
Submitted:
25 July 2025
Posted:
29 July 2025
You are already at the latest version
Abstract
Background: The identification of reliable biomarkers for early diagnosis and monitoring of chronic kidney disease (CKD) progression is crucial for improving prognosis and treatment. Neutrophil gelatinase-associated lipocalin (NGAL) is a promising candidate, already validated as a marker for acute kidney injury. This study evaluates NGAL's potential as a biomarker for early diagnosis and monitoring the progression of CKD. Seventy-one patients at CKD stages G1–G4 according to the KDIGO criteria were divided into three groups: Group 1 (eGFR ≥90 mL/min/1.73m²), Group 2 (eGFR 45–89 mL/min/1.73m²), and Group 3 (eGFR 15–44 mL/min/1.73m²). Blood samples were collected and analyzed via standard biochemical and immunological techniques. Serum NGAL levels were measured using ELISA. Results: NGAL levels increased significantly with disease progression and strongly correlated with declining eGFR. Higher NGAL levels were linked to elevated serum creatinine and inflammatory markers, indicating progressive damage to the kidney tissue against the backdrop of persistent systemic inflammation. Conclusions: NGAL demonstrates considerable potential as a biomarker for early detection and monitoring of kidney damage progression. Its use in clinical practice could enrich the traditional methods of diagnosis and monitoring of patients with CKD.
Keywords:
chronic kidney disease (CKD)
; neutrophil gelatinase-associated lipocalin (NGAL)
; biomarkers of kidney disease progression
; chronic systemic inflammation
1. Introduction
The prevalence of chronic kidney disease (CKD) is rising globally, impacting more than 10% of people worldwide [1]. CKD is often asymptomatic in its early stages, making timely diagnosis challenging [2]. Consequently, identifying suitable biomarkers for the early detection of kidney damage and monitoring kidney function could significantly improve patient prognosis [3]. One promising biomarker for assessing kidney function is neutrophil gelatinase-associated lipocalin (NGAL). NGAL has been established as a reliable biomarker for acute kidney injury (AKI) [4,5], but increasing evidence reveals its biomarker potential also for assessing the degree and progression of renal dysfunction in CKD [6].
NGAL is a small secretory glycoprotein belonging to the lipocalin family, which participates in the nonspecific immune response and inflammatory processes. It was originally isolated from human neutrophils in complex with matrix metalloproteinase-9 (MMP-9). NGAL exists as a monomer (25 kDa), a disulfide-linked homodimer (approximately 45 kDa), and in a heterodimeric complex with MMP-9 (135 kDa) [5,7,8]. NGAL is expressed in various organs, including the kidney. Due to its low molecular weight, it is freely filtered through the glomeruli and actively reabsorbed in the proximal tubules, with only a small fraction excreted in the urine. The normal plasma concentration of NGAL ranges from 70 to 104 ng/mL [9]. In cases of renal injury, tubular epithelial cells predominantly secrete the monomeric form of NGAL, whereas neutrophils release the dimeric form, leading to increased levels in both serum and urine [8].
The purpose of this research was to determine the utility of serum NGAL as a biomarker for renal dysfunction progression in predialysis CKD patients.
2. Materials and Methods
2.1. Study Population and Design
This study involved 71 patients in pre-dialysis CKD stages (G1–G4), according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria [10]. The diagnoses included diabetic nephropathy in 20 cases (28%), hypertensive nephropathy in 22 (31%), chronic glomerulonephritis in 8 (11%), chronic pyelonephritis in 14 (20%), chronic interstitial nephritis in 5 (7%), and polycystic kidney disease in 2 (3%).The stage of the disease was determined based on the estimating glomerular filtration rate (eGFR), which was calculated using the Modification of Diet in Renal Disease (MDRD) equation [11]. The study population were divided into three groups – Group 1 (normal or near-normal renal function) included patients with an eGFR ≥ 90 ml/min/1.73 m2 (stage G1), Group 2 (mild to moderately decreased renal function) included patients with a eGFR of 45-89 ml/min/1.73 m2 (stages G2 and G3a), and Group 3 (moderately to severely decreased renal function) included patients with a eGFR of 15-44 ml/min/1.73 m2 (stages G3b and G4). Patients with acute renal failure, end-stage renal disease (stage G5, eGFR <15 ml/min/1.73 m²), liver disease, active inflammatory diseases or infections, as well as those who have undergone kidney transplantation, were excluded from the study. This research was conducted in accordance with the ethical principles for medical research as specified in the Declaration of Helsinki and received approval from the Research Ethics Committee of Medical University-Pleven.
2.2. Biochemical and Immunological Analyses
Blood samples were collected in the morning after overnight fasting and were centrifuged at 2500 rpm for 10 min to separate the serum. The concentrations of serum creatinine (SCr), uric acid (UA), calcium (Ca), inorganic phosphate (Pi), parathyroid hormone (PTH), alkaline phosphatase (ALP), high-sensitivity C-reactive protein (hs-CRP) and interleukin-6 (IL-6) were measured using Roche Cobas E 311 and Cobas E 411 analyzers. NGAL concentrations were measured using enzymelinked immunosorbent assay kit (DLCN20, R&D Systems, USA), according to the manufacturer’s instructions.
2.3. Statistical Analysis
Statistical analyses were conducted using SPSS version 23.0 (SPSS, Inc., Chicago, IL, USA). The normality of data distribution was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Data that followed a normal distribution were analyzed using One-way analysis of variance (ANOVA). If the ANOVA indicated significant differences, Tukey’s HSD post hoc test was performed to identify specific group differences. For data that does not follow a normal distribution, the Kruskal-Wallis test was used for group comparisons, followed by the Mann-Whitney U test for pairwise comparisons. Data are presented as mean ± standard deviation (SD) for variables with a normal distribution, and as median and interquartile range (IQR) for variables with a non-normal distribution. Pearson correlation analysis and Spearman’s rank correlation were used to determine the relationship between parameters. Statistical significance was considered at p < 0.05.
3. Results
3.1. Baseline Patient Characteristics
Statistically significant differences between the groups were observed across multiple parameters that reflect the progression of CKD. Specifically, eGFR markedly decreased from Group 1 to Group 3 (p < 0.001), while SCr and UA levels rose significantly (p < 0.001 and p = 0.010, respectively). Serum Ca levels decreased significantly (p=0.029) from Group 1 to Group 3. This indicates disrupted mineral homeostasis and a potential risk for osteodystrophy in advanced CKD stages. Unlike calcium, phosphate concentrations show a gradual increase with disease severity (p = 0.041). Although the difference is statistically significant, the change is moderate, highlighting impaired phosphate clearance due to declining renal function. PTH levels increased significantly with disease progression (p < 0.001), indicating the development of secondary hyperparathyroidism. ALP levels also increased significantly (p = 0.011), suggesting increased bone turnover and osteopathic activity in advanced CKD stages. A significant rise in hs-CRP was observed from Group 1 to Group 3 (p = 0.009), reflecting increased systemic inflammation associated with disease progression. Additionally, IL-6 levels showed a significant increase across the groups (p = 0.007), indicating heightened inflammatory response. In our study, the detection limit of the IL-6 kit was 1.50 pg/mL, with a reference limit of < 7 pg/mL. The results showed that in the first and second groups, median values were close to or below the detection limit, with minimal increase in the second stage (IQR between 1.50 and 3.21), indicating that the inflammatory response remains moderate and within low levels. In the third group, representing the advanced stage of the disease, IL-6 levels were significantly higher (median 3.08, IQR between 1.50 and 9.46), reflecting increased inflammation with disease progression. Although leukocyte counts increased from Group 1 to Group 3, this difference was not statistically significant (p = 0.340). NGAL levels increased markedly from Group 1 to Group 3 (p < 0.001), demonstrating its potential as a sensitive biomarker for early detection and monitoring of tubular damage in CKD. Overall, these findings suggest that declining GFR is linked to substantial disruptions in mineral balance, increased systemic inflammation, and tubular damage, emphasizing the complex mechanisms underlying CKD progression. All measured parameters for the three groups are presented in Table 1.
3.2. Correlations Between NGAL and Various Clinical and Biochemical Parameters
The correlation analysis revealed significant relationships between NGAL levels and various clinical and biochemical parameters. Notably, NGAL was strongly negatively correlated with eGFR (r = –0.730, p < 0.001), indicating that higher NGAL levels are linked to decreased kidney filtration capacity. Additionally, a significant inverse association was found between NGAL and serum Ca levels (r = –0.334, p = 0.004). Conversely, a strong positive correlation was observed between NGAL and SCr (r = 0.736, p < 0.001), reaffirming the connection between elevated NGAL and impaired renal function. Furthermore, positive relationships emerged between NGAL and age (r = 0.284, p = 0.016), inflammatory markers such as hs-CRP (r = 0.334, p = 0.004), IL-6 (r = 0.509, p < 0.001), and leukocyte count (r = 0.362, p = 0.005). Additional positive associations were observed with Pi (r = 0.265, p = 0.025), UA (r = 0.260, p = 0.029), PTH (r = 0.494, p < 0.001), and ALP (r = 0.370, p = 0.001). Overall, these findings demonstrate that elevated NGAL levels are significantly associated with impaired renal function and systemic inflammation, highlighting its potential as a comprehensive biomarker for kidney injury (Table 2).
4. Discussion
In modern medical practice, the gold standard for assessing renal function is the examination of SCr levels and the calculation of glomerular filtration rate through its renal clearance (GFR). The most commonly used formulas for eGFR are Cockcroft-Gault [12], MDRD [13,14], and CKD-EPI [15]. These methods provide relatively accurate information about kidney function but have a number of limitations and specific features that can affect the interpretation of the results. This can lead to underestimation or overestimation of the extent of kidney damage when GFR is still preserved. In addition to GFR, the condition of the tubules must also be considered. Tubular damage can develop without significant changes in GFR, which means that standard tests may not accurately reflect the extent of kidney injury [16,17]. Creatinine is a breakdown product of muscle metabolism, and its serum levels vary depending on muscle mass, age, and the patient’s gender. Furthermore, transient changes in SCr levels caused by factors such as hydration status, diet, or physical activity can lead to inaccuracies in assessing kidney function [18]. Proteinuria is another classic marker that reflects both the progression of CKD and the risk of cardiovascular complications. However, it also has a number of limitations, including variability of levels, the influence of extrarenal factors (such as infections, febrile states, and physical activity), low sensitivity in early stages, and the inability to fully reflect the degree of kidney damage [19]. Due to these limitations, modern diagnosis of CKD requires an integrated approach, involving not only the assessment of GFR and proteinuria but also the use of new biomarkers that can provide earlier and more accurate detection of tubular and interstitial damage.
Currently, NGAL is recognized as a biomarker for acute kidney injury (AKI). It is secreted by tubular cells both during the destruction phase and during subsequent reparative processes. Levels of NGAL in plasma and urine can increase significantly within the first 2-6 hours after injury, which surpasses the capabilities of traditional markers such as SCr, whose values increase in the following 1-3 days. This characteristic makes NGAL testing a valuable tool for early detection of AKI, especially in high-risk patients, where timely treatment is of primary importance for improving prognosis [9,20]. Based on a detailed analysis of the literature, Di Somma et al. suggest threshold values of NGAL of 150 ng/mL as a cutoff for high sensitivity for predicting AKI and 400 ng/mL as a cutoff for high specificity for diagnosing AKI [21].
Studies in recent years have shown that NGAL is elevated not only in AKI but also in CKD, revealing its potential as a biomarker for the progression of kidney damage [6]. In our study, the analysis of serum NGAL levels in patients with CKD showed that the differences between the groups are statistically significant (p < 0.001). Specifically, NGAL levels in group 3 are almost double those in group 1 and significantly higher than in group 2. The increased NGAL values in group 2 (average 155.35 ng/mL) compared to group 1 (average 113.40 ng/mL) indicate a mild to moderate degree of kidney damage, which corresponds to lower eGFR values (60.94 ± 11.61 mL/min) and higher SCr levels (105.00 µmol/L). In group 3, where eGFR is significantly lower (25.82 ± 9.71 mL/min) and SCr reaches 244.00 µmol/L, NGAL levels are the highest (average 267.80 ng/mL). This underscores its good sensitivity as an early marker for the progression of kidney damage, whose levels increase synchronously with changes in classical indicators of renal dysfunction (Table 1 and Figure 1). Additionally, our results show significant correlations between NGAL and various parameters of kidney function in CKD patients. A significant positive correlation was observed between NGAL and SCr, UA, Pi, PTH, ALP, hs-CRP, IL-6, and leukocytes. A significant negative correlation was found between NGAL and eGFR, as well as with Ca. Our findings confirm that NGAL actively participates in processes of chronic low-grade inflammation, which is a key driver for the development and progression of CKD. Elevated NGAL levels correlate with markers of systemic inflammation such as hs-CRP and IL-6, reflecting ongoing tubular damage and the development of interstitial fibrosis (Table 2).
NGAL is released in response to a number of metabolic and hemodynamic changes such as hyperglycemia, hypertension, and inflammation, which contribute to renal tubular damage and endothelial dysfunction [22]. Tubulointerstitial ischemia and hypoxia associated with these processes play a key role in the pathogenesis of tubular dysfunction. They lead to atrophy of the tubular epithelium and an inflammatory reaction in the peritubular space, resulting in the subsequent development of interstitial fibrosis [23]. These pathological changes are usually irreversible, which further worsens hemodynamics and potentiates glomerular dysfunction. Damage to the renal tubules plays a crucial pathogenic role in the progression of CKD. This is also observed in diseases characterized by primary glomerular damage, such as diabetic nephropathy, IgA nephropathy (IgAN), and kidney involvement in systemic lupus erythematosus (SLE). In these cases, the extent and rate of decline in renal function, as well as the long-term prognosis, are more closely related to the severity of tubulointerstitial damage than to the extent of glomerular lesions.
Several authors report that serum concentrations of NGAL increase in diabetic nephropathy and correlate with the severity of kidney damage [23,24]. It is believed that the increase in NGAL results from tubular damage, which may precede glomerular damage in diabetes. Of particular interest is the fact that elevated NGAL levels in patients with diabetes occur in the earliest stages of kidney damage, even in the absence of albuminuria, indicating the potential of NGAL for early diagnosis of diabetic nephropathy [25]. Ding et al. analyzed the levels of NGAL, creatinine, and N-acetyl-β-D-glucosaminidase (NAG) in urine among 40 healthy participants and 70 patients with IgAN. According to their reported results, NGAL emerges as the most sensitive biomarker for tubular damage in IgAN [26]. This idea is also supported by Rhee et al., who emphasize the prognostic value of serum NGAL levels in IgAN [27]. Chen et al. found that NGAL is highly expressed in CD4+ T cells and kidney tissues and is associated with severe kidney damage in mice with experimental SLE. They demonstrated that NGAL promotes the Th1 inflammatory response, which exacerbates kidney injury. On the other hand, blocking NGAL with specific neutralizing antibodies in SLE-prone mice alleviates the development of nephritis [28]. Obesity is also an important factor in the development and progression of CKD. It is associated with increased blood pressure, insulin resistance, and dyslipidemia, which contribute to kidney tissue damage. Pathological changes in the kidney are linked to mechanisms such as oxidation of low-density lipoprotein (LDL), activation of mesangial cells, and initiation of inflammatory processes that cause damage to both glomeruli and tubules. Mesangial cells in the glomerulus possess receptors for LDL and oxidized LDL, which bind these lipoproteins and induce the production of pro-inflammatory cytokines. This stimulates mesangial proliferation and leads to the development of glomerulosclerosis [29]. A study by Gubina et al. provides experimental data on patients with kidney damage associated with obesity, where serum NGAL is elevated and correlates with markers of lipid imbalance and tubular injury [30].
Experimental models and human studies show that serum NGAL levels are elevated early and in CKD with predominantly tubular and interstitial involvement. For example, in models of nephron reduction and autosomal dominant polycystic kidney disease (ADPKD), NGAL levels rise even before histological lesions develop in the tubular epithelial cells. These elevated levels correlate with tubular proliferation, cyst formation, and fibrosis [31]. Elevated NGAL levels correlate with tubular lesions and interstitial fibrosis, which are key features of hypertensive kidney damage. Interesting results are provided by Danquah et al., who, comparing 140 hypertensive patients with healthy controls, found that plasma NGAL levels were significantly increased in hypertensive individuals. This increase reflects early kidney damage associated with hypertension, even when SCr levels are still within normal ranges [32]. In another study, Song et al. concluded that higher circulating NGAL levels correlate with higher blood pressure and insulin resistance, which are associated with increased oxidative stress, endothelial dysfunction, and inflammation [33].
Our study also demonstrates the presence of a direct relationship between NGAL, PTH, Ca, and Pi levels, suggesting a new, unique mechanism associated with the development of mineral bone disease in CKD (CKD-MBD) (Table 2). In recent years, scientific research has focused on the role of NGAL in bone metabolism, particularly its influence on the activity of osteoblasts and osteocytes, related to the production of fibroblast growth factor-23 (FGF23). It is possible that NGAL enhances the effects of FGF23-dependent pathways, which may represent an additional mechanism linking tubular damage with systemic mineral and bone disorders [34]. Elevated NGAL levels in CKD are generally associated with more severe inflammation and damage to the renal tubules, which affects their regulatory capacity. This process may contribute to disturbances in phosphate secretion and vitamin D activation, thereby promoting calcium-phosphorus imbalance. Furthermore, NGAL may participate in the regulation of cellular proliferation and apoptosis within kidney tissues, which could also influence the kidney’s ability to maintain mineral homeostasis [35,36].
Our results also showed that as age increases, NGAL levels rise. This is likely related to age-related changes in kidney function and a higher prevalence of chronic inflammatory processes or other conditions associated with aging (Table 2).
In summary, it can be said that NGAL complements and improves classical kidney tests such as SCr, eGFR, and proteinuria, by providing more accurate information about kidney damage, especially in the early stages of CKD. While creatinine and eGFR reflect glomerular function and change later during disease progression, NGAL responds already in the initial stages of tubular damage, before significant changes occur in standard markers. Furthermore, NGAL is associated with tubular and interstitial pathology, inflammatory processes, and metabolic disturbances that are not reflected by classical tests. Thus, it enhances diagnosis as a sensitive early marker for tubular dysfunction and progression in CKD patients. In the context of pathogenetic therapy, especially in immune-mediated nephropathies affecting the glomeruli, it is important to use a marker that also reflects tubular damage, since suppressing the pathological process in the glomeruli does not always guarantee the halting of damage processes in the tubules and interstitium. This is especially important because, through non-immune mechanisms, tubular atrophy and fibrosis can develop, which continue to damage the kidney even after controlling glomerular inflammation. Therefore, using NGAL as an early marker for tubular and interstitial damage is essential for more accurate monitoring and management of CKD, improving early diagnosis and opportunities for timely therapy.
A strength of our study is that it demonstrates the role of NGAL as a biomarker for early diagnosis and monitoring of CKD progression. Currently, there are few similar studies on this topic, which underscores the significance and originality of our findings. A limitation is the small size of the study group, highlighting the need for larger future studies.
5. Conclusions
Our results clearly show that NGAL is a sensitive and early biomarker for renal damage in CKD patients. NGAL levels increase significantly with disease progression, with the highest values observed in the more advanced stages. Additionally, we found significant correlations between NGAL and markers of kidney damage and inflammation, highlighting its role as a sensitive indicator of tubular dysfunction and systemic inflammation. These data suggest that NGAL can be used for both early diagnosis and monitoring of CKD progression and its associated systemic complications, including disturbances in mineral balance and bone metabolism.
Author Contributions
Conceptualization, B.I., K.K.; methodology, K.K., B.I. and A.B.; software, K.K., T.S. and A.B.; validation, B.I., K.K.; formal analysis, B.I., K.K.; investigation, B.I., K.K., T.E., T.S. and A.B.; resources, K.K., B.I., T.E., T.S. and A.B.; data curation, B.I., K.K., T.E. and T.S.; writing—original draft preparation, B.I., K.K.; writing—review and editing, K.K., B.I.; visualization, T.S., K.K. and B.I.; project administration, K.K. and B.I. All authors have read and agreed to the published version of the manuscript.
Funding
The APC was funded by Medical University-Pleven, Bulgaria.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Research Ethics Committee of Medical University Pleven (IRB approval No. 797-REC/21 June 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The authors confirm that the data supporting the findings of this report are available within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.R. Global prevalence of chronic kidney disease–a systematic review and meta-analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- Francis, A.; Harhay, M.N.; Ong, A.C.; Tummalapalli, S.L.; Ortiz, A.; Fogo, A.B.; Fliser, D.; Roy-Chaudhury, P.; Fontana, M.; Nangaku, M. Chronic kidney disease and the global public health agenda: An international consensus. Nat. Rev. Nephrol. 2024, 20, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Wetterstrand, V.J.R.; Schultz, M.; Kallemose, T.; Torre, A.; Larsen, J.J.; Friis-Hansen, L.; Brandi, L. Plasma neutrophil gelatinase-associated lipocalin as a single test rule out biomarker for acute kidney injury: A cross-sectional study in patients admitted to the emergency department. PLoS ONE 2025, 20, e0316897. [Google Scholar] [CrossRef]
- Virzì, G.M.; Morisi, N.; Oliveira Paulo, C.; Clementi, A.; Ronco, C.; Zanella, M. Neutrophil Gelatinase-Associated Lipocalin: Biological Aspects and Potential Diagnostic Use in Acute Kidney Injury. J. Clin. Med. 2025, 14, 1570. [Google Scholar] [CrossRef] [PubMed]
- Romejko, K.; Markowska, M.; Niemczyk, S. The review of current knowledge on neutrophil gelatinase-associated lipocalin (NGAL). Int. J. Mol. Sci. 2023, 24, 10470. [Google Scholar] [CrossRef]
- Kjeldsen, L.; Johnsen, A.H.; Sengeløv, H.; Borregaard, N. Isolation and primary structure of NGAL, a novel protein associated with human neutrophil gelatinase. J. Biol. Chem. 1993, 268, 10425–10432. [Google Scholar] [CrossRef]
- Cai, L.; Rubin, J.; Han, W.; Venge, P.; Xu, S. The origin of multiple molecular forms in urine of HNL/NGAL. Clin. J. Am. Soc. Nephrol. 2010, 5, 2229–2235. [Google Scholar] [CrossRef] [PubMed]
- Bourgonje, A.R.; Abdulle, A.E.; Bourgonje, M.F.; Kieneker, L.M.; la Bastide-Van Gemert, S.; Gordijn, S.J.; Hidden, C.; Nilsen, T.; Gansevoort, R.T.; Mulder, D.J. Plasma neutrophil gelatinase-associated lipocalin associates with new-onset chronic kidney disease in the general population. Biomolecules 2023, 13, 338. [Google Scholar] [CrossRef]
- Foundation, N.K. KDOQI clinical practice guideline for diabetes and CKD: 2012 update. Am. J. Kidney Dis. 2012, 60, 850–886. [Google Scholar] [CrossRef]
- Eddy, A.A.; Neilson, E.G. Chronic kidney disease progression. J. Am. Soc. Nephrol. 2006, 17, 2964–2966. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Gault, H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D.; Group*, M.o.D.i.R.D.S. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.; Hendriksen, S.; Kusek, J.W.; Van Lente, F.; Collaboration*, C.K.D.E. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro III, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Perazella, M.A.; Rosner, M.H. Drug-induced acute kidney injury. Clin. J. Am. Soc. Nephrol. 2022, 17, 1220–1233. [Google Scholar] [CrossRef]
- Obert, L.A.; Elmore, S.A.; Ennulat, D.; Frazier, K.S. A review of specific biomarkers of chronic renal injury and their potential application in nonclinical safety assessment studies. Toxicol. Pathol. 2021, 49, 996–1023. [Google Scholar] [CrossRef]
- Ávila, M.; Mora Sánchez, M.G.; Bernal Amador, A.S.; Paniagua, R. The Metabolism of Creatinine and Its Usefulness to Evaluate Kidney Function and Body Composition in Clinical Practice. Biomolecules 2025, 15, 41. [Google Scholar] [CrossRef]
- Glassock, R.J.; Warnock, D.G.; Delanaye, P. The global burden of chronic kidney disease: Estimates, variability and pitfalls. Nat. Rev. Nephrol. 2017, 13, 104–114. [Google Scholar] [CrossRef]
- Cho, S.Y.; Hur, M. New Issues With Neutrophil Gelatinase-associated Lipocalin in Acute Kidney Injury. Ann. Lab. Med. 2023, 43, 529–530. [Google Scholar] [CrossRef] [PubMed]
- Di Somma, S.; Magrini, L.; De Berardinis, B.; Marino, R.; Ferri, E.; Moscatelli, P.; Ballarino, P.; Carpinteri, G.; Noto, P.; Gliozzo, B. Additive value of blood neutrophil gelatinase-associated lipocalin to clinical judgement in acute kidney injury diagnosis and mortality prediction in patients hospitalized from the emergency department. Crit. Care 2013, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, X.; Shengbu, M.; Shi, Q.; Jiaqiu, S.; Lai, X. Biomarkers: New Advances in Diabetic Nephropathy. Nat. Prod. Commun. 2025, 20, 1934578X251321758. [Google Scholar] [CrossRef]
- Kaul, A.; Behera, M.; Rai, M.; Mishra, P.; Bhaduaria, D.; Yadav, S.; Agarwal, V.; Karoli, R.; Prasad, N.; Gupta, A. Neutrophil gelatinase-associated lipocalin: As a predictor of early diabetic nephropathy in type 2 diabetes mellitus. Indian J. Nephrol 2018, 28, 53–60. [Google Scholar] [CrossRef]
- Prashant, P.; Dahiya, K.; Bansal, A.; Vashist, S.; Dokwal, S.; Prakash, G. Neutrophil Gelatinase-Associated Lipocalin (NGAL) as a potential early biomarker for diabetic nephropathy: A meta-analysis. Int. J. Biochem. Mol. Biol. 2024, 15, 1. [Google Scholar] [CrossRef]
- Bolignano, D.; Lacquaniti, A.; Coppolino, G.; Donato, V.; Fazio, M.R.; Nicocia, G.; Buemi, M. Neutrophil gelatinase-associated lipocalin as an early biomarker of nephropathy in diabetic patients. Kidney Blood Press. Res. 2009, 32, 91–98. [Google Scholar] [CrossRef]
- Ding, H.; He, Y.; Li, K.; Yang, J.; Li, X.; Lu, R.; Gao, W. Urinary neutrophil gelatinase-associated lipocalin (NGAL) is an early biomarker for renal tubulointerstitial injury in IgA nephropathy. Clin. Immunol. 2007, 123, 227–234. [Google Scholar] [CrossRef]
- Rhee, H.; Shin, N.; Shin, M.J.; Yang, B.Y.; Kim, I.Y.; Song, S.H.; Lee, D.W.; Lee, S.B.; Kwak, I.S.; Seong, E.Y. High serum and urine neutrophil gelatinaseassociated lipocalin levels are independent predictors of renal progression in patients with immunoglobulin A nephropathy. Korean J. Intern. Med. 2015, 30, 354. [Google Scholar] [CrossRef]
- Chen, W.; Li, W.; Zhang, Z.; Tang, X.; Wu, S.; Yao, G.; Li, K.; Wang, D.; Xu, Y.; Feng, R. Lipocalin-2 exacerbates lupus nephritis by promoting Th1 cell differentiation. J. Am. Soc. Nephrol. 2020, 31, 2263–2277. [Google Scholar] [CrossRef]
- Schuchardt, M.; Tölle, M.; van der Giet, M. High-density lipoprotein: Structural and functional changes under uremic conditions and the therapeutic consequences. Handb. Exp. Pharmacol. 2015, 423–453. [Google Scholar]
- Gubina, N.V.; Kupnovytska, I.H.; Romanyshin, N.M.; Mishchuk, V.H. Lipocalin level and indicators of lipid metabolism in the initial stages of chronic kidney disease against the background of obesity. Clin. Pract. 2023, 20, 1–9. [Google Scholar]
- Viau, A.; El Karoui, K.; Laouari, D.; Burtin, M.; Nguyen, C.; Mori, K.; Pillebout, E.; Berger, T.; Mak, T.W.; Knebelmann, B. Lipocalin 2 is essential for chronic kidney disease progression in mice and humans. J. Clin. Invest. 2010, 120, 4065–4076. [Google Scholar] [CrossRef] [PubMed]
- Danquah, M.; Owiredu, W.K.; Jnr, B.E.; Serwaa, D.; Odame Anto, E.; Peprah, M.O.; Obirikorang, C.; Fondjo, L.A. Diagnostic value of neutrophil gelatinase-associated lipocalin (NGAL) as an early biomarker for detection of renal failure in hypertensives: A case–control study in a regional hospital in Ghana. BMC Nephrol. 2023, 24, 114. [Google Scholar] [CrossRef]
- Song, E.; Fan, P.; Huang, B.; Deng, H.B.; Cheung, B.M.Y.; Félétou, M.; Vilaine, J.P.; Villeneuve, N.; Xu, A.; Vanhoutte, P.M. Deamidated lipocalin-2 induces endothelial dysfunction and hypertension in dietary obese mice. J. Am. Heart Assoc. 2014, 3, e000837. [Google Scholar] [CrossRef]
- Courbon, G.; Francis, C.; Gerber, C.; Neuburg, S.; Wang, X.; Lynch, E.; Isakova, T.; Babitt, J.L.; Wolf, M.; Martin, A. Lipocalin 2 stimulates bone fibroblast growth factor 23 production in chronic kidney disease. Bone Res. 2021, 9, 35. [Google Scholar] [CrossRef]
- Han, M.; Li, Y.; Wen, D.; Liu, M.; Ma, Y.; Cong, B. NGAL protects against endotoxin-induced renal tubular cell damage by suppressing apoptosis. BMC Nephrol. 2018, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Steflea, R.M.; Stoicescu, E.R.; Aburel, O.; Horhat, F.G.; Vlad, S.V.; Bratosin, F.; Banta, A.M.; Doros, G. Evaluating Neutrophil Gelatinase-Associated Lipocalin in Pediatric CKD: Correlations with Renal Function and Mineral Metabolism. Pediatr. Rep. 2024, 16, 1099–1114. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Comparison of the NGAL levels between the three groups. p < 0.05, statistically significant.
Figure 1.
Comparison of the NGAL levels between the three groups. p < 0.05, statistically significant.
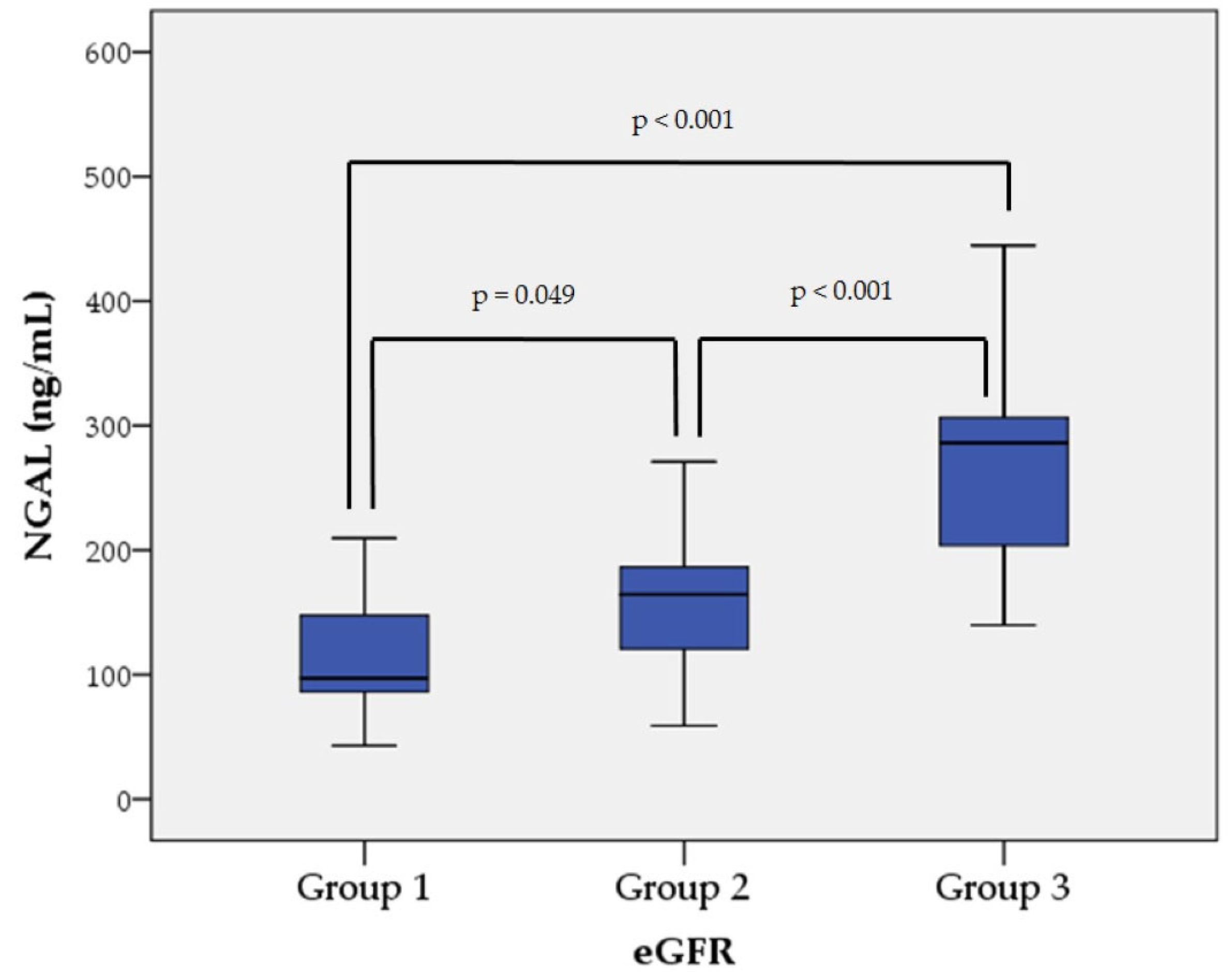

Table 1.
Characteristics of patients in the study groups.
| Variables | Group 1 (n=16) |
Group 2 (n=33) |
Group 3 (n=22) |
p-Value |
|---|---|---|---|---|
| Male/Female (n/n) | 5/11 | 23/10 | 11/11 | |
| Age (years) 1 | 48.81 ± 16.97 | 67.03 ± 9.69 | 68.09 ± 11.48 | <0.001 |
| eGFR (mL/min) 1 | 102.31 ± 11.75 | 60.94 ± 11.61 | 25.82 ± 9.71 | <0.001 |
| SCr (µmol/L) 2 | 61.00 (59.25-78.75) | 105.00 (91.50-131.50) | 244.00 (164.50-281.25) | <0.001 |
| UA (µmol/L) 1 | 275.00 ± 80.73 | 340.15 ± 71.44 | 351.86 ± 78.62 | 0.010 |
| Ca (mmol/L) 1 | 2.42 ± 0.11 | 2.39 ± 0.09 | 2.32 ± 0.15 | 0.029 |
| Pi (mmol/L) 1 | 1.11 ± 0.15 | 1.15 ± 0.20 | 1.28 ± 0.27 | 0.041 |
| PTH (pg/mL) 2 | 21.77 (17.89-34.92) | 29.10 (20.38-41.92) | 61.73 (32.80-130.80) | <0.001 |
| ALP (U/L) 1 | 74.38 ± 25.51 | 73.58 ± 19.79 | 94.32 ± 33.06 | 0.011 |
| hs-CRP (mg/L) 2 | 1.50 (1.13-2.96) | 2.97 (2.31-5.60) | 3.72 (2.47-10.55) | 0.009 |
| IL-6 (pg/mL) 2 | 1.50 (1.50-1.50) | 1.50 (1.50-3.21) | 3.08 (1.50-9.46) | 0.007 |
| WBC (G/L) 2 | 7.40 (5.70-10.40) | 7.85 (6.73-8.67) | 8.40 (7.10-10.15) | 0.340 |
| NGAL (ng/mL) 1 | 113.40 ± 46.47 | 155.35 ± 50.18 | 267.80 ± 72.50 | <0.001 |
1 mean ± SD; 2 median and IQR. Abbreviations: eGFR, estimating glomerular filtration rate; SCr, serum creatinine; UA, uric acid; Ca, calcium; Pi, inorganic phosphate; PTH, parathyroid hormone; ALP, alkaline phosphatase; hs-CRP, high-sensitivity c-reactive protein; IL-6, interleukin-6; WBC, white blood cell count; NGAL, neutrophil gelatinase-associated lipocalin. p < 0.05, statistically significant.
Table 2.
Correlations of NGAL with key clinical and biochemical parameters.
| Correlations | Correlation Coefficient |
p-Value |
|---|---|---|
| NGAL and Age | 0.284 * | 0.016 |
| NGAL and eGFR | –0.730 ** | <0.001 |
| NGAL and SCr | 0.736 ** | <0.001 |
| NGAL and UA | 0.260 * | 0.029 |
| NGAL and Ca | –0.334 ** | 0.004 |
| NGAL and Pi | 0.265 * | 0.025 |
| NGAL and PTH | 0.494 ** | <0.001 |
| NGAL and ALP | 0.370 ** | 0.001 |
| NGAL and hs-CRP | 0.334 ** | 0.004 |
| NGAL and IL-6 | 0.509 ** | <0.001 |
| NGAL and WBC | 0.362 ** | 0.005 |
* Correlation is significant at the 0.05 level, ** Correlation is significant at the 0.01 level. Abbreviations: NGAL, neutrophil gelatinase-associated lipocalin; eGFR, estimating glomerular filtration rate; SCr, serum creatinine; UA, uric acid; Ca, calcium; Pi, inorganic phosphate; PTH, parathyroid hormone; ALP, alkaline phosphatase; hs-CRP, high-sensitivity c-reactive protein; IL-6, interleukin-6; WBC, white blood cells.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



