
Submitted:
29 July 2025
Posted:
31 July 2025
You are already at the latest version
Abstract
Diabetes is a chronic disease that occurs either when the pancreas does not produce enough insulin or when the body cannot effectively use the insulin it produces or both. Type 1 Diabetes Mellitus has for long been managed using insulin, while Type 2 is managed by oral hypoglycemic agents. However, these agents are associated with a number of short comings and adverse effects. Local communities in different parts of Uganda have resorted to using extracts from medicinal plants. There is paucity of data on the efficacy, safety and probable phytochemicals that are responsible for the medicinal plant-based diabetes treatment. This study, therefore, was conducted to investigate the crude leaf extract of Aspiliapluriseta in order to validate its claimed oral hypoglycemic efficacy, its safety and phytochemical composition.The plant extract was subjected to phytochemical analysis, acute toxicity testing and evaluation of its oral hypoglycemic effects against streptozotocin-induced diabetes in Wistar rats. The results from the study showed that tannins, reducing sugars, anthracenosides, coumarins and saponins plus steroid glycosides and flavonoid derivatives were present in significant quantities while alkaloids and phenols were in trace amounts. The results for the oral hypoglycemic study indicated that an increase in dose of the extract led to a significant decrease in the blood glucose levels of the treated animals (p-value up to p < 0.001) compared to the negative controls. The results from acute toxicity test showed some acute toxic effects, although no fatality was observed.From the results, it was concluded that the aqueous leaf extract of Aspilia pluriseta contains phytochemicals like coumarins, flavonoids and glycosides, among other phytochemicals which may be responsible for antidiabetic effects. The extract also had a significant hypoglycemic effect but with some acute toxic autonomic and CNS effect.
Keywords:
diabetes
; Aspilia pluriseta
; hyperglycemia
; medicinal plants
; hypoglycemic activity
; phytochemicals
; phytochemical analysis
Introduction
Diabetes mellitus is a disorder of carbohydrate, fat and protein metabolism [24]. A major complication of Diabetes Mellitus is diabetic ketoacidosis (DKA), which is an acute and life-threatening complication that mainly occurs in patients with Type 1 Diabetes, although it may also occur among Type 2 diabetic patients. Diabetic ketoacidosis occurs because lack of insulin deprives the body of glucose which it needs for energy, which, in turn, leads to break down of fat to get an alternative source of energy. This process results in fatty acids called keto-acids, the build-up of which makes the blood acidic [7]. Some of the symptoms of DKA include excessive thirst, increased urine output, body wasting and general weakness, vomiting, loss of appetite, confusion, abdominal pain, dyspnea, increased heart rate, low blood pressure, increased breathing rate, and if not treated, it can lead to coma or even death [2,7].
According to International Diabetes Federation (IDF), 415 million people in 2015 had diabetes worldwide and this trend was projected to rise to 642 by 2040 [6]. On the African continent, 14.2 million people had diabetes in 2015 and this number was projected to rise to 34.2 million people in 2040 [6]. Also according to the same IDF report, 215.2 million men in 2015 had diabetes worldwide and this was project to rise to 328.4 million in 2040. In the same year, 199.5 million women were reported to have diabetes and this figure was project to rise to 313.3 million women in 2040 [6]. Furthermore, IDF reported in 2015 that one person died of diabetes every six seconds worldwide, meaning that 5 million people died from diabetes in 2015 alone [6]. In the same year, IDF also reported that seventy-five out of every one hundred persons with diabetes lived in low and middle-income countries [6]. Regarding Uganda, the diabetic population was estimated at about 98,000 in 2000, and this trend increased more than fifteen times to 1.5 million in a decade [11]. Based on the country’s estimated population of 30 million people in 2010, the figure implied that about five percent of the country’s population was diabetic, which was a very large proportion of the country’s population [11].
Treatment of Type 1 DM is by use of various insulin preparations while Type 2 DM is managed by using various types of oral hypoglycemic agents. The oral hypoglycemic agents used in the management of diabetes exert their effects by various mechanisms like: [1] stimulation of beta cells in the pancreas to produce more insulin (sulfonylureas and meglitinides); [2] increasing the sensitivity of muscles and other tissues to insulin (thiazolidinediones); [3] decreasing gluconeogenesis by the liver (biguanides); and [4] delaying the absorption of carbohydrates from the gastrointestinal tract (alpha-glucosidase inhibitors) [25]. However, these treatments have their own drawbacks ranging from the high cost and adverse effects, to lack of responsiveness in a large segment of patient population [1].
Moreover, none of these glucose-lowering agents adequately controls the hyperlipidemia that is frequently associated with diabetes [1].Apart from the complications associated with the use of oral hypoglycemic agents used in the treatment of diabetes, most of these drugs are too expensive for most of the patients especially those in rural areas when compared to the use of herbal remedies.
However, since the herbs are usually used without scientific validation, their use may be associated with various dangers like being toxic to the body organs like the liver, spleen and kidney, among others [20]. Another disadvantage regarding the use of herbal remedies in the management of DM is that they may not produce any pharmacological effect but the patients may only experience psychological relief from disease symptoms which is dangerous as it may lead to exacerbation of the disease. This, therefore, contributes to the need to explore alternative interventions for diabetes treatment that are efficacious, safe and affordable in low resource countries like Uganda.
The prevailing situation led to most local communities in Uganda resorting to the use of herbal remedies for the management of diabetes and diabetic complications. Some of the antidiabetic medicinal herbs include Aspilia pluriseta, which has been reported as being used ethnobotanically in the management of diabetes mellitus among other uses like wound healing and HIV symptoms [20]. Despite the wide spread use of Aspilia pluriseta for the traditional treatment of DM in Uganda in general, and in Bushenyi district in particular, there is scanty published literature on the antidiabetic activity and safety profile of this plant, especially the leaves. Even the study carried out by Ngugi, et al, [10], did not report anything about the activity of the leaves of this plant. The leaves usually have different phytochemical composition or phytochemicals in different concentrations from those in the roots. This difference in concentrations can be caused by translocation of the phytochemicals from the leaves to the roots [14,17]. The ability of the leaves to contain different phytochemicals from the roots can also be due to continuous exposure of the leaves to sunlight, rain and wind. There is further literature that suggests that some selected plants get negative effects from the volatile organic compounds that are soil derived [19]. Therefore, there was need to validate the ethnobotanical claims and safety of the leaves of this plant, which is the part that is used by Ugandan communities, particularly in Bushenyi district, where this study was conducted.
The present work was aimed at determining the oral hypoglycemic activity of the aqueous crude leaf extract of Aspilia pluriseta in streptozotocin-induced diabetic wistar rats, its acute toxicity and phytochemical composition.
Materials and methods
Plant harvesting and leaf processing
The leaves of Aspilia pluriseta were obtained from the bush in Kibare village, Nyakabirizi division, Bushenyi District. They were then transported to the Pharmacology Laboratory of Kampala International University for drying under the shade. The plant was identified taxonomically by a taxonomist from Mbarara University of Science and Technology. A voucher specimen was then deposited in the herbarium at Mbarara University of Science and Technology and a voucher number (PM/001) was obtained.
The leaves of the plant were then dried under the shade in the pharmacology laboratory until constant weight was attained. Drying under the shed was to avoid the ultra violet radiations from the direct sunlight destroying some phytochemicals within the plant leaves. The dry material was then pulverized using a metallic grinder to get powder.
The powder was then weighed and put into conical flasks and a specified amount of distilled water was added (50g of powder for 200ml of distilled water). The flasks were then covered with aluminum foil and shaken on a mechanical shaker for 12 hours. The mixture was then strained using a clean white piece of cloth to obtain the solution. The solution was filtered using a Buchner funnel and Whatman filter paper to obtain the filtrate. The filtrate obtained was concentrated using the oven at a temperature of 50oC. The resulting filtrate was then dried using an oven at 50oC. The dried extract was then weighed and stored in a refrigerator at a temperature of 2oC in amber jars during the experimental process. Before administration, the extract was reconstituted with distilled water to give the concentration of 10mg/ml from which different doses in mg/kg of body weight were obtained as well as the injectable volume.
The injectable volume (IV) was calculated from the formula below:
Body weight (g) x Dose (mg/kg)
Injectable volume (IV) =
Concentration (mg/ml) x1000
Phytochemical analysis
The tests for the presence of various phytochemical constituents were done using the methods described by Trease and Evans [26]. Phytochemical tests were done for tannins, saponins, reducing sugars, anthracenocides, coumarins, steroid glycosides, flavonosides, alkaloids, starch, Phenols, Anthraquinones, and Terpenes
Experimental animals
Twenty young adult wistar albino rats (Rattus norvegicus); 10 males and 10 females of average weight between 80 to 200g, and of average age 8 to 12 weeks were used for oral hypoglycemic study [5]. Animals with a normal typical weight of ± 20% were considered fit for experiment [5]. The animals were randomly assigned to different groups. Twelve female rats of the same age and similar weight but which were not pregnant, were used for acute toxicity study [12]. The animals were purchased from the Pharmacology Department of Kampala International University, Western Campus. They were then acclimatized to the environment of the laboratory and to the handlers for five days, prior to the study [12]. The animals were housed at room temperature and given plenty of feeds (rat pellets) and water ad-libitum.The rat feeds were purchased from a shop which deals in animal feeds in Ishaka town Bushenyi district. The animals were then fasted for 24 hours before the study begun but they had continuous access to water. They were then provided with food and water four hours post dosing.
Acute toxicity study
The acute toxicity study was carried out using Lorke’s method as described below.
Lorke’s method has an advantage over other methods used in acute toxicity study in that it uses fewer experimental animals. The procedure involves two phases.
Phase 1:This phase requires nine rats. The nine rats were divided into three groups of three rats each. Each group of rats was administered different doses (10, 100 and 1000 mg/kg) of plant extract orally. Group one received the extract at dose of 10mg/kg orally.
Group two received the extract at dose of 100mg/kg orally, while group three received the extract at a dose of 1000mg/kg orally. The dosed rats were then observed immediately for three hours. After the first three hours, observations were done at a 5-hour intervals and then after 24 hours, for any signs of toxicity including mortality.
Phase 2:This phase involved the use of three rats, which were distributed into three groups of one rats each. The three groups of rats (1, 2 and 3) were respectively administered higher doses of the extract at 1600, 2900 and 5000 mg/kg and then observed for 24 hours for behavioral changes and other signs of acute toxicity including mortality. The doses used in acute toxicity study are the standard doses recommended by the Lorke’s method. Depending on the method used for toxicity study, the initial dose and the limit dose are always standard depending on the method used [5]. The observations were done similarly as in phase 1 above. The geometric mean of the least dose that killed rats and the highest dose that did not kill the rats were taken as the median lethal dose (LD50) which was calculated from the formula:
D0 = Highest dose that gave no mortality,
D100 = Lowest dose that produced mortality.
The signs of toxicity that were considered included changes in motor activity, tremors, arching and rolling, convulsions, increased breathing rate, lacrimation, piloerection, salivation, muscle spasms, loss of righting reflex, sedation, hypnosis and diarrhea, as well as mortality.
Induction of hyperglycemia in experimental animals
Hyperglycemia was induced in experimental rats by an intraperitoneal injection of streptozotocin which was prepared by dissolving it in ice cold 50mM of sodium citrate buffer (pH 4.5) containing 0.9% sodium chloride. The agent was prepared immediately prior to use to avoid oxidation and loss of stability [5]). The dose of streptozotocin that was used to induce hyperglycemia in experimental rats was 60mg/kg body weight and the concentration was 60mg/ml. The administration of the agent (STZ) was done two days prior to administering the extract, after starving the animals for 24 hours. Rats with blood glucose levels greater than 200mg/dl were considered to be hyperglycemic and diabetic [5].
Administration of doses of the plant extract
A total of 20 young adult wistar albino rats were used for the oral hypoglycemic study. The rats were both adult male and female, but female rats were not pregnant or nursing. The animals were randomly divided into 5groups of 4 rats each as described above, after 24 hours of diabetes induction, using streptozotocin. Basing on the results of the acute toxicity study, three dose levels of the leaf extract, (100, 300 and 500) mg/kg body weight were selected for administration to 3 groups of rats with streptozotocin induced diabetes [5]. The above doses were chosen in comparison to those used by Ngugi et al., [10] who also carried out the hypoglycemic study on the root bark of the same plant (Aspilia pluriseta) but since they used the mice for their study, the doses used in this study had to be a bit higher since the rats are heavier than the mice. The fourth group was given insulin at a dose of 6 iu/kg body weight, which is the standard regimen for type 1DM to serve as a positive control, while the fifth group of diabetic rats was treated with normal saline at a dose of 10mg/kg body weight to be used as negative control.
The extract was administered orally daily for 20 days, while insulin and normal saline were given by subcutaneous route for the same period of time. Blood glucose levels were measured using a glucometer before extract administration, and then at a four-day interval post administration of the extract and the standard drug, plus the normal saline. Different blood glucose levels were recorded at a four-day interval for 20 days.Blood was obtained from the tail vein by snipping the tail tips with sterile scissors which was sterilized using an alcohol swab prior to use. Bleeding to get the blood sample was enhanced by gently “milking” the tail from the top towards its tip. The amount of blood that was collected from each animal was 0.05mls and blood was drawn 5 times every after 4 days during the study period of 20 days. Therefore, a total of 0.25mls of blood was collected from each animal for the whole study period and the tails of rats were sterilized using alcohol swab after each blood collection to avoid infection. In addition, the rats were weighed every day before administration of the next dose, to determine the changes in body weight. During the experimental period, all the rats were given food and water ad libitum.
Data analysis
SPSS version 20 for analysis in which ANOVA was used to determine the differences amongst the groups. The information was then subjected to post hoc test (Tukey’s test) to identify the sources of the differences observed earlier. Results with probability values (p-values) less than or equal to 0.05 were considered statistically significant. The results were presented as Mean± SEM
Ethical considerations
Ethical approval was obtained from the Institutional Research and Ethics Committee (REC) of Kampala International University-Western Campus. The OECD guidelines for the use, care and handling of laboratory animals were followed [12]). The animals were handled with care to minimize the pain and stress to them during the experiment, and only thirty two animals were used for the whole experimental process to reduce on the number [12]. The rats were kept in clean cages with adequate light and air. The animals were given water and food as described by the study.
Results
Phytochemical analysis of the plant extract
Various phytochemicals were found present in the plant extract. This is summarized in Table 1.
Oral hypoglycemic test
For the oral hypoglycemic study that was carried out in streptozotocin induced diabetic wistar rats, the changes in blood glucose levels as well as the changes in body weight were observed over a period of 20 days. The results of oral hypoglycemic study are presented in Table 2
The results from the above table indicate that an increase in dose of the extract led to a significant decrease in the blood glucose levels of the treated diabetic rats compared to the negative controls (p-value up to p < 0.001). Insulin (positive control) at 6IU/kg caused a decrease in the blood glucose level of the animals that was comparable to the effect of the plant extract at 500 mg/kg.
Mean blood glucose levels for all the treatment groups
The results in the graph above show how blood glucose levels changed during the experimental period. The high dose of the extract and the positive control showed lowering of blood glucose levels as compared to other treatment groups. The negative control produced an increase in blood glucose levels instead. The initial is when the blood glucose levels were taken after induction of diabetes but before treatment begun, while different intervals is the subsequent times at which blood glucose levels were taken during the experimental study, which was every after four days. This is illustrated in Figure 1.
Percentage reduction in the blood glucose levels of the animals for the three significant groups
The results in Figure 2 show the effects of the median and high dose of the extract and the positive control. The two doses of the extract caused a significant reduction in blood glucose levels and so did the positive control.
Acute toxicity of the extract
The results from Table 3 indicate that the extract has got some acute toxic effects especially autonomic and central nervous system effects as well as some degree of GIT effects although no fatality was observed with in the observation period for acute toxicity test.
Discussion
Percentage yield of Extract
A percentage yield of 28.15%is a comparatively high yield of extract considering the fact that distilled water was used, which tends to extract only polar phytochemicals. Different extraction solvents tend to produce different percentage yields depending on which phytochemicals can be extracted, whether polar or non-polar. This implies that use of a solvent mixture with both polar and non-polar elements could produce a much higher yield. A good yield of phytochemicals increases the prospects for commercialization since one of the most common hindrances with plant-derived products is limited yield [15].
Phytochemical analysis
The results of the study showed that tannins, reducing sugars, anthracenosides and coumarins were in abundant amounts, saponins, steroid glycosides, flavonoid derivatives, alkaloids and phenols were in trace amounts. The results from this study differed from those obtained by other researchers [10] in that the leaf extract was found to contain alkaloids and tannins, which were not reported in the study on root back (Table 3). This difference is one indication that the difference in the amount of different phytochemicals present was attributed to the method and solvent used for extraction. The absence of some phytochemicals could also be attributed to the solvent used for extraction since different extraction solvents tend to extract different classes of secondary metabolites. Others could be due to the habitat where the plant was harvested from, because plants of the same species growing in different habitats tend to have different phytochemical constituents [9]. For example, a plant growing in a valley will have different chemical constituents from the plant of the same species growing on a hilltop. Likewise, a plant growing in the shade may contain different chemical constituents from a plant of the same species growing in an open space. The part of the plant harvested because different plant parts tend to contain different phytochemical constituents. For example, chemical constituents in the plant leaves are usually different or present in different amounts compared to those in the roots, root bark or stem back is different from leaves. Plants develop phytochemicals as defense mechanisms to protect themselves against biotic and abiotic stresses, like temperature, light intensity, herbivory and microbial attack [9].
Also, the concentration of these secondary metabolites is different at different developmental stages [9]. These secondary metabolites are also useful to humans especially in terms of herbal medicines. External factors like rain, wind and sunshine quantitatively affect the plant's metabolic processes through their effects on plant development and growth rates. These factors can also trigger abrupt activation of qualitative changes in secondary metabolite production [27]. Since plants cannot escape from the environmental extremes of light, temperature, and drought, nor move to regions with better nutritional conditions, they have evolved highly complex mechanisms to integrate physiology and metabolism in order to adapt to the conditions to which they are exposed [9]. Some of the environmental conditions that can influence phytochemical composition of plants include: [1] Light which tends to influence the quantity of phytochemicals like terpenoids, alkaloids, flavonoids, flavanols and glycosides among others; [2] Moisture which influences the quantity of phytochemicals like tannins; [3] Temperature which has influence on metabolism of phenolic compounds, isoprene anthocyanins, alkaloids, flavonoids and tannins; and [4] Soil nutrients which tend to influence metabolism of phenolic compounds, gallotannins, condensed tannins, shikonin, cyanogenic compounds and glycosides [9].Screening of different parts of Aspilia pluriseta have revealed that different phytochemicals exist in different parts: Aspilia pluriseta aqueous root bark extract has been reported to contain flavonols, flavones, flavonoids, tannins, and bound anthraquinones and trace amounts of sterols [13]. This difference has been validated by the fact that some of the chemicals which Ngugi et al., [10] found absent in the root bark extract were actually found to be present in the leaves (Tables 1). Different phytochemicals with antidiabetic activity have been reported and that they use different mechanisms to cause this effect [28]. Alkaloids have been shown to contain hypoglycemic effects through several mechanisms. The specific alkaloids that have been proved to contain hypoglycemic effects include; barberine obtained from the stem bark of Barberida aristata and Barberida vulgaris among other barberida species. Barberine acts by inhibiting alpha glucosidase, thereby decreasing glucose transport through the intestinal epithelium, hence reducing the blood glucose levels. Casaurine an alkaloid isolated from the methanol extract of the bark of Syzygium malaccense has also been proved to have hypoglycemic effects. Other alkaloids like catheranthine, vindoline and vindolinine obtained from the leaves of Catheranthus roseus were shown to lower blood glucose levels in both normal and streptozotocin induced diabetic rat models[21]. The alkaloid jamboline present in the seeds of Syzygium cumini was also found to possess antidiabetic properties. Jamboline produces its hypoglycemic effects by preventing the conversion of starch into sugars. It also reduces the quantity of sugar in urine and reduces thirst by reducing urine output. The glycosides of leucopelargonidin isolated from the bark of Ficus bengalensis were also demonstrated to have significant hypoglycemic and serum insulin raising effects in streptozotocin induced diabetic rats[21]..The flavonoids like anthocyanins, catechins, flavanols, and flavanones have been confirmed to have hypoglycemic effects in humans and animal models. These flavonoids have been shown to act by preventing glucose absorption from the gut and its production from the liver. A low dose of cyanidin-3-galactosidase was shown to have a synergistic effect on intestinal α-glucosidase when used in combination with Acarbose an oral hypoglycemic agent used in the treatment of type two DM. Andrographolide, a flavonoid obtained from the leaves of Andrographis paniculata was found to contain significant hypoglycemic effects. In streptozotocin induced diabetic rats, it was observed that andrographolide lowers serum glucose by activating alpha1 and enhances the secretion of beta-endorpin and reduces hepatic gluconeogenesis and increases glucose uptake by the muscles resulting in reduction of serum glucose levels. Polysaccharides found in Ocimum sanctum and Alpinia galangal have also been reported to have hypoglycaemic effects. Polysaccharides act by increasing serum insulin levels and improving glucose tolerance [21].
Dietary fibres have also been proven to play a role in regulating blood glucose levels. This has been shown to be very useful in type one DM [21]. The presence of tannins, reducing sugars, saponins, steroid glycosides, flavonoid derivatives and alkaloids tend to agree with previous studies that have reported such classes of phytochemicals as having antidiabetic activities, although alkaloids were found in trace amounts.From the studies mentioned above, it is clear that Aspilia pluriseta could be getting its antidiabetic effects from any of the phytochemicals including tannins, reducing sugars, saponins, steroid glycosides, flavonoids or combinations of them since synergism cannot be ruled out at this stage. Furthermore, the results of this study are in close agreement with the results from studies carried out on the same plant, and other related plant species like Aspilia Africana [10] although two studies reflect some variation in the distribution of phytochemicals between the root bark and leaves of the Aspilia pluriseta. However, the various studies agree that the plant, Aspilia pluriseta and related species contain phytochemicals with antidiabetic effects.
Oral hypoglycemic study
The present study found that Aspilia pluriseta have a significant hypoglycaemic effect in the STZ-induced diabetes model in rats (Table 4). The results of the study were in agreement with the reported antidiabetic activity of the same plant or related species [10]. For example, the study carried out by Ngugiet al., [10] on Aspilia pluriseta root bark aqueous extract reported an increasing hypoglycaemic effect at increasing doses of the extract [10]. However, the results are not exactly in agreement in that their study used the alloxan-model and their observations were only for acute effects within a fourhour period while this study used the streptozotocin model, which is known to produce a more stable diabetic effect, and also went up to 20 days of observations with repeated doses. This study, therefore, has revealed real antidiabetic effect since a 20-day observation period cannot be compared with a fourday period that just determined acute hypoglycaemic effects. Furthermore, this study also used leaves which have been found to contain some of the phytochemicals, including alkaloids and saponins that were found absent in the root bark extract (Table 1).
Furthermore, the results showed that all the animals treated with the extract of Aspilia pluriseta showed a continued reduction in blood glucose levels with increasing time indicating that the extract has a longer duration of action [10]. However, optimum reduction in their study was observed in those animals which received an extract dose of 150mg/kg, whereas in the present study, the maximum reduction was observed at 500 mg/kg bw.
This study, therefore, has added to the body of knowledge about the antidiabetic effects of Aspilia pluriseta [10]. This is an important finding considering that the communities have been using the plant without scientific validation of its efficacy. Considering that the plant has a relatively good yield of extract, it opens up an avenue for continued use of the plant and possible commercialization if active ingredients could be isolated from the plant, more especially if it is also found to be safe when used chronically. This has a precedent, considering that metformin, a biguanide used as an oral hypoglycaemic agent was actually isolated from a plant, Gelega officinalis [3].
Acute toxicity study
According to the observations in acute toxicity study, the plant has an LD50 above 5000mg/kg bw, which puts it in the safe range. However, since all the animals treated with the extract presented with scratching of the lips, it implied that the plant has got irritant effects. This irritant effect of the extract could also be responsible for diarrhoea, which was observed in the animals at high doses [22]. The irritant effect could be attributed to phytochemicals like coumarins and flavonoids [22].The animals also exhibited piloerection, reduced motor activity, increased urination, sedation, and reduced appetite. The piloerection is an indication that the extract could be having sympathetic effects. The observed reduced motor activity could be a result of central effects although this could also be a peripheral effect [22]. Increased urination is usually an indication of action on the kidney tubules to decrease water reabsorption and hence increase urination. The observed sedation could be an indication that the extract crosses the blood brain burrier and therefore produces CNS sedative effects [8]. Low or no appetite observed could be attributed to central effects of the extract or it could be due to the fact that the extract causes GIT disturbance and irritation [8].Although it was concluded that the aqueous leaf extract of Aspilia pluriseta is relatively safe in the short run, since doses up to 5000mg/kg did not produce any mortality. This cannot be construed to mean that the plant is safe for chronic use. There is a likelihood that the extract could be having long term toxic effects which should be investigated by doing chronic toxicity tests. This is because diabetes mellitus is a chronic condition and the plant is likely to be used chronically in the management of this condition, hence some toxic effects may ensue in the long run. The results from other studies tend to support this view (4, 10, 18). That the plant might not be very safe can be revealed from the report by Njeru and Obonyo [18], which reported that the Aspilia pluriseta root bark extract had cytotoxic effects [18]. Also, Ngugiet al., [10] in a study carried out in Kenya about the in vivo toxicity of Aspilia pluriseta root back aqueous extract in mice, revealed that the spleen of the mice treated with the extract of Aspilia pluriseta displayed moderate lymphoid depopulation, implying toxic effects of the extract on the spleen [10].
According to a study carried out by Taziebou et al., [8], on acute and sub-acute effects of Aspilia africana leaf extract, the medium lethal dose (LD50) was found to be greater in females than male rats [8]. The results from the study by Taziebou et al., [8] showed the median lethal dose value (LD50) of 6000 mg/kg and 7000mg/kg body weight for males and females respectively with an average of 6000 mg/kg body weight. According to Schorderet [16], substances with (LD50) values greater than 5000 mg/kg body weight are classified as substances with low toxicity. Therefore, the aqueous leaf extract of Aspilia africana was considered as a substance with low toxicity according to results of that study [8]. The same study revealed that male animals were more sensitive to toxic effects of Aspilia Africana than female animals, because male animals died at a low dose compared to the females [8].In a histological study to determine the effect of Apilia africana leaf extract on the ovaries of female wistar rats, the ovaries of the control group showed normal histological features while the ovaries of the treated groups showed some cellular hypertrophy of the theca folliculi, and complete distortion [4]. Degenerative and atrophic changes were also observed in the oocyte and zona granulosa of the mice treated with the oral extract of Aspilia africana [4]. This tends to suggest that the results of this study have to be treated with caution although the findings helped to evaluate the unknown phytochemicals found in the leaves of Aspilia pluriseta and to demonstrate antidiabetic effects. Although the local people who use the herb for DM treatment will have the basis for continuing to use the plant, they need to be conscious about the possible chronic toxic effects. Most of the acute toxic effects started appearing 3 hours post dosing. This caution is in line with a finding by other researchers in Western Uganda who found out that the communities that dwell in the Rwenzori region are so much dependent on herbal medication for management of a wide range of diseases. This practice was ongoing despite the availability of modern medications [23].
Conclusion
The aqueous leaf extract of Aspilia pluriseta contains phytochemicals like flavanols, coumarins, flavonoids and glycosides, among other phytochemicals, which may be responsible for antidiabetic effects. The aqueous leaf extract of Aspilia pluriseta has hypoglycemic effects which was evidenced by its ability to lower blood glucose levels in STZ- induced diabetic rats. The aqueous leaf extract of Aspilia pluriseta has an LD50 above 500mg/kbw although it has some acute toxic effects like diarrhea and sedation as was observed in acute toxicity study although its chronic need to be ascertained.
Recommendations
Further studies should be carried out on the same plant to find out the specific phytochemical (s) that is/are responsible for the hypoglycemic effects of the plant. The plant has got various phytochemicals and either a specific phytochemical is responsible for hypoglycemic effects or different phytochemicals work in synergy to produce hypoglycemic effects. Sub-acute and chronic toxicity studies should also be carried out on the same plant to find out the effects that might result from chronic use of the plant. Since the plant produced some acute toxic effects, it could also be having some chronic toxic effects that could not be observed with acute toxicity method.
References
- Chang, C. L. T., Lin, Y., Bartolome, A. P., Chen, Y., Chiu, S., & Yang, W. Herbal Therapies for Type 2 Diabetes Mellitus : Chemistry , Biology , and Potential Application of Selected Plants and Compounds. Evidence-Based Alternative and Complementary medicine. Volume 2013 Article ID 378657 2013. [CrossRef]
- Cicero L. T. Chang,Yenshou Lin, Arlene P. Bartolome,Yi-Ching Chen, Shao-Chih Chiu, and Wen-Chin Yang Herbal Therapies for Type 2 Diabetes Mellitus: Chemistry, Biology, and Potential Application of Selected Plants and Compounds. Evidence-Based Complementary and Alternative Medicine, vol. 2013, Article ID 378657, 33 pages 2013. [CrossRef]
- DiTomaso, J.M., G.B. Kyser et al. Weed Control in Natural Areas in the Western United States. Weed Research and Information Center, University of California. 2013.
- Eweka, A. O. Histological studies of the effects of oral administration of Aspiliaafricana( Asteraceae ) leaf extract on the ovaries of female wistar rats. African Journal of Traditional, Complementary and Alternative Medicines, 6:57–61. 2009. [CrossRef]
- Ghosh M N. Fundamentals of experimental pharmacology.Indian Journal of Pharmacology 3: 36-39 1984.
- International Diabetes Federation. (2015). IDF Diabetes Atlas 2015.
- Jean-Louis Chiasson, NahlaAris-Jilwan, RaphaëlBélanger, Sylvie Bertrand, Hugues Beauregard, Jean-Marie Ékoé, Hélène Fournier, and Jana Havrankova. Diagnosis and treatment of diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Canadian Medical Association Journal 168(7): 859-866 2003.
- LC Taziebou, F-X Etoa, B Nkegoum, CA Pieme, DPD Dzeufiet. Acute and subacute toxicity of Aspilia Africana leaves. African Journal of Traditional, Complementary and Alternative Medicines 4(2) 127-134 2007. [CrossRef]
- Ncube, B J, Finnie, J& Van Staden. Quality from the field: The impact of environmental factors as quality determinants in medicinal plants. South African Journal of Botany, 82(12):6-9 2012. [CrossRef]
- Ngugi M P, Murugi N J, Kibiti M C, Ngeranwa J J, Njue M W, Maina D, Gathumbi K P and Njagi N EHypoglycemic Activity of Some Kenyan Plants Traditionally used to Manage Diabetes Mellitus in Eastern Province. Journal of diabetes and metabolism, 2(8):2-4. 2011.
- Nyanzi R, Wamala R and Atuhaire L K, Diabetes and Quality of Life: A Ugandan Perspective. Makerere University. Kampala Uganda. 2013. [CrossRef]
- OECD (2001). Guidance document on the recognition, assessment and use of clinical signs as humane endpoints for experimental animals used in safety evaluation. Series on Testing and Assessment No 19. ENV/JM/MONO.
- Osadebe, P. O., Odoh, E. U., &Uzor, P. F. Natural Products as Potential Sources of Antidiabetic Drugs. British Journal of Pharmacutical Research, 4(17): 2075–2095. 2014.
- Panawala P B, D.C. Abeysinghe, R.M. Dharmadasa. Phytochemical Distribution and Bioactivity of Different Parts and Leaf Positions of PimentaDioica (L.) Merr (Myrtaceae) World Journal of Agricultural Research., 4(5): 143-146 2016. [CrossRef]
- Quy Diem Do, Artik Elisa, AngkawijayaPhuong ,LanTran-Nguyen, Lien HuongHuynh, FelyciaEdiSoetaredjo and SuryadiIsmadji Yi-HsuJu. Effect of extraction solvent on total phenol content, total flavonoid content, and antioxidant activity of Limnophila aromatic I; Journal of Food and Drug Analysis. 22(3): 296-302 2014. [CrossRef]
- Schorderet, M. Pharmacologie des conce Editions Slatkine Genève, Edition Frison-Roche Paris. Pp33-34. 1992.
- Shrivastava A, Suchita Singh, Sanchita Singh. Phytochemical investigation of different plant parts of Calotropisprocera: International Journal of Scientific and Research Publications,3(8) 1-42018.
- SospeterNgociNjeru, MeshackObonyo. Potency of extracts of selected plant species from Mbeere, Embu County-Kenya against Mycobacterium tuberculosis.Journal of Medicinal Plants Research 10(12):149-157 2016. [CrossRef]
- Spilvallo R, Novero M, Bertea CM, Bossi S, Bonfante P. Truffle volatiles inhibit growth and induce an oxidative burst in Arabidopsis thaliana. New Phytol 175:417–424 2007. [CrossRef]
- Ssegawa, P., &Kasenene, J. M. Medicinal plant diversity and uses in the Sango bay area, Southern Uganda. Journal of Ethnopharmacology,113 (3): 521–540. 2007. [CrossRef]
- Switi B. Gaikwad, G. Krishna Mohan and M. Sandhya Rani. Phytochemicals for Diabetes Management. Pharmaceutical Crops 5(1):11-28 2014.
- Syed Saeed ul Hassan2, ShahidRasool, Muhammad Khalil-ur-Rehman, SaiqaIshtiaq, Shahidul Hassan, Imran Waheed& M. Asif Saeed. Phytochemical Investigation of Irritant Constituents of Cuscutareflexa. International Journal of Agriculture & Biology, 14 (5). 3-5 2014.
- UmbaTolo, C., Kahwa, I., Nuwagira, U. . ., Weisheit, A. ., &Ikiriza, H. Medicinal plants used in treatment of various diseases in the Rwenzori Region, Western Uganda. Ethnobotany Research and Applications, 25, 1–16. 2023.
- American Diabetes Association Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 32(Suppl 1): S62–S67.2009.
- Hatem A. Abuelizz,ElHassaneAnouar,Rohaya Ahmad,Nor Izzati Iwana Nor Azman,Mohamed Marzouk,Rashad Al-Salahi. Triazoloquinazolines as a new class of potent α-glucosidase inhibitors: in vitro evaluation and docking studyPlos One14(8): e0220379.2019. [CrossRef]
- Trease, G.E. and Evans, W.C. (1996) A Textbook of Pharmacology. Baillier Tidally, London.
- Inbathamizh L, Padmini E. Quinic acid as a potent drug candidate for prostate cancer—a comparative pharmacokinetic approach. Asian J Pharm Clin Res. 6(4):106–1122013.
- Firdous S.M. Phytochemicals for treatment of diabetes. EXCLI Journal 13: 451–453. 2014.
Figure 1.
A graph showing the mean blood glucose levels for all the treatment groups.
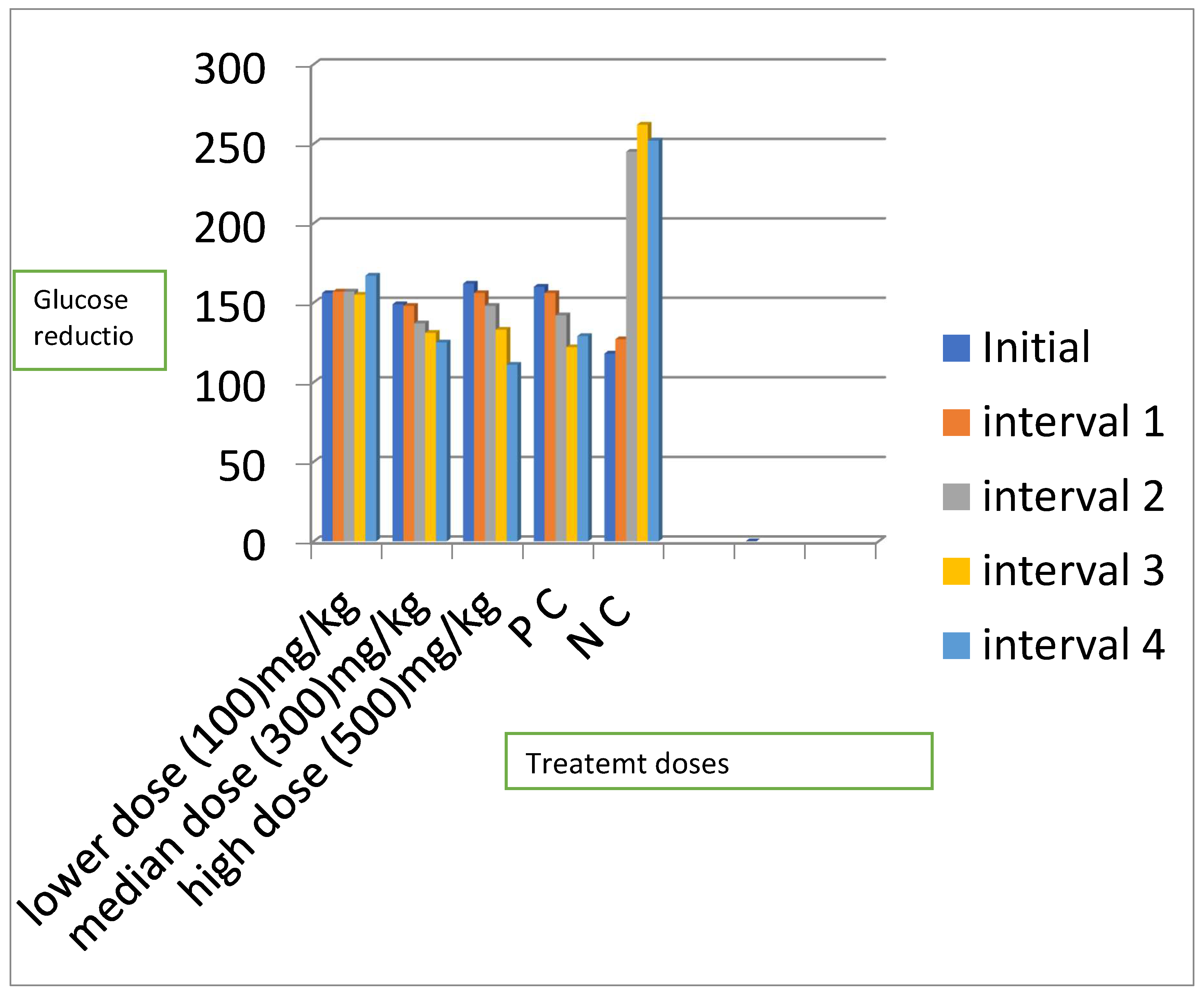
Figure 2.
A graph showing the percentage reduction in the blood glucose levels of the animals for the three significant groups.
Figure 2.
A graph showing the percentage reduction in the blood glucose levels of the animals for the three significant groups.
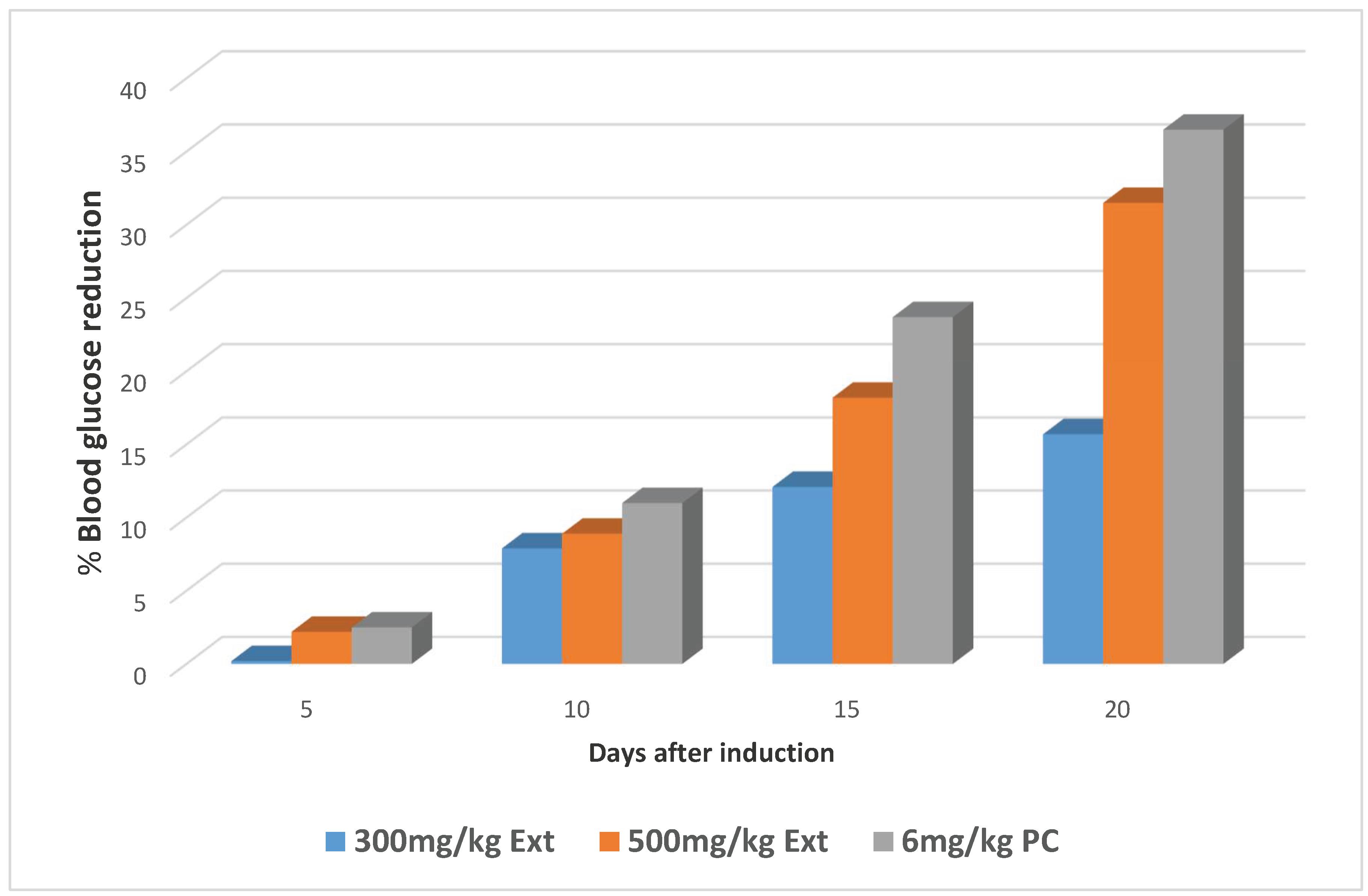

Table 1.
Results for phytochemical analysis.
| Phytochemicals | Observations | Conclusion |
| Tannins | ++ | Garlic tannins present |
| Reducing sugars | ++ | Reducing sugars present |
| Anthracenocides | ++ | Anthracenocides present |
| Coumarins | ++ | Coumarins present |
| Saponins | ++ | Saponins present |
| Steroid glycosides | ++ | Steroids present |
| Flavonosides | ++ | Flavanones present |
| Anthocyanins | + | Anthocyanins present |
| Alkaloids | + | Alkaloids present |
| Starch | + | Starch present |
| Phenols | + | Phenols present |
| Amino acids | - | Amino acids absent |
| Anthraquinones | - | Anthraquinones absent |
Key: ++ Present in large quantities; + Present in trace amounts; - Absent.
Table 2.
Results of one way analysis of variance and the Tukey’s post hoc tests for changes in blood glucose levels.
Table 2.
Results of one way analysis of variance and the Tukey’s post hoc tests for changes in blood glucose levels.
| Treatment | Fasting Blood Glucose Level, Mean ± SEM (mg/dl) | ||||
| Initial | 5th day | 10th day | 15th day | 20th day | |
| Ext;100mg | 155.7±11.28 | 157.0±11.68 (-0.8) | 157.2±10.73 (-1.0)a | 154.7±8.81 (0.6)c | 167.0±11.50 (-7.2)a |
| Ext;300mg | 148.5±16.04 | 148.2±15.46 (0.2) | 136.7±10.23(7.9)a | 130.5±11.50 (12.1)b | 125.2±2.32 (15.7)a |
| Ext;500mg | 162.2±8.86 | 158.7±9.25 (2.2) | 147.7±7.23 (8.9)a | 132.7±7.86 (18.2)b | 111.2±3.94 (31.5)a |
| PC | 159.5±3.50 | 155.5±3.57 (2.5) | 142.0±2.86 (11.0)a | 121.7±4.27 (23.7)b | 101.7±5.12 (36.2)a |
| NC | 118.0±15.77 | 127.0±213.34(7.6) | 245.0±18.60 (-107.6) | 262.2±44.85 (-122.2) | 251.5±22.50 (-11.3) |
| P value | 0.115 | 0.309 | 0.001 | 0.002 | 0.001 |
N=4,abc significant; a p< 0.001, b p value <0.01 and c p value = 0.021; PC (Positive Control)NC (Negative Control); percentage blood glucose reduction ().
Table 3.
Showing the observations for acute toxicity tests.
| Group | Number of animals | Dose (mg/kg) | Observations |
| Phase one | |||
| Group one | 3 | 10 | Scratching of the lips |
| Group two | 3 | 100 | Scratching of the lips |
| Group three | 3 | 1000 | Scratching of the lips |
| Phase two | |||
| Group one | 1 | 1600 | Increased breathing rate, Piloerection, Reduced movement |
| Group two | 1 | 2900 | Increased urination, Reduced movement Piloerection, No desire for food & water, Increased breathing rate |
| Group three | 1 | 5000 | Increased urination, Sedation, Increased breathing rate, No movement, Piloerection, No desire for food & water |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



