
Submitted:
10 July 2025
Posted:
11 July 2025
You are already at the latest version
Abstract
Background/Objectives: Previous studies assessing dietary intake have used self-report methods, prone to misreporting. Using researcher-conducted weighed food records, we assessed rural and urban mothers' energy and nutrient intakes and compared them to recommended nutrient intakes (RNIs). Methods: This cross-sectional study was conducted in rural (Asaase Kokoo) and urban (University of Ghana Staff Village) communities. Dietary data were collected from fifty-four mothers (26 rural, 28 urban) on 2 weekdays and 1 weekend day and were analyzed with software, programmed with West African, FNDDS, Kenyan, Ugandan, USDA food composition databases. Results: Mean (SD) ages (years) were 35.8 (11.6) and 44.4 (7.6), and mean energy intakes (kcal) were 2026 (461) and 1669 (385) for rural and urban mothers, respectively. Mean percentage contributions of macronutrients to daily energy intake were within recommended ranges for rural and urban mothers. All participants met or exceeded vitamin A RNI, irrespective of location. While all rural mothers met or exceeded iron RNI, some urban mothers (14.3%) did not. Few rural (7.7%) and urban mothers (10.7%) did not meet zinc RNI. About half of rural (46.2%) and urban mothers (53.6%) did not meet folate RNI. Most rural (96.1%) and urban mothers (92.8%) met or exceeded fiber RNI. Conclusions: Overall, rural mothers had higher energy and nutrient intakes than urban mothers. While most met RNIs, there were some micronutrient inadequacies, particularly folate, where almost half of rural and urban mothers consumed below RNI. Our findings indicate the need for tailored interventions to prevent nutrient deficiencies or excesses in Ghanaian mothers.
Keywords:
mothers
; recommended nutrient intake
; dietary assessment
; weighed food records
; Ghana
1. Introduction
Malnutrition exists in different forms, including overnutrition (overweight and obesity) and undernutrition (underweight, stunting, wasting, and micronutrient deficiencies) [1]. Over the past decade, the prevalence of overweight and obesity have increased significantly among women in low- and middle-income countries (LMICs) [2]. Micronutrient deficiencies thrive in many countries across the globe, with LMICs bearing the greatest burden because of factors such as inadequate food and nutrient intake, low dietary diversity, food insecurity, and sociocultural and geographical factors [3,4,5]. Likewise, the prevalence of overweight and obesity are on ascendancy in Ghana, while deficiencies in vitamin A, folate, iron, and zinc remain significant public health concerns [6,7]. Among Ghanaian women, the prevalence of overweight and obesity have been reported to be higher in urban areas (45.8%) than in rural areas (25.3%) [8,9]. Higher prevalence of overweight and obesity, alongside micronutrient deficiencies, were reported among some Ghanaian women [10,11]. To address malnutrition and its associated health implications, the government of Ghana has implemented various intervention strategies, including weight management programs, salt iodization, micronutrient supplementation, wheat flour fortification, and the use of micronutrient powder sprinkles [12,13,14]. However, despite these efforts, micronutrient deficiencies persist, and the prevalence of overweight and obesity continue to increase, particularly in urban populations and among women [6,7].
There is currently a dearth of information on the dietary intake of mothers in rural and urban communities of Ghana. Few studies that have assessed dietary intake in the Ghanaian population have relied on self-report methods, such as the 24-hour dietary recall [15,16] and food frequency questionnaire [17,18]. However, findings from these self-report dietary assessment methods have been conflicting. Compared to weighed food records, while one study reported that the 24-hour dietary recall underestimated energy and nutrient intakes [19], another study observed that the 24-hour dietary recall overestimated intakes [20]. Additionally, a study found that the food frequency questionnaire overestimated nutrient intake compared to the weighed food records [21]. These inconsistencies indicate that self-report methods are prone to misreporting, highlighting the need for more accurate dietary assessment tools. To the best of our knowledge in the literature, no study has used researcher-conducted weighed food records (rWFR), considered the gold standard for dietary assessment to assess dietary intake in rural and urban mothers at the household level in Ghana. Therefore, we assessed the energy and nutrient intakes (protein, fat, carbohydrate, fiber, vitamin A, folate, iron, and zinc) of rural and urban mothers using rWFR, and compared them to the World Health Organization (WHO)’s recommended nutrient intakes (RNIs) [22,23]. The selected micronutrients were chosen due to their significant public health concerns in Ghana. We also compared the percentage contributions of protein, fat, and carbohydrate to the total daily energy intake against the recommended ranges [22]. We hypothesized that the daily energy intake of rural and urban mothers would exceed the RNIs, with a higher energy intake expected in urban mothers than in rural mothers. We anticipated that the daily intakes of fiber, vitamin A, folate, iron, and zinc among rural and urban mothers would fall below the RNIs and that the percentage contributions of protein, fat, and carbohydrate to daily energy intake would fall within the recommended ranges. This study was part of a larger research project to validate passive innovative technologies for dietary assessment in LMICs [24].
2. Materials and Methods
2.1. Study Design, Eligibility Criteria, and Sample Size
This cross-sectional study was conducted in rural and urban communities of Ghana, targeting mothers in selected households. For the rural community, Asaase Kokoo in the Akuapem North Municipal Assembly in the Eastern Region was selected, while the University of Ghana Staff Village in the Greater Accra Region was the urban community. As part of the larger research project, per the study protocol, eligibility included household having a mother, father, and an index child (adolescent and/or child under 5 years of age) residing in the same household and consuming most of their meals at home. The full methodology and eligibility criteria are described elsewhere [24]. Purposive sampling was used to select 60 households (30 in rural and 30 in urban), with the assistance of community leaders in identifying eligible households. Household members who showed interest in participating in the study either signed or thumb-printed informed consent forms.
2.2. Data Collection
Data collection was done by field staff in households. All field staff were multi-lingual (spoke English and at least one other local language) to facilitate effective communication with participants from diverse ethnic backgrounds in rural and urban communities. Field staff also had at least a bachelor’s degree in nutritional sciences and were trained in standardized protocols and interviewing techniques to ensure accurate data collection. In rural households, data collection began in November 2020 and continued until the end of February 2021, with a break for the Christmas holidays. In urban households, data collection began in March 2021 and ended in May 2021, with a break for the Easter holidays.
On a typical day of data collection, two field staff arrived at the household early in the morning. Upon arrival, the field staff verified that no foods or beverages had been consumed. They remained nearby so as not to interfere with the normal daily activities of the household, but responded to calls from participants. During food preparation and consumption, the field staff were invited into the household to weigh all raw food ingredients (recipes) that were used to prepare meals, snacks, and portions to be consumed. Foods and beverages consumed by the mother alone, as well as leftovers, and those shared with other household members, were weighed and recorded on record sheets. The identities of individuals who shared foods and beverages with the mother in the household during meal-sharing and eating events were also recorded. Foods and beverages purchased from food vendors outside of the home and consumed at home by the mother were weighed and recorded.
2.3. Socio-Demographic Data and Anthropometric Measurement
In addition to dietary intake assessment in the household, the mother participated in a brief interview to complete a survey on the household’s socio-demographic characteristics. The mother’s weight and height were measured using a Seca 769 digital column weighing scale equipped with a stadiometer (Hammer Steindamm, Hamburg, Germany). Height was measured in centimeters, while weight was measured in kilograms, following standard protocol (participants wearing full clothing with no heavy accessories on their bodies and standing upright without shoes on the scale for height and weight measurements the morning of a study day). The measured height and weight were used to calculate body mass index (BMI) (kg/m2). BMI values were categorized according to WHO’s weight classification criteria for adults [25]: < 18.5 kg/m2 as underweight, 18.5 – 24.9 kg/m2 as normal weight, 25.0 – 29.9 kg/m2 as overweight, and ≥ 30.0 kg/m2 as obese. After dinner, when all food preparation and consumption activities were completed for the day, the field staff departed from the home. All data collected were reviewed independently by the project coordinator, who was not directly involved in the data collection process at the household level. Finally, the data were uploaded to the database (password-protected cloud space) of the larger research project.
2.4. Nutritional Analysis
Foods and beverages consumed by the mother alone and those shared with other household members were recorded separately and analyzed by one analyst trained in portion size estimation and database item selection using custom AIM annotation software [26]. The software was programmed with the West African, Food and Nutrient Database for Dietary Studies (FNDDS), Kenyan, Ugandan, and the United States Department of Agriculture (USDA) food and nutrient composition databases. The software provided simultaneous access to all five food and nutrient composition databases, but a prioritization was set to use them in the order stated above. A recipe calculation (informed by the ingredients used for meal or beverage preparation) approach was used to analyze foods and beverages that were not directly present in the food composition databases programmed into the software. With this approach, the ingredients in recipe preparation served as a guide in estimating the proportions of ingredients (all ingredients or suitable substitutes were present in the food and nutrient databases used), and the corresponding quantity of dish consumed by the mother.
For analysis of foods and beverages shared with other household members, standardized ratios (1:1 for a mother and father sharing a meal, 3:2 for a mother and adolescent sharing a meal, and 3:1 for a mother and child under five years sharing a meal) were assigned to the mother and each household member who shared in the eating of the specific meal or beverage to estimate the amount of food or beverage consumed by each person and, subsequently, the portion size consumed by the mother [27]. Once each food or beverage item and portion consumed by the mother was entered into the software, it calculated the energy and nutrient content for each food/beverage item, by eating occasion, and for the whole day.
2.5. Calculations and Statistical Analysis
Statistical analysis was conducted using IBM SPSS Software 29.0 (Armonk, NY). Among the 60 mothers who participated in the study, dietary intake data were incomplete or missing for 4 mothers in rural households and 2 mothers in urban households. Therefore, the data presented in this paper are for 26 rural mothers and 28 urban mothers. Socio-demographic and anthropometric data were analyzed using descriptive statistics. Three-day mean daily energy and nutrient intakes of mothers were calculated by averaging the daily intakes from the nutritional analysis over the three days. The mean daily energy and nutrient intakes of rural versus urban mothers were compared using independent sample t-tests, while one-sample t-tests were used to compare intakes to RNIs. The z-scores for mean daily energy, fiber, vitamin A, iron, folate, and zinc intakes were computed relative to RNIs and were used to determine the percentages of rural and urban mothers who fell below, met, or exceeded the RNIs. Mothers with mean z-scores between -1 and +1 were designated as having met the recommended intakes, mean z-scores above +1 indicated intake exceeded the recommendation, while below -1 indicated intake that fell below the recommendation [28]. Pearson correlation and regression analyses were performed to assess the strength of the association between energy intake and BMI of rural and urban mothers.
2.6. Recommended Energy and Nutrient Intakes
The 3-day mean was calculated for each individual. Group mean daily energy, protein, fat, carbohydrate, fiber, vitamin A, folate, iron, and zinc intakes, as well as the percentage contributions of macronutrients, were compared to the RNIs as outlined in the handbooks of WHO’s recommended energy and nutrient intakes [22,23]. The ages and BMI of rural and urban mothers, and a moderate physical activity level (based on the Ghana Health Service report [29] on the normal activity level of adult Ghanaian women) were used to determine the recommended energy and nutrient intakes from the handbooks for the participants.
3. Results
Rural mothers were younger than urban mothers: 35.8 (11.6) vs 44.4 (7.6) years (p = 0.002), but did not differ in BMI (28.2 (5.5) for rural and 28.2 (5.1) kg/m2 for urban, p = 0.871). Among rural mothers, 30.8% (n = 8) were normal weight, 34.6% (n = 9) overweight, and 34.6% (n = 9) obese, while in urban mothers, 32.1% (n = 9) were normal weight, 32.1% (n = 9) overweight, and 35.7% (n = 10) obese.
The mean (SD) percentage of protein, fat, and carbohydrate contributions to total daily energy in rural versus urban mothers were as follows: protein 13.1 (2.1) vs 13.7 (2.8) % (p = 0.169); fat 21.9 (6.1) vs 25.3 (6.7) % (p = 0.029); carbohydrate 62.4 (6.9) vs 59.2 (8.3) % (p = 0.063), which were all within the recommended ranges (protein = 10.0 to 15.0 %), fat = 15.0 to 30.0 %, and carbohydrate = 55.0 to 75.0 %) [22].
Energy intake was positively associated with BMI in rural and urban mothers (Figure 1). Pearson’s correlation coefficients indicated a stronger relationship in rural mothers (r = 0.77, 95% CI: 0.55, 0.89) compared to urban mothers (r = 0.58, 95% CI: 0.26, 0.78). Linear regression analysis further confirmed this association, indicating that for every 1 kcal higher in energy intake, BMI was higher by 0.009 kg/m2 in rural mothers (β = 0.009, SE = 0.002, R2 = 0.593, p < 0.001) and by 0.008 kg/m2 in urban mothers (β = 0.008, SE = 0.002, R2 = 0.334, p = 0.001).
Table 1 presents rural and urban mothers’ mean daily energy and nutrient intakes. Overall, the mean intakes of rural mothers were higher than urban mothers, with no significant difference observed for most nutrients, apart from energy (p = 0.002), protein (p = 0.040), carbohydrate (p < 0.001), and iron (p = 0.004).
Mean daily intakes exceeded the RNIs for all nutrients examined, except for mean energy in urban mothers and mean folate in both rural and urban mothers, which were below the RNIs (Figure 2).
Table 2 while all rural mothers met or exceeded the RNI for iron, a few urban mothers fell below the RNI. About half of rural and urban mothers did not meet the RNI for folate from their diet. A few rural and urban mothers did not meet the RNIs for zinc and fiber. All rural and urban mothers met or exceeded the RNIs for vitamin A.
4. Discussion
We compared the energy and nutrient intakes of rural and urban mothers to WHO’s recommended nutrient intakes using the gold-standard dietary assessment method of rWFR. Our most important findings were that rural mothers, on average, consumed more energy than their urban counterparts, and energy intakes in rural and urban mothers were positively associated with BMI. The percentage contributions of protein, fat, and carbohydrate to daily energy intake in rural and urban mothers were within the recommended ranges. While most mothers met the RNIs for most nutrients, some did not, and disparities were observed between rural and urban mothers. Specifically, about half of rural and urban mothers did not meet the RNI for folate, indicating that dietary sources alone may be insufficient to meet their daily folate needs.
In Ghana, studies assessing dietary intake in populations have primarily used the 24-hour dietary recall [15,16] and food frequency questionnaire methods [17,18]. Although these self-report methods are simple, less expensive, and more convenient to use, they are prone to misreporting [30,31,32,33]. While in one study, the 24-hour dietary recall significantly underestimated energy and nutrient intakes compared to weighed food records [19], the food frequency questionnaire overestimated intakes compared to the weighed food records in another study [21]. We observed a positive association between energy intake and BMI in both rural and urban mothers, consistent with the findings of a previous study [34]. In contrast, underreported energy intake from the 24-hour dietary recall showed a weaker association with BMI [16]. Another study observed a spurious association when misreporters were included in the analysis of energy intake and its association with BMI [35]. However, after excluding the misreporters from the analysis, a positive association with BMI emerged, suggesting that misreporting energy intake can distort the relationship between energy intake and BMI. While the rWFR method used in our study provided a more accurate estimation of energy and nutrient intake, it is not feasible for assessing dietary intake in large-scale studies because it is expensive, labor-intensive, time-consuming, and intrusive [30]. This underscores the need for other objective, less intrusive and burdensome dietary assessment methods, including passive technologies for dietary intake assessment in the Ghanaian population, as they have the potential to objectively assess dietary intake in free-living individuals with less respondent burden and improved accuracy [24].
Our finding that about one-third of rural and urban mothers had a BMI in the obese category is consistent with a study that estimated the prevalence of obesity among Ghanaian women to be 35.5% [9]. As reviewed previously, the prevalence of obesity has been shown to be higher in women than men, higher in urban areas than rural areas, and rapidly increasing in rural areas compared to previous years [36]. Surprisingly, we observed that rural mothers consumed more energy compared to urban mothers. The higher intake in rural mothers is consistent with the rapid increase in overweight and obesity reported in rural areas compared to urban areas in Ghana. However, this observation likely also reflects differences in physical activity levels in rural vs urban areas and may in part be attributable to farming being the primary occupation of most rural women, compared to urban women typically engaging in blue-collar jobs that are less labor-intensive and therefore, requiring less energy intake to support [37,38]. Additionally, rural women are often more involved in household chores, which require a higher energy expenditure, compared to urban women [37,38]. While energy intake in excess of expenditure is a significant contributor to the obesity pandemic, urbanization and nutrition transition have been reported as key drivers of the increasing prevalence of obesity among women in Ghana [39]. Consequently, obesity has been linked to chronic diseases, such as gestational diabetes, cardiovascular diseases, and hypertension in Ghanaian women [40,41,42]. The government of Ghana must prioritize strategies to curb urbanization and promote physical activity through healthy community planning to address the growing burden of obesity and associated chronic diseases among Ghanaian women.
Traditional Ghanaian foods are typically prepared from starchy staple foods (main sources of calories), accompanied by any protein of choice (beef, poultry, fish, eggs, etc.), and consumed with different types of soups and stews (prepared from vegetables) [43,44]. Most of these traditional Ghanaian foods are excellent sources of fiber and vitamin A because of the minimal use of processed food ingredients in their preparation [43,44]. Our finding that all rural and urban mothers met the recommended intake for vitamin A, with few rural and urban mothers not meeting the recommended fiber intake, suggests that traditional Ghanaian foods are indeed rich sources of vitamin A and fiber. Adequate consumption of fiber has several health benefits, such as reducing the risk of obesity, improving glycemic control and insulin sensitivity, and reducing the risk of type 2 diabetes and certain cancers [45]. Promoting adequate fiber intake could potentially play an essential role in preventing chronic diseases and enhancing the overall health and well-being of Ghanaian women.
All rural mothers met the recommended iron intake, but some urban mothers did not. This could partly be due to the diversity in dietary patterns in rural versus urban areas. In Ghana, rural residents usually grow iron-rich leafy green vegetables, such as kontomire (taro leaves), typically harvested fresh for cooking, and raise livestock (e.g., cattle, goats, poultry & pork) for household consumption [46,47]. This ensures a more consistent supply of fresh iron-rich foods that contribute to higher iron intake in rural areas than in urban areas, where residents may rely on more processed and fast foods, which are usually lower in essential micronutrients like iron [48,49]. Zinc intake was adequate in most rural and urban mothers however, higher prevalence of zinc and iron deficiencies have previously been reported among some Ghanaian women [10,11,50]. Therefore, dietary practices that promote adequate intake of zinc and iron, such as promoting regular consumption of traditional or fortified foods rich in these nutrients and the use of micronutrient supplements, must be encouraged in Ghanaian women to reduce the risk of deficiencies.
We found that about half of both rural and urban mothers did not meet the recommended folate intake. This indicates that foods consumed by mothers may have low folate content, consistent with a study that observed that some Ghanaian traditional foods contributed poorly to the daily folate needs of women [51]. A high prevalence of folate deficiency has been reported in Ghanaian women [13], and low birth weights, premature births, and neural tube defects have been documented as associated health consequences [52,53]. Higher prevalence of neural tube defects, such as myelomeningocele, meningocele, and cranium bifida, have been reported in some rural and urban areas in Ghana [54,55]. This calls for interventions that encourage, particularly, women of childbearing age to consume folic acid-fortified foods and supplements to minimize the risk associated with inadequate folate intake. Although some interventions have been implemented by the government of Ghana to prevent micronutrient deficiencies in the Ghanaian population, our findings indicate the need to prioritize strategies aimed at intensifying folic acid supplementation in women in rural and urban areas of Ghana because it appears diet alone may not be sufficient to meet their daily recommended folate intake.
A major strength of our study is the use of the rWFR method, considered the gold standard for dietary intake assessment. We measured the dietary intake of mothers on two weekdays and one weekend day to account for day-to-day variations in dietary intake, which provided a more comprehensive view of their usual dietary intakes. Variations in the dietary intake of mothers based on their geographical location were also examined. However, we acknowledge that the study had some limitations. The sample size was small; the study was done in only two communities (1 rural and 1 urban); therefore, our findings may not be generalizable to all rural and urban communities in Ghana. Additionally, seasonal variations could affect the dietary intake of rural and urban mothers, especially energy intake, thereby also limiting the generalizability of our findings.
5. Conclusions
We observed that rural mothers consumed more energy than urban mothers. The daily energy intakes of rural and urban mothers were positively associated with BMI. The percentages of protein, fat, and carbohydrate contributing to the daily energy intake of rural and urban mothers were all within recommended ranges. Overall, most rural and urban mothers met or exceeded the recommended micronutrient intakes, apart from folate. Our findings indicate that dietary sources alone may be inadequate to meet the micronutrient needs of some Ghanaian women, particularly folate. Micronutrient supplementation, especially folic acid for women of childbearing age, and food fortification programs in Ghana must be expanded and made more accessible to a wider population in rural and urban communities. Additionally, nutrition programs aimed at promoting dietary diversity and increasing fruit and vegetable consumption must be intensified to reduce the risk of micronutrient deficiencies and improve the health and overall well-being of women in Ghana.
Author Contributions
The study was conceived by AKA, MAM, MSA, ES, GF, and BL. CAD was involved in data collection. Nutritional analysis was done by PKO. PKO wrote the initial draft of the manuscript, which was reviewed, and inputs were provided by all co-authors. All co-authors read and approved the final manuscript for publication.
Funding
This research was funded by the Bill & Melinda Gates Foundation (Grant No. INV-006713) and the Georgia Agricultural Experiment Station (Grant No. GEO00701).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Human Subjects Institutional Review Board of the University of Georgia (STUDY00006121) and the Institutional Review Board Committee of the Noguchi Memorial Institute for Medical Research at the University of Ghana (#-046/18-19).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Dataset available on request from the authors.
Acknowledgments
The authors are thankful to the field staff, community leaders, and the mothers who participated in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Dukhi, N. Global prevalence of malnutrition: evidence from literature. Malnutrition. 2020, 1, 1-6. [CrossRef]
- Azeez TA. Obesity in Africa: the challenges of a rising epidemic in the midst of dwindling resources. Obes Medicine. 2022, 13-22. [CrossRef]
- World Health Organization. Micronutrient deficiencies. Available online: https://www.who.int/health-topics/micronutrients. (Accessed on 10th June 2025).
- Liu, J.; Qi, X.; Wang, X.; Qin, Y.; Jiang, S.; Han, L.; Kang, Z.; Shan, L.; Liang, L.; Wu, Q. Evolving Patterns of Nutritional Deficiencies Burden in Low- and Middle-Income Countries: Findings from the 2019 Global Burden of Disease Study. Nutrients. 2022, 14, 9-31. [CrossRef]
- Baldi, A.; Pasricha, S.R. Anemia: Worldwide Prevalence and Progress in Reduction in Nutritional Anemia. Springer. 2022, 3-17. [CrossRef]
- Rohner, F.; Tanumihardjo, S.; Steiner-Asiedu, M.; Williams, T. N.; Wirth, J. P.; Petry, N.; Woodruff, B.A. Revised Survey Protocol: Ghana Micronutrient Survey. 2017. (GMS 2017). Available online: https://osf.io/vk53j/download.
- Ofori-Asenso, R.; Agyeman, A. A.; Laar, A.; Boateng, D. Overweight and Obesity epidemic in Ghana - a systematic review and meta-analysis. BMC Public Health. 2016, 16, 1-18. [CrossRef]
- Asosega, K.A.; Adebanji, A.O.; Abdul, I.W. Spatial analysis of the Prevalence of Obesity and Overweight among women in Ghana. BMJ Open. 2021, 11(1), 3-21. [CrossRef]
- Asosega, K. A.; Aidoo, E. N.; Adebanji, A. O.; Owusu-Dabo, E. (2023). Examining the risk factors for Overweight and Obesity among women in Ghana: A multilevel perspective. Heliyon. 2023, 9(5), 2-14. [CrossRef]
- Christian, A.K.; Steiner-Asiedu, M.; Bentil, H.J.; Rohner, F.; Wegmüller, R.; Petry, N.; Wirth, J.P.; Donkor, W.E.S.; Amoaful, E.F.; Adu-Afarwuah, S. Co-Occurrence of Overweight/Obesity, Anemia and Micronutrient Deficiencies among Non-Pregnant Women of Reproductive Age in Ghana: Results from a Nationally Representative Survey. Nutrients. 2022, 14, 1427. [CrossRef]
- Kushitor, S.B.; Owusu, L.; Kushitor, M.K. The prevalence and correlates of the double burden of malnutrition among women in Ghana. Plos one. 2022, 15(12), 3-15. [CrossRef]
- Kyei-Arthur, F.; Situma, R.; Aballo, J.; Mahama, A.B.; Selenje, L.; Amoaful, E.; Adu-Afarwuah, S. Lessons learned from implementing the pilot Micronutrient Powder Initiative in four districts in Ghana. BMC Nutr. 2020, 6, 1-13. [CrossRef]
- Wegmüller, R.; Bentil, H.; Wirth, J.P.; Petry, N.; Tanumihardjo, S.A.; Allen, L.; Williams, T.N.; Selenje, L.; Mahama, A.; Amoaful, E.; Steiner-Asiedu, M. Anemia, micronutrient deficiencies, malaria, hemoglobinopathies and malnutrition in young children and non-pregnant women in Ghana: Findings from a national survey. PloS one. 2020, 15(1), p.e0228258. [CrossRef]
- Sakyi, S.A.; Antwi, M.H.; Ahenkorah, F.L.; Laing, E.F.; Ephraim, R.K.D.; Kwarteng, A.; Amoani, B.; Appiah, S.C.; Oppong Afranie, B.; Opoku, S. et al. Vitamin D deficiency is common in Ghana despite abundance of sunlight: a multicentre comparative cross-sectional study. J Nutr Metab. 2021, 1, 12-31. [CrossRef]
- Wiafe, M.A.; Apprey, C.; Annan, R.A. Dietary Diversity and Nutritional Status of Adolescents in Rural Ghana. Nutr Metab Insights. 2023, 16, 117-28. [CrossRef]
- Asare, J.; Lim, J.J.; Amoah, J. Low Dietary Diversity and Low Haemoglobin Status in Ghanaian Female Boarding and Day Senior High School Students: a cross-sectional study. Medicina. 2024, 60(7), 11-23. [CrossRef]
- Abizari, A.R.; Ali, Z. Dietary patterns and associated factors of schooling Ghanaian adolescents. J Health Popul Nutr. 2019, 38(1), 105-13. [CrossRef]
- Galbete, C.; Nicolaou, M.; Meeks, K.A.; de-Graft Aikins, A.; Addo, J.; Amoah, S.K.; Smeeth, L.; Owusu-Dabo, E.; Klipstein-Grobusch, K.; Bahendeka, S. et al. Food consumption, nutrient intake, and dietary patterns in Ghanaian migrants in Europe and their compatriots in Ghana. Food and Nutr Res. 2017, 12-23. [CrossRef]
- Gelli, A.; Nwabuikwu, O.; Bannerman, B.; Ador, G.; Atadze, V.; Asante, M.; Bempong, S.; McCloskey, P.; Nguyen, P.H.; Hughes, D. et al. Computer vision–assisted dietary assessment through mobile phones in female youth in urban Ghana: validity against weighed records and comparison with 24-h recalls. Am J of Clin Nutr. 2024, 120(5), 1105-13. [CrossRef]
- Folson, G.K., Bannerman, B., Atadze, V., Ador, G., Kolt, B., McCloskey, P., Gangupantulu, R., Arrieta, A., Braga, B.C., Arsenault, J. et al. Validation of mobile artificial intelligence technology–assisted dietary assessment tool against weighed records and 24-hour recall in adolescent females in Ghana. J of Nutr. 2023, 153(8), 2328-38. [CrossRef]
- Kowalkowska, J.; Slowinska, M.A.; Slowinski, D.; Dlugosz, A.; Niedzwiedzka, E.; Wadolowska, L. Comparison of a Full Food-Frequency Questionnaire with the Three-Day Unweighted Food Records in Young Polish Adult Women: Implications for Dietary Assessment. Nutrients. 2013, 5, 2747-2776. [CrossRef]
- Human Energy Requirements. Report of a Joint FAO/WHO/UNU Expert Consultation Rome. Available online: https://www.fao.org/4/y5686e/y5686e00.htm (Accessed on 12th January 2025).
- World Health Organization. Vitamin and Mineral Requirements in Human Nutrition. Available online: https://www.who.int/publications/i/item/9241546123. (Accessed on 12th January 2025).
- Jobarteh, M.L.; McCrory, M.A.; Lo, B.; Sun, M.; Sazonov, E.; Anderson, A.K.; Jia, W.; Maitland, K.; Qiu, J.; Steiner-Asiedu, M. et al. Development and validation of an objective, passive dietary assessment method for estimating food and nutrient intake in households in low-and middle-income countries: A study protocol. Curr Dev Nutr. 2020, 4(2), 3-19. [CrossRef]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. (Accessed on 11th April 2025).
- Ghosh, T.; McCrory, M.A.; Marden, T.; Higgins, J.; Anderson, A.K.; Domfe, C.A.; Jia, W.; Lo, B.; Frost, G.; Steiner-Asiedu, M. et al. I2N: image to nutrients, a sensor-guided semi-automated tool for annotation of images for nutrition analysis of eating episodes. Front Nutr. 2023, 10, 3-21. [CrossRef]
- Domfe, C.A.; McCrory, M.A.; Sazonov, E.; Ghosh, T.; Raju, V.; Frost, G.; Steiner-Asiedu, M.; Sun, M.; Jia, W.; Baranowski, T. et al. Objective assessment of shared plate eating using a wearable camera in urban and rural households in Ghana. Front Nutr. 2024, 11, 4-11. [CrossRef]
- Wilson, T.A.; Adolph, A.L.; Butte, N.F. Nutrient Adequacy and Diet Quality in Non-Overweight and Overweight Hispanic Children of Low Socioeconomic Status: The Viva la Familia Study. J Am Diet Assoc. 2009, 109(6), 1012-21. [CrossRef]
- Ghana Steps Report. Nationwide Non-Communicable Diseases Risk Factors Assessment Using the World Health Organization’s Stepwise Approach in Ghana. Available online: https://www.afro.who.int/sites/default/files/2024-11/ghana%20steps%20report%202023. (Accessed on 12th February 2025).
- Block, G.; Hartman, A.M. Dietary assessment methods. In Nutrition and Cancer Prevention. CRC Press. 2021, 1, 159-180. [CrossRef]
- Gibson, R.S.; Charrondiere, U.R.; Bell, W. Measurement errors in dietary assessment using self-reported 24-hour recalls in low-income countries and strategies for their prevention. Advances in Nutr. 2017, 8(6), 980-91. [CrossRef]
- Kirkpatrick, S.I.; Guenther, P.M.; Durward, C.; Douglass, D.; Zimmerman, T.P.; Kahle, L.L.; Atoloye, A.T.; Marcinow, M.L.; Savoie-Roskos, M.R., Herrick, K.A. et al. The accuracy of portion size reporting on self-administered online 24-hour dietary recalls among women with low incomes. J of the Aca of Nutr and Dietetics. 2022, 122(12), 2243-2256. [CrossRef]
- Rossato, S.L.; Fuchs, S.C. Handling random errors and biases in methods used for short-term dietary assessment. Revista de saude publica. 2014, 845-50. [CrossRef]
- Murakami, K. Nutritional quality of meals and snacks assessed by the Food Standards Agency nutrient profiling system in relation to overall diet quality, body mass index, and waist circumference in British adults. Nutr J. 2017, 16, 101-22. [CrossRef]
- Huang, T.T.K.; Roberts, S.B.; Howarth, N.C.; McCrory, M.A. Effect of screening out implausible energy intake reports on relationships between diet and BMI. Obes Res. 2005, 13(7), 1205-17. [CrossRef]
- Agyemang, C.; Kushitor, S.B.; Afrifa-Anane, G.F. Obesity in Africa: A Silent Public Health Crisis. Metabolic Syndrome: A Comprehensive Textbook: Springer. 2024, 47-64. [CrossRef]
- Owoo, N.S.; Lambon-Quayefio, M.P. Mixed methods exploration of Ghanaian women’s domestic work, childcare and effects on their mental health. PLoS One. 2021, 16(2), 2-19. [CrossRef]
- de Jager, I.; van de Ven, G.W.J.; Giller, K.E. Seasonality and nutrition-sensitive farming in rural Northern Ghana. Food Secur. 2023, 15(2), 381-94. [CrossRef]
- Rousham, E.K.; Pradeilles, R.; Akparibo, R.; Aryeetey, R.; Bash, K.; Booth, A.; Muthuri, S.K.; Osei-Kwasi, H.; Marr, C.M.; Norris, T. Dietary behaviours in the context of nutrition transition: a systematic review and meta-analyses in two African countries. Public Health Nutr 2020, 23(11), 1948-64. [CrossRef]
- Niyi, J.L.; Li, Z.; Zumah, F. Association between Gestational Weight Gain and Maternal and Birth Outcomes in Northern Ghana. BioMed Res Int. 2024, 11-29. [CrossRef]
- Hamid, S.; Groot, W.; Pavlova, M. Trends in cardiovascular diseases and associated risks in sub-Saharan Africa: a review of the evidence for Ghana, Nigeria, South Africa, Sudan, and Tanzania. The aging male. 2019, 22(3), 169-76. [CrossRef]
- Acheampong, K.; Nyamari, J.M.; Ganu, D.; Appiah, S.; Pan, X.; Kaminga, A.; Liu, A. Predictors of hypertension among adult female population in Kpone-Katamanso District, Ghana. Int J of hypertension. 2019, 11-23. [CrossRef]
- Appiah, C.A.; Samwini, A.M.; Brown, P.K.; Hayford, F.E.A.; Asamoah-Boakye, O. Proximate composition and serving sizes of selected composite Ghanaian soups. Afr J Food, Agric Nutr Dev. 2020, 20(3), 22-43. [CrossRef]
- Eyeson, K.; Ankrah, E. Composition of foods commonly used in Ghana: Council for Scientific and Industrial Research (CSIR). Food Res. 2001, 3-12. [CrossRef]
- Waddell, I.S.; Orfila, C. Dietary fiber in the prevention of obesity and obesity-related chronic diseases: From epidemiological evidence to potential molecular mechanisms. Crit Rev Food Sci Nutr. 2022, 1-16. [CrossRef]
- Nti CA (2008) Household dietary practices and family nutritional status in rural Ghana. Nutr Res Pract. 2008, 2(1), 35-40. [CrossRef]
- Osei, P.K.; McCrory, M.A.; Steiner-Asiedu, M.; Sazonov, E.; Sun, M.; Jia, W.; Baranowski, T.; Frost, G.; Lo, B.; Anderson, A.K. Food-related behaviors of rural (Asaase Kooko) and peri-urban (Kaadjanor) households in Ghana. Frontiers in Nutr. 2025, 12, 2-13. [CrossRef]
- Kushitor, S.B.; Alangea, D.O.; Aryeetey, R.; de-Graft Aikins, A. Dietary patterns among adults in three low-income urban communities in Accra, Ghana. Plos one. 2023, 18(11), p.e0293726. [CrossRef]
- Hiamey, S.E.; Hiamey, G.A. Street food consumption in a Ghanaian Metropolis: the concerns determining consumption and non-consumption. Food Control. 2018, 92, 121-7. [CrossRef]
- Ayensu, J.; Annan, R.; Lutterodt, H.; Edusei, A.; Peng, L.S. Prevalence of anaemia and low intake of dietary nutrients in pregnant women living in rural and urban areas in the Ashanti region of Ghana. PLoS One. 2020, 15(1), 2-16. [CrossRef]
- Dass, M.; Nyako, J.; Tortoe, C.; Fanou-Fogny, N.; Nago, E.; Hounhouigan, J.; Berger, J.; Wieringa, F.; Greffeuille, V. Comparison of micronutrient intervention strategies in Ghana and Benin to cover micronutrient needs: simulation of benefits and risks in women of reproductive age. Nutrients. 2021, 13(7), 9-19. [CrossRef]
- Imbard, A.; Benoist, J-F.; Blom, H.J. Neural tube defects, folic acid, and methylation. Int J Environ Res Public Health. 2013, 10(9), 10-26. [CrossRef]
- Barua, S.; Kuizon, S.; Junaid, M.A. Folic acid supplementation in pregnancy and implications in health and disease. J Biomed Sci. 2014, 21, 1-9. [CrossRef]
- Alhassan, A.; Adam, A.; Nangkuu, D. Prevalence of neural tube defect and hydrocephalus in Northern Ghana. J Med Biomed Sci. 2017, 6(1), 18-23. [CrossRef]
- Ankwah, Y.K.; Larbie, C.; Genfi, A.K.A. Assessing the prevalence and risk factors of neural tube defects at a tertiary hospital in Ghana. Int J Child Health Hum Dev. 2022, 15(2), 193-203. Available online: https://www.proquest.com/scholarly-journals/assessing-prevalence-risk-factors-neural-tube/docview/2779948796/se-2?accountid=14537. (Accessed on 10th January 2025).
Figure 1.
Associations between energy intake and body mass index of rural and urban mothers.
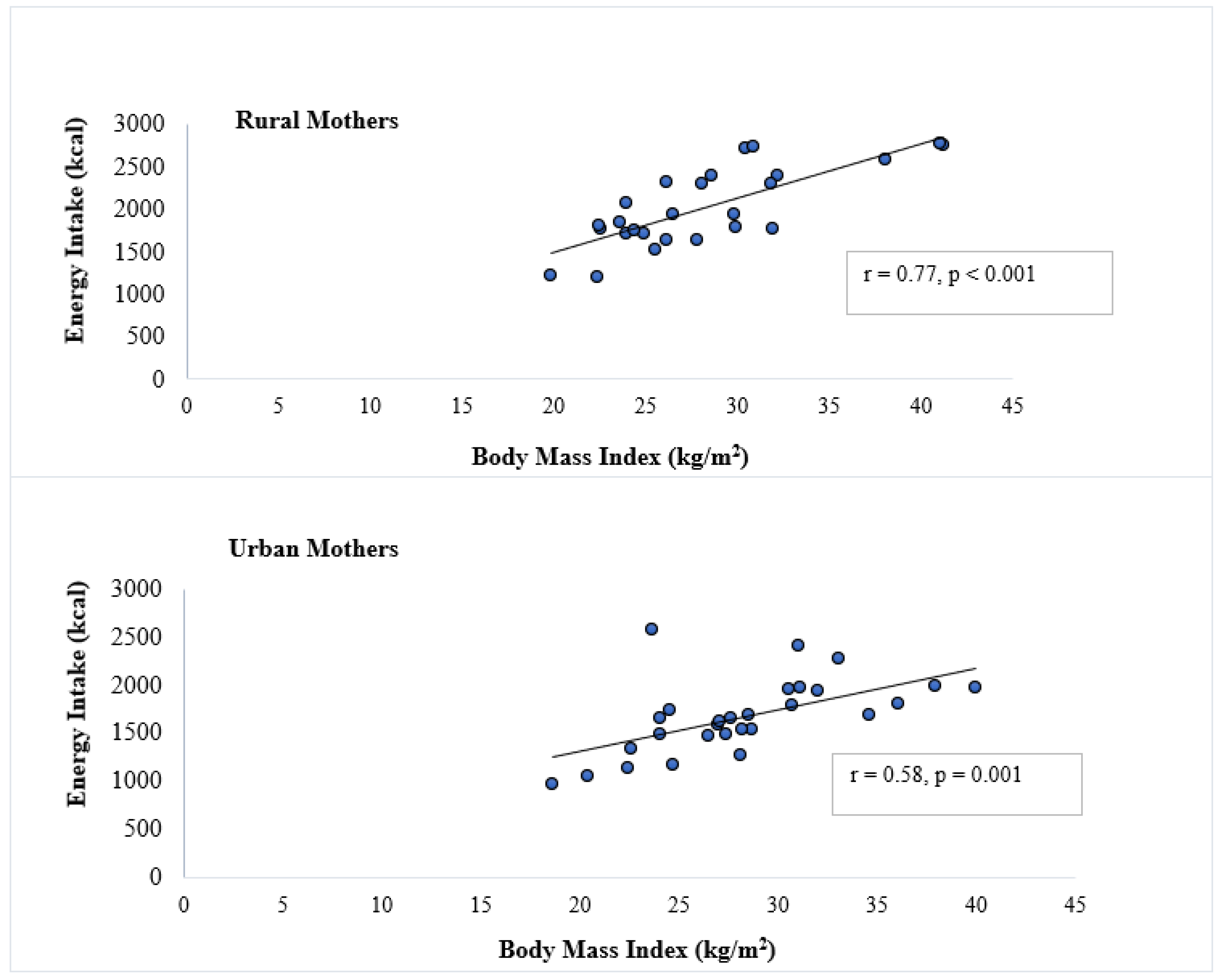
Figure 2.
Comparison of rural and urban mothers’ mean daily energy and nutrient intakes to recommended nutrient intakes (RNIs) (represented by a black horizontal line). p-values were statistically significant at p < 0.05.
Figure 2.
Comparison of rural and urban mothers’ mean daily energy and nutrient intakes to recommended nutrient intakes (RNIs) (represented by a black horizontal line). p-values were statistically significant at p < 0.05.
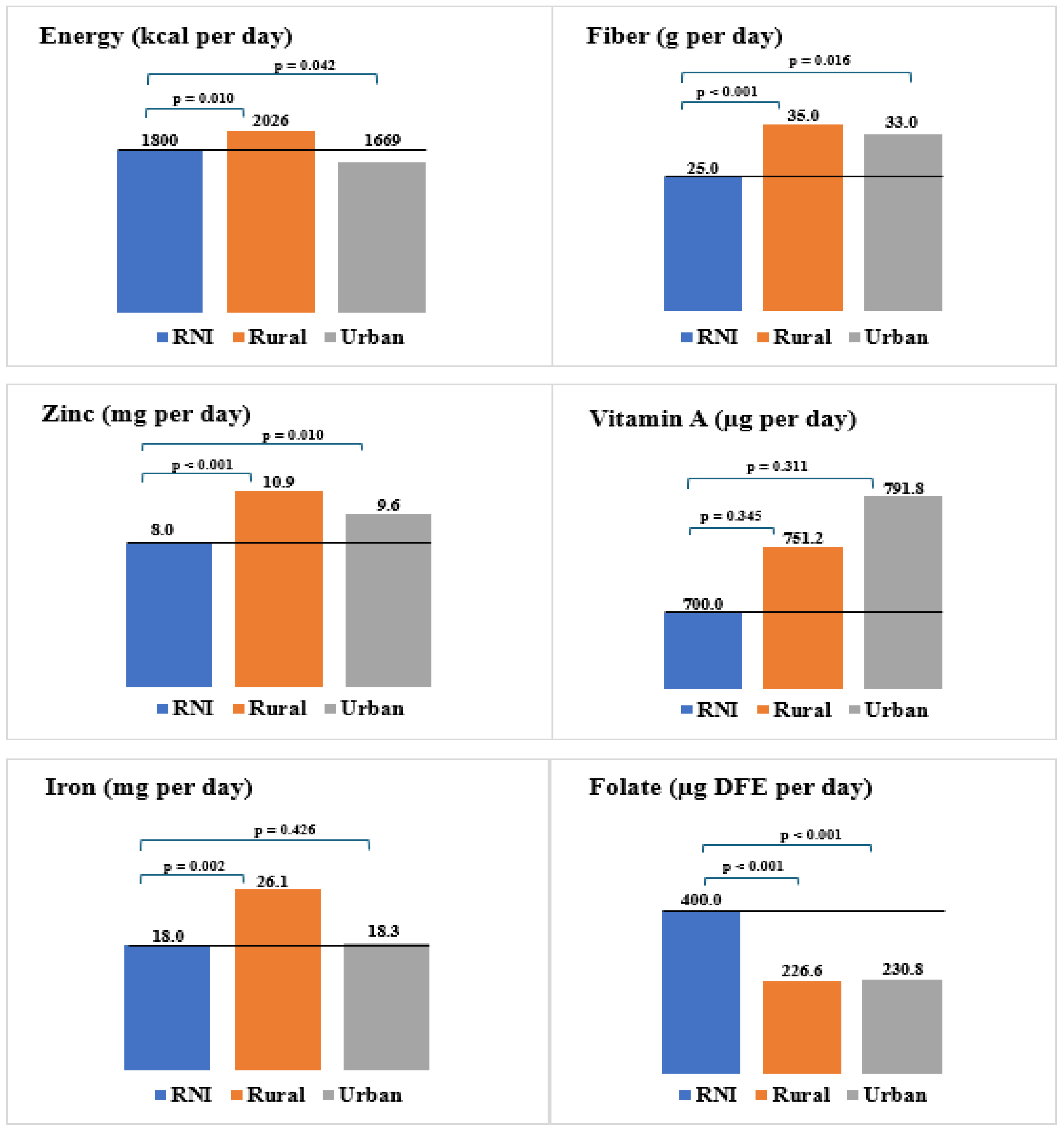

Table 1.
Comparison of mean daily energy and nutrient intakes of rural and urban mothers.
| Outcome variables | Rural (n = 26) | Urban (n = 28) | p-value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Energy (kcal) | 2026 ± 461 | 1669 ± 385 | 0.002 |
| Carbohydrate (g) | 325.8 ± 43.6 | 249.6 ± 42.2 | < 0.001 |
| Protein (g) | 66.6 ± 21.4 | 57.5 ± 12.3 | 0.040 |
| Fat (g) | 51.0 ± 10.6 | 49.1 ± 9.7 | 0.431 |
| Fiber (g) | 35.0 ± 11.5 | 33.0 ± 18.7 | 0.317 |
| Zinc (mg) | 10.9 ± 3.6 | 9.6 ± 3.4 | 0.089 |
| Iron (mg) | 26.1 ± 13.1 | 18.3 ± 7.4 | 0.004 |
| Vitamin A (µg) | 751.2 ± 126.5 | 791.8 ± 184.3 | 0.429 |
| Folate (µg DFE) | 226.6 ± 95.1 | 230.8 ± 122.6 | 0.444 |
Table 2.
Percentage of rural and urban mothers who fell below, met, or exceeded RNIs.
| Outcome Variables | Below RNIs % (n) | Met RNIs % (n) | Exceeded RNIs % (n) | |||
|---|---|---|---|---|---|---|
| Rural | Urban | Rural | Urban | Rural | Urban | |
| Energy (kcal) | 7.7 (2) | 21.4 (6) | 42.3(14) | 67.9 (20) | 38.5 (10) | 7.1 (2) |
| Fiber (g) | 3.8 (1) | 7.1 (2) | 84.6 (22) | 82.1 (23) | 11.5 (3) | 10.7 (3) |
| Zinc (mg) | 7.7 (2) | 10.7 (3) | 80.8 (21) | 78.6 (22) | 11.5 (3) | 10.7 (3) |
| Iron (mg) | 0.0 (0) | 14.3 (4) | 76.9 (20) | 82.1 (23) | 23.1 (6) | 3.6 (1) |
| Vitamin A (µg) | 0.0 (0) | 0.0 (0) | 92.3 (24) | 92.9 (26) | 7.7 (2) | 7.1 (2) |
| Folate (µg DFE) | 46.2 (12) | 53.6 (15) | 53.8 (14) | 46.4 (13) | 0.0 (0) | 0.0 (0) |
RNIs = Recommended Nutrient Intakes, n = frequency, RNIs were obtained from the FAO/WHO Human Energy/Vitamin and Mineral Requirements Handbooks. Z-scores for mean intakes below -1 were classified as below RNIs, between -1 and +1 met RNIs, and above +1 exceeded RNIs.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



