
Submitted:
24 July 2025
Posted:
25 July 2025
You are already at the latest version
Abstract
Introduction. Dental caries is one of the most widespread oral diseases globally, and Streptococcus mutans is one of the main pathogenic microorganisms involved. The increasingly common use of transparent orthodontic aligners, while offering aesthetic and functional advantages, can promote microbial accumulation and, consequently, increase the risk of caries. The aim of this ex vivo study was to evaluate the antimicrobial efficacy of an ozonized extra virgin olive oil spray (Ialozon Clean), applied to removable orthodontic masks. Material and Methods. Three upper aligners worn by three patients were used for this ex vivo work. Samples were taken with a brush from seven specific points on each device, before and after treatment with the spray. The samples were cultured on Schaedler Agar, analyzed through Gram staining, and colony-forming units (CFU) were counted. Results. A predominance of Gram-positive streptococci in pre-treatment samples and an average reduction of 99.9% in CFU/mL after product application was found. The antimicrobial effect was significant in all patients and analyzed points (p < 0.01).The Discussion. Data support the use of ozonized olive oil as a natural, safe, and effective antimicrobial agent for oral hygiene in orthodontic patients. Furthermore, the ex vivo experimental model developed in this study represents a useful and reproducible tool for testing other formulations with antibacterial action.
Keywords:
ozonized olive oil
; transparent aligners
; streptococcus mutans
; dental caries prevention
; ex vivo model
; oral microbiota
; biofilm control
; orthodontics
; antimicrobial therapy
; dental hygiene
1. Introduction
Dental caries represents one of the most widespread oral diseases worldwide and constitutes a significant public health issue. It results from a multifactorial process involving the demineralization of the hard tissues of the tooth following the metabolic activity of cariogenic microorganisms present in the oral biofilm [1]. Among these, Streptococcus mutans, a Gram-positive bacterium belonging to the mutans streptococci group, plays a central role due to its ability to adhere to dental surfaces, form structured biofilms, metabolize fermentable sugars, and produce organic acids that lower the local pH, promoting enamel demineralization. However, other acidogenic and aciduric cocci such as Streptococcus sobrinus, Streptococcus sanguinis, and Streptococcus gordonii have also been implicated in the cariogenic process, contributing to the ecological shift of the biofilm and the progression of the disease. [1].
In recent years, there has been a growing spread of transparent orthodontic aligners, chosen by many patients for aesthetic and comfort reasons compared to traditional fixed appliances. However, several studies have highlighted how these devices can negatively impact oral health if not accompanied by meticulous oral hygiene. The presence of aligners reduces the natural cleansing action of saliva, creates humid microenvironments with limited oxygen, and can promote the accumulation and maturation of pathogenic biofilm on both the covered dental surfaces and inside the device itself [2,3]. Specifically, it has been demonstrated that patients undergoing treatment with aligners shows increased levels of S. mutans, Lactobacilli, and other acidogenic microorganisms, with a microbial composition similar to that associated with initial caries [4,5].
In this context, prevention becomes a key element, and complementary therapies aimed at reducing the oral bacterial load can provide valuable support. Among the non-pharmacological alternatives gaining increasing interest, ozone has established itself for its known antimicrobial, anti-inflammatory, and tissue regenerative properties. In particular, ozonized vegetable oil, such as extra virgin olive oil, represents a stable, safe, and well-tolerated form for daily use in oral prevention. This type of formulation allows controlled release of ozone in situ, with documented bactericidal effects on numerous oral pathogens, including Gram-positive bacteria, Gram-negative bacteria, yeasts, and fungi [6,7].
Several in vitro studies have demonstrated the effectiveness of ozonized oil in reducing the bacterial load of Streptococcus mutans, suggesting its potential use as an adjunct in caries prevention. The antimicrobial activity is attributed to ozone’s ability to oxidize phospholipids and bacterial membrane proteins, compromising the microorganism’s cellular integrity. Nardi et al. showed significant inhibition of S. mutans growth using a mouthwash based on ozonized olive oil, opening the way for possible clinical applications in home hygiene protocols [7]. Similar results have been confirmed by studies employing ozonized oils on other oral bacterial species, demonstrating a broad spectrum of action [8,9].
Therefore, the home use of ozonized oil could represent a useful and complementary strategy for managing the risk of caries in patients undergoing orthodontic therapy with transparent aligners, thanks to its targeted action against cariogenic microorganisms and ease of use in daily contexts. In this regard, there is a clear need for a cleansing product specifically designed for aligners that is effective against cariogenic bacteria and does not require rinsing after application—such as a spray formulation—which would offer both practicality and compliance in everyday oral hygiene routines.
The purpose of this study was to evaluate, using an ex vivo experimental model, the antimicrobial effectiveness of a sanitizing spray based on ozonized extra virgin olive oil (Ialozon Clean, Gemavip,Cagliari, Italy) applied to removable invisible orthodontic aligners previous worn and no longer used, by real patients. The investigation aimed to quantify the impact of the treatment on the overall bacterial load, with particular reference to Gram-positive bacteria and cariogenic streptococci.
Specifically, the objectives were:
- To determine the quantitative variation of the microbial load before and afterexposure;
- To observe the prevalence of Gram-positive bacteria through Gram staining;
- To evaluate the distribution of microorganisms in different zones of the aligners;
- To verify the feasibility of the experimental protocol for future applications.
2. Results
2.1. Count of Colony-Forming Units (CFU)
The ex vivo analysis of the microbial load on invisible orthodontic aligners showed a significant presence of bacteria, mainly Gram-positive, particularly streptococci. The results related to CFU/mL counts, before and after treatment with the spray based on ozonized oil (Ialozon Clean), highlighted a marked reduction in bacterial load, with inhibition of 99% of CFU/ml.
2.2. Distribution of the Bacterial Load at Different Sampling Points
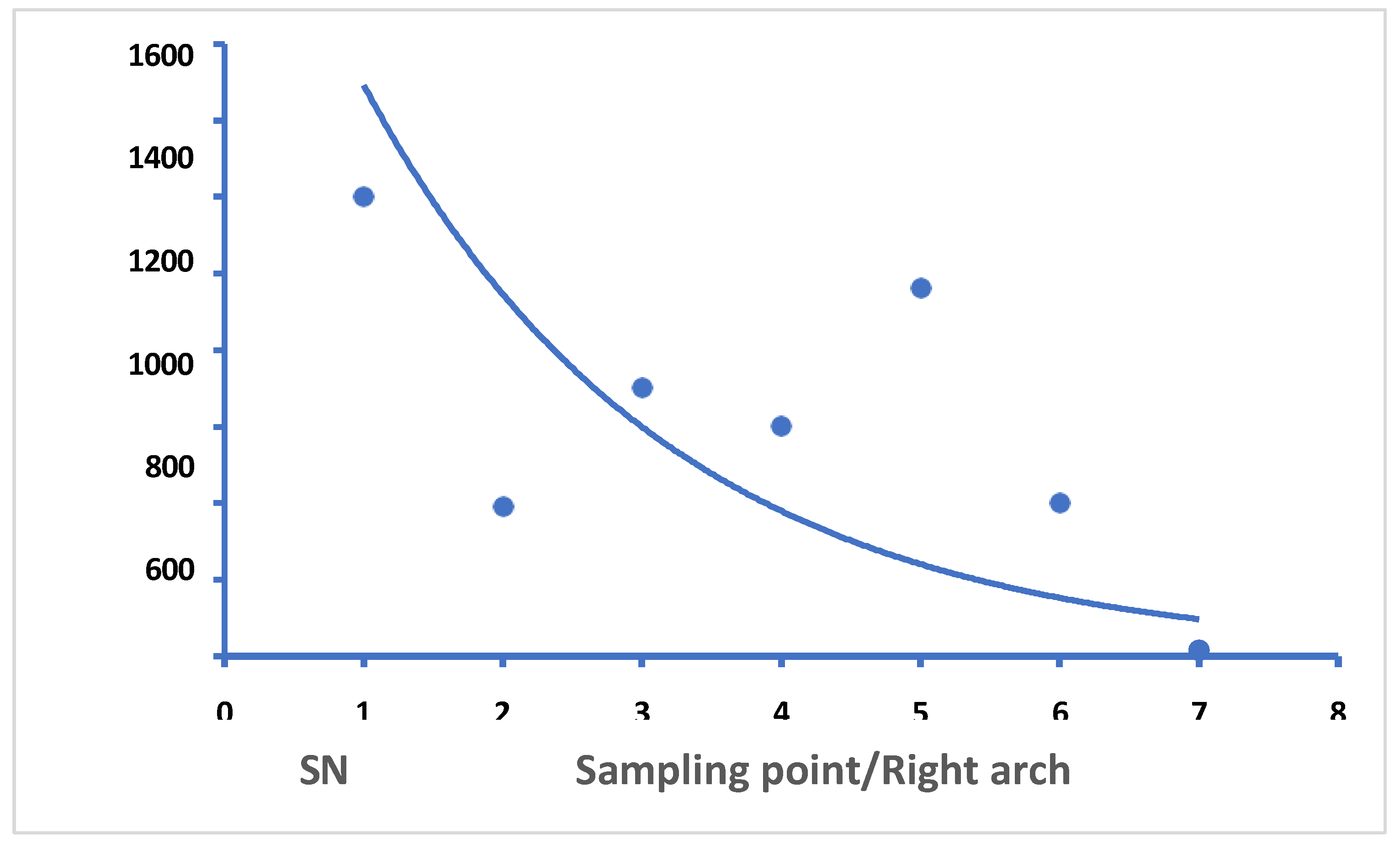
In pre-treatment conditions, samples obtained from the 7 sampling points showed an uneven distribution of CFU along the upper arch. On average, the left semi-arch (points 1–3) had a bacterial density approximately 1000 CFU/mL higher than the right semi-arch (points 5–7), as you can see in Graph 1. This data was confirmed both by direct seeding on agar and by the biofilm imprint (Figure 1), which visually showed a more extensive biofilm on the left portion of the device.
Graph 1.
Bacterial density detected at the 7 sampling points on the aligners worn by patients before treatment. It is possible to notice the great difference between point 1-2 and point 5-6-7.
Graph 1.
Bacterial density detected at the 7 sampling points on the aligners worn by patients before treatment. It is possible to notice the great difference between point 1-2 and point 5-6-7.
The samples taken before treatment, subjected to Gram staining, showed a predominance of Gram-positive microorganisms arranged in short or long chains, morphologically compatible with oral streptococci. Observation confirmed that the microbial flora was mainly composed of cariogenic bacteria associated with dental biofilm, such as Streptococcus mutans, S. sobrinus, and other similar species.
After treatment with the ozonized spray, microscopic observation revealed a clear reduction in microbial density and almost total absence of cellular aggregates in the prepared slides.
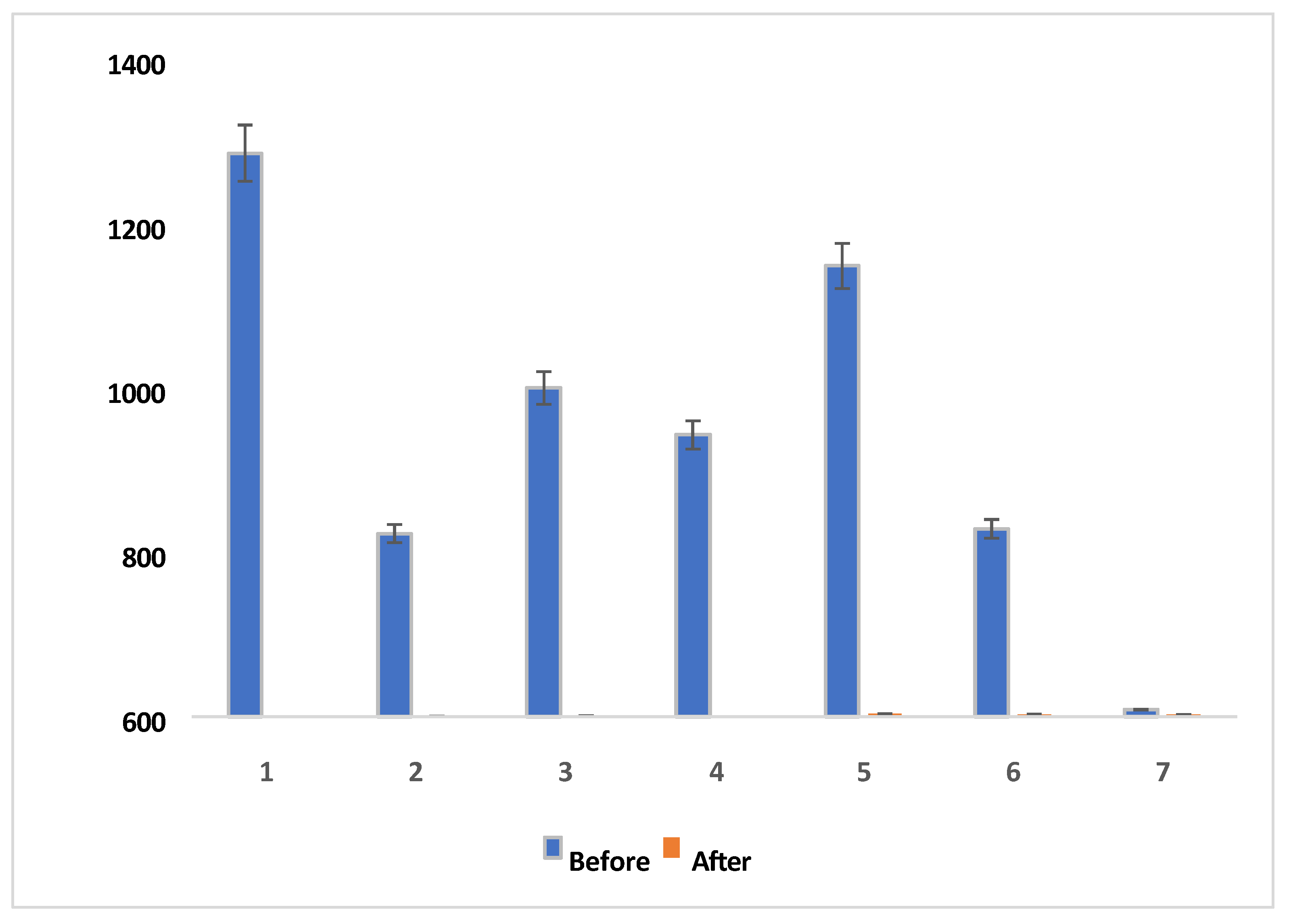
The treatment with Ialozon Clean resulted in an average reduction of microbial load by 99.9% in all analyzed samples. This effect was consistent across all sampling points of all aligners tested (Graph 2).
Graph 2.
direct comparison between the average values of CFU/mL before and after treatment at points 1 and 7 (representative example).
Graph 2.
direct comparison between the average values of CFU/mL before and after treatment at points 1 and 7 (representative example).
Imprinting culture of aligners after spray application showed no macroscopic bacterial growth, with plates sterile or almost sterile, confirming the antimicrobial effectiveness of the product.
2.3. Statistical Analysis
The statistical analysis, conducted with Fisher’s exact test, confirmed the significance of the reduction in microbial load after treatment in all analyzed sites (p < 0.01). The significance was also confirmed for the difference between semi-arches (right vs. left) in pre-treatment conditions (p < 0.05), suggesting a possible asymmetry of contamination related to individual factors (such as predominant chewing, tongue posture, or selective hygiene) (Table 1).
3. Discussion
Dental caries is one of the most common oral diseases, caused by a multifactorial interaction between diet, oral hygiene, biofilm composition, and individual predisposition. Streptococcus mutans is universally recognized as the main pathogenic agent involved in the development of caries due to its high adhesion capacity, production of organic acids, and formation of protective biofilm [10].
The increasing use of transparent orthodontic aligners, although advantageous from an aesthetic and functional point of view, presents a new clinical challenge. Literature has shown that these devices, covering the entire dental surfaces for many hours a day, reduce the buffering effect of saliva and create microenvironments conducive to bacterial accumulation [2,3]. Several studies have reported an increase in oral streptococcal load in patients wearing aligners, with changes in microbial composition compatible with a state of dysbiosis and an increased risk of caries [11].
In our study, treating aligners with Ialozon Clean – an ozone-infused extra virgin olive oil spray – resulted in an average reduction of 99.9% of the total bacterial load. This reduction was statistically significant at all sampling points analyzed, as confirmed by statistical analysis (p < 0.01), and was accompanied by the almost complete disappearance of visible bacterial aggregates under the microscope. The results confirm the antimicrobial efficacy of the formulation even in ex vivo conditions, simulating realistic patient use.
Comparing our data with the literature, there is consistency with what was reported by Nardi et al., who demonstrated the effectiveness of an ozone-infused mouthwash in reducing S. mutans in an in vitro study, highlighting the potential of this formulation in caries prevention [7]. Our ex vivo experimental protocol, based on direct sampling of worn aligners, adds clinical value to these observations, confirming the product’s effectiveness under operational conditions closer to everyday reality.
Pietropaoli et al. compared an ozone oil-based gel with two formulations containing chlorhexidine, showing comparable effectiveness in reducing periodontal pathogens (S. mutans, A. actinomycetemcomitans, P. intermedia), although the effect on S. mutans was slightly lower, probably due to limited penetration of the gel into the biofilm matrix [12]. However, our spray administration allowed for more uniform distribution and greater contact surface with the device, likely improving antimicrobial efficacy, as evidenced by post-treatment cultures.
The antibacterial activity of ozone is well known and extensively documented. Sechi et al. demonstrated that ozone oil is effective against Gram-positive and Gram-negative bacteria, involving a mechanism of action that includes direct oxidation of cell membranes and intracellular components [6]. Kurek-Górecka et al. confirmed that ozonized oils can be considered a modern alternative for treating various oral infections, thanks to their stability, safety, and good tolerability [8]. Consistently, Cvikl et al. demonstrated in vitro the impact of ozone on S. mutans and C. albicans, observing a marked inhibition of bacterial growth and vitality [9].
A general review on the use of ozonized water and oils in dentistry was proposed by Kshitish and Laxman [13], highlighting the benefits related to biocompatibility and antimicrobial efficacy.
Ozonized water has also been proposed as an alternative to traditional mouthwashes: studies like that of Ramzy et al. reported good efficacy in managing aggressive periodontitis [14]. Moreover, some studies have demonstrated the effectiveness of ozone as an adjunctive therapy in non-surgical periodontal treatment [15]. Researchers have recently found interesting results of ozonized water against S. mutans, with a decrease of CFU/ml from 108 to 104 after exposure to an ozone concentration of 0,060 mg/l, but no product in the literature reduced the Streptococci load nearly 100% [16]. However, the need for immediate preparation and the limited stability restricts the applicability of ozone in aqueous form. Conversely, oil-based formulations like Ialozon Clean are stable, ready to use, and easy to administer, facilitating patient adherence and ensuring a gradual and prolonged release of ozone.
Another interesting element from our study was the uneven distribution of bacterial load between the two hemi-arches, with higher values on the left side. This asymmetry, statistically significant (p < 0.05), could reflect individual variables such as dominant mastication, lingual position, manual preference in oral hygiene, or palatal anatomical conformation. Although not the main objective of the study, this observation opens avenues for further research on biofilm ecology in relation to behavioral factors.
The clinical relevance of this finding is particularly significant given the widespread adoption of clear aligner therapy, which has become a common orthodontic approach due to its aesthetic and functional advantages. Recent reports estimate that the global clear aligner market will reach over USD 30 billion by 2030, driven by increasing demand among adolescents and adults [17]. Simultaneously, dental caries remains the most prevalent oral disease globally, with over 2.5 billion people affected by untreated caries in permanent teeth, as reported by the Global Burden of Disease Study [18]. The combination of the growing use of removable orthodontic appliances and the persistently high global burden of caries underscores the urgent need for effective preventive strategies aimed at minimizing biofilm accumulation and reducing caries risk in this specific patient population.
Finally, the almost total absence of bacterial growth observed on plates inoculated with the impression of the aligners after treatment suggests not only the product’s effectiveness in reducing microbial load but also a potential contribution to maintaining the transparency of the device, improving aesthetics and overall hygiene of orthodontic treatment.
Overall, the results confirm that using spray of ozonized oil, as our product tested, can be an effective and safe strategy for reducing microbial load in patients treated with transparent aligners. The direct spray administration, product stability, and clinical tolerability make it a valuable home adjunct in caries prevention. These data justify the design of future controlled clinical in vivo studies, with medium-long-term follow-up and a larger number of subjects.
4. Materials and Methods
4.1. Design of the Study and Selection of Samples
The study was conducted with an ex vivo experimental design on removable transparent orthodontic devices (invisible aligners) worn by real patients and not longer used by them.
Aligners belonging to 3 volunteer subjects (2 females, 1 male; aged between 18 and 35 years) were used, all patients were subjected to active orthodontic treatment with invisible aligners on the upper arch for at least two weeks.
Inclusion criteria:
- Age ≥18 years
- Orthodontic treatment in progress with invisible aligners (upper arch)
- Worn documented ≥20 hours per day
- Absence of active carious lesions visible at the time of sampling
- Absence of clinically evident gingivitis or periodontitis
- Availability to sign an informed written consent
Exclusion criteria:
- Antibiotic or systemic antimicrobial therapy in the previous 2 weeks
- Systemic immunosuppressive or chronic diseases
- Pharmacological therapies that alter the oral flora (antihistamines, corticosteroids, etc.)
- Pregnancy or breastfeeding
- Use of oral antiseptic products within 48 hours prior to sampling
The study did not involve human participants, but only the analysis of discarded orthodontic aligners. The aligners were voluntarily donated by patients after clinical use. All participants provided written informed consent authorizing the use of their no-longer-needed aligners for research purposes.
4.2. Samples Collection
Each aligner-donor patient was instructed not to remove the aligner for at least 2 hours before sampling. The upper arch aligner was then removed directly at the chair and placed in a sterile Petri dish (diameter 90 mm) with pre- and post-treatment identification labels.
Seven distinct samples were taken from each aligner (21 in total), corresponding to specific contact points between the mask and dental surface (Figure 2). The points were selected to cover the entire maxillary arch evenly.
The samples were collected using sterile cotton swabs, vigorously rubbed for 10 seconds on each designated area. Each swab was then immersed in a sterile Eppendorf tube containing 1 mL of Brain Heart Infusion (BHI) broth, a nutrient medium with high support capacity for demanding oral microorganisms, particularly Streptococcus mutans.
4.3. Preparation and Cultivation of Samples
After immersion, each test tube was manually shaken for 30 seconds to homogenize the microbial suspension. Subsequently, 100 µL of solution with Eppendorf® tube was taken from each sample and put in a 90 mm Petri dish containing Schaedler Agar medium (Microbiol, Uta, Itly, a selective medium for aerobic and facultative anaerobic microorganisms of the oral cavity).
The 21 Petri dishes contaminated were incubated at 37°C for 24 hours in a controlled atmosphere with 5% CO₂, to favor the growth of the specific bacteria. After incubation, the colony-forming units (CFU) were counted in each Petri dish, evaluating the growth density for each sampled point.
4.4. Treatment with Ozonized Oil
After the first cycle of withdrawals and sowing, each aligner was treated with Ialozon Clean (Gemavip, Cagliari, Italy), a disinfectant spray based on:
- Ozonized extra virgin olive oil
- Hyaluronic acid
- Tea Tree Oil
- Cetilpiridinio Cloruro
- Aloe Vera
- Amine fluoride
- Vitamin E
- Zinc
- Sodium bicarbonate
The application method involved 3-4 direct sprays from about 5 cm away onto the inner surface of the aligner. After application, the device was air-dried for 2 minutes without rinsing, following the product’s instructions for daily home treatment.
The second collection cycle was performed using the same method as the first, replicating points and sequences, in this way we have other 21 Petri dishes contaminated with sample taken in each of 7 points for each of the three aligners, that are incubated with the same procedures previous described.
A comparison of the CFUs for each Petri dish contaminated with brushes in each points selected, before and after spray exposure was performed.
4.5. Gram Staining and Microscopic Observation
For each sample, a slide was prepared for Gram staining, used to identify the microbiological composition of the bacterial biofilm. The swab content was smeared on a microscope slide, dried, and fixed with a flame.
The coloring protocol provided (Figure 3):
- Application of crystal violet dye for 60 seconds
- Wash with water
- Application of iodine solution (Lugol) for 60 seconds
- Quick decolorization with alcohol-acetone (5–10 seconds)
- Counterstaining with basic fuchsin for 40–60 seconds
- Final washing, air drying, and observation at 1000x magnification with immersion oil
The morphological characteristics and coloration (Gram-positive = purple; Gram-negative = red) of microorganisms have been documented.
4.6. Statistical Analysis
All measurements (CFU) were performed in triplicate for each sampling point. The data were processed by calculating geometric means and standard deviations.
The significance of differences between pre- and post-treatment conditions was assessed using Fisher’s exact test, with the SocialStatistics software (https://www.socscistatistics.com/tests/fisher/). Differences were considered statistically significant for p < 0.01.
5. Conclusions
This experimental ex vivo study demonstrated that the ozone-based olive oil spray Ialozon Clean can significantly reduce (99.9%) the bacterial load on invisible orthodontic aligners, with documented effects both microbiologically and microscopically.
The proposed protocol, simple, repeatable, and free of side effects, is suitable for daily home use in orthodontic patients, representing a valid alternative to traditional chemical disinfectants. The product’s action extends not only to reducing the cariogenic streptococcal component but also to the overall improvement of the hygienic quality of the aligners, with potential aesthetic and functional benefits.
The results obtained provide a concrete basis for the clinical application of the product, as well as for further in vivo research on larger samples and prolonged observation periods, aimed at validating its effectiveness in real-world settings. Additionally, the ex vivo experimental model used in this thesis can be replicated and adapted for the study of other formulations with antibacterial action, contributing to the evolution of oral hygiene practices in modern orthodontics.
The study also aims to serve as a methodological basis for the validation of additional antimicrobial devices or formulations intended for the decontamination of aligners, thereby contributing to the prevention of carious lesions in orthodontic patients
Funding
This research received no external funding
Institutional Review Board Statement
Ethical review and approval were not required for this study, as it did not involve human participants but only the analysis of discarded orthodontic aligners. The study was conducted in accordance with the Declaration of Helsinki. The aligners were voluntarily donated by patients who had completed their clinical use. All patients provided written informed consent authorizing the use of their no-longer-needed aligners for research purposes. The donated aligners were not reused by the patients and would have otherwise been discarded.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007;369(9555):51-59. [CrossRef]
- Levrini L, Mangano A, Montanari P, Margherini S, Caprioglio A. Periodontal health status in patients treated with the Invisalign® system and fixed orthodontic appliances: a 3 months clinical and microbiological evaluation. Eur J Dent. 2015;9(3):404-410. [CrossRef]
- Lombardo L, Arreghini A, Bratti E, et al. Changes in the oral microbiota due to clear aligners: a prospective study. Prog Orthod. 2021;22(1):26. [CrossRef]
- Mummolo S, Marchetti E, Giuca MR, et al. In-office bacteria test for a microbial monitoring during orthodontic treatment. Head Face Med. 2013;9:7. [CrossRef]
- Guo R, Lin Y, Zheng Y, Li W. The microbial changes in subgingival plaques of orthodontic patients: a systematic review and meta-analysis of clinical trials. BMC Oral Health. 2017;17(1):90. [CrossRef]
- Sechi LA, Lezcano I, Nunez N, et al. Antibacterial activity of ozonized sunflower oil (Oleozon). J Appl Microbiol. 2001;90(2):279-284. [CrossRef]
- Nardi GM, Fais S, Casu C, et al. Mouthwash based on ozonated olive oil in caries prevention: a preliminary in-vitro study. Int J Environ Res Public Health. 2020;17(23):9106. [CrossRef]
- Kurek-Górecka A, Górecki M, Rzepecka-Stojko A, Balwierz R, Stojko J. Ozonated oils as a modern therapy in dentistry and medicine. Molecules. 2021;26(10):3261. [CrossRef]
- Cvikl B, Lussi A, Gruber R. The in vitro impact of ozone on the growth of Streptococcus mutans and Candida albicans. Clin Oral Investig. 2015;19(2):303-309. [CrossRef]
- Loesche, WJ. Role of Streptococcus mutans in human dental decay. Microbiol Rev. 1986;50(4):353-380.
- Guo R, Lin Y, Zheng Y, et al. Alteration of oral microbiota in patients with clear aligners. Appl Microbiol Biotechnol. 2019;103(1):1323–1330.
- Pietropaoli D, Ortu E, Mummolo S, et al. Ozonized olive oil in the treatment of chronic periodontitis: a clinical and microbiological study. J Clin Exp Dent. 2018;10(11):e1103-e1108. [CrossRef]
- Kshitish D, Laxman VK. The use of ozonated water and ozonated oil in dentistry: a review. Indian J Dent Res. 2010;21(4):537–539.
- Ramzy MI, Gomaa HE, Mostafa MI. Management of aggressive periodontitis using ozonized water. Egypt Med J NRC. 2005;6:229–245.
- Butera A, Scribante A, Maiorani C, Chiesa A, Segù M, Rodriguez Y R. Split mouth randomized controlled trial: Standard therapy vs ultrasonic therapy with ozone gas application. International Journal of Clinical Dentistry, March 2021;14(2):115-131.
- Casu C, Orrù G, Fais S, Mazur M, Grassi R, Grassi RF, Nardi GM. Efficacy of ozonated water as a PS in photodynamic therapy: A tool for dental caries management? An in vitro study. J Public Health Res. 2023 Jun 24;12(2):22799036231182267. [CrossRef] [PubMed] [PubMed Central]
- MarketsandMarkets. Clear Aligners Market by Age Group (Teen, Adult), Material Type (Polyurethane, Plastic Polyethylene Terephthalate Glycol), End User (DSO, Hospitals, Standalone Practices), and Region - Global Forecast to 2030. 2022.
- GBD 2019 Oral Disorders Collaborators. Global, regional, and national burden of oral conditions in 195 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. J Dent Res. 2022;101(4):392–400. [CrossRef]
Figure 1.
Result of bacterial growth around the orthodontic appliance through imprint culture.
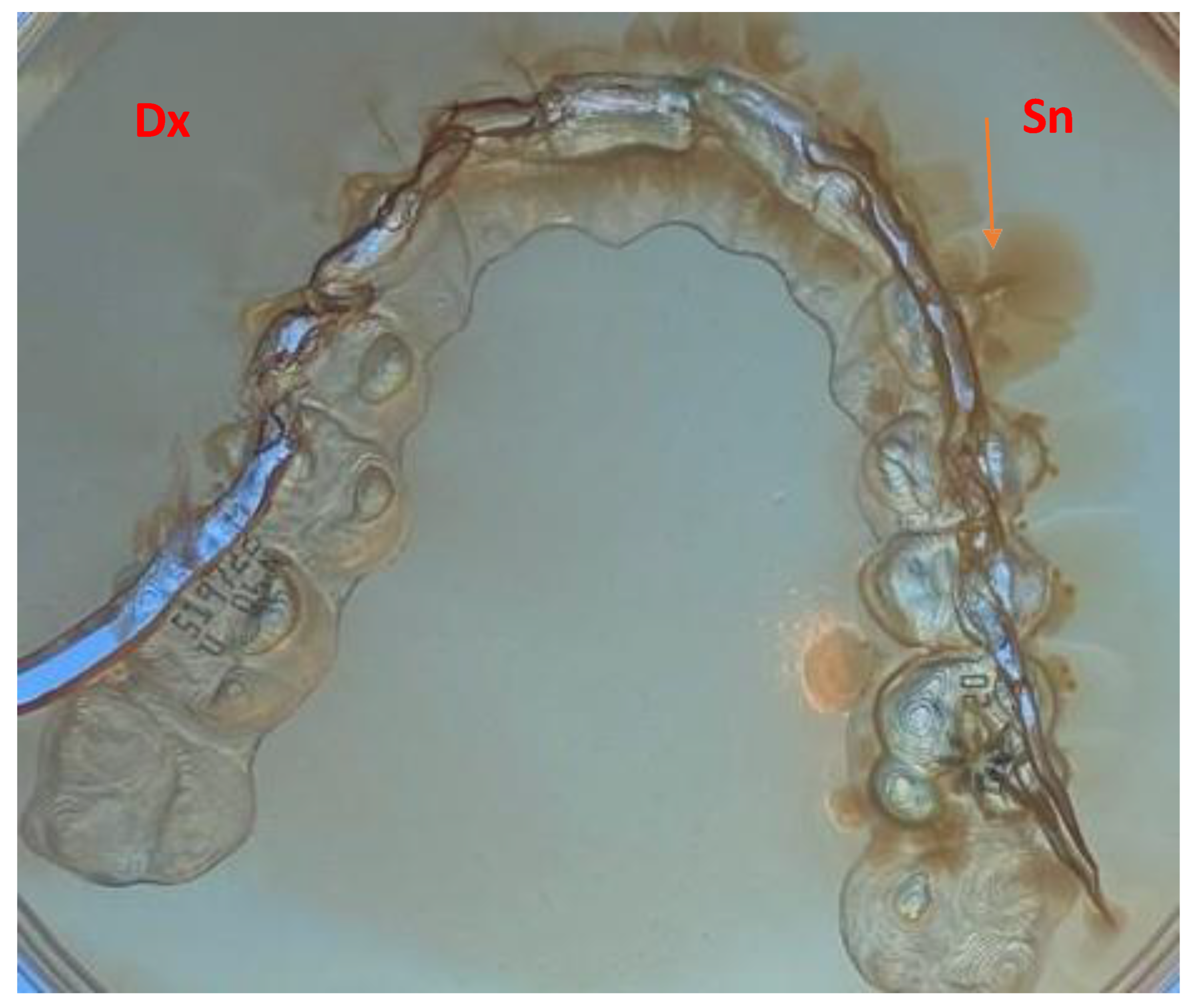
Figure 2.
transparent orthodontic appliance used and site of sampling.

Figure 3.
Diagram of the Gram staining procedure.
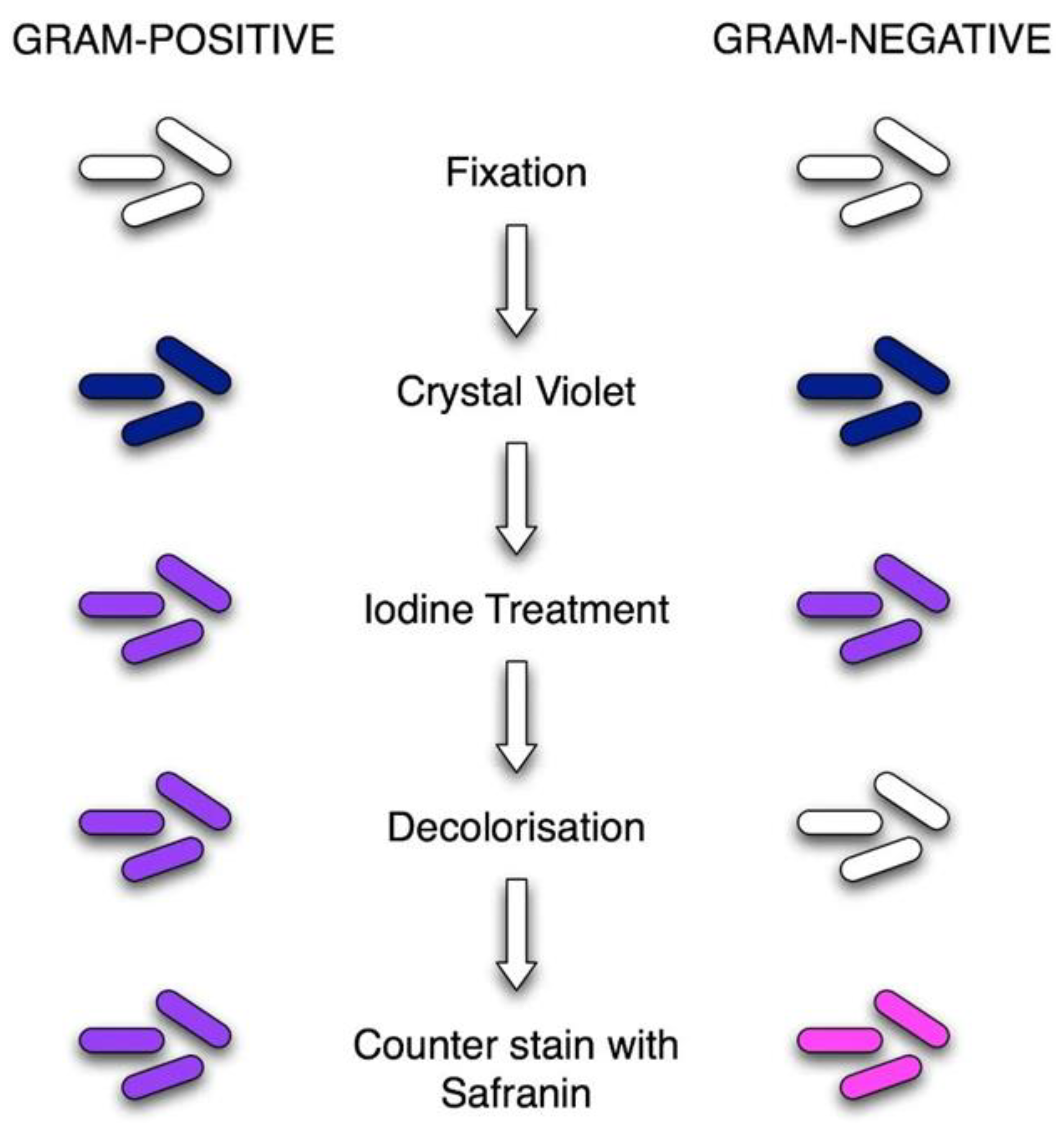

Table 1.
Summary of Results obtained with comparison of CFU values before and after treatment for point 1,4,7.
Table 1.
Summary of Results obtained with comparison of CFU values before and after treatment for point 1,4,7.
| PARAMETER | PRE-TREATMENT (MEAN ± SD) | POST-TREATMENT (MEAN ± SD) | REDUCTION % | SIGNIFICANCE |
|---|---|---|---|---|
| CFU/ML POINT 1 | 1400 ± 120 | 12 ± 5 | 99,1% | p < 0.01 |
| CFU/ML POINT 4 | 1350 ± 100 | 10 ± 4 | 99,3% | p < 0.01 |
| CFU/ML POINT 7 | 1500 ± 140 | 8 ± 3 | 99,5% | p < 0.01 |
| GENERAL MEDIA | 1380 ± 130 | 10 ± 4 | 99,3% | p < 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



