
Submitted:
23 July 2025
Posted:
23 July 2025
You are already at the latest version
Abstract
Background: In light of the concerning increase in burnout among healthcare professionals, it is essential to identify the specific factors that contribute to this phenomenon and that can be addressed. This review examines the relationship between burnout and emotional intelligence (EI) among healthcare professionals, alongside additional factors that may influence both concepts. Methods: A comprehensive search of OVID, PubMed, Medline, Scopus, and Web of Science databases was conducted for peer-reviewed articles published in English between 2000 and 2024. Inclusion criteria required studies to investigate both burnout and EI in healthcare professionals. 31 eligible peer-reviewed studies were included in the final analysis. Results: The findings suggest a consistent inverse correlation between EI and burnout across various healthcare professionals, including doctors, nurses, and residents. Higher EI was associated with reduced levels of emotional exhaustion and depersonalization, and a greater sense of personal accomplishment. Burnout was found to be prevalent among younger healthcare workers, particularly residents, with contributing factors including exposure to workplace violence, high workload, and diminished psychological ownership. Oppositely, protective influences on emotional intelligence included spiritual intelligence, self-control, income, and healthy habits, such as sufficient sleep and physical activity. Conclusions: Higher EI appears to be inversely associated to burnout among healthcare professionals. Given that both burnout and EI are affected by adjustable individual and organizational elements, specific interventions aimed at enhancing EI and improving workplace conditions may provide effective techniques to boost clinician well-being and performance.
Keywords:
burnout
; emotional intelligence
; healthcare professionals
; occupational well-being
1. Introduction
In recent years, the prevalence of burnout syndrome among healthcare workers has sharply increased, being estimated to be double as the one reported in general population [1]. According to recent literature, half of the investigated doctors technically meet the criteria for burnout [2], even if they do not complain or act as professionally impaired.
Maslach and Leiter consider burnout as a „breakdown in the relationship of people and their work” [3], which occurs as a psychological syndrome response to the exposure to chronic personal and interpersonal stressors associated with job. It includes three dimensions:
- emotional exhaustion (EE), perceived by the individual as an emotional depletion, as if „their reserves are consumed” [1];
- depersonalization (DP), characterized by a subjective feeling of detachment and even diminished empathy [4];
- decreased sense of personal accomplishment (PA), which can distort one’s self-evaluation of their work and leads them to feel less competent than they actually are [5].
The consequences of burnout can influence both the physical and mental health, and they might vary from muscle tension, sleep disorders, anxiety, cognitive disfunction, social disconnection, or depression [6]. As a whole, burnout and its outcomes can surpass the professional level and significantly decrease the overall functionality and well-being. Sometimes, burnout evolution can go as far as to contribute to the development of a serious condition, making it rather an extensive problem, than a syndrome in itself. Moreover, burnout can be self-perpetuated, by inadequate coping strategies and reluctance in seeking support from others, possibly accentuating the stigma around seeking help [7,8].
On the long term, all these effects can influence not only health professionals, but also their patients and families. Possible mechanisms involved include, for example, the higher risk of taking careless decisions, poor communication and an overall decline of their professional performance [9].
Since burnout has such an impact over a great array of domains in the individual’s life and because it can have such a great toll on how one’s work is perceived and influenced, it becomes increasingly important to identify the variables contributing to its occurrence. They include individual and organizational factors. Specific individual factors comprise the presence of certain individual traits, such as high neuroticism and low resilience, alexithymia, and perfectionism [10,11], alongside maladaptive coping mechanisms, such as avoidance, denial, substance use, and lack of emotional regulation [7]. A distinct category of individual factors is represented by demographic variables (e.g., age and gender), with lower age and female gender being correlated with a higher predisposition to burnout, an effect which could be due to lower resilience [12].
When it comes to the organizational factors predisposing to burnout, a meta-analysis conducted by Bria et al. [13] concluded that perceived stress, high workload and the imbalance between personal and professional life were the most frequently identified contributors. In addition, the level of work experience, core organizational values and perceived recognition of work were also identified as key environmental variables in the development of burnout [14,15,16].
In regard to protective factors, a meta-analysis conducted by de Mendonça et al. [17] indicated that higher emotional intelligence (EI) mitigates burnout risk, with similar effects brought by mindfulness and stress-management strategies, time-management skills and self-care practices [18,19]. Organizational factors preventing or delaying burnout include work-life balance, meaningful work, a positive workplace culture and good-quality relationships with colleagues and superiors [20,21]. Among the abovementioned factors, EI plays a distinctive role, as it has not only a protective role against burnout, but also a significant positive effect on overall well-being and on the wise use of stress-management skills [22]. Accordingly, EI is a concept which has triggered a lot of debate and has been studied consistently in relationship to the individual capacities to adapt and succeed in social environments [23].
EI reflects one’s capacity to understand, express and regulate their own or others’ emotions [24]. Literature data point out that individuals who are able to experience emotions with clarity, and who can process these emotions, are more efficient at applying mood-regulation strategies. These skills transcend the individual use and can be extrapolated when it comes to interpersonal relationships [25]. When the management of emotions is put into action, the interacting experience becomes a more empathetic one [26]. According to the model structured by Goleman [27], EI is associated to five major personality traits:
- self-awareness: represents an individual’s ability to recognise their own emotions, as well as the impact of those emotions over other people;
- self-management (or self-regulation): assumes the recognition of negative emotions, as well as controlling and forwarding them towards a more productive purpose;
- inner motivation: represents the tendency to be driven by values and passion, not just by external reward;
- social awareness: includes the ability to manage and guide the relationship with others;
The consistent study of EI in current literature and the rise in the popularity of the concept itself is challenged by a number of difficulties:
- -
- -
- diversity when it comes to cultural and contextual differences regarding work ethic, work-life balance, or the approach of expressing feelings in certain regions. In the context of obtaining most of the data used by self-administered questionnaires, the cultural stigma or reveal bias may be an important contributor to the accuracy of data. The individualistic vs. collectivist models can also shape the way not only work is perceived, but also how individuals tend to seek or receive support and guidance [30].
Regarding challenges in understanding how exactly does EI influence burnout, the exact mechanism is still unclear. According to Glenn [31], EI could improve coping strategies and emotional regulation, enhance the use of social support, and even influence stress-response, but the precise underlying mechanisms are yet unknown. Furthermore, the multitude of individual psychological factors associated to EI and their interdependence increases the difficulty of pinpointing a specific pattern.
When focusing on healthcare workers, better EI skills should result in better communication and increased empathy towards the patients and their families, therefore, a better therapeutic relationship [32]. However, when it comes to applying the same skills on oneself, it is debatable if having better developed emotional skills is efficient in delaying or even preventing the effects of chronic occupational stress.
This study aims to investigate the relationship between EI and burnout in healthcare workers following three research questions (RQ):
RQ 1: What is the burnout prevalence among healthcare workers and which are the main contributing factors to burnout?
RQ 2: Does EI play a role in protecting against burnout?
RQ 3: Which additional factors influence EI in healthcare workers?
2. Materials and Methods
OVID, PubMed, Medline, Scopus and Web of Science databases were searched for English language literature published between 2000–2024, and focused on the topics of EI and burnout in healthcare workers. In order to enhance accuracy of findings, we limited the search to peer-reviewed articles. The search terms were “emotional intelligence” AND (“burnout” OR “the burnout syndrome”) IN (“healthcare workers” OR “healthcare professionals” OR “doctors” OR “nurses” OR “physician” OR “residents”).
Inclusion criteria were studies in English, focused on healthcare professionals, and which investigated the correlation between EI and burnout.
Exclusion criteria were represented by studies focused on students or personnel who did not work in a hospital, veterinarian doctors, centered only on a limited number of burnout components (such as emotional exhaustion or depersonalization), or which did not corelate EI to burnout.
The first search yielded 360 hits, which resulted in 233 articles after removing duplicates. Their titles and abstracts were screened for adequacy, defined as addressing both burnout and EI in healthcare workers. After the analysis of content, a number of 31 articles were finally selected (Figure 1).
Given the diversity of study designs, respondents and assessment tools that were used, the narrative review format was the one selected to comprehensively map the evidence on the relationship between healthcare workers’ EI and burnout.
3. Results
3.1. General Findings
All 31 articles presented in Table 1 measured EI, burnout and the correlation between them. Sample sizes varied from 28 to 12,704 respondents, covering a large cultural background and demographical diversity. Eleven articles were specifically focused on resident doctors, eight articles on nurses, and five on doctors. Seven articles studied healthcare workers with different professions combined (doctors, nurses, interns, physical therapists, and other caregivers). The comparative high number of studies centered on residents illustrate their depiction in current literature as one of the most predisposed categories to burnout.
All identified articles were published within the last 15 years, which could also indicate an increasing interest for the study of EI potential benefits, on one side, and the increasing burnout prevalence in healthcare workers, on another side.
Across all identified articles, burnout syndrome was consistently understood as an occupational phenomenon, resulting from the prolonged exposure to work-related stress, while EI was seen as the ability to recognize, understand, manage and even change individual emotions, or the emotions of others.
When it comes to measuring burnout levels, most of the identified studies (22) opted for using The Maslach Burnout Inventory (MBI) or one of its available variants: Maslach Burnout Inventory – General Survey (MBI-GS) or Maslach Burnout Inventory – Human Services Survey (MBI-HSS). Other questionnaires used for evaluating burnout were The Brief Burnout Questionnaire (CBB), The Tedium Index, The Questionnaire for the Assessment of Occupational Burnout Syndrome (CESQT), The Link Burnout Questionnaire (LBQ), The Oldenburg Burnout inventory (OBLI), and the Shirom-Melamed Burnout Measure (SMBM). This diversity reflects in part the various different conceptualizations of the burnout syndrome, which resulted in a multitude of measurement instruments, which overlap to some extent [33].
Regarding the scales used to measure EI, the majority of the identified studies (13) used The Trait Emotional Intelligence Questionnaire (TEIQ), or its short form, TEIQ-SF, followed by the use of The Emotional Intelligence Scale (EIS). The other instruments used to determine the levels of EI were The Schutte Self-Report Emotional Intelligence Test (SSEIT), The Brief Inventory of Emotional Intelligence for Adults (EQ-i-20M), The Trait Meta-Mood Scale 24 (TTMS-24), The Swinburne University Emotional Intelligence Test, The Nurses Job Emotions Scale (NJES), The Emotional Quotient Test, The Emotional Intelligence Questionnaire of Cyber or sharing-EI, The Scale of Emotional Functioning: Health Service Provider, and The Wong and Law Emotional Intelligence Scale (WLEIS). According to a review conducted by Bru-Luna et al. [34], there has been an increase in the number of instruments used to measure EI, with over 40 scaled available at the time being. This reflects both the increasing interest in the concept and its utility, but also the difficulty of constructing objective criteria to measure EI.
3.2. RQ1: What Is the Burnout Prevalence Among Healthcare Professionals and Which Are the Main Contributing Factors to Burnout?
Despite using a wide variety of instruments and identifying a large range of burnout prevalence, most of the studies - with only two exceptions [36,39] - concluded that burnout represents a substantial problem for healthcare workers. In each of the identified studies, medical personal was at risk of developing burnout, and even presented symptoms in some cases (Table 1). For instance, in the study conducted by Lindeman et al. [37], 51 % of the evaluated resident doctors met criteria for high burnout and only 9% had low levels or no burnout. In the study with the largest sample size [56], 12,704 clinical nurses from 32 general hospitals across China were investigated using the MBI-GS scale and resulting in moderate scores of EE (15.87, SD 6.02), moderate scores of DP (10.80, SD 5.09), and significant scores of decreased PA (25.53, SD 8.65). Overall, they were assessed as displaying moderate to high burnout, with a tendency to experience psychiatric comorbidities, under the form of anxiety and depression.
Since 16 of the identified articles used the Maslach Burnout Inventory, we analyzed their comparative results. Across them, EE ranged from 3.41 to 31.24 (a score of less than 18 means low EE, and over 27 signifies high levels of EE). DP levels varied from 2.2 to 11.9 (scores lower than 5 meaning low levels of DP, and above 10- higher levels of DP). PA ranged from 2.84 to 38.13 (levels under 33 mean high levels of PA, and levels over 40 mean low PA).
Several studies identified additional factors involved in burnout development. By categories, they were depicted as:
a) demographic factors (age and gender);
b) psychological variables (e.g., psychological ownership and agreeableness);
c) physiological factors (e.g., coenzyme Q10 - CoQ10 levels);
d) environmental variables (exposure to violence, positive work experience, workload, type of work contract, dissatisfaction with career choices).
a) Demographic factors
When it comes to gender influence in burnout, several studies [37,43,60] pointed out that higher burnout levels were corelate to female gender.
Regarding age and work experience, Lindeman et al. [37] reported higher risk of burnout with increased age, whereas other studies [40,42,53] found a negative correlation between age and experience and burnout levels. Sharaf et al. [64] also pointed out that the risk for burnout increased sharply at the beginning of residency training.
b) Psychological variables
According to Kaur et al. [36], psychological ownership (PO) amongst medical personnel creates a sense of responsibility, which influences behavior and was found to have a negative relation to burnout. The concept of PO represents a state in which an individual feels as though the target of ownership - whether it is a job or an organization - is theirs, therefore, one’s possessions are felt as extensions of the self. PO can mitigate the effects of burnout, by making the employees experience greater autonomy over their work, fostering more meaning into their efforts, and by making the entire distressing experience feel more meaningful [66].
Additionally, Lindeman et al. [37] pointed out that the personal trait of agreeableness was inversely corelated with burnout. The trait of agreeableness refers to a person’s tendency to be considerate towards others, polite, and compassionate.
c) Physiological factors
The study conducted by Kasemy et al. [42] found a correlation between the functioning of the immune system, expressed in the individual CoQ10 levels, and burnout: higher burnout levels seem to deplete the body’s CoQ10 reserves, therefore making the protective mechanisms weaker. CoQ10 is a vitamin-like compound, with roles in energy production and antioxidant protection.
d) Environmental variables
Ünal [39] identified marital status as a factor contributing to burnout protection, with married individuals reporting lower burnout levels.
Cao et al. [35] identified exposure to violence as a strong burnout predictor, with up to 98% of respondents experiencing verbal violence in the last year, and the personnel exposed to violence displaying higher levels of burnout.
In the study conducted by Lindeman et al. [37], positive work experience showed a strong inverse correlation with individual burnout. The magnitude of the relationship for positive work experience was larger than the one for negative work experience, proving that an overall positive work experience might have a protective role against burnout in surgical residents. Resident doctors examined by Gleason et al. [47] were more prone to burnout, if their work environment was aversive and if they were subjects to disruptive behaviors, especially when others took credit for their work or exposed them to public humiliation. Dissatisfaction with their career choice, the low income and the marginal role in the operating room were also factors contributing to resident doctors’ burnout, according to Kirkpatrick et al. [62].
3.3. RQ 2: Does Emotional Intelligence Play a Role in Protecting Against Burnout?
With the exception of the study conducted by Năstasă & Fărcaş [43], all the other papers included in this review identified EI as an important contributor in the protection against burnout (Table 1). In what concerns the particular article mentioned above, despite not identifying a significant correlation between EI and burnout levels in the examined population, it still points out a relationship between EI and personal accomplishment in healthcare workers, which in turn lead to the authors’ conclusion about the need to develop EI in this work category.
As a confirmatory finding, higher EI in the categories of healthcare professionals were negatively associated with burnout by the studies included in this review (Table 1), except for the abovementioned one. Among the studies that employed the most used assessment instrument for burnout MBI and the three-dimensions model (EE, DP and PA), all of them, except the one mentioned before, found that high levels of EI were inversely correlated with all burnout dimensions.
3.4. RQ 3: Which Additional Factors Influence EI in Healthcare Workers?
A part of the researched studies [35,36,37,64] identified several additional factors significantly related to EI (age and experience, gender, spiritual intelligence and PO, perceived stress levels, income, exercise levels and sleep hours).
From a longitudinal perspective, PO, spiritual intelligence and low perceived stress not only were correlated to EI, but also had a significant association to burnout.
When it comes to age and experience influence in EI levels, Lindeman et al. [37] found that EI global scores decreased significantly with increasing age, while Tiwari & Bhagat [53] found a significant positive correlation between EI and age.
In terms of gender, many studies were inconclusive about which gender is more EI privileged, although the association of gender to EI seemed significant. Cao et al. [35] reported higher EI in women, while, oppositely, Almeneessier et al. [41] found higher EI in men.
Ünal and Molero Jurado et al. [38,39] did not find any correlation of EI to gender or age, and explained this finding through other cultural differences than feminine stereotypes, potentially obscuring the role of gender.
The study conducted by Tiwari & Bhagat [53] found a positive correlation between EI and income, which could be explained by the EI skills potentially playing a key role in successful careers, especially if they have a higher social exposure.
Sharaf et al. [64] identified an association between EI and healthy daily habits (sleep and exercise). Specifically, they found that the average number of sleeping hours was correlated with the total EI score, and that one extra hour of sleeping a night is associated with a 0.44-unit increase in the average EI score (using the TEIQue-SF). The same study showed that exercise determined an EI 0.52-unit increase in residents who exercised, compared to those who did not exercise.
4. Discussion
The primary goals of this review were (a) to assess the prevalence of burnout in healthcare professionals and to highlight the contributing factors to burnout; (b) to identify if EI provides protection against burnout, and (c) to expose additional variables contributing to EI and which could potentially be subjects to change.
4.1. Burnout Prevalence and Variability
In terms of burnout prevalence in healthcare professionals, this has been a consistently reported issue, which has additionally grown in interest since the COVID-19 pandemic [67]. In the studies we identified, burnout rates were not always explicitly stated, since most of them focused on the correlations between burnout and predictive variables. However, those who reported burnout prevalence displayed great variability, from low burnout (2.15 on the MBI scale) [36], to high or even alarming burnout, with up to 70 % from the maximum values [35]. This great variability can be explained by the heterogeneity of the used instruments and protocols, the substantial array of geographical and cultural backgrounds covered by the included studies, and the use of self-reported questionnaires, which may have induced bias by itself, via the underreporting or overreporting of emotional distress and burnout symptoms.
Amongst the articles who used the MBI, high global burnout scores were mostly associated with high EE, DP, or both. According to Maslach & Leiter [68], EE is considered to be the closest parameter to a conventional stress variable, making it more reliable in predicting burnout-related symptoms.
All the identified articles were published in the last 15 years, illustrating an obvious increase of interest in the topic. A number of factors could explain this, such as the official recognition of burnout as an “occupational phenomenon” by The World Health Organization [69]. The COVID-19 pandemic may have also played an important role, not just in the increased demands that the medical system had to face, but also in the way that work-life balance has been perceived since [67].
Furthermore, the exposure of mental health issues has recently grown, while the stigma around talking about one’s struggles has steadily decreased. As more and more people come forward, testifying about their professional and personal struggles, the need to identify their root causes and to address them as early as possible has become imperative [70].
Regarding the gender influence in burnout, the identified studies stated that women were more prone to burnout development. According to a review conducted by Purvanova & Muros [71], these differences stem most probably from higher reporting of burnout by women, specifically when it comes to the EE component. As stated before, in literature the EE component tends to be considered the most representative for burnout, while in the same time it is typically easily identified by women [72]. Self-reporting bias associated with cultural stereotypes surrounding masculine traits could be also involved, with men being less likely to report exhaustion, in order to not be perceived as either weak or unprofessional [73]. To avoid this bias and make future studies more reliable, it could be helpful to use qualitative methods and cross-cultural validation of psychometric instruments assessing burnout and, specifically, EE. Using terminology that is not gender-specific or culture-specific could also assist in reduce the existent research biases.
When it comes to age and work experience, several identified studies [40,42,53,63] found that the lack of experience associated with young age and the beginning of residency was correlated with higher burnout, while, oppositely, Lindeman et al. [37] pointed out that there is a tendency of burnout increasing with age. The first result was supported by a meta-analysis by Brewer & Shapard [74], which concluded that higher burnout levels have been corelated with lower age and less job experience, and by a separate study conducted by Gómez-Urquiza et al. [75], who found that younger age was a significant risk factor for the EE and DP component of burnout, and less influential regarding PA. The sharp increase in prevalence of burnout at the beginning of residency could be explained by the multitude of changes in a young professional’s life, such as gaining responsibility, changes in schedule and workload, all while not yet having the experience to effectively cope with these new challenges. Therefore, it is reasonable to presume that interventions applied at this point in the medical career, targeting resident support and mentorship, are important for addressing this problem and preventing its aggravation.
Factors found as having a protective role against burnout were two-folded: individual (PO, agreeableness and CoQ10 levels), but also environmental (marital status, exposure to violence, workload, positive work experiences, and dissatisfaction with career choices). Part of these factors (such as workload, PO, exposure to violence) are circumstantial, so they can be targeted by personalized interventions. A good example is PO, with strategies increasing it leading to higher autonomy, especially by being given decision-making power, promoting hands-on contributions, the use of group symbols, and non-monetary recognition, such as public acknowledgement [76]. These outcomes could not only contribute to more cohesive work environment and increased personal well-being, but could also improve PA scores [77].
Agreeable healthcare professionals tend to reframe patient interaction as rather meaningful than draining, they tend to develop better workplace relationships, and even have lower rates of conflict, due to their prosocial behavior [78]. According to Roberts et al. [79], the idea of personality plasticity implies that certain traits, such as agreeableness could improve with consistent practice, by employing multiple strategies, such as social skills training, reinforcement of the prosocial behavior, perspective taking, and even cognitive intervention techniques. Increasing agreeableness could not only have an impact on individual burnout, but could also have a substantial effect on the therapeutic relationship and perceived quality of care [80].
The decrease of CoQ10 levels as a consequence of exhaustion could be effectively target by using nutritional supplements, according to Tsai et al. [81]. The use of CoQ10-only formulations proved to be more effective than CoQ10 compounds, and the longer duration of the treatment had a positive correlation to fatigue reduction. CoQ10 supplementation could thereby represent an additional tool, alongside psychological interventions, in the comprehensive targeting of burnout.
Marital status was identified as playing a protective role against burnout development. These findings are consistent with a meta-analysis conducted by Cañadas-De la Fuente et al. [82], reporting individuals with single or divorced marital statuses as being exposed to higher burnout. In contrast, married individuals would benefit from protection against burnout through an array of mechanisms, from which social support plays a key role.
Regarding work-associated environmental factors, exposure to violence was linked to increased burnout, this being supported by other literature data [83,84]. Adding violence prevention to larger organizational plans for employee well-being, like mental health assistance, systematic debriefing after events, and encouraging a culture of self-reporting, can make employees more resilient and less likely to burnout. Weng et al. [58] found that the EI development could be useful in preventing burnout, not only directly, but also mediated by less exposure to violence. Individual trainings in EI development, self-defense and de-escalating techniques, alongside with changes in logistics and workplace design (such as an increase in safety strategies and increased security) could be effectively employed to address or prevent burnout [85,86].
In terms of work stability, healthcare workers with temporary contracts are exposed to a higher risk of burnout, because of higher perceived insecurity, but also as a result of often higher workload or fewer paid hours. Personal resources, such as resilience and EI, could act as compensating factors in such work conditions. Their positive role is reported also at those employees who have a stable job, but feel like caught in a trap, with more administrative tasks, less meaningful work time, and without any exit options [87].
Since both workload and dissatisfaction with career choices were found to increase burnout, while positive work experience might have a protective role, organizational interventions could prove to be of critical importance. Alongside the beforementioned mentorship programs for residents, an early target component could be vocational assistance, in order to help with early career dissatisfaction.
4.2. Protective Role of EI
In terms of the correlation between burnout and EI, our selected studies identified an inverse relationship, which was identified in existing literature not only for EI as a whole, but also for its distinct subcomponents (well-being, self-control, emotionality and sociability) [88]. Specifically, Mitra et al. [59] pointed out that burnout had a significant negative correlation with EI’s well-being component and a positive correlation with self-control and sociability. Among distinct EI components, self-control seems to have an important role, as it is connected to adaptability in changing environments, but also with personal values and personal accomplishments [89]. The study conducted by Jahanazeb et al. [60] claims that self-control has a direct inverse relationship to burnout, with higher self-control ensuring a better control of emotional reactions to stressors, which in turn lowers the risk of burnout. Encouraging self-control (via therapies like mindfulness training, cognitive-behavioral methods, and programs that boost emotional intelligence) could be not only a valuable strategy to prevent or delay burnout, but also to impede mental illness resulting from the failure of emotional self-regulation mechanisms. The inclusion of such programs seems to have substantial benefits among healthcare students and residents [37,41,90,91].
4.3. Factors Influencing EI
The gender-related influences regarding EI levels in the identified articles showed either higher EI in women, in men or did not find any correlation of EI to gender or age. This is explained, just as in the case of the relationship gender-burnout, as being possibly influenced by cultural differences, particularly by feminine stereotypes, potentially obscuring the role of gender. In current literature, many studies were inconclusive about which gender is more EI-privileged, although the association of gender to EI seemed significant. Some studies in current literature [92,93] reported higher EI in women, while, oppositely, Almeneessier et al. [41] found higher EI in men. The higher number of articles reporting EI as more prevalent in women could result from the dimensions of EI tightly related to “feminine” stereotypes (such as emotional attention, emotional regulation, emotional clarity), therefore potentially creating a self-reporting bias [94]. In order to address this taxonomy-induced misinterpretation, future studies could use gender-neutral language in the self-reported questionnaires.
Regarding the connection between age and EI, the identified articles found inconsistent associations, with some of them [37,53] stating that either higher or lower age were related to higher EI, while others [38,39] claimed that age plays no role. The study conducted by Cabello et al. [92] found that EI levels varied with age according to a U-inverted curve, with younger and older adults scoring lower than middle-aged adults. Another study conducted by Fariselli et al. [95] concluded that several components of EI increase with age, whereas others do not, further raising the issue of the selection of the EI components potentially developing through training. These findings emphasize the importance of future research focused on specific EI domains and their development in relation with other variables.
The studies included in this review identified a positive correlation between high EI and higher income. This could be important at least from two perspectives: firstly, the choice of EI developing strategies could be influenced by the existent outcome, thereby limiting the access of low-income individuals to all kind of programs of EI development. Secondly, EI could predict income itself, making its development a path to better societal rewards. This hypothesis is backed up by the results of a recent meta-analysis by Sanchez-Gomez et al. [96], who found that, after taking all the other variables into consideration, participants who displayed higher levels of EI and emotional-repair capacities, had higher salaries, making EI one of the relevant variables when talking about building professional success.
The included papers suggested a positive relationship between sleep, exercise, and EI. This is consistent with the results of Killgore et al. [97], who found that sleep duration and habitual sleep quality are both independently associated with self-perceived dispositional aspects of EI. These benefits are further supported by the study of Sepdanius et al. [98], who also found a positive correlation between sleep quality and EI. Acebes-Sánchez et al. [99] found a gender-specific positive effect of physical activity, associated to higher emotional clarity and emotional repair in men, and higher emotional attention in women. These findings could be the subject of a series of a chain-related individual interventions. Therefore, by tackling the development of healthy habits such as the ones described, not only the individual could improve EI levels, but ultimately, indirectly prevent burnout.
5. Limitations
This study has several limitations. It was run as a narrative review, so some relevant articles may have been excluded. Other limitations were derived from the heterogeneity of scales used for evaluating burnout and EI, the self-reporting method, and the heterogeneity of the cultural backgrounds of respondents. Although the general focus was on health professionals, these studies included medical personnel from different categories and specialties as participants, each of them having particular burnout and EI characteristics.
6. Conclusions
The current paper had the main goal to analyze the connection between burnout and EI in healthcare professionals. During this research, it became increasingly obvious that the burnout syndrome has evolved, to become a significant concern of employees in the healthcare sector. In this context, the identified protective role of EI is important, because it suggests EI as both a target and a reliable instrument against professional exhaustion. Among the determinants of EI, many could be the subject of individual and organizational interventions. Although the current study was not specifically focused on evaluating the comparative efficacy of direct vs. indirect (e.g., EI-enhancing) burnout-reducing strategies, this topic is very attractive for future research, considering its potential for building cost-effective systems of psychological support for healthcare professionals.
Supplementary Materials
not applicable.
Author Contributions
Conceptualization, I.R.S.B. and O.P.-V.; Methodology, I.R.S.B., A.I.M., and O.P.-V.; Software, L.V.D. and A.I.M.; Validation, I.R.S.B., L.V.D., A.M.C., and O.P.-V.; Formal analysis, A.I.M. and S.V.S.; Investigation, I.R.S.B., L.V.D. and A.I.M.; Resources, L.V.D., A.I.M., and O.P.-V.; Data curation, S.V.S. and O.P.-V.; Writing—original draft preparation, I.R.S.B. and A.M.C.; Writing—review and editing, L.V.D., A.I.M., S.V.S. and O.P.-V.; Visualization, A.I.M., A.M.C., and O.P.-V.; Supervision, I.R.S.B, L.V.D., A.M.C., and O.P.-V.; Project administration, S.V.S. and O.P.-V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data supporting the findings and interpretations are available in the cited peer-reviewed articles included in the reference list. No new datasets were generated or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| EI | Emotional Intelligence |
| EE | Emotional Exhaustion |
| DP | Depersonalization |
| PA | Personal Accomplishment |
| PO | Psychological Ownership |
References
- Grow, H.M.; McPhillips, H.A.; Batra, M. Understanding physician burnout. Current Problems in Pediatric and Adolescent Health Care 2019, 49, 100656. [Google Scholar] [CrossRef]
- Shalaby, R.; Oluwasina, F.; Eboreime, E.; El Gindi, H.; Agyapong, B.; Hrabok, M.; Agyapong, V.I.O. Burnout among residents: Prevalence and predictors of depersonalization, emotional exhaustion and professional unfulfillment among resident doctors in Canada. International Journal of Environmental Research and Public Health 2023, 20, 3677. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Leiter, M.P. New insights into burnout and health care: Strategies for improving civility and alleviating burnout. Medical Teacher 2017, 39, 160–163. [Google Scholar] [CrossRef]
- Kumar, S. Preventing and Managing Burnout: What have we learned. Biomedical Journal 2018, 2, 45–51. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory. Scarecrow Education 1997. [Google Scholar]
- Tavella, G.; Hadzi-Pavlovic, D.; Parker, G. Burnout: Redefining its key symptoms. Psychiatry Research 2021, 302, 114023. [Google Scholar] [CrossRef]
- Bittner, J.G.; Khan, Z.; Babu, M.; Hamed, O. Stress, burnout, and maladaptive coping. Bulletin of the American College of Surgeons 2011, 96, 17–22. [Google Scholar]
- Canu, I.G.; Marca, S.C.; Dell’Oro, F.; Balázs, Á.; Bergamaschi, E.; Besse, C.; Wahlen, A. Harmonized definition of occupational burnout: A systematic review, semantic analysis, and Delphi consensus in 29 countries. Scandinavian Journal of Work, Environment & Health 2021, 47, 95–107. [Google Scholar] [CrossRef]
- Kumar, S. Burnout and doctors: Prevalence, prevention and intervention. Healthcare 2016, 4, 37. [Google Scholar] [CrossRef]
- Popa-Velea, O.; Diaconescu, L.V.; Gheorghe, I.R.; Olariu, O.; Panaitiu, I.; Cerniţanu, M.; Spinei, L. Factors associated with burnout in medical academia: An exploratory analysis of Romanian and Moldavian physicians. International Journal of Environmental Research and Public Health 2019, 16, 2382. [Google Scholar] [CrossRef]
- Genly, B. Safety and job burnout: Understanding complex contributing factors. Professional Safety 2016, 61, 45–49. [Google Scholar]
- McKinley, N.; Karayiannis, P. N.; Convie, L.; Clarke, M.; Kirk, S. J.; Campbell, W.J. Resilience in medical doctors: a systematic review. Postgraduate medical journal, 95. [CrossRef]
- Bria, M.; Băban, A.; Dumitraşcu, D.L. Systematic review of burnout risk factors among European healthcare professionals. Cognition, Brain, Behavior: An Interdisciplinary Journal 2012, 16, 423–452. [Google Scholar]
- Renger, D.; Miché, M.; Casini, A. Professional Recognition at Work: The Protective Role of Esteem, Respect, and Care for Burnout Among Employees. Journal of Occupational and Environmental Medicine 2020, 62, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Dahiya, R.; Raghuvanshi, J. Do values reflect what is important? Exploring the nexus between work values, work engagement and job burnout, International Journal of Organizational Analysis 2023, 31, 1414-1434. [CrossRef]
- Liao, T.; Liu, Y.; Luo, W.; Duan, Z.; Zhan, K.; Lu, H.; Chen, X. Non-linear association of years of experience and burnout among nursing staff: a restricted cubic spline analysis. Frontiers in Public Health, 1343; 12. [Google Scholar] [CrossRef]
- de Mendonça, N.R.F.; de Santana, A.N.; Bueno, J.M.H. The relationship between burnout and emotional intelligence: A meta-analysis. Revista Psicologia: Organizações e Trabalho 2023, 23, 2471–2478. [Google Scholar] [CrossRef]
- Klein, A.; Taieb, O.; Xavier, S.; Baubet, T.; Reyre, A. The benefits of mindfulness-based interventions on burnout among health professionals: A systematic review. Explore 2020, 16, 35–43. [Google Scholar] [CrossRef]
- Hricová, M. The mediating role of self-care activities in the stress-burnout relationship. Health Psychology Report 2020, 8, 1–9. [Google Scholar] [CrossRef]
- Koh, M.Y.H.; Khoo, H.S.; Gallardo, M.D.; Hum, A. How leaders, teams and organisations can prevent burnout and build resilience: A thematic analysis. BMJ Supportive & Palliative Care 2020, 14, e827–e836. [Google Scholar] [CrossRef]
- Tan, K.-L.; Yeap, P.F. The impact of work engagement and meaningful work to alleviate job burnout among social workers in New Zealand”, Management Decision, 2022, 60, 3042-3065. [CrossRef]
- Ciarrochi, J.; Deane, F.P.; Anderson, S. Emotional intelligence moderates the relationship between stress and mental health. Personality and Individual Differences 2002, 32, 197–209. [Google Scholar] [CrossRef]
- Ebrahimi, M.R.; Khoshsima, H.; Zare-Behtash, E. The impacts of enhancing emotional intelligence on the development of reading skill. International Journal of Instruction 2018, 11, 573–586. [Google Scholar] [CrossRef]
- Kanesan, P.; Fauzan, N. Models of emotional intelligence: A review. e-BANGI Journal 2019, 16, 1–12. [Google Scholar]
- Mayer, J.D.; Gaschke, Y.N. The experience and meta-experience of mood. Journal of Personality and Social Psychology 1988, 55, 102–111. [Google Scholar] [CrossRef]
- Mayer, J.D.; Salovey, P.; Gomberg-Kaufman, S.; Blainey, K. A broader conception of mood experience. Journal of Personality and Social Psychology 1991, 60, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Goleman, D. Emotional Intelligence: Why It Can Matter More Than IQ. N: Bantam Books, 1995. [Google Scholar]
- Goleman, D. Emotional intelligence: Issues in paradigm building. The Emotionally Intelligent Workplace 2001, 13, 26–44. [Google Scholar]
- Angelini, G. Big five model personality traits and job burnout: A systematic literature review. BMC Psychology 2023, 11, 49. [Google Scholar] [CrossRef]
- Listopad, I.W.; Michaelsen, M.M.; Werdecker, L.; Esch, T. Bio-psycho-socio-spirito-cultural factors of burnout: A systematic narrative review of the literature. Frontiers in Psychology 2021, 12, 722862. [Google Scholar] [CrossRef] [PubMed]
- Glenn, M. Preventing Burnout: Controlling Emotions, the Right Way. Master’s thesis, Lamar University-Beaumont.
- Kadadi, S.; Bharamanaikar, S.R. Role of emotional intelligence in healthcare industry. Drishtikon: A Management Journal 2020, 11, 1–37. [Google Scholar]
- Edú-Valsania, S.; Laguía, A.; Moriano, J.A. Burnout: A review of theory and measurement. International Journal of Environmental Research and Public Health 2022, 19, 1780. [Google Scholar] [CrossRef]
- Bru-Luna, L.M.; Martí-Vilar, M.; Merino-Soto, C.; Cervera-Santiago, J.L. Emotional intelligence measures: A systematic review. Healthcare 2021, 9, 1696. [Google Scholar] [CrossRef]
- Cao, Y.; Gao, L.; Fan, L.; Jiao, M.; Li, Y.; Ma, Y. The influence of emotional intelligence on job burnout of healthcare workers and mediating role of workplace violence: A cross-sectional study. Frontiers in Public Health 2022, 10, 892421. [Google Scholar] [CrossRef]
- Kaur, D.; Sambasivan, M.; Kumar, N. Effect of spiritual intelligence, emotional intelligence, psychological ownership and burnout on caring behaviour of nurses: A cross-sectional study. Journal of Clinical Nursing 2013, 22, 3192–3202. [Google Scholar] [CrossRef]
- Lindeman, B.; Petrusa, E.; McKinley, S.; Hashimoto, D.A.; Gee, D.; Smink, D.S.; Phitayakorn, R. Association of burnout with emotional intelligence and personality in surgical residents: Can we predict who is most at risk? Journal of Surgical Education 2017, 74, e22–e30. [Google Scholar] [CrossRef]
- Cofer, K.D.; Hollis, R.H.; Goss, L.; Morris, M.S.; Porterfield, J.R.; Chu, D.I. Burnout is associated with emotional intelligence but not traditional job performance measurements in surgical residents. Journal of Surgical Education 2018, 75, 1171–1179. [Google Scholar] [CrossRef]
- Ünal, Z. The contribution of emotional intelligence on the components of burnout: The case of health care sector professionals. Electronic Journal of Business Ethics and Organization Studies 2014, 19, 1–9. [Google Scholar]
- Molero Jurado, M.D.M.; Pérez-Fuentes, M.D.C.; Gázquez Linares, J.J.; Simón Márquez, M.D.M.; Martos Martínez, Á. Burnout risk and protection factors in certified nursing aides. International Journal of Environmental Research and Public Health 2018, 15, 1116. [Google Scholar] [CrossRef]
- Almeneessier, A.S.; Azer, S.A. Exploring the relationship between burnout and emotional intelligence among academics and clinicians at King Saud University. BMC Medical Education 2023, 23, 673. [Google Scholar] [CrossRef]
- Kasemy, Z.A.; Sharif, A.F.; Bahgat, N.M.; Abdelsattar, S.; Latif, A.A.A. Emotional intelligence, workplace conflict and job burn-out among critical care physicians: A mediation analysis with a cross-sectional study design in Egypt. BMJ Open 2023, 13, e074645. [Google Scholar] [CrossRef]
- Năstasă, L.E.; Fărcaş, A.D. The effect of emotional intelligence on burnout in healthcare professionals. Procedia-Social and Behavioral Sciences 2015, 187, 78–82. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.D.C.; Molero Jurado, M.D.M.; Martos Martínez, Á.; Gázquez Linares, J.J. Analysis of the risk and protective roles of work-related and individual variables in burnout syndrome in nurses. Sustainability 2019, 11, 5745. [Google Scholar] [CrossRef]
- Satterfield, J.; Swenson, S.; Rabow, M. Emotional intelligence in internal medicine residents: Educational implications for clinical performance and burnout. Annals of Behavioral Science and Medical Education 2009, 14, 65–71. [Google Scholar]
- Soto-Rubio, A.; Giménez-Espert, M.D.C.; Prado-Gascó, V. Effect of emotional intelligence and psychosocial risks on burnout, job satisfaction, and nurses’ health during the COVID-19 pandemic. International Journal of Environmental Research and Public Health 2020, 17, 7998. [Google Scholar] [CrossRef]
- Gleason, F.; Baker, S.J.; Wood, T.; Wood, L.; Hollis, R.H.; Chu, D.I.; Lindeman, B. Emotional intelligence and burnout in surgical residents: A 5-year study. Journal of Surgical Education 2020, 77, e63–e70. [Google Scholar] [CrossRef]
- Kaul, I.; Reddy, K.J. Relationship of Emotional Intelligence and Burnout among MBBS Doctors of Himachal Pradesh. Indian Journal of Psychological Science 2022, 15, 45–56. [Google Scholar]
- Vlachou, E.M.; Damigos, D.; Lyrakos, G.; Chanopoulos, K.; Kosmidis, G.; Karavis, M. The relationship between burnout syndrome and emotional intelligence in healthcare professionals. Health Science Journal 2016, 10, 1–12. [Google Scholar]
- Arnone, R.; Cascio, M.I.; Parenti, I. The role of Emotional Intelligence in health care professionals burnout. European Journal of Public Health 2019, 29, 186–553. [Google Scholar] [CrossRef]
- Görgens-Ekermans, G.; Brand, T. Emotional intelligence as a moderator in the stress-burnout relationship: A questionnaire study on nurses. Journal of Clinical Nursing 2012, 21, 2275–2285. [Google Scholar] [CrossRef]
- Szczygiel, D.D.; Mikolajczak, M. Emotional intelligence buffers the effects of negative emotions on job burnout in nursing. Frontiers in Psychology 2018, 9, 2649. [Google Scholar] [CrossRef]
- Tiwari, S.; Bhagat, D. The role of emotional intelligence on health care professionals occupational stress and burnout. International Journal of Current Research and Review 2020, 12, 187–196. [Google Scholar] [CrossRef]
- Samaei, S.E.; Khosravi, Y.; Heravizadeh, O.; Ahangar, H.G.; Pourshariati, F.; Amrollahi, M. The effect of emotional intelligence and job stress on burnout: A structural equation model among hospital nurses. International Journal of Occupational Hygiene 2017, 9, 52–59. [Google Scholar]
- Beierle, S.P.; Kirkpatrick, B.A.; Heidel, R.E.; Russ, A.; Ramshaw, B.; McCallum, R.S.; Lewis, J.M. Evaluating and exploring variations in surgical resident emotional intelligence and burnout. Journal of Surgical Education 2019, 76, 628–636. [Google Scholar] [CrossRef]
- Yu, C.; Liu, Z.; Zhao, M.; Liu, Y.; Zhang, Y.; Lin, A.; Wan, H. The mediating role of emotion management, self-efficacy and emotional intelligence in clinical nurses related to negative psychology and burnout. Psychology Research and Behavior Management 2023, 16, 3333–3345. [Google Scholar] [CrossRef]
- Swami, M.K.; Mathur, D.M.; Pushp, B.K. Emotional intelligence, perceived stress and burnout among resident doctors: An assessment of the relationship. The National Medical Journal of India 2013, 26, 210–213. [Google Scholar]
- Weng, H.C.; Hung, C.M.; Liu, Y.T.; Cheng, Y.J.; Yen, C.Y.; Chang, C.C.; Huang, C.K. Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction. Medical Education 2011, 45, 835–842. [Google Scholar] [CrossRef]
- Mitra, S.; Sarkar, A.P.; Haldar, D.; Saren, A.B.; Lo, S.; Sarkar, G.N. Correlation among perceived stress, emotional intelligence, and burnout of resident doctors in a medical college of West Bengal: A mediation analysis. Indian Journal of Public Health 2018, 62, 27–31. [Google Scholar] [CrossRef]
- Jahanzeb, Z.; Parveen, S.; Khizar, U. Self-control as mediator between emotional intelligence and burnout among doctors. Journal of Positive School Psychology 2023, 7, 388–400. [Google Scholar]
- Bin Dahmash, A.; Alhadlaq, A.S.; Alhujayri, A.K.; Alkholaiwi, F. , Alosaimi, N.A. (2019). Emotional Intelligence and Burnout in Plastic Surgery Residents: Is There a Relationship? Plastic and Reconstructive Surgery. Global Open 2019, 7, e2057. [Google Scholar] [CrossRef]
- Kirkpatrick, H.; Wasfie, T.; Laykova, A.; Barber, K.; Hella, J.; Vogel, M. Emotional intelligence, burnout, and wellbeing among residents as a result of the COVID-19 pandemic. The American Surgeon 2022, 88, 1856–1860. [Google Scholar] [CrossRef]
- Wasfie, T.; Kirkpatrick, H.; Barber, K.; Hella, J.R.; Anderson, T.; Vogel, M. Burnout and well-being of medical and surgical residents in relation to emotional intelligence: A 3-year study. Surgery 2024, 175, 856–861. [Google Scholar] [CrossRef]
- Sharaf, A.M.; Abdulla, I.H.; Alnatheer, A.M.; Alahmari, A.N.; Alwhibi, O.A.; Alabduljabbar, Z.; Alkholaiwi, F.M. Emotional intelligence and burnout among otorhinolaryngology-head and neck surgery residents. Frontiers in Public Health 2022, 10, 851408. [Google Scholar] [CrossRef]
- Wasfie, T.; Kirkpatrick, H.; Barber, K.; Hella, J.R.; Anderson, T.; Vogel, M. Longitudinal study of emotional intelligence, well-being, and burnout of surgical and medical residents. The American Surgeon 2023, 89, 3077–3083. [Google Scholar] [CrossRef]
- Dawkins, S.; Tian, A.W.; Newman, A.; Martin, A. Psychological ownership: A review and research agenda. Journal of Organizational Behavior 2017, 38, 163–183. [Google Scholar] [CrossRef]
- Reshetnikov, A.; Abaeva, O.; Prisyazhnaya, N.; Romanova, T.; Romanov, S.; Sobolev, K.; Manukyan, A. The Impact of the COVID-19 Pandemic on Burnout Levels among Healthcare Workers: A Comparative Analysis of the Pandemic Period and Post-Pandemic Period. Heliyon. [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Burn-out an “Occupational Phenomenon”: International Classification of Diseases. WHO. 2019. Available online: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases (accessed on 01.07.2025).
- Goldberg, D.G.; Soylu, T.; Hoffman, C.F.; Kishton, R.E.; Cronholm, P.F. “Anxiety, COVID, Burnout and Now Depression”: A Qualitative Study of Primary Care Clinicians’ Perceptions of Burnout. J. Gen. Intern. Med. 2024, 39(8), 1317–1323. [Google Scholar] [CrossRef]
- Purvanova, R.K.; Muros, J.P. Gender differences in burnout: A meta-analysis. Journal of Vocational Behavior 2010, 77, 168–185. [Google Scholar] [CrossRef]
- Mahalik, J.R.; Di Bianca, M. Help-Seeking for Depression as a Stigmatized Threat to Masculinity. Prof. Psychol. Res. Pr. 2021, 52, (2), 146. [Google Scholar] [CrossRef]
- Wong, Y.J.; Ho, M.-H.R.; Wang, S.-Y.; Miller, I.S.K. Meta-Analyses of the Relationship between Conformity to Masculine Norms and Mental Health-Related Outcomes. Journal of Counselling Psychology 2017, 64(1), 80–93. [Google Scholar] [CrossRef] [PubMed]
- Brewer, E.W.; Shapard, L. Employee burnout: A meta-analysis of the relationship between age or years of experience. Human Resource Development Review 2004, 3, 102–123. [Google Scholar] [CrossRef]
- Gómez-Urquiza, J.L.; Vargas, C.; De la Fuente, E.I.; Fernández-Castillo, R.; Cañadas-De la Fuente, G.A. Age as a risk factor for burnout syndrome in nursing professionals: A meta-analytic study. Research in Nursing & Health 2017, 40, 99–110. [Google Scholar] [CrossRef]
- van Zyl, L.; van der Vaart, L.; Stemmet, L. Positive Psychological Interventions Aimed at Enhancing Psychological Ownership. In Theoretical Orientations and Practical Applications of Psychological Ownership. In Theoretical Orientations and Practical Applications of Psychological Ownership; Publisher: Place, Country, 2017; pp. 119–134. [Google Scholar]
- O’Connor, K.; Muller Neff, D.; Pitman, S. Burnout in mental health professionals: A systematic review and meta-analysis of prevalence and determinants. European psychiatry: the journal of the Association of European Psychiatrists, 2018, 53, 74–99. [Google Scholar] [CrossRef]
- Alarcon, G.; Eschleman, K.J.; Bowling, N.A. Relationships between personality variables and burnout: A meta-analysis. Work & Stress 2009, 23, 244–263. [Google Scholar] [CrossRef]
- Roberts, B.W.; Luo, J.; Briley, D.A.; Chow, P.I.; Su, R.; Hill, P.L. A Systematic Review of Personality Trait Change Through Intervention. Psychol. Bull. 2017, 143(2), 117–141. [Google Scholar] [CrossRef]
- Teng, C.-I.; Hsu, W.-H. The Impact of Health Service Provider Agreeableness on Care Quality Variation. Serv. Sci. 2012, 4(4), 295–307. [Google Scholar] [CrossRef]
- Tsai, I.C.; Hsu, C.W.; Chang, C.H.; Tseng, P.T.; Chang, K.V. Effectiveness of Coenzyme Q10 Supplementation for Reducing Fatigue: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Frontiers in Pharmacology, 2022, 13, 883251. [Google Scholar] [CrossRef] [PubMed]
- Cañadas-De la Fuente, G.A.; Ortega, E.; Ramirez-Baena, L.; De la Fuente-Solana, E.I.; Vargas, C.; Gómez-Urquiza, J.L. Gender, marital status, and children as risk factors for burnout in nurses: A meta-analytic study. International Journal of Environmental Research and Public Health 2018, 15, 2102. [Google Scholar] [CrossRef] [PubMed]
- Isaksson, U.; Graneheim, U.H.; Richter, J.; Eisemann, M.; Åström, S. Exposure to violence in relation to personality traits, coping abilities, and burnout among caregivers in nursing homes: A case-control study. Scandinavian Journal of Caring Sciences 2008, 22, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Converso, D.; Sottimano, I.; Balducci, C. Violence exposure and burnout in healthcare sector: Mediating role of work ability. La Medicina del Lavoro 2021, 112, 58–73. [Google Scholar] [CrossRef]
- Somani, R.; Muntaner, C.; Hillan, E.; Velonis, A.J.; Smith, P. A Systematic Review: Effectiveness of Interventions to De-escalate Workplace Violence against Nurses in Healthcare Settings. Saf. Health Work 2021, 12, 289–295. [Google Scholar] [CrossRef]
- Phillips, J.P. Workplace Violence against Health Care Workers in the United States. N. Engl. J. Med. 2016, 374, 1661–1669. [Google Scholar] [CrossRef]
- Molino, M.; Cortese, C.G.; Ghislieri, C. The Promotion of Technology Acceptance and Work Engagement in Industry 4.0: From Personal Resources to Information and Training. Int. J. Environ. Res. Public Health 2020, 17, 2438. [Google Scholar] [CrossRef]
- Siegling, A.B.; Vesely, A.K.; Petrides, K.V.; Saklofske, D.H. Incremental validity of the trait emotional intelligence questionnaire-short form (TEIQue-SF). Journal of Personality Assessment 2015, 97, 525–535. [Google Scholar] [CrossRef]
- de Ridder, D.T.; Lensvelt-Mulders, G.; Finkenauer, C.; Stok, F.M.; Baumeister, R.F. Taking stock of self-control: a meta-analysis of how trait self-control relates to a wide range of behaviors. Pers Soc Psychol Rev. 2012, 16, 76–99. [Google Scholar] [CrossRef]
- Mattingly, V.; Kraiger, K. Can emotional intelligence be trained? A meta-analytical investigation. Human Resource Management Review, 2019, 29, 140–155. [Google Scholar] [CrossRef]
- Taylor, M.J.; Andreatta, R.; Woltenberg, L.; Cormier, M.; Hoch, J.M. The relationship of emotional intelligence to burnout and related factors in healthcare profession students, Nurse Education Today, 2024, 143, 106387. [CrossRef]
- Cabello, R.; Sorrel, M.A.; Fernández-Pinto, I.; Extremera, N.; Fernández-Berrocal, P. Age and gender differences in ability emotional intelligence in adults: A cross-sectional study. Developmental Psychology 2016, 52, 1486–1492. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, S.K.; Shipley, N.; Jackson, M.; Segrest, S.; Sharma, D.; Chapman, B.P.; Hayslip, B. Emotional intelligence: A comparative study on age and gender differences. International Journal of Basic and Applied Research 2018, 8, 670–681. [Google Scholar]
- Lopez-Zafra, E.; Gartzia, L. Perceptions of gender differences in self-report measures of emotional intelligence. Sex Roles 2014, 70, 479–495. [Google Scholar] [CrossRef]
- Fariselli, L.; Ghini, M.; Freeman, J. (2008). Age and emotional intelligence: white paper. http://www.6seconds.org/sei/media/WP_EQ_and_Age.pdf (Accessed at th, 2025). 8 April.
- Sanchez-Gomez, M.; Breso, E.; Giorgi, G. Could Emotional Intelligence Ability Predict Salary? A Cross-Sectional Study in a Multioccupational Sample. Int. J. Environ. Res. Public Health 2021, 18, 1322. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Vanuk, J.R.; Persich, M.R.; Cloonan, S.A.; Grandner, M.A.; Dailey, N.S. Sleep quality and duration are associated with greater trait emotional intelligence. Sleep Health 2022, 8, 230–233. [Google Scholar] [CrossRef]
- Sepdanius, E.; Harefa, S.K.; Indika, P.M.; Effendi, H.; Rifki, M.S.; Afriani, R. Relationship between physical activity, stress and sleep quality and emotional intelligence. International Journal of Human Movement and Sports Sciences 2023, 11, 224–232. [Google Scholar] [CrossRef]
- Acebes-Sánchez, J.; Diez-Vega, I.; Esteban-Gonzalo, S.; Rodríguez-Romo, G. Physical Activity and Emotional Intelligence among Undergraduate Students: A Correlational Study. BMC Public Health 2019, 19, 1241. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of included articles.
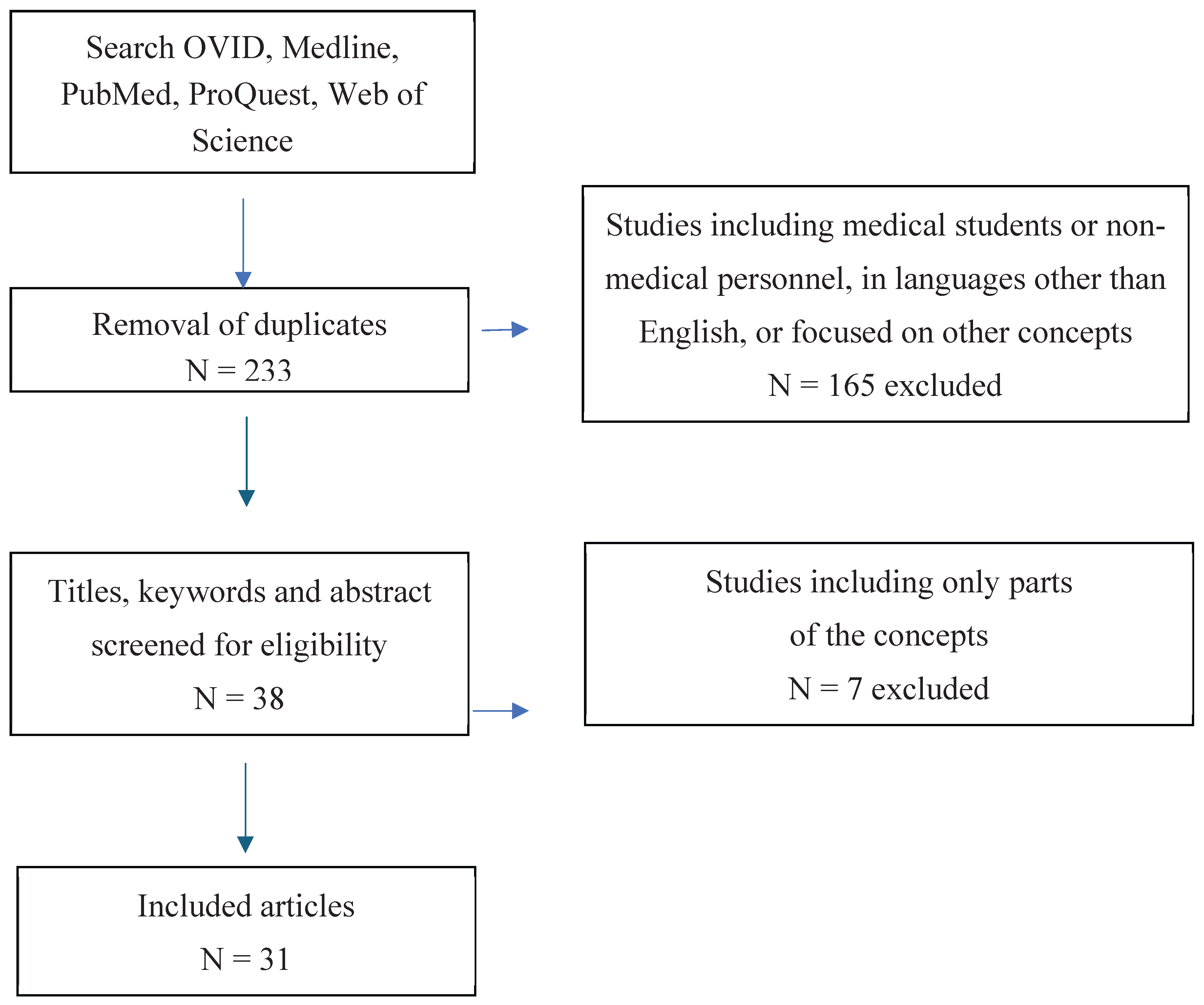

Table 1.
Selected studies’ summary of correlations between EI, burnout and additional factors.
| No. | Study title | Authors, position in Reference list | Year | Country | Study design | Sample size | Type of personnel | Instruments used for measuring Burnout | Instruments used for measuring EI | Correlations between Burnout and EI | Factors contributing to Burnout | Modulating factors for EI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | The Influence of Emotional Intelligence on Job Burnout of Healthcare Workers and Mediating Role of Workplace Violence: A Cross-Sectional Study | Cao, Y., Gao, L., Fan, L., Jiao, M., Li, Y., & Ma, Y. [35] | 2022 | China | Cross-sectional | 2061 | Physician, nurses, and medical technicians | MBI-GS | EIS | EI was significantly negatively associated with all three dimensions of job burnout | Exposure to violence is corelated with higher burnout | Female gender significantly corelated with higher EI |
| 2 | Effect of spiritual intelligence, emotional intelligence, psychological ownership and burnout on caring behaviour of nurses: a cross-sectional study | Kaur, D., Sambasivan, M., Kumar, N. [36] | 2013 | Malaysia | Cross-sectional | 550 | Nurses | MBI-HSS | SSEIT | Nurses with higher levels of EI suffer lesser levels of burnout | Psychological ownership corelates with lower levels of burnout | Spiritual intelligence influences EI |
| 3 | Association of Burnout With Emotional Intelligence and Personality in Surgical Residents: Can We Predict Who Is Most at Risk? | Lindeman, B., Petrusa, E., McKinley, S., Hashimoto, D. A., Gee, D., Smink, D. S., ... & Phitayakorn, R. [37] | 2017 | United States | Longitudinal cohort | 143 | Resident doctors | MBI | TEIQ-SF | Burnout scores were significantly inversely correlated with all 4 facets of EI and EI total | Female sex and older age are associated with higher burnout levels Agreeableness and positive work experiences was inversely corelated with burnout | EI global scores decrease significantly with age |
| 4 | Burnout is Associated With Emotional Intelligence but not Traditional Job Performance Measurements in Surgical Residents | Cofer, K. D., Hollis, R. H., Goss, L., Morris, M. S., Porterfield, J. R., Chu, D. I. [38] | 2018 | United States | Cross-sectional | 40 | Resident doctors | MBI-HSS | TEIQ-SF | The mean EI scores were lower in residents with burnout versus residents without burnout | ||
| 5 | The Contribution of Emotional Intelligence on the Components of Burnout: The Case of Health Care Sector Professionals | Ünal, Z [39] | 2014 | Turkey | Cross-sectional | 136 | Trainees, interns, nurses and doctors | MBI | EIS | EI has a positive contribution on PA whereas negative contribution on EE and DP | Married individuals report lower levels of burnout | |
| 6 | Burnout Risk and Protection Factors in Certified Nursing Aides | Molero Jurado, M. D. M., Pérez-Fuentes, M. D.C., Gázquez Linares, J.J.G., Simón Márquez, M. D.M., Martos Martínez, Á. [40] | 2018 | Spain | Cross-sectional | 278 | Nurses | CBB | EQ-i-20M | Burnout Syndrome score is significantly related negatively with all the EI factors | Lower age is linked to a higher burnout risk, the group of professionals with a permanent contract showed a significantly higher mean score in burnout | |
| 7 | Exploring the relationship between burnout and emotional intelligence among academics and clinicians at King Saud University | Almeneessier, A.S., Azer, S. A. [41] | 2023 | Saudi Arabia | Cross-sectional | 126 | Medical academics, doctors | MBI-HSS | TEIQ-SF | There is an inverse interrelation was reported between burnout and EI | Workplace risk factors for burnout: workload, job control, lack of a supportive environment, recognition and rewards, equitability, and organizational values | In contrast with other studies, we reported EI and its elements higher in men than in women, which can be explained based on cultural differences |
| 8 | Emotional intelligence, workplace conflict and job burn-out among critical care physicians: a mediation analysis with a cross-sectional study design in Egypt | Kasemy, Z. A., Sharif, A. F., Bahgat, N.M., Abdelsattar, S., Latif, A.A. A. [42] | 2023 | Egypt | Cross-sectional | 144 | Doctors | MBI | TEIQ | EI could significantly predict job burn-out across various dimensions, and it showed EI showed a negative association with EE, depersonalisation, and reduced personal achievement. | Age and years of experience, conflict management skills and CoQ10 levels have a negative correlation with burnout Exposure to violence and inadequate resources and facilities had a positive correlation with burnout levels | Conflict management and CoQ10 levels exhibited positive correlations with EI |
| 9 | The Effect of Emotional Intelligence on Burnout in Healthcare Professionals | Năstasă, L. E., Fărcaş, A. D. [43] | 2015 | Romania | Cross-sectional | 120 | Doctors and nurses | MBI | EIS | The level of burnout experienced by the medical personnel did not correlate with the level of EI development. | The burnout syndrome is felt more acutely by women | |
| 10 | Analysis of the Risk and Protective Roles of Work-Related and Individual Variables in Burnout Syndrome in Nurses | Pérez-Fuentes, M. D.C., Molero Jurado, M. D.M., Martos Martínez, Á., Gázquez Linares, J. J. [44] | 2019 | Spain | Cross-sectional | 1236 | Nurses | CBB | EQ-I-M20 | There was a negative association between burnout and various factors of EI | Spending more time with colleagues and patients and reporting good-quality relationships exhibit a negative relationship with burnout Nurses with permanent contracts had a higher mean score for burnout than those on temporary contracts | |
| 11 | Emotional Intelligence in Internal Medicine Residents: Educational Implications for Clinical Performance and Burnout | Satterfield, J., Swenson, S., Rabow, M. [45] | 2010 | United States | Cross-sectional | 28 | Resident doctors | The Tedium Index | EIS | EI scores increased over the course of an academic year and higher year-end scores correlated with less burnout and higher overall clinical performance and interviewing ratings. | ||
| 12 | Effect of Emotional Intelligence and Psychosocial Risks on Burnout, Job Satisfaction, and Nurses’ Health during the COVID-19 Pandemic | Soto-Rubio, A., Giménez-Espert, M.D.C., Prado-Gascó, V. [46] | 2020 | Spain | Cross-sectional | 125 | Nurses | CESQT | TMMS-24 | The emotional repair component stands out as an element of EI that should be enhanced to prevent the possible adverse effects of psychosocial risks on nurses, specifically those related to burnout, psychosomatic complaints, and job satisfaction. | ||
| 13 | Emotional Intelligence and Burnout in Surgical Residents: A 5-Year Study | Gleason, F., Baker, S.J., Wood, T., Wood, L., Hollis, R.H., Chu, D.I., Lindeman, B. [47] | 2020 | United States | Longitu-dinal cohort | 236 | Resident doctors | MBI | TEIQ-SF | Burnout scores showed significant inverse correlation with the 4 domains of EI, total job resources score, and all 4 sub-domains of job resources. | Individuals who were subjected to disruptive behaviors (particularly others taking credit for work and public humiliation) were more likely to experience higher burnout levels Each additional PGY year demonstrated an incremental increase in burnout | |
| 14 | Relationship of Emotional Intelligence and Burnout among MBBS Doctors of Himachal Pradesh | Kaul, I., Reddy, K.J. [48] | 2022 | India | Cross-sectional | 190 | Doctors | MBI | SSEIT | A highly negative correlation is found between EI, EE and DP, and a positive correlation between EI and PA | ||
| 15 | The Relationship between Burnout Syndrome and Emotional Intelligence in Healthcare Professionals | Vlachou, E. M., Damigos, D., Lyrakos, G., Chanopoulos, K., Kosmidis, G., Karavis, M. [49] | 2016 | Greece | Cross-sectional | 148 | Doctors, nurses, physical therapists | MBI | TEIQ-SF | There is a positive relationship between EI and Burnout syndrome as EI acts protectively against Burnout syndrome and even reduces it | ||
| 16 | The role of Emotional Intelligence in health care professionals burnout | Arnone, R., Cascio, M.I., Parenti, I. [50] | 2019 | Italy | Cross-sectional | 148 | Doctors, nurses, and other caregivers | LBQ | SSEIT | There is a negative and significant correlation between Burnout and EI | ||
| 17 | Emotional intelligence as a moderator in the stress–burnout relationship: a questionnaire study on nurses | Görgens-Ekermans, G., Brand, T. [51] | 2012 | South Africa | Cross-sectional | 122 | Nurses | MBI | The Swinburne University Emotional Intelligence Test | Consistent inverse relationships between emotional control and management as dimensions of EI, and stress and burnout emerged. A differential effect of high vs. low EI on the stress–burnout relationship was evident. | Workload and the work/family interface emerged as significant predictors of burnout | |
| 18 | Emotional Intelligence Buffers the Effects of Negative Emotions on Job Burnout in Nursing | Szczygiel, D. D., Mikolajczak, M. [52] | 2018 | Poland | Cross-sectional | 188 | Nurses | OLBI | NJES | Negative emotions do not always lead to burnout, but that they particularly do for nurses who lack EI. | ||
| 19 | The Role of Emotional Intelligence on Health Care Professionals Occupational Stress and Burnout | Tiwari, S., Bhagat, D. [53] | 2020 | India | Cross-sectional | 388 | Nurses and Doctors | OLBI | Emotional Quotient Test | The dimensions of EI, emotional sensitivity, emotional maturity, and emotional competency have been reported to significantly predict the all the seven dimensions of occupational stress and the dimensions of burnout and the order and strength of the predictors differ across the two groups of healthcare professionals. | A positive relationship was found between age, working experience, and stress, with younger healthcare professionals and those with a shorter length of service experiencing more stress | EI levels increased with the age and experience of the respondents on emotional intelligence |
| 20 | The Effect of Emotional Intelligence and Job Stress on Burnout: A Structural Equation Model among Hospital Nurses | Samaei, S.E., Khosravi, Y., Heravizadeh, O., Ahangar, H. G., Pourshariati, F., Amrollahi, M. [54] | 2017 | Iran | Cross-sectional | 300 | Nurses | MBI-HSS | The Emotional Intelligence Questionnaire of Cyber or sharing-EI | There was meaningful relationship between EI and job stress with nurses’ occupational burnout. The EI was effective on job stress | A significant difference was found in correlation with income- the higher the income with increasing EI levels | |
| 21 | Evaluating and Exploring Variations in Surgical Resident Emotional Intelligence and Burnout | Beierle, S.P., Kirkpatrick, B.A., Heidel, R.E., Russ, A., Ramshaw, B., McCallum, R.S., Lewis, J.M. [55] | 2019 | United States | Longitu-dinal cohort | 86 | Resident doctors | MBI | Scale of Emotional Functioning: Health Service Provider | The data confirm an inverse relationship between EI and burnout | ||
| 22 | The Mediating Role of Emotion Management, Self-Efficacy and Emotional Intelligence in Clinical Nurses Related to Negative Psychology and Burnout | Yu, C., Liu, Z., Zhao, M., Liu, Y., Zhang, Y., Lin, A., ... & Wan, H. [56] | 2023 | China | Cross-sectional | 12704 | Nurses | MBI-GS | ETS | EI among nurses could reduce the incidence of burnout | ||
| 23 | Emotional intelligence, perceived stress and burnout among resident doctors: An assessment of the relationship | Swami, M. K., Mathur, D.M., Pushp, B.K. [57] | 2013 | India | Cross-sectional | 56 | Resident doctors | SMBM | TEIQ | There is a significant negative correlation between burnout and trait EI and a positive correlation with perceived stress indicating that burnout is probably influenced by perception of stress and EI. | ||
| 24 | Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction | Weng, H.C., Hung, C.M., Liu, Y.T., Cheng, Y.J., Yen, C.Y., Chang, C.C., Huang, C.K. [58] | 2011 | Taiwan | Observa-tional | 110 | Doctors | MBI | WLEIS | Higher EI was significantly associated with less burnout and higher job satisfaction. In addition, less burnout was not only associated with higher levels of patient satisfaction, but also with higher levels of job satisfaction. | ||
| 25 | Correlation among Perceived Stress, Emotional Intelligence, and Burnout of Resident Doctors in a Medical College of West Bengal | Mitra, S., Sarkar, A.P., Haldar, D., Saren, A.B., Lo, S., Sarkar, G.N. [59] | 2018 | India | Cross-sectional | 63 | Resident doctors | SMBM | TEIQ | Burnout had a significant positive correlation with perceived stress and in negative correlation with EI-well-being and positive correlation with EI-self-control and sociability. | ||
| 26 | Self-control as mediator between emotional intelligence and burnout among doctors | Jahanzeb, Z., Parveen, S., & Khizar, U. [60] | 2023 | Pakistan | Quantita-tive | 150 | Doctors | MBI | EIS | EI is negatively correlated with burnout. The result showed a significant negative correlation between burn out and self-control. | Burnout appears to be a more female experience, with women reporting it at a higher rate than men | |
| 27 | Emotional Intelligence and Burnout in Plastic Surgery Residents: Is There a Relationship? | Bin Dahmash, A.B., Alhadlaq, A. S., Alhujayri, A.K., Alkholaiwi, F., Alosaimi, N.A. [61] | 2019 | Saudi Arabia | Cross-sectional | 37 | Resident doctors | MBI | TEIQ-SF | There is a positive correlation between higher levels of EI and sense of personal achievement, whereas a negative correlation was observed between higher level of EI and EE and DP among the residents in this study. | Significant risk factors for burnout included dissatisfaction with plastic surgery as a career choice, dissatisfaction with income, and dissatisfaction with the role in the operating room | |
| 28 | Emotional Intelligence, Burnout, and Wellbeing Among Residents as a Result of the COVID-19 Pandemic | Kirkpatrick, H., Wasfie, T., Laykova, A., Barber, K., Hella, J., Vogel, M. [62] | 2022 | United States | Cross-sectional | 81 | Resident doctors | MBI | TEIQ-SF | EI continues to partially protect our residents’ burnout and wellbeing. | The COVID-19 pandemic initial surge appeared to negatively alter the protective effect of residents’ emotional intelligence on their burnout and wellbeing in our community hospital. | |
| 29 | Burnout and well-being of medical and surgical residents in relation to emotional intelligence: A 3-year study | Wasfie, T., Kirkpatrick, H., Barber, K., Hella, J., Lange, M., Vogel, M. [63] | 2024 | United States | Longitudinal | 77 | Resident doctors | MBI | TEIQ-SF | EI was inversely related to burnout and distress and is related to wellness factors in this community–hospital–based resident study sample. | ||
| 30 | Emotional Intelligence and Burnout Among Otorhinolaryngology–Head and Neck Surgery Residents | Sharaf, A. M., Abdulla, I.H., Alnatheer, A.M., Alahmari, A.N., Alwhibi, O.A., Alabduljabbar, Z., ... & Alkholaiwi, F.M. [64] | 2022 | Saudi Arabia | Cross-sectional | 51 | Resident doctors | MBI | TEIQ-SF | This study showed that surgical specialty residents with higher EI levels had a lower risk of burnout | One extra sleeping hour is associated with a 0.44-unit increase in the average EI score; the average EI score was 0.52 units higher in residents who exercised than in those who did not | |
| 31 | Longitudinal study of emotional intelligence, well-being, and burnout of surgical and medical residents | Wasfie, T., Kirkpatrick, H., Barber, K., Hella, J. R., Anderson, T., Vogel, M. [65] | 2023 | United States | Longitudinal | 80 | Resident doctors | MBI | TEIQ-SF | EI is associated with well-being and burnout in individual residents |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



