Submitted:
15 July 2025
Posted:
15 July 2025
You are already at the latest version
Abstract
Background: Contemplative practices encompass a variety of static and dynamic practices. A theoretical introduction traces differences among contemplative and meditative states; bottom-up and top-down embodied contemplative practices; implications of polyvagal theory in trauma recovery. Contemplative practices, by fostering insights, heightened awareness, and a deeper connection to a broader framework of meaning, may play a crucial role in significantly reducing trauma-related symptoms in both young and adult populations.
Methods: The current narrative literature review used Scopus and PubMed to search studies published in the last five years that examined the effects of contemplative practices, as umbrella term that includes Mindfulness-based Interventions, Yoga, Tai Chi, Qigong, meditation, on trauma recovery and PTSD symptoms among adults and youth.
Results: The literature search identified 281 articles. Forty-two studies met the inclusion criteria and were critically evaluated. Among the various approaches, mindfulness emerged as the most employed and investigated practice for supporting trauma recovery. Contemplative practices have been shown to effectively reduce various dimensions of traumatic experience, such as reactivity, intrusion, hyperarousal, and negative cognitions and mood. Controversial results were found on avoidance symptoms and physiological parameters.
Conclusions: Results give support to the idea of combining contemplative practices with trauma-focused psychotherapeutic interventions to foster a sense of safety, enhance emotional expression and awareness of feelings of fear, shame, guilt, or inferiority while improving metacognitive processes. This, in turn, supports healing the sense of self, restoring a sense of basic trust in self and others, which is often deeply affected in individuals who have experienced trauma.
Keywords:
Contemplative practices
; Trauma
; Trauma recovery
; Trauma-related symptoms
; Mindfulness
; Yoga
; Umbrella review
1. Introduction
1.1. Contemplative Practices: Theoretical Frameworks
The growing body of research on contemplative practices testifies a peak attention of researchers over recent decades, focusing on the melting point between eastern and western approaches to science and recognizing psychosocial and psychobiological benefits in clinical and non-clinical settings (Bruce et al., 2018). Originally, these practices were designed to investigate the essence of reality in pursuit of truth, rather than as methods. However, many studies revealed the therapeutic effects in several psychological domains with a decrease in symptoms, emotional and behavioural problems (Ghiroldi et al., 2020; Scafuto et al., 2022), and an increase in well-being outcomes (Scafuto et al., 2024) and real happiness (Salzberg, 2017).
Contemplative practices appear to be an umbrella term, including a variety of static and dynamic practices, such as mindfulness meditation, but also embodied and movement-based practices, such as Tai Chi, Qigong, and Yoga. They often require formal activities for 20 min or more, once or twice daily (Bruce et al., 2018; Poli et al., 2021). Religious practices (e.g., prayer and chanting) also can be included in the range of contemplative practices. Despite most studies consider contemplative practices a broader term that also includes mindfulness meditation, some scholars underline crucial differences.
Meditative practices, as described by Sparby and Sacchet (2022), are currently utilized primarily for their health benefits, often emphasizing direct and non-judgmental experience over analytical thinking, with little reference to their traditional purposes. In contrast, contemplative practices focus on training meditation toward specific spiritual goals, such as "liberation," "enlightenment," or "awakening" (Rose, 2016). For example, within Contemplative Christian Traditions, contemplation—rooted in the Latin term contemplari (from cum templum, referring to the space in the sky observed by oracles for prophecies)—is viewed as a state of effortless joy and profound pleasure derived from an intimate relationship with the divine (God). This form of contemplation, as highlighted in Summa contra Gentiles (IV, 22), is considered a mystical state of unity, beyond earlier forms of prayer such as mental, verbal, meditative, or re-collective prayer, as emphasized by Saint Thomas Aquinas and Saint Teresa of Ávila. While the meditative life enables one to perceive truth, the contemplative life fosters a love for truth, leading to a receptive state in which cognitive contents (such as images or thoughts), reasoning, memory, and will are pacified, awakening one's divine nature (Summa Theologica, II-II, 180, 7, ad 1; Jäger, 2003).
Tibetan masters such as Chogyal Namkhai Norbu, within the Dzogchen tradition, similarly define contemplation as the ultimate goal of meditation—a non-dual and aconceptual state that is self-liberating and free from any intentional activity of the mind (Norbu & Shane, 1987). This state is one of pure experience, where the distinction between the knower and the known dissolves, leaving only the act of knowing itself (Macy, 1991).
Among the various subtypes of contemplative practices, mindfulness meditation is the most prevalent in the West and implies attentional and constructive practices (Conversano et al., 2020). Attentional practices include focused attention - for instance, bringing gently the attention to the breath, the body districts or to cognitions, emotions and the reactions to a specific external object - and open monitoring (also known as choiceless awareness), which involves observing the most prominent aspects of moment-to-moment experience within the flow of awareness. Differently, loving-kindness, compassion and self-compassion practices can be listed in the range of the so-called constructive practices (Germer & Sieger, 2014). Loving-kindness meditation focuses on intentionally cultivating a feeling of happiness and love toward oneself and others, while compassion meditation emphasizes fostering goodwill and empathy, particularly in response to suffering. According to the broaden-and-build theory, negative emotions arise in response to perceived threats through habitual responses (e.g., fight/flight), whereas positive emotions arise through recognition of perceived opportunities in the context and an attitude of openness to new situations and ideas (Lang et al., 2012).
1.2. Trauma and Post-Traumatic Symptoms: Recovery Pathways Through Contemplative Practices
The association between trauma-related symptoms, emotion dysregulation and contemplative practices has been investigated in several previous reviews and meta-analysis (Kim et al., 2013; Lang et al., 2012; Poli et al., 2021¸ Prati & Pietrantoni, 2009). According to the DSM-5, Post-Traumatic Stress Disorder (PTSD) is defined by a qualifying exposure to a traumatic event that includes “actual or threatened death, serious injury, or sexual violence” (APA, p. 271). There are four main types of qualifying exposure: direct personal exposure, witnessing of trauma to others, indirect exposure through trauma experience of a family member or other close associates, repeated or extreme exposure to aversive details of a traumatic event (Pai et al., 2017). The DSM-5 lists 20 symptoms along four groups: intrusion (e.g., re-experiencing the traumatic memories), avoidance; negative alterations in cognition and mood (e.g., negative self-perception, blame, guilty); and alterations in arousal and reactivity (e.g., hyperarousal).
Mindfulness-based interventions for PTSD have demonstrated clinically meaningful improvement in PTSD symptoms immediately post-treatment (Jasbi et al., 2018). Embodied contemplative practices are supposed to work better for trauma (Amihai & Kozhevnikov, 2014) as well as somatic therapies, in comparison with conventional psychotherapies. Indeed, considering polyvagal theory and the stress-reactive dissociation of traumatic experience from prefrontal modulation and left-sided verbal processing, discursive psychotherapy is less likely to work on trauma than somatic approaches, including psychodramatic re-enactments, narrative and poetic reframing, posture yoga and intensive breath-work (Van der Kolk, 2015).
Embodied contemplative practices consist of two broad types of methods: top-down (i.e., the downregulation started from mental processing at the level of the cerebral cortex) and bottom-up (i.e., pathways from the periphery to the brainstem and cerebral cortex, Taylor et al., 2011). Both work supporting implicit memory and procedural conditioning to calm the post-traumatic reactivity (Loizzo, 2014). Top-down embodied practices include for instance corrective body imagery (visualization), prosocial prosody (recitation); bottom-up embodied practices include for instance expressive movement (posture-gesture) and energizing breath-activation (e.g., kundalini yoga). Movement-based contemplative practices, such as Tai Chi, Qigong, and Yoga, can be seen as bottom-up practices that emphasize the use of spontaneous and active movement and breathing, playing a key role in the regulation of both autonomic nervous system and hypothalamic-pituitary-adrenal axis (Kelly et al., 2018), which are central to PTSD and stress physiological symptoms (Riley & Park, 2015). Furthermore, movement-based contemplative practices may reduce PTSD symptoms by increasing interoceptive ability (van der Kolk et al., 2014; Schmalzl et al., 2014), which is crucial in emotional experience and regulation (Critchley & Garfinkel, 2017; Lazzarelli et al., 2024).
Contemplative practices, characterized by the attentive regulation of breathing or of body movements and postures, are believed to affect vagal activation. VVC is activated, for instance, by glossopharygeal and auditory feedbacks that derive from expressing soothing vocal tones in prayer or chanting (Lazar et al., 2000; Porges, 2011). Imagining or voluntary rhythmic breathing activates the smart vagus and its medullary nucleus, regulating reflex autonomic stress-reactivity (Shannahoff-Khalsa, 2008). Similarly, rhythmic movement and deep abdominal breathing activate feedbacks sent to the solitary nucleus from visceral vagal afferents, promoting the bottom-up regulation of stress reactivity (Loizzo, 2016).
According to polyvagal theory (Porges, 2001; 2011), contemplative practices affect trauma responses since they can be seen as neural exercises expanding the capacity of the ventral vagal complex to regulate the present state and to increase neuroception of safety and social engagement system, rather than threat. Indeed, contemplative practices were found to increase baseline Respiratory Sinus Arrhythmia (RSA), which reflects the activation of the Ventral Vagal Complex (VVC), thus promoting PTSD recovery (Poli et al., 2021).
Given the premises above, we can better understand the effectiveness of contemplative practices combined with health programs in preventing post-traumatic stress disorders. At the same time, if combined with psychotherapies in the clinical setting, contemplative practices become important interventions in the treatment of PTSD. Structured Psychotherapy for Adolescents Responding to Chronic Stress (SPARCS; DeRosa & Pelcovitz, 2009) is for instance a group trauma treatment for urban adolescents that aims to develop stress identification skills, awareness of the body responses to stress and emotional states, a non-judging mindful approach, communication and problem-solving skills, the ability to self-soothe and to tolerate distress. RAP Club, a trauma-informed intervention for eighth graders as core component is based on SPARCS (DeRosa & Pelcovitz, 2009; Mendelson et al., 2020), a group treatment for urban adolescents exposed to chronic stress and adversity. SPARCS uses psycho-education, cognitive behavioural therapy (CBT), and mindfulness strategies to promote self-regulation among young people.
For individuals with PTSD, such as veterans, trauma-informed adaptations to contemplative practices have been developed. These adaptations include psychoeducation on trauma and stress physiology, fostering autonomy and a sense of control during exercises, and offering flexibility in practice (e.g., not requiring to close their eyes, which may trigger fear or overwhelming negative emotions). Additionally, grounding exercises are incorporated at the start of each session, and the duration of sitting meditations is reducing to accommodate the needs of participants. Contemplative practices combined with trauma-informed practices and trauma-based psychotherapies are also included into teaching and educational environments (Ross & Beardall, 2022), targeting social workers (Warren & Chappell Decker, 2020), nurses, and practitioners. These practices help to develop skills to manage vicarious trauma, compassion fatigue, and work-related stress, while also fostering a sense of hopefulness (Fiske et al., 2020).
Finally, an interesting perspective is given by emancipatory contemplative practices, which are aimed to in tentionally create opportunities to access our embodied cultural, collective, and ancestral memory. The focus of these practices is the decolonization of traditional wisdom of indigenous people that has been stolen or erased, starting from the reconnection to our bodies, hearts, and minds (Hopson & Hopson, 1999). Trauma is framed in an intergenerational, histori cal, and collective context, hence the healing process is culturally-grounded and based on connecting to inner aliveness through soulful experiencing, coming into harmony with nature and in alignment with the activity of spirit (Duran et al., 2008). An example is the contemplative practice called Rising Up Rooted offered as a meth odology for awakening Black wisdom (LaVallie & Sasakamoose, 2023). Indeed, Black cultural expressions (e.g., music, dance, poetry, spoken word) and cul tural practices (e.g., rituals, ceremonies) can be powerful means for cultural connection and healing trauma (DeLoach & Peterson, 2010; Monteiro & Wall, 2011).
While the theoretical rationale for the benefits of contemplative practices in trauma recovery is strong, more empirical evidence is still needed to address methodological limitations, such as small sample sizes and lack of randomized control groups in clinical trials (Lang et al., 2017). Furthermore, one of the prominent issues that makes the investigation still needed is the report of several side effects, most commonly revealed as increase in anxiety, traumatic re-experiencing, and emotional sensitivity (Goldberg et al., 2022). In a population-based survey to evaluate the occurrence of a broad range of Meditation-Related Adverse Effects (MRAE; Goldberg et al., 2022), some degree of functional impairment was reported by 10.6% of participants, with impairment lasting more than one month for 1.2%. Childhood adversity was associated with elevated risk for MRAE. Half of participants reported at least one clinically relevant symptom (e.g., hyperarousal, dissociation or feeling to be cut off from other people, sleep difficulties). An additional result was that participants with more and longer meditation practice experience, whether current or previous, were more likely to report MRAE.
Some side effects of contemplative practices may be understood as part of the meditative process, as discomfort may accompany both healing and meditative insights (Lindahl et al., 2017). Early Buddhist accounts also acknowledge such challenges along the meditative path (e.g., Bodhi, 2012). However, when initial discomfort is overcome and traumatic experiences and symptoms repertory are elaborated, trauma can become an opportunity of personal growth. Indeed, participants reporting MRAE were equally glad to have practiced meditation as those not reporting MRAE (Goldberg et al., 2022). Reflecting in depth about a traumatic event tends to promote a search for new purpose and meaning in one’s life, a process that has been documented as post-traumatic growth (Calhoun et al., 2000).
2. Methods
2.1. Search Strategy
The present narrative review was conducted to examine the effects of contemplative practices on trauma recovery. Two databases were selected for this review: Scopus and Pubmed. The search was performed on 7th August 2023, restricting the search to studies published from January 1, 2018, in light of an existing review (i.e., Boyd et al., 2018). Finally, the references of the included papers were also examined to potentially identify additional articles not found in the search.
The search strategy included the the following search terms: (“Historical trauma” OR “Sexual trauma” OR “Psychological Trauma” OR “Trauma and Stressor Related Disorders” OR “Stress Disorders, Traumatic, Acute" OR "Stress Disorders, Post-Traumatic") AND (“Contemplative practices” OR “Mindfulness” OR “Meditation” OR “Yoga” OR “Tai chi” OR “Tai Ji” OR “Qigong” OR “Self-compassion”).
2.2. Eligibility Criteria
We included only studies where researchers analysed quantitative data of effects of contemplative practices on trauma recovery. The articles were restricted to those published in English and within the field of psychology, specifically excluding books, books’ chapters and dissertations. Additionally, articles that were not peer-reviewed or published in languages other than English were excluded. After the initial search, two inclusion criteria were added: (1) a publication data after 1st January 2018 to limit the time span, given the presence of a previous review on earlier studies (i.e., Boyd et al., 2018); and (2) the study design, including both non-randomized clinical trials and randomized-controlled trials (RCTs).
2.3. Data Extraction
Data were initially extracted from the included studies by one reviewer (X.X.). Two additional reviewers (X.X. & X.X.) independently verified the accuracy of the extracted information. The extracted data included the type of contemplative practices, traumatic experiences/events or disorder, study sample, study design, measurements, and outcomes. Several secondary outcomes were tracked, but only those correlated with the effects of contemplative practices were reported. A summary of data is illustrated in Table 1, which includes study design, sample size, type of trauma, type of contemplative practices, duration, measures, and primary and secondary outcomes.
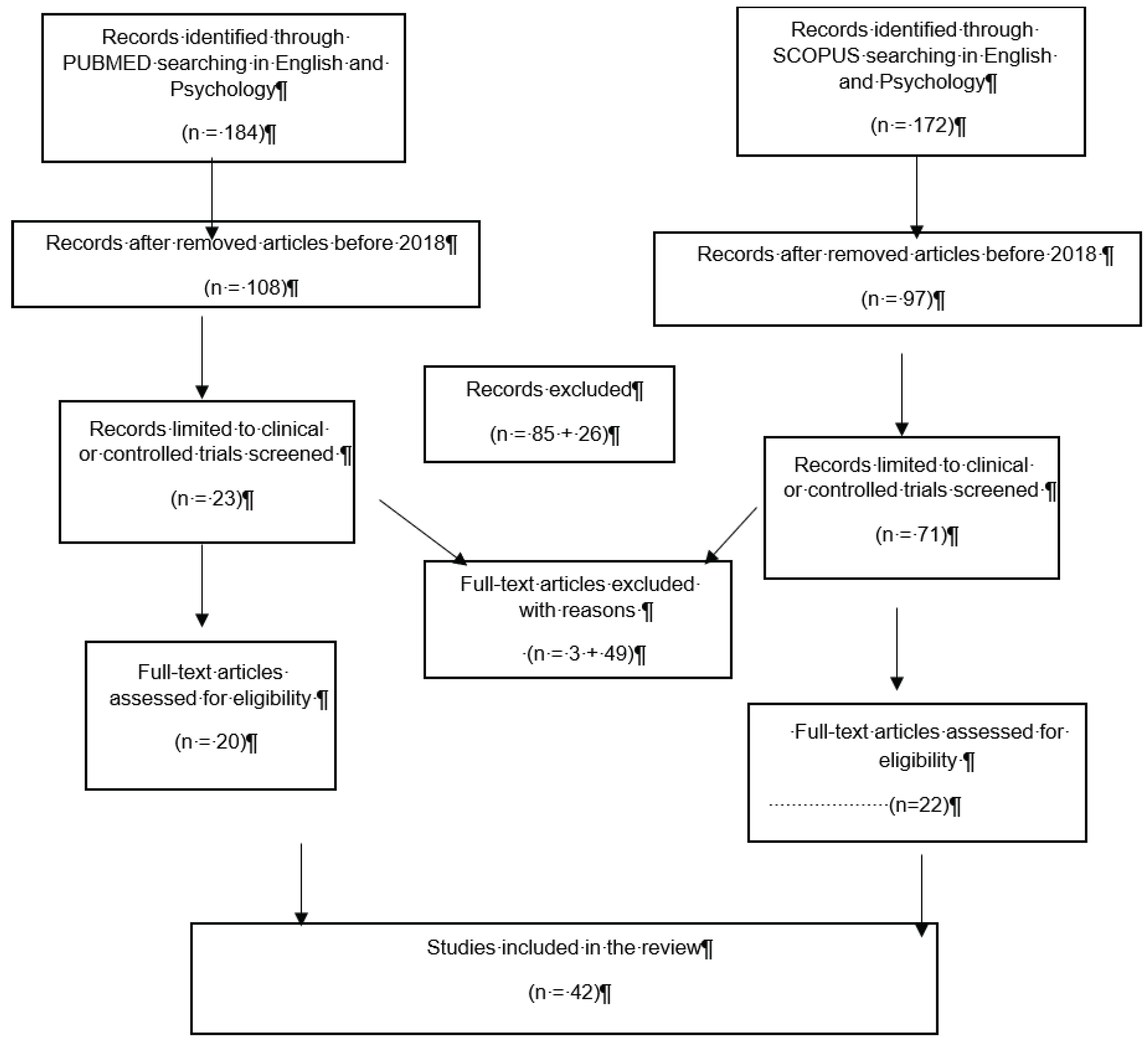
Figure 1.
Flow diagram of the review process.
3. Results
3.1. Study Selection
The database search yielded 375 records. After the removal of duplicates, 209 title and abstracts were screened. A total of 94 records was retained for full-text screening. After screening the full-text of studies selected, 52 records were excluded based on the inclusion criteria. Specifically, the excluded studies relied on qualitative data, did not consider trauma-related measures as outcome variables, or treated mindfulness as a dispositional trait rather than as a psychological intervention. Overall, 42 studies were included in this narrative review.
3.2. Study Characteristics: Design and Samples
Regarding the study design, the majority of selected articles were based on RCTs. These included active control (1, 2, 3, 5, 6, 9, 10, 12, 13, 14, 15, 18, 19, 20, 22, 23, 24, 25, 26, 29, 33) or waitlist control group (4, 11, 32, 36, 40, 41, 42), single-group design study (7, 8, 16, 17, 21,27, 28, 30, 31, 34, 35, 37, 38), and collective case study (39). Half of the l studies included multiple assessments with follow-up from one to twelve months (2, 4, 7, 10, 11, 12, 14, 15, 17, 18, 21, 22, 26, 28, 29, 31, 32, 35, 38, 40, 41).
The active control groups were based for instance on psychoeducation, and low-intensity CBT skill training, relaxation techniques (1), or a group training in integrated coping skills (ICS) (3). Other control groups related to informal activities were based on exchanging daily life experiences and playing board games (5) or multisport activity (12). Other examples of active control groups were PTSD intervention for problem solving and symptom management, the so-called Present-Centered Group Therapy (PCGT) (6), Enhance usual care control (ETU) (15) and Wellness control group, that included information on different aspects of health (9).
Most samples were composed of WEIRD population. A couple of studies targeted black adults or partly included black adults (2, 12). In nine studies, samples included veterans with PTSD symptoms (6, 10, 16, 21, 26, 27, 35, 40, 41). Other studies focused on samples composed entirely by women (3, 5, 7, 8, 11, 12, 22, 39), of which two studies (7, 8) specifically selected women with PTSD symptoms and substance abuse disorder. Interestingly, only three studies (1, 4, 32) selected asylum-seekers with forced displacement trauma and exposure to correlated collective stressors. Four studies targeted adolescents and young adults (30, 32, 33, 36), while the others recruited adults. Several interventions required adaptations since targeted populations with specific sociocultural conditions (1, 2, 4, 12, 15, 29, 30, 32, 36, 39, 40, 41), one study also involved a program for Christian Church attenders (24).
3.3. Type of Trauma
The most common trauma investigated was PTSD from combat among male veterans (6, 10, 16, 21, 26, 27, 35, 40, 41). Other common traumas included PTSD related to comorbid substance use disorder (3, 7, 8, 15), violence such as intimate partner violence (12, 39), domestic violence (22), and physical, sexual, and emotional abuse (20, 28, 38) among women. Additional traumas included forced displacement and multiple traumatic experiences correlated with migration (1, 4, 32).
Three studies explicitly refer to a larger definition of trauma, called Complex Trauma (C-PTSD), also associated to multiple childhood trauma (11, 28, 35). Those traumas specifically regarded abuse, the threat of survival, experiencing helplessness, fear or horror for witnessed or directly suffered violence early in life.
3.4. Type of Contemplative Practices
In light of the call for novel mental health interventions and given the severity of large scale mental problems, contemplative practices were investigated as cost-effective and feasible interventions for traumatic symptoms in comparison with more conventional therapies, such as Narrative Exposure Therapy (NET; Elbert et al., 2015; Robjant & Fazel, 2010); individual psychotherapy, CBT (Carlsson et al., 2018), psychosocial interventions (Silove et al., 2017), Problem Management Plus (PM+) and e-health Self Help Plus (SH+; Tol et al., 2020).
The most evident result from the final dataset is that mindfulness meditation is the most common contemplative practice investigated in the last five years in association with trauma. Traditional programs Mindfulness Based- Stress Reduction (MBSR) were administrated alone (6, 12, 31), targeting veterans (6), women who experienced intimate partner violence (12) and police officers with occupational stress (31). A fourth study examined the effects of trauma-adapted intervention with explicit references to loving-kindness meditation and MBSR (38). Other studies combined mindfulness with cognitive behavioural treatments (15, 16, 19, 20, 32), with trauma-adapted intervention from loving-kindness meditation (38) or with programs based on cultural adaptations (2, 32).
Seven studies involved constructive practices, such as compassion and loving kindness meditation (1, 16, 21, 23, 27, 28, 38), delivered as structured programs. Only one study evaluated the effects of a single audio taped session based on the compassion meditation (LKM-S) on physiological recordings, where participants were asked to direct loving/friendly feelings toward themselves and others (27). Considering the relevance of the concordance between behaviour and values in recovering psychological wellbeing, a study examined the role of Acceptance and Commitment Therapy (ACT) in patients with the distress due to the diagnosis of cancer (25).
Recent empirical evidence showed that ACT as mindfulness-based psychotherapy has beneficial effects on trauma-related symptoms (Rowe-Johnson, Browning, , & Scott, B., 2024).
One intervention, called Cognitively-based Compassion Training (CBCT), targeted veterans with PTSD (16) and combined present-moment practices (i.e., focused attention and open monitoring) with analytical contemplative methods, which encourage cognitive reappraisal and alteration of usual mental patterns to expand compassion.
Three studies examined the effects of Transcendental Meditation (TM) on traumatic symptoms (22, 26, 36). For instance, they assessed the effectiveness of a standardized mantra-based form of meditation that enables a person to drift into a psychophysiological state of restful alertness (22).
It is worth noting that several programs in trauma conditions combined more standard treatments, such as Cognitive Therapy Group for trauma (2), Cognitive Behavioural Therapy (32), Trauma adapted relapse prevention (3, 8), Trauma and the Body Group (11), Internal Family System therapy (28) with different types of meditation that included a variety of techniques. The combination of contemplative practices with trauma-related issues required training on strategies to manage flashbacks and the overload of intense emotions, such as the use of a deep breath as anchor, placing hands on one’s belly (to get a physical reminder of breathing) and breathing until the response fades away. Moreover, this combination also emphasized the importance of a group setting, rather than individual one, as the group dynamic help to reinforce the learning of meditation skills and enhances compassion by exposure to others’ experiences shared in the class. Group sharing focused on the difficulties and positive outcomes of the meditation learning process, rather than the content of traumatic experiences and symptoms, which could often evoke uncomfortable feelings. Over time, as trust developed within the group, participants felt more comfortable sharing their distressing experiences and coping strategies, creating a foundation for trauma-focused psychotherapy, although this was not the initial focus of the practice.
The only movement-based contemplative practice investigated in the last five years in association with trauma is Yoga (5, 13, 30, 34, 37, 39). Kripalu Yoga Program combined physical postures, breathing, and moving meditation (5, 42), while Hatha Yoga program is an alignment-focused practice always linking breath with movement (34). Like with mindfulness, it was adapted for trauma conditions, generating programs such as the so-called trauma informed yoga (30) and trauma sensitive yoga (13, 39). In trauma informed yoga, yoga forms were used as a tool for self-exploring various body movements, promoting physiological safety and calmness and helping to reorient the perceived danger, which could improve the ability to manage social relationships (Van der Kolk, 2014). Trauma Sensitive Yoga (TSY) was a structured body-oriented practice to discern curative elements of yoga that can enhance the healing of complex trauma by cultivating self-regulation, self-awareness and nourishing a compassionate relationship with the body (40). Three principles of TSY to facilitate recovery for women with Intimate Partner Violence include: creating a safe environment to develop a sense of safety, consistency, non-judgment, and gentleness; only verbal assists used if demonstrating respect for their physical boundaries; invitatory language.
No clinical trials examined the effects of Tai Chi and Qi Gong on trauma recovery in the last five years.
More integrated programs were Intensive Treatment Program (ITP), where yoga was combined with Cognitive Processing therapy (CPT), mindfulness, psychoeducation, art therapy, and integrative exercise (IE) (35). Integrative exercises included aerobic and resistance training exercises (40, 41).
Yoga and Mindfulness-Based Cognitive Therapy (Y-MBCT) were both included in the program named Trauma Intervention Mindfulness Based Extinction and Reconsolidation (TIMBER), aimed to allow the cognitive reprocessing and neutral/detached reappraisal of the trauma memories. Furthermore, this program was the only one to be combined with a single sub-anaesthetic dose of ketamine, chosen for its efficacy in the treatment of depression and PTSD, but also for its ability to induce neurogenesis and to affect synaptic plasticity (20).
For childhood trauma complex PTSD symptoms, the Trauma and the Body Group (TBG) was developed as a group psychotherapy that combined mindfulness with sensorimotor psychotherapy. This included breath exercises, somatic check-in, discussions on home practice, brief mindfulness exercise, psychoeducation on the impact of trauma on body weekly exercises (11). Furthermore, another program targeting complex PTSD symptoms for multiple childhood trauma was the Internal Family System therapy (IFS). This approach integrated systems theory and trauma theories with mindfulness, self-compassion, and self-acceptance practices (28).
Meditation was integrated in the culturally adapted cognitive behavioural therapy (CA-CBT), which also involves psychoeducation, stretching exercises, and problem solving (e.g. management of social problems, motivational barriers and dissociation), targeting refugees with multiple trauma pre-post displacement (32). Similarly, Mindfulness-Based Cognitive Therapy (MBCT) was adapted for trauma exposed Black adults, also including psychoeducation, and feedback and supportive group discussion of exercises beyond the skills training and in-class practice in mindfulness techniques (2). Regarding migration and displacement trauma, beyond CA-CBT, another specific program, the Mindfulness-Compassion Based Trauma Recovery for Refugees program (MBTR-R), was analysed. The program was delivered in a group with a similar structure of MBSR and MBCT aimed to train in formal and informal mindfulness practices (e.g., body scan, sitting meditation, mindful movement, 3-min breathing space, formal and informal loving-kindness and self-compassion practices). It also included psychoeducation on trauma-related mental health problems in refugees, trauma-sensitive themes (e.g., safe place practice), and sociocultural adaptations (e.g., separate groups for men and women, socio-culturally specific metaphors) (1, 4).
Contemplative practices integrated with trauma-based interventions also targeted comorbidities and gender differences. Indeed, people with post-traumatic disorders often report symptoms of substance use disorder (SUD; Ibañez et al., 2022). Low levels of acting with awareness, a facet of mindfulness skill, for instance may worsen trauma symptoms after emotional, physical, and sexual abuse (ETE) which in turn may lead to more craving for women in substance use treatment. A program especially designed for women with PTSD, called Trauma-integrated Mindfulness Based Relapse Prevention (Ti-MBRP) was also a Gender Responsive Program, included gender-themes, such as interpersonal relationships, parenting, and women empowerment, together with trauma-themes, such as blame, overgeneralization of perception of threat to safe situations, and strategies to deal with hyperarousal (3, 7, 8). It also consisted in practices designed to bring awareness to cognitive and behavioural processes underlying substance use, reduce initial reactivity and promote non-judgmental acceptance, and explore substance use as a mechanism to cope with PTSD symptoms.
Another intervention targeting comorbid addiction was called Intervention for dual problems and early action (IIDEA). It draws from a combination of cognitive behavioural therapy and mindfulness, with more emphasis on cultural factors, motivation, and therapeutic alliance, considering the difficulties of building a trust relationship with this type of beneficiaries. It also includes psychoeducation, cognitive restructuring, substance use recovery skills (15).
As part of preventive programs addressing occupational stress, a curriculum designed for police officers was inspired by the Mindfulness-Based Resilience Training Program. This curriculum included both formal and informal homework practices, body scan, movement, breath awareness, mindful eating, compassion practice. Additionally, it placed a special emphasis on building resilience to stress and promoting neuroplasticity (31).
Among all the programs, two were fully delivered online. The mobile and telephone mindfulness program required the recordings and homework on awareness of breathing, external stimuli (e.g., sound), emotions and mindful acceptance (17). The other study was the game-based meditation intervention (MUSE) that utilized neurofeedback and included relaxation tutorials (e.g., deep-breathing techniques), followed by 3-min meditation sessions (33). After each meditation session, the participants were provided with feedback on their performance in the form of points and awards that reflect participants’ capacity to regulate their arousal.
MUSE program, along with Learning to Breathe (L2B) were the only two programs delivered for adolescents with chronic stress (33, 18). It is particularly important to underline that online mHealth technology as MUSE program that was delivered online (e.g., smartphone apps) may have side effects since meditation adverse effects are more likely to occur when practicing alone and without a qualified instructor (Schlosser et al., 2019).
Unlike MUSE, L2B was an in presence program that combined mentoring and mindfulness. Its effectiveness was compared with the mentoring as usual program, but it lasted just four sessions (18). Finally, only one study reported a personalization of mindfulness interventions on subject’s scores on Assessment Scale for Mindfulness Interventions (ASMI, clinician rated) (20) while a second study included an individualized program of CBT-based treatment for depressive disorders and PTSD (23).
The intervention duration in the selected studies spanned from one 1,5-hour session for the shortest intervention (27) to 36 sessions in 12 weeks for the longest interventions (40, 41). On average, the duration consisted in almost 11 weekly sessions. It is worth noting that positive outcomes were associated to interventions with average duration, while no significant difference from baseline or from the control group applies to short-time interventions. For instance, in a 6-days program combining scuba diving with mindfulness exercises (9) no significant changes in the total PTSD symptoms were reported but only in intrusion symptoms, and in the shortest study heart rate response increased contrary to the expected decrease (27). The association between duration of formal mindfulness practice (i.e., minutes for practice) and PTSD Symptoms was explicitly found in a pilot RCT study at 6-month follow-up, suggesting that the more the intervention was long, the more avoidance, arousal, and reactivity symptoms were reduced (8).
3.5. Primary Outcome: Measures
Except for the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) (2, 3, 6, 16, 20, 26, 28, 38, 39, 41, 42), self-report measures are the prevalent type of assessments. Self-reported PTSD symptoms and traumatic events were measured using a variety of questionnaires: the PTSD Symptom Scale Self Report PSS (3); the Davidson Trauma Scale (DTS) (28, 38); the Structured Interview for Disorders of Extreme Stress-Self-Report (SIDES-SR) (28); the Harvard Trauma Questionnaire (HTQ) (1); the Traumatic Events Inventory (TEI) (2); the Impact of Events Scale-Revised (IES-R) (5, 42); the PTSD Checklist for DSM-5 (PCL-5) (6, 8, 9, 11, 12, 16, 20, 21, 22, 26, 27, 32, 35); the Childhood Trauma Questionnaire (CTQ-SF) and the Life Stressor Checklist Revised (LSCR-R) at baseline for recruitment (11); the Intimate Partner Violence Exposure (IPVE) and Life Events Checklist (LEC-5) at baseline for recruitment (12); the Child PTSD Symptom Scale on Distressing Events (18); the PTSD Checklist–Civilian (PCL-C) (23, 31, 36, 42); the Trauma History Questionnaire (36).
CAPS-5 is the most used measure, a 30-item structured interview that corresponds to the DSM-5 criteria for PTSD, considered the gold standard in PTSD assessment and often used in combination with PCL, the PTSD checklist. For the assessment of DESNOS, the measure used was Structured Interview for Disorders of Extreme Stress-Self-Report (SIDES-SR), while for developmental trauma disorder and multiple childhood trauma measures included: Child PTSD Symptom Scale on Distressing Events, a self-report scale that assesses PTSD symptoms in 8-18 years children who have experienced a traumatic event; Childhood Trauma Questionnaire-Short Form (CTQ-SF), a self-report questionnaire that assesses several types of childhood abuse and maltreatment in adults.
3.6. Secondary Outcomes: Measures
Other specific symptoms measured through self-report assessments include: depression through the Patient Health Questionnaire PHQ-9 (1, 2, 4, 6, 16, 17, 23, 27, 32) PHQ-8 (35), PHQ-15 (6), the Beck Depression Inventory (BDI) (11, 26, 28, 36, 38), the clinician-administered Hamilton Depression Rating Scale (Ham-D) (20), the Depressive Experiences Questionnaire (21); the Depression, Anxiety and Stress Scale (DASS-21) (5, 21), the Hospital Anxiety and Depression Scale (HADS) (25); anxiety through the Beck Anxiety Inventory (BAI) (11, 20, 26), the Generalized Anxiety Disorder Scale (GAD-7) (15).
Mindfulness dimensions were measured using the Five Factor Mindfulness Questionnaire (FFMQ) (2, 3, 18, 38, 40), Freiburg Mindfulness Inventory (FMI) (9), Philadelphia Mindfulness Scale (PHLMS) (11, 16), Mindfulness Awareness Attention Scale (MAAS) (15), Cognitive and Affective Mindfulness Scale-Revised (CAMS-R) (17), all self-report assessments.
In some studies, emotion regulation capability associated to trauma and interventions was measured using self-report questionnaires such as the Difficulties in Emotional regulation Scale (DERS) that includes non-acceptance of emotional responses, difficulties engaging in goal-directed behaviour, impulse-control difficulties, lack of emotional awareness, limited access to emotion regulation strategies (3, 12, 18, 32), the Emotion Regulation Questionnaire (ERQ) (27), the Differential Emotion Scale (DES’) (16). Also, two studies measured interoception using the Multidimensional Assessment of Interoceptive Awareness (MAIA) (28, 40).
In addition, it is worth mentioning that a few studies included physiological parameters to measure: brain waves in resting-meditation and heartbeat-evoked brain responses (HEBR) through EEG and ECG (6); heart rate variability (HRV) (27) and basal ANS activity (33) through ECG; skin conductance levels (SCL) (27); HPA axis activity through hair (33) and salivary cortisol levels (37).
Finally, combined with quantitative results, some studied added qualitative and explorative methods, especially aimed to evaluate the feasibility and acceptability of the intervention, or to amply the subjective meaning of trauma recovery. These studies reported what participants felt as benefits from the treatment and developed multiple interpretations that optimize an understanding of trauma recovery (2, 15, 39).
3.7. Effects of Contemplative Practices on Trauma Recovery
The primary finding regarding the effectiveness of contemplative practices was a significant reduction of PTSD symptoms severity. For example, the average reduction of 31 points observed on the total CAPS score, a measure of PTSD symptom severity, was observed. This reduction met or exceeded the outcomes reported in other trials of veterans with PTSD for empirically supported psychotherapies, such as cognitive processing therapy or prolonged exposure therapy (40).
The impact on PTSD was frequently associated with a remarkable reduction of symptoms of depression and anxiety. With only a few exceptions (29, 32), in most cases (1, 4, 5, 10, 16, 19, 21, 22, 26, 31, 35, 36) depression, anxiety, stress and PTSD symptoms were highly correlated and decreased together after the intervention. In a veterans’ sample (29), the Mind-body Skills group reduced PTSD symptoms but had no significant effects on depression and anxiety. Conversely, Culturally Adapted Cognitive Behavioural Therapy (CA-CBT) reduced depression and somatic symptoms in refugees, but did not result in significant changes on the PTSD checklist (32).
Data from physiological parameters support the above results: a first study (6) reported an increase in frontal theta Heartbeat-evoked brain response (HEBR); other studies reported lower basal activity of Sympathetic Nervous System (33) and cortisol level (37). A counterintuitive result was revealed in a fourth study that showed a lower Skin Conductance Levels (SCL) (meaning a reduction of sympathetic arousal), but contrary to what expected a higher Hearth Rate response (indicating higher physiological arousal), and not significant change in Heart Rate Variability followed the intervention (27).
It is interesting to note that programs may have different impact on the several dimensions of PTSD symptoms. For instance, a study on a program that combined mindfulness with scuba diving had non-significant overall effect on PTSD symptoms, except for the subscale of Intrusion that was significantly reduced at post-test and at a first follow-up (9). The subscale of Intrusion together with Avoidance were also reduced after Kripalu Yoga, while not-significant effect was observed on Hyperarousal subscale (5). Avoidance was the dimension most notably affected by Trauma-adapted intervention from LKM and MBSR, with effect that persisted at follow-up (38). A mind-body skills group affected avoidance and hyperarousal, together with sleep disturbance and anger (29). Other studies showed a decrease in all the subscales: intrusions, avoidance, negative changes in cognitions and mood, and changes in arousal and reactivity (e.g., 19).
Regarding to follow-up studies, some research found no significant effects at follow-up, for instance neither formal nor informal practice predicted reduction in intrusion symptoms and craving at 6-month follow-up in women with SUD and PTSD after MBRP (8). No significant effects were found neither for overall PTSD score and Mindfulness at 3-month follow-up after a brief program of mindfulness and scuba diving (9). Similarly, Hatha Yoga did not produce significant effects on Intrusion and Avoidance symptoms at follow-up in people with comorbid chronic pain (34). On the contrary, other studies found effects of MBSR on PTSD symptoms at 5-month follow-up (31) up to one-year follow-up (32). This latest intervention, named Culturally Adapted Cognitive Behavioural Therapy (CA-CBT), increased emotion regulation skills, somatic symptoms, quality of life and general health with main effects maintained at one-year follow-up in migrants with multiple displacement trauma (32).
Regarding the effects of the two programs fully delivered online, it is worth to note that the mobile program showed higher level of drop-out in comparison with the telephone program, and no significant effects on Mindfulness and Coping Orientation (17). The MUSE program based on game meditation in adolescents showed a reduction of Sympathetic Nervous System basal activity, but just an increase of Hypothalamic-Pituitary-Adrenal Axis reactivity, without a significant change of Autonomic Nervous System reactivity to acute stress (33).
Other significant changes associated to contemplative practices regard positive dimensions of well-being, social feelings, and behaviours. Fewer studies reported outcomes of the effectiveness of the interventions on psychological wellbeing in its eudaimonic or hedonic aspects, rather than measures of symptoms and psychopathology. MBSR for occupational stress in police officers reduced Operational Stress, Exhaustion subscale of burn-out, Negative Affect but did not significantly influence Positive Affect (31). It also increased eudaimonic well-being, as measured with the Psychological Well-being Scale (31). Other interventions showed positive effects on Health responsibility, Stress Management, not feeling dominated by symptoms (10), Life satisfaction (37), and Quality of life (21, 32, 38, 40, 41). Studies especially focused on compassioned intervention reported increase in self-compassion (4, 27, 38). A study that delivered Internal Family System therapy did not show significant increase in self-compassion after the intervention in comparison to control, while revealing effects on PTSD symptoms and psychological distress (28).
Regarding results on social domains, studies reported an increase in social connectedness (16), social role functioning (34) and on the other side a decrease in fear of compassion, feeling of self-inadequacy, levels of external shame (21). A compassioned mind training targeting not only ex-service personnel of Defence Force with PTSD, but also their female partners, evaluated positive relational outcomes, such as social safeness and relationship satisfaction (21). Only one study investigated and revealed positive effects of the treatment on improvement of values-consistent behaviour (BEVS) after an intervention based on acceptance commitment therapy for cancer survivors (25).
As for emotion regulation in combination with PTSD symptoms, two studies (12, 18) reported a decrease in Difficulties in Emotional Regulation Scale, one study (32) reported an increase in emotion regulation (ERS), and one study (16) reported no significant change as measured by the Differential Emotional Scale. Theoretically correlated to emotion regulation, there is the Soothing Receptivity, that is the experience of being soothed physically, capacity to be soothed, experiencing soothing by disclosing to others, and self-soothing (Glassman, 1988). The soothing receptivity, often missed in traumatic victims, was strongly increased after the mind-body group therapy (TBG) applied on childhood complex trauma (11). Indeed, this type of therapy allowed participants to engage in both self-soothing and relational soothing, giving the opportunity to experience their bodies and others not anymore as a source of hurt but as a place of healing.
Research on contemplative practices in trauma recovery also assessed the effect on a relevant correlate of emotion regulation, that is interoceptive ability as measured by the Scale of Body Connection (SBC) (11) or by the MAIA (28). It is interesting to note that the above mentioned program led to higher awareness of somatic experience, i.e. body awareness subscale of SBC, but did not significantly affect bodily dissociation subscale of SBC and Dissociative Experiences Scale (DES) (11). Regarding MAIA, a large positive effect on the dimension of Trusting, a medium effect on Attention Regulation, Self-Regulation, Body Listening at post-test, while an increase in Not-Distracting at 1-month follow-up after the intervention (IFS) were revealed in an uncontrolled clinical trial study (28); significant increase of Emotional Awareness, Self-Regulation and Body Listening in a RCT with multiple assessments after Integrative Exercises (IE) (40). Self-regulation, that is, the ability to regulate psychological distress by attention to body sensations, was the largest effect size revealed in parallel with the reduction in hyperarousal on the PTSD symptoms and the increase in the Mindfulness facet of Non-Reactivity, that denotes the tendency to allow thoughts and feelings to come and go, without getting caught up in or carried away by them (40).
Interestingly, a collective case study design provided data from interviews (pre- and post-intervention) analysed through content thematic analysis (39). Trauma recovery benefits were conceptualized as Body sensitivity, emotional benefits such as confidence and peace, and improvement in social relationships. After participating in Trauma-Sensitive Yoga, individuals reported several key themes regarding its benefits. The first theme highlighted improvements in physiological functioning, including better sleep, enhanced body attunement, and a greater sense of relaxation. Other reported physical benefits were the release or reduction of tension and pain, increased physical strength, improved balance and alignment, and increased attention to muscle soreness. Participants also described heightened sensitivity to physical warmth, visceral sensations, and overall boost in energy. A second theme centered on emotional benefits: participants experienced increased feelings of peace, pride, confidence, hopefulness, along with a greater self-permission and self-acceptance. Simultaneously, they noted a reduction in negative feelings, such as anxiety and irritability. Responses to previously triggering events became calmer, suggesting a reduced perception of threat in safe conditions. A third theme focused on enhanced and more stable interpersonal relationships. Participants reported increased trust in others, as they wished in the pre-interviews, and felt better able to navigate challenging interactions with family members because they were calmer and more connected. Additionally, they highlighted benefits stemming from a commitment to self-care and a sense of accomplishment in completing tasks, such as attending and finishing the TSY classes.
A study assessing feasibility and acceptability of a culturally adapted MBCT (2) identified several key benefits through narrative analysis. Participants frequently reported improvements in awareness and attention, enhanced emotion regulation, and better coping skills to manage stress or depression. Additionally, benefits included an increased sense of control, energy and positive affect, greater relaxation and calm, experiencing less physical pain, and fewer interpersonal conflicts. The group format also provided valuable peer support, which participants found beneficial. In addition to the reported benefits, the study also examined the barriers to participation in the treatment. The most common challenges were related to physical and transportation issues, which impacted attendance. Other barriers included stigma, lack of motivation, no availability of services, emotional concerns, misfit of therapy to needs, and time constraints. According to qualitative reports, more than half of respondents expressed that the cost of treatment too high to be sustained over time.
In a mixed method study, participants with double diagnosis (Substance abuse and chronic stress) found useful: being listened without judgement, learning relaxation and emotional regulation techniques, gaining a sense of self-control, and managing the double diagnosis symptoms (15). The study completed previous research (Alegria et al., 2019), that revealed quantitative effects on physiological tests, such as urine test, therapeutic alliance, mindfulness, illness management and recovery, depression, anxiety and PTSD symptoms.
Regarding co-occurring substance use disorder, it is worth noting that a study found the effectiveness of the interventions incorporating contemplative practices for certain PTSD symptoms, specifically avoidance, arousal, and reactivity. However, these interventions were not as effective for addressing symptoms related to intrusion and re-experiencing (8). Another research by the same authors showed a reduction of craving and PTSD symptoms after the two compared programs (MBRP and Ti-MBRP) over the 12-month follow-up period with effect sizes similar to other PTSD-SUD interventions, but with high level of attrition and level of retention lower than expected (7). Level of completion of the program in double diagnosis patients depended on PTSD Symptom Score: participants with larger symptoms severity were more likely to drop out in both groups (3). Conversely, higher level of completion occurred in women in the experimental group with lower PTSD symptoms and higher Mindfulness, as measured with FFMQ (3). A clinical trial with veterans showed large effect size on hyperarousal, reexperiencing, negative alterations in cognitions, depression but not significant effects on Positive and Negative Emotions (DES) and neither in Alcool Consumption (16).
Few studies pointed out a process analysis to understand how the interventions affected the outcome variables, PTSD symptoms. Specifically, two studies revealed the mediating effects of self-criticism and shame (1, 25) in the relationship between treatments (respectively Mindfulness-Compassion Based Trauma Recovery for Refugees program (MBTR-R) and Acceptance Commitment Therapy) and PTSD symptoms, while a study focused on the change of PTSD symptoms not just by the decrease of self-criticism but also by the increase of self-compassion (4). A study focusing on mediation analysis showed that Acceptance and Commitment Therapy (ACT) led to an increase in self-compassion, coping strategies of emotional processing and expression. These improvements, in turn, contributed to a reduction in cancer-related trauma symptoms. Additionally, self-compassion, emotional approach coping, and values-aligned behaviour marginally mediated improvements in fear of recurrence and general anxiety symptoms (25).
A study on electrophysiological indicators revealed that frontal theta heartbeat evoked brain responses (HEBR) was a mediator in the relationship between MBSR and PTSD symptoms. Hence, the intervention reduced PTSD symptoms through an increase in frontal theta HEBR (6). Finally, a fifth study found Mindfulness, in particular Positive States of Mind Scales and the subscale Non-Reactivity of FFMQ, to partially mediate the treatment effect on Hyperarousal (CAPS subscale), and Psychological Quality of Life (40).
A study examining moderator factors found that the level of adult interpersonal experiences influenced the relationship between treatment and PTSD symptoms (13). Indeed, the Trauma-Sensitive Yoga intervention was more effective for people with a history of less adult-onset interpersonal trauma experiences. Depression, dissociative symptoms, and affect dysregulation were not moderated by experiences of adult interpersonal trauma in the TCTSY intervention. Furthermore, all pre-intervention measures, except from pre-test depression score (dissociative symptoms, affect dysregulation, emotional control problems, PTSD symptoms) moderated intervention condition effects for participants exposed to fewer (i.e., one) forms of adult interpersonal trauma. In sum, the overall result indicated that the efficacy of the intervention conditions was less predictable among those with more interpersonal trauma experiences.
Finally, only two studies pointed out the adverse effects of the programs. A study on transcendental meditation reported twelve mild adverse events as referred by six participants (i.e., nausea, headache, irritability, weight gain). Two participants self-reported a severe adverse event that they believed was related to the intervention (i.e., cold-sore, body feeling heavy) (22). A second study on Trauma-informed yoga reported psychological effects referred just by a few respondents: feeling upset, anxious, or stressed after class. It is interesting to note that the group involved in substance use treatment, which retrospectively reported feeling upset, anxious or stressed before yoga class, was also the group that showed the least amount of change in self-regulation skills (30).
4. Discussion
Do contemplative practices promote trauma recovery? Most of the reviewed studies showed significant improvements in PTSD symptoms. Specifically, contemplative practices have shown to be effective in reducing most dimensions of trauma, including avoidance, reactivity, intrusion, hyperarousal, and negative cognitions and mood. Nevertheless, although this review revealed that contemplative practices improve PTSD symptoms overall, it remains unclear whether these interventions may reduce all specific facets of post-traumatic disorder. If some studies revealed changes in all the dimensions (Jasbi et al., 2018), other studies reported discrepancies in the effects of contemplative interventions. For instance, Goldstein et al. (2018) investigated the effects of a group-based Integrative Exercise (IE) program on PTSD symptoms in a group of military veterans, founding that participants in the IE group did not report improvements in symptoms of re-experiencing and avoidance when compared with the control group. Similarly, Chopin et al. (2021) tested the efficacy of a yoga program among military veterans, finding that re-experiencing and avoidance PTSD symptom subscales did not improve after treatment. Grupe et al. (2021) examined the effects of mindfulness meditation among police officers, finding large reductions in hyperarousal immediately after training and at 5-month follow up, reductions in re-experiencing immediately after treatment but not at follow-up, and no changes in avoidance symptoms at either time point. Gibert et al. (2022) examined the effects of a diving program called Bathysmed® protocol on PTSD symptoms, reporting that, except for intrusion dimension, none of the other facets changed after treatment; moreover, the effects on intrusion subscale did not persist at three-month follow up. Lang et al. (2019) found that a Cognitively-Based Compassion Training did not have significant effects on avoidance subscale in a group of military veterans. Differently, Yi et al. (2022) reported that intrusion and avoidance subscale, but not hyperarousal, significantly reduced in women with PTSD immediately after a Kripalu-based yoga intervention and at 3-months follow up. Somohano et al. (2022) examined the effects of a mindfulness intervention among women with PTSD, reporting that higher duration of mindfulness practice predicted lower avoidance, arousal, reactivity, negative cognitions and mood, but did not predict improvements in intrusion subscale at six-month follow up. Muller-Engelmann et al. (2019) found that the dimension Avoidance was especially reduced by Trauma-adapted intervention from LKM and MBSR, keeping its effect at follow-up. Similarly, Staples et al. (2022) found that a mind-body skills group especially reduced avoidance and hyperarousal. In sum, Integrative Exercise (IE), general yoga program, Cognitively-Based Compassion Training did not affect avoidance, differently from Kripalu-based yoga intervention, Trauma-adapted intervention from LKM and MBSR, and mind-body skills group. Mindfulness meditation had different outcomes on the dimension Avoidance. This discrepancy may, in part, be attributed to the type of intervention administrated. Many treatments that did not significantly impact the dimensions of Avoidance and Intrusion consisted solely of contemplative practices without incorporating trauma-based interventions. Indeed, avoidant behaviours, which are often triggered by aversive events reminiscent of traumatic experiences, and the re-experiencing of traumatic memories (i.e., intrusion) are particularly challenging symptoms to address. These symptoms may require a psychotherapeutic approach specifically designed for trauma and an extended duration of treatment to achieve meaningful improvements. This result is in line with existing literature that indicates that interventions explicitly focused on traumatic experiences—such as those incorporating trauma narratives—tend to be more effective than approaches that do not directly address trauma (Watts et al., 2013). This can be one fundamental reason why contemplative practices do not appear to yield improvements across all dimensions of PTSD, suggesting that trauma-focused psychotherapies may be necessary to achieve more comprehensive outcomes.
The hypothesis of a dose-response effect could also be supported by some controversial results from physiological parameters (6, 33, 37, 27). Authors suggested that a longer intervention is needed to produce physiological changes (such as a change in heart rate variability), considering that shifting from threat to soothing emotion system is not immediate (Gilbert, 2009). At the same time, a longer treatment might be needed in order to increase a sense of security and reduce the threat related to aversive experiences and, consequently, avoidant behaviours that have a self-protective function.
Furthermore, physiological results showed a reduction of sympathetic arousal and lower basal activity of SNS (Sympathetic Nervous System). The dysregulation of SNS together with parasympathetic disinhibition might be a marker of behavioural activation or inhibition (Beauchaine, 2001), according to the neurovisceral integration model (Thayer & Lane, 2000) and it is theorized to precede cognitive changes (Nishith et al., 2002). Moreover, the studies reviewed has shown that reductions in sympathetic activity during rest were associated with decreases in self-reported posttraumatic symptoms. This finding is in line with research indicating that lower levels of sympathetic activity are associated with decreased feelings of fear (Raine, 2002) and threat (Blascovich, 2008). Future research could deepen the complex causality of the relation between physiological and psychological parameters in PTSD symptoms.
According to our results, mindfulness is the contemplative practice most used to promote trauma recovery. Mindfulness meditation is defined as paying attention to the present moment, being aware and non-judgementally accepting (Brown & Ryan, 2003). Thus, several authors stated that mindfulness meditation is effective in reducing PTSD due to a top-down approach (e.g., Chiesa et al., 2013). Indeed, as mindfulness is focused on the ability to act with awareness and non-judgementally, as well as on the capacity of reorientation of habitual patterns of thinking, it may be therapeutic for the trauma-related rumination and reduce emotional distress and hyperarousal, even without a direct discussion of trauma-related content (e.g., Boyd et al., 2018). Participants are encouraged to attend to arising and passing stimuli, including aversive trauma-related memories, increasing tolerance for experiencing negative affective states, and reduce numbing and hyperarousal when faced with trauma symptoms.
Interestingly, our findings revealed that contemplative practices also improved various secondary outcomes, including anxiety, depression, operational stress, negative affect, interoception and emotion regulation. In most cases, reductions in PTSD were intuitively associated with the decrease in anxiety and depression. This is not surprising if we consider the literature on the effects of MBIs on internalizing symptoms (Ghiroldi et al., 2020; Scafuto et al., 2022; 2023).
Regarding interoception, interventions predicted positive effects almost on all the dimensions of the MAIA, revealing Self-regulation to be the largest effect size in parallel with hyperarousal and Non-Reactivity (40). Interoception was also correlated to emotion regulation and Soothing Receptivity.
In addition to reducing distress-related psychological outcomes, findings showed the ability of these interventions to enhance eudaimonic well-being, social domains such as increase in social connectedness (16), social role functioning (34), and overall quality of life. Qualitative results found changes participants’ search for life meaning, a narrative revaluation of life experiences, and a reordering of spiritual and universalistic values. Participants also reported shifts in time perspective, an increased attitude of self-care, and the adoption of positive coping strategies (15). These results recall previous qualitative studies that testify the so-called post-traumatic growth, which is often reinforced by formal and informal contemplative practices (Durà-Vilà et al., 2013; Emmerich, 2022), in the aftermath of traumatic events. In addition, results seem to give support to the Mindfulness-to-Meaning Theory (MMT; Garland et al., 2015), as mindfulness appears to facilitate the cognitive reappraisal of traumatic events and rebuild a new meaning and purpose in life. Previous results showed effects of MBIs programs on eudaimonic well-being, especially on purpose in life in adolescents (Scafuto et al., 2023).
Another perspective on the effectiveness of these interventions concerns the specific diagnoses characterizing the study samples. For example, individuals with co-occurring SUD (Substance Use Disorder) required more intensive mindfulness skills training either prior to or during treatment to enhance their willingness to experience distressing thoughts, feelings, or substance cravings. Previous studies supporting the efficacy of MBIs for managing craving highlighted several mediators of this effect, including reductions in negative affect as well as improvements in emotion regulation, emotional well-being, and group cohesiveness (Vago et al., 2019).
Regarding the process analysis, it is interesting to reveal that just five of the reviewed studies (1, 4, 6, 25, 40) carried out mediation analyses in order to examine the psychological or physiological mechanisms, which may explain the improvements in PTSD symptoms following contemplative practices. For example, Aizik-Reebs et al. (2022) found that reduced levels of self-criticism as well as improved self-compassion following a Mindfulness-Based Trauma Recovery for Refugees (MBTR-R) program mediated the therapeutic effects of the intervention on PTSD symptoms. This result recalls similar previous results in a different population characterized by double diagnosis of SUD and PTSD, where contemplative practices predicted a reduction of shame and no-judgmental attitude and these, in turn, affected substance use severity and PTSD symptoms (La Bash & Papa, 2014; Sancho et al., 2018). In another study with MBTR-R, Oren-Schwartz et al. (2023) found the mediating role of shame in the relationship between the therapeutic effects of MBTR-R and PTSD symptoms. Kang et al. (2021) found that MBSR reduced PTSD symptom severity by improving the frontal theta heartbeat-evoked brain response (HEBR) in a group of military veterans with PTSD. Fishbein et al. (2022) carried out a multiple mediation model wherein self-compassion and emotional coping mediated the relationship between Acceptance and Commitment Therapy effects and the cancer-related trauma symptoms among cancer survivors. Finally, Mehling et al. (2018) found Mindfulness facet of non-reactivity and Positive state of Mind to partially mediate the treatment effect on Hyperarousal and Psychological Quality of Life.
These processes, which involved both psychological and physiological mechanisms, seem to be of relevance to reduce or improve the effects of contemplative practices on trauma recovery. In particular, contemplative practices physiologically increase heartbeat-evoked brain responses that are interoceptive signals, thereby improving attentional control and resting brain states. Interoceptive neural functions seem to be a primary cerebral mechanism that improves symptoms of PTSD, given that contemplative practices train to cultivate attention to the present moment and bodily sensations, reinforcing interoception. The somatic component of contemplative practices is pivotal in facilitating the trauma recovery process, by allowing individuals to notice visceral feelings and forge somatic connections (Emerson, 2015). In fact, contemplative practices based on body movements and active breathing, which can be considered bottom-up interventions, could enhance interoceptive ability by triggering involuntary attention on the unblocked feelings that were repressed (Lazzarelli et al., 2024).
Another mechanism through which contemplative practices contribute to trauma recovery is their influence on fostering positive states of mind, particularly self-compassion vs. self-criticism and self-blame. After experiencing traumatic stressors, individuals often develop negative, self-critical appraisals and beliefs (e.g., “I am worthless/weak/wrong because I am not able to deal with it”). These self-critical patterns can perpetuate chronic stress over time (Harman & Lee, 2010). In contrast, self-compassion – a multidimensional construct – offers an alternative approach. It encompasses self-kindness, recognition and understanding the universality of suffering, tolerating it without judgement and committing to actions that reduce further suffering (Neff, 2003; Strauss et al., 2016). Contemplative practices actively cultivate these qualities, helping individuals replace self-criticism with self-compassion, which may alleviate the psychological burden of trauma and support recovery. It is reasonable to hypothesize that enhanced attention to the present moment, combined with the compassionate thoughts and feeling elicited by explicit self-compassion practices, transforms the way individuals relate to mental states such as rumination and self-blame. By bringing these states into awareness as object of observation, contemplative practices reduce identification with negative thoughts and actively foster attitudes of self-kindness and common humanity.
A core goal of those programs is to strengthen specific mental states that help the engagement of the individual’s compassionate Self, bolstering a safe internal environment that improves processing of traumatic memories and assist healing, involving curiosity, calm, clarity, connectedness, courage, and creativity (Anderson et al., 2017). Future studies could investigate the protective effect of self-compassion for the intrusive and pervasive thinking associated with traumatic experiences and amplify the psychological changes following contemplative practices.
5. Limitations
This review also points out some limitations. First, outcome data were collected using self-report measures, which can be susceptible to issues such as practice effects and response bias. Moreover, other factors, such as cohesion, treatment engagement, therapist characteristics, are not always available in the studies here selected and should be included as covariates in future research. Second, most studies are based on a small sample size. In clinical contexts, it is usual to have fewer participants in the trials, since the sample size should not be a limitation if we investigate our research questions with a more adequate methodology that fits with the sample and the aims. The lack of significant effects in some cases, indeed, could cover relevant effects that do not emerge because of the small sample size, while in some studies we assist to a variety of variables, too many investigated in a single study, that could overestimate significant effects on the other side. Hence, we argue that there is a problem of methodology and that clinical questions could be addressed more properly using qualitative methods for small scales, leaving more complex statistical models for larger samples (type II error). A third limitation is related to the uncertainty on the relationship between treatments and effects. This applies particularly to mixed interventions (e.g. mindfulness with trauma therapy), in which it is impossible to know exactly what produces the effects. Future studies could combine interviews and focus group with quantitative studies, in order to investigate what exactly produced a change in the participants according to their qualitative reports. Fourth, in most cases the sample is composed of White participants living in an urban context. Although we are aware that white or WEIRD (Western, Educated, Industrialized, Rich, and Democratic) people are more likely recruited in this kind of clinical trials because they have a better access to contemplative practices, the lack of ethnic, cultural and geographical heterogeneity in the sample limits its cross-cultural validity. It is unclear whether the findings would be translatable to others, no-WEIRD, living in non-metropolitan regions. Furthermore, data show that the feasibility rates were lower in the treatment groups, emphasizing that barriers to engaging in a treatment exist and need to be addressed to improve outcomes. High drop-out in several studies make difficult to interpret the results on the effectiveness and feasibility of the proposed interventions. Besides, most studies did not analyse the effects of interventions, comparing completers and non-completers. The retention issue is especially present for no WEIRD population due to psychosocial problems, material and financial reasons, and cultural barriers among others. Understanding barriers to retaining those in the experimental group is a key factor for future implementation. For instance, it is crucial to consider cultural difference in experiencing self-criticism as shame or guilt and in their impact on psychopathology and traumatic symptoms. In WEIRD population, guilt could have a prominent role, having psychopathogenic or traumatogenic effects independent of shame (Kubany & Watson, 2003). Contrarily, among asylum-seekers and general non-WEIRD population, shame rather than guilt seems to have a bigger impact on psychopathology and traumatic symptoms (1, 4). This may be due to the fact that no-WEIRD population generally belong to a more community-oriented culture, where shame is more associated with the fear that one’s problems will result in the loss of union with, or expulsion from the group (Creighton, 1990). Some studies focused on alternative samples like groups of refugee population (1, 4), yet they pose a limit to the generalizability of findings considering their stressful, uncertain, and insecure urban post-displacement setting. Nevertheless, this type of PTSD disorder’s victims represents a common and fast-growing population, given the global spread of wars, famine, climate disasters, and pandemics. It is, indeed, a limitation to find little attention to collective traumas. In this regard, future studies should overcome this gap of literature, investigating more community treatments for collective traumas, given the global emergencies that we are dealing with such as climate crisis with a huger number of victims of acute and chronic environmental stressors.
6. Conclusions
The present review showed the effectiveness of programs integrating contemplative practices in the treatment of PTSD victims. It also underlined controversial results and limitations that could be overcome in future investigations. In dealing with the fast-growing large scale mental distress, especially due to the emergent global collective traumatic events and conditions, contemplative practices could be cost-effective and feasible interventions for traumatic symptoms. Nevertheless, their overall effectiveness depends on the duration and the combination with trauma-focused treatments. Given the large variety of health programs for trauma, the authors do not call for novel interventions, rather they suggest a combination of programs that integrate somatic components with cognitive and emotional ones. On one side, people with posttraumatic stress need a support to learn to stay with the discomfort of emotions, thoughts, bodily sensations, the faint-freeze response to acute stress and the defensive mechanisms activated for the neuroperception of threat. On the other side, by allowing a neuroperception of safety and cultivating self-compassion attitude, interventions and practices can focus on emotions, bodily sensations, and thoughts as an opportunity to reframe past memories. If needed, they also can facilitate the completion of emotional action sequences that were interrupted or restrained in the past, when the traumatic events or relationships occurred. Contemplative practices could contribute to promote this sense of safety, allowing psychotherapeutic interventions focused on trauma to work on reframing dysfunctional beliefs, emotion expression, and metacognitive processes in order to heal the sense of self, often wounded in post-traumatic victims.
Glossary
| Abbreviation | Description |
| AAOc | Acceptance and Action Questionnaire-Cancer |
| ANS | Autonomous Nervous System |
| AQoL-8D | Australian Quality of Life (8-dimension) |
| ASI | Addiction Severity Index |
| AUDIT-C | Alcohol Use Disorders Identification Test |
| BAI | Beck Anxiety Inventory |
| BDI | Beck Depression Inventory |
| BDI-II | Beck Depression Inventory-II |
| BEAQ | Brief Experiential Avoidance Questionnaire; |
| BEVS | Bull’s-Eye Values Survey |
| BPM | Brief Problem Monitor |
| BRIEF | Behavioral Rating Inventory of Executive Function |
| BSI | Brief Symptom Inventory |
|
BSI-18 BSSS |
Brief Symptom Inventory Brief Sensation Seeking Scale |
| CAMS-R | Cognitive and Affective Mindfulness Scale-Revised |
| CAPS | Clinician-Administered Posttraumatic Stress Disorder Scale |
| CAPS-5 | Clinician-Administered PTSD Scale for DSM-5 |
| CARS | Concerns About Recurrence Scale |
| COPE | Coping Orientation to the Problems Experienced |
| CSQ | Client Satisfaction Questionnaire |
| CSQ-8 | Client Satisfaction Questionnaire |
| CTQ-SF | Childhood Trauma Questionnaire Short Form |
| DASS-21 | Depression Anxiety and Stress Scale |
| DERS | Difficulties in Emotional Regulation Scale |
| DES | Dissociative Experiences Scale |
| DES’ | Differential Emotions Scale |
| DTS | Davidson Trauma Scale |
| EAC | Emotional Approach Coping scale |
| ECG | Electrocardiogram |
| ERQ | Emotion Regulation Questionnaire |
| ERS | Emotion Regulation Scale |
| FCS | fears of compassion scales |
| FFMQ | Five-Facet Mindfulness Questionnaire |
| FMI | Freiburg Mindfulness Inventory |
| FSCRS | Forms of Self-Criticizing/attacking and Self-Reassuring Scale |
| GAD-7 | Generalized Anxiety Disorder Scale |
| GHQ-28 | General Health Questionnaire |
| HADS-A | Hospital Anxiety and Depression Scale-Anxiety subscale |
| Ham-D | Hamilton Depression Rating Scale |
| HEBR | Heartbeat-evoked brain response |
| HR | Heart Rate |
| HRV | Heart Rate Variability |
| HSCL | Hopkins Symptom Checklist |
| HTQ | The Harvard Trauma Questionnaire |
| IASC | Inventory of Altered Self-Capacities |
| ICG | Impedance Cardiography |
| IES | Impact of Events Scale |
| IES-R | Impact of Events Scale-Revised |
| IIP-32 | Inventory of Interpersonal Problems |
| IMR | Illness Management and Recovery |
| IPDE | International Personality Disorder Examination |
| IPVE | Intimate Partner Violence exposure |
| ISI | Insomnia Severity Index |
| K10 | Kessler Psychological Distress Scale |
| LEC-5 | Life Events Checklist |
| LKM | loving-kindness meditation |
| LKM-S | loving-kindness meditation for self-compassion |
| LSCL-R | Life Stressor Checklist Revised |
| LSI | Leisure Score Index |
| MAAS | Mindfulness Awareness Attention Scale |
| MAIA | Multidimensional Assessment of Interoceptive Awareness |
| MBE | Mindful-Breathing Exercise |
| MINI | Mini International Neuropsychiatric Interview |
| MoCA | Montreal Cognitive Assessment |
| NIH PROMIS | National Institutes of Health’s Patient-Reported Outcomes Measurement Information System |
| OAS | Other as Shamer Scale |
| OCSS | Overall Course Satisfaction Survey |
| OLBI | Oldenburg Burnout Inventory |
| PACS | Penn Alcohol Craving Scale |
| PANAS | Positive and Negative Affect Schedule |
| PBPT | Perceived Barriers to Psychological Treatments |
| PCL-5 | PTSD checklist for DSM-5 |
| PCL-C | PTSD Checklist-Civilian Version |
| PCL-M | PTSD Checklist-Military Version |
| PHLMS | Philadelphia Mindfulness Scale |
| PHQ | Patient Health Questionnaire |
| PHQ-8 | Patient Health Questionnaire Eight-item version |
| PHQ-9 | Brief Patient Health Questionnaire for Depression |
| PMLD | Postmigration Living Difficulties Scale |
| PROMIS | Patient Reported Outcomes Measurement Information System 43-item version |
| PSOM | Positive States of Mind Scales |
| PSQ | Police Stress Questionnaire |
| PSQI | Pittsburgh Sleep Quality Index |
| PSS | PTSD Symptom Scale-Self Report |
| PTSS | The Post-Traumatic Stress Scale |
| PWB | Psychological Well-Being Scale |
| Q-LES-SF | Quality of Life Enjoyment and Satisfaction Questionnaire–Short Form |
| RAS | Relationship Assessment Scale |
| RCT | Randomized Controlled Trial |
| REDS | Reward-based Eating Drive Scale |
| RMSSD | Root Mean Square of Successive Differences |
| RTSQ | Ruminative Thought Style Questionnaire |
| S-Ang | State Anger scale |
| SBC | Scale of Body Connection |
| SCID-I | Structured Clinical Interview for DSM-IV |
| SCL | Skin Conductance Levels |
| SCS | Self- Compassion Scale |
| SCS-R | Social Connectedness Scale–Revised |
| SCS-S | Self- Compassion Scale- Short Form |
| SDQ-20 | Somatoform Dissociation Questionnaire |
| SIDES-SR | Structured Interview for Disorders of Extreme Stress, Self- Report version |
| SLESQ | Stressful Life Events Screening Questionnaire |
| SRET | Self-Referential Encoding Task |
| SRS | Soothing Receptivity Scale |
| SSGS | State Shame and Guilt Scale |
| SSPS | Social Safeness and Pleasure Scale |
| SSS-8 | Eight-item Somatic Symptom Scale |
| SSST | Sing-a-Song Stress Test |
| STAXI-2 | State–Trait Anger Expression Inventory–2 |
| SUD | Subjective Units of Distress Scale |
| TEI | Traumatic Events Inventory |
| TEQ | Toronto Empathy Questionnaire |
| TF | Time Frequency |
| TLFB | Timeline Follow Back |
| TM | Transcendental Meditation |
| TRIER-C | Trier Social Stress Task for Children |
| TSK-11 | Tampa Scale of Kinesiophobia |
| UFOV | Useful Field of View Test |
| VAS | Visual Analogue scales |
| VLQ | Valued Living Questionnaire |
| VU-AMS | VU University Monitoring System |
| WAI-SR | Working Alliance Inventory-Short Revised |
| WGO-5 | WHO-Five Well-Being Index |
| WHOQOL | World Health Organization Quality of Life, Brief Version |
| WQL-8 | Work Limitations Questionnaire-Short Form |
| WSAS | Work and Social Adjustment Scale |
References
- *Aizik-Reebs, A., Amir, I., Yuval, K., Hadash, Y., & Bernstein, A. (2022). Candidate mechanisms of action of mindfulness-based trauma recovery for refugees (MBTR-R): Self-compassion and self-criticism. Journal of Consulting and Clinical Psychology, 90(2), 107-122. [CrossRef]
- Amihai, I., & Kozhevnikov, M. (2014). Arousal vs. relaxation: A comparison of the neurophysiological and cognitive correlates of Vajrayana and Theravada meditative practices. PloS One, 9(7), e102990. [CrossRef]
- Aquinas, T. (1869). Summa theologica (Vol. 5). Guerin.
- Aquinas, T. (1975). Summa contra gentiles. Book Two: Creation. University of Notre Dame.
- *Bandy, C. L., Dillbeck, M. C., Sezibera, V., Taljaard, L., Wilks, M., Shapiro, D., de Reuck, J., & Peycke, R. (2020). Reduction of PTSD in South African University Students Using Transcendental Meditation Practice. Psychological Reports, 123(3), 725–740. [CrossRef]
- *Bellehsen, M., Stoycheva, V., Cohen, B. H., & Nidich, S. (2022). A Pilot Randomized Controlled Trial of Transcendental Meditation as Treatment for Posttraumatic Stress Disorder in Veterans. Journal of traumatic stress, 35(1), 22–31. [CrossRef]
- Bodhi, B. (2012) The Numerical Discourses of the Buddha: A Translation of the Aṅguttara Nikāya. Pāli Text Society in association with Wisdom Publications.
- Boyd, J. E., Lanius, R. A., & McKinnon, M. C. (2018). Mindfulness-based treatments for posttraumatic stress disorder: a review of the treatment literature and neurobiological evidence. Journal of Psychiatry and Neuroscience, 43(1), 7-25. [CrossRef]
- Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822-848. [CrossRef]
- Bruce, M. M., Kassam-Adams, N., Rogers, M., Anderson, K. M., Sluys, K. P., & Richmond, T. S. (2018). Trauma Providers’ Knowledge, Views, and Practice of Trauma-Informed Care. Journal of Trauma Nursing: The Official Journal of the Society of Trauma Nurses, 25(2), 131–138. [CrossRef]
- Calhoun, L. G., Cann, A., Tedeschi, R. G., & McMillan, J. (2000). A correlational test of the relationship between posttraumatic growth, religion, and cognitive processing. Journal of Traumatic Stress, 13(3), 521–527. [CrossRef]
- Chiesa, A., Serretti, A., & Jakobsen, J. C. (2013). Mindfulness: Top–down or bottom–up emotion regulation strategy?. Clinical Psychology Review, 33(1), 82-96. [CrossRef]
- *Chopin, S. M., Sheerin, C. M., & Meyer, B. L. (2020). Yoga for warriors: An intervention for veterans with comorbid chronic pain and PTSD. Psychological Trauma: Theory, Research, Practice and Policy, 12(8), 888–896. [CrossRef]
- *Classen, C. C., Hughes, L., Clark, C., Hill Mohammed, B., Woods, P., & Beckett, B. (2021). A pilot RCT of a body-oriented group therapy for complex trauma survivors: an adaptation of sensorimotor psychotherapy. Journal of Trauma & Dissociation, 22(1), 52-68. [CrossRef]
- Conversano, C., Di Giuseppe, M., Miccoli, M., Ciacchini, R., Gemignani, A., & Orrù, G. (2020). Mindfulness, Age and Gender as Protective Factors Against Psychological Distress During COVID-19 Pandemic. Frontiers in Psychology, 11, 1900. [CrossRef]
- *Cox, C. E., Hough, C. L., Jones, D. M., Ungar, A., Reagan, W., Key, M. D., ... & Porter, L. S. (2019). Effects of mindfulness training programmes delivered by a self-directed mobile app and by telephone compared with an education programme for survivors of critical illness: a pilot randomised clinical trial. Thorax, 74(1), 33-42. [CrossRef]
- Critchley, H. D., & Garfinkel, S. N. (2017). Interoception and emotion. Current Opinion in Psychology, 17, 7–14. [CrossRef]
- *Davis, L. W., Schmid, A. A., Daggy, J. K., Yang, Z., O'Connor, C. E., Schalk, N., ... & Knock, H. (2020). Symptoms improve after a yoga program designed for PTSD in a randomized controlled trial with veterans and civilians. Psychological Trauma: Theory, Research, Practice, and Policy, 12(8), 904. [CrossRef]
- DeLoach, C. D., & Petersen, M. N. (2010). African spiritual methods of healing: The use of Candomblé in traumatic response. Journal of Pan African Studies, 3(8), 40-65.
- DeRosa, R., & Pelcovitz, D. (2009). Group treatment for chronically traumatized adolescents: Igniting SPARCS of change. In Treating traumatized children: Risk, resilience and recovery (pp. 225–239). Routledge/Taylor & Francis Group.
- Duran, E., Firehammer, J., & Gonzalez, J. (2008). Liberation Psychology as the Path Toward Healing Cultural Soul Wounds. Journal of Counseling & Development, 86. [CrossRef]
- Durà-Vilà, G., Littlewood, R., & Leavey, G. (2013). Integration of sexual trauma in a religious narrative: Transformation, resolution and growth among contemplative nuns. Transcultural Psychiatry, 50(1), 21–46. [CrossRef]
- *Fishbein, J. N., Judd, C. M., Genung, S., Stanton, A. L., & Arch, J. J. (2022). Intervention and mediation effects of target processes in a randomized controlled trial of Acceptance and Commitment Therapy for anxious cancer survivors in community oncology clinics. Behaviour Research and Therapy, 153, 104103. [CrossRef]
- Fiske, E., Martin, S., & Luetkemeyer, J. (2020). Building Nurses’ Resilience to Trauma Through Contemplative Practices. Creative Nursing, 26(4), e90–e96. [CrossRef]
- *Fortuna, L. R., Falgas-Bague, I., Ramos, Z., Porche, M. V., & Alegría, M. (2020). Development of a cognitive behavioral therapy with integrated mindfulness for Latinx immigrants with co-occurring disorders: Analysis of intermediary outcomes. Psychological Trauma: Theory, Research, Practice, and Policy, 12(8), 825-835. [CrossRef]
- *Gallegos, A. M., Heffner, K. L., Cerulli, C., Luck, P., McGuinness, S., & Pigeon, W. R. (2020). Effects of mindfulness training on posttraumatic stress symptoms from a community-based pilot clinical trial among survivors of intimate partner violence. Psychological Trauma: theory, research, practice, and policy, 12(8), 859-868. [CrossRef]
- Garland, E. L., Geschwind, N., Peeters, F., & Wichers, M. (2015). Mindfulness training promotes upward spirals of positive affect and cognition: Multilevel and autoregressive latent trajectory modeling analyses. Frontiers in Psychology, 6, 15. [CrossRef]
- *Gerdes, S., Williams, H., & Karl, A. (2022). Psychophysiological responses to a brief self-compassion exercise in armed forces veterans. Frontiers in Psychology, 12, 780319. [CrossRef]
- Germer, C.K., & Siegel, R.D. (2014). Wisdom and Compassion in Psychotherapy. Deepening Mindfulness in Clinical Practice. Guilford Press.
- Glassman, E. (1988). Development of a self-report measure of soothing receptivity [Ph.D.]. York University.
- Ghiroldi, S., Scafuto, F., Montecucco, N.F. et al. Effectiveness of a School-Based Mindfulness Intervention on Children’s Internalizing and Externalizing Problems: the Gaia Project. Mindfulness 11, 2589–2603 (2020). [CrossRef]
- *Gibert, L., Coulange, M., Reynier, J. C., Le Quiniat, F., Molle, A., Bénéton, F., ... & Trousselard, M. (2022). Comparing meditative scuba diving versus multisport activities to improve post-traumatic stress disorder symptoms: a pilot, randomized controlled clinical trial. European Journal of Psychotraumatology, 13(1), 2031590. [CrossRef]
- Goldberg, S. B., Riordan, K. M., Sun, S., & Davidson, R. J. (2022). The Empirical Status of Mindfulness-Based Interventions: A Systematic Review of 44 Meta-Analyses of Randomized Controlled Trials. Perspectives on Psychological Science: A Journal of the Association for Psychological Science, 17(1), 108–130. [CrossRef]
- *Goldstein, L. A., Mehling, W. E., Metzler, T. J., Cohen, B. E., Barnes, D. E., Choucroun, G. J., Silver, A., Talbot, L. S., Maguen, S., Hlavin, J. A., Chesney, M. A., & Neylan, T. C. (2018). Veterans Group Exercise: A randomized pilot trial of an Integrative Exercise program for veterans with posttraumatic stress. Journal of Affective Disorders, 227, 345–352. [CrossRef]
- *Grupe, D. W., McGehee, C., Smith, C., Francis, A. D., Mumford, J. A., & Davidson, R. J. (2021). Mindfulness training reduces PTSD symptoms and improves stress-related health outcomes in police officers. Journal of Police and Criminal Psychology, 36(1), 72–85. [CrossRef]
- Hanley, A. W., Garland, E. L., & Tedeschi, R. G. (2017). Relating dispositional mindfulness, contemplative practice, and positive reappraisal with posttraumatic cognitive coping, stress, and growth. Psychological Trauma: Theory, Research, Practice and Policy, 9(5), 526–536. [CrossRef]
- *Hodgdon, H. B., Anderson, F. G., Southwell, E., Hrubec, W., & Schwartz, R. (2022). Internal Family Systems (IFS) Therapy for Posttraumatic Stress Disorder (PTSD) among Survivors of Multiple Childhood Trauma: A Pilot Effectiveness Study. Journal of Aggression, Maltreatment & Trauma, 31(1), 22–43. [CrossRef]
- Hopson, D. P., & Hopson, D. S. (1999). The power of soul: Pathways to psychological and spiritual growth for African Americans. Harper Perennial.
- Ibañez, G. E., Sanchez, M., Villalba, K., & Amaro, H. (2022). Acting with awareness moderates the association between lifetime exposure to interpersonal traumatic events and craving via trauma symptoms: a moderated indirect effects model. BMC Psychiatry, 22(1), 287. [CrossRef]
- Jäger, W. (2003). Search for the meaning of life: Essays and reflections on the mystical experience. Liguori/Triumph.
- *Jasbi, M., Sadeghi Bahmani, D., Karami, G., Omidbeygi, M., Peyravi, M., Panahi, A., ... & Brand, S. (2018). Influence of adjuvant mindfulness-based cognitive therapy (MBCT) on symptoms of post-traumatic stress disorder (PTSD) in veterans–results from a randomized control study. Cognitive Behaviour Therapy, 47(5), 431-446. [CrossRef]
- *Javidi, Z., Prior, K.N., Sloan, T.L. et al. A randomized controlled trial of self-compassion versus cognitive therapy for complex psychopathologies. Current Psychology, 42, 946–954 (2023). [CrossRef]
- *Kananian, S., Soltani, Y., Hinton, D., & Stangier, U. (2020). Culturally Adapted Cognitive Behavioral Therapy Plus Problem Management (CA-CBT+) With Afghan Refugees: A Randomized Controlled Pilot Study. Journal of Traumatic stress, 33(6), 928–938. [CrossRef]
- *Kang, S. S., Sponheim, S. R., & Lim, K. O. (2022). Interoception underlies therapeutic effects of mindfulness meditation for posttraumatic stress disorder: A randomized clinical trial. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 7(8), 793-804. [CrossRef]
- Kelly, U. A., Evans, D. D., Baker, H., & Noggle Taylor, J. (2018). Determining Psychoneuroimmunologic Markers of Yoga as an Intervention for Persons Diagnosed With PTSD: A Systematic Review. Biological Research for Nursing, 20(3), 343–351. [CrossRef]
- *Killeen, T. K., Wen, C. C., Neelon, B., & Baker, N. (2023). Predictors of Treatment Completion among Women Receiving Integrated Treatment for Comorbid Posttraumatic Stress and Substance Use Disorders. Substance Use & Misuse, 58(4), 500-511. [CrossRef]
- Kim, S. H., Schneider, S. M., Kravitz, L., Mermier, C., & Burge, M. R. (2013). Mind-body practices for posttraumatic stress disorder. Journal of Investigative Medicine, 61(5), 827-834. [CrossRef]
- *Knabb, J. J., Vazquez, V. E., Pate, R. A., Lowell, J. R., Wang, K. T., De Leeuw, T. G., Dominguez, A. F., Duvall, K. S., Esperante, J., Gonzalez, Y. A., Nagel, G. L., Novasel, C. D., Pelaez, A. M., Strickland, S., & Park, J. C. (2022). Lectio divina for trauma symptoms: A two-part study. Spirituality in Clinical Practice, 9(4), 232–252. [CrossRef]
- Lang, A. J., Casmar, P., Hurst, S., Harrison, T., Golshan, S., Good, R., … Negi, L. (2017). Compassion meditation for veterans with posttraumatic stress disorder (PTSD): A nonrandomized study. Mindfulness, 1–12. [CrossRef]
- *Lang, A. J., Malaktaris, A. L., Casmar, P., Baca, S. A., Golshan, S., Harrison, T., & Negi, L. (2019). Compassion meditation for posttraumatic stress disorder in veterans: A randomized proof of concept study. Journal of Traumatic Stress, 32(2), 299-309. [CrossRef]
- Lang, A. J., Strauss, J. L., Bomyea, J., Bormann, J. E., Hickman, S. D., Good, R. C., & Essex, M. (2012). The theoretical and empirical basis for meditation as an intervention for PTSD. Behavior Modification, 36, 759–786. [CrossRef]
- LaVallie, C., & Sasakamoose, J. (2023). Promoting indigenous cultural responsivity in addiction treatment work: The call for neurodecolonization policy and practice. Journal of Ethnicity in Substance Abuse, 22(3), 477–499. [CrossRef]
- Lazar, S. W., Bush, G., Gollub, R. L., Fricchione, G. L., Khalsa, G., & Benson, H. (2000). Functional brain mapping of the relaxation response and meditation. Neuroreport, 11(7), 1581–1585. [CrossRef]
- Lazzarelli, A., Scafuto, F., Crescentini, C., Matiz, A., Orrù, G., Ciacchini, R., ... & Conversano, C. (2024). Interoceptive Ability and Emotion Regulation in Mind–Body Interventions: An Integrative Review. Behavioral Sciences, 14(11), 1107. [CrossRef]
- *Leach, M. J., & Lorenzon, H. (2024). Transcendental Meditation for women affected by domestic violence: A pilot randomised, controlled trial. Journal of Family Violence, 39(8), 1437-1446. [CrossRef]
- Lindahl, J. R., Fisher, N. E., Cooper, D. J., Rosen, R. K., & Britton, W. B. (2017). The varieties of contemplative experience: A mixed-methods study of meditation-related challenges in Western Buddhists. PloS One, 12(5), e0176239. [CrossRef]
- Loizzo J. J. (2016). The subtle body: an interoceptive map of central nervous system function and meditative mind-brain-body integration. Annals of the New York Academy of Sciences, 1373(1), 78–95. [CrossRef]
- Loizzo, J. (2014). Meditation research, past, present, and future: Perspectives from the Nalanda contemplative science tradition. Annals of the New York Academy of Sciences, 1307(1), 43–54. [CrossRef]
- Macy, J. (1991). Mutual causality in Buddhism and general systems theory: The dharma of natural systems. Suny Press. [CrossRef]
- *Mehling, W. E., Chesney, M. A., Metzler, T. J., Goldstein, L. A., Maguen, S., Geronimo, C., Agcaoili, G., Barnes, D. E., Hlavin, J. A., & Neylan, T. C. (2018). A 12-week integrative exercise program improves self-reported mindfulness and interoceptive awareness in war veterans with posttraumatic stress symptoms. Journal of Clinical Psychology, 74(4), 554–565. [CrossRef]
- Mendelson, T., Clary, L. K., Sibinga, E., Tandon, D., Musci, R., Mmari, K., ... & Ialongo, N. (2020). A randomized controlled trial of a trauma-informed school prevention program for urban youth: Rationale, design, and methods. Contemporary Clinical Trials, 90, 105895. [CrossRef]
- *Miller, R. L., Moran, M., Shomaker, L. B., Seiter, N., Sanchez, N., Verros, M., ... & Lucas-Thompson, R. (2021). Health effects of COVID-19 for vulnerable adolescents in a randomized controlled trial. School Psychology, 36(5), 293-302. [CrossRef]
- Monteiro, N. M., & Wall, D. J. (2011). African dance as healing modality throughout the diaspora: The use of ritual and movement to work through trauma. Journal of Pan African Studies, 4(6), 234-252. [CrossRef]
- *Müller-Engelmann, M., Schreiber, C., Kümmerle, S., Heidenreich, T., Stangier, U., & Steil, R. (2019). A trauma-adapted mindfulness and loving-kindness intervention for patients with PTSD after interpersonal violence: A multiple-baseline study. Mindfulness, 10(6), 1105–1123. [CrossRef]
- *Nguyen-Feng, V. N., Hodgdon, H., Emerson, D., Silverberg, R., & Clark, C. J. (2020). Moderators of treatment efficacy in a randomized controlled trial of trauma-sensitive yoga as an adjunctive treatment for posttraumatic stress disorder. Psychological Trauma: theory, research, practice, and policy, 12(8), 836-846. [CrossRef]
- Norbu, N., & Shane, J. (1987). Il cristallo e la via della luce: Sutra, tantra e Dzog-chen. Ubaldini. [CrossRef]
- *Ong, I., Cashwell, C. S., & Downs, H. A. (2019). Trauma-sensitive yoga: A collective case study of women’s trauma recovery from intimate partner violence. Counseling Outcome Research and Evaluation, 10(1), 19–33. [CrossRef]
- *Oren-Schwartz, R., Aizik-Reebs, A., Yuval, K., Hadash, Y., & Bernstein, A. (2023). Effect of mindfulness-based trauma recovery for refugees on shame and guilt in trauma recovery among African asylum-seekers. Emotion, 23(3), 622-632. [CrossRef]
- Poli, A., Gemignani, A., Soldani, F., & Miccoli, M. (2021). A Systematic Review of a Polyvagal Perspective on Embodied Contemplative Practices as Promoters of Cardiorespiratory Coupling and Traumatic Stress Recovery for PTSD and OCD: Research Methodologies and State of the Art. International Journal of Environmental Research and Public Health, 18(22), 11778. [CrossRef]
- Porges, S. W. (2001). The polyvagal theory: Phylogenetic substrates of a social nervous system. International Journal of Psychophysiology, 42(2), 123–146. [CrossRef]
- Porges, S. W. (2003). The Polyvagal Theory: Phylogenetic contributions to social behavior. Physiology & Behavior, 79(3), 503–513. [CrossRef]
- Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. Norton & Co. [CrossRef]
- *Possemato, K., Bergen-Cico, D., Buckheit, K., Ramon, A., McKenzie, S., Smith, A. R., ... & Pigeon, W. R. (2022). Randomized clinical trial of brief primary care–based mindfulness training versus a psychoeducational group for veterans with posttraumatic stress disorder. The journal of Clinical Psychiatry, 84(1), 44829. [CrossRef]
- *Powers, A., Lathan, E. C., Dixon, H. D., Mekawi, Y., Hinrichs, R., Carter, S., ... & Kaslow, N. J. (2022). Primary Care-Based Mindfulness Intervention for PTSD and Depression Symptoms among Black Adults: A Pilot Feasibility and Acceptability Randomized Controlled Trial. Psychological Trauma: theory, research, practice and policy, 15(5), 858-867. [CrossRef]
- *Pradhan, B., Mitrev, L., Moaddell, R., & Wainer, I. W. (2018). d-Serine is a potential biomarker for clinical response in treatment of post-traumatic stress disorder using (R, S)-ketamine infusion and TIMBER psychotherapy: a pilot study. Biochimica et Biophysica Acta (BBA)-Proteins and Proteomics, 1866(7), 831-839. [CrossRef]
- Prati, G., & Pietrantoni, L. (2009). Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: A meta-analysis. Journal of Loss and Trauma, 14(5), 364–388. [CrossRef]
- *Reinhardt, K. M., Noggle Taylor, J. J., Johnston, J., Zameer, A., Cheema, S., & Khalsa, S. B. S. (2018). Kripalu Yoga for Military Veterans With PTSD: A Randomized Trial. Journal of clinical psychology, 74(1), 93–108. [CrossRef]
- Riley, K. E., & Park, C. L. (2015). How does yoga reduce stress? A systematic review of mechanisms of change and guide to future inquiry. Health Psychology Review, 9(3), 379–396. [CrossRef]
- *Romaniuk, M., Hampton, S., Brown, K., Fisher, G., Steindl, S. R., Kidd, C., & Kirby, J. N. (2023). Compassionate mind training for ex-service personnel with PTSD and their partners. Clinical Psychology & Psychotherapy, 30(3), 643–658. [CrossRef]
- Rowe-Johnson, M. K., Browning, B., & Scott, B. (2024). Effects of acceptance and commitment therapy on trauma-related symptoms: A systematic review and meta-analysis. Psychological Trauma: Theory, Research, Practice, and Policy;17(3):668-675. [CrossRef]
- Rose, K. (2016). Yoga, meditation, and mysticism: Contemplative universals and meditative landmarks. Bloomsbury Publishing. [CrossRef]
- Ross, C. B., & Rocha Beardall, T. (2022). Promoting Empathy and Reducing Hopelessness Using Contemplative Practices. Teaching Sociology, 50(3), 256-268. [CrossRef]
- Salzberg, S. (2011). Mindfulness and Loving-Kindness. Contemporary Buddhism, 12(1), 177–182. [CrossRef]
- Scafuto, F., Ghiroldi, S., Montecucco, N. F., De Vincenzo, F., Quinto, R. M., Presaghi, F., & Iani, L. (2024). Promoting well-being in early adolescents through mindfulness: A cluster randomized controlled trial. Journal of adolescence, 96(1), 57–69. [CrossRef]
- Scafuto, F., Ghiroldi, S., Montecucco, N. F., Presaghi, F., & Iani, L. (2022). The Mindfulness-Based Gaia Program Reduces Internalizing Problems in High-School Adolescents: A Cluster Randomized Controlled Trial. Mindfulness, 13(7), 1804–1815. [CrossRef]
- Schmalzl, L., Crane-Godreau, M. A., & Payne, P. (2014). Movement-based embodied contemplative practices: Definitions and paradigms. Frontiers in Human Neuroscience, 8, 205. [CrossRef]
- *Schuurmans, A. A. T., Nijhof, K. S., Scholte, R., Popma, A., & Otten, R. (2021). Effectiveness of game-based meditation therapy on neurobiological stress systems in adolescents with posttraumatic symptoms: a randomized controlled trial. Stress, 24(6), 1042–1049. [CrossRef]
- Shannahoff-Khalsa, D. (2008). Kundalini Yoga meditation techniques in the treatment of obsessive compulsive and OC spectrum disorders. In A.R., Roberts (Ed.), Social Workers’ Desk Reference, second edition, pp. 606–612. Oxford University Press. [CrossRef]
- *Somohano, V. C., & Bowen, S. (2022). Trauma-integrated mindfulness-based relapse prevention for women with comorbid post-traumatic stress disorder and substance use disorder: a cluster randomized controlled feasibility and acceptability trial. Journal of Integrative and Complementary Medicine, 28(9), 729-738. [CrossRef]
- *Somohano, V. C., Kaplan, J., Newman, A. G., O’Neil, M., & Lovejoy, T. (2022). Formal mindfulness practice predicts reductions in PTSD symptom severity following a mindfulness-based intervention for women with co-occurring PTSD and substance use disorder. Addiction Science & Clinical Practice, 17(1), 51. [CrossRef]
- *Staples, J. K., Gordon, J. S., Hamilton, M., & Uddo, M. (2022). Mind-body skills groups for treatment of war-traumatized veterans: A randomized controlled study. Psychological Trauma: Theory, Research, Practice and Policy, 14(6), 1016–1025. [CrossRef]
- Sparby, T., & Sacchet, M. D. (2022). Defining meditation: foundations for an activity-based phenomenological classification system. Frontiers in Psychology, 12, 795077. [CrossRef]
- Taylor, V. A., Grant, J., Daneault, V., Scavone, G., Breton, E., Roffe-Vidal, S., Courtemanche, J., Lavarenne, A. S., & Beauregard, M. (2011). Impact of mindfulness on the neural responses to emotional pictures in experienced and beginner meditators. NeuroImage, 57(4), 1524–1533. [CrossRef]
- *Tibbitts, D. C., Aicher, S. A., Sugg, J., Handloser, K., Eisman, L., Booth, L. D., & Bradley, R. D. (2021). Program evaluation of trauma-informed yoga for vulnerable populations. Evaluation and Program Planning, 88, 101946. [CrossRef]
- Van der Kolk, B. A., Stone, L., West, J., Rhodes, A., Emerson, D., Suvak, M., & Spinazzola, J. (2014). Yoga as an adjunctive treatment for posttraumatic stress disorder: A randomized controlled trial. The Journal of Clinical Psychiatry, 75(6), e559-565. [CrossRef]
- Van Gordon, W., Sapthiang, S., & Shonin, E. (2022). Contemplative psychology: History, key assumptions, and future directions. Perspectives on Psychological Science, 17(1), 99-107. [CrossRef]
- Vujanovic, A. A., Smith, L. J., Green, C., Lane, S. D., & Schmitz, J. M. (2020). Mindfulness as a predictor of cognitive-behavioral therapy outcomes in inner-city adults with posttraumatic stress and substance dependence. Addictive Behaviors, 104, 106283. [CrossRef]
- Warren, S., & Chappell Deckert, J. (2020). Contemplative Practices for Self-Care in the Social Work Classroom. Social work, 65(1), 11–20. [CrossRef]
- Watts B.V, Schnurr P.P, Mayo L., Young-Xu Y., Weeks W.B, Friedman M.J. (2013). Meta-analysis of the efficacy of treatments for posttraumatic stress disorder. J Clin Psychiatry, 74(6):e541-50. [CrossRef]
- *Yi, L., Lian, Y., Ma, N., & Duan, N. (2022). A randomized controlled trial of the influence of yoga for women with symptoms of post-traumatic stress disorder. Journal of Translational Medicine, 20(1), 162. [CrossRef]
- *Zaccari, B., Callahan, M. L., Storzbach, D., McFarlane, N., Hudson, R., & Loftis, J. M. (2020). Yoga for veterans with PTSD: Cognitive functioning, mental health, and salivary cortisol. Psychological Trauma: Theory, Research, Practice, and Policy, 12(8), 913–917. [CrossRef]
- *Zalta, A. K., Pinkerton, L. M., Valdespino-Hayden, Z., Smith, D. L., Burgess, H. J., Held, P., Boley, R. A., Karnik, N. S., & Pollack, M. H. (2020). Examining Insomnia During Intensive Treatment for Veterans with Posttraumatic Stress Disorder: Does it Improve and Does it Predict Treatment Outcomes?. Journal of Traumatic Stress, 33(4), 521–527. [CrossRef]

Table 1.
Studies’ Characteristics.
| N | Authors | Study Design | Sample Size | Type of Trauma | Type of Contemplative Practices | Duration | Measures | Outcomes |
|---|---|---|---|---|---|---|---|---|
| 1 | Oren-Schwarz, 2023 | RCT with active control | 158 Eritrean asylum-seekers (55.7% female); Mage= 31,8 (SD= 5.2) residing in high-risk urban setting in the Middle East |
Forced Displacement | Mindfulness-Compassion Based Trauma Recovery for Refugees program (MBTR-R) | 9-weekly sessions (2.5 hr for each) | HTQ; PHQ-9; SSGS; PMLD | MBTR-R, relative to waitlist control →shame (no guilt) at post-test → PTSD symptom severity (HTQ subscale) / Depression (PHQ-9) at post-test |
| 2 | Powers et al., 2023 | RCT with active control and 1-month follow-up | 42 Black adults (85% women); Age from 18 to 65; screened positive for PTSD and depression, 57,1% (55.5% of MBCT, 87.5% of WLC) |
PTSD and chronic trauma exposure to multiple events |
Adapted mindfulness-based cognitive therapy (MBCT) group for trauma exposed Black adults |
8-weekly sessions (1,5 hr for each) | TEI; PHQ-9; CAPS-5; MINI for screening; CSQ-8; PBPT | Good feasibility (75% completers) Good Acceptability: high levels of satisfaction (CSQ-8) and several perceived benefits regarding physical, emotional state and interpersonal relationships; The most frequently reported barriers (PBPT): participation restrictions, stigma, lack of motivation, no availability of services, emotional concerns, misfit of therapy to needs, time constraints, and negative evaluation. |
| 3 | Killeen et al., 2023 | RCT with active control Integrative Coping Skills (ICS) | 90 Women (53,3% non-completers); Age from 18 to 65 |
PTSD-Substance Use Disorder (SUD) | Trauma adapted mindfulness-based relapse prevention (TA-MBRP) | 8 weekly sessions | Rate of Retention in the treatment; PSS; FFMQ; MINI; CAPS-5; TLFB; DERS | 48 women met the definition of non-completers (attending < 75% sessions); ↓ Lowest rate of completion among unemployed women in the ICS control group, with low FFMQ; ↑ Higher rate of completion in women in TA-MBRP group with low PSS and high FFMQ; ↓ Both the TA-MBRP and ICS groups had low probability of completion for those with high-PSS scores. |
| 4 | Aizik-Reebs et al., 2022 | RCT with waitlist and 5 weeks follow-up | 158 Eritrean asylum-seekers (46% female); Mage=31.8 (SD=5.2); in an urban post displacement setting. |
Traumatized and chronically stressed; Forced Displacement |
Mindfulness-Based Trauma Recovery for Refugees Program (MBTR-R) |
9-weekly sessions (2.5 hr for each) | HTQ; PHQ-9; SRET | ↓Posttest change in self-criticism (endorsement and drift rate) ↔Posttest change in drift rates to self-compassion stimuli ↑ Posttest increase in self-compassion (endorsement) Type of treatment (MBTR-R; Waitlist) →change of self-criticism (at post-test) → PTSD symptoms (HTQ) and depression (PHQ-9); Type of treatment (MBTR-R; Waitlist) →change of self-compassion (at post-test) → PTSD symptoms (HTQ), but not depression (PHQ-9) |
| 5 | Yi. et al., 2022 | RCT with active controlk | 94 women; Mage= 40.8 (SD= 13,2), Most drivers with almost two months since MVA |
PTSD from Motor vehicle Accident (MVA) | Kripalu Yoga | 6 sessions (45 min for each) for 12 weeks | IES-R; DASS-21 | ↓IES-R at post-test ↓Subscales Intrusion and Avoidance ↔Subscale Hyperarousal ↔IES-R at 3-month follow-up ↓DASS-21 at post-test and 3-month follow-up and Tot score˂Control ↓Subscales Depression and Anxiety ↔Subscale Stress |
| 6 | Kang, Sponheim & Lim, 2022 | RCT with active control (Present-centered group therapy) | 98 veterans with PTSD symptoms (PCL) (14,3% women); Mage= 58.6 (SD= 10.4) |
PTSD from combat | Mindfulness Based Stress Reduction (MBSR) | 8 weekly sessions | PCL-5; CAPS; PHQ-9; PHQ-15 EEG recorded with BioSemi Active Two EEG system in resting-meditation-resting procedure ECG Flanker cognitive task (as attentional task) Spectral power of theta and alpha frequency oscillations of the spontaneous EEG and the TF; HEBR |
↓ PCL-5 ↑ spontaneous alpha power (8–13 Hz) in the posterior electrode cluster but ↔ in the follow-up analysis ↑task-related frontal theta power (4–7 Hz in 140–220 ms after stimulus) ↑ frontal theta heartbeat-evoked brain responses (HEBR) (3–5 Hz and 265–336 ms after R peak). ↓ CAPS ↓ PHQ Type of treatment (MBSR, Control)→ frontal theta heartbeat evoked brain responses→ PCL-5 |
| 7 | Somohano & Bowen, 2022 | Single cluster-randomized repeated measures design | 83 women with PTSD symptoms and substance abuse disorder (SUD) (30% ethnic minority); Mage= 36.1 (SD= 7.9) |
PTSD-SUD | Mindfulness, trauma-focused and gender responsive Program (Ti-MBRP) |
4 weekly sessions (one hr for each) | For PTSD symptom severity in primary care settings: BSSS; PACS; Acceptability: homework compliance and course satisfaction; self-reported duration of formal practices and frequency of informal practices Feasibility: recruitment, enrolment, and retention. Satisfaction: OCSS |
↓Craving (PACS) and PTSD symptoms (BSSS) in both conditions over the 12-month follow-up period and effect sizes similar to other PTSD-SUD interventions ↑Larger effect of Craving and PTSD in both programs after 1-month ↓MBRP had lower BSSS at post-test and 1-month follow-up in comparison with TI-MBRP; TI-MBRP acceptability: homework practice was as expected (in both conditions), retention was below the target but 60%; attrition was higher (64%) at post-test and 1-month follow-up in Ti-MBRP than in MBRP. High satisfaction (OCSS). |
| 8 | Somohano et al., 2022 | Pilot RCT with follow-up | 23 women; Mage= 36.1 (SD= 7.9); most users of methamphetamines, with PTSD symptoms and substance abuse disorder (SUD) |
PTSD-SUD | Mindfulness- based relapse prevention (MBRP) program |
8 sessions (one hour for each) in a 4-week period | PCL-5; PACS; self-reported minutes of daily meditation practice, and self-reported frequency of daily engagement in mindfulness skills to everyday activities | Higher duration (i.e., minutes per practice) of formal mindfulness practice → lower PTSD Symptoms (avoidance, arousal, reactivity, negative cognitions and mood in PCL-5) at 6-month follow-up; ↔Informal practice did not predict any outcomes. ↔Formal and informal practice did not predict reduction in intrusion symptoms (PCL-5) and craving at 6-month follow-up. |
| 9 | Gibert et al., 2022 | RCT with active control | 34 people (Dive Group=17); (32,4% women); Mage= 36 (SD= 6,9) |
PTSD from Paris terroristic attack of 2015 | Scuba diving with mindfulness exercises (the Bathysmed protocol) | 6 days with 10 dives | PCL-5; FMI | ↔PCL-5 at post-test but: ↓Subscale Intrusion symptoms (PCL-5) at post-test and 1-month follow-up; ↑ Mindfulness (FMI) at Post-test; Large effect size Cohen’s d at 1-month follow-up; ↔ PCL-5 and FMI at 3-month follow-up |
| 10 | Possemato et al., 2022 | RCT with active control and follow-up | 55 primary care veterans | PTSD from Combat | Primary Care Brief Mindfulness Training (PCBMT) | 4 weeks | PCL-5; PHQ-9; Health responsibility; Stress management; Not feeling dominated by symptoms | ↓ PTSD symptoms at post-test ↓Depression at 16-24 months follow-up ↑Health responsibility ↑Stress Management, not feeling dominated by symptoms. |
| 11 | Classen et al., 2020 | RCT with waitlist and follow-up | 32 women; Mage =43.5(SD= 10) Eligible if they had previous group experience |
Childhood trauma, complex PTSD symptoms. | Trauma and the Body Group (TBG) | 20-session program (hr for each): | CTQ-SF; LSCL-R; SBC; BAI; SRS; PCL-5; SDQ-20); DES; BDI-II; PHLMS; IIP-32 | ↑Body awareness subscale (SBC) ↔ Body dissociation subscale (SBC) ↓ Anxiety (BAI) ↑Soothing receptivity (SRS) ↔ PCL-5; SDQ-20; DES; PHLMS; IIP-32 ↓ BDI-II |
| 12 | Gallegos et al., 2020 | RCT with active control and follow-up | 29 women (65% in MBSR group); Mage 42.7 (SD=13.1); 50% Black, most unemployed and applying for order of protection |
Intimate Partner Violence (IPV) Survivors | MBSR | 8 weekly sessions | IPVE; LEC-5; PCL-5; DERS; UFOV; RMSSD between normal heartbeats during a 5-min rest period and a sub-sequent trauma imagery task | No statistical power to test between-group differences; Time effects in MBSR group: Improvement but ↔ divided and selective attention (UFOV) ↔ HRV by RMSSD but increase ↓DERS ↓PCL-5 at post-test and follow-up. Decrease for 50% of the total of participants. |
| 13 | Nguyen-Feng et al., 2020 | RCT | 64 women | PTSD and childhood interpersonal trauma histories |
Trauma Center Trauma-Sensitive Yoga (TCTSY) |
1 hr weekly for 10 weeks |
SLESQ; CAPS; DTS; BDI-II; DES; IASC | TCTSY was most efficacious for those with fewer adult-onset interpersonal traumas. Within this subgroup, TCTSY was more effective in reducing PTSD than the active control condition. clinician-rated PTSD, selfreported PTSD, and emotional control problems, although effects were relatively small to moderate. The efficacy of the intervention conditions was less predictable among those with a history of greater adult-onset interpersonal trauma. |
| 14 | Davis et al., 2020 | RCT with 7 months follow-up | 209 participants (91.4% veterans; 66% male; 61.7% White) who met diagnostic criteria for PTSD Mage= 50.6 (SD= 12.9) |
PTSD (59,3% Combat-related index trauma) | Holistic Yoga Program (HYP); Wellness Lifestyle Program (WLP) | 16 weekly interventions | CAPS-5; PCL-5; | ↓PCL-5; CAPS-5 |
| 15 | Fortuna et al., 2020 | RCT with active control and follow-up |
341 Ispanic migrants (24% US and 76% Spain) (172 assigned to IIDEA); Age from 18 to 70 |
Dual diagnosis of Substance abuse, depression, anxiety, and chronic stress | IIDEA (Intervention for dual problems and early action) (CBT + Mindfulness). | Training of clinicians (Two days) who conducted 10-session IIDEA trial (1 hour weekly sessions) | Qualitative report on what was useful of the intervention (content analysis); WAI-SR; IMR; MAAS; ASI; Lite and urine test results; HSCL-20; GAD-7; PCL-10; PHQ-9 | Intermediary variables: ↑WAI-SR (alliance), MAAS and IMR (from a medium to small effect size) also at 6-month follow-up; Outcomes: ↓ Urine test and substance use ASI; PCL-10; GAD; PHQ-9; HSCL-20 (results shown in Alegria et al., 2019). Qualitative results: participants found more useful being listened without judgement, learning relaxation and emotional regulation techniques, gaining a sense of self-control, and managing the double diagnosis. |
| 16 | Lang et al., 2019 | Pilot RCT | 28 Veterans; Mage=49.6 (SD=16.2) |
PTSD from Combat | Cognitively-based Compassion Training (CBCT). | 10 weekly sessions (1 hr for each) | CAPS-5; PCL-5; PHQ-9; BSI-18; STAXI-2; Sleep-Related Disturbance Measures from NIH PROMIS; AUDIT-C; SCS-R; SCS; PHLMS; TEQ; RTSQ; DES’ |
↑ Social connectedness (SCS-R) ↓PCL-5, PHQ-9, CAPS-5 (subscale Hyperarousal), large effect size in hyperarousal, reexperiencing, negative alterations in cognitions Medium effect size in empathy, mindful awareness, anxiety, rumination Large effect size in depression ↔ Differential Emotion Scale (DES): Positive and Negative Emotions ↔Alcool Consumption and all the other variables |
| 17 | Cox et al., 2019 | Pilot RCT with follow-up | 80 allocated to mobile/telephone mindfulness (77,5%) or education (22,5%); 56,2% men; Mage= 49.5; admitted for a surgical or trauma diagnosis (69%) |
Post discharge of critical illness | Mobile and telephone mindfulness program (awareness of breathing; body systems; emotion and mindful acceptance, and awareness of sound) |
4 weekly sessions (hr for each) | System Usability Scale; CSQ; Rate of completion of the program; PTSS; GAD-7; PHQ-9; CAMS-R; Brief COPE; qualitative data: Report and rate the severity of perceived stressors, open-ended feedback on the app group | Higher drop-out and less CSQ in Mobile program ↓Similar decrease between Mobile and Telephone Mindfulness in PHQ-9, GAD-7; PTSS at 3 months follow-up; ↓Education program had a similar impact of Mindfulness Program on PTSS but less impact than others on PHQ-9 and GAD-7 at 3-months follow-up; ↔CAMS-R and Brief-COPE |
| 18 | Miller et al., 2019 | RCT with active control and follow-up | 35 adolescents; Mage= 12.9 (SD= 1,8); (37% female) 32 parents; Mage= 44.7 (SD= 9,8); (80% female) |
40% reported clinical levels of PTSD symptoms, related but not specific to COVID-19 Pandemic | Mentoring + mindfulness program (Learning to Breathe, L2B) | 4 mindfulness sessions (30 minutes each) in 12 weeks | Internalizing subscale of BPM; Child PTSD Symptom Scale on distressing events; PROMIS Sleep-Related Disturbance—SF, PROMIS Pediatric Physical Activity-SF; (REDS); (BRIEF), DERS-SF; FFMQ-SF | ↓ Child PTSD symptoms ↓Emotional impulsivity (DERS-SF) ↓Difficult in engaging in goal-directed behavior (DERS-SF) ↔Remaining variables |
| 19 | Jasbi et al., 2018 | RCT with active control (Citalopram + social meetings) | 48 male veterans; Mage=53 (SD=2,5) |
PTSD from combat | Mindfulness-based cognitive therapy (MBCT) + Citalopram | 8 weekly sessions (60-70 minutes each) | PCL-5; DASS | ↓ PCL-5 (Re-experiencing the events, Avoidance, Negative mood and cognition, Hyperarousal) ↓ DASS (Depression, Anxiety, Stress) |
| 20 | Pradhan et al., 2018 | Pilot RCT with active control and follow-up | 20 subjects (60% female) with PTDS resistant to treatment as usual Age 30-60 |
Mostly physical sexual and emotional abuse | TIMBER (trauma Interventions using Mindfulness Based Extinction and Reconsolidation) combined with a single sub-anesthetic dose of ketamine. | 12 sessions (9 after the relapse of Ketamine or placebo) weekly 1 hr | PCL; CAPS; Ham-D; BAI; MoCA | ↑Duration of response in TIMBER-K (compared to TIMBER-Placebo): in average 34 days with no or minimal PTSD symptoms (PCL, CAPS) (twice longer than the remission with Mindfulness Therapy alone and 5-fold longer than Ket therapy alone); ↓PCL and CAPS at the relapse were lower than the pre-test; ↔the average DSR (Serine) Plasma Concentration was lower than basal DSR (but not significant) ↔Positive correlation but not significant between DSR and PTSD severity |
| 21 | Romaniuk et al., 2023 |
Uncontrolled Clinical Trial with 3-month follow-up | 12 couples (50% male); Mage= 61.90 (SD= 11.09) for the males Mage=61.33 (SD= 8.65) for the females; Ex-service personnel of Defence Force with PTSD and their female partners. |
PTSD from combat | Compassioned Mind Training (CMT) compared to Compassion Focused Therapy (CFT) based on psychoeducational skills. | 12 biweekly group sessions 2 hr each) | FCS, FSCRS, OAS, SSPS, Depressive experiences questionnaire—Self-criticism subscale, PCL-5, DASS-21, Q-LES-Q-SF, RAS, Post-program feedback questionnaire. | ↓ fear of compassion (FCS) towards others and self from pre-test to follow-up ↓ feelings of self-inadequacy (FSCRS) from pre-test to follow-up ↓ levels of external shame (OAS) at follow-up ↓ PCL-5 in the ex-service personnel ↓ Anxiety (DASS-21) at follow-up. ↓ Stress (DASS-21) at follow-up. ↔ PCL-5 in the partner group ↔ Depression (DASS-21) ↑ social safeness (SSPS) at follow-up ↑ Quality of life and satisfaction (Q-LES-Q-SF) at post-test but not at follow-up ↑ Relationship satisfaction (RAS) at post-test but not at follow-up |
| 22 | Leach & Lorenzon, 2023 | RCT with active control (facilitated group support) and two month-follow-up | 42 women; Mage 47.8 (SD= 12.3); Most unemployed/retired (57.1%) and had experienced domestic violence more than 12 months ago (64.3%). |
Traumatic experience of domestic violence | Transcendental Meditation (TM) technique | 9 individual and group sessions (1–2 hr each): tot 12 h in 8 weeks | AQoL8D, DASS-21, PCL-5, subjective experience was assessed through open-ended questions in the data collection form and trial exit form. | ↓ DASS-21 depression, anxiety and stress severity scores ↓ PCL-5 Total Symptom Severity Score ↑ AQoL-8D utility score, superdomain scores and domain scores (except for pain and senses domain scores) ADVERSE EFFECTS Twelve mild adverse events reported by six participants (i.e. nausea, headache, irritability, weight gain). Two participants self-reported a severe adverse event that they believed was related to the intervention (i.e. cold-sore, body feeling heavy). |
| 23 | Javidi et al., 2023 | RCT with active control, Cognitive Therapy and Behavioral therapy (BT) | 82 participants with a diagnosis of depressive disorder or PTSD; Mage= 40.3 years (SD= 12.0); The dominant level of education was secondary school (45.2%), while 35.5% were students and 30.6% employed |
PTSD for non specified traumatic experiences | Self-Compassion Therapy combined with Behavioural Therapy (BT) | 12 session program of individualised CBT-based treatment for depressive disorders and PTSD | SCS, K10, PHQ9; PCL-C; WSAS. | ↑ SCS ↓ K10 ↓ PHQ9 ↓ PCL-C ↓ WSAS |
| 24 | Knabb et al., 2022 |
RCT with control group (Loving Kindness Meditation) | 26 participants belonging to Christian religion; Mage= 42,8 (SD=12,80 ); | Exposure to crime related events, physical and sexual experiences and general disasters | Christian Meditative Intervention (Lectio Divina) | 2 weeks | Christian Contentment Scale; Christian Gratitude Scale; Positive and Negative Affect Schedule; Trauma Symptom Checlist-40 | ↓ PTSD symptoms ↔ Positive affect (small effect size) ↔ Christian contentment ↔ Christian gratitude ↔ Anxiety, depression, stress (medium effect size) |
| 25 | Fishbein et al., 2022 |
RCT with active control (MEUC, Minimally enhanced usual care) | 134 (88% female); Mage= 56.24 (SD=11.58). |
Cancer survivors | Acceptance and Commitment Therapy (ACT) | 10 sessions | Mediators: SCS; BEAQ; BEVS; VLQ; EAC. Outcomes: HADS; IES-R; CARS. |
↓ Bull’s eye Values BEVS (improvement) ↔VLQ ACT →SCS, EAC→IES-R ACT→SCS, EAC, BEVS→ CARS and General Anxiety HADS-A (marginal mediation) ↑SCS ↑ EAC |
| 26 | Bellehsen et al., 2022 |
RCT with active control (Treatment as Usual) and 3-month follow-up | 40 veterans (85% male); Mage=51.6 (SD= 11.4); Non caucasian (42.5%). |
PTSD from Combat (60%), sexual trauma (15%)Life-threatening illness/serious injury (15%), other (5%) | Transcendental Meditation (TM) | 16 sessions over 12 weeks (1 hr each). |
CAPS-5; PCL-5; BDI-II; BAI; S-Anger subscale of STAXI-2; Q-LES-Q-SF; ISI. | ↓PCL-5; BDI-II; BAI; ISI; ↓50% TM group reduced CAPS-5 and 50.0% no longer met the criteria for a PTSD diagnosis after 3 months ↔S-anger ↔Q-LES/ Q-SF |
| 27 | Gerdes et al., 2022 |
Uncontrolled Clinical Trial | 56 veterans (92.9% male); Mage= 52.1 (SD= 12.9). |
PTSD from Physical injury on deployment (48.2%) and from combat (32.1%) | Listening to the compassion meditation (LKM-S) | 1 session audio-taped (1.5 h) |
HR and HRV from ECG; SCL; ERQ; PCL-5; PHQ-9; VAS. |
↓ self-reported hyperarousal state ↓ SCL, meaning a reduction in sympathetic arousal ↔HRV response was not different from 0, meaning that did not increase parasympathetic activation (no as expected an increase) ↔ Social Connectedness State self-compassion at both pre and post time points were associated with PCL-5, trait self-compassion (SCS) and emotion suppression (ERQ) ↑HR response (physiological arousal) (not as expected a decrease) ↑HR response to directing compassion towards the self ↑ self-compassion state at the end of LKM |
| 28 | Hodgdon et al., 2022 |
Uncontrolled Pilot Clinical Trial with 1 month follow-up | 17 participants (76% women); Mage=46; range 28-58 76% exposed to two types of trauma prior to the age of 18; and current diagnosis of PTSD on the CAPS and clinical depression. |
PTSD from Multiple Childhood Trauma with sexual (65%), psychological (65%) and physical (59%) abuse |
Internal Family System therapy (IFS) | 16 individual sessions (1,5 hr) | DTS; CAPS; BDI; SIDES-SR; SCS; MAIA. | ↓CAPS at post-test and 1-month follow-up At 1-month follow up, 92% of participants no longer met criteria for PTSD ↓DTS at post-test and 1-month follow-up ↓ BDI at post-test and 1-month follow-up ↓SIDES total score at the 1-month follow up ↔Somatization ↔SCS ↑ Large effect size on Trusting and medium effect sizes on Attention Regulation, Self-Regulation and Body Listening ↑Not-Distracting subscale of MAIA just at 1-month follow-up ↔ No significant time effect for other subscales of MAIA |
| 29 | Staples et al., 2022 |
RCT with active control (standard treatment) and 2-month follow-up | 108 veterans (96% male); Mage 55.97 (SD=11,7). |
PTSD from combat; | MBSG (mind-body skills group) | 10 weeks | PCL- M; STAXI-2; PSQI; PHQ-9. |
↓ Hyperarousal and avoidance ↓ PTSD symptoms ↓ Anger and sleep disturbance ↔ Depression, anxiety, post traumatic growth and health related quality of life |
| 30 | Tibbitts et al., 2021 |
Retrospective pre-post approach | 152 students (59% woman), community of colour (44 %); 73% ≥ 21 years; 51% attended trauma-informed yoga classes in the corrections and reentry sector, 21% in the substance use treatment and recovery, 28% in community and mental health sectors. |
Not revealed | Trauma-informed yoga | From 2 to 10 Yoga Classes | Survey instrument: Not standardized questionnaire developed ad hoc informed by the framework of self-regulation to evaluate: self-regulation, perceived emotional and physical wellbeing. | ↓Reported decreased feeling pain or negative emotional states ↑Use of self-regulation skills was uniformly higher. ↑Reported increased awareness of physical sensations (e.g. breathing and muscle movement) ↑Students in the corrections and reentry sector had the largest benefit after beginning yoga. Adverse effects: For negative emotional states, only few students reported feeling upset, anxious, or stressed after class. Fewer respondents from substance use treatment retrospectively reported feeling upset and anxious or stressed before yoga class. This group showed the least amount of change in self-regulation skills |
| 31 | Grupe et al., 2021 |
RCT with 5 month follow-up | 30 police officers; Mage= 38,4 (SD= 7,7). |
Occupational stress | Mindfulness Based Stress Reduction (MBSR) | 8 sessions in 8 weeks |
PSQ; OLBI with separate subscales for exhaustion and disengagement; PSQI; PCL-C); PROMIS; WLQ-8); PWB; PANAS; Creactive protein, diastolic/systolic blood pressure, resting pulse rate, skin conductance; Breath Count task. | ↓PSQ Operational stress and moderated by gender and years of police experience: younger men showed greater decline in stress also at follow-up; ↓ PCL at post-test and at 5-month follow-up; ↓ Exhaustion subscale of OLBI ↓PROMIS anxiety symptoms and depression symptoms; ↓PANAS Negative affect; ↔PROMIS subscales of pain interference; pain intensity, or physical functioning ↔ Disengagement subscale of OLBI ↔PANAS positive affect; ↔ Physical parameters ↑ Sleep quality PSQI ↑PWB; |
| 32 | Kananian et al., 2020 |
RCT with waitlist and 12-weeks and 1-year follow-up | 24 male; Mage= 22.1 (SD=3.6); refugees diagnosed with DSM-5 PTSD, major depressive disorder, and anxiety disorder; with elementary school degree. |
Multiple trauma pre-post displacement | Culturally adapted cognitive behavioral therapy (CA-CBT) | 12 sessions in 6 weeks (1.30 hr for each) | GHQ-28; PCL-5; PHQ-9; SSS-8; WHOQOL-BREF; ERS. | ↓ PHQ-9; SSS-8; ↔PCL-5 ↑WHOQOL-BREF ↑ERS ↑GHQ-28 at both follow-up; At 1-year follow-up main effects were maintained |
| 33 | Schuurmans et al., 2021 |
RCT versus TAU | 77 adolescents (59.7% male); Mage= 15.25 (SD = 1.79). |
PTSD from non-intentional multiple traumatic events (e.g. neglect, domestic violence, emotional abuse, interpersonal traumatic events) | MUSE (game-based meditation intervention) | 6 weeks: 2 times a week for 15-20 minutes | Basal ANS activity using ECG and ICG by VU-AMS. Basal HPA axis activity using hC levels pg/mg hair. TRIER-C combined with SSST. |
↓ Basal activity of SNS (Sympathetic Nervous System) ↔ Reactivity of SNS and PNS (Parasympathetic Nervous System) to acute stress ↑ HPA (Hypothalamic-Pituitary-Adrenal Axis) reactivity to acute stress |
| 34 | Chopin et al., 2020 |
RCT versus control | 87 (61% male); Mage 51.41 (SD 11.32); 69 % African Americans; 49 completers (56,3%). |
PTSD with comorbid chronic pain | Hatha Yoga | 10 cohorts (2 to 8 weeks): 90 minutes for each class | PCL-5; PROMIS; Client Satisfaction Questionnaire-8; TSK-11. | ↓ PTSD symptoms, kinesiophobia, depression and anxiety Follow-up results: ↔ Intrusion and avoidance symptoms ↑ Social role functioning PROMIS |
| 35 | Zalta et al., 2020 | RCT with 10 assessments | 165 veterans (64,2% male); Mage= 40.8 (SD= 9.57); most white; most who served After 9/11; most retired; with PTSD. |
Combat (67.9%), military sexual trauma (32.1%) and additional childhood trauma history (61.6%) | Intensive treatment program (ITP) | 3-week: 14 individual sessions of CPT, 13 sessions of group VPT, 13 session group mindfulness adapted from MBSR and 12 sessions of yoga | ISI; PCL-5-18; PHQ-8. | ↓ ISI in just 23.4%; ↓ PCL-5-18; PHQ-8 (already shown in Zalta et al., 2018) ↔ baseline ISI did not predict PCL-5 and PHQ-8 across all time points but larger improvements in ISI was associated with greater improvement in PCL-5 and PHQ |
| 36 | Bandy et al., 2020 |
Uncontrolled Pilot Clinical Study | 116 (61,2% women); Mage= 20.6 (SD= 2.75); South African students in experimental group with PTSD (PCL-C >44); 61 (70,5% women) in the waiting list: 34 participants also met DSM-IV criteria in a clinician’s diagnosis. |
Several among natural disasters, severe accidents, sexual and criminal victimization and combat experiences | Transcendental Meditation (TM) | 4 consecutive days (1.30 hr daily), and weekly follow-up meetings and home practices | PCL-C; Trauma history Questionnaire; BDI. | ↓PCL-C in experimental group after 15, 60 and 105 days of practice. In this point, PCL-C was not symptomatic anymore. ↓BDI at both 60 and 105 days ↓ BDI Depression and PTSD were highly correlated and decreased together through the practice; Regular TM practice predicted ↓PCL-C especially during the first 15 days of practice |
| 37 | Zaccari et al., 2020 |
Uncontrolled Clinical Trial | 27 veterans; final sample (N = 17), 41% endorsed military sexual trauma (85% of women and 10% of men). Of participants who completed postintervention assessment (male n = 10 and female n = 7), 11 attended eight or more classes, four attended five to seven classes, and two attended three classes. |
PTSD from combat | Yoga protocol | 10 weeks | Response Inhibition; PTSD symptoms; depression; sleep disorder; quality of life; neurocognitive complaints. Cognitive functioning, self-report measures of mental health symptoms, and salivary cortisol were measured within two weeks prior to beginning and following completion. |
↑ Life satisfaction ↓ depression, cortisol ↔ cognitive performance |
| 38 | Muller-Engelmann et al., 2019 |
RCT with multiple weekly assessments until 8 weeks follow-up |
14 (78,6% women); Mage=41.14 (SD= 12.30); PTSD patients; 92.9% fulfilled the criteria for comorbid affective or anxiety disorders. |
Interpersonal violence Childhood sexual or physical abuse; Physical violence in adulthood |
Trauma-adapted intervention from loving-kindness meditation and MBSR | 8 individual sessions (1.30 hr for each) | CAPS-5; SCID-I; IPDE; LEC-5; DTS; BSI; BDI-II; WHO-5; FFMQ; SCS; MBE. | ↓CAPS-5 at follow-up (especially on avoidance) (9 out of 12 did not meet PTSD criteria); ↓DTS at post-test and follow-up; ↓BDI-II at follow-up; ↓ self-criticism at follow-up ↔BSI medium effect sizes ↑mindfulness skills of nonjudging and acting with awareness ↑ attention to breath in MBE at follow-up ↑self-compassion at follow-up ↑WHO-5 (75%): half of them at post-test |
| 39 | Ong et al., 2019 |
Collective case study design | 3 women; Age from 26 to 52; PTSD who have left the abusive relationship for at least 6 months. |
Intimate Partner Violence (IPV) | Trauma-sensitive Yoga (TSY) | 8 group sessions in 8 weeks (1 hr for each) | CAPS-5; SUD; pre- and post-TSY scaling question worksheet observations on how they made meaning of their recovery; semistructured interviews. | ↓CAPS-5 (but one for floor effect): reduced number and severity Enhanced physiological, intrapsychic functioning, emotional benefits, enhanced perceptions of self and others, shift in time perspective, interpersonal relationships, self-care, spiritual benefits and positive coping strategies. |
| 40 | Mehling et al., 2018 |
RCT with waitlist and multiple assessment (4,8,12 weeks) | 47 (81% male); Mage =46.8; from 24 to 69 war veterans with PTSD and from racial or ethnic minority (60%). |
PTSD from Combat | Integrative exercise (IE) | 36 sessions in 12 weeks (50 min for each) | FFMQ; MAIA; PSOM; CAPS-5; WHOQOL. | ↓CAPS-5 (average reduction of 31 points) ↑FFMQ Non reactivity, Observing ↑ MAIA Emotional Awareness, Self-Regulation, Body Listening; ↑PSOM total, Focused Attention, Restful Repose PSOM and FFMQ Non-Reactivity → CAPS Hyperarousal subscale/ Psychological WHOQOL (partial mediation) |
| 41 | Goldstein et al., 2018 |
RCT with waitlist and multiple assessment (4,8,12 weeks) | 47 (81% male); Mage= 46.8 (SD= 14.9); war veterans with PTSD, mostly and from racial or ethnic minority (60%). |
PTSD from Combat | Integrative exercise (IE) | 36 sessions in 12 weeks (1 hour for each) | SCID-I; CAPS-5; WHOQOL-BREF; Feasibility and Acceptability Questionnaire; Godin Leisure-Time Exercise Questionnaire. | ↓CAPS-5 Tot. 31 point reduction at post-test ↓Subscale of hyperarousal ↑ LSI (more physical activity) ↑WHOQOL-BREF greater improvement in the psychological domain but a smaller improvement in the physical domain greater number of sessions attended was associated with an improvement in physical quality of life and psychological quality of life High levels of satisfaction |
| 42 | Reinhardt et al., 2018 | RCT with waitlist | 51 (11.8 % female); Mage= 47.76 (SD= 13.77); (out of 74 participants screened). |
PTSD from Combat | Kripalu Yoga Program | 20 sessions in 10 weeks (1.30 hr for each) | PTSD Checklist (PCL-C and M); CAPS-5; IES-R. | CAPS-5 up to moderate PTSD symptoms at post-test in Yoga group but ↔ between differences in CAPS, PCL-M and IES ↓ large effect PCL-M (correlated with PCL-C), self-reported PTSD symptoms were reduced in the yoga group (below the cutoff) while marginally increased in the control group, 51% drop out (higher in the Yoga Group), Self-selectors (from Waitlist) improved more than Randomized Veterans in CAPS and PCL. |
Note: ↑= the variables improved and were statistically significant from baseline or from the control group; ↔= no or no statistically significant difference from baseline or from the control group; ↓=the variables declined and were statistically significant from baseline or from the control group; →=the independent variables significantly predict the outcome variables or the mediators.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



