Submitted:
24 July 2025
Posted:
25 July 2025
You are already at the latest version
Abstract
Background: Proximal hamstring tendinopathy (PHT) is a debilitating musculoskeletal condition characterized by severe pain in the posterior thigh. It is very common in athletes subjected to repetitive hamstring muscle contractions, such as runners and other athletes. This condition can impact the athlete's performance, limiting high-level athletic activity. Return to sport (RTS) becomes a medical, physical, athletic, and economic necessity. Conservative approaches for PHT treatments include various options, such as: physiotherapy, corticosteroids, plasma-rich-platelet shockwave therapy and collagen. Porcine collagen demonstrated to be a validated option for tendinopathies treatment, however no one studies of porcine collagen application in PHT were reported. Aim of present study is to evaluate the efficacy of porcine collagen injection in athletes, affected by PHT. Methods: Twenty-height athletes were included in the study and randomly sorted in two arms of treatment: COL I (porcine collagen injection) and REHAB (rehabilitation program). Victorian Institute of Sport Assessment (VISA questionnaire) Hamstring (-H) questionnaire and RTS time, were quantitatively evaluated in order to found the significant difference between the treatments (COL I vs REHAB). Results: The two group of treatment were very homegenius and showed parametric distribution concerning the biological and pathophysiological conditions. The mean times to RTS were 57 and 72 days for COL I and REHAB, respectively (p=0.0083). The VISA-H results revealed a better condition in COL I treatment with respect to REHAB (p<0.0001) and the Long-Rank test showed a higher odd ratio (HR) to RTS equal to 5.35 (p=0.0008) for COL I athletes. Finally, the COL I treatment seems to uniform the response to treatment batter than REHAB. Conclusions: This Study seems to demonstrate the usefulness of COL I treatment in PHT athletes. A largest cohort of athletes might be necessary to harvest better information about the conservative treatment in PHT pathology.
Keywords:
porcine collagen Injection therapy
; hamstring injury
; athletes
; return to sport
; VISA-H score
; efficacy
; safety
1. Introduction
The Hamstring strain injuries (HSI) are quite common in several sports disciplines and account for 1.2-4 injuries per 1000 hours of athlete exposure to sports activity [1,2]. The main symptom of proximal hamstring tendinopathy (PHT) is lower gluteal pain, especially during running or prolonged sitting [2,3,4,5]. When athletes express acute pain in the posterior thigh, following a mechanical stimulus, often sudden (typical of Hamstring Strain Injury; HSI), the clinical examination is primarily focused on the rehabilitation needs in order to perform the return to sport (RTS), rather than the search for the true diagnosis, leaving ample space for the problem of prognosis and the athlete's "post-traumatic shock syndrome" [6,7,8]. However, athletes who present pain in the posterior thigh require a differential diagnosis to confirm or exclude the presence of pathologies typical of this type of injury which include: Proximal hamstring tendon avulsion, Proximal hamstring tendinopathy, Lumbar spine radiculopathy and adductor muscle injury [6]. The causes triggering the HSI event are often controversial and it is often unclear whether the traumatic event occurs following a repeated and accumulated microscopic muscle damage or in response to a single (distinct) event that goes beyond the physic-mechanical limits of the biological muscle-tendon structure [9]. HSI can also result from a constant wear of the tissue integrity associated with repeated damage over time, leaving the athlete vulnerable to a triggering and therefore harmful sporting event. While, in other words, the HSI can be caused by a single or another macro-traumatic event (independent with the athlete's muscular integrity, for example, a hip flexion). By the way, the mechanisms that lead to the formation of a type HSI lesion probably involve a combination of several factors that include: (A) a high load of high forces on the muscle-tendon unit, (2) an excessive elongation compared to the structure of the muscle-tendon unit and (3) execution of high-velocity movements (e.g. sudden sprints) [5,10]. There are several medical classification systems for muscle injuries. In addition these classification methods are 10 years old or more (O'Donoghue, Jackson, Takebayashi, Peetrons, Ryan, Durey and Rodineau, Stoller, Cohen, Chan, etc.) [11], indeed, several expert groups have recently developed new classification systems. These include:
- The Munich consensus statement [12], which differentiates, among indirect muscle injuries, functional disorders (type 1a = fatigue-induced functional disorders; type 1b = delayed onset muscle soreness – DOMS; types 2a and 2b = neuromuscular disorders of central or peripheral origin) and structural lesions (type 3a = minor partial muscle injury; type 3b = moderate partial injury; type 4 = (sub) total muscle ruptures and tendon avulsions).
- The British Athletics Muscle Injury Classification (BAMIC) [13], proposes to associate, on the one hand, the extent of the injury according to 5 progressive lesion stages based on magnetic resonance imaging (stage 0 = DOMS; stage 1 = minimal lesion in terms of longitudinal dimensions of the injury and percentage of fibers involved; stage 2 = moderate lesion; stage 3 = extensive lesion; stage 4 = complete lesion) and, on the other hand, the site of the lesion (a = myofascial; b = muscular/musculotendinous; c = intratendinous).
- The acronym MLG-R, resulting from a collaboration between FC Barcelona and “Aspetar”, this classification refers to the use of four letters: M for mechanism of injury (direct, indirect “sprinting-type” or indirect “stretching-type”), L for location (proximal, middle or distal third of the muscle), G for grade (lesion stages 0 to 3) and R for number of recurrences (0 = first episode; 1 = first recurrence) [14].
A recent DELPHI consensus reported that specialists in the field used classification systems for hamstring injuries, as follows: BAMIC (58%), Munich Consensus (12%), and the Barcelona Consensus (6%) [15]. This round-table assessed the most important following points. Here, we are reporting three of them that might touch the important key aspect of HSI in athletics management.
- While there are three major classification systems for hamstring (HSI) injuries that incorporate anatomical and imaging criteria, these classification systems are not specific to any individual athlete's individual muscle injuries.
- Specialists most frequently use the British Athletics Muscle Injury Classification (BAMIC) system, but the Munich and Barcelona systems are also considered valid for the classification of musculoskeletal injuries (HSI).
- The expert panel reports that MRI is the recommended diagnostic test, while few use diagnostic ultrasound. However, neither is recommended for monitoring rehabilitation progress or assessing readiness to return to sports (RTS).
However, in this document the expert opinion concludes that there is a need for more research into the effectiveness of classification systems to prognosticate and guide for treatment decision choice [15]. Traditional treatment methods for PHT are by the majority comparable to those of other tendinopathies: they include rest and ice for symptoms relief in the initial phase [16], reduction or pause of sports activity [17], non steroidal anti-inflammatory drugs (NSAIDs) [18], physiotherapy and continuous home exercise program focusing on progressive eccentric hamstring strengthening and core stabilization [6,19,20,21]. Novel therapeutic approaches are recognized including: shockwave therapy (SWT) [22], ultrasound (US) therapy [23,24], ultra-sound-guided corticosteroid injection [25,26], Platelet rich plasma (PRP) injection [27,28,29] and collagen injection [30,31]. S-guided corticosteroid injection of the tendons heath is used in PHT [32], however detrimental effects such as slowed long-term tissue healing caused by inhibition of collagen linkage, incomplete healing and recurrent injury have been reported [33]. Additionally, symptoms often recur after initial good short-term results [9]. Furthermore, SWT [22] , US-therapy [23,24] and PRP injection demonstrated positive effects against the pathology spanning across 2-4 months of applications [27,28,29]. Tendinopathy is a chronic, painful tendon disease characterized by histological modifications such as disorganization of collagen (COL) [34] and the mechanical properties of tendons are based on the structure and composition of the extracellular matrix (ECM), which consists mainly of type I collagen [35]. The content of type I fibers, inside the tendons, play a pivotal role in remodeling the ECM and to increase the physic characteristic of tendons. Tenocytes support the mechanical adaptation of tendons by adapting to the mechanical stimuli imposed during loading, thus influencing the homeostasis of the extracellular matrix (ECM). Overall, type I collagen acts as a mechanical scaffold, constituting an effective therapeutic and regenerative tool to promote tendon healing in tendinopathies. [36]. Randelli et Al. demonstrated the effectiveness of porcine collagen in tenocytes in vitro, in which tenocytes cultured in a porcine collagen environment, showed an increased proliferation rate and migration potential toward the site of lesion [35,37]. While, recent evidences, demonstrated a positive effects of porcine collagen injections in orthopedic field, against the greater trochanter pain syndrome (GTPS) [35,38]. Nevertheless, other studies revealed the efficacy of collagen injection therapy in musculoskeletal disorders in a short time-frame [39,40,41]. Other studies showed the positive effects of porcine collagen in reducing the tendinopathies [42] and increased the body muscle strength [43]. Several positive effects were documented above by collagen applications representing a novel biological approach to treat tendinopathies and musculotendinous reconstructions; they are also considered a cost effective, easy to use and a regenerative solution [44].
Indeed, the Time to RTS, for athletes and their medical staff represent the main goal because of the an excessive extension of RTS, affect the psychological behaviors, the performance of athletes and the economic impact of sportive teams [45].
The Purpose of the present case series analyses is to compare the efficacy of the ultrasound-guided injection of porcine collagen treatment, in the sportive professionals affected by PHT, with respect to physiotherapy alone.
2. Materials and Methods
2.1. General Aspects and Eligibility Criteria
Data were acquired during the time frame of treatment. Data acquisition was performed by the authors (S.R. and M.B.) in order to build an “ad hoc” database including clinical and anonymized personal data. An encrypted code was associated at the beginning of this phase of the study allowed to maintain the anonymity of the patients. For data collection, the patients satisfied the following eligibility criteria:
- Clinical and MRI-confirmed diagnosis of proximal biceps femur tendinopathy.
- Age between 18 and 50 years.
- Acute symptoms present for less than 3 months.
- Active or athletic individuals.
- Subject had not previously undergone reconstructive or conservative surgical treatments.
- They had not benefited from infiltrative and/or other conservative treatment.
- They had no other concomitant pathologies within PHT.
- They completed treatment with MD-Muscle (Guna spa, Milano, Italy).
The exclusion criteria include:
- Complete tendon tears.
- Previous local injections or regenerative treatments.
- Rheumatologic or neurologic comorbidities.
- Known allergy to collagen or components of the product.
- Refusal to sign consent or poor compliance with follow-up.
2.1. Data Assessment
All data procedures were performed in agreement with the legal standards of human data manipulation as per the Helsinki Declaration of 1975, updated in 2000 and 2008. The patient data employed for clinical evaluation concerned a total of 2 visits (T0 and T1). The T1 visit, represent the final point for results harvesting. Them were compared with respect to the baseline data acquisition (T0). All patients included in the database first signed, their informed consent; after that, the treatments were performed.
2.1. Treatment and Technical Procedure
In this case series there two groups of intervention:
(COL I; Collagen) The patient inside this group received 2 weekly ultrasound-guided injections of 4 ml MD-Muscle (porcine collagen, GUNA), in addition to an individualized rehabilitation program. (REHAB; Control group) The patient inside this group received rehabilitation program only. All COL patients received the injection of the collagen in the proximal biceps femur tendon through Ultrasound-guided injection with 21G needle (23mm in length). Before the injection of the product, the target area was disinfected with alcohol or another antiseptic solution. The treatments consisted of 1 administration of 4 ml (2 vials) of porcine collagen. The procedures were performed by a specialist of musculoskeletal pathologies, using the ultrasound machine. The correct deposition confirmed via ultrasound and MRI imaging (Figure 1).
2.4. Follow-Up and Score Evaluation the Follow-Up Duration
The duration of the follow-up was evaluated until the time of suitability for the return to sports activity. In any case, the follow-up was established for a period of no less than 56 days, i.e. 8 weeks. The assessment of the clinical status of the athletes was assessed through the Victorian Institute of Sport Assessment (VISA questionnaire) Hamstring (-H) Questionnaire is a self-report clinical outcome measure used in patients with proximal Hamstring tendinopathy (PHT) [46]. It consists of eight questions that measure the domains of pain, function in daily life and sporting activities. This assessment was performed at baseline, before the start of treatment (T0) and at least 8 weeks after treatment. On a weekly basis, the athletes clinical conditions were monitored by evaluating the following biophysical parameters, as well: pain, functionality and general condition for return to sport (RTS) [23,47,48].
2.1. Statistical Procedures
2.5.1. General Methodology
All data were listed and sorted by gender, analysis population, and type of sport. All the summary tables of the efficacy data were structured with a column for each target and were annotated with the total population size relevant to that table/treatment, including any missing observations, if any. The continuous variables were summarized using the following descriptive statistics: n (number), mean, standard deviation, median, maximum, and minimum. The frequency and percentages (based on the non-missing sample size) were reported for all categorical measures. The data generated in this study were recorded in a study-specific electronic system, and the original rows of data can be made available on demand. After the completion of data entry in the system and the resolution and closure of all discrepancies, the database was blocked to avoid any further modification. After quality checks, the SAS format database was used for statistical analysis.
2.5.2. Study Variables
For participants demography and clinical data documentation, the following variables were documented: year of birth, age (years), gender (male/female), weight, height, BMI calculation, pain evaluation and (VISA-H score) and return to sport (RTS) time.
2.5.3. Analytical Test Application (ATA)
The GraphPad 8.0 version for Apple Computer was used for statistical analysis (PRISM, San Diego, CA, USA). The Shapiro–Wilk test was performed in order to determine whether the data were parametrically distributed. Both W- and p-values were calculated for all distribution of data. The Student’s Test (parametric and paired) was used in order to compare treatment results at T0 and T1 visits. These analyses were performed to evaluate VISA-H output in both (COL I) and (REHAB) treatments. These tests point out was used to catch (if any) among the differences between before and after treatment in the degree of clinical improvements in PHT. While, the Student’s Test (parametric and unpaired) was used in order to compare the values of VISA-H at T0 in both group of treatment (COL I) and (REHAB) and time to return to sport (RTS). All the parameters measured in this study were evaluated by using the classical descriptive statistics of mean, SD, minimum and maximum and frequencies (for qualitative variables). For quantitative analyses, all statistical results were considered significant if the p-value was less than 0.05 (p < 0.05).
3. Results
3.1. Athletes Distribution
In total, 28 athletes were included in this study (Figure 2). Two groups of 14 athletes each were trained to perform (COL I) and (REHAB) treatments. The athletes belong to six different sports disciplines including: Football, Basketball, Cycling, Triathlon, Volleyball, and Crossfit (Figure 2A). The two treatment groups demonstrated parametric data distribution for age (2B) and identical distribution of data concerning: global gender distribution (2C), gender distribution for treatment (2D) and gender distribution for Level of sport activities (2E). Indeed, the two group of analyses (COL I) and (REHAB) were two really homogeneous groups. The results of the Shapiro-Wilk test for parametric data distribution were reported in Figure 2F.
3.1. VISA-H Questionnaire Scores at T0 Visit
In order to compare the statistical differences between the two treatment groups, the evaluation of the VISA-H questionnaire score was done for all athletes, before the start of the treatment, visit at T0. The questionnaire scores for the COL I and REHAB groups were 43.50 ±1.317 and 43.21 ±1.219, respectively (Figure 3). These differences did not show a significant value through the parametric unpaired T-test (p=0.8728). For this reason the groups were considered identical at T0. In addition, the Saphiro-wilk test revealed that the two treatment groups also had parametric distributions (Table 1).
3.1. Follow-Up
The duration of follow-up (FU) of the athletes ranged from 7 to 14 weeks. The maximum FU in COL I treatment was equal to 65 days, while, the maximum FU in REHAB protocol was equal to 95 days.
3.1. Return to Sports (RTS) Results
The time to return to sport (RTS) in the most important parameter for both clinicians and athletes' point of view. The RTS analyses revealed that COL I and REHAB treatments had different times to RTS after treatment. The COL I group had a mean time to RTS equal to 57±5.588 days (about 8 weeks), while the REHAB group was on average equal to with 72.50±17.51. The minimum and the maximum values of time to RTS, were equal to 47 and 95 days, respectively (concerning both treatment). The confidence intervals (CI; 95%) were 53.77-60.23 days, for COL I and 62.30-82.61 days for REAHAB treatments, respectively. These analyses revealed statistically differences between the two treatments (p=0.0083), by parametric and unpaired T-Test (Figure 4). In the following Table 2 are reported the analyses of parametric distribution. These data suggested that COL I treatment seems to compact the results of RTS, in all sportive subjects, better the REHAB one.
3.1. VISA-H Score Results in COL I Treatment
The scores of VISA-H questionnaires were used in order to evaluate the clinical condition of all athletes during the follow-up until the time to RTS. The comparison between the starting point (T0) and the end point (T1) was made separately in both group of treatment (COL I and REHAB). The mean scores in COL I group were equal to 43.50±4.926 and 62.00±3.305 at T0 and T1 visit, respectively. The VISA-H scores showed statistically differences through T-test (parametric and paired test) analyses (p=0.0001; Figure 5). In the following Table 3 are reported the analyses of parametric distribution of data. These analyses suggested that COL I treatment seems to compact the results of VISA-H score at T1 point (Figure 5).
3.1. VISA-H Score Results in REHAB Treatment
The scores of VISA-H questionnaires were used in order to evaluate the clinical condition of all athletes during the follow-up until the time to RTS in REHAB treatment. The mean scores in REHAB group were equal to 43.21±4.560 and 67.00±4.o57 at T0 and T1 visit, respectively. The VISA-H scores showed statistically differences through T-test (parametric and paired test) analyses (p=0.0001; Figure 6). In the following Table 4 are reported the analyses of parametric distribution of data. These data suggested that COL I treatment seems not to compact the results of VISA-H score at T1 point, as well was found in COL I point (Figure 6).
3.1. VISA-H Analyses (Delta an Speed Evaluation)
In order to further evaluate whether the COL I treatment was more effective than the REHAB treatment, were analyzed the VISA-H variation (delta) and its speed (acceleration; delta VISA-H points per week), using data from the comparison between the twovisits (T1-T0), for both treatments. The T-tests (parametric and unpaired) were performed for delta and speed analyses too. The mean delta points variation of VISA-H results were 18.50±0.4776 and 13.79±1.692, for COL I and REHAB treatment, respectively (Figure 7, right graph). While, the mean speed values were equal to 3.085±0.0795 and 2.298±0.388, for COL I and REHAB treatment, respectively (Figure 7, Right graph). Both analyses looking for the difference between COL I vs REHAB revealed significant statistical differences: delta VISA-H (p=0.0171) and VISA-H speed (p=0.0263). Nonetheless, these differences indicated a positive increment for delta VISA-H score and VISA-H speed in treatment COL I, with respect to REHAB (+34,24%) and the COL I treatment confirmed this action in order to compact the clinical evaluation for athletes reducing the variation of VISA-H data among them (Figure 7).
3.1. Proportion and Hazard Ratio (HR) to RTS
In order to evaluate whether the two different populations in terms of proportion on treatment, a Kaplan-Meyer (MK) long-rank analysis was investigated. Here was assumed that censored event was associated to RTS, indeed, the proportion revealed the percent of sportives still under the treatment. The result revealed statistical differences among the population (COL I vs REHAB p=0.0008). Nevertheless, the Hazard ratio to return to sport (RTS) for COL I treatment was equal to 5.359 (95% CI of ratio; 2.004 to 14.330; Figure 8). These data suggested that COL I treatment increased the probability to RTS five time more than REHAB protocol (Figure 8).
4. Discussion
The Hamstring injuries (HIs) are one of the most common types of illness affecting athletes and sportive people [23,49,49,50,51]. Despite the optimal management, including diagnosis [20,23] and treatments [47,48,52], the cause of hamstring muscle injuries is not well defined [23,33]. Indeed, the differential diagnosis inside the HSIs is often mandatory [6]. The principal pathologies associated with the diagnosis of HSIs are: proximal hamstring tendinopathy (PHT) [53,54] , proximal hamstring tendon avulsion (PHTA) [3], Lumbar spine radiculopathy (LSR) [6] and adductor muscle injury (AMI) . The manifestation of symptoms includes the pain in the back of the thigh, sometimes accompanied by an audible or sensory popping sound, causing immediate cessation of activity [8]. The main symptom of proximal hamstring tendinopathy (PHT) is lower gluteal pain, especially during running or prolonged sitting [54]. According the classification of HI consensus [15], in this study were correctly included 28 athletes affect by PHT. The subjects were splinted in two group associated with two different treatment: the former was associated with porcine collagen treatment (COL I), while, in the second one group was performed an usual rehabilitation program (REHAB) [33]. These traditional treatment methods for PHT are by the majority comparable to those of other tendinopathies: they include rest and ice for symptoms relief in the initial phase, reduction or pause of sports activity, no steroidal anti-inflammatory drugs (NSAIDs), soft tissue mobilization, physiotherapy and continuous home exercise program focusing on progressive eccentric hamstring strengthening and core stabilization [55]. Novel therapeutic approaches are recognized including shockwave (SWT)[22] and ultrasound (US) therapy [24], ultra-sound-guided corticosteroid [25] and Platelet-rich-plasma (PRP) injections [27]. However, the efficacy of collagen application in tendon field, was represented by Randelli et Al., whom reported the efficacy of porcine collagen in human tenocytes [36], indeed, other clinical studies reported porcine collagen efficacy in human [31,56,57].
By the way, the first aim of all treatment mentioned above point this out to increase the benefit for athletes and to reduce the time to return to Sport (RTS). The faster treatment seems to be representing by corticosteroid injections (RTS= 1 month). However, several clinicians reported a several side-effects associated with the treatment including: including local irritation, skin depigmentation, suppression of tenocyte activity and collagen synthesis, and tendon avulsion [23,58,59]. The other options offer a RTS condition after 3 (SWT) or 4.5 (PRP) months. In particular, the ratio efficacy/benefit in PRP injection is quite controversial [23,60]. The porcine collagen injection (COL I treatment), required the same specialization needed for the corticosteroids and plasma application, but demonstrated better results in terms of RTS. In fact the mean of COL I group was equal to 57 days less than two months). The analyses of this study included also the clinical evaluation of athletes by the VISA-H questionnaire. This procedure is very well document and currently used in Europe for football players PHT evaluation [54,61]. The normal score of VISA-H in this study was evaluated around 60.9 (mean value) [61]. The evaluation of VISA-H, was positive in both group after treatment (COL I at T1 and REHAB at T1). However, in the COL I group the VISA-H score was better than REHAB one and it’s mean score was equal to 62.00. This data were evaluated congruent according the literature report below.
Nonetheless, the COL I treatment demonstrated better result (vs. REHAB group) in term of RTS (57 vs. 72 days), delta VISA-H (18.50 vs. 13.79 points) and VISA-H speed (3.085 vs. 2.298 points/week). Finally, the long-rank test revealed a strong p-value (p=0.0008) for the ratio of athletes staying in treatment. Therefore, the analyses revealed a HR=5.359 for COL I group with respect to REHAB treatment, in reducing RTS time.
Probably, The explanations for why collagen has such a positive effect are probably to be found in the biological mechanisms involved in the repair process after a hamstring strain injury [33]. At the beginning of the healing process, a significant increase in the production of type III collagen has been documented [62]. This type of collagen fibrils has a much smaller diameter and therefore a lower resistance to tensile force than type I collagen fibrils. This fact implies lower load-bearing capacities compared to healthy muscle tissue, where the percentage of type I collagen is much more abundant [63,64]. As time passes, the ratio of type I/III collagen fibers, i.e., the tensile strength of the repaired tissue increases significantly [62,65,66]. To provide mechanical support and form a fiber capable of withstanding physical stress, collagen fibers must be highly cross-linked [62]. These analyses demonstrate the two population analyzed are very homogeneous and the distribution are parametric. Indeed, the statistical differences demonstrated above seem not be affected by anagraphical data or levels of their sport activities. Nevertheless, the COL I approach demonstrated to stratify better the results of athletes in terms of RTS and VISA-H. As a general concept, it is necessary to emphasize that PHT injuries also represent an important economic turning point in the professional discipline, where the athlete works. It has been demonstrated the enormous budget lost due to injuries in the world of professional sports (i.e. football) [45]. Therefore, RTS time becomes a requirement for sports health, recovery of athletic performance, reduction of economic losses in terms of medical expenses and profits.
5. Conclusions
The Proximal Hamstring Tendinopathy (PHT) is one a most important pathology affecting professional athletes and their performances, inducing them the stop from activities. The time to return to sport (RTS) is a crucial elapsed time frame influencing the status the performances and the budget of athlete staff. Indeed, shorter RTS changes many aspects of professional sports. The conservative approaches (starting from rehabilitation to injective therapies) point out to modify RTS. The analyses of the new conservative treatment (COL I; MD-MUSCLE) seem to demonstrate several advantages with respect to rehabilitation protocol, including: 1) to reduce the RTS, 2) to improve clinical condition, 3) to accelerate clinical benefit and to uniform better the result after treatment. The porcine collagen injection showed a shorter RTS with respect other treatment as well SWT and PRP injection. The turnover between type I and type III collagen fibers, seem to explain the particular efficacy of collagen injection. However, a largest cohort of athletes might be investigated in order to confirm the clinical benefit of porcine collagen conservative treatment in PHT.
Author Contributions
Conceptualization, M.B.; methodology, M.B.; software, S.R.; validation, S.R., D.G. and L.P.; formal analysis, S.R., D.G. and L.P.; investigation, S.R., D.G. and L.P.; resources, R.B.; data curation, M.B.; writing—original draft preparation, M.B.; writing—review and editing, M.B. and S.R.; visualization, R.B.; supervision, R.B.; project administration, S.R.; funding acquisition, R.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding and the APC was funded by GUNA.
Institutional Review Board Statement
For this study, the approval of the ethics committee was not necessary since it is a retrospective analysis on anonymized data. The data in possession for the analyses can be considered anonymized, when it is not possible to trace the identity of the subjects even using subsequent operations at the informatic level. This aspect is regulated by law no. 675/1996 of the Guarantor of Privacy in Italy, in compliance with the use of personal data for scientific purposes.
Informed Consent Statement
The signed Informed consent was obtained from all subjects involved in the study and all subject agreed.
Data Availability Statement
All data obtained from this study are available for consultation. The data controller is Dr. Matteo Baldassarri.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Waldén, M.; Hägglund, M.; Magnusson, H.; Ekstrand, J. ACL Injuries in Men’s Professional Football: A 15-Year Prospective Study on Time Trends and Return-to-Play Rates Reveals Only 65% of Players Still Play at the Top Level 3 Years after ACL Rupture. Br. J. Sports Med. 2016, 50, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Roe, M.; Murphy, J.C.; Gissane, C.; Blake, C. Hamstring Injuries in Elite Gaelic Football: An 8-Year Investigation to Identify Injury Rates, Time-Loss Patterns and Players at Increased Risk. Br. J. Sports Med. 2018, 52, 982–988. [Google Scholar] [CrossRef] [PubMed]
- Bertiche, P.; Mohtadi, N.; Chan, D.; Hölmich, P. Proximal Hamstring Tendon Avulsion: State of the Art. J. ISAKOS 2021, 6, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Nicoletti, P.; Baldin, G.; Bragazzi, N.L.; Crimì, A.; Ruggieri, P. Hamstring Strain Injury (HSI) Prevention in Professional and Semi-Professional Football Teams: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public. Health 2021, 18, 8272. [Google Scholar] [CrossRef]
- Heiderscheit, B.C.; Hoerth, D.M.; Chumanov, E.S.; Swanson, S.C.; Thelen, B.J.; Thelen, D.G. Identifying the Time of Occurrence of a Hamstring Strain Injury during Treadmill Running: A Case Study. Clin. Biomech. 2005, 20, 1072–1078. [Google Scholar] [CrossRef]
- Hickey, J.T.; Opar, D.A.; Weiss, L.J.; Heiderscheit, B.C. Hamstring Strain Injury Rehabilitation. J. Athl. Train. 2022, 57, 125–135. [Google Scholar] [CrossRef]
- Whiteley, R.; Van Dyk, N.; Wangensteen, A.; Hansen, C. Clinical Implications from Daily Physiotherapy Examination of 131 Acute Hamstring Injuries and Their Association with Running Speed and Rehabilitation Progression. Br. J. Sports Med. 2018, 52, 303–310. [Google Scholar] [CrossRef]
- Jacobsen, P.; Witvrouw, E.; Muxart, P.; Tol, J.L.; Whiteley, R. A Combination of Initial and Follow-up Physiotherapist Examination Predicts Physician-Determined Time to Return to Play after Hamstring Injury, with No Added Value of MRI. Br. J. Sports Med. 2016, 50, 431–439. [Google Scholar] [CrossRef]
- Opar, D.A.; Williams, M.D.; Shield, A.J. Hamstring Strain Injuries: Factors That Lead to Injury and Re-Injury. Sports Med. 2012, 42, 209–226. [Google Scholar] [CrossRef]
- Chumanov, E.S.; Heiderscheit, B.C.; Thelen, D.G. Hamstring Musculotendon Dynamics during Stance and Swing Phases of High-Speed Running. Med. Sci. Sports Exerc. 2011, 43, 525–532. [Google Scholar] [CrossRef]
- Delvaux, F.; Croisier, J.-L.; Carling, C.; Orhant, E.; Kaux, J.-F. [Hamstring muscle injury in football players - Part I : epidemiology, risk factors, injury mechanisms and treatment]. Rev. Med. Liege 2023, 78, 160–164. [Google Scholar] [PubMed]
- Mueller-Wohlfahrt, H.-W.; Haensel, L.; Mithoefer, K.; Ekstrand, J.; English, B.; McNally, S.; Orchard, J.; Van Dijk, C.N.; Kerkhoffs, G.M.; Schamasch, P.; et al. Terminology and Classification of Muscle Injuries in Sport: The Munich Consensus Statement. Br. J. Sports Med. 2013, 47, 342–350. [Google Scholar] [CrossRef]
- Pollock, N.; James, S.L.J.; Lee, J.C.; Chakraverty, R. British Athletics Muscle Injury Classification: A New Grading System. Br. J. Sports Med. 2014, 48, 1347–1351. [Google Scholar] [CrossRef]
- Valle, X.; Alentorn-Geli, E.; Tol, J.L.; Hamilton, B.; Garrett, W.E.; Pruna, R.; Til, L.; Gutierrez, J.A.; Alomar, X.; Balius, R.; et al. Muscle Injuries in Sports: A New Evidence-Informed and Expert Consensus-Based Classification with Clinical Application. Sports Med. 2017, 47, 1241–1253. [Google Scholar] [CrossRef]
- Paton, B.M.; Court, N.; Giakoumis, M.; Head, P.; Kayani, B.; Kelly, S.; Kerkhoffs, G.M.M.J.; Moore, J.; Moriarty, P.; Murphy, S.; et al. London International Consensus and Delphi Study on Hamstring Injuries Part 1: Classification. Br. J. Sports Med. 2023, 57, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Pihl, E.; Laszlo, S.; Rosenlund, A.-M.; Kristoffersen, M.H.; Schilcher, J.; Hedbeck, C.J.; Skorpil, M.; Micoli, C.; Eklund, M.; Sköldenberg, O.; et al. Operative versus Nonoperative Treatment of Proximal Hamstring Avulsions. NEJM Evid. 2024, 3. [Google Scholar] [CrossRef]
- Vermeulen, R.; Whiteley, R.; Van Der Made, A.D.; Van Dyk, N.; Almusa, E.; Geertsema, C.; Targett, S.; Farooq, A.; Bahr, R.; Tol, J.L.; et al. Early versus Delayed Lengthening Exercises for Acute Hamstring Injury in Male Athletes: A Randomised Controlled Clinical Trial. Br. J. Sports Med. 2022, 56, 792–800. [Google Scholar] [CrossRef]
- Clanton, T.O.; Coupe, K.J. Hamstring Strains in Athletes: Diagnosis and Treatment: J. Am. Acad. Orthop. Surg. 1998, 6, 237–248. [Google Scholar] [CrossRef]
- Jankaew, A.; Chen, J.-C.; Chamnongkich, S.; Lin, C.-F. Therapeutic Exercises and Modalities in Athletes With Acute Hamstring Injuries: A Systematic Review and Meta-Analysis. Sports Health Multidiscip. Approach 2023, 15, 497–511. [Google Scholar] [CrossRef]
- Ishøi, L.; Krommes, K.; Husted, R.S.; Juhl, C.B.; Thorborg, K. Diagnosis, Prevention and Treatment of Common Lower Extremity Muscle Injuries in Sport – Grading the Evidence: A Statement Paper Commissioned by the Danish Society of Sports Physical Therapy (DSSF). Br. J. Sports Med. 2020, 54, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, R.; Whiteley, R.; Van Der Made, A.D.; Van Dyk, N.; Almusa, E.; Geertsema, C.; Targett, S.; Farooq, A.; Bahr, R.; Tol, J.L.; et al. Early versus Delayed Lengthening Exercises for Acute Hamstring Injury in Male Athletes: A Randomised Controlled Clinical Trial. Br. J. Sports Med. 2022, 56, 792–800. [Google Scholar] [CrossRef]
- Schroeder, A.N.; Tenforde, A.S.; Jelsing, E.J. Extracorporeal Shockwave Therapy in the Management of Sports Medicine Injuries. Curr. Sports Med. Rep. 2021, 20, 298–305. [Google Scholar] [CrossRef]
- Chu, S.K.; Rho, M.E. Hamstring Injuries in the Athlete: Diagnosis, Treatment, and Return to Play. Curr. Sports Med. Rep. 2016, 15, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Korakakis, V.; Whiteley, R.; Tzavara, A.; Malliaropoulos, N. The Effectiveness of Extracorporeal Shockwave Therapy in Common Lower Limb Conditions: A Systematic Review Including Quantification of Patient-Rated Pain Reduction. Br. J. Sports Med. 2018, 52, 387–407. [Google Scholar] [CrossRef]
- Zissen, M.H.; Wallace, G.; Stevens, K.J.; Fredericson, M.; Beaulieu, C.F. High Hamstring Tendinopathy: MRI and Ultrasound Imaging and Therapeutic Efficacy of Percutaneous Corticosteroid Injection. Am. J. Roentgenol. 2010, 195, 993–998. [Google Scholar] [CrossRef]
- Silvers-Granelli, H.J.; Cohen, M.; Espregueira-Mendes, J.; Mandelbaum, B. Hamstring Muscle Injury in the Athlete: State of the Art. J. ISAKOS 2021, 6, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Seow, D.; Shimozono, Y.; Tengku Yusof, T.N.B.; Yasui, Y.; Massey, A.; Kennedy, J.G. Platelet-Rich Plasma Injection for the Treatment of Hamstring Injuries: A Systematic Review and Meta-Analysis With Best-Worst Case Analysis. Am. J. Sports Med. 2021, 49, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Desouza, C.; Shetty, V. Efficacy of Platelet-Rich Plasma in Grade 2 Hamstring Muscle Injuries: Results from a Randomized Controlled Trial. Eur. J. Orthop. Surg. Traumatol. 2025, 35, 259. [Google Scholar] [CrossRef] [PubMed]
- Poursalehian, M.; Lotfi, M.; Zafarmandi, S.; Arabzadeh Bahri, R.; Halabchi, F. Hamstring Injury Treatments and Management in Athletes: A Systematic Review of the Current Literature. JBJS Rev. 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Corrado, B.; Mazzuoccolo, G.; Liguori, L.; Chirico, V.A.; Costanzo, M.; Bonini, I.; Bove, G.; Curci, L. Treatment of Lateral Epicondylitis with Collagen Injections: A Pilot Study. Muscle Ligaments Tendons J. 2019, 09, 584. [Google Scholar] [CrossRef]
- Godek, P.; Szczepanowska-Wolowiec, B.; Golicki, D. Collagen and PRP in Partial Thickness Rotator Cuff Injuries. Friends or Only Indifferent Neighbours? Randomized Controlled Trial; In Review, 2021; pp. 1–19. [Google Scholar]
- Park, P.Y.S.; Cai, C.; Bawa, P.; Kumaravel, M. Platelet-Rich Plasma vs. Steroid Injections for Hamstring Injury—Is There Really a Choice? Skeletal Radiol. 2019, 48, 577–582. [Google Scholar] [CrossRef]
- Pieters, D.; Wezenbeek, E.; Schuermans, J.; Witvrouw, E. Return to Play After a Hamstring Strain Injury: It Is Time to Consider Natural Healing. Sports Med. 2021, 51, 2067–2077. [Google Scholar] [CrossRef] [PubMed]
- Giai Via, A.; Papa, G.; Oliva, F.; Maffulli, N. Tendinopathy. Curr. Phys. Med. Rehabil. Rep. 2016, 4, 50–55. [Google Scholar] [CrossRef]
- Koszela, K.; Woldańska-Okońska, M.; Słupiński, M.; Gasik, R. The Role of Injection Collagen Therapy in Greater Trochanter Pain Syndrome. A New Therapeutic Approach? Rheumatology 2025. [Google Scholar] [CrossRef]
- Randelli, F.; Sartori, P.; Carlomagno, C.; Bedoni, M.; Menon, A.; Vezzoli, E.; Sommariva, M.; Gagliano, N. The Collagen-Based Medical Device MD-Tissue Acts as a Mechanical Scaffold Influencing Morpho-Functional Properties of Cultured Human Tenocytes. Cells 2020, 9, 2641. [Google Scholar] [CrossRef]
- Randelli, F.; Menon, A.; Giai Via, A.; Mazzoleni, M.; Sciancalepore, F.; Brioschi, M.; Gagliano, N. Effect of a Collagen-Based Compound on Morpho-Functional Properties of Cultured Human Tenocytes. Cells 2018, 7, 246. [Google Scholar] [CrossRef] [PubMed]
- Randelli, F.; Fioruzzi, A.; Mazzoleni, M.G.; Radaelli, A.; Rahali, L.; Verga, L.; Menon, A. Efficacy of Ultrasound-Guided Injections of Type I Collagen-Based Medical Device for Greater Trochanteric Pain Syndrome: A Pilot Study. Life 2025, 15, 366. [Google Scholar] [CrossRef]
- Corrado, B.; Bonini, I.; Chirico, V.A.; Filippini, E.; Liguori, L.; Magliulo, G.; Mazzuoccolo, G.; Rosano, N.; Gisonni, P. Ultrasound-Guided Collagen Injections in the Treatment of Supraspinatus Tendinopathy: A Case Series Pilot Study. J. Biol. Regul. Homeost. Agents 2020, 34, 33–39. [Google Scholar]
- De Pascalis, M.; Mulas, S.; Sgarbi, L. Combined Oxygen–Ozone and Porcine Injectable Collagen Therapies Boosting Efficacy in Low Back Pain and Disability. Diagnostics 2024, 14, 2411. [Google Scholar] [CrossRef]
- Godek, P.; Szczepanowska-Wolowiec, B.; Golicki, D. Collagen and PRP in Partial Thickness Rotator Cuff Injuries. Friends or Only Indifferent Neighbours? Randomized Controlled Trial; In Review, 2021; pp. 1–19. [Google Scholar]
- Praet, S.F.E.; Purdam, C.R.; Welvaert, M.; Vlahovich, N.; Lovell, G.; Burke, L.M.; Gaida, J.E.; Manzanero, S.; Hughes, D.; Waddington, G. Oral Supplementation of Specific Collagen Peptides Combined with Calf-Strengthening Exercises Enhances Function and Reduces Pain in Achilles Tendinopathy Patients. Nutrients 2019, 11, 76. [Google Scholar] [CrossRef]
- Jendricke, P.; Centner, C.; Zdzieblik, D.; Gollhofer, A.; König, D. Specific Collagen Peptides in Combination with Resistance Training Improve Body Composition and Regional Muscle Strength in Premenopausal Women: A Randomized Controlled Trial. Nutrients 2019, 11, 892. [Google Scholar] [CrossRef]
- Tarantino, D.; Mottola, R.; Palermi, S.; Sirico, F.; Corrado, B.; Gnasso, R. Intra-Articular Collagen Injections for Osteoarthritis: A Narrative Review. Int. J. Environ. Res. Public. Health 2023, 20, 4390. [Google Scholar] [CrossRef]
- Nieto Torrejón, L.; Martínez-Serrano, A.; Villalón, J.M.; Alcaraz, P.E. Economic Impact of Muscle Injury Rate and Hamstring Strain Injuries in Professional Football Clubs. Evidence from LaLiga. PLOS ONE 2024, 19, e0301498. [Google Scholar] [CrossRef]
- Cacchio, A.; De Paulis, F.; Maffulli, N. Development and Validation of a New Visa Questionnaire (VISA-H) for Patients with Proximal Hamstring Tendinopathy. Br. J. Sports Med. 2014, 48, 448–452. [Google Scholar] [CrossRef]
- Degen, R.M. Proximal Hamstring Injuries: Management of Tendinopathy and Avulsion Injuries. Curr. Rev. Musculoskelet. Med. 2019, 12, 138–146. [Google Scholar] [CrossRef]
- Lauf, K.; Van Der Made, A.D.; Jaspers, R.; Tacken, R.; Maas, M.; Kerkhoffs, G. Successful Rapid Return to Performance Following Non-Operative Treatment of Proximal Hamstring Tendon Avulsion in Elite Athletes. BMJ Open Sport Exerc. Med. 2025, 11, e002468. [Google Scholar] [CrossRef]
- Biz, C.; Nicoletti, P.; Baldin, G.; Bragazzi, N.L.; Crimì, A.; Ruggieri, P. Hamstring Strain Injury (HSI) Prevention in Professional and Semi-Professional Football Teams: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public. Health 2021, 18, 8272. [Google Scholar] [CrossRef] [PubMed]
- Hickey, J.T.; Opar, D.A.; Weiss, L.J.; Heiderscheit, B.C. Hamstring Strain Injury Rehabilitation. J. Athl. Train. 2022, 57, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.L.; Cibulka, M.T.; Bolgla, L.A.; Koc, T.A.; Loudon, J.K.; Manske, R.C.; Weiss, L.; Christoforetti, J.J.; Heiderscheit, B.C. Hamstring Strain Injury in Athletes: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health From the Academy of Orthopaedic Physical Therapy and the American Academy of Sports Physical Therapy of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2022, 52, CPG1–CPG44. [Google Scholar] [CrossRef]
- Pihl, E.; Laszlo, S.; Rosenlund, A.-M.; Kristoffersen, M.H.; Schilcher, J.; Hedbeck, C.J.; Skorpil, M.; Micoli, C.; Eklund, M.; Sköldenberg, O.; et al. Operative versus Nonoperative Treatment of Proximal Hamstring Avulsions. NEJM Evid. 2024, 3, EVIDoa2400056. [Google Scholar] [CrossRef] [PubMed]
- Rich, A.; Cook, J.; Hahne, A.; Ford, J. Treatment of Proximal Hamstring Tendinopathy with Individualized Physiotherapy: A Clinical Commentary. Int. J. Sports Phys. Ther. 2025, 20. [Google Scholar] [CrossRef]
- Rich, A.L.F.; Cook, J.L.; Hahne, A.J.; Ford, J.J. A Pilot Randomised Trial Comparing Individualised Physiotherapy versus Shockwave Therapy for Proximal Hamstring Tendinopathy: A Protocol. J. Exp. Orthop. 2023, 10, 55. [Google Scholar] [CrossRef]
- Afonso, J.; Olivares-Jabalera, J.; Fernandes, R.J.; Clemente, F.M.; Rocha-Rodrigues, S.; Claudino, J.G.; Ramirez-Campillo, R.; Valente, C.; Andrade, R.; Espregueira-Mendes, J. Effectiveness of Conservative Interventions After Acute Hamstrings Injuries in Athletes: A Living Systematic Review. Sports Med. 2023, 53, 615–635. [Google Scholar] [CrossRef]
- Corrado, B.; Bonini, I.; Alessio Chirico, V.; Rosano, N.; Gisonni, P. Use of Injectable Collagen in Partial-Thickness Tears of the Supraspinatus Tendon: A Case Report. Oxf. Med. Case Rep. 2020, 2020, omaa103. [Google Scholar] [CrossRef]
- Corrado, B.; Mazzuoccolo, G.; Liguori, L.; Chirico, V.A.; Costanzo, M.; Bonini, I.; Bove, G.; Curci, L. Treatment of Lateral Epicondylitis with Collagen Injections: A Pilot Study. Muscle Ligaments Tendons J. 2019, 09, 584. [Google Scholar] [CrossRef]
- Nicholson, L.T.; DiSegna, S.; Newman, J.S.; Miller, S.L. Fluoroscopically Guided Peritendinous Corticosteroid Injection for Proximal Hamstring Tendinopathy: A Retrospective Review. Orthop. J. Sports Med. 2014, 2, 2325967114526135. [Google Scholar] [CrossRef] [PubMed]
- Scutt, N.; Rolf, C.G.; Scutt, A. Glucocorticoids Inhibit Tenocyte Proliferation and Tendon Progenitor Cell Recruitment. J. Orthop. Res. 2006, 24, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, B.; Tol, J.L.; Almusa, E.; Boukarroum, S.; Eirale, C.; Farooq, A.; Whiteley, R.; Chalabi, H. Platelet-Rich Plasma Does Not Enhance Return to Play in Hamstring Injuries: A Randomised Controlled Trial. Br. J. Sports Med. 2015, 49, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Medina-Porqueres, I.; Rosado-Velazquez, D.; Moya-Torrecilla, F.; Orava, S.; Cacchio, A. Translation, Linguistic Validation, and Readability of the Spanish Version of VISA-H Scale in Elite Athletes. Arch. Bone Jt. Surg. 2021. [Google Scholar] [CrossRef]
- Lehto, M.; Sims, T.J.; Bailey, A.J. Skeletal Muscle Injury—Molecular Changes in the Collagen during Healing. Res. Exp. Med. (Berl.) 1985, 185, 95–106. [Google Scholar] [CrossRef]
- Wiedemann, H.; Fujii, T.; Kuhn, K.; Chung, E.; Miller, E.J. Comparative Electron-Microscope Studies on Type-III and Type-I Collagens. Eur. J. Biochem. 1975, 51, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Stauber, W.T.; Knack, K.K.; Miller, G.R.; Grimmett, J.G. Fibrosis and Intercellular Collagen Connections from Four Weeks of Muscle Strains. Muscle Nerve 1996, 19, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, T.A.H.; Järvinen, T.L.N.; Kääriäinen, M.; Kalimo, H.; Järvinen, M. Muscle Injuries: Biology and Treatment. Am. J. Sports Med. 2005, 33, 745–764. [Google Scholar] [CrossRef] [PubMed]
- Best, T.M.; Shehadeh, S.E.; Leverson, G.; Michel, J.T.; Corr, D.T.; Aeschlimann, D. Analysis of Changes in mRNA Levels of Myoblast- and Fibroblast-derived Gene Products in Healing Skeletal Muscle Using Quantitative Reverse Transcription-polymerase Chain Reaction. J. Orthop. Res. 2001, 19, 565–572. [Google Scholar] [CrossRef]
Figure 1.
Procedure concerning the injection therapy. A) Ultrasound-guided injection of MD-Muscle (porcine collagen) in the proximal hamstring region. The patient is in prone position, and the physician uses an ultrasound probe for real-time needle guidance to ensure precise delivery into the tendon of proximal biceps femur. B) Ultrasound image showing needle entry into the hamstring tendon. The labeled structures highlight the muscle tissue and the hamstring tendon. This imaging confirms the correct positioning of the needle under ultrasound guidance.
Figure 1.
Procedure concerning the injection therapy. A) Ultrasound-guided injection of MD-Muscle (porcine collagen) in the proximal hamstring region. The patient is in prone position, and the physician uses an ultrasound probe for real-time needle guidance to ensure precise delivery into the tendon of proximal biceps femur. B) Ultrasound image showing needle entry into the hamstring tendon. The labeled structures highlight the muscle tissue and the hamstring tendon. This imaging confirms the correct positioning of the needle under ultrasound guidance.
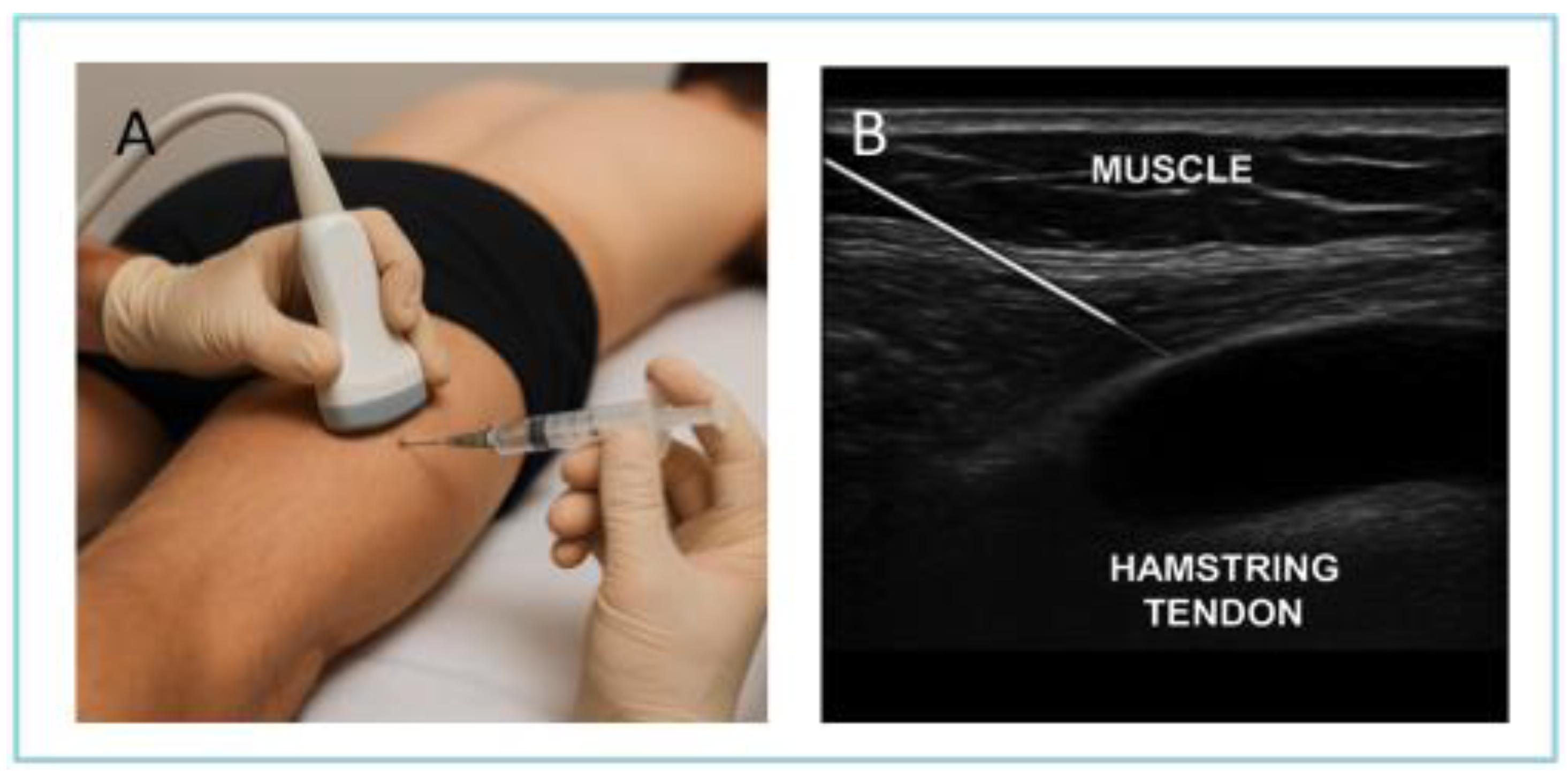
Figure 2.
Data representation concerning athletes distribution. A) Sport activities; from Left Football, Basketball, Cycling, Triathlon, Volleyball, and Crossfit; B) Mean Age concerning the treatment: COL I (Orange) and REHAB (Peach). Gender distribution concerning: C) Global distribution; D) type of treatment and Level of sport activity. F) Statistics concerning the parametric distribution of athletes (Age).
Figure 2.
Data representation concerning athletes distribution. A) Sport activities; from Left Football, Basketball, Cycling, Triathlon, Volleyball, and Crossfit; B) Mean Age concerning the treatment: COL I (Orange) and REHAB (Peach). Gender distribution concerning: C) Global distribution; D) type of treatment and Level of sport activity. F) Statistics concerning the parametric distribution of athletes (Age).
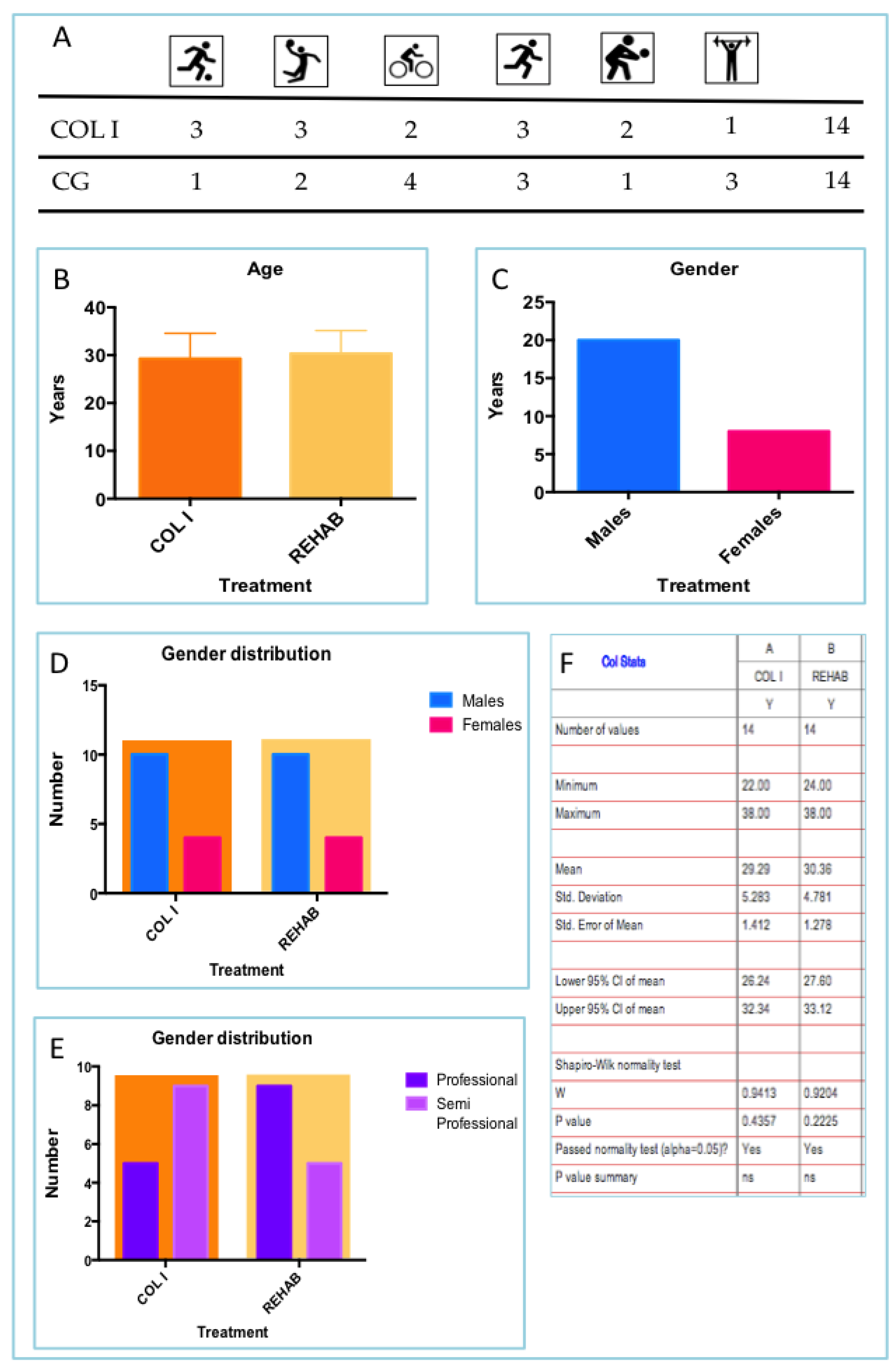
Figure 3.
Results concerning VISA-H scores at starting point (T0). The differences are not statistically different (p=0.8728). T-test analyses (parametric, unpaired).
Figure 3.
Results concerning VISA-H scores at starting point (T0). The differences are not statistically different (p=0.8728). T-test analyses (parametric, unpaired).
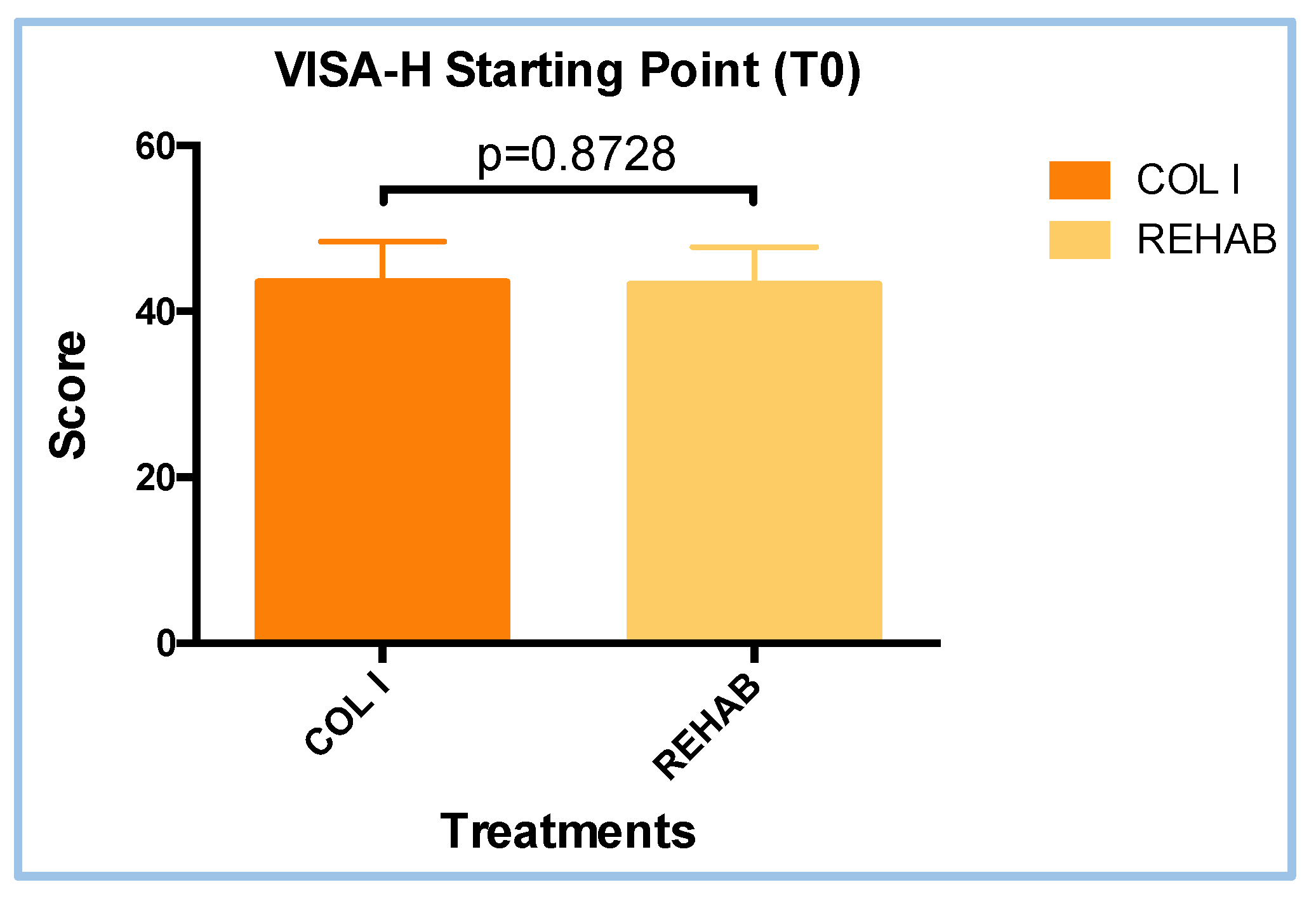
Figure 4.
Return to Sport (RTS) results. The difference between COL I and REHAB were statistically different (p=0.0083). T-test analyses (parametric, unpaired).
Figure 4.
Return to Sport (RTS) results. The difference between COL I and REHAB were statistically different (p=0.0083). T-test analyses (parametric, unpaired).
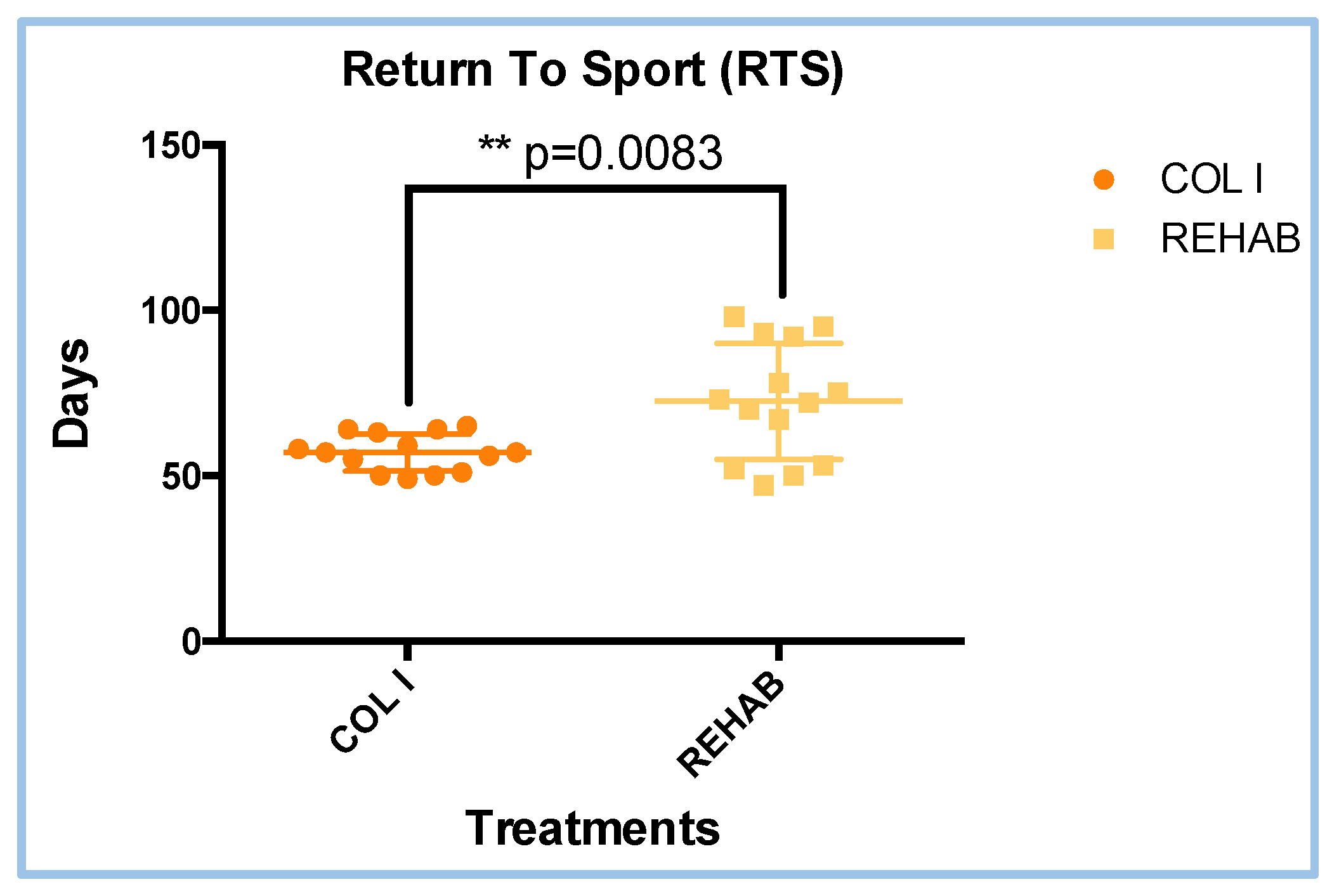
Figure 5.
VISA-H score in COL I treatment The difference between T0 and T1 visit were statistically different (p<0.0001). T-test analyses (parametric, paired).
Figure 5.
VISA-H score in COL I treatment The difference between T0 and T1 visit were statistically different (p<0.0001). T-test analyses (parametric, paired).
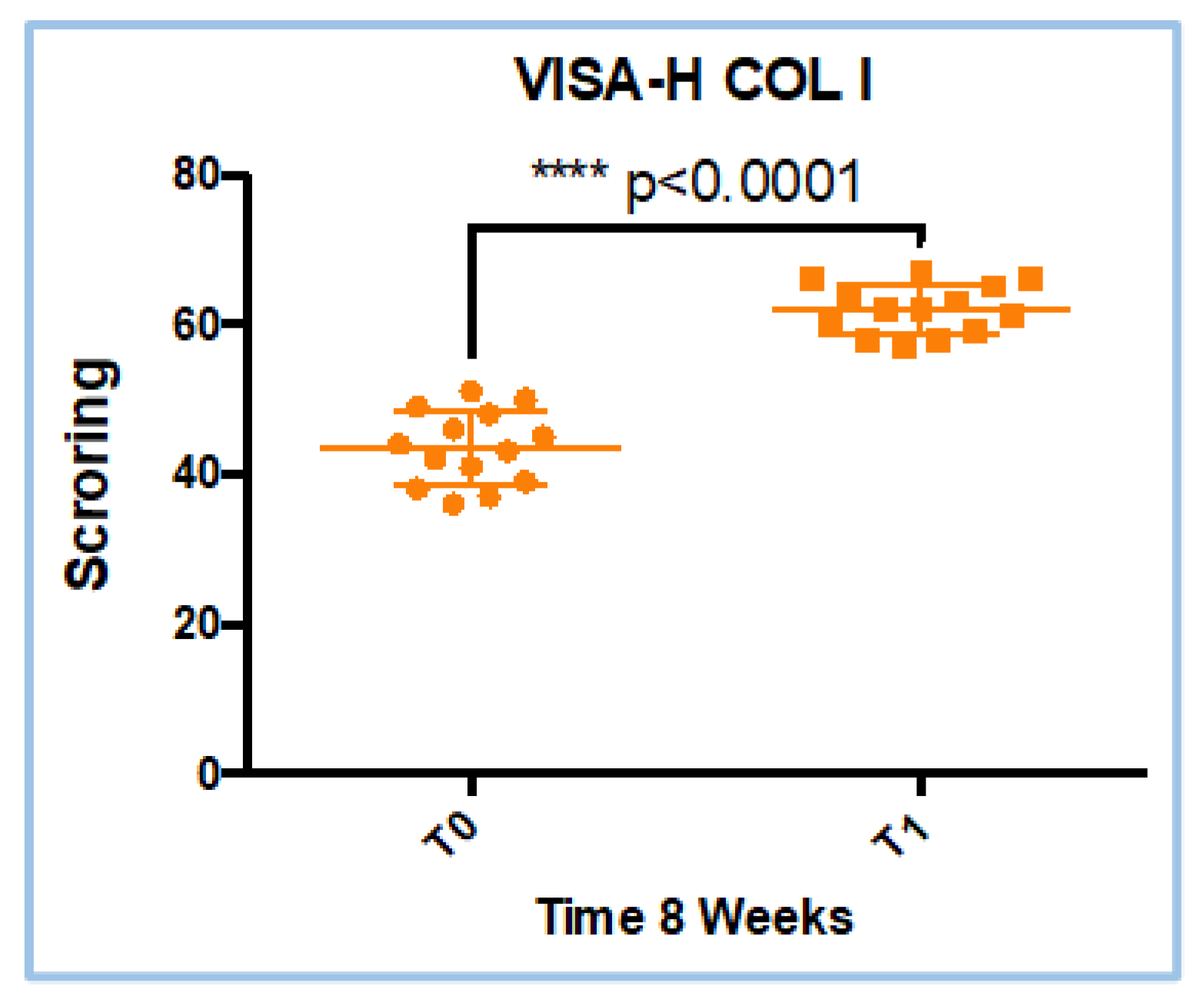
Figure 6.
VISA-H score in REHAB treatment. The difference between T0 and T1 visit were statistically different (p<0.0001). T-test analyses (parametric, paired),.
Figure 6.
VISA-H score in REHAB treatment. The difference between T0 and T1 visit were statistically different (p<0.0001). T-test analyses (parametric, paired),.
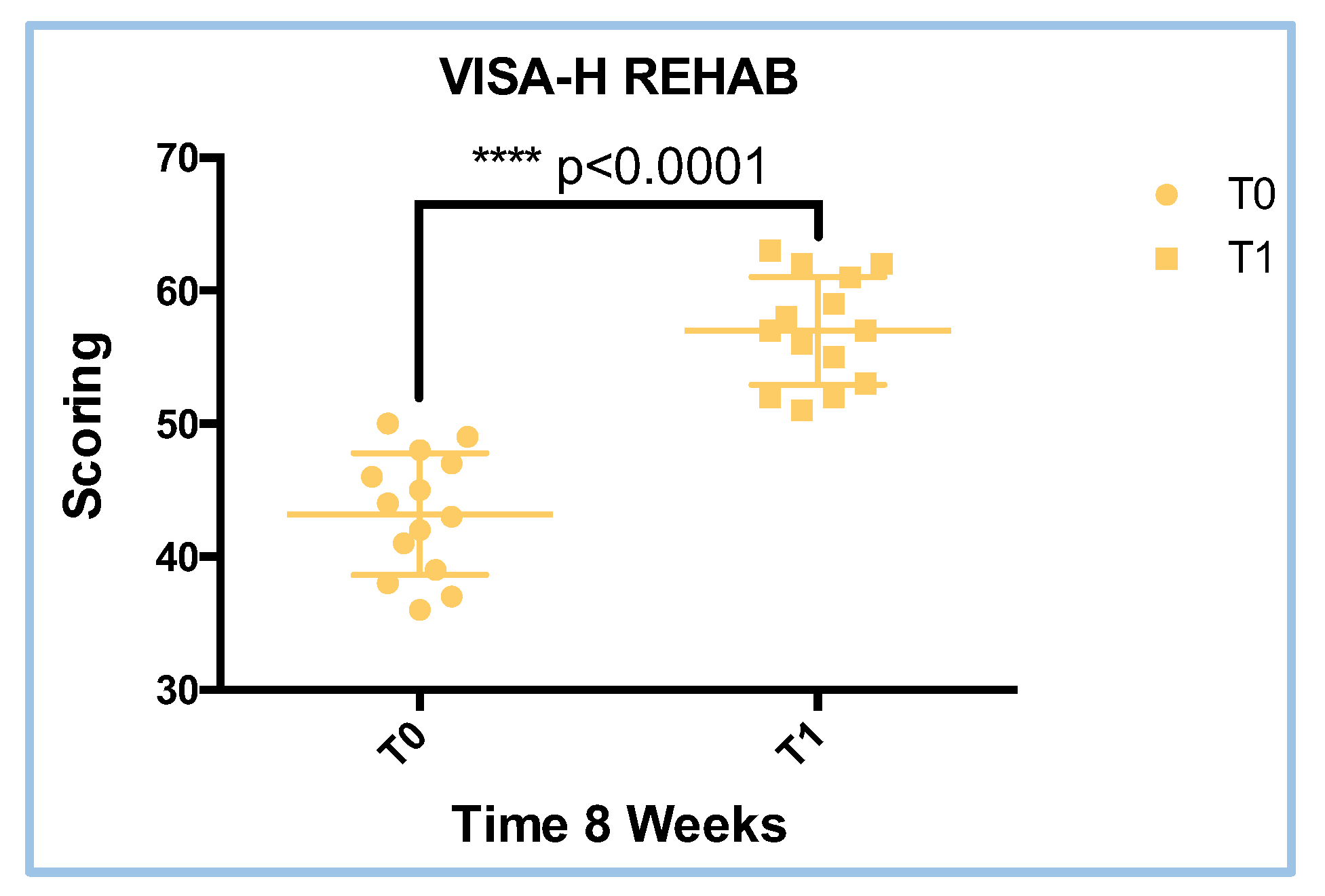
Figure 7.
Results of delta VISA-H (left) and VISA-H speed (right) analyses.
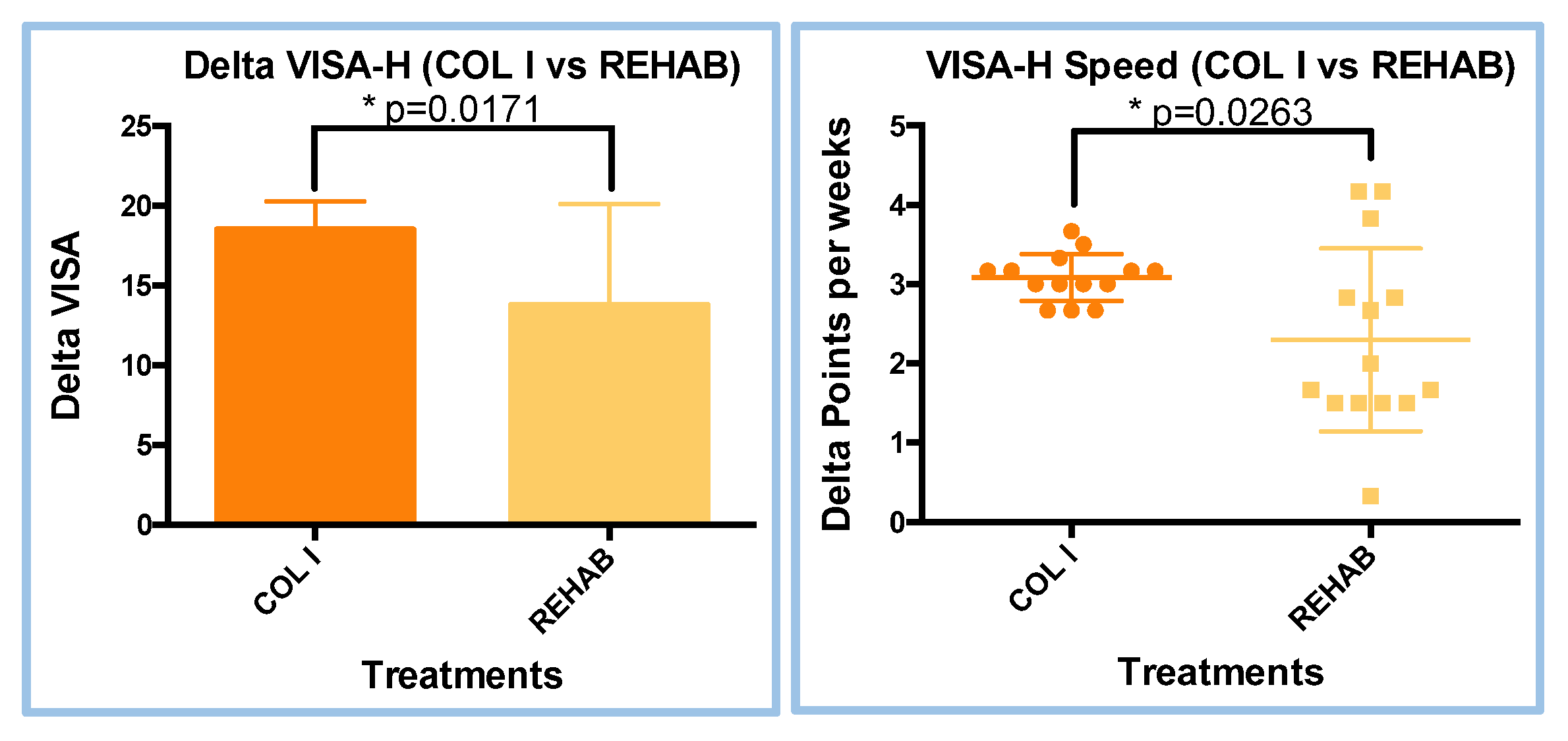
Figure 8.
KM proportion for COL I and REHAB population.
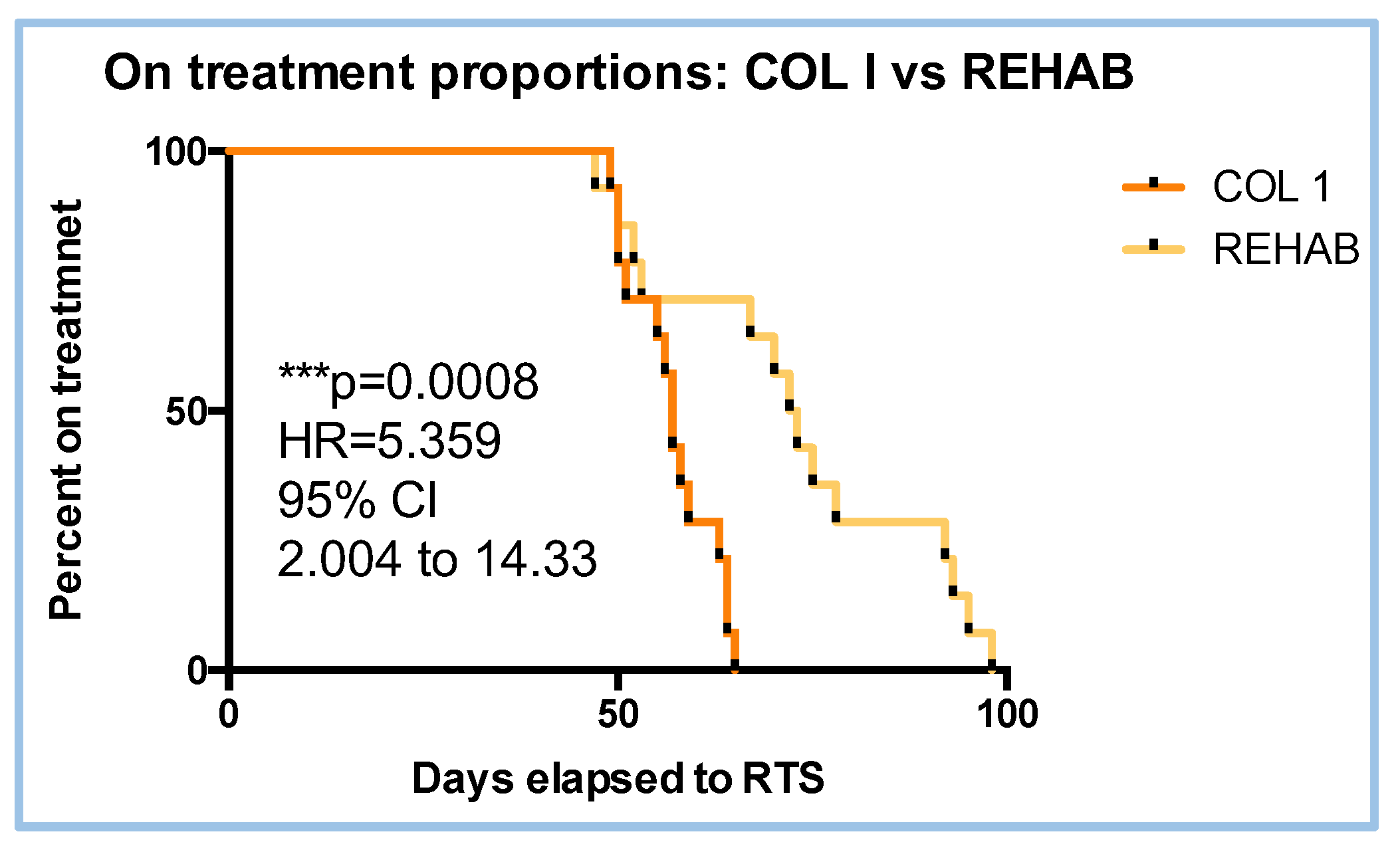

Table 1.
Saphiro-Wilk test results regarding Figure 2.
Table 1.
Saphiro-Wilk test results regarding Figure 2.
| Treatment | W value | P value | Parametric data |
|---|---|---|---|
| COL I | 0.9573 | 0.6787 | YES |
| REHAB | 0.9583 | 0.6952 | YES |
Note. The W and P value are referred to Saphiro-Wilk normally test.
Table 2.
Saphiro-Wilk test results regarding Figure 4.
Table 2.
Saphiro-Wilk test results regarding Figure 4.
| Treatment | W value | P value | Parametric data |
|---|---|---|---|
| COL I | 0.9168 | 0.1974 | YES |
| REHAB | 0.9201 | 0.2268 | YES |
Note. The W and P value are referred to Saphiro-Wilk normally test.
Table 3.
Saphiro-Wilk test results regarding Figure 5.
Table 3.
Saphiro-Wilk test results regarding Figure 5.
| Treatment | W value | P value | Parametric data |
|---|---|---|---|
| COL I (T0) | 0.9573 | 0.6787 | YES |
| COL I (T1) | 0.9468 | 0.5123 | YES |
Note. The W and P value are referred to Saphiro-Wilk normally test.
Table 4.
Saphiro-Wilk test results regarding Figure 6.
Table 4.
Saphiro-Wilk test results regarding Figure 6.
| Treatment | W value | P value | Parametric data |
|---|---|---|---|
| REHAB (T0) | 0.9583 | 0.6952 | YES |
| REHAB (T1) | 0.9371 | 0.3820 | YES |
Note. The W and P value are referred to Saphiro-Wilk normally test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



