
Submitted:
16 July 2025
Posted:
18 July 2025
You are already at the latest version
Abstract
Background/Objective: Prenatal cytogenetic testing is essential for pregnancies at high risk of chromosomal abnormalities. While conventional karyotyping detects large aneuploidies and structural rearrangements (>5–10 Mb), chromosomal microarray analysis (CMA) identifies smaller copy number variants (CNVs), increasing diagnostic yield by approximately 5%. CMA is now recommended as the first-tier test for evaluating fetal structural anomalies detected by ultrasound. Method: From March 2023 to September 2024, 344 prenatal samples were analyzed using conventional karyotyping and SNP-based CMA. Karyotyping was performed via flask culture, and CMA was conducted using the Infinium Global Screening Array Cyto (GSA-Cyto) on the Illumina iScan platform. CNVs were interpreted using NxClinical v6.0 and curated databases including ClinVar, DECIPHER, OMIM, ClinGen, and others. Results were aligned to the GRCh37/hg19 reference genome. Results: Chromosomal abnormalities were identified in 57/344 cases (16.5%). Of these, 39 were numerical chromosomal anomalies and 18 were pathogenic or likely pathogenic CNVs. Notably, 11 CNVs (3.2%) were undetectable by conventional karyotyping, emphasizing the added value of CMA. Conclusion: CMA enhances prenatal diagnostic accuracy by detecting submicroscopic CNVs that are not visible with conventional methods, supporting its routine use in prenatal genetic evaluation.
Keywords:
microarray analysis
; prenatal diagnosis
; amniocentesis
; chorionic villus sampling
; fetal blood sampling
1. Introduction
Conventional cytogenetic analyses are typically offered as the first option in prenatal diagnosis to couples at high risk of having a child with a chromosomal abnormality. However, conventional cytogenetic analyses can detect aneuploidy and large chromosomal rearrangements of 5–10 megabases (Mb) in size. Thanks to advances in prenatal cytogenetic diagnosis, in recent years, fluorescence in situ hybridization (FISH) and chromosomal microarray analysis (CMA) have begun to be used in addition to conventional cytogenetic analyses. Recently, chromosomal microarray (CMA), CGH array, or SNP array (depending on the internal technology used in their design and reading) have been added to the group of genomic tools used in genetic diagnosis. Chromosomal microarray analysis (CMA) is a cytogenetic molecular technique that can detect microscopic and submicroscopic chromosomal abnormalities smaller than 5 Mb with high sensitivity in patients. Specifically, SNP CMA can identify genetic changes as small as 50–100 kilobases (kb). This enables CMA to provide approximately 100 times higher resolution compared to conventional karyotyping, depending on the probe spacing and platform used. The ability to examine the genome at this high resolution has led to the discovery of widespread copy number variations (CNVs) in the human genome, including polymorphic variations in healthy individuals and novel pathogenic copy number imbalances [1]. This has had a major impact on genetic diagnosis over the past decade [2]. Furthermore, CMA provides additional clinically useful information in approximately 5% (range: 2.3–8.3%) of cases [3,4]. While CMA provides higher resolution information compared to conventional cytogenetic analyses, it cannot detect low-level mosaicism and balanced chromosomal rearrangements. In addition, it can lead to the detection of chromosomal variants of uncertain significance (VOUS) and present challenges in interpreting these findings. With the more frequent use of genome-wide and high-resolution array platforms, the prevalence of VOUS is steadily increasing.
A high-risk pregnancy may be indicated by factors such as risk determination in prenatal maternal serum screening (MSS) tests, advanced maternal age (AMA), intrauterine growth restriction (IUGR), increased nuchal translucency (NT), the detection of a structural anomaly in a prenatal ultrasound, a family history of chromosomal abnormalities, and risk determination in NIPT tests. CMA has become the first-tier technique for genetic follow-up when structural anomalies are detected in prenatal ultrasound [5].
The detection rate of pathogenic copy number variations (CNVs) can vary depending on the indication for prenatal diagnosis. For example, studies have reported pathogenic CNVs at a rate of 0–15.0% in fetuses with increased nuchal translucency (NT; ≥2.5 to 3.5 mm, corresponding to the 95th to 99th percentile in the general population) or cystic hygroma [6,7] whereas this rate has been reported as high as 18–22% in all cases of coronary heart disease (CHD). Among pregnancies with CHD, the most common causes are trisomy 21 and 18, along with 22q11 microdeletion [8,9]. Other frequently affected organ systems associated with pathogenic CMA results are the skeletal system, genitourinary system, and central nervous system [10,11,12]. There is limited information regarding the incidence of clinically significant CNVs in fetuses with ultrasound soft marker abnormalities such as echogenic intracardiac focus (EICF), mild ventriculomegaly, enlarged cisterna magna, choroid plexus cysts (CPCs), thickened nuchal fold, echogenic bowel, mild hydronephrosis and in pregnant women who undergo invasive prenatal testing due to other indications such as advanced maternal age (AMA), abnormal MSS results, and abnormal Non-Invasive Prenatal Test (NIPT) results. Additionally, no studies from Turkey have been found that include a cohort of this size. In this study, we report a retrospective cohort study of 344 high-risk pregnancies that underwent prenatal diagnosis at our center using G-banding karyotyping along with CMA. These analyses were performed due to the observation of a structural anomaly during prenatal diagnosis or the suspicion of a high-risk pregnancy.
2. Materials and Methods
2.1. Ethics
The research received ethical approval from the Ankara Etlik City Hospital Scientific Research Evaluation and Ethics Committee with the document number: AESH-BADEK-2024-876.
In this study, the chromosomal microarray analysis (CMA) results of high-risk pregnancies that underwent prenatal diagnosis at Ankara Etlik City Hospital between March 2023 and September 2024 were evaluated. As of now, 344 pregnant women have undergone CMA as part of their prenatal diagnosis, and various chromosomal anomalies have been detected in 57 patients. The data used in the research will only include genetic report results, and access will be restricted to researchers. The identities of the patients included in the study will remain confidential.
2.2. Inclusion Criteria:
- Patients with an indication for prenatal CMA due to prenatal maternal serum screening (MSS) tests risk with increased NT, advanced maternal age (AMA), intrauterine growth restriction (IUGR), increased nuchal translucency (NT), the detection of a structural anomaly or a soft marker in a prenatal ultrasound, a family history of chromosomal abnormalities, and risk determination in NIPT tests.
- Patients who signed an informed consent form agreeing to undergo prenatal genetic testing.
2.3. Exclusion Criteria:
- Patients with biochemical risks in prenatal screening but without increased nuchal translucency, prenatal USG abnormalities, or parental karyotype anomalies are required for a prenatal CMA indication.
- Patients who did not sign the informed consent form and declined prenatal genetic testing.
2.4. Parameters to be Examined:
- Presence of possible aneuploidy
- Presence of possible microdeletions/microduplications
- Mosaicism
- Uniparental disomy (UPD)
2.5. Karyotype Analysis:
Samples obtained from patients, such as chorionic villus sampling (CVS), amniocentesis (AS), or fetal cordocentesis, depending on gestational age, were subjected to cell culture via the flask method for genetic testing.
2.6. CMA Analysis:
In patients meeting the inclusion criteria, chromosomal microarray analysis (CMA) was performed in addition to conventional cytogenetic analysis. For this purpose, DNA was first isolated from prenatal samples. Maternal DNA was also isolated by obtaining a peripheral blood sample from the mother. The isolated DNAs were compared to exclude maternal contamination, and CMA analysis was then initiated. Chromosomal microarray analysis was performed using Infinium Global Screening Array Cyto (GSA-Cyto) chips on the Illumina iScan platform. Copy number variations were detected and visualized using the NxClinical (v.6.0) analysis software developed by Biodiscovery. The relevant genomic positions were reported based on the Human Genome Build 37 (GRCh37/hg19) reference assembly. The obtained DATA were evaluated using current databases, including PubMed, OMIM, DGV, ClinVar, DECIPHER, and ClinGen.
2.7. Statistical Analysis:
Statistical analysis of the DATA in the study was performed using SPSS 25 for Windows and the R programming language. Quantitative variables (discrete or continuous numerical variables) were expressed as mean and standard deviation when they showed normal distribution, otherwise as median and interquartile range (IQR). Qualitative (nominal and ordinal) variables were explained using numbers and percentages. Ordinal variables were arranged in the table according to their hierarchical order.
3. Results
Pregnant women enrolled in the study were aged 17 to 45 years, with an average age of 30.66 years, and they were 9–33 weeks pregnant, with an average of ~19.93 ± 1.63 weeks. A total of 344 prenatal samples were analyzed by chromosomal microarray analysis (CMA). The clinical indications for testing included abnormal ultrasound findings, congenital anomalies, multiple anomalies, increased nuchal translucency (NT), central nervous system (CNS) anomalies, skeletal anomalies, biochemical risk, family history, hydrops fetalis, positive non-invasive prenatal testing (NIPT) results, advanced maternal age (AMA), cystic hygroma, intrauterine growth restriction (IUGR), and amniotic fluid abnormalities (anhydramnios/oligohydramnios). The distribution of abnormal findings according to clinical indications is summarized in Table 1.
Overall, chromosomal abnormalities were detected in 57 cases, corresponding to a total abnormality detection rate of 16.5% (The screenshots of the abnormal results have been included as supplemental material.). Among these, 18 cases involved pathogenic or likely pathogenic copy number variations (P/LP CNVs) and 39 cases involved numerical chromosomal abnormalities (aneuploidies). A total of 11 cases with CNVs that could not be detected by conventional cytogenetic analysis were identified (Table 2).
The distribution of chromosomal abnormalities across different clinical indications is visually summarized in Figure 1. The highest diagnostic yield was observed in the cystic hygroma group, where chromosomal abnormalities were identified in 83% of cases. This was followed by cases with high-risk non-invasive prenatal testing (NIPT) results (58%) and those presenting with multiple sonographic findings (26%). Notably, the group with congenital heart disease (CHD) showed a substantial yield of 37%, whereas increased nuchal translucency (NT) and central nervous system (CNS) anomalies yielded lower detection rates of 15% and 8.8%, respectively (Table 3).
Among the 41 cases with ultrasound abnormalities, abnormalities were detected in 7.3%, including two pathogenic CNVs and one aneuploidy. Congenital anomalies were identified in 39 cases, with a 5.3% abnormality rate.
Notably, in the group with multiple sonographic findings (n=38), the abnormality rate increased significantly to 26%, highlighting the cumulative risk when multiple structural anomalies are present. Multiple sonographic findings are detailed in Table 4.
In the hydrops fetalis group (n=15), chromosomal abnormalities were detected in two cases (14%), both corresponding to aneuploidies. No pathogenic findings were identified in cases with isolated IUGR (n=5) or amniotic fluid abnormalities (n=3).
Among the 19 cases tested due to biochemical risk factors, two chromosomal abnormalities were detected (10.5%). In the "other" category, including cases with positive family history (n=18), the abnormality rate was 17%.
In the AMA group (n=21), only one chromosomal abnormality was detected (4.7%), suggesting a relatively lower diagnostic yield when AMA was the sole indication for testing.
These results underscore the clinical value of chromosomal microarray analysis (CMA) particularly in pregnancies with multiple or specific sonographic anomalies, while also emphasizing the lower likelihood of pathogenic findings in isolated or less specific indications.
4. Discussion
Array-based methods, especially SNP microarrays, are frequently used in prenatal diagnosis. SNP-microarray can detect > 1 kb microdeletions and microduplications with a higher resolution than karyotyping and does not require cell culture. In 2013, the American College of Obstetrics and Gynecology (ACOG) recommended the use of CMA instead of traditional karyotyping for invasive prenatal diagnosis when one or more ultrasound anomalies are detected in the fetüs [13]. In this study, we analyzed the results of 344 prenatal SNP-microarray cases to assess the abnormal findings associated with different prenatal diagnosis indications, and we showed that CMA could detect an additional (11/344, 3.2%) genetic abnormalities compared to karyotype analysis. This rate has been considered consistent with previous studies [4,5]. The overall abnormal rate in our cohort was 16.5%, with pathogenic/likely pathogenic copy number variants (P/LP CNVs) detected in 5.2% of cases and aneuploidy identified in 11.3%. In a study conducted by Wapner et al., more than 4,000 samples from 29 centers were analyzed, and cases that were reported as having normal karyotypes by conventional methods were re-evaluated using CMA [3]. As a result, small deletions and duplications (CNVs) were identified in 6% of the cases. The study concluded that CMA is beneficial in diagnosing aneuploidies and unbalanced rearrangements but may be insufficient for detecting balanced translocations and triploidy. In a review by Callaway et al., CMA was applied to pregnant women who had normal results from conventional karyotyping [14]. The rate of CNV detection ranged between 0.8% and 5.5%, with an average rate of 2.4%. In these pregnant women, the incidence of abnormal fetal ultrasound (US) findings ranged from 6.0% to 11.1%, with an average of 6.5%. The review also included an analysis of pregnant women with abnormal fetal US findings and reported that CNVs were detected in 7% of fetuses with abnormal US. Based on these findings, the authors suggested that CMA could be recommended as a first-tier test. In a study conducted in Turkey involving 320 patients, the CNV detection rate was reported to be 12.3% [15]. The abnormality rates varied significantly depending on clinical indications, highlighting the differential diagnostic yield of prenatal microarray analysis across different risk categories.
In our study, among the highest detection rates, cystic hygroma (83%) and high-risk NIPT results (58%) showed the strongest correlation with chromosomal abnormalities. These findings are consistent with previous studies suggesting that cystic hygroma is frequently associated with aneuploidy, particularly Turner syndrome and trisomy 21, 18, or 13 [16]. Similarly, the high diagnostic yield in cases with abnormal NIPT results underscores the efficacy of NIPT as a screening tool for common chromosomal aneuploidies.
Cases with multiple indications (26%) and those with major structural anomalies such as central nervous system (CNS) abnormalities (8.8%), as well as cases with increased nuchal translucency (15%), showed a higher abnormality rate. This highlights the importance of detailed fetal ultrasound evaluation in guiding prenatal genetic testing. The presence of congenital anomalies as a standalone indication yielded a lower diagnostic rate (5.3%). Given that congenital anomalies are generally known to have multifactorial inheritance, this finding is not surprising (Figure 2).
As expected, cases with skeletal anomalies (3.8%) showed a relatively lower rate of abnormal findings. This may reflect the limitations of chromosomal microarray in detecting single-gene disorders or non-structural genetic etiologies associated with these phenotypes. Similarly, intrauterine growth restriction (IUGR) and anhydramnios/oligohydramnios cases did not yield any abnormal microarray results in our cohort. This may be due to the limited sample size of our cohort, which consists of only 344 patients. However, it should also be considered that such conditions may result from multifactorial inheritance or non-genetic etiologies.
Our findings emphasize the importance of selecting appropriate prenatal genetic testing strategies based on clinical indications. In cases with ultrasound (USG) findings in addition to prenatal diagnosis indications such as biochemical risk or advanced maternal age, CMA should be planned simultaneously with prenatal diagnosis. While microarray analysis provides higher-resolution chromosomal anomaly detection and a more precise phenotype expectation, complementary approaches such as whole-exome sequencing (WES) or targeted gene panels may be required in cases with suspected monogenic disorders. Additionally, the identification of P/LP CNVs in certain cases highlights the necessity of accurate genetic counseling to discuss potential implications for fetal prognosis and familial recurrence risks.
As far as we know, our study is the largest and most comprehensive conducted in Türkiye. Future studies with larger cohorts, along with the integration of CMA methods into the prenatal diagnosis process, will be crucial for further refining the prenatal diagnostic approach. Our results contribute to the growing body of evidence supporting the role of prenatal microarray analysis, particularly in high-risk pregnancies with structural anomalies or positive NIPT findings.
5. Conclusion
Our study highlights the diagnostic value of prenatal chromosomal microarray analysis in a cohort of 344 cases with various clinical indications. The overall abnormality detection rate was 16.5%, with significant variations across different prenatal indications. The highest diagnostic yields were observed in cases with cystic hygroma and high-risk NIPT results, confirming the strong association between these findings and chromosomal abnormalities. In contrast, indications such as skeletal anomalies, isolated congenital anomalies, and advanced maternal age showed lower detection rates, suggesting that additional genetic testing approaches, such as whole-exome sequencing (WES) or targeted gene panels, may be necessary in selected cases.
Our findings reinforce the importance of integrating prenatal ultrasound, biochemical screening, and non-invasive prenatal testing (NIPT) results into the decision-making process for genetic testing. The identification of pathogenic and likely pathogenic CNVs in certain cases highlights the necessity of comprehensive genetic counseling to discuss clinical implications and recurrence risks.
As prenatal genetic testing continues to advance, future research involving larger cohorts and advanced genomic technologies is expected to play a crucial role in refining diagnostic strategies. Expanding the use of genome-wide sequencing approaches may enhance our ability to detect underlying genetic etiologies in fetuses with unexplained structural anomalies. Overall, our results contribute to the growing body of evidence supporting the role of prenatal microarray analysis in high-risk pregnancies and emphasize the need for a personalized, multidisciplinary approach in prenatal diagnosis.
Author Contributions
A.B., H.S., M.T.A., U.C.T., and S.S. have performed patient evaluation and data collection. All authors had full access to all of the DATA in the study, and take responsibility for the accuracy of the DATA analysis. A.B. designed the study and wrote the manuscript. A.B., H.S., M.T.A., and İ.K. contributed to editing/reviewing the final version. All authors checked and arranged the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
This research received no external funding
Institutional Review Board Statement
All of the procedures were carried out in accordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from the participants for molecular genetic analysis and the publication of patient DATA prior to their enrolment in the study. The research received ethical approval from the Ankara Etlik City Hospital Scientific Research Evaluation and Ethics Committee with the document number: AESH-BADEK-2024-876.
Informed Consent Statement
All patients were informed about the study, and verbal and written consent forms from patients or their parents were obtained.
Data Availability Statement
The DATA used and analyzed during this study are available from the corresponding author on reasonable request.
Acknowledgments
We thank the patients and their families for their participation and cooperation and for allowing us to conduct the study with their data. We also acknowledge the contributions of the clinical geneticists, laboratory technicians, and genetic counselors who were involved in the sample collection, data generation, and interpretation processes.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACOG | American College of Obstetrics and Gynecology |
| AS | Amniocentesis |
| AVSD | Atrioventricular septal defect |
| CFM | Craniofacial morphology |
| CGH | Comparative genomic hybridization |
| CHD | Coronary heart disease |
| CMA | Chromosomal microarray analysis |
| CNS | Central nervous system |
| CNV | Copy number variants |
| CPC | Choroid plexus cysts |
| CSP | Cavum septi pellucidi |
| CVS | Cardiovascular system |
| CVS | Chorionic villus sampling |
| EICF | Echogenic intracardiac focus |
| GUS | Genitourinary System |
| IUGR | Intrauterine growth restriction |
| LP | Likely pathogenic |
| MSS | Maternal serum screening |
| NIPT | Non-Invasive Prenatal Test |
| NT | Nuchal translucency |
| P | Pathogenic |
| SNP | Single nucleotide polymorphism |
| TGA | Transposition of Great Arteries |
| UPD | Uniparental disomy |
| US | Ultrasound |
| VOUS | Variants of uncertain significance |
| WES | Whole-exome sequencing |
References
- Kearney HM, Thorland EC, Brown KK, Quintero-Rivera F, South ST. American College of Medical Genetics standards and guidelines for interpretation and reporting of postnatal constitutional copy number variants. Genet Med. 2011;13(7):680-685. [CrossRef]
- Levy B, Wapner R. Prenatal diagnosis by chromosomal microarray analysis. Fertil Steril. 2018;109(2):201-212. [CrossRef]
- Wapner RJ, Martin CL, Levy B, Ballif BC, Eng CM, Zachary JM, et al. Chromosomal microarray versus karyotyping for prenatal diagnosis. N Engl J Med. 2012;367(23):2175-2184. [CrossRef]
- Zhu X, Chen M, Wang H, Guo Y, Chau MHK, Yan H, et al. Clinical utility of expanded non-invasive prenatal screening and chromosomal microarray analysis in high-risk pregnancy. Ultrasound Obstet Gynecol. 2021;57(3):459-465. [CrossRef]
- South ST, Lee C, Lamb AN, Higgins AW, Kearney HM. ACMG Standards and Guidelines for constitutional cytogenomic microarray analysis, including postnatal and prenatal applications: revision 2013. Genet Med. 2013;15(11):901-909. [CrossRef]
- Vogel I, Petersen OB, Christensen R, Hyett J, Lou S, Vestergaard EM. Chromosomal microarray as primary diagnostic genomic tool for pregnancies at increased risk within a population-based combined first-trimester screening program. Ultrasound Obstet Gynecol. 2018;51(4):480-486. [CrossRef]
- Zhang Z, Hu T, Wang J, Li Q, Wang H, Liu S. Prenatal Diagnostic Value of Chromosomal Microarray in Fetuses with Nuchal Translucency Greater than 2.5 mm. Biomed Res Int. 2019;2019:6504159. [CrossRef]
- Mademont-Soler I, Morales C, Soler A, Martínez-Crespo JM, Shen Y, Margarit E, et al. Prenatal diagnosis of chromosomal abnormalities in fetuses with abnormal cardiac ultrasound findings: evaluation of chromosomal microarray-based analysis. Ultrasound Obstet Gynecol. 2013;41(4):375-382. [CrossRef]
- Zhu X, Li J, Ru T, Wang Y, Xu Y, Yang Y, et al. Identification of copy number variations associated with coronary heart disease by chromosomal microarray analysis and next-generation sequencing. Prenat Diagn. 2016;36(4):321-327. [CrossRef]
- Huang R, Fu F, Zhou H, Zhang L, Lei T, Cheng K, et al. Prenatal diagnosis in the fetal hyperechogenic kidneys: assessment using chromosomal microarray analysis and exome sequencing. Hum Genet. 2023;142(6):835-847. [CrossRef]
- Xie X, Wu X, Su L, Cai M, Li Y, Huang H, Xu L. Application of Single Nucleotide Polymorphism Microarray in Prenatal Diagnosis of Fetuses with Central Nervous System Abnormalities. Int J Gen Med. 2021;14:4239-4246. [CrossRef]
- Donnelly JC, Platt LD, Rebarber A, Zachary J, Grobman WA, Wapner RJ. Association of copy number variants with specific ultrasonographically detected fetal anomalies. Obstet Gynecol. 2014;124(1):83-90. [CrossRef]
- On Genetics GC. Committee opinion no. 581: the use of chromosomal microarray analysis in prenatal diagnosis. Obstetrics and gynecology. 2013;122(6):1374-1377.
- Callaway JL, Shaffer LG, Chitty LS, Rosenfeld JA, Crolla JA. The clinical utility of microarray technologies applied to prenatal cytogenetics in the presence of a normal conventional karyotype: a review of the literature. Prenat Diagn. 2013;33(12):1119-1123. [CrossRef]
- Bütün Z, Kayapınar M, Şenol G, Akca E, Gökalp EE, Artan S. Comparison of conventional karyotype analysis and CMA results with ultrasound findings in pregnancies with normal QF-PCR results. 2025.
- Benn P, Cuckle H, Pergament E. Non-invasive prenatal testing for aneuploidy: current status and future prospects. Ultrasound in Obstetrics & Gynecology. 2013;42(1):15-33.
Figure 1.
Patient distribution of abnormal and normal result groups in terms of indications.
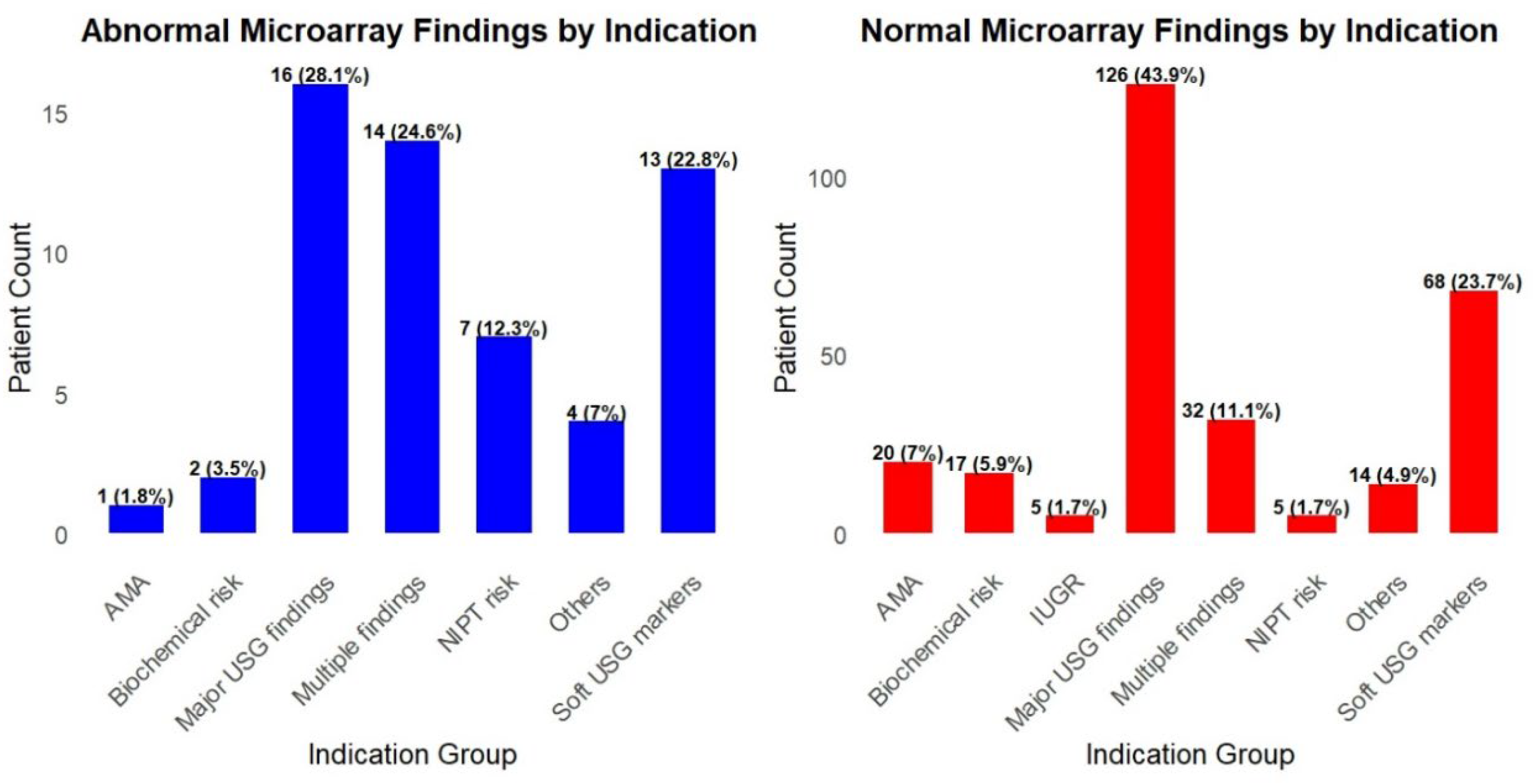
Figure 2.
Abnormal Results Rates according to the type of USG abnormalities.
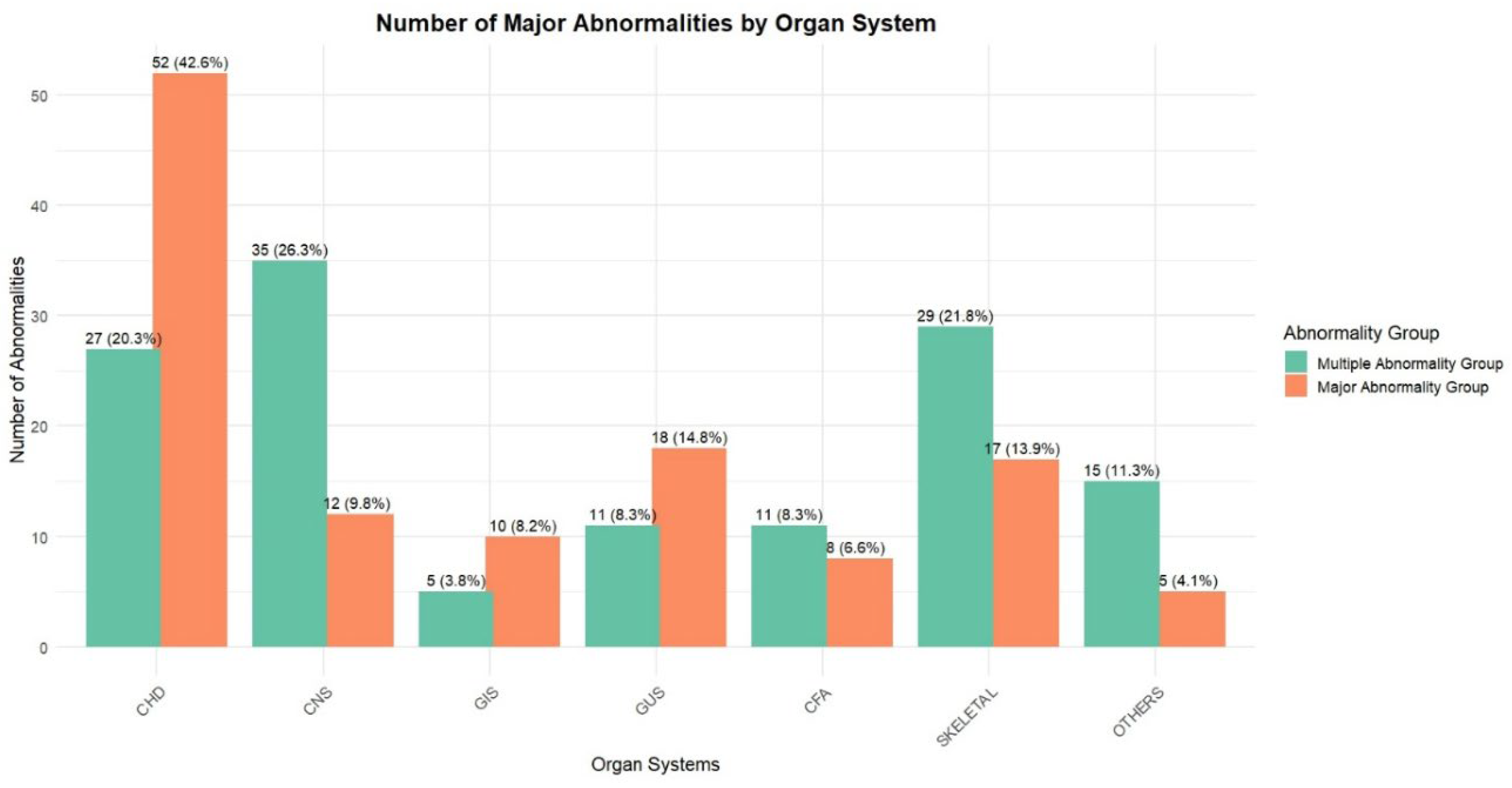

Table 1.
Abnormal results of overall patients.
| Sample | Results (Hg19) | Week | USG | Maternal Age | Group |
|---|---|---|---|---|---|
| AS | 16p13.11(14975292_16295863)x1 | 23+4 | Enlarged ventricle | 30 | USG findings |
| AS | 16p12.2p11.2(21575087_29319922)x1 | 26 | Enlarged ventricle | 35 | USG findings |
| AS | Trisomy 21 | 21+2 | Hepatic calcification, echogenic cardiac focus | 28 | USG findings |
| AS | 15q11.2(22766739_23226254)x1 | 22 | Ambiguous genitals, hydronephrosis | 20 | Congenital anomaly |
| AS | Trisomy 21 | 23+2 | Renal pyelectasis | 33 | Congenital anomaly |
| AS | Trisomy 13 | 24+3 | Ventriculomegaly, renal pyelectasis, hypospadias, coarctation of the aorta | 38 | Multiple findings |
| AS | Trisomy 18 | 30 | Anal atresia, polyhydramniosis, IUGR, single umblical artery | 24 | Multiple findings |
| AS | Trisomy 21 | 18+3 | Renal pelviectasis, AVSDa | 36 | Multiple findings |
| AS | 8p23.3p23.1(170692_12009597)x3, 9p24.3p11.2(10201_44888946)x3, 9q13q22.33(68158106_101087286)x3 | 16+6 | Cleft palate, CHD | 35 | Multiple findings |
| AS | Klinefelter Syndrome | 22 | Pulmonary stenosis, cleft lip and palate, renal pelviectasis, thymus hypoplasia | 26 | Multiple findings |
| AS | Trisomy 18 | 28 | Clenched hand, VSD | 26 | Multiple findings |
| AS | Trisomy 18 | 22 | IUGR, clench hand, mandibular hypoplasia, VSD, horseshoe kidney | 35 | Multiple findings |
| AS | Trisomy 21 | 17 | Duodenal atresia, NT:6mm | 39 | Multiple findings |
| AS | Trisomy 13 | 23 | Inferior Vermis Hypoplasia, Polyhydramnios, Mesochardia, TGAb | 37 | Multiple findings |
| Chord sample |
Trisomy 13 | 24 | Cleft Lip/Palate, Hyperecogenic Bowel, Hypoplastic Left Heart, Aortic Coarctation, Holoprosencephaly | 24 | Multiple findings |
| AS | 22q11.21(18877787_21461607)x1, Di George | 28 | Truncus Arteriosus, hypoplastic tymus, VSD | 35 | CHD |
| AS | Trisomy 21 | 21+4 | Hypoplastic nasal bone, AVSDa | 33 | CHD |
| AS | 14q32.2q32.33(99718925_107289511)x1 | 32 | Craniosynostosis, hypoplastic left heart, aortic hypoplasia, doubled collecting system of the left kidney | 25 | CHD |
| AS | Klinefelter Syndrome | 16+3 | D-TGAb | 38 | CHD |
| AS | Turner Syndrome | 25 | Aort hypoplasia | 21 | CHD |
| AS | 4p16.3p11(84414_49620838)x3, 13q11q12.11(19020095_21578150)x1 | 23+2 | Pulmonary hypoplasia, VSD, Fallot tetralogy, overriding aorta, clenched hand | 23 | CHD |
| CVS | Turner Syndrome | 14+1 | Hypoplastic left heart | 23 | CHD |
| AS | Trisomy 13 | 21+5 | AVSDa | 23 | CHD |
| AS | Trisomy 21 | 17+2 | VSD, echogenic liver focus | 37 | CHD |
| AS | 11q23.3q25(119110984_134946504)x1, 11q23.3(118545797_119103406)x3 | 22+4 | Hypoplastic left heart | 31 | CHD |
| AS | Xq27.2q28(140856453_155234707)x1, 4q28.3q35.2(134134331_190484505)x3 | 23 | VSD, truncus arteriosus, left-sided gall bladder | 33 | CHD |
| AS | Trisomy 18 | 22 | IUGR, Perimembranous VSD | 35 | CHD |
| AS | 13q21.33q33.2(73157290_105760332)x1 | 30 | Vernian hypoplasia, Pes equinovarus | 25 | CNS anomaly |
| AS | 16p11.2(29323692_30364805)x3 | 22+5 | Hydrocephaly, lemon sign, cerebellar hypoplasia, left multicyclic dysplastic kidney, Sacral meningomyelocele. | 37 | CNS anomaly |
| AS | Trisomy 21 | 16+5 | Alobar holoprosencephaly | 37 | CNS anomaly |
| CVS | Trisomy 18 | 12 | NT:7mm | 43 | Increased NT |
| CVS | Trisomy 21 | 12+5 | NT:5, Cystic hygroma | 32 | Increased NT |
| AS | 10p11.1(38784659_39150257)x1 , 10q11.22q11.23(49262918_51832748)x1 | 16 | NT 2.6 | 36 | Increased NT |
| AS | Trisomy 21 | 13+4 | NT 5, diffuse edema, echogenic cardiac focus | 38 | Increased NT |
| C.V.S | 4q31.3q35.2(155190509_191044208)x3 | 13 | NT:4mm | 39 | Increased NT |
| AS | Trisomy 13 | 18 | Polydactyly of the right foot, hyperecogenic heart | 37 | Skeletal anomaly |
| AS | Xp22.31(6453470_8126718)x0 | 15+4 | N | 23 | Biochemical risk |
| AS | 4q22.2q22.3(94006191_97808388)x1 | 17 | N | 34 | Biochemical risk |
| AS | 15q11.2(22766739_23226254)x1 | 22 | N | 20 | Other |
| AS | 47,XYY | 20+4 | CSPc | 38 | Other |
| C.V.S | 6q14.3q22.31(85761559_120871846)x1 | NA | NA | 25 | Other |
| AS | Mosaic UPD of chromosome 3 | 20 | CSPc | 41 | Other |
| AS | Trisomy 18 | 17 | Megacystit, clenched hand, hydrops, club foot, VSD | 40 | Hydrops |
| AS | Trisomy 21 | 28 | Hydrops, polyhydramniosis | 34 | Hydrops |
| AS | Yp11.31p11.2(2657176_10057648)x2,Yq11.1q11.221(13133499_19567718)x2,Yq11.222q11.223(20804835_24522333)x0 | 20 | N | 24 | NIPT risk |
| AS | Trisomy 21 | 19+2 | Fallot tetralogy | 35 | NIPT risk |
| C.V.S | Trisomy 21 | 13+5 | NIPT Tr.21 risk | 24 | NIPT risk |
| AS | 16q11.2q23.1(46501717_75493481)x3 | 14 | N | 24 | NIPT risk |
| AS | Trisomy 21 | 17 | NT:3.4MM | 17 | NIPT risk |
a Atrioventricular septal defect, b Transposition of Great Arteries, c Cavum septi pellucidi
Table 2.
Abnormal Result ratios of prenatal microarrays, where conventional karyotyping was normal.
| Results (Hg19) | Size | Detected by Karyotyping | Week | USG |
|---|---|---|---|---|
| 16p13.11(14975292_16295863)x1 | 1.32 Mb | No | 23+4 | Enlarged ventricle |
| 16p12.2p11.2(21575087_29319922)x1 | 7.74 Mb | Yes | 26 | Enlarged ventricle |
| 15q11.2(22766739_23226254)x1* | 460 Kb | No | 22 | Ambiguous genitals, hydronephrosis |
| 8p23.3p23.1(170692_12009597) x3 9p24.3p11.2(10201_44888946) x3 9q13q22.33(68158106_101087286) x3 |
11.8MB 44.8Mb 33Mb |
Yes | 16+6 | Cleft palate, CHD |
| 22q11.21(18877787_21461607)x1 | 2.583 kb | No | 28 | Truncus Arteriosus, hypoplastic tymus, VSD |
| 14q32.2q32.33(99718925_107289511)x1 | 7.5 Mb | Yes | 32 | Craniosynostosis, hypoplastic left heart, aortic hypoplasia, doubled collecting system of the left kidney |
| 4p16.3p11(84414_49620838) x3, 13q11q12.11(19020095_21578150)x1 |
49.5 Mb 2.6Mb |
Yes No |
23+2 | Pulmonary hypoplasia, VSD, Fallot tetralogy, overriding aorta, clenched hand |
| 11q23.3q25(119110984_134946504) x1 11q23.3(118545797_119103406)x3 |
15.8Mb 558Kb |
Yes No |
22+4 | Hypoplastic left heart |
| Xq27.2q28(140856453_155234707)x1 4q28.3q35.2(134134331_190484505)x 3 |
14.2Mb 56.3 Mb |
Yes | 23 | VSD, truncus arteriosus, left-sided gall bladder |
| 13q21.33q33.2(73157290_105760332)x1 | 33 Mb | Yes | 30 | Vermian hypoplasia, Pes equinovarus |
| 16p11.2(29323692_30364805)x3 | 1.04Mb | No | 22+5 | Hydrocephaly, lemon sign, cerebellar hypoplasia, left multicyclic dysplastic kidney, Sacral meningomyelocele. |
| 10p11.1(38784659_39150257) x1, 10q11.22q11.23(49262918_51832748)x1 |
366Kb 2.6 Mb |
No | 16 | NT 2.6 |
| 4q31.3q35.2(155190509_191044208)x3 | 36Mb | Yes | 13 | NT:4mm |
| Xp22.31(6453470_8126718)x0 | 1.7Mb | No | 15+4 | N |
| 4q22.2q22.3(94006191_97808388)x1 | 3.8Mb | No | 17 | N |
| 15q11.2(22766739_23226254)x1* | 460 Kb | No | 22 | N |
| 6q14.3q22.31(85761559_120871846)x1 | 35.1 Mb | Yes | NA | NA |
| Mosaic UPD of whole chromosome 3 | No | 20 | CSP | |
| Yp11.31p11.2(2657176_10057648)x2, Yq11.1q11.221(13133499_19567718)x2, Yq11.222q11.223(20804835_24522333)x0 |
7.4Mb 6.4 Mb 3.7Mb |
Yes | 20 | N |
| 16q11.2q23.1(46501717_75493481)x3 | 29Mb | Yes | 14 | N |
Table 3.
Detection Rates of Chromosomal Abnormalities According to Clinical Indications.
| Indications | N | Abnormal | P/LP CNV | Aneuploidi | Abnormal Rate (%) |
|---|---|---|---|---|---|
| USG findings | 41 | 3 | 2 | 1 | 0.073 |
| Congenital anomaly | 39 | 2 | 1 | 1 | 0.053 |
| Multiple indications | 38 | 10 | 1 | 9 | 0.26 |
| CHD | 35 | 13 | 5 | 8 | 0.37 |
| CNS anomaly | 34 | 3 | 2 | 1 | 0.088 |
| Increased NT | 33 | 5 | 2 | 3 | 0.15 |
| Skeletal anomaly | 26 | 1 | - | 1 | 0.038 |
| Biochemical risk1 | 19 | 2 | 1 | 1 | 0.105 |
| Other (Family history) | 18 | 3 | 2 | 1 | 0.17 |
| Hydrops | 15 | 2 | - | 2 | 0.14 |
| NIPT risk | 12 | 7 | 2 | 5 | 0.58 |
| AMA | 21 | 1 | - | 1 | 0.047 |
| Cystic hygroma | 6 | 5 | - | 5 | 0.83 |
| IUGR | 5 | - | - | - | 0 |
| Anhydramnios/oligohydramnios | 3 | - | - | - | 0 |
| Total | 344 | 57 | 18 | 39 | 0.165 |
Table 4.
Multiple congenital anomaly distribution according to systems.
| CVS* | CNS* | GUS* | GIS* | CFM* | Skeletal | Others | |
|---|---|---|---|---|---|---|---|
| P1 | Ilial atresia | Pelviectasis | |||||
| P2 | Cleft palate | Nasal bone: 6MM | |||||
| P3 | Coarctation of the aorta | Eophageal atresia, | Hypoplastic radius and ulna, left hemihypoplasia | ||||
| P4 | Ventriculomegaly, | Pelviectasis | |||||
| P5 | Ventriculomegaly, ARSA | ||||||
| P6 | Ventriculomegaly, Coarctation of the aorta |
Renal pyelectasis, hypospadias |
|||||
| P7 | VSD | NT:5.5 | |||||
| P8 | Hemivertebra | NT:5.5 | |||||
| P9 | Echogenic intracardiac focus, VSD | NT:6 mm | |||||
| P10 | Single umbilical artery | Anal atresia | Polyhydramniosis | IUGR | |||
| P11 | AVSD | Renal pelviectasis | |||||
| P12 | Hypoplastic left heart | Hydrops | |||||
| P13 | Occipital cephalocele, Corpus callosum dysgenesis, spina bifida | Hypoplastic thorax | NT:9 mm, IUGR | ||||
| P14 | CHD | Cleft palate | |||||
| P15 | Club foot, clenched hand | Hydrops fetalis | |||||
| P16 | Pulmonary stenosis | Renal pelviectasis | cleft lip and palate | Thymus hypoplasia | |||
| P17 | Muscular vsd | Renal pelviectasis, | |||||
| P18 | Hypoplastic left heart, | Tubular hypoplasia | |||||
| P19 | Aortic arch anomaly, | Tethered cord, CSP | |||||
| P20 | pulmonary artery hypoplasia | Omphalocele | Polyhydramnios | Clenched hands | |||
| P21 | Coarctation of the aorta, Ebstein anomaly | Hydrops fetalis | |||||
| P22 | VSD | Clenched hand | |||||
| P23 | Omphalocele | Hydrops fetalis | |||||
| P24 | VSD | Horseshoe kidney | mandibular hypoplasia | Clenched hand | IUGR | ||
| P25 | Renal pelviectasis, polyhydramniosis |
||||||
| P26 | Echogenic cardiac focus, VSD | Oligohydroamniosis | |||||
| P27 | VSD | Clenched hand, rocker bottom feet | |||||
| P28 | Ventriculomegaly, | Hydrocephalus | Clench Hand, Pes Echinovarus, | Cystic Hygroma, Pleural Effusion | |||
| P29 | Tetralogy Of Fallot | Encephalocele | Hypertelorism | ||||
| P30 | Echogenic cardiac focus | NT: 6.2 mm | |||||
| P31 | Tricuspid Atresia, Right Ventricular Hypoplasia, | Polyhydroamniosis | Diaphragmatic Hernia | ||||
| P32 | Subarachnoid hemorrhage, AMA | Edema,Hydrops fetalis, | |||||
| P33 | Unilateral cardiac ventriculomegaly, VSD | Polyhydroamniosis | |||||
| P34 | Bilateral pes equinovarus, narrow thorax | NT:7.71mm | |||||
| P35 | Ectopia Cordis | Omphalocele | Cystic Hygroma, NT:6.3mm | ||||
| P36 | Encephalocele | NT:6mm | |||||
| P37 | Choroid plexus cyst | Echogenic bowel | , NT:4mm | ||||
| P38 | Ventriculomegaly | cleft lip | |||||
| P39 | Bilateral pes equinovarus, narrow thorax | NT:7.71mm | |||||
| P40 | Duodenal atresia | NT:6mm | |||||
| P41 | Mesocardia, TGA | Inferior Vermis Hypoplasia | Polyhydramnios | ||||
| P42 | Hypoplastic Left Heart, Aortic Coarctation, | Holoprosophechaly | Hyperecogenic Bowel | Cleft Lip/Palate | |||
| P43 | Truncus Arteriosus, VSD | Hypoplastic tymus | |||||
| P44 | Pulmonary stenosis, Fallot tetralogy, right aortic arch, | Hypoplasia of the thymus | |||||
| P45 | Hypoplastic left heart, aortic hypoplasia, | Double collecting system of the left kidney | Craniosynostosis | ||||
| P46 | Pulmonary hypoplasia, VSD, Fallot tetralogy, overriding aorta | Clenched hand | |||||
| P47 | VSD, truncus arteriosus | Left-sided gall bladder |
*CVS: Cardiovascular System, CNS: Central Nervous System, GUS: Genitourinary System, CFM: Craniofacial Morphology
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



