Submitted:
19 July 2025
Posted:
22 July 2025
You are already at the latest version
Abstract
Human papillomavirus (HPV) plays a major role in the development of head and neck cancers (HNCs), particularly oropharyngeal squamous cell carcinoma. This review highlights the key molecular mechanisms of HPV-driven carcinogenesis, focusing on the oncogenic E6 and E7 proteins and their disruption of tumor suppressor pathways and epigenetic regulation. We discuss the rising prevalence of HPV-related HNCs, their distinct clinical features, and diagnostic approaches such as p16 immunohisto-chemistry and HPV DNA/RNA detection. HPV-positive tumors show better prognosis and response to treatment, prompting interest in therapy de-escalation. Emerging strategies including immune checkpoint inhibitors, therapeutic vaccines, CRISPR-based gene editing, and ctDNA monitoring are advancing precision oncology in this field. We also examine the preventive potential of HPV vaccination and ongoing research into its role across various HNC subtypes. A deeper understanding of HPV’s molecular impact may guide more effective, targeted, and less toxic interventions.
Keywords:
human papillomavirus
; HPV
; Head and neck squamous cell carcinoma
; HNSCC
; E6/E7 oncoproteins
; Biomarkers
1. Introduction
Head and neck cancers (HNCs) ranks among the top 10 most common cancers worldwide. This type of cancer, which affects the upper respiratory and digestive tracts [1], includes various histological types, primarily squamous cell carcinomas [2]. Risk factors for this cancer include tobacco use, excessive alcohol consumption, and Human Papillomavirus (HPV). In the United States and some regions of Europe, 60-70% of diagnosed cases are reported to be HPV related [3,4]. Given the role of oncogenic viruses such as HPV, a multidisciplinary approach is required for the management of this cancer type [5].
Epidemiological data indicate that head and neck cancers are increasing globally, with more than 660,000 new cases reported each year [4]. The proportion of HPV related oropharyngeal cancers is rapidly rising, and it is projected that by 2030, the majority of these cancers will be associated with HPV [6].
HPV is a common viral infection known to cause various cancers, including those of the cervix, anus, and oropharynx [7]. Its role in oncogenesis has been extensively studied, and HPV is now recognized as a significant contributor to the global cancer burden [8]. HPV is a DNA virus known for its role in causing various cancers, particularly cervical cancer, and more recently, head and neck squamous cell carcinomas (HNSCCs) [9].
The oncogenic potential of HPV lies in its high-risk types, primarily HPV16 and HPV18, which have been implicated in the development of these cancers through the expression of viral oncoproteins E6 and E7 [10]. These proteins disrupt normal cell cycle regulation by inactivating tumor suppressor proteins p53 and retinoblastoma protein (pRb), leading to uncontrolled cell proliferation and the potential for malignant transformation [11].
Recent research has increasingly linked HPV to a subset of head and neck cancers, particularly oropharyngeal cancers, raising concerns about its broader impact on public health.
Given the virus's ability to integrate into the host genome and disrupt normal cellular processes, HPV has been investigated not only as a causative agent but also as a potential biomarker in cancer diagnosis and prognosis [12]. Understanding the mechanisms by which HPV contributes to the pathogenesis of HNCs could be crucial in developing more effective strategies for prevention, early detection, and treatment.
This review aims to comprehensively examine the impact of HPV on head and neck cancers, exploring its epidemiology, virology, clinical presentation, and the current state of research in this rapidly evolving field.
2. Epidemiology, Prevalence and Demographic Trends of HPV Related HNCs
The epidemiology of HNCs has undergone significant changes in recent years due to the increasing prevalence of HPV related subtypes. Traditionally, tobacco and alcohol use have been considered the primary risk factors for HNCs [13]. However, the growing recognition of HPV as an etiological factor, particularly in oropharyngeal cancers, has led to a notable shift in the epidemiological profile of HNCs [14].
HPV related HNCs exhibit regional variations globally, with a particularly significant upward trend observed in developed countries. This increase is largely attributed to the rising rates of HPV transmission through sexual activity. For instance, in North America and Europe, a substantial proportion of oropharyngeal cancers are now identified as HPV related, contributing to an overall increase in HNC incidence [15]. In contrast, the incidence of HPV nonrelated HNCs, traditionally linked to tobacco and alcohol use, has shown a decreasing trend. Between 1988 and 2004, the prevalence of HPV related oropharyngeal carcinoma increased by 225%, while HPV nonrelated cases decreased by 50% [16].
HPV related head and neck cancers frequently develop in specific regions such as the oropharynx, tonsils, and base of the tongue. This association highlights risk factors that facilitate viral transmission, including having multiple sexual partners and engaging in oral sex [17].
HPV related HNCs affect a different patient population compared to HPV nonrelated HNCs. HPV related HNCs are more commonly observed in younger age groups, predominantly in males rather than females, and are more prevalent among individuals of Caucasian descent [17]. Particularly in oropharyngeal cancers, HPV related patients have been observed among individuals who do not smoke and do not consume alcohol (Table 1) [18]. Additionally, these patients tend to have higher overall survival rates compared to HPV nonrelated patients, indicating that HPV related HNCs are associated with a better prognosis [19].
Among HPV subtypes, HPV16 is the most prevalent cause of head and neck cancers. Studies have shown that more than 90% of head and neck cancers are associated with HPV16 [20]. This subtype's higher oncogenic potential compared to other HPV types plays a determining role in the epidemiology of HNCs. Conversely, HPV18 and low-risk HPV types are less frequently detected in HNCs [21].

Table 1.
Comparative Clinical and Clinicopathological Features of HPV Positive and HPV Negative HNSCC [18,22].
| Clinical and Clinicopathological Features | HPV Positive HNSCC | HPV Negative HNSCC |
|---|---|---|
| Age | Younger and older patients (typically younger) | Older patients (median 61 years) |
| Sex | Male > Female (4:1) | Male > Female (3:1) |
| Anatomic Location | Oropharynx (tonsil, base of tongue, soft palate); rarely nasopharynx | Oral cavity, oropharynx, larynx, hypopharynx |
| Risk Factors | HPV, higher number of oral sex partners, low tobacco and alcohol use, marijuana | Tobacco, alcohol |
| Exposures | Increased number of sexual partners and frequency of oral sex | Smoking, smokeless tobacco (e.g., chewing tobacco), alcohol |
| Presenting Signs and Symptoms | Asymptomatic neck masses; typically lack symptoms like odynophagia or otalgia | Dysphagia, hoarseness, odynophagia, otalgia, neck pain, weight loss |
| Primary Tumor and Lymph Node Involvement | Smaller primary tumors, but high risk of advanced cervical lymphadenopathy | Larger primary tumors, widespread cervical lymphadenopathy |
| Distant Organ Metastasis | Unusual sites: skin, brain | Lung |
| Histopathological Features | Non-keratinizing or basaloid | Keratinizing |
| Tumor Differentiation | Undifferentiated | Differentiated |
| Sensitivity to Chemoradiotherapy | Better response | Worse response |
| Prognosis (Survival) | Better prognosis | Worse prognosis |
3. Virology and Mechanism of HPV in HNCs
Human papillomaviruses are non-enveloped viruses belonging to the Papillomaviridae family [23]. They possess a circular double-stranded DNA genome consisting of approximately 8,000 base pairs [24]. The HPV genome is divided into three main regions (Figure 1): the early (E) region, the late (L) region, and the long control region (LCR) or upstream regulatory region (URR). The early region encodes proteins essential for viral replication and transcription regulation, including E1, E2, E4, E5, E6, and E7. The late region encodes the structural proteins L1 and L2, which constitute the viral capsid [25].
Human papillomavirus is a central factor in the etiology of various malignancies, including head and neck cancers. The oncogenic potential of HPV primarily stems from its ability to disrupt critical tumor suppressor pathways within host cells [29].
3.1. Oncogenic Mechanism of HPV
HPV is categorized into high-risk and low-risk types based on its association with cancer. Low-risk HPVs, such as HPV6 and HPV11, are primarily associated with benign conditions such as genital warts and recurrent respiratory papillomatosis. These types have low malignant potential and rarely lead to cancer [30].
In contrast, high-risk HPVs, including HPV16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 70, 73, and 82 are known to cause precancerous lesions and play a role in cancers globally. High-risk HPVs are responsible for over 90% of cervical cancers, the majority of anal cancers, and a significant portion of vaginal, vulvar, penile, and head and neck cancers [31].
A critical difference between high-risk and low-risk HPVs is the manner in which their genomes integrate into host cells [32]. In benign lesions, such as genital warts, the HPV genome typically exists in an episomal form, remaining separate from the host cell's genome. However, the integration of HPV DNA into the host genome is a pivotal event in the transformation of normal epithelial cells into malignant cells [33]. This integration disrupts the normal cellular machinery, leading to persistent expression of E6 and E7 oncoproteins and interference with crucial tumor suppressor pathways. The continuous expression of these viral proteins drives the uncontrolled cell proliferation and survival characteristic of malignancies [34].
The papillomavirus E5 protein localizes to the endoplasmic reticulum and Golgi apparatus, where it inhibits the transport of major histocompatibility complex class I molecules to the cell surface, thereby impairing the recognition of infected cells by cytotoxic T lymphocytes. Studies have demonstrated that E5 proteins from both bovine papillomavirus and HPV types 16 and 6 similarly downregulate surface expression of MHC I molecules. This mechanism facilitates immune evasion, enabling persistent HPV infection and potentially contributing to the development of cancer [35].
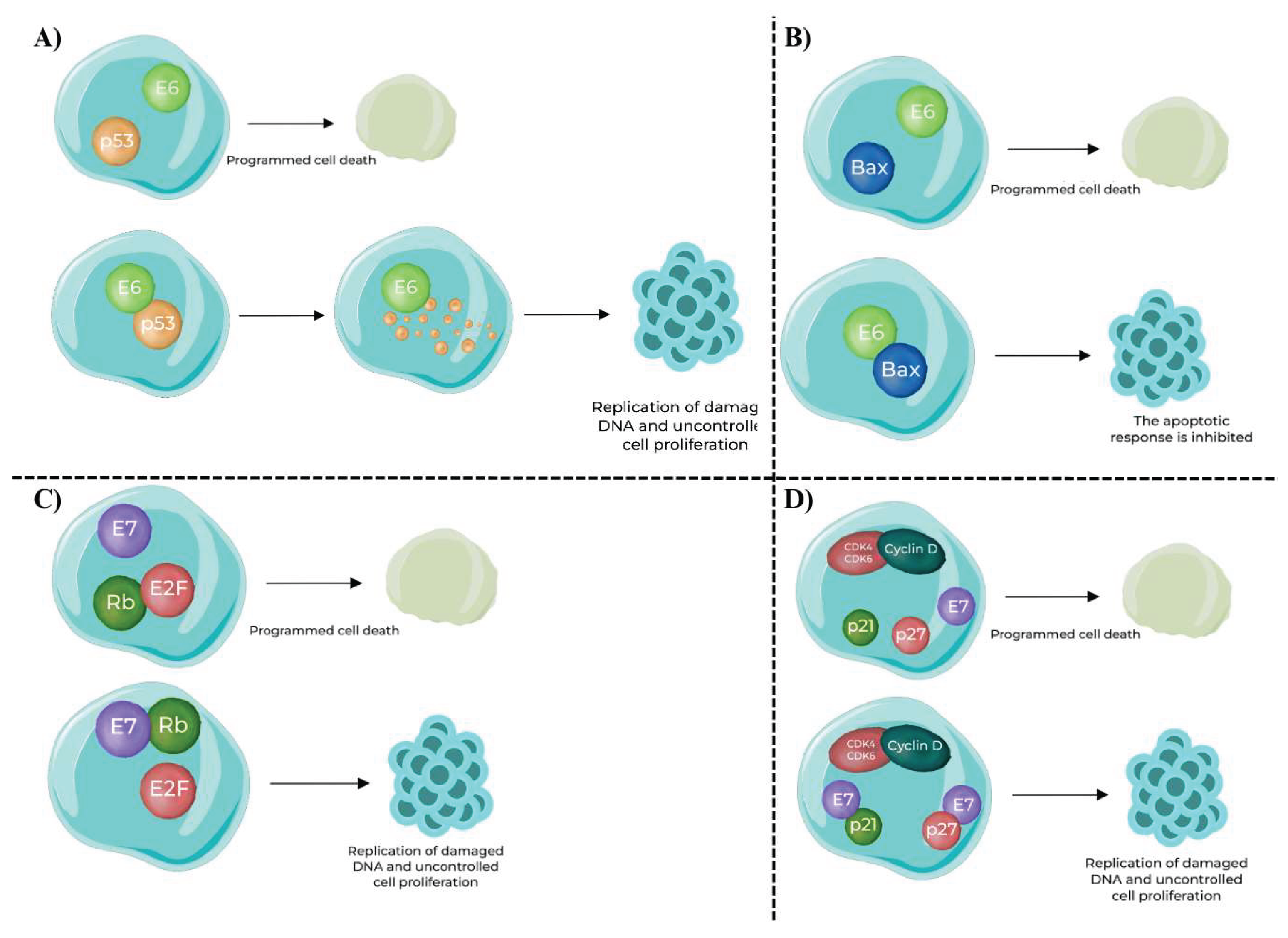
Role of E6 and E7 Oncoproteins (Figure 2):
The oncogenic potential of high-risk HPV types is largely mediated by two viral proteins: E6 and E7. These oncoproteins interfere with key tumor suppressor proteins, leading to uncontrolled cell proliferation and evasion of apoptosis [36,37,38,39,40,41].
E6 Oncoprotein:
- Interaction with p53 (Figure 2.A): E6 binds to the p53 tumor suppressor protein, a critical regulator of the cell cycle and apoptosis. The binding of E6 to p53 leads to its ubiquitination and subsequent degradation, thus eliminating its growth-inhibitory effects.
- Impact on Apoptosis (Figure 2.B): E6 also facilitates the degradation of Bax, a pro-apoptotic protein that promotes apoptosis. By targeting Bax for degradation, E6 inhibits the apoptotic response, allowing cells with damaged DNA to survive and proliferate.
E7 Oncoprotein:
- Interaction with Rb Protein (Figure 2.C): E7 binds to pRb, another pivotal tumor suppressor. Rb normally functions by sequestering the E2F transcription factor, thereby preventing it from activating genes required for cell cycle progression. E7’s binding to Rb releases E2F, which then promotes the transcription of genes necessary for cell cycle progression, such as those involved in DNA replication and mitosis.
- Inactivation of Cyclin – Dependent Kinase (CDK) Inhibitors (Figure 2.D): E7 also inhibits CDK inhibitors like p21 and p27. Normally, these inhibitors prevent the activation of cyclin D and CDK4, which are critical for progression through the G1 phase of the cell cycle. By inhibiting these inhibitors, E7 promotes the activation of cyclin D and CDK4, further facilitating cell cycle progression and malignancy.
Figure 2.
Role of E6 and E7 Oncoproteins [41].
Figure 2.
Role of E6 and E7 Oncoproteins [41].
In conclusion, the virological mechanisms of HPV related head and neck cancers involve a sophisticated interplay between viral oncoproteins and host cellular regulatory pathways. The integration of HPV DNA into the host genome and the subsequent disruption of tumor suppressor proteins, particularly p53 and Rb, are central to the malignant transformation process. Understanding these mechanisms is crucial for developing targeted therapies and preventive strategies for HPV related cancers [42,43].
3.2. HPV Mechanism Affected by Epigenetic Regulation
The mechanism by which HPV genes become active is largely influenced by epigenetic regulation, which involves chemical and structural modifications to DNA. Specifically, the p97 promoter, located within LCR of the HPV genome, is regulated by epigenetic marks and transcription factors, determining which HPV genes are expressed [43]. Transcription factors are proteins that control the activation and repression of genes. For instance, the transcription factor Yin Yang 1 (YY1) plays a crucial role in suppressing the expression of the oncogenes E6 and E7, which are associated with cancer development. However, as epithelial tissues mature, the repressive effect of YY1 diminishes, leading to the activation of the E6 and E7 genes, both of which are critical in promoting carcinogenesis (Figure 3.A) [24].
In addition, the CCCTC-binding factor (CTCF) protein forms a repressive chromatin structure within the HPV genome, thereby restricting gene expression. However, during cellular differentiation, this repressive structure is disrupted, allowing for the expression of the E6 and E7 genes [44]. Proteins such as Sirtuin1 (SIRT1) and Werner Syndrome Protein (WRN) are also involved in controlling HPV replication and modulating the epigenetic modifications of the viral genome. The way in which these epigenetic mechanisms function determines the level of HPV gene activity and, consequently, the virus's oncogenic potential (Figure 3.B) [45].
Interestingly, HPV31’s E7 protein has been observed to increase the levels of SET-domain containing protein 2 (SETD2), a protein that introduces the epigenetic mark H3K36me3 on viral DNA. This mark facilitates the activation of certain viral genes and plays a critical role in the viral life cycle. Notably, this epigenetic mark is absent from the E6 and E7 oncogenes, indicating that these genes remain epigenetically unsuppressed and thus potentially active. As a result, this lack of repression may increase the risk of cancer development, as E6 and E7 continue to function unchecked (Figure 3.C) [46,47].
These epigenetic mechanisms play a key role in determining the extent of HPV's pathogenicity within the host, contributing to its potential to induce malignancy.
3.3. The Role of DNA Methylation in the HPV Mechanism
HPV's DNA methylation profiles play a crucial role in the virus’s life cycle, cellular differentiation, and oncogenic processes (Figure 4) [48]. Specifically, methylation changes in certain genomic regions, such as the long control region and the E6 gene, vary significantly depending on the HPV genotype and viral integration status. In the case of HPV16, E2 binding regions remain demethylated in low-grade lesions, while in high-grade lesions, methylation levels increase, which is associated with early promoter activation and viral integration. Methylation of viral DNA, particularly in the L1 region, has been strongly correlated with high-grade lesions and cervical cancer [49].
Methylation profiles have also been reported to differ based on the viral integration status, with HPV18 exhibiting more frequent integration than HPV16. However, viral integration is not necessarily required for malignant transformation; rather, DNA methylation at E2 binding sites (E2BS) may contribute to cancer development by dysregulating the expression of the E6 and E7 oncogenes [50]. Additionally, micronutrients such as folate and vitamin B12 have been shown to enhance methylation in the E6 gene region, providing a protective effect against low-risk CIN2+ lesions [43,51].
These findings suggest that HPV methylation profiles are not only critical in regulating viral replication and gene expression but also play a key role in determining cancer risk. Understanding DNA methylation and its consequences in HPV related cancers, including not only cervical cancer but also head and neck cancers, provides valuable insights for the development of diagnostic and therapeutic approaches.
3.4. Long Non-Coding RNAs
HPV has the capacity to produce specific molecules that play a role in cancer development. These molecules are referred to as non-coding RNAs (ncRNAs) because, unlike classical RNAs involved in protein synthesis, they do not code for proteins. Instead, they perform various regulatory functions within the cell [52]. It is known that HPV synthesizes small RNAs, such as microRNAs (miRNAs) and circular RNAs (circRNAs), which influence cellular processes. Furthermore, it is believed that the expression of certain long non-coding RNAs (lncRNAs) increases in response to the oncogenic E6 and E7 proteins produced by HPV [53].
LncRNAs are RNA molecules longer than 200 nucleotides that lack the capacity to code for proteins. Oncogenic long non-coding RNAs play a significant role in head and neck cancers. The HPV E6 and E7 oncoproteins can alter the expression of lncRNAs, disrupting the genetic balance within the cell. These alterations can lead to impaired cellular function and contribute to the development of a cancerous phenotype [54,55,56]. Among various lncRNAs, CCEPR and FAM83H-AS1 stand out [43].
CCEPR is particularly localized in both the nucleus and cytoplasm of oral squamous cell carcinoma (OSCC) cells and acts as an oncogene by competitively binding to miR-922, thereby enhancing the expression of PAK2, which promotes OSCC progression. This finding highlights the importance of evaluating whether this expression is associated with the presence of viral oncoproteins in OSCC [57].
On the other hand, the lncRNA FAM83H-AS1 is highly expressed in both cervical cancer cells and HPV16-positive head and neck cancer cell lines, compared to HPV16 negative cells. This lncRNA is associated with elevated levels in the early stages of carcinogenesis, and it is known that HPV regulates this molecule via a p53-independent mechanism involving the presence of p300. The suppression of FAM83H-AS1 expression may inhibit cell proliferation, migration, and apoptosis, potentially serving as a barrier to cancer progression [58].
In addition to oncogenic lncRNAs, PRINS is particularly noteworthy among the suppressing lncRNAs. PRINS is highly expressed in HPV related HNSCC patients and is correlated with antiviral response genes. The expression of this lncRNA modulates the gene expression of inflammatory responses, growth factors, pro-inflammatory genes, chemokines, and immune stimulators. A greater number of immune cells have been observed in tumors of HPV positive HNSCC patients, which may explain why these patients respond better to treatment compared to HPV negative patients [59].
Furthermore, studies have shown that in HPV positive patients, lncRNAs such as PRINS, CDKN2B-AS1, TTTY14, TTTY15, MEG3, and H19 are expressed differently compared to HPV negative patients. These findings contribute to a better understanding of the molecular mechanisms underlying HPV related head and neck cancers and may play a crucial role in explaining factors that influence treatment response [43,56].
3.5. Epigenetic Alterations and Their Potential as Biomarker
Various studies have identified distinct methylation profiles in specific genomic regions of HPV positive cancers [43,60]. These methylation profiles are used to distinguish between healthy and cancerous tissues, as well as to predict the risk of disease recurrence. Additionally, certain epigenetic signatures play a crucial role in determining the biological behavior and prognosis of tumors associated with different HPV genotypes. Methylation levels increase with the severity of the lesions, and this increase is directly related to tumor aggressiveness and patient survival rates [60,61].
The detection of these epigenetic changes in HPV positive cancers has emerged as a more sensitive and effective biomarker for diagnosis and prognosis than traditional methods. In this context, further investigation of epigenetic profiles in HPV related neoplasms could significantly contribute to the development of personalized treatment approaches and the implementation of more targeted strategies in cancer management.
4. Clinical Presentation and Diagnosis
4.1. Symptoms and Presentation
HNCs present a diverse spectrum of clinical symptoms depending on their etiology, particularly when distinguishing between HPV related and HPV nonrelated tumors. The clinical manifestations of HPV related HNCs often contrast starkly with those of HPV nonrelated HNCs, reflecting underlying differences in tumor biology and pathogenesis [62].
HPV related HNCs, predominantly arising in the oropharyngeal region, are frequently characterized by a subtle and insidious onset. These tumors are known for their asymptomatic progression in the early stages, which often leads to delayed clinical detection [63]. Patients with HPV related HNCs typically present with painless cervical lymphadenopathy, which may be the first and only sign of the disease. This is often accompanied by a persistent sore throat, dysphagia (difficulty swallowing), otalgia (ear pain), and unexplained weight loss. In cases where the larynx is involved, patients may experience hoarseness or other vocal changes. The predilection of HPV related tumors for lymphoid-rich areas, such as the tonsils and the base of the tongue, often results in localized symptoms reflective of the tumor’s anatomical origin [21,64].
Despite the relatively small size of HPV related tumors at presentation, they are frequently associated with advanced lymph node metastasis. The presence of poorly differentiated cells and the propensity for early nodal involvement can complicate the clinical course, although distant metastases occur at rates comparable to HPV nonrelated tumors. Notably, when distant metastases do occur, they tend to exhibit a more aggressive pattern of spread in HPV related cancers [65].
In contrast, HPV nonrelated HNCs generally present with more pronounced and diverse symptoms, often reflecting the more aggressive nature of these tumors. HPV nonrelated tumors are typically found in patients with a significant history of tobacco and alcohol use, which are well-established risk factors [66]. Clinically, these patients may report more severe throat pain, pronounced dysphagia, persistent otalgia, and significant vocal changes, such as hoarseness. HPV nonrelated HNCs are more likely to be detected at a later stage, given their association with extensive local invasion and symptomatic burden at the time of diagnosis [67].
HPV nonrelated tumors more commonly arise in the oral cavity, larynx, and hypopharynx, regions less frequently affected by HPV related tumors. The larger size and more advanced stage of HPV negative tumors at diagnosis are reflective of their aggressive clinical course and poorer prognosis compared to their HPV related counterparts [67].
4.2. Diagnostic Methods and Challenges
The clinical presentation of HPV related HNCs often involves asymptomatic or minimally symptomatic lymphadenopathy, which can delay the recognition and diagnosis of these cancers. Additionally, HPV related tumors tend to have a better prognosis and a different response to treatment, making accurate and early diagnosis crucial [68].
The diagnosis of HPV related HNCs presents unique challenges and opportunities compared to HPV nonrelated HNCs. HPV related HNCs, predominantly affecting the oropharyngeal region, are associated with distinct clinical and molecular features that necessitate specialized diagnostic approaches [69].
4.2.1. Key Diagnostic Differences
-
Histopathology and p16 Immunohistochemistry:
- p16 Overexpression: One of the hallmark features of HPV related HNCs is the overexpression of p16, a cyclin-dependent kinase inhibitor. Immunohistochemistry (IHC) for p16 is widely used as a surrogate marker for HPV infection, particularly in oropharyngeal cancers. p16 positivity, although not entirely specific for HPV, correlates strongly with the presence of oncogenic HPV, especially HPV16 [70,71,72].
-
HPV DNA/RNA Testing:
-
Comparison with HPV Negative HNCs:
- HPV negative HNCs are less likely to show p16 overexpression and typically do not harbor HPV DNA/RNA. Instead, these cancers are more often associated with mutations in genes like TP53, which are linked to tobacco exposure. The absence of HPV biomarkers in HPV nonrelated HNCs highlights the importance of differentiating between these two subtypes for accurate diagnosis and appropriate treatment planning [80,81,82].
4.2.2. Emerging Diagnostic Methods for HPV related HNCs
As the understanding of HPV related HNCs evolves, so do the diagnostic techniques used to identify and characterize these cancers. Several emerging methods offer the potential to improve the accuracy and specificity of HPV related HNC diagnosis [83].
- Next-Generation Sequencing (NGS): NGS allows for comprehensive genomic profiling of tumors, providing insights into the genetic landscape of HPV related HNCs [84]. This technique can identify viral integration sites, mutation signatures, and other molecular features unique to HPV related tumors. NGS also helps in distinguishing HPV related from HPV nonrelated tumors by identifying characteristic mutations or the absence thereof [85].
- Liquid Biopsy: Liquid biopsy is an innovative, non-invasive diagnostic tool that analyzes circulating tumor DNA (ctDNA) or HPV DNA in the bloodstream. This approach holds promise for early detection, monitoring disease progression, and assessing treatment response in HPV related HNC patients. Liquid biopsy could potentially overcome some of the limitations of tissue biopsies, particularly in cases where tumor tissue is difficult to access [86].
- Circulating Biomarkers: Beyond ctDNA, circulating biomarkers such as antibodies against HPV oncoproteins (E6 and E7) and miRNAs are being studied for their potential role in the diagnosis and prognosis of HPV related HNCs. These biomarkers could offer a non-invasive method to monitor disease status and guide therapeutic decisions [87,88].
4.2.3. Challenges in the Diagnosis of HPV Related HNCs
- False Positives and Negatives: While p16 IHC is a valuable tool, it is not infallible. False positives can occur in HPV nonrelated tumors that exhibit p16 overexpression without the presence of HPV DNA. Conversely, false negatives may arise in HPV related tumors with low p16 expression. Combining p16 IHC with HPV DNA/RNA testing is essential to mitigate these risks [71].
- Tumor Heterogeneity: HPV related HNCs exhibit considerable heterogeneity, not only in terms of HPV subtypes but also in their biological behavior and response to treatment. This heterogeneity complicates the diagnostic process, necessitating a multifaceted approach that includes histopathology, molecular testing, and biomarker analysis [89,90].
4.2.3. Role of Biomarkers in Diagnosis
Biomarkers play a crucial role in the accurate diagnosis of HPV related HNCs, offering insights into tumor biology, prognosis, and potential therapeutic targets. As previously discussed, p16 remains the most widely used surrogate marker for HPV in oropharyngeal cancers [80]. However, its use should be complemented by other diagnostic tests to confirm HPV status [91,92]. Detection of E6/E7 mRNA provides strong evidence of active HPV infection and oncogenic activity, making it a critical biomarker for confirming HPV-driven carcinogenesis in HNCs [87,88].
Research into additional biomarkers, such as specific miRNAs and proteins, is ongoing. These biomarkers could help stratify patients based on their risk and guide personalized treatment approaches. For example, lower expression of certain miRNAs may be associated with more aggressive disease and poorer outcomes [93,94,95].
The diagnosis of HPV related head and neck cancers requires a nuanced approach that integrates clinical evaluation, histopathological assessment, and advanced molecular testing. Emerging diagnostic techniques and biomarkers hold the promise of improving diagnostic accuracy and enabling earlier detection of these cancers. As research continues to unfold, the hope is that these advancements will lead to more personalized and effective treatment strategies for patients with HPV related HNCs.
5. Treatment and Prognosis
The management of head and neck cancers has evolved significantly with the recognition of distinct subgroups based on HPV status [96]. HPV related HNCs, particularly those originating in the oropharynx, display unique biological behaviors that influence both treatment strategies and prognosis [97].
5.1. Standard Treatment Approaches for HPV Related HNCs
- Radiotherapy: Radiotherapy (RT) is often the cornerstone of treatment for HPV related oropharyngeal cancers, particularly in patients with early-stage disease. HPV related tumors are generally more radiosensitive compared to HPV nonrelated tumors, which allows for effective tumor control with potentially lower doses of radiation. Given the favorable prognosis of HPV related HNCs, there has been increasing interest in treatment de-escalation, aiming to reduce the long-term toxicity associated with standard doses of radiation. Studies are exploring reduced radiation doses and the omission of concurrent chemotherapy in selected patients with favorable prognostic features [98,99,100,101].
- Chemoradiotherapy (CRT): For locally advanced HPV related HNCs, concurrent chemoradiotherapy remains a standard approach. The combination of radiation with platinum-based chemotherapy, such as cisplatin, enhances treatment efficacy by sensitizing tumor cells to radiation. Given the high response rates observed in HPV related tumors, there is ongoing research into reducing chemotherapy intensity or exploring alternative agents with fewer side effects [102,103,104,105].
- Surgery: Minimally invasive surgical techniques, such as Transoral Robotic Surgery (TORS), are increasingly being used for HPV related oropharyngeal cancers. TORS allows for precise tumor resection with minimal morbidity and may be followed by adjuvant radiation or chemoradiotherapy depending on the pathological findings [106,107].
5.2. Emerging and Investigational Treatment Modalities
Immune checkpoint inhibitors (ICIs) have revolutionized treatment for recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC), especially in HPV-related cases. Pembrolizumab and nivolumab, both anti–PD-1 agents, are standard treatments. In the KEYNOTE-048 trial, pembrolizumab monotherapy or in combination with platinum/5-FU improved survival over the EXTREME regimen, establishing its role as a first-line option—monotherapy for PD-L1 CPS ≥1 and in combination regardless of PD-L1 status [108].
In platinum-refractory disease, both agents are approved second-line therapies. Nivolumab demonstrated a survival benefit in CheckMate-141 [109], and pembrolizumab showed durable responses in KEYNOTE-012/055 trials, especially in PD-L1 positive patients [110,111].
Building on this immunotherapeutic backbone, novel strategies have emerged. Therapeutic vaccines targeting HPV oncoproteins E6/E7 aim to enhance tumor-specific immunity and are under evaluation for both adjuvant and recurrent settings [112,113,114,115]. CUE-101, an HPV16-specific Immuno-STAT, achieved a 47% objective response rate (ORR) in HPV16+ R/M HNSCC and defined a recommended Phase II dose of 4 mg/kg [116]. HB-200, an arenavirus-based vector therapy, showed a 43% ORR with pembrolizumab, increasing to 59% in PD-L1 CPS ≥20 [117]. In the neoadjuvant setting, HB-200 plus chemotherapy led to ≥50% tumor shrinkage in 81% of patients and a 93% response rate at higher doses [118]. Similarly, neoadjuvant sintilimab plus platinum-based chemotherapy yielded 100% partial response, 96% major pathological response, and 52% complete response [119].
Dual checkpoint and EGFR blockade also shows promise. Nivolumab combined with cetuximab resulted in a 66% one-year survival rate, benefiting both p16-negative and p16-positive patients [120]. ISA101b vaccine with cemiplimab improved ORR and median overall survival in patients with PD-L1 CPS ≥20, underscoring the importance of biomarker-driven selection [121].
Targeted therapies have focused on molecular pathways activated by HPV. E6/E7 oncoproteins upregulate PI3K/Akt/mTOR signaling. While mTOR inhibitor everolimus showed limited efficacy, a Phase II trial is investigating its impact on progression-free survival (PFS) in the adjuvant setting [122,123,124].
Given the favorable prognosis of HPV-positive oropharyngeal carcinoma, de-intensification strategies have been extensively explored. Hypoxia-directed radiation de-escalation to 30 Gy achieved a 2-year locoregional control rate of 95% and 99% overall survival with reduced toxicity [125]. Transoral robotic surgery with pathology-driven adjuvant therapy produced a 54-month PFS of 90.6% and OS of 95.3%, with comparable outcomes between 50 Gy and 60 Gy groups [126]. Moreover, intensity-modulated proton therapy (IMPT) was non-inferior to IMRT in a Phase III trial, with lower gastrostomy tube dependence and treatment-related malnutrition [127].
Liquid biopsies, particularly circulating tumor HPV DNA, have emerged as a promising tool for minimal residual disease (MRD) monitoring. The HPV-DeepSeek assay detected recurrence a median of 207 days before clinical diagnosis and correlated with poorer 2-year PFS in patients with persistent ctHPV DNA, supporting its role in risk-adapted strategies [128].
Gene-editing technologies targeting HPV oncogenes are also being explored. CRISPR/Cas9 targeting of E6/E7 in preclinical models induced apoptosis and growth arrest [129]. Combining CRISPR-mediated gene silencing with PD-1 blockade enhanced immune responses [130]. Additionally, CRISPR/Cas13a successfully degraded E6/E7 transcripts and upregulated tumor suppressors (p53, RB) in HPV-positive cell lines, offering a novel post-transcriptional therapeutic strategy [131].
Cell-based therapies are advancing. TCR-engineered T cells targeting HPV16 E7 showed responses in 6 of 12 patients, including PD-1 inhibitor-resistant cases [132]. CAR-T cells directed against HPV16 E6 also demonstrated potent in vitro cytotoxicity [133].
In summary, the treatment paradigm in HPV-related HNSCC is shifting toward personalized, immune- and biomarker-driven approaches. The integration of ICIs, vaccines, molecular targets, and cell therapies is reshaping clinical trial designs, with radiation de-escalation and liquid biopsy technologies further enabling risk-adapted strategies.
5.3. Prognosis and Survival Outcomes
Patients with HPV related HNCs generally have a better prognosis compared to those with HPV negative tumors. The improved survival rates are attributed to the tumor’s responsiveness to treatment and the typically younger, healthier patient population [134]. Five-year survival rates for HPV related oropharyngeal cancers can exceed 80%, significantly higher than those for HPV negative HNCs [135].
While HPV related status is a strong prognostic factor, the presence of concurrent smoking can negatively impact outcomes. Smokers with HPV related HNCs may experience a prognosis more akin to HPV negative cases, underscoring the importance of smoking cessation as part of the treatment plan [136].
HPV negative HNCs, often associated with extensive tobacco and alcohol use, tend to present at a more advanced stage with more aggressive biological behavior. These tumors are less responsive to treatment, and five-year survival rates are typically lower, around 47% [137].
The more aggressive treatment required for HPV negative HNCs often results in higher rates of acute and long-term toxicities. This contributes to a reduced quality of life and increased risk of treatment-related morbidity and mortality [138].
Table 2.
Comparison of HPV Related and HPV Nonrelated Head and Neck Cancers: Clinical Features and Diagnostic Differences.
Table 2.
Comparison of HPV Related and HPV Nonrelated Head and Neck Cancers: Clinical Features and Diagnostic Differences.
| Key Features | HPV Related HNC | HPV Nonrelated HNC |
|---|---|---|
| Symptoms and Presentation | Subtle and insidious onset | More pronounced and diverse symptoms |
| Often asymptomatic in early stages | Severe throat pain, dysphagia, otalgia, vocal changes | |
| Painless cervical lymphadenopathy | Often detected at a later stage | |
| Localized symptoms | Associated with tobacco and alcohol use | |
| Associated with lymphoid-rich areas (e.g., tonsils, base of tongue) | ||
| Methods | p16 overexpression used as a surrogate marker | More traditional diagnostic approaches |
| HPV DNA/RNA testing | Less reliance on p16 and HPV biomarkers | |
| Emerging techniques like NGS and liquid biopsy | Diagnosis often based on clinical presentation and histopathology | |
| Biomarkers in Diagnosis | p16 immunohistochemistry | Less reliance on HPV biomarkers |
| HPV DNA/RNA testing | Often associated with mutations in genes like TP53 | |
| Emerging biomarkers such as circulating miRNAs and antibodies against HPV oncoproteins (E6/E7) | Importance of differentiating from HPV related HNCs for accurate diagnosis and treatment planning | |
| Treatment | Radiotherapy, Chemoradiotherapy | More aggressive treatment required |
| Transoral Robotic Surgery | Often involves higher doses of radiation and more intensive chemotherapy | |
| Ongoing research in treatment de-escalation | Higher rates of treatment-related toxicities | |
| Immunotherapy, targeted therapies, and personalized medicine | Challenges in treating more advanced disease | |
| Prognosis and Survival | Generally favorable prognosis | Poorer prognosis |
| Five-year survival rates can exceed 80% | Five-year survival rates typically around 47% | |
| Better response to treatment | Higher rates of acute and long-term toxicities | |
| Prognosis negatively impacted by concurrent smoking | Reduced quality of life |
6. HPV Vaccines and Avoiding HPV Related HNCs
Vaccination against human papillomavirus has emerged as a significant step in preventing HPV related diseases, particularly head and neck cancers [139]. Understanding the role and mechanisms of these vaccines, as well as their potential to reduce the incidence of HPV related cancers, is crucial in the global fight against such malignancies. The global implementation of HPV vaccines initially aimed to reduce the incidence of cervical cancer, as it is directly linked to HPV infection [140,141]. However, as HPV was recognized as a cause of HNCs, particularly oropharyngeal cancers, the potential of vaccines to prevent these cancers expanded [142,143]. HPV vaccines have been shown to be effective primarily against the most common high-risk HPV types responsible for HPV related cancers, particularly HPV16 and HPV18 [144].
To date, three different HPV vaccines have been approved, each differing in their valency. The first to be marketed was Gardasil, a quadrivalent vaccine, which provides protection against HPV types 6, 11, 16, and 18. Cervarix is a bivalent vaccine that targets HPV16 and HPV18, while Gardasil9, a nonavalent vaccine, offers protection against HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58 [145,146]. Research continues to develop vaccines that target a broader range of HPV subtypes.
Not all vaccine varieties are available worldwide. In the United States, the 9-valent vaccine is available and is used with the aim of preventing HPV related cancers, including HNCs [147]. HPV vaccines work by priming the immune system to recognize and combat the virus before it establishes infection. These vaccines are prophylactic, not therapeutic, meaning they are designed to prevent infection rather than treat existing HPV related diseases [41]. While the exact mechanism of the 9-valent HPV vaccine (9vHPV) is not fully understood, researchers believe it activates humoral immunity. The vaccine is formulated using virus-like particles (VLPs) derived from the L1 protein, the major capsid protein of HPV serotypes 6, 11, 16, 18, 31, 45, 52, and 58. Additionally, studies have shown that the level of antibodies produced in response to vaccination is 10 to 100 times higher than that produced by natural infection [147].
6.1. Studies of Therapeutic Vaccines
Although prophylactic vaccines provide protection against HPV, they are insufficient for treating existing infections or HPV related neoplasms. Therefore, the development of therapeutic vaccines that offer more effective solutions for the treatment of HPV related diseases is of great importance [148].
Clinical studies have shown that therapeutic vaccines targeting oncogenic proteins such as E6 and E7 hold the potential to treat HPV related cancers. However, these vaccines have yet to elicit a durable and effective immune response in clinical practice. Currently, prophylactic vaccines targeting the L1 protein are ineffective against existing lesions, and therapeutic vaccines targeting E6 and E7 have not been successful in generating long-lasting immune responses. This suggests that other viral proteins, such as the L2 capsid protein, may induce more effective immunological responses [149,150].
Additionally, research into the combination of therapeutic vaccines with immune checkpoint inhibitors and other treatment options has shown promising results [151]. Ongoing studies are also investigating the advantages and limitations of various platforms, such as DNA-based and vector-based vaccines, which could lead to novel approaches in the treatment of HPV related cancers [152].
6.2. Effectiveness of HPV Vaccines in Preventing Head and Neck Cancers
Human papillomavirus vaccines have garnered substantial attention due to their potential to prevent a wide range of HPV related cancers, including head and neck cancers, particularly oropharyngeal cancers (OPC). While originally developed to prevent cervical and other anogenital cancers, the expanding role of these vaccines in reducing the incidence of HPV related HNCs is becoming more evident, especially in high-income countries where the prevalence of HPV related oropharyngeal cancers is rising, primarily driven by HPV16 [153,154,155].
Several studies have demonstrated the efficacy of HPV vaccines in preventing oral HPV infections, which are a significant precursor to HPV related oropharyngeal cancers. For example, a meta-analysis revealed that individuals vaccinated against HPV were 46% less likely to acquire oral HPV infections. Additionally, the vaccine’s efficacy against HPV16 and HPV18 – the types most associated with oropharyngeal cancers – was as high as 93.3% in some studies. The World Health Organization (WHO) and regulatory bodies like the U.S. FDA have also recognized the importance of HPV vaccination in preventing head and neck cancers [156,157].
6.3. HPV Vaccination Strategies and Challenges: A Critical Step in Cancer Prevention
Human Papillomavirus is one of the leading causes of several cancers, including cervical, vulvar, vaginal, anal, and oropharyngeal cancers. HPV vaccines are a highly effective tool for preventing these cancers. The primary vaccination strategies prioritize immunizing children between the ages of 9 and 15, as this age group can acquire immunity before becoming sexually active [160]. However, the global implementation of HPV vaccination strategies faces several challenges [161,162,163].
In particular, the application of HPV vaccines is limited in low- and middle-income countries. These vaccination programs are often impacted by resource constraints, inadequate healthcare infrastructure, misconceptions, and vaccine hesitancy [160,163]. For instance, in Kenya, only 33% of the targeted population received the first dose of the vaccine when the program was initiated in 2019, and only 16% completed the second dose [162]. Similarly, vaccination programs in China are restricted by regional limitations, resulting in low vaccination rates in some areas[161,164]. In Turkey, HPV vaccination is not yet included in the national immunization schedule, leading to low vaccination rates and limited public awareness [165,166]. In low- and middle-income countries, vaccination programs targeting young girls are typically conducted in schools, posing significant challenges in reaching girls who are not in school. This creates barriers to achieving target coverage and expanding vaccine reach [160,163]. In Kenya, although vaccination programs for young girls are conducted through schools, reaching those who are out of school or in remote areas is challenging [162]. Similarly, in China and Senegal, efforts have been made to extend vaccination programs to broader age groups; however, these initiatives are often limited by costs and supply constraints [161,163].
HPV vaccines are generally administered before the onset of sexual activity, as they provide immunity prior to exposure to the virus. WHO and other international health authorities identify children between 9 and 14 as the ideal target population for vaccination. However, vaccine hesitancy remains a significant obstacle to widespread vaccination in many countries [167]. Misinformation about vaccine safety, cultural barriers, and social stigma are critical factors in some countries. To address these concerns, countries should collaborate with healthcare providers, educators, and community leaders to conduct education and awareness campaigns on the safety and efficacy of the vaccine [168,169]. Emphasizing the importance of vaccinating boys is also crucial, as HPV can cause cancer in men as well as women.
Studies in Latin America have shown that cultural barriers, misinformation, and safety concerns negatively impact vaccine acceptance. A significant drop in second-dose vaccination rates has been observed, limiting the vaccine’s overall effectiveness [170]. Similarly, public mistrust in vaccines and access challenges contribute to lower vaccination rates in China [166]. As HPV vaccination is often associated with sexual activity, some parents hesitate to vaccinate their children (Turkey). Studies in Turkey have shown low awareness of the HPV vaccine, which is reflected in vaccination rates. In one study, only 55.4% of participants had heard of the HPV vaccine, and only 3.6% had been vaccinated. These figures demonstrate how lack of awareness and financial barriers directly affect vaccination rates [166]. Furthermore, fear of side effects is common. Studies have reported that participants were hesitant to get vaccinated due to a lack of information on the vaccine’s side effects [165,171].
Although HPV vaccination initially targeted children and adolescents, vaccination strategies have expanded in recent years. Adult vaccination programs can also be effective, even among individuals who are already sexually active. The United States Food and Drug Administration (FDA) has approved the use of HPV vaccines for adults between the ages of 27 and 45. Vaccination in this age group is essential for protecting individuals who have not yet been exposed to the virus [167,169]. However, catch-up vaccination programs are often limited due to access and cost issues [161]. Such strategies are particularly important for adults who have missed the vaccination window or have been outside the scope of vaccination programs. Further research is needed to better understand vaccine efficacy in adults, especially concerning age-related immune system decline and its impact on vaccine effectiveness [167].
HPV vaccines provide an effective and safe method of protection against a virus that causes cancer. Widespread vaccination can potentially prevent not only cervical cancer but also other HPV related cancers, including HNC. However, the success of vaccination programs is directly related to making the vaccine more accessible globally and overcoming vaccine hesitancy [169].
Moreover, even healthcare professionals lack sufficient knowledge about HPV. For example, one study reported that only 44.1% of participants knew HPV could cause cervical cancer, while 63.4% were unsure if the vaccine was effective against other cancer types [171]. This highlights the need for more awareness among both the public and healthcare providers.
In conclusion, to ensure the success of vaccination strategies, governments and health organizations must raise public awareness, expand target populations, and address financial and logistical barriers to make vaccine protection sustainable. Increased financial support, public awareness, and strengthened vaccination strategies are essential, especially in low-income countries. Eliminating HPV related cancers is achievable through the effective implementation of global vaccination programs, marking a significant milestone in public health [168,169,170].
7. Conclusion and Future Directions
Human papillomavirus has emerged as a critical factor in the etiology, diagnosis, and treatment of various head and neck cancers, particularly oropharyngeal squamous cell carcinoma. With the rising global incidence of HPV related HNCs, understanding its role in tumorigenesis has become essential in guiding research and clinical practice. This review highlights the complex interplay between viral oncoproteins, host cellular pathways, and epigenetic regulation in driving cancer development. The distinct epidemiological, clinical, and molecular features of HPV positive HNCs underscore the need for tailored diagnostic and therapeutic approaches.
Current diagnostic methods for HPV related HNCs rely heavily on surrogate markers such as p16 immunohistochemistry and HPV DNA/RNA testing, while emerging techniques like liquid biopsies and next-generation sequencing offer new opportunities for early detection and disease monitoring. Despite these advancements, challenges remain, including tumor heterogeneity, asymptomatic presentation, and the risk of diagnostic inaccuracies. Further research into circulating biomarkers, such as tumor-derived HPV DNA and specific microRNAs, could enhance diagnostic precision and improve patient outcomes.
Treatment strategies for HPV positive HNCs are evolving with a focus on treatment de-escalation to minimize toxicity without compromising efficacy. HPV related tumors are more responsive to radiotherapy and chemoradiotherapy, leading to higher survival rates and better prognosis compared to HPV negative HNCs. Innovative approaches, including immunotherapy, therapeutic vaccines targeting viral oncoproteins, and targeted therapies, show promise in enhancing treatment effectiveness while reducing long-term adverse effects.
HPV vaccination programs have demonstrated significant success in preventing HPV related cancers, yet the global uptake of these vaccines remains uneven. In regions where vaccination rates are low, efforts must focus on addressing vaccine hesitancy, improving public awareness, and expanding access. Achieving widespread vaccination coverage could lead to a substantial reduction in HPV related HNCs, especially among future generations.
Future research should aim to elucidate the full spectrum of HPV’s role in less common HNC subtypes, such as laryngeal, hypopharyngeal, sinonasal, nasopharyngeal, and salivary gland cancers. Investigating the molecular and immune mechanisms underlying the differential behavior of HPV related tumors in these sites will provide valuable insights for developing more targeted and personalized therapeutic approaches. Additionally, studies exploring the integration of epigenetic alterations and non-coding RNA profiles into clinical practice could offer new biomarkers for risk stratification and prognosis.
In conclusion, continued advancements in the understanding of HPV related head and neck cancers are essential for improving prevention, early diagnosis, and treatment strategies. Collaborative efforts between researchers, healthcare providers, and policymakers are crucial to fully realize the potential of HPV vaccines and innovative therapies in reducing the global burden of these cancers. With sustained research and public health initiatives, there is hope for better clinical outcomes and enhanced quality of life for patients affected by HPV related HNCs.
Funding
The authors received no extramural funding for the study.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Abbreviations
The following abbreviations are used in this manuscript:
| HNCs | Head and neck cancers |
| 9vHPV | 9-valent HPV vaccine |
| CDK | Cyclin-dependent kinase |
| circRNAs | Circular RNAs |
| CRT | Chemoradiotherapy |
| CTCF | CCCTC-binding factor |
| ctDNA | Circulating tumor DNA |
| E2BS | E2 binding sites |
| FDA | Food and Drug Administration |
| HNSCCs | Head and neck squamous cell carcinomas |
| HPSCC | Hypopharyngeal squamous cell carcinoma |
| HPV | Human papillomavirus |
| HPV+NPC | HPV related nasopharyngeal carcinoma |
| ICIs | Immune checkpoint inhibitors |
| IMPT | Intensity-modulated proton therapy |
| ISH | In situ hybridization |
| LCR | The long control region |
| lncRNAs | Long non-coding RNAs |
| LSCC | Laryngeal squamous cell carcinoma |
| me | Methylation |
| miRNAs | MicroRNAs |
| MRD | Minimal residual disease |
| NCDB | National Cancer Database |
| ncRNAs | Non-coding RNAs |
| NGS | Next-generation sequencing |
| OPC | Oropharyngeal cancers |
| OPSCC | Oropharyngeal squamous cell carcinoma |
| OSCC | Oral squamous cell carcinoma |
| PCR | Polymerase chain reaction |
| PFS | Progression-free survival |
| pRb | Retinoblastoma protein |
| R/M HNSCC | Recurrent/metastatic head and neck squamous cell carcinoma |
| RT | Radiotherapy |
| SETD2 | SET-domain containing protein 2 |
| SIRT1 | Sirtuin1 |
| SNSCC | Sinonasal squamous cell carcinoma |
| TORS | Transoral Robotic Surgery |
| URR | Upstream regulatory region |
| VLPs | Virus-like particles |
| WHO | World Health Organization |
| WRN | Werner Syndrome Protein |
| YY1 | Yin Yang 1 |
References
- Anderson, G.; Ebadi, M.; Vo, K.; Novak, J.; Govindarajan, A.; Amini, A. An Updated Review on Head and Neck Cancer Treatment with Radiation Therapy. Cancers (Basel) 2021, 13, 4912. [Google Scholar] [CrossRef] [PubMed]
- Mody, M.D.; Rocco, J.W.; Yom, S.S.; Haddad, R.I.; Saba, N.F. Head and Neck Cancer. The Lancet 2021, 398, 2289–2299. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and Neck Cancers, Version 2. 2020. JNCCN Journal of the National Comprehensive Cancer Network 2020, 18, 873–898. [Google Scholar] [CrossRef] [PubMed]
- Gormley, M.; Creaney, G.; Schache, A.; Ingarfield, K.; Conway, D.I. Reviewing the Epidemiology of Head and Neck Cancer: Definitions, Trends and Risk Factors. Br Dent J 2022, 233, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.; Ebadi, M.; Vo, K.; Novak, J.; Govindarajan, A.; Amini, A. An Updated Review on Head and Neck Cancer Treatment with Radiation Therapy. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Menezes, F. dos S. ; Fernandes, G.A.; Antunes, J.L.F.; Villa, L.L.; Toporcov, T.N. Global Incidence Trends in Head and Neck Cancer for HPV-Related and -Unrelated Subsites: A Systematic Review of Population-Based Studies. Oral Oncol 2021, 115, 105177. [Google Scholar] [CrossRef] [PubMed]
- Oropharyngeal Cancer Treatment (PDQ®) - NCI.
- Stelzle, D.; Tanaka, L.F.; Lee, K.K.; Ibrahim Khalil, A.; Baussano, I.; Shah, A.S. V; McAllister, D.A.; Gottlieb, S.L.; Klug, S.J.; Winkler, A.S.; et al. Estimates of the Global Burden of Cervical Cancer Associated with HIV. Lancet Glob Health 2021, 9, e161–e169. [Google Scholar] [CrossRef] [PubMed]
- Cosper, P.F.; Bradley, S.; Luo, Q.; Kimple, R.J. Biology of HPV Mediated Carcinogenesis and Tumor Progression. Semin Radiat Oncol 2021, 31, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Shu, X.; Xu, Q.; Zhu, C.; Kaufmann, A.M.; Zheng, Z.M.; Albers, A.E.; Qian, X. Current Status of Human Papillomavirus-Related Head and Neck Cancer: From Viral Genome to Patient Care. Virol Sin 2021, 36, 1284–1302. [Google Scholar] [CrossRef] [PubMed]
- Vats, A.; Trejo-Cerro, O.; Thomas, M.; Banks, L. Human Papillomavirus E6 and E7: What Remains? Tumour Virus Res 2021. [CrossRef] [PubMed]
- Marur, S.; D’Souza, G.; Westra, W.H.; Forastiere, A.A. HPV-Associated Head and Neck Cancer: A Virus-Related Cancer Epidemic. Lancet Oncol 2010, 11, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Yu, V.X.; Long, S.; Tassler, A. Smoking and Head and Neck Cancer. JAMA Otolaryngology–Head & Neck Surgery 2023, 149, 470. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Shu, X.; Xu, Q.; Zhu, C.; Kaufmann, A.M.; Zheng, Z.M.; Albers, A.E.; Qian, X. Current Status of Human Papillomavirus-Related Head and Neck Cancer: From Viral Genome to Patient Care. Virol Sin 2021, 36, 1284–1302. [Google Scholar] [CrossRef] [PubMed]
- Ndon, S.; Singh, A.; Ha, P.K.; Aswani, J.; Chan, J.Y.K.; Xu, M.J. Human Papillomavirus-Associated Oropharyngeal Cancer: Global Epidemiology and Public Policy Implications. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Vani, N. V.; Madhanagopal, R.; Swaminathan, R.; Ganesan, T.S. Dynamics of Oral Human Papillomavirus Infection in Healthy Population and Head and Neck Cancer. Cancer Med 2023, 12, 11731–11745. [Google Scholar] [CrossRef] [PubMed]
- Szymonowicz, K.A.; Chen, J. Biological and Clinical Aspects of HPV-Related Cancers. Cancer Biol Med 2020, 17, 864–878. [Google Scholar] [CrossRef] [PubMed]
- Clinical Characteristics of HPV Associated versus Non-HPV Associated Squamous Cell Carcinoma of the Head and Neck (HNSCC) Clinical Characteristics HPV Status; 2024.
- Mehanna, H.; Taberna, M.; von Buchwald, C.; Tous, S.; Brooks, J.; Mena, M.; Morey, F.; Grønhøj, C.; Rasmussen, J.H.; Garset-Zamani, M.; et al. Prognostic Implications of P16 and HPV Discordance in Oropharyngeal Cancer (HNCIG-EPIC-OPC): A Multicentre, Multinational, Individual Patient Data Analysis. Lancet Oncol 2023, 24, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Hisamatsu, K.; Suzui, N.; Hara, A.; Tomita, H.; Miyazaki, T. A Review of HPV-Related Head and Neck Cancer. J Clin Med 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Clinical Characteristics of HPV Associated versus Non-HPV Associated Squamous Cell Carcinoma of the Head and Neck (HNSCC) Clinical Characteristics HPV Status; 2024.
- Thompson, L.D.R. HPV-Related Multiphenotypic Sinonasal Carcinoma. Ear Nose Throat J 2020, 99, 94–95. [Google Scholar] [CrossRef] [PubMed]
- Balaji, D.; Kalarani, I.B.; Mohammed, V.; Veerabathiran, R. Potential Role of Human Papillomavirus Proteins Associated with the Development of Cancer. Virusdisease 2022, 33, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Burley, M.; Roberts, S.; Parish, J.L. Epigenetic Regulation of Human Papillomavirus Transcription in the Productive Virus Life Cycle. Semin Immunopathol 2020, 42, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Petca, A.; Borislavschi, A.; Zvanca, M.; Petca, R.-C.; Sandru, F.; Dumitrascu, M. Non-Sexual HPV Transmission and Role of Vaccination for a Better Future (Review). Exp Ther Med 2020, 20, 1–1. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-J.; Yang, A.; Wu, T.-C.; Hung, C.-F. Immunotherapy for Human Papillomavirus-Associated Disease and Cervical Cancer: Review of Clinical and Translational Research. J Gynecol Oncol 2016, 27. [Google Scholar] [CrossRef] [PubMed]
- Structure of Human Papillomavirus (HPV) LEAM Solution Fluorescence Microscope Epidemiology of Human Papillomavirus (HPV) Transmission of Human Papillomavirus (HPV) Replication of Human Papillomavirus (HPV) Pathogenesis of Human Papillomavirus (HPV) Clinical Manifestations of Human Papillomavirus (HPV) How You Can See Earth in a Whole New Light With These Insane Time-Lapses.
- Antonishyn, N.A. The Utility of Hpv Typing and Relative Quantification of HPV-16 Transcripts for Monitoring HPV Vaccine Efficacy and Improving Colposcopy Triage of Women with Abnormal Cervical Cyto; 2014.
- Ullah, M.I.; Mikhailova, M. V.; Alkhathami, A.G.; Carbajal, N.C.; Zuta, M.E.C.; Rasulova, I.; Najm, M.A.A.; Abosoda, M.; Alsalamy, A.; Deorari, M. Molecular Pathways in the Development of HPV-Induced Oropharyngeal Cancer. Cell Communication and Signaling 2023, 21, 351. [Google Scholar] [CrossRef] [PubMed]
- Ashrafi, G.H.; Salman, N.A. Pathogenesis of Human Papillomavirus – Immunological Responses to HPV Infection. In Human Papillomavirus - Research in a Global Perspective; InTech, 2016.
- Kombe Kombe, A.J.; Li, B.; Zahid, A.; Mengist, H.M.; Bounda, G.-A.; Zhou, Y.; Jin, T. Epidemiology and Burden of Human Papillomavirus and Related Diseases, Molecular Pathogenesis, and Vaccine Evaluation. Front Public Health 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- McBride, A.A.; Warburton, A. The Role of Integration in Oncogenic Progression of HPV-Associated Cancers. PLoS Pathog 2017, 13, e1006211. [Google Scholar] [CrossRef] [PubMed]
- Parfenov, M.; Pedamallu, C.S.; Gehlenborg, N.; Freeman, S.S.; Danilova, L.; Bristow, C.A.; Lee, S.; Hadjipanayis, A.G.; Ivanova, E. V.; Wilkerson, M.D.; et al. Characterization of HPV and Host Genome Interactions in Primary Head and Neck Cancers. Proc Natl Acad Sci U S A 2014, 111, 15544–15549. [Google Scholar] [CrossRef] [PubMed]
- Yeo-Teh, N.S.L.; Ito, Y.; Jha, S. High-Risk Human Papillomaviral Oncogenes E6 and E7 Target Key Cellular Pathways to Achieve Oncogenesis. Int J Mol Sci 2018, 19, 1706. [Google Scholar] [CrossRef] [PubMed]
- Ashrafi, G.H.; Tsirimonaki, E.; Marchetti, B.; O’Brien, P.M.; Sibbet, G.J.; Andrew, L.; Campo, M.S. Down-Regulation of MHC Class I by Bovine Papillomavirus E5 Oncoproteins. Oncogene 2002, 21, 248–259. [Google Scholar] [CrossRef] [PubMed]
- Faraji, F.; Zaidi, M.; Fakhry, C.; Gaykalova, D.A. Molecular Mechanisms of Human Papillomavirus-Related Carcinogenesis in Head and Neck Cancer. Microbes Infect 2017, 19, 464–475. [Google Scholar] [CrossRef] [PubMed]
- Vats, A.; Trejo-Cerro, O.; Thomas, M.; Banks, L. Human Papillomavirus E6 and E7: What Remains? Tumour Virus Res 2021, 11, 200213. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.W.; Lilie, H.; Kalbacher, H.; Roos, N.; Frecot, D.I.; Feige, M.; Conrady, M.; Votteler, T.; Cousido-Siah, A.; Bartoli, G.C.; et al. Evidence for Direct Interaction between the Oncogenic Proteins E6 and E7 of High-Risk Human Papillomavirus (HPV). Journal of Biological Chemistry 2023, 299. [Google Scholar] [CrossRef] [PubMed]
- Skelin, J.; Sabol, I.; Tomaić, V. Do or Die: HPV E5, E6 and E7 in Cell Death Evasion. Pathogens 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Cosper, P.F.; Bradley, S.; Luo, Q.; Kimple, R.J. Biology of HPV Mediated Carcinogenesis and Tumor Progression. Semin Radiat Oncol 2021, 31, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Mo, Y.; Ma, J.; Zhang, H.; Shen, J.; Chen, J.; Hong, J.; Xu, Y.; Qian, C. Prophylactic and Therapeutic HPV Vaccines: Current Scenario and Perspectives. Front Cell Infect Microbiol 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- McBride, A.A. Human Papillomaviruses: Diversity, Infection and Host Interactions. Nat Rev Microbiol 2022, 20, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Castro-Oropeza, R.; Piña-Sánchez, P. Epigenetic and Transcriptomic Regulation Landscape in HPV+ Cancers: Biological and Clinical Implications. Front Genet 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Groves, I.J.; Tang, G.; Pentland, I.; Parish, J.L.; Coleman, N. CTCF Association with Episomal HPV16 Genomes Regulates Viral 1 Oncogene Transcription and Splicing 2 3. [CrossRef]
- James, C.D.; Das, D.; Morgan, E.L.; Otoa, R.; Macdonald, A.; Morgan, I.M. Werner Syndrome Protein (WRN) Regulates Cell Proliferation and the Human Papillomavirus 16 Life Cycle during Epithelial Differentiation. mSphere 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Mac, M.; Moody, C.A. Epigenetic Regulation of the Human Papillomavirus Life Cycle. Pathogens 2020, 9, 483. [Google Scholar] [CrossRef] [PubMed]
- Mac, M.; DeVico, B.M.; Raspanti, S.M.; Moody, C.A. The SETD2 Methyltransferase Supports Productive HPV31 Replication through the LEDGF/CtIP/Rad51 Pathway. J Virol 2023, 97. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Kurokawa, T.; Mima, M.; Imamoto, S.; Mizokami, H.; Kondo, S.; Okamoto, Y.; Misawa, K.; Hanazawa, T.; Kaneda, A. DNA Methylation and HPV-Associated Head and Neck Cancer. Microorganisms 2021, 9, 801. [Google Scholar] [CrossRef] [PubMed]
- von Knebel Doeberitz, M.; Prigge, E.-S. Role of DNA Methylation in HPV Associated Lesions. Papillomavirus Research 2019, 7, 180–183. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.A.; Wentzensen, N.; Mirabello, L.; Ghosh, A.; Wacholder, S.; Harari, A.; Lorincz, A.; Schiffman, M.; Burk, R.D. Human Papillomavirus DNA Methylation as a Potential Biomarker for Cervical Cancer. Cancer Epidemiology, Biomarkers & Prevention 2012, 21, 2125–2137. [Google Scholar] [CrossRef] [PubMed]
- Yenigul, N.N.; Yazıcı Yılmaz, F.; Ayhan, I. Can Serum Vitamin B12 and Folate Levels Predict HPV Penetration in Patients with ASCUS? Nutr Cancer 2021, 73, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Casarotto, M.; Fanetti, G.; Guerrieri, R.; Palazzari, E.; Lupato, V.; Steffan, A.; Polesel, J.; Boscolo-Rizzo, P.; Fratta, E. Beyond MicroRNAs: Emerging Role of Other Non-Coding RNAs in HPV-Driven Cancers. Cancers (Basel) 2020, 12, 1246. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, P.; Borrelli, A.; Tuccillo, F.M.; Buonaguro, F.M.; Tornesello, M.L. The Role of CircRNAs in Human Papillomavirus (HPV)-Associated Cancers. Cancers (Basel) 2021, 13, 1173. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Munger, K. The Role of Long Noncoding RNAs in Human Papillomavirus-Associated Pathogenesis. Pathogens 2020, 9, 289. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Liu, F.; Yang, A.-G.; Wang, W.; Zhang, R. The Role of Long Non-Coding RNAs in the Pathogenesis of Head and Neck Squamous Cell Carcinoma. Mol Ther Oncolytics 2022, 24, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Dias, T.R.; Santos, J.M.O.; Gil da Costa, R.M.; Medeiros, R. Long Non-Coding RNAs Regulate the Hallmarks of Cancer in HPV-Induced Malignancies. Crit Rev Oncol Hematol 2021, 161, 103310. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Munger, K. Expression of the Cervical Carcinoma Expressed PCNA Regulatory (CCEPR) Long Noncoding RNA Is Driven by the Human Papillomavirus E6 Protein and Modulates Cell Proliferation Independent of PCNA. Virology 2018, 518, 8–13. [Google Scholar] [CrossRef]
- Barr, J.A.; Hayes, K.E.; Brownmiller, T.; Harold, A.D.; Jagannathan, R.; Lockman, P.R.; Khan, S.; Martinez, I. Long Non-Coding RNA FAM83H-AS1 Is Regulated by Human Papillomavirus 16 E6 Independently of P53 in Cervical Cancer Cells. Sci Rep 2019, 9, 3662. [Google Scholar] [CrossRef] [PubMed]
- Kopczyńska, M.; Kolenda, T.; Guglas, K.; Sobocińska, J.; Teresiak, A.; Bliźniak, R.; Mackiewicz, A.; Mackiewicz, J.; Lamperska, K. PRINS LncRNA Is a New Biomarker Candidate for HPV Infection and Prognosis of Head and Neck Squamous Cell Carcinomas. Diagnostics 2020, 10, 762. [Google Scholar] [CrossRef] [PubMed]
- Hinić, S.; Rich, A.; Anayannis, N. V.; Cabarcas-Petroski, S.; Schramm, L.; Meneses, P.I. Gene Expression and DNA Methylation in Human Papillomavirus Positive and Negative Head and Neck Squamous Cell Carcinomas. Int J Mol Sci 2022, 23, 10967. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Lian, Y.; Tao, H.; Zhao, Y.; Wang, Z.; Zhou, J.; Zhang, Z.; Jiang, S. Relationship between P16/Ki67 Immunoscores and PAX1/ZNF582 Methylation Status in Precancerous and Cancerous Cervical Lesions in High-Risk HPV-Positive Women. BMC Cancer 2024, 24, 1171. [Google Scholar] [CrossRef] [PubMed]
- Powell, S.F.; Vu, L.; Spanos, W.C.; Pyeon, D. The Key Differences between Human Papillomavirus-Positive and -Negative Head and Neck Cancers: Biological and Clinical Implications. Cancers (Basel) 2021, 13, 5206. [Google Scholar] [CrossRef] [PubMed]
- Batool, S.; Sethi, R.K.V.; Wang, A.; Dabekaussen, K.; Egloff, A.M.; Del Vecchio Fitz, C.; Kuperwasser, C.; Uppaluri, R.; Shin, J.; Rettig, E.M. Circulating Tumor-Tissue Modified HPV DNA Testing in the Clinical Evaluation of Patients at Risk for HPV-Positive Oropharynx Cancer: The IDEA-HPV Study. Oral Oncol 2023, 147, 106584. [Google Scholar] [CrossRef] [PubMed]
- Fahmy, M.D.; Clegg, D.; Belcastro, A.; Smith, B.D.; Eric Heidel, R.; Carlson, E.R.; Hechler, B. Are Throat Pain and Otalgia Predictive of Perineural Invasion in Squamous Cell Carcinoma of the Oropharynx? Journal of Oral and Maxillofacial Surgery 2022, 80, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Rajasekaran, K.; Carey, R.M.; Lin, X.; Seckar, T.D.; Wei, Z.; Chorath, K.; Newman, J.G.; O’Malley, B.W.; Weinstein, G.S.; Feldman, M.D.; et al. The Microbiome of HPV-Positive Tonsil Squamous Cell Carcinoma and Neck Metastasis. Oral Oncol 2021, 117, 105305. [Google Scholar] [CrossRef] [PubMed]
- Singhania, N.; Mishra, A. Alcohol Consumption, Tobacco Use, and Viral Infections: A Multifactorial Approach to Understanding Head and Neck Cancer Risk.
- McIlwain, W.R.; Sood, A.J.; Nguyen, S.A.; Day, T.A. Initial Symptoms in Patients With HPV-Positive and HPV-Negative Oropharyngeal Cancer. JAMA Otolaryngology–Head & Neck Surgery 2014, 140, 441. [Google Scholar] [CrossRef]
- Blitzer, G.C.; Smith, M.A.; Harris, S.L.; Kimple, R.J. Review of the Clinical and Biologic Aspects of Human Papillomavirus-Positive Squamous Cell Carcinomas of the Head and Neck. International Journal of Radiation Oncology*Biology*Physics 2014, 88, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Amaral, M.N.; Faísca, P.; Ferreira, H.A.; Gaspar, M.M.; Reis, C.P. Current Insights and Progress in the Clinical Management of Head and Neck Cancer. Cancers (Basel) 2022, 14, 6079. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; Koch, W.M.; Capone, R.B.; Spafford, M.; Westra, W.H.; Wu, L.; Zahurak, M.L.; Daniel, R.W.; Viglione, M.; Symer, D.E.; et al. Evidence for a Causal Association Between Human Papillomavirus and a Subset of Head and Neck Cancers.
- Simoens, C.; Gheit, T.; Ridder, R.; Gorbaslieva, I.; Holzinger, D.; Lucas, E.; Rehm, S.; Vermeulen, P.; Lammens, M.; Vanderveken, O.M.; et al. Accuracy of High-Risk HPV DNA PCR, P16(INK4a) Immunohistochemistry or the Combination of Both to Diagnose HPV-Driven Oropharyngeal Cancer. BMC Infect Dis 2022, 22, 676. [Google Scholar] [CrossRef] [PubMed]
- Gallus, R.; Nauta, I.H.; Marklund, L.; Rizzo, D.; Crescio, C.; Mureddu, L.; Tropiano, P.; Delogu, G.; Bussu, F. Accuracy of P16 IHC in Classifying HPV-Driven OPSCC in Different Populations. Cancers (Basel) 2023, 15, 656. [Google Scholar] [CrossRef] [PubMed]
- Cubilla, A.L.; Lloveras, B.; Alejo, M.; Clavero, O.; Chaux, A.; Kasamatsu, E.; Velazquez, E.F.; Lezcano, C.; Monfulleda, N.; Tous, S.; et al. The Basaloid Cell Is the Best Tissue Marker for Human Papillomavirus in Invasive Penile Squamous Cell Carcinoma: A Study of 202 Cases From Paraguay. American Journal of Surgical Pathology 2010, 34, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Oppel, F.; Gendreizig, S.; Martinez-Ruiz, L.; Florido, J.; López-Rodríguez, A.; Pabla, H.; Loganathan, L.; Hose, L.; Kühnel, P.; Schmidt, P.; et al. Mucosa-like Differentiation of Head and Neck Cancer Cells Is Inducible and Drives the Epigenetic Loss of Cell Malignancy. Cell Death Dis 2024, 15, 724. [Google Scholar] [CrossRef] [PubMed]
- Chaux, A.; Sanchez, D.F.; Fernández-Nestosa, M.J.; Cañete-Portillo, S.; Rodríguez, I.M.; Giannico, G.A.; Cubilla, A.L. The Dual Pathogenesis of Penile Neoplasia: The Heterogeneous Morphology of Human Papillomavirus-Related Tumors. Asian J Urol 2022, 9, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Baněčková, M.; Cox, D. Top 10 Basaloid Neoplasms of the Sinonasal Tract. Head Neck Pathol 2023, 17, 16–32. [Google Scholar] [CrossRef] [PubMed]
- Giorgi Rossi, P.; Carozzi, F.; Ronco, G.; Allia, E.; Bisanzi, S.; Gillio-Tos, A.; De Marco, L.; Rizzolo, R.; Gustinucci, D.; Del Mistro, A.; et al. P16/Ki67 and E6/E7 MRNA Accuracy and Prognostic Value in Triaging HPV DNA-Positive Women. JNCI: Journal of the National Cancer Institute 2021, 113, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Giorgi Rossi, P.; Ronco, G.; Mancuso, P.; Carozzi, F.; Allia, E.; Bisanzi, S.; Gillio-Tos, A.; De Marco, L.; Rizzolo, R.; Gustinucci, D.; et al. Performance of <scp>HPV E6</Scp> / <scp>E7 MRNA</Scp> Assay as Primary Screening Test: Results from the <scp>NTCC2</Scp> Trial. Int J Cancer 2022, 151, 1047–1058. [Google Scholar] [CrossRef] [PubMed]
- Suresh, K.; Shah, P. V.; Coates, S.; Alexiev, B.A.; Samant, S. In Situ Hybridization for High Risk HPV E6/E7 MRNA in Oropharyngeal Squamous Cell Carcinoma. Am J Otolaryngol 2021, 42, 102782. [Google Scholar] [CrossRef] [PubMed]
- Klussmann, J.P.; Gültekin, E.; Weissenborn, S.J.; Wieland, U.; Dries, V.; Dienes, H.P.; Eckel, H.E.; Pfister, H.J.; Fuchs, P.G. Expression of P16 Protein Identifies a Distinct Entity of Tonsillar Carcinomas Associated with Human Papillomavirus. Am J Pathol 2003, 162, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Blons, H.; Laurent-Puig, P. TP53 and Head and Neck Neoplasms. Hum Mutat 2003, 21, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Qin, T.; Li, S.; Henry, L.E.; Liu, S.; Sartor, M.A. Molecular Tumor Subtypes of HPV-Positive Head and Neck Cancers: Biological Characteristics and Implications for Clinical Outcomes. Cancers (Basel) 2021, 13, 2721. [Google Scholar] [CrossRef] [PubMed]
- Krsek, A.; Baticic, L.; Braut, T.; Sotosek, V. The Next Chapter in Cancer Diagnostics: Advances in HPV-Positive Head and Neck Cancer. Biomolecules 2024, 14. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.H.; Sais, D.; Tran, N. Advances in Human Papillomavirus Detection and Molecular Understanding in Head and Neck Cancers: Implications for Clinical Management. J Med Virol 2024, 96. [Google Scholar] [CrossRef] [PubMed]
- Kocjan, B.J.; Bzhalava, D.; Forslund, O.; Dillner, J.; Poljak, M. Molecular Methods for Identification and Characterization of Novel Papillomaviruses. Clinical Microbiology and Infection 2015, 21, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Chantre-Justino, M.; Alves, G.; Delmonico, L. Clinical Applications of Liquid Biopsy in HPV-negative and HPV-positive Head and Neck Squamous Cell Carcinoma: Advances and Challenges. Explor Target Antitumor Ther 2022, 533–552. [Google Scholar] [CrossRef] [PubMed]
- Eberly, H.W.; Sciscent, B.Y.; Lorenz, F.J.; Rettig, E.M.; Goyal, N. Current and Emerging Diagnostic, Prognostic, and Predictive Biomarkers in Head and Neck Cancer. Biomedicines 2024, 12, 415. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Tjoa, T.; Armstrong, W.B. Circulating Tumor <scp>HPV</Scp> - <scp>DNA</Scp> in the Management of <scp>HPV</Scp> -Positive Oropharyngeal Carcinoma: A Systematic Review. Head Neck 2025. [CrossRef]
- Reid, P.; Marcu, L.G.; Olver, I.; Moghaddasi, L.; Staudacher, A.H.; Bezak, E. Diversity of Cancer Stem Cells in Head and Neck Carcinomas: The Role of HPV in Cancer Stem Cell Heterogeneity, Plasticity and Treatment Response. Radiotherapy and Oncology 2019, 135, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Keck, M.K.; Zuo, Z.; Khattri, A.; Stricker, T.P.; Brown, C.D.; Imanguli, M.; Rieke, D.; Endhardt, K.; Fang, P.; Brägelmann, J.; et al. Integrative Analysis of Head and Neck Cancer Identifies Two Biologically Distinct HPV and Three Non-HPV Subtypes. Clinical Cancer Research 2015, 21, 870–881. [Google Scholar] [CrossRef] [PubMed]
- Schindele, A.; Holm, A.; Nylander, K.; Allard, A.; Olofsson, K. Mapping Human Papillomavirus, Epstein–Barr Virus, Cytomegalovirus, Adenovirus, and P16 in Laryngeal Cancer. Discover Oncology 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Lauritzen, B.B.; Sjöstedt, S.; Jensen, J.M.; Kiss, K.; von Buchwald, C. Unusual Cases of Sinonasal Malignancies: A Letter to the Editor on HPV-Positive Sinonasal Squamous Cell Carcinomas. Acta Oncol (Madr) 2023, 62, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Vojtechova, Z.; Sabol, I.; Salakova, M.; Smahelova, J.; Zavadil, J.; Turek, L.; Grega, M.; Klozar, J.; Prochazka, B.; Tachezy, R. Comparison of the MiRNA Profiles in HPV-Positive and HPV-Negative Tonsillar Tumors and a Model System of Human Keratinocyte Clones. BMC Cancer 2016, 16, 382. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, S.; Sharma, P.; Wise, P.; Sposto, R.; Hollingshead, D.; Lamb, J.; Lang, S.; Fabbri, M.; Whiteside, T.L. MRNA and MiRNA Profiles of Exosomes from Cultured Tumor Cells Reveal Biomarkers Specific for HPV16-Positive and HPV16-Negative Head and Neck Cancer. Int J Mol Sci 2020, 21, 8570. [Google Scholar] [CrossRef] [PubMed]
- Sannigrahi, M.K.; Sharma, R.; Singh, V.; Panda, N.K.; Rattan, V.; Khullar, M. DNA Methylation Regulated MicroRNAs in HPV-16-Induced Head and Neck Squamous Cell Carcinoma (HNSCC). Mol Cell Biochem 2018, 448, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Wang, Z.; Qiu, S.; Wang, R. Therapeutic Strategies of Different HPV Status in Head and Neck Squamous Cell Carcinoma. Int J Biol Sci 2021, 17, 1104–1118. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-Associated Oropharyngeal Cancer: Epidemiology, Molecular Biology and Clinical Management. Nat Rev Clin Oncol 2022, 19, 306–327. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M. De-Escalation Treatment for Human Papillomavirus–Related Oropharyngeal Cancer: Questions for Practical Consideration. Cancer Network 2023.
- Nissi, L. P16 AND XCT AS BIOMARKERS IN OROPHARYNGEAL SQUAMOUS CELL CARCINOMA AND BEYOND.
- García-Anaya, M.; Segado-Guillot, S.; Cabrera-Rodríguez, J.; Toledo-Serrano, M.; Medina-Carmona, J.; Gómez-Millán, J. Dose and Volume De-Escalation of Radiotherapy in Head and Neck Cancer. Crit Rev Oncol Hematol 2023, 186, 103994. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.J.; Vokes, E.E. Optimizing Treatment De-Escalation in Head and Neck Cancer: Current and Future Perspectives. Oncologist 2021, 26, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Rahman, Md.T.; Ghosh, A.K.; Khatun, R.A.; Hussain, Q.M.; Mollah, Md.N.U.; Hussain, S.Md.A.; Habib, A.K.M.A.; Hosen, M.M.A.; Rahim, I.U. Comparison of Outcome of Concurrent Chemoradiotherapy and Sequential Chemoradiotherapy in Locally Advanced, Inoperable Squamous Cell Carcinoma of Head and Neck Region. Saudi Journal of Medical and Pharmaceutical Sciences 2024, 10, 293–300. [Google Scholar] [CrossRef]
- Wong, S.J.; Torres-Saavedra, P.A.; Saba, N.F.; Shenouda, G.; Bumpous, J.M.; Wallace, R.E.; Chung, C.H.; El-Naggar, A.K.; Gwede, C.K.; Burtness, B.; et al. Radiotherapy Plus Cisplatin With or Without Lapatinib for Non–Human Papillomavirus Head and Neck Carcinoma. JAMA Oncol 2023, 9, 1565. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Wang, Z.; Qiu, S.; Wang, R. Therapeutic Strategies of Different HPV Status in Head and Neck Squamous Cell Carcinoma. Int J Biol Sci 2021, 17, 1104–1118. [Google Scholar] [CrossRef] [PubMed]
- Lassen, P.; Huang, S.H.; Su, J.; Waldron, J.; Andersen, M.; Primdahl, H.; Johansen, J.; Kristensen, C.A.; Andersen, E.; Eriksen, J.G.; et al. Treatment Outcomes and Survival Following Definitive (Chemo)Radiotherapy in <scp>HPV</Scp> -positive Oropharynx Cancer: Large-scale Comparison of <scp>DAHANCA</Scp> vs <scp>PMH</Scp> Cohorts. Int J Cancer 2022, 150, 1329–1340. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, A.J.; Herberg, M.; Strohl, M.; Ochoa, E.; Feng, A.L.; Abt, N.B.; Mokhtari, T.E.; Suresh, K.; McHugh, C.I.; Parikh, A.S.; et al. Impact of Surgical Margins on Local Control in Patients Undergoing <scp>single-modality</Scp> Transoral Robotic Surgery for <scp>HPV-related</Scp> Oropharyngeal Squamous Cell Carcinoma. Head Neck 2021, 43, 2434–2444. [Google Scholar] [CrossRef] [PubMed]
- Goel, S.; Gunasekera, D.; Krishnan, G.; Krishnan, S.; Hodge, J.; Lizarondo, L.; Foreman, A. Is Transoral Robotic Surgery Useful as a Salvage Technique in Head and Neck Cancers: A Systematic Review and Meta Analysis. Head Neck 2024. [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab Alone or with Chemotherapy versus Cetuximab with Chemotherapy for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck (KEYNOTE-048): A Randomised, Open-Label, Phase 3 Study. The Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef] [PubMed]
- Saba, N.F.; Pamulapati, S.; Patel, B.; Mody, M.; Strojan, P.; Takes, R.; Mäkitie, A.A.; Cohen, O.; Pace-Asciak, P.; Vermorken, J.B.; et al. Novel Immunotherapeutic Approaches to Treating HPV-Related Head and Neck Cancer. Cancers (Basel) 2023, 15, 1959. [Google Scholar] [CrossRef] [PubMed]
- Powell, S.F.; Liu, S. V.; Sukari, A.; Chung, C.H.; Bauml, J.; Haddad, R.I.; Gause, C.K.; Niewood, M.; Gammage, L.L.; Brown, H.; et al. KEYNOTE-055: A Phase II Trial of Single Agent Pembrolizumab in Patients (Pts) with Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma (HNSCC) Who Have Failed Platinum and Cetuximab. Journal of Clinical Oncology 2015, 33, TPS3094–TPS3094. [Google Scholar] [CrossRef]
- Muro, K.; Chung, H.C.; Shankaran, V.; Geva, R.; Catenacci, D.; Gupta, S.; Eder, J.P.; Golan, T.; Le, D.T.; Burtness, B.; et al. Pembrolizumab for Patients with PD-L1-Positive Advanced Gastric Cancer (KEYNOTE-012): A Multicentre, Open-Label, Phase 1b Trial. Lancet Oncol 2016, 17, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, N.G.; Evangelopoulos, A.; Kounatidis, D.; Panagopoulos, F.; Geladari, E.; Karampela, I.; Stratigou, T.; Dalamaga, M. Immunotherapy in Head and Neck Cancer: Where Do We Stand? Curr Oncol Rep 2023, 25, 897–912. [Google Scholar] [CrossRef] [PubMed]
- Julian, R.; Savani, M.; Bauman, J.E. Immunotherapy Approaches in HPV-Associated Head and Neck Cancer. Cancers (Basel) 2021, 13, 5889. [Google Scholar] [CrossRef] [PubMed]
- Pereira, D.; Martins, D.; Mendes, F. Immunotherapy in Head and Neck Cancer When, How, and Why? Biomedicines 2022, 10, 2151. [Google Scholar] [CrossRef] [PubMed]
- Shamseddine, A.A.; Burman, B.; Lee, N.Y.; Zamarin, D.; Riaz, N. Tumor Immunity and Immunotherapy for HPV-Related Cancers. Cancer Discov 2021, 11, 1896–1912. [Google Scholar] [CrossRef] [PubMed]
- A Phase 1 Dose-Escalation and Expansion Study of CUE-101, given as Monotherapy and in Combination with Pembrolizumab, in Patients with Recurrent:Metastatic HPV16+ Head and Neck Squamous Cell Cancer (R:M HNSCC).
- Ho, A.L.; Nabell, L.; Neupane, P.C.; Posner, M.R.; Yilmaz, E.; Niu, J.; Naqash, A.R.; Pearson, A.T.; Wong, S.J.; Nieva, J.J.; et al. HB-200 Arenavirus-Based Immunotherapy plus Pembrolizumab as First-Line Treat-Ment of Patients with Recurrent/Metastatic HPV16-Positive Head and Neck Cancer: Updated Results; 2025.
- Rosenberg, A.J.; Juloori, A.; Izumchenko, E.; Cursio, J.; Gooi, Z.; Blair, E.A.; Lingen, M.W.; Cipriani, N.; Hasina, R.; Starus, A.; et al. Neoadjuvant HPV16-Specific Arenavirus-Based Immunotherapy HB-200 plus Chemotherapy Followed by Response-Stratified de-Intensification in HPV16+ Oro-Pharyngeal Cancer: TARGET-HPV; 2025.
- Yan, S.; Chen, S.; Zhang, X.; Hu, W.; Li, H.; Ma, Y.; Han, L.; Zhang, S.; Wang, J.; Zhang, J.; et al. Neoadjuvant Sintilimab and Platinum-Doublet Chemotherapy Followed by Transoral Robotic Surgery for HPV-Associated Resectable Oropharyngeal Cancer: Single-Arm, Phase II Trial; 2025.
- Chung, C.H.; Li, J.; Steuer, C.E.; Bhateja, P.; Johnson, M.; Masannat, J.; Poole, M.I.; Song, F.; Hernandez-Prera, J.C.; Molina, H.; et al. Phase II Multi-Institutional Clinical Trial Result of Concurrent Cetuximab and Nivolumab in Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma. Clinical Cancer Research 2022, 28, 2329–2338. [Google Scholar] [CrossRef] [PubMed]
- Results of a Randomized, Double-Blind, Placebo-Controlled, Phase 2 Study (OpcemISA) of the Combination of ISA101b and Cemiplimab versus Cemiplimab for Recurrent:Metastatic (R:M) HPV16-Positive Oropharyngeal Cancer (OPC).
- Li, Q.; Tie, Y.; Alu, A.; Ma, X.; Shi, H. Targeted Therapy for Head and Neck Cancer: Signaling Pathways and Clinical Studies. Signal Transduct Target Ther 2023, 8, 31. [Google Scholar] [CrossRef] [PubMed]
- Aguayo, F.; Perez-Dominguez, F.; Osorio, J.C.; Oliva, C.; Calaf, G.M. PI3K/AKT/MTOR Signaling Pathway in HPV-Driven Head and Neck Carcinogenesis: Therapeutic Implications. Biology (Basel) 2023, 12, 672. [Google Scholar] [CrossRef] [PubMed]
- Aguayo, F.; Perez-Dominguez, F.; Osorio, J.C.; Oliva, C.; Calaf, G.M. PI3K/AKT/MTOR Signaling Pathway in HPV-Driven Head and Neck Carcinogenesis: Therapeutic Implications. Biology (Basel) 2023, 12, 672. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.Y.; Sherman, E.J.; Schöder, H.; Wray, R.; White, C.; Dunn, L.; Hung, T.; Pfister, D.G.; Ho, A.L.; Mcbride, S.M.; et al. Intra-Treatment Hypoxia Directed Major Radiation de-Escalation as Definitive Treatment for Human Papillomavirus-Related Oropharyngeal Cancer; 2025.
- Burtness, B.; Flamand, Y.; Quon, H.; Weinstein, G.S.; Mehra, R.; Garcia, J.J.; Kim, S.; O, B.W.; Jr, malley; Ozer, E.; et al. Long-Term Follow up of E3311, a Phase II Trial of Transoral Surgery (TOS) Followed by Pathology-Based Adjuvant Treatment in HPV-Associated (HPV+) Oropharynx Cancer (OPC): A Trial of the ECOG-ACRIN Cancer Research Group; 2025.
- Frank, S.J.; Busse, P.; Ira Rosenthal, D.; Hernandez, M.; Michael Swanson, D.; Garden, A.S.; Sturgis, E.M.; Ferrarotto, R.; Brandon Gunn, G.; Patel, S.H.; et al. Phase III Randomized Trial of Intensity-Modulated Proton Therapy (IMPT) versus Intensity-Modulated Photon Therapy (IMRT) for the Treatment of Head and Neck Oropharyngeal Carcinoma (OPC); 2025.
- Hirayama, S.; Al-Inaya, Y.; Aye, L.; Bryan, M.E.; Das, D.; Mendel, J.; Naegele, S.; Faquin, W.C.; Sadow, P.; Fisch, A.S.; et al. Prospective Validation of CtHPVDNA for Detection of Minimal Residual Disease and Prediction of Recurrence in Patients with HPV-Associated Head and Neck Cancer Treated with Surgery; 2025.
- Wei, Y.; Zhao, Z.; Ma, X. Description of CRISPR-Cas9 Development and Its Prospects in Human Papillomavirus-Driven Cancer Treatment. Front Immunol 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Zhen, S.; Lu, J.; Liu, Y.H.; Chen, W.; Li, X. Synergistic Antitumor Effect on Cervical Cancer by Rational Combination of PD1 Blockade and CRISPR-Cas9-Mediated HPV Knockout. Cancer Gene Ther 2020, 27, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Jiang, H.; Wang, T.; He, D.; Tian, R.; Cui, Z.; Tian, X.; Gao, Q.; Ma, X.; Yang, J.; et al. In Vitro and in Vivo Growth Inhibition of Human Cervical Cancer Cells via Human Papillomavirus E6/E7 MRNAs’ Cleavage by CRISPR/Cas13a System. Antiviral Res 2020, 178. [Google Scholar] [CrossRef] [PubMed]
- Nagarsheth, N.B.; Norberg, S.M.; Sinkoe, A.L.; Adhikary, S.; Meyer, T.J.; Lack, J.B.; Warner, A.C.; Schweitzer, C.; Doran, S.L.; Korrapati, S.; et al. TCR-Engineered T Cells Targeting E7 for Patients with Metastatic HPV-Associated Epithelial Cancers. Nat Med 2021, 27, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Sandberg, M.L.; Martin, A.D.; Negri, K.R.; Gabrelow, G.B.; Nampe, D.P.; Wu, M.-L.; McElvain, M.E.; Toledo Warshaviak, D.; Lee, W.-H.; et al. Potent, Selective CARs as Potential T-Cell Therapeutics for HPV-Positive Cancers. Journal of Immunotherapy 2021, 44, 292–306. [Google Scholar] [CrossRef] [PubMed]
- Sharkey Ochoa, I.; O’Regan, E.; Toner, M.; Kay, E.; Faul, P.; O’Keane, C.; O’Connor, R.; Mullen, D.; Nur, M.; O’Murchu, E.; et al. The Role of HPV in Determining Treatment, Survival, and Prognosis of Head and Neck Squamous Cell Carcinoma. Cancers (Basel) 2022, 14, 4321. [Google Scholar] [CrossRef] [PubMed]
- Šimić, I.; Božinović, K.; Milutin Gašperov, N.; Kordić, M.; Pešut, E.; Manojlović, L.; Grce, M.; Dediol, E.; Sabol, I. Head and Neck Cancer Patients’ Survival According to HPV Status, MiRNA Profiling, and Tumour Features—A Cohort Study. Int J Mol Sci 2023, 24, 3344. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.-H.; Su, C.-C.; Wu, S.-Y.; Hsueh, W.-T.; Wu, Y.-H.; Chen, H.H.W.; Hsiao, J.-R.; Liu, C.-H.; Tsai, Y.-S. Impact of Alcohol and Smoking on Outcomes of HPV-Related Oropharyngeal Cancer. J Clin Med 2022, 11, 6510. [Google Scholar] [CrossRef] [PubMed]
- de Roest, R.H.; van der Heijden, M.; Wesseling, F.W.R.; de Ruiter, E.J.; Heymans, M.W.; Terhaard, C.; Vergeer, M.R.; Buter, J.; Devriese, L.A.; de Boer, J.P.; et al. Disease Outcome and Associated Factors after Definitive Platinum Based Chemoradiotherapy for Advanced Stage HPV-Negative Head and Neck Cancer. Radiotherapy and Oncology 2022, 175, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Wang, Z.; Qiu, S.; Wang, R. Therapeutic Strategies of Different HPV Status in Head and Neck Squamous Cell Carcinoma. Int J Biol Sci 2021, 17, 1104–1118. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.Z.; Jou, J.; Cohen, E. Vaccine Strategies for Human Papillomavirus-Associated Head and Neck Cancers. Cancers (Basel) 2021, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- St. Laurent, J.; Luckett, R.; Feldman, S. HPV Vaccination and the Effects on Rates of HPV-Related Cancers. Curr Probl Cancer 2018, 42, 493–506. [CrossRef] [PubMed]
- Malagón, T.; Franco, E.L.; Tejada, R.; Vaccarella, S. Epidemiology of HPV-Associated Cancers Past, Present and Future: Towards Prevention and Elimination. Nat Rev Clin Oncol 2024, 21, 522–538. [Google Scholar] [CrossRef] [PubMed]
- Petca, A.; Borislavschi, A.; Zvanca, M.; Petca, R.-C.; Sandru, F.; Dumitrascu, M. Non-Sexual HPV Transmission and Role of Vaccination for a Better Future (Review). Exp Ther Med 2020, 20, 1–1. [Google Scholar] [CrossRef] [PubMed]
- Du, E.Y.; Adjei Boakye, E.; Taylor, D.B.; Kuziez, D.; Rohde, R.L.; Pannu, J.S.; Simpson, M.C.; Patterson, R.H.; Varvares, M.A.; Osazuwa-Peters, N. Medical Students’ Knowledge of HPV, HPV Vaccine, and HPV-Associated Head and Neck Cancer. Hum Vaccin Immunother 2022, 18. [Google Scholar] [CrossRef] [PubMed]
- Porras, C.; Tsang, S.H.; Herrero, R.; Guillén, D.; Darragh, T.M.; Stoler, M.H.; Hildesheim, A.; Wagner, S.; Boland, J.; Lowy, D.R.; et al. Efficacy of the Bivalent HPV Vaccine against HPV 16/18-Associated Precancer: Long-Term Follow-up Results from the Costa Rica Vaccine Trial. Lancet Oncol 2020, 21, 1643–1652. [Google Scholar] [CrossRef] [PubMed]
- Gribb, J.P.; Wheelock, J.H.; Park, E.S. Human Papilloma Virus (HPV) and the Current State of Oropharyngeal Cancer Prevention and Treatment. Dela J Public Health 2023, 9, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Roy, V.; Jung, W.; Linde, C.; Coates, E.; Ledgerwood, J.; Costner, P.; Yamshchikov, G.; Streeck, H.; Juelg, B.; Lauffenburger, D.A.; et al. Differences in HPV-Specific Antibody Fc-Effector Functions Following Gardasil® and Cervarix® Vaccination. NPJ Vaccines 2023, 8, 39. [Google Scholar] [CrossRef] [PubMed]
- Human Papillomavirus Vaccination INTRODUCTION.
- Rumfield, C.S.; Roller, N.; Pellom, S.T.; Schlom, J.; Jochems, C. Therapeutic Vaccines for HPV-Associated Malignancies. Immunotargets Ther 2020, 9, 167–200. [Google Scholar] [CrossRef] [PubMed]
- Boilesen, D.R.; Nielsen, K.N.; Holst, P.J. Novel Antigenic Targets of HPV Therapeutic Vaccines. Vaccines (Basel) 2021, 9, 1262. [Google Scholar] [CrossRef] [PubMed]
- Gardella, B.; Gritti, A.; Soleymaninejadian, E.; Pasquali, M.; Riemma, G.; La Verde, M.; Schettino, M.; Fortunato, N.; Torella, M.; Dominoni, M. New Perspectives in Therapeutic Vaccines for HPV: A Critical Review. Medicina (B Aires) 2022, 58, 860. [Google Scholar] [CrossRef] [PubMed]
- Yan, F.; Cowell, L.G.; Tomkies, A.; Day, A.T. Therapeutic Vaccination for HPV-Mediated Cancers. Curr Otorhinolaryngol Rep 2023, 11, 44–61. [Google Scholar] [CrossRef] [PubMed]
- Skolnik, J.M.; Morrow, M.P. Vaccines for HPV-Associated Diseases. Mol Aspects Med 2023, 94, 101224. [Google Scholar] [CrossRef] [PubMed]
- Diana, G.; Corica, C. Human Papilloma Virus Vaccine and Prevention of Head and Neck Cancer, What Is the Current Evidence? Oral Oncol 2021, 115, 105168. [Google Scholar] [CrossRef] [PubMed]
- Ndon, S.; Singh, A.; Ha, P.K.; Aswani, J.; Chan, J.Y.-K.; Xu, M.J. Human Papillomavirus-Associated Oropharyngeal Cancer: Global Epidemiology and Public Policy Implications. Cancers (Basel) 2023, 15, 4080. [Google Scholar] [CrossRef] [PubMed]
- Timbang, M.R.; Sim, M.W.; Bewley, A.F.; Farwell, D.G.; Mantravadi, A.; Moore, M.G. HPV-Related Oropharyngeal Cancer: A Review on Burden of the Disease and Opportunities for Prevention and Early Detection. Hum Vaccin Immunother 2019, 15, 1920–1928. [Google Scholar] [CrossRef] [PubMed]
- Diana, G.; Corica, C. Human Papilloma Virus Vaccine and Prevention of Head and Neck Cancer, What Is the Current Evidence? Oral Oncol 2021, 115, 105168. [Google Scholar] [CrossRef] [PubMed]
- Weekly Epidemiological Record Relevé Épidémiologique Hebdomadaire Sommaire.
- Morand, G.B.; Cardona, I.; Cruz, S.B.S.C.; Mlynarek, A.M.; Hier, M.P.; Alaoui-Jamali, M.A.; da Silva, S.D. Therapeutic Vaccines for HPV-Associated Oropharyngeal and Cervical Cancer: The Next De-Intensification Strategy? Int J Mol Sci 2022, 23, 8395. [Google Scholar] [CrossRef] [PubMed]
- Tsentemeidou, A.; Fyrmpas, G.; Stavrakas, M.; Vlachtsis, K.; Sotiriou, E.; Poutoglidis, A.; Tsetsos, N. Human Papillomavirus Vaccine to End Oropharyngeal Cancer. A Systematic Review and Meta-Analysis. Sex Transm Dis 2021, 48, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Tsu, V.D.; LaMontagne, D.S.; Atuhebwe, P.; Bloem, P.N.; Ndiaye, C. National Implementation of HPV Vaccination Programs in Low-Resource Countries: Lessons, Challenges, and Future Prospects. Prev Med (Baltim) 2021, 144. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Jiang, Y.; Wang, Q.; Lai, Y.M.; Holloway, A. The Status and Challenges of HPV Vaccine Programme in China: An Exploration of the Related Policy Obstacles. BMJ Glob Health 2023, 8. [Google Scholar] [CrossRef] [PubMed]
- Karanja-Chege, C.M. HPV Vaccination in Kenya: The Challenges Faced and Strategies to Increase Uptake. Front Public Health 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Casey, R.M.; Adrien, N.; Badiane, O.; Diallo, A.; Loko Roka, J.; Brennan, T.; Doshi, R.; Garon, J.; Loharikar, A. National Introduction of HPV Vaccination in Senegal—Successes, Challenges, and Lessons Learned. Vaccine 2022, 40, A10–A16. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Xie, X.; Liu, J.; Qiao, Y.; Zhao, F.; Wu, T.; Zhang, J.; Ma, D.; Kong, B.; Chen, W.; et al. Elimination of Cervical Cancer: Challenges Promoting the HPV Vaccine in China. Indian J Gynecol Oncol 2021, 19. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, J.; Yücel, M.; Kızılkaya, S.; Yıldırım, G.; Özyiğit, I.İ.; Yuluğkural, Z. HPV, HPV VACCINATION WORLDWIDE AND CURRENT STATUS OF HPV VACCINATION IN TURKEY: A LITERATURE REVIEW. TURKISH MEDICAL STUDENT JOURNAL 2022, 9, 48–54. [Google Scholar] [CrossRef]
- Agadayi, E.; Karademir, D.; Karahan, S. Knowledge, Attitudes and Behaviors of Women Who Have or Have Not Had Human Papillomavirus Vaccine in Turkey about the Virus and the Vaccine. J Community Health 2022, 47, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Waheed, D. e. N.; Schiller, J.; Stanley, M.; Franco, E.L.; Poljak, M.; Kjaer, S.K.; del Pino, M.; van der Klis, F.; Schim van der Loeff, M.F.; Baay, M.; et al. Human Papillomavirus Vaccination in Adults: Impact, Opportunities and Challenges – a Meeting Report. In Proceedings of the BMC Proceedings; BioMed Central Ltd, August 1 2021; Vol. 15.
- Osazuwa-Peters, N.; Graboyes, E.M.; Khariwala, S.S. Expanding Indications for the Human Papillomavirus Vaccine: One Small Step for the Prevention of Head and Neck Cancer, but One Giant Leap Remains. JAMA Otolaryngol Head Neck Surg 2020, 146, 1099–1101. [Google Scholar] [CrossRef] [PubMed]
- Dilley, S.; Miller, K.M.; Huh, W.K. Human Papillomavirus Vaccination: Ongoing Challenges and Future Directions. Gynecol Oncol 2020, 156, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Nogueira-Rodrigues, A.; Flores, M.G.; Macedo Neto, A.O.; Braga, L.A.C.; Vieira, C.M.; Sousa-Lima, R.M. de; de Andrade, D.A.P.; Machado, K.K.; Guimarães, A.P.G. HPV Vaccination in Latin America: Coverage Status, Implementation Challenges and Strategies to Overcome It. Front Oncol 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Erbıyık, H.I.; Palalıoğlu, R.M. HPV Infection, HPV Vaccines and Cervical Cancer Awareness: A Multi-Centric Survey Study in Istanbul, Turkey. Women Health 2021, 61, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Taberna, M.; Mena, M.; Pavón, M.A.; Alemany, L.; Gillison, M.L.; Mesía, R. Human Papillomavirus-Related Oropharyngeal Cancer. Annals of Oncology 2017, 28, 2386–2398. [Google Scholar] [CrossRef] [PubMed]
- Gribb, J.P.; Wheelock, J.H.; Park, E.S. Human Papilloma Virus (HPV) and the Current State of Oropharyngeal Cancer Prevention and Treatment. Dela J Public Health 2023, 9. [Google Scholar] [CrossRef] [PubMed]
- Weeramange, C.E.; Tang, K.D.; Irwin, D.; Hartel, G.; Langton-Lockton, J.; Ladwa, R.; Kenny, L.; Taheri, T.; Whitfield, B.; Vasani, S.; et al. Human Papillomavirus (HPV) DNA Methylation Changes in HPV-Associated Head and Neck Cancer. Carcinogenesis 2024, 45, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Wookey, V.B.; Appiah, A.K.; Kallam, A.; Ernani, V.; Smith, L.M.; Ganti, A.K. HPV Status and Survival in Non-Oropharyngeal Squamous Cell Carcinoma of the Head and Neck. Anticancer Res 2019, 39, 1907–1914. [Google Scholar] [CrossRef] [PubMed]
- Mandić, K.; Milutin Gašperov, N.; Božinović, K.; Dediol, E.; Krasić, J.; Sinčić, N.; Grce, M.; Sabol, I.; Barešić, A. Integrative Analysis in Head and Neck Cancer Reveals Distinct Role of MiRNome and Methylome as Tumour Epigenetic Drivers. Sci Rep 2024, 14. [Google Scholar] [CrossRef] [PubMed]
- Shomorony, A.; Puram, S. V.; Johnson, D.N.; Chi, A.W.; Faquin, W.C.; Deshpande, V.; Deschler, D.G.; Emerick, K.S.; Sadow, P.M. A Non-Oropharyngeal Squamous Cell Carcinoma and the Pitfalls of HPV Testing: A Case Report. Otolaryngology Case Reports 2019, 13. [Google Scholar] [CrossRef]
- Yom, S.S.; Torres-Saavedra, P.; Caudell, J.J.; Waldron, J.N.; Gillison, M.L.; Xia, P.; Truong, M.T.; Kong, C.; Jordan, R.; Subramaniam, R.M.; et al. Reduced-Dose Radiation Therapy for HPV-Associated Oropharyngeal Carcinoma (NRG Oncology HN002). Journal of Clinical Oncology 2021, 39, 956–965. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Shibata, H.; Adkins, D.; Uppaluri, R. Neoadjuvant Immunotherapy Strategies in HPV-Related Head-and-Neck Cancer. Curr Otorhinolaryngol Rep 2022, 10, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-M.; Wu, M.; Han, F.-Y.; Sun, Y.-M.; Yang, J.-Q.; Liu, H.-X. Role of HPV Status and PD-L1 Expression in Prognosis of Laryngeal Squamous Cell Carcinoma. Int J Clin Exp Pathol 2021, 14, 107–115. [Google Scholar] [PubMed]
- Allegra, E.; Bianco, M.R.; Mignogna, C.; Caltabiano, R.; Grasso, M.; Puzzo, L. Role of P16 Expression in the Prognosis of Patients With Laryngeal Cancer: A Single Retrospective Analysis. Cancer Control 2021, 28. [Google Scholar] [CrossRef] [PubMed]
- King, R.E.; Bilger, A.; Rademacher, J.; Lambert, P.F.; Thibeault, S.L. Preclinical Models of Laryngeal Papillomavirus Infection: A Scoping Review. Laryngoscope 2023, 133, 3256–3268. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.; Lin, L.; Huang, Q.; Hu, C.; Zhang, M. HPV16 Status Might Correlate to Increasing Tumor-Infiltrating Lymphocytes in Hypopharyngeal Cancer. Acta Otolaryngol 2023, 143, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Burbure, N.; Handorf, E.; Ridge, J.A.; Bauman, J.; Liu, J.C.; Giri, A.; Galloway, T.J. Prognostic Significance of Human Papillomavirus Status and Treatment Modality in Hypopharyngeal Cancer. Head Neck 2021, 43, 3042–3052. [Google Scholar] [CrossRef] [PubMed]
- Patel, E.J.; Oliver, J.R.; Jacobson, A.S.; Li, Z.; Hu, K.S.; Tam, M.; Vaezi, A.; Morris, L.G.T.; Givi, B. Human Papillomavirus in Patients With Hypopharyngeal Squamous Cell Carcinoma. Otolaryngology - Head and Neck Surgery (United States) 2022, 166, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Hebsgaard, M.; Eriksen, P.; Ramberg, I.; von Buchwald, C. Human Papillomavirus in Sinonasal Malignancies. Curr Otorhinolaryngol Rep 2023, 11, 109–116. [Google Scholar] [CrossRef]
- Sjöstedt, S.; von Buchwald, C.; Agander, T.K.; Aanaes, K. Impact of Human Papillomavirus in Sinonasal Cancer—a Systematic Review. Acta Oncol (Madr) 2021, 60, 1175–1191. [Google Scholar] [CrossRef] [PubMed]
- Abi-Saab, T.; Lozar, T.; Chen, Y.; Tannenbaum, A.P.; Geye, H.; Yu, M.; Weisman, P.; Harari, P.M.; Kimple, R.J.; Lambert, P.F.; et al. Morphologic Spectrum of HPV-Associated Sinonasal Carcinomas. Head Neck Pathol 2024, 18. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.Y.; Hirayama, S.; Goss, D.; Zhao, Y.; Faden, D.L. Human Papillomavirus-Associated Nasopharyngeal Carcinoma: A Systematic Review and Meta-Analysis. Oral Oncol 2024, 159. [Google Scholar] [CrossRef] [PubMed]
- Naegele, S.; Efthymiou, V.; Das, D.; Sadow, P.M.; Richmon, J.D.; Iafrate, A.J.; Faden, D.L. Detection and Monitoring of Circulating Tumor HPV DNA in HPV-Associated Sinonasal and Nasopharyngeal Cancers. JAMA Otolaryngology–Head & Neck Surgery 2023, 149, 179. [Google Scholar] [CrossRef]
- Hung, S.H.; Yang, T.H.; Cheng, Y.F.; Chen, C.S.; Lin, H.C. Association of Nasopharynx Cancer with Human Papillomavirus Infections. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Sheth, S.; Walburn, T.; Tasoulas, J.; Patel, S.; Agarwal, A.; Gulley, M.L. Plasma Circulating HPV DNA Surveillance in a Patient With Nasopharyngeal Cancer. Ear Nose Throat J 2024. [CrossRef] [PubMed]
- Hung, S.H.; Yang, T.H.; Lee, H.C.; Lin, H.C.; Chen, C.S. Association of Salivary Gland Cancer with Human Papillomavirus Infections. European Archives of Oto-Rhino-Laryngology 2024. [CrossRef]
- Mohamed, F.E.; Aldayem, L.N.; Hemaida, M.A.; Siddig, O.; Osman, Z.H.; Shafig, I.R.; Salih, M.A.M.; Muneer, M.S.; Hassan, R.; Ahmed, E.S.; et al. Molecular Detection of Human Papillomavirus-16 among Sudanese Patients Diagnosed with Squamous Cell Carcinoma and Salivary Gland Carcinoma. BMC Res Notes 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Costin, C.A.; Chifu, M.B.; Pricope, D.L.; Grigoraş, A.; Balan, R.A.; Amălinei, C. Are HPV Oncogenic Viruses Involved in Salivary Glands Tumorigen(esis? Rom J Morphol Embryol. 2024, 65, 395–407. [Google Scholar] [PubMed]
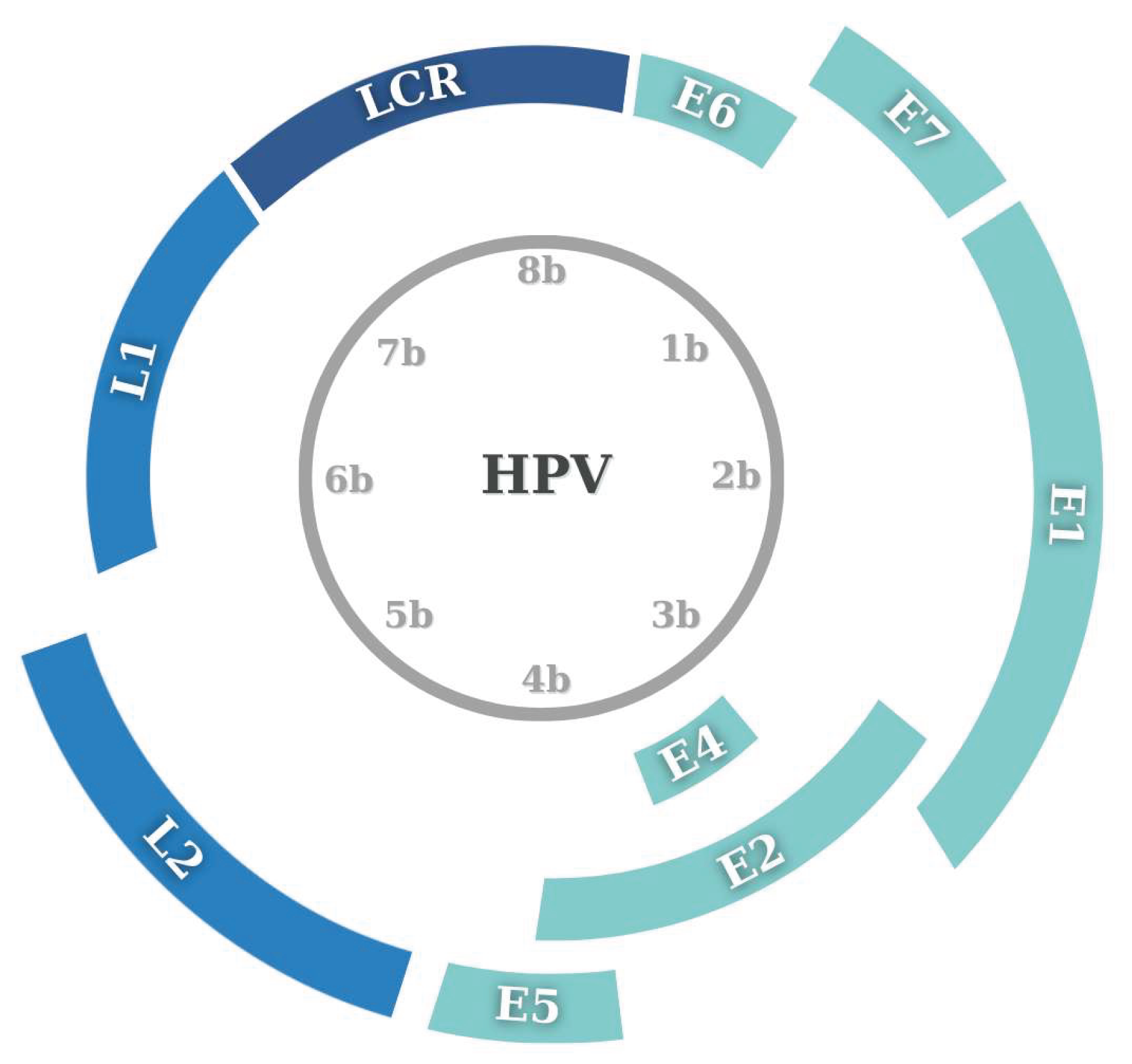
Figure 3.
Epigenetic regulation of HPV oncogene expression in different cellular and chromatin contexts. A) In young epithelial cells, the transcription factor YY1 binds to the LCR and represses the p97 promoter, preventing expression of the E6 and E7 oncogenes. In aged cells, YY1 binding is lost, leading to derepression and expression of E6/E7. B) The chromatin architectural protein CTCF forms a repressive chromatin loop in undifferentiated cells, preventing RNA polymerase access and E6/E7 expression. During differentiation, the chromatin loop is disrupted, RNA polymerase gains access, and E6/E7 are transcribed. C) SETD2, a histone methyltransferase, deposits the active epigenetic mark H3K36me3 on viral chromatin. While this mark enhances transcription of some HPV genes, it is absent from E6/E7 loci, allowing them to evade repression and remain highly expressed.
Figure 3.
Epigenetic regulation of HPV oncogene expression in different cellular and chromatin contexts. A) In young epithelial cells, the transcription factor YY1 binds to the LCR and represses the p97 promoter, preventing expression of the E6 and E7 oncogenes. In aged cells, YY1 binding is lost, leading to derepression and expression of E6/E7. B) The chromatin architectural protein CTCF forms a repressive chromatin loop in undifferentiated cells, preventing RNA polymerase access and E6/E7 expression. During differentiation, the chromatin loop is disrupted, RNA polymerase gains access, and E6/E7 are transcribed. C) SETD2, a histone methyltransferase, deposits the active epigenetic mark H3K36me3 on viral chromatin. While this mark enhances transcription of some HPV genes, it is absent from E6/E7 loci, allowing them to evade repression and remain highly expressed.
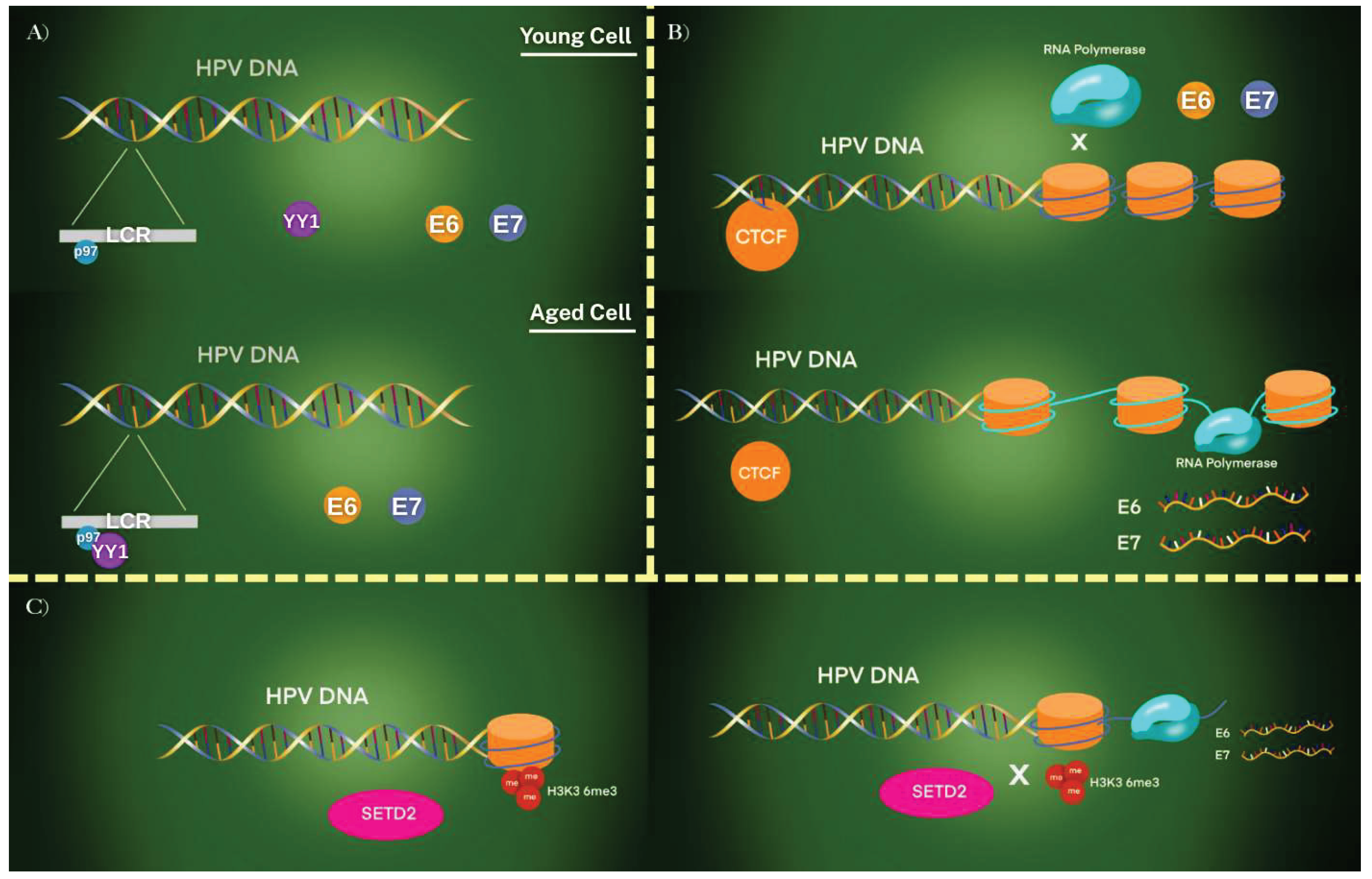
Figure 4.
Schematic illustration of DNA methylation-mediated regulation of HPV genome regions and its oncogenic consequences. The circular HPV genome is shown with key regulatory and coding regions including LCR, early genes (E6, E7, E1, E2, E4, E5), and late genes (L1, L2). DNA methylation (me) in specific regions such as the LCR, E2, E6, and L1 modulates transcriptional activity.
Figure 4.
Schematic illustration of DNA methylation-mediated regulation of HPV genome regions and its oncogenic consequences. The circular HPV genome is shown with key regulatory and coding regions including LCR, early genes (E6, E7, E1, E2, E4, E5), and late genes (L1, L2). DNA methylation (me) in specific regions such as the LCR, E2, E6, and L1 modulates transcriptional activity.
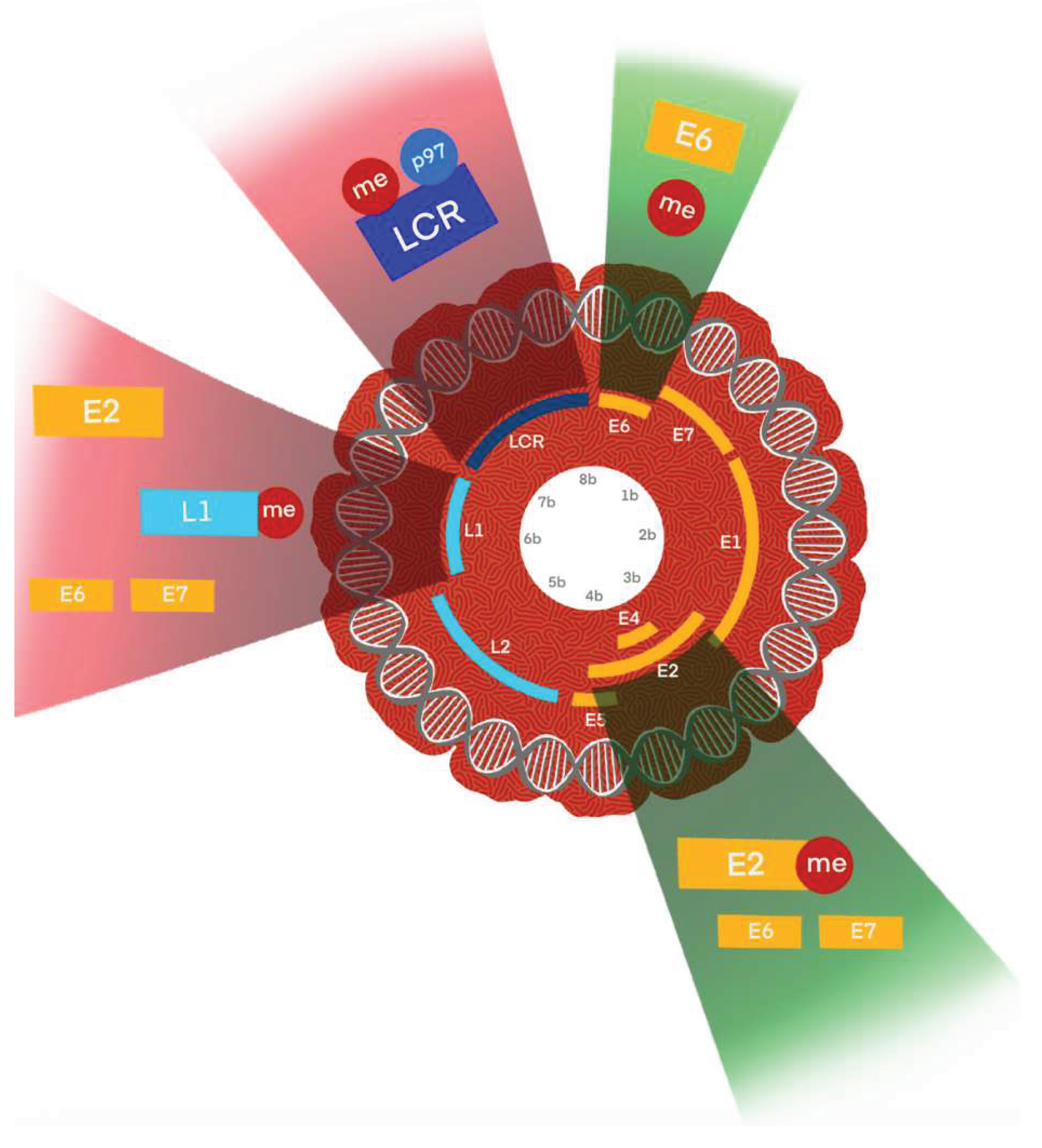
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



