
Submitted:
15 February 2024
Posted:
16 February 2024
You are already at the latest version
Abstract
Evidence regarding the role of oral antibiotics (oA) alone or combined with mechanical bowel preparation (MoABP) for elective colorectal surgery remains controversial. A prospective database of 8,359 colorectal resections gathered over a 32-month period in 78 Italian surgical units (the iCral 2 and 3 studies), reporting patient-, disease-, and procedure-related variables together with 60-day adverse events, was re-analyzed to identify a subgroup of 1,013 cases (12.1%) that received either oA or MoABP. This dataset was analyzed using a 1:1 propensity score-matching model including 20 covariates. Two well-balanced groups of 243 patients each were obtained: group A (oA), and group B (MoABP). The primary endpoints were anastomotic leakage (AL) and surgical site infections (SSIs) rates. Group A vs. group B showed a significantly higher AL risk [14 (5.8%) vs 6 (2.5%) events; OR 3.77; 95%CI 1.22-11.67; p = .021], while no significant difference was recorded between the two groups regarding SSIs. These results strongly support the use of MoABP for elective colorectal resections.
Keywords:
Colorectal surgery
; Mechanical bowel preparation
; Oral antibiotics
; Anastomotic leakage
; Surgical site infections
; Morbidity
1. Introduction
The earliest literature report on bowel decontamination and surgery dates back to 1899 [1]. During the last 80 years, the use of mechanical bowel preparation (MBP), oral antibiotics (oA), and perioperative intravenous antibiotic prophylaxis (PIVAP) to reduce the incidence of anastomotic leakage (AL) and surgical site infections (SSIs) in elective colorectal surgery have shown time-related and geographic fluctuating trends, with clinical practice and guidelines remaining non-unique and inconclusive despite the extraordinary number of published studies [2]. The use of MBP started at the beginning of the last century, becoming usual practice in the 1930s until the beginning of the 1940s when the use of multiple oral nonabsorbable sulfa derivatives, active only against aerobic species in the colon, was studied together with MBP [3]. After the Second World War, the discovery of several new oral non-absorbable antibiotics active against aerobic and anaerobic species (Aminoglycosides, Tetracyclines, Polimixines, Macrolides, and, later on, nitroimidazoles) influenced the bowel preparation before elective colorectal surgery, favoring oA combined with MBP (MoABP) and the diffusion of intraperitoneal resections with immediate anastomosis [4]. Landmark studies from surgeons in Chicago [5,6] using oral administration of neomycin and erythromycin showed a dramatic reduction in AL and SSIs rates, leading to the widespread diffusion of MoABP among North American surgeons, reaching approximately 86% of cases at the end of the previous century [7]. At the same time, the introduction of parenteral cephalosporins and amoxicilline/clavulanate in the decades 1970-80 shifted the attention towards a major role of PIVAP in reducing SSIs rates, and led to the current evidence [8] and the strong recommendation of the World Health Organization [9] to administer a single preoperative (30 to 120′ minutes before the operation) intravenous dose of a cephalosporin and metronidazole, albeit with a conditional recommendation for the use of oA. At the beginning of current century, several randomized controlled trials (RCTs) failed to demonstrate any clear benefit of MBP alone, supporting the concept of no bowel preparation (NBP), leading to the recommendation to avoid MBP in systematic reviews [10,11], in both European [12] and Italian [13] Enhanced Recovery After Surgery (ERAS) society guidelines, and WHO guidelines [9]. Thereafter, the use of MoABP for colorectal surgery in North America dropped down to a 30-40% rate [14].
During the last ten years, however, the results of several large retrospective series stemming from the American College of Surgeons - National Surgical Quality Improvement Program (ACS-NSQIP) led to the resurgence of the belief that MoABP significantly decreases SSIs and overall morbidity (OM) rates compared with NBP [15,16,17,18,19,20,21,22]. Consequently, the guidelines of four large North-American societies (The American Society of Colon and Rectal Surgeons, the Society of American Gastrointestinal and Endoscopic Surgeons, the American Society for Enhanced Recovery, and the Perioperative Quality Initiative) recommended MoABP [23,24,25]. Thereafter, the number of patients treated with MoABP in North America rose again up to 80% of the cases [26]. The rate of adoption of MoABP among European surgeons seems to be more variable. It is currently used by 50% of Austrian-German [27] surgeons, while its use is much more limited (about 10% of cases) in Italy [28]. These figures will probably change in a near future, as very recently the European Association of Endoscopic Surgery, the European Society of ColoProctology, together with the Society of American Gastrointestinal and Endoscopic Surgeons published a joint guideline recommending MoABP [29], albeit supported by low-quality evidence due to variable adherence to PIVAP and great heterogeneity regarding oral antibiotics schedules [30].
During the last five years, three RCTs on this topic have been published. The first one, comparing NBP with MoABP [31] failed to detect significant differences in SSIs and AL rates, but it was largely underpowered. Another RCT comparing NBP with oA [32] showed that oral administration of ciprofloxacin 750 mg b.i.d. and metronidazole 250 mg t.i.d. the day before colon surgery significantly reduced SSIs. This trial, however, received some criticism related to the very low AL and major morbidity rates in both arms [33]; its authors launched another RCT comparing oA with MoABP, which is currently still recruting [34]. Finally, the third study compared PIVAP alone with PIVAP combined with oA [35] using different MBP schedules. It showed significantly reduced SSIs rates in the oA arm, particularly when oA was coupled with MBP, although the PIVAP schedule did not include metronidazole, as currently recommended since 2014 [8]. Moreover, although several other RCTs were launched, only one study comparing MoABP with MBP for rectal cancer [36] completed the planned enrollment, although its results are not yet available. Unfortunately, an interesting, long-awaited, four-arm RCT comparing NBP with oA, MBP, and MoABP for colon resections [37] was recently closed before completion owing to poor accrual.
The great heterogeneity of both oral and intravenous antibiotic prophylaxis schedules, coupled with the heterogeneity of mechanical bowel preparations (polyethylene glycol, sodium phosphate, picosulfate, etc.), determined an extraordinary number of possible combinations potentially evaluable by RCTs. Current evidence regarding the “optimal” bowel preparation for elective colorectal surgery, therefore, is inconclusive because: 1) MoABP probably reduces SSIs as well as anastomotic leakage compared with MBP alone; 2) oA alone might be as effective as MoABP, but this cannot be clearly determined yet; 3) whether NBP compared with MoABP has an influence on morbidity could not be determined yet [2]. When conclusive evidence from RCTs is lacking, or when researchers need to assess treatment effects based on real-life data, propensity score-matching analysis (PSMA) performed on data from prospective observational studies offers an alternative approach for estimating treatment effects. Based on these considerations, the Italian ColoRectal Anastomotic Leakage (iCral) study group estimated the effects of oA plus PIVAP (treatment variable) versus MoABP plus PIVAP before elective colorectal surgery through a PSMA of data derived from two prospective open-label observational multicenter studies [38,39].
2. Materials and Methods
2.1. Study design
This was a secondary unplanned ad hoc propensity score-matched re-analysis of two prospective cohorts of patients who had undergone colorectal surgery for malignant and benign diseases.
2.2. Patient population and data collection
A total of 8,359 patients who underwent colorectal resection with anastomosis were enrolled in two consecutive studies on explicit inclusion/exclusion criteria, in 78 surgical centers in Italy from January 2019 to September 2021: iCral2 [38] and iCral3 [39]. The inclusion criteria were American Society of Anesthesiologists (ASA) class I, II or III; elective or delayed urgency setting (defined as > 48 hours from admission in iCral2 and > 24 hours from admission in iCral3); and written informed consent for inclusion in the study and processing of sensitive data. The exclusion criteria were pregnancy; hyperthermic chemotherapy (HIPEC) for carcinomatosis; and incomplete data. The iCral2 study excluded patients with a protective stoma proximal to the anastomosis; however, these cases were included in the iCral3 study. Both studies followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [40].
To control for data imbalance derived from several treatment confounders, the present PSMA study included 1,013 patients (12.1%) out of 8,359 enrolled in the parent studies based on explicit exclusion criteria (Figure 1). The descriptive variables considered for the 1,013 patients are shown in Table 1. All 1,013 patients were treated with PIVAP; however, intravenous antibiotic schedules were not available.
To optimize the effectiveness of the PSMA by reducing the number of unmatched cases, continuous variables were categorized according to their median values. The true population of interest, defined by the treatment variable oA, included 406 patients (40.0%); the control population, defined by the variable MoABP, included 607 patients (60.0%). The overall adherence percentage to the ERAS recommendations was calculated using 19 items common to both parental studies (Table 1). Significant differences in age, nutritional status, indication for malignancy, type of surgical procedure, end-to-end anastomosis, hospital type, unit type, and percentage of adherence to ERAS items were detected between the oA and MoA groups. Patients in the MoABP control population prepared their bowels by drinking products containing polyethylene glycol the day before surgery. Patients in both groups received several different oral antibiotic schedules, the majority of which contained metronidazole, all of which provided both aerobic and anaerobic coverage (Table 2).
All enrolled patients were followed up for at least 8 weeks after surgery, recording and grading any adverse events according to Clavien-Dindo [41] and the Japanese Clinical Oncology Group-extended criteria (JCOG-EC) [42], as well as any reoperation, readmission, or death. Anastomotic leakage (AL) was defined according to the international consensus [43].
2.3. Outcomes
All outcomes were calculated at 60 days after the surgery. The primary outcomes were AL and SSIs, defined as superficial and/or deep surgical site infections (sdiSSIs) and deep wound dehiscence and/or abdominal collection/abscess [44]. The secondary outcomes were: 1) overall morbidity (any adverse event), 2) major morbidity (any adverse event grade > II), and 3) reoperation (any unplanned operation) rates. In this retrospective study, mortality, sdiSSIs, deep wound dehiscence, and abdominal collection/abscess were not considered between outcomes because the very small number of events in relation to the sample size (1,013 patients) would make the statistical results of the comparison between oA and MoABP groups burdened by inconsistency and unreliable [65,66].
2.4. Statistical analysis
This was a retrospective PSMA of two prospective cohorts, with sample sizes calculated and reported in the respective core papers [38,39]. Events per variable guideline were followed [45]. There were no missing data in the database of the 1,013 patients. The target of estimands was represented by the average treatment effect in the true population of interest (ATT). A propensity score-matching model [47,48] was used for the analysis (Figure 1). An adjusted logistic regression was used to estimate the propensity scores of the treatment and control groups. The exposure variable was a treatment that implied oA in elective colorectal surgery. Twenty covariates potentially affecting the treatment [49] were selected: age, sex, American Society of Anesthesiologists (ASA) class, body mass index (BMI), diabetes, chronic renal failure, nutritional status measured through the Mini Nutritional Assessment—Short Form (MNA-SF) [50], surgery for malignancy, center volume, hospital type (academic/metropolitan versus local/regional), surgical unit type (general versus oncologic/colorectal), mini-invasive surgery, standard surgical procedure, operation length (minutes), intra- or extra-corporeal anastomosis, stapled versus handsewn anastomosis, end-to-end anastomosis, preoperative blood transfusion(s), intra- and/or postoperative blood transfusion(s), and overall ERAS pathway adherence rates. To ensure that the treatment groups were balanced [51], we performed PSMA using the software “R©” (Version 4.2.2, The R Foundation© for Statistical Computing, Vienna, Austria, 2022). We used a nearest-neighbor approach with a logit distance metric and a caliper of 0.1 to minimize differences between the groups. We also used adjusted logistic regression to estimate the association between the treatment variable and outcomes. Balance in the matched groups was assessed by calculating the standardized mean difference (SMD), using a threshold of 0.1 (a standardized mean difference of less than 0.1 typically indicates a negligible difference between the means of the groups) and the general variance ratio (a variance ratio close to 1 indicates that variances are equal in the two groups). For outcome modelling, an adjusted logistic regression was performed based on a treatment variable represented by oA in elective colorectal surgery and on the same 20 covariates selected for the PSMA [52], presenting odds ratios (OR) and 95% confidence intervals (95%CI). The eventual effect of any unobserved confounder was tested through a sensitivity analysis [53], using the library “SensitivityR5” of the software R© (Version 4.2.2, The R Foundation© for Statistical Computing, Vienna, Austria, 2022) and presenting the  values (each 0.1 increment of values representing a 10%-odds of differential assignment to treatment due to any unobserved variable). Sidak-Bonferroni’s adjustment for multiple comparisons was applied, setting α = 0.025, because the two primary outcomes were not independent and were selected based on literature evidence [2].
values (each 0.1 increment of values representing a 10%-odds of differential assignment to treatment due to any unobserved variable). Sidak-Bonferroni’s adjustment for multiple comparisons was applied, setting α = 0.025, because the two primary outcomes were not independent and were selected based on literature evidence [2].
values (each 0.1 increment of values representing a 10%-odds of differential assignment to treatment due to any unobserved variable). Sidak-Bonferroni’s adjustment for multiple comparisons was applied, setting α = 0.025, because the two primary outcomes were not independent and were selected based on literature evidence [2].3. Results
In this series of 1,013 patients undergoing elective colorectal surgery for malignant and benign diseases, mortality events occurred in 4 patients (0.4%), 2 in the oA group and 2 in the MoABP group. Before propensity score matching, univariate analysis of the entire population of 1,013 patients showed no statistically significant differences in the primary and secondary outcomes between the oA and MoABP groups (Table 3).

Table 3.
Univariate analysis of outcomes in the entire population.
| Overall (No. 1013) | MoABP (No. 607) | oA (No.406) | |||||
|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | *OR (95%CI) | |
| AL | 37 | 3.7 | 21 | 3.5 | 16 | 3.9 | 1.14 (0.59-2.22) p=.689 |
| SSIs | 32 | 3.2 | 17 | 2.8 | 15 | 3.7 | 1.33 (0.66-2.70) p=.425 |
| OM | 239 | 23.6 | 135 | 22.2 | 104 | 25.6 | 1.20 (0.90-1.62) p=.215 |
| MM | 61 | 6.0 | 30 | 4.9 | 31 | 7.6 | 1.59 (0.95-2.67) p=.077 |
| Reoperation | 49 | 4.8 | 27 | 4.5 | 22 | 5.4 | 1.23 (0.69-2.19) p=.480 |
MoABP: Mechanical bowel preparation plus oral Antibiotics; oA: oral Antibiotics; *univariate Odds ratio estimation with Wolf valuation of the confidence intervals (CIs); AL: anastomotic leakage; SSIs: Superficial Surgical Site Infections; OM: overall morbidity; MM: major morbidity.
After propensity score matching, 486 patients were included, and two groups of 243 patients each were generated (Figure 1): the oA group (true population of interest), and MoABP group (control population). A good balance between the two groups was achieved (Figure 2 and Table 3) with a model variance ratio of 1.089.
Table 3.
Variables distribution in control and treatment groups before and after propensity score-matching.
Table 3.
Variables distribution in control and treatment groups before and after propensity score-matching.
| Before PSM | After PSM | ||||||||
| MoABP No. 609 |
oA No.406 |
MoABP No. 243 |
oA No.243 |
||||||
| Covariates | Pattern | *p | **SMD | *p | **SMD | ||||
| Age | ≤ 69 years | 324 | 283 | .039 | 0.14 | 128 | 118 | .414 | 0.08 |
| > 69 years | 189 | 217 | .039 | -0.14 | 115 | 125 | .414 | -0.08 | |
| Sex | Male | 323 | 209 | .633 | 0.03 | 129 | 125 | .785 | 0.03 |
| Female | 284 | 197 | .633 | -0.03 | 114 | 118 | .785 | -0.03 | |
| ASA class | I-II | 407 | 255 | .186 | 0.09 | 165 | 156 | .444 | 0.08 |
| III | 200 | 151 | .186 | -0.09 | 78 | 87 | .444 | -0.08 | |
| Body Mass Index | ≤24.67 Kg/m2 | 295 | 212 | .287 | -0.07 | 124 | 121 | .856 | 0.02 |
| > 24.67 Kg/m2 | 312 | 194 | .287 | 0.07 | 119 | 122 | .856 | -0.02 | |
| Diabetes | Yes | 81 | 42 | .182 | 0.09 | 21 | 30 | .236 | -0.12 |
| No | 526 | 364 | .182 | -0.09 | 222 | 213 | .236 | 0.12 | |
| Chronic renal failure | Yes | 27 | 18 | 1.00 | 0.00 | 10 | 12 | .827 | -0.04 |
| No | 580 | 388 | 1.00 | -0.00 | 233 | 231 | .827 | 0.04 | |
| MNA-SF | ≤ 13 | 433 | 260 | .017 | 0.16 | 165 | 162 | .847 | 0.03 |
| > 13 | 174 | 146 | .017 | -0.16 | 78 | 81 | .847 | -0.03 | |
| Malignancy | Yes | 427 | 312 | .027 | -0.15 | 167 | 176 | .426 | -0.08 |
| No | 180 | 94 | .027 | 0.15 | 76 | 67 | .426 | 0.08 | |
| Mini-invasive surgery | Yes | 545 | 355 | .288 | 0.07 | 221 | 215 | .455 | 0.08 |
| No | 62 | 51 | .288 | -0.07 | 22 | 28 | .455 | -0.08 | |
| Standard procedures | Yes | 488 | 371 | .000 | -0.32 | 208 | 213 | .594 | -0.06 |
| No | 119 | 35 | .000 | 0.32 | 35 | 30 | .594 | 0.06 | |
| Anastomosis 1 | Intracorporeal | 432 | 300 | .381 | -0.06 | 177 | 172 | .687 | 0.05 |
| Extracorporeal | 175 | 106 | .381 | 0.06 | 66 | 71 | .687 | -0.05 | |
| Anastomosis 2 | Stapled | 514 | 354 | .304 | -0.07 | 212 | 205 | .436 | 0.08 |
| Handsewn | 93 | 52 | .304 | 0.07 | 31 | 38 | .436 | -0.08 | |
| Anastomosis 3 | End-to-end | 293 | 164 | .016 | 0.16 | 116 | 97 | .010 | 0.16 |
| Other shape | 314 | 242 | .016 | -0.16 | 127 | 146 | .010 | -0.16 | |
| Operation length | ≤160′ | 291 | 201 | .671 | -0.03 | 131 | 133 | .927 | -0.02 |
| ˃160′ | 316 | 205 | .671 | 0.03 | 112 | 110 | .927 | 0.02 | |
| Hospital type | Met/Ac | 516 | 257 | .000 | 0.51 | 178 | 175 | .839 | 0.03 |
| Local/Regional | 91 | 149 | .000 | -0.51 | 65 | 68 | .839 | -0.03 | |
| Unit type | Col/Onc | 144 | 22 | .000 | 0.54 | 24 | 22 | .877 | 0.03 |
| General | 463 | 384 | .000 | -0.54 | 219 | 221 | .877 | -0.03 | |
| Center volume | Low | 221 | 136 | .377 | 0.06 | 65 | 63 | .918 | 0.02 |
| High | 386 | 270 | .377 | -0.06 | 178 | 180 | .918 | -0.02 | |
| Preoperative BT(s) | Yes | 26 | 17 | 1.00 | 0.00 | 8 | 13 | .372 | -0.10 |
| No | 581 | 389 | 1.00 | -0.00 | 235 | 230 | .372 | 0.10 | |
| Intra/Post-operative BT(s) | Yes | 43 | 15 | .033 | 0.15 | 15 | 14 | 1.00 | 0.02 |
| No | 564 | 391 | .033 | -0.15 | 228 | 229 | 1.00 | -0.02 | |
| ERAS adherence | ≤78.95% | 450 | 166 | .000 | 0.71 | 140 | 147 | .580 | -0.06 |
| ˃ 78.95% | 157 | 240 | .000 | -0.71 | 103 | 96 | .580 | 0.06 | |
MoABP: Mechanical bowel preparation plus oral Antibiotics; oA: oral antibiotics; *Student’s test for proportions; **Standardized Mean Difference; ASA: American Society of Anesthesiologists; MNA-SF: Mini Nutritional Assessment—Short Form; ; Intracorporeal: anastomosis performed under visual control through the scope; Extracorporeal: anastomosis performed under direct visual control through an open access; Met/Ac: Metropolitan/Academic; Col/Onc: Colorectal/Oncologic; BT(s): blood transfusion(s); ERAS: enhanced recovery after surgery.
After the multivariate logistic regression analysis for the endpoints in the 486 patients evaluated after score matching, oA versus MoABP was significantly associated with a higher risk of AL [14 (5.8%) vs. 6 (2.5%) events; OR 3.77; 95%CI 1.22-11.67; p = .021]. The sensitivity analysis calculated a Γ = 1 (p upper bound = .057). No difference was recorded between the two groups for SSIs [9 (3.7%) vs. 7 (2.9%) events; OR 1.02; 95%CI 0.31-3.29; p = .977]. The oA group was also significantly associated with a higher risk of major morbidity [25 (10.3%) vs. 9 (3.7%) events; OR 4.55; 95%CI 1.82-11.38; p = .001; Γ = 1.4; p upper bound = .038], and a higher risk of reoperation [16 (6.6%) vs. 5 (2.1%) events; OR 5.05; 95%CI 1.55-16.49; p = .007; Γ = 1.3; p upper bound = .037]. No significant differences were recorded between the two groups in terms of overall morbidity (Table 4).
According to the types of adverse events reported in the two groups (Table 5), the higher risk of major morbidity recorded in the oA group vs. MoABP group resulted significantly related to AL and superficial and/or deep surgical site infections (sdiSSIs).
4. Discussion
The effectiveness of oA and MoABP in reducing AL and SSIs rates for elective colorectal resections remains largely controversial [2]. On one hand, a well-designed RCT showed that oA alone is able to significantly reduce SSIs rates compared to NBP, albeit with no influence on AL rates [32], while another large French RCT [33] showed the same finding, with the highest reduction achieved with MoABP, although the PIVAP schedule in this trial did not include metronidazole. On the other hand, two largely underpowered RCTs [54,55] showed inconclusive results. Analysis of the large retrospective databases of the ACS-NSQIP [17,18,20,21] and Veterans Affairs NSQIP [56] suggests that both oA and MoABP may be equally effective in reducing AL and SSIs rates compared to MBP alone or NBP. Therefore, while waiting for the results of the ongoing international RCT comparing oA to MoABP [34], it could be of particular interest to know how these different types of preoperative preparations work in real-life clinical practice.
To the best of our knowledge, the present study is the first PSMA comparing oA with PIVAP versus MoABP with PIVAP performed using data derived from a prospective multicenter database, representing a shapshot of real-life clinical practice in 1,013 Italian patients before elective colorectal surgery. There were no significant differences between groups in terms of SSIs rates and a significantly higher risk of AL, MM, and reoperation in the group treated by oA (Table 4). The sensitivity analysis [53] showed Γ = 1 for AL, Γ = 1.4 for MM, and Γ = 1.3 for reoperation, meaning that 10%, 40%, and 30% of patients in this study should have been treated by MoABP instead of oA to alter the significant association between oA and the higher risk of AL, MM, and reoperation, respectively. The significantly higher MM risk in the oA group was significantly related to AL and sdiSSIs, among several other adverse events (Table 5), and the significantly lower risk of reoperation in the MoABP group may be related to the causal link between AL and reoperation.
In summary the results of this PSMA suggest that oA alone expose the patients to a higher risk of AL and grade > II sdiSSIs. The reasons are mainly speculative and refer to the conviction [57] that luminal feces may lead to a reduced efficiency of topically acting antibiotics. In 2016 Fry suggested that retained stool yields a large bulk of microbes, dietary fiber, and exfoliated cells that will not permit a reduction in the density of potential pathogens on the colonic mucosal surface with oral antibiotics [58], supporting previous studies [3,5,59] performed in the 1940s and the 1970s. In patients treated with oA alone, it is possible that some members of the Bacteroidetes phylum [60] and other microbes such as Enterococcus faecalis and Pseudomonas aeruginosa [57,61] can remain in feces and colon mucosa, expressing enzymes that promote the degradation of synthesized tissue, leading to vulnerability of the newly created anastomosis in response to surgical trauma and resulting ischemia. The hypothesis that MBP could reduce the abundance of protective Bifidobacterium and Lactobacillus species with higher rates of postoperative infections [62] appears is less convincing mainly because changes in microbiota are only one of the factors influencing the rates of AL and postoperative complications after elective colorectal surgery [57,63].
Although the need for aerobic and anaerobic coverage is universally accepted, many different oral and intravenous antibiotic combinations have been previously reported [2], with prevalent geographic preferences. In the present study many different antibiotics and administration schedules were used (Table 2), and because of the small number of AL events in each oral antibiotic and administration schedule subgroup, it was not possible to conclude which antibiotic and administration schedule is better for preventing AL. Over 100 trillion microorganisms (microbiota, including fungi, viruses, protozoans, and bacteria) are present in the gastrointestinal tract of hosts [60]. Approximately 80 bacterial species are present in the colorectal tract, differing between individuals according to many factors including ethnicity, sex, age [60], cultural and social disparities [64], and antibiotic resistance due to extended-spectrum beta-lactamase (ESBL)-producing Enterobacterales due to previous antibiotic therapies [65]. Considering the recent shift of European guidelines towards recommending MoABP instead of NBP [23], many European surgeons (just like the authors) are currently asking themselves which oA regimen (molecules and schedules) should be implemented into their clinical practice. Based on the results of the most recent RCTs [32,35] a short-term (on the preoperative day) oral administration of a nitroimidazolic (i.e., ornidazole or metronidazole) combined with a quinolone (i.e., ciprofloxacin) is appealing due to an optimal aerobic and anaerobic coverage. However, even a short-term course of oral metronidazole and ciprofloxacin [66], shortly after determines profound changes in gut microbiota, with a drop in microbial diversity, overgrowth of the genera Streptococcus and Lactobacillus, and an early loss of anaerobic bacterial taxa with important roles in short-chain fatty acid metabolism (colonic butyrate-producing communities), that were demonstrated of paramount importance for colorectal mucosal integrity and anastomotic healing in animal studies [64,67]. Moreover, these changes require several months to return to the baseline [66], and quinolones may be involved in the worldwide raising incidence of the plague of multidrug-resistant microorganisms [68,69,70]. A possible answer may come, in a near future, from the ongoing Human Microbiome Project [71], whose worldwide mapping will allow perioperative microbiome manipulation through the targeted administration of antibiotics, probiotics or symbiotics to restore the ideal bowel flora selecting specific bowel strains rather than continuing to search for an impossible “one-size-fits-all” elimination of the intestinal microbiota.
Strengths of this study were the large number of enrolled patients in a well-defined time-lapse, representing a real-life snapshot of surgical units performing colorectal resections in Italy, and the PSMA methodology. Following recommendations for the use of propensity score methods [72,73], a rigorous patients’ selection from the parent population and a reasoned inclusion of 20 conditioning variables were performed to limit data imbalance. Moreover, both a clear and restrictive balance algorithm together with the evaluation of the treatment effect through an adjusted multiple regression model including the same 20 covariates used for matching, were used (Figure 1). Finally, a Rosenbaum’s sensitivity analysis for unmeasured confounders was applied [53].
On the other hand, this study has several limitations, and its results should be interpreted with caution: a) moderate heterogeneity of oral and intravenous antibiotic prophylaxis schedules, as reported by previous cohort studies [18,21,56]; b) the exclusion criteria applied to the parent database (Figure 1) practically excluded any resection performed for low rectal cancer, making the results not applicable to this subgroup of patients; c) several aspects of health-acquired infections preventive bundle (preoperative whole-body bathing, hair removal, and skin decontamination) and single surgeon’s experience [74] were not measured in the parent studies; d) finally, further bias from residual unknown factors and potential measurement errors by the participating investigators may have had an impact on the results.
5. Conclusions
The present study contains an important warning, reporting that oA alone compared to MoABP before elective colorectal surgery was significantly associated to a higher risk of AL, MM, and reoperation. These findings support the recent recommendations of two European societies guidelines [23] and suggest an update of European [12] and Italian [13] ERAS societies recommendations about preoperative bowel preparation for elective colorectal surgery.
Author Contributions
Marco Catarci, iCral Study Group coordinator, and Stefano Guadagni share the first co-authorship. They had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: Catarci, Guadagni, Masedu, Sartelli, Montemurro, Baiocchi, Tebala, Borghi, Marini, and Scatizzi. Acquisition, analysis, or interpretation of data: Catarci, Guadagni, Masedu, Sartelli, Montemurro, Baiocchi, Tebala, Borghi, Marini, and Scatizzi. Drafting of the manuscript: Catarci, Guadagni, and Masedu. Critical revision of the manuscript for important intellectual content: Catarci, Guadagni, Masedu, Sartelli, Montemurro, Baiocchi, Tebala, Borghi, Marini, and Scatizzi. Statistical analysis: Masedu, Guadagni, and Catarci. All the collaborators participated to data acquisition & quality control for the iCral2 and iCral3 studies.
Funding
This research received no external funding.
Institutional Review Board Statement
Both iCral2 and iCral3 studies were conducted in accordance with the Declaration of Helsinki and guidelines for good clinical practice E6 (R2). The study protocols were approved by the ethics committee of the coordinating center (Marche Regional Ethics Committee [CERM] 2018/334 released on 11/28/2018 for iCral2 and 2020/192 released on 07/30/2020 for iCral3) and registered at ClinicalTrials.gov (NCT03771456 for iCral2 and NCT04397627 for iCral3). Subsequently, all other centers were authorized to participate in their local ethics committees.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the parent studies.
Data Availability Statement
Individual participant-level anonymized datasets are available upon reasonable request by contacting the study coordinator.
Conflicts of Interest
Dr. Catarci reports personal fees from Baxter Spa outside the submitted work. Dr. Guadagni, Masedu, Sartelli, Montemurro, Baiocchi, Tebala, Borghi, Marini, and Scatizzi have no competing interests to declare.
Appendix
**Collaborators: iCral2 and iCral3 investigators are Paolo Ciano, MD, Michele Benedetti, MD, Matteo Di Carlo, MD General Surgery Unit; Sandro Pertini Hospital, ASL Roma 2; Marco Clementi, MD, General Surgery Unit, University of L’Aquila; Paolo Delrio, MD, Ugo Pace, MD, Andrea Fares Bucci, MD, Colorectal Surgical Oncology, Istituto Nazionale per lo Studio e la Cura dei Tumori, “Fondazione Giovanni Pascale IRCCS-Italia”, Napoli; Gianluca Garulli, MD, Francesco Monari, MD, General Surgery Unit, Infermi Hospital, Rimini; Felice Pirozzi, MD, Antonio Sciuto, MD, General Surgery Unit, ASL Napoli 2 Nord, Pozzuoli (NA); Lorenzo Pandolfini, MD, Alessandro Falsetto, MD, General Surgery Unit, Santa Maria Annunziata & Serristori Hospital, Firenze; Giacomo Ruffo, MD, Elisa Bertocchi, MD, Gaia Masini, MD, General Surgery Unit, IRCCS Sacro Cuore Don Calabria Hospital, Negrar di Valpolicella (VR); Massimo Giuseppe Viola, MD, Amedeo Altamura, MD, Francesco Rubichi, MD, General Surgery Unit, Cardinale G. Panico Hospital, Tricase (LE); Ferdinando Ficari, MD, Francesco Giudici, MD, Fabio Cianchi, MD, General Surgery and IBD Unit, Careggi University Hospital, Firenze; Desirée Cianflocca, MD, Marco Migliore, MD, General & Oncologic Surgery Unit, Department of Surgery, Santa Croce e Carle Hospital, Cuneo; Michele Simone, MD, Raffaele De Luca, MD, Department of Surgical Oncology, IRCCS Istituto Tumori “Giovanni Paolo II”, Bari; Alessandro Rizzo, MD, Department of Medical Oncology, IRCCS Istituto Tumori “Giovanni Paolo II”, Bari; Anna Albano, MS, Trial Office (AA), IRCCS Istituto Tumori “Giovanni Paolo II”, Bari; Alberto Patriti, MD, Marcella Lodovica Ricci, MD, Department of Surgery, Marche Nord Hospital, Pesaro e Fano (PU); Walter Siquini, MD, Alessandro Cardinali, MD, General Surgery Unit, S. Lucia Hospital, Macerata; Stefano D’Ugo, MD, PhD, FEBS, FACS, Marcello Spampinato, MD, PhD, FEBS (HPB), General Surgery Unit, “V. Fazzi” Hospital, Lecce; Stefano Scabini, MD, Alessandra Aprile, MD, Domenico Soriero, MD, General & Oncologic Surgery Unit, IRCCS “San Martino” National Cancer Center, Genova; Marco Caricato, MD, FACS, Gabriella Teresa Capolupo, MD, FACS, Colorectal Surgery Unit, Policlinico Campus BioMedico, Roma; Giusto Pignata, MD, Jacopo Andreuccetti, MD, Ilaria Canfora, MD, 2nd General Surgery Unit 2, Spedali Civili di Brescia; Andrea Liverani, MD, Andrea Scarinci, MD, General Surgery Unit, Regina Apostolorum Hospital, Albano Laziale (RM); Roberto Campagnacci, MD, Angela Maurizi, MD, General Surgery Unit, “C. Urbani” Hospital, Jesi (AN); Pierluigi Marini, MD, Grazia Maria Attinà, MD, General & Emergency Surgery Unit, San Camillo-Forlanini Hospital, Roma; Ugo Elmore, MD, Giulia Maggi, MD, Department of Gastrointestinal Surgery Unit, San Raffaele Research Hospital and “Vita-Salute” San Raffaele University, Milano; Francesco Corcione, MD, Umberto Bracale, MD, Roberto Peltrini, MD, Maria Michela Di Nuzzo, MD, Minimally Invasive General and Oncologic and Surgery Unit, “Federico II” University, Napoli; Roberto Santoro, MD, Pietro Amodio, MD, General Oncologic Surgery Unit, Belcolle Hospital, Viterbo; Massimo Carlini, MD, FACS, Domenico Spoletini, MD, PhD, FACS, Rosa Marcellinaro, MD, Giorgio Lisi, MD, General Surgery Unit, S. Eugenio Hospital, ASL Roma 2; Antonio Giuliani, MD, Giovanni Del Vecchio, MD, General Surgery Unit, S. Carlo Hospital, Potenza; Mario Sorrentino, MD, Massimo Stefanoni, MD, General Surgery Unit, Latisana-Palmanova Hospital, Friuli Centrale University (UD); Giovanni Ferrari, MD, Carmelo Magistro, MD, General Oncologic and Mininvasive Surgery Unit, Great Metropolitan Niguarda Hospital, Milano; Gianandrea Baldazzi, MD, Diletta Cassini, MD, General Surgery Unit, ASST Ovest Milanese, Nuovo Ospedale di Legnano, Legnano (MI); Alberto Di Leo, MD, Lorenzo Crepaz, MD, General and Minimally Invasive Surgery Unit, San Camillo Hospital, Trento; Augusto Verzelli, MD, Andrea Budassi, MD, General Surgery Unit, Profili Hospital, Fabriano (AN); Giuseppe Sica, MD, Bruno Sensi, MD, Minimally Invasive Surgery Unit, Policlinico Tor Vergata University Hospital, Roma; Stefano Rausei, MD, Silvia Tenconi, MD, General Surgery Unit, Gallarate Hospital (VA); Davide Cavaliere, MD, Leonardo Solaini, MD, Giorgio Ercolani, MD, General & Oncologic Surgery Unit, AUSL Romagna, Forlì (FC); Gian Luca Baiocchi, MD, FACS, Sarah Molfino, MD, General Surgery Unit 3, Department of Clinical and Experimental Sciences, University of Brescia; Marco Milone, MD, Giovanni Domenico De Palma, MD, General & Endoscopic Surgery Unit, “Federico II” University, Napoli; Giovanni Ciaccio, MD, Paolo Locurto, MD, General Surgery Unit, S. Elia Hospital, Caltanissetta; Antonio Di Cintio, MD, General Surgery Unit, S. Maria Hospital, Terni; Luigi Boni, MD, FACS, Elisa Cassinotti, MD, General Surgery Unit, Fondazione IRCCS Ca’ Granda, Policlinico Maggiore Hospital, Milano; Stefano Mancini, MD, Andrea Sagnotta, MD, PhD, General & Oncologic Surgery Unit, San Filippo Neri Hospital, ASL Roma 1; Mario Guerrieri, MD, Monica Ortenzi, MD, Surgical Clinic, Torrette Hospital, University of Ancona; Roberto Persiani, MD, Alberto Biondi, MD, General Surgery Unit, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Roma; Andrea Lucchi, MD, FACS, Alban Cacurri, MD, General Surgery Unit, “Ceccarini” Hospital, Riccione (RN); Dario Parini, MD, Maurizio De Luca, MD, General Surgery Unit, S. Maria della Misericordia Hospital, Rovigo; Antonino Spinelli, MD, Francesco Carrano, MD, Department of Biomedical Sciences, Humanitas University, Pieve Emanuele (MI) and IRCCS Humanitas Research Hospital, Rozzano (MI); Michele Genna, MD, Francesca Fior, MD, General Surgery Unit, University Hospital, Verona; Vincenzo Bottino, MD, Antonio Ferronetti, MD, General & Oncologic Surgery Unit, Evangelico Betania Hospital, Napoli; Andrea Coratti, MD, Giuseppe Giuliani, MD, Roberto Benigni, MD, General and Emergency Surgery Unit, Misericordia Hospital, Grosseto; Dario Scala, MD, Graziella Marino, MD, Battistino Puppio, MD, Abdominal Oncologic Surgery Unit, IRCCS CROB Basilicata Referral Cancer Center, Rionero in Vulture (PZ); Andrea Muratore, MD, Patrizia Marsanic, MD, Nicoletta Sveva Pipitone Federico, MD, General Surgery Unit, “E. Agnelli” Hospital, Pinerolo (TO); Maurizio Pavanello, MD, Carlo Di Marco, MD, General Surgery Unit, AULSS2 Marca Trevigiana, Conegliano Veneto (TV); Umberto Rivolta, MD, Camillo Leonardo Bertoglio, MD, PhD, General Surgery Unit, Fornaroli Hospital, ASST Ovest Milanese, Magenta (MI); Micaela Piccoli, MD, FACS, Francesca Pecchini, MD, General Surgery Unit, Civil Hospital, Baggiovara (MO); Carlo Talarico, MD, Vincenzo Greco, MD, General Surgery Unit, Villa dei Gerani Hospital, Vibo Valentia (VV); Alessandro Carrara, MD, Michele Motter, MD, Giuseppe Tirone, MD, 1st General Surgery Unit, S. Chiara Hospital, Trento; Mauro Totis, MD, Nicolò Tamini, MD, Colorectal Surgery Unit, San Gerardo Hospital, ASST Monza; Franco Roviello, MD, Riccardo Piagnerelli, MD, General & Oncologic Surgery Unit, AOU Senese, Siena; Alessandro Anastasi, MD, Giuseppe Canonico, MD, General Surgery Unit, San Giovanni di Dio Hospital, Firenze; Gianluca Guercioni, MD, Simone Cicconi, MD, General Surgery Unit, “C. e G. Mazzoni” Hospital, Ascoli Piceno; Giuseppe Maria Ettorre, MD, Marco Colasanti, MD, General & Transplant Surgery Unit, San Camillo-Forlanini Hospital, Roma; Mauro Montuori, MD, Enrico Pinotti, MD, General & Mininvasive Surgery Unit, S. Pietro Hospital, Ponte San Pietro (BG); Pierpaolo Mariani, MD, Roberta Carminati, MD, General Surgery Unit, Pesenti Fenaroli Hospital, Alzano Lombardo (BG); Nicolò de Manzini, MD, Edoardo Osenda, MD, Surgical Clinic, University of Trieste; Annibale Donini, MD, Luigina Graziosi, MD, General & Emergency Surgery Unit, University of Perugia; Mariano Fortunato Armellino, MD, Ciro De Martino, MD, Giovanna Ioia, MD, General & Emergency Surgery Unit, S. Giovanni di Dio e Ruggi d’Aragona Hospital, Salerno; Lucio Taglietti, MD, Arianna Birindelli, MD, General Surgery Unit, ASST Valcamonica, Esine (BS); Gabriele Anania, MD, Matteo Chiozza, MD, General & Laparoscopic Surgery Unit, University Hospital, Ferrara; Mariantonietta Di Cosmo, MD, Daniele Zigiotto, MD, General & Upper GI Surgery Unit, University Hospital, Verona; Carlo Vittorio Feo, MD, Fioralba Pindozzi, MD, General Surgery Unit, Delta Hospital, Lagosanto (FE); Paolo Millo, MD, Manuela Grivon, MD, General Surgery Unit, “U. Parini” Regional Hospital, Aosta; Corrado Pedrazzani, MD, Cristian Conti, MD, General & HPB Surgery Unit, University Hospital, Verona; Silvio Guerriero, MD, Lorenzo Organetti, MD, General Surgery Unit, “A. Murri” Hospital, Fermo; Andrea Costanzi, MD, Michela Monteleone, MD, General Surgery Unit, S. Leopoldo Hospital, Merate (LC); Nereo Vettoretto, MD, Emanuele Botteri, MD, General Surgery Unit, Spedali Civili of Brescia, Montichiari (BS); Federico Marchesi, MD, Giorgio Dalmonte, MD, Surgical Clinic, University of Parma; Massimo Basti, MD, Diletta Frazzini, MD, General Surgery Unit, Spirito Santo Hospital, Pescara; Graziano Longo, MD, Simone Santoni, MD, General Surgery Unit, Policlinico Casilino, Roma; Moreno Cicetti, MD, Gabriele La Gioia, MD, General Surgery Unit, S. Maria della Misericordia Hospital, Urbino (PU); Italy.
References
- Yeo B, Harley V, Goodbody F, Pope FM, Herschell G, Wild RB, Haig A. A discussion on intestinal antiseptics. BMJ 1899;2:1250-1257.
- Willis MA, Toews I, Soltau SLV, Kal JC, Meerpohl JJ, Vilz TO. Preoperative combined mechanical and oral antibiotic bowel preparation for preventing complications in elective colorectal surgery. Cochrane Database Syst Rev 2023;2:CD014909.
- Poth EJ, Ross CA. The clinical use of phthalylsulfathiazole. J Lab Clin Med 1944; 29:785– 808.
- Lloyd-Davies OV, Morgan CN, Goligher JC. The treatment of carcinoma of the colon. In British Surgical Practice: Progress volume; Carling ER and Ross JP, Eds. London: Butterworth, UK, 1953; p. 71.
- Nichols RL, Condon RE, Gorbach SL, Nyhus LM. Efficacy of preoperative antimicrobial preparation of the bowel. Ann Surg 1972;176:227-232. [CrossRef]
- Nichols RL, Broido P, Condon RE, Gorbach SL, Nyhus LM. Effect of preoperative neomycin-erythromycin intestinal preparation on the incidence of infectious complications following colon surgery. Ann Surg 1973;178(4):453-462. [CrossRef]
- Nichols RL, Smith JW, Garcia RY, Waterman RS, Holmes JW. Current practices of preoperative bowel preparation among North American colorectal surgeons. Clin Infect Dis 1997;24:609-619. [CrossRef]
- Nelson RL, Gladman E, Barbateskovic M. Antimicrobial prophylaxis for colorectal surgery. Cochrane Database Syst Rev 2014;2014(5):CD001181. [CrossRef]
- Global guidelines for the prevention of surgical site infection, 2nd ed. Geneva: World Health Organization; 2018.
- Guenaga KF, Matos D, Castro AA, Atallah AN, Wille-Jørgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev 2005;(1):CD001544. [CrossRef]
- Guenaga KF, Matos D, Wille-Jorgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev 2011;9:CD001544.
- Gustafsson UO, Scott MJ, Hubner M, et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS©) Society Recommendations: 2018. World J Surg 2019;43:659-695. [CrossRef]
- Ficari F, Borghi F, Catarci M, et al. Enhanced recovery pathways in colorectal surgery: a consensus paper by the Associazione Chirurghi Ospedalieri Italiani (ACOI) and the PeriOperative Italian Society (POIS). G Chir 2019;40(4 Suppl.):1-40.
- Markell KW, Hunt BM, Charron PD, Kratz RJ, Nelson J, Isler JT, Steele SR, Billingham RP. Prophylaxis and management of wound infections after elective colorectal surgery: a survey of the American Society of Colon and Rectal Surgeons membership. J Gastrointest Surg 2010;14:1090-1098. [CrossRef]
- Toneva GD, Deierhoi RJ, Morris M, et al. Oral antibiotic bowel preparation reduces length of stay and readmissions after colorectal surgery. J Am Coll Surg 2013;216:756–763. [CrossRef]
- Kim EK, Sheetz KH, Bonn J, et al. A statewide colectomy experience: the role of full bowel preparation in preventing surgical site infection. Ann Surg 2014;259:310–314.
- Morris MS, Graham LA, Chu DI, Cannon JA, Hawn MT. Oral antibiotic bowel preparation significantly reduces surgical site infection rates and readmission rates in elective colorectal surgery. Ann Surg 2015;261:1034–1040. [CrossRef]
- Scarborough JE, Mantyh CR, Sun Z, Migaly J. Combined mechanical and oral antibiotic bowel preparation reduces incisional surgical site infection and anastomotic leak rates after elective colorectal resection: an analysis of colectomy-targeted ACS NSQIP. Ann Surg 2015;262:331–337.
- Garfinkle R, Abou-Khalil J, Morin N, et al. Is there a role for oral antibiotic preparation alone before colorectal surgery? ACS-NSQIP analysis by coarsened exact matching. Dis Colon Rectum 2017; 60: 729–737. [CrossRef]
- Koller SE, Bauer KW, Egleston BL, et al. Comparative effectiveness and risks of bowel preparation before elective colorectal surgery. Ann Surg 2018;267:734–742. [CrossRef]
- Midura EF, Jung AD, Hanseman DJ, et al. Combination oral and mechanical bowel preparations decreases complications in both right and left colectomy. Surgery 2018;163:528–534. [CrossRef]
- Klinger AL, Green H, Monlezun DJ, et al. The role of bowel preparation in colorectal surgery. Ann Surg 2019;269:671–677. [CrossRef]
- Holubar SD, Hedrick T, Gupta R, et al. American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on prevention of postoperative infection within an enhanced recovery pathway for elective colorectal surgery. Perioper Med (Lond) 2017;6:4. [CrossRef]
- Carmichael JC, Keller DS, Baldini G, et al. Clinical practice guidelines for enhanced recovery after colon and rectal surgery from the American Society of Colon and Rectal Surgeons and Society of American Gastrointestinal and Endoscopic Surgeons. Dis Colon Rectum 2017;60:761–784. [CrossRef]
- Migaly J, Bafford AC, Francone TD, et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the use of bowel preparation in elective colon and rectal surgery. Dis Colon Rectum 2019;62:3–8. [CrossRef]
- McChesney SL, Zelhart MD, Green RL, et al. Current U.S. Pre-operative bowel preparation trends: a 2018 survey of the American Society of Colon and Rectal Surgeons Members. Surg Infect (Larchmt) 2020; 21: 1-8. [CrossRef]
- Willis MA, Keller PS, Sommer N, et al. Adherence to fast-track measures in colorectal surgery - a survey among German and Austrian surgeons. Int J Colorectal Dis 2023;38:80. [CrossRef]
- Catarci M, Guadagni S, Masedu F, et al. Mechanical bowel preparation in elective colorectal surgery: a propensity score-matched analysis of the Italian colorectal anastomotic leakage (iCral) study group prospective cohorts. Updates Surg 2024;76(1):107-117. [CrossRef]
- Antoniou SA, Huo B, Tzanis AA, et al. EAES, SAGES, and ESCP rapid guideline: bowel preparation for minimally invasive colorectal resection. Surg Endosc 2023;37: 9001-9012. [CrossRef]
- Rollins KE, Javanmard-Emamghissi H, Acheson AG, Lobo DN. The Role of Oral Antibiotic Preparation in Elective Colorectal Surgery: A Meta-analysis. Ann Surg 2019;270: 43–58.
- Koskenvuo L, Lehtonen T, Koskensalo S, et al. Mechanical and oral antibiotic bowel preparation versus no bowel preparation for elective colectomy (MOBILE): a multicentre, randomised, parallel, single-blinded trial. Lancet 2019; 394: 840-848. [CrossRef]
- Espin Basany E, Solís-Peña A, Pellino G, et al. Preoperative oral antibiotics and surgical-site infections in colon surgery (ORALEV): a multicentre, single-blind, pragmatic, randomised controlled trial. Lancet Gastroenterol Hepatol 2020;5(8):729-738. [CrossRef]
- Preoperative oral antibiotics in colon surgery (letters to the editor). Lancet Gastroenterol Hepatol 2020;5(9):800-803.
- Pellino_G, Solís-Peña_A, KraP_M, Huguet_BM, Espín-Basany_E. Preoperative oral antibiotics with versus without mechanical bowel preparation to reduce surgical site infections following colonic resection: Protocol for an international randomized controlled trial (ORALEV2). Colorectal Dis 2021;23(8):2173–2181.
- Futier E, Jaber S, Garot M, et al.; COMBINE study group. Effect of oral antimicrobial prophylaxis on surgical site infection after elective colorectal surgery: multicentre, randomised, double blind, placebo controlled trial. BMJ 2022;379:e071476. [CrossRef]
- Assistance Publique - Hôpitaux de Paris. Mechanical Bowel Preparation and Oral Antibiotics Before Rectal Cancer Surgery (PREPACOL2). NCT03491540. ClinicalTrials.gov – NIH – US National Library of Medicine, Available at: https://clinicaltrials.gov/ct2/show/NCT03491540 (last accessed January 11, 2024).
- Assistance Publique - Hôpitaux de Paris. Mechanical Bowel Preparation and Oral Antibiotics Before Colon Cancer Surgery (COLONPREP). NCT03475680. ClinicalTrials.gov – NIH – US National Library of Medicine, Available at: https://clinicaltrials.gov/ct2/show/NCT03475680 (last accessed January 11, 2024).
- Catarci M, Ruffo G, Viola MG, et al. ERAS program adherence-institutionalization, major morbidity and anastomotic leakage after elective colorectal surgery: the iCral2 multicenter prospective study. Surg Endosc 2022;36:3965-3984. [CrossRef]
- Italian ColoRectal Anastomotic Leakage (iCral) study group. Patient-reported outcomes, return to intended oncological therapy and enhanced recovery pathways after colorectal surgery: a prospective multicenter observational investigation by the Italian ColoRectal Anastomotic Leakage (iCral 3) study group. Ann Surg Open 2023;4: e267.
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg 2014;12(12):1495-1499. [CrossRef]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240: 205-213.
- Katayama H, Kurokawa Y, Nakamura K, et al. Extended Clavien-Dindo classification of surgical complications: Japan Clinical Oncology Group postoperative complications criteria. Surg Today 2016; 46: 668-685. [CrossRef]
- Rahbari NN, Weitz J, Hohenberger W, et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: a proposal by the International Study Group of Rectal Cancer. Surgery 2010; 147: 339-351. [CrossRef]
- Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 2008; 36: 309–332. [CrossRef]
- Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol 1996; 49: 1373–1379. [CrossRef]
- Bujang MA, Sa’at N, Sidik TMITAB, Joo LC. Sample Size Guidelines for Logistic Regression from Observational Studies with Large Population: Emphasis on the Accuracy Between Statistics and Parameters Based on Real Life Clinical Data. Malays J Med Sci 2018; 25: 122-130. [CrossRef]
- Austin PC. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivariate Behav Res 2011; 46: 399-424. [CrossRef]
- Rosenbaum PR, Rubin DB. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biometrika 1983; 70: 41-55.
- Brookhart MA, Schneeweiss S, Rothman KJ, Glynn RJ, Avorn J, Stürmer T. Variable selection for propensity score models. Am J Epidemiol 2006; 163: 1149-1156. [CrossRef]
- Kaiser MJ, Bauer JM, Ramsch C, et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): a practical tool for identification of nutritional status. J Nutr Health Aging 2009; 13: 782.
- Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat 2011; 10:150-161. [CrossRef]
- Ho DE, Imai K, King G, et al. Matching as nonparametric preprocessing for reducing model dependence in parametric causal inference. Polit Anal 2007; 15: 199-236. [CrossRef]
- Rosenbaum PR. The power of a sensitivity analysis and its limit. In: Design of Observational studies, 2nd Ed. Springer Series in Statistics. Springer Nature Switzerland AG, 2020. pp. 317-336.
- Zmora O, Mahajna A, Bar-Zakai B, et al. Colon and rectal surgery without mechanical bowel preparation: a randomized prospective trial. Ann Surg 2003; 237:363–367.
- Suzuki T, Sadahiro S, Tanaka A, Okada K, Saito G, Miyakita H, Ogimi T. al. Usefulness of preoperative mechanical bowel preparation in patients with colon cancer who undergo elective surgery: a prospective randomized trial using oral antibiotics. Dig Surg 2020; 37:192-198. [CrossRef]
- Cannon JA, Altom LK, Deierhoi RJ, Moris M, Richman JS, Vick CC, Itani KMF, Hawn MT. Preoperative oral antibiotics reduce surgical site infection following elective colorectal resections. Dis Colon Rectum 2012; 55:1160–1166. [CrossRef]
- Schardey HM, Rogers S, Schopf SK, Ahnen T, Wirth U. Are gut bacteria associated with the development of anastomotic leaks ? A review of experimental and clinical studies. Coloproctology 2017; 39: 94–100. [CrossRef]
- Fry DE. Antimicrobial Bowel Preparation for Elective Colon Surgery. Surg Infect (Larchmt) 2016;17(3):269-274. [CrossRef]
- Poth EJ. Historical development of intestinal antisepsis. World J Surg 1982; 6: 153–159. [CrossRef]
- Cao Y, Shang F, Jin M, et al. Changes in Bacteroides and the microbiota in patients with obstructed colorectal cancer: retrospective cohort study. BJS Open 2023;7(6):zrad105. [CrossRef]
- Shogun BD, Smith DP, Christley S, Gilbert JA, Zaborina O, Alverdy JC. Intestinal anastomotic injury alters spatially defined microbiome composition and function. Microbiome 2014; 2: 35. [CrossRef]
- Ljungqvist O, Lobo DN. Bowel Preparation for Colorectal Surgery: Have All Questions Been Answered? JAMA Surg 2022; 157: 41-42.
- Sell NM, Francone TD. Anastomotic Troubleshooting. Clin Colon Rectal Surg 2021; 34: 385–390.
- Guyton K, Alverdy JC. The gut microbiota and gastrointestinal surgery. Nat Rev Gastroenterol Hepatol 2017; 14: 43-54. [CrossRef]
- Kirby A, Santoni N. Antibiotic resistance in Enterobacteriaceae: What impact on the efficacy of antibiotic prophylaxis in colorectal surgery? J Hosp Infect 2015; 89: 259-263.
- Haak BW, Lankelma JM, Hugenholtz F, Belzer C, de Vos WM, Wiersinga WJ. Long-term impact of oral vancomycin, ciprofloxacin and metronidazole on the gut microbiota in healthy humans. J Antimicrob Chemother 2019;74(3):782-786. [CrossRef]
- Hajjar R, Santos MM, Dagbert F, Richard CS. Current evidence on the relation between gut microbiota and intestinal anastomotic leak in colorectal surgery. Am J Surg 2019;218:1000-1007. [CrossRef]
- Correia S, Poeta P, Hébraud M, Capelo JL, Igrejas G. Mechanisms of quinolone action and resistance: where do we stand? J Med Microbiol 2017;66(5):551-559.
- Ben-Ami R, Schwaber MJ, Navon-Venezia S, Schwartz D, Giladi M, Chmelnitsky I, Leavitt A, Carmeli Y. Influx of extended-spectrum beta-lactamase-producing enterobacteriaceae into the hospital. Clin Infect Dis 2006;42(7):925-934.
- Sartelli M, Coccolini F, Labricciosa FM, Al Omari AH, Bains L, Baraket O, Catarci M, Cui Y, Ferreres AR, Gkiokas G, Gomes CA, Hodonou AM, Isik A, Litvin A, Lohsiriwat V, Kotecha V, Khokha V, Kryvoruchko IA, Machain GM, O’Connor DB, Olaoye I, Al-Omari JAK, Pasculli A, Petrone P, Rickard J, Sall I, Sawyer RG, Téllez-Almenares O, Catena F, Siquini W. Surgical Antibiotic Prophylaxis: A Proposal for a Global Evidence-Based Bundle. Antibiotics (Basel) 2024;13(1):100. [CrossRef]
- Turnbaugh PJ, Ley RE, Hamady M, Fraser-Liggett CM, Knight R, Gordon JI. The human microbiome project. Nature 2007;449(7164):804-10. [CrossRef]
- Yao XI, Wang X, Speicher PJ, et al. Reporting and Guidelines in Propensity Score Analysis: A Systematic Review of Cancer and Cancer Surgical Studies. J Natl Cancer Inst 2017; 109:djw323.
- Simoneau G, Pellegrini F, Debray TPA, Rouette J, Muñoz J, Platt RW, Petkau J, Bohn J, Shen C, de Moor C, Karim ME. Recommendations for the use of propensity score methods in multiple sclerosis research. Multiple Sclerosis Journal 2022; 28: 1467–1480. [CrossRef]
- García-Granero E, Navarro F, Cerdán Santacruz C, et al. Individual surgeon is an independent risk factor for leak after double-stapled colorectal anastomosis: An institutional analysis of 800 patients. Surgery 2017;162:1006-1016. [CrossRef]
Figure 1.
Study flowchart.
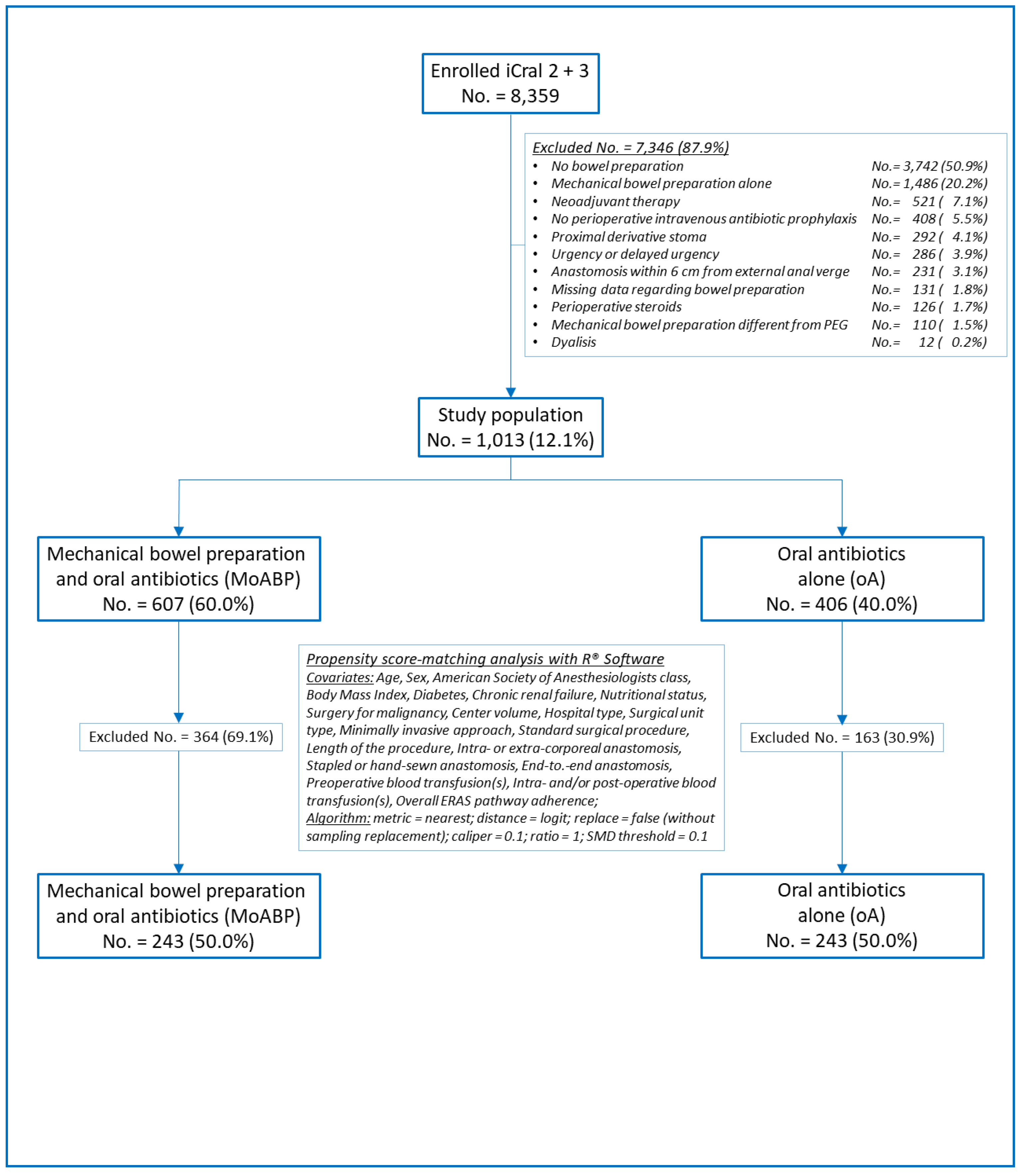
Figure 2.
Love plot of covariates’ standardized mean differences between the treatment and control groups before and after matching; the vertical lines represent the interval of ± 0.1 within which balance is considered acceptable.
Figure 2.
Love plot of covariates’ standardized mean differences between the treatment and control groups before and after matching; the vertical lines represent the interval of ± 0.1 within which balance is considered acceptable.
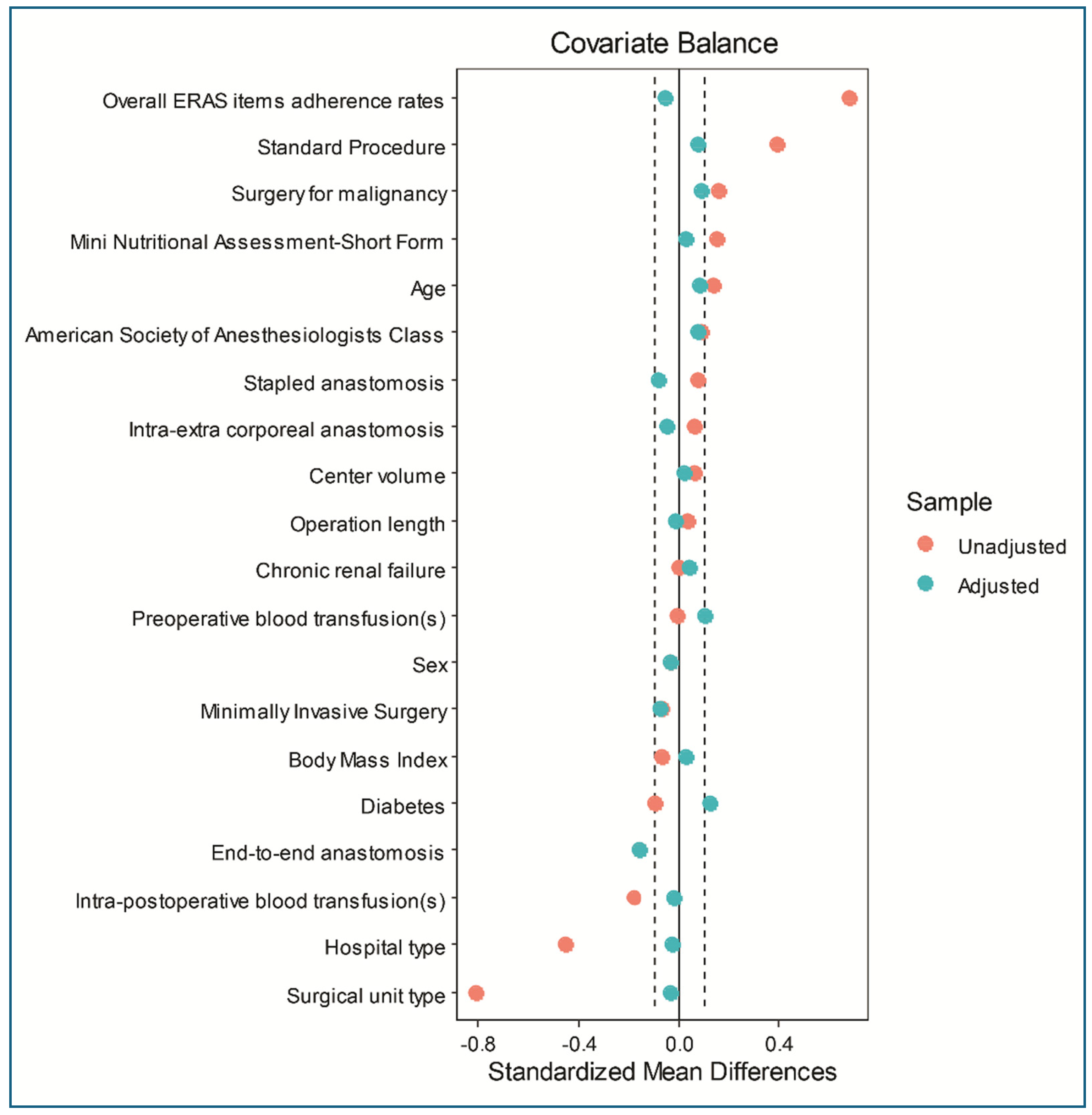
Table 1.
Descriptive analysis of the variables considered in the entire population.
| Overall | MoABP | oA | ||||||
| No. 1,013 | No. 607 | No. 406 | ||||||
| Variables | Pattern | No. | % | No. | % | No. | % | *p |
| Age (years) | ≤ 69 | 513 | 50.6 | 324 | 53.4 | 189 | 46.5 | .033 |
| > 69 | 500 | 49.4 | 283 | 46.6 | 217 | 53.5 | ||
| Sex | Male | 532 | 52.5 | 323 | 53.2 | 209 | 51.5 | .588 |
| Female | 481 | 47.5 | 284 | 46.8 | 197 | 48.5 | ||
| ASA class | I-II | 662 | 65.3 | 407 | 67.0 | 255 | 62.8 | .164 |
| III | 351 | 34.7 | 200 | 33.0 | 151 | 37.2 | ||
| Body Mass Index (Kg/m2) | ≤ 24.67 | 507 | 50.1 | 295 | 48.6 | 212 | 52.2 | .259 |
| > 24.67 | 506 | 49.9 | 312 | 51.4 | 194 | 47.8 | ||
| Diabetes | Yes | 123 | 12.1 | 81 | 13.3 | 42 | 10.3 | .152 |
| No | 890 | 87.9 | 526 | 86.7 | 364 | 89.7 | ||
| Chronic renal failure | Yes | 45 | 4.4 | 27 | 4.5 | 18 | 4.4 | .991 |
| No | 968 | 95.6 | 580 | 95.5 | 388 | 95.6 | ||
| MNA-SF | ≤ 13 | 693 | 68.4 | 433 | 71.3 | 260 | 64.0 | .014 |
| > 13 | 320 | 31.6 | 174 | 28.7 | 146 | 36.0 | ||
| Malignancy | Yes | 739 | 73.0 | 427 | 70.4 | 312 | 76.9 | .022 |
| No | 274 | 27.0 | 180 | 29.6 | 94 | 23.1 | ||
| Diverticular disease | 167 | 60.9 | 107 | 59.4 | 60 | 63.8 | 167 | |
| Endometriosis | 2 | 0.8 | 0 | 0 | 2 | 2.2 | ||
| Polyps | 35 | 12.8 | 17 | 9.5 | 18 | 19.1 | ||
| IBD | 28 | 10.2 | 22 | 12.2 | 6 | 6.4 | ||
| Other | 42 | 15.3 | 34 | 18.9 | 8 | 8.5 | ||
| Mini-invasive surgery | No | 113 | 11.1 | 62 | 10.2 | 51 | 12.6 | .245 |
| Yes | 900 | 88.9 | 545 | 89.8 | 355 | 87.4 | ||
| Laparoscopic | 826 | 81.5 | 509 | 93.4 | 317 | 89.3 | ||
| Robotic | 32 | 3.2 | 17 | 3.1 | 15 | 4.2 | ||
| Converted | 42 | 4.2 | 19 | 3.5 | 23 | 6.5 | ||
| Standard procedure | Yes | 859 | 84.8 | 488 | 80.4 | 371 | 91.4 | .000 |
| Right colectomy | 407 | 47.4 | 199 | 40.8 | 208 | 56.1 | 407 | |
| Left colectomy | 356 | 41.4 | 223 | 45.7 | 133 | 35.9 | ||
| Anterior resection | 96 | 11.2 | 66 | 13.5 | 30 | 8.1 | ||
| No | 154 | 15.2 | 119 | 19.6 | 35 | 8.6 | ||
| Transverse colectomy | 28 | 18.2 | 18 | 15.1 | 10 | 28.6 | ||
| Splenic flexure colectomy | 26 | 16.9 | 14 | 11.8 | 12 | 34.3 | ||
| Hartmann reversal | 16 | 10.4 | 12 | 10.1 | 4 | 11.4 | ||
| (Sub) total colectomy | 23 | 14.9 | 19 | 16.0 | 4 | 11.4 | ||
| Other | 61 | 39.6 | 56 | 47.0 | 5 | 14.3 | ||
| Anastomosis 1 | Intracorporeal | 732 | 72.3 | 432 | 71.2 | 300 | 73.4 | .343 |
| Extracorporeal | 281 | 27.7 | 175 | 28.8 | 106 | 26.1 | ||
| Anastomosis 2 | Stapled | 868 | 85.7 | 514 | 84.7 | 354 | 87.2 | .263 |
| Handsewn | 145 | 14.3 | 93 | 15.3 | 52 | 12.8 | ||
| Anastomosis 3 | End-to-end | 457 | 45.1 | 293 | 48.3 | 164 | 40.4 | .014 |
| Other shape | 556 | 54.9 | 314 | 51.7 | 242 | 59.6 | ||
| Operation length | ≤ 160′ | 521 | 51.4 | 316 | 52.1 | 205 | 50.5 | .625 |
| ˃ 160′ | 492 | 48.6 | 291 | 47.9 | 201 | 49.5 | ||
| Hospital type | Met./Ac. | 773 | 76.3 | 516 | 85.0 | 257 | 63.3 | .000 |
| Local/Regional | 240 | 23.7 | 91 | 15.0 | 149 | 36.7 | ||
| Unit type | Colorectal/Oncologic | 166 | 16.4 | 144 | 23.7 | 22 | 5.4 | .000 |
| General | 847 | 83.6 | 463 | 76.3 | 384 | 94.6 | ||
| Center volume | < 4 cases/month | 357 | 35.2 | 221 | 36.4 | 136 | 33.5 | .342 |
| ≥ 4 cases/month | 656 | 64.8 | 386 | 63.6 | 270 | 66.5 | ||
| Preoperative BT(s) | Yes | 43 | 4.2 | 26 | 4.3 | 17 | 4.2 | .941 |
| No | 970 | 95.8 | 581 | 95.7 | 389 | 95.8 | ||
| Intra/postoperative BT(s) | Yes | 58 | 5.7 | 43 | 7.1 | 15 | 3.7 | .023 |
| No | 955 | 94.3 | 564 | 92.9 | 391 | 96.3 | ||
| ERAS adherence (%) | ≤ 78.95 | 616 | 60.8 | 450 | 74.1 | 166 | 40.9 | .000 |
| ˃ 78.95 | 397 | 39.2 | 157 | 25.9 | 240 | 59.1 | ||
| Nutritional screening | 711 | 70.2 | 410 | 67.6 | 301 | 74.1 | ||
| Prehabilitation | 411 | 40.6 | 183 | 30.2 | 228 | 56.2 | ||
| Counseling | 747 | 73.7 | 471 | 77.6 | 276 | 68.0 | ||
| Immune enhancing nutrition | 330 | 32.6 | 113 | 18.6 | 217 | 53.5 | ||
| Antithrombotic prophylaxis | 938 | 92.6 | 550 | 90.6 | 388 | 95.6 | ||
| Preoperative carbohydrates load | 582 | 57.5 | 326 | 53.7 | 256 | 63.1 | ||
| No preanesthesia | 741 | 73.2 | 448 | 73.8 | 293 | 72.2 | ||
| Standard anesthesia protocol | 980 | 96.7 | 584 | 96.2 | 396 | 97.5 | ||
| Normothermia | 974 | 96.2 | 576 | 94.9 | 398 | 98.0 | ||
| Goal-directed or restrictive fluid therapy | 898 | 88.7 | 539 | 88.8 | 359 | 88.4 | ||
| Postoperative nausea/vomit prophylaxis | 935 | 92.3 | 543 | 89.5 | 392 | 96.6 | ||
| Multimodal analgesia | 975 | 96.3 | 573 | 94.4 | 402 | 99.0 | ||
| No nasogastric tube | 882 | 87.1 | 491 | 80.9 | 391 | 96.3 | ||
| Minimally invasive surgery | 900 | 88.9 | 545 | 89.8 | 355 | 87.4 | ||
| No drains | 420 | 41.5 | 178 | 29.3 | 242 | 59.6 | ||
| Urinary catheter < 24-48 hours | 864 | 85.3 | 484 | 79.7 | 380 | 93.6 | ||
| Early mobilization | 842 | 83.1 | 469 | 77.3 | 373 | 91.9 | ||
| Early oral feeding | 726 | 71.7 | 374 | 61.6 | 352 | 86.7 | ||
| Pre-discharge check | 848 | 83.7 | 503 | 82.9 | 345 | 85.0 | ||
MoABP: Mechanical bowel preparation plus oral Antibiotics; oA: oral Antibiotics; *Chi-square independence test with one degree of freedom; ASA: American Society of Anesthesiologists; MNA-SF: Mini Nutritional Assessment—Short Form; IBD: Inflammatory bowel disease; Intracorporeal: anastomosis performed under visual control through the scope; Extracorporeal: anastomosis performed under direct visual control through an open access; Met./Ac.: Metropolitan/Academic; BT: blood transfusion(s); ERAS: Enhanced recovery after surgery pathway.
Table 2.
Oral antibiotic schedules in the oA and MoA groups before propensity score matching.
| Oral Antibiotic(s) | Administration schedule | oA (No. 406) | MoABP (No. 607) | *p | ||
| No. | % | No. | % | |||
| Metronidazole (500 mg) Paromomycin (250 mg) |
Started 2 days preop., TID Started 2 days preop., BID |
118 | 29.1 | 29 | 4.8 | .006 |
| Metronidazole (500 mg) Cefazolin (2000 mg) |
Started 1 day preop., TID Started 1 day preop., OD |
76 | 18.7 | 50 | 8.2 | .102 |
| Metronidazole (500 mg) Trimethoprim (160 mg) + Sulfamethoxazole (800 mg) |
Started 1 day preop., TID Started 1 day preop., TID |
68 | 16.7 | 61 | 10.0 | .267 |
| Metronidazole (500 mg) Neomicin + Bacitracin (300 mg) |
Started 1 day preop., TID Started 1 day preop., TID |
47 | 11.6 | 6 | 0.9 | .419 |
| Metronidazole (500 mg) Amoxicilline (1000 mg) |
Started 3 days preop., BID Started 3 days preop., BID |
25 | 6.2 | 5 | 0.8 | .623 |
| Metronidazole (250 mg) Ciprofloxacin (500 mg) |
Started 1 day preop., TID Started 1 day preop., BID |
20 | 4.9 | 21 | 3.5 | .823 |
| Metronidazole (500 mg) Rifaximin (400 mg) |
Started 7 days preop., TID Started 7 days preop., BID |
5 | 1.2 | 9 | 1.5 | .963 |
| Metronidazole (250 mg) Amoxicilline (1000 mg) |
Started 1 day preop., BID Started 1 day preop., BID |
0 | 0 | 50 | 8.2 | n.e. |
| Paramomycin (250 mg) | Started 4 days preop., QID | 44 | 10.8 | 0 | 0 | n.e. |
| Paromomycin (1000 mg) | Started 1 day preop., OD | 0 | 0 | 37 | 6.1 | n.e. |
| Metronidazole (250 mg) Rifaximin (200 mg) |
Started 1 day preop., TID Started 1 day preop., BID |
3 | 0.8 | 0 | 0 | n.e. |
| Metronidazole (500 mg) Rifaximin (200 mg) |
Started 1 day preop., BID Started 1 day preop., BID |
0 | 0 | 68 | 11.2 | n.e. |
| Metronidazole (1000 mg) Rifaximin (400 mg) |
Started 1 day preop., TID Started 1 day preop., TID |
0 | 0 | 11 | 1.8 | n.e. |
| Metronidazole (500 mg) Paromomycin (500 mg) Rifaximin (400 mg) |
Started 1 day preop., BID Started 1 day preop., BID Started 1 day preop., BID |
0 | 0 | 126 | 20.8 | n.e. |
| Rifaximin (400 mg) | Started 1 day preop., TID | 0 | 0 | 102 | 16.8 | n.e. |
| Amoxicilline (1000 mg) | Started 3 days preop., TID | 0 | 0 | 17 | 2.8 | n.e. |
| Neomicin + Bacitracin (300 mg) | Started 1 day preop., TID | 0 | 0 | 15 | 2.5 | n.e. |
oA: oral Antibiotics; MoABP: Mechanical bowel preparation plus oral Antibiotics; * t test for proportions comparison; OD: Once daily; BID: 2 times per day; TID: 3 times per day; (QID): 4 times per day; preop.: preoperatively; n.e. : test not executable because there are cells with insufficient values.
Table 4.
Multivariate logistic regression analysis of the endpoints considered in the 486 patients evaluated using PSMA.
Table 4.
Multivariate logistic regression analysis of the endpoints considered in the 486 patients evaluated using PSMA.
| Propensity score-matched analysis | ||||||||
| MoABP No. 243 | oA No. 243 | *Sensitivity | ||||||
| Endpoint | No. | % | No. | % | OR (95%CI) | p | Γ | **p |
| Anastomotic leakage | 6 | 2.5 | 14 | 5.8 | 3.77 (1.22-11.67) | .021 | 1.0 | .057 |
| SSIs | 7 | 2.9 | 9 | 3.7 | 1.02 (0.31 - 3.29) | .977 | ||
| Overall morbidity | 49 | 20.2 | 64 | 26.3 | 1.52 (0.96 - 3.40) | .075 | ||
| Major Morbidity | 9 | 3.7 | 25 | 10.3 | 4.55 (1.82-11.38) | .001 | 1.4 | .038 |
| Reoperation | 5 | 2.1 | 16 | 6.6 | 5.05 (1.55-16.49) | .007 | 1.3 | .037 |
MoABP: Mechanical bowel preparation plus oral Antibiotics; oA: oral Antibiotics; *Rosenbaum’s sensitivity analysis; **p upper bound; OR (95%CI): odds ratio estimation with 95% confidence intervals; SSIs: surgical site infections.
Table 5.
Adverse events contributing to overall morbidity and major morbidity in the 486 patients evaluated using PSMA.
Table 5.
Adverse events contributing to overall morbidity and major morbidity in the 486 patients evaluated using PSMA.
| MoABP No. 243 | oA No. 243 | |||||
| Adverse events | OM (%) | MM (%) | OM (%) | MM (%) | *p (OM) | *p (MM) |
| Anastomotic leakage | 6 (2.5) | 4 (1.6) | 14 (5.8) | 12 (4.9) | .068 | .042 |
| sdiSSIs | 2 (0.8) | 0 (0) | 6 (2.5) | 4 (1.6) | .154 | .045 |
| Deepwound dehiscence | 1 (0.4) | 1 (0.4) | 2 (0.8) | 2 (0.8) | .562 | .562 |
| Abdominal collection/abscess | 4 (1.7) | 1 (0.4) | 3 (1.2) | 3 (1.2) | .703 | .315 |
| Small bowel obstruction | 7 (2.9) | 5 (2.1) | 4 (1.6) | 3 (1.2) | .360 | .476 |
| Anastomotic bleeding | 2 (0.8) | 1 (0.4) | 8 (3.3) | 1 (0.4) | .055 | 1.00 |
| Abdominal bleeding | 2 (0.8) | 1 (0.4) | 1 (0.4) | 1 (0.4) | .562 | 1.00 |
| Small bowel perforation | 0 (0) | 0 (0) | 0 (0) | 0 (0) | n.e. | n.e. |
| Trocar/wound site bleeding | 1 (0.4) | 0 (0) | 1 (0.4) | 0 (0) | 1.00 | n.e. |
| Anemia | 6 (2.5) | 0 (0) | 9 (3.7) | 1 (0.4) | .431 | .317 |
| Paralytic ileus | 9 (3.7) | 0 (0) | 8 (3.3) | 0 (0) | .805 | n.e. |
| Fever | 6 (2.5) | 0 (0) | 8 (3.3) | 0 (0) | .588 | n.e. |
| DVT/PE | 0 (0) | 0 (0) | 1 (0.4) | 0 (0) | .317 | n.e. |
| Neurologic | 1 (0.4) | 1 (0.4) | 1 (0.4) | 0 (0) | 1.00 | .317 |
| Pneumonia and pulmonary failure | 5 (2.1) | 0 (0) | 7 (2.9) | 2 (0.8) | .559 | .156 |
| Urinary retention | 1 (0.4) | 0 (0) | 2 (0.8) | 0 (0) | .562 | n.e. |
| Urinary tract infection | 0 (0) | 0 (0) | 1 (0.4) | 0 (0) | .317 | n.e. |
| Acute renal failure | 0 (0) | 0 (0) | 4 (1.6) | 0 (0) | .062 | n.e. |
| Acute mesenteric ischemia | 0 (0) | 0 (0) | 0 (0) | 0 (0) | n.e. | n.e. |
| Acute peptic ulcer/erosive gastritis | 0 (0) | 0 (0) | 0 (0) | 0 (0) | n.e. | n.e. |
| Cardiac dysfunction and failure | 2 (0.8) | 1 (0.4) | 2 (0.8) | 2 (0.8) | 1.00 | .562 |
| Other | 14 (5.8) | 1 (0.4) | 7 (2.9) | 2 (0.8) | .118 | .562 |
MoABP: Mechanical bowel preparation plus oral antibiotics; oA: oral antibiotics; OM: overall morbidity (number of events); MM: major morbidity (number of events); *Chi square independence test with one degree of freedom; sdiSSIs: superficial and/or deep incisional surgical site infections; DVT: deep venous thrombosis; PE: pulmonary embolism; n.e.: test not executable because there are cells with insufficient values.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



