
Submitted:
15 July 2025
Posted:
17 July 2025
You are already at the latest version
Abstract
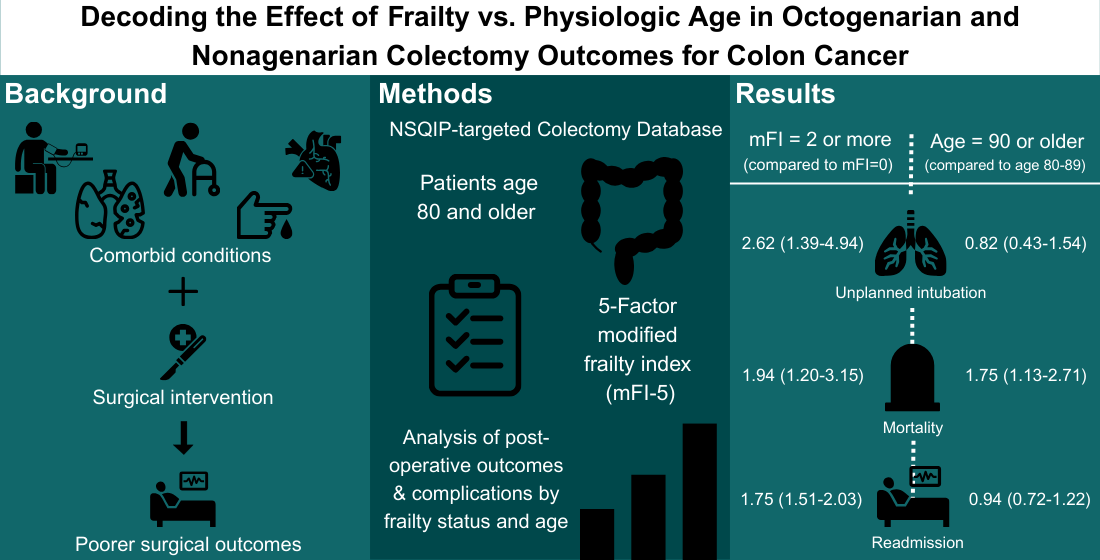
Background/Objectives: Colorectal surgeons continue to care for an aging cancer population with increasing co-morbidities and frailty. Frailty, characterized by a systemic physiologic decline associated with aging, is an increasingly popular focus in surgical outcomes research. This retrospective study aimed to investigate the impact of frailty on outcomes in the octogenarian and nonagenarian populations undergoing surgical treatment for colon cancer. Methods: Data from the National Surgical Quality Improvement Program (NSQIP) colectomy-targeted variables dataset from 2015 to 2021 were utilized for this analysis. Inclusion criteria included patients 80 years of age and older. Frailty was assessed using the 5-factor modified frailty index (mFI-5). The study examined post-operative outcomes across frailty groups in this population. Results: From 2015-2021, 10,815 patients >=80 years old with colon cancer underwent colectomy, 11.9% (n=1,285) were 90 years or older. Frailty significantly impacted post-operative colectomy outcomes in this population. On univariate analysis, frail patients had higher rates of pneumonia (p=0.002), unplanned intubation (p<0.001), mechanical ventilation for >48 hours (p=0.027), stroke (p<0.001), myocardial infarction (p = 0.010), sepsis (p=0.039), unplanned re-operation (p=0.029), and readmission (p < 0.001) compared to non-frail patients. On multivariate analysis, severe frailty (mFI-5 of 2 or more) was associated with an increased odds of unplanned intubation (p=0.003), length of stay >5 days (p<0.001), readmission (p<0.001), and mortality (p=0.007) compared to non-frail patients. Conclusions: Frailty plays a critical role in influencing the outcomes of octogenarians and nonagenarians undergoing colectomy for colon cancer within the NSQIP dataset. Future work should investigate whether addressing frailty prior to surgery in this population can improve patient’s post-operative course.
Keywords:
frailty
; octogenarian
; nonagenarian
; elderly patients
; colorectal cancer
; colectomy
; post-operative complications
; surgical outcomes
; risk stratification
1. Introduction
Advancements in medicine have led to increased life expectancy. Consequently, surgeons frequently encounter elderly populations with complex health challenges. Elderly individuals are more likely to have complex comorbidities and frailty, defined as the systemic physiologic decline associated with aging [1,2]. Frailty is highlighted in the surgical literature as an important determinant of post-operative outcomes, and is a better predictor of morbidity and mortality than chronological age [3]. Generally, frail patients are at risk for post-operative complications and poorer outcomes; however, less is known about the impact of frailty in the very elderly population. Understanding the impacts of frailty in the very elderly may allow surgeons to educate patients on risk of surgery with greater accuracy and to identify targets for optimization in the treatment of very elderly patients undergoing surgery for colon cancer.
Discussion of surgical care of the elderly and very elderly is becoming increasingly important given the rapidly growing advanced aged population, and surgical care of the elderly patient with colon cancer should be no exception. As of 2017, the percentage of individuals diagnosed with colorectal cancer aged 80 or above was 18% and 27% for males and females, respectively. Yet this same age group accounted for 27% and 40% of all colorectal cancer deaths [4]. Focused discussion of octogenarians and nonagenarians is underrepresented in colon cancer literature. Given that these very elderly patients are overrepresented in colon cancer deaths, there is a need to identify specific risk factors for morbidity and mortality in this population. Additionally, there is a need to understand the impacts of frailty in this very elderly population, given that frail patients with colorectal cancer treated with curative intent have worse oncologic and survival outcomes after controlling for age [5]. Studies have demonstrated that frail patients have increased rates of post-operative hemorrhage and infection, longer lengths of stay, discharge to assisted living facilities, and mortality [6,7]. Frail patients undergoing colectomy for colon cancer experience increases rates of infections, cardiopulmonary complications, anastomotic leakage, and numerous other complications, as well as increased mortality; however, the impact of frailty on specific post-operative complications in octogenarians and nonagenarians has not been studied [8]. Understanding specific complications more likely to occur in the frail, very elderly population is critical for gaining insight into how to best medically optimize patients pre-operatively and take preventative measures in their post-operative care.
The objective of this study was to investigate the impact of frailty on specific post-operative complications after colectomy for colon cancer in the octogenarian and nonagenarian population. The broad intention of this work is to provide insight into patient selection and areas of potential pre- and post-operative optimization for these patients.
2. Materials and Methods
2.1. Population and Data
The 2015-2021 American College of Surgeons National Surgical Quality Improvement Program (NSQIP) -targeted colectomy database was used identify octogenarian and nonagenarians undergoing any elective colectomy for colon cancer. NSQIP provides patient data from over 400 hospitals, including demographics, outcomes, and pre-operative, intra-operative, and post-operative variables for major surgical procedures. The database benefits from several unique features of its data collection, including trained data collectors, standardized variable definitions, and the diverse range of participating hospitals.
We included all patients with age 80 years or older undergoing elective operation for colon cancer with or without obstruction. Of note in NSQIP, all patients who are 90 years or older are assigned an age of 90 years to avoid potential identification of patients. We excluded patients that underwent an emergent operation, those with known metastatic disease prior to surgery, and those with unknown metastatic status prior to surgery.
Variables collected included age, sex, self-reported race and ethnicity, body mass index (BMI), comorbidities, American Joint Committee on Cancer 8th Edition clinical stage (AJCC clinical stage), pre-operative mechanical bowel preparation, pre-operative oral antibiotic administration, chemotherapy within the last 90 days, operative approach, and total operative time.
Frailty was measured using the modified 5-factor frailty index (mFI-5), which assigns one point to each of the following co-morbidities: diabetes mellitus (DM), congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), hypertension requiring medication, and non-independent functional status [9]. Frailty was subsequently categorized for analysis as non-frail (mFI-5 of 0), mildly frail (mFI-5 of 1), and severely frail (mFI-5 of 2 or more). These groups are based off prior literature [10,11]. Race was categorized into four groups (Asian American and Pacific Islander (AAPI), Black, Other, and White). ‘Other’ included American Indian or Alaska Native and patients with multiple races, other race, or unknown race. BMI was categorized as [underweight (<18.5), normal weight (18.5-24.9), overweight (25.0-29.9), obese (>29.9)]. AJCC clinical stage was calculated using provided values for pathologic T, N, and M staging.
We analyzed univariate differences in rates of the following post-operative complications between frailty groups: mortality, readmission, unplanned re-operation, length of hospital stay, anastomotic leak, prolonged nasogastric tube, superficial incisional surgical site infection (SSI), deep incisional SSI, organ/space SSI, sepsis, septic shock, Clostridioides difficile (C. diff) infection, wound disruption, pneumonia, unplanned intubation, pulmonary embolism (PE), mechanical ventilation for greater than 48 hours, acute renal failure, urinary tract infection (UTI), stroke or cerebrovascular accident (CVA), cardiac arrest requiring cardiopulmonary resuscitation (CPR), myocardial infarction (MI), intra-operative or post-operative blood transfusions, and deep vein thrombosis (DVT) requiring therapy. Of note, NSQIP collects and reports post-operative outcomes occurring within 30 days of the index surgical procedure, regardless of whether the patient is still hospitalized or has been discharged.
We performed multivariate analysis to test for independent association of frailty and age group with long length of stay (defined as hospital stay greater than 5 days), unplanned re-operation, unplanned intubation, readmission, and mortality while controlling for covariates.
2.2. Statistical Analysis
Univariate analyses were performed using chi-square tests for association for categorical variables, and the Mann-Whitney U test for length of stay, which was a nonparametric continuous variable. Multivariate analyses were performed with multivariable logistic regression and included variables with a p-value of less than 0.2 on chi-square or Mann-Whitney U tests. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were calculated. Multiple comparisons were adjusted for using a Bonferroni correction for 5 outcomes, with adjusted statistical significance set at α <0.01. All analyses were conducted using IBM SPSS Statistics (Version 28).
3. Results
3.1. Patient Factors by Frailty Group and Age Group
Of 10,815 patients included in our analysis, 9,530 (88.1%) were octogenarians and 1,285 (11.9%) were nonagenarians. In terms of frailty, 2,372 (21.9%) were non-frail, 5,540 (51.2%) were mildly frail, and 2,903 (26.8%) were severely frail. Table 1 presents all patient factors categorized by frailty group. Sex distribution varied significantly across groups, with the proportion of males increasing with increasing frailty (p<0.001). Regarding race, most patients in all groups were White, with proportions of White patients decreasing as frailty increased (Table 1). Most patients in all groups were non-Hispanic, but a higher proportion of patients in the severely frail group were Hispanic compared to the non-frail group (5.1% vs. 3.9%, p<0.001). BMI varied significantly among groups, with the proportion of obese patients increasing with increasing frailty, and the proportion of underweight patients decreasing with increasing frailty (p<0.001). There were no significant differences between frailty groups for receipt of pre-operative mechanical bowel prep, receipt of pre-operative oral antibiotic prep, receipt of chemotherapy within 90 days, AJCC stage, operative approach, or total operation time.
3.2. Post-Operative Outcomes by Frailty
Post-operative outcomes categorized by frailty group are described in Table 2. Length of hospital stay > 5 days was seen in greater proportions in mildly frail (41.8%) and severe frail (48.9%), compared to non-frail patients (38.1%) (p<0.001). The mortality rate was significantly higher in severely frail (3.5%) patients compared to non-frail (7.0%) and mildly frail (2.0%) patients (p<0.001). Severely frail patients also had higher rates of readmission (10.7%) than non-frail (7.0%) and mildly frail (9.7%) patients (p<0.001). Patients with increasing frailty had higher rates of pulmonary complications (pneumonia, unplanned intubation, mechanical ventilation for greater than 48 hours), cardiac complications (cardiac arrest requiring CPR and myocardial infarction), and neurologic complications (stroke or cerebrovascular accident). Some infectious complications were more frequent with increasing frailty (UTI [p=0.004], sepsis [p=0.039], septic shock [p=0.040], and C. diff [p=0.040]), however for other infectious complications the trend with frailty was not consistent or there were no significant differences between groups (superficial incisional SSI, deep incisional SSI, and organ/space SSS). Patients with increasing frailty had higher rates of prolonged nasogastric tube use (p<0.001), need for intra-operative/post-operative blood transfusions (p<0.001), and unplanned re-operation (p=0.029). There were no significant differences in rates of anastomotic leak and wound disruption. There were also no significant differences in rates of acute renal failure, pulmonary embolism, or deep vein thrombosis.
3.3. Post-Operative Outcomes by Age
Post-operative outcomes categorized by age group are described in Table 3. When outcomes were stratified by age, nonagenarian patients had a higher rate of mortality than octogenarians (3.3% vs. 2.2%, p=0.016). Nonagenarians were also more likely to have a length of stay >5 days (49.2% vs. 42.0%, p<0.001) but were not more likely than octogenarians to have unplanned operations (4.0% vs. 3.1%, p=0.132) or readmissions (9.4% vs. 8.7%, p=0.407). In terms of pulmonary complications, nonagenarians were more likely to have pneumonia in the postoperative period than octogenarians (3.9% vs 2.9%) but were not more likely to have unplanned intubation (1.7% vs. 1.3%, p=0.332). Interestingly, nonagenarians were less likely to require ventilator support >48 hours than octogenarians (0.4% vs 1.0%, p=0.033). Nonagenarians were more likely to require intra-operative/post-operative transfusions (12.1% vs 14.6%, p=0.010). Cardiac, neurologic, and other infectious complications did not differ between octogenarians and nonagenarians. Age was not significantly associated with any of the other complications in Table 3.
3.4. Multivariate Analysis
After controlling for confounding variables, the nonagenarian age group was significantly associated with longer length of stay (aOR 1.41, 95% CI 1.21-1.64). However, unplanned re-operation, unplanned intubation, readmission, and mortality did not significantly differ between octogenarians and nonagenarians (Table 4 and Table 5). Severe frailty was significantly associated with unplanned intubation (aOR 2.62, 95% CI 1.39-4.94), long length of stay (aOR 1.84, 95% CI 1.42-2.39), readmission (aOR 1.75, 95% CI 1.51-2.03), and mortality (aOR 1.94, 95% CI 1.20-3.15). Severe frailty was not associated with unplanned re-operation. Mild frailty was associated with long length of stay (aOR 1.57 95% CI 1.24-1.99) and readmission (aOR 1.24, 95% CI (1.09-1.42), but not unplanned re-operation, unplanned intubation, or mortality. Male sex was associated with an increased risk of unplanned re-operation, long length of stay, and mortality compared to female patients. Having an underweight BMI was associated with an increased risk of mortality compared to normal weight BMI. Total OR time was associated with unplanned re-operation. Pre-operative oral antibiotics were significantly associated with a reduced risk of unplanned intubation and a reduced risk of long length of stay. Ethnicity, chemotherapy within 90 days, pre-operative mechanical bowel prep, and clinical stage were not associated with any of the tested outcomes
4. Discussion
Our study found that among octogenarians and nonagenarians undergoing elective colectomy for colon cancer, frailty had a stronger impact than extremes of age on post-operative morbidity and mortality. Increasing frailty was associated with greater mortality, higher readmission rates, and longer hospital stays. For severe frailty, these associations persisted on multivariate analysis, indicating that having an mFI score of 2 or more is an independent predictor of mortality, long length of stay, and readmission in the octogenarian and nonagenarian population undergoing colectomy for colon cancer. Interestingly, nonagenarian age group was only associated with an increased risk of long length of stay, but not mortality or readmission. Overall, frailty was significantly associated with 16 of the 24 complications in this study, while age was only significantly associated with 5 complications. This indicates that frailty may be a better predictor than age for morbidity and mortality after colectomy in the octogenarian and nonagenarian population. This study contributes to existing literature by focusing specifically on octogenarians and nonagenarians undergoing colectomy for colon cancer and the impact of frailty on post-operative outcomes.
Prior work has examined post-operative colectomy outcomes in frail patients. However, few have focused on the very elderly. Sibia et al. (2023) used NSQIP to compare post-operative colectomy outcomes of frail vs non-frail patients, and found that frail patients of any age had an increased risk of superficial SSI, pneumonia, unplanned intubation, ventilator requirements for greater than 48 hours, acute renal failure, UTI, stroke, MI, transfusion, DVT, re-operation and readmission, but did not find a difference in rates of sepsis [12]. Notably, our study did not find differences in rates of superficial SSI, acute renal failure, or DVT, and did find an increased risk of sepsis and septic shock among frail patients, differing from the above findings. The mean age in the study by Sibia et al. was 64.3, and the mean age of frail patients was 69.6, which may influence the differences in outcomes between the two studies, highlighting the idea that frail very elderly patients behave differently than their younger, frail counterparts, and emphasizing the need for our study. Both our study and Sibia et al. found that severe frailty (mFI of 2 or more) was associated with readmission but not associated with reoperation on multivariate analysis. Interestingly, a study by Spence et al. (2021) found that age and American Society of Anesthesiologists (ASA) classification were better predictors of anastomotic leak than frailty, which is concordant with our finding that anastomotic leak was not associated with frailty [13].
Most studies of frailty in patients undergoing colectomy have utilized the modified 5-factor frailty index [10,11,12]. However, several studies have used other frailty measures, such as Obeid et al. (2012) whose study utilized an 11-factor modified frailty index based on the Canadian Study of Health and Aging Frailty Index and found that frail patients had greater rates of Clavien-Dindo class IV and V complications [14]. Another study by Normann et al. (2025) which utilized the Clinical Frailty Score (CFS-9) found that frail patients age 70 and older had higher 90-day and 1-year mortality rates [15]. While specific validated prospective frailty measures have been developed for other fields, including a trauma-specific validated frailty index by Joseph et al. (2022), there are not yet validated frailty measures for the colorectal surgery population that are based on clinically relevant variables available in the pre-operative setting [16]. The 5 factor mFI utilized in our study, from Subramaniam et al. (2018), has been validated in numerous retrospective studies of colorectal patients; however, it is not meant to be used prospectively [9]. Thus, additional research is needed to determine the optimal frailty metric for prospective use in the colorectal surgery population which could aid in patient selection and optimization.
Careful selection of patients who are candidates for surgical treatment is paramount in the care of very elderly patients with colon cancer, especially those who are also frail [17]. It is important to note that while frail patients are often multimorbid, not all multimorbid patients will be classified as frail [18]. Thus, considering both multimorbidity and frailty is necessary for ensuring careful patient selection in the very elderly population. Our study’s findings reveal specific combinations of multimorbidity and frailty that may be of higher priority to consider. Frailty in our study was associated with post-operative pulmonary, cardiac, and neurologic complications. It follows that frail, very elderly patients with pulmonary, cardiac, or neurologic comorbidities may be at even greater risk of adverse post-operative outcomes and decision to proceed with surgical management of colon cancer should be carefully considered in these patients. One area that our study did not closely investigate was the influence of operative approach on post-operative outcomes in very elderly patients undergoing colectomy. In this dataset, information about the surgical approach was missing for nearly 40% of patients and we chose not to include it in multivariate analyses. A study by Chok et al. (2023), which studied post-operative colectomy outcomes in patients 80 years of age and over, found that laparoscopic resection was associated with decreased length of hospital stay compared to an open approach [19]. A study by Lu et al. (2024) found that elderly patients undergoing right hemicolectomy for colon cancer had shorter lengths of hospital stay when a robotic-assisted approach rather than a laparoscopic approach was used [20]. This study focused on octogenarians and nonagenarians, but did not consider frailty, and there remains a need for further research into the influence of the operative approach in the post-operative course of frail, very elderly patients. Finally, future work should also consider the potential role of prehabilitation in the pre-operative management of frail, very elderly patients being considered for surgical treatment of colon cancer. The latest American Society of Colon and Rectal Surgeons (ASCRS) guidelines report that frail patients may benefit from prehabilitation, or multimodal optimization of risk factors, including nutritional optimization, exercise therapy, aggressive medical management of comorbidities, and psychosocial dynamics [21]. The guidelines also provide a strong recommendation for the integration of prehabilitation into surgical pathways for frail patients [21].
This study has several limitations. As a retrospective cohort study based on a large, administrative data set, there is a predetermined number of variables that can be analyzed, and certain variables, such as presence of arrhythmia, post-operative ileus, delirium, and more are inevitably omitted. In addition, the NSQIP dataset tracks only 30-day outcomes after surgery, limiting the conclusions that can be drawn in terms of time frame. This invites future studies to investigate the effects of frailty on post-operative colectomy outcomes in frail elderly patients in the even longer term. Other inherent limitations to utilizing NSQIP include potential loss to follow up with patients presenting to hospitals other than the index hospital or missed comorbidities that were not captured by medical coding. Additionally, only including data from NSQIP hospitals may lead to selection bias for patients treated at hospitals with more robust quality improvement programs, potentially skewing toward better outcomes. Finally, limitations of using mFI-5 as frailty as opposed to a more comprehensive frailty measure like the Clinical Frailty Score include limited discrimination of more frail patients and omission of certain domains of frailty – such as cognitive ability and daily functioning. While these limitatons exist, the latest ASCRS recommendations endorse the mFI-5 as a valuable marker of frailty [9].
5. Conclusions
This study examines the impact of frailty on post-operative outcomes after colectomy for colon cancer among octogenarians and nonagenarians. We found that frailty was independently associated with an increased risk of unplanned intubation, long length of stay, readmission, and mortality. Frailty was also associated with cardiac, pulmonary, and neurologic complications. These findings underscore the importance of using frailty as a screening tool to guide patient selection for colectomy. Frailty screening may also identify patients who would benefit from prehabilitation prior to surgery. Future studies may look further into more detailed measures of frailty, the effects of frailty on longer-term outcomes (>30 days), and the efficacy of utilizing prehabilitation methods to improve surgical care of elderly patients.
Author Contributions
Conceptualization: AH, KK, VH.; Methodology: AH, KK, AR; Formal analysis: AH, AR; Resources: VH; Writing—original draft preparation: PD, CC, AH, AR; Writing—review and editing: All authors; Supervision: VH; Project administration: AH, AR, VH. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not involve direct patient contact and was conducted using de-identified data from a large administrative database. As such, it was except from Institutional Review Board review at our institution.
Informed Consent Statement
This study utilized de-identified data obtained from a large administrative database. Therefore, individual informed consent was not required or obtained.
Data Availability Statement
The data used in this study were obtained from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) colectomy-targeted dataset for the years 2015 to 2021. These data are not publicly available due to privacy and ethical restrictions, but access can be requested through the American College of Surgeons NSQIP Participant Use File (PUF) program for eligible institutions.
Acknowledgments
The authors would like to acknowledge the support of the Dewitt Daughtry Family Department of Surgery at the University of Miami Miller School of Medicine in this work.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| NSQIP | National Surgery Quality Improvement Program |
| mFI-5 | 5 factor modified frailty index |
| ACS | American College of Surgeons |
| BMI | Body mass index |
| AJCC | American Joint Committee on Cancer |
| DM | Diabetes mellitus |
| CHF | Congestive heart failure |
| COPD | Chronic obstructive pulmonary disease |
| AAPI | Asian American and Pacific Islander |
| SSI | Surgical site infection |
| C. diff | Clostridioides difficile |
| PE | Pulmonary embolism |
| UTI | Urinary tract infection |
| CVA | Cerebrovascular accident |
| CPR | Cardiopulmonary resuscitation |
| MI | Myocardial infraction |
| DVT | Deep vein thrombosis |
| aOR | Adjusted odds ratio |
| CI | Confidence interval |
| IQR | Interquartile range |
| OR | Operating room |
| ASA | American Society of Anesthesiologists |
| ICU | Intensive care unit |
References
- Itatani, Y., K. Kawada, and Y. Sakai. Treatment of Elderly Patients with Colorectal Cancer. BioMed Research International, 2018. 2018: p. 1-8.
- Agathis, A.Z.; Bangla, V.G.; Divino, C.M. Assessing the mFI-5 frailty score and functional status in geriatric patients undergoing inguinal hernia repairs. Hernia 2023, 28, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-S.; Watts, J.N.; Peel, N.M.; Hubbard, R.E. Frailty and post-operative outcomes in older surgical patients: a systematic review. BMC Geriatr. 2016, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA: A Cancer Journal for Clinicians, 2017. 67(3): p. 177-193.
- Davey, M.G.; Joyce, W.P. Impact of frailty on oncological outcomes in patients undergoing surgery for colorectal cancer – A systematic review and meta-analysis. Surg. 2022, 21, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Niemeläinen, S.; Huhtala, H.; Ehrlich, A.; Kössi, J.; Jämsen, E.; Hyöty, M. Surgical and functional outcomes and survival following Colon Cancer surgery in the aged: a study protocol for a prospective, observational multicentre study. BMC Cancer, 2021. 21(1).
- Moreno-Carmona, M.R.; Serra-Prat, M.; Riera, S.A.; Estrada, O.; Ferro, T.; Querol, R. Effect of frailty on postoperative complications, mortality, and survival in older patients with non-metastatic colon cancer: A systematic review and meta-analysis. J. Geriatr. Oncol. 2023, 15, 101639. [Google Scholar] [CrossRef] [PubMed]
- Dressler, J.A.; Shah, N.; Lueckel, S.N.M.; Cioffi, W.G.J. Predicting Anastomotic Leak After Elective Colectomy: Utility of a Modified Frailty Index. Dis. Colon Rectum 2021, 65, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, S.; Aalberg, J.J.; Soriano, R.P.; Divino, C.M. New 5-Factor Modified Frailty Index Using American College of Surgeons NSQIP Data. J. Am. Coll. Surg. 2018, 226, 173–181e8. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Stem, M.; Cerullo, M.; Gearhart, S.L.; Safar, B.; Fang, S.H.; Weiss, M.J.; He, J.; Efron, J.E. The Effect of Frailty Index on Early Outcomes after Combined Colorectal and Liver Resections. J. Gastrointest. Surg. 2017, 22, 640–649. [Google Scholar] [CrossRef] [PubMed]
- McGovern, J.; Grayston, A.; Coates, D.; Leadbitter, S.; Hounat, A.; Horgan, P.G.; Dolan, R.D.; McMillan, D.C. The relationship between the modified frailty index score (mFI-5), malnutrition, body composition, systemic inflammation and short-term clinical outcomes in patients undergoing surgery for colorectal cancer. BMC Geriatr. 2023, 23, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sibia, U.S.; Badve, S.B.; Istl, A.C.; Klune, J.R.; Riker, A.I. Impact of Frailty Upon Surgical Decision-Making for Left-Sided Colon Cancer. Ochsner J. 2023, 23, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Spence, R.T.; Hirpara, D.H.; Doshi, S.; Quereshy, F.A.; Chadi, S.A. Will My Patient Survive an Anastomotic Leak? Predicting Failure to Rescue Using the Modified Frailty Index. Ann. Surg. Oncol. 2020, 28, 2779–2787. [Google Scholar] [CrossRef] [PubMed]
- Obeid, N.M.; Azuh, O.; Reddy, S.; Webb, S.; Reickert, C.; Velanovich, V.; Horst, H. M.; Rubinfeld, I. Predictors of critical care-related complications in colectomy patients using the National Surgical Quality Improvement Program: exploring frailty and aggressive laparoscopic approaches. J Trauma Acute Care Surg, 2012. 72(4): p. 878-83.
- Normann, M.; Ekerstad, N.; Angenete, E.; Prytz, M. Frailty Is an Independent Marker of Post-Operative Mortality Following Colorectal Cancer Resection Surgery in Older Adults. J. Surg. Oncol. 2025. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.; Saljuqi, A.T.; Amos, J.D.; Teichman, A.; Whitmill, M.L.; Anand, T.; Hosseinpour, H.; Burruss, S.K.; Dunn, J.A.; Najafi, K.; et al. Prospective validation and application of the Trauma-Specific Frailty Index: Results of an American Association for the Surgery of Trauma multi-institutional observational trial. J. Trauma Acute Care Surg. 2022, 94, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Neuman, H.B.; O'COnnor, E.S.; Weiss, J.; LoConte, N.K.; Greenblatt, D.Y.; Greenberg, C.C.; Smith, M.A. Surgical treatment of colon cancer in patients aged 80 years and older. Cancer 2012, 119, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Samaniego, L.L.; Rodríguez-Mañas, L.; Bernabei, R.; Onder, G. Frailty and Multimorbidity: A Systematic Review and Meta-analysis. Journals Gerontol. Ser. A 2018, 74, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Chok, A.Y.; Tan, I.E.-H.; Zhao, Y.; Chee, M.Y.M.; Chen, H.L.R.; Ang, K.A.; Au, M.K.H.; Tan, E.J.K.W. Clinical outcomes and cost comparison of laparoscopic versus open surgery in elderly colorectal cancer patients over 80 years. Int. J. Color. Dis. 2023, 38, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.-C.; Lu, C.-T.; Chang, K.-Y.; Chun-Li, W.; Wu, C.-Y. Robot-assisted vs. laparoscopic right hemicolectomy in octogenarians and nonagenarians: an analysis of the US nationwide inpatient sample 2005–2018. Aging Clinical and Experimental Research, 2024. 36(1).
- Saur, N.M.; Davis, B.R.; Montroni, I.M.; Shahrokni, A.M.; Rostoft, S.M.; Russell, M.M.; Mohile, S.G.M.; Suwanabol, P.A.; Lightner, A.L.; Poylin, V.; et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Perioperative Evaluation and Management of Frailty Among Older Adults Undergoing Colorectal Surgery. Dis. Colon Rectum 2022, 65, 473–488. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Patient factors by frailty of patients undergoing elective colectomy for colon cancer in ACS-NSQIP database, 2015-2021.
Table 1.
Patient factors by frailty of patients undergoing elective colectomy for colon cancer in ACS-NSQIP database, 2015-2021.
|
Overall N=10,815 |
Non-frail (mFI-5=0) N=2,372 (21.9%) |
Mildly frail (mFI-5=1) N=5,540 (51.2%) |
Severely Frail (mFI-5=2 or more) N=2,903 (26.8%) |
p-value | |
| Age Group | <0.001* | ||||
| 80-89 (octogenarian) | 9,530/10,815 (88.1) | 2,088/2,372 (88.0) | 4,824/5,540 (87.1) | 2,618/2,903 (90.2) | |
| 90+ (nonagenarian) | 1,285/10,815 (11.9) | 284/2,372 (12.0) | 716/5,540 (12.9) | 285/2,903 (9.8) | |
| Sex | <0.001* | ||||
| Female | 6,027/10,815 (55.7) | 1,341/2,372 (56.5) | 3,168/5,540 (57.2) | 1,518/2,903 (52.3) | |
| Male | 4,788/10,815 (44.3) | 1,031/2,372 (43.5) | 2,372/5,540 (42.8) | 1,385/2,903 (47.7) | |
| Race | <0.001* | ||||
| AAPI | 465/8,340 (5.6) | 89/1,740 (5.1) | 217/4,340 (5.0) | 159/2,260 (7.0) | |
| Black | 545/8,340 (6.5) | 68/1,740 (3.9) | 265/4,340 (6.1) | 212/2,260 (9.4) | |
| White | 7,284/8,340 (87.3) | 1,570/1,740 (92.0) | 3,841/4,340 (88.5) | 1,873/2,260 (82.9) | |
| Other | 46/8,340 (0.6) | 13/1,740 (0.7) | 17/4,340 (0.4) | 16/2,260 (0.7) | |
| Hispanic Ethnicity | <0.001* | ||||
| Yes | 316/8,454 (3.7) | 69/1,763 (3.9) | 128/4,377 (2.9) | 119/2,314 (5.1) | |
| No | 8,138/8,454 (96.3) | 1,694/1,763 (96.1) | 4,249/4,377 (97.1) | 2,195/2,314 (94.9) | |
| BMI | <0.001* | ||||
| Normal Weight 18.5-24.9 | 4,108/10,815 (38.0) | 1,137/2,372 (47.9) | 2,102/5,540 (37.9) | 869/2,903 (29.9) | |
| Underweight <18.5 | 400/10,815 (3.7) | 148/2,372 (6.2) | 167/5,540 (3.0) | 85/2,903 (2.9) | |
| Overweight 25.0-29.9 | 3,926/10,815 (36.3) | 765/2,372 (32.3) | 2,101/5,540 (37.9) | 1,060/2,903 (36.5) | |
| Obese >29.9 | 2,381/10,815 (22.0) | 322/2,372 (13.6) | 1,170/5,540 (21.1) | 889/2,903 (30.6) | |
| Pre-operative Mechanical Bowel Prep | 0.522 | ||||
| Yes | 6,906/9,590 (72.0) | 1,509/2,124 (71.0) | 3,531/4,880 (72.4) | 1,866/2,586 (72.2) | |
| No | 2,684/9,590 (28.0) | 615/2,124 (29.0) | 1,349/4,880 (27.6) | 720/2,586 (27.8) | |
| Pre-operative Oral Antibiotic Prep | 0.385 | ||||
| Yes | 5,732/9,713 (59.0) | 1,238/2,144 (57.7) | 2,954/4,966 (59.5) | 1,540/2,603 (59.2) | |
| No | 3,981/9,713 (41.0) | 906/2,144 (42.3) | 2,012/4,966 (40.5) | 1,063/2,603 (40.8) | |
| Chemotherapy within 90 Days | 0.135 | ||||
| Yes | 407/10,700 (3.8) | 104/2,343 (4.4) | 206/5,491 (3.8) | 97/2,866 (3.4) | |
| No | 10,293/10,700 (96.2) | 2,239/2,343 (95.6) | 5,285/5,491 (96.2) | 2,769/2,866 (96.6) | |
| Clinical Stage |
0.173 |
||||
| Stage 0 | 178/10,289 (1.7) | 39/2,264 (1.7) | 91/5,253 (1.7) | 48/2,772 (1.7) | |
| Stage I | 2,298/10,289 (22.3) | 468/2,264 (20.7) | 1,207/5,253 (23.0) | 623/2,772 (22.5) | |
| Stage II | 4,467/10,289 (43.4) | 998/2,264 (44.1) | 2,302/5,253 (43.8) | 1,167/2,772 (42.1) | |
| Stage III | 3,346/10,289 (32.5) | 759/2,264 (33.5) | 1,653/5,253 (31.5) | 2934/2,772 (33.7) | |
| Operative Approach | 0.591 | ||||
| Laparoscopic | 4,401/6,564 (67.0) | 958/1,418 (67.6) | 2,314/3,462 (67.5) | 1,129/1,720 (65.5) | |
| Robotic | 736/6,564 (11.2) | 149/1,418 (10.5) | 382/3,462 (11.2) | 205/1,720 (11.9) | |
| Open | 1,472/6,564 (21.7) | 311/1,418 (21.9) | 730/3,462 (21.3) | 386/1,720 (22.4) | |
| Total Operation Time | |||||
| Median [IQR] | 150 [110,204] | 150 [112,203] | 149 [108,202] | 152 [112,207] | 0.069 |
*p<0.05; Abbreviations: ACS-NSQIP=American College of Surgeons National Surgery Quality Improvement Program, mFI=modified frailty index, AAPI=Asian American or Pacific Islander, BMI=body mass index, IQR=interquartile range.
Table 4.
Regression models for unplanned re-operation, unplanned intubation, and mortality.
| Unplanned re-operation | Unplanned intubation | Mortality | ||||
| aOR (95% CI) | p-value | aOR (95% CI) | p-value | aOR (95% CI) | p-value | |
| Age (years) | ||||||
| 80-89 (octogenarian) | Ref | --- | Ref | --- | Ref | --- |
| 90+ (nonagenarian) | 0.83 (0.55-1.27) | 0.393 | 0.82 (0.43-1.54) | 0.531 | 1.75 (1.13-2.71) | 0.012 |
| Sex | ||||||
| Female | Ref | --- | Ref | --- | Ref | --- |
| Male | 1.42 (1.10-1.85) | 0.005* | 1.45 (0.99-2.13) | 0.056 | 1.88 (1.34-2.65) | <0.001* |
| Race | ||||||
| Black | 1.41 (0.68-2.93) | 0.355 | 1.77 (0.70-4.77) | 0.257 | 2.39 (0.86-6.60) | 0.093 |
| Other | 0.82 (0.10-6.55) | 0.853 | --- | --- | 6.07 (1.14-32.30) | 0.035 |
| AAPI | Ref | --- | Ref | --- | Ref | --- |
| White | 1.38 (0.78-2.43) | 0.265 | 1.33 (0.60-2.94) | 0.490 | 2.21 (0.95-5.14) | 0.066 |
| Ethnicity | ||||||
| Hispanic | 1.45 (0.75-2.81) | 0.269 | 2.04 (0.87-4.77) | 0.100 | 0.62 (0.19-2.00) | 0.426 |
| Non-Hispanic | Ref | --- | Ref | --- | Ref | --- |
| BMI | ||||||
| Normal weight 18.5-24.9 | Ref | --- | Ref | --- | Ref | --- |
| Underweight <18.5 | 0.74 (0.34-1.61) | 0.444 | 1.09 (0.38-3.08) | 0.875 | 3.74 (2.05-6.83) | <0.001* |
| Overweight 25.0-29.9 | 0.78 (0.58-1.04) | 0.090 | 0.84 (0.54-1.32) | 0.448 | 1.00 (0.68-1.48) | 0.998 |
| Obese >29.9 | 0.58 (0.40-0.85) | 0.005* | 0.90 (0.54-1.50) | 0.690 | 0.79 (0.48-1.29) | 0.345 |
| Chemotherapy within 90 days | ||||||
| Yes | 0.74 (0.36-1.54) | 0.420 | 0.62 (0.19-2.01) | 0.428 | 1.29 (0.59-2.84) | 0.530 |
| No | Ref | --- | Ref | --- | Ref | --- |
| Pre-operative mechanical bowel prep | ||||||
| Yes | 0.73 (0.52-1.02) | 0.062 | 1.22 (0.75-2.00) | 0.422 | 0.85 (0.56-1.29) | 0.440 |
| No | Ref | --- | Ref | --- | Ref | --- |
| Pre-operative oral antibiotic prep | ||||||
| Yes | 0.93 (0.68-1.28) | 0.668 | 0.49 (0.32-0.75) | 0.001* | 0.62 (0.42-0.90) | 0.013 |
| No | Ref | --- | Ref | --- | Ref | --- |
| Clinical stage | ||||||
| Stage 0 | Ref | --- | Ref | --- | Ref | --- |
| Stage I | 2.21 (0.53-9.30) | 0.278 | 0.89 (0.21-3.90) | 0.881 | 1.28 (0.30-5.53) | 0.743 |
| Stage II | 2.52 (0.61-10.43) | 0.203 | 0.97 (0.23-4.14) | 0.972 | 1.25 (0.29-5.27) | 0.766 |
| Stage III | 2.27 (0.54-9.45) | 0.261 | 0.88 (0.21-3.80) | 0.868 | 1.61 (0.38-6.82) | 0.520 |
| mFI | ||||||
| 0 | Ref | --- | Ref | --- | Ref | --- |
| 1 | 1.40 (0.98-2.00) | 0.068 | 1.78 (0.96-3.27) | 0.066 | 1.09 (0.69-1.75) | 0.706 |
| 2 or more | 1.49 (1.01-2.22) | 0.047 | 2.62 (1.39-4.94) | 0.003* | 1.94 (1.20-3.15) | 0.007* |
| Total OR time | 1.003 (1.001-1.004) | 0.001* | 1.002 (1.000-1.004) | 0.077 | 1.000 (0.998-1.003) | 0.670 |
*p<0.01; Abbreviations: aOR=adjusted odds ratio, CI=confidence interval; AAPI=Asian American or Pacific Islander; BMI=body mass index; mFI=modified frailty index; OR=operating room.
Table 2.
Post-operative outcomes by frailty of patients undergoing elective colectomy for colon cancer in ACS-NSQIP database, 2015-2021.
Table 2.
Post-operative outcomes by frailty of patients undergoing elective colectomy for colon cancer in ACS-NSQIP database, 2015-2021.
|
Overall N=10,815 |
Non-frail (mFI-5=0) N=2,372 (21.9%) |
Mildly frail (mFI-5=1) N=5,540 (51.2%) |
Severely Frail (mFI-5=2 or more) N=2,903 (26.8%) |
p-value | |
| Anastomotic leak | 247/10,815 (2.3) | 51/2,372 (2.2) | 123/5,540 (2.2) | 73/2,903 (2.5) | 0.662 |
| Prolonged Nasogastric Tube | 1,554/10,815 (14.4) | 276/2,372 (11.6) | 812 /5,540 (14.7) | 466/2,903 (16.1) | <0.001* |
| Superficial Incisional SSI |
246/10,815 (2.3) | 58/2,372 (2.4) | 110/5,540 (2.0) | 78/2,903 (2.7) | 0.100 |
| Deep Incisional SSI | 33/10,815 (0.3) | 11/2,372 (0.5) | 10/5,540 (0.2) | 12/2,903 (0.4) | 0.052 |
| Organ/Space SSI | 304/10,815 (2.8) | 66/2,372 (2.8) | 142/5,540 (2.6) | 96/2,903 (3.3) | 0.145 |
| Wound Disruption | 49/10,815 (0.5) | 12/2,372 (0.5) | 24/5,540 (0.4) | 13/2,903 (0.4) | 0.906 |
| Pneumonia | 322/10,815 (3.0) | 54/2,372 (2.3) | 156/5,540 (2.8) | 112/2,903 (3.9) | 0.002* |
| Unplanned Intubation | 178/10,815 (1.6) | 24/2,372 (1.0) | 84/5,540 (1.5) | 70/2,903 (2.4) | <0.001* |
| Pulmonary Embolism | 87/10,815 (0.8) | 17/2,372 (0.7) | 45/5,540 (0.8) | 25/2,903 (0.9) | 0.839 |
| Mechanical Ventilation for > 48 Hours | 100/10,815 (0.9) | 15/2,372 (0.6) | 47/5,540 (0.8) | 38/2,903 (1.3) | 0.027* |
| Acute Renal Failure | 43/10,815 (0.4) | 10/2,372 (0.4) | 20/5,540 (0.4) | 13/2,903 (0.4) | 0.816 |
| Urinary Tract Infection | 274/10,815 (2.5) | 61/2,372 (2.6) | 117/5,540 (2.1) | 96/2,372 (3.3) | 0.004* |
| Stroke/CVA | 65/10,815 (0.6) | 6/2,372 (0.3) | 25/5,540 (0.5) | 34/2,903 (1.2) | <0.001* |
| Cardiac Arrest Requiring CPR | 77/10,815 (0.7) | 9/2,372 (0.4) | 40/5,540 (0.7) | 28/2,903 (1.0) | 0.042* |
| Myocardial Infarction | 173/10,815 (1.6) | 22/2,372 (0.9) | 95/5,540 (1.7) | 56/2,903 (1.9) | 0.010* |
| Transfusions intra-op/post-op | 1,343/10,815 (12.4) | 240/2,372 (10.1) | 672/5,540 (12.1) | 431/2,903 (14.8) | <0.001* |
| DVT Requiring Therapy | 98/10,815 (0.9) | 15/2,372 (0.6) | 53/5,540 (1.0) | 30/2,903 (1.0) | 0.264 |
| Sepsis | 197/10,815 (1.8) | 35/2,372 (1.5) | 94/5,540 (1.7) | 68/2,903 (2.3) | 0.039* |
| Septic Shock | 140/10,815 (1.3) | 23/2,372 (1.0) | 67/5,540 (1.2) | 50/2,903 (1.7) | 0.040* |
| C. diff | 162/10,815 (1.5) | 28/2,372 (1.2) | 74/5,540 (1.3) | 60/2,903 (2.1) | 0.040* |
| Unplanned Re-operation | 419/10,815 (3.9) | 70/2,372 (3.0) | 226/5,540 (4.1) | 123/2,903 (4.2) | 0.029* |
| Any Readmission | 1,011/10,815 (9.3) | 166/2,372 (7.0) | 535/5,540 (9.7) | 310/2,903 (10.7) | <0.001* |
| Length of hospital stay > 5 days | 4,598/10,727 (42.9) | 897/2,356 (38.1) | 2,300/5,507 (41.8) | 1,401/2,864 (48.9) | <0.001* |
| Mortality | 251/10,815 (2.3) | 38/2,372 (1.6) | 111/5,540 (2.0) | 102/2,902 (3.5) | <0.001* |
*p<0.05; Abbreviations: ACS-NSQIP=American College of Surgeons National Surgery Quality Improvement Program, mFI=modified frailty index, SSI=surgical site infection, CVA=cerebral vascular accident, CPR=cardiopulmonary resuscitation, DVT=deep vein thrombosis, C. diff=Clostridioides difficile.
Table 3.
Post-operative outcomes by age of patients undergoing elective colectomy for colon cancer in ACS-NSQIP database, 2015-2021.
Table 3.
Post-operative outcomes by age of patients undergoing elective colectomy for colon cancer in ACS-NSQIP database, 2015-2021.
|
Overall N=10,815 |
Age 80-89 N=9,530 (88.1%) |
Age 90+ and older N=1,285 (11.9%) |
p-value | |
| Anastomotic leak | 247/10,815 (2.3) | 222/9,530 (2.3) | 25/1,285 (1.9) | 0.787 |
| Prolonged Nasogastric Tube | 1,554/10,815 (14.4) | 1,369/9,530 (14.4) | 185/1,285 (14.1) | 0.748 |
| Superficial Incisional SSI |
246/10,815 (2.3) | 213/9,530 (2.2) | 33/1,285 (2.6) | 0.452 |
| Deep Incisional SSI | 33/10,815 (0.3) | 29/9,530 (0.3) | 4/1,285 (0.3) | 0.966 |
| Organ/Space SSI | 304/10,815 (2.8) | 276/9,530 (2.9) | 28/1,285 (2.2) | 0.144 |
| Wound Disruption | 49/10,815 (0.5) | 44/9,530 (0.5) | 5/1,285 (0.4) | 0.716 |
| Pneumonia | 322/10,815 (3.0) | 272/9,530 (2.9) | 50/1,285 (3.9) | 0.040* |
| Unplanned Intubation | 178/10,815 (1.6) | 161/9,530 (1.7) | 17/1,285 (1.3) | 0.332 |
| Pulmonary Embolism | 87/10,815 (0.8) | 79/9,530 (0.8) | 8/1,285 (0.6) | 0.437 |
| Mechanical Ventilation for > 48 Hours | 100/10,815 (0.9) | 95/9,530 (1.0) | 5/1,285 (0.4) | 0.033* |
| Acute Renal Failure | 43/10,815 (0.4) | 41/9,530 (0.4) | 2/1,285 (0.2) | 0.142 |
| Urinary Tract Infection | 274/10,815 (2.5) | 238/9,530 (2.5) | 36/1,285 (2.8) | 0.515 |
| Stroke/CVA | 65/10,815 (0.6) | 55/9,530 (0.6) | 10/1,285 (0.8) | 0.381 |
| Cardiac Arrest Requiring CPR | 77/10,815 (0.7) | 71/9,530 (0.7) | 6/1,285 (0.5) | 0.266 |
| Myocardial Infarction | 173/10,815 (1.6) | 150/9,530 (1.6) | 23/1,285 (1.8) | 0.563 |
| Transfusions intra-op/post-op | 1,343/10,815 (12.4) | 1,155/9,530 (12.1) | 188/1,285 (14.6) | 0.010* |
| DVT Requiring Therapy | 98/10,815 (0.9) | 82/9,530 (0.9) | 16/1,285 (1.2) | 0.172 |
| Sepsis | 197/10,815 (1.8) | 175/9,530 (1.8) | 22/1,285 (1.7) | 0.755 |
| Septic Shock | 140/10,815 (1.3) | 119/9,530 (1.2) | 21/1,285 (1.6) | 0.251 |
| C. diff | 162/10,815 (1.5) | 137/9,530 (1.4) | 25/1,285 (1.9) | 0.370 |
| Unplanned Re-operation | 419/10,815 (3.9) | 379/9,530 (4.0) | 40/1,285 (3.1) | 0.132 |
| Any Readmission | 1,011/10,815 (9.3) | 899/9,530 (9.4) | 112/1,285 (8.7) | 0.407 |
| Length of hospital stay > 5 days | 4,598/10,727 (42.9) | 3,973/9,456 (42.0) | 625/1,271 (49.2) | <0.001* |
| Mortality | 251/10,815 (2.3) | 209/9,530 (2.2) | 42/1,285 (3.3) | 0.016* |
*p<0.05; Abbreviations: ACS-NSQIP=American College of Surgeons National Surgery Quality Improvement Program, SSI=surgical site infection, CVA=cerebrovascular accident, CPR=cardiopulmonary resuscitation, DVT=deep vein thrombosis, C. diff=Clostridioides difficile.
Table 5.
Regression models for long length of stay (>5 days) and readmission.
| Long length of stay (>5 days) | Readmission | |||
| aOR (95% CI) | p-value | aOR (95% CI) | p-value | |
| Age (years) | ||||
| 80-89 | Ref | --- | Ref | --- |
| 90+ | 1.41 (1.21-1.64) | <0.001* | 0.94 (0.72-1.22) | 0.627 |
| Sex | ||||
| Female | Ref | --- | Ref | --- |
| Male | 1.21 (1.09-1.34) | <0.001* | 1.08 (0.92-1.28) | 0.361 |
| Race | ||||
| Black | 0.85 (0.64-1.13) | 0.272 | 1.51 (0.97-2.34) | 0.067 |
| Other | 0.49 (0.23-1.03) | 0.058 | 1.05 (0.35-3.15) | 0.927 |
| AAPI | Ref | --- | Ref | --- |
| White | 0.84 (0.68-1.04) | 0.111 | 1.11 (0.78-1.58) | 0.561 |
| Ethnicity | ||||
| Hispanic | 0.90 (0.65-1.23) | 0.492 | 1.26 (0.80-2.00) | 0.317 |
| Non-Hispanic | Ref | --- | Ref | --- |
| BMI | ||||
| Normal weight 18.5-24.9 | Ref | --- | Ref | --- |
| Underweight <18.5 | 1.33 (1.01-1.75) | 0.045 | 1.31 (0.86-2.01) | 0.214 |
| Overweight 25.0-29.9 | 0.92 (0.81-1.03) | 0.137 | 1.07 (0.89-1.30) | 0.483 |
| Obese >29.9 | 0.99 (0.86-1.14) | 0.877 | 0.94 (0.75-1.18) | 0.604 |
| Chemotherapy within 90 days | ||||
| Yes | 1.02 (0.79-1.32) | 0.900 | 1.11 (0.75-1.65) | 0.609 |
| No | Ref | --- | Ref | --- |
| Pre-operative mechanical bowel prep | ||||
| Yes | 0.96 (0.84-1.10) | 0.573 | 1.06 (0.85-1.32) | 0.601 |
| No | Ref | --- | Ref | --- |
| Pre-operative oral antibiotic prep | ||||
| Yes | 0.58 (0.51-0.65) | <0.001* | 0.85 (0.70-1.03) | 0.096 |
| No | Ref | --- | Ref | --- |
| Clinical stage | ||||
| Stage 0 | Ref | --- | Ref | --- |
| Stage I | 0.95 (0.64-1.41) | 0.786 | 0.67 (0.37-1.19) | 0.169 |
| Stage II | 1.19 (0.80-1.76) | 0.391 | 0.88 (0.51-1.55) | 0.662 |
| Stage III | 1.21 (0.82-1.80) | 0.337 | 0.74 (0.42-1.32) | 0.308 |
| mFI | ||||
| 0 | Ref | --- | Ref | --- |
| 1 | 1.57 (1.24-1.99) | <0.001* | 1.24 (1.09-1.42) | 0.001* |
| 2 or more | 1.84 (1.42-2.39) | <0.001* | 1.75 (1.51-2.03) | <0.001* |
| Total OR time | 1.001 (1.000-1.002) | 0.024 | 1.001 (1.000-1.002) | 0.024 |
*p<0.01; Abbreviations: aOR=adjusted odds ratio, CI=confidence interval; AAPI=Asian American or Pacific Islander; BMI=body mass index; mFI=modified frailty index; OR=operating room.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



