
Submitted:
17 July 2025
Posted:
17 July 2025
You are already at the latest version
Abstract
Anatomic liver resection (AR) is a surgical technique that aims to completely remove the tumor-bearing portal territory (PT) and improve the oncological efficacy of hepatocellular carcinoma (HCC). However, the classical AR technology system has some limitations in achieving this goal. Indocyanine green (ICG) fluorescence laparoscopy is an emerging technology that can accurately delineate the PT and guide the AR. However, the evidence of its efficacy compared to conventional laparoscopy is scarce. This systematic review and meta-analysis aims to compare the effectiveness of laparoscopy and ICG fluorescence laparoscopy in AR for HCC patients. This systematic review was registered on the International Prospective Register of Systematic Reviews platform (ID: CRD42023456121). Empirical research comparing perioperative effectiveness between ICG fluorescence laparoscopy and conventional laparoscopy published from inception to 26th November 2023 in several academic literature databases was included. Cochrane risk-of-bias tool (RoB) and the Newcastle-Ottawa scale (NOS) were used for study quality evaluations. Information on clinical characteristics, operative, postoperative, prognosis, and pathological outcomes was retrieved for review. Publication bias and heterogeneity were tested for each outcome. The effect size odds ratio (OR) and standard mean difference (SMD) were calculated and synthesized. The quality of evidence was evaluated using the GRADE system. A total of 13 studies were included. Clinical characteristics were comparable between the ICG fluorescence laparoscopy group and the conventional laparoscopy group. Compared with conventional laparoscopy, ICG fluorescence laparoscopy is associated with superior short- and long-term clinical outcomes in HCC patients undergoing hepatectomy. Especially in the aspects of reduced intraoperative blood loss (SMD=-0.743, P=0.002), decreased risks of blood transfusion (OR=0.459, P=0.004), and shorter postoperative hospitalization times (SMD=-0.391, P<0.001). ICG fluorescence laparoscopy also showed implications for fewer postoperative complications (OR=0.657, P=0.071), higher R0 resection rates (OR=3.013, P=0.068), greater margin distances (SMD=0.559, P=0.072), and longer recurrence-free survival, although these findings were not statistically significant and require further investigation. ICG fluorescence laparoscopy is a safe and effective technique for AR in HCC patients. It can achieve accurate and complete resection of tumor-bearing PT and Glisson systems, as well as preserve the function and venous outflow of the future remaining liver. This study provides valuable evidence to support the clinical application of ICG fluorescence laparoscopy in AR for HCC.
Keywords:
hepatocellular carcinoma
; laparoscopic portal territory staining guided anatomic liver resection
; indocyanine green fluorescence laparoscopy
; systematic review
1. Introduction
Primary liver cancer is the fourth most common malignant tumor and the third leading cause of cancer-related mortality worldwide in 2020[1]. Hepatocellular Carcinoma (HCC) accounts for nearly 90% of primary liver cancers, with a relatively insidious onset, which has posed a substantial burden on global health[2]. However, early diagnosis and curative treatments can improve the overall survival of HCC patients[3]. The most efficacious surgical interventions for HCC include liver resection (LR) and liver transplantation, with LR being the most recommended therapy[4]. However, the tumor recurrence rate of HCC post-LR remains high, and research indicated that over 50% of HCC patients experience loco-regional recurrence within five years following resection, since HCC is a highly invasive malignancy[5,6]. Dissemination along the portal territory (PT) system is the main pathological route of the spread of HCC and is also one of the important causes of intrahepatic metastasis and postoperative local recurrence[7]. In the 1980s, the concept of anatomic liver resection (AR) was introduced[8]. AR employs the PT liver segment or subsegment as the fundamental anatomical framework for the systematic resection of tumor-bearing PT. It can also completely resect the tumor-bearing Glisson system supplied and labeled by PT, ultimately improving oncological efficacy[9]. In contrast, nonanatomic liver resection (NAR) focused on the limited resection of the liver without considering the underlying hepatic anatomy[10]. Some meta-analyses have revealed that AR is superior to NAR in terms of long-term outcomes in HCC patients[11,12]. While some studies indicated a controversial clinical effectiveness between NAR and AR[13,14,15].
The inception of the classic AR theory was marked by technical limitations that precluded accurate preoperative PT analysis and impeded the realistic intraoperative display of PT through methylene blue staining. Researchers combined the hepatic vein (HV) trunk exposure technique, derived from the Couinaud liver segmentation method, with methylene blue staining to approximate the effectiveness of PT resection during AR. However, AR is an individualized PT liver segmentectomy, whereas the Couinaud liver segmentation method is an artificial segmentation based on the HV trunk, rather than the true PT segmentation physiologically and oncologically. Additionally, A significant discrepancy arises from the intersegmental plane of the PT liver segment, which, unlike the uniform plane divided along the vein trunk as suggested by the Couinaud method, is a three-dimensional, irregularly curved surface[16]. This longstanding discrepancy between the classical AR theory and practice has potentially obscured the true oncological efficacy of AR. With advancements in liver surgery theory and technology, such as three-dimensional reconstruction, territory analysis systems, and indocyanine green (ICG) fluorescence navigation systems, a more precise and effective approach has emerged[17,18]. The integration of these technologies into the laparoscopic liver resection system has given rise to laparoscopic portal territory staining guided anatomic liver resection (LPTAR)[19,20]. LPTAR leverages preoperative three-dimensional reconstruction and territory analysis to accurately identify the tumor-bearing PT area, enabling precise surgical planning. During surgery, the PT liver segment or subsegment is the primary anatomical unit, with laparoscopic ICG fluorescence staining navigation facilitating the exact resection of the tumor-bearing PT system, including the Glisson system. This approach ensures the complete removal of the tumor-bearing PT and the preservation of the functional future liver remnant (FLR) volume. Theoretically, LPTAR represents a comprehensive resection of the tumor-bearing Glisson system at all levels, with the cone unit as the minimal anatomical unit[21,22]. This method not only achieves complete tumor removal but also preserves the intact Glisson system of the FLR, thereby ensuring FLR function. Emerging research has indicated that radical resection and functional preservation of the FLR are independent prognostic factors for HCC and align with the principles of modern precision liver resection[22]. Hence, based on the classical AR core theory, LPTAR is expected to address the discrepancies present in classical AR theory and practice. This may further promote the development of the AR theoretical and technical system, resulting in improved oncological outcomes for HCC patients[20,23].
Existing empirical studies have primarily focused on the comparison of efficacy between fluorescent laparoscopy and laparotomy operation or laparoscopy and laparotomy operation among patients undergoing AR[24]. The evidence of the efficacy between laparoscopy and fluorescent laparoscopy in HCC patients undergoing AR remains elusive currently, and related studies had small sample sizes with limited ability to guide clinical practice. Thus, it is necessary to systematically review the efficacy of fluorescent laparoscopy compared with laparoscopy in AR in HCC patients. This study aimed to systematically compare the effectiveness of laparoscopy and fluorescent laparoscopy in HCC patients undergoing AR and to provide robust evidence and guide the clinical practice of LPTAR in HCC patients.
2. Materials & Methods
2.1. PRISMA Compliance in Study Design
This systematic review was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement[25]. All authors have participated in the study design, data collection, analysis, interpretation, and manuscript preparation. This systematic review was registered on the International Prospective Register of Systematic Reviews (PROSPERO) on September 24, 2023, with the registration ID CRD42023456121. The registration process ensures transparency, reduces the risk of bias, and enhances the reliability and validity of our review by providing a detailed and predefined methodological plan before the commencement of the review. This process also prevents unnecessary duplication of reviews, thus promoting efficiency and collaboration in the research community.
2.2. Search Strategy
We conducted a systematic search of the following academic databases from inception to 26th November 2023: Pubmed, Web of Science, OVID, Embase, Cochrane Library, China National Knowledge Infrastructure Database (CNKI), and Chinese Wanfang Database (Wanfang). The search strategies are displayed in Supplementary Table S1. An alternative search of the references and cited references in relevant studies, clinical trial and systematic review registration platform, dissertation database, Google Scholar, and the consultation of experts in related fields were further conducted to identify additional studies that could be included in this systematic review.
2.3. Data Collection and Analysis
2.3.1. Eligibility Criteria
The eligibility criteria are developed following the PICOS (Population, intervention, control, outcome, study design) principle, literature following the next criteria will be included in this study: (1)Population: HCC patients undergoing hepatectomy; (2) Intervention: Fluorescent laparoscopy using indocyanine green (ICG) fluorescence imaging technique, or laparoscopy; (3) Control: Conventional laparoscopy operation; (4) Outcome: Clinical characteristics, including age, gender, ASA grade, HBV infection, liver cirrhosis, Child-Pugh classification, and tumor size; Operative outcomes, including operation time, blood loss, and blood transfusion; Postoperative outcomes, including complication and postoperative hospitalization time; Prognosis outcomes, including Overall survival (OS) and Recurrence-free survival (RFS); pathological outcomes, including R0 resection and margin distance. The literature should also Report enough information for effect size estimation in meta-analysis; (5) Study design: Randomized controlled trials (RCT), cohort studies, or case-control studies. The exclusion criterion is full text not available.
2.3.2. Data Collection and Management
Excel and Endnote X9 were employed to manage all collected records and remove duplicates. Two reviewers independently evaluated the titles and abstracts of literature collected based on the search strategies and determined their relevance to our study using the eligibility criteria. Literature that was deemed relevant by both reviewers proceeded to full-text review, while literature deemed relevant by only one reviewer was discussed among the authors to determine whether it should be reviewed in full. The original authors were contacted when any information was unclear or missing. Discussion and consultations with an experienced reviewer were used to resolve discrepancies about the final inclusion.
2.3.3. Data Extraction
Following the data inclusion, two reviewers performed data extraction using Excel. The following information was extracted: (1) Author of the literature; (2) Publication years; (4) Study sample; (5) Study method/design/sample size; (6) General information of the patients; (7) outcomes and its measurements; (8) types of intervention; (9) types of control.
2.3.4. Study Quality Evaluation
The quality of the included studies was assessed by two independent authors (CT and ML) using the Cochrane risk-of-bias tool (RoB) for RCT and the Newcastle-Ottawa scale (NOS) for retrospective studies. Disagreements were resolved by consultation with a third experienced reviewer.
2.3.5. Measurement of Treatment Effect
The effect size odds ratio (OR) and standard mean difference (SMD) were calculated to compare the efficacy of laparoscopy and fluorescent laparoscopy.
2.3.6. Grading the Quality of Evidence
To better help healthcare professionals understand the evidence level and make informed decisions about patients, the quality of evidence for this systematic review was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system, which uses four levels of evidence quality: high, moderate, and low. The grading was completed using GRADE Profiler 3.6.
2.3.7. Statistical Analysis
The Begg and Mazumdar rank correlation test and Egger’s regression intercept test of each comparison from the literature were used to evaluate publication bias, where the P values of <0.05 indicated publication bias, and Duval and Tweedie’s trim and fill was used for the correction of publication bias. Q test and I2 were used for the heterogeneity test, where a statistically significant Q value and I2≥50 indicated heterogeneity. The effect sizes were integrated with a fixed effect model if they were homogenous, and with a random effect model if they were heterogeneous. The comparisons between the efficacy of laparoscopy and fluorescent laparoscopy were synthesized by effect sizes SMD or OR, and 95% CI with corresponding models, and were summarized using forest plots. Meta-regression analysis was used to explore the sources of heterogeneity. Sensitivity analysis was used to examine the impact of individual studies on the overall effect size and heterogeneity. The significant level in this study is determined at α=0.05. All statistical analyses were completed using CMA 3.3.
2.4. Ethics and Dissemination
This systematic review was conducted following the highest ethical standards. All data used in this systematic review was obtained from publicly available sources, and no primary data collection was conducted. Therefore, no ethical approval is required for this study. The authorship of any publication resulting from this systematic review was determined based on the contributions of each team member, following the guidelines of the International Committee of Medical Journal Editors (ICMJE). The research team has no competing interests to declare. The research team is committed to making the findings of this systematic review widely available to inform future research and practice.
3. Results
3.1. Description of Included Studies
We finally included 13 studies (10 retrospective studies and 3 RCTs) in this systematic review, and all of them were of high quality after evaluation. The flowchart of study selection is shown in Figure 1. The general descriptions of the 13 studies are displayed in Table 1[26,27,28,29,30,31,32,33,34,35,36,37,38].
Note: ICG: indocyanine green fluorescence laparoscopy; CL: conventional laparoscopy; RCT: randomized controlled trial.
3.2. Quality Assessment
The included RCTs in this study predominantly exhibited a low or unclear risk of bias. However, the blinding of participants and personnel was identified as a significant source of bias. Given the inherent characteristics of these RCTs, an open-label design was inevitable. The details are summarized in Figure 2 and Figure 3. Additionally, the retrospective studies included in our analysis demonstrated a relatively low bias concerning participant selection, comparability, and exposure measurements., see Table 2.
3.3. Quantitative Meta-Analysis
3.3.1. Publication Bias and Heterogeneity Test
In this study, the data of prognosis (OS and RFS) are not integrated and completed enough for meta-analysis, which was included in further qualitative systematic review.
In the meta-analysis, the Child-Pugh classification showed obvious publication bias (All P<0.05). Tumor size (Q=38.889, P<0.001, I2= 79.43%), operation time (Q=58.025, P<0.001, I2= 82.77%), blood loss (Q=108.948, P<0.001, I2= 90.82%), and margin distance (Q=18.385, P<0.001, I2= 83.68%) had heterogeneity and will be fitted with random effect models. The details of publication bias and heterogeneity tests are shown in Table 3.
3.3.2. Clinical Characteristics Between Indocyanine Green Fluorescence Laparoscopy Group and Conventional Laparoscopy Group
The distributions of age (OR=1.070, P=0.630), gender (OR=1.007, P=0.969), ASA (OR=0.669, P=0.162), HBV infection condition (OR=0.934, P=0.770), liver cirrhosis (OR=1.257, P=0.172), child-Pugh classification (OR=0.972, P=0.024), and tumor size (SMD=-0.227, P=0.230) between ICG fluorescence laparoscopy group and conventional laparoscopy group were all statistically insignificant. To be noted, after Duval and Tweedie’s trim and fill correction for publication bias for the Child-Pugh classification, its association with the two groups was still insignificant (OR=0.837, 95%CI: 0.496~1.411). The details of the clinical characteristics between the ICG fluorescence laparoscopy group and the conventional laparoscopy group are summarized in Supplementary Figure S1~S7.
3.3.3. Operative Outcomes Between Indocyanine Green Fluorescence Laparoscopy Group and Conventional Laparoscopy Group
In the meta-analysis, the operation time of the ICG fluorescence laparoscopy group was comparable to that of the conventional laparoscopy group (SMD=-0.238, P=0.160). After adjusting for publication bias, the insignificance still existed (SMD=0.122, 95%CI: -0.242~0.487). However, the perioperative blood loss of the ICG fluorescence laparoscopy group was significantly lower than that of the conventional laparoscopy group (SMD=-0.743, P=0.002). Additionally, fewer patients experienced blood transfusion in the ICG fluorescence laparoscopy group than in the conventional laparoscopy group (OR=0.459, P=0.004). See Figure 4, Figure 5 and Figure 6.
3.3.4. Postoperative Outcomes Between Indocyanine Green Fluorescence Laparoscopy Group and Conventional Laparoscopy Group
Patients of the ICG fluorescence laparoscopy group experienced marginally fewer postoperative complications compared with those of the conventional laparoscopy group with an insignificant trend (OR=0.657, P=0.071). However, the postoperative hospitalization time was significantly shorter in the ICG fluorescence laparoscopy group (SMD=-0.358, P<0.001). The details are illustrated in Figure 7 and Figure 8.
3.3.5. Pathological Outcomes Between Indocyanine Green Fluorescence Laparoscopy Group and Conventional Laparoscopy Group
In this study, it was observed that patients in the ICG fluorescence laparoscopy group exhibited a higher R0 resection rate (OR=3.013, P=0.068) and larger margin distance (SMD=0.559, P=0.072) in comparison to their counterparts in the conventional laparoscopy group, albeit with a statistically insignificant trend. See Figure 9 and Figure 10.
3.3.6. Meta-Regression Analysis
In the analysis of heterogeneity sources, we considered potential moderators including age, gender, ASA, HIV status, liver cirrhosis status, Child-Pugh classification, tumor size, and study type. The results suggested that gender significantly contributed to the heterogeneity of operation time (β=0.010, P=0.027), reducing the I² from 82.77% to 73.52%. Additionally, RCTs reported less blood loss compared to retrospective studies (β=-1.180, P=0.021), and the study type accounted for a reduction in the I² of blood loss from 90.82% to 86.13%. The detailed results are shown in Table 4. We excluded results that lacked sufficient data, such as the impact of ASA and tumor size on blood loss.
3.3.7. Sensitivity Analysis
Sensitivity analyses were performed on all outcomes to examine whether the overall effect sizes were impacted by individual studies. The analyses showed that the exclusion of the studies by Liu in 2023 or Wang in 2022, resulted in a statistically significant reduction in postoperative complications in the ICG fluorescence laparoscopy group compared to the conventional laparoscopy group (OR=0.573/0.576, P=0.037/0.022). Similarly, the removal of the study by Chen in 2019 resulted in a statistically significant increase in the R0 resection rate in the ICG fluorescence laparoscopy group compared to the conventional laparoscopy group (OR=5.268, P=0.040). Furthermore, the exclusion of the study by Zhou in 2019 resulted in a statistically significant increase in the margin distance in the ICG fluorescence laparoscopy group compared to the conventional laparoscopy group (SMD=0.840, P<0.005). The details are presented in Figure 11. The sensitivity analyses did not significantly alter the effect sizes of the other outcomes, and these results are provided in Supplementary Figures S8–S11.
3.3.8. Evidence Quality Examination
We conducted a post-hoc GRADE assessment for the evidence concluded from meta-analysis, and found that the evidence on operation time was very low; the evidence on postoperative hospitalization time and margin distance was low; and the evidence on blood loss, blood transfusion, postoperative complications, and R0 resection were moderate. See Figure 14.
3.4. Qualitative Systematic Review of Prognosis Outcomes
Respectively 4 and 2 studies included information on RFS and OS between the ICG fluorescence laparoscopy group and the conventional laparoscopy group[27,28,29,32,33,34]. Among the 4studies examining RFS, 3 reported an insignificant difference in RFS between the 2 groups, while 1 study indicated that patients in the ICG fluorescence laparoscopy group were 2 times more likely to have longer RFS than the conventional laparoscopy group (HR=0.462, P=0.024). In addition, both studies focusing on OS reported a statistically insignificant difference in OS between the two groups.
4. Discussion
This systematic review and meta-analysis suggested that, in comparison to conventional laparoscopy, ICG fluorescence laparoscopy is associated with improved short- and long-term clinical outcomes for HCC patients undergoing AR. Specifically, it demonstrates advantages such as reduced intraoperative blood loss, decreased risks of blood transfusion, and reduced length of postoperative hospitalization times. ICG fluorescence laparoscopy also showed implications for fewer postoperative complications, higher rates of achieving R0 resection, greater margin distances, and extended RFS, although these findings were not statistically significant and require further investigation. Complete resection of the tumor-bearing PT can improve the surgical oncological efficacy in treating HCC, which is the fundamental principle of AR[39].
Similar to the result of the current research, a study found that ICG fluorescence real-time imaging-guided technology in laparoscopic hepatectomy could increase the R0 resection rate, shorten postoperative hospital stays, and reduce blood loss and the occurrence of postoperative complications[40]. Another study conducted in patients with HCC found that although ICG fluorescence laparoscopic hepatectomy took longer to perform, it could result in reduced rates of postoperative complications[32]. In LPTAR, ICG fluorescence is utilized to delineate the tumor-bearing PT[41,42]. Subsequently, the tumor-bearing PT is traced to the corresponding tumor-bearing Glisson system, leading to the complete resection of combined tumor-bearing Glisson systems at all hierarchical levels[43,44]. Theoretically, the liver transection plane in LPTAR should be located between the various levels of the Glisson system, manifesting as a three-dimensional curved surface denoted as the physiological liver cleft[45]. This cleft manifests in regions characterized by insufficiency or paucity of vascular branches, commonly acknowledged as the “vascular bare area”, and various levels of inter-territory hepatic veins (IHVs) traverse within this region[9,46]. Guided by fluorescence, the individualized curved surface anatomy of the Glisson systems is meticulously followed during liver dissection[47,48]. This methodology firstly is beneficial in mitigating the challenge of orientation loss within the deep liver parenchyma[49,50]. More importantly, the complete resection of tumor-bearing Glisson systems and preservation of the FLR Glisson system can reduce complications such as bleeding, ischemia, and bile leakage stemming caused by the severance of hepatic pedicle branches[51,52]. Concurrently, the fluorescence reveals the various levels of IHVs within the Glisson systems, ensuring hepatic venous outflow and mitigating congestion[53,54]. Therefore, the complete resection of tumor-bearing Glisson systems with LPTAR, while preserving FLR Glisson systems and hepatic venous outflow, could potentially reduce the risk of disorientation of anatomical direction and complications such as bleeding, ischemia, bile leakage, congestion, and liver dysfunction. This strategic approach is anticipated to result in superior perioperative outcomes.
The heterogeneity source exploration revealed that RCTs reported less blood loss compared to retrospective studies. This finding emphasized the high clinical efficacy of ICG fluorescence in minimizing intraoperative blood loss, particularly in studies with rigorous designs. This evidence, graded as “moderate,” provides relatively reliable guidance for clinical practice. However, heterogeneity persists even after controlling for study type, suggesting the necessity for further research to comprehensively understand when laparoscopy with ICG fluorescence may be most effective in reducing blood loss. Sensitivity analyses indicated that the exclusion of certain retrospective studies could result in improved clinical benefits of ICG fluorescence in reducing postoperative complications and increasing the margin distance, which further highlights the potential advantages of ICG fluorescence since a higher proportion of high-quality RCTs were included in the analyses following the exclusion of retrospective studies[32]. However, we also found that the removal of an RCT resulted in a statistically significant increase in the R0 resection rate in the ICG fluorescence laparoscopy group. This could be attributed to the inclusion of only 2 articles (1 retrospective study and 1 RCT) in the R0 resection rate analysis. The exclusion of the RCT could merely reflect the result of the retrospective study, rather than confirming the benefit of ICG fluorescence laparoscopy on the R0 resection rate[28,30]. Further RCTs are still required to examine the effect of ICG fluorescence on the clinical benefit derived from the R0 resection rate. Moreover, in the demographic information of the patients included in this systematic review, we observed heterogeneity in tumor size between the ICG fluorescence laparoscopy and conventional laparoscopy groups. Although limited evidence focused on the oncological efficacy of LPTAR based on tumor size, a retrospective study revealed that in patients with HCCs exceeding 5cm, the implementation of AR might inadvertently fail to result in the intended benefits compared with NAR[55]. Further studies are warranted to identify which HCC patients would truly benefit from LPTAR with ICG fluorescence to provide valuable guidance for optimizing surgical outcomes.
To be noted, similar to LPTAR, researchers also proposed the dynamic liver blood watershed theory to redefine the distribution of blood vessels and blood flow in the liver[56]. This concept deviates from LPTAR but is susceptible to confusion. Dynamic liver blood watershed theory pointed out that the interrelationships between liver segments cannot be ignored, and the liver should be dissected and analyzed as a whole. The liver tissue within a certain watershed (river section) is supplied by multiple peripheral hepatic arteries and portal vein branches, forming a dynamic balance. For a portion of liver malignant tumors in special areas, watershed resection will be carried out. While ensuring liver function, the entire watershed of the tumor area, including its blood vessels, will be removed. The main idea advocated in the current study is watershed liver resection. The anatomy of liver segments is described as a “tree trunk” structure, with the main trunk being the portal vein and branches being the segmental portal vein. The liver segments are directly supplied by the segmental portal vein, and there are no communicating branches between the liver segments. Each segment is a functional and anatomical independent unit that can be independently excised.
Compared to NAR, AR may improve the long-term survival rate of HCC patients, but the presence of residual tumor-bearing PT in classical AR may contribute to local recurrence and negatively impact the oncological therapeutic efficacy of AR[57]. Therefore, it is imperative to accurately perform LPTAR and ensure that this theoretical technology is safe, effective, and widely applicable[58]. Due to the lack of sufficient evidence on the efficacy of fluorescent laparoscopy in AR, this systematic review is the first to synthesize evidence comparing fluorescent laparoscopy and laparoscopy. The results could provide a reference for further clinical guidance on the intraoperative use of fluorescent laparoscopy in AR.
However, this study has certain limitations. First, the results may be influenced by potential selection bias due to some of the non-randomized nature of some studies included in the systematic review. Second, the observed heterogeneity in several outcomes and the variability in surgical techniques employed across the included studies may affect the generalizability of the findings. Third, the absence of long-term follow-up data within the selected studies limits the ability to confidently draw conclusive inferences regarding the enduring effects of fluorescent laparoscopy on patient outcomes. Fourth, given the present technical constraints, this study provisionally classified the ICG fluorescence laparoscopy surgery as LPTAR, which may potentially underestimate the actual effectiveness and efficacy of LPTAR. Despite these limitations, this systematic review and meta-analysis provides valuable insights into the potential benefits of ICG fluorescent laparoscopy in LPTAR and highlights the need for further high-quality, randomized controlled trials to definitively establish its role in the management of HCC. An expert consensus in China has established the technical standard of LPTAR as: (1) The procedure involves the complete resection of the tumor-bearing PT under the guidance of ICG navigation while ensuring the full preservation of the remaining liver (staining first, positive or negative); (2) The process adheres strictly to the physiological hepatic fissure surface to separate the liver under the guidance of fluorescence, which allows for the complete resection of the tumor-bearing Glisson system, ensuring that no hepatic pedicle is encountered in the section. (3) The procedure requires the exposure of the typical inter-territory hepatic vein (TIHV), which involves the stereoscopic exposure of all levels of intrahepatic veins (IHVs); (4) The smallest resection unit should be the sub-segment supplied by the fourth-level hepatic pedicle. This is determined by either puncture or ligation at the root of the hepatic pedicle, as indicated by classic AR theory. (5) The procedure mandates a resection margin of ≥1 cm, in accordance with established guidelines and ethical requirements[23]. Future research could focus on standardizing the use of ICG fluorescent laparoscopy in LPTAR in clinical settings to ensure consistent and optimal outcomes. Further systematic reviews comparing LPTAR and NAR are also essential to identify the most appropriate patient population with HCC for each approach.
5. Conclusion
This systematic review and meta-analysis demonstrated that ICG fluorescence laparoscopy is a safe and effective technique for AR in HCC patients. Compared to conventional laparoscopy, ICG fluorescence laparoscopy resulted in reduced blood loss, lower blood transfusion rates, and shorter hospital stays. These advantages are attributed to the accurate and complete resection of tumor-bearing PT and Glisson systems, as well as the preservation of FLR function and venous outflow. This study provides valuable evidence to support the clinical application of ICG fluorescence laparoscopy in LPTAR for HCC.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
References
- Sung, H.; et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021, 71 209–249. 71.
- Llovet, J.M.; et al. Hepatocellular carcinoma. Nat Rev Dis Primers 2021, 7, 6. [Google Scholar] [CrossRef]
- Allaire, M.; et al. New frontiers in liver resection for hepatocellular carcinoma. JHEP Rep 2020, 2, 100134. [Google Scholar] [CrossRef] [PubMed]
- Glantzounis, G.K.; et al. The role of liver resection in the management of intermediate and advanced stage hepatocellular carcinoma. A systematic review. Eur J Surg Oncol 2018, 44, 195–208. [Google Scholar] [CrossRef]
- Singal, A.G., F. Kanwal, and J.M. Llovet, Global trends in hepatocellular carcinoma epidemiology: implications for screening, prevention and therapy. Nat Rev Clin Oncol 2023 20, 864–884.
- Pang, T.C. and V. World J Hepatol 2015, 7, 245–252. [Google Scholar] [CrossRef]
- Zhang, M.; et al. Progress on the molecular mechanism of portal vein tumor thrombosis formation in hepatocellular carcinoma. Exp Cell Res 2023, 426, 113563. [Google Scholar] [CrossRef]
- Makuuchi, M., H. Hasegawa, and S. Yamazaki, Ultrasonically guided subsegmentectomy. Surg Gynecol Obstet, 1985, 161, 346–350. [Google Scholar]
- Shindoh, J.; et al. Complete removal of the tumor-bearing portal territory decreases local tumor recurrence and improves disease-specific survival of patients with hepatocellular carcinoma. J Hepatol 2016, 64, 594–600. [Google Scholar] [CrossRef]
- Garancini, M.; et al. Non-anatomical liver resection for hepatocellular carcinoma: the SegSubTe classification to overcome the problem of heterogeneity. Hepatobiliary Pancreat Dis Int 2023. [CrossRef]
- Liu, H.; et al. Anatomical vs nonanatomical liver resection for solitary hepatocellular carcinoma: A systematic review and meta-analysis. World J Gastrointest Oncol 2021, 13, 1833–1846. [Google Scholar] [CrossRef]
- Shin, S.W.; et al. Effect of anatomical liver resection for hepatocellular carcinoma: a systematic review and meta-analysis. Int J Surg 2023, 109, 2784–2793. [Google Scholar] [CrossRef]
- Ju, M. and A. Cancers (Basel) 2019, 11, 10. [Google Scholar]
- Zeindler, J.; et al. Anatomic versus non-anatomic liver resection for hepatocellular carcinoma-A European multicentre cohort study in cirrhotic and non-cirrhotic patients. Cancer Med 2024, 13, e6981. [Google Scholar] [CrossRef] [PubMed]
- Nevarez, N.M. and A. Hepatoma Research 2021, 7, 66. [Google Scholar]
- Shindoh, J.; et al. The intersegmental plane of the liver is not always flat--tricks for anatomical liver resection. Ann Surg 2010, 251, 917–922. [Google Scholar] [CrossRef]
- Harimoto, N.; et al. Laparoscopic hepatectomy and dissection of lymph nodes for intrahepatic cholangiocarcinoma. Case report. Surg Endosc 2002, 16, 1806. [Google Scholar] [CrossRef]
- Croome, K.P. and M. Arch Surg 2010, 145, 1109–1118. [Google Scholar]
- Wang, X.; et al. Approaches of laparoscopic anatomical liver resection of segment 8 for hepatocellular carcinoma: a retrospective cohort study of short-term results at multiple centers in China. Int J Surg 2023, 109, 3365–3374. [Google Scholar] [CrossRef]
- Cao, J.; et al. Theory and technical practice of anatomic liver resection based on portal territory for the treatment of hepatocellular carcinoma. Chinese Journal of Digestive Surgery 2022, 21, 591–597. [Google Scholar]
- Yoshida, H.; et al. Segmentectomy of the liver. J Hepatobiliary Pancreat Sci 2012, 19, 67–71. [Google Scholar] [CrossRef]
- Wang, X., J. Cao, and J. JAMA Surg 2024.
- Surgery, >E.B.o.C.J.o.D. Surgery;, E.B.o.C.J.o.D. and S.f.H.-p.-b.S.o.C.R.H. Association, Chinese expert consensus on the theoretical and technical system of laparoscopic portal terri-tory staining guided anatomic liver resection (2023 edition). 22, 2023; 22. [Google Scholar]
- Cho, H.D.; et al. Minimally invasive donor hepatectomy, systemic review. Int J Surg 2020, 82S, 187–191. [Google Scholar] [CrossRef]
- Page, M.J.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; et al. Real-Time Navigation Guidance Using Fusion Indocyanine Green Fluorescence Imaging in Laparoscopic Non-Anatomical Hepatectomy of Hepatocellular Carcinomas at Segments 6, 7, or 8 (with Videos). Med Sci Monit 2019, 25, 1512–1517. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; et al. Effects of indocyanine green fluorescence imaging of laparoscopic anatomic liver resection for HCC: a propensity score-matched study. Langenbecks Arch Surg 2023, 408, 51. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; et al. Short- and Long-Term Outcomes of Indocyanine Green Fluorescence Navigation- Versus Conventional-Laparoscopic Hepatectomy for Hepatocellular Carcinoma: A Propensity Score-Matched, Retrospective, Cohort Study. Ann Surg Oncol 2023, 30, 1991–2002. [Google Scholar] [CrossRef]
- Wang Liangliang, Y.B.Z.W. , Comparison of fluorescent laparoscopic hepatectomy and conventional laparoscopic hepatectomy in the treatment of patients with HCC. Journal of Practical Hepatology 2020, 23, 427–430. [Google Scholar]
- Chen, S.; et al. Clinical analysis on safety and efficacy of ICG real-time fluorescence imaging in laparoscopic hepatectomy of HCC at special location. Medical Journal of Chinese People's Liberation Army 2019, 44, 336–340. 44.
- Yao, C. , Application of ICG fluorescence imaging in laparoscopic hepatectomy for primary liver cancer. 2021, Bengbu Medical University.
- Jianxi, W.; et al. Indocyanine green fluorescence-guided laparoscopic hepatectomy versus conventional laparoscopic hepatectomy for hepatocellular carcinoma: A single-center propensity score matching study. Front Oncol 2022, 12, p. 9300; 65. [Google Scholar]
- Wang, X. , Clinical study of indole green fluorescence navigation in laparoscopic liver tumor resection. 2020, China Medical University.
- Wang, S., J. Li, and W. The Practical Journal of Cancer 2023, 38, 443–446. [Google Scholar]
- Feng, B. , Clinical value of indocyanine green fluorescence imaging in laparoscopic curative resection of liver cancer. 2023, Jilin University.
- Guo, C.; et al. Application of indocyanine green fluorescence imaging technique in laparoscopic hepatectomy. Journal of Laparoscopic Surgery 2021, 26, 81–85. [Google Scholar]
- Liu, X.; et al. Application of Indocyanine Green Fluorescence Imageguided Laparoscopic Hepatectomy in Hepatocellular Carcinoma. Inner Mongolia Medical Journal 2023, 55, 659–662. [Google Scholar]
- Yang, H. , Application of indocyanine green fluorescence in hepatectomy of complex segment hepatocellular carcinoma. 2022, Zunyi Medical University.
- Hong, S.K.; et al. Pure Laparoscopic Donor Hepatectomy: A Multicenter Experience. Liver Transpl 2021, 27, 67–76. [Google Scholar] [CrossRef]
- Chen, H.; et al. Application Effect of ICG Fluorescence Real-Time Imaging Technology in Laparoscopic Hepatectomy. Front Oncol 2022, 12, 819960. [Google Scholar] [CrossRef] [PubMed]
- Gotohda, N.; et al. Expert Consensus Guidelines: How to safely perform minimally invasive anatomic liver resection. J Hepatobiliary Pancreat Sci 2022, 29, 16–32. [Google Scholar] [CrossRef] [PubMed]
- Takamoto, T. and M. Cancer Biol Med 2019, 16, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Berardi, G.; et al. Parenchymal Sparing Anatomical Liver Resections With Full Laparoscopic Approach: Description of Technique and Short-term Results. Ann Surg 2021, 273, 785–791. [Google Scholar] [CrossRef]
- Liang, X.; et al. Laparoscopic anatomical portal territory hepatectomy using Glissonean pedicle approach (Takasaki approach) with indocyanine green fluorescence negative staining: how I do it. HPB (Oxford) 2021, 23, 1392–1399. [Google Scholar] [CrossRef]
- Berardi, G.; et al. The Applications of 3D Imaging and Indocyanine Green Dye Fluorescence in Laparoscopic Liver Surgery. Diagnostics (Basel) 2021, 11, 12. [Google Scholar] [CrossRef]
- Wakabayashi, T.; et al. Indocyanine Green Fluorescence Navigation in Liver Surgery: A Systematic Review on Dose and Timing of Administration. Ann Surg 2022, 275, 1025–1034. [Google Scholar] [CrossRef]
- Sutton, P.A.; et al. Fluorescence-guided surgery: comprehensive review. BJS Open 2023, 7, 3. [Google Scholar] [CrossRef]
- Inoue, Y.; et al. Anatomical Liver Resections Guided by 3-Dimensional Parenchymal Staining Using Fusion Indocyanine Green Fluorescence Imaging. Ann Surg 2015, 262, 105–111. [Google Scholar] [CrossRef]
- Tao, H.; et al. Indocyanine green fluorescence imaging to localize insulinoma and provide three-dimensional demarcation for laparoscopic enucleation: a retrospective single-arm cohort study. Int J Surg 2023, 109, 821–828. [Google Scholar] [CrossRef]
- Leiloglou, M.; et al. Indocyanine green fluorescence image processing techniques for breast cancer macroscopic demarcation. Sci Rep 2022, 12, 8607. [Google Scholar] [CrossRef]
- Hiroyoshi, J.; et al. Identification of Glisson's Capsule Invasion During Hepatectomy for Colorectal Liver Metastasis by Contrast-Enhanced Ultrasonography Using Perflubutane. World J Surg 2021, 45, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Nishino, H.; et al. Real-time Navigation for Liver Surgery Using Projection Mapping With Indocyanine Green Fluorescence: Development of the Novel Medical Imaging Projection System. Ann Surg 2018, 267, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; et al. Perioperative and Disease-Free Survival Outcomes after Hepatectomy for Centrally Located Hepatocellular Carcinoma Guided by Augmented Reality and Indocyanine Green Fluorescence Imaging: A Single-Center Experience. J Am Coll Surg 2023, 236, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; et al. Laparoscopic Anatomical Portal Territory Hepatectomy with Cirrhosis by Takasaki's Approach and Indocyanine Green Fluorescence Navigation (with Video). Ann Surg Oncol 2020, 27, 5179–5180. [Google Scholar] [CrossRef]
- Kwon, J.H.; et al. Effects of Anatomical or Non-Anatomical Resection of Hepatocellular Carcinoma on Survival Outcome. J Clin Med 2022, 11, 5. [Google Scholar] [CrossRef]
- Liu, R.; et al. Clinical values of total laparoscopic liver resections:with experiences of 123 cases. Journal of laparoscopic surgery 2006, 479–481. [Google Scholar]
- Darido, E.F. and T. World J Surg 2011, 35, 2594–2595. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; et al. Laparoscopic liver resection versus open liver resection for intrahepatic cholangiocarcinoma: 3-year outcomes of a cohort study with propensity score matching. Surg Oncol 2020, 33, 63–69. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of study selection.
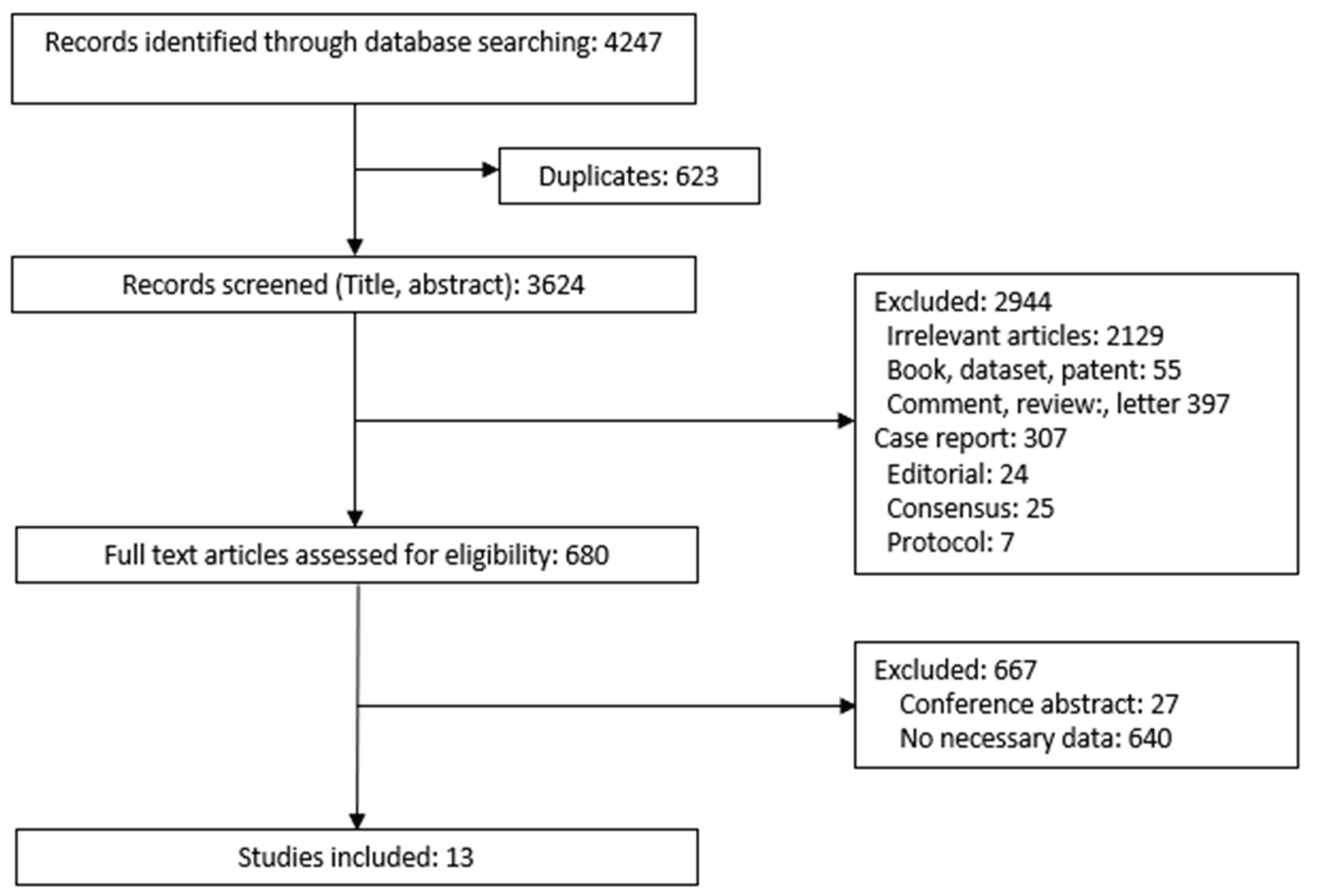
Figure 2.
Risk of bias graph.
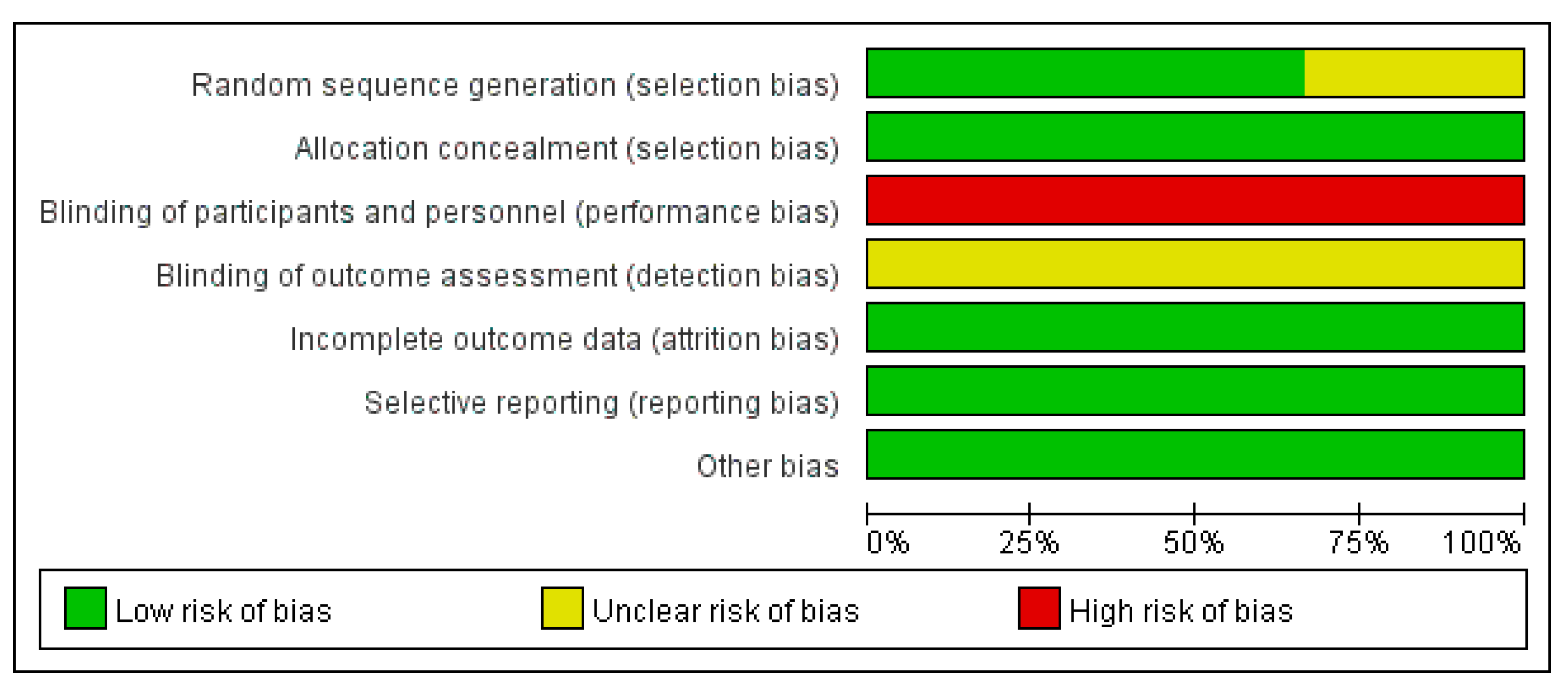
Figure 3.
Risk of bias summary.
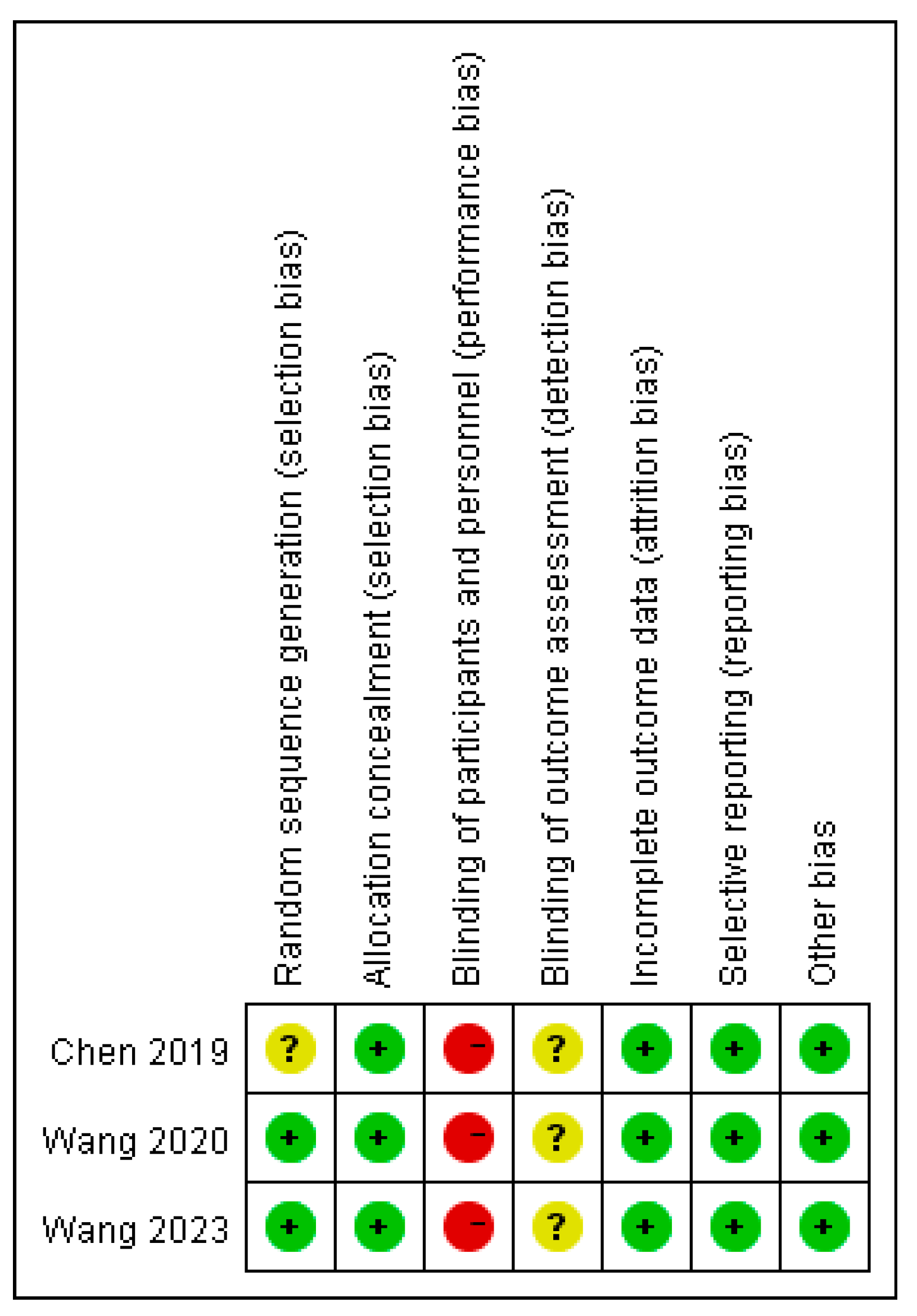
Figure 4.
Parameter estimation and forest plot of operation time distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 4.
Parameter estimation and forest plot of operation time distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
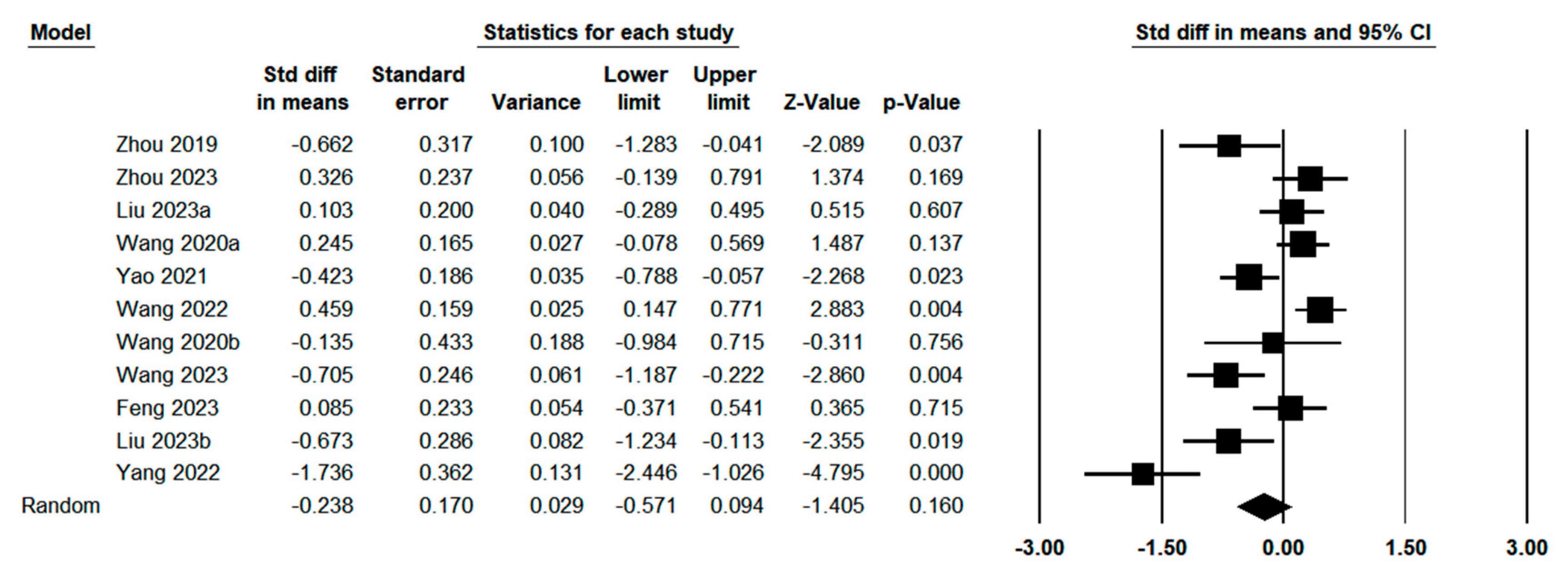
Figure 5.
Parameter estimation and forest plot of blood loss distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 5.
Parameter estimation and forest plot of blood loss distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
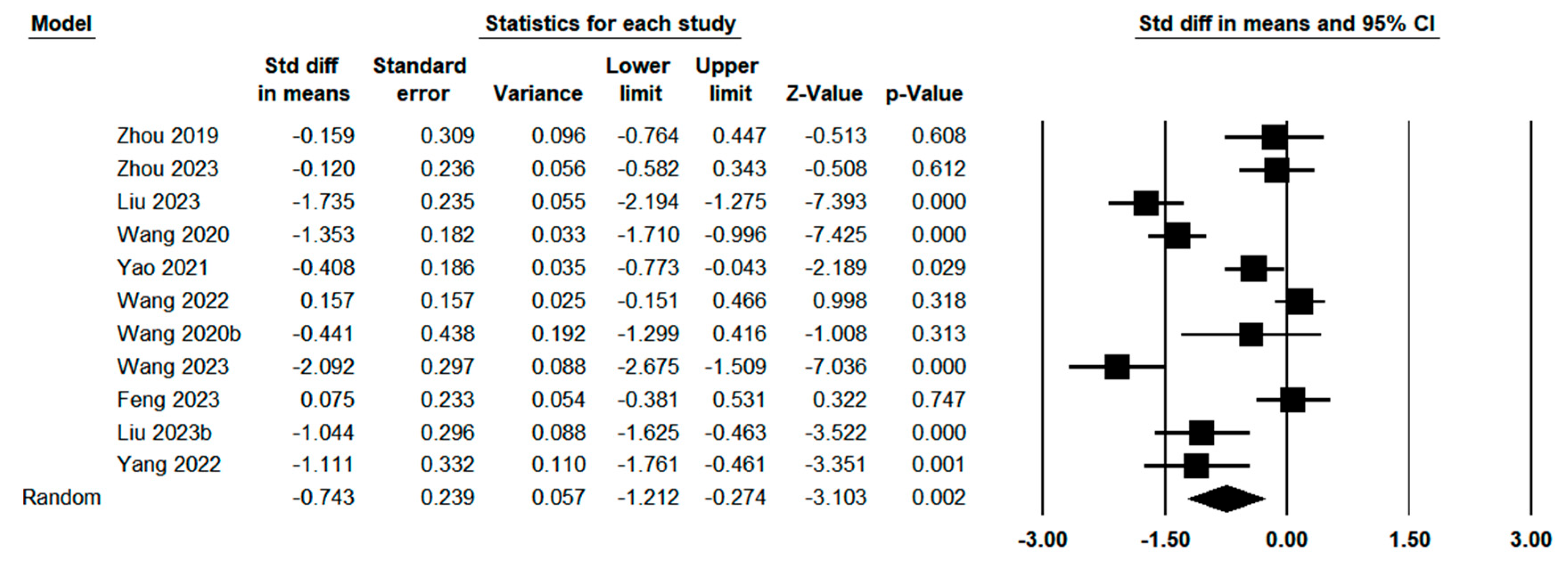
Figure 6.
Parameter estimation and forest plot of blood transfusion distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 6.
Parameter estimation and forest plot of blood transfusion distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
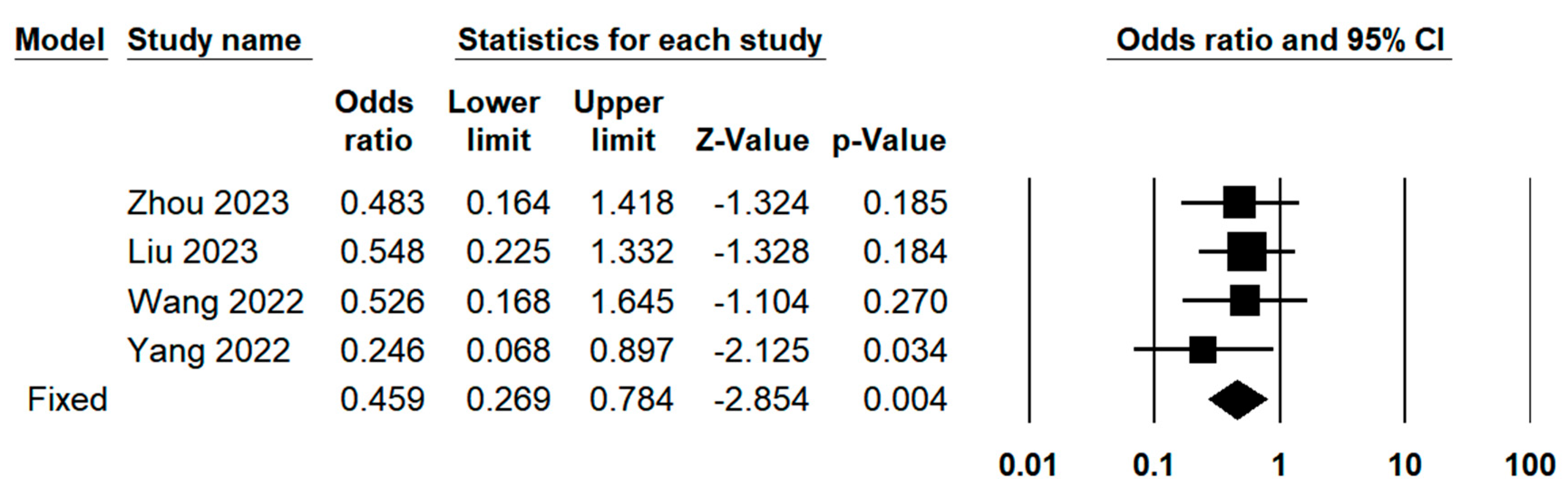
Figure 7.
Parameter estimation and forest plot of postoperative complications distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 7.
Parameter estimation and forest plot of postoperative complications distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
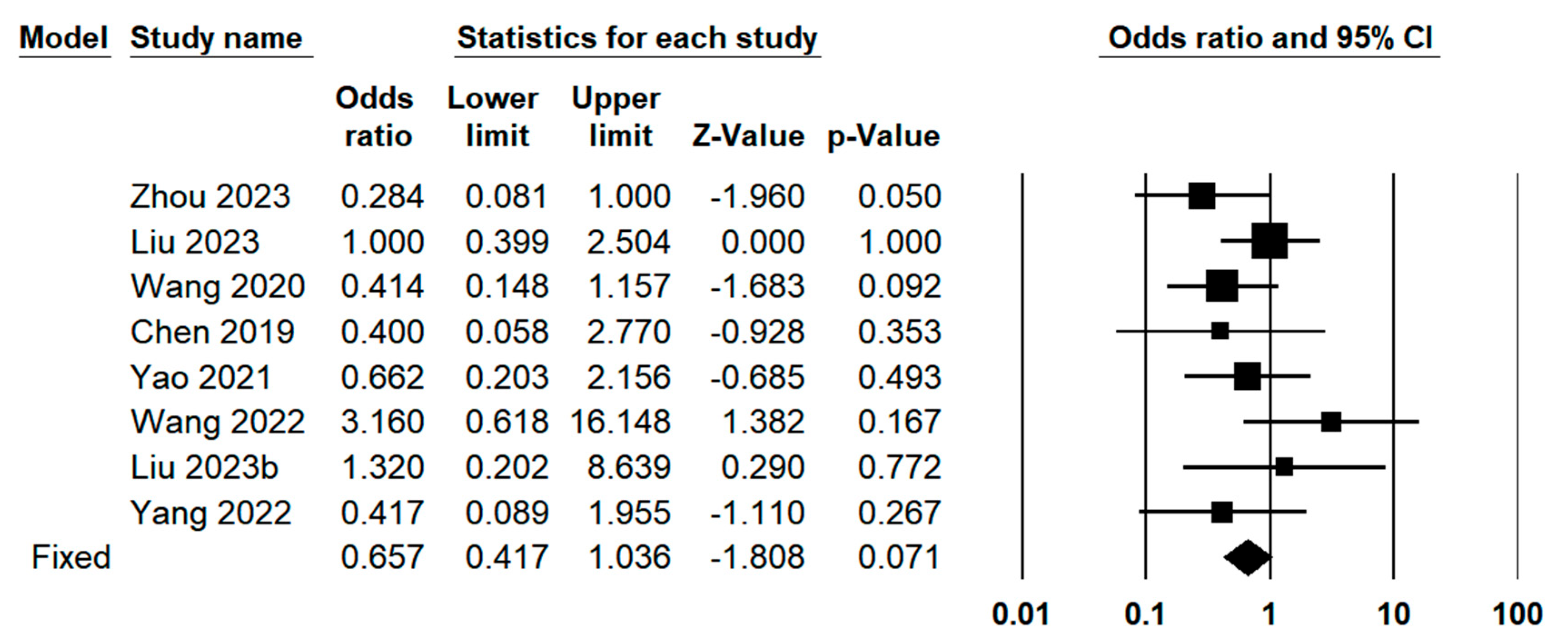
Figure 8.
Parameter estimation and forest plot of postoperative hospitalization time distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 8.
Parameter estimation and forest plot of postoperative hospitalization time distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
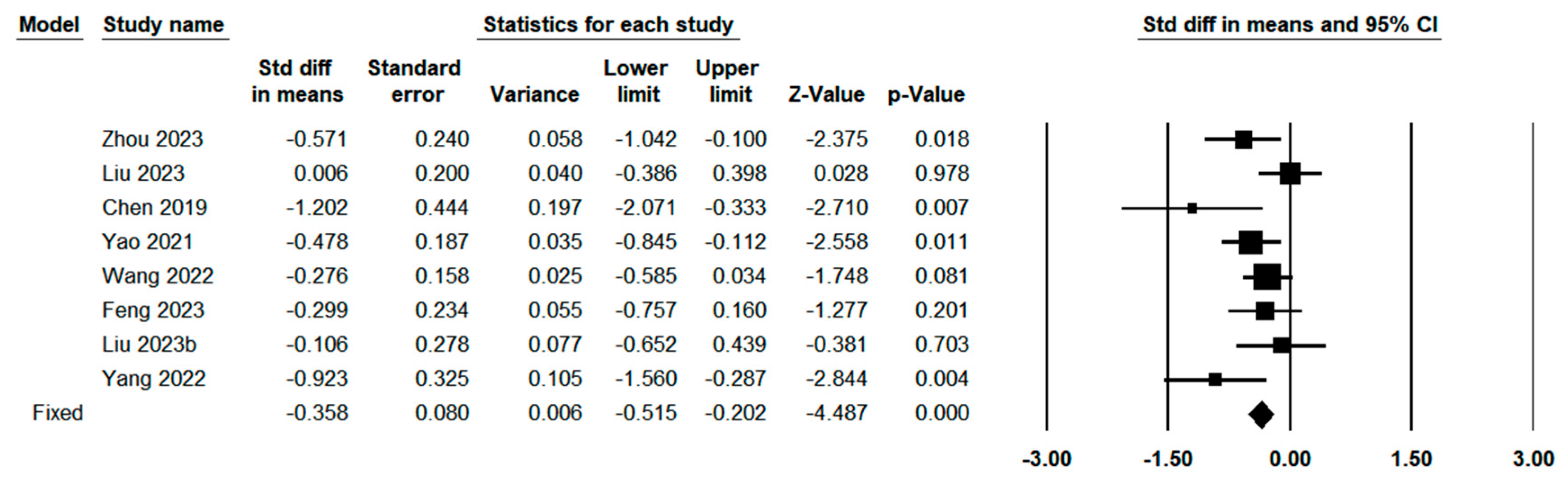
Figure 9.
Parameter estimation and forest plot of R0 resection distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 9.
Parameter estimation and forest plot of R0 resection distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
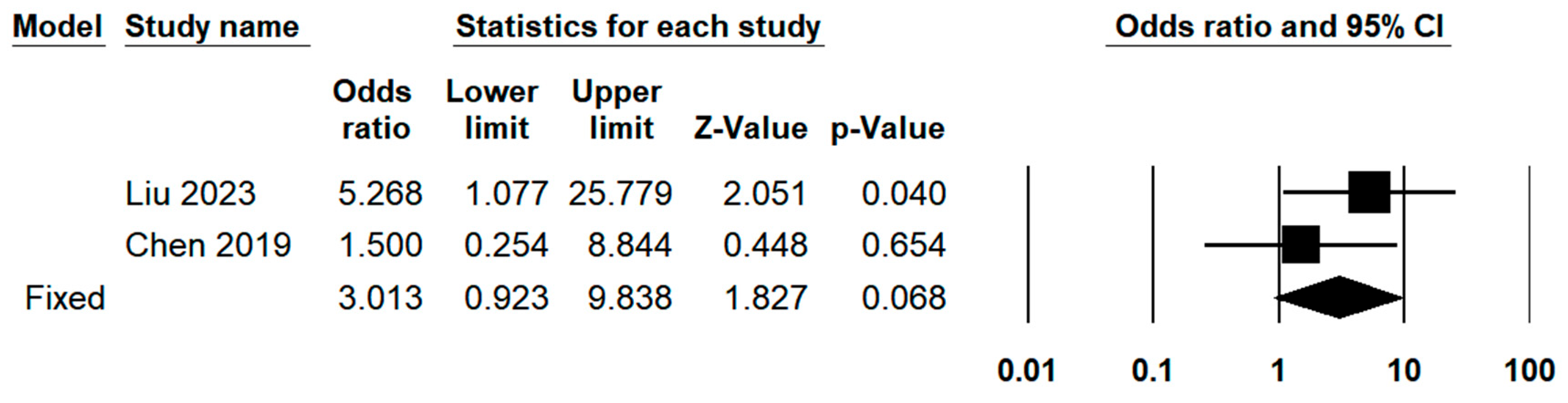
Figure 10.
Parameter estimation and forest plot of margin distance distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 10.
Parameter estimation and forest plot of margin distance distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
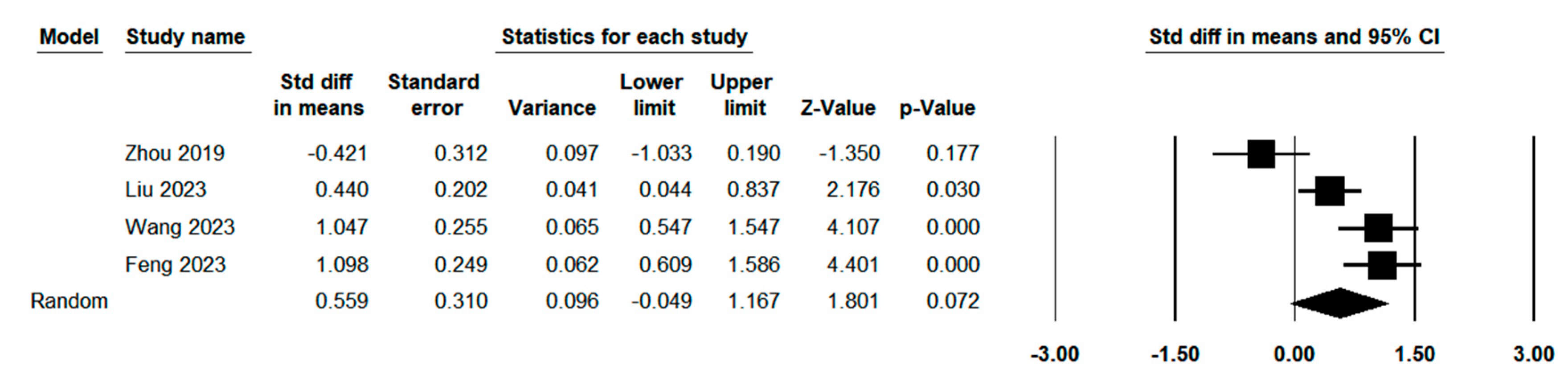
Figure 11.
Sensitivity analysis and forest plot of postoperative complications distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 11.
Sensitivity analysis and forest plot of postoperative complications distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
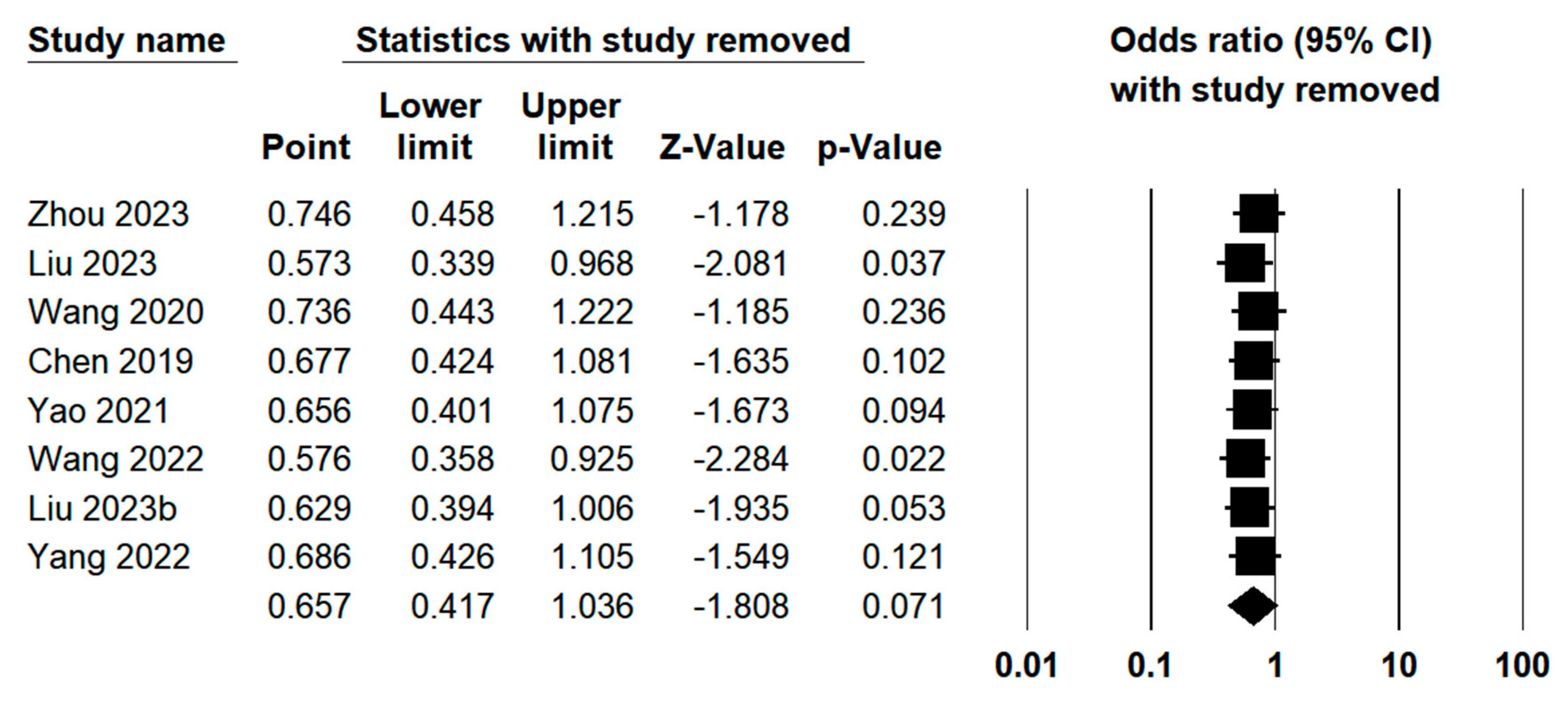
Figure 12.
Sensitivity analysis and forest plot of R0 resection distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 12.
Sensitivity analysis and forest plot of R0 resection distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
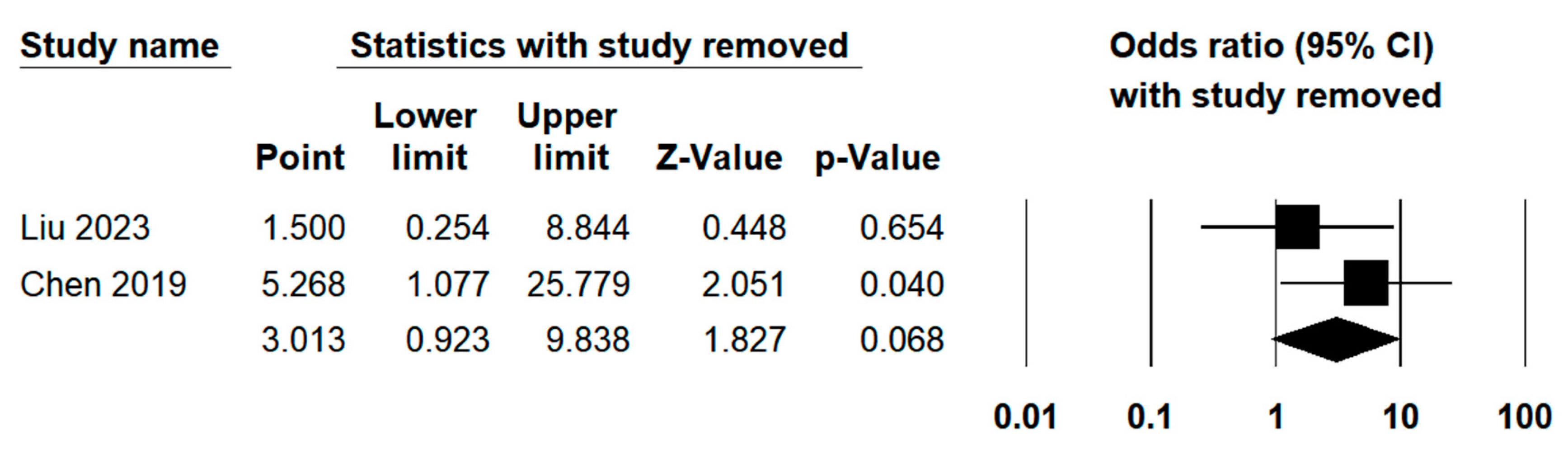
Figure 13.
Sensitivity analysis and forest plot of margin distance distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
Figure 13.
Sensitivity analysis and forest plot of margin distance distribution between indocyanine green fluorescence laparoscopy group and conventional laparoscopy group.
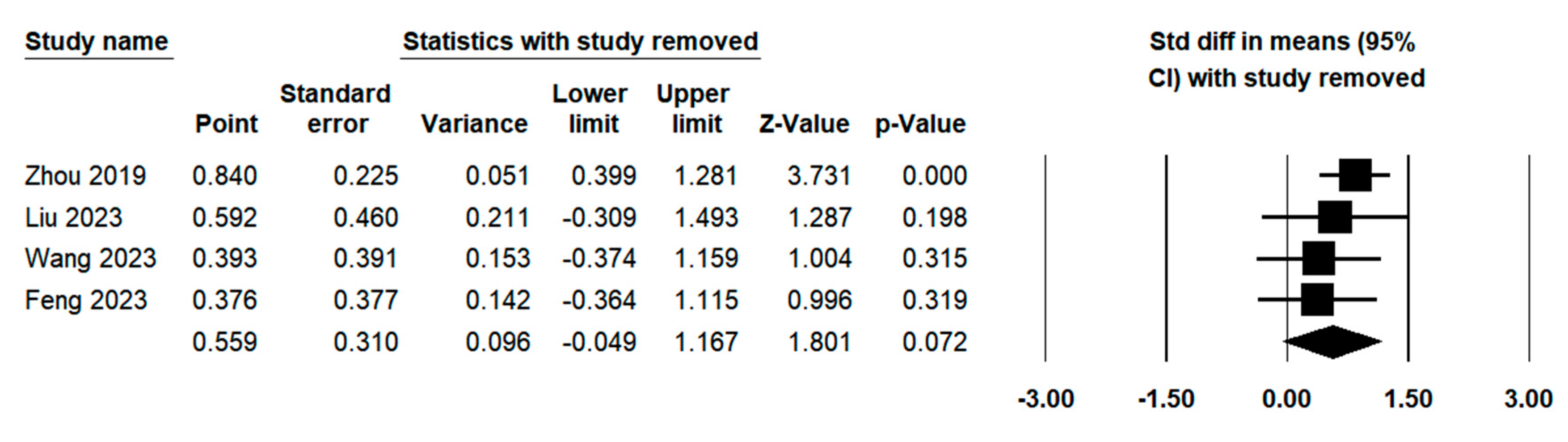
Figure 14.
Condensed summary of findings and certainty of evidence (as per GRADE).
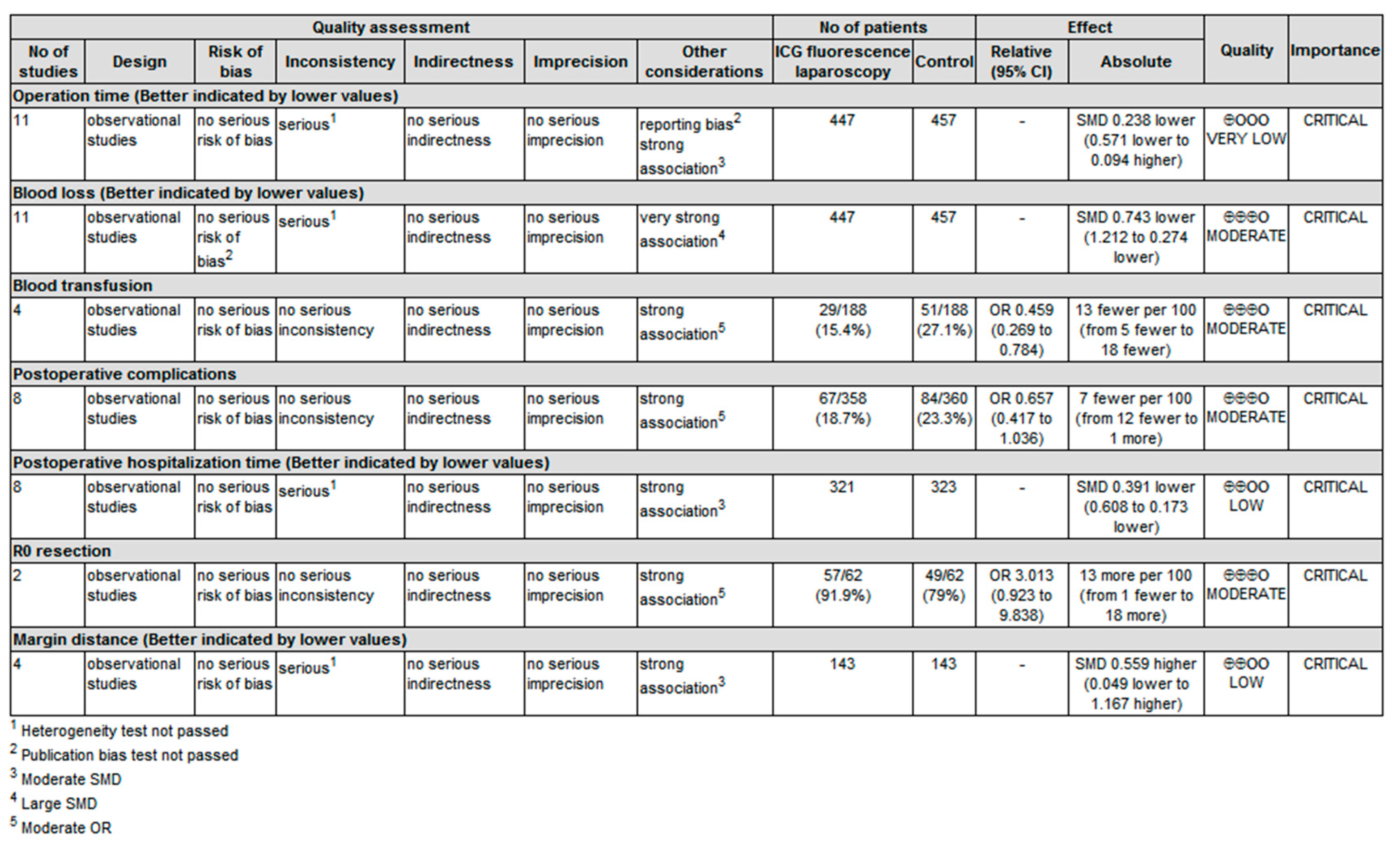

Table 1.
General descriptions of selected studies.
| ID | Author (Year) | Study design | Total Sample size | ICG sample size | CL sample size |
| 1 | Zhou 201926 | Retrospective study | 42 | 21 | 21 |
| 2 | Zhou 202327 | Retrospective study | 72 | 36 | 36 |
| 3 | Liu 202328 | Retrospective study | 100 | 50 | 50 |
| 4 | Wang 202029 | RCT | 148 | 74 | 74 |
| 5 | Chen 201930 | RCT | 24 | 12 | 12 |
| 6 | Yao 202131 | Retrospective study | 118 | 56 | 62 |
| 7 | Wang 202232 | Retrospective study | 162 | 81 | 81 |
| 8 | Wang 2020b33 | Retrospective study | 24 | 8 | 16 |
| 9 | Wang 202334 | RCT | 70 | 35 | 35 |
| 10 | Feng 202335 | Retrospective study | 74 | 37 | 37 |
| 11 | Guo 202136 | Retrospective study | 35 | 11 | 24 |
| 12 | Liu 2023b37 | Retrospective study | 52 | 28 | 24 |
| 13 | Yang 202238 | Retrospective study | 42 | 21 | 21 |
Table 2.
Quality assessments of the retrospective studies.
| Study | Selection | Comparability | Exposure |
| Zhou 2019 | *** | ** | *** |
| Zhou 2023 | *** | ** | ** |
| Liu 2023 | *** | ** | *** |
| Yao 2021 | *** | * | *** |
| Wang 2022 | *** | ** | *** |
| Wang 2020b | *** | * | ** |
| Feng 2023 | *** | ** | *** |
| Guo 2021 | *** | * | *** |
| Liu 2023b | *** | * | ** |
| Yang 2022 | *** | * | ** |
Table 3.
Results of publication bias and heterogeneity test in meta-analysis.
| Variables | N | Publication Bias | Heterogeneity Test | |||
| P value for rank correlation test | P value for regression intercept | I2 | Q | P | ||
| Basic Characteristics | ||||||
| Age | 11 | 0.815 | 0.890 | 17.02% | 12.052 | 0.282 |
| Gender | 10 | 0.929 | 0.441 | 0.00% | 5.937 | 0.746 |
| ASA | 3 | 0.602 | 0.591 | 0.00% | 0.788 | 0.674 |
| HBV infection | 7 | 0.881 | 0.776 | 0.00% | 1.733 | 0.943 |
| Liver cirrhosis | 9 | 0.677 | 0.984 | 0.00% | 2.315 | 0.970 |
| Child-Pugh classification | 6 | 0.005 | 0.026 | 0.00% | 0.882 | 0.972 |
| Tumor size (cm) | 9 | 0.404 | 0.466 | 79.43% | 38.889 | <0.001 |
| Operative outcomes | ||||||
| Operation time (min) | 11 | 0.036 | 0.043 | 82.77% | 58.025 | <0.001 |
| Blood loss (ml) | 11 | 0.312 | 0.370 | 90.82% | 108.948 | <0.001 |
| Blood transfusion | 4 | 0.174 | 0.210 | 0.00% | 1.107 | 0.775 |
| Postoperative outcomes | ||||||
| Complication | 8 | 0.805 | 0.767 | 12.10% | 7.964 | 0.336 |
| Postoperative hospitalization (day) |
8 | 0.108 | 0.109 | 43.13% | 12.308 | 0.091 |
| Pathological outcomes | ||||||
| R0 resection | 2 | 6.49% | 1.069 | 0.301 | ||
| Margin distance (mm) | 4 | 0.497 | 0.667 | 83.68% | 18.385 | <0.001 |
Table 4.
Meta-regression with potential moderators.
| Moderator | Operation time | Blood loss | Margin distance | ||||||
| β | P | I2 | β | P | I2 | β | P | I2 | |
| Age | 0.114 | 0.063 | 74.53% | 0.014 | 0.880 | 88.94% | |||
| Gender | 0.010 | 0.027 | 73.52% | 0.003 | 0.688 | 87.11% | |||
| ASA | -0.007 | 0.945 | 93.44% | ||||||
| HBV status | 0.006 | 0.270 | 83.69% | 0.003 | 0.698 | 88.87% | |||
| Liver cirrhosis status | 0.009 | 0.370 | 87.38% | 0.004 | 0.727 | 88.41% | |||
| Child-Pugh classification | 0.013 | 0.199 | 78.83% | -0.012 | 0.438 | 90.45% | |||
| Tumor size | -0.325 | 0.478 | 84.87% | ||||||
| Study type: RCT | 0.047 | 0.919 | 84.48% | -1.180 | 0.021 | 86.13% | 0.655 | 0.402 | 86.22% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



