Submitted:
18 July 2025
Posted:
21 July 2025
You are already at the latest version
Abstract
Biomarkers are now considered valuable adjunctive tests for the diagnosis, prognosis and management of heart failure (HF). Natriuretic peptides have considerably improved the assessment and management of HF patients, but they have several limitations. Given the complex HF pathophysiology, no single biomarker can adequately address the diagnosis, prognosis and outcomes. Therefore, the use of multiple biomarkers can improve HF management, applying a multifaceted pathophysiological approach. An exponential number of emerging biomarkers is reported in the literature, many of which have been shown to be independent HF risk factors, and, more significantly, when combined. They are also increasingly being used as targets in the development of innovative treatments, such as targeted and personalized therapies, also thanks to the application of artificial in-telligence models and use of multi-omics approaches. In this review, we have provided extensive evidence that highlights the need to revolutionize both HF management and therapies. A detailed overview of emerging biomarkers, potential targets and therapies is here reported, illustrating their advantages and limitations, as well as possible solutions to overcome them, and highlighting their strong promising potential. This could allow us to predict this disease in the general population, to perform an early diagnosis, limiting complications and mortality. The road to its realization is arduous, but feasible, and it will require further efforts by researchers and clinicians with different multidisciplinary skills.
Keywords:
heart failure
; biomarkers
; multi-biomarker panels
; artificial intelligence
; multi-omics
; targeted therapies
; benefits
; limitations
; solutions
The management of a complex disease such as heart failure requires the use of not only traditional blood biomarkers, but also panels of biochemical biomarkers, which reflect its complex pathophysiology. The aim of the review is therefore to provide the most up-to-date data from the available literature on emerging biomarkers, as well as on innovative treatments, such as targeted therapies, also developed thanks to the application of artificial intelligence and multi-omics technologies, with the aim of facilitating diagnosis, predicting prognosis and outcomes and suggesting more innovative and personalized therapies.
1. Introduction
Heart failure (HF) is a cardiac syndrome, characterized by the presence of unspecific signs and symptoms, such as asthenia and dyspnoea; signs, for instance oedema of the left ventricle, which overlap with other pathological conditions, such as chronic renal insufficiency and liver failure. However, in HF the symptoms reflect the deterioration of left ventricular function, well recognized to be associated with a high rate of morbidity and mortality, having a significant economic impact on health’s services [1]. HF is, indeed, considered now a major issue of public health. HF occurs when the heart cannot pump appropriate oxygen augment and blood to the other tissue and organs. Accordingly, ejection fraction (EF) is used to classify HF in general via. Three subtypes are hence identified: a) HF with reduced ejection fraction (HFrEF): EF≤40%; b) HF with mildly reduced ejection fraction (HFmrEF): EF between 41% and 49%; and c) HF with preserved ejection fraction (HFpEF): EF ≥ 50%. In this case, other criteria will be necessary to diagnose HF, such as the presence evident clinical symptoms, alterations in filling pressures, diastolic function, or an increase in biomarkers indicative of HF [2]. From a clinical point of view, the symptoms are categorized according to the New York Heart Association classification (NYHA), which allows a distinction into IV classes based on the progressive limitation of heart function determined by the dyspnoeic symptoms. Consistent with these observations, the HF diagnosis can be executed by using diverse modalities, which also can assist in delineation of HF subtypes (phenotypes):
- Clinical history (e.g. as complication of other diseases)
- By symptoms
- Physical examination
- Heart electrical activity
- Heart ultrasound imaging and MRI (magnetic resonance imaging)
- Blood biomarkers (e.g. classical biomarkers, i.e. b-type natriuretic peptide (BNP) and troponin)
The prevalence of HF is constantly growing in the world population, because of three principal variables: i) aging population; ii) increased incidence of risk factors or comorbidities; and iii) an improvement in survival after myocardial infarction onset. Precisely, it has raised in the last 50 years from 18.9% to 22.6% in women and from 19.1% to 25.3% in men [3]. Its aetiology is extremely heterogenous and partly influenced by geographical areas. For example, arterial hypertension is the most common cause of HF in Latin America, the Caribbean, Eastern Europe and sub-Saharan Africa; ischemic heart disease in North America and Europe, while valvular heart disease is the most common aetiology in East Asia and Asia-Pacific countries [4]. Consistent with more recent data from the Report of US and Global Data from the American Heart Association, a further enhance in HF is expected. It is estimated that more than 8 million people aged ≥18 years by 2030 will develop HF [5]. However, the incidence of HF, as expected, rises significantly in patients aged ≥ 65 years. According to a study cohort of the US National Health and Nutrition Examination Survey (NHANES), such increase will vary from 5.5% to 10.4%, 4.7% to 10.8%, and 6.2% to 12.2% for all subjects, women, and men, respectively [6]. The main recognized risk factors of HF coincide with the typical risk factors as cardiovascular diseases (Figure 1): ageing, systemic arterial hypertension, smoking, obesity, diabetes. Such risk factors seem to correlate with the development of a precise HF phenotype, as recently demonstrated. For example, advanced age is more responsible of the onset of HF with preserved ejection fraction [sHR (95% CI): 2.00 (1.86–2.16), p <0.0001]. In contrast, HF with reduced ejection fraction recognizes as main etiological factors: male sex [sHR (95% CI): 2.00 (1.69–2.37), p<0.0001], diabetes mellitus [sHR (95% CI): 2.34 (1.90–2.89), p<0.0001], previous myocardial infarction [sHR (95% CI): 2.95 (2.37–3.68), p<0.0001], left ventricular hypertrophy [sHR (95% CI): 2.60 (1.92–3.52), p<0.0001] and left bundle branch block [sHR (95% CI): 3.68 (2.51–5.40), p <0.0001] [7].
However, the wide range of etiological causes and associated comorbidities related to HF onset makes the identification of pathophysiology mechanisms very complex, many of which remain poorly understood [8]. Despite this, it is recognized that the deterioration of ventricular function results in an increase in filling pressures, with a progressive reduction in cardiac output initially under stress and in subsequent phases also at rest [9]. Deterioration of ventricular function includes both systolic and diastolic function, and is characterized by cardiac fibrosis, ventricular hypertrophy and subsequent unfavourable remodeling. Such alterations may first lead to diastolic dysfunction with reduction of cardiac compliance. Diastolic dysfunction of the left ventricle, due to the development of upstream pressures, affects the left atrium, pulmonary circulation and therefore right ventricle (Figure 2). The resulting hemodynamic alterations are responsible of the onset of the various comorbidities, such as the onset of atrial fibrillation and pulmonary hypertension which further worsen the prognosis of the pathology. Subsequently, due to alterations in the ventriculus-arterial coupling, systolic function will also be affected [9], which, moreover, lead to the onset of ventricular conduction delay, such as “widened QRS complex” o “broad QRS complex” (>100 ms), identified as an independent predictor for adverse outcomes [10]. The physiopathological alterations, resulting from the reduction of cardiac output, comprise different organs and systems, by implementing compensatory mechanisms, such as activation of sympathetic nervous system, renin–angiotensin–aldosterone system (RAAS), increased peripheral vasoconstriction [11], alteration of the NO signaling pathway responsible of alterations in smooth muscle relaxation and vascular permeability, as well as with activation of the inflammatory cascade [12].
1.1. Enigmatic Definition of HF
The challenge observed in identifying the etiopathogenetic mechanisms of HF also reflects the question about enunciation of a precise and unequivocal definition of HF. Table 1 shows the different definitions proposed in the last 10 years by European, American and Japanese guidelines.
The aspect that clearly emerges from the comparison of the proposed definitions (see Table 1) is the absence of unique and objective criteria for defining HF. In fact, speaking of “functional impairment of ventricular filling or ejection of blood” refers to a too generic evaluation of cardiomyopathy associated with an extremely variable spectrum of clinical presentations, sometimes very subjective, a picture that becomes even more complex in cases of preserved EF [20]. It should also be emphasized that the echocardiographic evaluation of EF is strictly operator-dependent and in clinical practice the evaluation of the same patient by the same operator is almost impossible to achieve.
The imperative necessity for more objective diagnostic criteria is not only extremely important in the clinical management of patients, but also in the validation of effective therapeutic tools, as well as in the enhancement of research objectives. These last also need precise and defined criteria.
From this great gap in the development of a univocal definition, the great interest in electronic recording systems of clinical data occurs so that these can be processed by artificial intelligence and machine learning mechanisms [20,21].
In our opinion, the two major milestones achieved in the field of HF definition are, on the one hand, having partially included in the HF classification also the preclinical state of asymptomatic patients so as to guarantee a timely therapeutic approach with significant improvement in prognosis promoted by the most recent American guidelines [14] and, on the other hand, in the recent European guidelines [17], having started to include in the diagnostic criteria the evaluation of natriuretic peptides, currently the only objective parameter for the categorization of the pathology.
2. Biomarkers and HF: the Classical Molecules and Their Advantages and Limitations
The hemodynamic alterations that affect cardiac compliance (increased filling pressures, reduced cardiac output) and the resulting peripheral changes (increased vasoconstriction, increased vascular permeability, activation of the RAAS, dysregulation of the autonomic nervous system, activation of inflammatory processes) determine the release of a series of biomarkers which, therefore, turn out to be extremely important laboratory data both for diagnostic and prognostic evaluation, as well as for the evaluation of the response to treatment. There is a lack of improvement in outcomes and care of HF patients, that might be the inability to recognize the different pathophysiological mechanisms, occurring during decompensation, failure to recognize when optimal fluid status is achieved, and difficulty in identifying which patients have a worse prognosis and need of more aggressive interventions. Biomarkers can play an important role in addressing these deficiencies and their routine incorporation into clinical practice can improve outcomes.
Biomarkers have become valuable tools to use in combination with other clinical information for the diagnosis, prognosis, and management of multiple cardiovascular diseases, especially HF. While many biomarkers are well-established for their use in cardiovascular disease and in chronic HF management, there are some specialized and nuanced uses specific to acute HF. Furthermore, multiple novel biomarkers have recently shown promising results specifically in acute HF that can potentially improve patient management. This review will be focussed on the use of biomarkers in HF highlighting the use of established biomarkers and the potential of novel biomarkers to improve diagnosis, prognosis, and management.
2.1. Traditional Biomarkers: BNP and NT-proBNP with Their Advantages and Limitations
2.1.1. BNP and NT-proBNP
The discovery of the cardiac endocrine system, which occurred more than 30 years ago, has allowed the discovery and, therefore, the clinical use of peptides with natriuretic and vascular smooth muscle-relaxing activity functions. They are classified as atrial natriuretic peptides (ANP), brain natriuretic peptides (BNP), first isolated in porcine brain cells and only subsequently isolated in even higher doses in ventricular cardiac cells, and C-type NP (CNP), expressed mainly in chondrocytes and endothelial cells exposed to cytokines [22]. In general, natriuretic peptides play a fundamental role in maintaining the volumetric balance of the cardiovascular system, counteracting pressure and volumetric overload [23]. ANP and BNP are the peptides mostly involved in this mechanism and, furthermore, since ANP is mostly stored at the intracellular level, while BNP is mostly secreted at the extracellular level, the latter finds a greater use as a diagnostic and prognostic marker of heart failure and will therefore be the subject of our review.
The precursor of BNP, pro-BNP, is secreted by cardiomyocytes subjected to stretch following an increase in cardiac preload. Mechanical stretch, in fact, activates signal transduction that leads to the downstream transcription and translation of a 134 amino acid precursor peptide, pre-pro-BNP [24]. Pre-pro-BNP will subsequently undergo two enzymatic cleavages that will lead to the production of the biologically active C-terminal peptide, BNP1-32, and an inactive N-terminal fragment, NT-proBNP [23].
The main systemic effects of BNP are mediated by the receptor Natriuretic peptide receptor A (NPRA), a receptor associated with guanylate cyclase and widely localized in the kidney, vascular smooth muscle cells, neuronal cells and myocardium. Therefore, the receptor-ligand binding determines the activation of cGMP-dependent protein kinases (PKG), cGMP-dependent ion channels and cGMP-regulated cyclic nucleotide phosphodiesterase [25]. The main effects consist in the increase of vascular smooth muscle relaxation (through the suppression of endothelin secretion), at the central nervous system level, in the reduction of vasopressin secretion and at the peripheral nervous system level in the inhibition of the sympathetic system, in the increase of diuresis and urinary Na+ excretion and in the inhibition of the RAAS with consequent effect of reduction of cardiac preload and afterload [26,27] (Figure 3).
For this reason, the secretion of the BNP hormone may be considered an “emergency” secretion in case of volume overload [28]. BNP degradation is due to two different degradation pathways: natriuretic peptide receptor C (NPR-C) and hydrolysis by neutral endopeptidase (NEP). However, a significant resistance of BNP to NEP has been shown, unlike other natriuretic peptides, which would explain the delayed metabolism of BNP [29].
Instead, the elimination of NT-proBNP is entirely dependent on renal activity, which is reflected in the different half-lives of the two natriuretic peptides. In fact, BNP has a half-life of about 20 minutes, while NT-proBNP has about 1-2 hours, therefore its values undergo less variation than BNP but depend to a greater extent on renal function [30,31].
2.1.2. NTproBNP and HF
The use of BNP and NT-proBNP in HF has acquired increasing value over time, both from a diagnostic and prognostic point of view, because these natriuretic peptides are secreted exclusively by cardiac cells. It is, however, essential to remember that in addition to not being the only biomarkers for the diagnosis of HF, their values, although determined by precise cut-offs for practical purposes, should be considered more based on their trend over time [32].
According to the latest European guidelines, the cut-off values for BNP and NT-pro-BNP to support the diagnostic hypothesis of heart failure are 100 pg/ml for BNP and 300 pg/ml for NT-proBNP or >450 pg/ml if aged <55 years, >900 pg/ml if aged 55-75 years and >1800 pg/ml if aged >75 years [17]. In fact, current guidelines suggest a diagnostic pathway in which the dosage of BNP and NT-proBNP values follows only the clinical and ECG examination, even before the evaluation of EF (Figure 4).
Furthermore, Fang et al have highlighted a role of NT-pro-BNP as an early diagnosis biomarker in patients with diabetes in the absence of a clear clinical expression of heart failure (subclinical cardiovascular disease). In fact, in a population of 10,304 subjects not affected by evident cardiovascular disease with or without diabetes, they have demonstrated how in diabetic subjects’ high values of NT-proBNP were independently associated with all-cause mortality [33]. Similarly, the Natriuretic Peptides Studies Collaboration in a previous meta-analysis had demonstrated that in the absence of a defined cardiovascular pathology, the dosage of NT-proBNP values could predict the onset of heart failure, coronary artery disease and stroke [34].
The diagnostic value of BNP and NT-pro-BNP has not only been recognized at European level, but by broader consensus that includes American and Japanese task forces, the two markers are considered indispensable elements to reach a diagnosis of heart failure, even though the definition of the pathology itself does not include natriuretic peptides. It is, however, necessary to underline that the increase in BNP and NT-proBNP may also depend on other comorbidities such as chronic renal failure or atrial fibrillation, the latter frequently associated with heart failure [20]. Furthermore, it has been highlighted that the value of NT-proBNP should also be correlated with sex and BMI [35]. Indeed, a U-shaped relationship between BMI and NP levels has been demonstrated with higher NP levels at both extremes of BMI distribution [36], such that severe levels of obesity are associated with a significant increase in NT-proBNP determined by increased expansion of plasma volume, with greater biventricular remodeling and consequent increase in filling pressures, thus identifying a subcategory of patients with heart failure even with preserved ejection fraction with a higher risk of cardiovascular events [36,37,38].
In a population of 18,356 individuals without previous cardiovascular disease, Welsh et al demonstrated that female patients were 7 times more likely to have levels higher than the cutoff value of NT-proBNP (≥125 pg/mL) after adjusting for age [39]. This evidence would suggest an increase in the cutoff to avoid diagnostic errors, around 400 pg/mL, however this would lead to a diagnostic delay in patients with an already evident diagnostic suspicion of heart failure [39].
Finally, the increase in NT-proBNP values with advancing age can be easily explained by the progressive deterioration of ventricular function, the increased incidence of cardiovascular diseases and the reduction of renal function [35].
NT-proBNP values cannot be considered as absolute values but must be related to the time of onset of the clinical picture of heart failure; for this reason, different cut-offs are used in cases where heart failure has an acute onset or in cases of outpatient management [40].
In particular, in cases of acute onset of heart failure, ICON- RELOADED (International Collaborative of NT-proBNP: Re-evaluation of Acute Diagnostic Cut-Offs in the Emergency Department), revised in 2018, has developed age-related cut-off values in order to confirm or exclude the diagnosis of acute onset heart failure (which are clearly higher than those of chronic patients, as the heart in the acute phase is subjected to greater traction of the fibers and therefore undergoes massive synthesis of NT-proBNP):
In patients aged <50 years for values ≥ 450pg/mL, aged between 50 and 75 years for values ≥ 900pg/mL, aged > 75 years for values ≥ 1800pg/mL there is a significant diagnostic suspicion of heart failure, which however requires clinical investigations and instrumental diagnosis.
Values ≥ 5,000pg/mL are instead indicative of a high diagnostic suspicion of heart failure as well as correlating with a worse prognosis [40,41].
In the absence of acute exacerbation, the cut-off value to raise a diagnostic suspicion of HF is a dosage of NT-proBNP ≥125 pg/mL, as also established by the European guidelines without however making any distinction based on age. However, the practical algorithms for early diagnosis of HF propose to define a high risk of HF for values ≥ 125 pg/mL in patients aged under 50 years, values ≥ 250 pg/mL in patients aged between 50 and 74 years and values ≥ 500 pg/mL in patients aged ≥ 75 years. Values ≥ 2,000 pg/mL are indicative of a high risk of heart failure such as to require further diagnostic investigations (echocardiogram, MRI) within two weeks [40].
From the identification of these cut-off values, it emerges that there is a significant “grey area” in which the diagnosis is rather indeterminate (for example in patients aged over 50 years and with values between 450 and 900 pg/mL) and which requires further diagnostic tests, in addition to the adjustments for sex, BMI, renal function discussed above.
Ianos et al, similarly, highlighted how high NT-proBNP values (above 2379 pg/mL) were significantly associated with increased odds of advanced HF after adjusting for demographic and clinical covariates and how measurement of NT-proBNP levels had the highest sensitivity and specificity values ( area under the receiver operating curve (AUC) 0.73, 95% C.I. 0.63-0.82), demonstrating not only the diagnostic but also the prognostic role of NT-pro-BNP [42]. Nguyen et al, similarly, in their prospective study correlated NT-pro-BNP values with the rate of 90-day post-discharge events in patients having heart failure with reduced ejection fraction, demonstrating that NT-proBNP had the highest predictive value both by univariate Cox proportional hazard analysis [HR (95%CI)= 2.49 (1.41–4.40), p value 0.002] and by multivariate analysis [HR (95%CI)=2.36 (1.31–4.24) p value 0.004] [43]. Finally, Ammar et al in their systematic review and meta-analysis of the reading also addressed the correlation between NT-proBNP values and the risk of adverse events in patients with heart failure with preserved ejection fraction. In particular, the authors, integrating the results of 22 articles published between 2008 and 2024 that included a population of 10,158 patients with HFpEF aged between 44 and 82 years, demonstrated a close correlation between high NT-proBN values and the risk of mortality [HR of 1.65 (95% CI: 1.55-1.76)] [44].
This further supports the solidity of using NT-proBNP not only for diagnostic purposes in heart failure but also in establishing its prognosis. Table 3 summarizes the main advantages and limitations on clinical use of NT-proBNP.
2.1.3. MR-pro-ANP: Another Biomarker Prevalently Associated with the HF Diagnosis
Like B-type peptides, a rapid boost of blood levels of atrial natriuretic peptide (ANP) also occurs after the cardiac stretch, but, because of its half-life of only 2–5 minutes linked to action of neprilysin, it is problematic to quantify [45]. In alternative, its immediate precursor protein, the pro-ANP, more stable and with a longer half-life, can be quantified in serum samples. Accordingly, a mid-regional pro-peptide assay for ANP (MR-pro-ANP) has permitted such quantification and its application in HF [46]. MR-pro-ANP has been used for the first time as diagnostic biomarker in the BACH (Biomarkers in the Acute Heart Failure) trial [46]. However, its comparison with BNP or NT-pro-BNP has demonstrated in such study, as well as in PRIDE study [47], that is not significantly performing: with a MR-pro-ANP cutoff point of ≥120 pmol/L and a sensitivity of 97%, specificity of 60% with accuracy of 74% respect to the BNP cutoff point of 100 pg/mL and a sensitivity of 96%, specificity of 62%, and accuracy of 73%. In case of chronic HF, the GISSI-HF study [48] has evaluated the capability of MR-pro-ANP to predict stable chronic HF. The results obtained have evidenced that values of MR-pro-ANP ≥278 pmol/L had a prognostic precision for 4-year mortality respect to other novel and established biomarkers included in the study (AUC=0.74; 95% CI, 0.70–0.76). Better findings have been achieved by adding BNP or NT-pro-BNP. This analysis has shown to improve diagnostic performance of MR-pro-ANP for chronic HF with an improved AUC and net reclassification index (NRI), which represent the statistical method for assessing a biomarker’s ability to appropriately classify a patient’s risk [49]. Nevertheless, the performance of MR-pro-ANP has been reported to be still diminished in patients with BNP and NT-pro-BNP values within the ‘gray-zone,’ [50]. In addition, another limitation is represented by the MR-pro-ANP assay, which shows the same interferences as the assays for BNP and NT-pro-BNP. Therefore, so far, limited data have been provided on the diagnostic potential of MR-pro-ANP, and the use of MR-pro-ANP is still largely referred to research. Our suggestion is that blood levels of MR-pro-ANP largely reproduce pathophysiological processes like those of BNP and NT-pro-BNP. Therefore, it is not surprising that MR-pro-ANP is inappropriate to significantly facilitate the diagnosis of HF [51]. A perfect biomarker that can integrate such molecules would reflect other pathophysiological processes occurring in HF [50].
2.1.4. Troponins as Myocardial Damage Biomarker
Cardiac troponins (cTn) [52] are regulatory proteins of cardiomyocytes, which contribute to the calcium-mediated interaction between the actin and myosin. They constitute a protein complex, consisting of three subunits: troponin T, troponin I and troponin C. Cardiac troponins represent the typical biomarkers of the management of acute coronary syndrome. However, they are also recognized as useful prognostic biomarkers of HF. Accordingly, increased blood levels of cTn in HF are ascribed to myocardial stress and cardiomyocyte death related to the persistent subendocardial ischemia [53]. Furthermore, cardiac troponins, as biomarkers of essential myocyte dysfunction, could also predict new HF, since low-level chronic myocyte damage may appear in individuals before the clinical onset of HF. Elevated circulating cTn levels have been reported to be associated with advanced HF, poor prognosis and mortality risk. In addition of such role, elevated cTn levels are also related to the development of HF in subjects with previous acute myocardial infarction, where higher levels are associated with a higher risk of HF [53]. In patients with acute HF, those with elevated baseline cTn levels have more frequent adverse events in hospital admissions, increased intensive care unit admissions and in-hospital mortality. Elevated cTn levels in patients with chronic HFrEF are also linked to increased long-term mortality and a higher risk of HF rehospitalization [54,55]. However, the increase in plasma cTn values varies by gender and race, being greater in males and blacks. In addition, the prevalence of cardiovascular disease, advanced age, hypertension, left ventricular hypertrophy, and chronic kidney disease may lead to an increase in cTn values or other clinical conditions not related to myocardial damage such as sepsis, acute respiratory distress syndrome, and stroke [56].
3. Emerging Biomarkers: from Diagnostic to Prognostic and Therapeutic Purpose
Recent evidence underlines that pathways related to systemic inflammation and oxidative stress show a crucial role in HF physiopathology than the activation of sympathetic nervous system and RAAS [57,58,59,60,61]. This has led to the study of the different pathophysiological pathways and the consequent identification of several potentially useful biomarkers. They might support clinical decision-making in HF screening and diagnosis, prognostic stratification and therapeutic guidance. On the other hand, B-type neurotransmitters (i.e. BNP and NT-proBNP, as largely described above) represent the gold standard in HF management, but in recent years other molecules have demonstrated a value independent than BNP and NT-proBNP, particularly in the prognostic assessment of HF, and some of them are starting to be used in clinical practice in specialized centers [52,59,60,62,63,64]. However, we cotemporally underline that the number of biomarkers evaluated in HF has grown exponentially, but only a few of them have been demonstrated with sufficient evidence to justify their use in clinical practice [52,58,59,60,62,63]. Furthermore, most studies have tested new biomarkers exclusively in the prognostic stratification of patients with HF, while in the literature there are few data on their use as screening, diagnosis and treatment guidance tools. This last aspect appears particularly relevant given the lack of reliable analytical indices that can be used as a reference for the titration of HF therapy. This might lead to the combination of multiple biomarkers belonging to the different pathophysiological pathways and facilitate both optimization and personalization of the clinical HF management. The integration of different omics technologies in such investigations, although still far from a possible routine clinical application, could contribute in the future to defining in a much more precise way the clinical phenotype of the individual HF patient. Below, we report a large list of emerging biomarkers, dividing them according to their molecular characteristics and functions [52,58,59,60,62,63].
3.1. Biomarkers of Neuro-Hormonal Activation
HF is a heterogeneous syndrome driven by multiple interconnected pathophysiological mechanisms, as mentioned above. Neurohormonal dysregulation, involving the activation of the RAAS and SNS, leads to fluid retention, vasoconstriction, and maladaptive cardiac remodeling. Here, we describe and discuss potential molecules related to these systems that might be used as biomarkers in HF.
Among these, plasma norepinephrine has been demonstrated for the first time a good predictor of prognosis in HF by the Cohn group [65]. This has been confirmed in some pharmacological trials [66,67]. However, a more recent study has observed that norepinephrine did not meliorate prognostic performance compared to BNP and a multivariate score, including clinical and laboratory parameters, the Seattle Heart Failure Model [67].
In addition to catecholamines, chromogranin A and B, contained in the granules of neuroendocrine cells, have also been shown to have an increased expression in a proportional manner to HF severity. A small study has reported that chromogranin A might be a good predictor of mortality in chronic HF patients [68].
Regarding the RRA system, the various components have been evaluated as prognostic biomarkers in HF, and plasma renin activity (PRA) has provided the most relevant results [69]. In a study of 996 patients with chronic HF, PRA was found to be an independent predictor of cardiac death with additive value to NT-proBNP and FEVS [70].
Another molecule to be included in this group is adrenomedullin (ADM), a hormone synthesized by nearly all tissues, but predominantly by the adrenal medulla, heart, lungs, and kidneys, in response to volume or pressure overload [71]. ADM has potent vasodilatory actions and has positive natriuretic and inotropic effects, as well as cardioprotective action. Plasma ADM concentrations increase in case of HF, but its routine dosing is limited by its short half-life and binding to transport proteins [46]. A fragment of its precursor, mid-regional proADM (MR-proADM), is more easily quantifiable and has been tested as a prognostic HF biomarker. In the Biomarkers in Acute Heart Failure (BACH) study, MR-proADM was revealed to be a better predictor of 90-day survival than BNP in patients with acute HF (accuracy 74% vs 62%, p < 0.001). This was confirmed by a sub-analysis of the PRIDE (N-terminal Pro-BNP Investigation of Dyspnea in the Emergency Department) study, in which MR-proADM was displayed to be the best predictor of mortality within 1 year of acute HF diagnosis, while MR-proANP and NT-proBNP showed a better prognostic performance after 1 year [46]. In 297 patients with chronic HF included in the Australia-New Zealand Heart Failure study, MR-proADM levels above the median predicted an increased risk of mortality (relative risk [RR] 3.92, 95% confidence interval [CI] 1.76-8.7) and hospitalization for HF (RR 2.4, 95% CI 1.3-4.5) at 1.5 years, independent of clinical and echocardiographic parameters. In another study of 501 patients with chronic HF, MR-proADM was a good predictor of 1-year survival, with an area under the curve (AUC) like that of NT-proBNP (p = 0.3) [47,72,73].
Vasopressin has also been studied as a potential biomarker of HF. It is a hormone with antidiuretic and vasoconstrictor activity, released by the hypothalamus in response to hyperosmolarity or hypovolemia [74]. In case of HF, inappropriate vasopressin secretion occurs mainly due to increased baroreceptor stimulation related to the reduction in cardiac output simulating a hypovolemic state. The C-terminal fragment of pro-vasopressin, called copeptin, is more easily detectable and has been evaluated as a HF biomarker. In the BACH study, patients with high systemic copeptin levels had greater pulmonary and peripheral congestion and an increased mortality at 3 months (hazard ratio [HR] 3.85, 95% CI 1.83-8.09; p<0.001), especially if affected by hyponatremia [75]. In a subsequent meta-analysis of 4,473 patients with acute and chronic heart failure, copeptin was reported to be a good predictor of all-cause mortality (RR 2.64, 95% CI 2.09-3.32), with a performance comparable to that of NT-proBNP [76].
Molecules also produced by the endothelium can be included in this group, such as Endothelin-1 (ET-1). It is produced by the vascular endothelium in response to shear stress (i.e. the effect of friction of flow along the longitudinal axis of the vessel on the intima), neurohormonal stimulation and inflammation and exerts vasoconstrictive, pro-inflammatory and pro-oxidative biological effects and promotes cardiac remodeling. The endothelium releases a precursor, ET-1, which is then converted in circulation to ET-1 by the endothelium [77].
Finally in this group we include Urocortin-1. It is a member of the corticotropin-releasing factor family. It is produced mainly in the central nervous system, but also in numerous peripheral tissues, such as the heart. Urocortin-1 has vasodilatory, cardiostimulating and cardioprotective properties. Circulating levels of urocortin-1 increase in HF, but this biomarker does not appear to have additional diagnostic or prognostic value over NT-proBNP [78].
3.2. Biomarkers of Fibrosis and Cardiac Remodeling
Fibrosis and cardiac remodeling result from chronic stress on the heart, disrupting myocardial function and increasing the risk of arrhythmias. Here, we report some molecules involved in these mechanisms that might be used as HF biomarkers [52,79,80,81].
The first to be included in this group is Galectin-3 (Gal-3), a member of the Galectin family. It plays a key role in inflammation and fibrosis. Accordingly, acute or chronic cardiac injury can activate immune cells in the myocardium that release cytokines. In turn, they activate fibroblasts and myofibroblasts, which deposit collagen and evocate cardiac fibrosis, two remarkable mechanisms in the HF onset [82,83,84,85]. However, it has been reported that Gal-3 levels enhance progressively with age and tend to be slightly higher in women than in men. In addition, Gal-3 also rises in other conditions, such as systemic inflammation and renal failure. Thus, it is not HF specific. Nevertheless, the Gal-3 expression linked to pro-inflammatory cytokines is upregulated in HF. However, its plasma Gal-3 levels are not helpful for the HF diagnosis, but for short-term mortality and rehospitalization. Gal-3 has also been suggested to be useful in predicting all-cause mortality and heart failure hospitalization. The prognostic power of Gal-3 is more significant in HFpEF than in HFrEF [82,83,84,85].
Potential component of such group also is Suppression of tumorigenesis-2 (ST2), a member of the interleukin-1 receptor family and has two key isoforms: a transmembrane receptor (ST2L) and a soluble isoform of ST2, known as sST2. sST2 is a decoy receptor that can be quantified in serum. Its ligand is interleukin-33 (IL-33) [86,87,88,89,90,91]. The ST2L and IL-33 pathway is involved in intramyocardial communication between fibroblasts and cardiomyocytes and appears upregulated during myocardial injury, where it plays a cardioprotective role. The soluble isoform, sST2, can bind IL-33 with a higher affinity, consequently competing with the interaction between IL-33 and ST2L. This results in an effect opposite to the cardioprotective one [86,87,88,89,90,91]. sST2 is produced predominantly extra-cardiacally in response to hemodynamic overload, inflammation and profibrotic stimuli, all of which are common in HF. As a non-cardio-specific marker, sST2 cannot be used for the diagnosis of acute HF, however, its measurement is useful in prognostic stratification [86,87,88,89,90,91]. A meta-analysis conducted on 4,835 patients with acute HF demonstrated that sST2 values at admission and discharge were predictive of all-cause mortality (HR 2.46, 95% CI 1.80-3.37 and HR 2.06, 95% CI 1.37-3.11, respectively) and cardiovascular mortality (HR 2.29, 95% CI 1.41-3.73 and HR 2.20, 95% CI 1.48-3.25, respectively) [92]. In contrast, sST2 concentration at discharge predicted rehospitalization for heart failure (HR 1.54, 95% CI 1.03-2.32). Repeated quantification of sST2 is particularly important, as demonstrated by a study of 150 patients with acute HF, in which the percentage change in sST2 during hospitalization was predictive of death at 3 months, independently of BNP or NT-proBNP values. Similarly, the Translational Initiative on Unique and novel strategies for Management of Patients with Heart failure (TRIUMPH) cohort study of 496 patients with acute HF, who underwent 7 repeat blood draws during 1 year of follow-up, demonstrated that baseline sST2 levels were predictive of all-cause death or hospitalization for heart failure (HR for each 1 SD increase in log2(ST2) value: 1.30, 95% CI 1.08-1.56), but, more importantly, that repeated sST2 measurement was an even stronger prognostic predictor (HR for each 1 SD increase in log2(ST2) value: 1.85, 95% CI 1.02-3.33), independently of serial NT-proBNP values [92,93]. The role of sST2 in the prognostic stratification of chronic HF is even more relevant, as demonstrated by several studies and confirmed by a recent meta-analysis. The prognostic value of sST2 in chronic HF is independent of NT-proBNP and hs-TnT and is less influenced by age than the latter [92,93]. The prognostic performance of sST2 is similar in HFrEF and HFpEF and is superior to that of Gal-3 in chronic HF. Furthermore, sST2 is an independent predictor of reverse remodeling, so much so that it has been included in a specific score, the ST2-R2 score, which includes an sST2 value <48 ng/ml (3 points), non-ischemic etiology (5 points), absence of left bundle branch block (4 points), history of heart failure <1 year (2 points), LVEF <24% (1 point), and treatment with beta-blockers (2 points). The ACC/AHA guidelines recommend the measurement of sST2 for the prognostic assessment of patients with chronic HF [92,93]. In contrast, the ESC guidelines state that there is insufficient evidence to recommend its use in clinical practice. However, most of the major studies on the role of sST2 in acute and chronic HF have been performed and published after the publication of the guidelines. There is still no unanimous consensus on the best prognostic cut-off for sST2 in chronic HF. However, a recent meta-analysis suggests a value of 28 ng/ml, while other studies have proposed a concentration of 35 ng/ml40 [92,93].
Growth/differentiation factor 15 (GDF-15) or macrophage inhibitory cytokine-1, MIC-1) might be included in such group. It has been revealed to be significantly related to HF [94,95]. GDF-15 expression is induced by cellular stressors, including inflammation, myocardial ischemia, and cancer. In the context of HF, GDF-15 levels have been shown to be independently associated with exercise capacity and quality of life. Additionally, the combination of GDF-15 and NT-proBNP appears better distinguishing patients with HFpEF from controls. GDF-15 levels increase in all stages of HF, even in asymptomatic heart failure stage B [94,95]. Elevated levels of GDF-15 in HF patients may be detected as early as 90 days before hospital admission for decompensated HF compared to a control group. However, the exact physiological role of GDF-15 has not been fully elucidated due to its pleotropic nature. GDF-15 is positively correlated with left ventricular remodeling [94,95]. Given the association between GDF-15 and adverse HF outcomes, the question remains whether the protein may play a counterregulatory or contribute to HF pathogenesis. Much evidence supports the protective and antihypertrophic effects of GDF-15 on the heart. Although positively correlated with left ventricular remodeling, many experiments have shown that GDF-15 exhibits an anti-hypertrophic effect through the SMAD signaling pathway. Furthermore, GDF-15 appears to have an anti-inflammatory effect. There are, however, some conflicting data regarding the cardioprotective role of GDF-15. Thus, further investigations are essential for eliminating such gaps and applying it in HF clinical management [94,95].
In HF, an alteration in the expression of several extracellular matrix degradation products, such as MMPs and TIMPs, is observed. These have been evaluated as diagnostic or prognostic biomarkers in HF, with variable results in individual studies [96,97]. A study by Zile et al. demonstrated that the combination of an increase in MMP-2, TIMP-4, procollagen type III amino-terminal peptide (PIIINP) and a decrease in MMP-8 was predictive of the presence of HFpEF (AUC 0.79) [96]. The concentration of these molecules probably reflects the extent of cardiac tissue remodeling, with important prognostic implications. In a subanalysis of the Randomized Evaluation of Aldactone Study (RALES), baseline PIIINP >3.85 μg/l were predictive of adverse outcomes and a reduction in PIIINP was observed only in the spironolactone group, confirming the antifibrotic effect of this drug. Furthermore, the prognostic benefit of spironolactone intake was significant only in subjects with high baseline levels of collagen degradation products. Likewise, in a sub-analysis of the PARAGON-HF (Prospective Comparison of ARNI With ARB Global Outcomes in HF With Preserved Ejection Fraction) study, treatment with sacubitril/valsartan resulted in a significant reduction in the levels of some extracellular matrix degradation products, including TIMP-1 and PIIINP, at 16 months of follow-up compared to valsartan alone [98].
Another potential biomarker of fibrosis of more recent discovery is Fibroblast Growth Factor 21 (FGF21) [99,100,101]. It is a polypeptide ligand primarily produced by liver and adipose tissue cells. Its traditional function is of hormonal regulator of metabolism, through endocrine, paracrine, and autocrine mechanisms. Its expression is also stimulated by various cardiac stresses. Serum FGF21 levels are strongly linked to left ventricular systolic dysfunction, and patients with higher levels show an increased risk of cardiac death compared to those with lower levels. In addition, its levels are independent of other comorbidities. This has led to hypothesizing a link between the liver and the heart, being the liver its principal producer. Precisely, it hypothesizes that congestive hepatopathy occurs in advanced HF, and consequently elevated FGF21 levels in this condition may indicate a compensatory protective feedback loop. Further research is needed [99,100,101].
More recently included in this group are osteopontin (OPN), syndecan-4 (SDC-4) and myostatin (MSTN) [54,102]. ONP is an extracellular matrix signal transduction protein, whose expression is related to biomechanical stress. Accordingly, OPN synthesis is significant in the post-myocardial infarction heart and in heart failure, because of dilated cardiomyopathy. This allows to quantify plasma OPN levels in heart failure, proving to be an excellent prognostic biomarker [103]. SDC-4 is a member of the syndecan family and has a glycoprotein structure as a transmembrane protein involved in signal transduction, tissue regeneration, angiogenesis and focal adhesion. Its expression increases due to activation by growth factors and extracellular matrix (ECM) proteins. In the context of HF, its increased levels are significantly associated with left ventricular hypertrophy. MSTN is an extracellular matrix (ECM) signaling molecule that is functionally considered a negative regulator of muscle mass [104]. Serum MSTN levels have been shown to increase with the severity of heart failure and clinical outcome. Patients with the chronic form of heart failure have higher serum MSTN levels, which are significantly associated with a lower survival rate and a higher number of rehospitalizations [105,106].
Finally, it has demonstrated that proteins related to collagen metabolism or ECM regulation, including Endotrophin, thrombospondin-2 (THBS-2) and a disintegrin and metalloproteinase with thrombospondin motifs like 2’ (ADAMTSL), the large extracellular matrix protein SVEP1 (sushi, von Willebrand factor type A, EGF and pentraxin domain containing 1), as well as Vascular endothelial growth factor-C (VEGF) have been also associated to cardiac remodeling and HF [54,102,107].
3.2. Biomarkers of Inflammation and Oxidative Stress
HF is characterized by a chronic subclinical inflammatory state that is self-sustaining from progressive cellular damage and is partly responsible for progressive cardiac remodeling. Inflammation in HF can be triggered by direct damage to cardiomyocytes (e.g. ischemia, pressure overload) or rather be the reflection of a systemic inflammatory state related to comorbidities; this latter mechanism seems crucial for the development and progression of HFpEF. The first demonstration of an elevation of C reactive protein (CRP) in HF dates is linked to a work conducted in 1953. Since then, numerous studies have investigated this association, highlighting a prognostic role in HF for CRP, tumor necrosis factor alpha (TNF-α) and IL-6 in chronic HF. The elevation of these three biomarkers has also been associated with an increased risk of developing HF in elderly subjects. However, the poor specificity of these biomarkers for cardiovascular diseases, HF included, and the current lack of anti-inflammatory therapies for HF limits their possible applications [108,109,110].
Recently, the attention has been focused on carbohydrate antigen-125 (CA125). Accordingly, sufficient literature data currently reports that CA125 has a potential role in the clinical management of patients with acute HF, as a prognostic biomarker, as well as of congestion and monitoring of decongestion therapy. However, CA-125 is known to be a worldwide used biomarker of ovarian cancer, as in other processes. It results, indeed, involved in fluid and cell transport, inflammation, tissue repair, and the well-recognized tumor dissemination. For example, N-glycans associated with CA-125 have been shown to modulate immune responses. In line with this role, CA-125 has been observed to suppress the activity of natural killer cells by interacting with several proteins. In the HF case, systemic levels of CA-125 augment, even if the exact mechanisms involved are not entirely identified. The involvement of Ca-125 in HF has been evidenced for the first time by Nagele and coworkers. They reported in two studies increased circulating levels of numerous tumor biomarkers, CA 125 included, in HF patients before and after heart transplantation [111,112]. Since then, other researchers have examined the role of this molecule in heart failure. Romina’s group has recently reviewed all studies of CA-125 in HF in a systematic review that included data from 170 studies. In many of these, they have highlighted the close association of CA-125 with a) the congestion observed in acute HF, b) the high rates of mortality and c) readmission at 6 months of follow-up after discharge from acute HF, and d) also the role of CA-125 in guiding HF therapy [113]. They also reported that some clinical studies have examined several peculiarities of CA-125, which make it even better than NT-proBNP in different scenarios of acute HF. However, the mechanisms related to the upregulation of serum CA 125 in patients with congestive HF have not been confirmed or fully understood. Therefore, CA-125 is a promising biomarker of congestion in the setting of acute HF and there also is evidence on its role in risk stratification, monitoring and guiding therapy in this setting. However, further studies are needed to implement CA-125 in clinical practice of HF management to establish reference intervals for HF and appropriate algorithms for diagnosis and treatment monitoring. Although it is commonly available, for a better clinical efficacy in screening and early diagnosis, serum CA-125 levels should be used by clinicians in combination with clinical manifestations, as well as other biomarkers, i.e. NT-proBNP, ultrasound and other multimodal methods [111,112].
Recently, it has been also described as an important prognostic biomarker, the CRP/Albumin ratio (CAR) in chronic HF. In patients with chronic HF, CAR was associated with unfavorable clinical picture, characterized by elevated pulmonary artery systolic pressure (PAPS), an increased left ventricle end-systolic volume (LVESV), and decreased tricuspid annular plane excursion TAPSE. This association might be supported by the inflammatory etiology of chronic HF. Precisely, in case of chronic HF, inflammatory mediators and pro-inflammatory cytokines induce a diastolic and systolic dysfunction of cardio muscle cells and later their atrophy and remodeling that result pathognomonic of such HF form [114,115,116,117,118].
Recent studies have also shown that the neutrophil-to-lymphocyte ratio (NLR) could
be related to adverse outcomes in patients with HF [119,120,121,122]. Accordingly, a recent meta-analysis, that included a total of 15 studies with 15,995 patients with acute HF, has evaluated whether NLR could predict mortality. By stratifying the patients based on a cut-off NLR, it has been observed that high NLR quartiles were associated with a significantly higher in-hospital mortality [HR 1.54, 95% CI (1.18–2.00), p < 0.001] and long-term all-cause mortality [HR 1.61, 95% CI (1.40–1.86), p < 0.001] compared to group with reduced NLR quartiles. In addition, the comparation with the highest against the lowest NLR quartiles, demonstrated that cases with the highest NLR quartiles had a significantly heightened risk of long-term all-cause mortality [HR 1.77, 95% CI (1.38–2.26), p < 0.001] compared to that of lowest NLR quartiles. Thus, elevated NLR levels can predict a raised risk of short- and long-term mortality and could be a useful biomarker of adverse outcome in patients with acute HF [121].
Another typical mechanism of HF is mitochondrial dysfunction responsible for increased oxidative stress. Reactive oxygen species (ROS), in turn, damage cellular structures and promote the initiation and perpetuation of inflammatory processes, generating a vicious circle. The intrinsic instability of ROS makes their measurement difficult, however, molecules that interact with ROS, including antioxidants, are good indicators of oxidative status. Some of these molecules have been evaluated as biomarkers in HF and the most interesting results in terms of prognostic stratification, although limited to a few studies, have been obtained with myeloperoxidase (MPO) and, to a lesser extent, with uric acid. MPO is an enzyme released by leukocytes during the inflammatory response. Plasma MPO concentration increases in chronic heart failure and a significant correlation with NYHA class and BNP levels has been demonstrated in one study. In another study of 667 patients with acute dyspnea, MPO was equally elevated in subjects with noncardiac and cardiac dyspnea, however in the latter it was an independent predictor of 1-year mortality compared with BNP [123,124,125].
3.4. Clinical Viewpoint: Considerations and Limitations
Fibrosis and cardiac remodeling represent two fundamental mechanisms in the pathophysiology of HF [79,80,126,127]. Currently, however, most of the described biomarkers have limited clinical applicability, although at the same time quite significant to identify pathways associated with HF onset and progression. Some studies using MMP inhibitors have not shown unequivocal positive results. However, the above-described biomarkers, as well as those of inflammation and oxidative stress, appear all to represent very promising therapeutic targets in both acute and chronic HF settings. Furthermore, the growing interest in the involvement of the lymphatic system in acute HF shows enormous promise for the clinical utility of biomarkers of lymphatic dysfunction and failure (such as VEGF-C) [128,129]. Finally, there are strong clinical reasons to believe that biomarkers of lymphatic dysfunction (i.e., members of the VEGF family) can be used as appropriate biomarkers of peripheral congestion, since the natriuretic peptides are biomarkers of intracardiac pressure, rather than biomarkers of interstitial pressure. Thus, further studies are necessary to include these biomarkers in clinical practice [130].
The biomarkers discussed so far with their relative advantages and limitations are summarized in Table 4.
4. Other Promising Biomarkers: Biomarkers of Negative HF Outcomes
Patients with HF have several comorbidities, from iron deficiency [131,132,133] to endocrine-metabolic alterations [134] to renal and hepatic function alterations [135,136,137,138]. Therefore, the use of appropriate biomarkers could facilitate the evaluation of HF outcomes. Emerging evidence is proposing many biomarkers, that we describe below, by highlighting their benefits and limitations.
4.1. Iron Deficiency
Iron deficiency (ID) is one of the most common comorbidities in heart failure [139]. 30-60% of patients with HF are affected by ID, and it particularly affects cases with chronic and anemic form [140]. ID is more prevalent in women with HF and a more advanced stage of severity. In fact, ID significantly correlates with higher levels of natriuretic peptides and NYHA classes III or IV [140]. Recent studies have also reported that ID is prevalent in 50-70% of cases with acute form. ID is a serious comorbidity because it highlights not only the anemic condition, but also the presence in patients of other alterations ranging from mitochondrial dysfunction, impaired energy processing, alterations of reactive oxygen species and abnormalities of the immune response, just to name a few [140]. This explains the attention paid to ID in HF also as an effective target for therapeutic interventions. Two forms of ID are typically distinguished: absolute and functional. The former reflects low (or even absent) iron stores in the body, while the latter characterizes a state with sufficient levels of stored iron and inadequate iron availability for all iron-using processes in the body [141]. In functional ID, poor iron availability may be the result of downregulation of ferroportin 1, a protein involved in the efflux of iron from enterocytes, macrophages and hepatocytes into the extracellular space and bloodstream [131,132,133].
The causes underlying the high prevalence of ID in HF cases appear multifactorial and not yet fully clear. However, it is hypothesized that ID in HF is related to impaired absorption from the duodenum due to intestinal edema, inadequate dietary iron intake, multiple drug interactions, chronic gastrointestinal bleeding, or other comorbidities (such as chronic renal dysfunction) [141,142]. A precise evaluation of iron metabolism and exact diagnosis of ID in HF remains a challenge. However, the bone marrow biopsy constitutes the gold standard tool for best quantifying the body’s depleted iron stores and for the diagnosis of absolute ID. Nonetheless, it is an invasive procedure, rarely used, and replaced by the quantification of levels of several blood biomarkers, which allow us to determine iron status and make ID diagnosis [131,132,133,143]. They are briefly discussed below.
4.1.1. ID Blood Biomarkers
They encompass ferritin, transferrin saturation, soluble transferrin receptor and hepcidin [144]. The ferritin represents the iron storage protein secreted by the liver and reticuloendothelial system, and its blood levels give information about its expression in the iron-storing tissues. However, in case of HF serum ferritin levels might be non-specifically elevated due to high inflammation [144,145,146,147].
Transferrin saturation (TSAT), the percentage of transferrin bound to iron, can be used as a parameter for quantifying the amount of iron available to cells. Malnutrition and catabolic metabolism can determine a reduction in serum transferrin than serum iron, resulting in a false increase in TSAT. TSAT and ferritin, are normally utilized to evaluate ID in patients. The 2021 ESC guidelines for HF recommend treatment of ID in patients with HF in case of serum ferritin levels <100 g/L, or between 100 and 299 g/L with TSAT <20% [148]. A recent study has investigated the usefulness of these two biomarkers in patients with HF and has suggested that TSAT is a useful diagnostic tool in identifying patients with HF, while the evaluation of ferritin levels is not essential [144,149].
The soluble transferrin receptor (sTfR) is a membrane receptor of cells that require iron. Its blood levels reflect the number of cells expressing the receptor and its cellular density, making it strongly associated with iron requirement and the rate of erythrocyte proliferation. Elevated sTfR levels indicate insufficient cellular iron availability, which translates into clinical outcome [144,149,150,151].
Hepcidin is a hormonal peptide produced in the liver in response to pro-inflammatory signals (mainly through the interleukin-6 pathway) and its key role is to decrease the efflux of iron from enterocytes, hepatocytes and macrophages into the bloodstream. This occurs by binding to ferroportin 1 and triggering its lysosomal degradation. Low serum hepcidin levels indicate depletion of iron stores, independent of anemia. Recent studies have combined low serum hepcidin and high serum sTfR as an alternative tool to diagnose ID in HF. In the study of 165 patients with acute HF, hepcidin and sTfR have been shown to be advantageous biomarkers for identifying ID (representing both depletion of iron stores and unmet need for iron utilization) independent of anemia, as well as a predictor of poor prognosis in patients with the most severe ID [144,152,153].
In addition to the biomarkers abovementioned, RDW, a measure of the heterogeneity of the distribution of red blood cell size, has been also used to diagnose ID. High RDW values also occur in conditions of decreased availability of iron due to ID, anemia (low ferritin) or due to functional ID in the anemia of inflammation (AI) (normal/high ferritin). A study revealed that RDW is a parameter with a sensitivity of 94% and specificity of 59% for the diagnosis of ID [154,155].
4.1.2. Clinical Viewpoint: Considerations and Limitations
Biomarkers of iron metabolism in HF appear as a perfect example of molecules with strong pathophysiological and clinical relevance, which are translated into daily practice. The relationship between iron metabolism, pathophysiological basis, HF symptoms (e.g., exercise tolerance) and prognosis significantly reflects the value and utility of such biomarkers, translated into HF guidelines. Consequently, it is strongly recommended that all HF patients must be screened periodically for anemia and ID, and any alteration identified must be treated as a therapeutic target in both acute HF and congestive HF [131,132,133].
In clinical application of such biomarkers, however, it is imperative to consider a very important aspect. It is historically known that serum ferritin levels <15-20 μg/L identify patients with bone marrow ID. Nevertheless, serum ferritin levels may be distorted by systemic inflammatory states, such as those observed in patients with chronic kidney disease or HF. Consequently, this had led, approximately 25 years ago, to enhance the diagnostic threshold of ferritin of 5- to 20-fold in patients with chronic kidney disease (i.e., iron deficiency was identified if the serum ferritin level was <100 μg/L, regardless of transferrin saturation [TSAT], or 100 to 299 μg/L if TSAT was <20%). However, this recommendation has been demonstrated to be not supported by the experimental data on total body or tissue iron depletion but only adopted for encouraging the use of iron supplements and augmenting the response to erythropoiesis-stimulating agents in patients with renal anemia [144,156]. However, in patients with HF, this definition has been soon considered not appropriate because it does not consent to differentially discriminate patients with absolute or functional ID. It allows, indeed, to identify individuals with TSAT (≥20%) and serum ferritin levels in the normal range (20-100 mg/L), who are not iron deficient and show a good prognosis and consequently do not respond favorably to iron therapy. In addition, in HF cases, serum ferritin levels may be influenced by therapeutic treatments, i.e. neprilysin and sodium-glucose co-transporter 2 inhibitors, known to mobilize endogenous iron stores [144,156]. In contrast, the definition that appears more appropriate and confirmed by clinical trials, is hypoferremia, represented by a TSAT <20%. Patients with such condition, respond to intravenous iron therapy, showing a meliorated tolerance at the exercise, a good functional capacity (when significantly impaired) and a pronounced decrease in the death or hospitalization risk (i.e., 20%-30%). Consequently, it proposes to abandon the current ferritin-based definition of ID in HF and adopt a definition based only on hypoferremia (TSAT <20%) [131,132,133].
4.2. Altered Renal Function: Related Biomarkers
Renal function measures such as creatinine and GFR are commonly used in clinical practice to monitor the effects of HF therapy, especially diuretics [157]. However, these parameters are also useful as prognostic biomarkers. In a study of 9,289 patients with chronic HF, GFR was estimated based on creatinine levels, and demonstrated to have an independent and additive prognostic value compared to NT-proBNP and hs-TnT [158,159]. Some studies have also suggested that cystatin C, a cysteine protease inhibitor with ubiquitous expression and a clearance entirely dependent on glomerular filtration, may be a predictor of prognosis in acute and chronic HF, potentially superior to creatinine. Other biomarkers are evaluated because a common comorbidity of HF is renal alterations. Among the different molecules studied, the most promising is neutrophil gelatinase-associated lipocalin (NGAL), a siderophore protein released by neutrophils and epithelial cells in response to acute kidney injury and inflammation [160]. In a study of 121 patients with acute HF, NGAL levels >167.5 ng/mL (75th percentile) were associated with a 2.7-fold increased risk of death and a 2.9-fold increased risk of death or hospitalization. In chronic HF, levels of renal injury molecule 1 (KIM-1) and N-acetyl-beta-(D)-glucosaminidase (NAG), two molecules expressed by proximal renal tubular cells, appear to correlate with NYHA class and worse LVEF, and these analytes have been proposed as additional markers of cardiorenal syndrome and prognosis in HF [160]. Remarkably, in a study of 2,130 patients from the GISSI-HF (Italian Group for the Study of Survival in Heart Failure) study, both NGAL and KIM-1 and NAG were independently associated with the combined endpoint of death and hospitalization for HF, even in patients with normal renal function [160].
4.2.1. Clinical Viewpoint: Considerations and Limitations
Such biomarkers are fundamental for HF prognosis. Consequently, it is strongly recommended that all HF patients must be screened periodically for renal alterations and therapeutic efficiency
4.3. Altered Hepatic Function: Related Biomarkers
In patients with advanced HF, it is common to find an alteration of liver function. This depends primarily on the congestion of the hepatic venous system resulting from the right ventricular dysfunction. Consequently, some indices of liver dysfunction, such as increased transaminases and bilirubin and hypoalbuminemia (the latter also dependent on an enteric loss secondary to intestinal congestion), can stratify patients with acute or chronic HF at greater risk of adverse events [137].
4.4. Endocrine-Metabolic Changes
Endocrine-metabolic changes partly indicate the state of cachexia that occurs in patients with HF and contribute to its progression by increasing neurohormonal activation and inflammation. Thyroid dysfunction, which may manifest subclinical hypothyroidism or low T3 syndrome, is common in patients with chronic HF and is associated with more severe symptoms and a worse prognosis. Serum and salivary cortisol levels are frequently elevated in patients with chronic HF and have been associated with increased mortality. Adipokines are a class of hormones implicated in the regulation of glucose and fatty acid metabolism. Among these, adiponectin, a protein secreted inversely proportional to the percentage of body fat, has been the most studied to date in HF. Adiponectin levels increase in chronic heart failure and appear to predict a poor prognosis [159,161].
5. Considerations: Towards the Development of Multi-Biomarkers Panels Through Artificial Intelligence and Multi-Omics???
The large number of emerging biomarkers described above encourages the development of multi-biomarker panels, reflecting the different pathophysiological pathways involved in the onset and progression of heart failure [162]. The reason for this interest lies in the high potential that such multi-biomarker panels offer in the clinical context of a disease, such as HF. In theory, they would allow not only to personalize and improve the clinical management of heart failure, but also to optimize the therapeutic strategy. Indeed, the possible increase or reduction of blood levels of a specific biomarker using such panels could offer us important information to translate into the context of a treatment, by suggesting introducing, reducing or increasing a treatment aimed at counteracting the pathophysiological pathway related to such increase or reduction. Consequently, this could allow better personalization of therapy, although this approach has not yet been tested in randomized controlled clinical trials [114,163,164,165].
In addition to this consideration, the positivity of such panels, correlated with the increase in levels of different biomarkers, could be used to develop prognostic scores for HF, as well as for screening to estimate the risk of developing HF in the general population [165]. Experimental support comes from several studies that have evaluated multi-biomarker scores for prognostic stratification of acute and chronic HF or to estimate the risk of developing HF in the general population. For example, in one study, the combined use of hs-TnT and NT-proBNP with cutoffs stratified by GFR categories was proposed for the stratification of patients with chronic HF [92]. Furthermore, in such studies, the choice of biomarkers to include in the models was generally discretionary. In a recent sub-analysis of the TOPCAT (Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist) study, a machine learning approach was used to generate a multi-biomarker panel (from 49 available analytes) to predict clinical outcome (death, hospitalization, or readmission) in patients with HFpEF [166]. Machine learning (ML) offers a robust approach for the development of multi-biomarker panels [167]. ML is also used to facilitate HF diagnosis, risk stratification, treatment optimization, and drug discovery, providing a data-driven approach to personalized care [168]. ML algorithms are also applied to improve HF risk prediction through the analysis of electronic health records (EHR), multi-omics data, and input from wearable sensors [168]. Furthermore, it is also applicating the digital twins ‘model [169]. Digital twins’ models consent to perform patient-specific simulations and to evaluate disease progression and response to therapy [169]. Thus, artificial intelligence (AI) is also revolutionizing HF management, as well as cardiac imaging and phenotyping algorithms [170]. For example, AI-assisted imaging is used for evaluating left ventricular function, myocardial fibrosis, and diastolic dysfunction with greater accuracy than manual interpretation. All these AI applications enable machine learning-based HFpEF phenotyping models to integrate clinical, biomarker, and imaging data to classify patients into pathophysiological distinct subgroups, facilitating the identification of targeted [171]. However, their validation on different imaging datasets (e.g., echocardiogram) and healthcare systems are still ongoing. AI also offers further benefits, such as the advancing of precision medicine by integrating genomic, proteomic, and metabolic profiles to identify HF phenotypes that respond to specific treatments [171]. Moreover, AI is reducing drug development time by analyzing biological datasets, predicting drug-target interactions, and adapting existing treatments. As AI continues to evolve, its integration with digital health technologies and adaptive clinical trials could optimize HF management and treatment selection. However, challenges related to data bias, interpretability, and ethical considerations need to be addressed to ensure fair and clinically relevant applications [171].
5.1. From the Application of Multi-Omics to the Identification of Further Emerging Biomarkers: Genetic, Genomic and Transcriptome Biomarkers
Probably, the application of omics technologies could also facilitate the development of multi-biomarker panels [102]. Omics has expanded over the past 20 years, allowing a more specific knowledge of disease pathophysiology at the molecular level, thus leading to identifying biomarkers and targets for targeted treatments [102]. Accordingly, omics allows the study of molecules or biological processes involved in a disease by using different omics, ranging from genomics, and transcriptomics, to epigenomics, proteomics, metabolomics, and more [172]. Thanks to multi-omics, many data may be obtained and combined, becoming even more appropriate tools for understanding biological processes and disease development pathways. For example, the use of multi-omics has recently allowed us to identify genetic and epigenetic factors involved in HF development and progression. Accordingly, diverse single nucleotide polymorphisms (SNPs), which represent genetic variations affecting individual susceptibility, disease progression, and response to treatment, have been associated with HF. In HFpEF cases, a significant genetic distribution of genetic variations in genes associated with inflammation and fibrosis, such as the interleukin-6 receptor (IL6R) gene, was detected. They consent to elucidate the systemic inflammatory and fibrosis mechanisms underlying HF pathophysiology [173]. Similarly, in HFrEF, SNPs in the beta-adrenergic receptor gene (ADRB1) gene, particularly the Arg389Gly variant, have been shown to influence the therapeutic response to beta-blockers. The Arg389 variant is associated with enhanced beta-adrenergic signaling, resulting in increased myocardial contractility and increased sensitivity to beta-blockers [174]. Furthermore, SNPs in the angiotensin-converting enzyme (ACE) gene, such as insertion/deletion (I/D) polymorphism, show significant effects on RAAS. The D allele is associated with increased circulating levels of ACE, resulting in increased production of angiotensin II, which contributes to myocardial remodeling and worsening heart failure outcomes. Consequently, HFrEF patients with the DD genotype may benefit more from ACE inhibitors, highlighting the potential of personalized RAAS-targeted therapy in the treatment of heart failure [175].
In addition to SNPs, cell-free DNA (cfDNA) has been detected as e biomarker in HF. cfDNA is delivered during apoptosis or cell necrosis, and its levels correlate with the degree of tissue damage and systemic inflammation. In HFrEF cases, elevated cfDNA levels reflect myocardial damage and disease severity. In HFpEFcases, cfDNA is while associated with endothelial dysfunction and microvascular pathology. By combining cfDNA with transcriptomic profiling might increase the potential of stratifying the risk and prognostic accuracy in all HF cases, especially in complex or borderline cases. Genome-wide association studies (GWAS) have while allow to identify genetic loci associated with myocardial stress and fibrosis, such as TTN and BAG3 (see below for additional information), which might represent further biomarkers for better predicting HF risk, and targets for more targeted therapy [176].
In addition to SNPs, transcriptomic molecules, particularly non-coding RNAs (ncRNAs), have attracted attention for their regulatory role in the pathophysiology of HF. Among them, the role of microRNAs (miRNAs) has been recently demonstrated. miRNAs are small endogenous non-coding molecules of RNA involved in gene expression regulation. miRNAs have different roles [177]. They can modulate infarct area size, cardiomyocyte restoration, collagen deposition, and macrophage polarization. miRNAs may be considered as specific biomarkers of hypertrophy and fibrosis. In HFpEF, miR-223 and miR-29 are clearly associated with myocardial fibrosis and systemic inflammation, [177,178]. Moreover, miR-503-5p and miR-193a-5p have been demonstrated to be promising biomarkers for the differential diagnosis between HFpEF and HFrEF [179,180]. Furthermore, in HFrEF cases, miR-208 and miR-499 have been associated with cardiac remodeling, myocardial stress and apoptosis, making them valuable indicators of disease severity and progression [181]. miRNAs have also been suggested as a therapeutical tool [179]. In fact, they can be administered, counting for example myocardial pathophysiological remodeling related to HF onset. Precisely, antimir and miRNA mimics are small oligonucleotides which may be administered in several manners and may be able to control the expression of specific and circulating miRNAs. Studies on animal models and on healthy humans prove that these molecules are well tolerated and effective, giving the possibility of using such treatment in cases of HF. The application of miRNAs for diagnosis, prognosis and therapy in HF adds another way for developing personalized and tailored approaches. Some examples of miRNA in HF are reported in Table 5. Further studies are, however, needed, since this field is still in a baby entity.
6. From Identifying New Molecules as Emerging Biomarkers to Applying Them as Targets for Innovative Treatments in HF
Classical HF therapy includes beta-blockers, angiotensin receptor neprilysin inhibitors (ARNIs), and mineralocorticoid receptor antagonists (MRAs), which lead to suboptimal outcome [171]. Recently, however, treatments with sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors), soluble guanylate cyclase stimulators (sGC stimulators), and cardiac myosin activators have shown good efficacy in both HF cases with HFrEF and HFpEF [171]. Furthermore, molecularly targeted therapies, including clustered regularly interspaced short palindromic repeats (CRISPR)-associated protein 9 (Cas9) gene editing, RNA therapies, and adeno-associated virus serotype 9 sarcoplasmic reticulum calcium ATPase therapy (AAV9-SERCA2a gene), are emerging as potential novel treatments for HF [171]. Some of these treatments are described below. Examples of their efficacy, highlighting their mechanism-specific interventions with respect to metabolic, contractile, and vascular abnormalities are also reported.
6.1. Molecular Targeted Therapies
CRISPR-Cas9 gene editing offers the potential to correct or silence genetic variants, such as mutations, associated with diverse dilatated cardiomyopathies [182]. For example, titin truncating variant (TTNtv), myosin-binding protein C3 (MYBPC3), lamin A/C gene (LMNA) and BCL2-associated athanogene-3 (BAG3) constitute the most common pathogenic mutations related to onset of dilatated cardiomyopathies [182], that cause HF as complication. Precisely, these mutations cause sarcomere disfunction, leading to HF. Preclinical studies conducted prevalently in iPSC-derived cardiomyocytes have obtained positive results [171]. However, diverse obstacles must be still resolved for applying this strategy in clinical setting. For example, off-target effects, immune responses to viral vectors, and difficulties in vivo delivery still represent significant challenges. In alternative, base editing and prime editing techniques provide more precise single-nucleotide corrections with minimal DNA damage and improve safety. Beyond these potential treatments, AAV9-SERCA2a gene therapy consents to target calcium homeostasis, representing a critical dysfunction in HF [171]. SERCA2a downregulation damages calcium cycling, leading to myocardial dysfunction. Calcium Upregulation by Percutaneous Administration of Gene Therapy in Cardiac Disease (CUPID-1) trial has evidenced that AAV9-SERCA2a overexpression enhanced ventricular function, while the CUPID-2 trial failed to confirm these promising results because of poor vector transduction [171].
Another targeted treatment is based on the use of RNA-based interventions. As mentioned above, antisense oligonucleotides (ASOs) and small interfering RNAs (siRNAs) provide an optional strategy for HF gene modulation. Among miRNAs associated with HF, miR-132 emerges as a key regulator of cardiac remodeling, and has been considered as an appropriate biomarker and treatment-target of HF [171]. A recent trail, the Cardior-132-L (CDR132L), is currently iPhase 1, and is evaluating the treatments with specific ASOs and siRNAs for reducing the levels of miR-132 and contemporary improving myocardial fibrosis and heart function. Another promising RNA therapy is inclisiran, known for reducing lipid levels. It might be applied to patients with HFpEF and systemic inflammation and dyslipidemia, limiting the atherosclerosis effects [171].
Another targeted treatment is focused on limiting inflammation in HF, to have a more positive outcome. For example, targeted inflammation treatment in trials conducted in HFpEF cases with biologics, such as ziltivekimab, shows promising results. Precisely, it reduced hs-CRP and enhanced vascular function and exercise capacity [171]. Certainly, combining anti-inflammatory biologics with metabolic or vascular-targeted therapies could be more effective in addressing the different mechanisms of the disease, since HF is also characterized by significant metabolic and vascular alterations. Therefore, further studies are needed. However, all these treatments seem promising, even if they are still in the experimental phase and far from routine clinical use. AI and multi-omics could probably refine all the variables that appear weak, such as patient selection. For example, polygenic risk scores or transcriptomic profiling could better identify patients, who could benefit from more specific treatments, thus personalizing therapy and improving outcomes.
6.2. Challenges and Future Directions
Despite significant progress in the development of novel pharmacological treatments, such as molecular-targeted therapies, several challenges impede their integration into routine HF management. For overcoming these obstacles is necessary to guarantee safety, scalability, affordability and clinical applicability. Long-term safety and efficacy constitute a primary concern. Gene-editing technologies like CRISPR-Cas9 can create consequences of off-target mutations, immune reactions and unintended genomic alterations. Likewise, RNA-based therapies and AAV-mediated gene delivery require extensive long-term monitoring to assess durability and potential adverse effects. Approval pathways for gene and cell-based treatments require rigorous long-term safety data and adaptive trial designs, prolonging regulatory timelines. For overcoming current challenges, advanced solutions are required, such as AI-driven platforms. This might permit us to translate these promising strategies into more personalized, accessible, and effective HF cares.
7. Conclusions
Many biomarkers have been studied in HF, but their clinical application is still far from being effective and largely insufficient, as most do not meet the criteria and therefore cannot yet be recommended. Considering the existing evidence, it is suggested to develop a multi-biomarker approach, given the complex pathophysiological processes underlying HF, as well as to develop promising targeted therapies oriented towards personalization. Here we provide a general overview of all emerging biomarkers and therapeutic targets, highlighting their advantages and limitations, as well as possible solutions to overcome them. We also emphasize that a meaningful collaboration between researchers and clinicians, as well as the will of policy makers, is crucial to validate such biomarkers and facilitate the application of innovative therapies, such as those extensively described and discussed in this review. The integration of advanced biomarkers, artificial intelligence, and multi-omics offers transformative, game-changing potential for HF management, paving the way for personalized and predictive cardiovascular care and significantly improving patient outcomes.
We also believe that in this appropriate framework, attention should also be paid to congenital cardiac malformations, such as single ventricle, which show a high risk of mortality in the first year of life in affected patients and of late complications [183]. Single ventricle reconstruction is the indicated therapy, but the ability to identify predictors of poor 3-year outcomes in patients with single ventricle physiology based on the type of initial shunt (Norwood procedure with Sano ventriculo-pulmonary shunt or modified Blalock subclavian pulmonary shunt) and the time of stage 2 palliation is not effective. For example, a 12-year longitudinal cohort study of patients with Fontan circulation (stage 3 procedure) found that the risk of death or cardiac transplantation was strongly associated with worse ventricular function [184]. Furthermore, no therapy has been shown to improve cardiac function in chronic volume or pressure overload, which tends to worsen the prognosis in patients with a single ventricle. However, early phase 1/2 clinical trials that administered cardiac progenitor cells intracoronarily have shown reliable and safe results in patients with single ventricle physiology [185,186,187]. Therefore, the administration of cardiac progenitor cells tends to improve ventricular function and reduce long-term complications in patients with a single ventricle [185]. Patients treated with cardiac progenitor cells and those with heart failure with reduced ejection fraction, but not with heart failure with intact ejection fraction, may experience a substantial improvement in clinical outcomes [185]. It would be worth testing this study in many patients.
Clonal hematopoiesis of indeterminate potential (CHIP), which has attracted considerable attention in HF research, because of its association with worse prognosis and adverse outcomes, is also worth considering as an excellent biomarker of HF. Accordingly, CHIP has also been observed to be associated with the various types of alterations of EFs and their etiologies. Precisely, some trials have reported that patients with ischemic HFrEF had a CHIP prevalence of about 18.5% [188]. Besides, they also had significantly negative long-term outcomes than patients without CHIP [188,189,190]. CHIP has also been associated with HF in patients with non-ischemic HFrEF. In patients without a known history of acute coronary atherosclerotic syndrome, CHIP has demonstrated to predict the HFrEF onset [191]. CHIP also has outcome’s significance in patients with both ischemic and non-ischemic HFrEF. In such patients, CHIP is related to augmented risk of HF-death and HF-hospitalization, as well as the development of cardiogenic shock [190,192]. CHIP has also been demonstrated to be an independent risk factor for incident HFpEF [193]. Patients who have HFpEF and CHIP have been shown to have a defective cardiac function and prognosis. Thus, CHIP is significant as a risk factor not only for hematological magnificence, but also as a novel cardiovascular risk factor particularly in patients with HF. However, its clinical efficacy is restricted until now. Adding it in combination of other prognostic and outcomes HF biomarkers above-described rapid advances in the clinical management of HF might be achieved and gene sequencing technology may be of help.
So, there is still a lot to study, validate and confirm, but we believe to be on the right track to revolutionize it.
Author Contributions
Conceptualization and design, C.R.B.; data curation, L.A., L.S., G.R., and A.S.; writing—original draft preparation, C.P. L.A. and C.R.B.; writing—review and editing, and C.R.B.; visualization, C.R.B.; supervision, C.R.B.; funding acquisition, C.R.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received external funding from Diego Gallo and Salvatore Pasta, from ASSOCIATE—Artificial intelligence powered support system for ascending aorta aneurysm—B53D23006200006—2022L7KK7L_002.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- van Riet EE, Hoes AW, Wagenaar KP, Limburg A, Landman MA, Rutten FH. , “Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review.,” Eur J Heart Fail., Vols. 18(3):242-52. , 2016. [CrossRef]
- Paulus WJ, Tschöpe C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, Marino P, Smiseth OA, De Keulenaer G, Leite-Moreira AF, Borbély A, Edes I, Handoko ML, Heymans S, Pezzali N, Pieske B, Dickstein K, Fraser AG, Brutsaert DL., “How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology.,” Eur Heart J, Vols. 28(20):2539-50. , 2007. [CrossRef]
- Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker-Smith CM, Beaton AZ, Boehme AK, Buxton AE, Commodore-Mensah Y, Elkind MSV, Evenson KR, Eze-Nliam C, Fugar S, Generoso G, Heard DG, Hiremath S, Ho JE, Kalani R, Kazi DS, Ko D, Levine DA, “Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association.,” Circulation , Vols. 147(8):e93-e621., 2023. [CrossRef]
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longeneck, “Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association,” Circulation, Vols. 141(9):e139-e596., 2020. [CrossRef]
- Martin SS, Aday AW, Allen NB, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker-Smith CM, Bansal N, Beaton AZ, Commodore-Mensah Y, Currie ME, Elkind MSV, Fan W, Generoso G, Gibbs BB, Heard DG, Hiremath S, Johansen MC, Kazi DS, Ko D, Leppert MH, Magnani, “2025 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association.,” Circulation, 2025.
- Siontis GC, Bhatt DL, Patel CJ., “Secular Trends in Prevalence of Heart Failure Diagnosis over 20 Years (from the US NHANES).,” Am J Cardiol., Vols. 172:161-164. , 2022. [CrossRef]
- Ho JE, Enserro D, Brouwers FP, Kizer JR, Shah SJ, Psaty BM, Bartz TM, Santhanakrishnan R, Lee DS, Chan C, Liu K, Blaha MJ, Hillege HL, van der Harst P, van Gilst WH, Kop WJ, Gansevoort RT, Vasan RS, Gardin JM, Levy D, Gottdiener JS, de Boer RA, Larson MG., “Predicting Heart Failure With Preserved and Reduced Ejection Fraction: The International Collaboration on Heart Failure Subtypes.,” Circ Heart Fail., 2016.
- Rasalam R, Sindone A, Deed G, Audehm RG, Atherton JJ. , “State of precision medicine for heart failure with preserved ejection fraction in a new therapeutic age.,” ESC Heart Fail, 2025. [CrossRef]
- Fernandes SL, Carvalho RR, Santos LG, Sá FM, Ruivo C, Mendes SL, Martins H, Morais JA., “Pathophysiology and Treatment of Heart Failure with Preserved Ejection Fraction: State of the Art and Prospects for the Future.,” Arq Bras Cardiol. , Vols. 114(1):120-129. , 2020.
- Achten A, Weerts J, van Koll J, Ghossein M, Mourmans SGJ, Aizpurua AB, van Stipdonk AMW, Vernooy K, Prinzen FW, Rocca HB, Knackstedt C, van Empel VPM, “Prevalence and prognostic value of ventricular conduction delay in heart failure with preserved ejection fraction.,” Int J Cardiol Heart Vasc., vol. 57:101622, 2025. [CrossRef]
- Dogheim GM, Amralla MT, Werida RH., “Role of neopterin as an inflammatory biomarker in congestive heart failure with insights on effect of drug therapies on its level.,” Inflammopharmacology., Vols. 30(5):1617-1622., 2022. [CrossRef]
- Vlachakis PK, Theofilis P, Kachrimanidis I, Giannakopoulos K, Drakopoulou M, Apostolos A, Kordalis A, Leontsinis I, Tsioufis K, Tousoulis D., “The Role of Inflammasomes in Heart Failure.,” Int J Mol Sci. , vol. 25(10):5372., 2024. [CrossRef]
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ,, “2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.,” J Am Coll Cardiol, Vols. 62(16):e147-239., 2013.
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson , “2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines.,” J Am Coll Cardiol., Vols. 79(17):1757-1780. , 2022. [CrossRef]
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA, Jaarsma T, Køber L, Lip GY, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Rønnevik PK, Rutten FH, Schwitter J, Seferovic P, Ste, “ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart,” Eur J Heart Fail. , Vols. 14(8):803-69., 2012.
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P;, “2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution,” Eur J Heart Fail., Vols. 18(8):891-975., 2016.
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo-Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray , “2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contributio,” Rev Esp Cardiol (Engl Ed)., vol. 75(6):523. , 2022. [CrossRef]
- Tsutsui H, Isobe M, Ito H, Ito H, Okumura K, Ono M, Kitakaze M, Kinugawa K, Kihara Y, Goto Y, Komuro I, Saiki Y, Saito Y, Sakata Y, Sato N, Sawa Y, Shiose A, Shimizu W, Shimokawa H, Seino Y, Node K, Higo T, Hirayama A, Makaya M, Masuyama T, Murohara T, Mo, “JCS 2017/JHFS 2017 Guideline on Diagnosis and Treatment of Acute and Chronic Heart Failure - Digest Version.,” Circ J., Vols. 83(10):2084-2184., 2019. [CrossRef]
- Tsutsui H, Ide T, Ito H, Kihara Y, Kinugawa K, Kinugawa S, Makaya M, Murohara T, Node K, Saito Y, Sakata Y, Shimizu W, Yamamoto K, Bando Y, Iwasaki YK, Kinugasa Y, Mizote I, Nakagawa H, Oishi S, Okada A, Tanaka A, Akasaka T, Ono M, Kimura T, Kosaka S, Kos, “JCS/JHFS 2021 Guideline Focused Update on Diagnosis and Treatment of Acute and Chronic Heart Failure.,” Circ J., Vols. 85(12):2252-2291., 2021. [CrossRef]
- Bozkurt B, Coats AJS, Tsutsui H, Abdelhamid CM, Adamopoulos S, Albert N, Anker SD, Atherton J, Böhm M, Butler J, Drazner MH, Michael Felker G, Filippatos G, Fiuzat M, Fonarow GC, Gomez-Mesa JE, Heidenreich P, Imamura T, Jankowska EA, Januzzi J, Khazanie P, “Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition o,” Eur J Heart Fail., Vols. 23(3):352-380., 2021.
- Blecker S, Katz SD, Horwitz LI, Kuperman G, Park H, Gold A, Sontag D. , “Comparison of Approaches for Heart Failure Case Identification From Electronic Health Record Data.,” JAMA Cardiol. , Vols. 1(9):1014-1020., 2016. [CrossRef]
- Volpe M, Carnovali M, Mastromarino V., “The natriuretic peptides system in the pathophysiology of heart failure: from molecular basis to treatment.,” Clin Sci (Lond), Vols. 130(2):57-77., 2016. [CrossRef]
- Maisel AS, Duran JM, Wettersten N., “Natriuretic Peptides in Heart Failure: Atrial and B-type Natriuretic Peptides.,” Heart Fail Clin., Vols. 14(1):13-25., 2018.
- Sudoh T, Maekawa K, Kojima M, Minamino N, Kangawa K, Matsuo H., “Cloning and sequence analysis of cDNA encoding a precursor for human brain natriuretic peptide.,” Biochem Biophys Res Commun, Vols. 159(3):1427-34., 1989. [CrossRef]
- McGrath MF, de Bold ML, de Bold AJ., “The endocrine function of the heart.,” Trends Endocrinol Metab., Vols. 16(10):469-77. , 2005.
- Vergani M, Cannistraci R, Perseghin G, Ciardullo S. , “The Role of Natriuretic Peptides in the Management of Heart Failure with a Focus on the Patient with Diabetes.,” J Clin Med., vol. 13(20):6225., 2024. [CrossRef]
- Yoshimura M, Yasue H, Morita E, Sakaino N, Jougasaki M, Kurose M, Mukoyama M, Saito Y, Nakao K, Imura H. , “ Hemodynamic, renal, and hormonal responses to brain natriuretic peptide infusion in patients with congestive heart failure,” Circulation. , Vols. 84(4):1581-8., 1991. [CrossRef]
- Nakagawa O, Ogawa Y, Itoh H, Suga S, Komatsu Y, Kishimoto I, Nishino K, Yoshimasa T, Nakao K, “Rapid transcriptional activation and early mRNA turnover of brain natriuretic peptide in cardiocyte hypertrophy. Evidence for brain natriuretic peptide as an “emergency” cardiac hormone against ventricular overload.,” J Clin Invest., Vols. 96(3):1280-7. , 1995.
- Smith MW, Espiner EA, Yandle TG, Charles CJ, Richards AM., “Delayed metabolism of human brain natriuretic peptide reflects resistance to neutral endopeptidase.,” J Endocrinol. , Vols. 167(2):239-46. , 2000. [CrossRef]
- Daniels LB, Maisel AS. , “Natriuretic peptides,” J Am Coll Cardiol, Vols. 50(25):2357-68. , 2007.
- Vickery S, Price CP, John RI, Abbas NA, Webb MC, Kempson ME, Lamb EJ., “B-type natriuretic peptide (BNP) and amino-terminal proBNP in patients with CKD: relationship to renal function and left ventricular hypertrophy.,” Am J Kidney Dis., Vols. 46(4):610-20., 2005. [CrossRef]
- Mueller C, McDonald K, de Boer RA, Maisel A, Cleland JGF, Kozhuharov N, Coats AJS, Metra M, Mebazaa A, Ruschitzka F, Lainscak M, Filippatos G, Seferovic PM, Meijers WC, Bayes-Genis A, Mueller T, Richards M, Januzzi JL Jr; Heart Failure Association of the , “Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations.,” Eur J Heart Fail., Vols. 21(6):715-731. , 2019. [CrossRef]
- Fang M, Wang D, Tang O, McEvoy JW, Echouffo-Tcheugui JB, Christenson RH, Selvin E., “Subclinical Cardiovascular Disease in US Adults With and Without Diabetes.,” J Am Heart Assoc., vol. 12(11):e029083., 2023. [CrossRef]
- Natriuretic Peptides Studies Collaboration, Willeit P, Kaptoge S, Welsh P, Butterworth AS, Chowdhury R, Spackman SA, Pennells L, Gao P, Burgess S, Freitag DF, Sweeting M, Wood AM, Cook NR, Judd S, Trompet S, Nambi V, Olsen MH, Everett BM, Kee F, Ärnlöv J,, “Natriuretic peptides and integrated risk assessment for cardiovascular disease: an individual-participant-data meta-analysis.,” Lancet Diabetes Endocrinol. , Vols. 4(10):840-9. , 2016. [CrossRef]
- Cleland JGF, Pfeffer MA, Clark AL, Januzzi JL, McMurray JJV, Mueller C, Pellicori P, Richards M, Teerlink JR, Zannad F, Bauersachs J, “The struggle towards a Universal Definition of Heart Failure-how to proceed?,” Eur Heart J., Vols. 42(24):2331-2343., 2021. [CrossRef]
- Pandey A, Berry JD, Drazner MH, Fang JC, Tang WHW, Grodin JL. , “Body Mass Index, Natriuretic Peptides, and Risk of Adverse Outcomes in Patients With Heart Failure and Preserved Ejection Fraction: Analysis From the TOPCAT Trial.,” J Am Heart Assoc. , vol. 7(21):e009664., 2018. [CrossRef]
- Ndumele CE, Matsushita K, Sang Y, Lazo M, Agarwal SK, Nambi V, Deswal A, Blumenthal RS, Ballantyne CM, Coresh J, Selvin E. , “N-Terminal Pro-Brain Natriuretic Peptide and Heart Failure Risk Among Individuals With and Without Obesity: The Atherosclerosis Risk in Communities (ARIC) Study.,” Circulation, Vols. 133(7):631-8., 2016.
- Obokata M, Reddy YNV, Pislaru SV, Melenovsky V, Borlaug BA. , “Evidence Supporting the Existence of a Distinct Obese Phenotype of Heart Failure With Preserved Ejection Fraction.,” Circulation, Vols. 136(1):6-19, 2017. [CrossRef]
- Welsh P, Campbell RT, Mooney L, Kimenai DM, Hayward C, Campbell A, Porteous D, Mills NL, Lang NN, Petrie MC, Januzzi JL, McMurray JJV, Sattar N. , “Reference Ranges for NT-proBNP (N-Terminal Pro-B-Type Natriuretic Peptide) and Risk Factors for Higher NT-proBNP Concentrations in a Large General Population Cohort.,” Circ Heart Fail., vol. 15(10):e009427., 2022. [CrossRef]
- Bayes-Genis A, Docherty KF, Petrie MC, Januzzi JL, Mueller C, Anderson L, Bozkurt B, Butler J, Chioncel O, Cleland JGF, Christodorescu R, Del Prato S, Gustafsson F, Lam CSP, Moura B, Pop-Busui R, Seferovic P, Volterrani M, Vaduganathan M, Metra M, Rosano , “Practical algorithms for early diagnosis of heart failure and heart stress using NT-proBNP: A clinical consensus statement from the Heart Failure Association of the ESC.,” Eur J Heart Fail., Vols. 25(11):1891-1898. , 2023. [CrossRef]
- Januzzi JL Jr, Chen-Tournoux AA, Christenson RH, Doros G, Hollander JE, Levy PD, Nagurney JT, Nowak RM, Pang PS, Patel D, Peacock WF, Rivers EJ, Walters EL, Gaggin HK;, “ ICON-RELOADED Investigators. N-Terminal Pro-B-Type Natriuretic Peptide in the Emergency Department: The ICON-RELOADED Study.,” J Am Coll Cardiol., Vols. 71(11):1191-1200, 2018.
- Ianos RD, Iancu M, Pop C, Lucaciu RL, Hangan AC, Rahaian R, Cozma A, Negrean V, Mercea D, Procopciuc LM. , “Predictive Value of NT-proBNP, FGF21, Galectin-3 and Copeptin in Advanced Heart Failure in Patients with Preserved and Mildly Reduced Ejection Fraction and Type 2 Diabetes Mellitus.,” Medicina (Kaunas)., vol. 60(11):1841., 2024. [CrossRef]
- Nguyen DV, Nguyen SV, Pham AL, Nguyen BT, Hoang SV., “Prognostic value of NT-proBNP in the new era of heart failure treatment.,” PLoS One., vol. 19(9):e0309948. , 2024.
- Ammar LA, Massoud GP, Chidiac C, Booz GW, Altara R, Zouein FA. , “BNP and NT-proBNP as prognostic biomarkers for the prediction of adverse outcomes in HFpEF patients: A systematic review and meta-analysis.,” Heart Fail Rev, Vols. 30(1):45-54, 2025. [CrossRef]
- Goetze JP, Bruneau BG, Ramos HR, Ogawa T, de Bold MK, de Bold AJ. , “Cardiac natriuretic peptides.,” Nat Rev Cardiol., Vols. 17(11):698-717., 2020 .
- Maisel A, Mueller C, Nowak R, Peacock WF, Landsberg JW, Ponikowski P, Mockel M, Hogan C, Wu AH, Richards M, Clopton P, Filippatos GS, Di Somma S, Anand I, Ng L, Daniels LB, Neath SX, Christenson R, Potocki M, McCord J, Terracciano G, Kremastinos D, Hartma, “Mid-region pro-hormone markers for diagnosis and prognosis in acute dyspnea: results from the BACH (Biomarkers in Acute Heart Failure) trial.,” J Am Coll Cardiol. , Vols. 55(19):2062-76. , 2010.
- Shah RV, Truong QA, Gaggin HK, Pfannkuche J, Hartmann O, Januzzi JL Jr., “Mid-regional pro-atrial natriuretic peptide and pro-adrenomedullin testing for the diagnostic and prognostic evaluation of patients with acute dyspnoea.,” Eur Heart J., Vols. 33(17):2197-205. , 2012. [CrossRef]
- Masson S, Latini R, Carbonieri E, Moretti L, Rossi MG, Ciricugno S, Milani V, Marchioli R, Struck J, Bergmann A, Maggioni AP, Tognoni G, Tavazzi L; GISSI-HF Investigators., “The predictive value of stable precursor fragments of vasoactive peptides in patients with chronic heart failure: data from the GISSI-heart failure (GISSI-HF) trial.,” Eur J Heart Fail., Vols. 12(4):338-47. , 2010. [CrossRef]
- Carella M, Magro D, Scola L, Pisano C, Guida E, Gervasi F, Giambanco C, Aronica TS, Frati G, Balistreri CR., “Corrigendum to “CAR, mGPS and hs-mGPS: Which of these is the best gero-biomarker for age-related diseases? And for what clinical application?” [Mech. Aging Dev. 220 (2024) 111952].,” Mech Ageing Dev. , vol. 221:111977. , 2024.
- Wettersten N., “Biomarkers in Acute Heart Failure: Diagnosis, Prognosis, and Treatment.,” Int J Heart Fail., Vols. 3(2):81-105. , 2021.
- Awwad A, Parashar Y, Bagchi S, Siddiqui SA, Ajari O, deFilippi C., “Preclinical screening for cardiovascular disease with high-sensitivity cardiac troponins: ready, set, go?,” Front Cardiovasc Med., vol. 11:1350573, 2024. [CrossRef]
- Netala VR, Hou T, Wang Y, Zhang Z, Teertam SK., “Cardiovascular Biomarkers: Tools for Precision Diagnosis and Prognosis.,” Int J Mol Sci., vol. 26(7):3218., 2025. [CrossRef]
- Breha A, Delcea C, Ivanescu AC, Dan GA. , “The Prognostic Value of Troponin Levels Adjusted for Renal Function in Heart Failure - A Systematic Review.,” Rom J Intern Med. , Vols. 63(2):107-126., 2025. [CrossRef]
- Lotfinaghsh A, Imam A, Pompian A, Stitziel NO, Javaheri A., “Clinical Insights from Proteomics in Heart Failure,” Curr Heart Fail Rep. , vol. 22(1):12., 2025. [CrossRef]
- Lee HK, McCarthy CP, Jaffe AS, Body R, Alotaibi A, Sandoval Y, Januzzi JL Jr. , “High-Sensitivity Cardiac Troponin Assays: From Implementation to Resource Utilization and Cost Effectiveness.,” J Appl Lab Med., Vols. 10(3):710-730. , 2025. [CrossRef]
- Raber I, McCarthy CP, Januzzi JL Jr., “A Test in Context: Interpretation of High-Sensitivity Cardiac Troponin Assays in Different Clinical Settings.,” J Am Coll Cardiol. , Vols. 77(10):1357-1367. , 2021. [CrossRef]
- Ibrahim M, Ahmad J, Abbas M, Zainullah, Umar Z, Nasir M, Zain K, Ahmad J, Arshad S, Bashir A, Ullah S, Ahmad Z, Safdar S., “The Role of N-terminal Pro-B-Type Natriuretic Peptide, Troponins, and D-dimer in Acute Cardio-Respiratory Syndromes: A Multi-specialty Systematic Review.,” Cureus., vol. 17(5):e84460., 2025.
- Luo Q, Zhang Q, Kong Y, Wang S, Wei Q., “ Heart failure, inflammation and exercise.,” Int J Biol Sci., Vols. 21(8):3324-3350. , 2025.
- Mylavarapu M, Kodali LSM, Vempati R, Nagarajan JS, Vyas A, Desai R., “Circulating microRNAs in predicting fibrosis in hypertrophic cardiomyopathy: A systematic review.,” World J Cardiol. , vol. 17(5):106123., 2025. [CrossRef]
- Roman-Pepine D, Serban AM, Capras RD, Cismaru CM, Filip AG., “A Comprehensive Review: Unraveling the Role of Inflammation in the Etiology of Heart Failure.,” Heart Fail Rev., 2025. [CrossRef]
- BaniHani HA, Khaled LH, Al Sharaa NM, Al Saleh RA, Bin Ghalaita AK, Bin Sulaiman AS, Holeihel A. , “Causes, Diagnosis, Treatment, and Prognosis of Cardiac Fibrosis: A Systematic Review.,” Cureus, vol. 17(3):e81264, 2025. [CrossRef]
- Shalmi TW, Jensen ASB, Goetze JP., “Cardiac natriuretic peptides.,” Adv Clin Chem, Vols. 122:115-139., 2024.
- Giovou AE, Gladka MM, Christoffels VM., “The Impact of Natriuretic Peptides on Heart Development, Homeostasis, and Disease.,” Cells., vol. 13(11):931. , 2024.
- Z. Q. K. Y. W. S. W. Q. Luo Q, “Heart failure, inflammation and exercise.,” Int J Biol Sci., Vols. 21(8):3324-3350., 2025.
- Cohn JN, Levine TB, Olivari MT, Garberg V, Lura D, Francis GS, Simon AB, Rector T. , “Plasma norepinephrine as a guide to prognosis in patients with chronic congestive heart failure.,” N Engl J Med., Vols. 311(13):819-23. , 1984. [CrossRef]
- Cabassi A, de Champlain J, Maggiore U, Parenti E, Coghi P, Vicini V, Tedeschi S, Cremaschi E, Binno S, Rocco R, Bonali S, Bianconcini M, Guerra C, Folesani G, Montanari A, Regolisti G, Fiaccadori E. , “Prealbumin improves death risk prediction of BNP-added Seattle Heart Failure Model: results from a pilot study in elderly chronic heart failure patients.,” Int J Cardiol., Vols. 168(4):3334-9., 2013. [CrossRef]
- Ceconi C, Ferrari R, Bachetti T, Opasich C, Volterrani M, Colombo B, Parrinello G, Corti A., “Chromogranin A in heart failure; a novel neurohumoral factor and a predictor for mortality.,” Eur Heart J, Vols. 23(12):967-74., 2022. [CrossRef]
- Røsjø H, Husberg C, Dahl MB, Stridsberg M, Sjaastad I, Finsen AV, Carlson CR, Oie E, Omland T, Christensen G., “Chromogranin B in heart failure: a putative cardiac biomarker expressed in the failing myocardium.,” Circ Heart Fail., Vols. 3(4):503-11, 2010.
- Azuma K, Nishimura K, Min KD, Takahashi K, Matsumoto Y, Eguchi A, Okuhara Y, Naito Y, Suna S, Asakura M, Ishihara M., “Plasma renin activity variation following admission predicts patient outcome in acute decompensated heart failure with reduced and mildly reduced ejection fraction.,” Heliyon., vol. 9(2):e13181., 2023. [CrossRef]
- Vaduganathan M, Cheema B, Cleveland E, Sankar K, Subacius H, Fonarow GC, Solomon SD, Lewis EF, Greene SJ, Maggioni AP, Böhm M, Zannad F, Butler J, Gheorghiade M. , “Plasma renin activity, response to aliskiren, and clinical outcomes in patients hospitalized for heart failure: the ASTRONAUT trial,” Eur J Heart Fail, Vols. 20(4):677-686., 2018. [CrossRef]
- Voors AA, Kremer D, Geven C, Ter Maaten JM, Struck J, Bergmann A, Pickkers P, Metra M, Mebazaa A, Düngen HD, Butler J., “Adrenomedullin in heart failure: pathophysiology and therapeutic application,” Eur J Heart Fail., Vols. 21(2):163-171. , 2019. [CrossRef]
- Richards AM, Doughty R, Nicholls MG, MacMahon S, Sharpe N, Murphy J, Espiner EA, Frampton C, Yandle TG; Australia-New Zealand Heart Failure Group., “Plasma N-terminal pro-brain natriuretic peptide and adrenomedullin: prognostic utility and prediction of benefit from carvedilol in chronic ischemic left ventricular dysfunction.,” J Am Coll Cardiol., Vols. 37(7):1781-7., 2001.
- von Haehling S, Filippatos GS, Papassotiriou J, Cicoira M, Jankowska EA, Doehner W, Rozentryt P, Vassanelli C, Struck J, Banasiak W, Ponikowski P, Kremastinos D, Bergmann A, Morgenthaler NG, Anker SD. , “Mid-regional pro-adrenomedullin as a novel predictor of mortality in patients with chronic heart failure.,” Eur J Heart Fail., Vols. 2(5):484-91., 2010. [CrossRef]
- Chatterjee K., “Neurohormonal activation in congestive heart failure and the role of vasopressin.,” Am J Cardiol. , Vols. 95(9A):8B-13B., 2005. [CrossRef]
- Maisel A, Xue Y, Shah K, Mueller C, Nowak R, Peacock WF, Ponikowski P, Mockel M, Hogan C, Wu AH, Richards M, Clopton P, Filippatos GS, Di Somma S, Anand IS, Ng L, Daniels LB, Neath SX, Christenson R, Potocki M, McCord J, Terracciano G, Kremastinos D, Hart, “Increased 90-day mortality in patients with acute heart failure with elevated copeptin: secondary results from the Biomarkers in Acute Heart Failure (BACH) study.,” Circ Heart Fail., Vols. 4(5):613-20., 2011.
- Zhong Y, Wang R, Yan L, Lin M, Liu X, You T., “Copeptin in heart failure: Review and meta-analysis.,” Clin Chim Acta, Vols. 475:36-43. , 2017. [CrossRef]
- Zhang CL, Xie S, Qiao X, An YM, Zhang Y, Li L, Guo XB, Zhang FC, Wu LL. , “Plasma endothelin-1-related peptides as the prognostic biomarkers for heart failure: A PRISMA-compliant meta-analysis.,” Medicine (Baltimore)., vol. 96(50):e9342. , 2017.
- Perez AL, Grodin JL, Wu Y, Hernandez AF, Butler J, Metra M, Felker GM, Voors AA, McMurray JJ, Armstrong PW, Starling RC, O’Connor CM, Tang WH., “Increased mortality with elevated plasma endothelin-1 in acute heart failure: an ASCEND-HF biomarker substudy.,” Eur J Heart Fail, Vols. 18(3):290-7. , 2016. [CrossRef]
- Guo S, Hu Y, Ling L, Yang Z, Wan L, Yang X, Lei M, Guo X, Ren Z. , “Molecular mechanisms and intervention approaches of heart failure (Review),” Int J Mol Med., vol. 56(2):125., 2025. [CrossRef]
- Malik MK, Kinno M, Liebo M, Yu MD, Syed M, “Evolving role of myocardial fibrosis in heart failure with preserved ejection fraction.,” Front Cardiovasc Med., vol. 12:1573346., 2025. [CrossRef]
- Ververeli CL, Dimitroglou Y, Soulaidopoulos S, Cholongitas E, Aggeli C, Tsioufis K, Tousoulis D., “Cardiac Remodeling and Arrhythmic Burden in Pre-Transplant Cirrhotic Patients: Pathophysiological Mechanisms and Management Strategies.,” Biomedicines., vol. 13(4):812. , 2025. [CrossRef]
- Vergaro G, Prud’homme M, Fazal L, Merval R, Passino C, Emdin M, Samuel JL, Cohen Solal A, Delcayre C., “Inhibition of Galectin-3 Pathway Prevents Isoproterenol-Induced Left Ventricular Dysfunction and Fibrosis in Mice.,” v, Vols. 67(3):606-12., 2016. [CrossRef]
- Meijers WC, Januzzi JL, deFilippi C, Adourian AS, Shah SJ, van Veldhuisen DJ, de Boer RA., “ Elevated plasma galectin-3 is associated with near-term rehospitalization in heart failure: a pooled analysis of 3 clinical trials.,” Am Heart J. , Vols. 167(6):853-60.e4., 2014. [CrossRef]
- Miró Ò, González de la Presa B, Herrero-Puente P, Fernández Bonifacio R, Möckel M, Mueller C, Casals G, Sandalinas S, Llorens P, Martín-Sánchez FJ, Jacob J, Bedini JL, Gil V., “The GALA study: relationship between galectin-3 serum levels and short- and long-term outcomes of patients with acute heart failure.,” Biomarkers, Vols. 22(8):731-739. , 2017. [CrossRef]
- Gehlken C, Suthahar N, Meijers WC, de Boer RA., “Galectin-3 in Heart Failure: An Update of the Last 3 Years.,” Heart Fail Clin., Vols. 14(1):75-92., 2018.
- Aimo A, Januzzi JL Jr, Bayes-Genis A, Vergaro G, Sciarrone P, Passino C, Emdin M., “Clinical and Prognostic Significance of sST2 in Heart Failure: JACC Review Topic of the Week.,” J Am Coll Cardiol., Vols. 74(17):2193-2203. , 2019.
- Emdin M, Aimo A, Vergaro G, Bayes-Genis A, Lupón J, Latini R, Meessen J, Anand IS, Cohn JN, Gravning J, Gullestad L, Broch K, Ueland T, Nymo SH, Brunner-La Rocca HP, de Boer RA, Gaggin HK, Ripoli A, Passino C, Januzzi JL Jr., “sST2 Predicts Outcome in Chronic Heart Failure Beyond NT-proBNP and High-Sensitivity Troponin T.,” J Am Coll Cardiol. , Vols. 72(19):2309-2320., 2018. [CrossRef]
- Richards AM., “ST2 and Prognosis in Chronic Heart Failure.,” J Am Coll Cardiol., Vols. 72(19):2321-2323., 2018. [CrossRef]
- Dalal JJ, Digrajkar A, Das B, Bansal M, Toomu A, Maisel AS. , “ST2 elevation in heart failure, predictive of a high early mortality.,” Indian Heart J., Vols. 70(6):822-827., 2018.
- Chen Y, Guan J, Qi C, Wu Y, Wang J, Zhao X, Li X, He C, Zhang J, Zhang Y. , “Association of point-of-care testing for sST2 with clinical outcomes in patients hospitalized with heart failure,” ESC Heart Fail. , Vols. 11(5):2857-2868. , 2024. [CrossRef]
- Chen Y, Zhao X, Liang L, Tian P, Feng J, Huang L, Huang B, Wu Y, Wang J, Guan J, Li X, Zhang J, Zhang Y., “sST2 and Big ET-1 as Alternatives of Multi-Biomarkers Strategies for Prognosis Evaluation in Patients Hospitalized with Heart Failure.,” Int J Gen Med., Vols. 16:5003-5016., 2023. [CrossRef]
- Aimo A, Januzzi JL Jr, Vergaro G, Richards AM, Lam CSP, Latini R, Anand IS, Cohn JN, Ueland T, Gullestad L, Aukrust P, Brunner-La Rocca HP, Bayes-Genis A, Lupón J, de Boer RA, Takeishi Y, Egstrup M, Gustafsson I, Gaggin HK, Eggers KM, Huber K, Gamble GD, , “Circulating levels and prognostic value of soluble ST2 in heart failure are less influenced by age than N-terminal pro-B-type natriuretic peptide and high-sensitivity troponin T,” Eur J Heart Fail., Vols. 22(11):2078-2088., 2020. [CrossRef]
- Aimo A, Maisel AS, Castiglione V, Emdin M., “sST2 for Outcome Prediction in Acute Heart Failure: Which Is the Best Cutoff?,” J Am Coll Cardiol., Vols. 74(3):478-479., 2019.
- Cotter G, Voors AA, Prescott MF, Felker GM, Filippatos G, Greenberg BH, Pang PS, Ponikowski P, Milo O, Hua TA, Qian M, Severin TM, Teerlink JR, Metra M, Davison BA., “Growth differentiation factor 15 (GDF-15) in patients admitted for acute heart failure: results from the RELAX-AHF study.,” Eur J Heart Fail., Vols. 17(11):1133-43., 2015. [CrossRef]
- Santema BT, Chan MMY, Tromp J, Dokter M, van der Wal HH, Emmens JE, Takens J, Samani NJ, Ng LL, Lang CC, van der Meer P, Ter Maaten JM, Damman K, Dickstein K, Cleland JG, Zannad F, Anker SD, Metra M, van der Harst P, de Boer RA, van Veldhuisen DJ, Rienstr, “The influence of atrial fibrillation on the levels of NT-proBNP versus GDF-15 in patients with heart failure.,” Clin Res Cardiol., Vols. 109(3):331-338. , 2020. [CrossRef]
- Zile MR, Desantis SM, Baicu CF, Stroud RE, Thompson SB, McClure CD, Mehurg SM, Spinale FG., “Plasma biomarkers that reflect determinants of matrix composition identify the presence of left ventricular hypertrophy and diastolic heart failure.,” Circ Heart Fail. , Vols. 4(3):246-56. , 2011. [CrossRef]
- Martin EM, Chang J, González A, Genovese F., “Circulating collagen type I fragments as specific biomarkers of cardiovascular outcome risk: Where are the opportunities?,” Matrix Biol., Vols. 137:19-32. , 2025. [CrossRef]
- Cunningham JW, Claggett BL, O’Meara E, Prescott MF, Pfeffer MA, Shah SJ, Redfield MM, Zannad F, Chiang LM, Rizkala AR, Shi VC, Lefkowitz MP, Rouleau J, McMurray JJV, Solomon SD, Zile MR., “Effect of Sacubitril/Valsartan on Biomarkers of Extracellular Matrix Regulation in Patients With HFpEF.,” J Am Coll Cardiol. , Vols. 76(5):503-514, 2020. [CrossRef]
- Sommakia S, Almaw NH, Lee SH, Ramadurai DKA, Taleb I, Kyriakopoulos CP, Stubben CJ, Ling J, Campbell RA, Alharethi RA, Caine WT, Navankasattusas S, Hoareau GL, Abraham AE, Fang JC, Selzman CH, Drakos SG, Chaudhuri D, “FGF21 (Fibroblast Growth Factor 21) Defines a Potential Cardiohepatic Signaling Circuit in End-Stage Heart Failure.,” Circ Heart Fail., vol. 15(3):e008910, 2022. [CrossRef]
- Fan L, Gu L, Yao Y, Ma G., “Elevated Serum Fibroblast Growth Factor 21 Is Relevant to Heart Failure Patients with Reduced Ejection Fraction.,” Comput Math Methods Med, vol. 2022:7138776., 2022. [CrossRef]
- Gu L, Jiang W, Zheng R, Yao Y, Ma G., “Fibroblast Growth Factor 21 Correlates with the Prognosis of Dilated Cardiomyopathy.,” Cardiology, Vols. 146(1):27-33., 2021. [CrossRef]
- Ghazal R, Wang M, Liu D, Tschumperlin DJ, Pereira NL. , “Cardiac Fibrosis in the Multi-Omics Era: Implications for Heart Failure.,” Circ Res, Vols. 136(7):773-802., 2025. [CrossRef]
- Soejima H, Irie A, Fukunaga T, Oe Y, Kojima S, Kaikita K, Kawano H, Sugiyama S, Yoshimura M, Kishikawa H, Nishimura Y, Ogawa H., “Osteopontin expression of circulating T cells and plasma osteopontin levels are increased in relation to severity of heart failure.,” Circ J., Vols. 71(12):1879-84. , 2007. [CrossRef]
- Li G, Xie J, Chen J, Li R, Wu H, Zhang X, Chen Q, Gu R, Xu B., “Syndecan-4 deficiency accelerates the transition from compensated hypertrophy to heart failure following pressure overload.,” Cardiovasc Pathol., Vols. 28:74-79, 2017. [CrossRef]
- Lim S, McMahon CD, Matthews KG, Devlin GP, Elston MS, Conaglen JV. , “Absence of Myostatin Improves Cardiac Function Following Myocardial Infarction.,” Heart Lung Circ., Vols. 27(6):693-701. , 2018. [CrossRef]
- Chen P, Liu Z, Luo Y, Chen L, Li S, Pan Y, Lei X, Wu D, Xu D., “Predictive value of serum myostatin for the severity and clinical outcome of heart failure.,” Eur J Intern Med. , Vols. 64:33-40., 2019. [CrossRef]
- Liu X, Xu X, Shang R, Chen Y. , “Asymmetric dimethylarginine (ADMA) as an important risk factor for the increased cardiovascular diseases and heart failure in chronic kidney disease.,” Nitric Oxide., Vols. 78:113-120., 2018. [CrossRef]
- Roumeliotis S, Veljkovic A, Georgianos PI, Lazarevic G, Perisic Z, Hadzi-Djokic J, Liakopoulos V, Kocic G., “Association between Biomarkers of Oxidative Stress and Inflammation with Cardiac Necrosis and Heart Failure in Non-ST Segment Elevation Myocardial Infarction Patients and Various Degrees of Kidney Function.,” Oxid Med Cell Longev., vol. 2021:3090120., 2021. [CrossRef]
- Liberale L, Duncker DJ, Hausenloy DJ, Kraler S, Bøtker HE, Podesser BK, Heusch G, Kleinbongard P., “Vascular (dys)function in the failing heart.,” Nat Rev Cardiol. , 2025. [CrossRef]
- Andreadou I, Ghigo A, Nikolaou PE, Swirski FK, Thackeray JT, Heusch G, Vilahur G., “Immunometabolism in heart failure.,” Nat Rev Cardiol., 2025.
- Nägele H, Bahlo M, Klapdor R, Schaeperkoetter D, Rödiger W. , “CA 125 and its relation to cardiac function.,” Am Heart J., Vols. 137(6):1044-9., 1999. [CrossRef]
- Núñez J, Miñana G, González M, Garcia-Ramón R, Sanchis J, Bodí V, Núñez E, Chorro FJ, Llàcer A, Miguel A. , “Antigen carbohydrate 125 in heart failure: not just a surrogate for serosal effusions?,” Int J Cardiol, Vols. 146(3):473-4. , 2011. [CrossRef]
- Marinescu MC, Oprea VD, Munteanu SN, Nechita A, Tutunaru D, Nechita LC, Romila A., “Carbohydrate Antigen 125 (CA 125): A Novel Biomarker in Acute Heart Failure.,” Diagnostics (Basel)., vol. 14(8):795., 2024. [CrossRef]
- Carella M, Magro D, Scola L, Pisano C, Guida E, Gervasi F, Giambanco C, Aronica TS, Frati G, Balistreri CR., “CAR, mGPS and hs-mGPS: What is among them the best gero-biomarker for age-related diseases? And for what clinical application?,” Mech Ageing Dev., vol. 220:111952., 2024. [CrossRef]
- Di Rosa M, Sabbatinelli J, Giuliani A, Carella M, Magro D, Biscetti L, Soraci L, Spannella F, Fedecostante M, Lenci F, Tortato E, Pimpini L, Burattini M, Cecchini S, Cherubini A, Bonfigli AR, Capalbo M, Procopio AD, Balistreri CR, Olivieri F. , “Inflammation scores based on C-reactive protein and albumin predict mortality in hospitalized older patients independent of the admission diagnosis.,” Immun Ageing., vol. 21(1):67., 2024.
- Kurniawan RB, Oktafia P, Saputra PBT, Purwati DD, Saputra ME, Maghfirah I, Faizah NN, Oktaviono YH, Alkaff FF. , “The roles of C-reactive protein-albumin ratio as a novel prognostic biomarker in heart failure patients: A systematic review.,” Curr Probl Cardiol., vol. 49(5):102475., 2024. [CrossRef]
- Bagheri A, Soltani S, Asoudeh F, Esmaillzadeh A., “Effects of omega-3 supplementation on serum albumin, pre-albumin and the CRP/albumin ratio in hospitalized patients: a systematic review and meta-analysis.,” Nutr Rev. , Vols. 81(3):237-251. , 2023. [CrossRef]
- do Nascimento DM, Bock PM, Nemetz B, Goldraich LA, Schaan BD., “Meta-Analysis of Physical Training on Natriuretic Peptides and Inflammation in Heart Failure.,” Am J Cardiol., Vols. 178:60-71. , 2022. [CrossRef]
- Rawat A, Vyas K., “ Neutrophil-to-Lymphocyte Ratio as a Predictor of Mortality and Clinical Outcomes in Heart Failure Patients.,” Cureus. , vol. 17(5):e83359., 2025. [CrossRef]
- Zhang X, Li D, Du Y., “Prognostic value of the neutrophil to lymphocyte ratio for cardiovascular diseases: research progress.,” Am J Transl Res. , Vols. 17(2):1170-1177. , 2025.
- Ang SP, Chia JE, Jaiswal V, Hanif M, Iglesias J., “Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Patients with Acute Decompensated Heart Failure: A Meta-Analysis.,” J Clin Med. , vol. 13(5):1212., 2024. [CrossRef]
- Vakhshoori M, Nemati S, Sabouhi S, Yavari B, Shakarami M, Bondariyan N, Emami SA, Shafie D., “Neutrophil to lymphocyte ratio (NLR) prognostic effects on heart failure; a systematic review and meta-analysis,” BMC Cardiovasc Disord., vol. 23(1):555. , 2023. [CrossRef]
- Zadorozny L, Du J, Supanekar N, Annamalai K, Yu Q, Wang M. , “Caveolin and oxidative stress in cardiac pathology.,” Front Physiol. , vol. 16:1550647., 2025. [CrossRef]
- Kittipibul V, Ambrosy AP, Greene SJ. , “Myeloperoxidase inhibition in the landscape of anti-inflammatory therapies for heart failure with preserved ejection fraction: the ENDEAVOR trial.,” Heart Fail Rev. , Vols. 30(4):735-738., 2025. [CrossRef]
- Yu F, Zhao H, Luo L, Wu W. , “Nicotinamide Adenine Dinucleotide Supplementation to Alleviate Heart Failure: A Mitochondrial Dysfunction Perspective.,” Nutrients., vol. 17(11):1855. , 2025. [CrossRef]
- Dan LX, Xie SP. , “Autophagy in cardiac pathophysiology: Navigating the complex roles and therapeutic potential in cardiac fibrosis.,” Life Sci., vol. 123761, 2025. [CrossRef]
- Sen I, Trzaskalski NA, Hsiao YT, Liu PP, Shimizu I, Derumeaux GA., “Aging at the Crossroads of Organ Interactions: Implications for the Heart.,” Circ Res., Vols. 136(11):1286-1305., 2025. [CrossRef]
- Xu J, Wang C, Xu Y, Wang H, Wang X. , “Network pharmacology and bioinformatics analysis reveals: NXC improves cardiac lymphangiogenesis through miR-126-3p/SPRED1 regulating the VEGF-C axis to ameliorate post-myocardial infarction heart failure.,” J Ethnopharmacol., vol. 350:119959., 2025. [CrossRef]
- Chen YL, Lin YN, Xu J, Qiu YX, Wu YH, Qian XG, Wu YQ, Wang ZN, Zhang WW, Li YC., “Macrophage-derived VEGF-C reduces cardiac inflammation and prevents heart dysfunction in CVB3-induced viral myocarditis via remodeling cardiac lymphatic vessels.,” Int Immunopharmacol., vol. 143(Pt 1):113377. , 2024. [CrossRef]
- Mericskay M, Zuurbier CJ, Heather LC, Karlstaedt A, Inserte J, Bertrand L, Kararigas G, Ruiz-Meana M, Maack C, Schiattarella GG. , “Cardiac intermediary metabolism in heart failure: substrate use, signalling roles and therapeutic targets.,” Nat Rev Cardiol., 2025.
- Auerbach M, DeLoughery TG, Tirnauer JS., “Iron Deficiency in Adults: A Review.,” JAMA, Vols. 333(20):1813-1823., 2025.
- Anghel L, Dinu C, Patraș D, Ciubară A, Chiscop I., “Iron Deficiency Treatment in Heart Failure-Challenges and Therapeutic Solutions.,” J Clin Med., vol. 14(9):2934., 2025. [CrossRef]
- Maidana D, Arroyo-Álvarez A, Barreres-Martín G, Arenas-Loriente A, Cepas-Guillen P, Brigolin Garofo RT, Caravaca-Pérez P, Bonanad C. , “Targeting Inflammation and Iron Deficiency in Heart Failure: A Focus on Older Adults.,” Biomedicines., vol. 13(2):462., 2025. [CrossRef]
- Maack C., “Metabolic alterations in heart failure.,” Nat Rev Cardiol., 2025.
- Ibrahim R, Takamatsu C, Alabagi A, Pham HN, Thajudeen B, Demirjian S, Tang WHW, William P, “Kidney Replacement Therapies in Advanced Heart Failure: Timing, Modalities and Clinical Considerations.,” J Card Fail. , Vols. 31(5):833-844. , 2025.
- Giangregorio F, Mosconi E, Debellis MG, Provini S, Esposito C, Garolfi M, Oraka S, Kaloudi O, Mustafazade G, Marín-Baselga R, Tung-Chen Y. , “A Systematic Review of Metabolic Syndrome: Key Correlated Pathologies and Non-Invasive Diagnostic Approaches.,” J Clin Med. , vol. 13(19):5880., 2024. [CrossRef]
- Bansal B, Lajeunesse-Trempe F, Keshvani N, Lavie CJ, Pandey A., “Impact of Metabolic Dysfunction-associated Steatotic Liver Disease on Cardiovascular Structure, Function, and the Risk of Heart Failure.,” Can J Cardiol., 2025.
- Bernhard J, Galli L, Speidl WS, Krychtiuk KA., “Cardiovascular Risk Reduction in Metabolic Dysfunction-Associated Steatotic Liver Disease and Metabolic Dysfunction-Associated Steatohepatitis.,” Curr Cardiol Rep. , vol. 27(1):28. , 2025. [CrossRef]
- Savarese G, von Haehling S, Butler J, Cleland JGF, Ponikowski P, Anker SD., “Iron deficiency and cardiovascular disease.,” Eur Heart J., Vols. 44(1):14-27, 2023. [CrossRef]
- Ghafourian K, Shapiro JS, Goodman L, Ardehali H., “Iron and Heart Failure: Diagnosis, Therapies, and Future Directions.,” JACC Basic Transl Sci., Vols. 5(3):300-313. , 2020.
- McDonagh T, Damy T, Doehner W, Lam CSP, Sindone A, van der Meer P, Cohen-Solal A, Kindermann I, Manito N, Pfister O, Pohjantähti-Maaroos H, Taylor J, Comin-Colet J. , “Screening, diagnosis and treatment of iron deficiency in chronic heart failure: putting the 2016 European Society of Cardiology heart failure guidelines into clinical practice.,” Eur J Heart Fail., Vols. 20(12):1664-1672. , 2018. [CrossRef]
- Lam CSP, Doehner W, Comin-Colet J; IRON CORE Group, “ Iron deficiency in chronic heart failure: case-based practical guidance.,” ESC Heart Fail. , Vols. 5(5):764-771., 2018. [CrossRef]
- Grote Beverborg N, Klip IT, Meijers WC, Voors AA, Vegter EL, van der Wal HH, Swinkels DW, van Pelt J, Mulder AB, Bulstra SK, Vellenga E, Mariani MA, de Boer RA, van Veldhuisen DJ, van der Meer P., “Definition of Iron Deficiency Based on the Gold Standard of Bone Marrow Iron Staining in Heart Failure Patients.,” Circ Heart Fail., vol. 11(2):e004519., 2018. [CrossRef]
- Gan S, Azzo JD, Zhao L, Pourmussa B, Dib MJ, Salman O, Erten O, Ebert C, Richards AM, Javaheri A, Mann DL, Rietzschel E, Zamani P, van Empel V, Cappola TP, Chirinos JA. , “Transferrin Saturation, Serum Iron, and Ferritin in Heart Failure: Prognostic Significance and Proteomic Associations.,” Circ Heart Fail., vol. 18(2):e011728. , 2025. [CrossRef]
- Graham FJ, Guha K, Cleland JG, Kalra PR., “Treating iron deficiency in patients with heart failure: what, why, when, how, where and who.,” Heart. , Vols. 110(20):1201-1207. , 2024.
- von Haehling S, Ebner N, Evertz R, Ponikowski P, Anker SD., “Iron Deficiency in Heart Failure: An Overview.,” JACC Heart Fail. , Vols. 7(1):36-46. , 2019.
- Dinatolo E, Dasseni N, Metra M, Lombardi C, von Haehling S., “Iron deficiency in heart failure.,” J Cardiovasc Med (Hagerstown). , Vols. 19(12):706-716., 2018.
- Gamage M, Manouras A, Hage C, Savarese G, Ljung K, Melin M., “Implementation of guidelines for intravenous iron therapy in heart failure patients.,” ESC Heart Fail. , 2025. [CrossRef]
- Sindone A, Doehner W, Comin-Colet J. , “Systematic review and meta-analysis of intravenous iron-carbohydrate complexes in HFrEF patients with iron deficiency.,” ESC Heart Fail., Vols. 10(1):44-56., 2023. [CrossRef]
- Pezel T, Audureau E, Mansourati J, Baudry G, Ben Driss A, Durup F, Fertin M, Godreuil C, Jeanneteau J, Kloeckner M, Koukoui F, Kesri-Tartière L, Laperche T, Roubille F, Cohen-Solal A, Damy T. , “Diagnosis and Treatment of Iron Deficiency in Heart Failure: OFICSel study by the French Heart Failure Working Group.,” ESC Heart Fail., Vols. 8(2):1509-1521., 2021. [CrossRef]
- Lee S, Houstis NE, Cunningham TF, Brooks LC, Chen K, Slocum CL, Ostrom K, Birchenough C, Moore E, Tattersfield H, Sigurslid H, Guo Y, Landsteiner I, Rouvina JN, Lewis GD, Malhotra R., “Transferrin Saturation Is a Better Predictor Than Ferritin of Metabolic and Hemodynamic Exercise Responses in HFpEF.,” JACC Heart Fail. , vol. 13(8):102478., 2025. [CrossRef]
- Aboelsaad IAF, Claggett BL, Arthur V, Dorbala P, Matsushita K, Lutsey PL, Yu B, Lennep BW, Ndumele CE, Farag YMK, Shah AM, Buckley LF., “Hepcidin, Incident Heart Failure and Cardiac Dysfunction in Older Adults: the ARIC Study.,” Eur J Prev Cardiol., vol. zwaf018. , 2025. [CrossRef]
- Mantovani A, Busti F, Borella N, Scoccia E, Pecoraro B, Sani E, Morandin R, Csermely A, Piasentin D, Grespan E, Castagna A, Bilson J, Byrne CD, Valenti L, Girelli D, Targher G. , “Elevated plasma hepcidin concentrations are associated with an increased risk of mortality and nonfatal cardiovascular events in patients with type 2 diabetes: a prospective study.,” Cardiovasc Diabetol., vol. 23(1):305., 2024. [CrossRef]
- Valenti AC, Vitolo M, Imberti JF, Malavasi VL, Boriani G., “Red Cell Distribution Width: A Routinely Available Biomarker with Important Clinical Implications in Patients with Atrial Fibrillation.,” Curr Pharm Des., Vols. 27(37):3901-3912., 2021. [CrossRef]
- García-Escobar A, Lázaro-García R, Goicolea-Ruigómez J, González-Casal D, Fontenla-Cerezuela A, Soto N, González-Panizo J, Datino T, Pizarro G, Moreno R, Cabrera JÁ. , “Red Blood Cell Distribution Width is a Biomarker of Red Cell Dysfunction Associated with High Systemic Inflammation and a Prognostic Marker in Heart Failure and Cardiovascular Disease: A Potential Predictor of Atrial Fibrillation Recurrence.,” High Blood Press Cardiovasc Prev, Vols. 31(5):437-449. , 2024. [CrossRef]
- Masini G, Graham FJ, Pellicori P, Cleland JGF, Cuthbert JJ, Kazmi S, Inciardi RM, Clark AL., “Criteria for Iron Deficiency in Patients With Heart Failure.,” J Am Coll Cardiol., Vols. 79(4):341-351. , 2022. [CrossRef]
- Pinsino A, Carey MR, Husain S, Mohan S, Radhakrishnan J, Jennings DL, Nguonly AS, Ladanyi A, Braghieri L, Takeda K, Faillace RT, Sayer GT, Uriel N, Colombo PC, Yuzefpolskaya M. , “The Difference Between Cystatin C- and Creatinine-Based Estimated GFR in Heart Failure With Reduced Ejection Fraction: Insights From PARADIGM-HF.,” Am J Kidney Dis., Vols. 82(5):521-533., 2023. [CrossRef]
- Łagosz P, Biegus J, Urban S, Zymliński R. , “Renal Assessment in Acute Cardiorenal Syndrome.,” Biomolecules. , vol. 13(2):239. , 2023. [CrossRef]
- Theodorakis N, Nikolaou M., “Integrated Management of Cardiovascular-Renal-Hepatic-Metabolic Syndrome: Expanding Roles of SGLT2is, GLP-1RAs, and GIP/GLP-1RAs.,” Biomedicines. , vol. 13(1):135., 2025.
- Cheng Z, Lin X, Xu C, Zhang Z, Lin N, Cai K., “Prognostic Value of Serum Neutrophil Gelatinase-Associated Lipocalin in Acute Heart Failure: A Meta-Analysis.,” Rev Cardiovasc Med. , vol. 25(12):428., 2024. [CrossRef]
- Theodorakis N, Nikolaou M., “From Cardiovascular-Kidney-Metabolic Syndrome to Cardiovascular-Renal-Hepatic-Metabolic Syndrome: Proposing an Expanded Framework.,” Biomolecules., vol. 15(2):213., 2025. [CrossRef]
- Bastos JM, Colaço B, Baptista R, Gavina C, Vitorino R., “Innovations in heart failure management: The role of cutting-edge biomarkers and multi-omics integration,” J Mol Cell Cardiol Plus., vol. 11:100290., 2025. [CrossRef]
- Massaccesi L, Balistreri CR. , “Biomarkers of Oxidative Stress in Acute and Chronic Diseases.,” Antioxidants (Basel)., vol. 11(9):1766., 2022. [CrossRef]
- Carella M, Porreca A, Piazza C, Gervasi F, Magro D, Venezia M, Verso RL, Vitale G, Agnello AG, Scola L, Aronica TS, Balistreri CR. , “Could the Combination of eGFR and mGPS Facilitate the Differential Diagnosis of Age-Related Renal Decline from Diseases? A Large Study on the Population of Western Sicily.,” J Clin Med., vol. 12(23):7352., 2023. [CrossRef]
- Sarhene M, Wang Y, Wei J, Huang Y, Li M, Li L, Acheampong E, Zhengcan Z, Xiaoyan Q, Yunsheng X, Jingyuan M, Xiumei G, Guanwei F., “Biomarkers in heart failure: the past, current and future.,” Heart Fail Rev, Vols. 24(6):867-903., 2019.
- Shah AM, Claggett B, Sweitzer NK, Shah SJ, Anand IS, O’Meara E, Desai AS, Heitner JF, Li G, Fang J, Rouleau J, Zile MR, Markov V, Ryabov V, Reis G, Assmann SF, McKinlay SM, Pitt B, Pfeffer MA, Solomon SD., “Cardiac structure and function and prognosis in heart failure with preserved ejection fraction: findings from the echocardiographic study of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) Trial.,” Circ Heart Fail. , Vols. 7(5):740-51., 2014.
- Abreu J, Seringa J, Magalhaes T., “Machine learning methods, applications and economic analysis to predict heart failure hospitalisation risk: a scoping review.,” BMJ Open, vol. 15(6):e093495., 2025. [CrossRef]
- Sharda M, Sharma S, Raikar S, Verhagen N, Wagle J, Mathur R, Gowda S, Kommu S, Prasad R, Bhandari S, Jha P., “The Role of Machine Learning in Predicting Hospital Readmissions Among General Internal Medicine Patients: A Systematic Review.,” Cureus., vol. 17(5):e84761., 2025. [CrossRef]
- Li X, Loscalzo J, Mahmud AKMF, Aly DM, Rzhetsky A, Zitnik M, Benson M., “Digital twins as global learning health and disease models for preventive and personalized medicine.,” Genome Med. , vol. 17(1):11., 2025. [CrossRef]
- Palaparthi EC, Aditya Reddy P, Padala T, Sri Venkata Mahi Karthika K, Paka R, Ami Reddy V, Ayub S, Khyati Sri V, Rebanth Nandan V, Patnaik PK, Medabala T, Sayana SB. , “The Rise of Personalized Medicine in Heart Failure Management: A Narrative Review.,” Cureus., vol. 17(5):e83731., 2025. [CrossRef]
- Palaparthi EC, Padala T, Singamaneni R, Manaswini R, Kantula A, Aditya Reddy P, Chandini P, Sathwika Eliana A, Siri Samhita P, Patnaik PK., “Emerging Therapeutic Strategies for Heart Failure: A Comprehensive Review of Novel Pharmacological and Molecular Targets.,” Cureus., vol. 17(4):e81573., 2025. [CrossRef]
- Magro D, Venezia M, Balistreri CR, “The omics technologies and liquid biopsies: Advantages, limitations, applications, Medicine in Omics,,” Medicine in Omics, vol. 11, 2024.
- Rai H, Colleran R, Cassese S, Joner M, Kastrati A, Byrne RA. , “Association of interleukin 6 -174 G/C polymorphism with coronary artery disease and circulating IL-6 levels: a systematic review and meta-analysis.,” Inflamm Res., Vols. 70(10-12):1075-1087., 2021. [CrossRef]
- McCrink KA, Lymperopoulos A, “β1-adrenoceptor Arg389Gly polymorphism and heart disease: marching toward clinical practice integration.,” Pharmacogenomics., Vols. 16(10):1035-8. , 2015. [CrossRef]
- Ha SK. , “ACE insertion/deletion polymorphism and diabetic nephropathy: clinical implications of genetic information.,” J Diabetes Res., vol. 2014:846068., 2024. [CrossRef]
- Lee DSM, Cardone KM, Zhang DY, Tsao NL, Abramowitz S, Sharma P, DePaolo JS, Conery M, Aragam KG, Biddinger K, Dilitikas O, Hoffman-Andrews L, Judy RL, Khan A, Kullo IJ, Puckelwartz MJ, Reza N, Satterfield BA, Singhal P; Penn Medicine Biobank; Arany Z, Cap, “Common-variant and rare-variant genetic architecture of heart failure across the allele-frequency spectrum,” Nat Genet., Vols. 57(4):829-838. , 2025. [CrossRef]
- Ionescu RF, Cretoiu SM., “MicroRNAs as monitoring markers for right-sided heart failure and congestive hepatopathy.,” J Med Life, Vols. 14(2):142-147., 2021. [CrossRef]
- Huang XH, Li JL, Li XY, Wang SX, Jiao ZH, Li SQ, Liu J, Ding J., “miR-208a in Cardiac Hypertrophy and Remodeling.,” Front Cardiovasc Med., vol. 8:773314., 2021. [CrossRef]
- Asjad E, Dobrzynski H. , “MicroRNAs: Midfielders of Cardiac Health, Disease and Treatment.,” Int J Mol Sci., vol. 24(22):16207., 2023.
- Tijsen AJ, Pinto YM, Creemers EE., “Circulating microRNAs as diagnostic biomarkers for cardiovascular diseases,” Am J Physiol Heart Circ Physiol., Vols. 303(9):H1085-95., 2012. [CrossRef]
- Colpaert RMW, Calore M., “MicroRNAs in Cardiac Diseases.,” Cells, vol. 8(7):737., 2019.
- Moradi A, Khoshniyat S, Nzeako T, Khazeei Tabari MA, Olanisa OO, Tabbaa K, Alkowati H, Askarianfard M, Daoud D, Oyesanmi O, Rodriguez A, Lin Y. , “The Future of Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR)-Cas9 Gene Therapy in Cardiomyopathies: A Review of Its Therapeutic Potential and Emerging Applications.,” Cureus., vol. 17(2):e79372., 2025. [CrossRef]
- Newburger JW, Sleeper LA, Frommelt PC, Pearson GD, Mahle WT, Chen S, Dunbar-Masterson C, Mital S, Williams IA, Ghanayem NS, Goldberg CS, Jacobs JP, Krawczeski CD, Lewis AB, Pasquali SK, Pizarro C, Gruber PJ, Atz AM, Khaikin S, Gaynor JW, Ohye RG; Pediatri, “Transplantation-free survival and interventions at 3 years in the single ventricle reconstruction trial.,” Circulation, Vols. 129(20):2013-20., 2014. [CrossRef]
- Atz AM, Zak V, Mahony L, Uzark K, D’agincourt N, Goldberg DJ, Williams RV, Breitbart RE, Colan SD, Burns KM, Margossian R, Henderson HT, Korsin R, Marino BS, Daniels K, McCrindle BW; Pediatric Heart Network Investigators. , “Longitudinal Outcomes of Patients With Single Ventricle After the Fontan Procedure.,” J Am Coll Cardiol. , Vols. 69(22):2735-2744. , 2017. [CrossRef]
- Ishigami S, Ohtsuki S, Eitoku T, Ousaka D, Kondo M, Kurita Y, Hirai K, Fukushima Y, Baba K, Goto T, Horio N, Kobayashi J, Kuroko Y, Kotani Y, Arai S, Iwasaki T, Sato S, Kasahara S, Sano S, Oh H., “Intracoronary Cardiac Progenitor Cells in Single Ventricle Physiology: The PERSEUS (Cardiac Progenitor Cell Infusion to Treat Univentricular Heart Disease) Randomized Phase 2 Trial.,” Circ Res. , Vols. 120(7):1162-1173. , 2017.
- Balistreri CR., “In reviewing the emerging biomarkers of human inflammatory bowel disease (IBD): Endothelial progenitor cells (EPC) and their vesicles as potential biomarkers of cardiovascular manifestations and targets for personalized treatments.,” Mech Ageing Dev. , vol. 222:112006. , 2024. [CrossRef]
- Balistreri CR, Buffa S, Pisano C, Lio D, Ruvolo G, Mazzesi G. , “Are Endothelial Progenitor Cells the Real Solution for Cardiovascular Diseases? Focus on Controversies and Perspectives.,” Biomed Res Int., vol. 2015:835934. , 2015. [CrossRef]
- Dorsheimer L, Assmus B, Rasper T, Ortmann CA, Ecke A, Abou-El-Ardat K, Schmid T, Brüne B, Wagner S, Serve H, Hoffmann J, Seeger F, Dimmeler S, Zeiher AM, Rieger MA., “Association of Mutations Contributing to Clonal Hematopoiesis With Prognosis in Chronic Ischemic Heart Failure.,” JAMA Cardiol., Vols. 4(1):25-33., 2019. [CrossRef]
- Pascual-Figal DA, Bayes-Genis A, Díez-Díez M, Hernández-Vicente Á, Vázquez-Andrés D, de la Barrera J, Vazquez E, Quintas A, Zuriaga MA, Asensio-López MC, Dopazo A, Sánchez-Cabo F, Fuster JJ. , “Clonal Hematopoiesis and Risk of Progression of Heart Failure With Reduced Left Ventricular Ejection Fraction.,” J Am Coll Cardiol. , Vols. 77(14):1747-1759., 2021. [CrossRef]
- Assmus B, Cremer S, Kirschbaum K, Culmann D, Kiefer K, Dorsheimer L, Rasper T, Abou-El-Ardat K, Herrmann E, Berkowitsch A, Hoffmann J, Seeger F, Mas-Peiro S, Rieger MA, Dimmeler S, Zeiher AM., “Clonal haematopoiesis in chronic ischaemic heart failure: prognostic role of clone size for DNMT3A- and TET2-driver gene mutations.,” Eur Heart J., Vols. 42(3):257-265., 2021. [CrossRef]
- Yu B, Roberts MB, Raffield LM, Zekavat SM, Nguyen NQH, Biggs ML, Brown MR, Griffin G, Desai P, Correa A, Morrison AC, Shah AM, Niroula A, Uddin MM, Honigberg MC, Ebert BL, Psaty BM, Whitsel EA, Manson JE, Kooperberg C, Bick AG, Ballantyne CM, Reiner AP, N, “Supplemental Association of Clonal Hematopoiesis With Incident Heart Failure.,” J Am Coll Cardiol. , Vols. 78(1):42-52., 2021.
- Scolari FL, Abelson S, Brahmbhatt DH, Medeiros JJF, Fan CS, Fung NL, Mihajlovic V, Anker MS, Otsuki M, Lawler PR, Ross HJ, Luk AC, Anker S, Dick JE, Billia F., “Clonal haematopoiesis is associated with higher mortality in patients with cardiogenic shock.,” Eur J Heart Fail., Vols. 24(9):1573-1582., 2022. [CrossRef]
- Schuermans A, Honigberg MC, Raffield LM, Yu B, Roberts MB, Kooperberg C, Desai P, Carson AP, Shah AM, Ballantyne CM, Bick AG, Natarajan P, Manson JE, Whitsel EA, Eaton CB, Reiner AP. , “Clonal Hematopoiesis and Incident Heart Failure With Preserved Ejection Fraction.,” JAMA Netw Open., vol. 7(1):e2353244. , 2024. [CrossRef]
Figure 1.
The main recognized risk factors of HF.
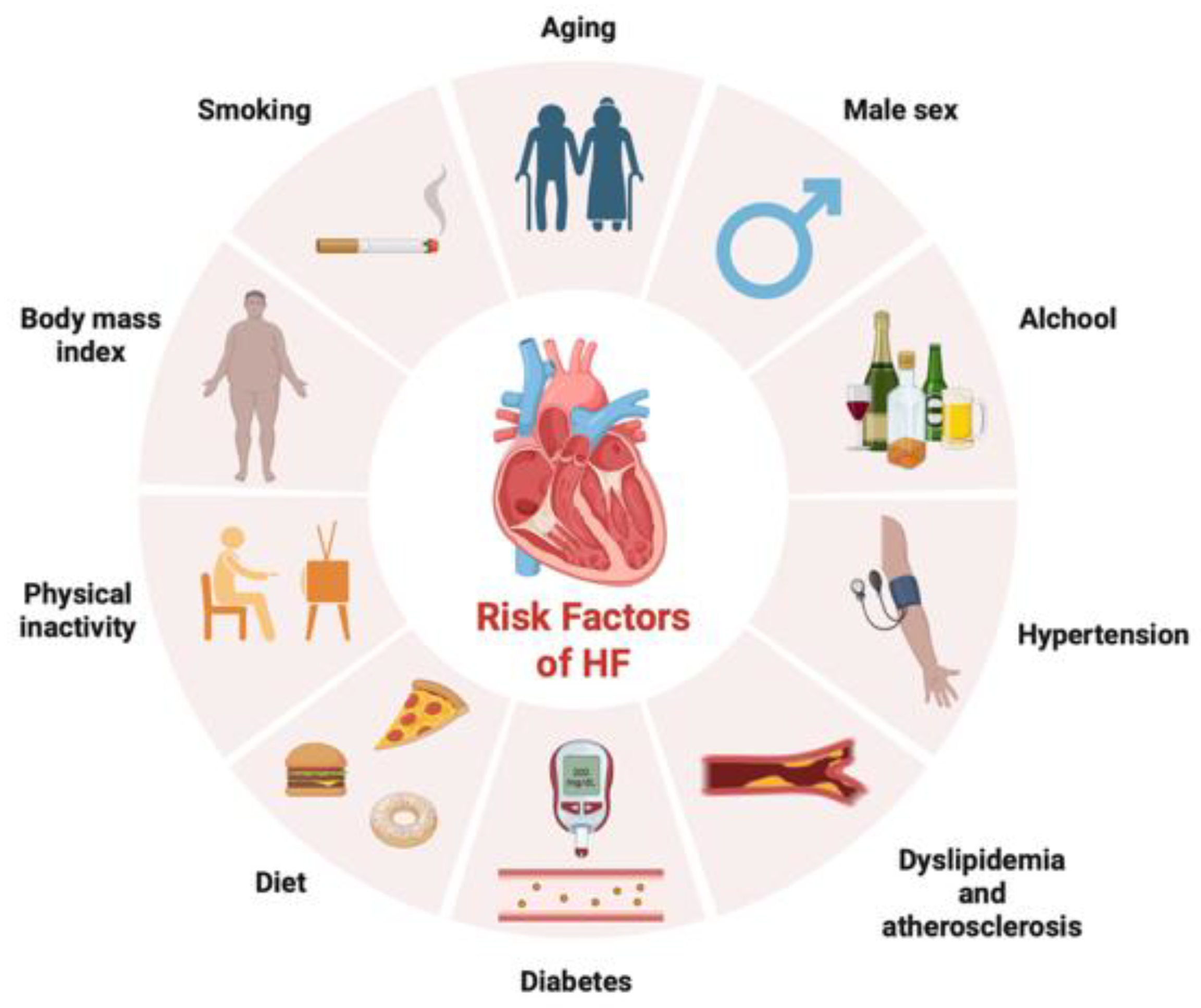
Figure 2.
The pathophysiological alterations in HF.
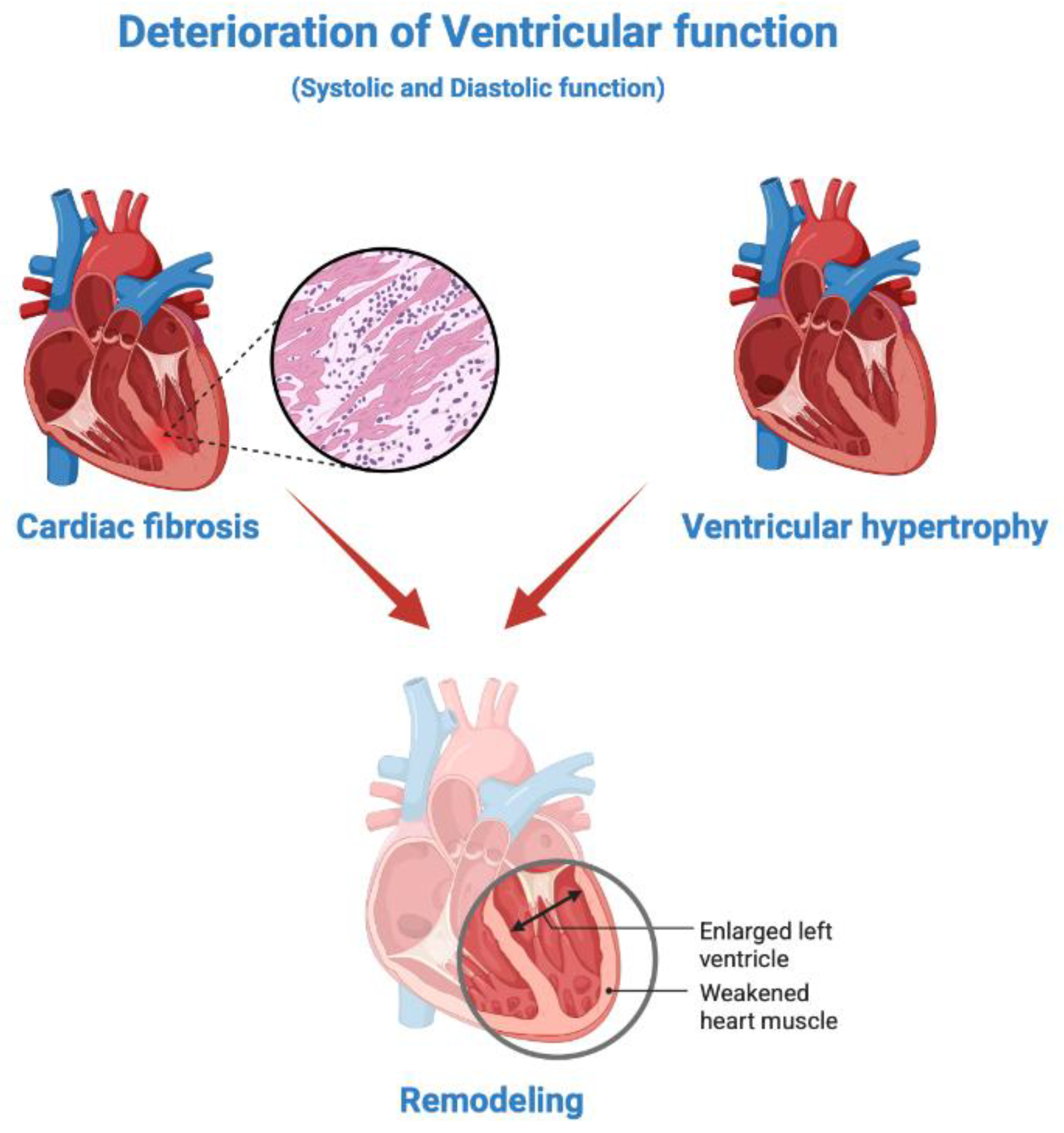
Figure 3.
NT-proBNP synthesis.
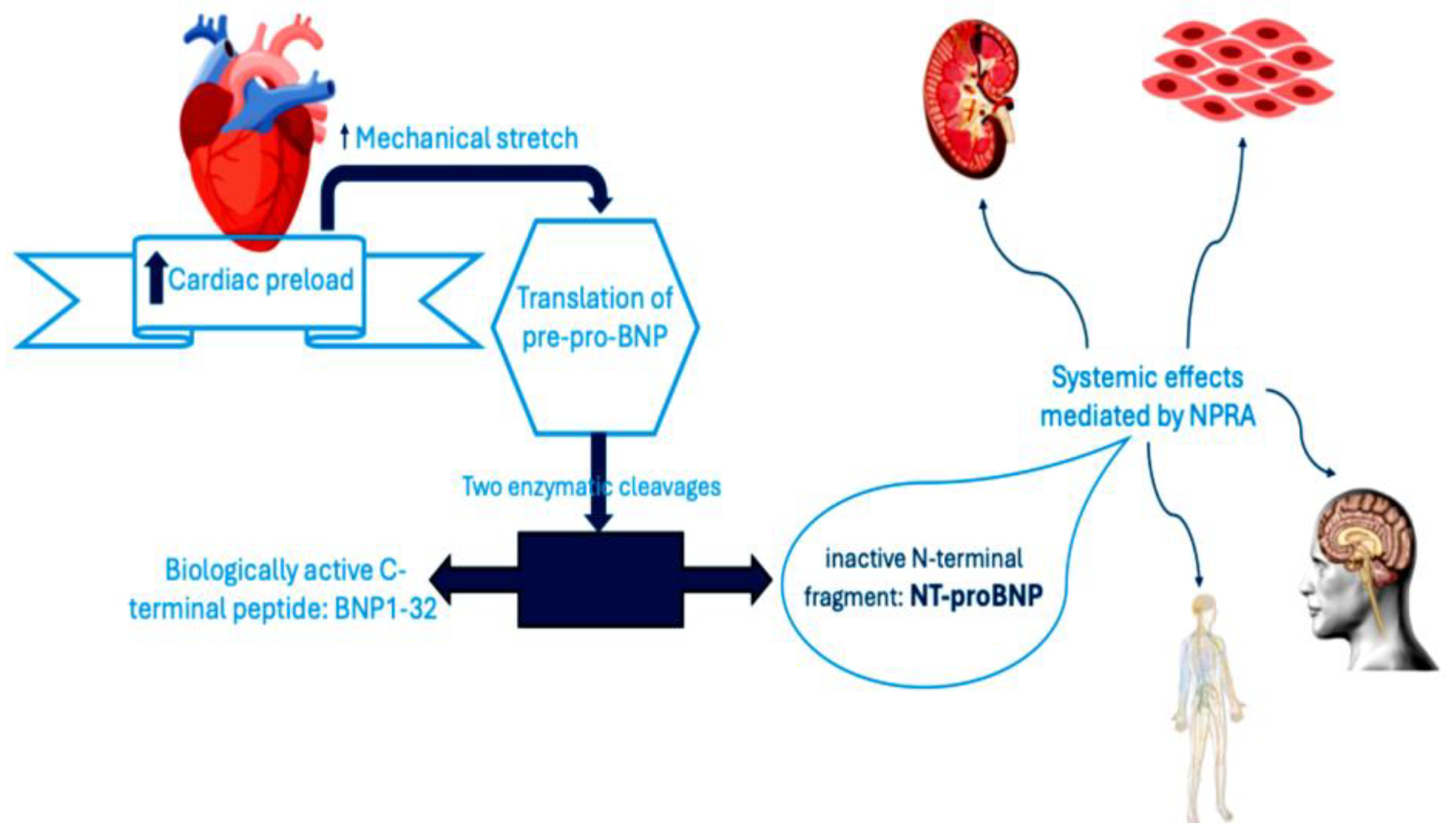
Figure 4.
ESC Guidelines [17].
Figure 4.
ESC Guidelines [17].
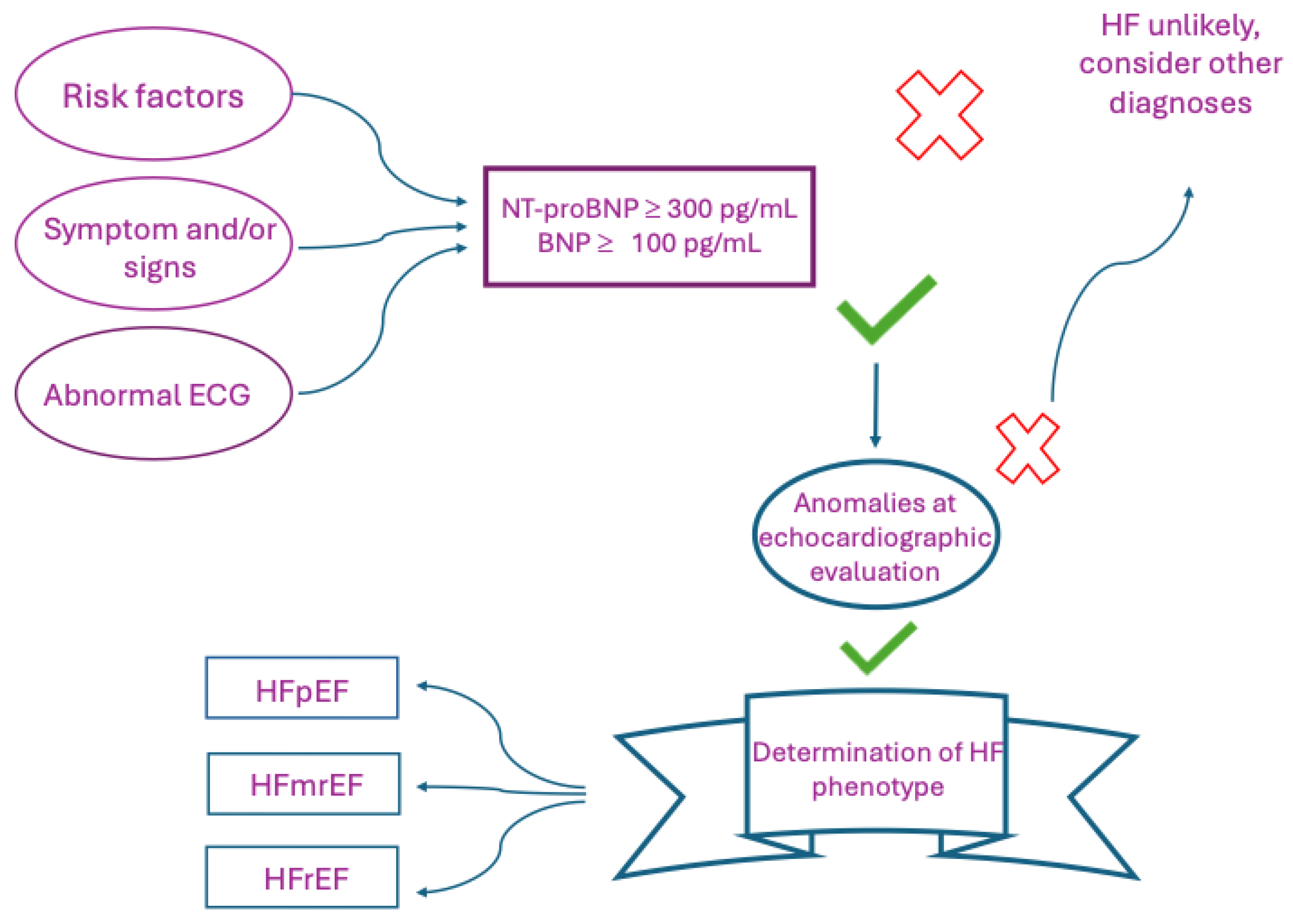

Table 1.
Different definitions proposed in the last 10 years.
| Guideline | Definition criterion | Definition |
|---|---|---|
| 2013 ACCF/AHA [13] | Presence of clinical symptoms and classification based on EF values | • HF is a complex clinical syndrome that results from any structural or functional impairment of ventricular filling or ejection of blood. • There is no single diagnostic test for HF because it is largely a clinical diagnosis based on careful history and physical examination. EF is considered important in classification of patients with HF because of differing patient demographics, comorbid, conditions, prognosis, and response to therapies. |
|
2022 AHA/ACC/HFSA [14] |
Clinical definition Distinction into 4 different stages to emphasize the development and progression of the disease Classification based on EF values |
HF is a complex clinical syndrome with symptoms and signs that result from any structural or functional impairment of ventricular filling or ejection of blood. Therapeutic interventions in each stage aim to modify risk factors (stage A, at risk of heart failure), treat risk and structural heart disease to prevent HF (stage B, Pre-heart failure), and reduce symptoms, morbidity, and mortality (stages C, symptomatic heart failure and D, Advanced heart failure). |
| 2012 ESC [15] | Presence of specific clinical symptoms and signs and reduction of EF. If EF is preserved, relevant structural heart disease and/or diastolic dysfunction must be present. |
HF is defined, clinically, as a syndrome in which patients have typical symptoms (e.g. breathlessness, ankle swelling, and fatigue) and signs (e.g. elevated jugular venous pressure, pulmonary crackles, and displaced apex beat) resulting from an abnormality of cardiac structure or function. |
| 2016 ESC [16] | Presence of symptoms and/or clinical signs and reduction of EF. If this is mildly reduced or preserved, the following must be present: - elevated natriuretic peptide values - one of the following conditions: 1- relevant structural heart disease diastolic disfunction |
HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle swelling and fatigue) that may be accompanied by signs (e.g. elevated jugular venous pressure, pulmonary crackles and peripheral oedema) caused by a structural and/or functional cardiac abnormality, resulting in a reduced cardiac output and/or elevated intracardiac pressures at rest or during stress. |
| 2021 ESC [17] | Presence of symptoms and/or clinical signs and reduction of EF. If EF is preserved, it is necessary that there is objective evidence of cardiac structural and/or functional abnormalities consistent with the presence of LV diastolic dysfunction/raised LV filling pressures, including raised natriuretic peptides. |
Heart failure is not a single pathological diagnosis, but a clinical syndrome consisting of cardinal symptoms (e.g. breathlessness, ankle swelling, and fatigue) that may be accompanied by signs (e.g. elevated jugular venous pressure, pulmonary crackles, and peripheral oedema). It is due to a structural and/or functional abnormality of the heart that results in elevated intracardiac pressures and/or inadequate cardiac output at rest and/or during exercise. |
| 2017 JCS/JHFS [18] | Presence of clinical symptoms and classification based on EF values | HF is defined as a clinical syndrome consisting of dyspnoea, malaise, swelling and/or decreased exercise capacity due to the loss of compensation for cardiac pumping function due to structural and/or functional abnormalities of the heart. |
| 2021 JCS/JHFS [19] | Presence of clinical symptoms and/or signs, personal and family history, ECG, chest X-ray and only lastly evaluation of markers (BNP, NT-proBNP). | HF is defined as a clinical syndrome consisting of dyspnoea, malaise, swelling, and/or decreased exercise capacity owing to the loss of compensation for cardiac pumping function owing to structural and/or functional abnormalities of the heart |
Table 3.
The main advantages and limitations of clinical use of NT-proBNP.
| Advantages | Limitations |
|---|---|
| • Early diagnosis marker in patients with diabetes in the absence of a clear clinical expression of heart failure | • The increase in BNP and NT-proBNP may also depend on other comorbidities such as chronic renal failure or atrial fibrillation |
| • In the absence of a defined cardiovascular pathology, the dosage of NT-proBNP values could predict the onset of heart failure, coronary artery disease and stroke | • The value of NT-proBNP should also be correlated with age, sex and BMI |
| • NT-proBNP values are significantly associated with increased odds of advanced HF | • There is a significant “grey area” in which the diagnosis is rather indeterminate |
| • Correlation between NT-proBNP values and the risk of adverse events in patients with heart failure with preserved ejection fraction. |
Table 4.
The main advantages and limitations of clinical use of HF biomarkers.
| Biomarker | Advantages | Limitations |
|---|---|---|
| MR-pro-ANP | • capability to predict stable chronic HF | • performance diminished in patients with BNP and NT-pro-BNP values within the ‘gray-zone’ • same interferences as the assays for BNP and NT-pro-BNP |
| cTn | • predict new HF • elevated levels are associated with advanced HF, poor prognosis, mortality risk and development of HF in subjects with previous acute myocardial infarction • In patients with acute HF → frequent hospital admissions, increased intensive care unit admissions and in-hospital mortality. • in patients with chronic HFrEF → increased long-term mortality and a higher risk of HF rehospitalization |
• different values based on sex and race • increase in serum values in the case of cardiovascular diseases not related to HF but also in non-cardiovascular diseases |
| Norepinephrine | • good predictor of prognosis | • no better prognostic performance than BNP |
| Chromogranin A-B | • expression proportional to the severity of HF | few studies available |
| PRA | • independent predictor of cardiac death | few studies available |
| ADM | • plasma concentrations increase in case of HF | • routine dosing limited by its short half-life and binding to transport proteins |
| MR-proADM | • good predictor of survival | few studies available |
| Copeptin | • good predictor of mortality | |
| Urocortin-1 | • Circulating levels increase in HF | • not appear to have additional diagnostic or prognostic value over NT-proBNP |
| Gal-3 | • Levels are helpful for short-term mortality and rehospitalization. • The prognostic power is more significant in HFpEF |
• Levels vary by sex and increase with age and in other conditions, such as systemic inflammation and renal failure. |
| sST2 | • repeated measurement is useful in prognostic stratification and predicted rehospitalization especially in chronic HF • an independent predictor of reverse remodeling |
• insufficient evidence to recommend its use in clinical practice • no unanimous consensus on the best prognostic cut-off in chronic HF |
| GDF-15 | • elevated levels in HF patients may be detected as early as 90 days before hospital admission | • conflicting data regarding the cardioprotective role |
| MMPs/TIMPs | • concentration probably reflects the extent of cardiac tissue remodeling, with important prognostic implications. | few studies available |
| FGF21 | • levels are strongly linked to left ventricular systolic dysfunction, and patients with higher levels show an increased risk of cardiac death and high levels are independent of other comorbidities | few studies available |
| OPN | • excellent prognostic biomarker | few studies available |
| SDC-4 | • its increased levels are significantly associated with left ventricular hypertrophy | few studies available |
| MSTN | • levels are significantly associated with a lower survival rate and a higher number of rehospitalizations | few studies available |
| CRP | • prognostic role • associated with an increased risk of developing HF in elderly subjects |
• poor specificity |
| CA125 | • • potential role in clinical management (monitoring of decongestant therapy) and prognosis | • further studies are needed to establish reference intervals for for diagnosis and treatment monitoring. |
| CAR | • In chronic HF, high levels are associated with elevated PAPs- LVESV and decreased TAPSE. | few studies available |
| NLR | • elevated levels can predict a raised risk of short- and long-term mortality and adverse outcome in patients with acute HF | few studies available |
| MPO | • Plasma concentration increases in chronic HF • Independent predictor of 1-year mortality compared with BNP |
few studies available |
Table 5.
Some examples of miRNA in HF.
| miRNA | Role |
|---|---|
| mir-22 | • regulates calcium reuptake by sarcoplasmic reticulum • associated with hypertrophy and myocardial fibrosis |
| miR-133/miR-223-3p | • their silencing reduces GLUT4 expression and thus increases myocardial glucose uptake in HF patients. |
| miR-21 | • involved in HF-related fibrosis through the stimulation of the ERK-MAP pathway |
| miR-1 | • involved in regulating myocardial hypertrophy |
| miR-212/132 | • associated with cardiac hypertrophy and HF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



