
Submitted:
12 June 2023
Posted:
13 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
To date, the impact of COVID-19 vaccination on formerly menstruating women remains unknown. For this reason, a retrospective observational cross-sectional study was conducted (N= 548) using an online survey. General characteristics, medical history, and adverse events following COVID-19 vaccination were recorded. In comparison with the first dose, significantly higher percentages of respondents experienced menstrual-related disturbances (dose 1: 38.5% vs. dose 2: 44.8%; McNemar=9.15; mid P-value=0.002), as well as the simultaneous occurrence of two or more of these symptoms (dose 1: 11.2% vs. dose 2: 15.3%; McNemar=13.53; mid P-value=0.044) after receiving the second one. Among them, those related with the length and flow stand out, being of long-term nature in about 17-20% of cases. Interindividual factors influencing this unexpected event after receiving the dose 1 may include weight (AOR 1.02, CI 95% 1.01–1.03, P<.001), perimenopause (AOR 2.28, CI 95% 1.37–3.77, P=.001), pre-existing diagnoses of non-autoimmune rheumatic/articular conditions (AOR 0.31, CI 95% 0.10–1.00, P=0.05), hormonal contraceptive use (AOR 0.25, CI 95% 0.07-0.82, P=0.02), suffering from other vaccine side effects − such as arm pain (AOR 0.61, CI 95% 0.39–0.95, P=0.03), headache (AOR 0.53, CI 95% 0.35 – 0.80, P=.003), swollen glands (AOR 0.29, CI 95% 0.15 – 0.60, P=.001) and nauseas (AOR 0.35, CI 95% 0.14 – 0.86, P=0.02) – and the number of previous pregnancies (AOR 2.70, CI 95% 1.54 – 4.76, P=.001). Formerly menstruating women may experience long-term menstrual-related disturbances following COVID-19 vaccination.
Keywords:
women’s health
; COVID-19 vaccine
; menstrual-related disturbances
; formerly menstruating women
; secondary amenorrhea
1. Introduction
The development of SARS-CoV-2 vaccines has been one of the main preventive strategies to halt the advance of the COVID-19 pandemic. To this end, the drug regulatory agencies accelerated the established procedures, which allow to perform mass vaccination campaigns all over the world in record time [1,2,3,4,5,6]. Short-term side effects are similar to those observed for other vaccines and medicines, the expected benefits have been considered to outweigh any currently known adverse events [7,8,9]. However, its safety must be under continuous study. Despite the logical doubts in a context of global health crisis, mass immunization campaigns have been a success in nations such as Spain, one of the most affected European countries since the pandemic began.
However, as with any vaccine or drug, its safety must be under continuous study. Since vaccination campaigns started, individuals and health professionals worldwide have shared their testimonies about the occurrence of menstrual changes (MC) after COVID-19 vaccination on social media, an unexpected event that has not been monitored in clinical trials [10,11,12,13]. Furthermore, a considerable number of reports has been also officially documented by national bodies responsible for public health surveillance [7,8,14,15]. In the light of a growing concern about this health issue, several studies were launched. It should be remembered that the menstrual cycle is a sign of female health and fertility. Driving by a complex hormonal process, it may be affected by several external factors [16,17]. Nevertheless, any abnormal changes hereof should not be ignored [18,19], even in a context of public health emergency.
To date, there are few available data about the link between SARS-CoV-2 vaccine and MC in menstruating people [14,16,17,20,21,22,23,24,25,26,27,28]. Furthermore, the prevalence of this event in formerly menstruating people remains unknown, because different causes of secondary amenorrhea − pregnancy, breastfeeding, menopause, contraceptives methods, and gynecological conditions [29,30] – has been considered as exclusion criteria in these studies. With the purpose to provide additional insights to the limited extant literature about this subpopulation [26], this study was aimed to analyze not only the occurrence of menstrual-related disturbances (MRD) but also the influencing factors.
2. Materials and Methods
2.1. Experimental design
A retrospective observational cross-sectional study was conducted on Spanish adult women using an online survey (Microsoft Forms®, Microsoft Corporation, Washington, USA).
2.2. Recruitment, data collection and participants
The online survey was released in December 2021 via social networks, applying the snowball method. An informed consent was only obtained from those who agree to be contacted via email by the research group for additional data collection. Thus, 17,512 were recruited within 15 days; from this sample, the data pertaining to a subpopulation of formerly menstruating women (FMW) was selected for the present analysis (N=548, Figure 1). The inclusion criteria were women: (i) over 18 years of age, (ii) having secondary amenorrhea for different causes and (iii) having received at least one dose of the COVID-19 vaccine.
2.3. Survey information
We designed a customized questionnaire based on the survey launched on April 2021 by Lee et al. [26]. It was composed of 56 multiple-choice and text entry questions divided into 6 sections. Participants were asked about 1) the general characteristics of their menstrual cycles −, 2) COVID-19 disease, 3) COVID-19 vaccine, 4) menstrual experiences both after the infection and after receiving each dose of the vaccine in comparison with the expected period symptoms, 5) other MRD, 6) time between infection/vaccine and MRD, 7) duration of MRD, 8) side effects from each dose of the vaccine, 9) reproductive history, 10) medical history, and 11) demographics. The survey took approximately 10-15 min to complete.
2.4. Statistical analysis
Participants were categorized according to the occurrence (MRD subgroup) or not (n-MRD subgroup) of MRD after vaccination against the SARS-CoV-2 virus. Values were expressed as mean±standard deviation for quantitative variables and number of participants and frequency (%) for qualitative ones. Chi-square and Mann-Whitney U tests were performed for qualitative and quantitative variables, respectively. McNemar mid-P test was applied to detect differences between doses of the COVID-19 vaccine in the occurrence of MRD. Subsequently, a bivariate logistic regression analysis was performed to investigate possible associations between the occurrence of MRD following vaccination (dependent variable) and the independent variables that were significant (P<0.05) in the previous analyses. Thus, the results were presented as adjusted odds ratios (ORAs) with 95% confidence intervals (CI). The aforementioned analyses were performed using the Statistical Package for Social Sciences (SPSS v.25, IBM, New York, USA) for Windows. Statistical significance was set at P≤0.05.
3. Results
3.1. Anthropometric characteristics and medical history
53.8% of the study participants (N=548, mean age 40.4±10.7 years) had normal weight (mean BMI value=25.0±5.5), 12.4% had autoimmune diseases, and 25.0% had other clinical conditions. The secondary amenorrhea at the time of vaccination was caused by the contraceptive use (29.6%), post-menopause (17.3%), perimenopause (16.8%), and breastfeeding (14.8%). 37.8% of women used contraceptives for less than 10 years (79.3%), 60.2% had been pregnant, and 54.4% reported having been diagnosed with a gynecological disease (Table 1).
3.2. Impact of vaccination on the menstrual health of formerly menstruating women
Pfizer-BioNTech Comirnaty® vaccine was received in most cases, followed by Moderna Spikevax® and Oxford-AstraZeneca® ones (Table 2).
3.3. Comparative analysis of the occurrence of MRD after COVID-19 vaccination
A significantly higher percentage of FMW experienced MRD after the second dose (Figure 2a), as is the case with the simultaneous occurrence of two or more symptoms (Figure 2b). Among the main disturbances, significant differences between doses were detected for the variables “spotting” (Figure 2c), “breast pain” (Figure 2e), and “abnormal bleeding (Figure 2h). Hot flashes were more frequent after the first dose (Figure 2f)
3.4. Comparative analysis of menstrual bleeding changes after COVID-19 vaccination
Significant differences between doses were observed for the variables “length” (Figure 3a) and “flow” (Figure 3b). Most surveyed did not experience abnormal bleeding, and those who reported it pointed that this change mainly occurred after more than 14 days after the vaccination (Figure 3c). It is noteworthy that, after receiving the second dose, 20.4% of women reported that these alterations last ‘’until today’’ compared to 17.1% who reported this situation after receiving dose 1, as well as for other durations (Figure 3d).
3.5. Comparative analysis of the side effects after COVID-19 vaccination
After the second dose, there was a higher occurrence of side effects compared to the first one (Figure 4a), as well as the simultaneous occurrence of two or more symptoms (Figure 4b). Fatigue (Figure 4d), fever (Figure 4e), headache (Figure 4f), and nauseas (Figure 4g) appeared more frequently after dose 2.
3.6. Factors associated with the occurrence or not of MRD after COVID-19 vaccination
The mean values of weight and body mass index (BMI) were significantly different between the two subgroups (n-MRD and MRD) and for the two doses.
Based on the gynaecological history data (Table 3), a higher number of women who have used contraceptives for less than 10 years were recorded in the MRD subgroup for dose 2; moreover, hormonal contraceptives were significantly more used by these FMW. The number of children was significantly different between subgroups for the first dose. On the other hand, the percentage of perimenopausal women was higher in the subgroup experiencing MRD after receiving both doses. Significant differences were also detected in relation to suffering from gynaecological diseases such as endometriosis or heavy menstrual bleeding, in both cases being higher in the MRD than n-MRD for the second dose. Other noteworthy results are those related to side effects. Thus, after receiving the first dose, the occurrence of breast lumps, fatigue, arm pain, headache, swollen glands, and nauseas were higher in the subgroup experiencing MRD; for the second dose, the different side effects between subgroups included breast lumps, fatigue, headache, and swollen glands. It should be noted that the analysis of each subgroup of amenorrhea separately (contraceptives, menopause and other causes) for the first (Appendix 1) and second (Appendix 2) doses of the vaccine did not altered the above findings.
Subsequently, in the case of the first dose (Table 4), the binary logistic regression analysis showed that those who have a higher weight and receive the vaccine during perimenopause are much likely to suffer from MRD. Conversely, not suffering from a rheumatic / articular condition, not having experienced other side effects − such as arm pain, headache, swollen glands, and nausea, and having 2 or more children decreases the probability of this unexpected event. For the second dose (Table 5), suffering MRD after receiving the first dose of the SARS-CoV-2 vaccine increases the probability of this event. In addition, the use of hormonal contraceptives was found to be an influential factor in experiencing MRD. Finally, as was observed for dose 1, being a perimenopausal woman increases the probability of the occurrence of this phenomenon.
4. Discussion
FMW may experience long-term MRD after receiving COVID-19 vaccine. Interindividual factors influencing this unexpected event may include weight, perimenopause, pre-existing diagnoses of rheumatic/articular conditions, hormonal contraceptive use, suffering from other vaccine side effects and the number of previous pregnancies.
Concurring with previous studies in menstruating women [14,20,27], the occurrence of MRD seems to be significantly higher following the second dose of the vaccine. As Male et al. [31] point out, any change that affects the post-dose 1 period could potentially still be in effect for the post-dose 2 period; in turn, it would depend on the time between doses established by the competent national body (in the case of Spain, 3-4 weeks) [32]. In this sense, it has been observed that the those who received both doses in the same cycle were more prone to suffer from more substantial and long-lasting MC [16,24]. Other possible explanations include that people who experienced MRD following dose 1 may be more likely to report it again.
Focusing on the menstrual bleeding disturbances, those related with the length and flow stand out. This observation is consistent with that found in previous studies reporting longer-lasting menstruation [14,20], and/or heavier flow [14,21,25,33,34] than usual in vaccinated women. Unexpectedly, increased bleeding has also been observed in women using hormonal contraception [14,21,25,33], which may indicate that certain immunological processes may be also involved. As for the duration of the changes, several studies agree that MC are of transient nature [14,16,20,23,24,27]. However, our results show far from negligible percentages of women who suffer from it more than 12 months, which has not been described previously. Moreover, abnormal bleeding was mostly experienced in the two weeks post-vaccination, which extends beyond the typical 7 days for the adverse symptoms monitoring established in vaccine trials, as observed by Lee et al. [25]. Similar percentages of vaccinated women experiencing MCD was found in this and other studies [20,28], independently of their previous history of SARS-CoV-2 infection. For their part, Li et al. [35] conclude that the average sex hormone concentrations and the ovarian reserve did not significantly change in those COVID-19 women of child-bearing age who experienced self-resolve menstrual changes. Altogether, this evidence would support the theory about the role of unknown immunological/inflammatory mechanisms as triggers of the MC resulting from both infection and vaccination, including thrombocytopenia [36,37] and changes in lymphocytes subpopulation patterns [38].
Other aspects must also be considered. Firstly, our results show that the presence of side effects was higher after receiving the second dose of the vaccine. Other authors [20,26] report a greater likelihood of MCD when such side effects are experienced; on the contrary, those who did not experience it had better premenstrual syndrome, whose symptoms seem to change following COVID-19 vaccination [17] Secondly, we agree with previous studies [20,22,23,24,27] that the occurrence of MCD seems not to be brand specific (data not shown) and, therefore, independent of the technology approach (adenovirus-vectored or mRNA vaccines). At this point, it should be emphasized that vaccine-induced immune thrombotic thrombocytopenia has been reported as a rare side effect associated to adenovirus-vectored vaccines [7,8,39,40,41]. It mostly affects individuals aged between 20-50 years old and occurs between 4-30 days after the exposure. Our study population was mostly inoculated with the Pfizer-BioNTech vaccine, as in similar researches [23,24]; thus, the non-detection of statistically significant differences may be due to the overrepresentation of this brand compared to others. Therefore, sociodemographic factors may also underlie the different rates of menstrual disturbances among nations. In this sense, the country of residence could be an influencing factor, resulting not only from the predominant use of certain brands of vaccines − and the corresponding schedule – but also from cultural reasons, which may discourage help-seeking behavior among young women [20,42,43].
As regards the factors influencing the occurrence of MRD in FMW after vaccination, the study performed by Popkin et al. [44] concludes that overweight/obesity increases the risk of SARS-CoV-2 infection, worsen COVID-19 outcomes, and may influence the effectiveness of the therapeutic treatments and the vaccines because of immune impairments, among other factors. Since individuals with BMIs higher than 35 are known to have greater baseline variations in menstrual cyclicity [16], it is not surprising that this feature also influences the risk of suffer from MC post-vaccination. On the other hand, no study has explored the potential influence of perimenopause, therefore, we cannot properly compare our results. Only Lee et al. [25] has described an increased chance of breakthrough bleeding after being vaccinated for those premenopausal respondents who were Hispanic/Latinx, had been pregnant in the past but had not given birth, had a diagnosed reproductive condition, were on long-acting reversible contraceptives only, or experienced fever after vaccination. Emerging evidence suggests that the endocrine transition that characterized perimenopause is associated with a rise in chronic low-grade inflammation, which in turn accelerates ovarian failure [45].
This is one of the few studies conducted worldwide to focus on the impact of COVID-19 vaccination on FMW, as well as on the potential influence of health-related factors. The sample analyzed was large enough to be statistically representative. Nevertheless, the experimental design could have influenced the detection of significant differences and causal relationships cannot be properly determined. On the other hand, the online questionnaire was not previously validated. At this point, we would like to make the following comments: first of all, the historic events derived from an unprecedented health crisis compels us to be less rigorous from a methodological point of view. By this way we and other research groups were able to sample a target population at real time and to collect a variety of variables related to women health, when official reports did not yet reflect the emerging phenomenon. Second, self-reported data potentially represent errors such as recall bias or self-selection; nevertheless, self-reports are considered the gold standard for menstrual cycle data and useful for rapidly identifying potential signals or rare adverse events. As in similar studies, our findings here might not be applicable to other countries than Spain, due to some of the above-mentioned reasons. Taking into account all of the above, we agree that a longitudinal and multinational study could help to establish the cause-effect relationship and to clarify the factors influencing the occurrence of alterations in the menstrual cycle after COVID-19 vaccination.
5. Conclusions
Our findings, together with previous evidence, highlight the need to further investigate the current prevalence of menstrual disturbances in women after receiving COVID-19 vaccine or any other vaccine, as well as the physiological mechanisms involved and their relationship with the hypothalamus-pituitary-gonadal axis. From our point of view, such investigations should in no case feed anti-vaccine theories, but rather serve to confirm the need that this and other side effects can no longer be overlooked in clinical trials. Research on the safety of COVID-19 vaccination on women´s health, whatever their reproductive circumstances, is necessary to apply a gender perspective in clinical research, an issue largely neglected. This evidence could help health professionals to provide scientifically up-to-date information to their patients, empowering them to choose the best option for their reproductive decisions, especially in those societies where menstrual health is still a taboo.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
MG and MA have contributed to this manuscript equally. Conceptualization: CC, ABR, MA; Methodology: CC, ABR, MA; Investigation: MG, CC, ABR; Visualization: CC, ABR; Supervision: CC, ABR; Writing—original draft: MG, CC; Writing—review & editing: MG, CC, ABR, MA.
Funding
This work was supported by the Regional Government of Extremadura-ERDF funds under Grant BBB021- GR21042; Dermofarm S.A. under research agreement with the University of Extremadura (ref. 431/22). Neither the government agency nor the sponsoring company have played a role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of University of Extremadura (ref. 180/2021).
Informed Consent Statement
An informed consent was only obtained from those who agree to be contacted via email by the research group for additional data collection.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions.
Acknowledgments
The research team would like to thank all the participants who have collaborated in the study in an unselfish manner.
Conflicts of Interest
Authors declare that they have no competing interests.
References
- Silveira MM, Garcia Moreia GMS, Mendonça M. DNA vaccines against COVID-19: Perspectives and challenges. Life Sci 2021; 267. [CrossRef]
- Sharma O, Sultan AA, Ding H, et al. A Review of the Progress and Challenges of Developing a Vaccine for COVID-19. Front Immunol 2020; 11: 585354. [CrossRef]
- Mostaghimi D, Valdez CN, Larson HT, et al. Prevention of host-to-host transmission by SARS-CoV-2 vaccines. Lancet Infect Dis 2022; 22(2): e52–e58. [CrossRef]
- Puhach O, Adea K, Hulo H, et al. Infectious viral load in unvaccinated and vaccinated individuals infected with ancestral, Delta or Omicron SARS-CoV-2. Nat Med 2022; 28(7): 1491–1500. [CrossRef]
- Singanayagam A, Hakki S, Dunning J, et al. ATACCC Study Investigators. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study. Lancet Infect Dis 2022; 22(2): 183–195. [CrossRef]
- Lopez Bernal J, Andrews N, Gower C, et al. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. N Engl J Med 2021;385(7):585-594. [CrossRef]
- Medicines and Healthcare Products Regulatory Agency (MHRA). “Coronavirus vaccine—summary of yellow card reporting” (United Kingdom, 2022; https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting).
- Spanish Agency of Medicines and Medical Devices (AEMPS). “17th COVID-19 vaccines pharmacovigilance report” (Government of Spain, 2022; https://www.aemps.gob.es/informa/17o-informe-de-farmacovigilancia-sobre-vacunascovid-19/).
- Therapeutic Goods Administration (TGA). “COVID-19 vaccine safety report” (Australia Government, 2022; https://www.tga.gov.au/news/covid-19-vaccine-safety-reports/covid-19-vaccine-safety-report-06-10-2022).
- Male V. Menstrual changes after covid-19 vaccination. BMJ. 2021;374:n2211. [CrossRef]
- Morgan EP. “Periods: why women’s menstrual cycles have gone haywire”. The Guardian, March 25, 2021. https://www.theguardian.com/society/2021/mar/25/pandemic-periods-why-womens-menstrual-cycles-have-gone-haywire.
- Brumfiel G. “Why reports of menstrual changes after COVID vaccine are tough to study”. National Public Radio, August 9, 2021. https://www.npr.org/sections/health-shots/2021/08/09/1024190379/covid-vaccine-period-menstrual-cycle-research.
- Robinson O, Schraer R. “Covid vaccine: Period changes could be a short-term side effect”. British Broadcasting Corporation, May 13, 2021. https://www.bbc.com/news/health-56901353.
- Trogstad L, Laake I, Robertson AH, et al. “Increased incidence of menstrual changes among young women after coronavirus vaccination” (Norwegian Institute of Public Health, 2021; www.fhi.no/en/studies/ungvoksen/increased-incidence-of-menstrual-changes-among-young-women/).
- Vaccine Adverse Event Reporting System (VAERS). “NOT-HD-21-035: notice of special interest (NOSI) to encourage administrative supplement applications to investigate COVID-19 vaccination and menstruation (admin supp clinical trial optional)” (United States Government, 2021; https://grants.nih.gov/grants/guide/notice-files/NOT-HD-21-035.html).
- Edelman A, Boniface ER, Benhar E, et al. Association Between Menstrual Cycle Length and Coronavirus Disease 2019 (COVID-19) Vaccination: A U.S. Cohort. Obstet Gynecol 2022;139(4):481-489. [CrossRef]
- Baena-García L, Aparicio VA, Molina-López A, et al. Premenstrual and menstrual changes reported after COVID-19 vaccination: The EVA project. Womens Health (Lond) 2022; 18:17455057221112237. [CrossRef]
- Critchley HOD, Babayev E, Bulun SE, et al. Menstruation: science and society. Am J Obstet Gynecol 2020;223(5):624-664. [CrossRef]
- Sharp GC, Fraser A, Sawyer G, et al. The COVID-19 pandemic and the menstrual cycle: research gaps and opportunities. Int J Epidemiol 2022;51(3):691-700. [CrossRef]
- Muhaidat N, Alshrouf MA, Azzam MI, et al. Menstrual Symptoms After COVID-19 Vaccine: A Cross-Sectional Investigation in the MENA Region. Int J Womens Health 2022; 14:395-404. [CrossRef]
- Rodríguez Quejada L, Toro Wills MF, Martínez-Ávila MC, et al AF. Menstrual cycle disturbances after COVID-19 vaccination. Womens Health (Lond) 2022; 18:17455057221109375. [CrossRef]
- Wang S, Mortazavi J, Hart JE, et al. A prospective study of the association between SARS-CoV-2 infection and COVID-19 vaccination with changes in usual menstrual cycle characteristics. Am J Obstet Gynecol 2022;227(5): 739.e1–739.e11. [CrossRef]
- Alvergne A, Woon EV, Male V. Effect of COVID-19 vaccination on the timing and flow of menstrual periods in two cohorts. Front Reprod Health 2022; 4:952976. [CrossRef]
- Edelman A, Boniface ER, Male V, et al. Association between menstrual cycle length and covid-19 vaccination: global, retrospective cohort study of prospectively collected data. BMJ Med 2022;1(1): e000297. [CrossRef]
- Lee KMN, Junkins EJ, Luo C, et al. Investigating trends in those who experience menstrual bleeding changes after SARS-CoV-2 vaccination. Sci Adv 2022;8(28): eabm7201. [CrossRef]
- Dabbousi AA, El Masri J, El Ayoubi LM, et al. Menstrual abnormalities post-COVID vaccination: a cross-sectional study on adult Lebanese women. Ir J Med Sci 2022; 26:1–8. [CrossRef]
- Laganà AS, Veronesi G, Ghezzi F, et al. Evaluation of menstrual irregularities after COVID-19 vaccination: Results of the MECOVAC survey. Open Med (Wars) 2022;17(1):475-484. [CrossRef]
- Abdollahi A, Naseh I, Kalroozi F, et al. Comparison of Side Effects of COVID-19 Vaccines: Sinopharm, AstraZeneca, Sputnik V, and Covaxin in Women in Terms of Menstruation Disturbances, Hirsutism, and Metrorrhagia: A Descriptive-Analytical Cross-Sectional Study. Int J Fertil Steril 2022;16(3):237-243. [CrossRef]
- Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), “Amenorrhea” (United States Government, 2021; https://www.nichd.nih.gov/health/topics/amenorrhea).
- Lord M, Sahni M. “Secondary Amenorrhea” in StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing (2022). https://www.ncbi.nlm.nih.gov/books/NBK431055.
- Male V. Effect of COVID-19 vaccination on menstrual periods in a retrospectively recruited cohort. medRxiv 2021. [CrossRef]
- Ministry of Health. “COVID-19 vaccination strategy” (Government of Spain, 2022; https://www.vacunacovid.gob.es).
- MM Al-Mehaisen L, A Mahfouz I, Khamaiseh K, et al. Short Term Effect of Corona Virus Diseases Vaccine on the Menstrual Cycles. Int J Womens Health 2022; 14:1385-1394. [CrossRef]
- Sualeh M, Uddin MR, Junaid N, et al. Impact of COVID-19 Vaccination on Menstrual Cycle: A Cross-Sectional Study From Karachi, Pakistan. Cureus 2022;14(8): e28630. [CrossRef]
- Li K, Chen G, Hou H, et al. Analysis of sex hormones and menstruation in COVID-19 women of child-bearing age. Reprod Biomed Online 2021;42(1):260-267. [CrossRef]
- Perricone C, Ceccarelli F, Nesher G, et al. Immune thrombocytopenic purpura (ITP) associated with vaccinations: a review of reported cases. Immunol Res 2014;60(2-3):226-35. [CrossRef]
- Merchant H. CoViD-19 post-vaccine menorrhagia, metrorrhagia or postmenopausal bleeding and potential risk of vaccine-induced thrombocytopenia in women. BMJ 2021;18.
- Kurmanova AM, Kurmanova GM, Lokshin VN. Reproductive dysfunctions in viral hepatitis. Gynecol Endocrinol 2016;32(sup2):37-40. [CrossRef]
- Centers for Disease Control and Prevention (CDC). “Updated Recommendations from the Advisory Committee on Immunization Practices for Use of the Janssen (Johnson & Johnson) COVID-19 Vaccine After Reports of Thrombosis with Thrombocytopenia Syndrome Among Vaccine Recipients — United States, April 2021” (United States Government, 2021; https://www.cdc.gov/mmwr/volumes/70/wr/mm7017e4.htm?s_cid=mm7017e4_w).
- Long B, Bridwell R, Gottlieb M. Thrombosis with thrombocytopenia syndrome associated with COVID-19 vaccines. Am J Emerg Med 2021; 49:58-61. [CrossRef]
- Islam A, Bashir MS, Joyce K, et al. An Update on COVID-19 Vaccine Induced Thrombotic Thrombocytopenia Syndrome and Some Management Recommendations. Molecules 2021;26(16):5004. [CrossRef]
- Schoenbaum EE, Hartel D, Lo Y, et al. HIV infection, drug use, and onset of natural menopause. Clin Infect Dis 2005;41(10):1517-24. [CrossRef]
- Liaquat A, Huda Z, Azeem S, et al. Post-COVID-19 vaccine-associated menstrual cycle changes: A multifaceted problem for Pakistan. Ann Med Surg (Lond) 2022; 78:103774. [CrossRef]
- Popkin BM, Du S, Green WD, et al. Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obes Rev; 21(11):e13128. Epub 2020 Aug 26. Erratum in: Obes Rev 2021;22(10): e13305. [CrossRef]
- McCarthy M, Raval AP. The peri-menopause in a woman's life: a systemic inflammatory phase that enables later neurodegenerative disease. J Neuroinflammation 2020;17(1):317. [CrossRef]
Figure 1.
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) flow diagram.
Figure 1.
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) flow diagram.
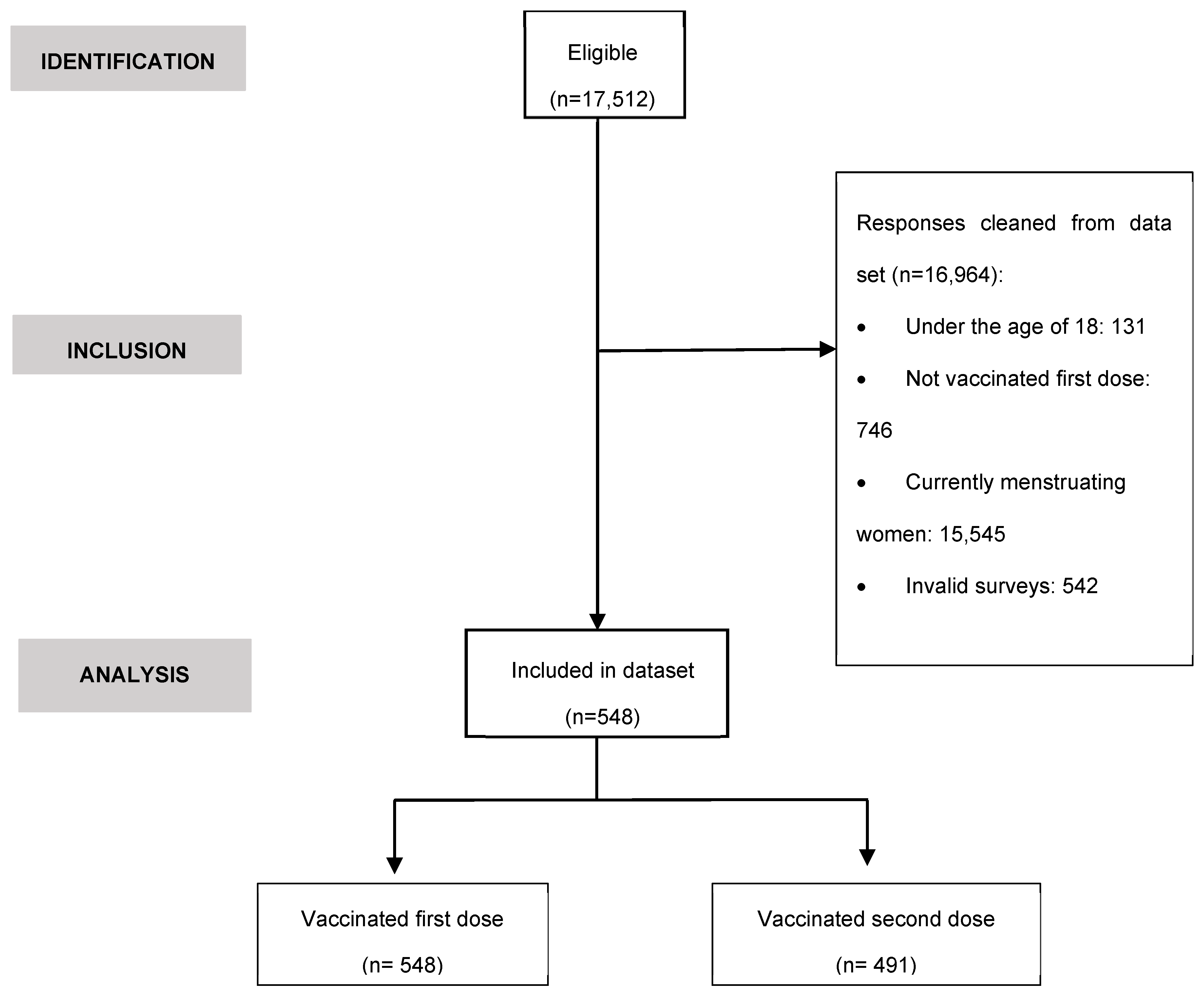
Figure 2.
Comparison between the frequencies (%) obtained for the variables linked to MRD after the administration of doses 1 and 2 of the SARS-CoV-2 vaccine (formerly menstruating women, N=548).
Figure 2.
Comparison between the frequencies (%) obtained for the variables linked to MRD after the administration of doses 1 and 2 of the SARS-CoV-2 vaccine (formerly menstruating women, N=548).
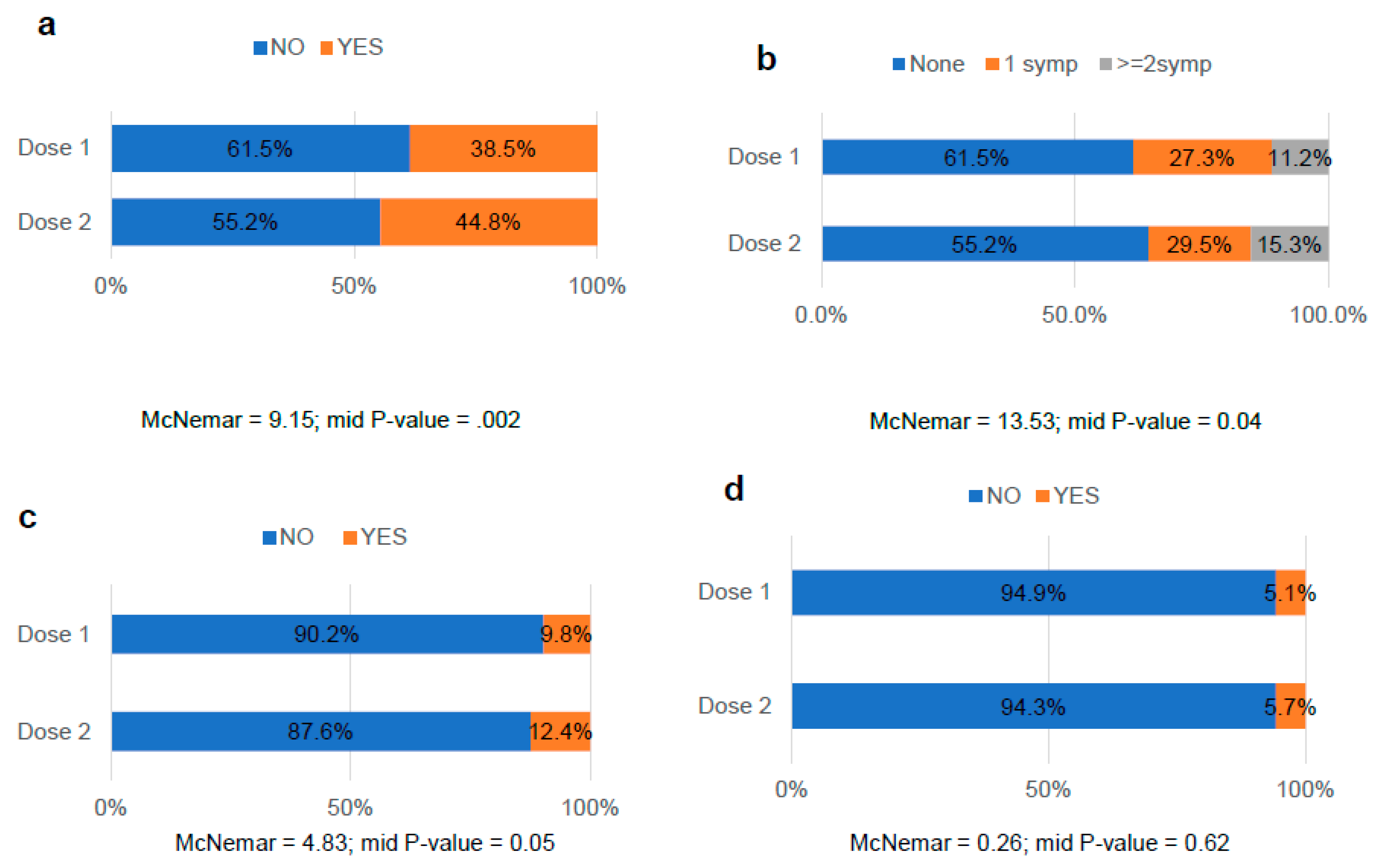
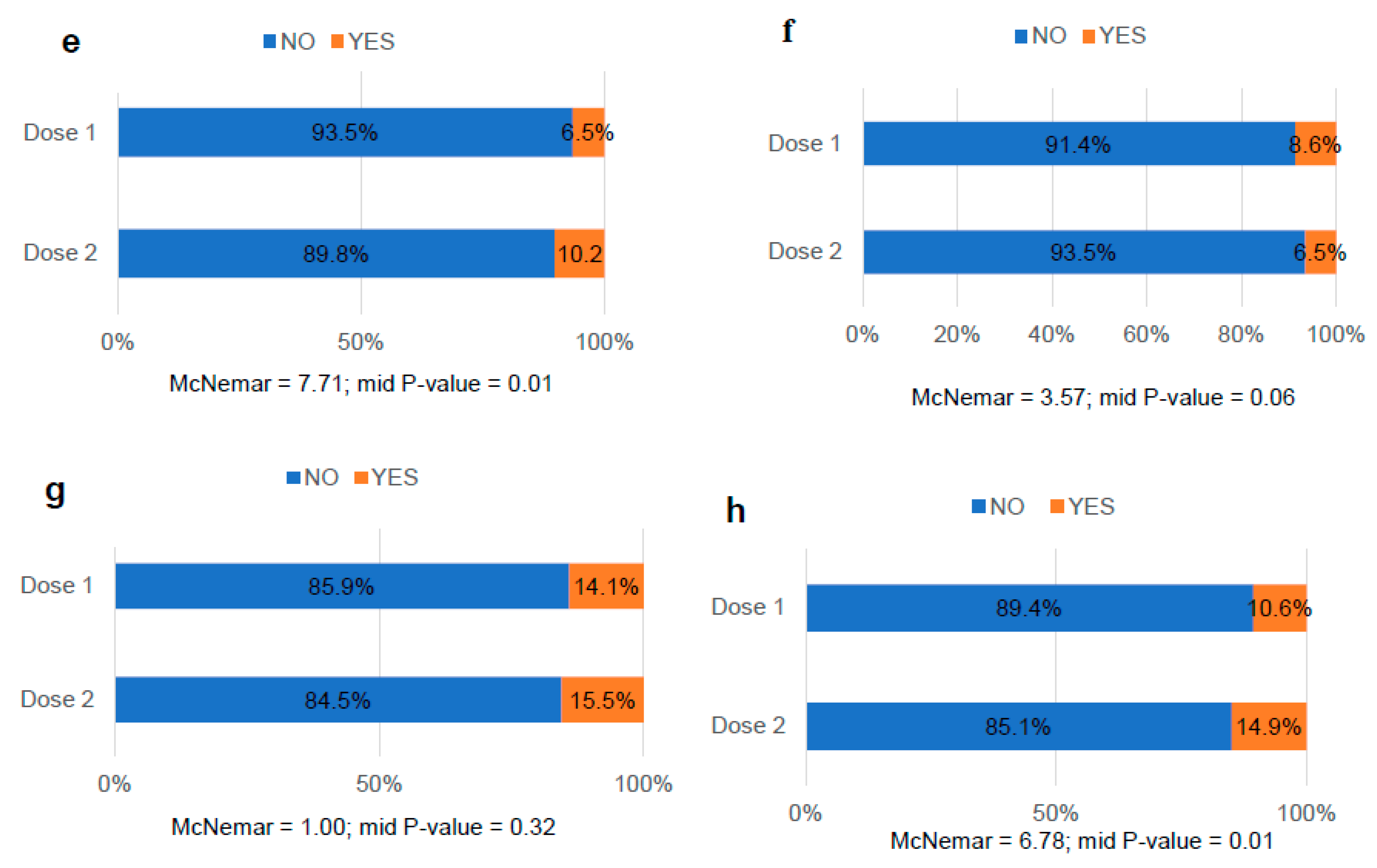
Figure 3.
Comparison between the frequencies (%) obtained for the variables linked to menstrual bleeding changes after the administration of doses 1 and 2 of the SARS-CoV-2 vaccine (formerly menstruating women, N= 548). a. Length; b. Flow; c. Abnormal bleeding; d. Duration of menstrual bleeding changes.
Figure 3.
Comparison between the frequencies (%) obtained for the variables linked to menstrual bleeding changes after the administration of doses 1 and 2 of the SARS-CoV-2 vaccine (formerly menstruating women, N= 548). a. Length; b. Flow; c. Abnormal bleeding; d. Duration of menstrual bleeding changes.
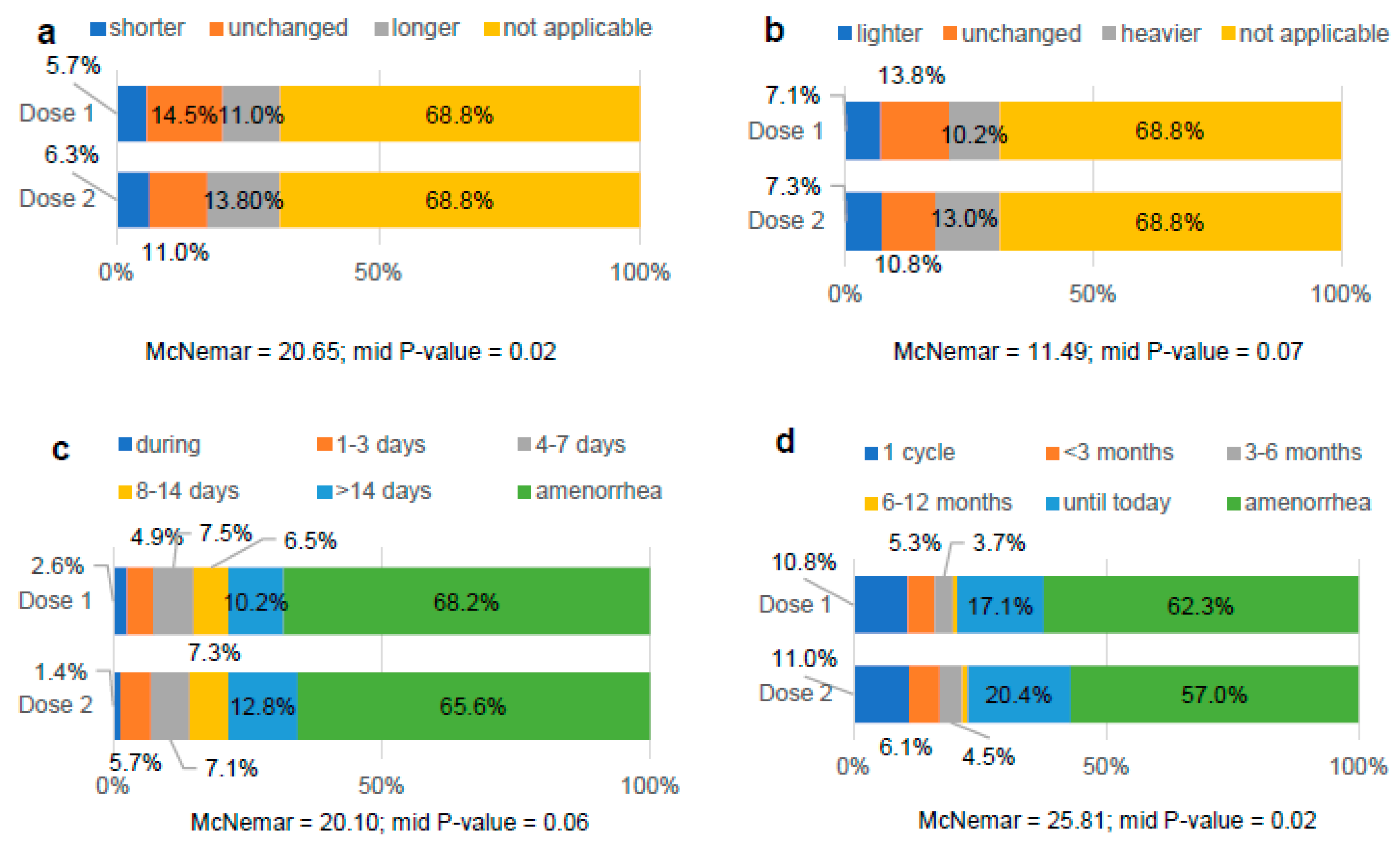
Figure 4.
Comparison between the frequencies (%) obtained for the variables related to the side effects after the administration of doses 1 and 2 of the SARS-CoV-2 vaccine (formerly menstruating women, N= 548). a. Occurrence of side effects; b. Number of side effects; c. Arm pain; d. Fatigue; e. Fever; f. Headache; g. Nauseas; h. Breast lumps; i. Swollen glands; j. Other side effects.
Figure 4.
Comparison between the frequencies (%) obtained for the variables related to the side effects after the administration of doses 1 and 2 of the SARS-CoV-2 vaccine (formerly menstruating women, N= 548). a. Occurrence of side effects; b. Number of side effects; c. Arm pain; d. Fatigue; e. Fever; f. Headache; g. Nauseas; h. Breast lumps; i. Swollen glands; j. Other side effects.
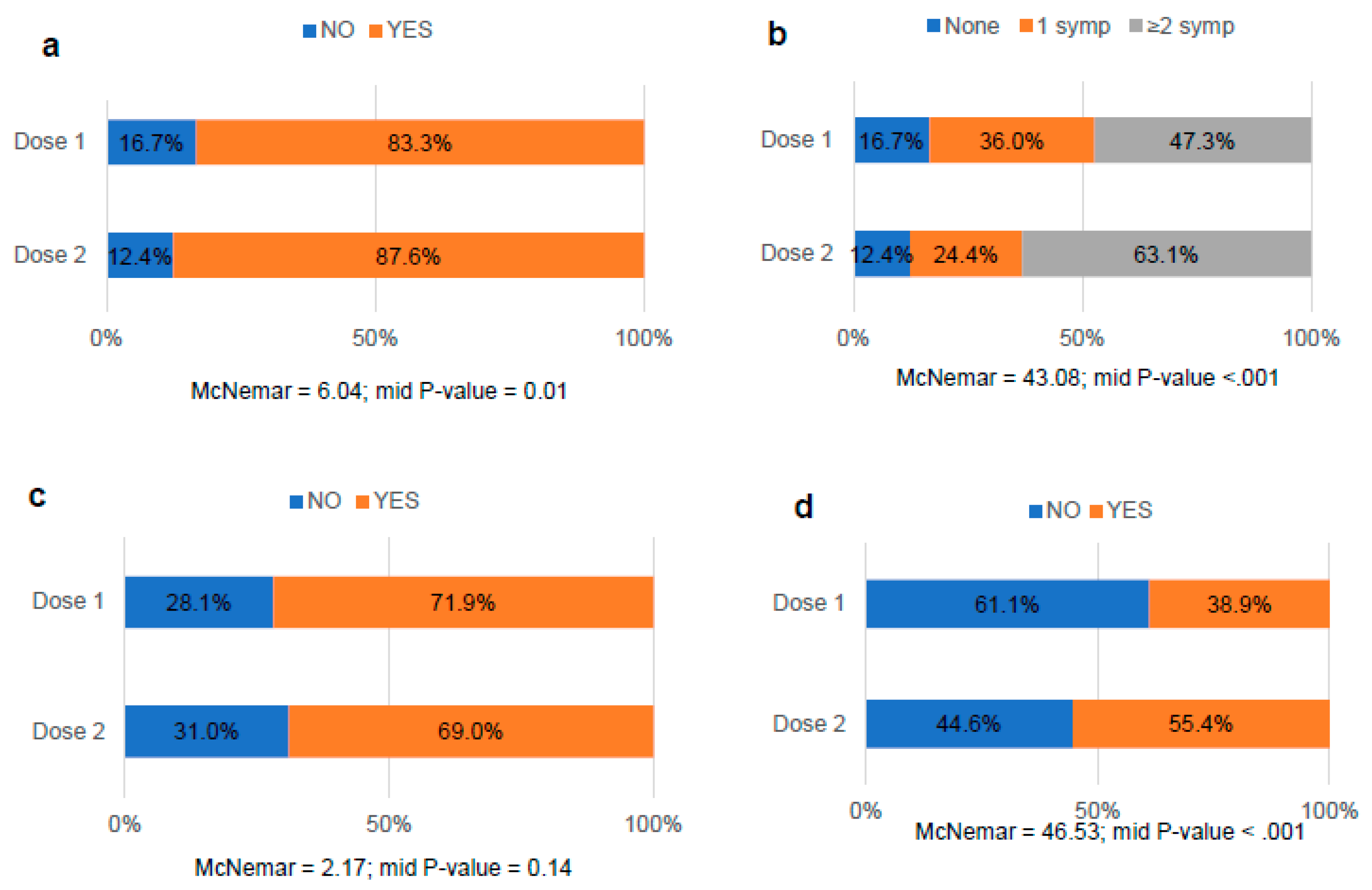
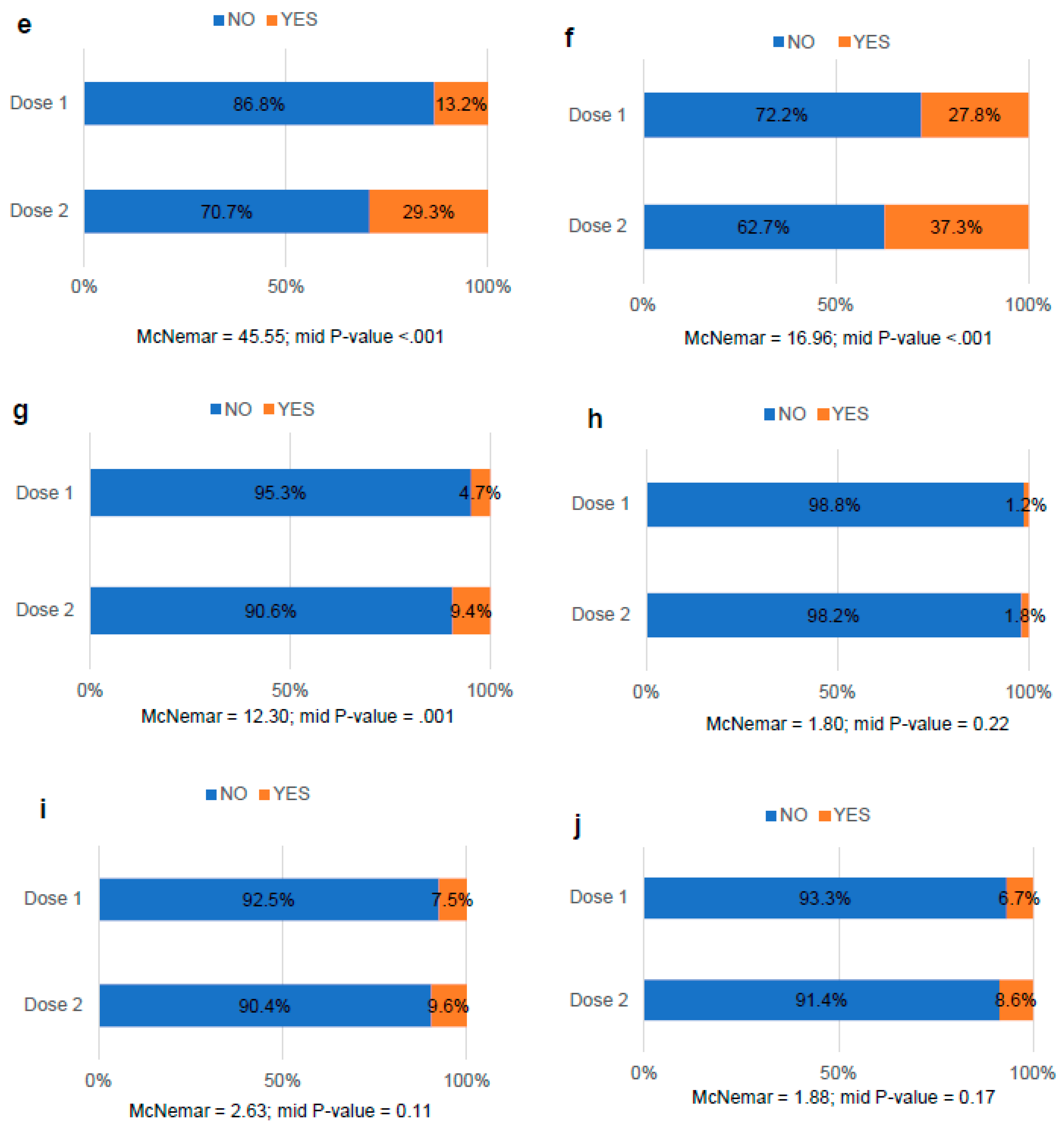

Table 1.
Anthropometric characteristics and medical history of the study population (formerly menstruating women, N=548).
Table 1.
Anthropometric characteristics and medical history of the study population (formerly menstruating women, N=548).
| Variable | Category | Total (N=548) | |
|---|---|---|---|
| Age (years)a | - | 40.4±10.7 | |
| Weight (kg) a | - | 67.3±15.3 | |
| Height (cm)a | - | 164.2±6.3 | |
| BMI a,b | - | 25.0±5.5 | |
| Underweight | 32 (5.8) | ||
| Normal weight | 295 (53.8) | ||
| Pre-obesity/overweight | 118 (21.5) | ||
| Obesity I | 67 (12.2) | ||
| Obesity II | 21 (3.8) | ||
| Obesity III | 9 (1.6) | ||
| Medical history a,b | |||
| Autoimmune diseases | Diagnosis | Yes | 68 (12.4) |
| No | 480 (87.6) | ||
| Comorbidity | Yes | 5 (7.4) | |
| No | 63 (92.6) | ||
| Types | Thyroid | 31 (5.4) | |
| Gastrointestinal | 14 (2.4) | ||
| Dermatological | 11 (1.9) | ||
| Rheumatic/articular | 7 (1.2) | ||
| None of the above | 7 (1.2) | ||
| Other clinical conditions | Diagnosis | Yes | 136 (25.0) |
| No | 407 (75.0) | ||
| Comorbidity | Yes | 39 (27.7) | |
| No | 102 (72.3) | ||
| Types | Gynecological | 30 (22.1) | |
| Cancer | 19 (14.0) | ||
| Neurological/mental | 17 (12.5) | ||
| Rheumatic/articular | 16 (11.8) | ||
| Gastrointestinal | 14 (10.3) | ||
| Respiratory | 14 (10.3) | ||
| Thyroid | 13 (9.6) | ||
| Dermatological | 6 (4.4) | ||
| HPV | 8 (5.9) | ||
| Cardiovascular | 7 (5.1) | ||
| None of the above | 37 (27.2) | ||
| Allergies | Diagnosis | Yes | 190 (34.7) |
| No | 358 (63.3) | ||
| COVID-19 | Diagnosis | Yes | 72 (13.1) |
| No | 476 (86.9) | ||
| Gynecological history a,b | |||
| Menarcheal age | 12.6±1.5 | ||
| Amenorrhea | Causes | Contraceptives | 162 (29.6) |
| Postmenopause | 95 (17.3) | ||
| Perimenopause | 92 (17.3) | ||
| Breastfeeding | 81 (14.8) | ||
| Hysterectomy | 7 (1.3) | ||
| None of the above | 111 (1.3) | ||
| Current/past use of contraceptives | Time of use | < 10 years | 161 (79.3) |
| > 10 years | 42 (20.7) | ||
| Types | None | 341 (62.2) | |
| Hormonal | 150 (27.4) | ||
| IUD (nonhormonal) | 57 (10.4) | ||
| Reproduction | Have you been pregnant? | Yes | 330 (60.2) |
| No | 218 (39.8) | ||
| Nº pregnancies | 0-2 | 470 (86.1) | |
| >2 | 76 (13.1) | ||
| Nº children | 0-2 | 523 (95.4) | |
| >2 | 25 (4.6) | ||
| Diseases | Diagnosis | Yes | 298 (54.4) |
| No | 250 (45.6) | ||
| Comorbidity | Yes | 70 (23.4) | |
| No | 229 (76.6) | ||
| Types | PCOS | 110 (36.8) | |
| Heavy menstrual bleeding | 105 (35.1) | ||
| Endometriosis | 57 (19.1) | ||
| Fibroids | 30 (10.1) | ||
| Menorrhagia | 21 (7.0) | ||
| Adenomyosis | 10 (3.3) | ||
| Uterine bleeding | 9 (3.0) | ||
| None of the above | 53 (17.7) |
Values are expressed as: a mean ± standard deviation; b n (%). Abbreviations: IUD, Intrauterine Device; BMI, Body Mass Index; PCOS, Polycystic Ovary Syndrome; HPV, Human Papillomavirus.
Table 2.
COVID-19 vaccination of the study population (formerly menstruating women, N=548), according to the dose received.
Table 2.
COVID-19 vaccination of the study population (formerly menstruating women, N=548), according to the dose received.
| Variable | Category | Dose 1 (n=548) | Dose 2 (n=491) |
|---|---|---|---|
| Vaccination | Yes | 517 (94.6) | 491 (89.6) |
| No | 31 (5.4) | 57 (10.4) | |
| Brand | Pfizer-BioNTech | 373 (68.1) | 352 (71.7) |
| Moderna | 95 (17.3) | 89 (18.1) | |
| Oxford-AstraZeneca | 54 (9.9) | 48 (9.8) | |
| None of the above | 26 (4.7) | 2 (0.4) |
Table 3.
Differences in the study variables according to the dose received (1 and 2) and the occurrence or not of MRD after COVID-19 vaccination (formerly menstruating women, N=548).
Table 3.
Differences in the study variables according to the dose received (1 and 2) and the occurrence or not of MRD after COVID-19 vaccination (formerly menstruating women, N=548).
| Dose1 | Dose2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Category | n-MRD (n=335) | MRD (n=213) | X2 | P-value | n-MRD (n=271) | MRD (n=220) | X2 | P-value | |
| Age (years)a | - | 40.6±11.1 | 40.0±9.9 | - | 0.66 | 40.4±11.6 | 40.2±9.7 | - | 0.91 | |
| Weight (kg)a | - | 65.4±24.5 | 70.3±15.9* | - | <.001 | 65.9±15.1 | 69.5±15.6• | - | 0.01 | |
| Height (cm)a | - | 163.9±6.2 | 164.6±6.3 | - | 0.18 | 164.0±6.0 | 164.4±6.5 | - | 0.78 | |
| BMI a,b | - | 24.3±5.2 | 26.0±5.8* | - | <.001 | 24.4±5.4 | 25.8±5.7• | - | 0.00 | |
| Underweight | 26 (7.8) | 6 (2.8)† | 13.96 | 0.03 | 18 (6.6) | 10 (4.5) | 7.46 | 0.28 | ||
| Normal weight | 190 (56.7) | 105 (49.3) | 153 (56.5) | 105 (47.7) | ||||||
| Pre-obesity /overweight | 66 (19.7) | 52 (24.4) | 55 (20.3) | 54 (24.5) | ||||||
| Obesity I | 37 (11.0) | 30 (14.1) | 28 (10.3) | 34 (15.5) | ||||||
| Obesity II | 10 (3.0) | 11 (5.2) | 9 (3.3) | 11 (5.0) | ||||||
| Obesity III | 3 (0.9) | 6 (2.8) | 4 (1.5) | 4 (1.8) | ||||||
| Medical history b | ||||||||||
| Autoimmune diseases | Types | Thyroid | 14 (4.2) | 17 (8.0) | 0.08 | 0.77 | 14 (5.2) | 15 (6.8) | 0.00 | 0.99 |
| Dermatological | 5 (1.5) | 6 (2.8) | 0.01 | 0.91 | 3 (1.1) | 6 (2.7) | 0.96 | 0.33 | ||
| Gastrointestinal | 5 (1.5) | 9 (4.2) | 0.91 | 0.34 | 6 (2.2) | 7 (3.2) | 0.03 | 0.86 | ||
| Rheumatic / articular | 3 (0.9) | 4 (1.9) | 0.06 | 0.81 | 2 (0.7) | 4 (1.8) | 0.60 | 0.44 | ||
| None of the above | 4 (1.2) | 3 (1.4) | 0.32 | 0.57 | 4 (1.5) | 3 (1.4) | 0.24 | 0.62 | ||
| Other clinical conditions | Types | Gynecological | 21 (6.3) | 9 (4.2) | 1.05 | 0.31 | 15 (5.5) | 13 (5.9) | 0.03 | 0.86 |
| Cancer | 13 (3.9) | 6 (2.8) | 0.44 | 0.51 | 11 (4.1) | 7 (3.2) | 0.27 | 0.61 | ||
| Neurological / mental | 8 (2.4) | 9 (4.2) | 1.46 | 0.23 | 5 (1.8) | 12 (5.5)† | 4.73 | 0.03 | ||
| Thyroid | 8 (2.4) | 5 (2.3) | .001 | 0.98 | 6 (2.2) | 5 (2.3) | 0.00 | 0.97 | ||
| Gastrointestinal | 7 (2.1) | 8 (3.8) | 1.36 | 0.24 | 7 (2.6) | 5 (2.3) | 0.05 | 0.83 | ||
| Respiratory | 7 (2.1) | 7 (3.3) | 0.75 | 0.39 | 5 (1.8) | 6 (2.7) | 0.43 | 0.51 | ||
| Dermatological | 6 (1.8) | 2 (0.9) | 0.66 | 0.42 | 4 (1.5) | 4 (1.8) | 0.09 | 0.77 | ||
| Cardiovascular | 5 (1.5) | 2 (0.9) | 0.66 | 0.42 | 4 (1.5) | 4 (1.8) | 0.09 | 0.77 | ||
| Rheumatic / articular | 5 (1.5) | 12 (5.6)• | 7.43 | 0.01 | 4 (1.5) | 12 (5.5)• | 6.10 | 0.01 | ||
| HPV | 5 (1.5) | 3 (1.4) | .006 | 0.94 | 2 (0.7) | 3 (1.4) | 0.47 | 0.49 | ||
| None of the above | 20 (6.0) | 18 (8.5) | 1.24 | 0.27 | 11 (4.1) | 21 (9.5)• | 6.00 | 0.01 | ||
| Allergies | - | 106 (31.6) | 84 (39.4) | 3.49 | 0.06 | 94 (34.7) | 74 (33.6) | 0.06 | 0.81 | |
| COVID-19 | - | 43 (12.8) | 29 (13.6) | 0.07 | 0.79 | 19 (7.0) | 13 (5.9) | 0.24 | 0.62 | |
| Gynecological history a,b | ||||||||||
| Menarcheal age | - | 12.7±1.4 | 12.5±1.7 | - | 0.18 | 12.6±1.5 | 12.6±1.6 | - | 0.69 | |
| Current/past use of contraceptives | Time of use | < 10 years | 88 (26.3) | 73 (34.3) | 0.32 | 0.57 | 61 (22.5) | 87 (39.5) | 3.43 | 0.06 |
| >10 years | 25 (7.5) | 17 (8.0) | 21 (7.7) | 15 (6.8) | ||||||
| Types | None | 219 (65.4) | 122 (57.3) | 3.63 | 0.16 | 186 (68.6) | 117 (53.2)• | 12.68 | .002 | |
| Hormonal | 84 (25.1) | 66 (31.0) | 60 (22.1) | 77 (35.0)• | ||||||
| IUD (nonhormonal) | 32 (9.6) | 25 (11.7) | 25 (9.2) | 26 (11.8) | ||||||
| Reproduction | Have you ever been pregnant? | Yes | 204 (60.9) | 126 (59.2) | 0.165 | 0.69 | 156 (57.6) | 134 (60.9) | 0.562 | 0.45 |
| No | 131 (39.1) | 87 (40.8) | 115 (42.4) | 86 (39.1) | ||||||
| Nº pregnancies | 0-2 | 290 (86.6) | 180 (84.5) | 0.399 | 0.53 | 234 (86.3) | 189 (85.9) | 0.014 | 0.91 | |
| >2 | 44 (13.1) | 32 (15.0) | 36 (13.3) | 6 (2.7) | ||||||
| Nº children | 0-2 | 314 (93.7) | 209 (98.1)• | 5.765 | 0.02 | 255 (94.1) | 214 (97.3) | 2.863 | 0.09 | |
| >2 | 21 (6.3) | 4 (1.9) | 16 (5.9) | 6 (2.7) | ||||||
| Amenorrhea | Types | Perimenopause | 41 (12.2) | 51 (23.9)* | 17.054 | <0.001 | 33 (12.2) | 47 (21.4)• | 10.596 | 0.01 |
| Postmenopause | 70 (20.9) | 25 (11.7)* | 57 (21.0) | 29 (13.2)• | ||||||
| None of the above | 224 (66.9) | 137 (64.3) | 181 (66.8) | 144 (65.5)• | ||||||
| Diseases | Types | Adenomyosis | 7 (2.1) | 3 (1.4) | 0.337 | 0.56 | 5 (1.8) | 5 (2.3) | 0.111 | 0.74 |
| PCOS | 67 (20.0) | 43 (20.2) | 0.003 | 0.96 | 61 (22.5) | 40 (18.2) | 1.392 | 0.24 | ||
| Heavy menstrual bleeding | 57 (17.0) | 48 (22.5) | 2.562 | 0.11 | 44 (16.2) | 53 (24.1)† | 4.726 | 0.03 | ||
| Endometriosis | 30 (9.0) | 27 (12.7) | 1.934 | 0.16 | 21 (7.7) | 29 (13.2)† | 3.918 | 0.05 | ||
| Fibroids | 20 (6.0) | 10 (4.7) | 0.420 | 0.52 | 16 (5.9) | 13 (5.9) | 0.000 | 0.99 | ||
| Menorrhagia | 14 (4.2) | 7 (3.3) | 0.282 | 0.60 | 13 (4.8) | 7 (3.2) | 0.811 | 0.37 | ||
| Uterine bleeding | 7 (2.1) | 2 (0.9) | 1.067 | 0.30 | 7 (2.6) | 2 (0.9) | 1.891 | 0.17 | ||
| None of the above | 37 (11.0) | 16 (7.5) | 1.860 | 0.17 | 28 (10.3) | 20 (9.1) | 0.212 | 0.65 | ||
| Side effects b | Types | Arm pain | 231 (69.0) | 167 (78.4)† | 5.847 | 0.02 | 180 (66.4) | 159 (72.3) | 1.946 | 0.16 |
| Fatigue | 126 (37.6) | 101 (47.4)† | 5.160 | 0.02 | 139 (51.3) | 133 (60.5)† | 4.126 | 0.04 | ||
| Headache | 78 (23.3) | 81 (38.0)* | 13.863 | <0.001 | 88 (32.4) | 95 (43.4)† | 5.957 | 0.02 | ||
| Fever | 41 (12.2) | 33 (15.5) | 1.181 | 0.28 | 76 (28.0) | 68 (30.9) | 0.481 | 0.49 | ||
| Swollen glands | 15 (4.5) | 27 (12.7)* | 12.367 | <0.001 | 18 (6.6) | 29 (13.2)• | 6.000 | 0.01 | ||
| Nauseas | 8 (2.4) | 20 (9.4)* | 13.166 | <0.001 | 20 (7.4) | 26 (11.9) | 2.817 | 0.09 | ||
| Breast lumps | 0 (0.0) | 7 (3.3)* | 11.125 | 0.001 | 0 (0.0) | 9 (4.1)* | 11.293 | 0.001 | ||
| None of the above | 19 (5.7) | 19 (8.9) | 2.129 | 0.15 | 22 (8.1) | 20 (9.1) | 0.147 | 0.70 | ||
Values are expressed as: a mean ± standard deviation; b n (%). *P≤.001; • P≤0.01; † P≤0.05 vs. n-MRD. Abbreviations: BMI, Body Mass Index; HPV, Human Papillomavirus; IUD, Intrauterine Device; MRD, menstrual-related disturbances subgroup; n-MRD, non-menstrual-related disturbances subgroup; PCOS, Polycystic Ovary Syndrome.
Table 4.
Factors associated with the occurrence of MRD after receiving the first dose of COVID-19 vaccine (formerly menstruating women, N= 548): binary logistic regression.
Table 4.
Factors associated with the occurrence of MRD after receiving the first dose of COVID-19 vaccine (formerly menstruating women, N= 548): binary logistic regression.
| Dose 1 | |||
|---|---|---|---|
| Variable | Category | MRD (n=213) AOR (CI 95%) | P-value |
| Weight | - | 1.02 (1.01-1.03) | <.001 |
| OCC rheumatic/articular | No | 0.31 (0.10-1.00) | 0.05 |
| Yes | 1 | ||
| Nº children | ≥ 2 | 0.25 (0.07-0.82) | 0.02 |
| 0-2 | 1 | ||
| Amenorrhea | Perimenopause | 2.28 (1.37-3.77) | .001 |
| Postmenopause | 0.74 (0.43-1.28) | 0.28 | |
| None of the above | 1 | ||
| Side effects | |||
| Arm pain | No | 0.61 (0.39-0.95) | 0.03 |
| Yes | 1 | ||
| Headache | No | 0.53 (0.35-0.80) | .003 |
| Yes | 1 | ||
| Swollen glands | No | 0.29 (0.15-0.59) | .001 |
| Yes | 1 | ||
| Nauseas | No | 0.35 (0.14-0.86) | 0.02 |
| Yes | 1 | ||
Note: reference subgroup n-MRD. AOR: adjusted odd radio; CI 95%: confidence interval. MRD: menstrual-related disturbances subgroup; OCC: other clinical conditions.
Table 5.
Factors associated with the occurrence of MRD after receiving the second dose of COVID-19 (formerly menstruating women, N = 491): binary logistic regression.
Table 5.
Factors associated with the occurrence of MRD after receiving the second dose of COVID-19 (formerly menstruating women, N = 491): binary logistic regression.
| Dose 2 | |||
|---|---|---|---|
| Variable | Category | MRD (n=220) AOR (CI 95%) | P-value |
| Alterations dose 1 | Yes | 13.88 (8.66-22.08) | <.001 |
| No | 1 | ||
| Contraceptives | Hormonal | 2.70 (1.54-4.76) | .001 |
| IUD | 1.85 (0.86-3.99) | 0.12 | |
| None | 1 | ||
| Amenorrhea | Perimenopause | 2.07 (1.06-4.06) | 0.03 |
| Postmenopause | 1.17 (0.60-2.29) | 0.64 | |
| None of the above | 1 | ||
| Arm pain | No | 0.64 (0.40-1.02) | 0.06 |
| Yes | 1 | ||
Note: reference subgroup n-MRD. AOR: adjusted odd radio; CI 95%: confidence interval. MRD: menstrual-related disturbances subgroup; IUD: intrauterine device.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



