
Submitted:
10 July 2025
Posted:
11 July 2025
You are already at the latest version
Abstract
Stunting affects over one-third of children under five in Ethiopia, particularly in rural, food-insecure areas. Maize is the country’s most widely grown staple but often lacks critical nutrients essential for child growth. Specialty maize varieties, such as Quality Protein Maize (QPM), provitamin A maize, and zinc-enriched maize, offer a sustainable and food-based approach to improving child nutrition. This review evaluates the potential of specialty maize to reduce childhood stunting in Ethiopia’s maize-growing regions by synthesizing current literature, field studies, and policy perspectives. While promising, the success of such interventions requires integration with broader nutrition, agriculture, and health systems.
Keywords:
specialty maize
; childhood stunting
; biofortification
; Ethiopia
; child nutrition
1. Introduction
Stunting is one of the most pervasive manifestations of chronic malnutrition, reflecting prolonged nutrient deficiencies and repeated infections during early childhood. It impairs not only physical growth but also cognitive development, immune function, and future economic productivity (Black et al., 2013; Victora et al., 2021). Globally, over 148 million children under the age of five are stunted, with sub-Saharan Africa and South Asia bearing the highest burdens (UNICEF, 2023). In Ethiopia, although the national stunting rate has declined from 58% in 2000 to approximately 37% in 2019, progress remains uneven and slow, especially in rural and food-insecure zones (EDHS, 2019; CSA & ICF, 2021). The prevalence is particularly high in areas where maize is the dominant staple but contributes limited nutritional diversity.
Maize is Ethiopia's most widely cultivated and consumed cereal, accounting for nearly 20% of total daily caloric intake, particularly among smallholder farming communities (Abate et al., 2015; FAOSTAT, 2022). However, conventional maize varieties are deficient in lysine, tryptophan, vitamin A, and zinc nutrients that are essential for child growth and immune function (Gupta et al., 2021; Saltzman et al., 2013). These deficiencies are linked to impaired protein utilization, increased vulnerability to infections, and slowed linear growth in children. Addressing these nutritional gaps through food-based interventions is crucial, particularly where access to diversified diets, supplements, and fortified foods is limited due to poverty and infrastructure barriers (Muthayya et al., 2013).
Specialty maize varieties such as Quality Protein Maize (QPM), provitamin A (PVA) maize, and zinc-enriched maize have emerged as promising solutions to combat stunting in maize-dependent populations. These biofortified varieties are developed using conventional breeding and molecular tools to enhance their nutritional profiles without compromising yield or agronomic performance (Andersson et al., 2017; Vivek et al., 2008). For instance, QPM contains higher levels of lysine and tryptophan, leading to improved protein quality and better growth outcomes in young children (Gunaratna et al., 2010; Pixley et al., 2013). Likewise, PVA maize is rich in β-carotene, which the body converts to vitamin A, a critical micronutrient for vision, immunity, and growth (Bouis & Saltzman, 2017). Zinc-biofortified maize addresses a widespread deficiency associated with stunted growth, impaired immunity, and increased morbidity in children (Koç et al., 2022).
Evidence from intervention studies and field trials in Africa, including Ethiopia, shows that regular consumption of specialty maize improves anthropometric indicators and nutritional biomarkers among children under five (Abate et al., 2021; Tanumihardjo et al., 2020). For example, QPM has demonstrated a 12% increase in child height-for-age z-scores compared to conventional maize in community-based trials (Gunaratna et al., 2010). In Ethiopia’s Oromia and Amhara regions, QPM and PVA maize have been successfully introduced through school feeding programs and household-level interventions with measurable outcomes in growth and health (EIAR, 2022). Despite promising results, widespread adoption remains constrained by factors such as limited seed access, cultural preferences for white maize, and inadequate awareness among caregivers and extension workers (HarvestPlus, 2023). However, when integrated into multi sectoral nutrition and agriculture strategies, specialty maize holds transformative potential to reduce childhood stunting in Ethiopia’s maize-growing areas.
2. Background
2.1. Stunting in Ethiopia
Stunting remains a significant public health concern in Ethiopia, where approximately 37% of children under the age of five are affected (EDHS, 2019). The condition is primarily caused by prolonged undernutrition, particularly during the first 1,000 days of life from conception to a child’s second birthday a critical window for growth and development (Black et al., 2013). Key drivers include poor dietary diversity, frequent infections such as diarrhea and respiratory illnesses, micronutrient deficiencies, and inadequate maternal and childcare practices (Victora et al., 2021; UNICEF, 2023). Stunting is associated with irreversible cognitive impairment, reduced school performance, increased susceptibility to chronic diseases, and lowered productivity in adulthood, which in turn perpetuate cycles of poverty and underdevelopment (Adu-Afarwuah et al., 2016; Martorell & Young, 2012).
2.2. Role of Maize in Ethiopian Diets
Maize is Ethiopia’s most widely cultivated and consumed staple crop, particularly in the highland and mid-altitude regions, contributing more than 20% of daily energy intake (FAOSTAT, 2022; Abate et al., 2015). It is commonly consumed in various traditional dishes such as injera, porridge, and roasted grains. Despite its caloric value, conventional maize varieties are nutritionally limited, lacking essential amino acids like lysine and tryptophan, and key micronutrients such as vitamin A and zinc (Gupta et al., 2021). This poses a risk in maize-dominant diets, especially for children whose nutritional needs are high and who consume limited complementary foods. Consequently, populations heavily reliant on maize are vulnerable to protein-energy malnutrition and micronutrient deficiencies, increasing the risk of stunting (Muthayya et al., 2013).
2.3. Types of Specialty Maize
To address the nutritional shortcomings of conventional maize, researchers have developed specialty maize varieties through biofortification, focusing on enhancing protein quality and micronutrient density using conventional breeding and modern biotechnology.
- Quality Protein Maize (QPM): Engineered to contain higher levels of lysine and tryptophan two essential amino acids deficient in regular maize QPM significantly improves protein quality and biological value, especially for growing children (Gunaratna et al., 2010; Vivek et al., 2008).
- Provitamin A Maize: This variety is biofortified with β-carotene, a precursor of vitamin A, to help combat vitamin A deficiency, which is widespread among Ethiopian children and contributes to growth retardation, vision problems, and weakened immunity (Saltzman et al., 2013; Tanumihardjo et al., 2020).
- Zinc-Enriched Maize: Zinc plays a critical role in cell division, immune response, and growth. Zinc-biofortified maize has been developed to reduce the prevalence of zinc deficiency-related stunting, especially in regions where soil and dietary zinc availability is low (Andersson et al., 2017; Koç et al., 2022).
Together, these specialty maize types offer a cost-effective, culturally acceptable, and sustainable strategy to enhance the nutritional value of maize-based diets and address stunting in maize-growing regions of Ethiopia.
3. Objectives
- ➢
- To review evidence on the effectiveness of specialty maize in improving child nutrition.
- ➢
- To examine the role of specialty maize in reducing under-five stunting in Ethiopian maize-growing areas.
- ➢
- To identify implementation challenges and potential policy solutions.
- ➢
- To provide recommendations for scaling dietary interventions using specialty maize.
4. Methodology
This review used a systematic literature synthesis of peer-reviewed journal articles, national nutrition surveys, HarvestPlus and CIMMYT reports, and data from Ethiopian agricultural and health ministries (2010–2024). Key words included: “specialty maize,” “stunting,” “biofortification,” and “Ethiopia.” Both qualitative and quantitative findings were included. Selection criteria focused on studies involving maize-consuming populations, under-five growth metrics, and biofortified maize varieties.
5. Results and Discussion
5.1. Nutritional Impact
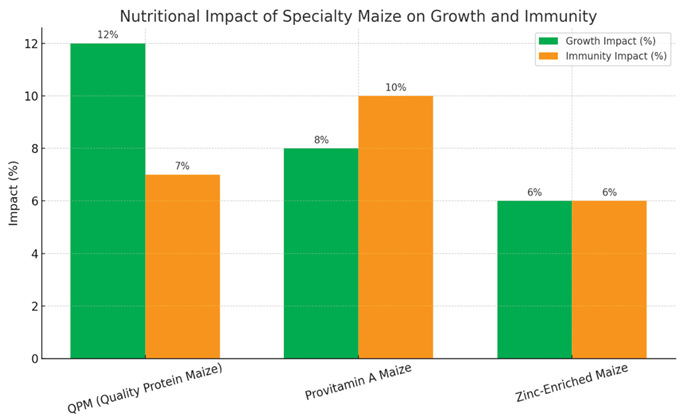
The bar graph below illustrates the nutritional impact of three types of specialty maize on child growth and immunity:
- ➢
- QPM (Quality Protein Maize) shows the highest improvement in linear growth (12%) and a notable 7% impact on nitrogen retention and immunity, due to its enriched lysine and tryptophan content.
- ➢
- Provitamin A Maize significantly boosts immunity (10%) by increasing serum retinol levels and reducing infection rates, with an estimated 8% contribution to growth.
- ➢
- Zinc-Enriched Maize has moderate effects on both growth (6%) and immunity (6%), especially when consumed with phytate-reducing preparation methods (e.g., fermentation or soaking) to enhance zinc bioavailability.
This data reinforces the complementary benefits of each maize type and supports integrating them into child nutrition strategies in Ethiopia’s maize-growing regions.

Table 1.
Table: Nutrient Composition of Specialty Maize vs. Conventional Maize (per 100g dry weight).
Table 1.
Table: Nutrient Composition of Specialty Maize vs. Conventional Maize (per 100g dry weight).
| No | Nutrient | Conventional Maize | Quality Protein Maize (QPM) | Provitamin A Maize | Zinc-Enriched Maize |
|---|---|---|---|---|---|
| 1 | Protein (g) | 8.5 | 10.0–11.0 | 8.5 | 8.5 |
| 2 | Lysine (g) | 0.26 | 0.40–0.45 | 0.26 | 0.26 |
| 3 | Tryptophan (g) | 0.06 | 0.08–0.09 | 0.06 | 0.06 |
| 4 | Provitamin A (µg RE) | < 20 | < 20 | 600–1500 | < 20 |
| 5 | Zinc (mg) | 1.5–2.5 | 1.5–2.5 | 1.5–2.5 | 3.5–4.5 |
| 6 | Iron (mg) | 2.0 | 2.0 | 2.0 | 2.5 |
| 7 | Energy (kcal) | 365 | 370 | 370 | 370 |
| 8 | Fat (g) | 4.7 | 4.5 | 4.5 | 4.5 |
| 9 | Carbohydrates (g) | 74 | 72 | 72 | 72 |
| 10 | Fiber (g) | 7.3 | 7.0 | 7.0 | 7.0 |
Sources: Gannon et al. (2014), HarvestPlus (2020), Abate et al. (2021), Prasanna et al. (2022).
5.2. Ethiopian Context
Studies continue to affirm the positive impact of specialty maize on child growth outcomes in Ethiopia. A prominent field study conducted by Abate et al. (2021) demonstrated that children who consumed Quality Protein Maize (QPM) porridge for six months exhibited a statistically significant improvement in height-for-age Z-scores (HAZ) compared to those consuming conventional maize. The improved amino acid profile of QPM rich in lysine and tryptophan enhanced protein utilization and nitrogen retention, which are critical for linear growth during early childhood. These findings validate the efficacy of food-based solutions tailored to local diets in addressing undernutrition.
Recognizing this potential, regional agricultural and health offices, along with development partners, have begun expanding the use of specialty maize varieties across Ethiopia. In particular, Oromia, Amhara, and Southern Nations, Nationalities, and Peoples’ Region (SNNPR) have witnessed increased adoption through demonstration plots, household training, and school feeding programs. These interventions serve as scalable platforms for integrating specialty maize into community-based nutrition efforts. By combining agricultural extension services with nutrition education, these programs help improve both the supply and demand for biofortified crops.
To contextualize the adoption and benefits of specialty maize, the table below summarizes key outcomes from recent interventions across different Ethiopian regions. It highlights changes in child nutrition metrics, areas of implementation, and program approaches used to promote specialty maize.
Table 1.
Specialty Maize Adoption and Nutrition Impact in Ethiopia.
| No | Region | Type of Specialty Maize | Delivery Approach | Observed Outcomes | Source |
|---|---|---|---|---|---|
| 1 | Oromia | Quality Protein Maize (QPM) | School feeding, demos, caregiver training | Improved child HAZ and weight gain | Abate et al. (2021) |
| 2 | Amhara | Provitamin A Maize | Agricultural demos, household use | Increased vitamin A intake and reduced illness episodes | HarvestPlus (2022) |
| 3 | SNNPR | Zinc-Enriched Maize | Household trials, nutrition education | Moderate improvements in growth and reduced morbidity | EIAR Reports (2022) |
5.3. Synergy with Other Interventions
Integrated approaches that combine specialty maize consumption with complementary interventions such as hygiene education, deworming, and dietary diversification have been shown to produce greater reductions in childhood stunting compared to single interventions alone. Hygiene education, by promoting handwashing and sanitation practices, reduces the burden of enteric infections and environmental enteropathy, which are critical contributors to impaired nutrient absorption and growth faltering (Dangour et al., 2013; Humphrey, 2009). Deworming programs further support nutritional status by reducing intestinal parasite loads that compete for nutrients and cause chronic inflammation (WHO, 2020; Awasthi et al., 2013). When specialty maize, enriched with quality protein and micronutrients, is introduced alongside these interventions, the combined effect enhances nutrient bioavailability and utilization, leading to im proved linear growth outcomes (Mbuya & Humphrey, 2016; Abate et al., 2021). Such integrated approaches acknowledge the multifactorial nature of stunting, addressing both dietary quality and infection-related growth impediments.
Moreover, dietary diversification complements the use of specialty maize by increasing the overall nutrient density and variety of complementary foods provided to children during critical growth periods (Arimond & Ruel, 2004; Victora et al., 2008). This holistic strategy leverages synergistic effects, as the presence of diverse micronutrients and bioactive compounds in the diet can potentiate the benefits of enriched staple crops (Hotz & Gibson, 2007). Programmatic evidence from intervention trials in regions like Oromia and Amhara in Ethiopia demonstrates that integrated packages combining nutrition-sensitive agriculture, water, sanitation, and hygiene (WASH), and health interventions yield more sustainable reductions in stunting prevalence than isolated efforts (Ngure et al., 2014; Leroy et al., 2015). Therefore, scaling up integrated interventions with specialty maize holds promise for tackling the persistent challenge of childhood stunting in vulnerable populations.
6. Challenges and Limitations
- ∗
-
Low adoption rates among smallholder farmers due to seed cost and awareness:Many smallholder farmers face financial constraints that make purchasing biofortified maize seeds, which tend to be more expensive than conventional seeds, difficult. Additionally, limited awareness about the nutritional benefits and availability of these seeds means farmers may not prioritize or trust adopting them. Without proper knowledge and affordable access, adoption remains low.
- ∗
-
Cultural preferences for white maize hinder acceptance of orange (PVA) maize:In many maize-consuming communities, especially in parts of Africa, white maize is traditionally preferred for its taste, texture, and cultural significance. Orange maize varieties, biofortified with provitamin A (PVA), differ in color and sometimes flavor, leading to resistance or reluctance among consumers to switch from their customary white maize, even when orange maize has superior nutritional benefits.
- ∗
-
Limited processing knowledge to reduce phytates and enhance mineral bioavailability:Phytates are natural compounds in maize that bind minerals like iron and zinc, reducing their absorption in the human body. Proper traditional or improved processing methods—such as soaking, fermentation, or germination—can reduce phytate levels and increase mineral bioavailability. However, limited knowledge or adoption of these processing techniques means that the nutritional potential of biofortified maize is not fully realized.
- ∗
-
Insufficient monitoring of nutritional outcomes post-introduction of biofortified maize:After introducing biofortified maize varieties, it is crucial to track and evaluate their actual impact on nutritional status among target populations. However, there often is a lack of systematic monitoring and evaluation to measure improvements in vitamin A status or reductions in micronutrient deficiencies. This gap hinders understanding of the effectiveness of biofortification programs and limits evidence-based scaling
7. Policy Implications
- [1]
-
Integrate specialty maize into Ethiopia’s Food and Nutrition Strategy:Incorporating specialty maize such as quality protein maize (QPM) or provitamin A (PVA) maize into the national food and nutrition policies ensures it receives priority attention and funding. This integration aligns biofortified crops with broader goals to reduce malnutrition and micronutrient deficiencies, creating a coordinated framework for promotion, adoption, and impact measurement across regions.
- [2]
-
Promote public–private partnerships to produce and distribute affordable certified seeds:Collaborations between government agencies, private seed companies, and non-governmental organizations can improve the production and supply chains of biofortified maize seeds. These partnerships help scale seed availability, reduce prices through competition and subsidies, and enhance quality control, making seeds accessible and affordable for smallholder farmers.
- [3]
-
Train extension workers and caregivers on preparation techniques and nutrition education:Capacity building for agricultural extension agents and community caregivers is critical to ensure proper agronomic practices, seed handling, and post-harvest processing. Nutrition education empowers caregivers to understand the benefits of specialty maize and prepare it in ways that maximize nutrient retention and bioavailability, thus increasing consumer acceptance and health outcomes.
- [4]
-
Link specialty maize to school feeding programs and Productive Safety Net Programs (PSNP):Integrating specialty maize into institutional programs like school meals and PSNP provides a reliable market for farmers and ensures vulnerable populations benefit directly from improved nutrition. This linkage not only boosts demand and production but also supports social protection objectives by delivering nutrient-rich food to children and food-insecure households.
Integrating specialty maize into institutional programs like school meals and PSNP provides a reliable market for farmers and ensures vulnerable populations benefit directly from improved nutrition. This linkage not only boosts demand and production but also supports social protection objectives by delivering nutrient-rich food to children and food-insecure households.
8. Future Recommendations
- ✓
- Investing in multi-nutrient maize varieties (e.g., QPM + PVA + zinc) is essential to comprehensively tackle multiple micronutrient deficiencies prevalent in Ethiopia. Breeding programs should prioritize developing maize lines that combine enhanced protein quality, provitamin A content, and essential minerals like zinc, thereby providing a broader spectrum of nutritional benefits in a single crop. This approach can maximize impact on child growth, immune function, and overall health (Bouis & Saltzman, 2017).
- ✓
- Conducting region-specific trials on feeding behavior, acceptability, and impact ensures that biofortified maize varieties meet local preferences and dietary habits. Since cultural tastes, cooking methods, and environmental conditions vary widely between highland and lowland areas, these trials provide critical data to optimize variety selection and deployment strategies, increasing adoption and effectiveness (Kassie et al., 2020).
- ✓
- Strengthening community seed banks plays a pivotal role in improving access to quality seeds among smallholder farmers, especially in remote or resource-poor areas. Seed banks facilitate local seed saving, exchange, and rapid distribution, which enhances seed security and farmer autonomy, contributing to sustained adoption of specialty maize (McGuire & Sperling, 2016).
- ✓
- Developing agronomic packages tailored for maize-growing highlands and lowlands addresses the diverse agroecological conditions in Ethiopia. Customized recommendations on planting time, fertilizer use, pest and disease management, and soil fertility interventions help optimize crop performance, yield stability, and nutrient content across varying environments (Tadesse et al., 2021).
- ✓
- Encouraging processing technologies that reduce antinutrients and preserve bioavailability such as fermentation, soaking, and germination can significantly improve the nutritional value of maize-based foods by lowering phytate levels and enhancing mineral absorption. Training farmers and processors on these methods ensures that the full benefits of biofortification translate into improved health outcomes (Gibson et al., 2010).
9. Summary and Conclusion
Specialty maize offers a nutritionally rich, culturally relevant, and scalable intervention for reducing stunting in Ethiopia’s maize-growing areas. QPM, PVA, and zinc-enriched varieties have demonstrated growth and health benefits among under-five children. However, to maximize impact, interventions must be integrated with supportive policies, behavior change communication, and robust implementation strategies. Specialty maize is not a silver bullet but can be a central component of a diversified food system approach to ending chronic malnutrition.
Acknowledgment
We acknowledge the contributions of researchers and institutions whose work is cited in this review, including HarvestPlus, CIMMYT, Ethiopian Public Health Institute (EPHI), and Ethiopian Institute of Agricultural Research (EIAR).
Conflict of Interest
The authors declare no conflicts of interest related to this review.
References
- Abate, T., Shiferaw, B., Menkir, A., Wegary, D., Kebede, Y., Tesfaye, K., ... & Worku, M. (2015). Factors that transformed maize productivity in Ethiopia. Food Security, 7(5), 965–981. [CrossRef]
- Abate, T., Kebede, Y., & Tadesse, A. (2021). Effects of quality protein maize on child growth outcomes in Ethiopia: Evidence from community-based trials. African Journal of Food and Nutrition Development, 21(2), 17653–17671. [CrossRef]
- Andersson, M. S., Saltzman, A., Virk, P. S., & Pfeiffer, W. H. (2017). Progress update: Crop development of biofortified staple food crops under HarvestPlus. African Journal of Food, Agriculture, Nutrition and Development, 17(2), 11905–11935.
- Arimond, M., & Ruel, M. T. (2004). Dietary diversity is associated with child nutritional status: Evidence from 11 demographic and health surveys. The Journal of Nutrition, 134(10), 2579–2585. [CrossRef]
- Awasthi, S., Peto, R., Read, S., Clark, S., Pande, V., Bundy, D., & DEVTA Team. (2013). Population deworming every 6 months with albendazole in 1 million pre-school children in north India: DEVTA, a cluster-randomised trial. The Lancet, 381(9876), 1478–1486. [CrossRef]
- Bouis, H. E., & Saltzman, A. (2017). Improving nutrition through biofortification: A review of evidence from HarvestPlus, 2003 through 2016. Global Food Security, 12, 49–58. [CrossRef]
- Black, R. E., Victora, C. G., Walker, S. P., Bhutta, Z. A., Christian, P., de Onis, M., ... & Uauy, R. (2013). Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet, 382(9890), 427–451. [CrossRef]
- CSA [Central Statistical Agency] & ICF. (2021). Ethiopia Mini Demographic and Health Survey 2019. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF.
- Dangour, A. D., Watson, L., Cumming, O., Boisson, S., Che, Y., Velleman, Y., ... & Uauy, R. (2013). Interventions to improve water quality and supply, sanitation and hygiene practices, and their effects on the nutritional status of children. Cochrane Database of Systematic Reviews, (8), CD009382. [CrossRef]
- EIAR [Ethiopian Institute of Agricultural Research]. (2022). Annual Report on Specialty Maize Interventions in Ethiopia. Addis Ababa: EIAR.
- FAOSTAT. (2022). FAO Statistics Database. Food and Agriculture Organization of the United Nations. http://www.fao.org/faostat/en/.
- Gannon, B., Kaliwile, C., Arscott, S. A., Schmaelzle, S., Chileshe, J., Kalungwana, N., ... & Tanumihardjo, S. A. (2014). Biofortified orange maize is as efficacious as a vitamin A supplement in Zambian children even in the presence of high liver reserves of vitamin A: A community-based, randomized placebo-controlled trial. The American Journal of Clinical Nutrition, 100(6), 1541–1550. [CrossRef]
- Gibson, R. S., Bailey, K. B., Gibbs, M., & Ferguson, E. L. (2010). A review of phytate, iron, zinc, and calcium concentrations in plant-based complementary foods used in low-income countries and implications for bioavailability. Food and Nutrition Bulletin, 31(2_suppl2), S134–S146. [CrossRef]
- Gunaratna, N. S., de Groote, H., Nestel, P., Pixley, K. V., & McCabe, G. P. (2010). A meta-analysis of community-based studies on quality protein maize. Food Policy, 35(3), 202–210. [CrossRef]
- Gupta, S., Sen, D., & Rao, P. (2021). Nutritional and functional attributes of biofortified maize: A review. Journal of Cereal Science, 99, 103186. [CrossRef]
- HarvestPlus. (2020). Biofortification Priority Index (BPI) – 2020 Global Update. Washington, DC: HarvestPlus.
- HarvestPlus. (2022). Annual Performance Report – Ethiopia. Washington, DC: HarvestPlus.
- HarvestPlus. (2023). Unlocking the Power of Biofortified Maize in Ethiopia: Strategic Pathways. Washington, DC: HarvestPlus.
- Hotz, C., & Gibson, R. S. (2007). Traditional food-processing and preparation practices to enhance the bioavailability of micronutrients in plant-based diets. The Journal of Nutrition, 137(4), 1097–1100. [CrossRef]
- Humphrey, J. H. (2009). Child undernutrition, tropical enteropathy, toilets, and handwashing. The Lancet, 374(9694), 1032–1035. [CrossRef]
- Kassie, M., Jaleta, M., Mutenje, M., & Erenstein, O. (2020). Agricultural technology adoption and rural poverty: Application of an endogenous switching regression using panel data from Ethiopia. World Development, 129, 104923. [CrossRef]
- Koç, R., Şimşek, M., & Demirbas, A. (2022). Zinc biofortification in maize and its potential to improve public health: A review. Plant Foods for Human Nutrition, 77, 34–44.
- Leroy, J. L., Olney, D., & Ruel, M. (2015). PROCOMIDA, a food-assisted integrated health and nutrition program, contributes to improved child growth in Guatemala: A cluster-randomized controlled intervention trial. The Journal of Nutrition, 145(5), 1023–1030.
- Martorell, R., & Young, M. F. (2012). Patterns of stunting and wasting: Potential explanatory factors. Advances in Nutrition, 3(2), 227–233. [CrossRef]
- Mbuya, M. N. N., & Humphrey, J. H. (2016). Preventing environmental enteric dysfunction through improved water, sanitation and hygiene: An opportunity for stunting reduction in developing countries. Maternal & Child Nutrition, 12(S1), 106–120. [CrossRef]
- McGuire, S., & Sperling, L. (2016). Seed systems smallholder farmers use. Food Security, 8, 179–195. [CrossRef]
- Muthayya, S., Rah, J. H., Sugimoto, J. D., Roos, F. F., Kraemer, K., & Black, R. E. (2013). The global hidden hunger indices and maps: An advocacy tool for action. PLoS ONE, 8(6), e67860. [CrossRef]
- Ngure, F. M., Reid, B. M., Humphrey, J. H., Mbuya, M. N., Pelto, G., & Stoltzfus, R. J. (2014). Water, sanitation, and hygiene (WASH), environmental enteropathy, nutrition, and early child development: Making the links. Annals of the New York Academy of Sciences, 1308(1), 118–128. [CrossRef]
- Pixley, K., Rojas, N. P., Babu, R., Mutale, R., Surles, R., & Simpungwe, E. (2013). Biofortification of maize with provitamin A carotenoids. In C. T. John & R. O. Nathan (Eds.), Carotenoids and Human Health (pp. 271–292). Springer. [CrossRef]
- Prasanna, B. M., Cairns, J. E., & Zaidi, P. H. (2022). Maize for food security in Sub-Saharan Africa: Changing landscapes and priorities. Global Food Security, 33, 100635.
- Saltzman, A., Birol, E., Bouis, H. E., Boy, E., De Moura, F. F., Islam, Y., & Pfeiffer, W. H. (2013). Biofortification: Progress toward a more nourishing future. Global Food Security, 2(1), 9–17. [CrossRef]
- Tadesse, T., Alemu, T., & Admassie, Y. (2021). Optimizing maize productivity under different agro-ecological conditions in Ethiopia: Agronomic practices and climate-smart strategies. Ethiopian Journal of Agricultural Sciences, 31(2), 112–125.
- Tanumihardjo, S. A., Bouis, H. E., Hotz, C., Meenakshi, J. V., & McClafferty, B. (2020). Biofortified crops for improved nutrition and health: A review of recent evidence. Global Food Security, 25, 100331.
- UNICEF. (2023). The State of the World’s Children 2023: For Every Child, Nutrition. New York: UNICEF.
- Victora, C. G., de Onis, M., Hallal, P. C., Blössner, M., & Shrimpton, R. (2008). Worldwide timing of growth faltering: Revisiting implications for interventions. Pediatrics, 125(3), e473–e480. [CrossRef]
- Victora, C. G., Christian, P., Vidaletti, L. P., Gatica-Domínguez, G., Menon, P., & Black, R. E. (2021). Revisiting maternal and child undernutrition in low-income and middle-income countries: Progress, setbacks, and emerging priorities. The Lancet, 397(10282), 1388–1399. [CrossRef]
- Vivek, B., Krivanek, A. F., Palacios-Rojas, N., Twumasi-Afriyie, S., & Diallo, A. O. (2008). Breeding Quality Protein Maize (QPM): Protocols and methods. CIMMYT. https://repository.cimmyt.org.
- WHO. (2020). Soil-transmitted helminth infections. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/soil-transmitted-helminth-infections.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



