
Submitted:
30 June 2023
Posted:
03 July 2023
You are already at the latest version
Abstract
Early diagnosis and appropriate treatments are crucial to reducing mortality risk in septic patients. Low SOFA scores and current biomarkers may not discern adequately patients that could develop severe organ dysfunction or have an elevated mortality risk. The aim of this prospective observational study is to evaluate the predictive value of the biomarkers midregional proadrenomedullin (MR-proADM), procalcitonin (PCT), C-Reactive Protein (CRP), and lactate for 28-day mortality in patients with sepsis and a SOFA score ≤ 6. 284 patients were included, with a 28-day all-cause mortality of 8.45 % (N=24). Non-survivors were older (p=0.003), required mechanical ventilation (p=0.04) and were ventilated for longer (p=0.02), had a higher APACHE II (p=0.015) and SOFA (p=0.027) scores. Lactate showed the highest predictive ability for all-cause 28-day mortality with an area under the receiver-operating characteristic curve (AUROC) of 0.67 (0.55–0.79). The AUROC for all-cause 28-day mortality in patients with community-acquired infection was 0.69 (0.57–0.84) for SOFA, and 0.70 (0.58–0.82) for MR-proADM. A 2.1 nmol/L cut-off point for this biomarker in this subgroup of patients discerned with 100% sensibility survivors from non-survivors at 28 days. In patients with community acquired sepsis and initial SOFA score ≤ 6, MR-proADM could help identify patients at risk of 28-day mortality.
Keywords:
Sepsis biomarkers
; mortality
; MR-proADM
; SOFA score
; Lactate
; molecular diagnosis
1. Introduction
Sepsis continues to be an important public health issue [1] and has been reported to be a leading cause of mortality worldwide [2,3,4]. Therefore, early diagnosis and effective and appropriate treatments are crucial to reducing mortality risk [5].
Various definitions and scoring systems have been developed to aid in screening and quick diagnosis. The Sequential Organ Failure Assessment (SOFA) score has become a well-established and widely used score that stratifies the risk of multi-organ failure, based on an objective score covering variables from six organ systems [6]. In 2016, the Third International Consensus Conference (Sepsis-3) for sepsis definition considered an increase of 2 or more in the SOFA score as diagnostic criteria, replacing the previously used SIRS criteria [2,7,8].
The SOFA score has been shown to be associated with mortality [2,7,9], and in those with initial low SOFA values less than six, mortality is lower than 10% [10,11]. However, despite the reported low mortality risk in patients with a SOFA ≤ 6, a subgroup of patients with sepsis and a low SOFA score still shows high mortality. Identifying this singular subgroup of patients with early sepsis and high mortality is crucial to be able to start early and appropriate treatment. Although score systems such as the qSOFA have been designed to screen for sepsis these may lack the sensitivity required, which has led to the Surviving Sepsis Campaign 2021 guidelines to recommend against using the qSOFA as a single-screening tool for sepsis [12]. Blood biomarkers may provide the extra information required to identify this subgroup of patients with high risk, or those who are developing organ failure, despite a low SOFA score. Hence, there is a need to identify biomarkers that may assist in mortality risk-stratification in patients with an initial low SOFA score. The combined use of midregional proadrenomedullin (MR-proADM), procalcitonin (PCT), and other commonly used biomarkers, such as C-Reactive Protein (CRP), Interleukin- 6 (IL-6), and lactate has been suggested in previous studies [5,7,13,14,15,16]. Nonetheless, MR-proADM has shown recent usefulness with better prognostic accuracy than CRP and APACHE [5], and is also correlated with 30-day mortality [7,18]. MR-proADM may also indicate risk for multiple organ failure in sepsis patients despite a low or moderate SOFA score [17], with its concentrations corresponding to endothelial permeability [19]. Moreover, its combination with PCT also improves diagnosis of sepsis [20]. PCT and CRP have also been well-documented for their use in sepsis and in discriminating between infectious and non-infectious etiology. However, neither has shown strong evidence for mortality prediction [5].
Therefore, we hypothesize that the biomarkers midregional proadrenomedullin (MR-proADM), procalcitonin (PCT), C-Reactive Protein (CRP) and lactate can help identify 28-day mortality in patients with sepsis and SOFA score ≤ 6.
2. Materials and Methods
2.1. Study design
The present study comprises a prospective observational analysis. This is a single-center observational study of patients who met the criteria for the activation of the in-hospital sepsis code (ISC) [5,21], between April 2016 and July 2018. The study endpoint was 28-day all-cause mortality following enrolment.
2.2. Setting and participants
Patients for whom the attending physician activated the in-hospital sepsis code (ISC) at Hospital Universitari Vall d'Hebron in the emergency department (ED), hospital wards, and intensive care unit (ICU) with a diagnosis of sepsis or septic shock and initial SOFA score ≤ 6 were enrolled consecutively from April 2016 to July 2018.
Inclusion criteria were as follows: adult patients ≥18 years of age presenting with either a suspected or documented infection and met at least one of the two sets of variables of the Vall d’Hebron University Hospital in-hospital sepsis code (ISC) [5,21]. The ISC variables include (1) an acute alteration in the level of consciousness not explained by other clinical conditions, or (2) hyperthermia (axillary temperature >38.3°C) or hypothermia (axillary temperature <36.0°C), and/or tachycardia (>110 beats per minute), tachypnea (>30 breaths per minute) or low oxygen saturation (SpO2 <90%), as well as arterial hypotension (Systolic Arterial Pressure <90 mmHg or Mean Arterial Pressure <65 mmHg, or a decrease of >40 mmHg of baseline Systolic Arterial Pressure).
Patients younger than 18 years, patients who were pregnant, or patients where no blood sample could be obtained were excluded. Patients were admitted to the ICU or relevant ward according to clinical criteria.
2.3. Variables and Data sources
Up on activation of the sepsis code, data were collected prospectively in the relevant database including patient comorbidities, demographics, site of admission (ED vs. ward), and whether sepsis was considered of nosocomial v. community origin. Triage data, laboratory results, microbiology tests, and final clinical diagnosis were also recorded.
The SOFA and APACHE II scores were calculated retrospectively on enrolment.
Sepsis code activation also triggered collection of blood samples, which were stored in the Sepsis Bank of Vall d'Hebron University Hospital Biobank until analysis. The samples used in this project were provided by the Sepsis Bank of Vall d'Hebron University Hospital Biobank and complied with appropriate ethics approval. Routine biomarker measurements tests include PCT (chemiluminescent immunoassay [CLIA]), CRP (immune turbidimetric test), and L-lactate (enzymatic color test). MR-proADM was analyzed retrospectively. MR-proADM was tested by blood sampling from the central catheter and stored at -80oC. Samples were batch tested using TRACE technology (Time-Resolved Amplified Cryptate Emission, KRYPTOR® platform, Thermo Fisher, Hennigsdorf, Germany). MR-proADM results were unavailable to the corresponding physician throughout patient enrolment and hospitalization.
2.4. Statistical methods
Descriptive data for continuous variables was displayed using mean and standard deviation, for discrete variables median and first to third quartile intervals were used, and categorical variables are represented in frequency and percentages. Variables were compared between surviving and non-surviving patients at 28 days following sepsis code activation. Differences were assessed using the chi-square test for categorical variables, Student’s t-test and Mann-Whitney U test for all other continuous and discrete variables.
The area under the receiver operating characteristic (AUROC) curves were used to evaluate each biomarker's predictive ability and identify the biomarker or clinical score with the greatest predictive value for the study endpoint. An AUROC of 0.5 was considered as non-predictive, and 1.0 perfect predictive ability. An AUROC of 0.70 to 0.80 was considered acceptable [19].
The performance of each indicator as a predictor of mortality was assessed using univariate and multivariate logistic regression models. In addition, each indicator was also assessed for the following subgroups: 28-day mortality v. 90-day mortality, nosocomial v. community infection, medical v. surgical patient and ward v. ICU admission. Results are presented as Odds Ratio (OR) for mortality prediction with the corresponding 95% confidence intervals.
Kaplan-Meier survival analysis were performed, and Log-rank test results were included when analyzing MR-proADM usefulness to detect differences in survivability according to both AUROC results in this study and cut-off points previously reported in the pertaining literature. Finally, since we hypothesize SOFA score ≤ 6 patients have a particular biomarker profile we conducted Pearson’s correlations to measure associations between MR-proADM, Lactate, PCT and other clinical variables of interest. All reported p-values were two-sided and set with significance levels at <0.05. Statistical analysis was performed with both SPSS version 18.0 (IBM) and Stata version 12.0 (StataCorp LP, College Station, TX).
3. Results
3.1. Participant characteristics
During the study period, the in-hospital sepsis code was activated in 1117 patients. 567 patients were excluded for presenting a SOFA score > 6. Of the remaining 550, 266 patients were excluded for the reasons described in Figure 1.
A total 284 patients were identified that met the inclusion criteria, with a 28-day all-cause mortality of 8.4% (N=24). Of the 284 patients included, 184 (64.8%) patients had a diagnosis of sepsis and 100 (35.2%) septic shock. Patients had a mean age of 63 years, female patients accounted for 37.7%, and most cases were identified in the emergency department (48.6%). Positive blood cultures were obtained in 38.2% (N=108) with predominantly Gram-negative bacteria growth (63.1%, N=70). ISC was activated in 56 (19.7%) patients already admitted into the ICU. Of the remaining 228 patients, 62 (27.2%) were admitted into the ICU from the Emergency Department or another hospital ward. The median of ICU length of stay was 4 days (2–8) and median of hospital length of stay was 13 (6–30) (Table 1).
3.2. Biomarker predictive ability in patients with sepsis and a SOFA score ≤6
Lactate showed the highest predictive ability for all-cause 28-day mortality with an AUROC of 0.67 (0.55–0.79). In contrast, the AUROC for MR-proADM was low, with an AUROC of 0.57 (0.45–0.69). Parallelly, the AUROC for CRP was 0.49 (0.36–0.62) and for PCT was 0.47 (0.35–0.59) (Table 2).
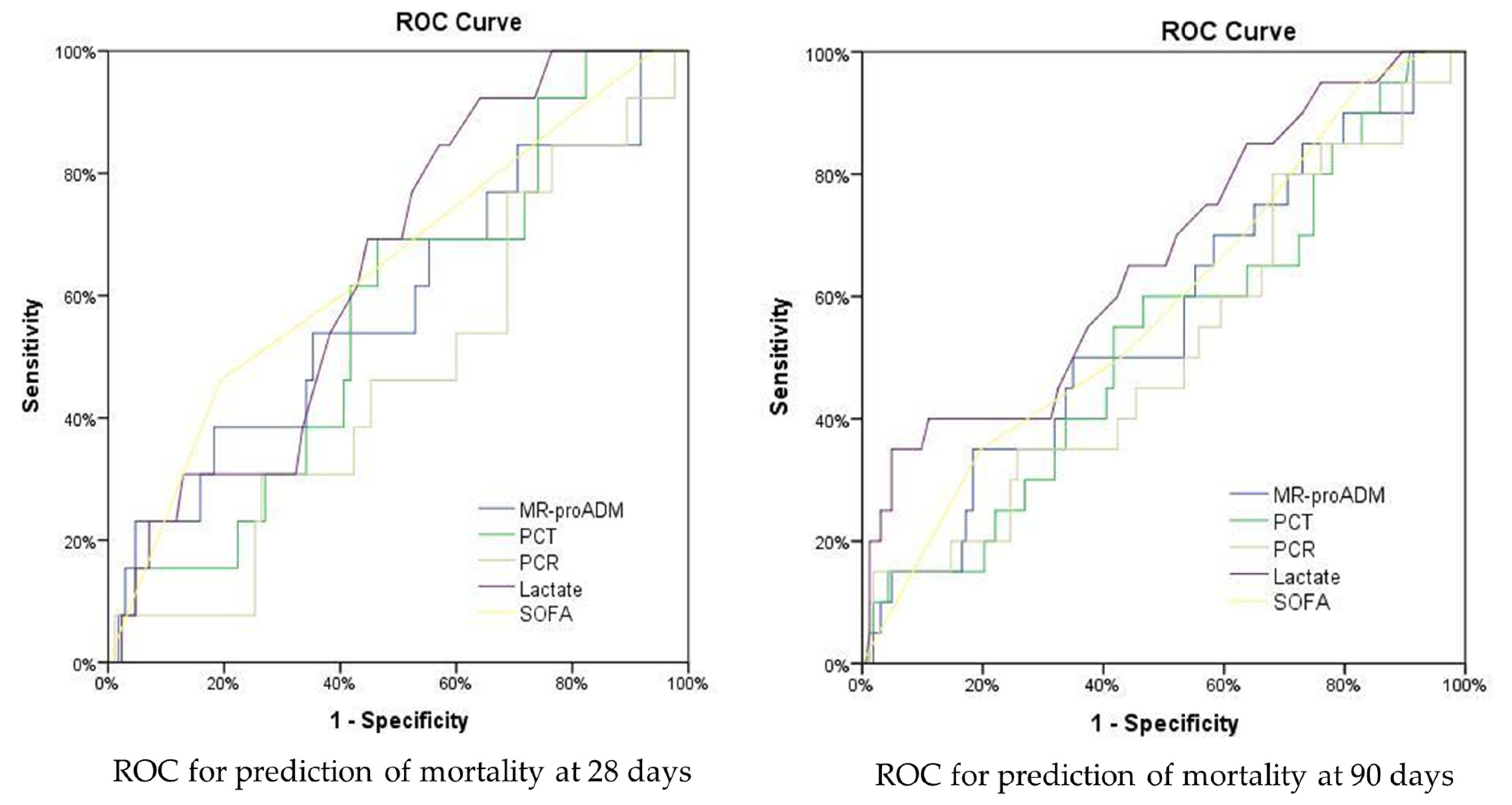

Table 2.
Area under the ROC for prediction of mortality at 28 days and 90 days.
| Analyses | ||||||||
| Univariate | Multivariate | |||||||
| Biomarker or clinical score | Patients (N) | AUROC | OR IQR (95% CI) | OR IQR (95% CI) | ||||
| M28d | MR-proADM | 284 | 0.57 [0.45 - 0.69] | 1.08 [0.94 – 1.24] | 1.13 [0.82 – 1.56] | |||
| PCT | 274 | 0.47 [0.35 - 0.59] | 0.99 [0.98 – 1.01] | 0.99 [0.97 – 1.02] | ||||
| CRP | 237 | 0.49 [0.36 - 0.62] | 1.00 [0.99 – 1.01] | 1.01 [0.98 – 1.04] | ||||
| Lactate | 229 | 0.67 [0.55 - 0.79] | 1.13 [0.95 – 1.34] | 0.85 [0.49 – 1.49] | ||||
| SOFA | 284 | 0.63 [0.52 - 0.73] | 1.43 [1.03 – 1.97] | 1.63 [0.69 – 3.84] | ||||
| M90d | MR-proADM | 284 | 0.59 [0.49 - 0.68] | 1.08 [0.96 – 1.21] | 0.93 [0.72 – 1.20] | |||
| PCT | 274 | 0.44 [0.34 - 0.54] | 1.00 [0.99 – 1.00] | 0.99 [0.97 – 1.01] | ||||
| CRP | 237 | 0.54 [0.43 - 0.65] | 1.00 [0.99 – 1.01] | 1.00 [0.98 – 1.03] | ||||
| Lactate | 229 | 0.66 [0.55 - 0.77] | 1.25 [1.07 – 1.46] | 1.50 [0.90 – 2.50] | ||||
| SOFA | 284 | 0.62 [0.54 - 0.71] | 1.40 [1.08 – 1.81] | 1.31 [0.70 – 2.43] | ||||
Abbreviations: AUROC, area under the ROC; CI, confidence interval; OR, odds ratio; IQR, interquartile range; M28d, 28-day mortality; M90d, 90-day mortality. Multivariate analyses show the OR for predictive ability of every biomarker when combined between themselves and the inclusion of other variables: age, SOFA, APACHE II and nosocomial infection.
Both the univariate and multivariate logistic regression analyses of mortality at 28 days by each and all biomarkers were not statistically significant, however, SOFA score had a significant OR (95% CI) of 1.43 for the same endpoint (Table 2).
When considering 90-day all-cause mortality, the AUROC for all biomarkers showed similar AUROCs to those established for 28-day mortality. In the same manner, univariate and multivariate ORs of all biomarkers and SOFA score were not statistically significant (Table 2).
The predictive ability of each biomarker for 28-day mortality was analyzed separately for either community-acquired or hospital-acquired infections. In patients with community-acquired infection, the best predictive AUROCs corresponded to MR-proADM (0.70 [0.58–0.82]) and SOFA score (0.69 [0.54–0.84]). In contrast, for hospital-acquired infection, only lactate showed a similarly high AUROC (0.70 [0.57–0.87]). Nonetheless, univariate and multivariate ORs of all biomarkers and SOFA score were not statistically significant (Table 3).
3.3. Inter-biomarker associations and 28-day survival analysis in patients with sepsis and a SOFA score ≤6
We found positive and significant correlations between MR-proADM, lactate and PCT (Figure 2). Interestingly, from this secondary analysis, we also found a positive correlation between MR-proADM and age (r=0.12, p<0.05).
Additionally, according to our best predictive AUROC, we established that a MR-proADM cut-off point of 2.1nmol/L classified with 100% sensitivity all non-survivors in patients with community-acquired infection. We generated a survival analysis for 28 days for this subgroup of patients using the 2.1nmol/L MR-proADM cut-off. a Log-rank test of the Kaplan-Meier survival curves found significant statistical differences between survivors and non-survivors (Figure 3).
4. Discussion
The present study analyzed the predictive ability of various biomarkers for 28-day all-cause mortality in sepsis patients with a SOFA score ≤6. The overall mortality rate observed in this study was 8.45%, aligning with the mortality rates reported in the existing literature on this particular subject [11].
MR-proADM showed an acceptable AUROC for 28-day mortality prediction in sepsis patients with community-acquired infection. In contrast, lactate showed the highest predictive ability in sepsis patients with hospital-acquired infection. Other biomarkers showed low predictive ability in sepsis patients with a SOFA ≤ 6.
The use of scoring systems and clinical and laboratory variables as tools to assist early diagnosis and determine severity are well-established, and many biomarkers have been extensively studied and implemented in ICUs and emergency departments. [5, 23–28] The SOFA score is widely applied and provides a screening score indicating risk of a poor outcome [29]. However, this score is not without inherent limitations and may not always be easy to apply [30,31,32]. Moreover, despite the low mortality risk in sepsis patients presenting with a SOFA <6 [10], a subgroup of patients still appears to have a high mortality rate. Identifying this subgroup of patients may allow the early initiation of appropriate treatment strategies, avoiding over or under-treatment and reducing mortality [33]. Interestingly in the present study, even in patients with a SOFA ≤6, SOFA remained the best individual predictor of survival. Thus, even in the lower SOFA range, organic dysfunction still discriminates severity better than the inflammatory response or hypoperfusion measured by biomarkers. Nonetheless, recent studies have indicated the potential of novel biomarkers such as MR-proADM and PCT [5, 34].
MR-proADM has been proposed as a potentially useful early marker in critically ill patients as its concentrations correspond to microcirculatory and endothelial damage in the early stages of organ dysfunction [35,36,37,38]. Hence, its consideration as an indicator of early microcirculatory damage in patients with a low SOFA score. Previous studies support this consideration showing that MR-proADM may be elevated in those sepsis patients likely to develop multiple organ failure even with a low or moderate SOFA score [17]. Our results are in line with these affirmations as inflammatory biomarkers are correlated with each other even with low SOFA scores.
Other authors have reported that MR-proADM indicates the development of organ failure 24h in advance [39]. Moreover, even with a SOFA score that does not meet the definition for sepsis, an elevated MR-proADM identifies septic patients allowing for early treatment initiation [7]. Parallelly, in this study, elevated MR-proADM levels correlated with age increase, a finding that has not been thoroughly investigated and that may lead to age dependent cut-off points, increasing the diagnostic accuracy of this inflammatory biomarker. MR-proADM has also shown good predictability for identifying patients that would require ICU admission and had good accuracy in identifying 28-day and 90-day mortality [5].
The current study results are in line with previous studies and provide further supportive evidence for considering its use as part of a panel of early biomarkers in sepsis patients. These results support those found by Elke et al. [17] and Andaluz-Ojeda et al. [40], with MR-proADM showing a reasonable AUROC for 28-day mortality in patients with a SOFA≤6. Although the study by Andaluz-Ojeda et al. reported a higher AUROC for 28-day mortality for MR-proADM, their study only included ICU patients. In contrast, the present study included all hospital patients that activated the sepsis code regardless of their ward.
Moreover, in our study, a MR-proADM cut-off point of 2.1 nmol/L had 100% sensibility to discern non-survivors at 28-days for patients with community-acquired infection, making MR-proADM a potentially useful screening biomarker for severity in out-of-hospital sepsis.
Our results also match with those of Spoto et al. [7,20], who considered that MR-proADM was essential for early diagnosis of sepsis in those with a negative SOFA score. Hence, these studies, along with the results of this study, point to the potential of MR-proADM to guide clinical decisions and stratify risk, including in those with less severe disease or early sepsis.
Biomarkers may vary based on whether the infection is nosocomial or has its origin in the community. In particular, as hospital-acquired sepsis patients were originally admitted for another cause that can affect these biomarkers—for example, major surgery, or other major illness—and may confound the results. In contrast, in community-acquired sepsis patients, any changes in biomarker values are most likely to represent only the effect of sepsis. Along these lines, the present study showed that MR-proADM might be more useful to predict mortality in community-acquired infections, while lactate may be better to forecast mortality for hospital-acquired infections.
4.1. Limitations
The results of this study should be interpreted considering some limitations. First, the relatively low number of enrolled patients in a single center may have resulted in many subgroups being underpowered. Further, larger studies are needed to build on this study and determine the usefulness of the biomarkers studied. Second, the present study also reflects real clinical practice, and we cannot ensure that during the study period the in-hospital sepsis code was activated in all patients with sepsis. Nevertheless, our results are consistent with those previously discussed in the literature [16,40], despite the patient population enrolled in this study being preselected based on fulfilling a particular hospital sepsis criterion. Hence, this study provides additional supportive data for these biomarkers and their use at different hospital settings and varying levels of illness.
5. Conclusions
The present study results suggest that in patients with community-acquired sepsis and an initial SOFA score ≤6, MR-proADM could help identify patients at risk of 28-day mortality. In those with hospital-acquired infection, lactate provided better predictive ability for 28-day mortality. Therefore, initial measurement of these biomarkers could facilitate early treatment strategies based in risk stratification after activation of a hospital sepsis code in patients with SOFA≤6 and sepsis or septic shock.
Author Contributions
JB: JCRR and RF conceived and designed the study. JB was the primary author, editor of the manuscript and the lead clinical investigator. All authors contributed to the enrolment of patients and sample collection. All authors critically reviewed and approved the final manuscript. RF and JCRR take responsibility for the paper as a whole. All authors read and approved the final manuscript.
Funding
This research was funded by a restricted grant from Thermo Fisher (Germany), consisting of free of charge kits. However, the funding organization had no role in the collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript, or decision to submit the manuscript for publication.
Institutional Review Board Statement
The study protocol was approved by the Clinical Research Ethics Committee of Vall d’Hebron University Hospital (PR(AG)333/2016, PR(AG)336/2016, PR(AG)11/2016) without the need for informed consent and in agreement with the Declaration of Helsinki and its later amendments.
Informed Consent Statement
Informed consent was signed by the patient or representatives for the collection and use of blood samples in the sepsis bank for research purposes (as per PR(AG)336/2016).
Data Availability Statement
The datasets used and/or analyzed during the present study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors are grateful to the Vall d’Hebron University Hospital staff for their continued vigilance in identifying patients presenting with infections and for enrolling patients in this study. The authors want to thank all patients with sepsis for donating their blood, being able to create the sepsis biobank. The authors wish to thank David Suárez for providing statistical advice and also Ingrid de Ruiter, MBChB, PhD, for editorial support in the preparation of the draft of this manuscript.
Conflicts of Interest
All authors have provided information on potential conflicts of interest directly or indirectly related to the work submitted in the journal's disclosure forms. RF received fees for participating in an advisory board of Thermofisher.
References
- Yébenes, J.C.; SOCMIC (Catalonian Critical Care Society) Sepsis Working Group; Ruiz-Rodriguez, J.C.; Ferrer, R.; Clèries, M.; Bosch, A.; Lorencio, C.; Rodriguez, A.; Nuvials, X.; Martin-Loeches, I.; et al. Epidemiology of sepsis in Catalonia: analysis of incidence and outcomes in a European setting. Ann. Intensiv. Care 2017, 7, 1–10. [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Marshall, J.C.; A Ñamendys-Silva, S.A.; François, B.; Martin-Loeches, I.; Lipman, J.; Reinhart, K.; Antonelli, M.; Pickkers, P.; Njimi, H.; et al. Assessment of the worldwide burden of critical illness: the Intensive Care Over Nations (ICON) audit. Lancet Respir. Med. 2014, 2, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, M.C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K.; International Forum of Acute Care Trialists. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Baldirà, J.; Ruiz-Rodríguez, J.C.; Wilson, D.C.; Ruiz-Sanmartin, A.; Cortes, A.; Chiscano, L.; Ferrer-Costa, R.; Comas, I.; Larrosa, N.; Fàbrega, A.; et al. Biomarkers and clinical scores to aid the identification of disease severity and intensive care requirement following activation of an in-hospital sepsis code. Ann. Intensiv. Care 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Jones, A.E.; Trzeciak, S.; Kline, J.A. The Sequential Organ Failure Assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation*. Crit. Care Med. 2009, 37, 1649–1654. [Google Scholar] [CrossRef]
- Spoto, S.; Nobile, E.; Carnà, E.P.R.; Fogolari, M.; Caputo, D.; De Florio, L.; Valeriani, E.; Benvenuto, D.; Costantino, S.; Ciccozzi, M.; et al. Best diagnostic accuracy of sepsis combining SIRS criteria or qSOFA score with Procalcitonin and Mid-Regional pro-Adrenomedullin outside ICU. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Martínez, M.L.; Ruiz-Rodríguez, J.C.; Ferrer, R. Improving knowledge about sepsis 3 definition in critically ill patients: new insights. J. Emerg. Crit. Care Med. 2018, 2, 39–39. [Google Scholar] [CrossRef]
- Sprung, C.L.; Schein, R.M.H.; Balk, R.A. The new sepsis consensus definitions: the good, the bad and the ugly. Intensiv. Care Med. 2016, 42, 2024–2026. [Google Scholar] [CrossRef]
- Vincent, J.-L.; de Mendonca, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Mélot, C.; Vincent, J.-L. Serial Evaluation of the SOFA Score to Predict Outcome in Critically Ill Patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef] [PubMed]
- Angeletti, S.; Spoto, S.; Fogolari, M.; Cortigiani, M.; Fioravanti, M.; De Florio, L.; Curcio, B.; Cavalieri, D.; Costantino, S.; Dicuonzo, G. Diagnostic and prognostic role of procalcitonin (PCT) and MR-pro-Adrenomedullin (MR-proADM) in bacterial infections. APMIS 2015, 123, 740–748. [Google Scholar] [CrossRef]
- Angeletti, S.; Dicuonzo, G.; Fioravanti, M.; De Cesaris, M.; Fogolari, M.; Presti, A.L.; Ciccozzi, M.; De Florio, L. Procalcitonin, MR-Proadrenomedullin, and Cytokines Measurement in Sepsis Diagnosis: Advantages from Test Combination. Dis. Markers 2015, 2015, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Angeletti, S.; Ciccozzi, M.; Fogolari, M.; Spoto, S.; Presti, A.L.; Costantino, S.; Dicuonzo, G. Procalcitonin and MR-proAdrenomedullin combined score in the diagnosis and prognosis of systemic and localized bacterial infections. J. Infect. 2015, 72, 395–398. [Google Scholar] [CrossRef]
- Valenzuela-Sánchez, F.; Valenzuela-Méndez, B.; Rodríguez-Gutiérrez, J.F.; Estella-García. ; González-García, M.. New role of biomarkers: mid-regional pro-adrenomedullin, the biomarker of organ failure. Ann. Transl. Med. 2016, 4, 329–329. [Google Scholar] [CrossRef]
- Elke, G.; the SepNet Critical Care Trials Group; Bloos, F. ; Wilson, D.C.; Meybohm, P. Identification of developing multiple organ failure in sepsis patients with low or moderate SOFA scores. Crit. Care 2018, 22, 147. [Google Scholar] [CrossRef]
- Kim, H.; Hur, M.; Struck, J.; Bergmann, A.; Di Somma, S. Circulating Biologically Active Adrenomedullin Predicts Organ Failure and Mortality in Sepsis. Ann. Lab. Med. 2019, 39, 454–463. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Morgenthaler, N.G.; Struck, J.; Harbarth, S.; Bergmann, A.; Müller, B. Mid-regional pro-adrenomedullin as a prognostic marker in sepsis: an observational study. Crit. Care 2005, 9, R816–R824. [Google Scholar] [CrossRef] [PubMed]
- Spoto, S.; Fogolari, M.; De Florio, L.; Minieri, M.; Vicino, G.; Legramante, J.; Lia, M.S.; Terrinoni, A.; Caputo, D.; Costantino, S.; et al. Procalcitonin and MR-proAdrenomedullin combination in the etiological diagnosis and prognosis of sepsis and septic shock. Microb. Pathog. 2019, 137, 103763. [Google Scholar] [CrossRef]
- Ferrer R, Ruiz-Rodriguez JC, Larrosa N, Llaneras J, Molas E, González-López JJ. Sepsis code implementation at Vall d'Hebron University Hospital: rapid diagnostics key to success. ICU Management & Practice. 2017;17(4).
- Li, F.; He, H. Assessing the Accuracy of Diagnostic Tests. Shanghai Arch Psychiatry 2018, 30, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Albrich, W.; Christ-Crain, M.; Chastre, J.; Mueller, B. Procalcitonin for guidance of antibiotic therapy. Expert Rev. Anti-infective Ther. 2010, 8, 575–587. [Google Scholar] [CrossRef]
- Schuetz, P.; Aujesky, D.; Müller, C.; Müller, B. Biomarker-guided personalised emergency medicine for all – hope for another hype? Swiss Med Wkly. 2015, 145, w14079–w14079. [Google Scholar] [CrossRef]
- Schuetz, P.; Christ-Crain, M.; Thomann, R.; Falconnier, C.; Wolbers, M.; Widmer, I.; Neidert, S.; Fricker, T.; Blum, C.; Schild, U.; et al. Effect of Procalcitonin-Based Guidelines vs Standard Guidelines on Antibiotic Use in Lower Respiratory Tract Infections. JAMA 2009, 302, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Batschwaroff, M.; Dusemund, F.; Albrich, W.; Bürgi, U.; Maurer, M.; Brutsche, M.; Huber, A.R.; Müller, B. Effectiveness of a procalcitonin algorithm to guide antibiotic therapy in respiratory tract infections outside of study conditions: a post-study survey. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 29, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Chiappa, V.; Briel, M.; Greenwald, J.L. Procalcitonin Algorithms for Antibiotic Therapy Decisions. Arch. Intern. Med. 2011, 171, 1322–1331. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Wirz, Y.; Sager, R.; Christ-Crain, M.; Stolz, D.; Tamm, M.; Bouadma, L.; E Luyt, C.; Wolff, M.; Chastre, J.; et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst. Rev. 2017, 2019, CD007498. [Google Scholar] [CrossRef]
- Singer, A.J.; Ng, J.; Thode, H.C.; Spiegel, R.; Weingart, S. Quick SOFA Scores Predict Mortality in Adult Emergency Department Patients With and Without Suspected Infection. Ann. Emerg. Med. 2017, 69, 475–479. [Google Scholar] [CrossRef]
- Simpson, S.Q. New Sepsis Criteria. Chest 2016, 149, 1117–1118. [Google Scholar] [CrossRef]
- Simpson, S.Q. SIRS in the Time of Sepsis-3. Chest 2018, 153, 34–38. [Google Scholar] [CrossRef]
- Simpson, S.Q.; Q. , S. Diagnosing sepsis: a step forward, and possibly a step back. Ann. Transl. Med. 2017, 5, 55–55. [Google Scholar] [CrossRef] [PubMed]
- van der Does, Y.; Limper, M.; Jie, K.E.; Schuit, S.C.; Jansen, H.; Pernot, N.; van Rosmalen, J.; Poley, M.J.; Ramakers, C.; Patka, P.; et al. Procalcitonin-guided antibiotic therapy in patients with fever in a general emergency department population: a multicentre non-inferiority randomized clinical trial (HiTEMP study). Clin. Microbiol. Infect. 2018, 24, 1282–1289. [Google Scholar] [CrossRef]
- Saeed, K.; del Castillo, J.G.; Backous, C.; Drevet, S.; Ferrer, R.; Gavazzi, G.; Gluck, E.; Jensen, J.-U.; Kanizsai, P.; Ruiz-Rodríguez, J.C.; et al. Hot topics on procalcitonin use in clinical practice, can it help antibiotic stewardship? Int. J. Antimicrob. Agents 2019, 54, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Temmesfeld-Wollbrück, B.; Hocke, A.; Suttorp, N.; Hippenstiel, S. Adrenomedullin and endothelial barrier function. Thromb. Haemost. 2007, 98, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Pittard, A.J.; Hawkins, W.J.; Webster, N.R. The role of the microcirculation in the multi-organ dysfunction syndrome. Clin. Intensiv. Care 1994, 5. [Google Scholar]
- Xie, Z.; Chen, W.-S.; Yin, Y.; Chan, E.C.; Terai, K.; Long, L.M.; Myers, T.G.; Dudek, A.Z.; Druey, K.M. Adrenomedullin surges are linked to acute episodes of the systemic capillary leak syndrome (Clarkson disease). J. Leukoc. Biol. 2018, 103, 749–759. [Google Scholar] [CrossRef] [PubMed]
- Vigué, B.; Leblanc, P.-E.; Moati, F.; Pussard, E.; Foufa, H.; Rodrigues, A.; Figueiredo, S.; Harrois, A.; Mazoit, J.-X.; Rafi, H.; et al. Mid-regional pro-adrenomedullin (MR-proADM), a marker of positive fluid balance in critically ill patients: results of the ENVOL study. Crit. Care 2016, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Viaggi, B.; Poole, D.; Tujjar, O.; Marchiani, S.; Ognibene, A.; Finazzi, S. Mid regional pro-adrenomedullin for the prediction of organ failure in infection. Results from a single centre study. PLOS ONE 2018, 13, e0201491. [Google Scholar] [CrossRef]
- Andaluz-Ojeda, D.; Nguyen, H.B.; Meunier-Beillard, N.; Cicuéndez, R.; Quenot, J.-P.; Calvo, D.; Dargent, A.; Zarca, E.; Andrés, C.; Nogales, L.; et al. Superior accuracy of mid-regional proadrenomedullin for mortality prediction in sepsis with varying levels of illness severity. Ann. Intensiv. Care 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow Chart of patients included in the present study.
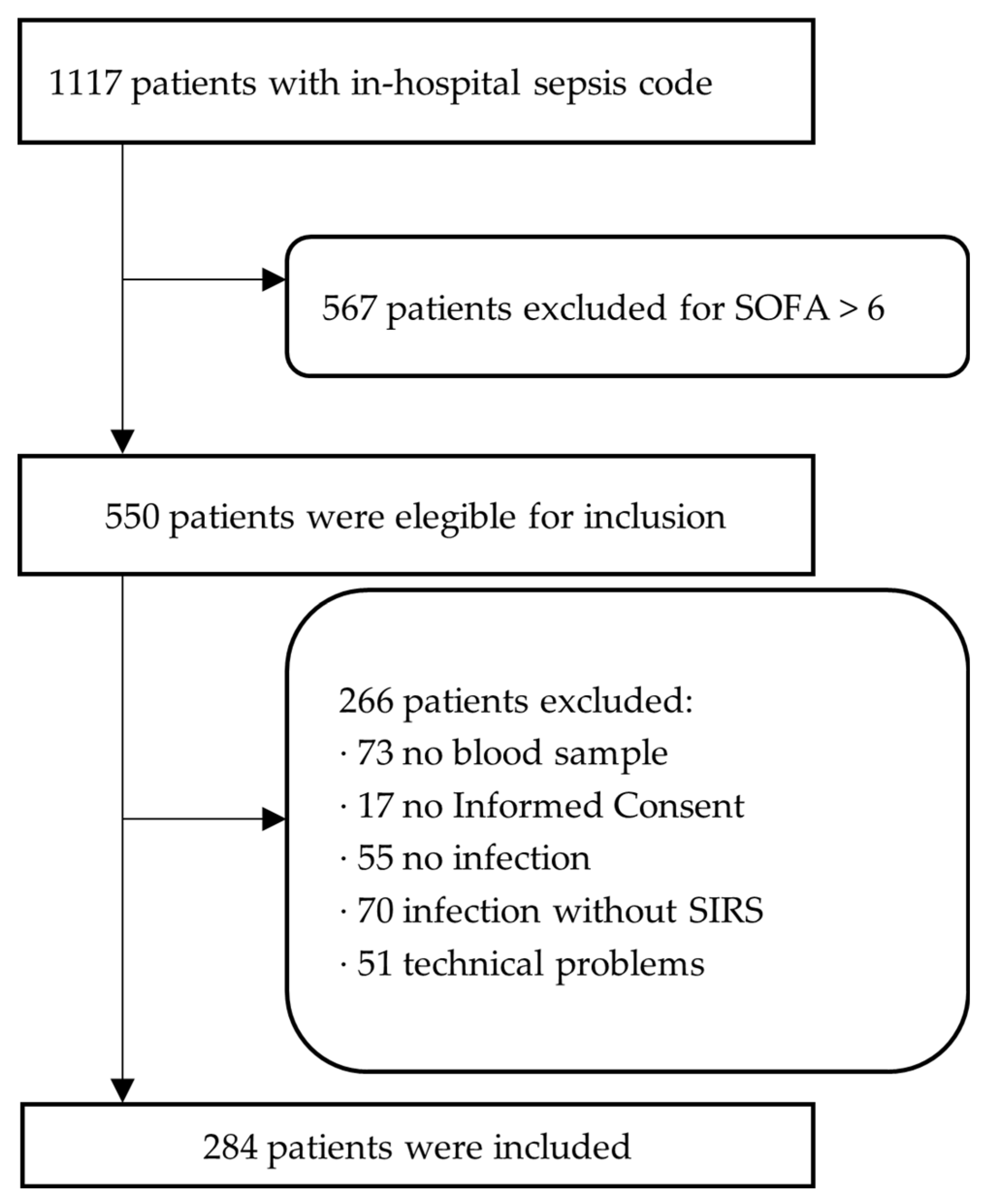
Figure 2.
Correlation between MR-proADM and lactate and MR-proADM and PCT.
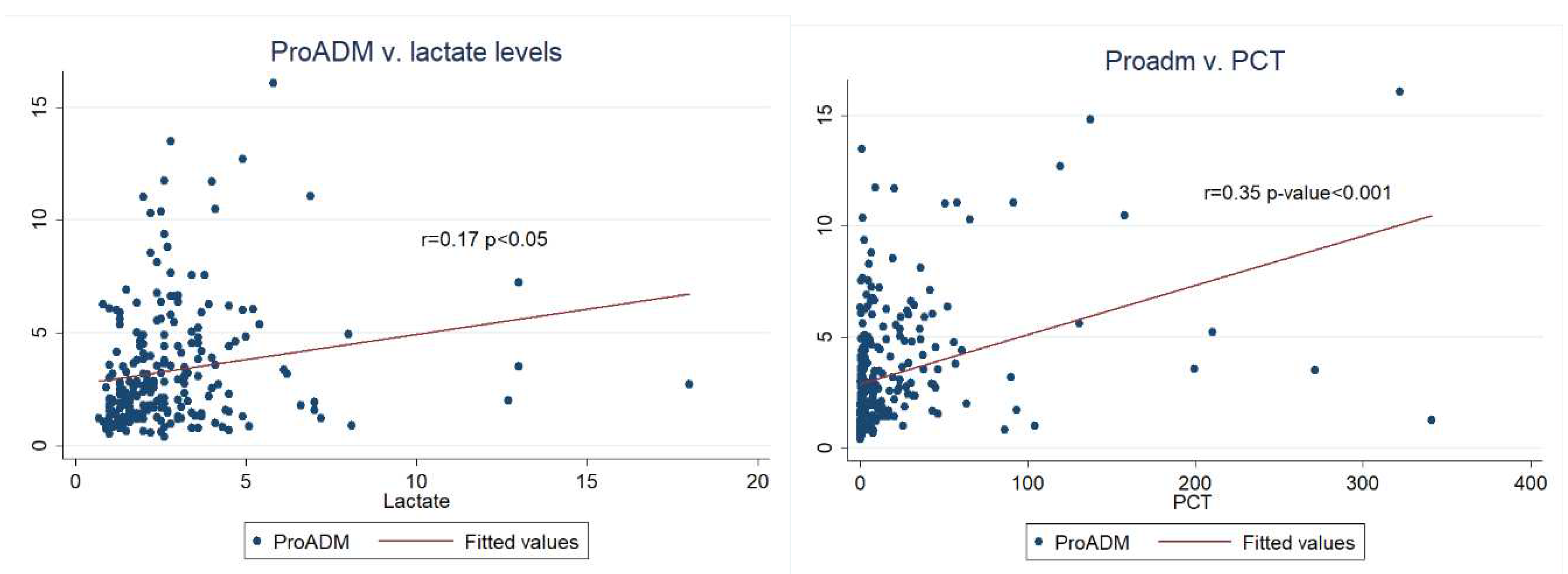
Figure 3.
Kaplan-Meier survival curves by MR-proADM in community acquired infection.
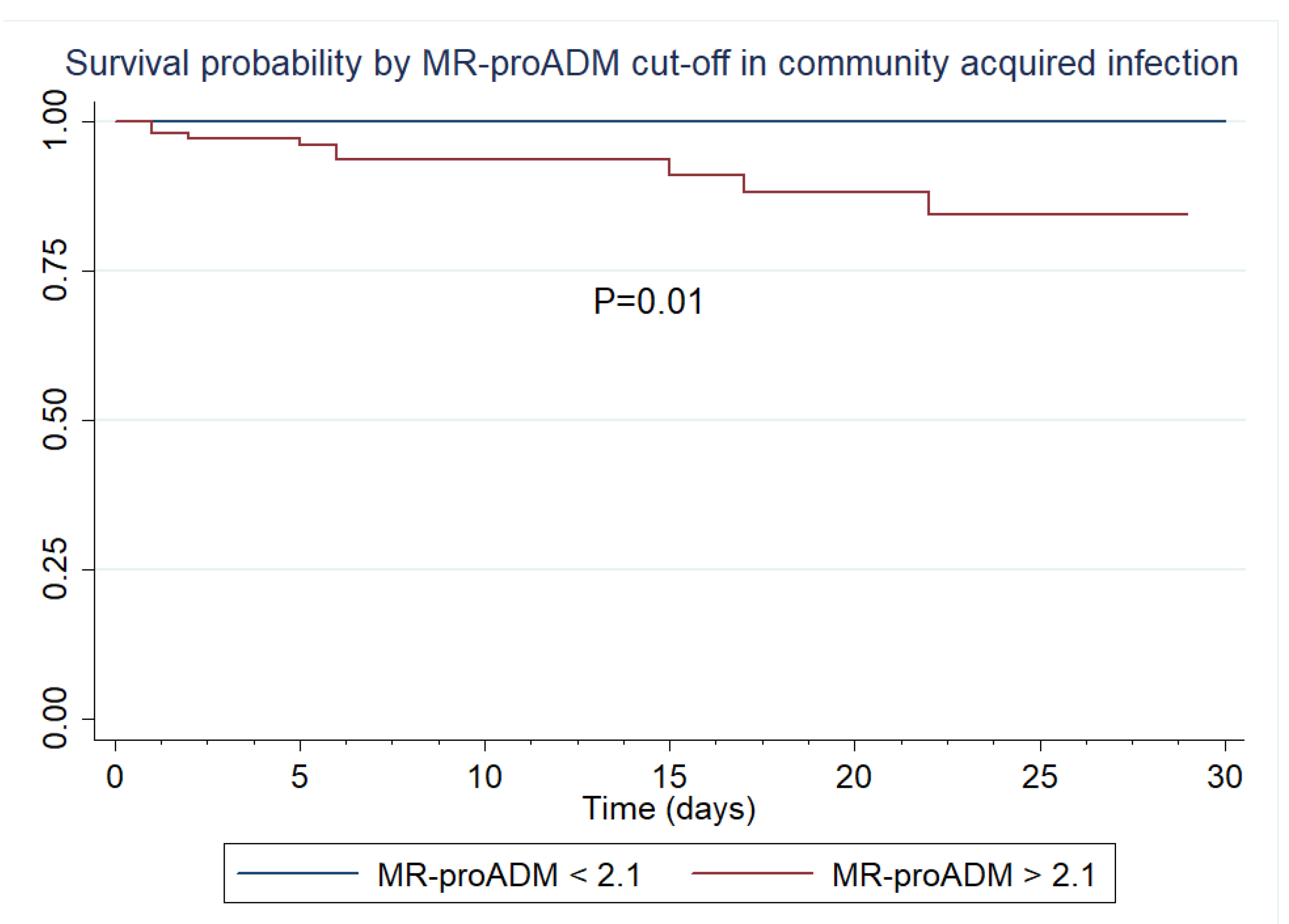
Table 1.
Clinical patient characteristics upon activation of the sepsis code with respect to the total infected patient population and subsequent 28-day mortality.
Table 1.
Clinical patient characteristics upon activation of the sepsis code with respect to the total infected patient population and subsequent 28-day mortality.
|
Patient population (N =284) |
Survivors (N = 260) |
Non-Survivors (N = 24) |
p-value | |
| Age (years) (mean, S.D.) | 63 (16) | 62 (16) | 70 (9) | 0.001 |
| Female gender (N, %) | 107 (37.7) | 100 (38.5) | 7 (29.2) | 0.36 |
| Definition of sepsis | ||||
| Severe sepsis (N, %) | 184 (64.8) | 170 (65.4) | 14(58.3) | 0.489 |
| Septic shock (N, %) | 100 (35.2) | 90 (34.6) | 10 (41.7) | 0.489 |
| Location of sepsis code activation | ||||
| Emergency Department (N, %) | 138 (48.6) | 127 (48.8) | 11 (45.8) | 0.793 |
| Ward (N, %) | 90 (31.7) | 83 (31.9) | 7 (29.2) | 0.781 |
| ICU (N, %) | 56 (19.7) | 50 (19.2) | 6 (25) | 0.497 |
| Surgical admissions (N, %) | 104 (36.6) | 95 (36.5) | 9 (37.5) | 0.925 |
| Medical admissions (N, %) | 180 (63.4) | 165 (63.5) | 15 (62.5) | 0.925 |
| ICU length of stay (days) (median, IQR) | 4 [2-9] | 3 [2-8] | 11 [5-15] | 0.125 |
| Hospital length of stay (days) (median, IQR) | 13 [6-30] | 14 [7-32] | 7 [3-17] | 0.016 |
| Life-supporting and intensive care therapies | ||||
| Vasopressors (N, %) | 100 (35.2) | 90 (34.6) | 10 (41.7) | 0.489 |
| Renal replacement therapy (N, %) | 11 (8.5) | 9 (7.5) | 2 (20) | 0.172 |
| Mechanical ventilation (N, %) | 51 (18) | 43 (16.5) | 8 (33.3) | 0.04 |
| Mechanical ventilation duration (days) (median, IQR) | 5 [3-12] | 4 [2-8] | 12 [7-16] | 0.02 |
| High Flow Nasal Cannula use (N, %) | 41 (31.5) | 35 (29.2) | 6 (60) | 0.044 |
| Pre-existing comorbidities | ||||
| Cardiopathy (N, %) | 71 (25) | 65 (25) | 6 (25) | 1.00 |
| Chronic Kidney Disease (N, %) | 50 (17.6) | 47 (18.1) | 3 (12.5) | 0.492 |
| COPD (N, %) | 49 (17.3) | 45 (17.3) | 4 (16.7) | 0.937 |
| Immunosuppression (N, %) | 129 (45.4) | 112 (43.1) | 17 (70.8) | 0.009 |
| Liver cirrhosis (N, %) | 12 (4.2) | 9 (3.5) | 3 (12.5) | 0.035 |
| Microbiology | ||||
| Positive blood culture (N, %) | 108 (38.2) | 99 (38.2) | 9 (37.5) | 0.622 |
| Gram-positive (N, %) | 39 (35.1) | 34 (33.3) | 5 (55.6) | 0.291 |
| Gram-negative (N, %) | 70 (63.1) | 66 (64.7) | 4 (44.4) | 0.343 |
| Fungal (N, %) | 2 (1.8) | 2 (2) | 0 (0) | 0.666 |
| Origin of infection | ||||
| Abdominal (N, %) | 76 (26.8) | 72 (27.7) | 4 (16.7) | 0.243 |
| Bacteria - primary (N, %) | 11 (3.9) | 10 (3.8) | 1 (4.2) | 0.938 |
| Catheter-related (N, %) | 11 (3.9) | 10 (3.8) | 1 (4.2) | 0.938 |
| Central Nervous System (N, %) | 1 (0.4) | 1 (0.4) | 0 (0) | 0.761 |
| Respiratory (N, %) | 68 (23.9) | 57 (21.9) | 11 (45.8) | 0.009 |
| Soft-tissue (N, %) | 18 (6.3) | 16 (6.2) | 2 (8.3) | 0.675 |
| Urinary (N, %) | 84 (29.6) | 79 (30.4) | 5 (20.8) | 0.327 |
| Unknown (N, %) | 8 (2.8) | 8 (3.1) | 0 (0) | 0.383 |
| Other (N, %) | 7 (2.5) | 7 (2.7) | 0 (0) | 0.416 |
| Source control | ||||
| Debridement of infectious foci (N, %) | 15 (5.4) | 14 (5.5 | 1 (4.3) | 0.799 |
| Drainage (N, %) | 40 (14.4) | 38 (14.9) | 2 (8.7) | 0.397 |
| Surgery (N, %) | 35 (12.6) | 33 (12.9) | 2 (8.7) | 0.534 |
| Biomarker and severity scores | ||||
| MR-proADM (nmol/L) (median, IQR) | 2.48 [1.46-4.38] | 2.43 [1.45-4.2] | 2.85 [1.8-4.98] | 0.236 |
| PCT (ng/mL) (median, IQR) | 3.09 [0.7-16,.1] | 3.10 [0.7-17.5] | 3.51[0.7-8.8] | 0.665 |
| Lactate (mmol/L) (mean, SD) | 2.75 (2.09) | 2.70 (2.10) | 3.48 (1.84) | 0.147 |
| CRP (mg/L) (mean, SD) | 56.43 (288.39) | 46.18 (258.14) | 156.57 (494) | 0.312 |
| SOFA (points) (median, IQR) | 4 [3-6] | 4 [3-6] | 5 [4-6] | 0.027 |
| APACHE II (points) (mean, SD) | 19.71 (8.29) | 19.10 (8.11) | 26.50 (7.61) | 0.015 |
Table 3.
AUROCs and ORs for 28-day mortality in hospital-acquired vs. community-acquired infections.
Table 3.
AUROCs and ORs for 28-day mortality in hospital-acquired vs. community-acquired infections.
| Analyses | ||||||||
| Univariate | Multivariate | |||||||
| Biomarker or clinical score | Patients (N) | AUROC | OR IQR (95% CI) | OR IQR (95% CI) | ||||
| Community | MR-proADM | 176 | 0.70 [0.58 – 0.82] | 1.11 [0.91 – 1.35] | 2.11 [0.7 –6.39] | |||
| PCT | 168 | 0.41 [0.30 – 0.52] | 0.92 [0.82 – 1.04] | 0.93 [0.79 –1.11] | ||||
| CRP | 147 | 0.55 [0.32 – 0.78] | 1.01 [1.00 – 1.03] | 1.01 [0.83 –1.25] | ||||
| Lactate | 142 | 0.65 [0.48 – 0.82] | 1.09 [0.75 – 1.56] | 1.31 [0.85 –20.20] | ||||
| SOFA | 176 | 0.69 [0.54 – 0.84] | 1.80 [0.98 – 3.30] | - | ||||
| Hospital | MR-proADM | 108 | 0.48 [0.30 – 0.66] | 1.07 [0.88 – 1.30] | 1.00 [0.69 – 1.46] | |||
| PCT | 106 | 0.53 [0.35 – 0.71] | 1.00 [0.99 – 1.00] | 1.01 [0.96 – 1.06] | ||||
| CRP | 87 | 0.49 [0.32 – 0.66] | 0.99 [0.98 – 1.01] | 1.00 [0.95 – 1.04] | ||||
| Lactate | 93 | 0.70 [0.54 – 0.86] | 1.14 [0.93 – 1.38] | 0.86 [0.44 – 1.65] | ||||
| SOFA | 108 | 0.57 [0.43 – 0.71] | 1.23 [0.85 – 1.77] | 1.18 [0.54 – 2.59] | ||||
Abbreviations: AUROC, area under the ROC; CI, confidence interval; OR, odds ratio; IQR, interquartile range; M28d, 28-day-mortality; M90d, 90-day mortality. Multivariate analyses show the OR for predictive ability of every biomarker when combined between themselves and the inclusion of SOFA and APACHE II scores.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



