
Submitted:
08 September 2025
Posted:
09 September 2025
You are already at the latest version
Abstract
Respiratory syncytial virus (RSV) is a major cause of respiratory illness, particularly in children, yet its burden in adults – especially in older adults – remains under-recognized. We analyzed RSV-related hospitalizations in Switzerland from 2017 to 2023 using national data from the Federal Statistical Office, including cases with RSV coded as either a primary or secondary diagnosis. Over 35,000 RSV-related hospitalizations were recorded. The highest incidence occurred in children under 10 years (390 per 100,000/year), with a second peak in adults ≥80 years (151 per 100,000/year). Older adults (≥60 years) accounted for more than 9,700 hospitalizations overall, with an average of over 16,600 total hospital days per year. Average length of stay (LOS) was shortest in young children (4.6 days) and highest in adolescents (13.9 days), while in adults it increased from 6.8 days (age 20-29) to 12.3 (age ≥80). Mechanical ventilation rates peaked at 12.6% in 60-69 year olds, and in-hospital mortality at 7.1% in those ≥80 years. In adults, RSV was more often recorded as a secondary diagnosis and commonly associated with chronic comorbidities, including chronic obstructive pulmonary disease, heart failure, kidney disease, and diabetes. Frailty-related diagnoses – such as cognitive or motor impairment, delirium, and need for nursing care – were also frequent. These findings highlight the importance of improved adult RSV surveillance and targeted prevention strategies in high-risk populations.
Keywords:
respiratory syncytial virus (RSV)
; hospitalization
; length of hospital stay
; mortality
; intensive care
; mechanical ventilation
; vaccination
; comorbidities
1. Introduction
Respiratory syncytial virus (RSV) is an enveloped RNA virus that primarily infects the respiratory tract. It can cause symptoms ranging from mild colds to more severe lower respiratory tract infections such as bronchiolitis and pneumonia, with severe cases particularly affecting infants, young children, and older adults [1]. The World Health Organization (WHO) estimates that RSV causes 33 million lower respiratory tract infections, 3 million hospitalizations, and approximately 59,600 deaths annually among children aged ≤5 years [2]. Despite its clinical importance, RSV surveillance and reporting remain inconsistent across Europe, with several countries – including Switzerland – yet to designate RSV as a notifiable disease [3].
In Switzerland, RSV surveillance exists but has traditionally focused on young children, who are known to experience high infection rates and hospitalizations [1,4]. However, this pediatric-centric approach may overlook a substantial burden of disease in adults, particularly older adults [5,6,7]. Systematic reviews suggest that RSV hospitalizations in adults may be underreported by factors ranging from 1.5 to over 20 [5,6,7]. Evidence suggests that there is a significant underestimation of adult RSV burden due to factors such as low awareness and testing rates, reduced assay sensitivity in adults, and lack of standardized case definitions [5,6,7,8,9]. Adult patients often present later in the disease course, when the virus is already in the lower airways, making standard upper respiratory swabs more likely to yield false negative results [5,9]. Additionally, lower viral loads and shorter viral shedding in adults complicate detection [10].
A growing body of literature highlights the clinical relevance of RSV in adult and immunocompromised populations. RSV is increasingly recognized as an important cause of medically attended acute respiratory illness in multimorbid patients [11]. Comorbidities such as hematologic malignancies, chronic heart failure, chronic obstructive pulmonary disease (COPD), and other chronic lung or cardiovascular conditions can exacerbate RSV disease and increase the risk of severe outcomes [12,13,14,15,16]. Immunocompromised individuals, including those with cancer or transplant recipients, appear to be particularly vulnerable, with elevated hospitalization and mortality rates. These findings are especially relevant in the Swiss context, where chronic comorbidities such as obesity, cardiovascular disease, and chronic lung disease are common in older adults [17].
A recent Swiss study by Stucki et al. (2024) used national hospital data from 2003 to 2021 to evaluate RSV-associated hospitalizations, focusing on RSV infection as a primary diagnosis, mainly in children. While confirming the expected high RSV burden in infants, the study likely underestimates the true adult burden, as it excluded cases with RSV infection as a secondary diagnosis, which is frequently the case in older and multimorbid patients [18].
To address these gaps, our study aimed to assess RSV-related hospitalizations across all age groups in Switzerland using data from the Swiss Federal Statistical Office (FSO) for the period 2017–2023. This more recent timeframe reflects increased awareness and improved RSV testing, particularly in adults. By including cases with RSV infection coded as either primary or secondary diagnosis, our analysis provides a more comprehensive picture of RSV-associated morbidity. Special emphasis is placed on older adults, in whom RSV infection is often overlooked despite a disproportionate burden of severe outcomes.
2. Materials and Methods
2.1. Data Collection and Analysis
This study used hospitalization data aggregated by age groups from the Swiss FSO. Specifically, all hospitalizations between 2017 and 2023 with a primary or secondary diagnosis of RSV infection, identified by the following four ICD-10 diagnosis codes, were included in the analyses: B97.4 (RSV as cause of diseases classified in other chapters), J12.1 (pneumonia caused by RSV), J20.5 (acute bronchitis caused by RSV), and J21.0 (acute bronchiolitis due to RSV). These codes represent all specific ICD-10 codes for RSV-associated hospitalizations in Swiss hospital data. Age groups were defined in bins of 10 years (0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, and 80+ years). For each age group, hospitalizations with a RSV-related primary or secondary diagnosis were analyzed for annual numbers of hospitalizations, length of hospital stay (LOS), intensive care unit (ICU) admissions, mechanical ventilations, and in-hospital mortality. Analyses were conducted using both absolute and relative frequencies, as well as rates per 100,000 inhabitants.
Data on population demographics was retrieved by year and calculated by age group based on data published by the FSO per age year [19].
2.2. Statistical Methods
Absolute numbers and mean LOS per age group were provided by the FSO. Swiss population numbers per age group as of 31st of December of each year were retrieved from data published by the FSO [19]. We conducted descriptive analyses such as the determination of relative frequencies and averages per age group. To account for differences in population size across age groups, hospitalization incidence rates were additionally expressed per 100,000 inhabitants per age group. This approach allows for direct comparison across age strata and better reflects the relative disease burden in the population. To better capture the overall healthcare burden of RSV-related hospitalizations, the total number of hospitalization days per year and age group were calculated by multiplying the number of hospitalizations by the average LOS. All calculations and figures were created with Excel 2016. For data protection reasons, the FSO did not provide values for case numbers between 1 and 3. In these cases, we used the lowest possible value of 1 in the calculations.
2.3. Ethical Considerations
This study was conducted in accordance with the ethical standards according to the Declaration of Helsinki. Ethical consent was not required, as the data were anonymized and collected as part of routine healthcare operations.
3. Results
3.1. Epidemiology
Between 2017 and 2023, a total of 35,489 RSV-related hospitalizations were documented in Switzerland, corresponding to an average of approximately 5,100 hospitalizations per year. Supplementary Figure S1 presents the annual absolute numbers, highlighting age-specific differences across years. A clear year-to-year variation was observed, most notably during the COVID-19 pandemic. In 2020, hospitalization numbers dropped well below average to 3,025 cases. A marked rebound followed in 2021, driven primarily by a pronounced wave in children aged 0–9 years, with 4,505 hospitalizations compared to 2,700–3,500 in the pre-pandemic years (2017–2019). In contrast, RSV-related hospitalizations among older adults did not return to pre-pandemic levels until 2022. Among individuals aged ≥80 years, case numbers rose from <100 in 2021 to approximately 1,100 in 2022 and 2023, exceeding the pre-pandemic range of 600–900. In addition to pandemic-associated fluctuations, an overall increasing trend in RSV-related hospitalizations was observed across the study period (Supplementary Figure S1). This likely reflects greater clinical awareness and more widespread diagnostic testing in adult populations, particularly among older individuals with comorbidities.
Figure 1 (a) summarizes the incidence of RSV-related hospitalizations 2017–2023, stratified by age group in 10-year increments and expressed per 100,000 inhabitants.
Figure 1.
Annual and average incidence of RSV-related hospitalizations per 100,000 inhabitants, stratified by age group in 10-year increments in Switzerland, 2017-2023. (a) All ages, including children, adolescents and adults; (b) Adults only, fold-change in hospitalization rates per adult age group compared to the 20–29-year reference group. Whiskers: minimum and maximum, box: interquartile range, ––: median, ×: mean, RSV: respiratory syncytial virus, inh.: inhabitants.
Figure 1.
Annual and average incidence of RSV-related hospitalizations per 100,000 inhabitants, stratified by age group in 10-year increments in Switzerland, 2017-2023. (a) All ages, including children, adolescents and adults; (b) Adults only, fold-change in hospitalization rates per adult age group compared to the 20–29-year reference group. Whiskers: minimum and maximum, box: interquartile range, ––: median, ×: mean, RSV: respiratory syncytial virus, inh.: inhabitants.
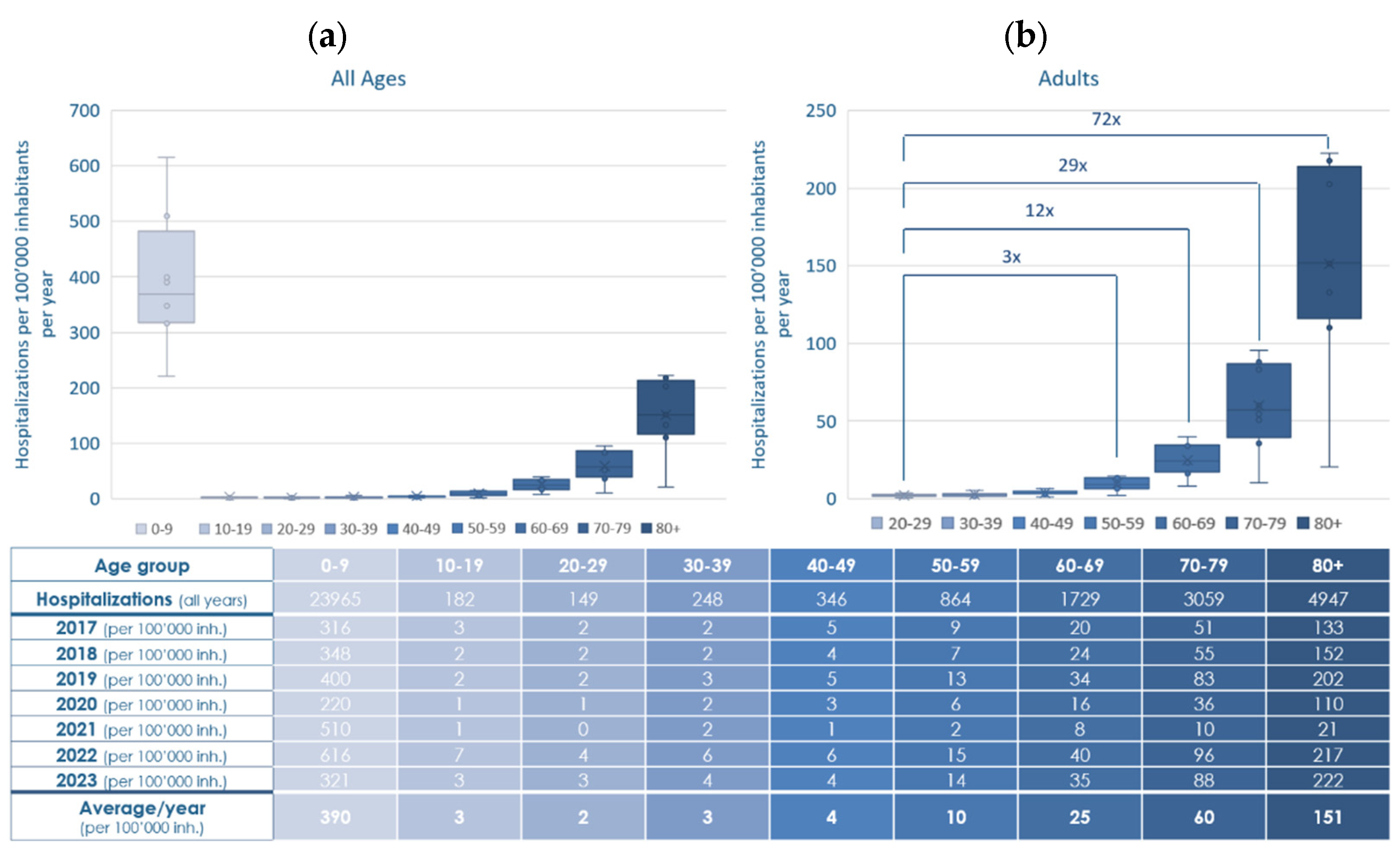
The highest hospitalization incidence by far was observed in children aged 0–9 years, with an annual mean of 390 cases per 100,000 population. Hospitalization incidence declined sharply in the older children and young adults (aged 10–49 years), remaining ≤ 4 cases per 100,000 annually. From age 50 onward, incidence increased steadily with rising age from 10 (ages 50–59) to 25 (ages 60–69) and 60 (ages 70–79), peaking at 151 in individuals aged ≥80 years per 100,000 population.
Comparison among adults only (Figure 1 (b)) shows a marked increase of hospitalizations from the age of 50 onward with rates 3- to 72-fold higher than in young adults (20–29 years). These findings highlight the substantial and age-dependent rise in RSV-related hospitalizations across the adult population.
3.2. Outcome
3.2.1. Length of Hospital Stay of RSV-Related Hospitalizations 2017–2023
Figure 2 (a) presents the average LOS for RSV-related hospitalizations in Switzerland stratified by age group, based on data from 2017 to 2023, showing notable differences between age groups. Children aged 0–9 years had the shortest hospital stays, with an overall average LOS of 4.6 days. Among adults aged 20-49 years LOS increased moderately with age (6.8 days in the 20-29 year group, 8.4 days in the 30-39 year group, 9.6 days in the 40-49 years group). In contrast, LOS was substantially longer in older adults, increasing with age: 11.2 days (50-59 years), 11.6 days (60-69 years and 70-79 years) and 12.3 days (≥80 years), thus a 2.4- to 2.7-fold increase compared to young children.
Figure 2.
Length of hospital stay (LOS) for RSV-related hospitalizations, stratified by age group in 10-year increments in Switzerland, 2017-2023. (a) Average mean LOS in days is shown for each age group; (b) Total hospitalization days (multiplication of LOS with number of hospitalizations) for RSV-related hospitalizations per age group and year, as well as the average over the years 2017–2023. Statistical significance assessed by t-test. Whiskers: minimum and maximum, box: interquartile range, ––: median, ×: mean, RSV: respiratory syncytial virus, LOS: length of hospital stay.
Figure 2.
Length of hospital stay (LOS) for RSV-related hospitalizations, stratified by age group in 10-year increments in Switzerland, 2017-2023. (a) Average mean LOS in days is shown for each age group; (b) Total hospitalization days (multiplication of LOS with number of hospitalizations) for RSV-related hospitalizations per age group and year, as well as the average over the years 2017–2023. Statistical significance assessed by t-test. Whiskers: minimum and maximum, box: interquartile range, ––: median, ×: mean, RSV: respiratory syncytial virus, LOS: length of hospital stay.
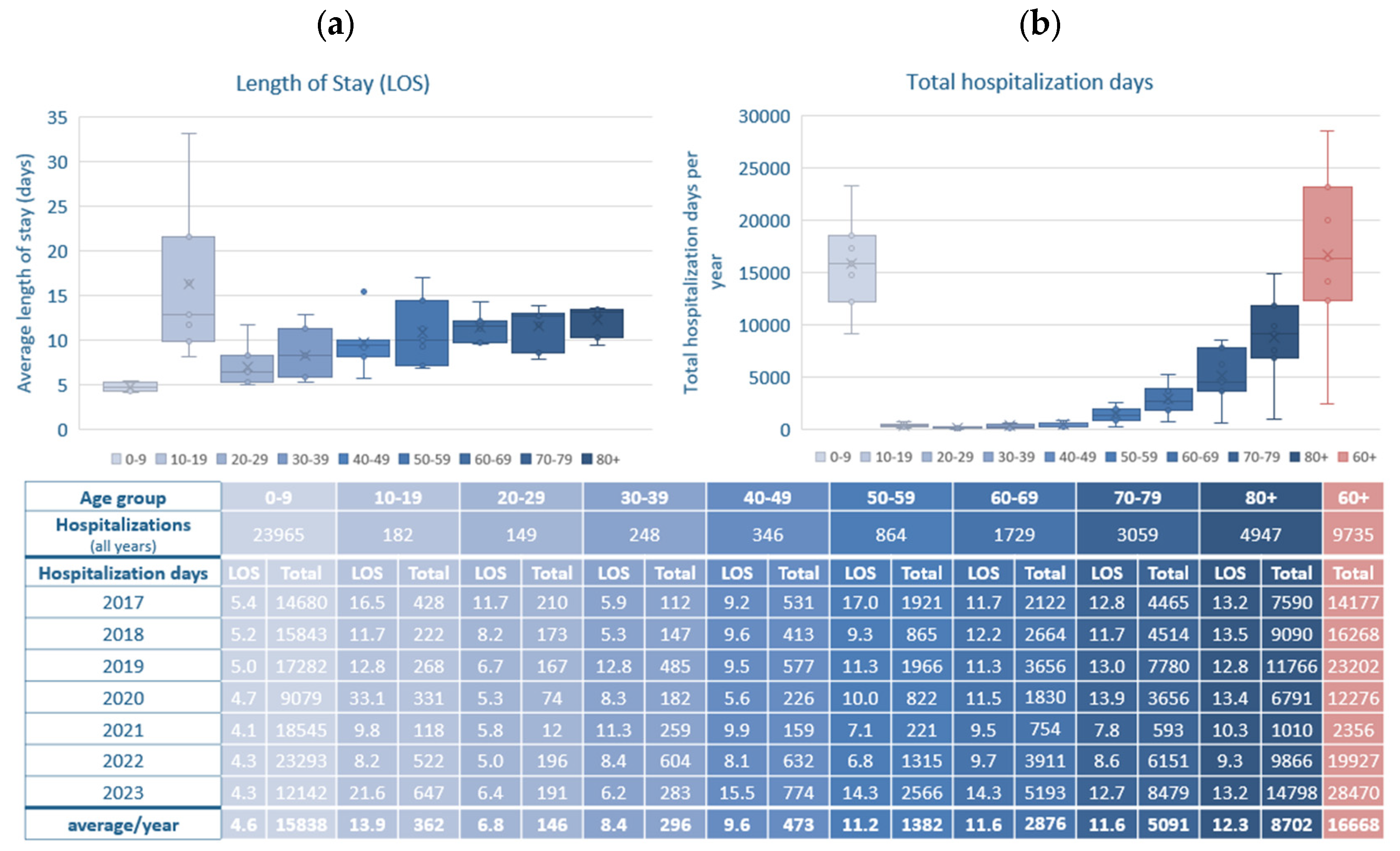
Interestingly, the longest average LOS across all age groups was observed in adolescents aged 10–19 years, with an overall average of 13.9 days, exceeding even that of the oldest patients. However, this finding should be interpreted with caution: adolescents represented the smallest number of hospitalizations overall, resulting in considerable year-to-year variation. The disproportionately long LOS may reflect the disproportionate severity in a small number of complex cases in this age group.
Figure 2 (b) illustrates the total hospitalization days per age group, providing insight into the cumulative strain on hospital resources across age cohorts. Between 2017 and 2023, the highest total number of hospitalization days was consistently attributed to children aged 0–9 years, with an average of 15,838 days per year. However, older adults (aged ≥60 years) collectively accounted for an even larger burden, averaging 16,668 total hospitalization days per year. Within this group, adults aged ≥80 years alone contributed over 8,700 hospitalization days annually, exceeding all other adult age bands. These data emphasize that although children account for the highest number of RSV hospitalizations, older adults—due to longer LOS—represent a major share of total inpatient burden.
3.2.2. RSV-Related Hospitalizations Admitted to Intensive Care Units 2017–2023
Between 2017 and 2023, a total of 3,441 ICU admissions were recorded in RSV-related hospitalizations in Switzerland, showing a distinct age-related pattern (Supplementary Figure S2). In terms of absolute numbers, children aged 0–9 years accounted for the highest ICU burden, with 166 to 473 admissions annually—making this group the largest contributor to total ICU admissions across all age groups. However, when considered in relative terms, their overall ICU admission rate was comparatively low at 8.6% of RSV-related hospitalizations (Figure 3, Supplementary Figure S3).
Figure 3.
Average rate of ICU admission, mechanical ventilation, and in-hospital mortality in % of overall RSV-related hospitalizations in Switzerland, 2017–2023, stratified by age group in 10-year increments. ICU: intensive care unit admission, Hospitaliz.: Hospitalizations, RSV: respiratory syncytial virus.
Figure 3.
Average rate of ICU admission, mechanical ventilation, and in-hospital mortality in % of overall RSV-related hospitalizations in Switzerland, 2017–2023, stratified by age group in 10-year increments. ICU: intensive care unit admission, Hospitaliz.: Hospitalizations, RSV: respiratory syncytial virus.
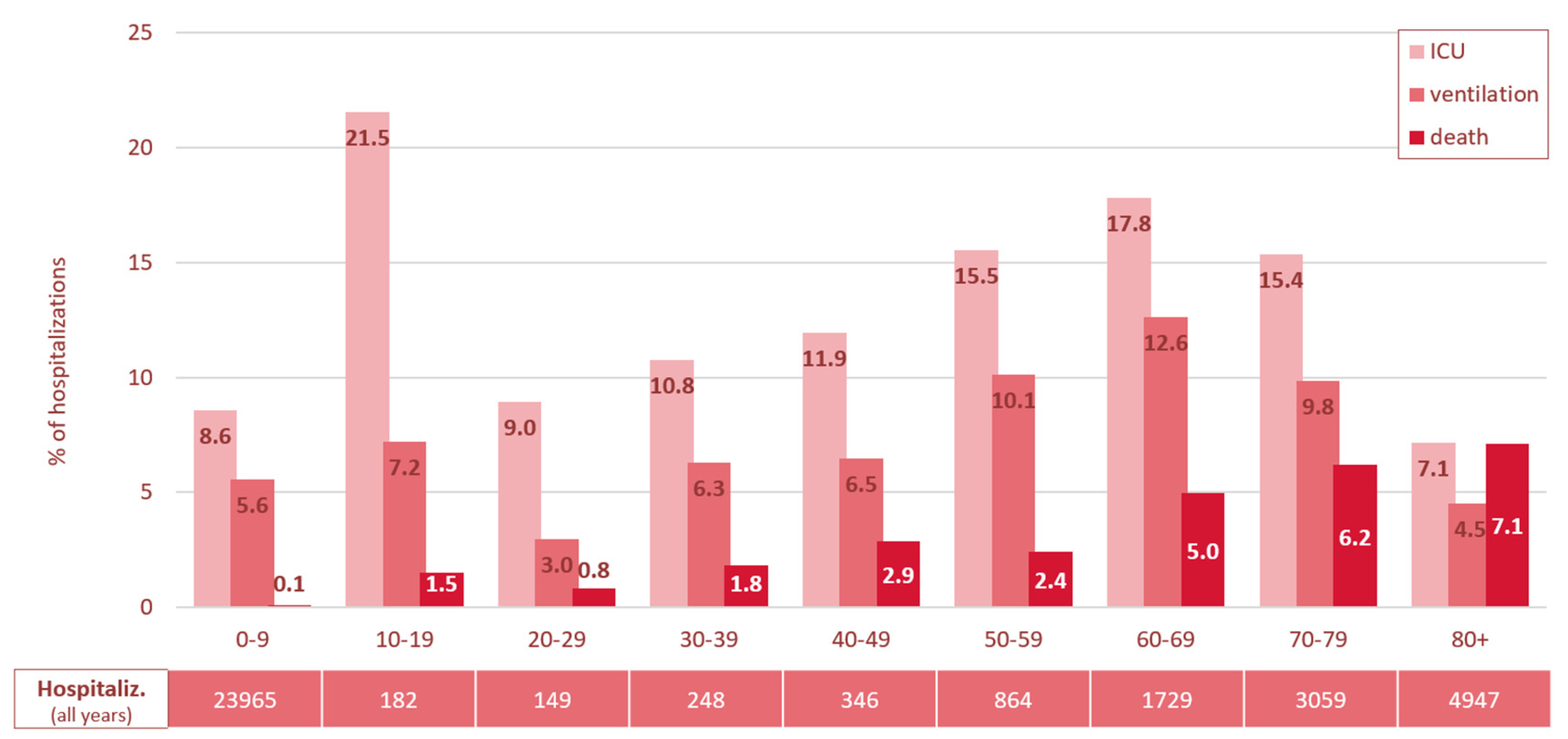
In contrast, adolescents aged 10–19 years showed the highest overall ICU admission rate (21.5%), despite having the lowest number of RSV-related hospitalizations (between 10 and 64 cases per year) compared to the other age groups.
Adults aged 20-39 years exhibited moderate ICU admission rates, ranging from 9-10.8%, among older adults ICU admission rates increased progressively with advancing age (40-49 years 11.9%, 50-59 years 15.5%, 60-69 years 17.8%), before declining again in those aged 70-79 years (15.4%) and dropping further to the lowest rate of 7.1% in individuals aged 80 years and older.
In summary, the burden of ICU admissions in RSV-related hospitalizations falls primarily on young children (0–9 years) in absolute numbers and on older adults (≥60 years) in relative severity. Adolescents exhibited the highest ICU admission rate.
3.2.3. RSV-Related Hospitalizations Requiring Mechanical Ventilation 2017–2023
The need for mechanical ventilation largely paralleled ICU admission trends across most age groups (Figure 3 and Supplementary Figures S2, S4). Children aged 0–9 years accounted for 60% of the overall ventilated cases in the seven-year period (1,317 / 2,179), but their average ventilation rate was comparatively low at 5.6%. Age groups between 10 and 49 years showed consistently low to moderate ventilation rates, ranging between 3.0% and 7.2%. For adults aged 50 and older, ventilation rates increased with age, peaking in the 60–69-year age group at 12.6%. In the age groups 70+, the rates declined to 9.8% in the 70–79-year group and further to 4.5% in individuals aged 80 and older.
In summary, young children (aged 0–9 years) and adults aged 60–79 years accounted for the highest burden of ventilation in absolute numbers, while adults between 50 and 79 had the highest ventilation rates. Lowest absolute and relative numbers of mechanical ventilation were observed in the youngest (<30 years) and oldest (≥80 years) adults.
3.2.4. In-Hospital Mortality in RSV-Related Hospitalizations 2017–2023
Overall, 656 RSV-related hospitalizations resulted in in-hospital death (1.8%). While the in-hospital mortality rates remained low in children and younger adults up to 39 years (< 2%), they rose progressively with age: between 2.4-2.9% in those aged 40-59 years, exceeding 5% from age 60 onward, and peaking at 7.1% in the oldest age group (≥80 years) (Figure 3 and Supplementary Figure S5).
In summary, the highest mortality rates occurred in individuals aged 60 and older, increasing progressively with age, while younger age groups, particularly those under 40, were least affected. Overall, the data reveal a clear age-related gradient in RSV disease severity: younger children (0–9 years) present with high hospitalization incidence but relatively mild clinical courses, whereas older adults, despite lower absolute numbers, face a disproportionately higher risk of ICU admission, need for mechanical ventilation, and in-hospital death.
3.3. RSV Infection as Primary vs. Secondary Diagnosis and Additionally Coded Diagnoses
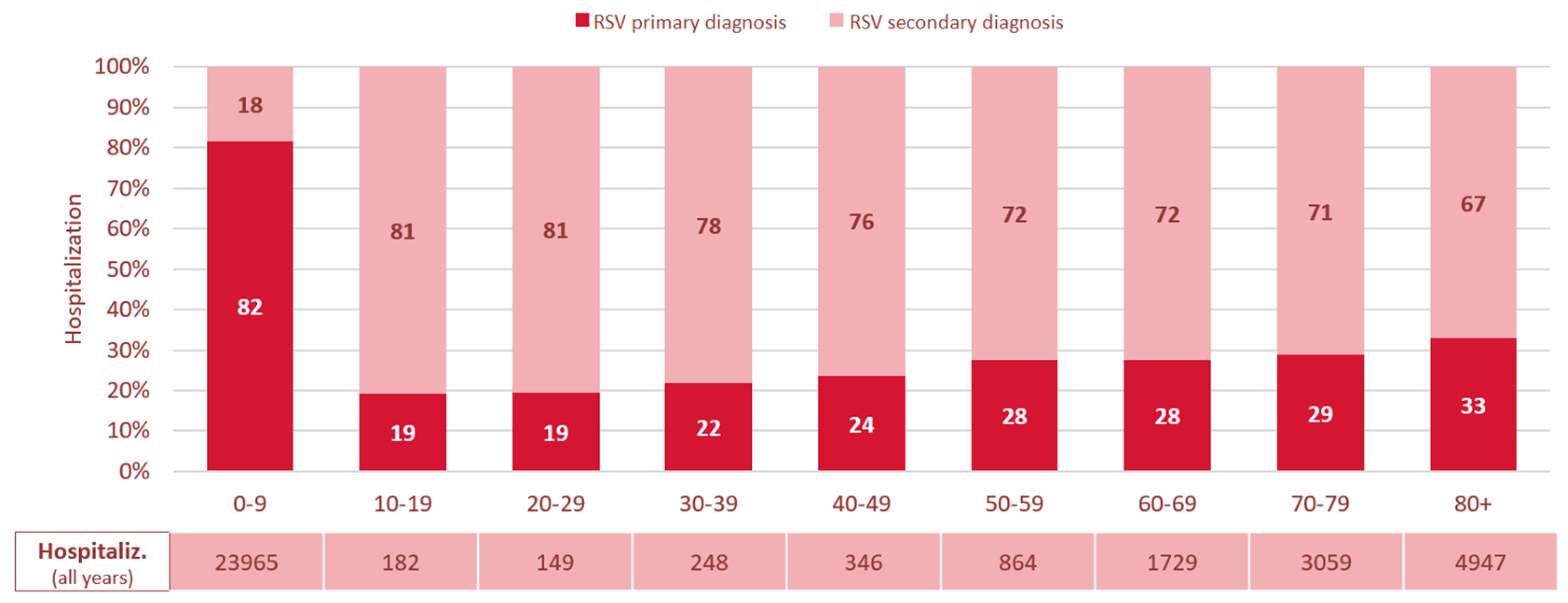
A clear age-related pattern was also observed in the coding of RSV infection as a primary versus secondary diagnosis (Figure 4). In children aged 0–9 years, RSV infection was recorded as the primary diagnosis in 82% of cases, suggesting it was the main reason for hospitalization in this group. In contrast, among individuals aged 10 years and older, RSV was coded as a secondary diagnosis in the majority of the cases. In adolescents aged 10–19 years, in 81% of RSV-related hospitalizations RSV infection was coded as a secondary diagnosis. From this age group onward, the proportion of cases with RSV infection coded as the primary diagnosis gradually increased, reaching 33% in those aged ≥80 years, while the proportion of RSV infection as a secondary diagnosis declined accordingly (Figure 4).
Figure 4.
Proportion of RSV infection coded as primary vs. secondary diagnosis in % of overall RSV-related hospitalizations in Switzerland, 2017–2023, stratified by age group in 10-year increments. RSV: respiratory syncytial virus, Hospitaliz.: Hospitalizations.
Figure 4.
Proportion of RSV infection coded as primary vs. secondary diagnosis in % of overall RSV-related hospitalizations in Switzerland, 2017–2023, stratified by age group in 10-year increments. RSV: respiratory syncytial virus, Hospitaliz.: Hospitalizations.
To provide a more comprehensive understanding of the disease burden and associated clinical context, we extended this analysis to examine the most frequent diagnosis codes recorded alongside RSV-related diagnoses, regardless of whether RSV infection was coded as the primary or secondary diagnosis. This approach allows for a more nuanced view of the underlying or concurrent medical conditions across age groups. The 10 most common additionally coded diagnoses are listed in Supplementary Table S1.
In children aged 0–9 years, additionally coded diagnoses were predominantly acute respiratory or infection-related conditions. The most common were respiratory failure (J96, 44.4%), SARS-CoV-2 testing procedures (U99, 31.1%), and feeding/fluid-related symptoms (R63, 24.5%). Diagnoses such as acute bronchiolitis (J21), acute bronchitis (J20), otitis media (H66, H65), and volume depletion (E86) were also frequently observed. These findings reflect the acute nature of RSV-related hospitalizations in this age group and a tendency towards broader diagnostic coding in pediatric care.
In adolescents aged 10–19 years, additionally coded diagnoses were more heterogeneous. While SARS-CoV-2 testing procedures (U99, 9.3%), and respiratory failure (J96, 7.7%) remained common, several chronic and severe conditions were also frequent, including asthma (J45, 8.2%), epilepsy (G40, 6.6%), lymphoid leukemia (C91, 2.7%), and post-transplant status (Z94, 2.7%). The frequent occurrence of hematologic malignancies and transplant-associated diagnoses underscores the vulnerability of affected patients, a small but often immunocompromised, patient group.
Among adults (aged ≥20 years), comorbidities were predominantly chronic. Among the most frequent additionally coded diagnoses were chronic obstructive pulmonary disease (J44, 17.1%), primary hypertension (I10, 10.8%), heart failure (I50, 10.6%), atrial fibrillation (I48, 8.3%), and chronic kidney disease (N18, 8.2%). Bacterial pneumonia (J15, 6.5%), and electrolyte disorders (E87, 6.2%) were also common. These patterns highlight the burden of RSV in older, multimorbid populations, where RSV may act as a trigger for decompensation of underlying chronic diseases rather than as the isolated cause of hospitalization.
3.4. Chronic Comorbidities in Patients with RSV-Related Hospitalizations
To better understand the clinical vulnerability of patients affected by RSV infection, we analyzed the prevalence of common chronic comorbidities and severe conditions among all RSV-related hospitalizations—whether RSV was coded as a primary or secondary diagnosis—between 2017 and 2023. The analysis includes chronic diseases or severe conditions observed at a frequency of ≥0.1% in children, and ≥1% in adolescents and adults.
In children aged 0–9 years, chronic comorbidities were rare, documented in fewer than 3% of RSV-related hospitalizations (Figure S6, Supplementary Table S2). Most frequently documented were congenital malformations of cardiac septa (Q21, 0.7%), epilepsy (G40, 0.6%), gastroesophageal reflux disease (K21, 0.5%), and asthma (J45, 0.5%). Other notable but even less frequent chronic conditions included Down syndrome (0.3%), congenital malformations (of multiple systems 0.3%, of great arteries 0.3%, of head, face, spine and thorax 0.2%) and cerebral palsy (0.2%), underscoring that a small subset of young children with RSV-related hospitalization had underlying complex medical needs.
Among adolescents aged 10–19 years, chronic conditions were much more prevalent (Figure S7, Supplementary Table S2). Asthma (J45, 8.2%) and epilepsy (G40, 6.6%) were the most common, but a variety of severe or immuno-compromising conditions were also observed. These included lymphoid leukemia (C91, 2.7%), post-transplant status (Z94, 2.7%), and cerebral palsy (G80, 2.2%). More rare but noteworthy diagnoses such as aplastic anemia (D61, 1.6%), sickle-cell disease (D57, 1.1%), congenital malformations (Q67, 1.1%, Q87, 1.1%), and Down syndrome (Q90, 1.1%) suggest that adolescents hospitalized with RSV infection frequently had serious underlying chronic disease, potentially contributing to longer hospital stays and high ICU admission rates in this age group.
In adults aged ≥20 years, chronic comorbidities were very common (Figure 5, Supplementary Table S2). The most frequently documented diagnoses were chronic obstructive pulmonary disease (COPD, J44, 17.1% of cases), hypertension (I10 and I11 combined 16.0%), heart failure (I50, 10.6%), atrial fibrillation or flutter (I48, 8.3%), chronic kidney disease (N18, 8.2%), type 2 diabetes mellitus (E11, 6.2%), and asthma (J45, 4.2%) (Figure 5, Supplementary Table S2).
Figure 5.
Prevalence of additionally coded diagnoses in RSV-related hospitalizations (primary or secondary diagnoses) in adults aged ≥20 years in Switzerland, 2017–2023. Analysis focused on chronic comorbidities, severe or frailty-associated conditions. All conditions shown had a prevalence of ≥2.0% in the study population. See Supplementary Table S2 for more complete ICD-10 code listings and prevalence across other age groups. RSV: respiratory syncytial virus.
Figure 5.
Prevalence of additionally coded diagnoses in RSV-related hospitalizations (primary or secondary diagnoses) in adults aged ≥20 years in Switzerland, 2017–2023. Analysis focused on chronic comorbidities, severe or frailty-associated conditions. All conditions shown had a prevalence of ≥2.0% in the study population. See Supplementary Table S2 for more complete ICD-10 code listings and prevalence across other age groups. RSV: respiratory syncytial virus.
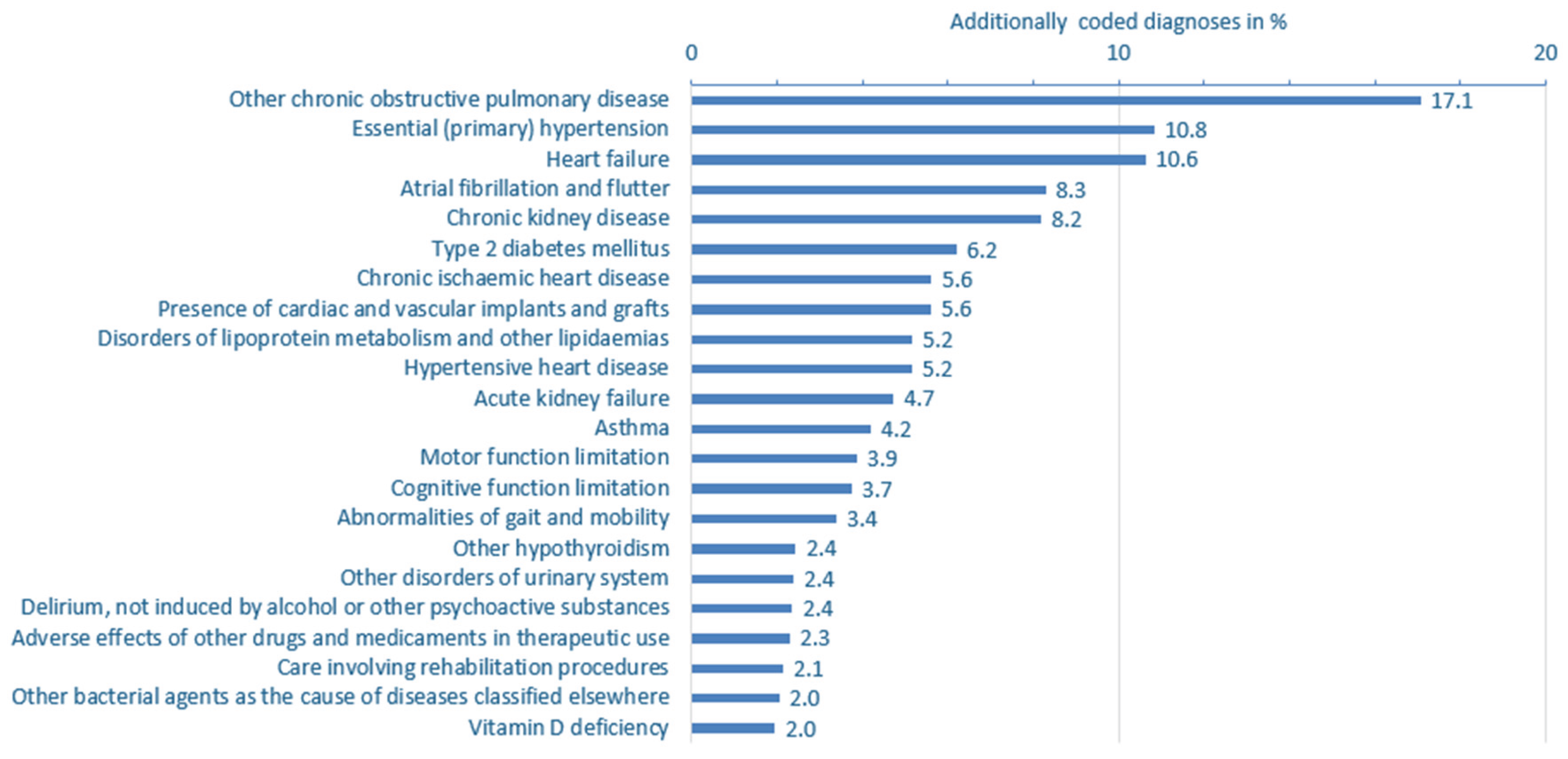
Beyond these common major comorbidities, a wide range of additionally coded conditions was observed. These encompassed further cardio-metabolic disorders such as chronic respiratory insufficiency, chronic ischemic and hypertensive heart disease, lipid metabolism disorders, hypothyroidism, and kidney dysfunction. Notably, several diagnostic codes pointed to frailty and complex care needs, including cognitive and motor impairments, gait and mobility limitations, delirium (non-substance-related), vitamin D deficiency, and signs of dehydration or volume depletion. Documentation of prior medical interventions, the presence of vascular implants, and the need for rehabilitation further highlighted the functional vulnerability of this patient population. Frequent coding of screening and follow-up procedures—particularly for infectious diseases—underscores the clinical complexity of adults hospitalized with RSV.
4. Discussion
Previous studies have shown that particularly in older adults, RSV infections are typically more severe than influenza, despite occurring less frequently [20,21,22]. Older adults hospitalized with RSV infection tend to experience longer hospital stays, higher rates of ICU admission and mechanical ventilation, and comparable or even higher mortality rates than those hospitalized with influenza [20,21,22].
Our findings demonstrate that RSV-related hospitalizations and outcomes, including LOS, ICU admission, mechanical ventilation, and in-hospital mortality, vary considerably by age. A bimodal distribution emerged: the highest absolute burden, excluding mortality, occurred in children aged 0–9 years and adults aged ≥60 years. While the highest absolute numbers of hospitalizations, ICU admissions, and mechanical ventilation were most observed in young children, in-hospital mortality was predominantly observed in older adults, increasing progressively with age. This aligns with previous reports of elevated RSV mortality in elderly populations [23,24].
We observed a substantial increase in RSV-related hospitalizations from 2017 to 2023, excluding the COVID-19 pandemic years 2020–2021, when non-pharmaceutical interventions suppressed respiratory virus transmission. During lockdowns, RSV prevalence among hospitalized children dropped significantly—a meta-analysis reported a drop from 25% to 5% [25]. The inclusion of the years 2020–2021 in our dataset likely lowered the average incidence, leading to an underestimation of the actual RSV burden in Switzerland.
When analyzing outcomes relative to the number of hospitalizations per age group, a nuanced pattern emerged. Although ICU admission rates were highest in the very small overall number of adolescent RSV-related hospitalizations, they were consistently elevated in older adults, particularly those aged 60–79 years. This suggests that, although fewer older adults are hospitalized with RSV infection compared to young children, those who are admitted tend to experience more severe disease, as reflected by higher rates of ICU admission, mechanical ventilation, and in-hospital mortality. The longer length of stay (LOS) observed in adults aged >50 years further underscores the increased clinical complexity and severity in this age group. This observation is likely due to older age and increasing number of comorbidities contributing to complications and more severe outcomes.
In contrast, while hospitalization numbers were highest in children under 10 years, their lower ICU admission, mechanical ventilation and very low mortality rates indicate a generally milder disease course in otherwise healthy pediatric patients.
An unexpected finding was the high average length of stay and ICU admission rate observed in adolescents. Although this age group accounted for a relatively small number of RSV-related hospitalizations—averaging around 26 cases per year—the severity of outcomes was notable. While previous research suggests that RSV infections in adolescents typically follow a mild clinical course [26], severe presentations can occur in this age group, particularly in individuals with underlying health conditions [27], potentially leading to the indication for intensive care. In our dataset, we observed markedly high numbers of lymphoid malignancies, epilepsy, and post-transplantation status among hospitalized adolescents, possibly explaining the elevated ICU admission rates in this group. Given the low absolute case numbers, small annual fluctuations can lead to large proportional changes, limiting the robustness of age-specific trend interpretation in this population.
In contrast, mortality was almost exclusively observed in patients aged ≥60 years, while those under 40 had very low mortality rates, consistent with the milder disease course in immunocompetent younger adults.
Interestingly, both ICU admission and mechanical ventilation rates declined with increasing age beyond 70, despite rising mortality. This suggests a shift in clinical decision-making, where intensive care is used more selectively in the very elderly—either due to frailty, comorbidity burden, or advance care planning.
A major finding of our study was the high proportion of RSV infection coded as a secondary diagnosis in adults, particularly in those with chronic conditions such as COPD and heart failure frequently listed as the primary diagnosis. This pattern suggests that comorbidities, which are generally more prevalent in older adults, both predispose individuals to a more severe course of RSV infection and may be exacerbated by the infection itself, ultimately contributing to hospitalization.
In contrast to pediatric cases—where RSV infection is typically the sole driver of disease—its role in older adults appears to be more complex, often interacting with underlying respiratory, cardiopulmonary or metabolic conditions and worsening the clinical trajectory [23,28,29,30]. However, our data do not allow us to determine whether RSV infection was the initial trigger for primary respiratory diagnoses such as pneumonia, or whether it was acquired secondarily during hospitalization. RSV infection is a known cause of COPD exacerbations [15,16], and patients with cardiopulmonary conditions have higher rates of RSV-related hospitalizations [14]. Heart failure, frequently associated with pulmonary congestion, may predispose patients to secondary respiratory complications [31,32]. Moreover, chronic heart failure may impair immune function, and consequently increase susceptibility to infections [33].
Together, these mechanisms likely contribute to the role of RSV infection in the hospitalization of older, multimorbid adults.
Thus, it is plausible that RSV infection plays a central, though under-recognized, role in the clinical deterioration of older adults. This is further supported by the high proportion of secondary RSV diagnoses among all hospitalizations in older age groups, indicating that RSV likely contributed to primary diagnoses such as acute decompensated heart failure and acute COPD exacerbation.
Furthermore, a recent European study reported that among patients hospitalized with a respiratory tract infection who tested positive for RSV, 57.6% were not recorded with an ICD-10 diagnosis for RSV infection during their admission, highlighting the extent of underreporting of RSV-coded hospitalizations [34].
The increasing prevalence of chronic comorbidities and frailty indicators in our older RSV patient population, together with the rise in RSV infection as a secondary diagnosis, underscore the substantial burden of RSV in this age group. This demonstrates the urgent need for enhanced awareness, improved testing strategies, and preventive approaches—particularly vaccination and risk-adapted clinical management—for older adults.
Limitations
The study has several limitations related to the use of administrative data. First, reliance on ICD-10 coding may lead to underreporting or misclassification of RSV infection cases, especially given variability in testing and documentation practices across hospitals and over time. Patients with confirmed RSV infection may not have been assigned a specific RSV-related ICD-10 code, and coding as a secondary diagnosis further complicates attribution. The use of diagnosis codes may also under-capture frailty and functional decline, which are often undercoded but clinically relevant in older populations.
Second, causality cannot be inferred from the data. It is unclear whether RSV infection was the primary reason for hospitalization or acquired during the hospital stay, particularly in older adults with multiple comorbidities where RSV infection may exacerbate underlying conditions.
Third, outcomes were limited to in-hospital events. Data on post-discharge mortality, functional recovery, or the need for rehabilitation are lacking, likely underestimating the true burden of RSV.
Furthermore, detailed clinical information on chronic pre-existing conditions (e.g., severity, immunosuppression, frailty) was not available. This is particularly relevant for adolescents aged 10-19-years, where a high proportion of severe cases was observed in a small number of patients in this age group, but could not be fully explained.
Lastly, temporal trends may be influenced by changes in testing behavior, coding practices, or healthcare utilization—especially during the COVID-19 pandemic—limiting interpretability across the full 2017–2023 period.
5. Conclusions
In summary, our findings highlight the importance of targeted prevention and management strategies, particularly in pediatric and geriatric populations as well as in individuals with high risk factors such as cardiopulmonary diseases, where the RSV burden is most pronounced. Switzerland authorized several new RSV prevention options more recently. These include the monoclonal antibody Beyfortus® for newborns and high-risk infants, the protein-based vaccines Arexvy® and Abrysvo®, and most recently, the mRNA-based vaccine mRESVIA®, all intended for use in adults aged 60 years and older [35,36,37,38]. In addition, Abrysvo® is also approved for maternal immunization between the 32nd and 36th week of gestation to confer passive protection to newborns against lower respiratory tract infections caused by RSV [37]. Arexvy® recently received a label extension for use in adults aged 50–59 years who are at increased risk of severe RSV disease [36].
In November 2024 the Swiss Federal Office of Public Health (FOPH) issued recommendation for RSV vaccination in individuals aged ≥ 75 years and those at high risk of severe disease ≥ 60 years [39]. However, RSV vaccines have not yet been included in the list of reimbursable vaccinations for this group (“Krankenpflege-Leistungsverordnung”) [40] and have not officially been included in the Swiss vaccination schedule [41].
As a result, RSV vaccination must currently be paid out-of-pocket, which is likely to impair uptake—especially among the elderly population for whom vaccination is recommended. Broader immunization strategies also targeting younger high-risk groups – such as persons with COPD, heart failure, chronic kidney disease, and diabetes mellitus – could further significantly decrease RSV-related hospitalizations, mitigate severe outcomes, and alleviate strain on healthcare resources. A recent Swiss review emphasized the relevance of vaccinations against respiratory infections in patients with chronic lung disease [42].
Future research should aim to identify risk factors for severe RSV progression refining vaccination strategies, and evaluating the health-economic impact of preventive interventions in adult populations.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/doi/s1, Figure S1: Annual RSV-related hospitalizations in Switzerland, 2017-2023, stratified by age group. Figure S2: Absolute number of intensive care admissions, mechanical ventilations, and in-hospital mortality in RSV-related hospitalizations in Switzerland, 2017-2023, stratified by age group. Figure S3: Cases of admission to intensive care unit in % of all RSV-hospitalizations, 2017–2023, stratified by age group. Figure S4: Cases of mechanical ventilation in % of all RSV-hospitalizations, 2017–2023, stratified by age group. Figure S5: In-hospital mortality in % of all RSV-hospitalizations, 2017–2023, stratified by age group. Table S1: The 10 most common additionally coded diagnoses (primary and secondary diagnosis) in RSV-related hospitalizations 2017-2023. Figure S6: Prevalence of additionally coded diagnoses in RSV-related hospitalizations (primary or secondary diagnosis) in children aged 0-9 years in Switzerland, 2017-2023. Analysis focused on chronic comorbidities, severe or frailty-associated conditions. Figure S7: Prevalence of additionally coded diagnoses in RSV-related hospitalizations (primary or secondary diagnosis) in adolescents aged 10-19 years in Switzerland, 2017-2023. Analysis focused on chronic comorbidities, severe or frailty-associated conditions. Table S2: Additionally coded diagnoses in RSV-related hospitalizations in Switzerland, 2017-2023, focusing only on chronic, severe or frailty-associated conditions (ICD-10 diagnosis categories) with threshold frequencies at ≥0.1% in young children (0-9 years), ≥1.0% in adolescent (10-19 years) and adults (≥20 years).
Author Contributions
Conceptualization, N.J.K., D.M.C.-P., J.D.L. and M.B.; methodology, E. D.B.-v.P., N.J.K. and M.B.; formal analysis, N.J.K. and M.B.; investigation, E.B.-v.P.,; data curation, N.J.K. and M.B.; writing—original draft preparation, E.D.B.-v.P., M.B.; writing—review and editing, N.J., N.J.K., D.M.C.-P., G.L.-C., F.J., J.D.L.; visualization, N.J.K., M.B.; supervision, J.D.L. and M.B.. All authors have read and agreed to the published version of the manuscript.
Funding
The costs associated with the processing and provision of data by the FSO as well as publication fees were covered by Moderna.
Institutional Review Board Statement
This study was conducted in accordance with the ethical standards according to the Declaration of Helsinki. Ethical consent was not required, as the data were anonymized and collected as part of routine healthcare operations.
Informed Consent Statement
Patient consent was waived due the sole use of fully anonymized aggregated data.
Data Availability Statement
Data is available from the authors upon reasonable request.
Conflicts of Interest
Nike Julia Kräutler and Daphne McCarthy-Pontier are employees of Moderna and hold stock or stock options in the company. This work was conducted as part of their employment responsibilities. The content reflects the authors' scientific assessment. Jörg Daniel Leuppi has received unrestricted grants from AstraZeneca AG Switzerland, GSK AG Switzerland, OM Pharma SA Switzerland, and Sanofi AG Switzerland. Grant-givers had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. All other authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| COVID-19 | coronavirus disease 2019 |
| FOPH | Federal Office of Public Health |
| FSO | Swiss Federal Statistical Office |
| ICU | intensive care unit |
| LOS | length of hospital stay |
| RSV | respiratory syncytial virus |
| WHO | World Health Organization |
References
- Piralla, A.; Chen, Z.; Zaraket, H. An update on respiratory syncytial virus. BMC Infect Dis. 2023, 23, 734. [Google Scholar] [CrossRef] [PubMed]
- WHO strategy for global respiratory syncytial virus surveillance project based on the influenza platform. Available online: https://www.who.int/publications/i/item/who-strategy-for-global-respiratory-syncytial-virus-surveillance-project-based-on-the-influenza-platform (accessed on 1 September 2025).
- Presser LD, van den Akker WMR, Meijer A, PROMISE Investigators. Respiratory Syncytial Virus European Laboratory Network 2022 Survey: Need for Harmonization and Enhanced Molecular Surveillance. J Infect Dis. 2024, 229 (Suppl. 1), S34–S39. [Google Scholar] [CrossRef] [PubMed]
- von Hammerstein, A.L.; Aebi, C.; Barbey, F.; Berger, C.; Buettcher, M.; Casaulta, C.; et al. Interseasonal RSV infections in Switzerland - rapid establishment of a clinician-led national reporting system (RSV EpiCH). Swiss Med Wkly. 2021, 151, w30057. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, J.M.; Khan, F.; Begier, E.; Swerdlow, D.L.; Jodar, L.; Falsey, A.R. Rates of Medically Attended RSV Among US Adults: A Systematic Review and Meta-analysis. Open Forum Infect Dis. 2022, 9, ofac300. [Google Scholar] [CrossRef]
- Li, Y.; Kulkarni, D.; Begier, E.; Wahi-Singh, P.; Wahi-Singh, B.; Gessner, B.; et al. Adjusting for Case Under-Ascertainment in Estimating RSV Hospitalisation Burden of Older Adults in High-Income Countries: a Systematic Review and Modelling Study. Infect Dis Ther. 2023, 12, 1137–1149. [Google Scholar] [CrossRef]
- Zheng, Z.; Warren, J.L.; Shapiro, E.D.; Pitzer, V.E.; Weinberger, D.M. Estimated incidence of respiratory hospitalizations attributable to RSV infections across age and socioeconomic groups. Pneumonia Nathan Qld. 2022, 14, 6. [Google Scholar] [CrossRef]
- Egeskov-Cavling AM, Johannesen CK, Lindegaard B, Fischer TK, PROMISE Investigators. Underreporting and Misclassification of Respiratory Syncytial Virus-Coded Hospitalization Among Adults in Denmark Between 2015-2016 and 2017-2018. J Infect Dis. 2024, 229 (Suppl. 1), S78–S83. [Google Scholar] [CrossRef]
- Onwuchekwa, C.; Moreo, L.M.; Menon, S.; Machado, B.; Curcio, D.; Kalina, W.; et al. Underascertainment of Respiratory Syncytial Virus Infection in Adults Due to Diagnostic Testing Limitations: A Systematic Literature Review and Meta-analysis. J Infect Dis. 2023, 228, 173–184. [Google Scholar] [CrossRef]
- MUNYWOKIPK; KOECHDC; AGOTICN; KIBIRIGEN; KIPKOECHJ; CANEPA; et al. Influence of age, severity of infection, and co-infection on the duration of respiratory syncytial virus (RSV) shedding. Epidemiol Infect. 2015, 143, 804–812. [Google Scholar] [CrossRef]
- Begley, K.M.; Leis, A.M.; Petrie, J.G.; Truscon, R.; Johnson, E.; Lamerato, L.E.; et al. Epidemiology of Respiratory Syncytial Virus in Adults and Children With Medically Attended Acute Respiratory Illness Over Three Seasons. Clin Infect Dis Off Publ Infect Dis Soc Am. 2024, 79, 1039–1045. [Google Scholar] [CrossRef]
- Chatzis, O.; Darbre, S.; Pasquier, J.; Meylan, P.; Manuel, O.; Aubert, J.D.; et al. Burden of severe RSV disease among immunocompromised children and adults: a 10 year retrospective study. BMC Infect Dis. 2018, 18, 111. [Google Scholar] [CrossRef] [PubMed]
- Khanna, N.; Widmer, A.F.; Decker, M.; Steffen, I.; Halter, J.; Heim, D.; et al. Respiratory syncytial virus infection in patients with hematological diseases: single-center study and review of the literature. Clin Infect Dis Off Publ Infect Dis Soc Am. 2008, 46, 402–412. [Google Scholar] [CrossRef] [PubMed]
- Ivey, K.S.; Edwards, K.M.; Talbot, H.K. Respiratory Syncytial Virus and Associations With Cardiovascular Disease in Adults. J Am Coll Cardiol. 2018, 71, 1574–1583. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, T.M.A.; Donaldson, G.C.; Johnston, S.L.; Openshaw, P.J.M.; Wedzicha, J.A. Respiratory syncytial virus, airway inflammation, and FEV1 decline in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2006, 173, 871–876. [Google Scholar] [CrossRef]
- Wiseman, D.J.; Thwaites, R.S.; Ritchie, A.I.; Finney, L.; Macleod, M.; Kamal, F.; et al. Respiratory Syncytial Virus-related Community Chronic Obstructive Pulmonary Disease Exacerbations and Novel Diagnostics: A Binational Prospective Cohort Study. Am J Respir Crit Care Med. 2024, 210, 994–1001. [Google Scholar] [CrossRef]
- MonAM– Schweizer Monitoring-System Sucht und nichtübertragbare Krankheiten |, F.O.P.H. Available online: https://ind.obsan.admin.ch/en/monam (accessed on 1 September 2025).
- Stucki, M.; Lenzin, G.; Agyeman, P.K.; Posfay-Barbe, K.M.; Ritz, N.; Trück, J.; et al. Inpatient burden of respiratory syncytial virus (RSV) in Switzerland, 2003 to 2021: an analysis of administrative data. Euro Surveill Bull Eur Sur Mal Transm Eur Commun Dis Bull. 2024, 29, 2400119. [Google Scholar] [CrossRef]
- Demografische Bilanz nach Alter. Available online: http://www.pxweb.bfs.admin.ch/pxweb/de/px-x-0102020000_103/px-x-0102020000_103/px-x-0102020000_103.px/ (accessed on 1 September 2025).
- Ison, M.G.; Papi, A.; Athan, E.; Feldman, R.G.; Langley, J.M.; Lee, D.G.; et al. Efficacy and Safety of Respiratory Syncytial Virus (RSV) Prefusion F Protein Vaccine (RSVPreF3 OA) in Older Adults Over 2 RSV Seasons. Clin Infect Dis Off Publ Infect Dis Soc Am. 2024, 78, 1732–1744. [Google Scholar] [CrossRef]
- Ambrosch, A.; Luber, D.; Klawonn, F.; Kabesch, M. Focusing on severe infections with the respiratory syncytial virus (RSV) in adults: Risk factors, symptomatology and clinical course compared to influenza A / B and the original SARS-CoV-2 strain. J Clin Virol Off Publ Pan Am Soc Clin Virol. 2023, 161, 105399. [Google Scholar] [CrossRef]
- Martinón-Torres, F.; Gutierrez, C.; Cáceres, A.; Weber, K.; Torres, A. How Does the Burden of Respiratory Syncytial Virus Compare to Influenza in Spanish Adults? Influenza Other Respir Viruses. 2024, 18, e13341. [Google Scholar] [CrossRef]
- Havers, F.P.; Whitaker, M.; Melgar, M.; Chatwani, B.; Chai, S.J.; Alden, N.B.; et al. Characteristics and Outcomes Among Adults Aged ≥60 Years Hospitalized with Laboratory-Confirmed Respiratory Syncytial Virus - RSV-NET, 12 States, July 2022-June 2023. MMWR Morb Mortal Wkly Rep. 2023, 72, 1075–1082. [Google Scholar] [CrossRef]
- Ackerson, B.; Tseng, H.F.; Sy, L.S.; Solano, Z.; Slezak, J.; Luo, Y.; et al. Severe Morbidity and Mortality Associated With Respiratory Syncytial Virus Versus Influenza Infection in Hospitalized Older Adults. Clin Infect Dis Off Publ Infect Dis Soc Am. 2019, 69, 197–203. [Google Scholar] [CrossRef]
- Leija-Martínez, J.J.; Esparza-Miranda, L.A.; Rivera-Alfaro, G.; Noyola, D.E. Impact of Nonpharmaceutical Interventions during the COVID-19 Pandemic on the Prevalence of Respiratory Syncytial Virus in Hospitalized Children with Lower Respiratory Tract Infections: A Systematic Review and Meta-Analysis. Viruses. 2024, 16, 429. [Google Scholar] [CrossRef]
- Coultas, J.A.; Smyth, R.; Openshaw, P.J. Respiratory syncytial virus (RSV): a scourge from infancy to old age. Thorax. 2019, 74, 986–993. [Google Scholar] [CrossRef]
- Guarnieri, V.; Macucci, C.; Mollo, A.; Trapani, S.; Moriondo, M.; Vignoli, M.; et al. Impact of respiratory syncytial virus on older children: Exploring the potential for preventive strategies beyond the age of 2 years. Vaccine. 2024, 42, 126170. [Google Scholar] [CrossRef] [PubMed]
- Branche, A.R.; Saiman, L.; Walsh, E.E.; Falsey, A.R.; Sieling, W.D.; Greendyke, W.; et al. Incidence of Respiratory Syncytial Virus Infection Among Hospitalized Adults, 2017-2020. Clin Infect Dis Off Publ Infect Dis Soc Am. 2022, 74, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- CDC Respiratory Syncytial Virus Infection (RSV). 2025 [cited 2025 Aug 21]. RSV in Adults. Available online: https://www.cdc.gov/rsv/adults/index.html.
- Abrams, E.M.; Doyon-Plourde, P.; Davis, P.; Lee, L.; Rahal, A.; Brousseau, N.; et al. Burden of disease of respiratory syncytial virus in older adults and adults considered at high risk of severe infection. Can Commun Dis Rep Releve Mal Transm Au Can. 2025, 51, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Bloom, M.W.; Greenberg, B.; Jaarsma, T.; Januzzi, J.L.; Lam, C.S.P.; Maggioni, A.P.; et al. Heart failure with reduced ejection fraction. Nat Rev Dis Primer. 2017, 3, 17058. [Google Scholar] [CrossRef]
- Herold, G. Innere Medizin 2023. Walter de Gruyter GmbH & Co KG; 2022. 1003 p.
- Kytömaa, S.; Hegde, S.; Claggett, B.; Udell, J.A.; Rosamond, W.; Temte, J.; et al. Association of Influenza-like Illness Activity With Hospitalizations for Heart Failure: The Atherosclerosis Risk in Communities Study. JAMA Cardiol. 2019, 4, 363–369. [Google Scholar] [CrossRef]
- Osei-Yeboah, R.; Johannesen, C.K.; Egeskov-Cavling, A.M.; Chen, J.; Lehtonen, T.; Fornes, A.U.; et al. Respiratory Syncytial Virus-Associated Hospitalization in Adults With Comorbidities in 2 European Countries: A Modeling Study. J Infect Dis. 2024, 229 (Suppl. 1), S70–S77. [Google Scholar] [CrossRef]
- Fachinformation Beyfortus. Available online: https://www.swissmedicinfo.ch/ShowText.aspx?textType=FI&lang=DE&authNr=69039 (accessed on 1 September 2025).
- Fachinformation Arexvy. Available online: https://www.swissmedicinfo.ch/ShowText.aspx?textType=FI&lang=DE&authNr=69310 (accessed on 1 September 2025).
- Fachinformation Abrysvo. Available online: https://www.swissmedicinfo.ch/ShowText.aspx?textType=FI&lang=DE&authNr=69691 (accessed on 1 September 2025).
- Fachinformation, m.R.E.S.V.I.A. Available online: https://www.swissmedicinfo.ch/ShowText.aspx?textType=FI&lang=DE&authNr=69995 (accessed on 1 September 2025).
- BAG-Bulletin 47/24: Impfempfehlungen gegen Erkrankungen mit dem Respiratorischen Synzytial-Virus (RSV). Available online: https://backend.bag.admin.ch/fileservice/sdweb-docs-prod-bagadminch-files/files/2025/03/18/7313288a-9ae7-4936-9ac8-6bfcc1756be2.pdf (accessed on 1 September 2025).
- AS 2025 419 - Verordnung des EDI über Leistungen in der obligatorischen Krankenpflegeversicherung (Krankenpflege-Leistungsverordnung, KLV). Available online: https://www.fedlex.admin.ch/eli/oc/2025/419/de (accessed on 1 September 2025).
- Schweizerischer Impfplan 2025. Available online: https://backend.bag.admin.ch/fileservice/sdweb-docs-prod-bagadminch-files/files/2025/06/24/043d49cc-dba5-487f-940d-2aec4b2f4d9f.pdf (accessed on 1 September 2025).
- Boesing, M.; Albrich, W.; Bridevaux, P.O.; Charbonnier, F.; Clarenbach, C.; Fellrath, J.M.; et al. Vaccination in adult patients with chronic lung diseases. Praxis. 2024, 113, 297–305. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



