Submitted:
09 July 2025
Posted:
10 July 2025
You are already at the latest version
Abstract
Tendinopathies are chronic, multifactorial conditions marked by inflammation, extracellular matrix (ECM) degradation, and impaired healing. Nutraceuticals are increasingly explored as adjunctive therapies to modulate these processes. This study evaluates the biological effects of Tenosan®, a dietary supplement, on human tenocytes under both physiological and inflammatory conditions. An in vitro model of tendinopathy was established by stimulating human tenocytes with interleukin-1β. The effect of Tenosan® in improving tendon wellness was evaluated by analysing matrix and inflammatory markers. Results shows that Tenosan® significantly increased the type I/III collagen ratio, reduced vascular endothelial growth factor (VEGF) secretion, and enhanced nitric oxide production, indicating improved extracellular matrix remodeling and pro-regenerative activity. These findings demonstrate that Tenosan® positively modulates key pathways involved in tendon healing, supporting its potential use as part of a multimodal strategy for managing tendinopathies.
Keywords:
Tenosan®
; tendinopathy
; tenocytes
; nutraceutical
; inflammation
; collagen remodeling
1. Introduction
Tendons are highly organized, dense connective tissues primarily made up of collagen fibers, predominantly type I collagen (∼95%), along with proteoglycans and elastin, which imparts tensile strength and elasticity essential for tendon function [1,2]. Tendons play a crucial role in the musculoskeletal system by connecting muscles to bones, enabling the transmission of force necessary for joint movement, stability, and postural control [3].
Tendinopathy refers to a high widespread group of chronic, often painful disorders, characterized by degeneration and impaired function of tendon tissue. These conditions are particularly prevalent in athletes and individuals engaged in repetitive mechanical tasks, but they also affect general population, with an increasing incidence linked to aging and lifestyles factors [4]. Metabolic factors such as hypoxia, chronic inflammation, oxidative stress, apoptosis, and hormonal imbalances play a critical role in its pathogenesis. Key histological and molecular characteristics of tendinopathy include collagen fiber degeneration, spread of microvascularization and innervation, increased inflammation and heightened cellular apoptosis [5]. In particular, growing evidence has highlighted the active role of inflammation in the progression of tendinopathies [6], characterized by the increase of pro-inflammatory cytokines (e.g., IL-1β, TNF-α), immune cell infiltration, and activation of inflammatory pathways, such as NF-κB and MAPK [7,8]. Moreover, under pathological stimuli, in tenocytes occurs a dysregulation of collagen turnover which contribute to tendon degeneration [9,10]. In addition, angiogenesis plays an essential role in tendons dysregulation and repair, and must be finely regulated in tendinopathies context. VEGF expression peaks after the initial inflammatory phase and acts as a potent stimulator of neovascularization [11]. While this process is critical in the early stages of healing, persistent VEGF overexpression is linked to pathological angiogenesis, characterized by disorganized collagen deposition, excessive scar formation, and impaired biomechanical properties of the tendon [12].
In this context, novel therapeutic approaches targeting the inflammatory environment of tendinopathies are increasingly. Current therapeutic strategies advocate for a comprehensive, multimodal approach that combines therapeutic exercise, targeted physical therapies (e.g., shockwave therapy), and specific nutritional support aimed at enhancing tendon healing processes [13,14,15]. Specifically, recent studies on patients with calcific shoulder tendinopathy treated with radial shockwave therapy (RSWT) demonstrated that adjunctive nutraceutical supplementation significantly reduced pain, inflammation, and intratendinous calcifications, improving range of motion, muscle strength, and quality of life. These benefits were sustained over time, with no relapses observed at 3-month follow-up and superior outcomes compared to the control group [16]. Moreover, in the postoperative setting, prolonged supplementation has been shown to reduce pain and enhance structural integrity following rotator cuff repair, supporting faster recovery and lower recurrence rates [17]. Likewise, its combination with extracorporeal shockwave therapy (ESWT) has shown promise in the treatment of insertional Achilles tendinopathy, suggesting a synergistic effect warranting further investigation [18].
Tenosan® is a commercially available dietary supplement formulated to support tendon, joint, and muscle health, particularly in individuals subjected to increased mechanical stress or affected by tendinopathies. Its composition includes bioactive compounds with antioxidant, anti-inflammatory, and structural support properties: L-arginine alpha-ketoglutarate (AAKG), methylsulfonylmethane optimized (OptiMSM®), beetroot extract (TruBeet®), polyphenols from Vitis vinifera (ViNitrox®), hydrolysed collagen I, vitamin D (Vit D), and vitamin C (Vit C). In particular, hydrolysed collagen I has garnered attention as a nutritional intervention in tendons health, thanks to its specific activity on tendons structure, since its positive effect on connective tissue is well-known [19,20,21]. AAKG is being marketed as ergogenic aid due to its potential to enhance vasodilation, through the upregulation of the endothelial L-arginine-nitric-oxide pathway [22]. Methylsulfonylmethane (MSM) is a sulfur-based nutritional supplement that is purported to have pain and inflammation reducing effects. In addition, as sulfur donator, it is essential for support protein synthesis, including collagen [23]. Beetroots are rich in dietary nitrates and betalains, pigments with antioxidant and anti-inflammatory properties. As a natural source of nitrate, beetroot consumption increases nitric oxide (NO) availability and is emerging as a potential strategy to prevent and manage pathologies associated with diminished NO bioavailability [24]. Also Vitis vinifera, a compound rich of polyphenols, increases the synthesis and bioavailability of NO, which is well known as the most important mediator of vasodilation. Vinitrox™ is a purified extract with more than 60% of total polyphenols [25]. Vit D has pleiotropic effects and multiples biological functions, among which tendons protection, exerted thought proliferative tenocytes stimulation [26]. Vit C has a key role in preventing and managing oxidative stress related conditions, including those affecting the musculoskeletal system [27,28,29]. In vitro studies have demonstrated that Vit C stimulates collagen synthesis in human tenocytes, while in vivo evidence supports its role in promoting tendon healing by enhancing angiogenesis, boosting collagen production, and reducing fibrosis and adhesion formation [30,31,32,33]. Furthermore, Vit C may enhance the efficacy of stem cell based regenerative approaches and has shown clinical benefits in improving recovery in tendinopathy patients [34].
The effectiveness of Tenosan® in supporting tendon healthy in tendinopathy conditions has already been demonstrated by several studies on patients. Specifically, preclinical and clinical trials have demonstrated that supplementation with Tenosan®, particularly when combined with low-frequency focused shockwave therapy, significantly improves pain and function scores in patients with plantar fasciopathy, with sustained benefits in the medium to long term [13]. Similar findings have been reported in the management of calcific tendon diseases, where supplementation facilitates the reduction of inflammatory catabolites and promotes connective tissue remodeling [35].
In the present study, the biological effects of Tenosan® on primary human tenocytes was investigated under both physiological and inflammatory conditions, that allowed to simulate an in vitro model of tendinopathy. It was assessed the impact of Tenosan® on key markers of tendon health, including collagen type I and III, VEGF, and NO production. Obtained findings demonstrate that Tenosan® promotes a favorable collagen I/III ratio, reduces VEGF secretion, and enhances NO levels. These data collectively support the rationale for integrating nutraceutical supplementation, such as Tenosan®, into a comprehensive treatment paradigm for tendinopathy, particularly in cases with underlying metabolic or inflammatory contributors.
2. Materials and Methods
2.1. Tenosan® Preparation
Tenosan® was provided in powder form, packaged in individual sachets. Fresh preparations were obtained by dissolving the powder in sterile distilled water (dH₂O) according to the manufacturer’s instructions. The resulting solution was sterilized by filtration through 0.22 µm pore-size filters.
2.2. Cells Cultures
Primary human tenocytes, isolated from the Achilles tendon of a healthy 74-year-old male donor, were purchased from Zen-Bio Inc. (Durham, NC, USA). Cells were maintained in Dulbecco’s Modified Eagle Medium (DMEM) supplemented with 10% fetal bovine serum (FBS), 1% L-glutamine, and 1% penicillin/streptomycin (P/S). Cultures were incubated at 37°C in a humidified atmosphere containing 5% CO₂. Only cells at passages ≤5 were used for experiments, to ensure phenotypic consistency.
2.3. Cytotoxicity Assay
The cytotoxic profile of Tenosan® was evaluated with MTT assay. Tenocytes were seeded in 96-well plates at a density of 1 × 10⁴ cells/well. After 24 h, cells were treated with serial dilutions of Tenosan®, starting from concentration of 25 mg/ml, in starvation condition. Following 24 h of exposure, cell viability was assessed by incubating the cultures with 0.5 mg/ml MTT (3-(4,5-dimethyltiazol-2-yl)-2,5-diphenyltetrazolium bromide) solution for 2 h at 37°C. Formazan crystals formed by metabolically active cells were solubilized in isopropanol, and absorbance was measured at 550 nm using an Infinite M Nano+ plate reader (Tecan).
2.4. Tendinopathy In Vitro Model
To mimic the pathological environment characteristic of tendinopathy, an in vitro inflammatory model was established by stimulating human tenocytes with IL-1β [36]. To define the optimal pro-inflammatory concentration, cells were treated with a range of IL-1β doses (1-50 ng/ml), and the inflammatory response was assessed by quantifying IL-6 secretion using ELISA assay (Ref. 88-7066-88, ThermoFisher Scientific).
2.5. Cells Treatment
The effects of Tenosan® in tendinopathy healing was evaluated on an in vitro healthy model, made by human primary tenocytes, and an inflammatory model, obtained by treating cells with IL-1β. Specifically, tenocytes were seeded in 48-well plates at a density of 1.5 × 10⁵ cells/well. After 24 h, inflammation was induced using IL-1β 10 ng/ml. Simultaneously, cells of healthy and inflammatory model were treated with Tenosan® at three non-cytotoxic concentrations: 0.8, 0.4, and 0.2 mg/ml, as determined in preliminary viability assays. Negative control (CTR) consisted of untreated cells. Following 24 h of treatment, cell culture supernatants were collected and analyzed to assess the expression of key markers involved in tendon matrix remodeling, angiogenesis and NO production.
2.6. Detection of Collagen, VEGF and NO Levels
As indicative of tissue remodelling processes, ELISA assays was performed on the supernatants of all the tested condition, in order to measure the secreted amount of collagen type I (Ref.AB285250, Abcam), collagen type III (Ref.LS-F26725, LSBio) and VEGF (Ref.KHG0111, ThermoFisher Scientific). Moreover, the amount of total NO produced following treatments was estimated using Nitric Oxide Assay Kit (Ref.EMSNO, ThermoFisher Scientific), providing further insight into the inflammatory modulation exerted by Tenosan®.
2.7. Statistical Analysis
Each experimental group included at least three replicates, and data were plotted as replicates means ± standard error. Statistical analysis was performed thought analysis of variance, using one way ANOVA, and statistical significance was set at p <0.05. Graph were generated using GraphPad Prism 10 (GraphPad Software, San Diego, CA, USA).
3. Results
3.1. Effects of Tenosan® on Tenocyte Viability and Tendinopathy In Vitro Model
The cytotoxic effect on Tenosan®, tested at different concentrations, was evaluated on human tenocytes. Cell viability following treatment was assessed using the MTT assay. Results (Figure 1A) showed that Tenosan® did not affect cell viability at concentrations equal or lower than 0.8 mg/ml, whereas a cytotoxic effect was observed at concentrations from 1.5 mg/ml upwards. Therefore, the concentrations chosen for cell treatment were: 0.8, 0.4, and 0.2 mg/ml.
To establish an appropriate in vitro model of cellular inflammation, tenocytes were treated with IL-1β at concentrations ranging from 50 to 1 ng/ml for 24 h. IL-6 levels in the culture medium were measured by ELISA and compared with the untreated control (CTR) (Figure 1B). Results showed that IL-1β significantly increased IL-6 production in a dose-dependent manner, triggering an inflammatory response. In contrast, untreated control cells displayed IL-6 levels close to 0. The dose selected for subsequent experiments and for establishing the inflamed tendon model was 10 ng/ml: this concentration elicits a clear inflammatory response without compromise cell viability.
3.2. Quantification of Collagen I and III Levels
To evaluate the efficacy of Tenosan® in matrix remodelling, in healthy model and tendinopathy-like condition, collagen production was assessed. Indeed, collagen plays a fundamental role in the reparative response following tissue injury [37]. Specifically, collagen type I is essential for structural repair and proper connective tissue organization, contributing to tissue strength, whereas collagen type III, characterized by more flexible fibers, is primarily involved in the early stages of healing and leads to the formation of a more disorganized and elastic scar tissue [38,39]. Based on this, collagen type I, collagen type III and their ratio of was investigated, after treating human tenocytes with Tenosan®, in presence or absence of IL-1β 10 ng/ml.
To this end, ELISA assays were performed to quantify the levels of collagen type I and type III in human tenocytes treated with different concentrations of Tenosan®, in the presence or absence of IL-1β (10 ng/ml). The results showed that collagen III levels remained unchanged between treated and untreated groups under both healthy (Figure 2C) and inflammatory conditions (Figure 2D). In contrast, collagen I levels were significantly upregulated following Tenosan® treatment, as shown in (Figure 2A,B). Specifically, the product exhibited a dose dependent effect, statistically significant for doses of 0,8 and 0,4 mg/ml, in both analysed conditions. The selective increase in collagen I, without a corresponding rise in collagen III, results in a higher collagen I/III ratio, both in healthy (Figure 2E) and inflammatory models (Figure 2F). Notably, this effect aligns with the expected activity of the product, which is specifically formulated to enhance collagen I synthesis, with the aim of promote the formation of stronger and more organized tendon matrix. Indeed, higher levels of collagen I in relation to collagen III allows the formation solid structure, suggesting the beneficial effects of the product in strengthen tendon structure in healthy condition. Moreover, Tenosan® could have a crucial role in supporting the structural tendons repair, by the synthesis of a proper matrix, in response to stress and inflammatory conditions.
3.3. Quantification of VEGF Levels
VEGF plays a crucial role in angiogenesis during tendon healing, but its effects are complex and time dependent. In early stages, VEGF facilitates repair by promoting blood vessel formation, delivering nutrients and regulating immune responses. However, persistent high VEGF expression may impair tendon repair in later stages [40]. For this reason, VEGF production in human tenocytes subjected to Tenosan® treatment, in both healthy (Figure 3A) and inflammatory model (Figure 3B), was evaluated using ELISA assay. Results showed the effect of the product in reducing VEGF secretion, in both in vitro models. Specifically, a statistically significant effect was displayed following the treatment with all the tested concentrations.
3.4. Quantification of Nitric Oxide Levels
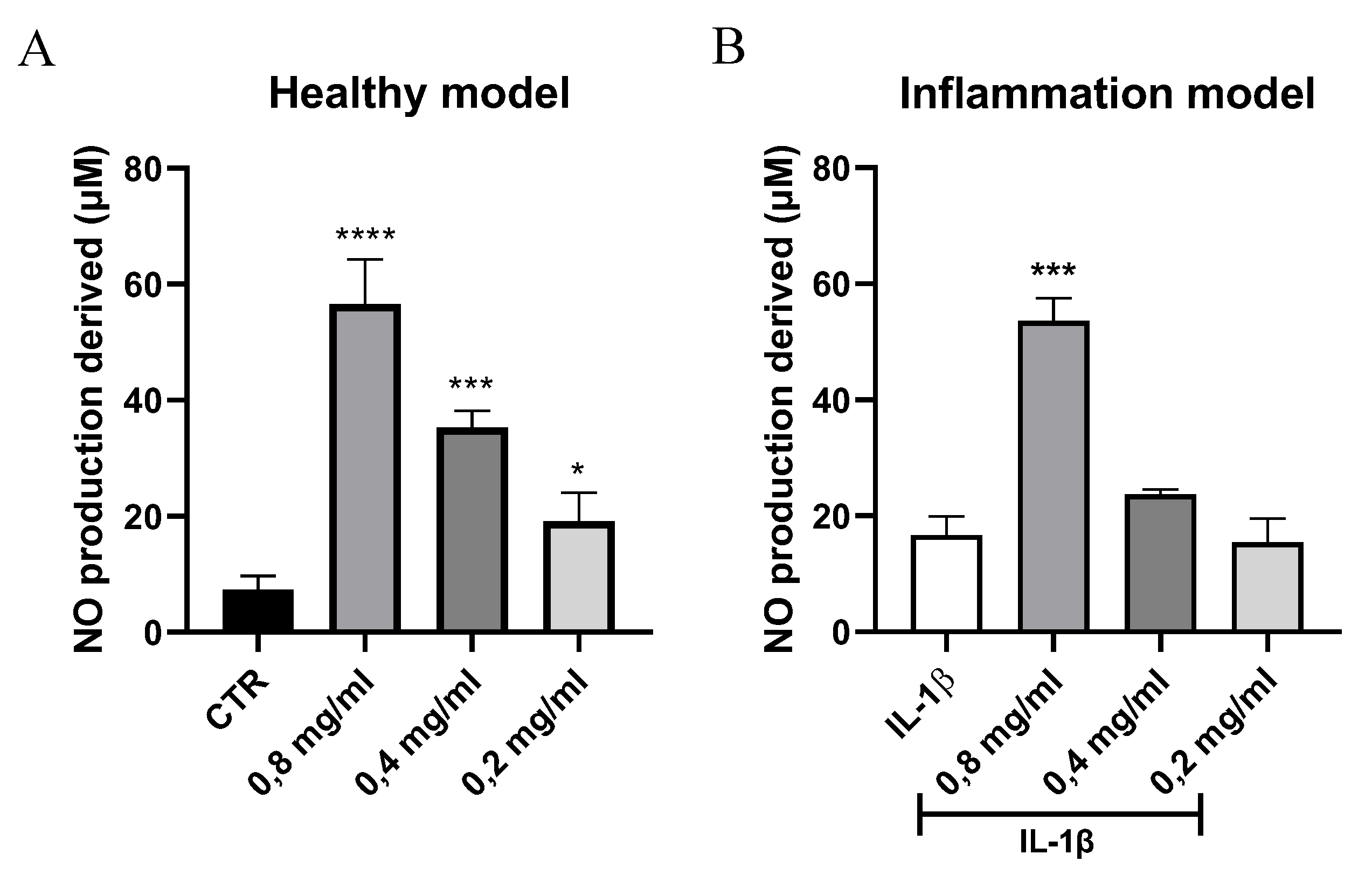
NO based therapies have well-known effects in enhancing tendon healing [41], for this reason are considered a promising treatment to induce tendons regeneration after injuries [42]. To assess the effect of Tenosan® in NO metabolism, levels of NO and its derivatives were measured in the supernatant of healthy and inflamed human tenocytes, treated with different concentrations of the product. Total NO levels were calculated as the sum of nitrite and nitrate, in accordance with the kit’s specifications. The results demonstrated a significant increase in NO levels in the supernatant of cells treated with the product compared to untreated control (CTR), with a dose-dependent effect (Figure 4A). Notably, the product at 0,8 mg/ml induced increase in NO levels also in inflamed condition (Figure 4B), indicating its potential beneficial effects under tendon damage conditions. These findings suggested that Tenosan® stimulates NO synthesis in tenocytes, both under basal and inflammatory conditions.
4. Discussion
Tendinopathies are multifactorial disorders characterized by inflammation, matrix degeneration and impaired tendons healing, often exacerbated by metabolic imbalances and oxidative stress. Recent strategies emphasize a multimodal approach that includes nutraceutical supplementation to support tendon repair. Tenosan®, a dietary supplement containing bioactive compounds with a focus on tendon protection, has shown clinical promise in improving outcomes in tendon-related disorders.
The aim of the present study was to investigate biologically relevant effects of Tenosan® on an in vitro model of primary human tenocytes, in order to deeply understand the pathways involved in its tendon regenerative action. In particular, experiments were performed under both physiological and inflammatory conditions, with the purpose of investigate Tenosan® efficacy in healthy condition and as a potential therapy for managing tendinopathies.
Firstly, the cell viability assay allowed to identify a safe concentration range of Tenosan® (0.8—0.2 mg/ml), below which no cytotoxic effects were observed. Accordingly, subsequent experiments were conducted using these non-toxic concentrations, to ensure the biological relevance of the results. To mimic tendinopathy-like conditions, an in vitro inflammatory model was established using IL-1β stimulation, which resulted in a dose-dependent increase in IL-6 secretion. The selected concentration of 10 ng/ml induced a robust inflammatory response without compromising cell viability, allowing the investigation of Tenosan® modulatory effects in tendinopathy-like condition.
A key finding of this study was the role of Tenosan® in the modulation of collagen synthesis, specifically through the selective upregulation of type I collagen. While collagen type III levels remained unchanged across treatment conditions, Tenosan® significantly increased collagen type I expression, leading to a higher type I/type III collagen ratio. This ratio is a well-established marker of effective tissue remodeling, as type I collagen is the predominant component of mature tendon tissue, providing tensile strength and structural integrity, whereas type III collagen is more prevalent during the early phases of healing and is associated with less organized extracellular matrix (ECM) structures [43]. Therefore, the ability of Tenosan® to selectively enhance type I collagen production suggests a shift toward a more functionally mature and mechanically robust matrix composition, thereby potentially promoting more effective and long-lasting tendon repair.
Additionally, a reduction in VEGF secretion was observed after Tenosan® treatment, in both physiological and inflamed conditions, highlighting a regulatory effect of Tenosan® on angiogenesis. While VEGF plays a crucial role in the early stages of tendon healing by promoting neovascularization and nutrient delivery, sustained overexpression has been associated with impaired matrix remodeling and the formation of disorganized scar tissue, potentially compromising the mechanical properties of the repaired tendon [44]. Therefore, modulation of VEGF signaling is increasingly recognized as a strategic therapeutic goal in promoting effective and functional tendon regeneration. For this reason, the effect of Tenosan® in downregulate VEGF could have a crucial role in helping to prevent maladaptive angiogenesis during the later stages of healing.
Furthermore, Tenosan® significantly increased NO production at the maximum dose tested. This effect was evident in both healthy and inflamed tenocytes and showed a dose-dependent trend. Several studies have demonstrated that increased NO production plays a beneficial role in tendon healing. In vitro experiments on human tendon cells [45] have shown that exogenous NO donors and upregulation of inducible nitric oxide synthase (iNOS) enhance collagen synthesis, a key component of tendon matrix repair. In support of this, inhibition of nitric oxide synthase (NOS) activity has been shown to impair tendon healing. Specifically, the competitive NOS inhibitor N^G-nitro-L-arginine methyl ester (L-NAME) has been employed in animal models to investigate the role of NO in tendon regeneration [46]. Treatment with L-NAME led to a marked reduction in both the cross-sectional area and mechanical strength of healing tendons, underlining the critical role of NO in this process [47]. Collectively, this evidence suggest that upregulation of NO contributes positively to tendon healing by promoting extracellular matrix formation, through direct enhance of collagen synthesis [48], and by improving tendon biomechanics. Moreover, NO signalling leads vasodilation, by inducing smooth muscle relaxation through cyclic GMP pathway [49], increasing blood flow. Furthermore, in vivo studies have reported beneficial effects of L-arginine supplementation, including enhanced blood circulation to tissues, and enhance protein synthesis [50]. Take this into account the combination of Arginine α -ketoglutarate, TruBeet® and Vinitrox® contained in Tenosan® could ensure blood flow to tendons.
In summary, the combined effects of Tenosan® on enhancing the type I/III collagen ratio, increasing NO levels and modulating VEGF expression underscore its potential as a therapeutic strategy for improving tendon healing outcomes. Specifically, results support the role of Tenosan® in promoting tendon reparation in inflammatory condition that mimic the tendinopathy environment, by enhancing the quality of the extracellular matrix and regulating key mediators involved in tissue regeneration. Moreover, the product showed efficacy also in healthy condition, by promoting a more organized ECM and regulating angiogenic responses. For this reason, Tenosan® could have a double effect, with a role both in counteracting and in preventing tendinopathy, by reinforcing tendon structure and function, with a consequent reduction of the risk of injury occurrence and escalation.
Author Contributions
Conceptualization, S.A. and D.T.; methodology, M.S.M and S.A.; validation, M.S.M. and S.R.; investigation, M.S.M.; data curation, M.S.M., S.R. and S.A.; writing—original draft preparation, M.S.M., S.R. and S.A.; writing—review and editing, S.A. and D.T.; visualization, M.S.M.; supervision, S.R., S.A., D.T.; project administration, S.A. and D.T.; funding acquisition, D.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Agave group.
Conflicts of Interest
Author S.A. and D.T. has been involved as Scientific Advisor and Medical Manager in Company Agave Group.
References
- C. T. Thorpe and H. R. C. Screen, ‘Tendon Structure and Composition’, Adv Exp Med Biol, vol. 920, pp. 3–10, 2016. [CrossRef]
- D. Zdzieblik, S. Oesser, M. W. Baumstark, A. Gollhofer, and D. König, ‘Collagen peptide supplementation in combination with resistance training improves body composition and increases muscle strength in elderly sarcopenic men: A randomised controlled trial’, British Journal of Nutrition, vol. 114, no. 8, pp. 1237–1245, Aug. 2015. [CrossRef]
- N. Maffulli, F. Cuozzo, F. Migliorini, and F. Oliva, ‘The tendon unit: biochemical, biomechanical, hormonal influences’, J Orthop Surg Res, vol. 18, no. 1, Dec. 2023. [CrossRef]
- N. L. Millar, G. A. C. Murrell, and I. B. Mcinnes, ‘Inflammatory mechanisms in tendinopathy - towards translation’, Nat Rev Rheumatol, vol. 13, no. 2, pp. 110–122, Feb. 2017. [CrossRef]
- N. L. Millar et al., ‘Tendinopathy’, Nat Rev Dis Primers, vol. 7, no. 1, Dec. 2021. [CrossRef]
- B. J. F. Dean, P. Gettings, S. G. Dakin, and A. J. Carr, ‘Are inflammatory cells increased in painful human tendinopathy? A systematic review’, Br J Sports Med, vol. 50, no. 4, pp. 216–220, Feb. 2016. [CrossRef]
- M. Abate et al., ‘Pathogenesis of tendinopathies: inflammation or degeneration?’, Arthritis Res Ther, vol. 11, no. 3, p. 235, Jun. 2009. [CrossRef]
- N. L. Millar, G. A. C. Murrell, and I. B. Mcinnes, ‘Inflammatory mechanisms in tendinopathy - towards translation’, Nat Rev Rheumatol, vol. 13, no. 2, pp. 110–122, Feb. 2017. [CrossRef]
- S. G. Dakin, J. Dudhia, and R. K. W. Smith, ‘Resolving an inflammatory concept: the importance of inflammation and resolution in tendinopathy’, Vet Immunol Immunopathol, vol. 158, no. 3–4, pp. 121–127, Apr. 2014. [CrossRef]
- G. Riley, ‘Tendinopathy--from basic science to treatment’, Nat Clin Pract Rheumatol, vol. 4, no. 2, pp. 82–89, Feb. 2008. [CrossRef]
- T. Molloy, Y. Wang, and G. A. C. Murrell, ‘The roles of growth factors in tendon and ligament healing’, Sports Medicine, vol. 33, no. 5, pp. 381–394, 2003. [CrossRef]
- H. Tempfer et al., ‘Bevacizumab Improves Achilles Tendon Repair in a Rat Model’, Cellular Physiology and Biochemistry, vol. 46, no. 3, pp. 1148–1158, Apr. 2018. [CrossRef]
- A. Notarnicola, V. Pesce, G. Vicenti, S. Tafuri, M. Forcignanò, and B. Moretti, ‘SWAAT study: Extracorporeal shock wave therapy and arginine supplementation and other nutraceuticals for insertional achilles tendinopathy’, Sep. 2012. [CrossRef]
- B. M. Andres and G. A. C. Murrell, ‘Treatment of tendinopathy: what works, what does not, and what is on the horizon’, Clin Orthop Relat Res, vol. 466, no. 7, pp. 1539–1554, 2008. [CrossRef]
- N. Maffulli, U. G. Longo, and V. Denaro, ‘Novel approaches for the management of tendinopathy’, J Bone Joint Surg Am, vol. 92, no. 15, pp. 2604–2613, Nov. 2010. [CrossRef]
- M. Scarselli, E. Torricelli, and P. Pasquetti, ‘Trattamento combinato nella tendinopatia calcifica di spalla’, 2012.
- S. Gumina, D. Passaretti, M. D. Gurzì, and V. Candela, ‘Arginine L-alpha-ketoglutarate, methylsulfonylmethane, hydrolyzed type i collagen and bromelain in rotator cuff tear repair: A prospective randomized study’, Nov. 2012. [CrossRef]
- M. Di Gesù and D. Tiso, ‘The multimodal management of patients with tendinopathy: percutaneous electrolysis, nutraceuticals and lifestyle – report from the 2022 I.S.Mu.L.T. Congress’, Drugs Context, vol. 12, pp. 1–5, Jan. 2023. [CrossRef]
- K. Iwai et al., ‘Identification of food-derived collagen peptides in human blood after oral ingestion of gelatin hydrolysates’, J Agric Food Chem, vol. 53, no. 16, pp. 6531–6536, Aug. 2005. [CrossRef]
- I. Burton and A. McCormack, ‘Nutritional Supplements in the Clinical Management of Tendinopathy: A Scoping Review’, J Sport Rehabil, vol. 32, no. 5, pp. 493–504, Jul. 2023. [CrossRef]
- A. León-López, A. Morales-Peñaloza, V. M. Martínez-Juárez, A. Vargas-Torres, D. I. Zeugolis, and G. Aguirre-Álvarez, ‘Hydrolyzed Collagen—Sources and Applications’, Molecules, vol. 24, no. 22, p. 4031, 2019. [CrossRef]
- D. S. Willoughby, T. Boucher, J. Reid, G. Skelton, and M. Clark, ‘Effects of 7 days of arginine-alpha-ketoglutarate supplementation on blood flow, plasma L-arginine, nitric oxide metabolites, and asymmetric dimethyl arginine after resistance exercise’, Int J Sport Nutr Exerc Metab, vol. 21, no. 4, pp. 291–299, 2011. [CrossRef]
- L. S. Kim, L. J. Axelrod, P. Howard, N. Buratovich, and R. F. Waters, ‘Efficacy of methylsulfonylmethane (MSM) in osteoarthritis pain of the knee: A pilot clinical trial’, Osteoarthritis Cartilage, vol. 14, no. 3, pp. 286–294, Mar. 2006. [CrossRef]
- T. Clifford, G. Howatson, D. J. West, and E. J. Stevenson, ‘The Potential Benefits of Red Beetroot Supplementation in Health and Disease’, Nutrients, vol. 7, no. 4, p. 2801, Apr. 2015. [CrossRef]
- G. Deley, D. Guillemet, F. A. Allaert, and N. Babault, ‘An acute dose of specific grape and apple polyphenols improves endurance performance: A randomized, crossover, double-blind versus placebo controlled study’, Nutrients, vol. 9, no. 8, Aug. 2017. [CrossRef]
- K. Min et al., ‘Restoration of Cellular Proliferation and Characteristics of Human Tenocytes by Vitamin D’, Journal of Orthopaedic Research, vol. 37, no. 10, pp. 2241–2248, Oct. 2019. [CrossRef]
- N. N. DePhillipo, Z. S. Aman, M. I. Kennedy, J. P. Begley, G. Moatshe, and R. F. LaPrade, ‘Efficacy of Vitamin C Supplementation on Collagen Synthesis and Oxidative Stress After Musculoskeletal Injuries: A Systematic Review’, Orthop J Sports Med, vol. 6, no. 10, p. 2325967118804544, Oct. 2018. [CrossRef]
- S. J. Padayatty et al., ‘Vitamin C as an Antioxidant: Evaluation of Its Role in Disease Prevention’, J Am Coll Nutr, vol. 22, no. 1, pp. 18–35, Feb. 2003. [CrossRef]
- C. Hoppe, M. Freuding, J. Büntzel, K. Münstedt, and J. Hübner, ‘Clinical efficacy and safety of oral and intravenous vitamin C use in patients with malignant diseases’, J Cancer Res Clin Oncol, vol. 147, no. 10, p. 3025, Oct. 2021. [CrossRef]
- K. K. Kang et al., ‘Vitamin C Improves Therapeutic Effects of Adipose-derived Stem Cell Transplantation in Mouse Tendonitis Model’, In Vivo (Brooklyn), vol. 31, no. 3, p. 343, May 2017. [CrossRef]
- M. Gallorini, C. Antonetti Lamorgese Passeri, A. Cataldi, A. C. Berardi, and L. Osti, ‘Hyaluronic Acid Alleviates Oxidative Stress and Apoptosis in Human Tenocytes via Caspase 3 and 7’, Int J Mol Sci, vol. 23, no. 15, p. 8817, Aug. 2022. [CrossRef]
- G. Shaw, A. Lee-Barthel, M. L. R. Ross, B. Wang, and K. Baar, ‘Vitamin C–enriched gelatin supplementation before intermittent activity augments collagen synthesis’, Am J Clin Nutr, vol. 105, no. 1, p. 136, Jan. 2016. [CrossRef]
- O. Evrova, D. Kellenberger, M. Calcagni, V. Vogel, and J. Buschmann, ‘Supporting Cell-Based Tendon Therapy: Effect of PDGF-BB and Ascorbic Acid on Rabbit Achilles Tenocytes In Vitro’, Int J Mol Sci, vol. 21, no. 2, p. 458, Jan. 2020. [CrossRef]
- D. C. Noriega-gonzález, F. Drobnic, A. Caballero-garcía, E. Roche, D. Perez-valdecantos, and A. Córdova, ‘Effect of Vitamin C on Tendinopathy Recovery: A Scoping Review’, Nutrients, vol. 14, no. 13, p. 2663, Jul. 2022. [CrossRef]
- I. Capparucci, A. Federici, C. Bartolucci, M. Valentini, V. Vita, and I. Testa, ‘Terapia del morbo di Duplay con associazione di EDTA calcico per via intrarticolare e supplementazione orale plurifattoriale’, 2013.
- M. Marzagalli et al., ‘Anti-Inflammatory and Antioxidant Properties of a New Mixture of Vitamin C, Collagen Peptides, Resveratrol, and Astaxanthin in Tenocytes: Molecular Basis for Future Applications in Tendinopathies’, Mediators Inflamm, vol. 2024, p. 5273198, 2024. [CrossRef]
- J. D. S. Antonio, O. Jacenko, A. Fertala, and J. P. R. O. Orgel, ‘Collagen Structure-Function Mapping Informs Applications for Regenerative Medicine’, Bioengineering 2021, Vol. 8, Page 3, vol. 8, no. 1, p. 3, Dec. 2020. [CrossRef]
- W. Li, N. Chi, R. A. C. Rathnayake, and R. Wang, ‘Distinctive roles of fibrillar collagen I and collagen III in mediating fibroblast-matrix interaction: A nanoscopic study’, Biochem Biophys Res Commun, vol. 560, pp. 66–71, Jun. 2021. [CrossRef]
- S. W. Volk, Y. Wang, E. A. Mauldin, K. W. Liechty, and S. L. Adams, ‘Diminished Type III Collagen Promotes Myofibroblast Differentiation and Increases Scar Deposition in Cutaneous Wound Healing’, Cells Tissues Organs, vol. 194, no. 1, pp. 25–37, Jun. 2011. [CrossRef]
- X. Liu et al., ‘The Role of Vascular Endothelial Growth Factor in Tendon Healing’, Oct. 25, 2021, Frontiers Media S.A. [CrossRef]
- A. R. Bokhari and G. A. C. Murrell, ‘The role of nitric oxide in tendon healing’, J Shoulder Elbow Surg, vol. 21, no. 2, pp. 238–244, Feb. 2012. [CrossRef]
- J. Chen et al., ‘MOFs-Based Nitric Oxide Therapy for Tendon Regeneration’, Nanomicro Lett, vol. 13, no. 1, pp. 1–17, Jan. 2021. [CrossRef]
- D. Singh, V. Rai, and D. K Agrawal, ‘Regulation of Collagen I and Collagen III in Tissue Injury and Regeneration’, Cardiol Cardiovasc Med, vol. 07, no. 01, 2023. [CrossRef]
- X. Liu et al., ‘The Role of Vascular Endothelial Growth Factor in Tendon Healing’, Oct. 25, 2021, Frontiers Media S.A. [CrossRef]
- G. A. C. Murrell, ‘Nitric oxide and tendon healing’, 2006. [CrossRef]
- G. A. C. Murrell et al., ‘Modulation of tendon healing by nitric oxide’, Inflammation Research, vol. 46, no. 1, pp. 19–27, 1997. [CrossRef]
- G. A. C. Murrell, ‘Oxygen free radicals and tendon healing’, J Shoulder Elbow Surg, vol. 16, no. 5 SUPPL., Sep. 2007. [CrossRef]
- W. Xia, Z. Szomor, Y. Wang, and G. A. C. Murrell, ‘Nitric oxide enhances collagen synthesis in cultured human tendon cells’, Journal of Orthopaedic Research, vol. 24, no. 2, pp. 159–172, Feb. 2006. [CrossRef]
- R. A. Cohen and T. Adachi, ‘Nitric-Oxide-Induced Vasodilatation: Regulation by Physiologic S-Glutathiolation and Pathologic Oxidation of the Sarcoplasmic Endoplasmic Reticulum Calcium ATPase’, Trends Cardiovasc Med, vol. 16, no. 4, pp. 109–114, May 2006. [CrossRef]
- B. Tong and A. Barbul, ‘Cellular and Physiological Effects of Arginine’, Mini-Reviews in Medicinal Chemistry, vol. 4, no. 8, pp. 823–832, Nov. 2012. [CrossRef]
Figure 1.
(A) Cell viability of human tenocytes treated with decreasing concentrations of Tenosan® (1.5 to 0.1 mg/ml) for 24 h, assessed via MTT assay. A cytotoxic effect was observed at doses ≥1.5 mg/ml, while lower concentrations (≤0.8 mg/ml) did not affect cell viability. (B) Quantification of IL-6 secretion in tenocytes treated with increasing concentrations of IL-1β (1–50 ng/ml) for 24 h. IL-1β induced a dose-dependent increase in IL-6 release, confirming the establishment of an in vitro inflammatory model. Data represent mean ± SD of replicates. **** p<0.0001, *** p<0.001, ** p<0.01.
Figure 1.
(A) Cell viability of human tenocytes treated with decreasing concentrations of Tenosan® (1.5 to 0.1 mg/ml) for 24 h, assessed via MTT assay. A cytotoxic effect was observed at doses ≥1.5 mg/ml, while lower concentrations (≤0.8 mg/ml) did not affect cell viability. (B) Quantification of IL-6 secretion in tenocytes treated with increasing concentrations of IL-1β (1–50 ng/ml) for 24 h. IL-1β induced a dose-dependent increase in IL-6 release, confirming the establishment of an in vitro inflammatory model. Data represent mean ± SD of replicates. **** p<0.0001, *** p<0.001, ** p<0.01.

Figure 2.
Effect of Tenosan® treatment in the modulation of levels of collagen type I (A, B), collagen type III (C,D) and their ratio (E, F) in human tenocytes. Left panel shows results under healthy conditions; right panel refers to the inflammatory model induced by IL-1β (10 ng/ml). In both models, Tenosan® modulated collagen I secretion in a dose-dependent manner, with an effect in increasing collagen I/III ratio, suggesting enhanced extracellular matrix remodeling. Data represent mean ± SD of replicates. **** p<0.0001, *** p<0.001, ** p<0.01, * p<0.05.
Figure 2.
Effect of Tenosan® treatment in the modulation of levels of collagen type I (A, B), collagen type III (C,D) and their ratio (E, F) in human tenocytes. Left panel shows results under healthy conditions; right panel refers to the inflammatory model induced by IL-1β (10 ng/ml). In both models, Tenosan® modulated collagen I secretion in a dose-dependent manner, with an effect in increasing collagen I/III ratio, suggesting enhanced extracellular matrix remodeling. Data represent mean ± SD of replicates. **** p<0.0001, *** p<0.001, ** p<0.01, * p<0.05.
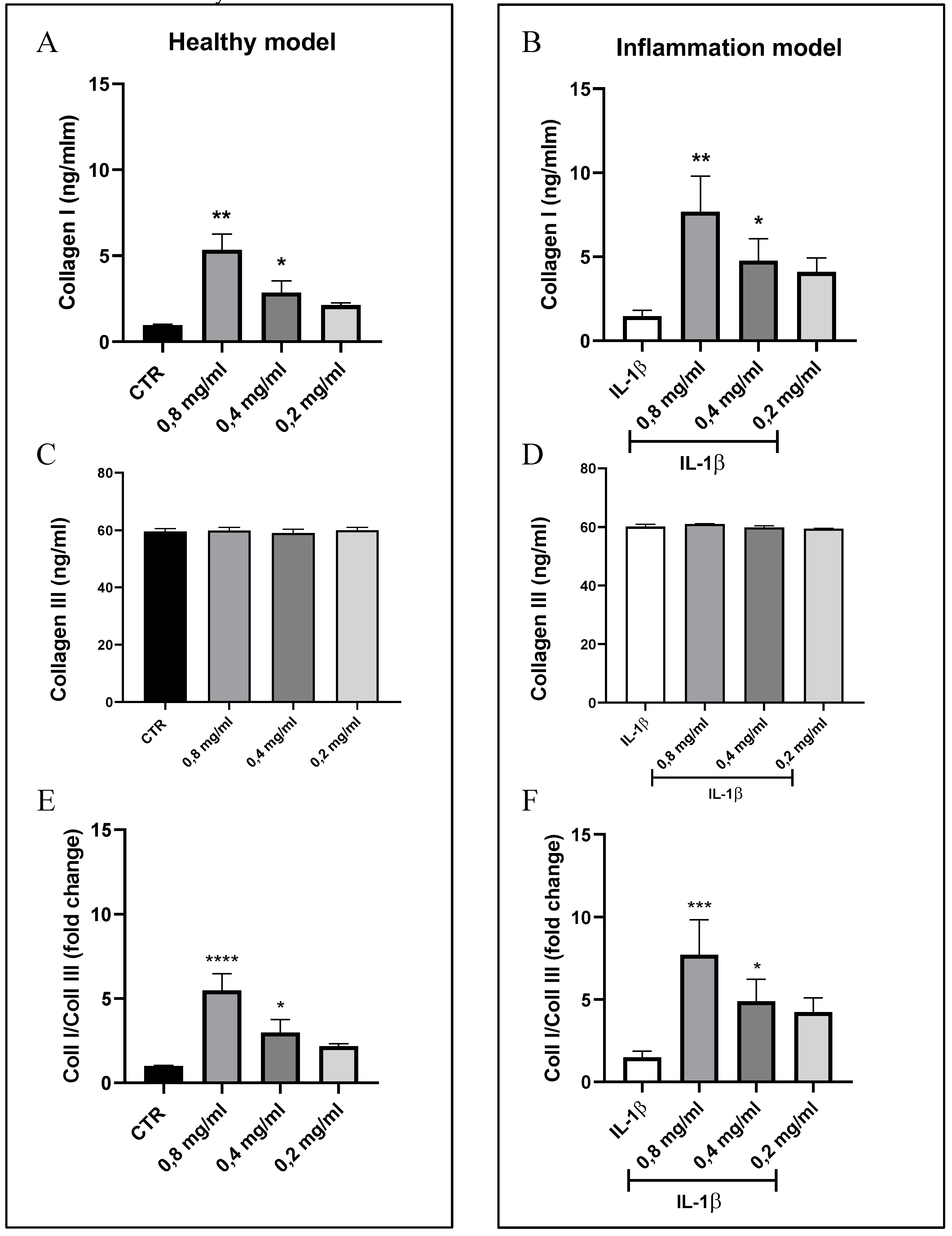
Figure 3.
VEGF levels, expressed as pg/ml, secreted by human tenocytes treated with Tenosan®. (A) VEGF levels in the supernatant of untreated (CTR) and Tenosan®-treated human tenocytes under healthy conditions. (B) VEGF levels in tenocytes exposed to IL-1β (10 ng/ml) and co-treated with Tenosan®, to mimic an inflamed condition. In both models, Tenosan® treatment resulted in reduction of VEGF secretion, suggesting a modulatory effect on angiogenesis. Data are expressed as mean ± SD of replicates. *** p<0.001, ** p<0.01.
Figure 3.
VEGF levels, expressed as pg/ml, secreted by human tenocytes treated with Tenosan®. (A) VEGF levels in the supernatant of untreated (CTR) and Tenosan®-treated human tenocytes under healthy conditions. (B) VEGF levels in tenocytes exposed to IL-1β (10 ng/ml) and co-treated with Tenosan®, to mimic an inflamed condition. In both models, Tenosan® treatment resulted in reduction of VEGF secretion, suggesting a modulatory effect on angiogenesis. Data are expressed as mean ± SD of replicates. *** p<0.001, ** p<0.01.
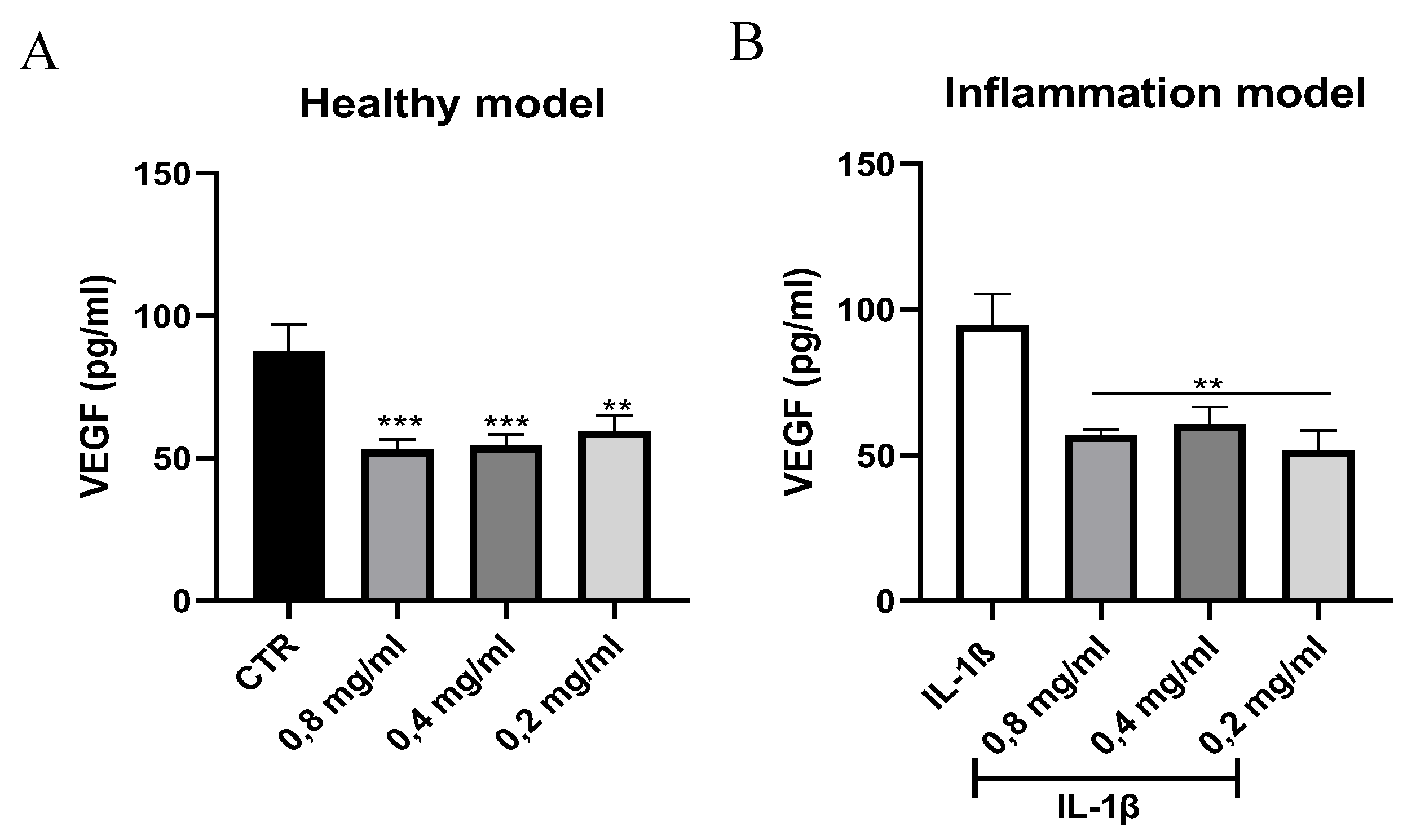
Figure 4.
NO levels (μM) produced in human tenocytes treated with Tenosan®. (A) NO levels measured in untreated (CTR) and Tenosan® treated tenocytes under physiological conditions. (B) NO levels in tenocytes exposed to IL-1β (10 ng/ml) and co-treated with Tenosan®, to simulate an inflamed tendon condition. In both models, Tenosan® induced a dose-dependent increase in NO production, suggesting its pro-regenerative activity. Data represent mean ± SD of replicates. **** p<0.0001, *** p<0.001, * p<0.05.
Figure 4.
NO levels (μM) produced in human tenocytes treated with Tenosan®. (A) NO levels measured in untreated (CTR) and Tenosan® treated tenocytes under physiological conditions. (B) NO levels in tenocytes exposed to IL-1β (10 ng/ml) and co-treated with Tenosan®, to simulate an inflamed tendon condition. In both models, Tenosan® induced a dose-dependent increase in NO production, suggesting its pro-regenerative activity. Data represent mean ± SD of replicates. **** p<0.0001, *** p<0.001, * p<0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



