
Submitted:
16 July 2025
Posted:
21 July 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Some women are experiencing menstrual adverse events including heavier bleeding following Coronavirus disease 2019 (COVID-19) spike immunization. The etiology of these menstrual adverse events associated with COVID-19 spike immunization remains unknown. The United States Department of Health and Human Services Vaccine Adverse Event Reporting System (VAERS) database was retrospectively analyzed for data reported adverse events affecting menstrual cycles by vaccine. Elevated normalized frequencies for menstrual adverse events were detected for multiple vaccines, including COVID-19 vaccines and human papillomavirus (HPV) vaccines. Lower normalized frequencies were detected for both COVID-19 bivariant vaccines and the HPV Gardasil 9 vaccines compared to higher normalized frequencies for COVID-19 Pfizer-BioNTech, COVID-19 Moderna, HPV Cervarix, and HPV Gardasil vaccines. Chi-squared 2x2 statistically significant differences in normalized frequencies were observed between different COVID-19 Pfizer-BioNTech lots (p < 0.00001) and also COVID-19 Moderna lots (p < 0.00001). Manufacturing contaminants (e.g., endotoxins) are likely candidates consistent with the observed data for reported menstrual adverse events.
Keywords:
menstruation
; menstrual cycle
; endotoxin
; mRNA vaccines
; COVID-19 vaccine
; HPV vaccine
Introduction
Menstrual disturbances including heavy menstrual bleeding were reported post COVID-19 vaccination [1,2,3,4,5]. Unexpected vaginal bleeding also occurs in some nonmenstruating women post COVID-19 vaccination [6]. A case-control study found an increased risk for heavy menstrual bleeding post COVID-19 immunization (Odds Ratio, 1.20 [95% confidence interval 1.07-1.35]) [7]. A cross-sectional online self-administered survey found 46.7% females reported menstrual symptoms post first COVID-19 vaccine dose, 66.3% reported menstrual symptoms post-vaccination, symptoms resolved within 2 months for 93.6% of participants, and participants who experienced general side effects had significantly more menstrual abnormalities (p < 0.001) [8]. Are the same frequencies of menstrual AEs being reported for newer COVID-19 and COVID-19 bivariant vaccines?
Herein, the VAERS database was retrospectively examined for several menstrual AEs across all vaccines. Elevated normalized frequencies for menstrual AEs were observed for multiple vaccines, including COVID-19 and HPV vaccines. Comparisons between vaccines detected lower normalized frequencies for COVID-19 Pfizer-BioNTech bivariant vs. COVID-19 Pfizer-BioNTech, COVID-19 Moderna bivariant vs. COVID-19 Moderna, HPV Gardasil vs. HPV Cervarix, HPV Gardasil 9 vs. HPV Gardasil, and HPV Gardasil 9 vs. HPV Cervarix. For these COVID-19 and HPV vaccines, the observed data is consistent with likely manufacturing contaminants (e.g., endotoxins) triggering the associated menstrual AEs.
Methods
This is a retrospective analysis of the VAERS database [9] from January 1, 1990 until May 30, 2025. VAERS was searched for the AEs: Amenorrhoea, Dysmenorrhoea, Heavy menstrual bleeding, Menstruation irregular, Menstrual disorder, Menorrhagia, and Vaginal haemorrhage. The Ruby program vaers_slice5f.rb [10] was used for retrospective analysis of the VAERS data files VAERSDATA, VAERSSYMPTOMS, and VAERSVAX for the years 1990 to 2025 and NonDomestic. Microsoft Excel was used for calculating Pearson correlation coefficients and graphing data. An online calculator was used for Chi-Square 2x2 tests [11].
For vaccine (Vname), and each adverse event (X=menstrual AE) in VAERS, normalized AE frequencies per P=100,000 VAERS reports per category AEs can be calculated with equation I.
Results
Tallying adverse events for females and normalizing to 100,000 VAERS reports identified 22 vaccines with at least 10 AEs for one or more of the seven menstrual AEs with a frequency at least 200 per 100,000 VAERS reports (Figure 1); another 10 vaccines had from 5 to 9 AEs (data not shown). Multiple COVID-19 and HPV vaccines were identified with higher frequencies of menstrual AEs (Figure 1). The normalized frequencies for COVID-19 bivalent vaccines are both lower than the original versions of Pfizer-BioNTech and Moderna vaccines (Figure 2). The menstrual AEs for COVID-19 Pfizer-BioNTech normalized frequency of 4,442 AEs per 100,000 VAERS reports are different from Pfizer-BioNTech bivalent booster shots 686 per 100,000 VAERS reports (chi-square p-value < 0.00001). The menstrual AEs for COVID-19 Moderna of 2,038 per 100,000 VAERS reports are different from COVID-19 Moderna bivalent of 463 per 100,000 (chi-square p-value < 0.00001). The menstrual AEs associated with HPV Gardasil are lower than HPV Cervarix and HPV Gardasil 9 are lower than HPV Gardasil (Figure 2). The menstrual AEs for HPV Cervarix of 6,090 per 100,000 VAERS reports are different from HPV Gardasil 2,959 per 100,000 VAERS reports (chi-square p-value < 0.00001). The menstrual AEs for HPV Gardasil 9 of 1,556 per 100,000 VAERS reports are different from HPV Gardasil of 2,959 per 100,000 VAERS reports (chi-square p-value < 0.00001). The age groups for menstrual AEs for multiple vaccines are illustrated in Figure 3; note that Influenza seasonal (Fluvirin) and Pneumo (Pneumovax) were included to illustrate background menstrual AEs frequencies. Yearly normalized frequencies are illustrated for COVID-19 vaccines (Figure 4A) and HPV vaccines (Figure 4A). The discordance between normalized frequencies for vaccines illustrated in Figure 2 is suggestive of possible manufacturing contaminants that differ between the vaccines. The normalized frequencies are illustrated for selected lots for COVID-19 Moderna (Figure 5A), COVID-19 Pfizer-BioNTech (Figure 5B), and COVID-19 Janssen (Figure 5C). For the HPV vaccines, the lots worth examining are Cervarix: AHPVA138BA, AHPVA146AA, AHPVA149AA, AHPVA149BA, AHPVA149CA, AHPVA156AB, AHPVA161BA, AHPVA162AA, & AHPVA164AA; Gardasil: 90649, 0063X, 0072X, & 0137U; Gardasil 9: 1659422, 1687290, & N035032.
Discussion
COVID-19 Vaccines
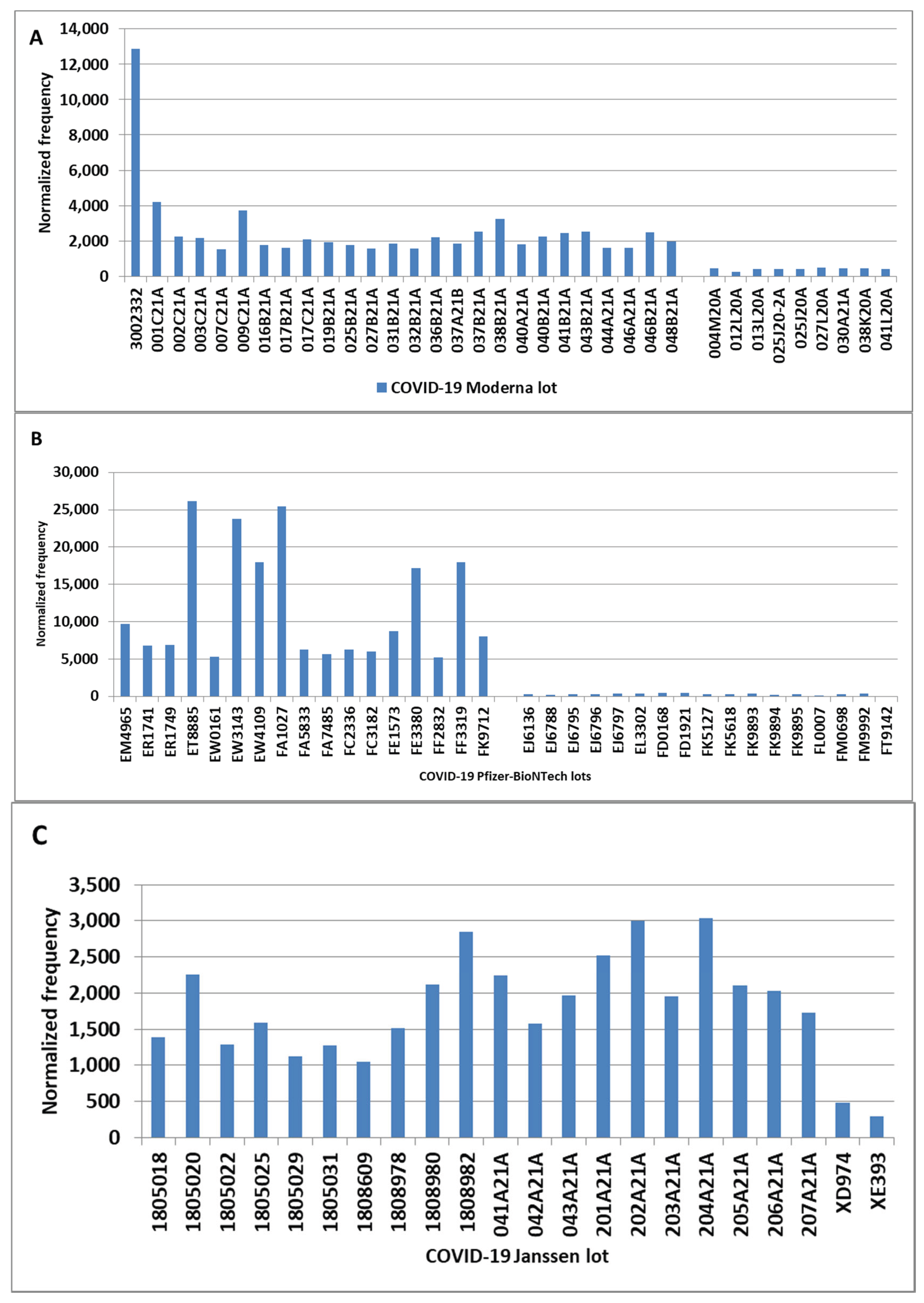
The COVID-19 vaccines Pfizer-BioNTech, Janssen, and Moderna have normalized frequencies higher than paired Pfizer-BioNTech bivalent and Moderna bivalent vaccines (Figure 1 & Figure 2). These normalized frequencies are higher than the control comparison vaccines: influenza seasonal (Fluvirin) and Pneumo (Pneumovax) (Figure 3). Yet, the components of the COVID-19 Pfizer-BioNTech and Moderna vaccines are the same as the corresponding bivalent versions; why is there such a discrepancy in the observed normalized frequencies? For the Pfizer-BioNTech vaccine, six lots have normalized frequencies above 10,000 per 100,000 (> 1 in 10 and as high as 1 in 4 for three lots: ET885, EW3143, & FA1027) (Figure 5B). Comparing Pfizer-BioNTech lots ET8885 (36,138 per 100,000 VAERS reports), EW0161 (5,361 per 100,000), and EJ6136 (272 per 100,000) have chi-square 2x2 p<0.00001 for ET8885 vs. EW0161 and EW0161 vs. EJ6136. For the COVID-19 Moderna vaccine, lot 3002332 has a normalized frequency of 12,880 per 100,000 (1 in 7.8) VAERS reports (Figure 5A); the menstrual AEs observed as statistically significant compared to the next lot 001C21A with a frequency of 4,219 (chi-square 2x2 p<0.00001). Also, lot 001C21A with normalized frequency of 4,219 is statistically different from lot 004M20A with a frequency of 439 per 100,000 VAERS reports (p<0.00001). For multiple COVID-19 Moderna, Pfizer-BioNTech, and Janssen vaccine lots have higher normalized frequencies (Figure 5A-C) while other Pfizer-BioNTech and Moderna lots have much lower normalized frequencies illustrated on the right side for Figure 5A & Figure 5B.
Hypothesis 1
: COVID-19 vaccines are contaminated with one or more manufacturing contaminants (e.g., endotoxins) that are causative for the menstrual AEs. The data (Figure 1 & Figure 2) suggest that multiple Pfizer-BioNTech, Janssen, and Moderna have higher concentration levels of manufacturing contaminant(s) than Pfizer-BioNTech bivalent and Moderna bivalent. Endotoxin, a possible manufacturing contaminant, is known to disrupt female reproductive function [12].
HPV Vaccines
The HPV vaccines have normalized frequencies for Cervarix of 6,090 per 100,000 VAERS reports, Gardasil of 2,959, and Gardasil 9 of 1,556 (Figure 1). The higher Menorrhagia normalized frequencies for HPV Cervarix and HPV Gardasil are not observed for the COVID-19 vaccines (Figure 2). For the HPV Gardasil vaccine, lot 90649 had the highest number of menstrual AE reports (3,516 per 100,000 VAERS reports). A self-controlled case series study reported an association between HPV vaccination associated with elevated risks of autonomic dysfunction and menstrual irregularities [13].
Hypothesis 2:
HPV vaccines are contaminated with one or more manufacturing contaminants (e.g., endotoxins) that are causative for menstrual AEs. The data suggest that Cervarix and Gardasil have higher concentration levels of manufacturing contaminant(s) than Gardasil 9 (Figure 1&Figure 2). These predicted manufacturing contaminant(s) likely have overlaps with those of the COVID-19 vaccines, but HPV Cervarix and Gardasil may contain an additional contaminant due to the higher Menorrhagia AEs observed (Figure 2).
All Vaccines
Hypothesis 3:
Menstrual AEs associated with vaccines may be from a set of one or more manufacturing contaminants shared by multiple vaccines (Figure 1). Increases in concentration levels of these manufacturing contaminants are predicted to be associated with higher frequencies of menstrual AEs.
Conclusions
Menstrual adverse events were retrospectively studied in the VAERS database. Comparisons between different COVID-19 vaccines, HPV vaccines, and normalized frequencies of menstrual AEs between different lots implicate manufacturing contaminants as a likely cause for reported menstrual AEs. Candidate vaccine lots with higher menstrual AEs normalized frequencies were identified for potential follow-up studies.
Funding
None
Author contributions
DOR: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. The author has read and approved the submitted version.
Availability of Data
Ricke, Darrell, 2025, "Vaccine Menstrual Adverse Events", https://doi.org/10.7910/DVN/HYZRX4, Harvard Dataverse, V1
Conflicts of interest
The author declares no conflict of interest.
Ethical approval
Not applicable.
Consent for Publication
Not applicable.
References
- Matar SG, Nourelden AZ, Assar A, et al (2023) Effect of COVID-19 vaccine on menstrual experience among females in six Arab countries: A cross sectional study. Influenza Other Respir Viruses 17:e13088. [CrossRef]
- Baena-García L, Aparicio VA, Molina-López A, Aranda P, Cámara-Roca L, Ocón-Hernández O (2022) Premenstrual and menstrual changes reported after COVID-19 vaccination: The EVA project. Womens Health 18:17455057221112237. [CrossRef]
- Rastegar T, Feryduni L, Fakhraei M (2023) COVID-19 vaccine side effects on menstrual disturbances among Iranian women. New Microbes New Infect 53:101114. [CrossRef]
- Dabbousi AA, El Masri J, El Ayoubi LM, Ismail O, Zreika B, Salameh P (2023) Menstrual abnormalities post-COVID vaccination: a cross-sectional study on adult Lebanese women. Ir J Med Sci 1971 - 192:1163– 1170.
- Lee KM, Junkins EJ, Luo C, Fatima UA, Cox ML, Clancy KB (2022) Investigating trends in those who experience menstrual bleeding changes after SARS-CoV-2 vaccination. medRxiv 2021.10.11.21264863.
- Blix K, Laake I, Juvet L, Robertson AH, Caspersen IH, Mjaaland S, Skodvin SN, Magnus P, Feiring B, Trogstad L Unexpected vaginal bleeding and COVID-19 vaccination in nonmenstruating women. Sci Adv 9:eadg1391.
- Botton J, Bertrand M, Jabagi M-J, et al (2024) Risk of heavy menstrual bleeding following COVID-19 vaccination: A nationwide case-control study. Vaccine 42:126252.
- Muhaidat N, Alshrouf MA, Azzam MI, Karam AM, Al-Nazer MW, Al-Ani A (2022) Menstrual Symptoms After COVID-19 Vaccine: A Cross-Sectional Investigation in the MENA Region. Int J Womens Health 14:395–404.
- VAERS (2025) Vaccine Adverse Event Reporting System. U.S. Department of Health & Human Services.
- Ricke DO (2025) VAERS-Tools. https://github.com/doricke/VAERS-Tools Accessed July 1, 2025.
- Social Science Statistics (2025) Chi Square Calculator for 2x2. https://www.socscistatistics.com/tests/chisquare/ Accessed July 1, 2025.
- Bidne KL, Dickson MJ, Ross JW, Baumgard LH, Keating AF (2018) Disruption of female reproductive function by endotoxins. Reproduction 155:R169–R181.
- Wastila L, Fu Y-H, Tung CC, Qato DM (2025) Association Between Vaccination for Human Papillomavirus (HPV) and Autonomic Dysfunction and Menstrual Irregularities: A Self-Controlled Case Series Analysis. Drugs - Real World Outcomes. [CrossRef]
Figure 1.
Menstrual adverse events normalized frequency by vaccine with minimum of 10 reported AEs and normalized frequency >= 200 per 100,000 VAERS reports.
Figure 1.
Menstrual adverse events normalized frequency by vaccine with minimum of 10 reported AEs and normalized frequency >= 200 per 100,000 VAERS reports.
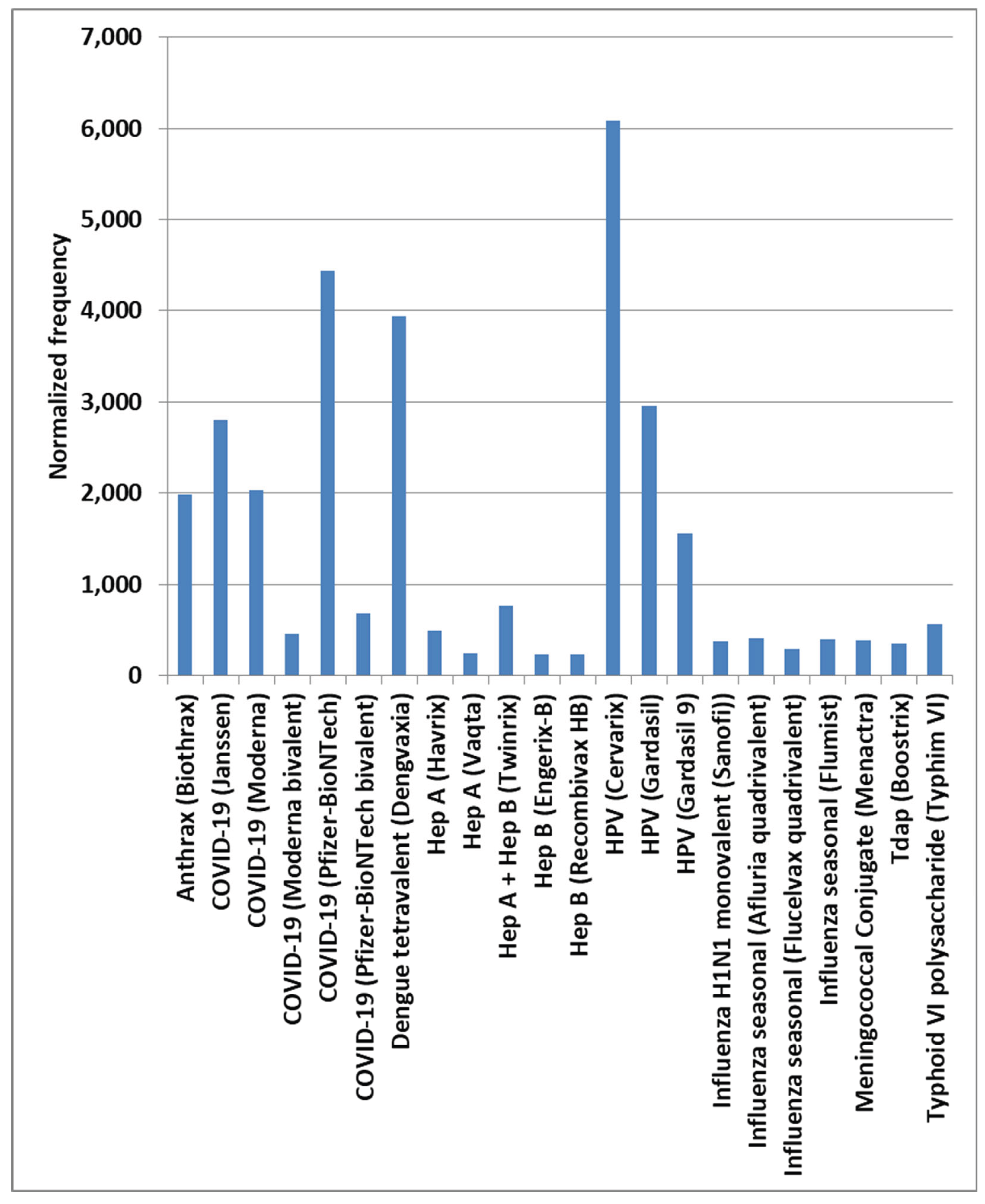
Figure 2.
COVID-19 and HPV menstrual adverse events normalized frequencies.
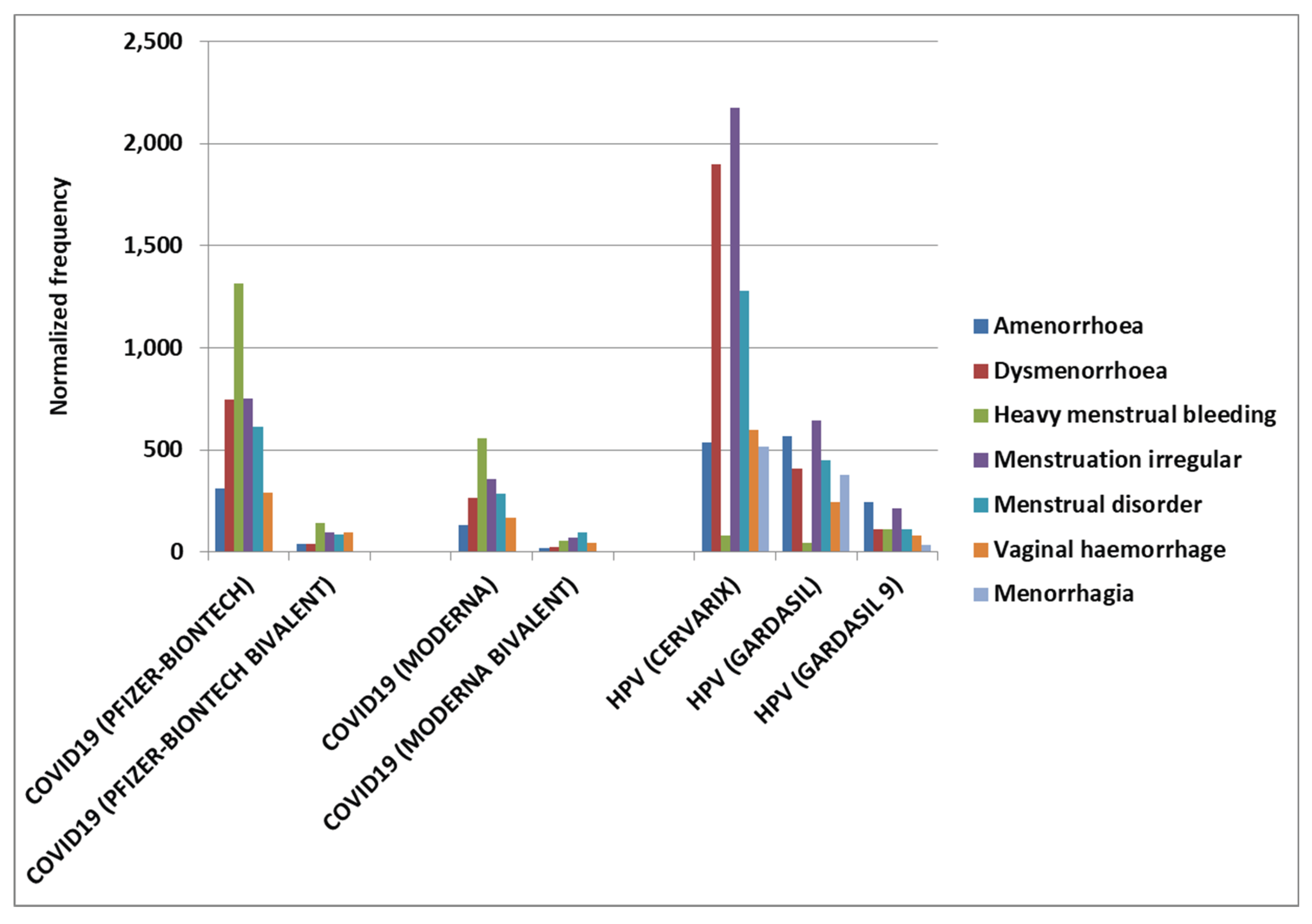
Figure 3.
Multiple menstrual AEs by age group with background control groups Influenza seasonal (Fluvirin) and Pneumo (Pneumovax) also included.
Figure 3.
Multiple menstrual AEs by age group with background control groups Influenza seasonal (Fluvirin) and Pneumo (Pneumovax) also included.
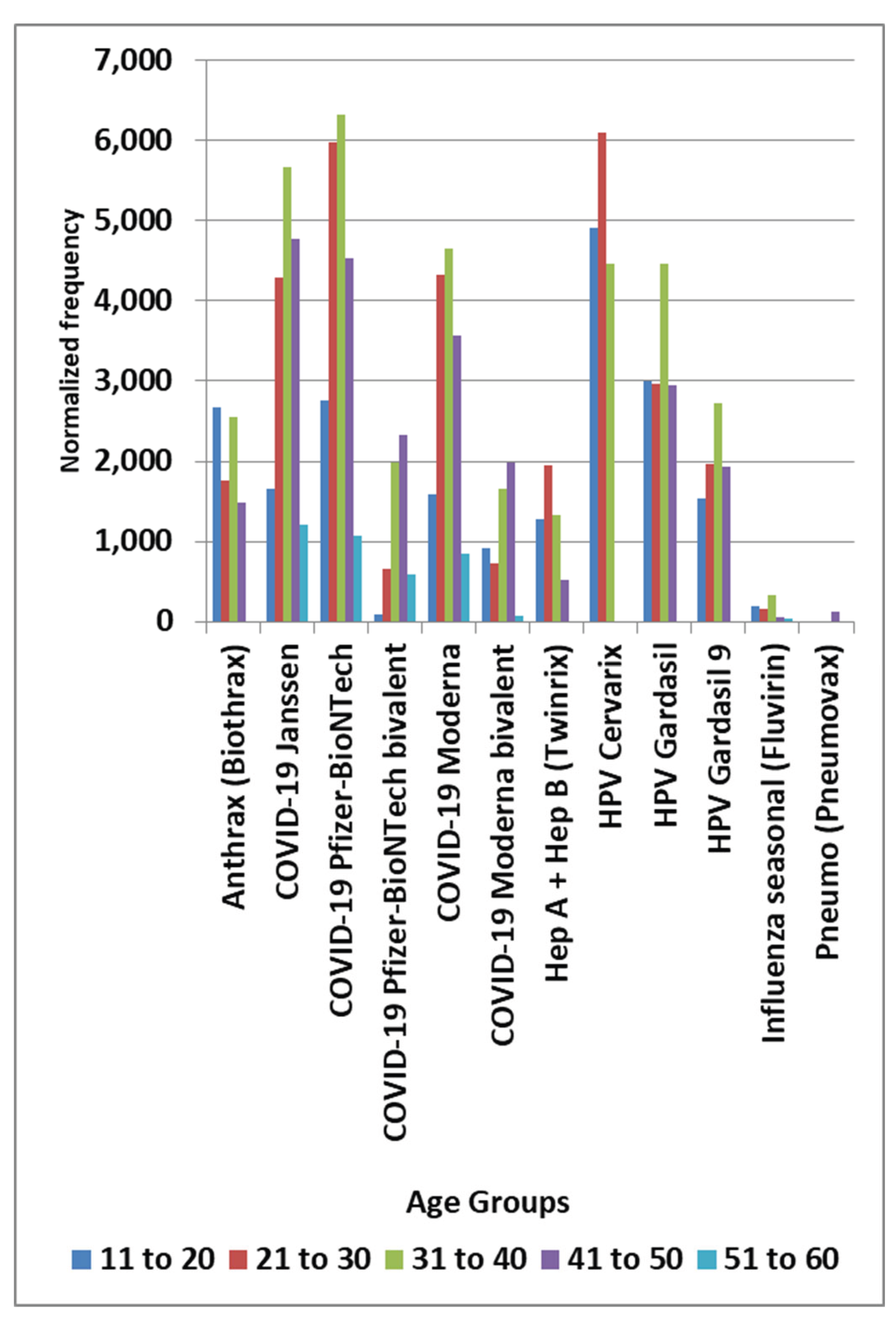
Figure 4.
(A) Multiple COVID-19 menstrual adverse events by vaccination year.
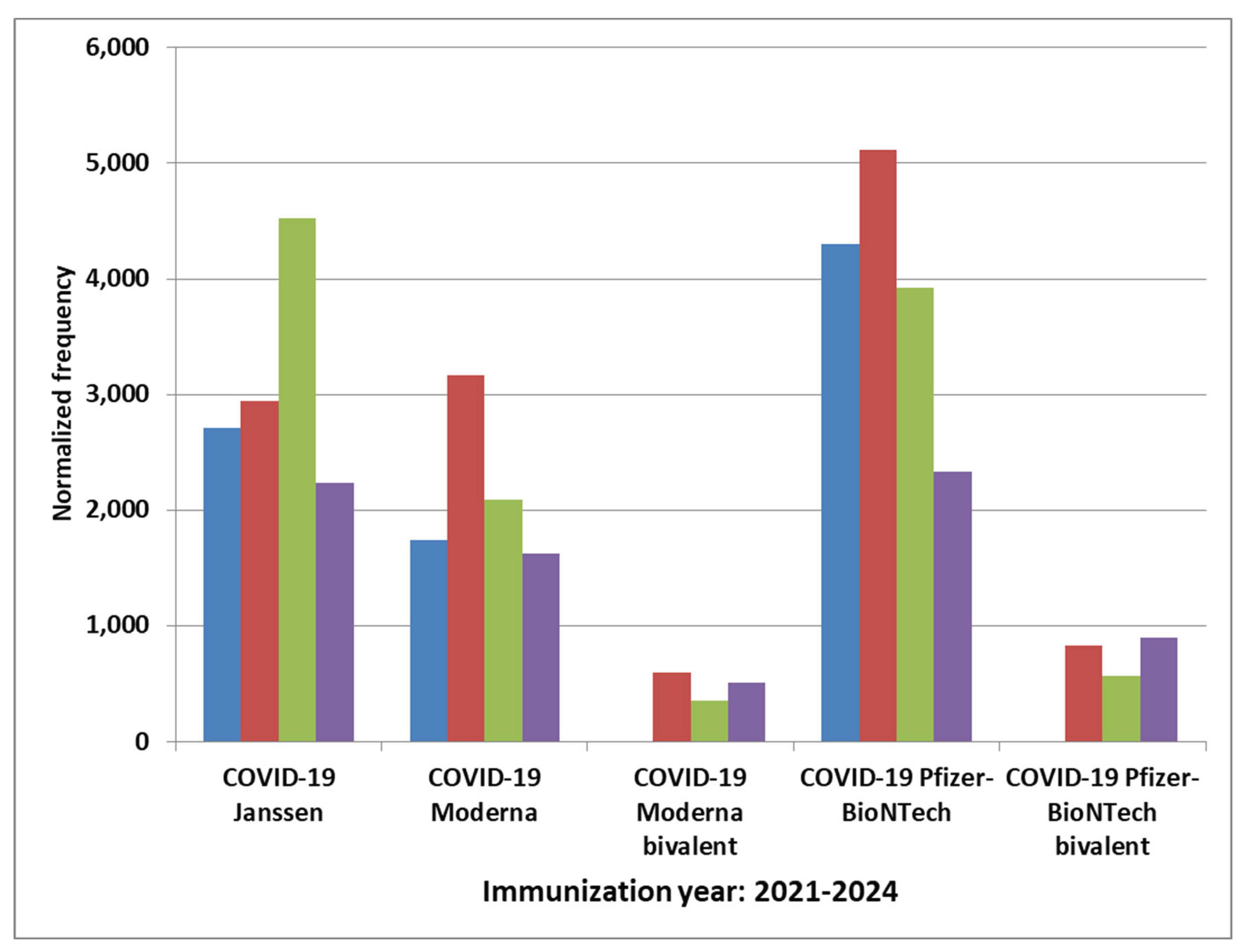
Figure 4.
(B) Multiple HPV menstrual adverse events normalized frequency by immunization year.
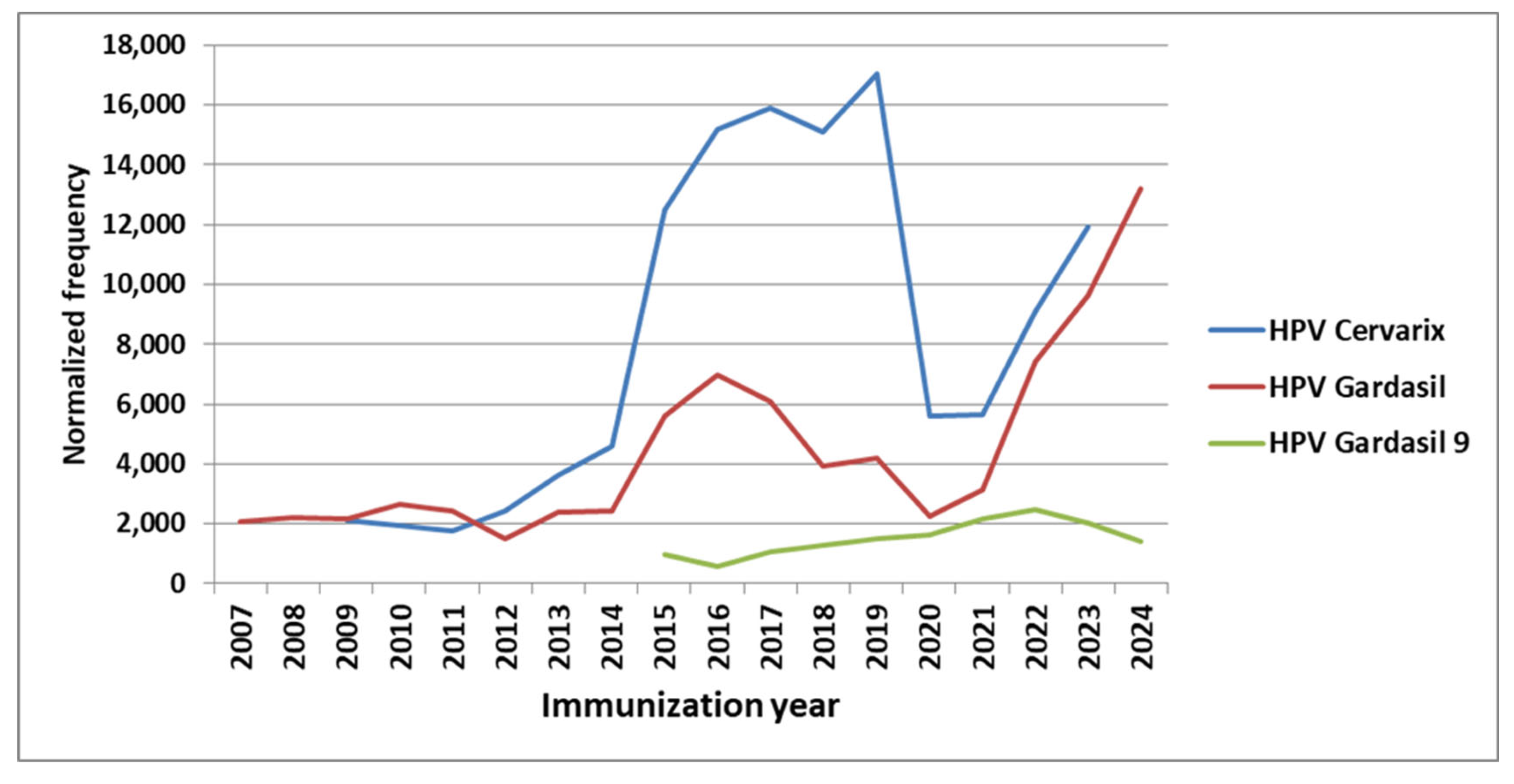
Figure 5.
COVID-19 lots menstrual AEs normalized frequencies (A) selected Pfizer-BioNTech lots (minimum 1,000 reports per lot and normalized frequency either >5,000 or <500 per 100,000 VAERS reports), (B) selected Moderna lots (minimum 1,000 reports per lot and normalized frequency either >1,500 or <500 per 100,000 VAERS reports), and (C) Janssen lots.
Figure 5.
COVID-19 lots menstrual AEs normalized frequencies (A) selected Pfizer-BioNTech lots (minimum 1,000 reports per lot and normalized frequency either >5,000 or <500 per 100,000 VAERS reports), (B) selected Moderna lots (minimum 1,000 reports per lot and normalized frequency either >1,500 or <500 per 100,000 VAERS reports), and (C) Janssen lots.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



