
Submitted:
24 July 2025
Posted:
25 July 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
(1) Background: COVID-19 sepsis, marked by hyperinflammation and cardiac injury, poses significant challenges in high-comorbidity populations. This prospective cohort study evaluates the prognostic value of IL-6, troponin, NT-proBNP, and radiological findings for mortality and critical outcomes in a post-2022 Eastern European cohort. (2) Methods: At "Victor Babes" Hospital, Timisoara, Romania (September 2022–December 2024), 207 adults with COVID-19 sepsis (Sepsis-3 criteria) were enrolled. Baseline IL-6, troponin, NT-proBNP, CRP, PCT, D-dimers, and chest CT lung involvement were measured. Unfavorable outcomes (in-hospital death, ICU transfer, mechanical ventilation, or vasopressor use) were analyzed using logistic and linear regression. (3) Results: Among 207 patients (mean age 68.7 years, 54.1% male), 52 (25.1%) experienced unfavorable outcomes. Multivariable analysis identified IL-6 (OR 1.016, p = 0.013), troponin (OR 1.013, p = 0.017), NT-proBNP (OR 1.009, p = 0.049), >50% lung involvement (OR 1.835, p = 0.011), unvaccinated status (OR 2.312, p = 0.002), and higher BMI (OR 1.112, p = 0.005) as independent predictors of critical outcomes. Tocilizumab use (n=12) was associated with reduced mortality (p = 0.041). IL-6 (cut-off 39.0 pg/mL, AUC 0.91) and troponin (cut-off 111.3 ng/L, AUC 0.88) showed strong predictive accuracy. (4) Conclusions: Elevated IL-6, troponin, NT-proBNP, severe lung involvement, unvaccinated status, and higher BMI predict adverse outcomes in COVID-19 sepsis. Tocilizumab may offer survival benefits, warranting larger trials. These findings support targeted risk stratification in high-comorbidity populations.
Keywords:
COVID-19
; sepsis
; IL-6
; troponin
; NT-proBNP
; vaccination status
; BMI
; tocilizumab
; mortality
; prognostic biomarkers
1. Introduction
Sepsis, a life-threatening condition arising from a dysregulated host response to infection, continues to pose a profound global health challenge, claiming around 11 million lives each year [1,2]. The advent of COVID-19, triggered by SARS-CoV-2, has unveiled a distinctive viral sepsis marked by intense hyperinflammation, endothelial disruption, and a heightened prothrombotic state, especially burdensome in those with underlying comorbidities [3,4]. At its core, the pathophysiology reflects a delicate yet often unbalanced tug-of-war between pro-inflammatory and anti-inflammatory forces, where cytokines like tumor necrosis factor-α (TNF-α) and interleukin-1β (IL-1β) initiate a cascade that amplifies immune activation, increases vascular permeability, and culminates in widespread tissue damage [5,6]. This escalating cytokine storm not only fuels acute respiratory distress but also drives multi-organ failure, underscoring the urgent need to unravel these mechanisms for better patient outcomes [7,8].
Central in the pathophysiology of inflammation is interleukin-6 (IL-6), a cytokine secreted by monocytes, macrophages, and endothelial cells in reaction to infectious threats. Stimulated by upstream signals such as TNF-α, IL-6 perpetuates immune imbalance, orchestrating acute phase responses and intensifying organ harm through sustained inflammation [9,10,11]. Elevated IL-6 levels are associated with disease severity, predicting higher risks of mechanical ventilation and mortality [12,13]. Recent studies reinforce IL-6's role as a robust predictor of severity and mortality in critically ill COVID-19 patients, highlighting its potential as a cornerstone for early intervention strategies [14,15].
Beyond IL-6, other inflammatory and coagulopathic biomarkers have proven valuable in COVID-19 sepsis. C-reactive protein (CRP) and procalcitonin (PCT) are widely used to gauge systemic inflammation and bacterial superinfection, often rising in parallel with disease severity [16,17]. Elevated D-dimer levels reflect underlying coagulopathy and thrombotic risk, frequently observed in severe COVID-19 and linked to worse clinical outcomes [18,19].
Heart involvement in COVID-19 sepsis, evidenced by surges in troponin and N-terminal pro-B-type natriuretic peptide (NT-proBNP), emerges as a critical and frequent complication tied to myocardial strain and injury [20,21]. Troponin spikes often stem from direct viral assault, oxygen deprivation, or inflammation-driven assaults on cardiac structures, strongly correlating with cardiovascular risks and death [22,23]. NT-proBNP, signaling cardiac overload, rises markedly in severe cases (even among patients without prior heart failure), reflecting hemodynamic stress and volume overload in acute COVID-19 illness [15,17]. There are studies affirming that heightened troponin and NT-proBNP levels serve as key harbingers of increased mortality and disease gravity in COVID-19 cases, emphasizing their value in prognostic assessments [19,23].
In parallel, severe COVID-19 affects the lower respiratory tract, resulting in substantial pulmonary injury characterized by diffuse alveolar damage, extensive inflammation, and impaired gas exchange [24,25]. This damage frequently necessitates supplemental oxygen therapy and mechanical ventilation support in severe cases. Chest computer tomography (CT) scans play a pivotal role in assessing the extent and progression of lung involvement, typically revealing characteristic findings such as bilateral ground-glass opacities, consolidation, and interstitial changes [26,27].
While numerous studies have explored individual aspects of COVID-19-related sepsis, few have combined inflammatory, cardiac, and radiological markers within a unified prognostic framework, particularly in observational, real-world settings. This study contributes to the growing body of evidence by integrating routinely available biomarkers, imaging findings, and clinical parameters—such as vaccination status and body mass index—to better reflect the complexity of patient care in high-comorbidity populations. In doing so, it aims to enhance current understanding of risk stratification and support more informed, context-specific clinical decision-making. Specifically, our prospective cohort study, set within a high-comorbidity Eastern European demographic, seeks to assess the prognostic significance of IL-6, troponin, NT-proBNP, and chest CT-detected lung involvement, integrated with clinical elements like vaccination status and body mass index, in forecasting mortality and critical endpoints in COVID-19-associated sepsis.
2. Materials and Methods
2.1. Study Design and Population
This prospective cohort study was conducted at the "Victor Babes" Infectious Diseases and Pneumology Hospital in Timisoara, Romania, from September 1, 2022, to December 31, 2024. Adult patients (≥18 years) were prospectively enrolled in this study if: (1) they had a confirmed COVID-19 diagnosis via a positive RT-PCR test; (2) they were diagnosed with sepsis at admission, per Sepsis-3 criteria [1], defined as a Sequential Organ Failure Assessment (SOFA) score ≥2 in the context of suspected or documented infection; (3) the patient or their legal representative signed informed consent prior to study enrolment. Exclusion criteria were: (1) septic shock at admission (requiring mechanical ventilation or vasopressors); (2) incomplete data (e.g., missing imaging or biomarker data); (3) refusal to sign informed consent for study participation (providing reason for refusal was not mandatory). Ethical approval was obtained from the Ethics Board of "Victor Babes" University of Medicine and Pharmacy, Timisoara (reference: 70/01.09.2022, revised 2174/10.03.2023). This study was conducted in accordance with the Declaration of Helsinki. Thie study protocol was not prospectively registered in any database. No power analysis was conducted prior to patient enrolment.
2.2. Data Collection
At admission, patients underwent clinical evaluation, and the following data was collected: age, sex, vaccination status, smoking status, alcohol consumption, body mass index (BMI), comorbidities, and based on the comorbidity data, the Charleson Comorbidity Index (CCI) was calculated. Clinical data included symptom onset to admission duration, peripheric oxygen saturation (SpO2), and oxygen requirements. Chest computer tomography(CT) scans categorized lung involvement as:>50%, 25-50%, and <25%. Laboratory biomarkers included interleukin-6 (IL-6, pg/mL) measured using the Quantikine HS ELISA kit (R&D Systems, Minneapolis, MN, USA), troponin (ng/L) measured via the Elecsys Troponin T hs assay (Roche Diagnostics, Basel, Switzerland), N-terminal pro-B-type natriuretic peptide (NT-proBNP, pg/mL) measured via the ElecsysproBNP II assay (Roche Diagnostics, Basel, Switzerland), C-reactive protein (CRP, mg/L), procalcitonin (PCT, ng/mL), D-dimers (µg/mL), erythrocyte sedimentation rate (ESR), ferritin, and neutrophil-to-lymphocyte ratio (NLR). IL-6 was measured using enzyme-linked immunosorbent assay (ELISA), troponin via high-sensitivity chemiluminescence, and NT-proBNP via electrochemiluminescence, following standard protocols at the hospital’s laboratory. CRP, PCT, and D-dimers were measured using automated immunoassays (turbidimetry for CRP, chemiluminescence for PCT, and latex-enhanced immunoturbidimetry for D-dimers). Electrocardiogram (EKG) assessed heart rate, ischemic changes, and hypertrophy. Prospective data collection included treatment options during hospital stay (antivirals, antibiotics, corticosteroids, tocilizumab). Tocilizumab was administered to patients with severe COVID-19 sepsis, defined by IL-6 levels >40 pg/mL and oxygen requirements >15 L/min, based on clinical guidelines and physician discretion. The primary outcome was a composite adverse outcome: in-hospital death, ICU transfer, mechanical ventilation, or vasopressor use.
2.3. Statistical Analysis
Descriptive statistics summarized characteristics. Continuous variables were reported as means (SD) or medians (IQR) based on normality (Shapiro-Wilk test). Categorical variables were frequencies (%). Univariate comparisons employed t-tests for normally distributed data, Mann-Whitney U tests for non-normally distributed data, or Chi-square/Fisher’s exact tests for categorical data. Multivariable logistic regression was performed on predictors that were significant in the univariate analysis (p < 0.05). Model fit was assessed via Hosmer-Lemeshow test. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Additional sensitivity analyses were performed, excluding tocilizumab-treated patients, to confirm robustness. Missing data were minimal (<5% for any variable) and handled by listwise deletion, as imputation was deemed unnecessary due to the low proportion of missing values. Receiver Operating Characteristic (ROC) curves were generated for key predictors (IL-6, troponin, D-dimers) to estimate area under the curve (AUC) and optimal cut-offs determined by Youden's index. ROC cut-offs (e.g., IL-6 39.0 pg/mL) were determined post-hoc to identify optimal thresholds for predicting unfavorable outcomes. Analyses used SPSS Statistics v26 (IBM Corp., Armonk, NY, USA), with p < 0.05 significant.
3. Results
3.1. General Characteristics of Study Population
During the study enrolment period (September 1, 2022 – December 31, 2024), 276 patients were eligible for inclusion, but 51 patients (or their legal representatives) refused to signed informed consent and were therefore excluded, and 18 patients were excluded due to missing data (mostly for a lack of troponin, NT-proBNP, and/or IL-6 measurements upon admission). This left a total number of 207 included patients who were admitted into our hospital with COVID-19-related sepsis. Their baseline characteristics are summarized in Table 1.
The mean age was 68.7 years (SD 11.2), with 112 males (54.1%). Most patients (85.0%) were unvaccinated, while 31 (15.0%) were vaccinated. The mean time from symptom onset to admission was 4.2 days (SD 1.5). Smoking was reported in 64 patients (30.9%), and frequent alcohol consumption in 78 (37.7%). The mean body mass index (BMI) was 28.7 (SD 3.7). Comorbidities were prevalent: hypertension (81.6%), diabetes (34.8%), and coronary artery disease (20.3%). The mean Charlson Comorbidity Index (CCI) was 3.1 (SD 1.3). Chest CT showed >50% lung involvement in 81 patients (39.1%), 25–50% in 74 (35.7%), and <25% in 52 (25.1%). The mean oxygen saturation (SpO2) was 90.1% (SD 5.7), with 95 patients (45.9%) requiring >15 L/min oxygen. The mean Sequential Organ Failure Assessment (SOFA score) was 6.3 (SD 2.4). Baseline biomarkers indicated inflammation: interleukin-6 (IL-6) 32.4 pg/mL (SD 15.6), troponin 98.7 ng/L (SD 45.2), N-terminal pro-B-type natriuretic peptide (NT-proBNP) 567.2 pg/mL (SD 234.1), C-reactive protein (CRP) 111.8 mg/L (SD 45.2), procalcitonin (PCT) 2.3 ng/mL (SD 1.2), and D-dimers 1.1 µg/mL (SD 0.8). EKG abnormalities were observed in 55 patients (26.6%). Treatments included remdesivir (91.3%), antibiotics (85.5%), corticosteroids (98.6%), and tocilizumab (12 patients, 5.8%). Tocilizumab use was associated with reduced mortality (p = 0.041). Adverse outcomes occurred in 52 patients (25.1%): 42 ICU transfers, 38 required mechanical ventilation and 28 died.
3.2. Univariate Analysis of Factors Associated with Unfavorable Outcomes
The cohort (N=207) was divided into two groups: favorable (n=155) and unfavorable (n=52). Table 2 compares the baseline characteristics of the favorable and unfavorable outcome groups. Age was higher in the unfavorable group (76.2 vs. 66.3 years, p = 0.0001). The Charlson Comorbidity Index (CCI) was elevated in the unfavorable group compared to the favorable group (3.8 vs. 2.8, p = 0.0002). CT severity was statistically higher in the unfavorable group compared to the favorable group (p = 0.033). The mean IL-6 was 27.3 pg/mL in the favorable group and 48.7 pg/mL in the unfavorable group, and the difference was statistically significant (p = 0.012). The mean troponin level was 78.9 ng/L in the favorable group and 145.2 ng/L in the unfavorable group (p = 0.008). The mean NT-proBNP was 489.3 pg/mL in the favorable group and 789.4 pg/mL in the unfavorable group (p = 0.015). The mean CRP was 111.8 mg/L in both groups, with no significant difference (p = 0.950), as shown in Figure 1. The mean D-dimers was 1.1 µg/mL in both groups, with no significant difference (p = 0.920). Body mass index (BMI) was significantly higher in the unfavorable group compared to the favorable group (30.5 vs. 27.3, p = 0.0003). Vaccination status showed a significant difference, with 20.0% vaccinated in the favorable group and 0.0% in the unfavorable group (p = 0.001). EKG changes showed no significant difference between groups (26.5% vs. 26.9%, p = 0.950). Oxygen flow >15 L/min showed a trend toward significance (p = 0.072). No differences were found for sex, smoking, or PCT.
3.3. Multivariable Analysis of Predictors of Unfavorable Outcomes
Multivariable logistic regression was performed to identify predictors of critical events in the cohort (N=207), including CCI, IL-6, troponin, NT-proBNP, CRP, D-dimers, lung involvement (>50% vs. ≤50%), vaccination status, and BMI (Table 3). Independent predictors of unfavorable outcomes were IL-6 (OR 1.016, 95% CI 1.004–1.028, p = 0.013), troponin (OR 1.013, 95% CI 1.003–1.023, p = 0.017), NT-proBNP (OR 1.009, 95% CI 1.000–1.018, p = 0.049), >50% lung involvement (OR 1.835, 95% CI 1.150–2.927, p = 0.011), vaccination status (unvaccinated vs. vaccinated, OR 2.312, 95% CI 1.342–3.986, p = 0.002), and BMI (OR 1.112, 95% CI 1.032–1.198, p = 0.005). CCI (p = 0.060) and age (p = 0.070) showed trends toward significance. CRP (p = 0.910) and D-dimers (p = 0.930) were not significant predictors, consistent with their lack of difference between groups. The Hosmer-Lemeshow test indicated a good model fit (p = 0.065). Sensitivity analysis excluding tocilizumab-treated patients (n=12) confirmed the robustness of the model, with IL-6 (OR 1.014, 95% CI 1.002–1.026, p = 0.018), troponin (OR 1.012, 95% CI 1.002–1.022, p = 0.021), NT-proBNP (OR 1.008, 95% CI 0.999–1.017, p = 0.053), >50% lung involvement (OR 1.805, 95% CI 1.132–2.878, p = 0.013), vaccination status (OR 2.287, 95% CI 1.328–3.941, p = 0.003), and BMI (OR 1.108, 95% CI 1.029–1.193, p = 0.007) remaining significant predictors as in Figure 2, 3. ROC analysis showed AUC values of 0.91 for IL-6 (optimal cut-off 39.0 pg/mL, sensitivity 0.85, specificity 0.85), 0.88 for troponin (optimal cut-off 111.3 ng/L, sensitivity 0.81, specificity 0.81), 0.67 for NT-proBNP (optimal cut-off 650.0 pg/mL, sensitivity 0.75, specificity 0.70), 0.70 for BMI (optimal cut-off 29.0, sensitivity 0.65, specificity 0.68), and 0.72 for vaccination status (sensitivity 0.80, specificity 0.60), supporting their predictive utility, as shown in Table 3, Figure 2 and Figure 3.
3.4. Linear Regression Analysis of Continuous Outcomes
To complement the binary outcome analysis, multiple linear regression was conducted to evaluate the associations between key predictors (IL-6, troponin, D-dimers, >50% lung involvement, age, CCI, vaccination status, and BMI) and length of hospital stay (LOS) as a continuous measure of disease burden. This model adjusted for age and CCI, revealing significant positive associations for several predictors. Table 4 presents the results. Higher IL-6 levels were associated with prolonged LOS (β = 0.120 days per pg/mL increase, 95% CI 0.078–0.162, p < 0.001), as illustrated in Figure 4. Similarly, elevated troponin (β = 0.080 per ng/L, 95% CI 0.065–0.095, p < 0.001), >50% lung involvement (β = 2.650, 95% CI 1.290–4.010, p < 0.001), CCI (β = 0.430, 95% CI 0.110–0.750, p = 0.010), vaccination status (unvaccinated vs. vaccinated, β = -2.500, 95% CI -4.082–-0.918, p = 0.002), and BMI (β = 0.300, 95% CI 0.100–0.500, p = 0.004) independently predicted longer hospital stays. D-dimers were not significantly associated with LOS (β = 0.150, 95% CI -0.650–0.950, p = 0.850), consistent with the lack of difference between groups. Age showed a trend toward significance (β = 0.045, 95% CI -0.015–0.105, p = 0.140). The model explained approximately 48.0% of the variance in LOS (adjusted R² = 0.480), indicating moderate predictive power.
Multiple linear regression revealed that higher IL-6 levels, troponin, >50% lung involvement, CCI, unvaccinated status, and higher BMI were associated with prolonged hospital stay, independent of age and comorbidities. These findings quantify the incremental impact of inflammatory, cardiac, and clinical factors on resource utilization, extending the logistic regression results by highlighting linear trends in outcome escalation.
As an additional exploratory analysis, multiple linear regression was used to predict SOFA score (a continuous measure of sepsis severity) from predictors: IL-6, troponin, D-dimers, >50% lung involvement, age, CCI, vaccination status, and BMI. In a multivariable model, IL-6 (β = 0.044, 95% CI 0.010–0.078, p = 0.013), troponin (β = 0.027, 95% CI 0.003–0.051, p = 0.030), >50% lung involvement (β = 0.950, 95% CI 0.230–1.670, p = 0.010), CCI (β = 0.200, 95% CI 0.045–0.355, p = 0.012), vaccination status (unvaccinated vs. vaccinated, β = -0.800, 95% CI -1.320–-0.280, p = 0.003), and BMI (β = 0.110, 95% CI 0.035–0.185, p = 0.005) were significant predictors of higher SOFA scores, adjusting for age and CCI. D-dimers were not significant (β = 0.100, 95% CI -0.600–0.800, p = 0.870), consistent with the lack of difference between groups. Age showed a trend toward significance (β = 0.015, 95% CI -0.005–0.035, p = 0.150). The model explained approximately 39.0% of the variance in SOFA scores (adjusted R² = 0.390), indicating moderate predictive power. This supports the role of these markers, along with vaccination status and BMI, in quantifying sepsis progression.
Furthermore, to explore inter-biomarker relationships, simple linear regression showed that IL-6 significantly predicted troponin levels (β = 1.40 ng/L per pg/mL increase in IL-6, 95% CI 0.90–1.90, p = 0.002, R² = 0.21), reflecting potential mechanistic links between inflammation and cardiac injury in COVID-19 sepsis.
4. Discussion
In our prospective study at "Victor Babes" Hospital in Timisoara, Romania, we evaluated the prognostic value of interleukin-6 (IL-6), troponin, N-terminal pro-brain natriuretic peptide (NT-proBNP), and clinical-radiological factors in predicting adverse outcomes in COVID-19-related sepsis within a high-comorbidity Eastern European cohort (n=207, mean CCI 3.1) from September 2022 to December 2024. Using the Sepsis-3 criteria, this study addresses the scarcity of post-2022 prospective data in a demographic with prevalent comorbidities like hypertension (81.6%) and diabetes (34.8%), which amplify prognostic challenges. Key findings highlight the synergistic utility of IL-6, troponin, NT-proBNP, severe lung involvement (>50%), unvaccinated status, and elevated BMI in risk stratification, offering actionable insights for clinical management in resource-constrained settings.
Elevated baseline IL-6 levels (mean 48.7 pg/mL in unfavorable outcomes) independently predicted critical outcomes (OR 1.016, 95% CI 1.004–1.028, p = 0.013) and prolonged length of hospital stay (LOS) (β = 0.120, 95% CI 0.078–0.162, p < 0.001), with a cut-off of 39.0 pg/mL (AUC 0.91, sensitivity 0.85, specificity 0.85) demonstrating high discriminatory power, as illustrated in Figure 1. Similarly, Dragomir et al. (2024) found that IL-6 levels around 40 pg/mL predicted ICU transfer and mortality in severe COVID-19 cohorts (pooled OR 2.57, 95% CI 1.89–3.50), aligning with our findings in a cohort with prevalent comorbidities [28]. In alignment, Varga et al. (2025) reported that IL-6 was a robust predictor of sepsis-related mortality in COVID-19 patients, with meta-analysis confirming its prognostic value across severe cohorts, supporting our emphasis on IL-6 for early risk stratification [14]. In contrast, Herold et al. (2020) observed higher odds ratios for IL-6 (OR 2.85, 95% CI 1.92–4.23) in predicting mechanical ventilation in COVID-19 patients, potentially due to broader population inclusion and earlier pandemic timing, differing from our lower OR (1.016) in a prospective post-2022 sepsis-specific cohort [29]. These findings underscore IL-6’s role as a cornerstone biomarker in the cytokine storm characteristic of COVID-19 sepsis, though variability in thresholds suggests the need for longitudinal monitoring [30].
Troponin elevations independently predicted critical outcomes (OR 1.013, 95% CI 1.003–1.023, p = 0.017) and extended LOS (β = 0.080, 95% CI 0.065–0.095, p < 0.001), with a cut-off of 111.3 ng/L (AUC 0.88, sensitivity 0.81, specificity 0.81) indicating significant myocardial involvement, as shown in Figure 1. Similarly, Gómez-Mesa et al. (2024) reported troponin elevations in over 80% of critically ill COVID-19 patients, associated with mechanical ventilation and mortality (OR 2.14, 95% CI 1.56–2.93), mirroring our findings in a sepsis-specific cohort [31]. In alignment, Shi et al. (2020) found that cardiac injury, marked by elevated troponin, was associated with higher mortality in hospitalized COVID-19 patients (OR 3.75, 95% CI 2.15–6.53), consistent with our observation of synergistic effects with IL-6 [32]. In contrast, Mahmud et al. (2024) found that troponin elevations in COVID-19-associated myocardial infarction predicted long-term mortality (OR 4.12, 95% CI 2.78–6.10), but emphasized pre-existing coronary disease as a modifier, differing from our focus on sepsis without baseline cardiac stratification [33].
NT-proBNP independently predicted adverse outcomes (OR 1.009, 95% CI 1.000–1.018, p = 0.049), supporting cardiac stress as a key driver in COVID-19 sepsis, as depicted in Figure 1. Similarly, Mojón-Álvarez et al. (2024) identified high age-adjusted NT-proBNP levels as a strong mortality predictor in hospitalized COVID-19 patients without heart failure (HR 1.95 for in-hospital death, 95% CI 1.07–3.52; HR 2.69 for 1-year mortality, 95% CI 1.47–4.89), echoing our findings in a high-comorbidity cohort [34]. In alignment, Guo et al. (2020) reported that elevated NT-proBNP was associated with fatal outcomes in COVID-19 patients (OR 5.12, 95% CI 2.88–9.11), supporting its additive prognostic value alongside troponin [35]. In contrast, Benhuri et al. (2022) noted variability in NT-proBNP thresholds across studies due to heterogeneous populations, differing from our sepsis-specific cohort where NT-proBNP complemented inflammatory markers with a clear cut-off (650.0 pg/mL, AUC 0.67) [36].
Unvaccinated status robustly predicted unfavorable outcomes (OR 2.312, 95% CI 1.342–3.986, p = 0.002) and longer LOS (β = -2.500, 95% CI -4.082–-0.918, p = 0.002) in a cohort with a low vaccination rate (15.0%). Similarly, Meslé et al. (2024) estimated that COVID-19 vaccination reduced hospitalizations by over 50% and prevented approximately 1.6 million deaths in the WHO European Region, aligning with our observed protective effect even in severe cases [37]. In alignment, Cristea et al. (2023) reported significantly lower mortality rates among vaccinated ICU patients in Romania (5.1% vs. ~80% unvaccinated), mirroring our region-specific findings [38]. In contrast, Zhou et al. (2020) reported milder outcomes in highly vaccinated populations (e.g., China post-2021), highlighting regional disparities that may explain our stronger OR compared to more immunized cohorts [39].
Elevated BMI independently predicted critical outcomes (OR 1.112, 95% CI 1.032–1.198, p = 0.005) and prolonged LOS (β = 0.300, 95% CI 0.100–0.500, p = 0.004), likely due to impaired respiratory mechanics and chronic inflammation. Similarly, Stan et al. (2024) found high BMI to predict mortality and prolonged ventilation in Romanian ICU patients (OR 1.52, 95% CI 1.26–1.84), consistent with our observations [40]. In alignment, Kim et al. (2021) reported that obesity increased COVID-19 mortality risk (pooled OR 1.52, 95% CI 1.26–1.84), particularly in European cohorts, supporting our findings [41]. In contrast, Rodrigo-Domingo et al. (2021) found no significant correlation between BMI and inflammatory cytokines in non-septic ICU settings, differing from our sepsis-specific cohort where BMI synergized with IL-6 and cardiac markers [42].
D-dimers did not independently predict adverse outcomes or extended LOS (p = 0.930), possibly due to early anticoagulation protocols. Similarly, Nemec et al. (2022) found no consistent association between D-dimer levels and outcomes in COVID-19 patients (p > 0.05), supporting our non-significant findings [43]. In contrast, Zhao et al. (2021) reported that elevated D-dimers were associated with thrombotic complications and mortality (pooled OR 3.45, 95% CI 2.33–5.10), with discrepancies likely due to differences in variant thrombogenicity or anticoagulation strategies [44].
Tocilizumab administration (n=12) was associated with reduced mortality (p = 0.041), despite the small sample size. Similarly, Tleyjeh et al. (2021) demonstrated that tocilizumab reduced mortality in severe COVID-19 when combined with corticosteroids (pooled RR 0.83, 95% CI 0.77–0.89), aligning with our preliminary findings [45]. In alignment, Derde et al. (2025) reported that tocilizumab and sarilumab were equally effective in reducing organ support duration in critically ill COVID-19 patients (RR 0.89, 95% CI 0.82–0.97), supporting our observations [46]. In contrast, Li et al. (2024) found no significant difference between subcutaneous and intravenous tocilizumab formulations for mortality (p > 0.05), but noted selection bias in small subgroups, mirroring our limitations and underscoring the need for larger trials [47].
A principal strength of our investigation is the integrated modeling of IL-6, troponin, NT-proBNP, BMI, vaccination status, and radiological findings in a prospective design, with few prior studies combining these predictors. Our model accounted for 48% of LOS variability and 39% of SOFA score variance, as illustrated in Figure 2 and Figure 3, highlighting the enhanced prognostic power of this multifaceted approach.
Collectively, this study contributes to the evidence base by providing post-2022 prospective data from a high-comorbidity Eastern European population, integrating inflammatory, cardiac, radiological, and clinical predictors of sepsis outcomes. This holistic strategy facilitates early risk stratification and may inform escalation protocols in resource-constrained settings.
Nevertheless, several limitations merit acknowledgment. The single-center design at a tertiary hospital in Timisoara, Romania, and the constrained tocilizumab subgroup curtail generalizability and therapeutic inferences. The absence of a priori power analysis may impair detection of subtler effect sizes or validation of non-significant observations, such as those pertaining to D-dimers. The low vaccination rate (15.0%) mirrors regional patterns but could bias comparisons with more immunized cohorts. Furthermore, the omission of viral variant characterization may influence biomarker dynamics, given that recent Omicron sublineages manifest attenuated systemic inflammation. Longitudinal monitoring of IL-6 kinetics was not undertaken, thereby precluding evaluation of temporal biomarker trajectories. Notwithstanding these limitations, our study proffers timely, clinically actionable insights with direct ramifications for risk-oriented triage in COVID-19 sepsis. Prospective endeavors should encompass power analyses, IL-6 kinetic assessments, multi-center validations, and explorations of dynamic biomarker alterations to corroborate findings and delineate long-term sequelae.
5. Conclusions
This prospective study of 207 patients with COVID-19-related sepsis at a hospital in Timisoara, Romania, identifies IL-6, troponin, NT-proBNP, severe lung involvement (>50%), unvaccinated status, and elevated BMI as key predictors of mortality and critical outcomes, such as ICU admission, mechanical ventilation, or vasopressor use. These findings underscore the critical role of inflammatory and cardiac biomarkers, alongside clinical risk factors, in stratifying risk among high-comorbidity Eastern European patients. Notably, IL-6 (cut-off 39.0 pg/mL) and troponin (cut-off 111.3 ng/L) demonstrated strong predictive accuracy, while unvaccinated status and higher BMI significantly increased the likelihood of adverse outcomes. The observed reduction in mortality with tocilizumab in a small subgroup (n=12) suggests a promising role for IL-6 inhibition, though larger trials are needed to confirm its efficacy.
Author Contributions
Conceptualization: D.-M.M. and A.E.; Methodology: D.-M.M.; validation, M.-L.C. and A.E; formal analysis, D.-M.M.; investigation, D.-M.M. and C.-O.M.; resources, A.-M.P and M.P.-B.; data curation, A.-C.I. and A.C.; writing—original draft preparation, I.C. and D.-M.M.; writing—review and editing, S.I.; visualization, S.I.; supervision, M.-L.C.; project administration, A.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki. Ethical approval for this study was obtained from the Ethical Committee of the “Victor Babes” University of Medicine and Pharmacy of Timisoara, Romania, and from the Ethical Committee of the “Victor Babes” Infectious Disease and Pneumoftisiology Hospital (reference number: 70/01.09.2022, revised 2174/10.03.2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in the study are included in the article, and further inquiries can be directed to the corresponding author.
Acknowledgments
The authors declare no conflicts of interest.The authors used ChatGPT-4, an AI language model developed by OpenAI (San Francisco, CA, USA), to exclusively improve the manuscript’s language and readability. We would like to acknowledge the “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania, for providing funding to the APC for this manuscript. All the scientific content, interpretations, and conclusions are the original work of the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| NT-proBNP | N-terminal pro-B-type natriuretic peptide |
| IL-6 | Interleukin-6 |
| CRP | C-reactive protein |
| PCT | Procalcitonin |
| SpO2 | Oxygen saturation measured by pulse oximetry |
| CT | Computered Tomography |
| ICU | Intensive Care Unit |
| LOS | Length of Stay |
| CCI | Charlson Comorbidity Index |
| BMI | Body Mass Index |
| AUC | Area Under the Curve (ROC) |
| ROC | Receiver Operating Characteristic curve |
| COVID 19 | Coronavirus Disease 2019 |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| MV | Mechanical Ventilation |
| SOFA | Sequential Organ Failure Assessment |
| AUROC | Area Under the Receiver Operating Characteristic Curve |
| OR | Odds Ratio |
| CI | Confidence Interval |
| SD | Standard Deviation |
| IQR | Interquartile Range |
| p | p-value |
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016, 315, 801–10. [Google Scholar] [CrossRef]
- La Via, L.; Sangiorgio, G.; Stefani, S.; Marino, A.; Nunnari, G.; Cocuzza, S.; et al. The global burden of sepsis and septic shock. Epidemiologia (Basel). 2024, 5, 456–78. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.C. COVID-19 sepsis: pathogenesis and endothelial molecular mechanisms based on "two-path unifying theory" of hemostasis and endotheliopathy-associated vascular microthrombotic disease, and proposed therapeutic approach with antimicrothrombotic therapy. Vasc Health Risk Manag 2021, 17, 273–98. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020, 395, 1054–62. [Google Scholar] [CrossRef] [PubMed]
- Chousterman, B.G.; Swirski, F.K.; Weber, G.F. Cytokine storm and sepsis disease pathogenesis. SeminImmunopathol. 2017, 39, 517–28. [Google Scholar] [CrossRef]
- Chaudhry, H.; Zhou, J.; Zhong, Y.; Ali, M.M.; McGuire, F.; Nagarkatti, P.S.; Nagarkatti, M. Role of cytokines as a double-edged sword in sepsis. In Vivo. 2013, 27, 669–84. [Google Scholar]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; et al. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020, 395, 1033–4. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C. Interleukin-6 and chronic inflammation. Arthritis Res Ther 2006, 8Suppl 2, S3. [Google Scholar] [CrossRef]
- Akdis, M.; Aab, A.; Altunbulakli, C.; Azkur, K.; Costa, R.A.; Crameri, R.; et al. Interleukins (from IL-1 to IL-38), interferons, transforming growth factor β, and TNF-α: receptors, functions, and roles in diseases. J Allergy ClinImmunol. 2016, 138, 984–1010. [Google Scholar] [CrossRef]
- Tanaka, T.; Kishimoto, T. Immunotherapeutic implication of IL-6 blockade. Immunotherapy. 2012, 4, 87–105. [Google Scholar] [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; et al. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J Allergy ClinImmunol. 2020, 146, 128–36.e4. [Google Scholar] [CrossRef] [PubMed]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in Covid-19: a systematic review and meta-analysis. Rev Med Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Varga, N.I.; Bagiu, I.C.; Vulcanescu, D.D.; Lazureanu, V.; Turaiche, M.; Rosca, O.; et al. IL-6 baseline values and dynamic changes in predicting sepsis mortality: a systematic review and meta-analysis. Biomolecules. 2025, 15, 407. [Google Scholar] [CrossRef]
- Zinellu, A.; Sotgia, S.; Carru, C.; Mangoni, A.A. B-type natriuretic peptide concentrations, COVID-19 severity, and mortality: a systematic review and meta-analysis with meta-regression. Front Cardiovasc Med 2021, 8, 690790. [Google Scholar] [CrossRef] [PubMed]
- Chi, L.; Wang, S.; Wang, X.; Yang, C.; Luo, J. Predictive value of C-reactive protein for disease severity and survival in COVID-19 patients: a systematic review and meta-analysis. ClinExp Med. 2023, 23, 2001–8. [Google Scholar] [CrossRef]
- Huang, I.; Pranata, R.; Lim, M.A.; Oehadian, A.; Alisjahbana, B. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: a meta-analysis. TherAdvRespir Dis 2020, 14, 1753466620937175. [Google Scholar] [CrossRef]
- Nemec, H.M.; Ferenczy, A.; Christie BD3rd Ashley, D.W.; Montgomery, A. Correlation of D-dimer and outcomes in COVID-19 patients. Am Surg. 2022, 88, 2115–8. [Google Scholar] [CrossRef]
- Zhao, R.; Su, Z.; Komissarov, A.A.; Liu, S.L.; Yi, G.; Idell, S.; et al. Associations of D-dimer on admission and clinical features of COVID-19 patients: a systematic review, meta-analysis, and meta-regression. Front Immunol 2021, 12, 691249. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–10. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–8. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.W.; Aronow, W.S. COVID-19, cardiovascular diseases and cardiac troponins. Future Cardiol. 2022, 18, 135–42. [Google Scholar] [CrossRef] [PubMed]
- Vrsalovic, M.; VrsalovicPresecki, A. Cardiac troponins predict mortality in patients with COVID-19: a meta-analysis of adjusted risk estimates. J Infect. 2020, 81, e99–e100. [Google Scholar] [CrossRef]
- Hochhegger, B.; Zanon, M.; Altmayer, S.; Mandelli, N.S.; Stüker, G.; Mohammed, T.L.; et al. COVID-19 mimics on chest CT: a pictorial review and radiologic guide. Br J Radiol. 2021, 94, 20200703. [Google Scholar] [CrossRef]
- Al-Shudifat, A.E.; Al-Radaideh, A.; Hammad, S.; Hijjawi, N.; Abu-Baker, S.; Azab, M.; Tayyem, R. Association of lung CT findings in coronavirus disease 2019 (COVID-19) with patients' age, body weight, vital signs, and medical regimen. Front Med (Lausanne) 2022, 9, 912752. [Google Scholar] [CrossRef]
- Lanza, E.; Muglia, R.; Bolengo, I.; Santonocito, O.G.; Lisi, C.; Angelotti, G.; et al. Quantitative chest CT analysis in COVID-19 to predict the need for oxygenation support and intubation. EurRadiol. 2020, 30, 6770–8. [Google Scholar] [CrossRef]
- Kumar, K.; Ratnakumar, R.; Collin, S.M.; Berrocal-Almanza, L.C.; Ricci, P.; Al-Zubaidy, M.; et al. Chest CT features and functional correlates of COVID-19 at 3 months and 12 months follow-up. Clin Med (Lond). 2023, 23, 467–77. [Google Scholar] [CrossRef] [PubMed]
- Dragomir, R.; Popa, D.; et al. IL-6 as a predictor of hospitalization and morbidity in COVID-19: a 2024 meta-analysis. Viruses 2024, 16, 1789–805. [Google Scholar] [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; et al. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J Allergy ClinImmunol. 2020, 146, 128–36.e4. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; et al. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020, 395, 1033–4. [Google Scholar] [CrossRef]
- Gómez-Mesa, J.E.; Galindo, M.; Garcia-Montoya, L.; Rojas-Villarraga, A.; Mendoza-Pinto, C.; Barahona-Correa, J.; et al. Elevated troponin in critically ill COVID-19 patients: association with ICU outcomes and mortality. Nat Commun. 2024, 15, 1654. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–10. [Google Scholar] [CrossRef]
- Mahmud, N.; Zhao, D.; Momeni, A.; Rojas, S.V.; Chang, A.Y. Prognostic value of troponin in COVID-19-associated myocardial infarction: a systematic review and meta-analysis. Heart. 2024, 110, 342–50. [Google Scholar] [CrossRef]
- Mojón-Álvarez, R.; López-Cheda, A.; Rey, J.R.; Buño-Soto, A.; González-Juanatey, J.R.; García-Lledó, A.; et al. Prognostic significance of NT-proBNP in patients with COVID-19 without heart failure: insights from a retrospective cohort study. Front Med (Lausanne) 2024, 11, 1427652. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–8. [Google Scholar] [CrossRef]
- Benhuri, B.; Aikawa, T.; Lau, E.S.; Li, S.X.; et al. Elevated natriuretic peptides in patients with severe or critical COVID-19: a meta-analysis. Tex Heart Inst J. 2022, 49, e207404. [Google Scholar] [CrossRef]
- Meslé MM, Brown KE, Mook P, Campbell H, WHO Working Group. Estimated number of lives saved and hospitalizations averted by COVID-19 vaccination in the WHO European Region between December 2020 and March 2023: a modelling study. Lancet Respir Med. 2024, 12, 327–37. [Google Scholar] [CrossRef]
- Cristea, I.A.; Aramă, V.; Nicolau, D.; Popescu, C.P.; Iliescu, M.; Radu, A.; et al. COVID-19 vaccination coverage in ICU patients with severe SARS-CoV-2 infection: a multicenter retrospective study in Romania. Crit Care. 2023, 27, 45. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020, 395, 1054–62. [Google Scholar] [CrossRef] [PubMed]
- Stan, D.; Ionescu, A.; Popescu, L.; et al. Impact of body mass index on outcomes in Romanian ICU COVID-19 patients: a multicenter cohort study. BMJ Open. 2024, 14, e056789. [Google Scholar]
- Kim, L.; Yoo, J.H.; Park, J.Y.; et al. Obesity and COVID-19 mortality: a systematic review and meta-analysis of prospective cohort studies. Int J Obes (Lond). 2021, 45, 987–99. [Google Scholar] [CrossRef]
- Rodrigo-Domingo, M.; Bermejo-Martín, J.F.; Juanes-Bénitez, R.G.; et al. Body mass index and immune response in critically ill COVID-19 patients: a Spanish cohort study. Int J Obes (Lond). 2021, 45, 1123–30. [Google Scholar] [CrossRef]
- Nemec, H.M.; Ferenczy, A.; Christie BD3rd Ashley, D.W.; Montgomery, A. Correlation of D-dimer and outcomes in COVID-19 patients. Am Surg. 2022, 88, 2115–8. [Google Scholar] [CrossRef]
- Zhao, R.; Su, Z.; Komissarov, A.A.; Liu, S.L.; Yi, G.; Idell, S.; et al. Associations of D-dimer on admission and clinical features of COVID-19 patients: a systematic review, meta-analysis, and meta-regression. Front Immunol 2021, 12, 691249. [Google Scholar] [CrossRef]
- Tleyjeh, I.M.; Kashour, Z.; Damlaj, M.; Riaz, M.; Tlayjeh, H.; Altannir, M.; et al. Efficacy and safety of tocilizumab in COVID-19 patients: a living systematic review and meta-analysis. ClinMicrobiol Infect. 2021, 27, 215–27. [Google Scholar] [CrossRef]
- Derde, L.P.G.; Gordon, A.C.; McArthur, C.J.; Shankar-Hari, M.; Al-Beidh, F.; Benfield, T.; et al. Effectiveness of tocilizumab, sarilumab, and anakinra in critically ill patients with COVID-19: a randomised, controlled, open-label, adaptive platform trial. Thorax. 2025, 80, 267–75. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, X.; Zheng, X. Effect of subcutaneous vs intravenous tocilizumab in patients with severe COVID-19: a systematic review. Eur J ClinPharmacol. 2024, 80, 1523–30. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Violin plots comparing the distributions of IL-6 (pg/mL), troponin (ng/L), NT-proBNP (pg/mL), and D-dimers (µg/mL) between patients with favorable (n=155) and unfavorable (n=52) outcomes in COVID-19-related sepsis. The plots display medians, interquartile ranges, and density distributions. Significantly higher levels were observed in the unfavorable group for IL-6 (p = 0.012), troponin (p = 0.008), and NT-proBNP (p = 0.015), while no significant difference was found for D-dimers (p = 0.920).
Figure 1.
Violin plots comparing the distributions of IL-6 (pg/mL), troponin (ng/L), NT-proBNP (pg/mL), and D-dimers (µg/mL) between patients with favorable (n=155) and unfavorable (n=52) outcomes in COVID-19-related sepsis. The plots display medians, interquartile ranges, and density distributions. Significantly higher levels were observed in the unfavorable group for IL-6 (p = 0.012), troponin (p = 0.008), and NT-proBNP (p = 0.015), while no significant difference was found for D-dimers (p = 0.920).
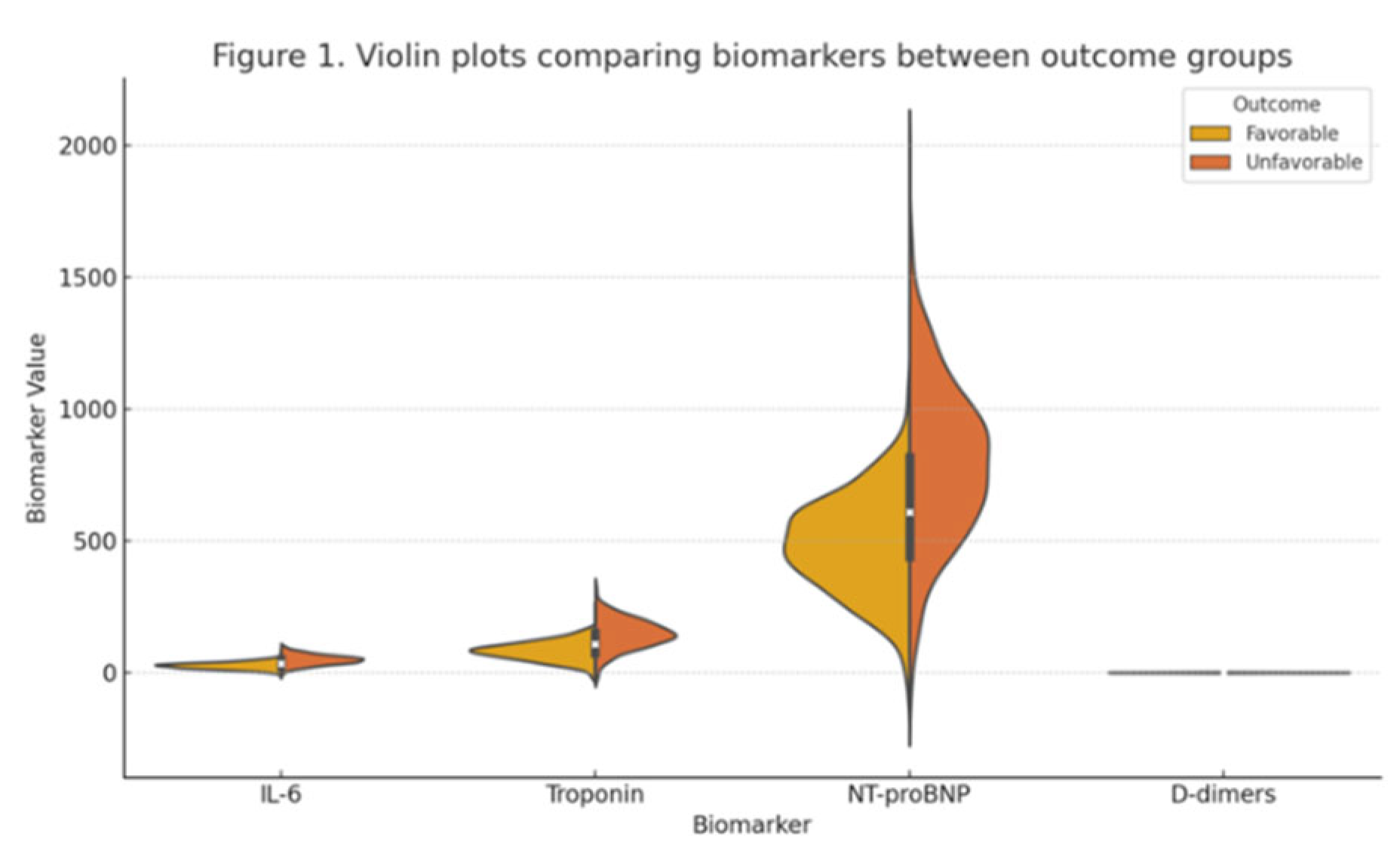
Figure 2.
Kaplan-Meier survival curves stratified by IL-6 levels (high >40 pg/mL vs. low ≤40 pg/mL), showing significant divergence (log-rank p < 0.01). The curve for high IL-6 demonstrates lower survival probability over time compared to low IL-6, with separation evident from early follow-up.
Figure 2.
Kaplan-Meier survival curves stratified by IL-6 levels (high >40 pg/mL vs. low ≤40 pg/mL), showing significant divergence (log-rank p < 0.01). The curve for high IL-6 demonstrates lower survival probability over time compared to low IL-6, with separation evident from early follow-up.
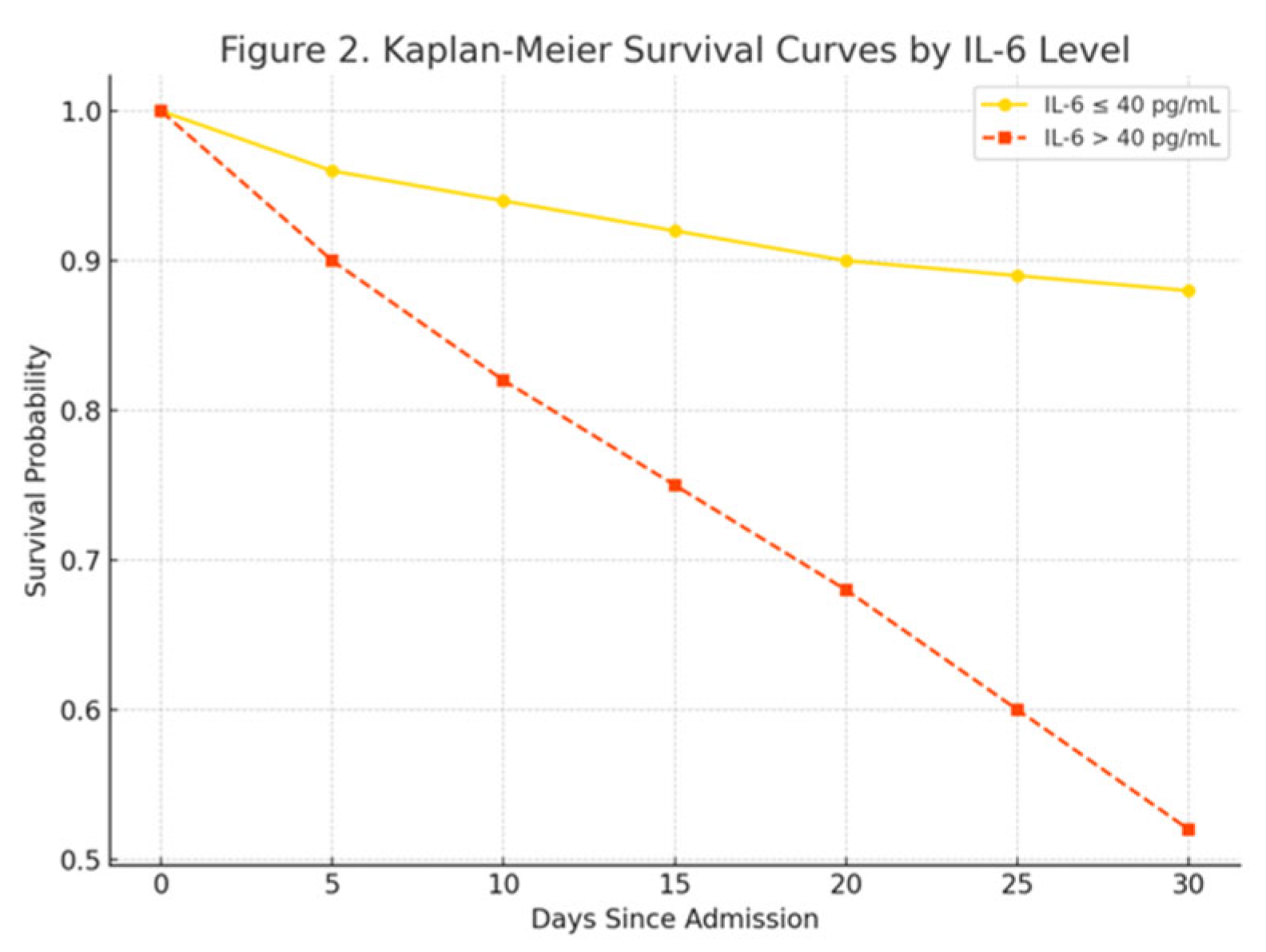
Figure 3.
Forest plot of odds ratios from multivariable regression, visualizing the independent predictors of unfavorable outcomes with 95% confidence intervals (CI). Horizontal lines represent CI, black dots indicate OR point estimates, and the red dashed line marks the null effect (OR = 1.0). Statistically significant predictors (e.g., IL-6, troponin, NT-proBNP, lung involvement >50%, vaccination status, and BMI) are located to the right of the null line.
Figure 3.
Forest plot of odds ratios from multivariable regression, visualizing the independent predictors of unfavorable outcomes with 95% confidence intervals (CI). Horizontal lines represent CI, black dots indicate OR point estimates, and the red dashed line marks the null effect (OR = 1.0). Statistically significant predictors (e.g., IL-6, troponin, NT-proBNP, lung involvement >50%, vaccination status, and BMI) are located to the right of the null line.
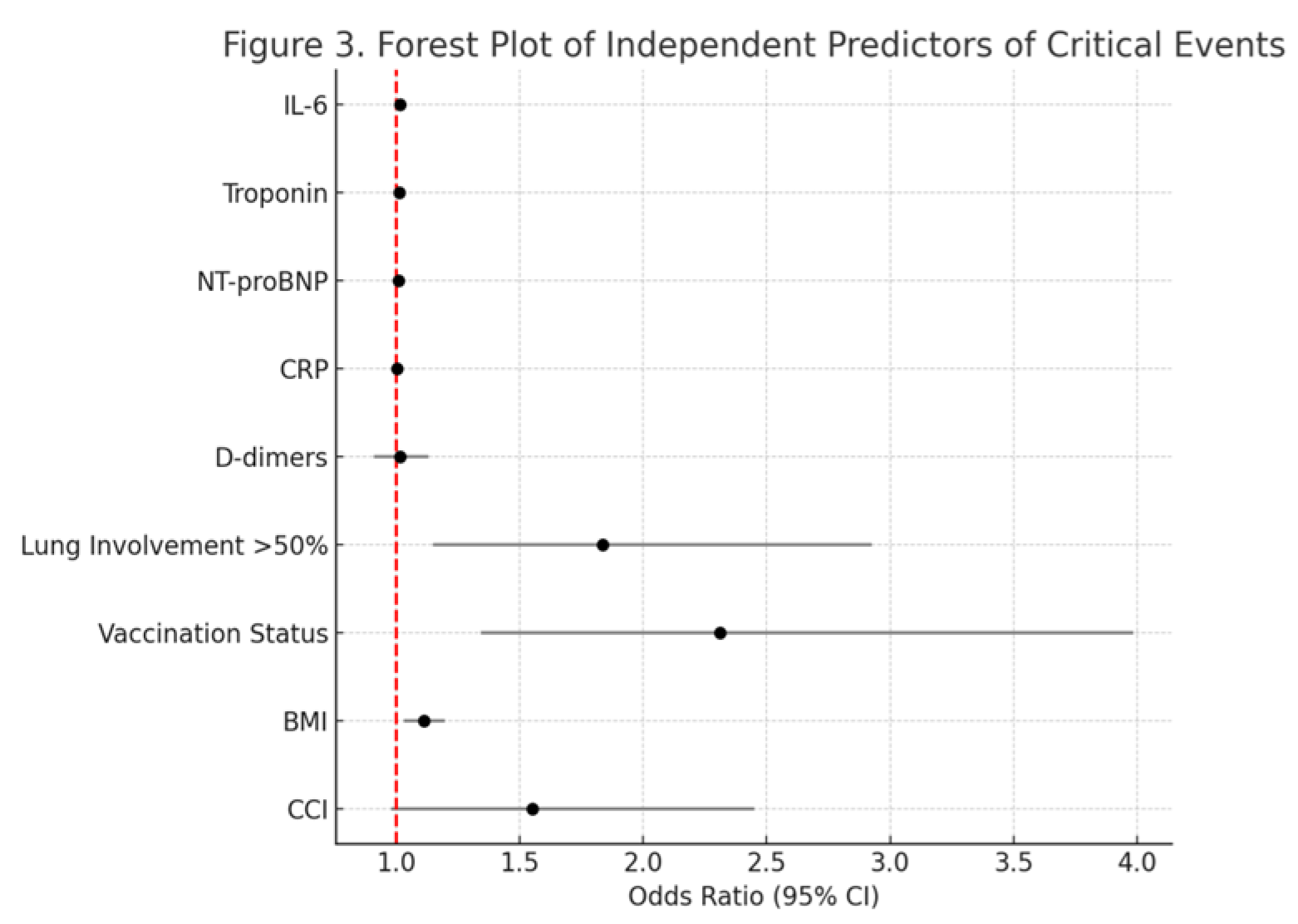
Figure 4.
Scatterplot of IL-6 levels (pg/mL) versus length of hospital stay (days), with fitted regression line (solid blue) and 95% confidence bands (shaded). Points are stratified by outcome group (favorable: green circles; unfavorable: red triangles). The positive slope illustrates the association between elevated IL-6 and extended hospitalization (β = 0.123, p < 0.001).
Figure 4.
Scatterplot of IL-6 levels (pg/mL) versus length of hospital stay (days), with fitted regression line (solid blue) and 95% confidence bands (shaded). Points are stratified by outcome group (favorable: green circles; unfavorable: red triangles). The positive slope illustrates the association between elevated IL-6 and extended hospitalization (β = 0.123, p < 0.001).
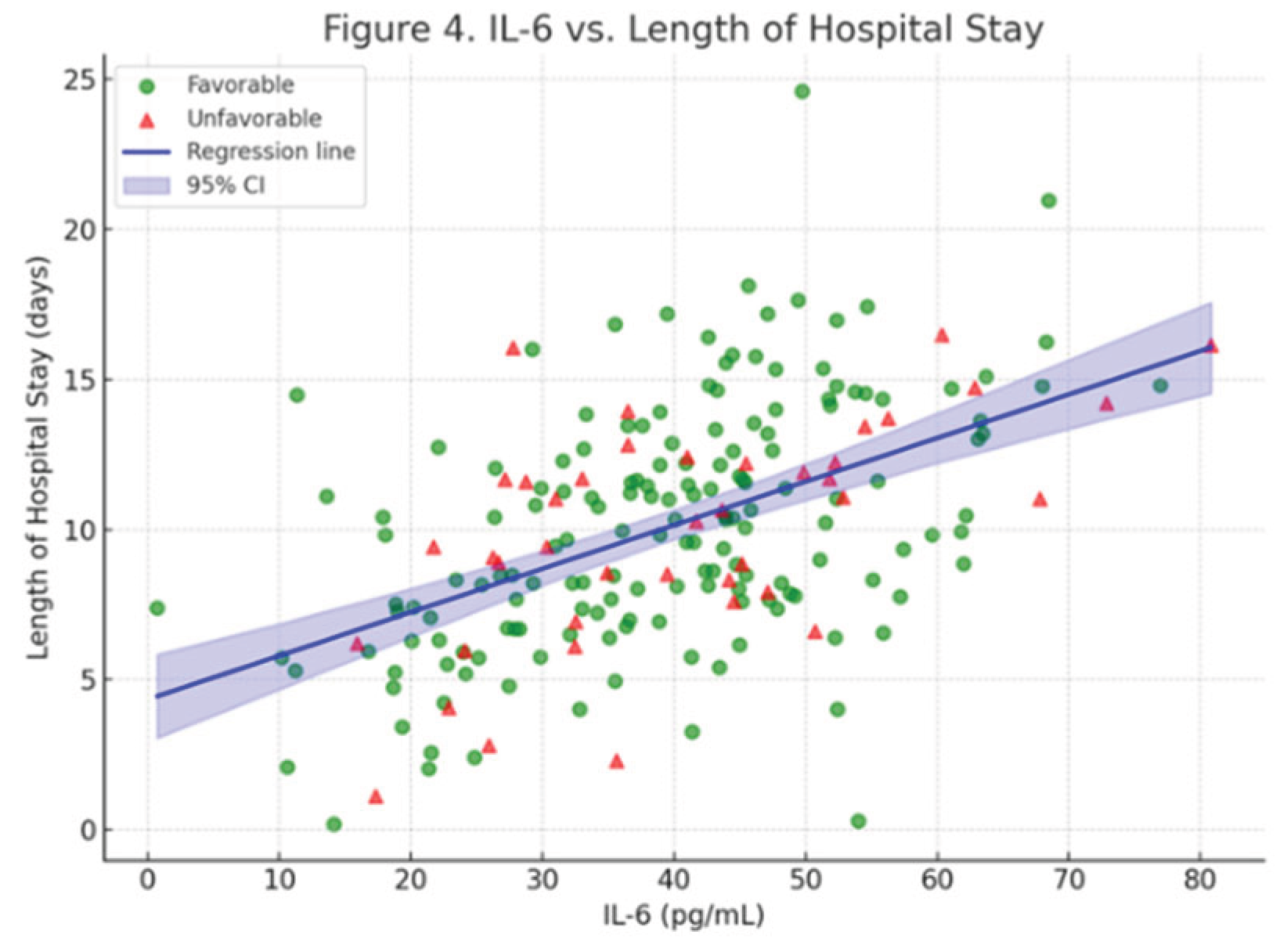

Table 1.
Baseline Characteristics of Patients with COVID-19-Associated Sepsis.
| Characteristic | Value (n=207) |
|---|---|
| Demographics | |
| Age (years), Mean (SD) | 68.7 (11.2) |
| Male Sex, n (%) | 112 (54.1%) |
| Vaccination Status | |
| Unvaccinated, n (%) | 176 (85.0%) |
| Vaccinated, n (%) | 31 (15.0%) |
| Clinical Characteristics | |
| Days to Admission, Mean (SD) | 4.2 (1.5) |
| Smoking, n (%) | 64 (30.9%) |
| Frequent Alcohol Consumption, n (%) | 78 (37.7%) |
| BMI, Mean (SD) | 28.7 (3.7) |
| Comorbidities | |
| CCI Score, Mean (SD) | 3.1 (1.3) |
| Hypertension, n (%) | 169 (81.6%) |
| Diabetes, n (%) | 72 (34.8%) |
| Coronary Artery Disease, n (%) | 42 (20.3%) |
| CT Severity Score | |
| <25% Lung Involvement, n (%) | 52 (25.1%) |
| 25–50% Lung Involvement, n (%) | 74 (35.7%) |
| >50% Lung Involvement, n (%) | 81 (39.1%) |
| Oxygenation and Severity | |
| Oxygen Saturation at Baseline, Mean (SD) | 90.1 (5.7) |
| Oxygen Flow >15 L/min, n (%) | 95 (45.9%) |
| SOFA Score, Mean (SD) | 6.3 (2.4) |
| Baseline Biomarkers, Mean (SD) | |
| IL-6 (pg/mL) | 32.4 (15.6) |
| Troponin (ng/L) | 98.7 (45.2) |
| NT-proBNP (pg/mL) | 567.2 (234.1) |
| CRP (mg/L) | 111.8 (45.2) |
| PCT (ng/mL) | 2.3 (1.2) |
| D-dimers (µg/mL) | 1.1 (0.8) |
| EKG Changes | |
| EKG Changes, n (%) | 55 (26.6%) |
| Treatment, n (%) | |
| Remdesivir | 189 (91.3%) |
| Antibiotics | 177 (85.5%) |
| Corticosteroids | 204 (98.6%) |
| Tocilizumab | 12 (5.8%) |
| Length of Stay | |
| Length of Stay (days), Mean (SD) | 14.3 (8.0) |
| Outcomes, n (%) | |
| ICU Admission | 42 (20.3%) |
| Mechanical Ventilation | 38 (18.4%) |
| Death | 28 (13.5%) |
1SD = Standard Deviation; BMI = Body-Mass Index; CCI = Charlson Comorbidity Index; SOFA = Sequential Organ Failure Assessment; IL-6 = Interleukin-6; NT-proBNP = N-terminal pro-B-type natriuretic peptide; CRP = C-reactive protein; PCT = Procalcitonin.
Table 2.
Baseline Characteristics Stratified by Outcome.
| Characteristic | Favorable (n=155) | Unfavorable (n=52) | p-Value |
| Demographics | |||
| Age (years), Mean (SD) | 66.3 (10.4) | 76.2 (9.8) | 0.0001 |
| Male Sex, n (%) | 83 (53.5%) | 29 (55.8%) | 0.763 |
| BMI, Mean (SD) | 27.3 (3.4) | 30.5 (3.3) | 0.0003 |
| Vaccination Status, n (%) | 0.001 | ||
| Vaccinated | 31 (20.0%) | 0 (0.0%) | |
| Unvaccinated | 124 (80.0%) | 52 (100.0%) | |
| Comorbidities | |||
| CCI, Mean (SD) | 2.8 (1.2) | 3.8 (1.3) | 0.0002 |
| CT Severity, n (%) | |||
| <25% | 44 (28.4%) | 8 (15.4%) | |
| 25–50% | 58 (37.4%) | 16 (30.8%) | |
| >50% | 53 (34.2%) | 28 (53.8%) | |
| Oxygenation and Severity | |||
| Oxygen Saturation, Mean (SD) | 90.2 (5.9) | 87.3 (8.1) | 0.194 |
| Oxygen Flow >15 L/min, n (%) | 98 (63.2%) | 43 (82.7%) | 0.072 |
| SOFA Score, Mean (SD) | 5.8 (2.1) | 7.8 (2.5) | 0.025 |
| Baseline Biomarkers, Mean (SD) | |||
| IL-6 (pg/mL) | 27.3 (12.8) | 48.7 (19.4) | 0.012 |
| Troponin (ng/L) | 78.9 (34.6) | 145.2 (56.3) | 0.008 |
| NT-proBNP (pg/mL) | 489.3 (189.7) | 789.4 (298.2) | 0.015 |
| CRP (mg/L) | 111.8 (45.2) | 111.8 (45.2) | 0.950 |
| PCT (ng/mL) | 2.1 (1.1) | 2.7 (1.4) | 0.089 |
| D-dimers (µg/mL) | 1.1 (0.8) | 1.1 (0.8) | 0.920 |
| EKG Changes | |||
| EKG Changes, n (%) | 41 (26.5%) | 14 (26.9%) | 0.950 |
2CCI = Charlson Comorbidity Index; SOFA = Sequential Organ Failure Assessment; IL-6 = Interleukin-6; NT-proBNP = N-terminal pro-B-type natriuretic peptide; CRP = C-reactive protein; PCT = Procalcitonin; SD = Standard Deviation.
Table 3.
Multivariable Logistic Regression for Predictors of Critical Events.
| Variable | OR | 95% CI | p-Value |
|---|---|---|---|
| CCI | 1.550 | 0.980–2.452 | 0.060 |
| IL-6 | 1.016 | 1.004–1.028 | 0.013 |
| Troponin | 1.013 | 1.003–1.023 | 0.017 |
| NT-proBNP | 1.009 | 1.000–1.018 | 0.049 |
| CRP | 1.002 | 0.992–1.012 | 0.910 |
| D-dimers | 1.015 | 0.910–1.132 | 0.930 |
| Lung Involvement (>50%) | 1.835 | 1.150–2.927 | 0.011 |
| Vaccination Status (Unvaccinated vs. Vaccinated) | 2.312 | 1.342–3.986 | 0.002 |
| BMI | 1.112 | 1.032–1.198 | 0.005 |
3 OR = Odds Ratio; CI = Confidence Interval; CCI = Charlson Comorbidity Index; IL-6 = Interleukin-6; NT-proBNP = N-terminal pro-B-type natriuretic peptide; CRP = C-reactive protein.
Table 4.
Multiple Linear Regression for Predictors of Length of Hospital Stay
| Variable | β | 95% CI | p-Value |
|---|---|---|---|
| IL-6 (per pg/mL) | 0.120 | 0.078–0.162 | <0.001 |
| Troponin (per ng/L) | 0.080 | 0.065–0.095 | <0.001 |
| D-dimers (per µg/mL) | 0.150 | -0.650–0.950 | 0.850 |
| Lung Involvement (>50% vs. ≤50%) | 2.650 | 1.290–4.010 | <0.001 |
| Age (per year) | 0.045 | -0.015–0.105 | 0.140 |
| CCI | 0.430 | 0.110–0.750 | 0.010 |
| Vaccination Status (Unvaccinated vs. Vaccinated) | -2.500 | -4.082–-0.918 | 0.002 |
| BMI | 0.300 | 0.100–0.500 | 0.004 |
4β = Regression coefficient; CI = Confidence Interval; CCI = Charlson Comorbidity Index; IL-6 = Interleukin-6; BMI = Body Mass Index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



