
Submitted:
28 July 2025
Posted:
29 July 2025
You are already at the latest version
Abstract
Background/Objectives: Toxic leadership has arisen as a matter of serious concern within the nursing profession, with growing evidence linking it to diminished job satisfaction, ineffective conflict management, and weakened organizational commitment. These ef-fects not only compromise nurse retention but also threaten the quality of patient care and overall healthcare outcomes. This scoping review aims to examine the impact of toxic nursing leadership on staff retention by synthesizing evidence from existing literature and a broad range of published studies. Methods: A comprehensive literature search was conducted across multiple databases, including PubMed/MEDLINE, Scopus, CINAHL and Science Direct databases yielding 1,356 articles. Of these, 18 met the predefined inclusion criteria. The scoping review followed the six-stage methodological framework proposed by Arksey and O’Malley. Thematic analysis identified two core categories: (a) key dimensions shaping perceptions of toxic leadership and (b) the impact of toxic leadership on nursing staff retention. Results: The findings reveal that toxic leadership contributes to organizational silence, emotional exhaustion, diminished psychological safety, and low professional commitment. Such behaviors not only jeopardize nurse engagement and productivity but also negatively affect patient safety and care quality. In contrast, leadership styles such as transformational and transactional leadership are as-sociated with higher job satisfaction, reduced burnout, and improved retention outcomes. Conclusions: This review underscores the need for healthcare organizations to identify and address toxic leadership behaviors promptly. By promoting supportive and ethical leadership styles, institutions can foster a healthier workplace, improve nurse retention, and ultimately enhance the quality of care. The study offers practical implications for healthcare administrators, emphasizing leadership development.
Keywords:
toxic leadership
; nursing staff
; staff retention
; job satisfaction
1. Introduction
Leadership is a complex and evolving concept with various definitions. It is often defined as an influencing process aimed at achieving goals, where leaders mobilize others to strive for shared aspirations [1]. It is also described as the ability to establish and accomplish objectives, react effectively to challenges and empower others within an organization [2]. The ambiguity and multiplicity of leadership pose significant challenges. The concept is often conflated with management, although some argue that leadership and management are distinct, yet complementary roles [1].
Nursing leadership is often described as the process of influencing and guiding nurses to attain joint outcomes, with a focus on improving patient outcomes and enhancing the work environment [3,4]. Key attributes of nursing leadership include the ability to motivate, support and develop team members, as well as to foster decision-making [5]. Effective nursing leadership is linked to better patient outcomes, reduced medical errors and enhanced patient safety. It encourages evidence-based practices, increases staff engagement, and promotes collaboration with other healthcare professionals [6,7,8]. Positive leadership styles such as relational leadership promote the nurses’ well-being and productivity, while addressing challenges and empower the nurses to strive for excellence and quality care [6,9].
On the other hand, negative leadership behaviors, such as toxic or exploitative leadership, are linked to decreased job satisfaction due to the stress caused by such managerial actions, which may lead to higher turnover rates and financial losses for the healthcare organizations [10,11]. Toxic leadership affects team dynamics, leading to poor conflict management and reduced organizational commitment [12]. This can result in a negative work environment, further impacting nurse retention and patient care quality. Negative leadership is also contributing to increased frequencies of adverse clinical events observed by nurses, with subsequent deterioration in care quality [11]. Toxic leadership in nursing may have adverse consequences on the workforce, including satisfaction with work, relationship with organization, psychological state, productivity, and patient safety outcomes. Understanding abusive leadership helps in developing strategies to mitigate its effects, as this style of leadership may undermine workforce stability by lowering satisfaction levels, weakening connection to the organization, and impairing psychological resilience, productivity, and patient safety outcomes [13]. This research area has gained attention due to its significant impact on both individuals and organizations but despite the growing body of knowledge, there is still an incomplete understanding of toxic leadership in the healthcare sector. This paper adds to the growing discourse on toxic leadership by exploring its effects on the nursing profession and its implications for staff well-being.
1.1. Toxic Leadership and the Toxic Leader
Toxic leadership is a detrimental style of leadership characterized by harmful behaviors and attitudes that negatively impact organizations and individuals. Smidt [14] suggested, that toxic leadership encompasses five core elements: abusive supervision, authoritarianism, narcissism, self-promotion, and behavioral inconsistency.
The concept of toxic leadership was introduced in 1996, initially explored within corporate and military settings. It wasn't until 2007 that empirical research began to connect abusive leadership with higher education systems, highlighting its influence on leadership culture in these environments [15,16]. Over the years, the research has expanded to include various organizational contexts, including education and manufacturing [17].
Dysfunctional leadership is marked by behaviors such as abuse, bullying, and destructive actions that create a harmful work environment. These leaders often aim to conceal their incompetence and maintain control, leading to increased ambiguity and confusion within the organization [18,19] They often exhibit behaviors of being autocratic, manipulative, controlling, deceitful, and callous. These demeaners distinguish them from merely difficult leaders and contribute to a toxic work environment [18,20]. The personality traits associated with toxic leaders include Machiavellianism, narcissism, and psychopathy, which contribute to organizational failures [21]. These dispositions often lead to unethical decision-making and a focus on personal gain over organizational well-being [21,22].
Destructive leadership negatively affects job satisfaction, commitment, and turnover intention, with organizational culture playing a mediating role in these outcomes [17]. It undermines employee well-being, health, morale, and productivity, ultimately impacting organizational effectiveness [23]. Within higher education institutions, oppressive leadership exerts detrimental effects on the psychological well-being of faculty, staff, and students, causing adverse outcomes such as emotional distress, diminished job satisfaction, and systemic organizational dysfunction [22]. Toxic leadership, as a destructive model, is characterized by behaviors—including manipulation, pressure, and recognized humiliation—that decompose organizational culture, undermine employee morale, and compromise institutional efficacy.
1.2. Nursing Staff Retention
The shortage of nurses is a critical issue affecting healthcare systems globally. This scarcity has been persistent and is exacerbated by various factors. The aging nursing staff, leading to a gap in the workforce as there are not enough new entrants to fill these positions. Declining enrolment in nursing programs further exacerbates this issue [24]. The strain of continuous high stress working conditions leads to professional burnout, ultimately increasing nurse turnover and diminishing workforce sustainability [25,26]. Economic challenges and other social factors, such as the impact of the COVID-19 pandemic, have intensified the shortage by increasing job vacancies and affecting the well-being of the existing nurses [27,28].
Nursing staff is integral to maintaining a safe hospital environment and ensuring high-quality patient care. Their engagement in hospital safety strategies is crucial for achieving optimal patient safety outcomes [29]. Adequate nursing staff levels are associated with better patient safety outcomes, such as reduced fall rates and hospital-acquired pressure ulcers. Retaining the experienced nurses, also plays a significant role in patient safety [30]. On the contrary, low nurse staffing levels are consistently associated with adverse patient outcomes. These include higher rates of in-hospital mortality, hospital-acquired infections, medication errors, and patient falls [31,32,33,34]. Studies have shown that inadequate staffing leads to increased missed care, which directly impacts the quality of care and patient safety [35,36,37]. Additionally, personnel shortage in emergency departments has been linked to longer door-to-discharge times and an increased number of patients leaving without being seen [38].
Nursing staff retention is a critical issue in healthcare, influenced by a variety of factors. A positive work environment and high job satisfaction are crucial for retaining nursing staff. Factors such as supportive management and leadership, group cohesion, and reduced job stress contribute significantly to retention [39,40,41,42]. Factors such as staffing levels, career advancement opportunities, and financial remuneration contribute significantly to the decrease of the turnover levels [43,44]. Nurses who feel appreciated and supported by their managers and peers are more likely to stay. Recognition of their work and contributions is vital for retention [39,44].
2. Materials and Methods
2.1. Aim of the Study
The aim of this scoping review was to explore the influence of toxic nursing leadership on the nursing staff retention. This research specifically aims to respond to the following research questions that were develop following the PIO (Population, Intervention, Outcome) framework where Population is the Nurses, Intervention is the toxic leadership and Outcome is the nursing staff retention:
Q1: What are the key dimensions and behaviors associated with toxic leadership in nursing as identified by the healthcare professionals?
Q2: How does toxic leadership influence nursing staff on their career decisions and retention in healthcare organizations?
2.2. Design
A scoping review is a rigorous exploratory methodology designed to systematically map the range of existing literature on a defined research topic. Unlike traditional systematic reviews, which focus on answering highly specific questions, scoping reviews employ a structured yet flexible approach to identify key concepts, evidence gaps, and emerging trends within a field. By applying predefined criteria, this methodology facilitates a comprehensive analysis and synthesis of existing literature, enabling researchers to address their study's broader research questions [45]. In alignment with well-known best practices, this study adopts the systematic six-stage framework originally developed by Arksey and O’Malley [45], ensuring methodological transparency and accuracy throughout the review process.
2.3. Identifying Relevant Studies
Eligibility criteria. This analysis incorporated peer-reviewed studies examining toxic leadership in healthcare organizations, including quantitative (cross-sectional, longitudinal), qualitative, and mixed-methods research designs. The inclusion criteria required that studies (a) specifically analyze toxic leadership behaviors and their organizational impacts, (b) be published in English between 2019-2025 to ensure contemporary relevance, and (c) provide empirical evidence from healthcare contexts. Studies that (a) addressed leadership generically without focusing on toxic behaviors, (b) were published prior to 2019, except those that were cited in the conceptual framework, (b) lacked peer-review validation, or (c) were unavailable as full-text articles, were excluded. Specific consideration was given to excluding studies that conflated toxic leadership with other negative leadership styles (e.g., laissez-faire or incompetent leadership) to maintain conceptual clarity. A thorough selection process ensured inclusion of the most relevant and methodologically robust research on the harmful impacts of toxic leadership in healthcare organizations.
Information sources and search strategy. A comprehensive, multi-database search strategy was executed across PubMed/MEDLINE, Scopus, CINAHL, and Science Direct to capture the full spectrum of research on toxic leadership in healthcare backgrounds. The search incorporated an in-depth set of leadership-related terms including "toxic leadership", "abusive leadership", "negative leadership", "oppressive leadership", and "destructive leadership," combined with healthcare-specific terms through Boolean operators (AND/OR/NOT) to ensure methodological consistency. The search strategy specifically targeted studies examining these leadership styles' impacts on nursing staff and healthcare organizations, with all search parameters and term combinations systematically documented in Table 1 to ensure transparency and reproducibility.

Table 1.
Search Strategy: Key Terms and Boolean Operators.
| Term | Boolean Operator | Term | Boolean Operator | Term |
|---|---|---|---|---|
| Toxic1 Leadership | AND | Healthcare Organizations | ||
| Toxic Leadership | AND | Nursing Staff | ||
| Toxic Leadership | AND | Healthcare Organizations | AND | Nursing Staff |
| Toxic Leadership | OR | Nursing Staff | AND | Healthcare Organizations |
| Healthcare Organizations | OR | Nursing Staff | AND | Toxic Leadership |
2.4. Study Selection
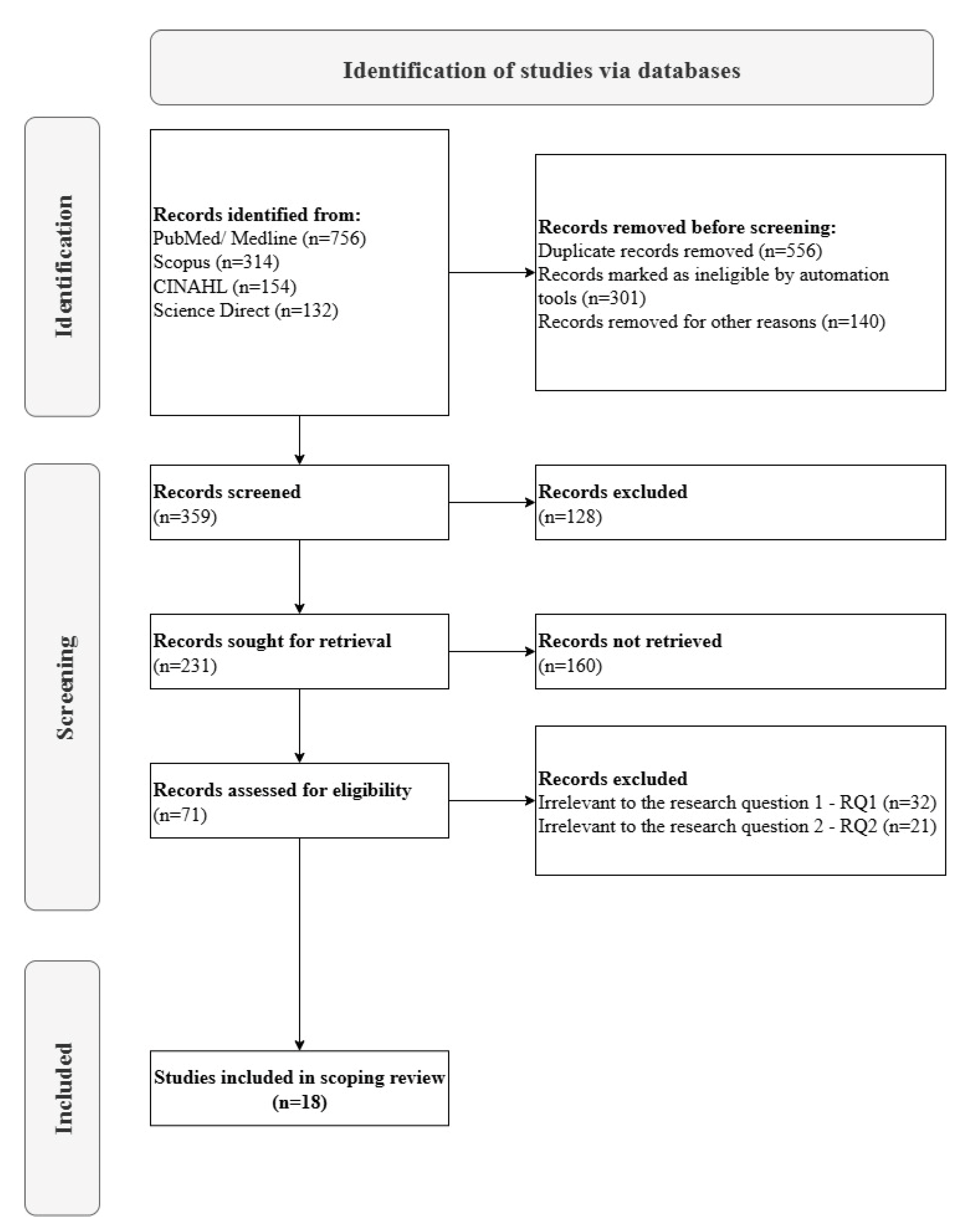
The study selection process followed a thorough, systematic approach, as detailed in the PRISMA flowchart (Figure 1) [4]. Initial database searches across PubMed/MEDLINE, Scopus, CINAHL, and Science Direct yielded 1,356 records. After removing duplicates (n=556) and records deemed ineligible through automated tools and manual screening (n=441), 359 studies underwent full-text assessment. Of these studies, 231 were sought for retrieval, with 160 unavailable, leaving 71 studies for eligibility evaluation. Following a stringent review, 53 studies were excluded – 32 for irrelevance to Research Question 1 (RQ1) and 21 to Research Question 2 (RQ2) – resulting in 18 studies that met all inclusion criteria. These studies were selected for their explicit focus on toxic leadership and its detrimental impacts within healthcare backgrounds. This deliberate selection ensures the review captures the most relevant evidence on toxic leadership’s consequences, providing a necessary contrast to dominant narratives of positive leadership.
Figure 1.
PRISMA Flow Diagram of Study Selection.
2.5. Charting the Data
In accordance with Arksey and O'Malley's established framework [45], a carefully data extraction and synthesis process was implemented to systematically examine toxic leadership in healthcare contexts. The methodology began with the development of a structured data extraction table designed to capture critical elements from each study, including specific toxic leadership behaviors, their healthcare-specific consequences, and key methodological characteristics. To ensure reliability, a pilot test on a subset of four studies (approximately 22% of the total studies) was conducted, allowing the research team to refine the extraction criteria and establish strong inter-rater reliability (IRR > 0.85). Three researchers with expertise in organizational behavior and healthcare leadership independently extracted data from the allocated studies. Any discrepancies were resolved through systematic consensus discussions, with all decisions documented to maintain transparency throughout the analysis process. The final synthesized data, presented in Appendix A, provides a comprehensive overview of the included studies. This includes detailed information on authorship, publication dates, geographic focus, research objectives, methodological approaches, and key findings related to toxic leadership's impact on healthcare environments (see Table A1). This methodical approach aligns with best practices in scoping reviews and the consensus-based validation process ensure the findings are both reproducible and accurate.
2.6. Data Analysis
The extracted data were systematically analyzed within two conceptual categories: (a) the key dimensions shaping perceptions of toxic leadership in healthcare environments, and (b) its measurable impact on nursing staff retention. These thematic dimensions were chosen, in order to reveal critical patterns across the literature, with the first thematic category exposing how nurses identify and experience toxic leadership through specific behavioral manifestations (e.g., psychological manipulation, bullying, and inconsistent decision-making), while the second category documented its devastating consequences on workforce stability (including increased turnover intentions, emotional exhaustion, and premature career abandonment). Three lead researchers conducted the primary analysis coding and categorize findings, followed by iterative consensus-building sessions with the entire research team to verify emerging themes. This collaborative methodology supported robust interpretation of the findings while preserving the contextual integrity of the original studies. The final synthesis was structured according to PRISMA-ScR guidelines [46]. This scoping review was registered on the Open Science Framework platform on 25th July 2025 (Registration DOI https://doi.org/10.17605/OSF.IO/UWY4G)
2.7. Consultation
Preliminary findings were presented to critical evaluation through discussions with the research team to ensure interpretive validity. So, a structured validation process with four external stakeholders from the healthcare sector was conducted. These individuals were selected based on their extensive leadership experience and expertise in organizational management within healthcare environments. They were then invited to critically assess the clarity, accuracy, and significance of these findings, offering feedback on whether the results resonated with their professional experiences. Additionally, they highlighted practical considerations for addressing toxic leadership in institutional settings, such as policy adjustments, leadership training programs, and support mechanisms for affected staff. Their insights provided valuable external perspectives on both the interpretation of the results including the identified dimensions of toxic leadership and its documented effects on nursing staff retention.
3. Results
3.1. Characteristics of the Included Studies
As presented in Table 2, the included studies varied by region, publication period, methodological approach, and thematic emphasis on toxic leadership dimensions or nurse retention outcomes.
Table 2.
Summary of Included Studies Characteristics.
| Characteristics | Studies n (%) |
|---|---|
| Area of Studies | |
| Europe | 2 (11.1) |
| Asia | 8 (44.4) |
| USA | 1 (5.6) |
| Africa | 7 (38.9) |
| Year of publication | |
| 2019 | 3 (16.7) |
| 2020 | 2 (11.1) |
| 2021 | 2 (11.1) |
| 2022 | 5 (27.8) |
| 2023 | 3 (16.7) |
| 2024 | 2 (11.1) |
| 2025 | 1 (5.6) |
| Type of studies | |
| quantitative study | 10 (55.6) |
| qualitative study | 2 (11.1) |
| mixed methods | 6 (33.3) |
| Categorization of studies | |
| key dimensions shaping perceptions of toxic leadership | 5 (27.8) |
| impact of toxic leadership on nursing staff retention | 13 (72.2) |
The scoping review incorporated 18 studies examining toxic leadership in healthcare, with distinct geographical and methodological patterns. Geographically, nearly half originated from Asia (44.4%, n=8), followed closely by Africa (38.9%, n=7), while European and North American studies were underrepresented (11.1% and 5.6%, respectively). Temporally, most publications emerged in the latter half of the review period (61.1%, n=11; 2022–2025), suggesting growing research interest. Methodologically, cross-sectional designs dominated (55.6%, n=10), with mixed methods approaches representing a third of studies (33.3%, n=6). Thematic analysis revealed a strong emphasis on toxic leadership’s impact on nurse retention (72.2%, n=13), outweighing investigations of its perceptual dimensions (27.8%, n=5). This distribution highlights a critical research gap in understanding how toxic leadership is identified versus its measurable workforce consequences.
3.2. Perceptions of Toxic Leadership Key Dimensions
Concerning the views of Chinese nurses on the nature, features, and response mechanisms related to toxic managerial behaviors in nursing leadership roles, Guo et al. [47] carried out a qualitative research conducting semi-structured in-depth interviews with 12 registered nurses in China. This study pointed out, that the toxic leader depicts self-centeredness, low emotional intelligence, narrow-mindness and competitiveness. Although the nurses notice their managers’ abusive leadership traits, they choose either to tolerate it or to ignore it, as they regard it as common or inevitable. They tendentially make positive evaluations about their oppressive managers for fear of receiving punishing or vindictive behaviors, purposeful unfairness, excessive pressure and workloads. The nurses develop silence as coping mechanism, they may choose the night shift to avoid interaction with their leader, and they even self-reflect, when they receive negative behaviors.
The staff withdrawal owing to corrosive leadership behaviors, was also studied by Durrah et al. [48], obtaining information from 413 healthcare workers in France. This study examined the two dimensions of staff turnover, the psychological and the physical individually and revealed that various negative leadership behaviors trigger different workforce reactions. More specifically this study concluded that authoritarian leadership is linked to physical resignation, whereas self-promotion is more influential on psychological withdrawal behaviors. Other destructive leadership characteristics were the unpredictability and uncertainty of the supervisor, which led to lower workforce engagement and eventually turnover.
Bakkal et al. [49] investigated the impact of harmful leadership on nurses’ and hospital employees’ job satisfaction and turnover intention and the mediating effect of their perceptions of dysfunctional leadership behaviors. The study was conducted in Turkey and included a sample of 658 participants The findings of this study indicate an inverse relationship between job satisfaction and the components of toxic leadership, specifically unappreciativeness, selfishness, and self-serving behavior. The study suggests that when employees' perception of self-respect is attacked, their self-confidence and individual performance deteriorate. Consequently, as job satisfaction declines, turnover intention tends to increase.
Ofei et al. [50] sought to evaluate the characteristics and he relationship between toxic leadership traits in nurse management and nurses’ perceived job fulfillment and productivity in the healthcare sector. Utilizing a sample of 943 nurses from various hospitals in Ghana, this study underlined intemperance, humiliation, narcissism, and self-promotion as the most common attributes of despotic leadership. The outcomes of this study also designate a significant positive correlation between autocratic leadership behaviors and turnover intentions. Moreover, job satisfaction appears to act as a mediating factor in this relationship, suggesting that the detrimental effects of toxic leadership on retention are, in part, driven by its impact on nurses' satisfaction at work.
In another study in Egypt [51], in which 250 nurses took part, two hospitals, a university hospital and a health insurance hospital, were compared. In this study each hospital was studied in terms of how nurses responded to adverse leadership behaviors. Results highlighted that nurses’ intent to stay was negatively affected by authoritarian and unpredictable leadership in the university hospital and by self-promoting leadership in the health insurance hospital.
3.3. Toxic Leadership and Its Impact on Staff Retention
Labrague L. et al. [52] in their study in 2020 in Philippines with 770 participants compared the impact of the toxic and transformational leadership on the nurses’ work attitudes. According to their findings, toxic leadership results in diminished job satisfaction, elevated stress levels, increased rates of absenteeism, and a heightened intent to leave the profession. On the other hand, transformational leadership leads to higher job satisfaction and lower turnover intentions.
Ofei et al. [53] in Ghana performed an investigation about the nature and effect of destructive nurse leadership conduct for nursing staff’s perceptions of job satisfaction and productivity. In this descriptive study 943 nurses took part and revealed that emotionally damaging leadership behaviors of nurse managers related to decreased psychological empowerment, job dissatisfaction, poor work performance and greater likelihood of departure from the nursing profession and the affiliated institution.
Ramdan and Eid [54] in their research in Egypt, with a sample size of 544 participants, compared the oppressive leadership among intensive care nursing staff at two hospitals. They assessed their nurse manager’s harmful leadership regarding their selected conflict management methods and organizational commitment levels. The study demonstrated a positive relationship between toxic leadership and confrontational conflict management styles and a negative correlation with the collaborative dispute resolution methods. The results also indicated a negative correlation between malicious leadership and the nurses’ organizational commitment in both hospitals highlighting the significance of the leader’s behavior regarding staff retainment and sustainability.
Siyal et al. [55] developed a research study in which 430 healthcare professionals took part, examined the impact of abusive supervision on the employees’ performance in China. The results of this study underscore, that destructive leadership has a negative impact on employee performance, with job satisfaction and extrinsic motivation mediating this relationship. Consequently, the healthcare organization’s image was also affected by the reduction of the quality of its services, due to the lack of interest of the employees receiving negative behaviors. On the other hand, employees who were motivated and satisfied with their leadership, depicted higher quality performance.
Regarding the impact of destructive leadership on the employee health, Trépanier et al. [56] undertook a research among 399 Canadian nurses. This study analyzed the mental and motivational processes involved in how tyrannical and laissez-faire leadership styles influence employee burnout, affective commitment, and job performance. According to the outcomes of this study, tyrannical leadership style is related to emotional dysregulation, low affective commitment and poor performance, which jeopardize both the patient safety and the organizational success. Also, laissez-faire leadership style is highly associated with autonomy frustration, burnout and low work engagement. Both negative managerial styles were found to erode motivation, self-determination, feelings of competence, self-worth and appreciation, leading ultimately to resignation figuratively or literally.
The impact of different leadership styles on healthcare personnel’s well-being was investigated by Erschens et al. [57] in Germany, using a sample of 1137 participants from all three occupational groups (physicians, nursing staff and administrative employees). The findings of this study underlined the positive effects of effective leadership as well as the negative repercussions of dysfunctional leadership. As far as the group of nurses is concerned, those who experienced transformational and transactional leadership styles, exhibited higher well-being scores than the ones who incurred destructive and laissez-faire leadership.
Low et al. [58] led a research initiative in Malaysia, in which 377 nurses took part, and pointed out the effects of abusive supervision on the nurses’ negative and absurd behaviors. More specifically this study showed that the nurses who perceived injustice or discrimination, had low power distance orientation and external locus of control, were more likely to acquire counterproductive behaviors. This is due to their difficulty in accepting inequalities and in order to restore justice. The outcomes of this study advocate, that applying unethical nursing leadership results in antisocial behaviors, reduces compliance with the rules and the nurses’ interest about organizational goals, increases organization-oriented aggression and bullying incidents.
Shipl et al. [59] studied the effect of manipulative leadership on the nurses’ followership effectiveness. In their study in Egypt participated 343 nurses and revealed, that workforce responsiveness negatively correlated with leadership practices that undermine team cohesion, due to the instability, stress, rigidly, discriminations and perceived threats. Furthermore, a weak but statistically significant negative correlation was observed, between harmful leadership and nurses’ overall effectiveness. This finding indicates that nurses, by employing professionalism and critical thinking, were able to buffer the adverse effects of toxic leadership on their performance. The study also identified a significant negative effect of abusive supervision on the nurses’ active engagement. This association may be attributed to characteristic behaviors of oppressive supervisors, including public belittlement of staff and persistent reminders of past errors and failures. Such actions serve as workplace stressors, eroding employees’ psychological resources and well-being. Consequently, staff exposed to corrosive supervision is more inclined to disengage and exhibit silence in the workplace, thereby reducing their levels of professional and organizational commitment.
Organizational silence among nurses and its repercussions, is a major problem addressed by Berma et al. [60] in their research, which took place in Egypt and had a total of 235 participants. This study underscored that workplace toxicity may originate from either managerial figures or colleagues, highlighting multiple potential sources of a detrimental work environment. One quarter of the nurses exhibited high levels of organizational silence as a coping mechanism. This silence may stem from various concerns, including fear of losing professional respect, harming relationships with senior management, an inability to openly discuss work-related issues, the presence of a bureaucratic and non-transparent hospital system, fear of punitive responses, self-neglect, inadequate organizational support, and former experiences of abusive supervision. Additionally, although the majority of the nurses were highly committed and passionate to thrive, workplace toxicity fosters increased organizational silence, hindering professional growth and productivity, and ultimately contributing to higher turnover intentions.
Budak & Erdal [61] examined the role of burnout syndrome as a mediator in the link between malevolent leadership and job satisfaction in healthcare environments. Utilizing a sample of 412 participants employed in public hospitals in Turkey, the results revealed that ego-driven and self-serving leadership appears to exert a significantly negative impact on job satisfaction related to managerial roles. Furthermore, it was found to be associated with aspects of burnout encompassing exhaustion, depersonalization, and decreased sense of personal achievement. Burnout resulting from problem-solving demands and efforts to contribute meaningfully also appeared to be influenced by counterproductive leadership practices.
Mrayyan [62] posited in her research in Jordan, the evident ramifications of destructive nursing leadership in workforce preservation. Involving 384 respondents, this study investigated the presence of toxic leadership among nursing leaders in Jordan and its relationship with nurses’ workplace satisfaction, job engagement, and turnover intention. Destructive leadership was identified as a critical determinant of reduced workplace satisfaction and diminished job engagement among nurses, primarily through the cultivation of a dysfunctional and unbalanced work environment. Such conditions contribute to both emotional disconnection and physical disengagement, driven by the sustained intensity and demands of the nursing role. Despite these adverse effects, many nurses demonstrated reluctance to leave their positions. This behavior may be attributed to a cost–benefit analysis shaped by financial constraints and familial obligations, which make employment mobility impractical. While a subset of nurses continued to exhibit professional pride and emotional investment in their work, overall job engagement appeared to be neither spontaneous nor sustainable under persistent tyrannical leadership. The findings of this study concluded, that this dynamic pose significant managerial concerns, as prolonged dissatisfaction may ultimately lead to increased turnover intentions and potential attrition from the nursing profession.
Labrague [63] carried out a research study in Philippines, utilizing a sample of 283 nurses. The study aimed to emphasize the direct and mediated influences of harmful leadership styles on occupational satisfaction and psychological discomfort, with work–family conflict serving as a mediating variable. The findings of the study demonstrated that authoritarian and oppressive leadership behaviors exhibited by nurse managers, exert a substantial detrimental effect on employee contentment and its influence on psychological well-being among nurses in emergency settings A critical insight from the analysis was that work–family conflict has partial mediating effects in the dynamic between malicious leadership and these adverse outcomes. This indicates that toxic leadership not only has a direct detrimental effect on nurses' well-being, but also indirectly exacerbates dissatisfaction and psychological strain by intensifying conflicts between professional and personal roles.
Farghaly Abdelaliem & Abou Zeid [64] in their study in Egypt evaluated the relationship between corrosive leadership and organizational functionality among nursing professionals in a university-affiliated hospital, while also examining how organizational silence mediates this relationship. The study identified a significant inverse relationship between dictatorial leadership and organizational performance. Furthermore, a pronounced negative correlation was observed between unethical leadership and nurses’ organizational silence, indicating that these leadership styles detrimentally affect both individual job satisfaction and the propensity of nurses to withhold their opinions. Organizational silence was found to act as a mediating factor in the relationship between arbitrary leadership and nurses’ organizational performance Furthermore, a negative correlation was identified between dictatorial leadership and organizational performance.
4. Discussion
The findings of our study yield that toxic leadership behaviors—characterized by self-centeredness, limited emotional intelligence, narrow-mindedness, and excessive competitiveness—significantly contribute to the perpetuation of a culture of silence within healthcare organizations. Furthermore, leadership practices that instill fear are associated with organizational silence, which, in turn, adversely impacts individual development and overall productivity. These dynamics collectively foster increased turnover intentions among nurses [47,49,60,64]. These findings are consistent with the study by Lukacik and Bourdage [65], which similarly identified a correlation between abusive supervision and heightened levels of self-promotion and intimidation. A growing body of literature across various disciplines, further supports the assertion that destructive leadership is significantly linked to reduced employee voice. Under such leadership, employees are more inclined to withhold their opinions or merely reiterate the perspectives favored by their superiors, thereby impeding organizational learning and growth [66,67,68]. Kazmi et al. [69] in their research also found that despotic leadership fosters increased employee withdrawal and silent acquiescence, mediated through leader-member exchange and work-life quality.
Furthermore, authoritarian leadership and laissez-faire leadership styles appeared to be toxic leadership traits that are linked to autonomy frustration, burnout and low work engagement increased turnover intentions, low job satisfaction and high work- related stress [48,51,56,63]. These findings align with the research of Schaubroeck et al. [70], who demonstrated that authoritarian leadership exerts a detrimental impact on employee performance, organizational commitment, and intention to remain with the organization. However, the results partially diverge from those of Chen et al. [71], who found that while authoritarian leadership may impede work performance through the activation of hindrance stressors, it may simultaneously enhance performance by eliciting challenge stressors, contingent upon the leader’s power distance orientation. Additionally, the laissez-faire leadership style has been consistently associated, across multiple studies, with adverse outcomes such as heightened job stress and workload, diminished job satisfaction and engagement, and ultimately, reduced staff retention rates [72,73,74,75].
Research evidence indicated that toxic leadership is associated with elevated absenteeism, heightened stress levels and increased intentions to leave the organization. In contrast, both transformational and transactional leadership were reflecting higher job satisfaction, enhanced well-being within nursing teams, and reduced staff attrition. [52,57]. A substantial body of research supports these findings, highlighting that both transformational and transactional leadership styles have been frequently associated with higher job satisfaction and lower rates of employee turnover among nursing professionals [76,77,78,79,80,81].
Moreover, toxic leadership behaviors are markedly associated with lower organizational and professional commitment. This relationship is manifested through poor employee performance, reduced psychological empowerment, and heightened job dissatisfaction, which collectively contribute to both organizational and professional withdrawal [50,54,59]. These findings are consistent with the study by Alsadaan et al. [82], which identified a link between toxic leadership and reduced organizational commitment among nurses. Similarly, Mahgob et al. [83] demonstrated that toxic leadership adversely affects staff nurses’ commitment to their professional roles.
Relevant research indicated a strong relationship between toxic leadership and burnout syndrome, comprising its fundamental elements: psychological fatigue, detachment, and reduced feelings of personal efficacy. These effects ultimately contribute to employee withdrawal, primarily driven by diminished job satisfaction, even though some may be more resilient due to emotional investment and professionalism [61,62]. These results are additionally corroborated by Palvimo et al. [84], who reported a positive association concerning destructive leadership, workplace demands, and burnout in nursing personnel. Similarly, Nunes and Palma-Moreira [85] found that toxic leadership contributes to increased burnout syndrome and turnover intentions. Their study also revealed that disengagement partially mediates this relationship.
Another key finding of the present study is that toxic leadership has detrimental effects not only on nurses but also on healthcare organizations. Specifically, it contributes to diminished employee performance, reduced job satisfaction, and weakened extrinsic motivation, all of which adversely impact the quality of organizational services and, ultimately, the institution’s public image [55]. This finding is further supported by the work of Solehudin and Syabanasyah [86], who demonstrated that toxic leadership exerts a negative influence on nurses’ motivation, occupational contentment, output, and staff turnover intentions, ultimately contributing to higher rates of employee attrition. Similarly, Labrague [11] found that toxic nursing leadership is associated with heightened occurrences of adverse events and a decrease in care effectiveness within medical units. Collectively, these studies corroborate the initial conclusion of our study, regarding the detrimental impact of toxic leadership in healthcare organizations.
The study also revealed that counterproductive work behaviors among nurses may serve as a response mechanism to toxic leadership traits, perceived injustice, and experiences of discrimination within the workplace [58]. This finding is further substantiated by multiple studies which have shown that behaviors such as abusive supervision, perceived unfair treatment, and negative management styles directly contribute to an increase in counterproductive work behaviors among nurses. These behaviors are often associated with a rise in adverse events, including patient complaints, medication errors, and healthcare-associated infections. Additionally, affected nurses tend to develop organizational cynicism and harbor negative attitudes towards their work environment [11,87,88,89,90].
5. Limitations and Strengths
This scoping review offers additional evidence regarding the relationship between toxic leadership and nursing staff retention. A key strength of the study lies in its synthesis of findings from multiple countries, thereby providing a comprehensive and globally informed perspective on the issue. Nonetheless, despite the rigorous search and selection strategy employed, it is possible that some relevant studies were excluded, particularly those published in languages other than English. A significant limitation of this review is the regional focus of the studies analyzed, predominantly drawn from Asia and Africa, with limited representation from the United States and Europe. Furthermore, another limitation pertains to cultural factors influencing leadership dynamics, as cultural variations may shape differing responses to toxic leadership behaviors, potentially affecting the generalizability of the findings.
6. Conclusions
Exploring toxic leadership in nursing is critical to enhancing nurse job satisfaction, reducing the incidence of adverse patient outcomes, and improving the overall quality of healthcare delivery. By identifying and addressing toxic behaviors, healthcare organizations can create a more supportive and effective work environment for nurses, increase staff retainment and decrease their intention to leave the profession, ultimately benefiting patient care. By identifying specific negative leadership patterns and their consequences on nursing staff retention, this paper provides evidence recommendations for healthcare administrators aiming to foster healthier, more resilient and sustainable workplace environments.
Author Contributions
E.T., A.S., G.K.: conceptualization, methodology, software, data curation: validation, and writing—original draft preparation. A.S., S.K. and M.M.: writing—reviewing and editing and project administration. E.T., G.K., M.R. and M.K.: writing—reviewing and editing and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Table A1.
Research studies by Author(s), Country, Aim, Data Sample, Study Design, Data Collection and Data Analysis Method and Finding(s).
Table A1.
Research studies by Author(s), Country, Aim, Data Sample, Study Design, Data Collection and Data Analysis Method and Finding(s).
| A/A | Author(s), Year | Country | Aim | Data Sample | Study Design | Data Collection Method | Data Analysis Method | Finding(s) |
|---|---|---|---|---|---|---|---|---|
| 1. | Labrague et al., 2020 [1] |
Philippines | This study examined the influence of toxic and transformational leadership practices on nurses' job satisfaction, psychological distress, absenteeism, and intent to leave the organization or the nursing profession. | 770 | Cross-sectional study | Toxic Leadership Behaviors of Nurse Managers Scale, Global Transformational Leadership , Job Satisfaction Index , Perceived Stress Scale, Two single-item measures developed by O'Driscoll and Beehr, Absenteeism was assessed using a researcher-designed single item question |
SPSS | Toxic leadership increased distress and absenteeism; transformational leadership improved job satisfaction. |
| 2. | Hossny et al., 2023 [2] | Egypt | This study was designed to assess nurses’ perception of the effects of organizational climate and toxic leadership behaviors on their intention to stay and the differences in these domains between the two hospitals studied |
250 | descriptive comparative study |
the organizational climate questionnaire (42 items categorized into nine domains), the toxic leadership scale (30 items categorized into five domains), and the Chinese version of the intent-to-stay scale. |
IBM SPSS Statistics Version 22.0, Microsoft Excel, GraphPad Prism 5 |
Positive organizational climate and supportive systems increased nurses' intention to stay. |
| 3. | Ofei, 2022 [3] | Ghana | This study aimed at assessing the nature and effect of toxic leadership of nurse managers on the perceived job satisfaction and productivity of the nursing workforce. | 943 | Cross-sectional descriptive study | Toxic Leadership Behaviors of Nurse Managers’ Scale, Perceived Productivity Questionnaire, and the Minnesota Satisfaction Questionnaire (MSQ-short version) |
SPSS software version 26 | Toxic leadership reduced nurses' job satisfaction and productivity. |
| 4. | Ramdan and Eid., 2020 [4] | Egypt | This study envisioned to compare toxic leadership among intensive care nursing staff at Tanta University Hospital and El Menshawy hospital and assess its relation to their conflict management style used and organizational commitment at the two hospitals. | 544 | Descriptive, comparative, cross-sectional study | Toxic Leadership Assessment Scale , Conflict Management Styles, Assessment Scale, Organizational Commitment Assessment Scale |
IBM SPSS software package version 20.0. |
Toxic leadership reduced organizational commitment and influenced conflict management styles. |
| 5. | Xueqin Guo et al., 2022 [5] | China | The aim of this study is to explore the perceptions of Chinese registered nurses on toxic leadership behaviors of nurse managers and to determine its type, cause and response measures | 12 | Phenomenological qualitative study | semi-structured in-depth interviews | Colaizzi seven-step analysis method | Nurses working with a transformational leader report higher job contentment and lower intent to leave the nursing profession. Nurses who work for a manager with toxic leadership behaviors demonstrated lower job contentment, higher stress levels, frequent absenteeism and higher intent to leave the nursing profession. |
| 6. | Siyal et al., 2021 [6] | China | The aim of this study is to develop and empirically test a mediation model to examine the indirect impact of abusive supervision on employee performance. |
430 | Empirical, experimental study | The 10-item scale version of the 15-item scale developed by Tepper, 4-item scale validated by Amabile et al., general satisfaction 5-item measure by Hackman and Oldham , the 4-item scale to measure employee performance developed by Liden et al. |
Model development and empirical testing | Abusive supervision reduced employee performance. |
| 7. | Durrah et al., 2024 [7] |
France | The current study aims to examine how toxic management styles can lead to both psychological and physical withdrawal of employees in the healthcare sector | 413 | Quantitative study | Self-developed questionnaire | SmartPLS 3.3.9 |
Toxic leadership increased both psychological and physical withdrawal behaviors |
| 8. | Trepanier et al., 2019 [8] | Canada | The aim of this paper is to investigate the psychological and motivational processes involved in the relationship between two forms of destructive leadership (tyrannical and laissez-faire) and employee health (burnout, affective commitment and job performance) | 399 | Cross-sectional study | The Destructive Leadership Scale, The French version of the Psychological Need Thwarting Scale, The Multidimensional Work Motivation Scale, The Maslach Burnout Inventory General Survey, The occupational commitment questionnaire A self-reported scale consisting of 4 items adapted from the in-role performance subscale of the organizational citizenship behavior scale |
Structural equation modeling analysis. | Tyrannical leadership frustrates autonomy, competence, and relatedness, leading to burnout and lower performance. |
| 9. | Erschens et al., 2022 [9] |
Germany | The aim of this study is to investigate the association of general well-being and different leadership styles among employees in a German tertiary hospital. | 1137 | Cross-sectional study | Module A and D of the standardized Questionnaire on Integrative Leadership, the five-item World Health Organization wellbeing index |
IBM SPSS version 25 |
Transformational and transactional leadership styles are associated with higher well-being scores among hospital employees, while laissez-faire and destructive leadership styles are associated with lower scores across all professional groups. |
| 10. | Low et al., 2019 [10] | Malaysia | The aims of this research are to address the two fundamental research questions: 1) What are the antecedents that lead to counterproductive work behavior (CWB) of nurses in public hospitals? 2) How effective are the moderating roles of power distance orientation (a cultural factor) and locus of control (an individual factor) in impacting CWB? |
337 | Quantitative study | Tepper’s (2000) 15-item abusive supervision Measure, Colquitt’s (2001) 20-item scale 24-item measure adapted from Mitchell and Ambrose (2007) and Bennett and Robinson , six-item scale developed by Dorfman and Howell (1988) and Farh, Hackett and Liang (2007), 16-item Work Locus of Control Scale |
structural equation modeling |
Abusive supervision leads to counterproductive work behavior in nurses |
| 11. | Shipl et al., 2022 [11] | Egypt | This study aimed to investigate the relationship between toxic leadership and nurse followership effectiveness | 343 | Cross-sectional study | The Toxic Leadership Scale and the Followership Styles Questionnaire |
IBM SPSS, version 25 |
Toxic leadership negatively correlated with nurse followership effectiveness |
| 12. | Berma et al., 2021[12] | Egypt | This study aimed to investigate the relationship between workplace toxicity, organizational silence and thriving among nurses. | 235 | descriptive correlational research | Toxic Workplace Environment Questionnaire, Organizational Silence Scale, Thriving at Work Scale |
SPSS version 22.0 |
Workplace toxicity leads to increased organizational silence, reducing thriving among nurses and potentially leading to staff resignation |
| 13. | Bakkal et al., 2019 [13] | Turkey | The aim of this study is to investigate the effects of the toxic leadership of healthcare employees on the turnover intention and the mediating effects of job satisfaction |
658 | cross-sectional descriptive study |
The Toxic Leadership Scale, the Minnesota Job Satisfaction Questionnaire, a turnover intention scale (Rosin & Korabik, 1995 |
Confirmatory Factor Analysis, Structural Equation Model SPSS 24.0 and AMOS 24.0 |
Toxic leadership negatively impacts job satisfaction, which in turn increases turnover intention among healthcare personnel |
| 14. | Budak & Erdal, 2022 [14] | Turkey | The aim of this study is to investigate the mediating effect of burnout syndrome on toxic leadership and job satisfaction |
412 | cross-sectional study | Toxic Leadership Scale, Burnout Scale, Job Satisfaction Scale |
Structural Model Analysis |
Toxic leadership negatively affects job satisfaction and increases burnout syndrome |
| 15. | Mrayyan, 2025 [15] |
Jordan | The aim of this research is to investigate nursing leaders' toxic leadership, nurses' workplace satisfaction, job engagement, and turnover intention in Jordan and whether toxic leadership and sample characteristics predict nurses' work- place satisfaction, job engagement, and turnover intention. |
384 |
cross-sectional study | Toxic Leadership Scale, Nursing Workplace Satisfaction Scale, Job Engagement Scale, Turnover Intention Scale |
Online survey, SPSS program version 25 |
Toxic leadership results in low job satisfaction, stress and emotional exhaustion, and, in turn, decreased quality of nursing care |
| 16. | Labrague, 2024 [16] | Philippines | The aim of this study is to examine the mediating effects of work-family conflict on the relationship between toxic leadership behaviors of nurse managers and psychological distress and work satisfaction among emergency nurses. |
283 | cross-sectional study | Toxic Leadership Behaviors of Nurse Managers Scale, Work-Family Conflict Scale, Job Stress Scale and the Job Satisfaction Index |
Mediation analyses were conducted using the PROCESS Macro with Model 4. |
Toxic leadership reduced work satisfaction and increased psychological distress |
| 17. | Farghaly Abdelaliem & Abou Zeid, 2023 [17] | Egypt | The aim of this study is to assess toxic leadership and organizational performance among nurses of a University Hospital, and explore the mediating effect of nurses ‘silence |
750 |
cross-sectional study |
The toxic leadership scale, the organizational performance questionnaire |
structured equation modeling |
Toxic leadership had a significant negative relationship with organizational performance and the nurses’ silence |
| 18. | Ofei et al., 2023 [18] | Ghana |
The aim of this study is to investigate the mediating role of job satisfaction on toxic leadership and turnover intentions of nurses |
943 |
cross-sectional study |
The Turnover Intention, Minnesota Satisfaction Scale and the Toxic Leadership Behaviors of Nurse Managers’ Scale |
SPSS software version 26, descriptive and differential statistics |
Job satisfaction acts as a mediating factor for toxic leadership behaviour and nurses’ turnover intentions |
References
- Benmira, S.; Agboola, M. Evolution of leadership theory. BMJ Leader 2021, 5, 3–5. [Google Scholar] [CrossRef]
- Rajoria, P.; Sharma, A.; Sharma, M.; Sumaiya, B. Leadership Style and Organisational Success. World Journal of English Language 2022, 12, 71. [Google Scholar] [CrossRef]
- Aydogdu, A.L.F. Exploring Different Aspects of Nursing Leadership: An Integrative Review of Qualitative Studies. Modern Care Journal 2023, 20. [Google Scholar] [CrossRef]
- Scully, N.J. Leadership in nursing: The importance of recognising inherent values and attributes to secure a positive future for the profession. Collegian 2015, 22, 439–444. [Google Scholar] [CrossRef]
- Ćeranić, J.; Peličić, D.; Saveljić, M. Building leadership in nursing practice. Sanamed 2024, 19, 93–99. [Google Scholar] [CrossRef]
- Hashlan, M.A.; et al. Nursing Leadership and Its Impact on Healthcare Quality: A Systematic Review. Journal of Ecohumanism 2024, 3. [Google Scholar] [CrossRef]
- Frazer, C.; Sullivan, D. The nuts & bolts of being a nursing leader. Part 1: Leadership in nursing series. Teaching and Learning in Nursing 2025, 20, 46–48. [Google Scholar] [CrossRef]
- Al-Naemi, I.A. Nursing Leadership Role in Healthcare Transformation – A Critical Overview. Saudi Journal of Nursing and Health Care 2023, 6, 310–312. [Google Scholar] [CrossRef]
- De Rezende, H. How relational leadership can enhance nurses’ well-being and productivity. Nursing Standard 2024, 39, 77–81. [Google Scholar] [CrossRef]
- Atalla, A.D.G.; Mostafa, W.H. Relationship between Toxic Leadership and Work Outcomes: A Cross-sectional Study. Egyptian Journal of Health Care 2023, 14, 199–211. [Google Scholar] [CrossRef]
- Labrague, L.J. Influence of nurse managers’ toxic leadership behaviours on nurse-reported adverse events and quality of care. J Nurs Manag 2021, 29, 855–863. [Google Scholar] [CrossRef]
- Alsadaan, N.; Alqahtani, M. Toxic Leadership in Emergency Nurses: Assessing Abusive Supervision and Its Team-Level Impacts on Conflict Management and Organizational Commitment. J Nurs Manag 2024, 2024, 1–11. [Google Scholar] [CrossRef]
- Labrague, L.J. Toxic leadership and its relationship with outcomes on the nursing workforce and patient safety: a systematic review. Leadership in Health Services 2024, 37, 192–214. [Google Scholar] [CrossRef]
- Schmidt, A.A.; Hanges, P.J. Title of Document: DEVELOPMENT AND VALIDATION OF THE TOXIC LEADERSHIP SCALE.
- Bas, B. Toxic Leadership in Education. International Journal of Educational Administration, Management, and Leadership, pp. 97–104, Nov. 2020. [CrossRef]
- Smith, N.; Fredricks-Lowman, I. Conflict in the workplace: a 10-year review of toxic leadership in higher education. International Journal of Leadership in Education 2020, 23, 538–551. [Google Scholar] [CrossRef]
- Paltu, A.; Brouwers, M. Toxic leadership: Effects on job satisfaction, commitment, turnover intention and organisational culture within the South African manufacturing industry. SA Journal of Human Resource Management 2020, 18. [Google Scholar] [CrossRef]
- Pelletier, K.L. Leader toxicity: An empirical investigation of toxic behavior and rhetoric. Leadership 2010, 6, 373–389. [Google Scholar] [CrossRef]
- Milosevic, I.; Maric, S.; Lončar, D. Defeating the Toxic Boss: The Nature of Toxic Leadership and the Role of Followers. J Leadersh Organ Stud 2020, 27, 117–137. [Google Scholar] [CrossRef]
- Satiani, B.; Satiani, A. Recognizing and Managing a Toxic Leader: A Case Study. Physician Leadersh J 2022, 9, 23–27. [Google Scholar] [CrossRef]
- Arbogast, G.; Jadav, A. Investigating business toxic leadership. Journal of Management and Engineering Integration 2024, 17, 107–116. [Google Scholar] [CrossRef]
- Siddiqui, H.; Iqbal, J. What Happens When a Leader is Toxic? A Qualitative Investigation. Bulletin of Business and Economics (BBE) 2024, 13. [Google Scholar] [CrossRef]
- Gupta, A.; Chawla, S. Toxic Leadership in Workplaces: Insights from Bibliometric, Thematic Analysis, and TCM Framework. International Journal of Organizational Leadership 2024, 13, 179–200. [Google Scholar] [CrossRef]
- Goodin, H.J. The nursing shortage in the United States of America: an integrative review of the literature. J Adv Nurs 2003, 43, 335–343. [Google Scholar] [CrossRef]
- Xie, A.; Duff, J.; Munday, J. Perioperative Nursing Shortages: An Integrative Review of Their Impact, Causal Factors, and Mitigation Strategies. J Nurs Manag 2024, 2024. [Google Scholar] [CrossRef]
- Peters, M. Time to solve persistent, pernicious and widespread nursing workforce shortages. Int Nurs Rev 2023, 70, 247–253. [Google Scholar] [CrossRef]
- van Wyk, S.N.; Naicker, V. A review of the effect of nurse shortages on existing nurse workforces in South Africa and Ukraine. Technology audit and production reserves 2023, 4, 28–32. [Google Scholar] [CrossRef]
- Harmon, M.; et al. How is ‘shortage’ defined? Exploring Nursing Workforce Data across Canada 2015-2022: An Ecological Study. Int J Popul Data Sci 2024, 9. [Google Scholar] [CrossRef]
- Gaboyan, Y.S.; Pivkina, A.I. Nursing staff as a provider of safe and high-quality medical care. Public Health 2022, 2, 35–41. [Google Scholar] [CrossRef]
- Wang, L.; et al. The effect of nurse staffing on patient-safety outcomes: A cross-sectional survey. J Nurs Manag 2020, 28, 1758–1766. [Google Scholar] [CrossRef]
- Griffiths, P.; et al. Nurse staffing and patient outcomes: Strengths and limitations of the evidence to inform policy and practice. A review and discussion paper based on evidence reviewed for the National Institute for Health and Care Excellence Safe Staffing guideline development. Int J Nurs Stud 2016, 63, 213–225. [Google Scholar] [CrossRef]
- Dall’Ora, C.; Saville, C.; Rubbo, B.; Turner, L.Y.; Jones, J.; Griffiths, P. Nurse staffing levels and patient outcomes: a systematic review of longitudinal studies. 2021. [CrossRef]
- Needleman, J.; Liu, J.; Shang, J.; Larson, E.L.; Stone, P.W. Association of registered nurse and nursing support staffing with inpatient hospital mortality. BMJ Qual Saf 2020, 29, 10–18. [Google Scholar] [CrossRef]
- Assaye, A.M.; Wiechula, R.; Schultz, T.J.; Feo, R. Impact of nurse staffing on patient and nurse workforce outcomes in acute care settings in low- and middle-income countries: a systematic review. JBI Evid Synth 2021, 19, 751–793. [Google Scholar] [CrossRef]
- Ball, J.E.; Murrells, T.; Rafferty, A.M.; Morrow, E.; Griffiths, P. ‘Care left undone’ during nursing shifts: associations with workload and perceived quality of care. BMJ Qual Saf 2014, 23, 116–125. [Google Scholar] [CrossRef]
- Griffiths, P.; et al. The association between nurse staffing and omissions in nursing care: A systematic review. J Adv Nurs 2018, 74, 1474–1487. [Google Scholar] [CrossRef]
- Cho, S.; Lee, J.; You, S.J.; Song, K.J.; Hong, K.J. Nurse staffing, nurses prioritization, missed care, quality of nursing care, and nurse outcomes. Int J Nurs Pract, 2020, 26. [CrossRef]
- Ramsey, Z.; Palter, J.; Hardwick, J.; Moskoff, J.; Christian, E.; Bailitz, J. Decreased Nursing Staffing Adversely Affects Emergency Department Throughput Metrics. Western Journal of Emergency Medicine 2018, 19, 496–500. [Google Scholar] [CrossRef]
- Marufu, T.C.; Collins, A.; Vargas, L.; Gillespie, L.; Almghairbi, D. Factors influencing retention among hospital nurses: systematic review. British Journal of Nursing 2021, 30, 302–308. [Google Scholar] [CrossRef]
- Leveck, M.L.; Jones, C.B. The nursing practice environment, staff retention, and quality of care. Res Nurs Health 1996, 19, 331–343. [Google Scholar] [CrossRef]
- Mara, S.O. 121 The factors influencing nursing staff retention in the ICU setting: a scoping review. Ann Work Expo Health 2024, 68 Suppl. 1, 1. [Google Scholar] [CrossRef]
- Conroy, N.; Patton, D.; Moore, Z.; O’Connor, T.; Nugent, L.; Derwin, R. The Relationship between Transformational Leadership and Staff Nurse Retention in Hospital Settings: A Systematic Review. J Nurs Manag 2023, 2023, 1–11. [Google Scholar] [CrossRef]
- Marufu, T.C.; Collins, A.; Vargas, L.; Gillespie, L.; Almghairbi, D. Factors influencing retention among hospital nurses: systematic review. British Journal of Nursing 2021, 30, 302–308. [Google Scholar] [CrossRef]
- Chamanga, E.; Dyson, J.; Loke, J.; McKeown, E. Factors influencing the recruitment and retention of registered nurses in adult community nursing services: an integrative literature review. Prim Health Care Res Dev 2020, 21, e31. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Guo, X.; et al. Chinese nurses’ perceptions on toxic leadership behaviours of nurse managers: A qualitative study. J Nurs Manag 2022, 30, 3256–3263. [Google Scholar] [CrossRef]
- Durrah, O.; Alkhalaf, T.; Sharbatji, O. Toxic leadership as a predictor of physical and psychological withdrawal behaviours in the healthcare sector. J Soc Psychol 2024, 164, 1159–1177. [Google Scholar] [CrossRef]
- BAKKAL, E.; SERENER, B.; MYRVANG, N.A. oxic Leadership and Turnover Intention: Mediating Role of Job Satisfaction. Revista de Cercetare si Interventie Sociala 2019, 66, 88–102. [Google Scholar] [CrossRef]
- Ofei, A.M.A.; Poku, C.A.; Paarima, Y.; Barnes, T.; Kwashie, A.A. Toxic leadership behaviour of nurse managers and turnover intentions: the mediating role of job satisfaction. BMC Nurs 2023, 22, 374. [Google Scholar] [CrossRef]
- Hossny, E.K.; et al. Influence of nurses’ perception of organizational climate and toxic leadership behaviors on intent to stay: A descriptive comparative study. Int J Nurs Stud Adv 2023, 5, 100147. [Google Scholar] [CrossRef]
- Labrague, L.J.; Nwafor, C.E.; Tsaras, K. Influence of toxic and transformational leadership practices on nurses’ job satisfaction, job stress, absenteeism and turnover intention: A cross-sectional study. J Nurs Manag 2020, 28, 1104–1113. [Google Scholar] [CrossRef]
- Ofei, A.M.A.; Paarima, Y.; Barnes, T.; Poku, C.A. Toxic leadership behaviour of nurse managers on perceived job satisfaction and productivity of nursing workforce in sub-Saharan Ghana: A multi-centre cross-sectional study. J Nurs Manag 2022, 30, 2733–2742. [Google Scholar] [CrossRef]
- Ramdan, A.H.A.; Eid, W.M. Toxic Leadership: Conflict Management Style and Organizational Commitment among Intensive Care Nursing Staff. Evidence-Based Nursing Research 2020, 2, 12. [Google Scholar] [CrossRef]
- Siyal, S.; Saeed, M.; Pahi, M.H.; Solangi, R.; Xin, C. They can’t treat you well under abusive supervision: Investigating the impact of job satisfaction and extrinsic motivation on healthcare employees. Rationality and Society 2021, 33, 401–423. [Google Scholar] [CrossRef]
- Trépanier, S.-G.; Boudrias, V.; Peterson, C. Linking destructive forms of leadership to employee health. Leadership & Organization Development Journal 2019, 40, 803–814. [Google Scholar] [CrossRef]
- Erschens, R.; et al. The association of perceived leadership style and subjective well-being of employees in a tertiary hospital in Germany. PLoS One 2022, 17, e0278597. [Google Scholar] [CrossRef]
- Low, Y.M.; Sambasivan, M.; Ho, J.A. Impact of abusive supervision on counterproductive work behaviors of nurses. Asia Pacific Journal of Human Resources 2021, 59, 250–278. [Google Scholar] [CrossRef]
- El Fatah Shipl, A.M.A.; Nabawy, Z.M.; Al anwer Ashour, H.M. The relationship between toxic leadership and nurses’ followership effectiveness. Central European Journal of Nursing and Midwifery 2022, 13, 730–740. [Google Scholar] [CrossRef]
- Berma, A.; Mohamed, H.; Nosier, H. Organizational Silence as a Mediator Factor between Workplace Toxicity and Thriving among Nurses. Assiut Scientific Nursing Journal 2021, 9, 10–20. [Google Scholar] [CrossRef]
- Budak, O.; Erdal, N. The Mediating Role of Burnout Syndrome in Toxic Leadership and Job Satisfaction in Organizations. Southeast European Journal of Economics and Business 2022, 17, 1–17. [Google Scholar] [CrossRef]
- Mrayyan, M.T. Effects of Nursing Leaders’ Toxic Leadership on Nurses’ Workplace Satisfaction, Job Engagement, and Turnover Intention: An Online Cross-Sectional Study. J Adv Nurs, Mar. [CrossRef]
- Labrague, L.J. Linking Toxic Leadership With Work Satisfaction and Psychological Distress in Emergency Nurses: The Mediating Role of Work-Family Conflict. J Emerg Nurs 2024, 50, 670–678. [Google Scholar] [CrossRef]
- Abdelaliem, S.M.F.; Zeid, M.A.G.A. The relationship between toxic leadership and organizational performance: the mediating effect of nurses’ silence. BMC Nurs 2023, 22, 4. [Google Scholar] [CrossRef]
- Lukacik, E.-R.; Bourdage, J.S. Exploring the Influence of Abusive and Ethical Leadership on Supervisor and Coworker-Targeted Impression Management. J Bus Psychol 2019, 34, 771–789. [Google Scholar] [CrossRef]
- Pandey, A.; Nambudiri, R.; Selvaraj, P.; Sadh, A. A temporal study on subordinate’s response to destructive leadership: voice withdrawal as a conflict coping mechanism. International Journal of Conflict Management 2021, 32, 886–911. [Google Scholar] [CrossRef]
- Li, H.; Zhu, J. Destructive Leadership, Employees’ Voice, and Organization. 2016, pp. 205–221. [CrossRef]
- Joseph, S.; Shetty, N. An empirical study on the impact of employee voice and silence on destructive leadership and organizational culture. Asian Journal of Business Ethics 2022, 11, 85–109. [Google Scholar] [CrossRef]
- Kazmi, S.A.; USMANI, S.; Raza, S. Effect of Despotic Leadership on the Employee Work Withdrawal Behavior and Acquiescent Silence. Reviews of Management Sciences 2022, 4, 31–49. [Google Scholar] [CrossRef]
- Schaubroeck, J.M.; Shen, Y.; Chong, S. A dual-stage moderated mediation model linking authoritarian leadership to follower outcomes. . Journal of Applied Psychology 2017, 102, 203–214. [Google Scholar] [CrossRef]
- Chen, L.; Huang, X.; Sun, J.; Zheng, Y.; Graham, L.; Jiang, J. The virtue of a controlling leadership style: Authoritarian leadership, work stressors, and leader power distance orientation. Asia Pacific Journal of Management 2024, 41, 507–547. [Google Scholar] [CrossRef]
- Mousa, W.; EldinFekry, N.; Elewa, A. Relationship between nurse manager leadership style and staff nurses’ work engagement. Egyptian Nursing Journal 2019, 16, 206. [Google Scholar] [CrossRef]
- Berger, R.; Glazer, S.; Leiva, D. Leaders Condition the Work Experience: A Test of a Job Resources-Demands Model Invariance in Two Countries. J Nurs Manag 2023, 2023, 1–11. [Google Scholar] [CrossRef]
- Asiri, A.M.; Mahran, S.M.; Elseesy, N.A. A study of staff nurses’ perceptions of nursing leadership styles and work engagement levels in Saudi general hospitals. International Journal of ADVANCED AND APPLIED SCIENCES 2023, 10, 55–61. [Google Scholar] [CrossRef]
- Pishgooie, A.H.; Atashzadeh-Shoorideh, F.; Falcó-Pegueroles, A.; Lotfi, Z. Correlation between nursing managers’ leadership styles and nurses’ job stress and anticipated turnover. J Nurs Manag 2019, 27, 527–534. [Google Scholar] [CrossRef]
- Specchia, M.L.; et al. Leadership Styles and Nurses’ Job Satisfaction. Results of a Systematic Review. Int J Environ Res Public Health 2021, 18, 1552. [Google Scholar] [CrossRef]
- Bellali, T.; et al. Assessing the Effect of Transactional Leadership and Empowerment on Nursing Staff’s Satisfaction: A Cross-Sectional Study. Florence Nightingale J Nurs 2024, 32, 277–283. [Google Scholar] [CrossRef]
- Suliman, M.; Almansi, S.; Mrayyan, M.; ALBashtawy, M.; Aljezawi, M. Effect of nurse managers’ leadership styles on predicted nurse turnover. Jul. 14, 2020, RCN Publishing Company Ltd. [CrossRef]
- Xie, Y.; Gu, D.; Liang, C.; Zhao, S.; Ma, Y. How transformational leadership and clan culture influence nursing staff’s willingness to stay. J Nurs Manag 2020, 28, 1515–1524. [Google Scholar] [CrossRef]
- Gashaye, M.; Tilahun, D.; Belay, A.; Bereka, B. Perceived Utilization of Leadership Styles Among Nurses. Risk Manag Healthc Policy 2023, 16, 215–224. [Google Scholar] [CrossRef]
- Malak, H.M.; Lorman, W.; Rundio, A.; Simion, D.; Simion, M.G. Predominantly practiced leadership styles of Chief Nursing Officers in healthcare organizations. J Interprof Educ Pract 2022, 28. [Google Scholar] [CrossRef]
- Alsadaan, N.; Alqahtani, M. Toxic Leadership in Emergency Nurses: Assessing Abusive Supervision and Its Team-Level Impacts on Conflict Management and Organizational Commitment. J Nurs Manag 2024, 2024, 1–11. [Google Scholar] [CrossRef]
- Mahgob, G.A.-N.H.; Adam, S.M.A.; El-sayed, S.M. Staff Nurses ’Perception Regarding Toxic Leadership Behavior of Head Nurses and it’s Relation to their Work Engagement. Egyptian Journal of Health Care 2024, 15, 511–524. [Google Scholar] [CrossRef]
- Palvimo, T.; Vauhkonen, A.; Hult, M. The Associations among Destructive Leadership, Job Demands and Resources, and Burnout among Nurses: A Cross-Sectional Survey Study. J Nurs Manag 2023, 2023, 1–10. [Google Scholar] [CrossRef]
- Nunes, A.; Palma-Moreira, A. Toxic Leadership and Turnover Intentions: The Role of Burnout Syndrome. Adm Sci 2024, 14, 340. [Google Scholar] [CrossRef]
- Solehudin, S.; Syabanasyah, I. Impact of toxic leadership on nurses’ motivation, job satisfaction, productivity, and turnover intentions. Journal of Health Science and Medical Therapy 2024, 2, 228–239. [Google Scholar] [CrossRef]
- Zaghini, F.; Fiorini, J.; Piredda, M.; Fida, R.; Sili, A. The relationship between nurse managers’ leadership style and patients’ perception of the quality of the care provided by nurses: Cross sectional survey. Int J Nurs Stud 2020, 101, 103446. [Google Scholar] [CrossRef]
- Ahmed, M.A.O.; Zhang, J.; Fouad, A.S.; Mousa, K.; Nour, H.M. The Dark Side of Leadership: How Toxic Leadership Fuels Counterproductive Work Behaviors Through Organizational Cynicism and Injustice. Sustainability 2024, 17, 105. [Google Scholar] [CrossRef]
- Lapalme, M.; Guerrero, S. How do I stand compared to agency workers? Justice perceptions and employees’ counterproductive work behaviours. J Nurs Manag 2019, 27, 1471–1478. [Google Scholar] [CrossRef] [PubMed]
- KAYANI, M.B.; ALASAN, I.I. Impact of Toxic Leadership on Counterproductive Work Behavior with the Mediating role of Psychological Contract Breach and Moderating role of Proactive Personality. Studies of Applied Economics 2021, 39. [Google Scholar] [CrossRef]
| 1 | The primary search term 'toxic leadership' was systematically expanded to include conceptually related terms such as 'abusive leadership,' 'destructive leadership,' and 'oppressive leadership' to ensure comprehensive coverage of the literature. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



