
Submitted:
12 July 2025
Posted:
15 July 2025
You are already at the latest version
Abstract
Background/Objectives: RSV infection can lead to significant complications, particularly among those with underlying cardiovascular and pulmonary complications. Patients with pulmonary hypertension (PH) are susceptible to clinical deterioration triggered by respiratory infections due to their limited cardiopulmonary reserve. This study aimed to assess the risk of hospitalization in RSV-infected adults with and without PH. Methods: : We conducted a retrospective cohort study using the research network TriNetX to assess the risk of hospitalization in a cohort of patients with RSV infection compared with and without PH. Propensity score matching was performed for demographic variables and RSV risk factors between the two cohorts. Risk of hospitalization was expressed as adjusted odds ratio (aOR) with 95% confidence interval(CI). Results: There were 193,256 patients in the RSV with PH cohort and 2,843,714 in the RSV without PH cohort (all aged >18 years). The mean age of the RSV with PH cohort was 68.2+/-15.3 years, 50.6% were females, 64% were white, and 64.2% were group 2 PH. The RSV with PH cohort was at an increased risk of hospitalization (aOR 1.89, 95% CI 1.87–1.92, p value 0.02). There was a significant risk (aOR 1.29, 95% CI 1.27–1.32) for the 32 composite outcome of hospitalization-related complications between the 2 cohorts. Comorbid conditions (diabetes, cardiovascular disease, chronic lung disease, and chronic kidney disease) increased the risk of hospitalization in the RSV with PH group, with the most effect noted with underlying cardiovascular disease. Similarly, Group 2 PH noted a higher risk of hospitalization compared to the other PH groups. Remarkably, all PH groups noted increased hospitalization risk compared to the RSV without PH cohort. Conclusions: We found that patients > 18 years of age with PH and RSV infection are at an increased risk of hospitalization with subsequently higher RSV infection-related complications. All PH groups noted higher hospitalization risk compared to RSV without PH, likely denoting PH as an independent risk factor for worse RSV infection-related outcomes. RSV vaccination, therefore, may benefit all age groups in patients with PH. Our study also reiterates the current RSV vaccination recommendation for patients with underlying cardiovascular disease.
Keywords:
pulmonary hypertension
; respiratory syncytial virus
; hospitalization risk
; RSV vaccination
; pulmonary hypertension WHO groups
1. Introduction
Pulmonary hypertension (PH) is a chronic, progressive condition characterized by increased pulmonary vascular resistance and remodeling of the pulmonary arteries, ultimately leading to right ventricular failure and premature mortality [1]. Based on the cause and mechanism, World Health Organization-sponsored 2008 Dana Point clinical classification schema (WHO) has divided pulmonary hypertension (PH) into five categories: Group 1, pulmonary arterial hypertension (PAH), comprises Idiopathic, heritable, drug-induced and connective tissue disease-associated forms; group 2 results from left heart disease, including valve problems or heart failure; group 3 consists of lung disorders or hypoxia, such as chronic obstructive pulmonary disease (COPD) or interstitial lung disease (ILD); group 4 includes unresolved clots causing chronic thromboembolic pulmonary hypertension; and lastly, group 5 PH which includes either uncertain or complex etiology [2].
Respiratory syncytial virus (RSV), a negative-sense RNA virus, is a well-established cause of severe lower respiratory tract infections in infants and young children. However, growing evidence underscores its significant disease burden in adults, particularly in older individuals and those with underlying cardiopulmonary comorbidities [3,4]. RSV infection has been associated with high morbidity, including pneumonia, acute exacerbations of chronic lung disease, and cardiovascular complications [5]. It is estimated that RSV leads to $1.2 billion in costs annually to the United States [6]. A systematic review and meta-analysis of RSV burden in adults aged 60 years and older in high-income countries estimated that RSV-associated acute respiratory infections (ARI) led to approximately 5.2 million cases, 470,000 hospitalizations, and 33,000 in-hospital deaths annually [7].
In pulmonary hypertension patients, infections are the leading cause of decompensation, and approximately 7% of the deaths in patients with PH are due to pneumonia [8]. There is also an increasing trend in PH mortality among the older population [9]. Patients with PH face a heightened risk of clinical deterioration triggered by respiratory infections due to their limited cardiopulmonary reserve [10]. Even mild viral infections can induce pulmonary vasoconstriction, exacerbate hypoxia, and precipitate acute decompensations that necessitate hospitalization [8].
Currently, the Centers for Disease Control and Prevention (CDC) recommends a single dose of RSV vaccine for all adults aged 75 years and older and adults ages 60-74 years who are at risk of severe RSV infection. Patients with chronic cardiovascular/lung disease, along with other chronic diseases, are at increased risk of severe RSV infection [11]. Despite these recommendations, patients with PH are not yet explicitly recognized as a high-risk subpopulation for RSV-related hospitalization.
It is unknown if the presence of PH increases the risk of serious RSV infection compared to the rest of the population without PH. Given the significant morbidity and mortality associated with both RSV infection and PH, we aimed to assess if RSV infection increased hospitalization risk in individuals with PH compared to those without PH. Secondary aims of the study were assessment of hospitalization-related complications, hospitalization risk due to various comorbidities and PH group-specific hospitalization risk assessment.
2. Materials and Methods
Study Design
We performed a retrospective cohort study using the TriNetX database (https://trinetx.com). TriNetX is a global collaborative network that provides access to real-time de-identified patient information from electronic medical records, which includes diagnoses, procedures, laboratory values, and genomic information obtained from both inpatient and outpatient settings from approximately 122 million patients from approximately 100 healthcare organizations (HCOs) in the United States. It also includes prescription drug claims. The study collected it’s data on April 7th, 2025.
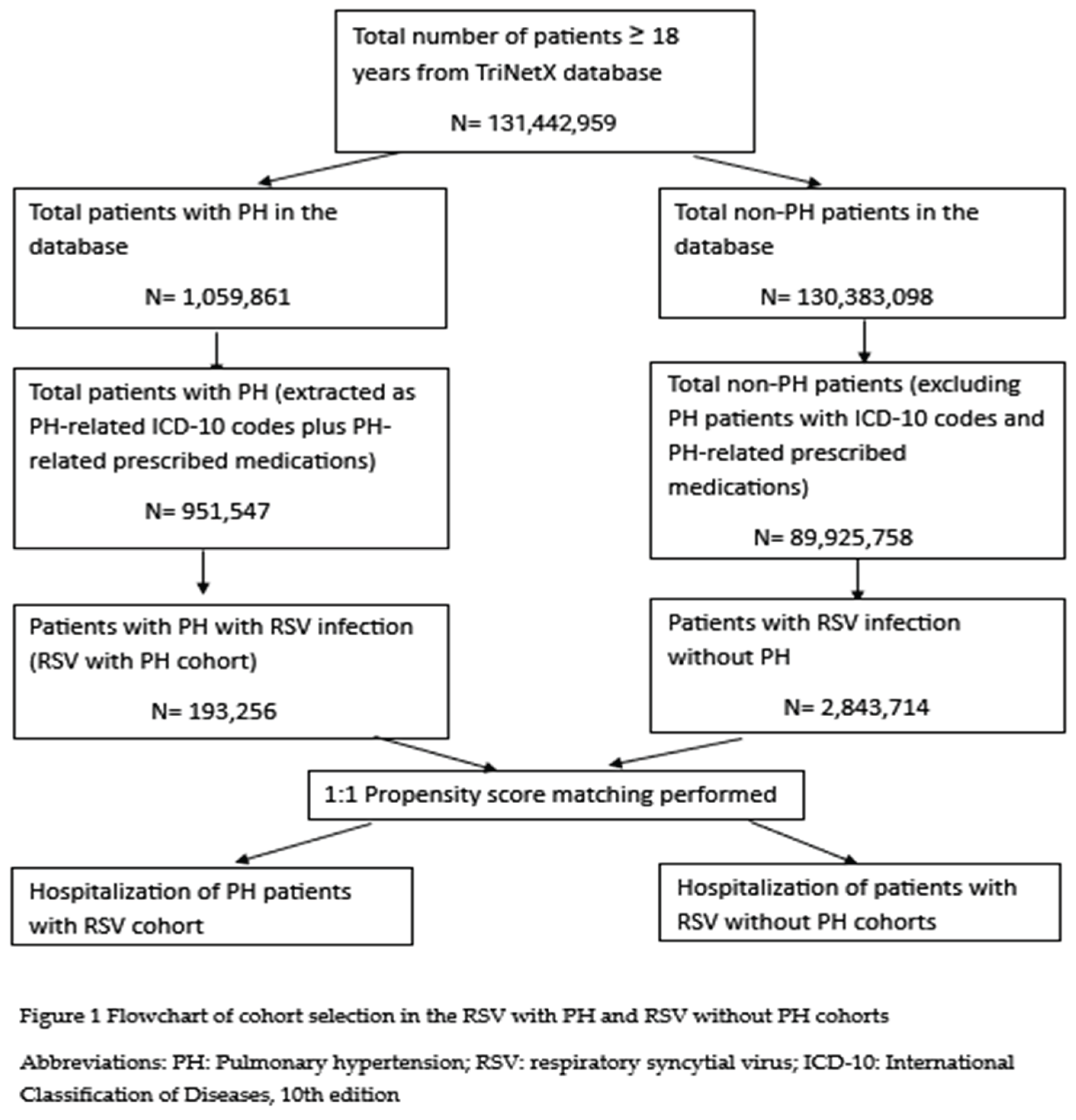
Two cohorts were selected, namely the RSV with PH cohort and the RSV without PH cohort. Both these cohorts included adult patients > 18 years of age. RSV with PH cohort was selected based on International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) codes for primary pulmonary hypertension (I27.0), secondary pulmonary arterial hypertension (I27.21), other secondary pulmonary hypertension (I27.29), pulmonary hypertension due to left heart disease (I27.22), pulmonary hypertension due to lung diseases and hypoxia (I27.23), other pulmonary heart disease (I27), pulmonary heart disease, unspecified (I27.9), chronic thromboembolic pulmonary hypertension (I27.24), pulmonary hypertension, unspecified (I27.20) plus RxNorm/VA:RE codes for ≥1 PH-related medications: ambrisentan, tadalafil, bosentan, macitentan, ambrisentan, riocoguat, sildenafil, Treprostinil, epoprostenol, sotatercept, selexipag, furosemide, torsemide, carvedilol, metoprolol, sacubitril-valsartan, bronchodilators, anticholinergic bronchodilators, sympathomimetic bronchodilators. The PH codes were selected from administrative claims data from multiple studies [12,13,14]. The RSV without PH group excluded all ICD-10-CM codes for PH along with PH-specific medications. Patients with RSV infection were identified using ICD-10-CM codes for RSV (J12.1, B97.4, J21.0, or J20.5) or Logical Observation Identifiers Names and Codes (LOINC) codes for a positive RSV laboratory test [15,16,17,18]. Supplementary table S1 summarizes the codes used for this study. Since this database does not associate hospitalizations with a particular diagnosis, we included hospitalizations within 1 week of RSV diagnosis/positive test to determine RSV-related hospitalizations. This study only included RSV infections that occurred after a PH diagnosis. Figure 1 depicts a flowchart for the study’s patient selection.
The primary aim of the study was to assess the risk of hospitalization in the RSV with PH cohort compared with the RSV without PH cohort. Hospitalization was determined by the Current Procedural Terminology (CPT) code for hospital inpatient services or inpatient acute/non-acute, short stay, inpatient encounter within one week of RSV-positive lab result or an ICD-10-CM code for RSV. The index date for both cohorts was chosen as the date of RSV infection in the database. We performed age-group stratified subgroup analysis (18-49, >50, >60 years) to assess hospitalization risk with PH in these age groups.
Our study’s secondary aims were as follows:
- Assess the risk of hospitalization-related complications, defined as the need for intensive care unit (ICU) care (identified as critical care services, CPT code 1013729), endotracheal intubation (CPT code 31500), vasopressor support into the peripheral vein/central vein (ICD-10 PCS codes 3E033XZ and 3E043XZ, respectively) or mortality (identified as deceased) within the next 30 days from the date of RSV-related hospitalization. We also assessed the risk of hospitalization for the composite outcome associated with these complications.
- Assess the risk of hospitalization in RSV with PH Groups 1-4 compared to the RSV without PH cohort, respectively. Supplementary Table S2 outlines the ICD-10-CM codes used for the PH groups 1-4.
- Assess the risk of hospitalization within the RSV with PH groups. The analysis was performed as individual groups compared with the other PH groups.
- Assess the risk of hospitalization in the RSV with PH cohort with and without the comorbid conditions: Chronic lung disease (CLD) identified with ICD-10-CM codes for asthma, chronic bronchitis, chronic obstructive lung disease, or bronchiectasis; Cardiovascular disease (CVD) identified by ICD-10-CM codes for ischemic heart disease, cerebrovascular accident, or peripheral vascular disease; diabetes mellitus (DM); and chronic kidney disease stage ≥ 3. The respective ICD-10-CM codes are listed in Supplementary table S3.
Statistical Analysis
We conducted our analyses using TriNetX LLC software. Our study included 91 HCOs. The baseline characteristics of the cohorts were presented as mean, standard deviation, and proportions. Propensity score matching was performed to account for potential confounders and ensure cohort comparability. Upon running the propensity score function, patients were matched based on propensity scores to create a 1:1 ratio between cohorts using nearest neighbor (greedy) without replacement. A default caliper of 0.10 SD was used [19]. Demographic data such as age at index event, gender, co-morbid conditions like DM, CVD, CKD, obesity, solid organ transplant status, alcohol, and nicotine dependence were selected and propensity matched as they have been associated with severe RSV infection [20,21,22,23]. P-values were calculated after propensity score matching, with <0.05 depicting statistical significance. Standard mean difference was also calculated, with <0.1 depicting good balance between groups. Outcomes were expressed as adjusted odds ratios (aOR) with 95% confidence intervals (CI).
3. Results
Baseline Characteristics of the Study Sample
Of the 1,059,861 PH patients, 193,256 patients were noted to have RSV infection. There were 2,843,714 patients with RSV without PH. Patients with RSV with PH were predominantly white (64%), older in age (68.2 +/- 15.3 vs. 49.7 +/- 21.4), and had 50.6% females compared to the RSV without PH cohort. The RSV with PH cohort had a
significantly higher number of comorbidities as listed in Table 1. We performed propensity score matching for the demographics and comorbidities between the two groups. All the variables were balanced well between the two cohorts as noted by the p-value (<0.05) and/or mean standard difference (<0.1). Propensity score matching was also performed between the cohorts for connective tissue disorders (systemic lupus erythematosus, rheumatoid arthritis, systemic sclerosis, overlap syndrome) because these disorders can lead to severe RSV infections and are also an etiological factor (approximately 15-25%) for group 1 PH [24,25,26,27].
Hospitalization Risk
There were 131,414 (68%) hospitalizations in the RSV with PH cohort compared to 1,059,066 (37.2%) in the RSV without PH cohort. The RSV with PH cohort noted higher odds of hospitalization risk compared to the RSV without PH cohort after propensity score matching (aOR 1.89, 95% CI of 1.873-1.924, p-value of 0.02). Interestingly, age groups 18-49 years (aOR 3.08, 95% CI of 2.939-3.229, p-value of 0.03), >50 years (aOR 1.808, 95% CI of 1.783-1.834, p-value of 0.015) and >60 years (aOR 1.701, 95% CI of 1.674-1.728, p-value < 0.05) also noted higher risk of hospitalization after propensity score matching for the RSV with and without PH cohorts. Table 2 summarizes the above findings.
Hospitalization-Related Complications
Composite outcomes were noted in 31.3% and 21.6% of RSV patients with and without PH, respectively. Mortality was noted in 8.2% of the RSV with PH cohort. A higher risk of composite outcomes (mortality, ICU care, need for intubation or vasopressor support) was noted in the RSV with PH group compared to the RSV without PH cohort after PSM (aOR 1.29, 95% CI of 1.274-1.321, p-value of <0.0001) within 30 days of hospitalization (Table 3). Similarly, the need for ICU care, intubation, and vasopressor support revealed higher risks (aOR 1.369, 1.375, 1.553 respectively) which were statistically significant. Interestingly, there was less risk of mortality in the RSV with PH cohort, with an aOR 0.920, 95% CI (0.892-0.948), with a p-value <0.0001.
Effect of Comorbid Conditions on Outcomes
RSV with PH cohort was compared with and without certain comorbid conditions, namely, DM, CVD, CKD, and CLD. Data after propensity score matching noted a higher risk of hospitalization in the RSV with PH cohort with DM, CVD, CKD, or CLD compared to the RSV with PH cohort without DM, CVD, CKD, or CLD, respectively, which were all statistically significant (Table 4). Patients with CVD notably had a higher risk of hospitalization relative to the other comorbidities (aOR 5.1, 95% CI 4.78-5.43, p-value < 0.0001).
Hospitalization Risk Among PH Subgroups
We assessed the hospitalization risk among various PH WHO groups. Among the groups 1,2, 3 and 4, group 2 had a statistically significant higher risk of hospitalization compared to the other PH groups (aOR 1.771, 95% CI 1.697-1.848, p-value < 0.0001). Notably, Group 1 and Group 3 had a lesser risk of hospitalization, which was statistically significant (Table 5). Group 4 did note a higher risk of hospitalization, but this was not statistically significant (aOR 1.02, 95% CI 0.781-1.328, p-value 0.892).
Comparison of Hospitalization Risk Among RSV with PH Subgroups vs Non-PH Cohort
PH WHO groups 1, 2, 3, and 4 were compared with the RSV without PH (Table 6). There were 16,505 (8.54%), 124,166 (64.25%), 49,628 (25.67%), 1645 (0.85%) patients in the RSV with PH Groups 1,2,3, and 4, respectively. After PSM, all groups noted higher risks of hospitalization, which were statistically significant.
4. Discussion
RSV is one of the most common causes of viral pneumonia. In some studies, patients admitted with influenza-like illness to the hospital noted an estimated prevalence of RSV at 12.5%, after influenza (18.7%) and rhinovirus/enterovirus (14.7%) [28,29]. PH also has been noted to have significant morbidity and mortality leading to hospitalizations [30]. In our study, we assessed the risk of hospitalization in patients with PH who develop RSV infection and compared it to RSV- infected patients without PH. We found that among adult patients >=18 years old, underlying PH increased their odds of hospital admission by 1.89 (95% CI 1.873 - 1.924, p-value 0.02). To our knowledge, this is the first study assessing the effect of RSV infection on patients with PH.
There are known risk factors for severe RSV infections, which include cardiac disease (congestive heart failure, coronary artery disease), lung disease (asthma, chronic obstructive pulmonary disease), cerebrovascular disease, chronic kidney disease, and diabetes mellitus [31,32]. Immunocompromised patients are at higher risk of acquiring RSV infection. Patients with hematopoietic stem cell transplants, lung transplants, and active chemotherapy demonstrate poorer outcomes [25,33]. Additional indicators of worse outcomes include smoking history, high altitude, leucopenia less than 100 cells/mm3, and history of total body radiation [33]. These conditions were therefore included in our study. We performed propensity score matching of the connective tissue disorders that are known to cause group 1 PH in approximately 15-25% of patients [26,27]. This reduced selection bias between the two cohorts.
Interestingly, our data noted that patients in the age group 18-49 years had the highest risk of hospitalization with an aOR 3.08 (95% CI 2.939-3.229, p-value 0.03). This finding may be crucial, as currently, for patients between 18 and 59 years, the bivalent RSVpreF vaccine has been suggested, but only if the patient is immunocompromised or has chronic lung, heart, or kidney disease, but not necessarily PH [34]. Our RSV with PH population was predominantly older than 50 years of age, similar to other studies [5,35].
Among patients admitted to the hospital with RSV infection, 10 to 30% of patients have been found to require intensive care unit (ICU) admission, with up to 17% requiring mechanical ventilation [36,37]. The rate of ICU admission for RSV (24.3%) has been shown to be higher than even COVID-19 (17.3%) and influenza (16.8%) in a cohort of patients over the age of 60 years admitted with respiratory failure [37]. Our study demonstrated that after propensity score matching, in patients with RSV-related hospitalization, the presence of underlying PH (28.7% vs 22.7%) was associated with increased odds of ICU admission by 1.369 (95% CI 1.343 - 1.395, p-value < 0.0001), intubation/mechanical ventilation by 1.375 (95% CI 1.324 - 1.429, p-value < 0.0001) and vasopressor support by 1.553 (95% CI 1.488 - 1.621, p-value < 0.0001) ) within 30 days of hospitalization in comparison to the RSV without PH cohort. Accordingly, the composite outcome of hospital-related complications was increased with an aOR of 1.369 (95% CI 1.343–1.395, p value<0.0001). Although our study noted a mortality rate of around 7.5% in the RSV with PH cohort, similar to mortality rates due to RSV without PH cohort of around 6-8% (also noted in the study by Colosia et al.), it did not reflect an increased mortality in the former (aOR 0.920 (95% CI 0.892- 0.948, p-value <0.0001) [36]. This possibly could be due to a smaller follow-up period of 30 days from hospitalization or a longer length of stay or earlier intervention in this cohort for management due to much more severe illness.
Cardiovascular disease has been linked to increased RSV incidence and complications. Children with congenital heart disease and cardiomyopathy have been found to have increased hospital admissions and severe RSV infections [38]. Loubet et al. found that around 45% of patients with lab-confirmed RSV had chronic heart disease [25]. Duncan et al. demonstrated that among patients admitted to the inpatient setting with RSV infection, 28% had congestive heart failure (CHF) as compared to 0% in the outpatient setting, with a trend towards more coronary artery disease (CAD) (25% vs 8%) [39]. Similar rates of CHF (21%) and coronary artery disease (28%) were observed by Dowell et al. in 57 patients admitted with RSV pneumonia [40]. McCraken and colleagues also determined that patients with underlying heart disease were more likely to develop a severe hospital outcome (OR 4.1; 95% confidence interval [CI]: 1.9 to 8.8) [41]. Even among patients with COPD, CHF was the only significant risk factor for developing severe RSV infection [42]. However, PH has not been assessed as a potential risk factor in any of these studies. Some studies have noted that almost 50% of patients with heart failure with preserved ejection fraction have PH [43,44]. Our study demonstrated that among patients with RSV with PH, concomitant CVD had a significantly higher risk of hospitalization (aOR of 5.102, 95% CI 4.787-5.438, p-value < 0.0001) compared to RSV with PH patients without CVD. Of note, we did not include heart failure in our analyses for CVD, as heart failure denotes PH disease progression [43]. The presence of chronic lung disease, chronic kidney disease, and diabetes mellitus increased the odds of hospitalization in PH patients with RSV infection. These comorbidities have previously been elucidated as risk factors for severe RSV infection [5,32].
Pulmonary hypertension in itself is an evolving paradigm, with recent changes to diagnostic criteria and newer medications being approved for therapy [45,46]. Most patients are categorized as Group 2 (69%) as compared to Group 1 (15%), Group 3 (9%), and Groups 4 and 5 (3% each) [47]. In our study, similarly, patients with Group 2 had a higher risk of hospitalization when compared to other PH WHO groups (aOR 1.771, 95% CI 1.697-1.848, p-value <0.0001) further emphasizing the importance of RSV prevention in patients with underlying heart disease. Interestingly, when we compared each PH group with RSV individually with RSV without PH cohort after propensity score matching, all groups revealed statistically significant increase in hospitalization risk. Though the sample size of these groups was small compared to the RSV without PH cohort, these findings depict a need for further studies to assess if PH by itself acts as an independent risk factor affecting RSV severity. Some studies have noted elevated serum cytokines (tumor necrosis factor-alpha, interferon-gamma, and interleukin-1beta, -2, -4, -5, -6, -8, -10, -12p70, and -13) in Group 1 PH patients [48,49]. This cytokine dysregulation may be responsible for exacerbating RSV-induced inflammation as a possible mechanism. Reciprocal RSV-induced PH has previously been demonstrated in mouse models, which could also help decipher the pathogenesis of PH in RSV [50].
Currently 3 different vaccines are approved by the US Food and Drug Administration (FDA). The mRNA RSV vaccine (mResvia) is approved for people older than 60 years, while an adjuvanted monovalent RSV vaccine (Arexvy) is approved for people between 50-59 years, and for persons 18-59 years of age, bivalent PreF vaccine (Abrysvo) [51]. On June 26, 2024, the Advisory Committee on Immunization Practices(ACIP), recommended one of these RSV vaccines for all adults aged ≥75 years, for adults aged 60-74 years with above risk factors, and for those with moderate to severe immunocompromise [52]. These recommendations were made in agreement with the Center of Disease Control (CDC), which in addition to the above-mentioned risk factors, include end-stage renal disease, morbid obesity, chronic liver disease, chronic hematologic conditions, neurological or neuromuscular conditions, nursing home residence, and medical judgement. Thus, the CDC recommends a one-time RSV vaccine in a larger group of individuals, either inpatient or outpatient [53].
Despite this, few studies have noted that for the year 2024-2025, of the 51.8% of facilities that voluntarily elected to report RSV vaccination, only 17.9% of patients received it, highlighting the large population at risk but without access to the RSV vaccine [54]. In multiple studies of vaccine efficacy in patients over 60 years of age, hospitalization rates have been reduced by 70-80% [55,56]. Although the RSV vaccines are well tolerated, safety data in patients >65 years revealed an increased risk of developing Guillain-Barre syndrome (incidence rate ratio 2.02; 95% CI 0.93–4.40) within the first 42 days of receiving the vaccine [57]. Patients under 60 years have not demonstrated this risk.
Our study has some limitations. This is a TriNetX database- based retrospective cohort study in which data was not available from physician notes for WHO functional class for severity assessment, as well as from the right heart catheterization procedure for hemodynamics (considered the gold standard for PH diagnosis). Echocardiogram data was also sparse. We therefore used ICD-10 codes for pulmonary hypertension in combination with PH-specific medications to improve the positive predictive value and specificity for our study [12,13,14]. We used propensity score matching to reduce confounding, but there might be some residual confounding due to the inherent nature of electronic health records data. Only patients with an outpatient/inpatient RSV positive test and/or ICD-10-CM code were included in our study to improve sensitivity and prevent misclassification bias. Finally, due to the real-time large and diverse data availability, we were able to perform our primary and secondary data analysis from a large sample size.
5. Conclusions
Our retrospective cohort study demonstrated that PH is a potential risk factor for severe RSV infections. The administration of newer RSV vaccines in PH patients of all age groups, >18 years of age, therefore might prove beneficial. Further research needs to be performed to understand the underlying mechanism to reduce the risk of RSV-related outcomes in this susceptible population.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: List of ICD-10-CM, RxNorm and LOINC codes used in cohort identification and outcome definition; Table S2: List of WHO PH groups with their respective ICD-10-CM/RxNorm codes; Table S3: List of ICD-10-CM codes used for identification of various co-morbid conditions.
Author Contributions
Conceptualization, M.M. and A.R.B..; methodology, M.M.; software, M.M; validation, M.M. and K.G.; formal analysis, M.M.; investigation, M.M.; resources, M.M.; data curation, M.M, A.R.B., K.G.; writing—original draft preparation, M.M, A.K.V., A.P.G., S.B., V.G., S.K.M., A.R.B,K.G; writing—review and editing, M.M., A.R.B.; visualization, M.M and K.G.; supervision, M.M., K.G.; project administration, M.M and K.G..;. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding research.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Simonneau, G.; Montani, D.; Celermajer, D.S.; Denton, C.P.; Gatzoulis, M.A.; Krowka, M.; et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. 2019, 53. [Google Scholar] [CrossRef] [PubMed]
- Rose-Jones, L.J.; McLaughlin, V.V. Pulmonary hypertension: types and treatments. Curr Cardiol Rev. 2015, 11, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Hennessey, P.A.; Formica, M.A.; Cox, C.; Walsh, E.E. Respiratory syncytial virus infection in elderly and high-risk adults. N Engl J Med. 2005, 352, 1749–1759. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Denouel, A.; Tietjen, A.K.; Campbell, I.; Moran, E.; Li, X.; et al. Global Disease Burden Estimates of Respiratory Syncytial Virus-Associated Acute Respiratory Infection in Older Adults in 2015: A Systematic Review and Meta-Analysis. J Infect Dis. 2020, 222 (Suppl 7), S577–S583. [Google Scholar] [CrossRef] [PubMed]
- Branche, A.R.; Saiman, L.; Walsh, E.E.; Falsey, A.R.; Sieling, W.D.; Greendyke, W.; et al. Incidence of Respiratory Syncytial Virus Infection Among Hospitalized Adults, 2017-2020. Clin Infect Dis. 2022, 74, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Hill-Ricciuti, A.; Branche, A.R.; Sieling, W.D.; Saiman, L.; Walsh, E.E.; et al. Cost determinants among adults hospitalized with respiratory syncytial virus in the United States, 2017-2019. Influenza Other Respir Viruses. 2022, 16, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Savic, M.; Penders, Y.; Shi, T.; Branche, A.; Pircon, J.Y. Respiratory syncytial virus disease burden in adults aged 60 years and older in high-income countries: A systematic literature review and meta-analysis. Influenza Other Respir Viruses. 2023, 17, e13031. [Google Scholar] [CrossRef] [PubMed]
- Villar-Alvarez, F.; Garcia-Ortega, A.; Entrenas-Castillo, M. Impact of Respiratory Syncytial Virus in Patients With Chronic Respiratory Disease. Open Respir Arch. 2024, 6, 100345. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Hart, C.M.; Kempker, J.A.; Veeraraghavan, S.; Trammell, A.W. Pulmonary hypertension mortality trends in United States 1999-2019. Ann Epidemiol. 2022, 75, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Thenappan, T.; Ormiston, M.L.; Ryan, J.J.; Archer, S.L. Pulmonary arterial hypertension: pathogenesis and clinical management. BMJ. 2018, 360, j5492. [Google Scholar] [CrossRef] [PubMed]
- RSV Vaccine guidance for older adults. [Available from: https://www.cdc.gov/rsv/hcp/vaccine-clinical-guidance/older-adults.html#:~:text=What%20to%20know,to%20spread%20in%20the%20community.
- Gillmeyer, K.R.; Nunez, E.R.; Rinne, S.T.; Qian, S.X.; Klings, E.S.; Wiener, R.S. Development and Validation of Algorithms to Identify Pulmonary Arterial Hypertension in Administrative Data. Chest. 2021, 159, 1986–1994. [Google Scholar] [CrossRef] [PubMed]
- Heresi, G.A.; Dean, B.B.; Castillo, H.; Lee, H.F.; Classi, P.; Stafkey-Mailey, D.; et al. Identifying Patients with Group 3 Pulmonary Hypertension Associated with COPD or ILD Using an Administrative Claims Database. Lung. 2022, 200, 187–203. [Google Scholar] [CrossRef] [PubMed]
- Mathai, S.C.; Hemnes, A.R.; Manaker, S.; Anguiano, R.H.; Dean, B.B.; Saundankar, V.; et al. Identifying Patients with Pulmonary Arterial Hypertension Using Administrative Claims Algorithms. Ann Am Thorac Soc. 2019, 16, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Mesa-Frias, M.; Rossi, C.; Emond, B.; Bookhart, B.; Anderson, D.; Drummond, S.; et al. Incidence and economic burden of respiratory syncytial virus among adults in the United States: A retrospective analysis using 2 insurance claims databases. J Manag Care Spec Pharm. 2022, 28, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.A.; Desai, A.; Barnes, E.L.; Hayney, M.; Kochhar, G.S.; Hashash, J.G.; et al. Patients With Inflammatory Bowel Disease Are at Increased Risk of Hospitalization Due to Respiratory Syncytial Virus. Am J Gastroenterol. 2024, 119, 1545–1554. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Tolksdorf, K.; Hirve, S.; Schuler, E.; Zhang, W.; Haas, W.; et al. Evaluation of using ICD-10 code data for respiratory syncytial virus surveillance. Influenza Other Respir Viruses. 2020, 14, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.A.; Calzavara, A.; Emerson, S.D.; Djebli, M.; Sundaram, M.E.; Chan, A.K.; et al. Validating International Classification of Disease 10th Revision algorithms for identifying influenza and respiratory syncytial virus hospitalizations. PLoS One. 2021, 16, e0244746. [Google Scholar] [CrossRef] [PubMed]
- Function propensity score matching. [Available from: https://lucid.trinetx.com/r/v1.0/reference/propensity_score_matching.html#details.
- Jha, A.; Jarvis, H.; Fraser, C.; Openshaw, P.J.M. Respiratory Syncytial Virus. In: Hui DS, Rossi GA, Johnston SL, editors. SARS, MERS and other Viral Lung Infections. Wellcome Trust-Funded Monographs and Book Chapters. Sheffield (UK), 2016. [Google Scholar]
- Villanueva, D.H.; Arcega, V.; Rao, M. Review of respiratory syncytial virus infection among older adults and transplant recipients. Ther Adv Infect Dis. 2022, 9, 20499361221091413. [Google Scholar] [CrossRef] [PubMed]
- Hamalainen, A.; Savinainen, E.; Hamalainen, S.; Sivenius, K.; Kauppinen, J.; Koivula, I.; et al. Disease burden caused by respiratory syncytial virus compared with influenza among adults: a retrospective cohort study from Eastern Finland in 2017-2018. BMJ Open. 2022, 12, e060805. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.H.; Ison, M.G. Respiratory syncytial virus infection in adults. BMJ. 2019, 366, l5021. [Google Scholar] [CrossRef] [PubMed]
- Chatzis, O.; Darbre, S.; Pasquier, J.; Meylan, P.; Manuel, O.; Aubert, J.D.; et al. Burden of severe RSV disease among immunocompromised children and adults: a 10 year retrospective study. BMC Infect Dis. 2018, 18, 111. [Google Scholar] [CrossRef] [PubMed]
- Loubet, P.; Lenzi, N.; Valette, M.; Foulongne, V.; Krivine, A.; Houhou, N.; et al. Clinical characteristics and outcome of respiratory syncytial virus infection among adults hospitalized with influenza-like illness in France. Clin Microbiol Infect. 2017, 23, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Sitbon, O.; Chaouat, A.; Bertocchi, M.; Habib, G.; Gressin, V.; et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006, 173, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- McGoon, M.D.; Benza, R.L.; Escribano-Subias, P.; Jiang, X.; Miller, D.P.; Peacock, A.J.; et al. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol. 2013, 62(25 Suppl), D51–D59. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Self, W.H.; Wunderink, R.G.; Fakhran, S.; Balk, R.; Bramley, A.M.; et al. Community-Acquired Pneumonia Requiring Hospitalization among U. S. Adults. N Engl J Med. 2015, 373, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; McElhaney, J.E.; Beran, J.; van Essen, G.A.; Duval, X.; Esen, M.; et al. Respiratory syncytial virus and other respiratory viral infections in older adults with moderate to severe influenza-like illness. J Infect Dis. 2014, 209, 1873–1881. [Google Scholar] [CrossRef] [PubMed]
- Benza, R.L.; Raina, A.; Abraham, W.T.; Adamson, P.B.; Lindenfeld, J.; Miller, A.B.; et al. Pulmonary hypertension related to left heart disease: insight from a wireless implantable hemodynamic monitor. J Heart Lung Transplant. 2015, 34, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Melgar, M.; Britton, A.; Roper, L.E.; Talbot, H.K.; Long, S.S.; Kotton, C.N.; et al. Use of Respiratory Syncytial Virus Vaccines in Older Adults: Recommendations of the Advisory Committee on Immunization Practices - United States, 2023. MMWR Morb Mortal Wkly Rep. 2023, 72, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Osei-Yeboah, R.; Johannesen, C.K.; Egeskov-Cavling, A.M.; Chen, J.; Lehtonen, T.; Fornes, A.U.; et al. Respiratory Syncytial Virus-Associated Hospitalization in Adults With Comorbidities in 2 European Countries: A Modeling Study. J Infect Dis. 2024, 229 (Supplement_1), S70–S77. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Guthrie, K.A.; Waghmare, A.; Walsh, E.E.; Falsey, A.R.; Kuypers, J.; et al. Respiratory syncytial virus in hematopoietic cell transplant recipients: factors determining progression to lower respiratory tract disease. J Infect Dis. 2014, 209, 1195–1204. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.; Towner, W.; DeHaan, E.; Jiang, Q.; Li, W.; Rahman, F.; et al. Bivalent RSVpreF Vaccine in Adults 18 to <60 Years Old With High-Risk Conditions. Clin Infect Dis. 2025, 80, 911–920. [Google Scholar] [PubMed]
- Branche, A.R.; Falsey, A.R.; Finelli, L.; Walsh, EE. Residency in Long-Term Care Facilities: An Important Risk Factor for Respiratory Syncytial Virus Hospitalization. J Infect Dis. 2024, 230, e1007–e11. [Google Scholar] [CrossRef] [PubMed]
- Colosia, A.D.; Yang, J.; Hillson, E.; Mauskopf, J.; Copley-Merriman, C.; Shinde, V.; et al. The epidemiology of medically attended respiratory syncytial virus in older adults in the United States: A systematic review. PLoS One. 2017, 12, e0182321. [Google Scholar] [CrossRef] [PubMed]
- Surie, D.; Yuengling, K.A.; DeCuir, J.; Zhu, Y.; Gaglani, M.; Ginde, A.A.; et al. Disease Severity of Respiratory Syncytial Virus Compared with COVID-19 and Influenza Among Hospitalized Adults Aged >/=60 Years - IVY Network, 20 U.S. States, February 2022-May 2023. MMWR Morb Mortal Wkly Rep. 2023, 72, 1083–1088. [Google Scholar] [PubMed]
- Chu, P.Y.; Hornik, C.P.; Li, J.S.; Campbell, M.J.; Hill, K.D. Respiratory syncytial virus hospitalisation trends in children with haemodynamically significant heart disease, 1997-2012. Cardiol Young. 2017, 27, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Duncan, C.B.; Walsh, E.E.; Peterson, D.R.; Lee, F.E.; Falsey, A.R. Risk factors for respiratory failure associated with respiratory syncytial virus infection in adults. J Infect Dis. 2009, 200, 1242–1246. [Google Scholar] [CrossRef] [PubMed]
- Dowell, S.F.; Anderson, L.J.; Gary, H.E.; Jr Erdman, D.D.; Plouffe, J.F.; File, T.M.; Jr, e.t. al. Respiratory syncytial virus is an important cause of community-acquired lower respiratory infection among hospitalized adults. J Infect Dis. 1996, 174, 456–462. [Google Scholar] [CrossRef] [PubMed]
- McCracken, J.P.; Prill, M.M.; Arvelo, W.; Lindblade, K.A.; Lopez, M.R.; Estevez, A.; et al. Respiratory syncytial virus infection in Guatemala, 2007-2012. J Infect Dis. 2013, 208 Suppl 3, S197–S206. [Google Scholar] [CrossRef] [PubMed]
- Mehta, J.; Walsh, E.E.; Mahadevia, P.J.; Falsey, A.R. Risk factors for respiratory syncytial virus illness among patients with chronic obstructive pulmonary disease. COPD. 2013, 10, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Rosenkranz, S.; Gibbs, J.S.; Wachter, R.; De Marco, T.; Vonk-Noordegraaf, A.; Vachiery, JL. Left ventricular heart failure and pulmonary hypertension. Eur Heart J. 2016, 37, 942–954. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.S.; Roger, V.L.; Rodeheffer, R.J.; Borlaug, B.A.; Enders, F.T.; Redfield, M.M. Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study. J Am Coll Cardiol. 2009, 53, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.A. Revised Definition of Pulmonary Hypertension and Approach to Management: A Clinical Primer. J Am Heart Assoc. 2023, 12, e029024. [Google Scholar] [CrossRef] [PubMed]
- Rahaghi, F.F.; Humbert, M.; Hoeper, M.M.; White, R.J.; Frantz, R.P.; Hassoun, P.M.; et al. Future treatment paradigms in pulmonary arterial hypertension: a personal view from physicians, health authorities, and patients. Lancet Respir Med. 2025, 13, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Weitsman, T.; Weisz, G.; Farkash, R.; Klutstein, M.; Butnaru, A.; Rosenmann, D.; et al. Pulmonary Hypertension with Left Heart Disease: Prevalence, Temporal Shifts in Etiologies and Outcome. Am J Med. 2017, 130, 1272–1279. [Google Scholar] [CrossRef] [PubMed]
- Soon, E.; Holmes, A.M.; Treacy, C.M.; Doughty, N.J.; Southgate, L.; Machado, R.D.; et al. Elevated levels of inflammatory cytokines predict survival in idiopathic and familial pulmonary arterial hypertension. Circulation. 2010, 122, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Rabinovitch, M.; Guignabert, C.; Humbert, M.; Nicolls, M.R. Inflammation and immunity in the pathogenesis of pulmonary arterial hypertension. Circ Res. 2014, 115, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Vu, L.D.; Saravia, J.; Jaligama, S.; Baboeram Panday, R.V.; Sullivan, R.D.; Mancarella, S.; et al. Deficiency in ST2 signaling ameliorates RSV-associated pulmonary hypertension. Am J Physiol Heart Circ Physiol. 2021, 321, H309–H17. [Google Scholar] [CrossRef] [PubMed]
- Graham, B.S. The Journey to RSV Vaccines - Heralding an Era of Structure-Based Design. N Engl J Med. 2023, 388, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Britton, A.; Roper, L.E.; Kotton, C.N.; Hutton, D.W.; Fleming-Dutra, K.E.; Godfrey, M.; et al. Use of Respiratory Syncytial Virus Vaccines in Adults Aged >/=60 Years: Updated Recommendations of the Advisory Committee on Immunization Practices - United States, 2024. MMWR Morb Mortal Wkly Rep. 2024, 73, 696–702. [Google Scholar] [CrossRef] [PubMed]
- United States Centers for Disease Control and Prevention. RSV vaccination for adults 60 years of age and over. [Available from: https://www.cdc.gov/vaccines/vpd/rsv/hcp/older-adults.html.
- Reses, H.E.; Segovia, G.; Dubendris, H.; Barbre, K.; Ananth, S.; Lape-Newman, B.; et al. Coverage with Influenza, Respiratory Syncytial Virus, and COVID-19 Vaccines Among Nursing Home Residents - National Healthcare Safety Network, United States, November 2024. MMWR Morb Mortal Wkly Rep. 2024, 73, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Surie, D.; Self, W.H.; Zhu, Y.; Yuengling, K.A.; Johnson, C.A.; Grijalva, C.G.; et al. RSV Vaccine Effectiveness Against Hospitalization Among US Adults 60 Years and Older. JAMA. 2024, 332, 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.B.; Watts, J.A.; Mitchell, P.K.; Dascomb, K.; Irving, S.A.; Klein, N.P.; et al. Respiratory syncytial virus (RSV) vaccine effectiveness against RSV-associated hospitalisations and emergency department encounters among adults aged 60 years and older in the USA, October, 2023, to March, 2024: a test-negative design analysis. Lancet. 2024, 404, 1547–1559. [Google Scholar] [CrossRef] [PubMed]
- Hause, A.M.; Moro, P.L.; Baggs, J.; Zhang, B.; Marquez, P.; Melgar, M.; et al. Early Safety Findings Among Persons Aged >/=60 Years Who Received a Respiratory Syncytial Virus Vaccine - United States, May 3, 2023-April 14, 2024. MMWR Morb Mortal Wkly Rep. 2024, 73, 489–494. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Patient demographics and co-morbidities for the PH-RSV and RSV only cohort before and after propensity score matching.
Table 1.
Patient demographics and co-morbidities for the PH-RSV and RSV only cohort before and after propensity score matching.
|
Before Propensity score matching After Propensity score matching RSV with PH RSV without p-value RSV with PH RSV without p-value Std.dif (N= 193, 256) PH (2,843,714) (N= 188,903) PH(N=188,903) | |||||||
| Demographics | |||||||
| Age at Index, Mean ± SD | 68.2 +/- 15.3 | 49.7 +/- 21.4 | <0.001 | 68.2 +/-15.3 | 69.5 +/- 14.6 | <0.001 | 0.088 |
| Female, N (%) | 96,537 (50.6%) | 1,454,243(56.4%) | <0.001 | 95,478 (50.5%) | 94,921(50.2%) | 0.070 | 0.006 |
| White | 122,159 (64.0%) | 1,649,239(63.9%) | 0.527 | 121,265(64.2%) | 124,174(65.7%) | <0.001 | 0.032 |
| Black or African American | 34,140 (17.9%) | 404,163(15.7%) | <0.001 | 33,436(17.7%) | 31,666(16.8%) | <0.001 | 0.025 |
| Hispanic or Latino | 13,814 (7.2%) | 320,991(12.4%) | <0.001 | 13,693(7.2%) | 12,741(6.7%) | <0.001 | 0.020 |
| Co-morbidities, N (%) | |||||||
| Diabetes mellitus | 85,058 (44.6%) | 426,208 (16.5%) | <0.001 | 83,604(44.3%) | 84,615(44.8%) | 0.001 | 0.011 |
| Ischemic heart diseases | 99,044 (51.9%) | 328,169 (12.7%) | <0.001 | 97,278 (51.5%) | 97,367 (51.5%) | 0.772 | 0.001 |
| Chronic lower respiratory diseases | 98,729 (51.7%) | 596,064 (23.1%) | <0.001 | 96,995 (51.3%) | 97,442 (51.6%) | 0.146 | 0.005 |
| Cerebral infarction | 21,530 (11.3%) | 93,726(3.6%) | <0.001 | 21,131(11.2%) | 21,282(11.3%) | 0.436 | 0.003 |
| Chronic kidney disease (CKD) | 76,033 (39.8%) | 228,903 (8.9%) | <0.001 | 74,347(39.4%) | 72,223(38.2%) | <0.001 | 0.023 |
| Alcohol related disorders | 16,765 (8.8%) | 136,459 (5.3%) | <0.001 | 16,501(8.7%) | 16,460(8.7%) | 0.813 | 0.001 |
| Nicotine dependence | 47,420 (24.8%) | 407,835 (15.8%) | <0.001 | 46,765 (24.8%) | 47,901(25.4%) | <0.001 | 0.014 |
| Obesity, unspecified | 62,099 (32.5%) | 364,533 (14.1%) | <0.001 | 60,750 (32.2%) | 58,805 (31.1%) | <0.001 | 0.022 |
| Liver transplant status | 2,074 (1.1%) | 6,276 (0.2%) | <0.001 | 1,870 (1%) | 1,783(0.9%) | 0.148 | 0.005 |
| Kidney transplant status | 4,930 (2.6%) | 15,060(0.6%) | <0.001 | 4,591 (2.4%) | 4,331 (2.3%) | 0.005 | 0.009 |
| Stem Cell Transplant | 1,144 (0.6%) | 11,343 (0.4%) | <0.001 | 1,126(0.6%) | 1,225(0.6%) | 0.041 | 0.007 |
| Human immunodeficiency virus [HIV] disease | 1,556 (0.8%) | 1,460 (0.8%) | 0.079 | 1,556(0.8%) | 1,460(0.8%) | 0.079 | 0.006 |
| Connective Tissue disorders | |||||||
| Systemic lupus erythematosus (SLE) | 3,609 (1.9%) | 3,289 (1.7%) | 0.963 | 3,609(1.9%) | 3,289(1.7%) | <0.001 | 0.013 |
| Rheumatoid arthritis | 8,924 (4.7%) | 8,930 (4.7%) | <0.001 | 8,924(4.7%) | 8,930(4.7%) | 0.963 | <0.001 |
| Systemic sclerosis [scleroderma] | 1,756 (0.9%) | 1,319 (0.7%) | <0.001 | 1,756(0.9%) | 1,319(0.7%) | <0.001 | 0.018 |
| Other overlap syndromes | 848 (0.4%) | 630 (0.3%) | <0.001 | 848 (0.4%) | 630(0.3%) | <0.001 | 0.018 |
Abbrviations: PH: pulmonary hypertension; RSV: respiratory syncytial virus; Std.diff: Mean standard difference.
Table 2.
Risk of hospitalization in the RSV with PH cohort and RSV without PH cohort after propensity score matching expressed as aOR with 95%CI.
Table 2.
Risk of hospitalization in the RSV with PH cohort and RSV without PH cohort after propensity score matching expressed as aOR with 95%CI.
| Age groups | RSV with PH group | RSV without PH group | aOR | 95% CI | p-value |
|---|---|---|---|---|---|
| >=18 years | 128,458 (68%) | 99,777 (53%) | 1.89 | 1.873, 1.924 | 0.02 |
| 18-49 years | 9,472 (63%) | 5,363 (35.8%) | 3.080 | 2.939, 3.229 | 0.03 |
| >50 years | 115,321 (68.4%) | 91,871 (54.5%) | 1.808 | 1.783, 1.834 | 0.015 |
| >60 years | 88,890 (67.3%) | 72,332 (54.8%) | 1.701 | 1.674, 1.728 | < 0.05 |
Abbreviation: aOR: Adjusted Odds ratio.
Table 3.
Risk of hospitalization-related complications between the RSV with PH cohort and RSV without PH cohort after propensity score matching.
Table 3.
Risk of hospitalization-related complications between the RSV with PH cohort and RSV without PH cohort after propensity score matching.
| Hospital complications | RSV with PH group | RSV without PH group | aOR | 95% CI | p-value |
|---|---|---|---|---|---|
| Composite | 36,041 (32%) | 29,987 (27%) | 1.298 | 1.274, 1.321 | <0.0001 |
| Mortality | 8,434 (7.5%) | 9,111 (8.1%) | 0.920 | 0.892, 0.948 | <0.0001 |
| Critical care services | 32,193 (28.7%) | 25,494 (22.7%) | 1.369 | 1.343, 1.395 | <0.0001 |
| Intubation | 6,580 (5.9%) | 4,862 (4.3%) | 1.375 | 1.324, 1.429 | <0.0001 |
| Vasopressor support | 5,500 (4.9%) | 3,604 (3.2%) | 1.553 | 1.488, 1.621 | <0.0001 |
Table 4.
Risk of hospitalization in the RSV with PH cohort in patients with and without comorbid conditions after propensity score matching expressed as aOR with 95% CI.
Table 4.
Risk of hospitalization in the RSV with PH cohort in patients with and without comorbid conditions after propensity score matching expressed as aOR with 95% CI.
| RSV with PH group with comorbidity | Number of patients | aOR | 95% CI | p-value |
| With DM | 16,760 (76.6%) | 1.083 | 1.078-1.089 | < 0.0001 |
| Without DM | 15,627 (71.4%) | |||
| With CVD | 26,367 (74.3%) | 5.102 | 4.787-5.438 | < 0.0001 |
| Without CVD | 23,708 (66.8%) | |||
| With CLD | 22,860 (75.8%) | 2.628 | 2.466-2.801 | < 0.0001 |
| Without CLD | 22,095 (73.2%) | |||
| With CKD | 51,749 (76.3%) | 3.076 | 2.894-3.269 | < 0.0001 |
| Without CKD | 48,885 (72.1%) |
Abbreviation: aOR :adjusted odds ratio, CVD: includes ischemic heart disease, mitral valve stenosis, congenital heart disease, cerebral infarction, peripheral vascular disease and arterial thrombosis; DM: diabetes mellitus; CLD: chronic lung disease including chronic bronchitis, COPD, asthma, bronchiectasis; CKD: chronic kidney disease including CKD stage>3 or ESRD.
Table 5.
In-group RSV with PH comparisons and risk of hospitalization.
| In-group RSV with PH comparisons | aOR | Confidence interval | p-value |
| Group 1 vs other PH groups | 0.735 | 0.686- 0.787 | <0.001 |
| Group 2 vs other PH groups | 1.771 | 1.697- 1.848 | <0.0001 |
| Group 3 vs other PH groups | 0.897 | 0.874- 0.922 | <0.001 |
| Group 4 vs other PH groups | 1.02 | 0.781-1.328 | 0.892 |
Abbreviation: aOR: adjusted odds ratio; PH: Pulmonary hypertension.
Table 6.
Hospitalization risk in PH WHO sub-groups vs RSV without PH cohort.
| RSV with PH sub-groups (Number of patients) | RSV without PH (2,843,714) |
||
| aOR | 95% CI | p-value | |
| Group 1 (16,505) | 2.576 | 2.437- 2.722 | < 0.001 |
| Group 2 (124,166) | 3.892 | 3.804- 3.982 | <0.0001 |
| Group 3 (49,628) | 3.741 | 3.644-3.841 | <0.001 |
| Group 4 (1645) | 3.872 | 3.181-4.713 | <0.0001 |
Abbreviation: aOR: Adjusted Odds ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



