
Submitted:
21 October 2025
Posted:
21 October 2025
Read the latest preprint version here
Abstract
Background: The use of oral home antibiotics (OHA) after discharge in children undergoing surgery for complicated acute appendicitis (CAA) remains controversial. This systematic review and meta-analysis aimed to evaluate whether OHA reduces the risk of infectious complications or readmissions compared to patients discharged without antibiotics (NHA).Methods: This systematic review was prospectively registered in PROSPERO (CRD420251049919). We searched PubMed, Web of Science, Scopus, Ovid, and Cochrane CENTRAL from inception to March 2025. Two independent reviewers screened the studies, extracted the data, and assessed the methodological quality using the ROBINS-I tool. Eight random-effects meta-analyses and four leave-one-out meta-analyses were conducted for intra-abdominal abscesses (IAA), surgical site infections (SSI), organ/space infections (OSI), and hospital readmissions (RA). Two exploratory random-effects meta-regression models were performed for RA. Certainty of evidence for all outcomes was formally graded using GRADE.Results: Fourteen studies comprising 26,174 pediatric patients with CAA were included. Meta-analyses showed no significant differences between intervention (IG) and comparator (CG) groups for IAA (RR 0.97; 95% CI: 0.38–2.47), OSI (RR 1.19; 95% CI: 0.73–1.93), or RA (RR 1.02; 95% CI: 0.73–1.41). In exposure-restricted analyses, OHA was associated with a significantly higher risk of readmission (RR 0.75; 95% CI 0.58–0.97, P < 0.03). The risk of SSI was significantly higher among patients in the CG (RR 0.77; 95% CI, 0.61–0.96; p = 0.02). However, this apparent association was not robust and was lost in sensitivity analyses restricted to studies with crude patient-level exposure data, where the effect reversed direction (RR > 1), consistent with protocol-based confounding. Meta-regression exploring differences in predischarge total leukocyte counts showed a non-significant trend toward increased RA in patients receiving OHA. Across all outcomes, certainty of evidence was rated very low, primarily driven by potential confounding by indication and non-randomized designs.Conclusions: OHA after discharge does not appear to reduce the risk of postoperative complications in children treated surgically for CAA. Given the lack of consistent benefit and potential for unnecessary harm, routine use of post-discharge OHA is not supported. The exposure-restricted analysis also raises a plausible signal of harm in terms of RA. Because the certainty of evidence is very low, further high-quality prospective research is needed to clarify the true effect of OHA in this context.
Keywords:
complicated acute appendicitis
; pediatric
; oral antibiotics
; discharge
; surgical site infection
; readmission
; stewardship
Introduction
Acute appendicitis (AA) is the most common surgical emergency in the pediatric population, with an estimated annual incidence of 9.68 per 10,000 children [1]. While most cases present as non-complicated appendicitis (NCAA), approximately 15–25% present as complicated acute appendicitis (CAA) [2,3]. Patients with CAA are more susceptible to postoperative complications and typically require prolonged antibiotic therapy and extended hospitalization, contributing to a substantial burden on healthcare systems and resource utilization [4]. While CAA generally includes gangrenous or perforated forms, it is crucial to outline that the specific operational definitions vary considerably across the literature. This heterogeneity constitutes a key challenge in synthesizing the data, and a detailed examination of the criteria used by each included study is a component of this review.
Despite consensus on the need for intravenous antibiotic therapy during hospitalization for CAA, and a growing trend toward institutional protocols promoting shorter intravenous courses or combined intravenous–oral regimens—with outcomes shown to be non-inferior to traditional approaches [5,6]—substantial variation persists in post-discharge management, particularly regarding the use of oral antibiotics. Current guidelines provide limited or no specific recommendations on antibiotic continuation after discharge, leading to heterogeneous institutional practices and variability among surgeons. Several studies have reported marked inter-professional variability in this aspect of care, underscoring both the lack of standardization and the ongoing uncertainty regarding its clinical benefit [7].
The rationale for prescribing oral antibiotics after hospital discharge in cases of CAA is primarily based on the assumption that continued antimicrobial coverage may reduce the risk of delayed infectious complications, such as surgical site infections (SSI), intra-abdominal abscesses (IAA), organ space infections (OSI), or unplanned readmissions (RA). Concerns over early hospital discharge and residual contamination in perforated or gangrenous appendicitis have traditionally justified this strategy. Oral home antibiotics (OHA) are often perceived as a low-cost, accessible intervention that may provide a safety buffer during the vulnerable post-discharge period.
However, prolonged antibiotic exposure is not without risks. The unnecessary use of antimicrobials contributes to adverse drug reactions, disruption of the gut microbiota, an increased risk of Clostridioides difficile infection, and a broader public health threat from antimicrobial resistance [8,9]. Given their developing immune and microbial systems, these concerns are particularly relevant in pediatric populations. Notably, emerging evidence suggests that post-discharge oral antibiotic therapy may offer limited or no benefit in reducing complications—and may even be associated with overtreatment and an increased risk of adverse events.
Given the widespread but inconsistent use of post-discharge OHA in children with surgically treated CAA—and the growing body of evidence questioning their effectiveness—there is a pressing need to synthesize the available data to inform clinical decision-making. The absence of clear guideline recommendations and the potential for both overuse and harm further underscore this gap. Therefore, the objective of this systematic review is to evaluate the impact of oral antibiotic therapy after hospital discharge on outcomes in pediatric patients with surgically treated CAA, with a specific focus on infectious complications (including SSI, OSI, and IAA) and readmissions.
Methods
Literature Search and Selection
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [10] and the Cochrane Handbook for Systematic Reviews of Interventions (version 6.5) [11]. The PRISMA checklist is provided in Supplementary File 1. This review was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO ID: CRD420251049919).
Eligible studies were identified by searching the primary existing medical bibliography databases (PubMed, Web of Science, Scopus, Ovid, and Cochrane Central). Supplementary File 2 shows the detailed search strategy for each bibliographic database. The search was last executed on 11.05.2025.
JAM and MRJ selected articles using the COVIDENCE ® tool. The search results were imported into the platform, and both authors independently screened the articles. Disagreements were resolved by consensus. Supplementary File 3 shows the inclusion and exclusion criteria.
Quality Assessment
The Cochrane Risk of Bias 2 (RoB 2) tool was selected to evaluate the methodological quality and risk of bias of randomized controlled trials (RCTs) [12]. In contrast, the Risk of Bias in Non-randomized Studies - of Interventions (ROBINS-I) tool was chosen to assess the methodological quality and risk of bias of non-randomized studies of interventions (NRSIs) [13]. No RCTs were ultimately identified during study selection; therefore, RoB2 was retained only as a pre-specified protocol element and was not applied in practice.
Data Extraction and Synthesis
Two reviewers (JAM, MRJ) independently extracted data from the included studies using a standardized and piloted form.
Extracted variables included: first author, year of publication, country of study, study design, sample size, age, sex distribution, Intervention and comparator groups definition, discharge criteria, total leukocyte count (TLC) admission values, TLC predischarge values, antibiotics employed (type, duration, and route), events by group including SSI, IAA, OSI, RA, reoperations (RO), and visits to the Emergency Department (EDV), and p-values for between-group comparisons. Given the known heterogeneity in defining CAA, a pre-specified variable for extraction was the explicit criteria used by each study. Data on the definition of CAA were extracted and categorized, including criteria based on intraoperative findings such as perforated acute appendicitis (PAA) identified as a “visible hole in the appendix”, the presence of a free fecalith in the abdominal cavity, the presence of an intra-abdominal abscess, diffuse fibrinopurulent exudate, contamination extending beyond the right lower quadrant or involving more than two quadrants, diffuse peritonitis, intra-abdominal stool, or endoluminal content leaking during surgery. We also extracted whether the definition included gangrenous appendicitis (GA) or was based on histopathological confirmation. Finally, we noted whether studies applied mixed criteria or did not specify the criteria used.
Disagreements during extraction were resolved by discussion or consultation with a third reviewer. Study authors were contacted for clarification when critical data were missing or unclear. In studies where raw data were available disaggregated by treatment group — OHA versus no home antibiotics (NHA) — these values were directly used; when not available, they were inferentially estimated, and if this was not possible, events were reported according to treatment protocol groups (e.g., “old protocol” versus “new protocol”), explicitly stating the lack of specific data for OHA and NHA. Unit standardization was not required.
Meta-Analysis
Four primary random-effects meta-analyses including all eligible studies, and four sensitivity analyses restricted to studies reporting crude patient-level exposure data were conducted using the restricted maximum likelihood (REML) estimator for both the pooled effect size and the between-study variance (τ²), following the Cochrane Handbook recommendations (version 6.5) [11,14,15,16]. For each outcome, the choice of confidence interval (CI) around the pooled effect was based on the number of included studies and the τ². When τ² was close to zero or only two studies were available, conventional Wald-type intervals were deemed acceptable. When more than two studies were included and τ² was greater than zero, CIs were computed using both the Hartung–Knapp–Sidik–Jonkman (HKSJ) [15] and the truncated modified Knapp–Hartung (mKH) methods [16]. The approach providing the most robust and interpretable inference was selected. For all primary random-effects models, 95% prediction intervals (PIs) were also calculated to quantify the expected range of true effects in future comparable settings. Because some studies reported outcomes based on institutional protocols rather than individual antibiotic exposure, we prospectively planned a sensitivity analysis stratifying studies by comparator structure (protocol-based vs. patient-level crude exposure OHA vs. NHA). This distinction was treated as a methodological moderator and explored in a pre-specified sensitivity meta-analysis. Exploratory leave-one-out sensitivity analyses were conducted for each one of the primary meta-analyses to assess the influence of individual studies on overall estimates. Where sufficient studies (≥10) were available, pre-specified univariable random-effects meta-regression analyses were performed to explore potential sources of heterogeneity. For studies with zero events in either treatment arm, a modified Haldane–Anscombe continuity correction was applied.
Publication Bias and Small Study Effects
In meta-analyses including at least ten studies, publication bias and small-study effects were explored through visual inspection of contour-enhanced funnel plots, which included significance contours at conventional thresholds (p < 0.01, p < 0.05, p < 0.10, and p > 0.10), as well as through Egger’s and Begg’s statistical tests [17,18]. To complement these assessments, Galbraith (radial) plots were generated to illustrate the contribution of each study to overall heterogeneity, and L’Abbé plots were used to visually examine the distribution and directionality of individual study effects across treatment groups, rather than heterogeneity per se. When funnel plot asymmetry was observed, the trim-and-fill method was applied to estimate the potential impact on the pooled effect size [19].
GRADE Assessment
The certainty of evidence for each primary outcome was evaluated using the GRADE framework. Because all included studies were non-randomized studies of interventions (NRSIs), certainty ratings started at low. Five domains were examined for potential downgrading: (1) risk of bias (ROBINS-I), (2) inconsistency (statistical heterogeneity: , , plus visual inspection of forest plots), (3) indirectness (differences in PICO alignment), (4) imprecision (95% CI width and whether it crossed clinically relevant decision thresholds), and (5) publication bias (funnel plot asymmetry and statistical testing when studies). Potential upgrading domains (large effect size, dose–response gradient, and residual confounding favoring the null) were considered but were not applicable. Final certainty ratings were categorized as high, moderate, low, or very low, with justifications presented in the Summary of Findings table.
Results
Summary of the Included Studies
The search yielded 331 articles (Scopus, n = 93; PubMed, n = 57; Web of Science, n = 106; Ovid, n = 12; Cochrane CENTRAL, n = 63). After removing 150 duplicates, 181 records remained. Of these, 167 were excluded based on the predefined inclusion and exclusion criteria. Ultimately, this systematic review included 14 studies encompassing data from 26,174 patients (15,488 males, 10,686 females) [20,21,22,23,24,25,26,27,28,29,30,31,32,33]. Minimal discrepancies (<0.5%) were identified between the numbers of patients included per group (IC and CG) and per gender (male/female) reported in the review, attributable to the lack of explicit reporting in some studies. Concerning study design, no randomized controlled trials were identified; all included studies were observational. The flowchart of the search and selection process is shown in Figure 1.
Sociodemographic and Clinical Characteristics
All studies were conducted between 2015 and 2025 in pediatric populations [20,21,22,23,24,25,26,27,28,29,30,31,32,33]. Thirteen were from the United States [20,21,22,23,24,25,26,27,28,29,31,32,33], and one was from Japan [30]. One prospective cohort study was identified [20], along with eight retrospective cohort studies [22,23,24,25,26,27,29,31], and five studies based on national databases, including the NSQIP Pediatric Database [21,28,32,33] and the Diagnosis Procedure Combination Database [30].
All included studies focused on patients with complicated acute appendicitis (CAA), although moderate variability in the definitions used was observed. Several authors defined CAA as PAA identified intraoperatively as a “visible hole in the appendix” [20,21,22,23,24,25,26,28,29,31,32,33], or as the presence of free fecalith in the abdominal cavity [20,21,23,24,28,31,32,33]. Others considered CAA to include the presence of intra-abdominal abscess [21,23,28,31,32,33], diffuse fibrinopurulent exudate within the peritoneal cavity [21,33], fibrinopurulent contamination extending beyond the right lower quadrant and pelvis [28], or involving more than two quadrants, including the pelvis [32]. Additional criteria used were the presence of diffuse peritonitis [23], intra-abdominal stool [24], and endoluminal content leaking outside the bowel during surgery [27]. Some authors also included gangrenous appendicitis (GA) under the CAA definition [22] or based the diagnosis on histopathological confirmation of PAA [29]. One study did not specify the criteria used to define CAA [30]. It is worth noting that many studies applied mixed criteria for defining CAA, and only a few explicitly referred to histopathological findings, despite histopathology being considered the diagnostic gold standard for acute appendicitis.
Regarding surgical technique, the information reported across studies is highly limited and heterogeneous. Some authors mentioned at some point in the manuscript that a laparoscopic approach was used [20,23], but did not specify whether any conversions occurred or whether 100% of patients underwent laparoscopy. Other studies included only laparoscopic procedures and explicitly excluded open appendectomies or conversions [24,31,33]. Authors using national databases adjusted odds ratios for the “laparoscopic technique” variable and reported the proportion of patients undergoing laparoscopy, with significant differences between groups (p < 0.01) [21]. In one study, propensity score matching was used to balance the number of open and laparoscopic procedures between groups, while retaining both techniques in the analysis [30]. In contrast, some authors provided no details on surgical technique [22,28,32], while others included both open and laparoscopic appendectomies indiscriminately [25,27]. One study explicitly stated that the intraoperative technique was not standardized [26]. Finally, another study specified that all procedures were laparoscopic, although one conversion occurred in the NHA group and was not excluded [29].
Post-Discharge Oral Home Antibiotics vs. No-Home Antibiotics
The intervention group (IG) was defined as the NHA group or as those managed under a protocol specifically implemented to reduce or eliminate post-discharge antibiotic use. In most studies, this corresponded to a “new protocol” cohort explicitly designed to minimize or avoid OHA. In some cases, raw data were reported specifically for NHA patients; in others, outcomes reflected the entire cohort managed under the revised protocol, even if not all patients were strictly NHA. The comparator group (CG) included patients who either received OHA at discharge or were managed according to standard protocols that did not restrict post-discharge antibiotic use. However, these protocols did not always guarantee that all patients in the CG actually received OHA. We clearly specified in the manuscript whether raw data were available or not for each study, and analyses were conducted accordingly.
A total of six studies directly compared patients discharged with OHA versus those discharged without them (NHA) [21,27,28,29,30,33], while eight studies compared outcomes across two distinct clinical protocols—typically a pre-implementation (baseline) phase versus a post-implementation phase [20,22,23,24,25,26,31,32]. In most cases, the pre-protocol group reflected routine or institutionally guided OHA administration, whereas the post-protocol group incorporated a clinical modification aimed at reducing OHA use. Although these constituted targeted interventions, they were primarily implemented as part of institutional practice changes rather than formal research initiatives, and most studies retained an observational retrospective design.
The specific characteristics of these institutional protocols, including their rationale and implications for antibiotic stewardship and discharge practices, are detailed in Table 1. Notably, one study (Ferguson [24]) inverted this structure: the authors standardized the routine prescription of OHA and designated that cohort as the intervention group. For this review, we reclassified this group as the comparator (CG) to maintain consistency in operational definitions across studies. These criteria and their application are detailed in Table 1.
Table 1 summarizes the data extracted from the fourteen studies that evaluated the role of post-discharge OHA in CAA.
Risk of Bias Assessment
In the domain of bias due to confounding, seven studies were rated as having a serious risk of bias [20,21,24,25,27,29,33], while the remaining seven were rated as moderate [22,23,26,28,30,31,32]. None were considered at low risk. One of the main reasons for assigning a serious risk rating was the presence of significant differences in baseline patient characteristics, with systematically sicker patients more likely to receive OHA. For instance, in the study by Anderson et al. [21], patients in the OHA group had significantly higher preoperative leukocyte counts, a greater prevalence of systemic inflammatory response syndrome, and higher rates of predischarge SSI. This phenomenon—known as confounding by indication—precludes a clear distinction between the effects of the treatment and the underlying severity of illness. Another key reason was the presence of concurrent interventions; for example, the study by Ferguson et al. [24] coincided with a quality improvement initiative on the use of intraoperative abdominal drains and a separate pilot randomized trial of intra-abdominal irrigation with povidone-iodine, making it difficult to isolate the effect of the antibiotic protocol alone. Other reasons included the use of historical controls, which introduces temporal confounding, and massive, unadjusted baseline differences in disease severity between hospital cohorts being compared (such as in the case of Desai et al.) [20].
For bias in the selection of participants into the study, no studies were identified as having a serious risk, 5 were rated as moderate [20,24,28,30,31], and 9 were rated as low risk [21,22,23,25,26,27,29,32,33].
In the domain of bias in the classification of interventions, no studies were found to pose a serious risk, 7 were rated as moderate [21,23,25,27,28,30,33], and 7 were rated as low risk [20,22,24,26,29,31,32].
Regarding bias due to deviations from intended interventions, one study was rated as having a serious risk [23], nine as moderate [21,24,25,27,28,29,30,31,32], and four as low risk [20,22,26,33]. The serious risk rating was assigned because the study explicitly reported that "overall compliance with protocol guidelines was not ideal," with participation at the surgeon's discretion. This led to substantial crossover, in which patients in the new protocol group continued receiving older treatments, contaminating the comparison groups and biasing the results toward finding no difference.
Regarding bias due to missing data, no studies posed a serious risk; 8 were rated as moderate [20,22,23,25,26,27,29,33]; and six were rated as low risk [21,24,28,30,31,32].
Regarding bias in the measurement of outcomes, none of the studies posed a serious risk, one study posed a moderate risk [20], and 13 were rated as low risk [21,22,23,24,25,26,27,28,29,30,31,32,33].
Finally, in the domain of bias in the selection of the reported result, no study was judged to be at serious or moderate risk; all 14 studies were rated as having a low risk of bias [20,21,22,23,24,25,26,27,28,29,30,31,32,33].
Figure 2 visually displays the ROBINS-I risk-of-bias assessments across individual domains for each included study.
Supplementary File 4 and Table 1 provide detailed information on the data used for each study, including whether raw exposure data were available.
Intra-Abdominal Abscess (Oral Home Antibiotics vs. No Home Antibiotics)
Six studies reported IAA rates stratified by treatment group [20,22,24,25,26,27]. Bonasso et al. [22] presented two separate cohorts. Five cohorts found no significant differences in IAA rates between groups [20,22,25,26,27]. One study reported a significantly higher IAA rate in the IG than in the CG [24]. In contrast, one cohort reported a significantly higher IAA rate in the CG than in the IG [22].
Notably, the only study reporting increased IAA rates in the IG was Ferguson et al. [24], which uniquely implemented a protocol to standardize the routine use of OHA, rather than to reduce them. This contrasts with the rest of the literature, where interventions consistently aimed to minimize post-discharge antibiotic use.
Meta-Analysis for Intra-Abdominal Abscess (Oral Home Antibiotics vs. No Home Antibiotics)
For the IAA meta-analysis, a random-effects model was fitted using restricted maximum likelihood (REML) with truncated modified Knapp–Hartung (mKH) adjustments. Seven studies were included, encompassing 788 patients in the IG and 1,011 patients in the CG. This meta-analysis included a combination of studies reporting raw group-level data (OHA vs NHA) and others presenting outcomes for cohorts managed under pre- or post-intervention protocols. The pooled risk ratio (RR) comparing IG versus CG was 0.97 (95% CI: 0.38-2.47; model p = 0.94), indicating no significant difference in IAA rates between the groups. Between-study heterogeneity was moderate-to-substantial (I² = 66.98%; Cochran’s Q p = 0.01), and the estimated between-study variance was τ² = 0.47. The 95% PI ranged from 0.13 to 7.26. Leave-one-out sensitivity analysis revealed that excluding any single study did not materially alter the overall result or achieve statistical significance in any iteration, supporting the robustness of the null finding (Figure 3). A sensitivity analysis was conducted on studies reporting raw event data for both OHA and NHA [20,22,25,27]. This analysis included five studies and, under a REML random-effects model with mKH adjustment, yielded a pooled RR of 0.74 (95% CI 0.15–3.61), τ² = 0.94, I² = 75%, Q = 13.35 (p = 0.01), with the model test non-significant (p = 0.62). Given that fewer than ten studies were included, between-study heterogeneity was not further explored using funnel plots or formal statistical tests for small-study effects (e.g., Egger’s or Begg’s tests). Similarly, no meta-regression analyses were conducted due to the low number of studies and limited statistical power.
For IAA, the certainty of evidence was rated very low after downgrading for serious risk of bias, serious inconsistency, and serious imprecision, with no applicable upgrading domains.
Surgical Site Infection (Oral Home Antibiotics vs. No Home Antibiotics)
Seven studies reported SSI rates stratified by treatment group [21,23,24,29,31,32,33]. Five studies found no significant differences in SSI rates between groups [23,24,29,32,33]. One study reported a significantly higher SSI rate in the IG than in the CG [31], whereas another reported a significantly higher SSI rate in the CG than in the IG [21].
Meta-Analysis for Surgical Site Infection (Oral Home Antibiotics vs. No Home Antibiotics)
For the SSI meta-analysis, a random-effects model was fitted using REML. Seven studies were included, encompassing 3,858 patients in the IG and 4,610 in the CG. This meta-analysis included a combination of studies reporting raw group-level data (OHA vs NHA) and others presenting outcomes for cohorts managed under pre- or post-intervention protocols. The pooled RR comparing IG versus CG was 0.77 (95% CI: 0.61-0.96; model p = 0.02), indicating a significant difference in SSI rates. Between-study heterogeneity was negligible (I² = 0%; Cochran’s Q p = 0.55), and the estimated between-study variance was τ² = 0. The 95% PI ranged from 0.571 to 1.033. Leave-one-out sensitivity analysis showed that this association was not robust, as the exclusion of Anderson et al. yielded a non-significant effect (RR = 0.96; 95% CI: 0.57–1.61; p = 0.88). In the sensitivity analysis restricted to studies reporting crude patient-level exposure data (n=2), the pooled point estimate shifted in the opposite (reversed) direction (RR 2.34; 95% CI 0.72–7.64; p = 0.16), suggesting higher SSI rates in the OHA group when the analysis is based on true exposure rather than protocol-defined cohorts. This reversed direction indicates that the apparent benefit of NHA is driven by protocol-based rather than true exposure-level comparisons, and does not reflect a consistent protective effect. Given that fewer than ten studies were included, between-study heterogeneity was not further explored using funnel plots or formal statistical tests for small-study effects (e.g., Egger’s or Begg’s tests). Similarly, no meta-regression analyses were conducted due to the low number of studies and limited statistical power.
For SSI, the certainty of evidence was rated very low after downgrading for serious risk of bias and serious imprecision, with no applicable upgrading domains.
Organ Space Infection (Oral Home Antibiotics vs. No Home Antibiotics)
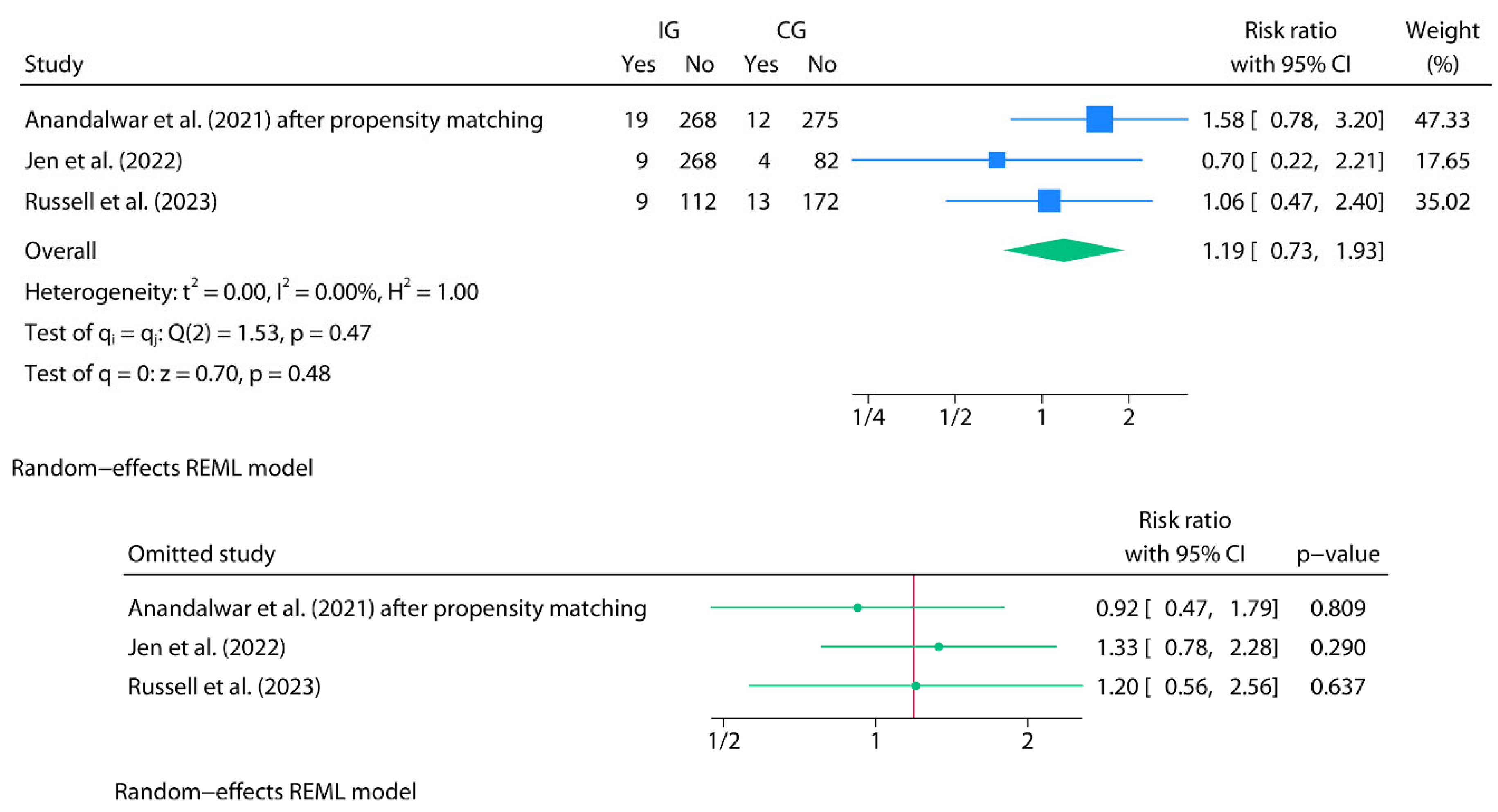
Meta-Analysis for Organ Space Infection (Oral Home Antibiotics vs. No Home Antibiotics)
For the OSI meta-analysis, a random-effects model was fitted using REML. Three studies were included, encompassing 685 patients in the IG and 558 in the CG. In the case of Anandalwar et al., only data from the propensity-matched cohort were included to avoid duplicating data from the same population and to ensure study independence. This meta-analysis included a combination of studies reporting raw group-level data (OHA vs NHA) and others presenting outcomes for cohorts managed under pre- or post-intervention protocols. The pooled RR comparing IG versus CG was 1.19 (95% CI: 0.73-1.93; model p = 0.48), indicating no significant difference in OSI rates. Between-study heterogeneity was negligible (I² = 0%; Cochran’s Q p = 0.47), and the estimated between-study variance was τ² = 0. Accordingly, confidence intervals were calculated using conventional Wald-type methods, as recommended when no heterogeneity is detected. The 95% PI ranged from 0.052 to 27.487. Leave-one-out sensitivity analysis revealed that no single study significantly altered the overall result or achieved statistical significance in any iteration (Figure 5). A sensitivity analysis was conducted on studies reporting raw event data for both OHA and NHA. This analysis included two studies [28,29] and, under a REML random-effects model without CI adjustment, yielded a pooled RR of 1.20 (95% CI 0.56–2.56; p = 0.64), with τ² = 0.10, I² = 29.08%, and Q = 1.41 (p = 0.24). Using a REML model with mHK produced an extremely wide estimate (RR 1.20, 95% CI 0.09–164.24; p = 0.72). These results illustrate that meta-analyses based on only two heterogeneous studies are methodologically unstable: Wald-type CIs tend to be overly optimistic, whereas mHK/HKSJ adjustments often become overly conservative under such conditions. Given that fewer than ten studies were included, between-study heterogeneity was not further explored using funnel plots or formal statistical tests for small-study effects (e.g., Egger’s or Begg’s tests). Similarly, no meta-regression analyses were conducted due to the low number of studies and limited statistical power.
For OSI, the certainty of evidence was rated very low after downgrading for serious risk of bias and serious imprecision, with no applicable upgrading domains.
Figure 4.
Top: Forest plot of the random-effects meta-analysis for surgical site infections (SSI) using REML (IG vs. CG). Bottom: Leave-one-out forest plot for the same analysis.
Figure 4.
Top: Forest plot of the random-effects meta-analysis for surgical site infections (SSI) using REML (IG vs. CG). Bottom: Leave-one-out forest plot for the same analysis.
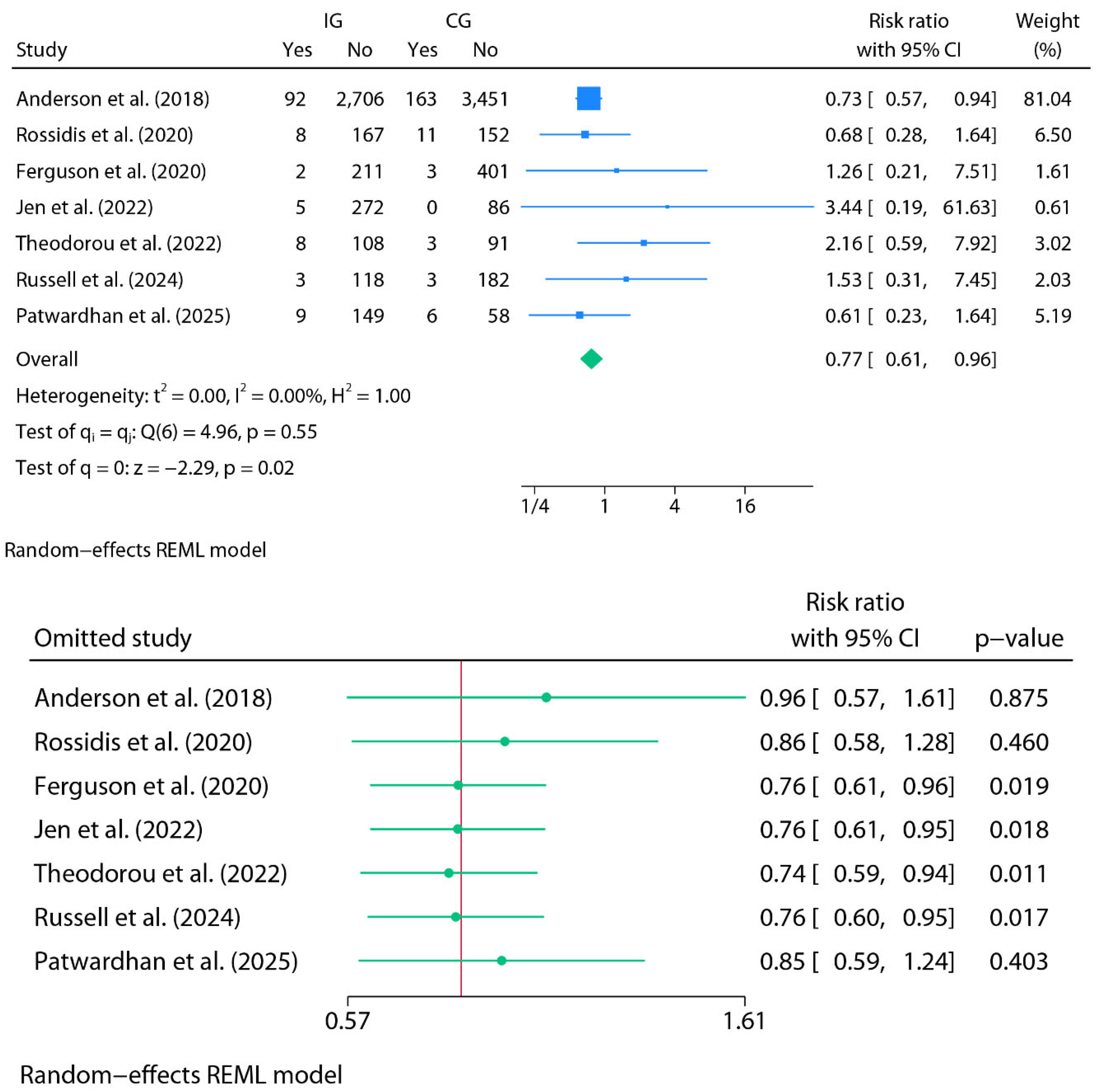
Figure 5.
Top: Forest plot of the random-effects meta-analysis for organ/space infections (OSI) using REML (IG vs. CG). Bottom: Leave-one-out forest plot for the same analysis.
Figure 5.
Top: Forest plot of the random-effects meta-analysis for organ/space infections (OSI) using REML (IG vs. CG). Bottom: Leave-one-out forest plot for the same analysis.
Readmissions (Oral Home Antibiotics vs. No Home Antibiotics)
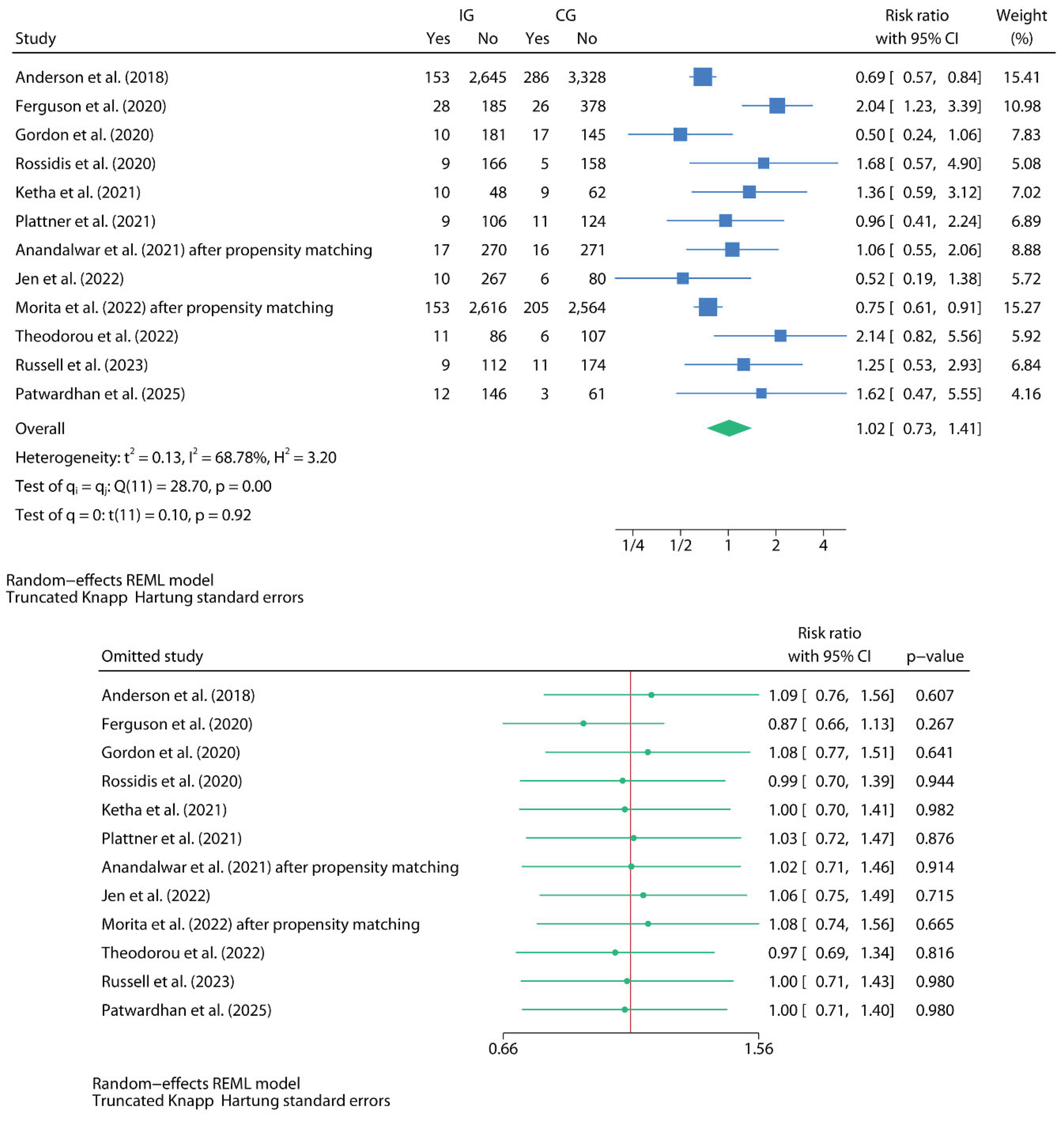
Thirteen studies reported RA rates stratified by treatment group [21,22,23,24,25,26,27,28,29,30,31,32,33]. Ten studies found no significant differences in RA rates between groups [22,23,24,25,26,27,28,29,31,32]. One study reported a significantly higher RA rate in the IG compared to the CG [24], whereas two studies reported significantly higher RA rates in the CG than in the IG [21,30]. In the case of Patwardhan et al. [33], although the difference did not reach statistical significance, a marginal p-value (0.06) was observed, suggesting a higher rate of events in the IG. Although most studies defined RA as occurring within 30 days of initial discharge, some—such as Morita et al. [30]—used a 60-day timeframe, which may influence effect estimates due to the extended follow-up window.
Meta-Analysis for Readmissions (Oral Home Antibiotics vs. No Home Antibiotics)
For the meta-analysis of RA, a random-effects model was fitted using REML with mKH adjustments. Bonasso et al. [22], which also reported RA rates, was excluded from the pooled analysis due to internal inconsistencies in patient numbers and reported events elsewhere in the study, precluding reliable extraction for pooling. Twelve studies were included, encompassing 7,259 patients in the IG and 8,053 in the CG. In the cases of Anandalwar et al. (2021) and Morita et al. (2022) [28,30], only data from the propensity-matched cohorts were included to ensure independence of observations. This meta-analysis included a combination of studies reporting raw group-level data (OHA vs NHA) and others presenting outcomes for cohorts managed under pre- or post-intervention protocols. The pooled RR comparing IG versus CG was 1.02 (95% CI: 0.73-1.41; model p = 0.92), indicating no significant difference in readmission rates. Between-study heterogeneity was substantial (I² = 68.68%; Cochran’s Q p = 0.00), with a between-study variance of τ² = 0.13. The 95% PI ranged from 0.422 to 2.443. Because this was the only meta-analysis including ≥10 studies, small-study effects and publication bias were formally assessed. Visual inspection of the contour-enhanced funnel and Galbraith (radial) plots did not reveal asymmetry, which was consistent with non-significant Egger and Begg tests (Egger p = 0.18; Begg p = 0.19). A L’Abbé plot was generated exclusively to illustrate between-study variability (heterogeneity) (Figure 7).
Leave-one-out sensitivity analysis revealed that no single study materially affected the overall result or achieved statistical significance. The exclusion of Ferguson et al. (2020) produced the most pronounced shift, but the result remained non-significant (Figure 6). A complementary sensitivity analysis including the five studies with available raw event data was also performed. Under a REML random-effects model with mHK adjustment, the pooled effect was RR 0.75 (95% CI 0.58–0.97; p = 0.03), with τ² = 0.00, I² = 0%, and Q = 3.07 (p = 0.55), indicating no detectable heterogeneity. This analysis of patient-level exposure data suggests that OHA may be associated with an increased risk of RA. Protocol-based comparisons are methodologically weaker because they conflate exposure with institutional timing and practice evolution. By contrast, crude exposure studies provide a cleaner estimate at the patient level. The fact that the association becomes stronger and statistically significant once protocol contamination is removed suggests that protocol-based designs were masking a potential adverse signal.
Figure 6.
Top: Forest plot of the random-effects meta-analysis for hospital readmissions (RA) using REML with Knapp–Hartung adjustment (IG vs. CG). Bottom: Leave-one-out forest plot for the same analysis.
Figure 6.
Top: Forest plot of the random-effects meta-analysis for hospital readmissions (RA) using REML with Knapp–Hartung adjustment (IG vs. CG). Bottom: Leave-one-out forest plot for the same analysis.
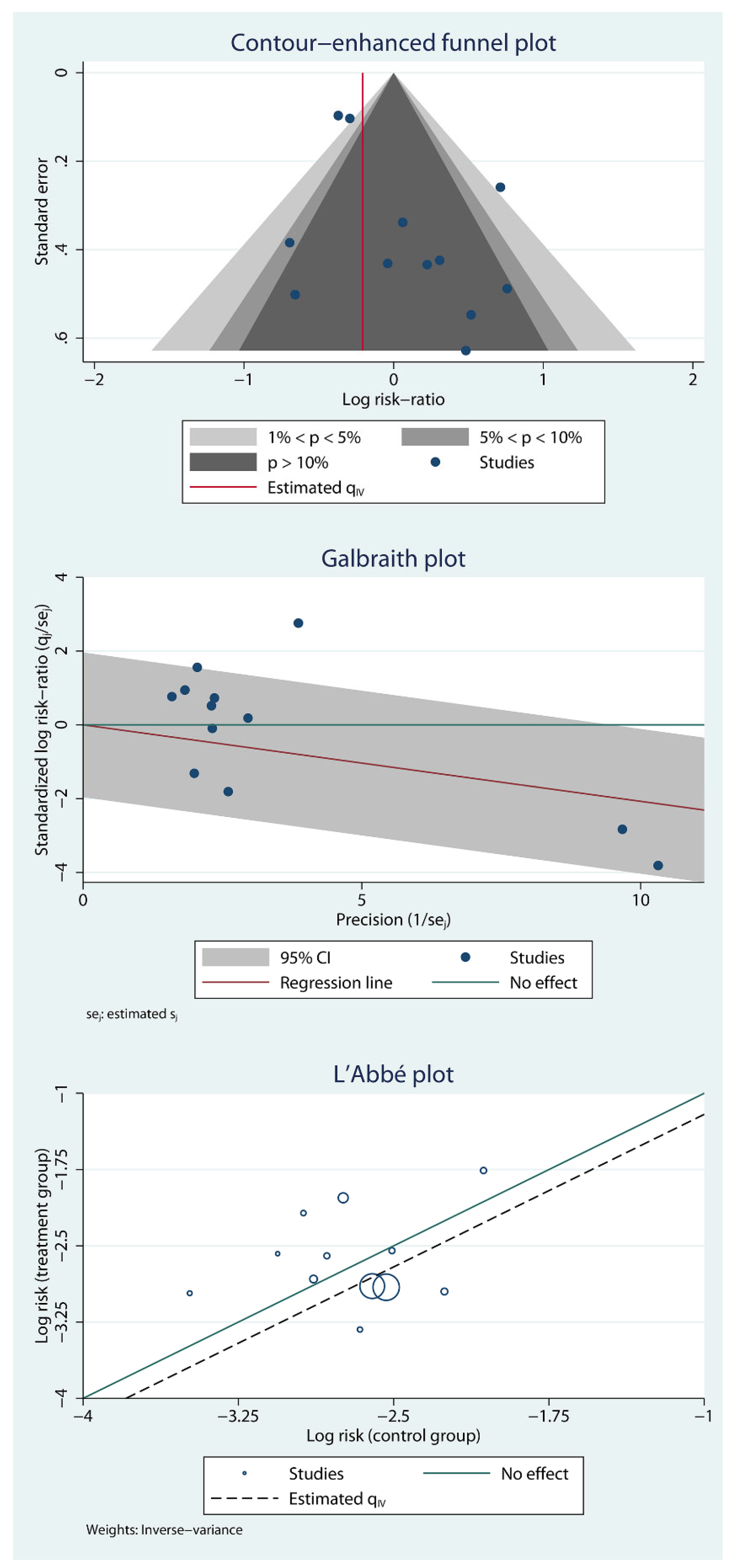
Figure 7.
Top: contour-enhanced funnel plot assessing small-study effects and potential publication bias. Middle: Galbraith (radial) plot assessing overall heterogeneity and study precision. Bottom: L’Abbé plot illustrating between-study variability in event rates (heterogeneity exploration).
Figure 7.
Top: contour-enhanced funnel plot assessing small-study effects and potential publication bias. Middle: Galbraith (radial) plot assessing overall heterogeneity and study precision. Bottom: L’Abbé plot illustrating between-study variability in event rates (heterogeneity exploration).
An univariable meta-regression was conducted, using differences in predischarge total leukocyte count (TLC) as a categorical moderator to examine whether discharge inflammatory status influenced the association between OHA and the risk of RA. The analysis compared studies reporting no differences in TLC between groups (reference category) with those reporting significant differences—most often reflecting higher TLC levels in the comparator group (CG, i.e., OHA)—and studies that did not specify this information. Studies with significant intergroup TLC differences showed a non-significant trend toward lower pooled risk ratios (β = –1.15; p = 0.14), suggesting fewer readmissions in the intervention group (IG, i.e., NHA). Importantly, these differences likely reflect clinical decision-making, whereby patients with signs of residual inflammation were more prone to receive antibiotics. Therefore, the lower RR observed in these studies in favor of NHA does not indicate a protective effect of OHA but rather the opposite: that despite being clinically selected for antibiotic treatment, OHA patients experienced more readmissions. This supports the interpretation that OHA does not reduce—and may even increase—the risk of hospital readmission, independent of predischarge inflammatory status. However, as the category with significant TLC differences included only two studies, this trend should be interpreted with caution, given the potential influence of individual study effects and limited statistical power.
Lastly, a univariable meta-regression comparing studies at high versus moderate risk of bias revealed a non-significant trend toward more favorable outcomes in the NHA group among high-risk studies (logRR difference: –0.34; 95% CI: –1.03 to 0.36; p = 0.30). However, this association did not reach statistical significance, explained none of the observed heterogeneity (R² = 0%), and should therefore be interpreted as clinically and methodologically uninformative.
For RA the certainty of evidence was rated very low, after downgrading for serious risk of bias, serious inconsistency, and serious imprecision, with no upgrading domains applicable.
Secondary Outcomes (Oral Home Antibiotics vs. No Home Antibiotics)
Some studies also examined alternative outcomes such as composite post-discharge morbidity [21], reoperations (RO) [21,23,24], and Emergency Department visits (EDV) [21,23,24,29]. Detailed outcome data are available in Table 1. Given the low number of studies reporting these outcomes and the heterogeneity and dispersion of available data, no meta-analytic models were fitted for these endpoints.
Discussion
This systematic review and meta-analysis provide the most comprehensive synthesis to date of the impact of OHA following surgical management of CAA in children. Across multiple outcomes—including IAA and OSI—no consistent benefit was observed with OHA use. Indeed, SSI were significantly more frequent among patients in the CG in the primary model; however, this finding was not robust and disappeared once analyses were restricted to crude exposure data, where the point estimate shifted in the opposite direction. This pattern is consistent with confounding by indication in protocol-based cohorts. Therefore, the primary SSI signal should be interpreted as artefactual rather than indicative of benefit. Lastly, in crude exposure analyses, RA rates were lower in the NHA cohort. Both individual study estimates and pooled risk ratios failed to support routine administration of post-discharge OHA. Despite their widespread use, this is the first synthesis to assess their effectiveness across these core outcomes. Notably, several analyses showed a trend in favor of NHA discharge strategies for RA, and in the exposure-restricted subset, this difference reached statistical significance, consistent with a potential harmful signal rather than a neutral effect.
Our findings challenge the traditional rationale for extended antibiotic coverage after discharge in pediatric CAA, particularly in cases with adequate source control. Previous guidelines and institutional practices often endorsed OHA as a safeguard against latent infections or undetected abscess formation. However, the current evidence, including recent protocol-based studies aimed at restricting OHA, suggests that this approach may offer no additional benefit—and may contribute to overtreatment, antimicrobial resistance, and unnecessary drug exposure. This underscores the importance of aligning postoperative management with principles of antimicrobial stewardship, especially in pediatric patients.
Interestingly, the only study reporting a significantly higher RA and IAA rate in the NHA group [24] was also the only one to implement a protocol aimed at standardizing rather than limiting post-discharge OHA. This divergence contrasts with the broader trend in the literature, where interventions were designed to reduce or eliminate OHA use. Thus, this deviation highlights how institutional culture and protocol framing may shape not only practices but also outcomes. It also raises the possibility of confounding by protocol context—underscoring the need for randomized comparisons within standardized care frameworks.
From a clinical standpoint, several included studies explored risk-adapted prescribing by preferentially giving OHA to patients with higher inflammatory markers or more severe intraoperative findings. However, because these decisions were observational and confounded by indication, the certainty of evidence supporting this approach is very low under GRADE. Therefore, while the concept may be clinically appealing, the current data do not validate risk-adapted selection of OHA, and any such strategy remains unproven until tested in higher-certainty designs. Although some relevant RCTs, such as the APPIC trial [34], evaluated inpatient intravenous antibiotic duration rather than post-discharge regimens, they provide indirect contextual relevance: even earlier in the treatment pathway, shortening antibiotic exposure has not resulted in worse outcomes when adequate source control is achieved. Its applicability to OHA is therefore indirect, but the directionality is consistent — the burden of justification seems to lie on prolonged antibiotic exposure, not on reduction.
Another potential source of bias stems from clinical decision-making criteria for prescribing antibiotics at discharge. Although some studies reported predischarge TLC and their comparability between groups, this information was frequently absent or insufficiently detailed. This limits the ability to determine whether the inflammatory status at discharge systematically influenced treatment allocation. In our exploratory meta-regression, studies reporting statistically significant differences in TLC between groups—typically indicating higher values in the antibiotic group—showed a trend toward lower pooled RR in the NHA. While this finding should be interpreted with caution due to the limited power and potential confounding, it suggests that patients perceived as being at higher risk (e.g., those with elevated TLC) may have been selectively prescribed antibiotics, yet did not show a corresponding reduction in readmission rates. This paradoxical trend may reflect residual confounding and highlight the complexity of interpreting observational data. This hypothesis-generating observation highlights the need for future studies to document clinical parameters that inform discharge decisions rigorously and to control for these factors in comparative analyses. Structured discharge algorithms incorporating inflammatory markers may help reduce selection bias and improve comparability in future research.
Importantly, confounding by indication should not be interpreted merely as a limitation but as a central interpretive lens. The bias is directional, not random: children perceived as higher-risk (e.g., elevated predischarge TLC or systemic inflammation) were systematically more likely to receive OHA. If OHA were truly protective, this clinical enrichment of the treated cohort should have amplified its observable benefit. Instead, no benefit was seen, and when analyses were restricted to studies with individual-level exposure data (OHA vs NHA), the signal moved toward potential harm. Far from weakening the null finding, this strengthens it: a therapy that fails to demonstrate benefit even in the subgroup most selectively “enriched” to benefit is unlikely to be effective in routine practice.
Another important consideration is the limited reporting and control of variables that may substantially influence outcomes but were inconsistently addressed across studies. For example, none of the included articles provided objective measures of patient compliance with prescribed oral antibiotics—a critical determinant of treatment efficacy. Similarly, the relationship between discharge antibiotic strategy and surgical technique (e.g., laparoscopic versus open approach), intraoperative findings, or postoperative management protocols was rarely explored in depth. These factors could interact with the effect of OHA and confound outcome estimates. Additionally, key elements such as discharge timing, the presence of drains, or concomitant antibiotic regimens (e.g., IV continuation) were often insufficiently detailed. Potential differences in microbiological etiology or resistance patterns were also largely unaddressed, limiting biological interpretability and external applicability. These gaps highlight the need for future prospective studies to standardize and report such variables systematically, enabling more precise estimation of the clinical utility—and limitations—of routine OHA in CAA.
From a biological standpoint, the rationale for OHA in this setting remains biologically questionable. The peritoneal cavity, particularly in the context of localized postoperative inflammation and fibrinous exudate, may offer limited penetration for orally administered antibiotics—especially in the absence of systemic signs of infection. Furthermore, the oral route introduces variability in absorption, particularly in children with reduced appetite, postoperative ileus, or gastrointestinal dysmotility. These pharmacokinetic limitations, combined with incomplete data on compliance and dosing, raise concerns about the real-world efficacy of oral agents in preventing deep or loculated infections. Additionally, unnecessary antibiotic exposure may select for resistant microbial strains, potentially altering the child's microbiome and increasing future vulnerability to infection. Altogether, these pharmacological considerations further support a risk-adapted rather than uniform approach to OHA use.
Moreover, none of the included studies systematically reported adverse events associated with oral antibiotic use, such as diarrhea, candidiasis, or intestinal dysbiosis, which represents an important limitation. The absence of statistically significant differences should not be interpreted as evidence of equivalence; limited power and unmeasured non-adherence may have attenuated the observed effects. However, the consistent directional pattern across leave-one-out and exposure-restricted analyses suggests that the null findings are unlikely to be explained solely by insufficient power. This omission prevents quantification of the potential collateral harms of unnecessary antibiotic administration, but it indirectly reinforces one of the core principles of antibiotic stewardship: avoiding treatments that provide no clinical benefit and may instead cause preventable adverse effects. In this context, our findings are particularly applicable to patients with favorable postoperative evolution—namely, those who are afebrile, tolerating oral intake, in good general condition, and with normalized inflammatory markers at discharge—for whom continued antibiotic treatment beyond discharge may offer no additional benefit. It should also be emphasized that the majority of included studies administered intravenous antibiotics during hospitalization, and thus, these results should not be extrapolated to settings in which early discharge with oral antibiotics alone is considered—an approach not evaluated in this review. Avoiding unnecessary OHA in these patients may also reduce the risk of avoidable harm in an already recovering pediatric population.
Lastly, an essential methodological concern highlighted by this review is the substantial variability in the reporting of surgical technique. We observed marked differences in both the inclusion/exclusion criteria based on surgical approach (open vs. laparoscopic) and the overall quality of reporting. While some studies explicitly excluded open appendectomies or documented conversions, others merely stated that laparoscopy was used without specifying whether this applied to all patients or whether any conversions occurred. Several studies failed to report the surgical approach altogether. This lack of standardization is concerning, given well-established evidence that open appendectomies carry a higher risk of surgical site infection than laparoscopic procedures, potentially introducing uncontrolled confounding into the interpretation of results. Similarly, relevant operative variables such as surgical duration—which may reflect case complexity and is associated with postoperative outcomes—were scarcely reported across the included studies. Given the well-established association between surgical approach and postoperative infection risk, this lack of standardization represents a critical gap in current evidence. Future research should systematically collect and transparently report key surgical variables to enable more accurate risk adjustment and a more robust interpretation of findings.
This review has several strengths. It adheres to PRISMA and Cochrane methodological standards. It applies modern, rigorous statistical techniques, such as random-effects REML meta-analysis with robust confidence intervals (HKSJ and the modified Knapp–Hartung) and prediction intervals, leave-one-out sensitivity analyses, and, when feasible, assessment of publication bias. Univariable meta-regression was used to explore sources of heterogeneity, including differences in predischarge TLC and the type of comparator group (raw OHA/NHA vs protocol-defined). Particular care was taken to distinguish studies reporting individual-level data from those reporting outcomes based on pre- and post-protocol cohorts, and all analyses were conducted accordingly. Importantly, statistical results were interpreted in light of the clinical context, considering how discharge practices and patient selection may have influenced both antibiotic use and outcomes. However, relevant limitations must be acknowledged. As detailed in our Results, a primary limitation is the substantial variability in the definition of CAA across studies. Definitions spanned a spectrum of findings (e.g., visible perforation, abscess, free fecalith) based on intraoperative, histopathological, or even unspecified criteria. This lack of standardization complicates direct comparisons and is a significant source of heterogeneity. Furthermore, individual-level OHA and NHA raw data were also often unavailable. Many studies lacked control for key variables such as antibiotic type, dosage, or precise discharge criteria. Additionally, the complications—particularly IAA and OSI—were not extensively characterized across articles, e.g., omitting severity grading or volumetric analysis of abscesses. Most studies were retrospective and based in the USA, and those using large databases, while offering substantial sample sizes, often lacked granular clinical information. Notably, only one study [27] included solid microbiological data, limiting the biological interpretability of the outcomes. Accordingly, the certainty of evidence was rated as low or very low across all primary outcomes using the GRADE framework [35], primarily due to the observational nature of the studies, moderate to high heterogeneity in some analyses, and imprecision of effect estimates. These conclusions should be interpreted with caution, given the overall low certainty of evidence. Lastly, because several included studies used NSQIP-derived cohorts, partial patient overlap cannot be definitively excluded. Individual-level identifiers are not available in NSQIP publications, preventing formal de-duplication, and therefore, a residual risk of double-counting remains. Although we found no demonstrable overlap based on study periods and sampling frames, this possibility should be acknowledged when interpreting pooled estimates.
In light of these findings, the routine prescription of OHA after discharge in pediatric patients with surgically treated CAA appears unwarranted. Across 26,000 patients, no consistent benefit was observed for IAA, SSI, OSI, or RA. Importantly, subgroup crude analyses even suggest that OHA may increase the risk of readmission, particularly in patients selected for treatment based on residual inflammation (TLC). However, the current body of evidence is based exclusively on observational studies, with heterogeneous definitions, limited adjustment for confounders, and no data on patient adherence. While the convergent pattern of results strengthens the biological and methodological plausibility of no benefit, the GRADE rating of very low certainty means that inference must remain cautious. The present synthesis supports a presumption against routine OHA, but clinical equipoise persists, and only well-designed prospective trials can definitively settle this question.
There is an urgent need for adequately powered, multicenter randomized controlled trials that rigorously control for clinical, surgical, and microbiological variables to definitively establish the role—or lack thereof—of oral home antibiotics in this setting. Future studies should clearly specify the surgical technique employed (e.g., open vs laparoscopic, use of peritoneal lavage), characterize microbiological findings and antibiotic susceptibility profiles, and distinguish individual-level antibiotic exposure (OHA vs NHA) rather than relying solely on protocol-based groupings. Critically, future trials must be based on a clear, internationally accepted consensus definition of CAA. Additionally, consistent definitions for outcomes such as IAA, SSI, and readmissions are essential to ensure comparability across studies. Until such trials are available, a cautious, individualized approach to OHA prescription—grounded in objective resolution criteria—may best balance safety with antimicrobial stewardship in pediatric CAA.
Authorship Contribution statement
JAM: Conceptualization and study design; literature search and selection; data curation and extraction; formal analysis; investigation; methodology; project administration; resources; validation; visualization; writing – original draft; writing – review and editing. MRJ: Literature search and selection; data curation and extraction; writing, review, and editing.
Conflicts Of Interest
The authors declare that they have no conflict of interest.
Financial Statement/Funding
This review did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors, and none of the authors has external funding to declare.
Ethical Approval
This study did not involve the participation of human or animal subjects, and therefore, IRB approval was not sought.
Statement Of Availability of the Data Used During the Systematic Review
All data used for the meta-analytical models are available in the accompanying supplementary dataset file.
Funding
None.
Registration
PROSPERO (CRD420251049919).
References
- Ossai, C.R.; Pu, L.; Kaelber, D. Using Aggregated Data from 1.4 Million Pediatric Patients to Describe the Epidemiology and Demographic Characteristics of Appendicitis. Pediatrics 2020, 146, 232–234. [Google Scholar] [CrossRef]
- Omling, E.; Salö, M.; Saluja, S.; Bergbrant, S.; Olsson, L.; Persson, A.; Björk, J.; Hagander, L. Nationwide study of appendicitis in children. Br. J. Surg. 2019, 106, 1623–1631. [Google Scholar] [CrossRef] [PubMed]
- Georgeades, C.; Bodnar, C.; Bergner, C.; Van Arendonk, K.J. Association of complicated appendicitis with geographic and socioeconomic measures in children. Surgery 2024, 176, 1475–1484. [Google Scholar] [CrossRef]
- Michelson, K.A.; Bucher, B.T.; Neuman, M.I. Cost and Late Hospital Care of Publicly Insured Children After Appendectomy. J. Surg. Res. 2024, 297, 41–46. [Google Scholar] [CrossRef]
- Wang, C.; Li, Y.; Ji, Y. Intravenous versus intravenous/oral antibiotics for perforated appendicitis in pediatric patients: a systematic review and meta-analysis. BMC Pediatr. 2019, 19, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.Y.; Beaudry, P.; Simms, B.A.; Brindle, M.E. Impact of implementing a fast-track protocol and standardized guideline for the management of pediatric appendicitis. Can. J. Surg. 2021, 64, E364–E370. [Google Scholar] [CrossRef]
- Muehlstedt SG, Pham TQ, Schmeling DJ. The management of pediatric appendicitis: a survey of North American Pediatric Surgeons. J Pediatr Surg. 2004 Jun;39(6):875-9; discussion 875-9. [CrossRef]
- Huttner B, Harbarth S, Carlet J, et al. Antibiotics are not automatic anymore—the French national campaign to cut antibiotic overuse. PLoS Med. 2010;7(7):e1000353. [CrossRef]
- Sabuncu, E.; David, J.; Bernède-Bauduin, C.; Pépin, S.; Leroy, M.; Boëlle, P.-Y.; Watier, L.; Guillemot, D. Significant Reduction of Antibiotic Use in the Community after a Nationwide Campaign in France, 2002–2007. PLOS Med. 2009, 6, e1000084. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement : an updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024). Cochrane, 2024. Available from www.cochrane.org/handbook.
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Veroniki, A.A.; Jackson, D.; Viechtbauer, W.; Bender, R.; Bowden, J.; Knapp, G.; Kuss, O.; Higgins, J.P.; Langan, D.; Salanti, G. Methods to estimate the between-study variance and its uncertainty in meta-analysis. Res. Synth. Methods 2015, 7, 55–79. [Google Scholar] [CrossRef]
- IntHout, J.; Ioannidis, J.P.; Borm, G.F. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med Res. Methodol. 2014, 14, 25–25. [Google Scholar] [CrossRef]
- Röver, C.; Knapp, G.; Friede, T. Hartung-Knapp-Sidik-Jonkman approach and its modification for random-effects meta-analysis with few studies. BMC Med Res. Methodol. 2015, 15, 1–7. [Google Scholar] [CrossRef] [PubMed]
- 2288-14-25. PMID: 24548571; PMCID: PMC4015721Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088-1101.
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Lin, L. The trim-and-fill method for publication bias: Practical guidelines and recommendations based on a large database of meta-analyses. Medicine 2019, 98, e15987. [Google Scholar] [CrossRef]
- Desai, A.A.; Alemayehu, H.; Holcomb, G.W.; Peter, S.D.S. Safety of a new protocol decreasing antibiotic utilization after laparoscopic appendectomy for perforated appendicitis in children: A prospective observational study. J. Pediatr. Surg. 2015, 50, 912–914. [Google Scholar] [CrossRef]
- Anderson, T.K.; Bartz-Kurycki, M.A.; Kawaguchi, A.L.; Austin, M.T.; Holzmann-Pazgal, G.; Kao, L.S.; Lally, K.P.; Tsao, K. Home Antibiotics at Discharge for Pediatric Complicated Appendicitis: Friend or Foe? J. Am. Coll. Surg. 2018, 227, 247–254. [Google Scholar] [CrossRef]
- Bonasso, P.C.; Dassinger, M.S.; Wyrick, D.L.; Smith, S.D.; Burford, J.M. Evaluation of white blood cell count at time of discharge is associated with limited oral antibiotic therapy in children with complicated appendicitis. Am. J. Surg. 2019, 217, 1099–1101. [Google Scholar] [CrossRef]
- Rossidis, A.C.; Brown, E.G.; Payton, K.J.; Mattei, P. Implementation of an evidence-based protocol after appendectomy reduces unnecessary antibiotics. J. Pediatr. Surg. 2020, 55, 2379–2386. [Google Scholar] [CrossRef]
- Ferguson, D.M.; Parker, T.D.; Arshad, S.A.; Garcia, E.I.; Hebballi, N.B.; Tsao, K. Standardized Discharge Antibiotics May Reduce Readmissions in Pediatric Perforated Appendicitis. J. Surg. Res. 2020, 255, 388–395. [Google Scholar] [CrossRef]
- Gordon, A.J.; Choi, J.-H.; Ginsburg, H.; Kuenzler, K.; Fisher, J.; Tomita, S. Oral Antibiotics and Abscess Formation After Appendectomy for Perforated Appendicitis in Children. J. Surg. Res. 2020, 256, 56–60. [Google Scholar] [CrossRef]
- Ketha, B.; Stephenson, K.J.; Dassinger, M.S.; Smith, S.D.; Burford, J.M. Eliminating Use of Home Oral Antibiotics in Pediatric Complicated Appendicitis. J. Surg. Res. 2021, 263, 151–154. [Google Scholar] [CrossRef]
- Plattner, A.S.; Newland, J.G.; Wallendorf, M.J.; Shakhsheer, B.A. Management and Microbiology of Perforated Appendicitis in Pediatric Patients: A 5-Year Retrospective Study. Infect. Dis. Ther. 2021, 10, 2247–2257. [Google Scholar] [CrossRef] [PubMed]
- Anandalwar, S.P.; Graham, D.A.; Kashtan, M.A.; Hills-Dunlap, J.L.; Rangel, S.J. Influence of Oral Antibiotics Following Discharge on Organ Space Infections in Children With Complicated Appendicitis. Ann. Surg. 2019, 273, 821–825. [Google Scholar] [CrossRef]
- Jen, J.; Hwang, R.; Mattei, P. Post-discharge antibiotics do not prevent intra-abdominal abscesses after appendectomy in children. J. Pediatr. Surg. 2022, 58, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Morita, K.; Fujiogi, M.; Michihata, N.; Matsui, H.; Fushimi, K.; Yasunaga, H.; Fujishiro, J. Oral Antibiotics and Organ Space Infection after Appendectomy and Intravenous Antibiotics Therapy for Complicated Appendicitis in Children. Eur. J. Pediatr. Surg. 2022, 33, 074–080. [Google Scholar] [CrossRef]
- Theodorou, C.M.; Lee, S.Y.; Lawrence, Y.; Saadai, P.; Hirose, S.; Brown, E.G. The Utility of Discharge Antibiotics in Pediatric Perforated Appendicitis Without Leukocytosis. J. Surg. Res. 2022, 275, 48–55. [Google Scholar] [CrossRef]
- Russell, K.W.; Skarda, D.E.; Jones, T.W.; Barnhart, D.C.; Short, S.S. Cessation of Antibiotics for Complicated Appendicitis at Discharge Does Not Increase Risk of Post-operative Infection. J. Pediatr. Surg. 2023, 59, 91–95. [Google Scholar] [CrossRef]
- Patwardhan, U.M.; Kahan, A.; Eldredge, R.S.; Russell, K.W.; Lee, J.; Short, S.S.; Padilla, B.; Cairo, S.B.; Acker, S.N.; Jensen, A.R.; et al. Comparison of Postoperative Antibiotic Protocols for Pediatric Complicated Appendicitis: A Western Pediatric Surgery Research Consortium Study. J. Pediatr. Surg. 2025, 60, 162165. [Google Scholar] [CrossRef] [PubMed]
- de Wijkerslooth, E.M.L.; Boerma, E.-J.G.; van Rossem, C.C.; van Rosmalen, J.; Baeten, C.I.M.; Beverdam, F.H.; Bosmans, J.W.A.M.; Consten, E.C.J.; Dekker, J.W.T.; Emous, M.; et al. 2 days versus 5 days of postoperative antibiotics for complex appendicitis: a pragmatic, open-label, multicentre, non-inferiority randomised trial. Lancet 2023, 401, 366–376. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart illustrating the search strategy and study selection process.
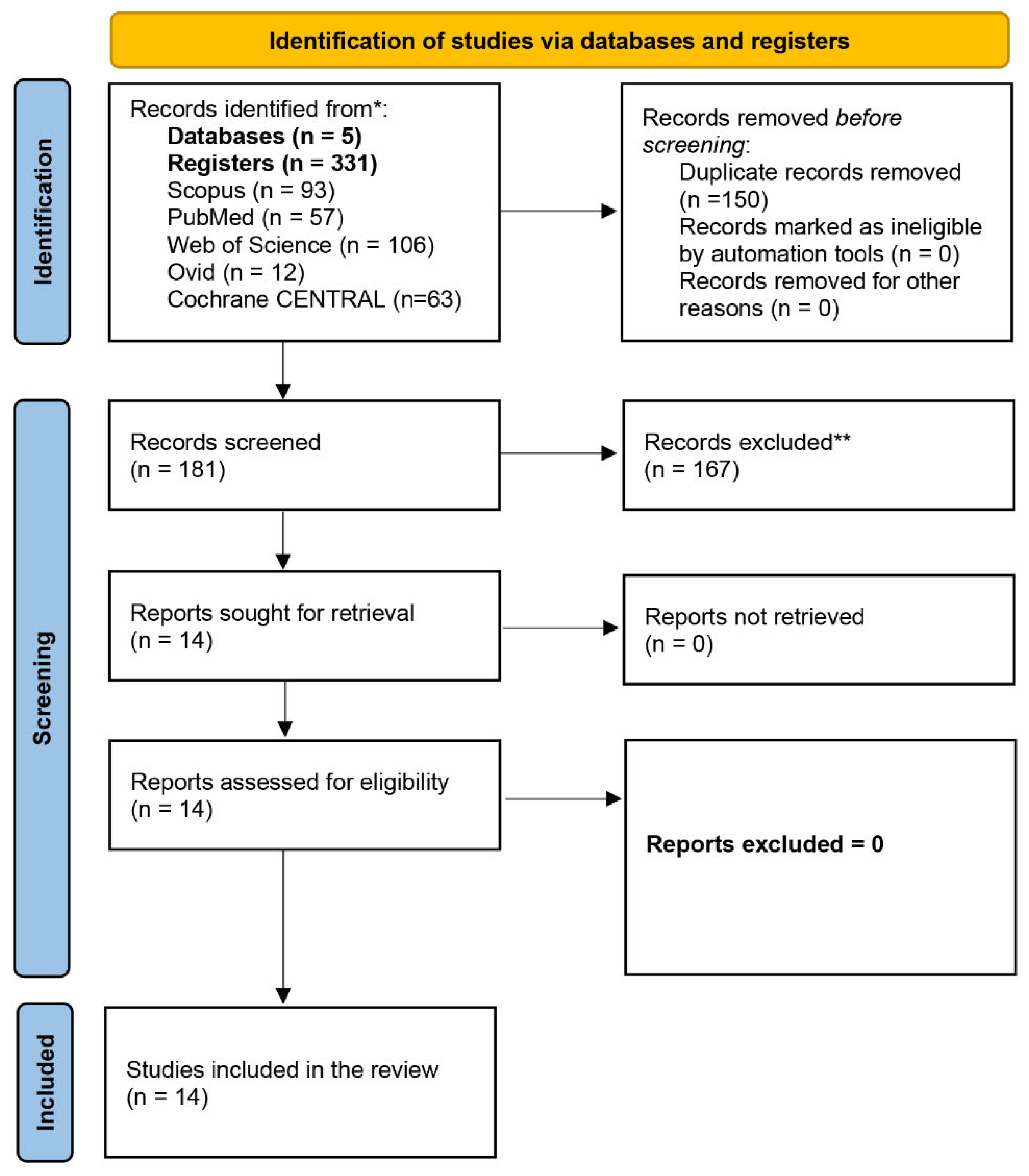
Figure 2.
Graphical summary of the risk of bias assessment using the ROBINS-I tool for the included non-randomized studies. Green circles with a plus sign indicate low risk of bias, yellow circles with a question mark represent moderate risk, and red circles with a minus sign denote high risk of bias.
Figure 2.
Graphical summary of the risk of bias assessment using the ROBINS-I tool for the included non-randomized studies. Green circles with a plus sign indicate low risk of bias, yellow circles with a question mark represent moderate risk, and red circles with a minus sign denote high risk of bias.
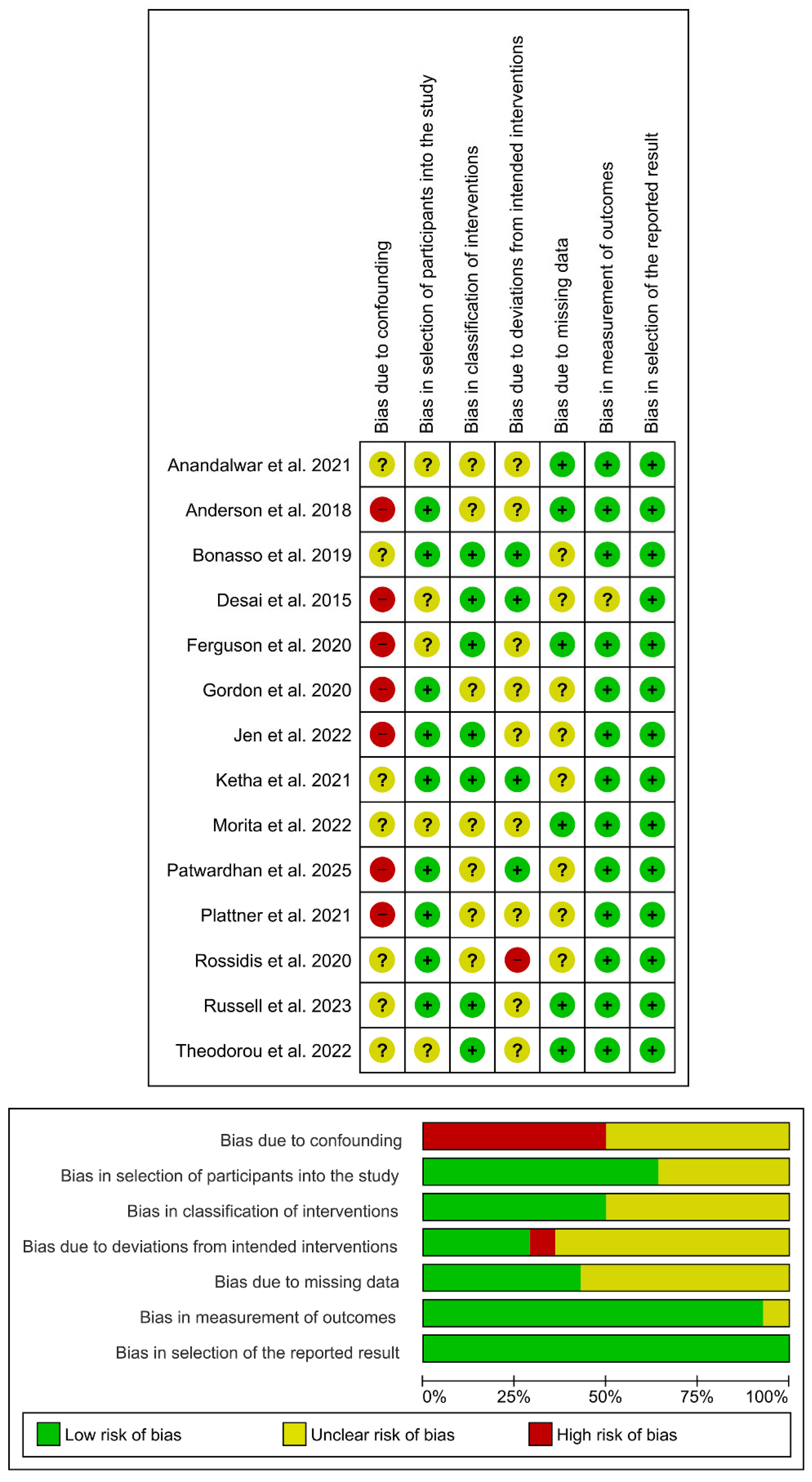
Figure 3.
Top: Forest plot of the random-effects meta-analysis for intra-abdominal abscesses (IAA) using REML with Knapp–Hartung adjustment for confidence intervals (IG vs. CG). Bottom: Leave-one-out forest plot for the same analysis.
Figure 3.
Top: Forest plot of the random-effects meta-analysis for intra-abdominal abscesses (IAA) using REML with Knapp–Hartung adjustment for confidence intervals (IG vs. CG). Bottom: Leave-one-out forest plot for the same analysis.
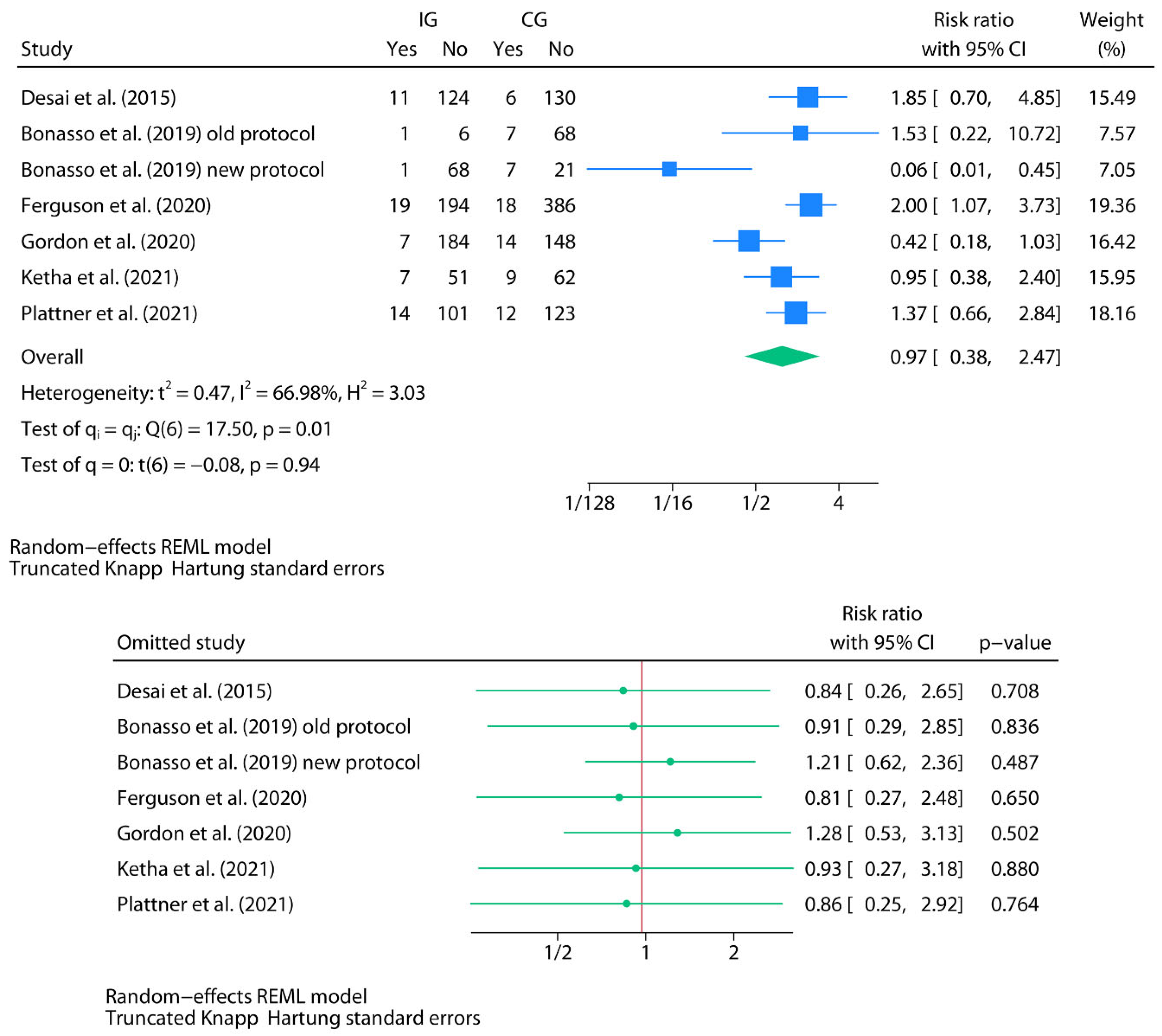

Table 1.
Summary of publications included in this review.
| f | Country | Study design | Age | Sex M/F | Total N | Group definitions | N in IG | N in CG | Discharge criteria and TLC value | Antibiotics and posology (type, duration, route) | Events by group (IG/CG) | p-value | Commentaries |
| Desai et al. (2015) [20] | USA | Prospective |
IG: 9.6(3.8)y1 CG: 10(3.9)y1 |
IG: 60/210 CG: 150/120 |
540 |
CAA (PAA): hole in the appendix or fecalith in the abdomen IG: new protocol CG: old protocol |
270 152 discharged before day 5 (135/152 NHA and 17/152 OHA) |
270 136 discharged before day 5 (136/136 OHA) |
DC: -Regular diet tolerance -Controlled pain with oral medications -No fever over the previous 12 hours Preoperative TLC by group: IG: 17.6 (5.7)1 CG: 17.4 (5.8)1 (p=0.7) Predischarge TLC by group: IG: 8.6 (2.4)1 CG: 16.9 (3.5)1 (p<0.001) |
Old protocol: Preoperative doses of ceftriaxone and metronidazole. 50 mg/kg (max. 2 gr) IV ceftriaxone and 30 mg/kg (max. 1 gr) IV metronidazole every 24 hours -If 5 days IVA: NHA -If <5 days IVA: 7 days OHA (amoxicillin-clavulanate) Newprotocol: Preoperative doses of ceftriaxone and metronidazole. 50 mg/kg (max. 2 gr) IV ceftriaxone and 30 mg/kg (max. 1 gr) IV metronidazole every 24 hours -If 5 days IVA: NHA -If <5 days IVA and leukocytosis: 7 days OHA (amoxicillin-clavulanate) If <5 days IVA and no leukocytosis: NHA |
IAA: IG (global): 12/152 IG (NHA): 11/135 IG (OHA): 1/17 CG (OHA): 6/136 |
IAA (IG vs. CG):0.3 | The number of male cases in the study group (60 out of 270) is strikingly low and does not realistically reflect the expected sex-based prevalence of the disease. |
| Anderson et al. (2018) [21] | USA | Retrospective (NSQIP-Pediatric 2015-2016 database) |
IG: 10.4(4)y1 CG: 10.1(4)y1 |
IG:1,699/1,099 CG: 2,116/1,498 |
6,412 |
CAA: visible hole in the appendix, fecalith in the peritoneal cavity outside the appendix, abscess, or diffuse fibrinopurulent exudate in the peritoneal cavity IG: NHA CG: IVHA + OHA |
2,798 |
3,614 OHA: 3,426/3,614 IVHA: 188/3,614 |
Preoperative TLC by group: IG: 16.0 (5.7)1 CG: 17.2 (5.3)1 (p<0.01) Predischarge TLC by group: NS |
NS |
CPDM: IG (NHA): 315/2,798 CG (IVHA+OHA): 522/3,614a EDV: IG (NHA): 269/2,798 CG (IVHA+OHA): 463/3,614a RA: IG (NHA): 153/2,798 CG (IVHA+OHA): 286/3,614a RO: IG (NHA): 17/2,798 CG (IVHA+OHA): 41/3,614a SSI: IG (NHA): 92/2,798 CG (IVHA+OHA): 163/3,614a |
CPDM, EDV, RA: <0.01 RO: 0.03 SSI: 0.01 |
188 patients (2.9%) received IVHA instead of OHA, and the analyses did not adequately stratify the OHA group from the IVHA group. The authors were contacted to request the raw data, but no response was received. This should be considered a limitation when interpreting the present study's data. As this was a retrospective review of a national database, there were no standardized discharge criteria prior to hospital discharge in either group nor was a antibiotics and posology report, which may represent a major source of heterogeneity. |
| Bonasso et al. (2019) [22] | USA | Retrospective |
IG:9.28y2 CG:9.37y2 |
IG: 55/42 CG:56/26 |
179 |
CAA: GA, PAA IG: NHA CG: OHA |
97 NHA: 69/97 OHA: 28/97 |
82 NHA: 7/82 OHA: 75/82 |
DC: -Diet tolerance -Controlled pain with oral medications -No fever (<38.5°C) Preoperative TLC by group: NS Predischarge TLC by group: NS |
Old protocol: Preoperative doses of ceftriaxone and metronidazole. 50 mg/kg IV ceftriaxone and 30 mg/kg IV metronidazole every 24 hours -If <10 days IVA: OHA until 10 days of ATB treatment completionb Newprotocol: Preoperative doses of ceftriaxone and metronidazole. 50 mg/kg IV ceftriaxone and 30 mg/kg IV metronidazole every 24 hours -If TLC was elevated: OHA until 7 days of ATB treatment completionb -If normal TLC: NHA |
IAA: CG (global): 8/82 IG (Global): 10/97 OHA: 7/75 NHA: 1/7 RA: CG (global): 11/82 IG (global): 12/97 OHA: 7/28 NHA: 1/69 |
RA: 1 | Although the authors reported 9 additional intra-abdominal abscesses in the CG group and 9 in the IG group (all corresponding to patients who remained hospitalized and continued on IV antibiotic therapy), these cases were excluded from the group-specific event counts (global), as they are not within the scope of the present review. The authors report 17 abscesses in the CG and 19 in the IG, with 9 inpatient abscesses in both groups. However, for the IG, the total counts are inconsistent: they report 19 abscesses, of which 9 occurred during hospitalization, 7 in the OHA subgroup, and 1 in the NHA subgroup, resulting in a discrepancy of 2 cases. We contacted the authors to clarify this issue, but did not receive a response. Although n=28 is inferred for the OHA subgroup (total N=97 minus n=69 discharged without antibiotics, per author's Table 1, the original study's Table 1 uses n=20 for calculating the mean duration of home oral antibiotics, indicating an internal data inconsistency. |
| Rossidis et al. (2020) [23] | USA | Retrospective |
IG:12(9-14)y3,c CG:11(8-14)y3,c |
IG: 489/325c CG: 448/300c |
1,562c (PAA: 338) |
PAA: a visible hole in the appendix, a free fecalith, diffuse peritonitis, or an abscess at the time of surgery IG: new protocol CG: old protocol |
814c (PAA: 175) OHA: 59/175 NHA: 116/175 |
748c (PAA: 163) OHA: 145/163 NHA: 18/163 |
DC: -Diet tolerance -Controlled pain with oral medications -No fever (≥ 24 hours) Preoperative TLC by group: NS Predischarge TLC by group: NS |
Old protocol: Postoperative ATB 7-14 days (empirically) Most patients with OHA (empirically) Newprotocol: NHA IG: 59/175 OHA CG: 145/163 OHA |
RA: CG (global): 5/163d IG (global): 9/175d SSI: CG (global): 11/163d IG (global): 8/175d EDV: CG (global): 13/163d IG (global): 18/175d RO: CG (global): 1/163d IG (global): 2/175d |
RA: 0.42 EDV: 0.57 SSI: 0.48 RO: 0.99 |
Although it is understood that the study refers to OHA rather than IVHA, this is not explicitly stated at any point in the manuscript. The authors were contacted to confirm this information, but they did not respond. The authors did not report having determined TLC before discharge. The article provides overall data for the old protocol and new protocol groups, but does not report raw data for patients with OHA and NHA. We contacted the corresponding author to clarify this information, but did not receive a response. |
| Ferguson et al. (2020) [24] | USA | Retrospective |
IG:9.7(3.9)y1 CG:10.1(3.9)y1, |
IG: 120/93 CG: 258/146 |
617 |
PAA: intra- operative visualization of a hole in the appendix, intra- abdominal stool, or intra-abdominal fecalith IG: old protocol CG: new protocol |
213 OHA: 12/213 NHA: 201/213 |
404 OHA: 397/404 NHA: 7/404 |
DC: -Diet tolerance -Controlled pain with oral medications -No fever (≥ 24 hours) -No unexpected abdominal pain -No emesis -Normal TLC Preoperative TLC by group: IG: 17.9 (5.7)1 CG: 17.5(5.3)1 (p=0.42) Predischarge TLC by group: NS |
Preoperative ATB Piperacillin-tazobactam 100 mg/kg/dose IV every 8 h (<40 kg) or 3.375 g IV every 6h (40 kg) Or Cefepime 50 mg/kg/dose IV every 12 h, (max. 2 g/dose) Plus Metronidazole 10 mg/kg/dose IV every 8 h (max. 500 mg/dose) Postoperative ATB Amoxicillin-clavulanate 25-45 mg/kg/d PO divided every 12 h (<40 kg) or 500-875 mg/ dose every 12 h (40 kg) Old protocol (IG): no OHA standardization (12/213 OHA, 201/213 NHA) New protocol (CG): OHA (7 additional days) to all patients at discharge (397/404 OHA, 7/404 NHA) Amoxicilin-clavulanate (n=382), ciprofloxacin + metronidazole (n=13), others (n=2) |
IAA IG (global): 19/213 CG (global): 18/404 SSI: IG (global): 2/213 CG (global): 3/404 EDV IG (global): 10/213 CG (global): 15/404 RAe IG (global): 28/213 CG (global): 26/404 ROe IG (global): 2/213 CG (global): 2/404 |
IAA: 0.03 SSI: 0.8 RO: 0.51 EDV: 0.56 RA: 0.005 |
Patients who underwent conversion to open surgery, as well as those who had primary open appendectomy or remained hospitalized for 8 or more days, were excluded, which may introduce a potential selection bias. For the purposes of this review, the pre-standardization group has been defined as the intervention group (IG) and the post-standardization group as the control group (CG), since the authors standardized the practice of prescribing, rather than withholding, OHA. The article provides overall data for the old protocol and new protocol groups, but does not report raw data for patients with OHA and NHA. We contacted the corresponding author to clarify this information, but did not receive a response. Patients were excluded if an open or laparoscopic-converted-to-open appendectomy was performed. |
| Gordon et al. (2020) [25] | USA | Retrospective |
IG: 8.0 (6.0-11)y 3 CG: 9.0 (6.0-12)y 3 |
157/96 | 253 |
CAA (PAA): Perforation of the appendix without abscess or phlegmon before surgery or identification of a perforated appendix intra- operatively IG: new protocol (NHA) CG: old protocol (OHA) |
91 | 162 |
DC: -Afebrile for at least 24 h -Tolerating a regular diet -Minimal abdominal tenderness -Normal TLC Preoperative TLC by group: IG: 16.6(13.9-19.7)3 CG: 16.8(13.8-20.3)3 (p=0.57) Predischarge TLC by group: IG: 8.1(6.8-10.4)3 CG: 9.5(7.4-10.9)3 (p=0.02) |
Old protocol: While admitted: IV piperacillin/tazobactam or IV meropenem OHA (ciprofloxacin/metronidazole or amoxicillin/clavulanate) New protocol: While admitted: IV piperacillin/tazobactam or IV meropenem NHA |
IAA IG (NHA): 7/91 CG (OHA): 14/162 RA IG (NHA): 10/91 CG (OHA): 17/162 |
IAA: 0.99 RA: 0.99 |
Although all patients who underwent appendectomy before November 2017 were discharged on OHA, the length of the antibiotic course was not standardized. This varied from 5 to 14 d based on the discretion of each surgeon. In addition, patients who were sent home without antibiotics (NHA) had significantly lower TLC counts at the time of discharge (p=0.02). |
| Ketha et al. (2021) [26] | USA | Retrospective |
IG: 8.8y2 CG: 9y2 |
72/57 | 129 |
PAA: clinically perforated appendicitis at time of surgery as noted on operative reports. IG: new protocol (NHA) CG: old protocol |
58 (OHA:0/58 NHA: 58/58) |
71 (OHA: 16/71 NHA: 55) |
DC: -Afebrile for 24 h (<38.5 C) - Adequate diet tolerance. - Adequate pain control with oral medications. Preoperative TLC by group: NS Predischarge TLC by group: NS |
Old protocol: Preoperative: ceftriaxone 50 mg/kg and metronidazole 30 mg/kg IV While admitted: ceftriaxone 50 mg/kg and metronidazole 30 mg/kg IV once daily If DC accomplished before day 7, TLC was checked. If TLC >13.5x109/L, OHA (amoxicillin/clavulanic acid) 7 days If TLC ≤ 13.5x109/L, NHA New protocol: Preoperative: ceftriaxone 50 mg/kg and metronidazole 30 mg/kg IV While admitted: ceftriaxone 50 mg/kg and metronidazole 30 mg/kg IV once daily NHA |
IAA IG (NHA): 7/58 CG (global): 9/71 RA IG (NHA): 10/58 CG (global): 9/71 |
IAA: 1 RA: 0.61 |
Doesn´t specify if the abscess occurs post-discharge The article provides overall data for the old protocol and new protocol groups but does not report raw data for patients with OHA and NHA. We contacted the corresponding author to clarify this information but did not receive a response. |
| Plattner el al. (2021) [27] | USA | Retrospective | 10.3 (3.9) y1 | 56%/44% 186/147g |
333 (295)f |
PAA: Presence of intra-luminal contents outside of the bowel at time of surgery (as per the operative note) IG: NHA CG: OHA, IVHA, OHA+IVHA |
NHA:115 | 180 (OHA, IVHA, OHA + IVHA) OHA: 135/180 |
DC: NS TLC: NS Preoperative TLC by group: NS Predischarge TLC by group: IG: 92 CG: 10.62 (p<0.001) |
Broad-spectrum antibiotic coverage: meropenem, piperacillin-tazobactam, and/or a fourth-generation cephalosporin. Narrow-spectrum antibiotic coverage: metronidazole plus a third-generation cephalosporin, most commonly ceftriaxone IG: NHA CG: OHA, IVHA, OHA+IVHA |
IAA IG (NHA): 14/115g CG (OHA+IVHA+OHA/IVHA): 38/180g CG (OHA): 12/135g RA IG (NHA): 9/115g CG (OHA+IVHA+OHA/IVHA): 14/180g CG (OHA): 11/135g |
IAA: OHA+IVHA+OHA/IVHA: <0.01 OHA vs. NHA: 0.79 RA: OHA vs. NHA: 0.39 |
The study included 333 patients, but only 295 underwent appendectomy. The choice between narrow and broad-spectrum antibiotic coverage was at surgeon´s discretion Initial broad-spectrum antibiotic use was associated with increased odds of postoperative abscess formation (OR 3.17, 95%CI 1.58-6.38) Patients with home antibiotics (OHA, IVHA and mixed OHA + IVHA) had a significantly higher rate of postoperative abscess formation than NHA while patients with OHA did not differ in abscess formation compared to the NHA group. The average discharge TLC was significantly higher in the group of patients who experienced readmission compared to those who did not (p<0.001). |
| Anandalwar et al. (2021) [28] |
USA | Retrospective (NSQIP-P database from January 2013 to June 2015) | 10 (7-17) y3 |
Before PM: 416/370 After PM: 334/240 |
Before PM: 711 (786) PM: 574 |
CAA: Presence of a visible hole, diffuse fibrinopurulent exudate extending outside the right lower quadrant and pelvis (defined as exudate in more than two quadrants of the abdomen and pelvis), intra-abdominal abscess, or an extra-luminal fecalith IG: NHA CG: OHA |
Before PM: 306 After PM: 287 |
Before PM: 405 After PM: 287 |
DC: NS Preoperative TLC by group (before PM): IG: 74 (24.2)5 CG: 91 (22.5)5 (p=0.02) Preoperative TLC by group (after PM): IG: 72 (25.1)5 CG: 77 (26.8)5 (p=0.89) Predischarge TLC by group: NS |
NS |
OSI (before PM)h: IG (NHA): 6.2% 19/306g CG (OHA): 4.4% 18/405g OSI (after PM)h: IC (NHA): 6.6% 19/287g CG (OHA): 4.2% 12/287g RA (after PM): IC (NHA): 5.9% 17/287g CG (OHA): 5.6% 16/287g |
OSI (before PM): 0.30 OSI (after PM: 0.21 RA (after PM): 0.71 IAA: 0.30 |
Since this work reports data from a database that includes 29 NSQIP-Pediatric hospitals, therefore it can´t be assumed that discharge criterion, and the antibiotic used and its posology was consistent among all the hospitals, as it has not been specified on the paper. Adjusted analyses (after PM) showed no statistically significant differences between groups (OHA/NHA) for either OSI or RA. The sex distribution table reflects the pre-exclusion cohort (n=786), which explains why male + female totals exceed the final sample. After excluding patients with inpatient imaging or IV antibiotics at discharge, the analytic cohort was reduced to 711 |
| Jen et al. (2022) [29] | USA | Retrospective | Main study arm (no initial DSI): IG: 9.9 (4.0)y1 CG: 10.2 (4.2) y1 |
232/173 Main study arm (no initial DSI): 203/160 |
405 Main study arm (no initial DSI):363 |
CAA: (PAA): either intraoperative or pathologic findings of PAA IG: NHA CG: OHA |
288 Main study arm (no initial DSI): 277 |
117 Main study arm (no initial DSI): 86 |
DC: based on attending surgeon preference but based on somewhat standardized guidelines that included remaining afebrile for at least 24 h, tolerating a regular diet, and having pain that was well-controlled with oral analgesics. Preoperative TLC by group: IG: 16.9(5.3)1 CG: 17.5(6.4)1 (p=0.36) Predischarge TLC by group: NS |
Initial antibiotics Ceftriaxone/metronidazole (CG,n=75; IG, n=259) Piperacillin/tazobactam (CG, n=6; IG, n=8) Other (CG, n=5; IG, n=10) OHA (CG): Ciprofloxacin/metronidazole (n=72) Amoxicillin-clavulanate (n=12) Other (n=2) |
OSI: IG (NHA): 9/277 CG (OHA): 4/86 EDV: IG (NHA): 23/277 CG (OHA): 10/86 RA: IG (NHA): 10/277 CG (OHA): 6/86 SSI: IG (NHA): 5/277 CG (OHA): 0/86 |
OSI: 0.54 EDV: 0.35 RA: 0.18 SSI: 0.21 |
The authors do not analyze the presence of OSI, EDV, RA or SSI based on the antibiotics administered. The use of multiple different antibiotics and regimens without protocol may constitute a relevant source of heterogeneity. |
| Morita et al. (2022) [30] | Japan | Retrospective (Diagnosis Procedure Combination database) | 3-18y4 | Before PM: 7,842/5,258 After PM: 3,330/2,208 |
Before PM: 13,100 After PM: 5,538 |
CAA: NS IG: NHA CG: OHA |
Before PM: 9,599 After PM:2,769 |
Before PM: 3,501 After PM:2,769 |
DC: NS Preoperative TLC by group: NS Predischarge TLC by group: NS |
NS |
RA due to OSI (before PM): IG (NHA): 333/9,599 CG (OHA): 163/3,501 RA due to OSI (after PM): IG (NHA): 93/2,769 CG (OHA): 145/2,769 Global RA (within 60 days of discharge) (before PM): IG (NHA): 549 /9,599 CG (OHA): 247/ 3,501 Global RA (within 60 days of discharge) (after PM): IG (NHA): 153/2,769 CG (OHA): 205/2,769 |
RA due to OSI (PM): 0.002 RA due to OSI (after PM: 0.001 Global RA (before PM): 0.005 Global RA (after PM): 0.004 |
Since this work reports data from a nationwide database that includes more than 1,200 hospitals, therefore it can´t be assumed that discharge criterion, and the antibiotic used and its posology was consistent among all the hospitals, as it has not been specified on the paper. |
| Theodorou et al. (2022) [31] | USA | Retrospective |
Old protocol: 8.9 (6.2-11.4) y3 New protocol: 9.2 (6.7-12.3) y3 |
132/78 | 210 |
CAA: PAA: hole in the appendix, a fecalith in the abdomen, with or without an associated abscess or purulent fluid. IG: New protocol CG: Old protocol |
97 OHA: 14/97 |
113 OHA: 80/113 |
DC: -Afebrile for 24 h - Tolerating a diet -Pain manageable with oral medications -A benign examination Preoperative TLC by group: IG: 16.3(14-18.23 CG: 18.5(14.8-21.93 (p=0.003) Predischarge TLC by group: IG: 9.2(7.3-10.7)3 CG: 8.9(7.7-10.9)3 (p=0.77) |
Preoperative administration of intravenous IV ceftriaxone and metronidazole Postoperative treatment: NS Old protocol: If normal TLC: 5 days OHA If abnormal TLC: 10 days OHA OHA: 80/113; NHA: 33/113 New protocol If normal TLC: NHA If abnormal TLC: 10 days OHA OHA: 14/97; NHA: 83/97 |
SSI: IG (global): 9/97 CG (global): 2/113 NHA: 8/116g OHA: 3/94g RA: IG (global): 11/97 CG (global): 6/113 |
SSI (CG vs. IG): 0.03 SSI (OHA vs. NHA): 0.53 RA: 0.13 |
Open appendectomy patients were excluded as there may be a higher rate of surgical site infections in this patient population compared to laparoscopic appendectomy The authors do not specify a cut-off point for TLC. There were no significant differences in TLC at discharge between the SSI and non-SSI groups. The article provides overall data for the old protocol and new protocol groups, but does not report raw data for patients with OHA and NHA. We contacted the corresponding author to clarify this information, but did not receive a response. The authors report proportions conditioned on outcome: 3/11 patients with SSI (27.3%) received antibiotics, and 91/199 without SSI (45.7%) did. However, restructuring the data by treatment group shows that 3 of 94 patients who received antibiotics developed SSI (3.2%), compared to 8 of 116 without antibiotics (6.9%). This corresponds to infected:non-infected ratios of 0.03 (3/91) in the antibiotic group and 0.07 (8/108) in the no-antibiotic group—identical to the original data but correctly aligned for effect estimation. |
| Russell et al. (2023) [32] | USA | Retrospective (NSQIP database from January 2015 to May 2022) |
Old protocol: 9.8(4) y1 New protocol: 9.6(4) y1 |
173/133g | 306 |
CAA: Presence of a visible hole, diffuse fibrinopurulent exudate (defined as exudate in >2 quadrants of the abdomen and pelvis), intra-abdominal abscess, or an extraluminal fecalith IG: new protocol CG: old protocol |
121 OHA:10/121 NHA:111/121 |
185 OHA:170/185g IVHA:1/185g NHA:14/185g |
DC: -Adequate oral intake -Feeling generally well. -No fever (<38.5ºC) Preoperative TLC by group: IG: 17(5.9)1 CG: 17.7(6.2)1 (p=0.24) Predischarge TLC by group: NS |
In both protocols, patients were treated with intravenous (IV) Ceftriaxone and IV Metronidazole while hospitalized. CG: The CG was discharged home on OHA (Augmentin or Cefdinir and Metronidazole if they had an allergy to Augmentin) if their TLC was elevated at the time of discharge IG: NHA. No predischarge TLC check. |
SSI: IG (global): 3/121 CG (global): 3/185 OSI: IG (global): 9/121 CG (global): 13/185 RA: IG (global): 9/121 CG (global): 11/185 |
SSI: 0.68 OSI: 1 RA: 0.64 |
The article provides overall data for the old protocol and new protocol groups but does not report raw data for patients with OHA and NHA. We contacted the corresponding author to clarify this information but did not receive a response. |
| Patwardhan Et al. (2025) [33] |
USA | Retrospective (NSQIP-P database from 2021 to 2023) |
No-OHA: 9.3 (4.3) y1 OHA if high TLC: 10.1 (4.0) y1 OHA to complete a minimum number of total postoperative ATB days: 9.5 (4.0) y1 Standardized OHA discharge: 10.1 (3.7) y1 |
827/515 | 1,342 |
CAA: Intraoperative findings of CAA: the presence of a visible hole in the appendix, an intraperitoneal fecalith, diffuse fibrinopurulent exudate, or the presence of an abscess. IG: NHA cohort (cohort 1) CG: OHA cohort (cohort 4) |
158 OHA: 7/158 NHA: 151/158 |
64 OHA: 59/64 NHA: 5/64 |
DC: -Lack of fever -Resolution or significantly improving abdominal pain -Tolerance of adequate oral intake Preoperative TLC by group: IG: 17.1(6.0)1 CG: 17.3(6.2)1 (p=0.8)(4-groups comparison) Predischarge TLC by group: NS |
Postoperative antibiotic protocol used at each site was collected, with 6/9 centers using ceftriaxone/metronidazole as intravenous therapy while inpatient and 7/8 centers using amoxicillin/clavulanic acid as the oral antibiotic of choice on discharge (Original articles` Supplemental Table 1) IG: 7/158 OHA; 151/158 NHA CG: 59/64 OHA; 5/64 NHA |
SSI: IG (Global): 9/158 CG (Global): 6/64 RA: IG (Global): 12/158 CG (Global): 3/64 |
SSI (4-protocols comparison): 0.43 RA (4-protocols comparison): 0.06 |
Since this work reports data from a database that includes 29 NSQIP-Pediatric hospitals, therefore it can´t be assumed that discharge criterion, and the antibiotic used and its posology was consistent among all the hospitals. Hospitals were classified into four groups based on their protocol: 1) No OHA, 2) OHA if high TLC on the day of discharge, 3) OHA to complete a minimum number of total post-operative ATB days, and 4) standardized OHA discharge regardless of inpatient antibiotic duration. Only patients undergoing laparoscopic appendectomy were included. The article provides overall data for different protocols and new protocol groups but does not report raw data for patients with OHA and NHA. We contacted the corresponding author to clarify this information, but did not receive a response. |
NS: Not specified; y: Years.DC: Discharge criteria; IG: Intervention group (no oral antibiotic group); CG: Control group (post-discharge oral antibiotic group); CAA: Complicated acute appendicitis; PAA: Perforated acute appendicitis; GA: Gangrenous appendicitis;IV: intravenous; OHA: oral antibiotics (home); IVA: intravenous antibiotics (hospitalization); IVHA: intravenous antibiotics (home); NHA: no-home antibiotics; ATB: Antibiotics; IAA: Intraabdominal abscess (post-discharge); SSI: surgical site infection (post-discharge); CPDM: Composite post-discharge morbidity; EDV: Emergency Department visit; RA: Readmission; RO: Reoperation; OSI: organ-space infection (post-discharge), DSI: Deep space infection; TLC: Total leukocyte count (WBC);gr: grams;NSQIP: National Surgical Quality Improvement Program; PM: Propensity matching;1: Mean (standard deviation); 2: Mean; 3: Median (interquartile range); 4: range; 5: Highest quartile, n, (%);a: The CG group includes, without stratification, both patients with oral home antibiotics (n=3,426) and patients with intravenous home antibiotics (n=188); b: Although Bonasso et al. use the expression 'sent home with oral antibiotics to complete X days of treatment', which may create ambiguity as to whether 'X days' refers to the total duration of antibiotic therapy including inpatient administration or only the outpatient course, Table 1 of the paper suggests that 'X days' refers to the total duration of treatment; c: Rossidis et al. report age and sex distribution data for the overall cohort, without specifying the sociodemographic characteristics of the PAA group, which is the focus of the present study; d: The reported data refer to complications by overall group; however, specific complication rates for the OHA group and the NHA group were not provided.; e: In the study by Ferguson et al., statistically significant differences in readmission (RA) rates are reported between the IG and CG. However, this includes a broad range of signs and symptoms, and there is considerable variability in the distribution of etiologies between groups. For instance, in the group where OHA administration at discharge was standardized, a higher number of patients were readmitted with nonspecific diagnoses such as 'abdominal pain'. The rate of intra-abdominal abscess (IAA) as the reason for RA was 68% and 69% in the IG and CG, respectively; f: In the study by Plattner et al. the total number of patients included was 333 of which only 295 were initially managed surgically; g: Data estimated through inferential analysis based on the results reported in the article; h: OSI as defined by NSQIP: must meet all three of the following criteria: 1. Infection involves any part of the anatomy (organ/space) that was: Opened or manipulated during the operation, and is not the incision itself (i.e., not superficial or deep incisional). 2 The patient has at least one of the following signs or symptoms: Fever (>38°C), localized pain or tenderness and other clinical evidence of infection. 3. One of the following must be true: Purulent drainage from a drain placed into the organ/space, organism isolated from a culture of fluid/tissue from the organ/space, abscess or other infection found during reoperation, direct exam, histopathology, or imaging, or diagnosis of an organ/space infection made by a physician;.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



