic assessment of cranial gunshot wounds. Neuroimaging Clin North Am 2002, 12, 229–248. [CrossRef]
- Offiah, C.; Twigg, S. Imaging assessment of penetrating craniocerebral and spinal trauma. Clin Radiol 2009, 64, 1146–1157. [CrossRef]
- Cooper, P.R. Gunshot wounds to the brain. In Head injury, 3rd ed.; Cooper, P.R., Ed.; Williams & Wilkins: Baltimore, MD, USA, 1993; pp. 355–371, ISBN 0-683-02108-7.
- Rosenfeld, J.V.; Bell, R.S.; Armonda, R. Current concepts in penetrating and blast injury to the central nervous system. World J Surg 2015, 39, 1352–1362. [CrossRef]
- Dawoud, F.M.; Feldman, M.J.; Yengo-Kahn, A.M.; Roth, S.G.; Wolfson, D.I.; Ahluwalia, R.; Kelly, P.D.; Chitale, R.V. Traumatic cerebrovascular injuries associated with gunshot wounds to the head: a single-institution ten-year experience. World Neurosurg 2021, 146, e1031-e1044. [CrossRef]
- Boffard, K.D.; White, J.O. Manual of Definitive Surgical Trauma Care: Incorporating Definitive Anaesthetic Trauma Care, 6th ed.; CRC Press: Boca Raton, FL, USA, 2024, ISBN 9781032157818.
- Smith, E.R.; Sarani, B.; Shapiro, G.; Gondek, S.; Rivas, L.; Ju, T.; Robinson, B.Rh.; Estroff, J.M.; Fudenberg, J.; Amdur, R.; et al. Incidence and cause of potentially preventable death after civilian public mass shooting in the US. J Am Coll Surg 2019, 229, 244–251. [CrossRef]
- Pryor, J.P.; Reilly, P.M.; Dabrowski, G.P.; Grossman, M.D.; Schwab, C.W. Nonoperative management of abdominal gunshot wounds. Ann Emerg Med 2004, 43, 344–353. [CrossRef]
- Wilkes, G. Abdominal trauma. In Textbook of Adult Emergency Medicine, 5th ed.; Cameron, P., Little, M., Mitra, B., Deasy, C, Eds.; Elsevier: Oxford, UK, 2020; pp. 92–95, ISBN 978-0-7020-7624-4.
- Aylwin, C.; Jenkins, M. Abdominal aortic trauma, iliac and visceral vessel injuries. In Rich’s Vascular Trauma, 4th ed.; Rasmussen, T.E., Tai, N.R.M., Eds.; Elsevier: Philadelphia, PA, USA, 2022; pp. 212–225. [CrossRef]
- Hughes, R.K. Thoracic trauma. Ann Thorac Surg 1965, 1, 778–804. [CrossRef]
- Khomenko, I.; Tsema, I.; Humeniuk, K.; Makarov, H.; Rahushyn, D.; Yarynych, Y.; Sotnikov, A.; Slobodianyk, V.; Shypilov, S.; Dubenko, D.; et al. Application of damage control tactics and transpapillary biliary decompression for organ-preserving surgical management of liver injury in combat patient. Mil Med 2022, 187, e781-e786. [CrossRef]
- Persad, I.J.; Reddy, R.S.; Saunders, M.A.; Patel, J. Gunshot injuries to the extremities: experience of a U.K. trauma centre. Injury 2005, 36,407-411. [CrossRef]
- Laubscher, M.; Ferreira, N.; Birkholtz, F.F.; Graham, S.M.; Maqungo, S.; Held, M. Civilian gunshot injuries in orthopedics: a narrative review of ballistics, current concepts, and the South African experience. Eur J Orthop Surg Traumatol 2021, 31, 923–930. [CrossRef]
- Sathiyakumar, V.; Thakore, R.V.; Stinner, D.J.; Obremskey, W.T.; Ficke, J.R.; Sethi, M.K. Gunshot-induced fractures of the extremities: a review of antibiotic and debridement practices. Curr Rev Musculoskelet Med 2015, 8, 276–289. [CrossRef]
- Hynes, A.M. Finding the missing bullet: A case report of an unusual trajectory from the left scapula into the left orbit. Trauma Case Rep 2021, 35, 100530. [CrossRef]
- Failla, A.V.M.; Licciardello, G.; Cocimano, G.; Di Mauro, L.; Chisari, M.; Sessa, F.; Salerno, M.; Esposito, M. Diagnostic challenges in uncommon firearm injury cases: a multidisciplinary approach. Diagnostics 2025, 15, 31. [CrossRef]
- Squire, L.F.; Novelline, R.A. Fundamentals of Radiology, 4th ed.; Harvard University Press: Cambridge, MA, 1988; Chapter 2: The invitation to think three-dimensionally, p. 17, ISBN 0-674-32926-0.
- Abbott, F.C. Surgery in the Græco-Turkish war. Lancet 1899, 153, 80–83. [CrossRef]
- Reynolds, L. The history of the use of the roentgen ray in warfare. Am J Roentgenol Radium Ther 1945, 54, 649–672.
- Ledgerwood, A.M. The wandering bullet. Surg Clin North Am 1977, 57, 97–109. [CrossRef]
- Rapp, L.G.; Arce, C.A.; McKenzie, R.; Darmody, W.R.; Guyot, D.R.; Michael, D.B. Incidence of intracranial bullet fragment migration. Neurol Res 1999, 21, 475–480. [CrossRef]
- Leone, A.; Parsons, A.D.; Willis, S.; Moawad, S.A.; Zanzerkia, R.; Rahme, R. Sinking bullet syndrome: A unique case of transhemispheric migration. Clin Neurol Neurosurg 2021, 204, 106607. [CrossRef]
- Aarabi, B.; Eisenberg, H. Surgical management and prognosis of penetrating brain injury. In Youmans & Winn Neurological Surgery, 8th ed.; Winn, H.R., Ed.; Elsevier: Philadelphia, PA, USA, 2023; pp. 3092–3104, ISBN 978-0-323-66192-8.
- Part2: Prognosis in penetrating brain injury (no authors listed). J Trauma 2001, 51(2 Suppl), S44-S86.
- Kothari, S.; Zhang, B.; Darji, N.; Woo, J. Prognosis after moderate to severe traumatic brain injury: A practical, evidence-based approach. In Brain injury Medicine: Principles and Practice, 3rd ed.; Zasler, N.D., Katz, D.I., Zafonte, R.D., Eds.; Demos Medical: New York, NY, USA, 2022; pp. 248–270. [CrossRef]
- Zakrison, T.L.; Essig, R.; Polcari, A.; McKinley, W.; Arnold, D.; Beyene, R.; Wilson, K.; Rogers, S., Jr.; Matthews, J.B.; Millis, J.M.; et al. Review paper on penetrating brain injury: Ethical quandaries in the trauma bay and beyond. Ann Surg 2023, 277, 66–72. [CrossRef]
- Nemzek, W.R.; Hecht, S.T.; Donald, P.J.; McFall, R.A.; Poirier, V.C. Prediction of major vascular injury in patients with gunshot wounds to the neck. AJNR Am J Neuroradiol 1996, 17, 161–167.
- Bagheri, S.C.; Khan, H.A.; Bell, R.B. Penetrating neck injuries. Oral Maxillofac Surg Clin North Am 2008, 20, 393–414. [CrossRef]
- Majors, J.S.; Brennan, J.; Holt, G.R. Management of high-velocity injuries of the head and neck. Facial Plast Surg Clin North Am 2017, 25, 493–502. [CrossRef]
- Scott, B.G. Approach to penetrating injuries of the neck. In Head, Face, and Neck Trauma: Comprehensive Management; Stewart, M.G., Ed.; Thieme: New York, NY, USA, 2005; pp. 202–206, ISBN 1-58890-308-7.
- Bean, A.S. Trauma to the neck. In Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9th ed.; Tintinalli, J.E., Ed.; McGraw-Hill: New York, NY, USA, 2020; pp. 1722–1729, ISBN 978-1-260-01993-3.
- Evans, C.; Chaplin, T.; Zelt, D. Management of major vascular injuries: neck, extremities, and other things that bleed. Emerg Med Clin North Am 2018, 36, 181–202. [CrossRef]
- Zhao, F.Z.; Biffl, W.L. Thoracic trauma. In Textbook of Critical Care, 8th ed.; Vincent, J-L., Moore, F.A., Bellomo, R., Marini, J.J., Eds.; Elsevier: Oxford, UK, 2024; pp. 1255–1263, ISBN 978-0-323-75929-8.
- Demetriades, D.; Benjamin, E.R. Emergency room resuscitative thoracotomy. In Color Atlas of Emergency Trauma, 3rd ed.; Demetriades, D., Chudnofsky C.R., Benjamin, E.R., Eds.; Cambridge University Press: Cambridge, UK, 2021; pp. 328–334. [CrossRef]
- Clare, D.; Baxley, S. An evidence-based approach to managing gunshot wounds in the emergency department. Emerg Med Pract 2023, 25, 1–28.
- Raja, A.S. Peripheral vascular trauma. In Rosen’s Emergency Medicine: Concepts and Clinical Practice, 10th ed.; Walls, R.M., Ed.; Elsevier: Philadelphia, PA, USA, 2023; Volume 1, pp. 429–437, ISBN 978-0-323-75847-5.
- Kauvar, D.S.; Sarfati, M.R.; Kraiss, L.W. National trauma databank analysis of mortality and limb loss in isolated lower extremity vascular trauma. J Vasc Surg 2011, 53, 1598–1603. [CrossRef]
- deSauza, I.S.; Benabbas, R.; McKee, S.; Zangbar, B.; Jain, A.; Paladino, L.; Boudourakis, L.; Sinert, R. Accuracy of physical examination, ankle-brachial index, and ultrasonography in the diagnosis of arterial injury in patients with penetrating extremity trauma: a systematic review and meta-analysis. Acad Emerg Med 2017, 24, 994–1017. [CrossRef]
- Kobayashi, L.; Coimbra, R.; Goes, A.M.O., Jr.; Reva, V.; Santorelli, J.; Moore, E.; Galante, J.; Abu-Zidan, F.; Peitzman, A.B.; Ordonez, C.; et al. American Association for the Surgery of Trauma𑁋World Society of Emergency Surgery guidelines on diagnosis and management of peripheral vascular injuries. J Trauma Acute Care Surg 2020, 89, 1183–1196. [CrossRef]
- Carpenter, C.R.; Raja, A.S. Penetrating trauma to the extremities and vascular injuries. In Evidence-Based Emergency Care: Diagnostic Testing and Clinical Decision Rules, 3rd ed.; Pines, J.M., Bellolio, F., Carpenter, C.R., Raja, A.S., Eds.; Wiley Blackwell: Chichester, West Sussex, UK, 2023; pp. 214–224. [CrossRef]
- Wahlgren, C.M.; Riddez, L. Penetrating arterial injuries below elbow/knee. In Penetrating Trauma: A Practical Guide on Operative Technique and Peri-Operative Management, 3 d ed.; Degiannis, E., Doll, D., Velmahos, G.C., Eds.; Springer: Cham, Switzerland, 2023; pp. 635–640. [CrossRef]
- Colip, C.G.; Gorantla, V.; LeBedis, C.A.; Soto, J.A.; Anderson, S.W. Extremity CTA for penetrating trauma: 10-year experience using a 64-detector row CT scanner. Emerg Radiol 2017, 24, 223–232. [CrossRef]
- Feliciano, D.V. Pittalls in the management of peripheral vascular injuries. Trauma Surg Acute Care Open 2017, 2, e000110. [CrossRef]
- Warwick, H.; Cherches, M.; Shaw, C.; Toogood, P. Comparison of computed tomography angiography and physical exam in the evaluation of arterial injury in extremity trauma. Injury 2021, 52, 1727–1731. [CrossRef]
- Romagnoli, A.N.; DuBose, J.; Dua, A.; Betzold, R.; Bee, T.; Fabian, T.; Morrison, J.; Skarupa, D.; Podbielski, J.; Inaba, K.; et al. Hard signs gone soft: A croitical evaluation of presenting signs of extremity vascular injury. J Trauma Acute Care Surg 2021, 90, 1–10. [CrossRef]
- Kauvar, D.S., Propper, B.W. Lower extremity vascular trauma. In Rich’s Vascular Trauma, 4th ed.; Rasmussen, T.E., Tai, N.R.M., Eds.; Elsevier: Philadelphia, PA, USA, 2022; pp. 273–287. [CrossRef]
- Hynes, A.M. Traumatic proximal brachial artery injury selectively managed non-operatively: A case report and review of the literature. Trauma Case Rep 2022, 38, 100612. [CrossRef]
- Guthrie, H.C.; Clasper, J.C.; Kay, A.R.; Parker, P.J.; Limb Trauma and Wounds Working Groups, ADMST. Initial extremity war wound debridement: a multidisciplinary consensus. J R Army Med Corps 2011, 157, 170–175. [CrossRef]
- Kennedy, T.M.; Russo, C.J. Management of specific soft tissue injuries. In Reichman’s Emergency Medicine Procedures, 3rd ed.; Reichman, E.F., Ed.; McGraw-Hill: New York, NY, USA, 2019; pp. 1034–1049, ISBN 978-1-259-86192-5.
- Bowyer, M.W.; Rhee, P.; DuBose, J.J. Soft tissue wounds and fasciotomies. In Front Line Surgery: A Practical Approach, 2nd ed.; Martin, M.J., Beekley, A.C., Eckert, M.J., Eds.; Springer: Cham, Switzerland, 2017; pp. 329–352, ISBN 978-3-319-56780-8.
- Stefanopoulos, P.K.; Aloizos, S.; Mikros, G.; Nikita, A.S.; Tsiatis, N.E.; Bissias, C.; Breglia, G.A., Janzon, B. Assault rifle injuries in civilians: ballistics of wound patterns, assessment and initial management. Eur J Trauma Emerg Surg 2024, 50, 2741–2751. [CrossRef]
- Sassoon, A.; Riehl, J.; Rich, A.; Langford, J.; Haidukewych, G.; Pearl, G.; Koval, K.J. Muscle viability revisited: Are we removing normal muscle? A critical evaluation of dogmatic debridement. J Orthop Trauma 2016, 30, 17–21. [CrossRef]
- Schmalbruch, H. Skeletal Muscle. Springer: Berlin, Germany, 1985; Chapter: Development, regeneration, growth, p. 282. [CrossRef]
Figure 1.
Various stages of construction of a full metal-jacketed military rifle bullet. The lead core (lower row) is enclosed by jacket which covers its tip but leaves its base semi-open. The canellure, around which the mouth of the cartridge case holds firmly the bullet, representing a weak point of the jacket acting as a stress concentrator, can also be seen (upper row, far right). War Museum of Athens.
Figure 1.
Various stages of construction of a full metal-jacketed military rifle bullet. The lead core (lower row) is enclosed by jacket which covers its tip but leaves its base semi-open. The canellure, around which the mouth of the cartridge case holds firmly the bullet, representing a weak point of the jacket acting as a stress concentrator, can also be seen (upper row, far right). War Museum of Athens.

Figure 2.
Destabilizing effect of the retarding force acting on a military (full metal-jacketed) rifle bullet. In the air, yaw tendency (due to inherent instability) is counteracted by the spin. During tissue penetration, the much higher tissue density generates a strong retarding force which increases in magnitude by positive feedback as the bullet undergoes irreversible yaw and its presented area increases.
Figure 2.
Destabilizing effect of the retarding force acting on a military (full metal-jacketed) rifle bullet. In the air, yaw tendency (due to inherent instability) is counteracted by the spin. During tissue penetration, the much higher tissue density generates a strong retarding force which increases in magnitude by positive feedback as the bullet undergoes irreversible yaw and its presented area increases.
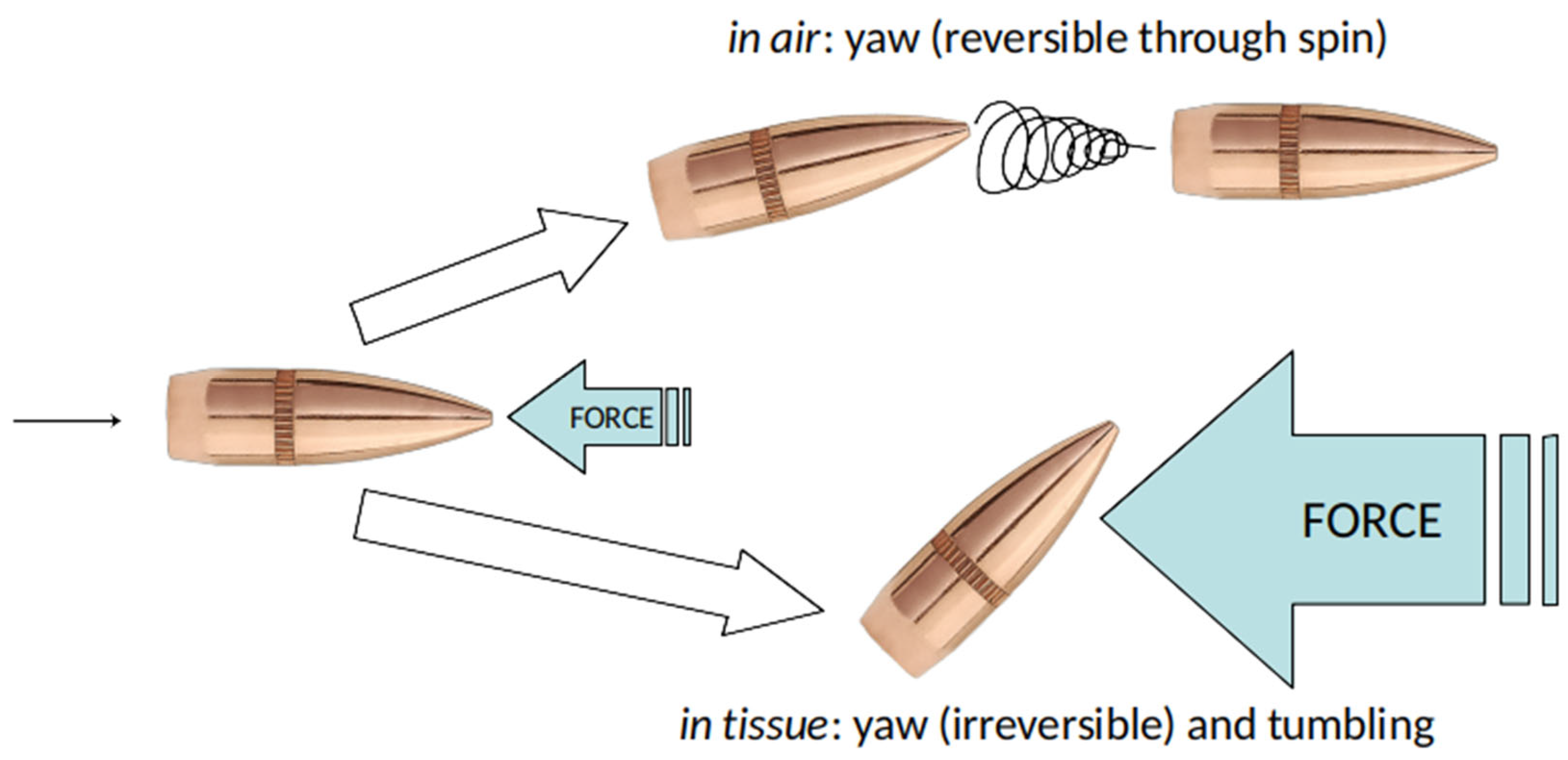
Figure 3.
Abdominal gunshot wound from a .45 cal. Handgun bullet, which resulted in laceration of the right internal iliac vein. (a) Emergency x-ray of the patient. (b) CT scan, 21 days later, which also reveals the FMJ construction of the projectile. Courtesy of D. Pinialidis, MD.
Figure 3.
Abdominal gunshot wound from a .45 cal. Handgun bullet, which resulted in laceration of the right internal iliac vein. (a) Emergency x-ray of the patient. (b) CT scan, 21 days later, which also reveals the FMJ construction of the projectile. Courtesy of D. Pinialidis, MD.
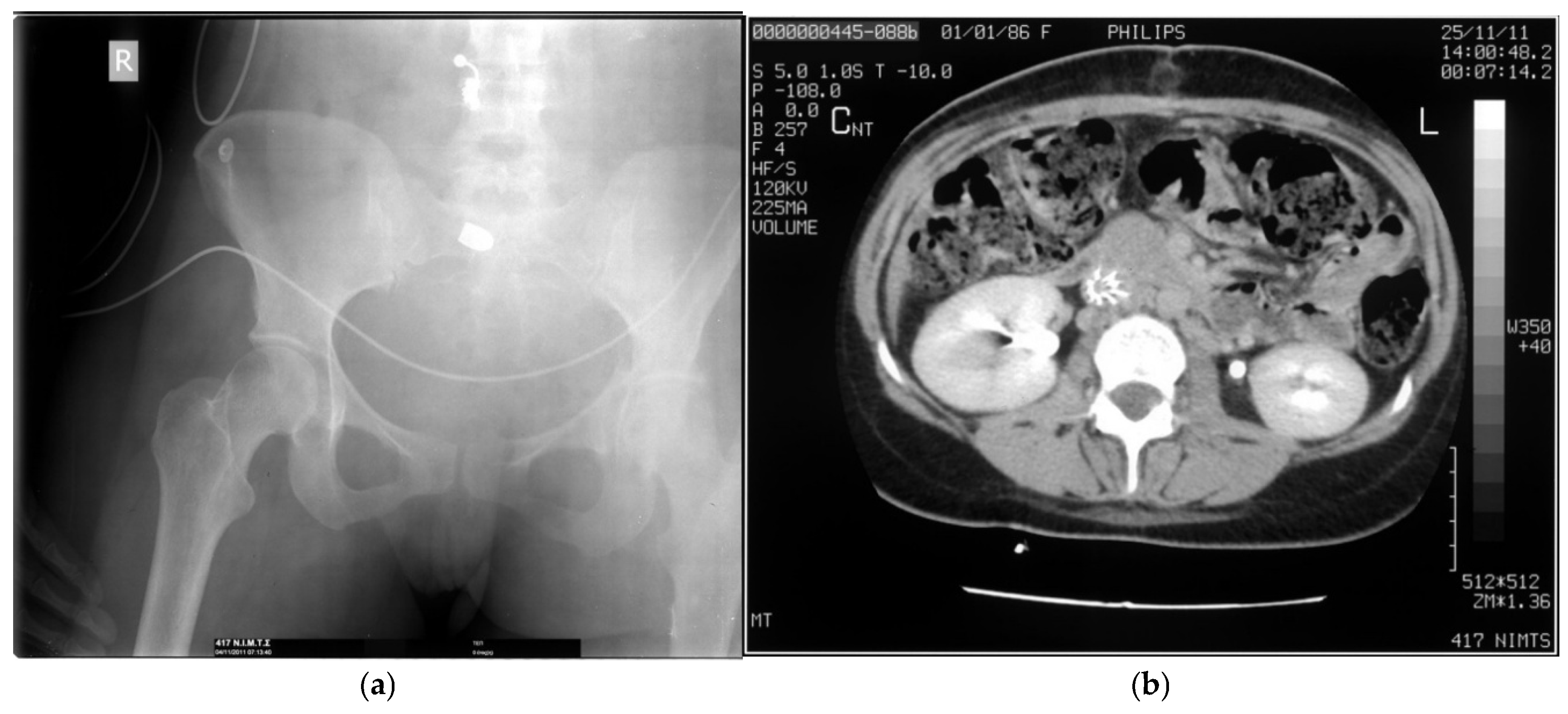
Figure 4.
Schematic depiction of the temporary cavity formation (pink) and expansion (blue arrows) in tissue by a tumbling military rifle bullet. Black arrow indicates direction of movement.
Figure 4.
Schematic depiction of the temporary cavity formation (pink) and expansion (blue arrows) in tissue by a tumbling military rifle bullet. Black arrow indicates direction of movement.
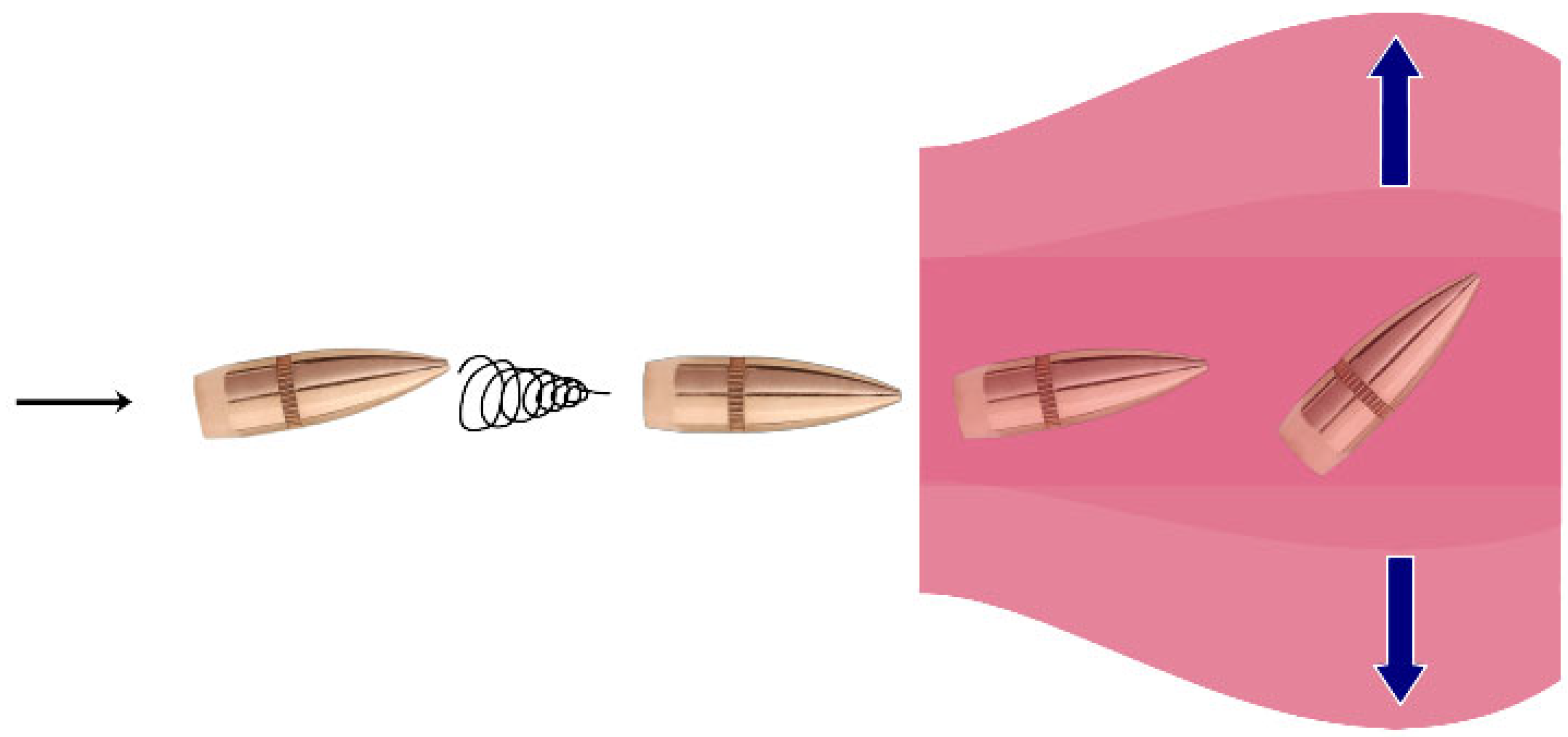
Figure 5.
The onset of maximum cavitation in a block of ballistic gelatin penetrated by a 5.56 mm NATO assault rifle bullet, as the latter moves sideways just before its breakup (courtesy of N. Tsiatis). Arrow indicates the direction of penetration.
Figure 5.
The onset of maximum cavitation in a block of ballistic gelatin penetrated by a 5.56 mm NATO assault rifle bullet, as the latter moves sideways just before its breakup (courtesy of N. Tsiatis). Arrow indicates the direction of penetration.
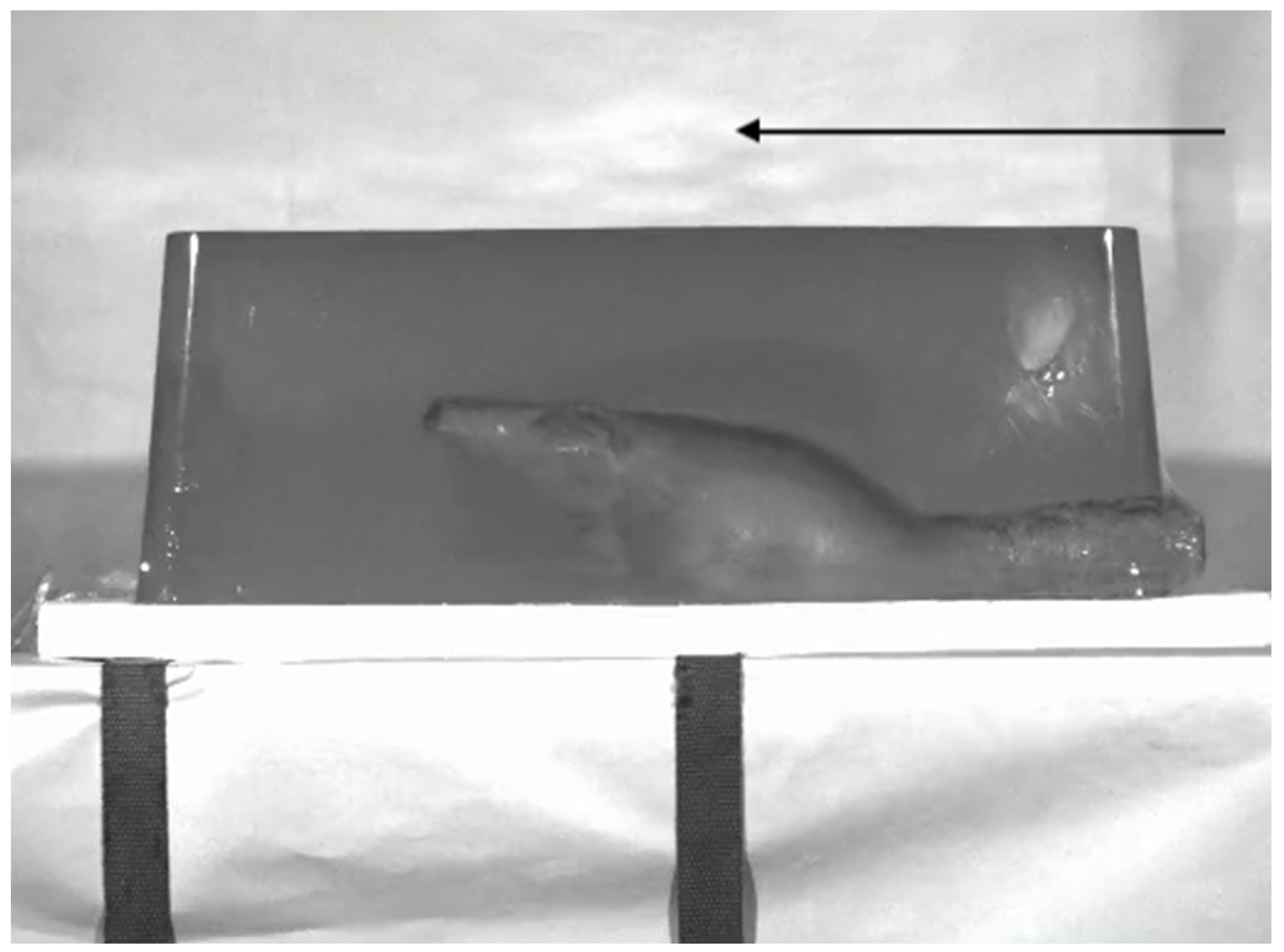
Figure 6.
Close-range hand injury from a .38 cal. handgun bullet, with extensive soft tissue damage from bullet deformation and cavitation as well as from bone shattering. Intraoperative photographs of the entry (a) and exit (b) wounds. (c) Emergency X-ray of the bone injury. Courtesy of G. Breglia, MD.
Figure 6.
Close-range hand injury from a .38 cal. handgun bullet, with extensive soft tissue damage from bullet deformation and cavitation as well as from bone shattering. Intraoperative photographs of the entry (a) and exit (b) wounds. (c) Emergency X-ray of the bone injury. Courtesy of G. Breglia, MD.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



