Submitted:
02 July 2025
Posted:
08 July 2025
You are already at the latest version
Abstract
People worldwide are living longer. However, the number of years with quality of life or ‘healthspan’ is decreasing due to age-related disorders/diseases. Carotenoids (health-promoting phytonutrients) benefit or enhance healthspan due to their powerful antioxidant and anti-inflammatory actions via daily fruit and vegetable consumption (FVC) that are metabolized and found in blood, skin and other tissues. Skin scanner spectroscopy-based technology that non-invasively quantifies carotenoid levels addresses bias/error found in dietary questionnaires and difficulties with processing invasive blood samples. The objective of this review was to determine whether skin carotenoid measurements are a predictor of antioxidant activity for improved healthspan by understanding: a) the chemical nature of carotenoids, the basic distribution of carotenoids in food products plus nutraceutical supplements and a comparision of the antioxidant activities of carotenoids, b) the benefits of carotenoids antioxidant activity in health/disease and how carotenoids antioxidant activities enhance health, c) the methods of spectroscopy quantification of skin carotenoids, and d) how data mining of published studies can determine global skin carotenoid antioxidant scores (via non-invasive methods) can contribute to helping address the declining trend of healthspan and provide people with actionable measures to increase their carotenoid intake via FVC and/or supplementation. In general, the findings of this review support the use of spectroscopy-based carotenoid antioxidant quantification for estimating and validating FVC in diverse populations of adults and children. However, further research is warranted to confirm this concept, especially with the ongoing advancements in spectroscopy-based technologies that will better quantify skin carotenoids in the future.
Keywords:
carotenoid
; spectroscopy measurement
; lifespan
; healthspan
; diet
; supplementation
; lifestyle
; factors
; nutrition
1. Introduction
People are living longer, and in fact, increases in life expectancy worldwide not only are recognized as a societal achievement but also have social/economic challenges and health concerns. For example, by 2030, 1 in 6 people in the world will be aged 60 years or older [1]. Notably, data show that while lifespan is increasing, the number of years with quality of life or ‘healthspan’ is decreasing (healthspan represents having good quality of life free of significant illnesses or disease) [2]. This is evident where cardiovascular, cancer, neurodegenerative and metabolic disorders [like obesity and type 2 diabetes (T2D)] represent the major four cornerstones of age-related diseases [3].
Optimal health and wellness can be greatly influenced by factors such as diet, lifestyle, quantity and quality of sleep, and social connections, etc. [4,5]. These form important foundations to maintain optimal wellbeing throughout one’s entire life [4,5]. Various factors contribute to aging or ill health, but as early as the 1950s it was proposed that aging is caused by free radical reactions [6]. However, recent theories include a link between epigenetics and lifestyle [7], and the most recent characteristics of aging include at least 9 factors that cover genetic, biochemical, molecular and cellular dysfunction/communication that have been reported elsewhere [8,9]. There is universal agreement that free radicals are involved in the physical, biochemical, and pathological changes associated with aging [10,11,12]. Clearly, oxidative stress leads to damage of proteins, lipids, and DNA, and this damage accumulates and increases with age that is associated with age-related diseases [10,11,12].
Diet is a key contributor providing many important nutrients to combat oxidative stress and promote health [11,12]. Dietary patterns have been identified, which are associated with healthy aging such as diets rich in plant-based foods and diets having moderate amounts of healthy animal-based foods [13,14]. One of the emerging heroes of dietary interventions are carotenoids due to their antioxidant ability to neutralize free radicals and their anti-inflammatory actions [15,16]. Carotenoids are naturally occurring pigments found in plants and have been linked to various health benefits including reducing the risk of age-related diseases and promoting healthy aging [13,14,15,16]. Studies suggest that higher dietary intake of carotenoids such as β-carotene, lutein, and zeaxanthin are associated with slower aging at the biological level [17]. For example, a cross-sectional study in 27,338 adults from NHANES 1999-2018 found that increased dietary intakes of carotenoids was associated with parameters reflecting lower biological aging [18]. But how would an individual know (determine) their carotenoid activity levels? Carotenoids derived from fruit and vegetable consumption (FVC) are metabolized then deposited into the blood, skin and tissues that enhance antioxidant activity [19]. The best method (traditionally) for monitoring carotenoids levels was to analyze blood samples using high-performance liquid chromatography (HPLC) or mass spectrometry (MS), which made the process invasive and time-consuming [19]. The advancements in technology have provided a non-invasive method to determine carotenoid antioxidant levels by scanning the skin by via spectroscopy measurements to quantitatively estimate and validate the FVC in diverse populations of adults and children [19].
Thus, the aim of this narrative review was to present: a) the chemical nature of carotenoids, the basic distribution of carotenoids in food products plus nutraceutical supplements and a comparison of the major carotenoids antioxidant activities, b) the benefits of carotenoids antioxidant activity in health/disease and how carotenoids antioxidant actions enhance health, c) the methods of spectroscopy quantification of skin carotenoids, and the main objective d) how data mining of published studies can determine global skin carotenoid antioxidant scores by non-invasive methods can contribute to helping address the declining trend of healthspan and provide people with actionable measures to increase their carotenoid intake via FVC and/or supplementation to boost their antioxidant activity. This was accomplished by identifying journal articles and reviews (with emphasis over the past 5 years; 86% of citations were within this interval) using the keywords – carotenoids, antioxidants, activity, spectroscopy measurement, disease/disorders, lifespan and healthspan using different keyword combinations (retrieved from May 20 to June 10, 2025). Over 3,100 articles were identified using the following databases [PubMed (US National Library of Medicine at the National Institutes of Health); Google Scholar; Science Direct and Scopus by Elsevier]. Further review limited this number to 1,200 articles (removing duplicates, off topic, etc.), and this was reduced to 132 articles that fit the criteria for inclusion (specific combination of keywords). Background references on carotenoids antioxidant activity where appropriate were without a year-limit range. This overview is based on previously conducted studies and does not contain new data/results of human participants or animals performed by the authors. In addition, we present the findings from mining a database of previously published reports of several million non-invasive skin carotenoid measurements to reveal lifelong profiles of carotenoid intake.
2. Carotenoids: Chemical Nature, Distribution in Foods & Supplements and Comparison of Antioxidant Activities
Carotenoids are essential compounds for the survival of photosynthetic plants, which characterize their antioxidant activity [16,20]. More than 600 naturally occurring carotenoids, fat-soluble yellow, orange, red and green leafy pigments mostly synthesized in fruits and vegetables, have been identified [20]. Traditionally, carotenoids are classified into two main structural groups: hydrocarbon carotenoids called carotenes that only have carbon and hydrogen atoms, and oxygenated carotenoids called xanthophylls that have different functional groups (i.e., the presence or absence of oxygen atoms) in addition to carbon and hydrogen atoms (Figure 1) [16,20].
Animals and humans cannot synthesize carotenoids; therefore, they must obtain these compounds from their diet [14,16,20]. Notably, forty to sixty carotenoids have been reported in humans, but the six most studied major carotenoids are α-carotene, β-carotene, lycopene, β-cryptoxanthin, lutein and zeaxanthin that are metabolized and then accumulate in human plasma, skin and tissues (Figure 2), which contribute to the antioxidant activity within the body [16,20].
The human diet contains two sources for vitamin A: preformed vitamin A (retinol and retinyl esters) and provitamin A carotenoids [16,20]. Preformed vitamin A is found in foods from animal sources including dairy products, eggs, fish and meats [14,16,20,21]. Provitamin A carotenoids are plant pigments that include α-carotene, β-carotene, and β-cryptoxanthin [16,20]. This classification is denoted by how the body converts provitamin A carotenoids into vitamin A in the intestine [20,21]. Other carotenoids in food such as lycopene, lutein, and zeaxanthin are not converted into vitamin A and are referred to as non-provitamin A carotenoids. They have other important activities not involving vitamin A formation such as acting as potent antioxidants protecting against oxidative stress, promoting eye, liver and immune health and decreasing the risk of certain types of cancer [21].
The major carotenoids present in food products, β-carotene, α-carotene, β-cryptoxanthin, lycopene, lutein and zeaxanthin, contribute to the antioxidant actions within the body [20,21]. However, the contents of carotenoids can vary widely due to various factors such as climate, soil and cultivation [20,21]. The food sources that contain the six major carotenoids at high levels (20 to 50 mg/100 grams) are β-carotene in carrots, paprika and red peppers; and lycopene in tomatoes. At moderate levels (5 to 19 mg/100 grams) are α-carotene in carrots, red peppers, pumpkin and carrot juice; β-carotene in carrots, red peppers, acai berry juice, carrot juice, chili powder, kale, parsley, pumpkin, spinach and turnip greens; β-cryptoxanthin in cayenne paprika, red peppers and squash (winter butternut); lutein & zeaxanthin in chard, chicory greens, kale, paprika, peppers, spinach, turnip greens, cress, basil, parsley, radicchio and watercress; and lycopene in guavas and tomato products (juice and soup). At low levels (0.4 to 4 mg/100 grams) are α-carotene in carrots, chili powder, and peppers; β-carotene in apricots, broccoli, cabbage (Chinese), cherries, chicory greens, endive, lettuce (green & red leaf), melons, oregano, parsley, peas (green), green peppers, plums, pumpkin, sweet potato, thyme and watercress; β-cryptoxanthin in chili powder, orange juice, persimmons, papayas, tangerines and squash (winter Hubbard); lutein & zeaxanthin are in asparagus, beans, broccoli, brussels sprouts, carrots, celery, corn, fava, leeks, lettuce (green & red leaf), kale, oregano, parsley, green peas, pistachio, pumpkin, squash-zucchini, thyme and tomatoes; lycopene is in grapefruit (pink & red), papayas and watermelon according to the US Department of Agriculture (USDA) [22].
Dietary supplements are also a source of carotenoids to increase antioxidant activity for body defenses [20,21]. Vitamin A is available as a stand-alone supplement and found in most multivitamins (in the form of retinyl acetate, retinyl palmitate, provitamin A beta-carotene, or some combination thereof) [21,23]. The amounts of vitamin A in supplements vary widely, but 3,000 microgram retinol activity equivalents (RAE) account for differences in the bioactivities of retinol and provitamin A carotenoids, all of which are converted in the body into retinol. Lutein, zeaxanthin, and lycopene are often combined in supplements particularly for eye health [15,16,17,21,23]. These carotenoids act as antixoidants protecting cells from damage and have been linked to reduced risk of eye diseases like age-related macular degeneration [15,16,17]. Lutein and zeaxanthin are particularly concentrated in the macula of the eye, where they help filter blue light and protect against oxidative stress [17,24]. Lycopene, while not as directly concentrated in the eye as lutein and zeaxanthin, also has antioxidant properties and can contribute to overall eye health [15,16,17].
There are several methods to determine antioxidant activity or capacity related to the clinical significance of carotenoids [25,26]. In brief, among all of the carotenoids, lycopene is reported to posess the greatest antioxidant activity (when compared to α-carotene, β-carotene, β-cryptoxanthin, lutein and zeaxanthin, etc.) plus it has greater antioxidant potential compared to astaxanthin, canthaxanthin, bixin, glutathione, crocin or lipoic acid [27,28,29,30]. For example, lycopene has two-times or up to one hundred-times more antioxidant potential than β-carotene and vitamin E [28,29,31,32]. So, an arbitary ranking of the carotenoids according to their antioxidant activity from one perspective might be: lycopene > α-carotene > β-carotene > β-cryptoxanthin > lutein & zeaxanthin [33]. For example, α-carotene seems to have more antioxidant potential compared to β-carotene [33] and is associated with muscle strength, while other carotenoids did not display this assocation [33]. Also, β-cryptoxanthin and α-carotene appears to have greater bioavailability than β-carotene in human dietary patterns in different countries [34]. β-Carotene is better as a provitamin A source, while lutein & zeaxanthin are better for age-related conditions for eye health [24,35]. Thus, in certain contexts this ranking may shift dependent upon the method of quantifying antioxidant actvity and health application parameters [36].
3. Benefits of Carotenoids in Health/Disease and How They Enhance Antioxidant Activity
Carotenoids are a diverse group of pigments synthesized by plants and other non-photosynthetic bacteria, and fungi [20,36] and are well known for their antioxidant properties and protective roles in various human biological conditions [17,18,20,36]. Recall, carotenoid compounds are not synthesized by humans but are essential for several biological functions, so they need to be obtained by dietary sources [17,18,20,36]. Dietary carotenoids, mainly from fruits and vegetables, have been associated with many health benefits, which are summarized below.
3.1. Carotenoids ↑ Antioxidant Capacity and ↓ Reactive Oxygen Species (ROS)
Carotenoids act as powerful antioxidants, which are known for their ability to quench singlet oxygen and scavenge free radicals, preventing damage to living cells [17,18,20,36,37]. This reduction of ROS plays an important role in increasing the antioxidant capacity of human blood and plasma, organs/glandular/tissue and cellular components [skin (stratum corneum high concentration), eyes, liver, adipose tissue, adrenal glands, gonads, cell membranes/lipoproteins and chylomicrons, etc.] [17,18,20,36]. In plants they are crucial for protecting against photo-oxidative stress. In humans, they play an indispensable role in the overall antioxidant defense system by upregulating antioxidant enzymes via the stimulating of Nrf2, which is the master gene for further antioxidant production, detoxification enzymes and mitochondrial function [20,37,38,39,40]. Additionally, carotenoids influence other cellular signaling pathways such as inhibiting the pro-inflammatory factor NFkB [17,18,20,36,37,38,39,40].
3.2. Benefits of Carotenoids as a Micronutrient (acts as a precursor for vitamin A)
Vitamin A, derived from carotenoids, plays a vital role that protects the human body from damage caused by free radicals [17,20,36,37,39,40]. Due to carotenoid’s antioxidant activity, other health benefits include boosting immune function, eye and skin health, and carotenoid’s pro-vitamin A actions support growth and development of bone remodeling and cell growth/function as well as reduce the risk of certain cancers, heart disease and cognitive decline [17,20,36,37,38,39,40], which will be presented in later sub-sections.
3.3. ↑ Healthspan (↓ Aging, Chronic and Age-related Diseases) with Carotenoids
Several studies suggest that carotenoids can positively impact aging and healthspan [17,18,20,37,39,40]. Increased dietary intake or nutraceutical supplementation of carotenoids has been linked to lower biological aging parameters by reducing oxidative stress [20,37,39,40]. Oxidative stress (OS) is an imbalance of free radicals and antioxidants in the body that leads to cell damage, lipid peroxidation, protein oxidation and DNA fragmentation, which can lead to multiple cells signaling dysfunctions [20,37,40,41]. OS plays a role in many conditions like cancer, diabetes, kidney disease, asthma and chronic obstructive pulmonary disease (COPD), and damage to the lining of blood vessels (endothelium), contributing to hypertension, atherosclerosis and several other cardiovascular disorders [20,37,40,41,42,43,44,45,46]. For example, Sahashi et al. in 2022 showed an inverse association between fruits and vegetables intake and all-cause mortality, suggesting a potential contribution to carotenoids for this outcome [45]. Additionally, Bohn et al., in 2021, reported dietary intake recommendations based on carotenoid intake corresponding to blood and tissue concentrations of carotenoids [46]. In 2023, Fekete et al. showed that nutritional supplementation may be an appropriate treatment to consider for COPD patients, especially the supplementation of carotenoids with their high antioxidant activity [47]. Finally, in 2024, Chen et al. showed from 19,280 participants in the NHANES survey from 2009 to 2018 that higher dietary intake of carotenoids was associated with reduced biological age acceleration, underscoring their protection role against aging [48].
3.4. ↓ Inflammation & Oxidative Stress (OS) with Carotenoids
Since carotenoids are powerful antioxidants that can scavenger free radicals and protect against oxidative stress (OS), they also interact with and inhibit inflammatory pathways, like NFkB, to reduce the production of pro-inflammatory molecules [20,39,40]. Furthermore, lutein has been shown to reduce retinal inflammation and prevent retinopathy [49]. In this case, lutein can suppress activation of NFkB, inhibit the inflammatory cytokines (IL-1β, IL-6, TNF-α and the inflammatory enzymes (cyclooxygenase-2 and inducible nitric oxide synthase) [49]. Carotenoids have been shown to reduce OS and inflammation to protect against kidney disease by enhancing mitochondrial function [50]. Finally, the potent antioxidant effects of carotenoids have demonstrated anti-inflammatory actions in cardiovascular disease [51].
3.5. ↓ Risk of Cardiovascular Disease with Carotenoids
Several studies suggest that carotenoids may help reduce the risk of cardiovascular disease (CVD), which have been reviewed elsewhere [15,16,17,20,36,37,39,40]. In brief, carotenoids, found in fruits and vegetables, act as strong antioxidants, and apparently prevent cholesterol oxidation in arteries (i.e., atherosclerosis), a key process in the development of CVD [20,39,40]. By preventing cholesterol oxidation in arterial walls, carotenoids slow down the buildup of plague, enhance endothelial cell wall function, reduce blood pressure and prevent clots [52,53]. In the study by Obana et al. skin carotenoid levels were estimated via refraction spectroscopy, which the authors suggested may be a good indicator for recommending carotenoids to prevent CVD [54]. Various studies have shown that higher intakes of carotenoid-rick foods or higher blood concentrations of carotenoids are linked to a lower incidence of CVD and cardiovascular mortality [53,54,55]. Finally, in 2015, Gammone et al. examined how carotenoid compounds might help lower blood pressure, reduce inflammation, and improve insulin sensitivity in muscle, liver and adipose tissues, which are which are factors that can contribute to cardiovascular health [55]. While the current evidence suggests that carotenoids reduce the risk of CVD, more research is warranted to understand the mechanisms by which they exert the many protective effects.
3.6. ↓ Eye Disorders (cataracts & age-related macular degeneration) with Carotenoids
Carotenoids help to maintain the macula in the eyes, which often degenerate with age [17,18,20,39,40]. Specifically, certain carotenoids like lutein and zeaxanthin can help reduce the risk of age-related macular degeneration (AMD) and cataracts [17,18,20,39,40]. Recall, Obana et al. in 2020 showed the positive effects of an antioxidant supplement containing high dose of lutein and zeaxanthin on macular pigment were correlated with skin carotenoid levels [35]. These powerful antioxidants protect the eye from damage caused by free radicals, OS and filter out harmful blue light, which can damage eye tissue [20,35,39,40] and help reduce the risk of cataracts [56,57]. A systematic review of carotenoids in the management of age-related macular degeneration was reported by Lem et al. in 2021 [58]. Their review highlighted the neuroprotective benefits of carotenoids, especially lutein and zeaxanthin, in conditions like glaucoma, AMD and managing diabetic retinopathy, which other investigators have also reported on [59,60,61].
3.7. Carotenoids ↑ Skin Health & Acts as a UV Protectant
Much research attention has been focused on carotenoid’s positive impact on skin health and as a protectant against ultraviolet (UV) rays, which have been reviewed elsewhere [62,63,64,65]. In summary, carotenoids, especially beta-carotene and lycopene, offer several skin health benefits, including photo-protection against sunburn, reducing skin aging, improving skin elasticity, hydration and stimulating collagen and elastin production to reduce the appearance of wrinkles and improve skin firmness [16,17,20,37,39,62,63,64,65,66]. Additionally, carotenoids may help reduce inflammation and improve skin texture [62,63,64,65,66]. Recent studies suggest the role of ingestible carotenoids in reference to skin protection inhibit molecular markers of OS such as intercellular adhesion molecule 1, heme oxygenase-1, and matrix metalloproteinases 1 and 9 [67]. However, while carotenoids offer some photoprotection, they should not replace the use of broad-spectrum sunscreen products. Reviews of clinical studies have shown that lycopene to be a promising topical and nutraceutical product for cosmetic applications to decrease skin photodamage and skin photo-aging and for the treatment of melasma [68,69,70]. Finally, Varghee et al. presented a recent report, in 2025, on the mechanisms of how carotenoids enhance skin health [71].
3.8. ↑ Immune Health via Carotenoids
There has been great interest in the potential role of carotenoids in enhancement of the immune response. Children with vitamin A deficiency suffer from compromised immunity and have difficulty protecting themselves from xerophthalmia (night blindness) and for morality from infections like measles or diarrhea [72]. In general, carotenoids, β-carotene and lutein specifically, are known for their role as antioxidants, and can benefit the immune system by supporting cell-mediated (increased lymphocyte production) and humoral immune (increased production of antibodies by B cells) responses, boost immune cells to stimulate phagocytic and bacteria-killing blood neutrophils and peritoneal macrophages and enhance natural killer (NK) cell cytotoxicity, which helps the immune system combat abnormal cells [73,74,75,76]. The presence of carotenoids in immune cells protects them against OS and cellular damage thus helping to ensure optimal functions that include apoptosis (programmed cell death), cell signaling, and gene regulation [74,75,76]. For example, carotenoids and their metabolites may interact with nuclear receptors involved in immune system regulation and influence downstream target genes and proteins involved in OS, inflammation and cellular differentiation [77]. Such immune system differentiation can act through vitamin-A-active retinoids receptors RAR/RXR [77]. Earlier studies on carotenoids, in the late 1990s, showed that β-carotene enhanced NK cells especially in elderly men [78,79], and a diet low in carotenoids had a suppressive effect on the mitogenic proliferation of blood lymphocytes, which was corrected with when the subjects increased their dietary intake of vegetables rich in carotenoids [80].
3.9. ↑ Bone Health (↓ in Osteoporosis) with Carotenoids
Studies have shown that higher intake of carotenoids is associated with a lower risk of osteoporosis and a higher bone mineral density (BMD), which have been reviewed elsewhere [16,17,37,39,81]. For example, higher β-carotene, β-cryptoxanthin along with lutein/zeaxanthin intake has been linked to positive effects on bone health, particularly in postmenopausal women [82,83,84,85]. Lycopene may offer some protection against bone loss, especially in the lumbar spine in women and pelvis (hip) region in men [86]. Thus, carotenoids may promote bone health through their antioxidant activity particularly in reducing OS and inhibiting bone resorption while stimulating bone formation [37,39,82,83,84,85]. While promising, more research is needed to fully understand the mechanisms, and to what extent carotenoids benefit bone health.
3.10. ↓ Neurodegenerative Disease (Alzheimer’s) with Carotenoids
Due to the very high interest in neurodegenerative diseases (Alzheimer's, Huntington’s, Parkinson’s and amyotrophic lateral sclerosis), there is an abundance of research suggesting that carotenoids may offer neuroprotective benefits and play a role in supporting brain health [16,20,37,39,66,87,88,89,90,91,92,93]. Neurodegenerative diseases are characterized by the gradual loss of neuronal structure/function and other protective mechanisms that lead to the loss of cognitive and motor function and intellectual impairment [94]. Currently, there are no cures or effective treatments for neurodegenerative diseases. However, carotenoids acting as: 1) powerful antioxidants, protect brain cells from damage by free radicals [88,89], 2) anti-inflammatory compounds to reduce inflammation, a key factor in neurodegeneration [88,91,92,93,94,95], 3) inhibitors of or reduce microglial function [66] and 4) anti-plague agents that reduce or prevent the buildup beta-amyloid (Aβ) plagues and fibril formation that are the hallmarks of neurodegeneration [91,92,93,96,97,98,99].
It is beyond the scope of this sub-subsection to present even a fraction of the available research that shows carotenoids help prevent age-related neurodegeneration. However, there appears to be a significant correlation (from several studies) between higher carotenoid levels with better cognitive function in humans [89,90,91,93,95], decreased incidence of Alzheimer’s disease and disease remediation [37,39,66,89,91], and even protection of the physical brain structures with aging [100]. For example, in a cross-sectional study of 2,050 people (median age, 61 years, 61 % female) underwent magnetic resonance imaging (MRI) scans to determine whether intake of carotenoids protected against neurodegenerative parameters (e.g., choroid plexus volume, lateral ventricle volume and perivascular spaces in the brain) [100]. The investigators showed that β-carotene concentrations in serum were associated with better neurological volumes and parameters, most likely due to the antioxidant activity maintaining the glymphatic system function of the brain [100]. Specifically, the glymphatic system is a unique clearance pathway in the brain that relies on cerebrospinal fluid (CSF) and glial cells to remove metabolic waste and other harmful substances and is an emerging therapeutic approach for neurological disorders [101].
While many studies have examined carotenoids, in general, other investigations have focused on lutein and lycopene that have promising in vitro and in vivo results supporting the amelioration of neurodegenerative parameters [102,103,104,105,106]. Finally, carotenoids are thought to act through several mechanisms in the fight against neurodegenerative diseases by- enhanced antioxidant defenses via the Keap1/Nrf2 pathway to decrease ROS and neuroinflammation by suppressing cytokines and reducing apoptotic factors, while promoting clearance of Aβ plagues [39,66,87,89,92,93]. Thus, carotenoids may help to reduce the risk of neurodegenerative disorders that are associated with aging.
3.11. ↓ Depression with Carotenoidss
Depression is often linked to neurodegenerative diseases and recent evidence suggests that both share mechanisms involving genetic and molecular pathophysiology, which has important implications for early treatment and therapeutic development [107]. For example, Wingo et al. in 2022, found an approximate 2.6-fold increase in protein-protein interactions among psychiatric and neurodegenerative disorders compared to expected rates by chance [107]. Depression is an emotional disorder and one of the leading causes of disability worldwide [108]. Women have a higher prevalence compared to men for depression, which peaks after postpartum and at or around menopause [109]. Currently, the pathophysiological mechanism of depression has not been elucidated, but in recent years the role of dietary supplements in the treatment/prevention of depression has been a topic of much research.
Several studies suggested that dietary intake of carotenoids (and in some investigations plasma carotenoids) are associated with a reduced risk of depressive symptoms by acting as strong antioxidants that protect neural tissue and brain function [111,112,113,114,115,116,117,118]. In general, higher consumption of carotenoids is linked to lower rates of depression and mood disorders [111,112,114,115,116]. Specifically, α-carotene, β-carotene, β-cryptoxanthin, lycopene, and lutein + zeaxanthin have been identified as having potential protective effects against depressive symptomatology [113,114]. Presumably, the mechanism by which carotenoids decrease the risk of depression is by reducing OS and inflammation both of which are implicated in the development of depression [111,112,113,114,115,116]. Recent findings, in 2025, suggest an association between dietary and plasma lutein + zeaxanthin lowering the risk of depression [117], which should be confirmed by randomized control trials to explore in relationship. Finally, Lin and Lan, in 2025, identified a U-shaped relationship with a reduction in depression risk associated with dietary lycopene suggesting that there may be an optimal levels of lycopene intake, and beyond which these benefits may plateau or even reverse [118]. While there is scientific evidence that increases in carotenoid intake may reduce the risk of depressive symptoms, further research is necessary to validate these findings and understand the mechanism that takes place in the brain.
3.12. ↓ Metabolic Syndrome, Type 2 Diabetes (T2D) & Weight Gain with Carotenoids
Several studies suggest that carotenoids are associated with reduced risk of metabolic syndrome [119,120,121,122,123,124], type 2 diabetes (T2D) [16,39,66,77,125,126,127], and weight gain [128,129,130,131,132].
For metabolic syndrome, there is an inverse association between higher intake of total carotenoids and the presence of metabolic syndrome [119,120,121,122,123,124]. Some studies have shown that specific carotenoids like α-carotene, β-carotene, lutein and zeaxanthin have been linked to reduced risk of metabolic syndrome particularly in women [124]. In this regard, carotenoids have an advantageous role in regulating lipid metabolism, reducing blood sugar levels, augmenting the activity of antioxidant enzyme (via Nrf2), averting tissue and cellular damage, and may reduce the risk of metabolic syndrome.
In examining T2D, evidence suggests that dietary intake of carotenoids (especially β-carotene) is associated with a reduced risk of T2D [3,9,16,66,77,125,126,127]. Also, lutein and zeaxanthin supplementation has been shown to have a positive impact on regulating sugar levels (HbA1c) [129].
Weight loss has also been shown to be linked to higher intake of carotenoids, where lower levels of carotenoids increase adiposity, including increased waist circumference, and visceral and subcutaneous fat mass. [125,128,129,130,131]. From animal studies some evidence suggests that carotenoids promote fatty acid oxidation, which may account, in part, for lower weight gain [129,130,131]. Moreover, carotenoids have been shown to improve obesity and fatty liver disease via the gut microbiome [132]. While these studies show associations, they may not prove causation, and the need for randomized controlled trials is needed to confirm the causal link between carotenoids and reduced risk of metabolic syndrome, T2D, and weight gain.
3.13. ↑ Gut Microbiome with Carotenoids
Carotenoids like lycopene, and especially β-carotene, can promote the growth of beneficial bacteria like Bifidobacterium and Lactobacillus, while potentially inhibiting the growth of less desirable bacteria (i.e., Proteobacteria that is associated with inflammation), and thereby, contributes to a more divers and balanced gut microbiome [16,39,77,132,133,134,135,136,137,138]. Additionally, studies have shown that carotenoids supplementation can lead to higher alpha diversity in the gut microbiome indicating a more diverse and robust microbial community [134]. The beneficial effects of carotenoids on the gut microbiome may be attributed to several factors that include: a) anti-inflammatory properties to reduce inflammation in the gut, b) antioxidant effects protecting gut lining from damage caused by free radicals and promoting growth of beneficial bacteria, and immune system modulation, by enhancing IgA production, which is important for gut barrier function and preventing dysbiosis [132,133,134,135,136,137,138]. Hence, incorporating carotenoids into the diet may positively impact the gut microbiome in several ways.
3.14. ↓ Incidence of Certain Cancers with Carotenoids
There is some evidence suggesting that carotenoids can reduce the incidence of certain cancers [16,37,39,66,139,140,141,142,143,144]. In fact, some reviews suggest that carotenoids can reduce cancer risk in many tissues and organs of the body [37,39,143], but more research needs to be done in this regard. However, studies have shown that higher levels of carotenoids in the blood or via dietary intake are associated with a lower risk of breast and prostate cancer [139,140,141,142,143,144]. Additionally, some carotenoids, like β-carotene, lycopene, and lutein, have been linked to protective effects against lung and gastric cancers [37,39,139,141,144]. How carotenoids may reduce cancer risk include: a) enhancing antioxidant action to help neutralize free radicals and reduce oxidative stress [37,66,139,140,141,142,143,144], b) affecting cell signaling pathways, which can influence cell growth, division, and death (i.e., apoptosis) in cancer cells along with interfering with the cell cycle progression [37,66,139,142,143,144], and c) reducing inflammation and/or modulating the expression of genes involved in cancer progression [37,66,139,142,144]. While carotenoids have shown promise in reducing cancer risk, some studies found no benefit, and thus, further research is needed to determine the optimal levels of carotenoids intake and/or supplementation. This is important because high concentrations of carotenoids have pro-oxidant activity, which could lead to increased OS and cellular damage [143]. Finally, this is an intriguing mechanism where optimizing OS via carotenoids in normal cells while enhancing OS in cancer cells, has been reviewed as a potential emerging technology to treat cancer [145].
3.15. ↑ Oral and Periodontal Health with Carotenoids
There is early research suggesting that carotenoids enhance oral periodontal health through their antioxidant and anti-inflammatory properties [39,146,147,148,149,150,151,152,153]. Some studies have shown that low blood levels of β-carotene, β-cryptoxanthin and lycopene have been associated with increased periodontitis prevalence [149,150,151,153]. Particularly, people with diabetes are more prone to periodontitis due to elevated OS and inflammation [152]. Carotenoids, especially lutein and zeaxanthin, might be beneficial in mitigating periodontitis in the population [146,152]. Since this is a relatively new research area, more investigations are needed to determine a clear link to carotenoid’s protective effects and to identify the optimal dosage for enhanced periodontal health.
3.16. ↑ Muscle Strength and Physical Function with Carotenoids
Muscle mass plays a crucial role in metabolic health, disease prevention, and overall longevity. Skeletal muscle, the body's largest organ by mass, regulates glucose metabolism and energy expenditure, thereby reducing the risk of metabolic diseases such as type 2 diabetes. [13,14,16,17]. As people age, muscle mass declines, leading to conditions like sarcopenia, which increases frailty and other health complications [13,16,17].
New research interest in carotenoids protecting muscle from damage by free radicals by their antioxidant activity and protecting muscle from inflammation have been reported [33,66,154,155,156,157,158,159,160,161]. Studies have shown that carotenoids, like β-carotene, may promote muscle growth and hypertrophy particularly when combined with resistance training [33,154,155,156,157,158,160,161]. Also, carotenoid intake has been linked to slower decline in muscle strength and physical function with age suggesting that they may help protect against age-related muscle loss (sarcopenia) [155,158]. For example, higher intake of carotenoids was associated with increased in grip strength and faster gait speed in adults [154,156,157,159], while low serum carotenoid levels were linked with poor muscle strength in older women [154,156,157,158,160]. While more investigations are needed to confirm these findings linking carotenoids to muscle health, these results highlight the protective effects of carotenoids in attenuating loss of muscle and physical function in older adults, which is an important aspect of health with aging.
3.17. Summary Linking Carotenoid Intake to Enhancing Healthspan
In summary carotenoids act through a variety of mechanisms to enhance healthspan. For example, they influence gene expression by regulating transcription factors and signal transduction pathways involved in aging [16,17]. Carotenoids may enhance SIRT1 activity, a critical enzyme linked to cellular longevity and stress resistance and can reduce chronic inflammation contributing to age-related disease by inhibiting NFkB signaling [37,39,43,44,66]. Carotenoids exert additional antioxidant activity by neutralizing ROS, inhibiting additional inflammatory compounds, and modulating cytokine production like interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), which contribute to systemic inflammation [43,44,73,74,75,76,77,78,79]. Carotenoids also improve mitochondrial function through their antioxidant activity by reducing oxidative damage and enhancing cellular energy metabolism [49,50]. Also, more direct effects on immune modulation include the ability of β-carotene to increase immunoglobulin synthesis, supporting adaptive immune defenses and stimulating macrophage function and T-cell proliferation, to strengthen innate immunity [43,44,75-80. Finally, carotenoid supplementation has been linked to protection from infections by fortifying both the epithelial barrier and immune surveillance mechanisms [133,162]. In this regard, Zhuang et al, in 2022, examined the effects of oral carotenoids on oxidative stress and other parameters in a 20-year meta-analysis showing that intake duration of 8 weeks should be sufficient to reach effective systemic concentrations for improved physiological function [163].
Figure 3 (below) displays the pleiotropic impact carotenoids have on 16 different functions in cellular, metabolic, physiological and health conditions in humans
4. Spectroscopy Methods for Quantification of Skin Carotenoids
Since humans cannot synthesize carotenoids, the concentrations of these pigments traditionally were determined, in blood samples, which provided the best markers of FVC through foods or supplements [164,165]. However, due to the invasive nature of blood collections and the associated high costs of conducting large-scale studies alternative methods have emerged, where non-invasive techniques for estimating carotenoid levels that reflect FVC were developed and have been in use for over 20 years that use spectroscopy-based technologies [164,165]. The two major methods employed to determine skin carotenoid levels are presented, in brief, below.
Pressure-Mediated Reflection Spectroscopy (RS) uses a broad-band light source (460-500 nm) to measure the levels of skin carotenoids [165,166]. Pressure is applied during the measurement to temporarily limit blood flow, minimizing interference from hemoglobin [166]. This RS method is considered to be more cost-effective and portable compared to Resonance Raman Spectroscopy (RRS), and the Veggie Meter® is an example of an RS-based device, which was invented in 2015 [166]. RS-based measurements have shown good correlations with both RRS and plasma carotenoid levels as reported in several journal articles and reviews over the past 7 years in infants, children, adolescents and adults [164,165,167,168,169]. The scores range from 0 to 800 with higher scores indicating a greater presence of carotenoids, suggesting more FVC. Each 100 units on the Veggie Meter is thought to generally correspond to about one cup of FVC daily [166,170]. Notably, the manufacturer of The Veggie Meter states it is not designed to give specific dietary advice [170]. However, a skin carotenoid score at 350 or below suggests an inadequate FVC, while a score above 400 indicates good FVC [166]. Finally, when comparing RS to Resonance Raman Spectroscopy (RRS) most reports point out that RRS measurement is more sensitive in displaying results especially in monitoring changes in FVC over (brief) time intervals [171,172]. An example of the Veggie Meter display is shown in Figure 4. While figure 4 is just an example, many reports describe skin carotenoid scan levels to range between 250 to 350 [165,166,168,169,171,172].
Resonance Raman Spectroscopy (RRS) uses a laser, typically around 488 to 514 nm, to excite the carotenoids in the skin. This excitation generates an inelastic scatter response including characteristic Stoke or spectral lines (around 530 nm), whose magnitude is used to determine the carotenoid levels in the skin. The RRS is a validated method via numerous published studies, which correlate with blood carotenoid levels and corresponding dietary intake journal surveys [164,165,171,172,173]. In general, it is highly specific to carotenoids in the skin due to the strong resonance enhancement of their Raman signal(s) when excited with their absorption bands [164,165,171,172,173]. For example, devices like the NuSkin BioPhotonic S1 Scanner® utilize RRS technology, which was invented in 2003, and subsequent next generation versions were introduced in 2006 (S2) and 2013 (S3 BioPhotonic Scanner) [174].
A typical Skin Carotenoid Score (SCS) measured by the Nu Skin BioPhotonic S3 Scanner® ranges from 10,000 to over 89,000 Raman Intensity Units (RIU), with 42,000 RIU being an average score. This range indicates a moderate consumption of fruits and vegetables. Scores below 37,000 RIU may suggest a need for increased FVC or antioxidant supplementation, while scores above 46,000 RIU indicate a high level of carotenoids likely from a diet rich in carotenoids and/or supplementation. As shown in Figure 5, the color-coded skin carotenoid scan scores are displayed.
There are other methods of estimating carotenoid levels. For example, spectrophotometers measure the absorption or reflection of light in the spectrum around 400 to 500 nm, however, melanin and hemoglobin can interfere with this measurement [175]. Some reports suggest that near-infrared, mid-infrared and molecular fluorescence can detect carotenoids in food samples [176]. Therefore, the two main methods of estimating carotenoids levels in a non-invasive manner are RRS and RS using skin scanners.
5. Non-invasive RS & RRS Spectroscopy-based Skin Carotenoid Levels, Implications to Healthspan
5.1. Can Daily Habits Influence Healthspan?
Since recent data shows that our diets are lacking in adequate micronutrients [177], and it is challenging to get people to change their diet to increase carotenoids by eating more fruit and vegetables, supplementation offers an attractive alternate approach. It is important to consider how we can effectively motivate people firstly to take a supplement, and then, for this to be continuous, in effect, creating a habitual change. With the growing increase in digital technologies, there are now a number of noninvasive measurement tools and trackers, which can be used to monitor various aspects of health like apps for glucose monitoring, sleep quality, number of steps on a daily basis, monitoring food intake etc. One approach that does seem to be proving effective in getting people to change their habits is leveraging these noninvasive tools to help individuals understand their current practices, monitor their health situation, and more importantly, provide feedback on how they can positively change their habits. For the first time, we see that when consumers are able to measure things regularly, it provides positive reinforcement to influence habits in a healthier direction.
For example, blood glucose levels are influenced by various factors such as nutritent composition, meal timing, physical activity, circadian rythym and stress (cortisol) levels [178]. Continous glucose monitoring (CGM) is now a behavior modification tool [179] not only for diabetes, but also non-diabetic individuals wearing CGM can avoid pre-diabetes or diabetic conditions, improve mental and physical performance and modify food intake pattern for a healthier life [178,179,180]. Similar benefits have been reported in tracking daily step counts that decrease all-cause mortality, cardiovascular disease and metabolic disorders [181,182,183]. Also tracking sleep patterns [184] enhance wellbeing, and using internet-base smartphone apps improve healthy eating behaviors [185], which all enhance an individual’s healthspan. As a result of the growth in these noninvasive tracking devices, there has been a rapid increase in consumer understanding of one’s own wellbeing with a goal to be healthier on an individual level as well as a desire for individuals to leverage this information for a more personalised approach. Not only does this allow a person to keep track over time, but also they can provide actionable insights on ways an individual can improve their health. Thus, putting all these pieces together, we propose that measuring carotenoids noninvasively can actually provide a guide to an individual’s overall healthspan with carotenoids playing a key role in many aspects leading to positive healthspan outcomes. Moreover, these measurements can be effective in helping to encourage behaviours and interventions to improve wellness.
5.2. Lifetime and Worldwide Skin Carotenoid Scanning RRS Data Scores
While skin carotenoid scanning data has advanced through non-invasive measurements that can estimate F&V intake and/or carotenoid supplementation, all previous published studies have defined and/or presented limited subject populations. Recent data mining of previous collected RS skin carotenoid scores (SCS) have now made it possible to demonstrate lifetime SCS from 0 (before 1 year of age) to 100 years of age [186,187]. Due to the volume of data collected for more than 20 years (from 2002 to 2025) using the BioPhotonic Scanner skin carotenoid scanner scores, which represent millions of scans, the magnitude of the results has now been presented for each world region (by country and by age), which reveals the lifelong profiles of skin carotenoid levels.
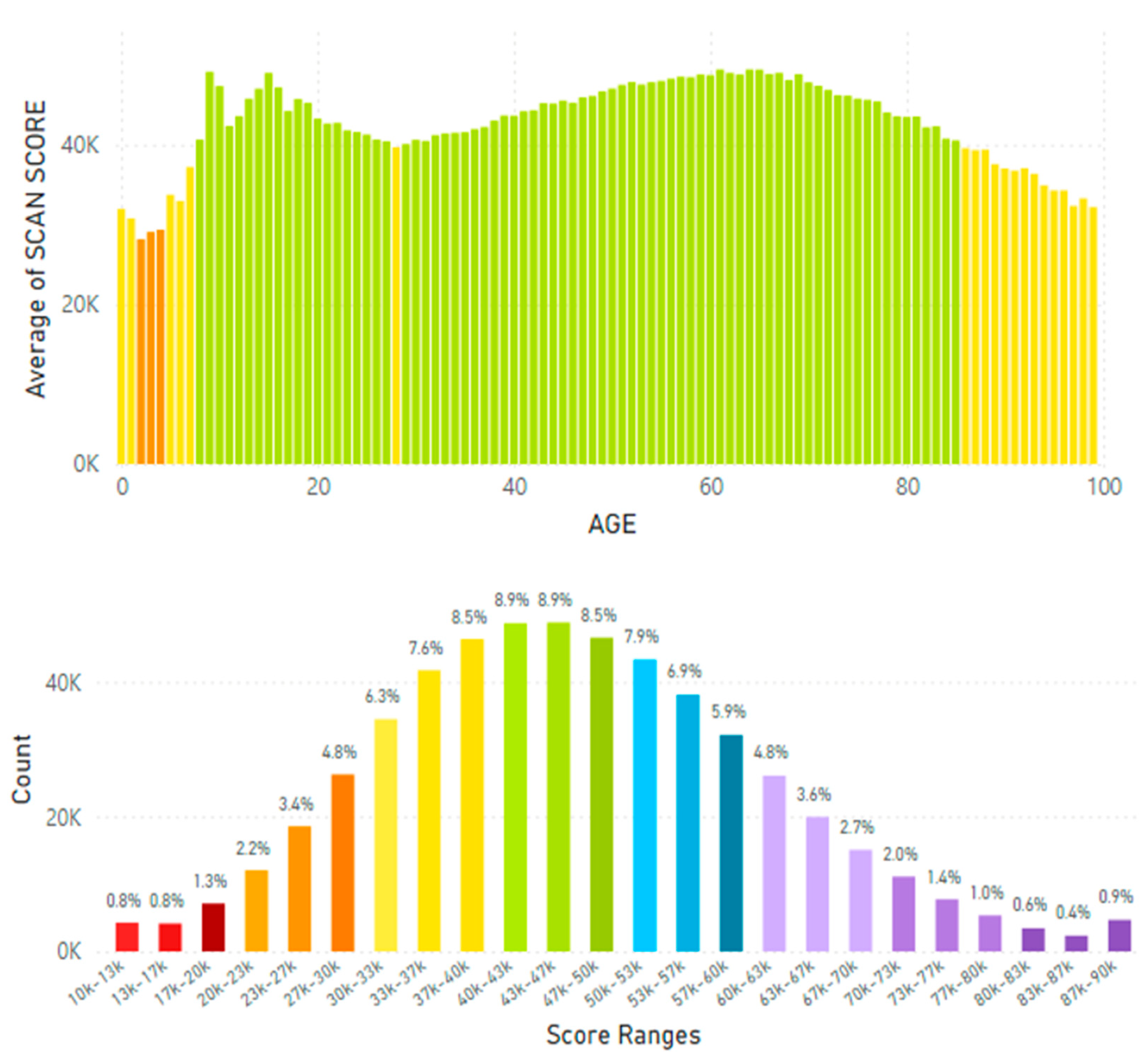
For example, lifetime SCS globally averaged 32.73K RIU. Korea displayed the highest SCS of 46.28K RIU of all countries studied (that had at least 100,000 scans) and displayed significantly higher SCS compared to the global average of 32.73K RIU (see Figure 6A and B for global data and 7A and B for Korean data).
The average skin carotenoid score was 32.74K RIU globally. The count on the y-axix represents the percentage of scans within a given bar of the histogram profile that is color-coded. Low Carotenoid Absorption into Tissue: Red – 10,000 - 19,000 RIU, Orange 20,000-29,000 RIU; Average Carotenoid Absorption into Tissue: Yellow – 30,000 – 39,000 RIU, Green 40,000 – 49,000 RIU and Above Carotenoid Absorption into Tissue: Blue 50,000 – 59,000 RIU, Platinum 60,000 – 89,000 RIU.
Figure 7.
A. Korean Carotenoid Scores by Age (from before 1 year of age = 0 to 100 years of age). Figure 7B. Korean Average Skin Carotenoid Score = 46.28K RIU from 547,780 scans. (See Figure 6B legend for additional information about this histogram.).
Japan displayed an average skin carotenoid score of 36.18K RIU from a total of 2.29 million scans (Figure 8A and B), which was significantly below that of the Korea average of 46.28K RIU.
Skin carotenoids scores from mainland China by age are shown in Figure 9A and the average skin carotenoid score = 32.23K RIU in Figure 9B (from 3.99 million scans), which was lower than the Korean or Japanese average scores.
Skin carotenoid scanner information from Taiwan is displayed in Figure 10A by age and Figure 10B for the average skin carotenoid score.
When other Southeastern Asia countries (Malaysia, Indonesia, Philippines, Singapore, Thailand & Vietnam) were examined the average skin carotenoid score = 27.20K RIU that was lower than the global average of 32.73K RIU (see Figure 11A and 11B).
In particular the Phillipines and Indonesia displayed the lowest average skin carotenoid scores compard to the global data at 20.65K RIU and 25.29K RIU, respectively. Notably, the age distribution for the Philippines and Indonesia showed that individuals 30 to 40 years of age displayed particularly low skin carotenoid scores at a level that would be considered at risk of cartenoid deficiency (see Figure 12A and 12B).
In analyzing the data from Thailand the skin carotenoids scores by age are shown in Figure 13A and the average skin carotenoid score = 29.16K RIU from 705,790 scans shown in Figure 13B.
The data from South East Asia and Pacific region that included Australia and New Zealand are shown in Figure 14A and 14B for age and score range profiles.
When Europe was examined the skin carotenoid scores by age are shown in Figure 15A and the average skin carotenoid score = 34.50K RIU from 3.18 million scans (Figure 15B).
In examining certain European regions, the skin carotenoid data from the United Kingdom is displayed in Figure 16A and 16B, while data from France and Germany that were combined due to the similarly of the data results, which are displayed in Figure 17A and 17B.
When the European data was analyzed during the period of the pandemic (April 2020 to January 2025) interesting results were discovered where skin carotenoid scores increased, possibly reflecting a greater interest in a healthier lifestyle and dietary FVC. This information is displayed in Figure 18A and 18B.
When North America (Canada and the United States of America) data were analyzed this data is displayed in Figure 19A and 19B.
In analyzing results from Latin America for skin carotenoid scores this data is displayed in Figure 20A and 20B.
Skin carotenoid score data from Iceland, Sweden, Norway and Russia were also analyzed as displayed in Table 1.
During the pandemic (February 21, 2020 to January 31, 2025) the average skin carotenoid scores increase by almost eleven percent in Sweden, suggesting that like the data from the United Kingdom individuals become more interested in a healthier lifestyle and dietary intake of fruits and vegetables, even though there was a hesitancy to vaccinate, especially children, in Sweden [188]. RIU = Raman Intensity Units
Additionally, the global average skin carotenoid scores were analyzed by ethinicity which is shown in Table 2 for White Caucasians, for African Americans, for Hispanics and for Asians (see below).
By ethnicity Asians displayed the highest average skin carotenoid score at 32.00K RIU, while African Americans displayed the lowest score at 25.99K RIU. Both White Caucasians and Hispanics scores were similar at 30.30K RIU and 30.00K RIU, respectively. These differences suggest that geographical location and national dietary patterns play a greater role on skin carotenoid levels compared to an individual’s ethnic origin.
Finally, the ranking of the global lifetime average skin carotenoid scores are displayed in Table 3 for 20 different countries/regions (including specific time periods), see below.
It should be noted that, in general, the “peaks” in the skin carotenoid profiles at a youthful age appear to be universal, and this pattern is displayed in a global fashion for all countries/regions. Additionally, for most countries there was a “dip” in the carotenoid profiles from ages 25 to 40. Indonesia and the Philippines displayed the most profound “dip”. However, one may speculate the “dip” in carotenoid levels may be due to individuals entering the workforce and not consuming a healthy diet due to their busy schedules. Although, the reasons for these characteristics are unknown.
6. Can Nutraceutical Supplementation Increase Skin Carotenoids Levels?
Early studies published in the 1990s clearly showed that administering an oral nutraceutical supplement containing carotenoids increased serum and skin carotenoid levels to enhance skin attributes in women [189]. However, in a recent published review in 2023, some authors suggested that “is it not currently known whether the magnitude of these increases (with carotenoid oral supplementation) is greater than that produced by a similar intake of caroteniods from food sources” [67]. While this may or may not be the case depending on the nutraceutical supplment administrated, there are several current reviews published in 2025 that suggest nutraceutical interventions to be effective for a variety of human health applications [190,191,192,193].
For example, a recent randomized, doubled-blind, placebo-controlled study compared two non-invasive methods (RS and RRS) to detect changes in skin carotenoid levels with the 12-week administration of a multivitamin supplement to men and women ages 20 to 65 years old (n = 46) that subsequently quantified six quality of life parameters at the end of the treatment [194]. The effectiveness of the supplementation treatment was validated by significant increases in vitamin C (by 44 %) and selenium (by 25 %) in plasma compared to placebo values, where the treatment supplement contained vitamins, minerals, carotenoids and phytonutrients, while the placebo supplement contained maltodextrin. The comparison of the RRS vs RS skin carotenoid levels are shown in Figure 21.
This comparison suggests that oral nutraceutical supplementation can increase skin carotenoid levels, but it appears that the RRS method was more sensitive compared to the RS method in detecting changes in skin carotenoid levels. However, both the RRS and RS methods were able to detect the significant changes in skin carotenoid levels from taking a nutraceutical supplement for 12 weeks [194]. Finally, all six of the quality of life parameters (energy, health, immune, recovery from illness, improved life quality and enhancement in long-term health) were significantly improved that ranged from 44% to 58 % over control values.
Again through data mining of published studies, it is now possible to determine how oral nutraceutical supplementation of carotenoids compare with FVC recorded over a very large data set of 21.27 million scans performed with RRS technology along with correlating information for dietary intake questionnaires [186,187]. This information is shown in Figure 21, which shows that individuals consuming less that 2 servings of FVC daily displayed skin in carotenoid scores between 27-30K RIU indicating low asbsorption of cartenoids into tissues. For individuals consuming more than 6 servings daily, they displayed skin carotenoid scores between 33-37K RIU, which suggested above asborption of carotenoids, while individuals taking the supplement Life Pak twice daily improved skin carotenoids levels to 37-40K RIU also in the above absorption range, but greater than multiple serving of FVC daily (Figure 22).
The data presented in Figure 22 suggests that oral nutraceutical supplementation can provide a similar or greater magnitude for the increase in skin carotenoid levels compared to high or multiple daily servings from food sources [186,187].
Of course, while carotenoids exhibit protective effects at low concentrations, high doses (20-30 mg/day) may lead to pro-oxidative effects and toxic metabolic interactions. For example, in smokers β-carotene can degrade into reactive aldehydes and epoxides, which can lead to tissue damage, and high doses of β-carotene can disrupt retinoid receptor balance and potentially increase cancer risk [191,195].
A proposal of scanning your skin to know your carotenoid levels in order to go forward and enhance one’s healthspan by lifestyle factors is shown in Figure 23.
7. Conclusions
The growing interest in natural antioxidants with their potential health benefits has fueled academic, industrial and corporate reseach to investigate and report on the antioxidant capabilities of carotenoids. Carotenoids are essential to protect and maintain human health and well-being. The therapeutic potential of carotenoids in preventing and managing human disorders/diseases covers a variety of tissues, organs and conditions for nutraceutical, pharmaceutical and cosmetic applications. A recent study revealed that the carotenoid market is projected to reach up to 1.9 billion USD by 2026 [196]. It is well established that non-invasive spectroscopy-based technologies can estimate carotenoid levels via skin carotenoid scans [164,165,166,167,168,169] in order for individuals to determine their carotenoid status to improve their health and quality of life. In this regard, while lifespan in years is increasing, healthspan (representing a good quality of life free of significant illnesses or disease) is decreasing. This narrative review proposes that the multi-faceted impact that carotenoids have on human health can enhance healthspan, and the non-invasive methods to determine skin carotenoid levels can assist individuals in monitoring and maintaing healthy carotenoid levels. Using data mining of published studies, where millions of skin carotenoids scans have been performed worldwide, provides an exploration into the variation of carotenoid levels in individuals that may reflect health and wellness. Nutraceutical supplementation results representing a vast database suggest that this method of consuming carotenoids may be as good or better compared to multiple dietary servings of carotenoids daily from food sources. By harnessing the synergistic potential of carotenoids to improve health, healthspan may be enhanced through advancing modern technology.
8. Future Directions
The future is now, we have wearable technologies from fitness trackers to smart clothing [197]. Back in the 1930s, the iconic comic book character Dick Tracy used a wrist radio to communicate with authorities when solving crimes. The creator Chester Gould had no idea how ahead of his time that was [197]. With wearable glucose monitors that are the norm it is not unrealistic that in the not so distant future individuals would have wearable carotenoid monitors and other devices that would indicate the status of general health similar to what was displayed in Star Trek? New Raman techniques such as spatially offset Raman spectroscopy (SORS), coherent anti-stokes Raman spectroscopy (CARS) and stimulated Raman scattering spectroscopy (SRS) along with applications of artifical intelligence may move us in this direction [198]. The advances in the therapeutic potential of carotenoids is rapidly progressing [123,199,200] from the extraction of carotenoids from natural sources [201,202] to the construction of enhanced nutrient delivery systems for carotenoids to maximize their antioxidant and anti-inflammatory activities [203] and combine carotenoids with precise targeting to multiligand receptors [like scavenger receptor class B member 1 (SR-B1)]. This may represent a strategic advance to improve human well-being in the fight against cancer as well as enhance the human healthspan [204].
Author Contributions
HK was involved in conceptualization, formal analysis, investigation, data curation, writing-original draft preparation, further writing, review and editing, providing supervision, project administration and funding acquisition of this work. EDL was involved in data analysis, data organization, writing-original draft preparation, further writing, review and editing and funding acquisition for this work. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by NSE Products Inc. and, in part, by the College of Life Sciences at Brigham Young University (grant number 19-2215).
Institutional Review Board Statement
Not applicable, this narrative review is based upon previously conducted studies and does not contain new data/results of human participants or animals performed by the authors.
Informed Consent Statement
Not applicable, this narrative review is based upon previously conducted studies and does not contain new data/results of human participants or animals performed by the authors.
Data Availability Statement
The data cited in this review are contained within the publications/presentations, etc. within the publications referenced.
Acknowledgments
The authors express thanks to Janet Lephart (SDRD) for editorial assistance
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design, presentation, collection of research information and scientific references, or in the analyses, interpretation of the presented data/information, in the writing of the manuscript; or in the decision to publish the contents of this narrative review.
Abbreviations
The following abbreviations are used in this manuscript:
| α | alpha |
| β | beta |
| AMD | age-related macular degeneration |
| BMD | bone mineral density |
| CARS | coherent anti-strokes Raman spectroscopy |
| CGM | continuous glucose monitoring |
| COPD | chronic obstructive pulmonary disease |
| CSF | cerebral spinal fluid |
| CVD | cardiovascular disease |
| FVC | fruit and vegetable consumption |
| FVI | fruit and vegetable intake |
| HPLC | high performance liquid chromatography |
| mg | milligram |
| MS | mass spectrometry |
| NFkB | nuclear factor kappa B |
| Nrf2 | nuclear factor erythroid 2-related factor 2 |
| OS | oxidative stress |
| RAE | retinol activity equivalent |
| ROS | reactive oxygen species |
| RS | reflective spectroscopy |
| RRS | resonance Raman spectroscopy |
| SCS | skin carotenoid score |
| SORS | spatially offset Raman spectroscopy |
| SR-B1 | scavenger receptor class B member 1 |
| SRS | stimulated Raman scattering spectroscopy |
| T2D | type 2 diabetes |
| TNF | tumor necrosis factor |
| USDA | United States Department of Agriculture |
| UV | ultraviolet |
References
- United Nations Department of Economic and Social Affairs. World population prospect 2022: release note about major differences in total population estimates for mid-2021 between 2019 and 2022 revisions; Population Division: New York, 2022. [Google Scholar]
- Garmany, A.; Terzic, A. Global health span-lifespan gaps among 183 world health organization member states. JAMA Network Open 2024, 7, e2450241. [Google Scholar] [CrossRef] [PubMed]
- Attia, P. The Long Game. In Outlive, the science & art of longevity; Harmony: New York, NY, 2023; p. 10. [Google Scholar]
- Rippe, J.M. Lifestyle Medicine: The health promoting power of daily habits and practices. Am J Lifestyle Med. 2018, 12, 499–512. [Google Scholar] [CrossRef]
- Knaggs, H.; Lephart, E.D. Enhancing skin anti-aging through healthy lifestyle factors. Cosmetics 2023, 10, 142. [Google Scholar] [CrossRef]
- Harman, D. Free radical theory of aging. Mutat Res. 1992, 275, 257–266. [Google Scholar] [CrossRef]
- Alegria-Torres, J.A.; Baccarelli, A.; Bollati, V. Epigenetics and lifestyle. Epigenetics 2011, 3, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Garagnani, P.; Parini, P.; Giuliani, C.; Santoro, A. Inflammaging: a new immune-metabolic viewpoint for age-related diseases. Nature Rev Endocrinol. 2018, 14, 576–590. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, Z.; Ren, Y.; Wang, Y.; Fang, J.; Yue, H.; Ma, S.; Guan, F. Aging and age-related diseases: from mechanisms to therapeutic strategies. Biogerontology 2021, 22, 165–187. [Google Scholar] [CrossRef]
- Rahaman, K. Studies on free radicals, antioxidants, and co-factors. Clin Interventions Aging 2007, 2, 219–236. [Google Scholar]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; Abete, P. Oxidative stress, aging and disease. Clin Interventions Aging 2018, 13, 757–772. [Google Scholar] [CrossRef]
- Chandimali, N.; Bak, S.G.; Park, E.H.; Lim, H.-J.; Won, Y.-S.; Kim, E.-K.; Park, S.-I.; Lee, S.J. Free radicals and their impact on health and antioxidant defenses: a review. Cell Death Discovery 2025, 11, 19. [Google Scholar] [CrossRef]
- Kassis, A.; Fochot, M.-C.; Horcajada, M.-N.; Horstman, A.M.H.; Duncan, P.; Bergonzelli, G.; Preitner, N.; Zimmermann, D.; Bosco, N.; Vidal, K.; et al. Nutritional and lifestyle management of the aging journey: A narrative review. Front Nutr. 2023, 9, 1087505. [Google Scholar] [CrossRef] [PubMed]
- Tessier, A.-J.; Wang, F.; Korat, A.A.; Eliassen, A.H.; Chavarro, J.; Grodstein, F.; Li, J.; Liang, L.; Willett, W.C.; Sun, Q.; Stampher, M.J.; Hu FBGuasch-Ferre, M. Optimal dietary patterns for healthy aging. Nat Med. 2025, 31, 1644–1652. [Google Scholar] [CrossRef]
- Roa, A.V.; Rao, L.G. Carotenoids and human health. Pharmacol Res. 2007, 55, 207–216. [Google Scholar]
- Crupi, P.; Faienza, M.F.; Naeem, M.Y.; Corbo, F.; Clodoveo, M.L.; Muraglia, M. Overview of the potential beneficial effects of carotenoids on consumer health and well-being. Antioxidants 2023, 12, 1069. [Google Scholar] [CrossRef] [PubMed]
- Bakac, E.R.; Percin, E.; Gunes-Bayir, A.; Dadak, A. A narrative review: The effects and importance of carotenoids on aging and aging-related diseases. Int J Mol Sci. 2023, 24, 15199. [Google Scholar] [CrossRef]
- Qi, X.; Wang, X.; Cheng, L.; Li, Y.; Dang, K.; Yang, S.; Wang, Y.; Zhou, R.; Zhang, C.; Li, Y. Dietary carotenoids intakes and biological aging among US adults, NHANES 1999-2018. Nutr J. 2025, 24, 9. [Google Scholar] [CrossRef]
- Madore, M.; Hwang, J.-E.; Park, J.-Y.; Ahn, S.; Joung, H.; Chun, O.K. A narrative review of factors associated with skin carotenoid levels. Nutrients 2023, 15, 2156. [Google Scholar] [CrossRef]
- Terao, J. Revisiting carotenoids as dietary antioxidants for human health and disease prevention. Food Function. 2023, 14, 7799–7824. [Google Scholar] [CrossRef]
- Toti, E.; Chen, C.-Y.O.; Palmery, M.; Valencia, D.V.; Peluso, I. Non-provitamin A and provitamin A carotenoids as immunomodulators: Recommended dietary allowance, therapeutic index, or personalized nutrition? Oxidative Med Cell Longevity 2018, 4637861. [Google Scholar] [CrossRef]
- USDA. National Agriculture Library, Food Composition, nal.usda.gov/human-nutrition-and-food-safety/food-composition Accessed 3 JUN 2025.
- National Institutes of Health (USA) Office of Dietary Supplements, Vitamin A and Carotenoids https://ods.od.nih.gov/factsheets/VitaminA-Consumer/#:~:text=Vitamin%20A%20is%20a%20fat,Teen%20females%2014%E2%80%9318%20years Accessed 3 JUN 2025.
- Mrowicka, M.; Mrowicki, J.; Kucharska, E.; Majsterek, I. Lutein and zeaxanthin and their roles in age-related macular degeneration- Neurodegenerative disease. Nutrients 2022, 14, 827. [Google Scholar] [CrossRef]
- Munteanu, I.G.; Apetrei, C. Analytical methods used in determining antioxidant activity: A review. Int J Mol Sci. 2021, 22, 3380. [Google Scholar] [CrossRef] [PubMed]
- Silvertrini, A.; Meucci, E.; Ricerca, B.M.; Mancini, A. Total antioxidant capacity: Biochemical aspects and clinical significance. Int J Mol Sci. 2023, 24, 10978. [Google Scholar] [CrossRef]
- Tufail, T.; Ain, H.B.U.; Noreen, S.; Ikram, A.; Arshad, M.T.; Abdullahi, M.A. Nutritional benefits of lycopene and beta-carotene: A comprehensive review. Food Sci Nutr. 2024, 12, 8715–8741. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Valverde, N.; Lopez-Valverde, A.; de Sousa, B.M.; Blanco Rueda, J.A. Systematic review and meta-analysis of the antioxidant capacity of lycopene in the treatment of periodontal disease. Front Bioeng Biotechnol. 2024, 11, 1309851. [Google Scholar] [CrossRef]
- E-Reay, M.A.; Ibrahim, G.E.; Eldahshan, O.A. Lycopene and lutein: A review for their chemistry and medicinal uses. J Pharmacognosy Phytochem. 2013, 2, 245–254. [Google Scholar]
- Shafe, M.O.; Gunede, N.M.; Nyakudya, T.T.; Chivandi, E. Lycopene: A potent antioxidant with multiple health benefits. J Nutr Metab. 2024, 6252426. [Google Scholar] [CrossRef]
- Joshi, B.; Kar, S.K.; Yadav, P.K.; Yadav, S.; Shrestha, L.; Bera, T.K. Therapeutic and medicinal uses of lycopene: a systematic review. Int J Res Med Sci. 2020, 8, 1195–1201. [Google Scholar] [CrossRef]
- Leh, H.E.; Lee, L.K. Lycopene: a potent antioxidant for the amelioration of type II diabetes mellitus. Molecules 2022, 27, 2335. [Google Scholar] [CrossRef]
- Bruno, R.R.; Rosa, F.C.; Nahas, P.C.; de Branco, F.M.S.; de Oliveira, E.P. Serum α-carotene, but not other antioxidants, is positively associated with muscle strength in older adults: NHANES 2001-2002. Antioxidants 2022, 11, 2386. [Google Scholar] [CrossRef]
- Omedilla-Alonso, B.; Rodriguez-Rodriguez, E.; Beltran-de-Miguel, B.; Estevez-Santiago, R. Dietary β-cryptoxanthin and α-carotene have greater apparent bioavailability than β-carotene in subjects from countries with different dietary patterns. Nutrients 2020, 12, 2639. [Google Scholar] [CrossRef]
- Obana, A.; Gohto, Y.; Nakazawa, R.; Moriyama, T.; Gellermann, W.; Berstein, P.S. Effect of an antioxidant supplement containing high dose lutein and zeaxanthin on macular pigment and skin carotenoid levels. Sci Reports 2020, 10, 10262. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Amaya, D.B. Carotenes and xanthophylls as antioxidants. In Handbook of Antioxidants for Food Preservation; Woodhead Publishing: Cambridge, UK, 2015; pp. 17–52. [Google Scholar]
- Rivera-Madrid, R.; Caballo-Uicab, V.M.; Cardenas-Conejo, Y.; Aguliar-Espinosa, M.; Siva, R. Chapter 1, Overview of carotenoids and beneficial effects on human health. In Carotenoids: Properties, Processing and Applications; Elsevier: London, UK, 2025; pp. 1–40. [Google Scholar]
- Hammad, M.; Raftari, M.; Cesario, R.; Salma, R.; Godoy, P.; Emami, S.N.; Haghdoost, S. Roles of oxidative stress and Nrf2 signaling in pathogenic and non-pathogenic cells. Antioxidants 2023, 12, 1371. [Google Scholar] [CrossRef] [PubMed]
- Bufka, J.; Vankova, L.; Sykora, J.; Krizkova, V. Exploring carotenoids: Metabolism, antioxidants, and impacts on human health. J Funct Foods 2024, 118, 106284. [Google Scholar] [CrossRef]
- Arslansoy, N.; Fidan, O. Carotenoids and their antioxidant power. In The Power of Antioxidants – Unleashing Nature’s Defense Against Oxidative Stress; Barros, A.N., Abraao, A.C., Eds.; Intech, 2024. [Google Scholar]
- Betteridge, D.J. What is oxidative stress? Metabolism 2000, 49, 3–8. [Google Scholar] [CrossRef]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P. Greenwood DC. Dietary intake and blood concentrations of antioxidants and the risk of cardiovascular disease, total cancer, and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies. Am J Clin Nutr. 2018, 108, 1069–1091. [Google Scholar] [CrossRef]
- Bohn, T. Carotenoids and markers of oxidative stress in human observational studies and intervention trials: implications for chronic diseases. Antioxidants 2019, 8, 179. [Google Scholar] [CrossRef]
- Bohn, T.; Bonet, M.L.; Borel, P.; Keijer, J.; Landrier, J.F.; Milisav, I. Mechanistic aspects of carotenoid health benefits – where are we now? Nutr Res Rev. 2021, 34, 267–302. [Google Scholar] [CrossRef]
- Sahashi, Y.; Goto, A.; Takachi, R.; Ishihara, J.; Kito, K.; Kanehara, R.; Yamaji, T.; Iwasaki, M.; Inoue, M.; Tsugane, S.; Sawada, N. Inverse association between fruit and vegetable intake and all-cause mortality: Japan public health center-based prospective study. J Nutr. 2022, 152, 2245–2254. [Google Scholar] [CrossRef]
- Bohm, V.; Lietz, G.; Olmedilla-Alonso, B.; Phelan, D.; Reboul, E.; Banati, D.; Borel, P.; Corte-Real, J.; de Lera, J.-F.; Desmarchelier, C. From carotenoid intake to carotenoid blood and tissue concentrations-implications for dietary intake recommendations. Nutr Rev. 2021, 79, 544–573. [Google Scholar] [CrossRef]
- Fekete M, Csipo T, Fazekas-Pongor V, Fehar A, Szarvas Z, Kaposvari C, Horvath K, Lehoczki A, Tarantini S, Varga JT, The effectiveness of supplementation with key vitamins, minerals, antioxidants and specific nutritional supplements in COPD- A review. Nutrients 2023, 15, 2741. [CrossRef]
- Chen, Z.; He, C.; Yu, W.; Ma, L.; Gou, S.; Fu, P. Association between dietary carotenoid and biological age acceleration: insights from NHANES 2009-2018. Biogerontology 2024, 26, 24. [Google Scholar] [CrossRef]
- Ahn, Y.J.; Kim, H. Lutein as a modulator of oxidative stress-mediated inflammatory diseases. Antioxidants 2021, 10, 1448. [Google Scholar] [CrossRef]
- Ademowo, O.S.; Oyedode, O.; Edward, R.; Conway, M.E.; Griffiths, H.R.; Dias, I.H.K. Effects of carotenoids on mitochondrial dysfunction. Biochem Soc Transactions 2024, 52, 65–74. [Google Scholar] [CrossRef]
- Ciccone, M.M.; Cortese, F.; Gesualdo, M.; Carbonara, S.; Zito, A.; Ricci, G.; De Pascalis, F.; Scicchitano, P.; Riccioni, G. Dietary intake of carotenoids and their antioxidant and anti-inflammatory effects in cardiovascular care. Mediators of Inflammation 2013, 782137. [Google Scholar] [CrossRef]
- Wang, M.; Tang, R.; Zhou, R.; Qian, Y.; Di, D. The protective effect of serum carotenoids on cardiovascular disease: a cross-sectional study form the general US adult population. Front Nutr. 2023, 10, 1154239. [Google Scholar] [CrossRef] [PubMed]
- Sumalla-Cano, S.; Eguren-Garcia, I.; Lasarte-Garcia, A.; Prola, T.A.; Martinez-Diaz, R.; Elio, I. Carotenoids intake and cardiovascular prevention: A systematic review. Nutrients 2024, 16, 3859. [Google Scholar] [CrossRef] [PubMed]
- Obana, A.; Nakamura, M.; Miura, A.; Nozue, M.; Muto, S.; Asaoka, R. Association between atherosclerotic cardiovascular disease score and skin carotenoids levels estimated via refraction spectroscopy in the Japanese population: a cross-sectional study. Sci Reports 2024, 14, 12173. [Google Scholar] [CrossRef]
- Gammone, M.A.; Riccioni, G.; D’Orazio, N. Carotenoids: potential allies of cardiovascular health? Food Nutr Res. 2015, 59, 26762. [Google Scholar] [CrossRef] [PubMed]
- Bungau, S.; Abdel-Daim, M.M.; Tit, D.M.; Ghanem, E.; Sato, S.; Maruyama-Inoue, M.; Yamane, S.; Kadonosono, K. Health benefits of polyphenols and carotenoids in age-related eye diseases. Oxidative Med Cell Longevity 2019, 9783429. [Google Scholar] [CrossRef]
- Nguyen, D.; Thrimawithana, T.; Piva, T.J.; Grando, D.; Huynh, T. Benefits of plant carotenoids against age-related macular degeneration. J Funct Foods 2023, 106, 105597. [Google Scholar] [CrossRef]
- Lem, D.W.; Davey, P.G.; Gierhart, D.L.; Rosen, R.B. A systematic review of carotenoids in the management of age-related macular degeneration. Antioxidants 2021, 10, 1255. [Google Scholar] [CrossRef] [PubMed]
- Arunkmar, R.; Gorusupudi, A.; Berstein, P.S. The macular carotenoids: A biochemical overview. Biochim Biophys Acata Mol Cell Lipids 2020, 1865, 158617. [Google Scholar] [CrossRef]
- Chew, E.Y.; Clemons, T.E.; Agron, E.; Dormalpally, A.; Keenan, E.D.L.; Vitale, S.; Weber, C.; Smith, D.C.; Christen, W. Long-term outcomes of adding lutein/zeaxanthin and omega-3 fatty acids to the AREDS supplements on age-related macular degeneration progression: AREDS2 report 28. JAMA Ophthalmol. 2022, 140, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Fathalipour, M.; Fathalipour, H.; Safa, O.; Nowrouzisoharbi, P.; Mikhani, H.; Hassanipour, S. The therapeutic role of carotenoids in diabetic retinopathy: A systematic review. Diabetes Metab Snydr Obes Targets Ther. 2020, 13, 2347–2358. [Google Scholar] [CrossRef] [PubMed]
- Darvin, M.E.; Sterry, W.; Lademan, J.; Vergou, T. The role of carotenoids in human skin. Molecules 2011, 16, 10491–10506. [Google Scholar] [CrossRef]
- Zerres, S.; Stahl, W. Carotenoids in human skin. Biochimica et Biophysica Acta (BBA) – Molecular and Cellular Biology 2020, 1865, 158588. [Google Scholar] [CrossRef]
- Michalak, M. Plant-derived antioxidants: Significance in skin health and the ageing process. Int J Mol Sci. 2022, 23, 585. [Google Scholar] [CrossRef]
- Darvin, M.E.; Lademan, J.; von Hagen Jorg Lohan, S.B.; Kolmar, H.; Meinke, M.C.; Jung, S. Carotenoids in human skin in vivo: Antioxidant and photo-protectant role against external and internal stressors. Antioxidants 2022, 11, 1451. [Google Scholar] [CrossRef]
- Metibemu, D.S.; Ogungbe, I.V. Carotenoids in drug discovery and medicine: Pathways and molecular targets implicated in human disease. Molecules 2022, 27, 6005. [Google Scholar] [CrossRef]
- Madore, M.P.; Hwang, J.-E.; Park, J.-Y.; Ahn, S.; Joung, H. A narrative review of factors associated with skin carotenoid levels. Nutrients 2023, 15, 2156. [Google Scholar] [CrossRef]
- Baswan, S.M.; Klosner, A.E.; Weir, C.; Salter-Venzon, D.; Gellenbeck, K.W.; Leverett, J.; Krutmann, J. Role of ingestible carotenoids in skin protection: A review of clinical evidence. Photodermatol Photoimmunol Photomed. 2012, 37, 490–504. [Google Scholar] [CrossRef]
- Bavarsad, N.; Mapar, M.A.; Safaezadeh, M.; Latiff, S.M. A double-blind, placebo-controlled randomized trial of skin-lightening cream containing lycopene and wheat bran extract on melasma. J Cosmet Dermatol. 2020, 20, 1795–1800. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, Q.; Qi, Y.; Chen, X.; Deng, J.; Zhang, Y. The effect of tomato and lycopene on clinical characteristics and molecular markers of UV-induced skin deterioration: A systematic review and meta-analysis of intervention trials. Critical Rev Food Sci Nutr. 2024, 64, 6198–6217. [Google Scholar] [CrossRef] [PubMed]
- Varghee, R.; Emerson, A.; Vannier, B.; Doss, C.G.P.; Priyadharshini, R.; Efferth, T.; Ramamoorthy, S. Substantial effects of carotenoids on skin health: A mechanistic perspective. Phytother Res. 2025. [Google Scholar] [CrossRef]
- Stevens, G.A.; Bennett, J.; Hennocq, Q.; Lu, Y.; De-Regil, L.M.; Rogers, L.; Danaei, G.; Li, G.; White, R.A.; Flaxman, S.R.; Oehrle, S.-P.; Finucane, M.M.; Guerrero, R.; Bhutta, Z.A.; Then-Paulino, A.; Fawzi, W.; Black, R.E.; Ezzati, M. Trends and mortality effects of vitamin A deficiency in children in 138 low-income and middle-income countries between 1991-2013: a pooled analysis of population-based surveys. Lance Glob Health 2015, 3, e528–e536. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.A. Effects of carotenoids on human immune function. Pro Nutr Soc. 1999, 58, 713–718. [Google Scholar] [CrossRef]
- Bas, T.G. Bioactivity and bioavailability of carotenoids applied in human health: Technological advances and innovation. Int J Mol Sci. 2024, 25, 7603. [Google Scholar] [CrossRef] [PubMed]
- Anjani, G.; Ayustaningwarno, F.; Eviana, R. Critical review on the immunomodulatory activities of carrot’s β-carotene and other bioactive compounds. J Funct Foods. 2022, 99, 105303. [Google Scholar] [CrossRef]
- Chew, B.P.; Park, J.S. Cartenoids action in the immune response. J Nutr. 2004, 134, 257S–261S. [Google Scholar] [CrossRef]
- Bohn, T.; Balbuena, E.; Ulus, H.; Iddir MWang, G.; Crook, N.; Eroglu, A. Carotenoids in health as studies by omics-related endpoints. Adv Nutr. 2023, 14, 1538–1578. [Google Scholar] [CrossRef]
- Santos, M.S.; Meydani, S.N.; Leka, L.; Wu, D. Fotouhi N, Meydani M, Hennekens CH, Gaziano JM. Natural killer cell activity in elderly men is enhance by beta-carotene supplementation. Am J Clin Nutr. 1996, 64, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.S.; Gaziano, J.M.; Leka, L.S.; Beharka, A.A.; Hennekens, C.H.; Meydani, S.N. Beta-carotene-induced enhancement of natural killer cell activity in elderly men: an investigation of the role of cytokines. Am J Clin Nutr. 1998, 68, 164–170. [Google Scholar] [CrossRef]
- Kramer, T.R.; Burri, B.j. Modulated mitogenic proliferative responsiveness of lymphocytes in whole-blood cultures after low-carotene diet and mixed-carotenoid supplementation in women. Am J Clin Nutr. 1997, 65, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Kulczynski, B.; Sidor ABrzozowska, A.; Gramza-Michlowska, A. The role of carotenoids in bone health – A narrative review. Nutrition 2024, 119, 112306. [Google Scholar] [CrossRef]
- Regu, G.M.; Kim, H.; Kim, Y.J.; Paek, J.E.; Lee, G.; Chang, N.; Kwon, O. Association between dietary carotenoid intake and bone mineral density in Korean adults aged 30-75 years using data from the fourth and fifth Korean national health and nutrition examination surveys (2008-2011). Nutrients 2017, 16, 1025. [Google Scholar] [CrossRef] [PubMed]
- Kan, B.; Guo, D.; Yuan, B.; Vuong, A.M.; Jiang, D.; Zhang, M.; Cheng, H.; Zhao, Q.; Li, B.; Feng, L.; Huang, F.; Wang, N.; Shen, X.; Yang, S. Dietary carotenoids intake and osteoporosis: the national health and nutrition examination survey, 2005-2018. Arch Osteoporos. 2021, 17, 2. [Google Scholar] [CrossRef]
- Zhen, Y.; Zhou, W.; Zhang, J.; Lan, T.; Zhang, R. Association between dietary carotenoid intake and vertebral fracture in people aged 50 years and older: a study based on the national health and nutrition examination survey. Arch Osteoporos. 2025, 20, 39. [Google Scholar] [CrossRef]
- Sahni, S.; Hannan, M.T.; Blumberg, J.; Cupples, L.A.; Kiel, D.P.; Tucker, K.L. Protective effect of total carotenoid and lycopene intake on risk of hip fracture: A 17-year follow-up from the Framingham Osteoporosis Study. J Bone Mineral Res. 2009, 24, 1086–1095. [Google Scholar] [CrossRef]
- Sahni, S.; Hannan, M.T.; Blumberg, J. Cupples L, Kiel DP, Tucker K. Inverse association of carotenoid intakes with 4-year change in bone mineral density in elderly men and women: the Framingham Osteoporosis Study. Am J Clin Nutr. 2009, 89, 416–424. [Google Scholar] [CrossRef]
- Bhatt, T.; Patel, K. Carotenoids: Potent to Prevent Diseases Review. Nat Prod Bioprospecting 2020, 10, 109–117. [Google Scholar] [CrossRef]
- Davinelli, S.; Ali, S.; Solfrizzi, V.; Scapagnini, G.; Corbi, G. Carotenoids and cognitive outcomes: A meta-analysis of randomized intervention trials. Antioxidants 2021, 10, 223. [Google Scholar] [CrossRef]
- Liu, X.; Dhana, K.; Furtado, J.D.; Agarwal, P.; Aggarwal, N.T.; Tangney, C.; Laranjo, V.; Barnes, L.I.; Sacks, F.M. Higher circulating α-carotene was associated with better cognitive function: an evaluation among the MIND trial participants. J Nutr Sci. 2021, 10, e64. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhao, T.; Zhy, X.; Jiang, Q. Low blood carotenoid status in dementia and mild cognitive impairment: A systematic review and meta-analysis. BMC Geriatrics. 2023, 23, 195. [Google Scholar] [CrossRef] [PubMed]
- Flieger, J.; Forma, A.; Flieger, W.; Flieger, M.; Gawlik, P.J.; Dzierzynski, E.; Maciejewski, R.; Terensinski, G.; Baj, J. Carotenoid supplementation for alleviating the symptoms of Alzheimer’s disease. Int J Mol Sci. 2024, 25, 8982. [Google Scholar] [CrossRef]
- Christimann, G.; Rocha, G.; Sattler, J.A.G. Bioactive compounds and dietary patterns in Alzheimer's disease. J Alzheimer's Dis. 2025, 104, 597–610. [Google Scholar] [CrossRef]
- Govindaswamy, B.; Stephen, K.N.; Keerthana, S.; Perumal, S.; Thirumurugan, M. Recent advances on therapeutic mechanism and potential of flavonoids and carotenoids: A focus on Alzheimer's and Parkinson’s disease. In Bioactive Ingredients for Healthcare Industry; Lahiri, D., Nag, M., Bhattacharya, D., Pati, S., Sarkar, T., Eds.; Springer: Singapore, 2025; Volume 2, pp. 75–107. [Google Scholar]
- Wilson, D.M.I.I.I.; Cookson, M.R.; Den Bosch, L.V.; Zetterberg, H.; Holtzman, D.M.; Dewachter, I. Hallmarks of neurodegenerative diseases. Cell 2022, 186, 693–714. [Google Scholar] [CrossRef] [PubMed]
- Kabir, M.T.; Rahman, M.H.; Shah, M.; Jamiruddin, M.R.; Basak, D.; Al-Harrasi, A.; Bhatia, S.; Ashraf, G.M.; Najda, A.; El-Kott, A.F.; Mohamed, H.R.H.; Al-Malky, H.; Germoush, M.O.; Altyar, A.E.; Alwafai, E.B.; Ghaboura, N.; Abdel-Daim, M.M. Therapeutic promise of carotenoids as antioxidants and anti-inflammatory agents in neurodegenerative disorders. Biomed Pharmacother. 2022, 146, 112610. [Google Scholar] [CrossRef]
- Manochkumar, J.; Doss, C.G.P.; El-Seedi, H.R.; Efferth, T.; Ramaoorthy, S. The neuroprotective potential of carotenoids in vitro and in vivo. Phytomedicine 2021, 91, 153676. [Google Scholar] [CrossRef]
- Gandla, K.; Babu, A.K.; Unnisa, A.; Sharma, I.; Singh, L.P.; Haque, M.A.; Dashputre, N.L.; Baig, S.; Siddiqui, F.A.; Khandaker, M.U.; Almujally, A.; Tamam, N.; Sulieman, A.; Khan, S.L.; Emran, T.B. Carotenoids: Role in neurodegenerative diseases remediation. Brain Sci 2023, 13, 457. [Google Scholar] [CrossRef]
- Yuan, C.; Chen, H.; Wang, Y.; Schneider, J.A.; Willett, W.C.; Morris, M.C. Dietary carotenoids related to risk of incident Alzhemier’s dementia (AD) and brain AD neuropathy: a community-based cohort of older adults. Am J Clin Nutr. 2021, 113, 200–208. [Google Scholar] [CrossRef]
- Bej, E.; Cesare, P.; d’Angelo, M.; Volpe, A.R.; Castelli, V. Neuronal cell rearrangement during aging: Antioxidant compounds as a potential therapeutic approach. Cells. 2024, 13, 1945. [Google Scholar] [CrossRef]
- Kudo, J.; Watanabe, K.; Sasaki, M.; Ushida, Y.; Matsuzaka, M.; Kakeda, S. Serum carotenoids concentrations are associated with enlarged choroid plexus, lateral ventricular volume, and perivascular spaces on magnetic resonance imaging: A large cohort study. Academic Radiology in press. 2025. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Liu, K.; Zhu, J. Glymphatic system: an emerging therapeutic approach for neurological disorders. Front Mol Neurosci. 2023, 16, 1138769. [Google Scholar] [CrossRef]
- Crowe-White, K.M.; Phillips, T.A.; Ellis, A.C. Lycopene and cognitive function. J Nutr Sci. 2019, 8, e20. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.-W.; Yin, Z.-L.; Lin, R.; Fan, Z.-L.; Chen, S.-J.; Zhu, Y.-M.; Zhao, X.-Z. Possible mechanisms of lycopene amelioration of learning and memory impairment in rats with vascular dementia. Neural Regen Res. 2020, 15, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Shen, Y.; Li, M.; Li, T.; Shi, D.; Shi, D.; Lu, S.; Qiu, F.; Wu, Z. Lycopene treatment attenuates D-galactose-induced cognitive decline by enhancing mitochondrial function and improving insulin signaling in the brains of female CD-1 mice. J Nutr Biochem. 2023, 118, 109361. [Google Scholar] [CrossRef]
- Iyer, S.; Bhat, I.; Sheshappa, M.B. Luetin and the underlying neuroprotective promise against neurodegenerative diseases. Mol Nutr Food Res. 2024, 68, e2300409. [Google Scholar] [CrossRef]
- Jayakanthan, M.; Manochkumar, J.; Efferth, T.; Ramamoorthy, S. Lutein, a versatile carotenoid: Insight on neuroprotective potential and recent advances. Phytomedicine 2024, 135, 156185. [Google Scholar] [CrossRef]
- Wingo, T.S.; Liu, Y.; Gerasimov, E.S.; Vattathil, S.M.; Wynne, M.E.; Liu, J.; Lori, A.; Faundez, V.; Bennett, D.A.; Seyfried, N.T.; Levey, A.I.; Wingo, A.P. Shared mechanisms across the major psychiatric and neurodegenerative diseases. Nature Communications. 2022, 13, 4314. [Google Scholar] [CrossRef]
- Anderson, E. Crawford CM, Fava M, Ingelfinger J, Nikayin S. Sanacora G. Depression – understanding, identifying, and diagnosing. N Engl Med. 2024, 390, e41. [Google Scholar] [CrossRef]
- Kulkarni, J. Why depression in women is so misunderstood. Nature 2022, 608, S54. [Google Scholar] [CrossRef] [PubMed]
- McCarron, R.M.; Shapiro, B. Rawles J, Luo J. Depression. Ann Intern Med. 2021, 174, ITC65-80. [Google Scholar] [CrossRef]
- Ge, H.; Yang, T.; Sun, J.; Zhang, D. Associations between dietary carotenoid intakes and the risk of depressive symptoms. Food Nutr Res. 2020, 64. [Google Scholar] [CrossRef]
- Bardinet, J.; Pouchieu, C.; Chuy, V.; Helmer, C.; Etheve, S.; Gaudout, D.; Samieri, C.; Berr, C.; Delcourt, C.; Cougnard-Gregoire, A.; Feart, C. Plasma carotenoids and risk of depressive symptomatology in a population-based cohort of older adults. J Affective Disorders 2023, 339, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Xue, F.; Li, Z.; Li, X.; Ai, L.; Jin, M.; Xie, M.; Yu, Y. Dietary intake of carotenoids and risk of depressive symptoms: A systematic review and meta-analysis. Antioxidants 2022, 11, 2205. [Google Scholar] [CrossRef]
- Rasmus, P.; Kozlowska, E. Antioxidant and anti-inflammatory effects of carotenoids in mood disorders: An overview. Antioxidants 2023, 12, 676. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Fang, M.-S. Association of dietary antioxidant intake with depressive risk and all-cause mortality in people with prediabetes. Sci Reports 2024, 14, 20009. [Google Scholar]
- Zhang, W.; Cheng, Z.; Lin, H.; Fu, F.; Zhan, Z. Serum carotenoid levels inversely correlate with depression symptoms among adults: Insights from NHANES data. J Affective Disorders 2024, 362, 869–876. [Google Scholar] [CrossRef]
- Lu, J.-H.; Zhong, W.-W.; Tan, Y.-L.; Zhuo, L.; Luo, G.-Z. Association of dietary and plasma lutein + zeaxanthin with depression in US adults: findings from NHANES. Asia Pac J Clin Nutr. 2025, 34, 153–164. [Google Scholar]
- Li, X.; Lan, Y. Association between higher dietary lycopene intake and reduced depression risk among American adults: evidence from NHANES 2007-2016. Front Nutr. 2025, 12, 1538396. [Google Scholar] [CrossRef]
- Yen, C.-H.; Chang, P.-S.; Ghiu, C.-J.; Huang, Y.-Y.; Lin, P.-T. β-Carotene status is associated with inflammation and two components of metabolic syndrome in patients with and without osteoarthritis. Nutrients 2021, 12, 2280. [Google Scholar] [CrossRef]
- Takayanagi, Y.; Obana, A.; Muto, S.; Asaoka, R.; Tanito, M.; Ermakov, I.V.; Bernstein, P.S.; Gellermann, W. Relationships between skin carotenoid levels and metabolic syndrome. Antioxidants 2021, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Hata, J.; Shibata, M.; Honda, T.; Sakata, S.; Furuta, Y.; Oishi, E.; Kitazono, T.; Ninomiya, T. Skin carotenoid score and metabolic syndrome in general Japanese population: the Hisayama study. Internat J Obesity 2024, 48, 1465–1471. [Google Scholar] [CrossRef]
- Sun, Q.; Fan, Z.; Yao, F.; Zhao, X.; Jiang MYang, M.; Mao, M.; Yang, C. Association of dietary and circulating antioxidant vitamins with metabolic syndrome: an observational and Mendelian randomization study. Front Endocrinol. 2024, 15, 1446719. [Google Scholar] [CrossRef]
- Ortega-Regules, A.E.; Martinez-Thomas, J.A.; Schurenkamper-Carrillo, K.; de Parrodi, C.A.; Lopez-Mena, E.R.; Mejia-Mendez, J.L.; Lozada-Ramirez, J.D. Recent advances in the therapeutic potential of carotenoids in preventing and managing metabolic disorders. Plants 2024, 13, 1584. [Google Scholar] [CrossRef] [PubMed]
- Bouayed, J.; Vahid, F. Carotenoid pattern intake and relation to metabolic status, risk and syndrome, and its components-divergent findings from the ORISCAV-LUX-2 survey. British J Nutr. 2024, 132, 50–66. [Google Scholar] [CrossRef] [PubMed]
- Marceline, G.; Machate, D.J.; de Cassia Freitas, K.; Hiane, P.A.; Rodrigues Maldonade, I.; Pott, A.; Asato, M.A.; Candido, C.J.; de Cassia Avellaneda Guimaraes, R. β-Carotene: Preventive role for type 2 diabetes mellitus and obesity: A review. Molecules 2020, 25, 5803. [Google Scholar] [CrossRef]
- Jiang, Y.-W.; Sun, Z.-H.; Tong, W.-W.; Yang, K.; Guo Kpq Liu, G.; Pan, A. Dietary intake and circulating concentrations of carotenoids and risk of type 2 diabetes: A dose-response meta-analysis of prospective observational studies. Adv Nutr. 2021, 12, 1723–1733. [Google Scholar] [CrossRef]
- Leh, H.E.; Sopian, M.M.; Abu Bakar, M.H.; Lee, L.K. The role of lycopene for the amelioration of glycaemic status and peripheral antioxidant capacity among the type 2 diabetes patients: a case-control study. Ann Med. 2021, 53, 1060–1066. [Google Scholar] [CrossRef]
- Coronel, J.; Pinos, I.; Amengual, J. β-Carotene in obesity research: Technical considerations and current status of the field. Nutrients 2019, 11, 842. [Google Scholar] [CrossRef]
- Anzar, C.A.; Joseph, M.V.; Vadiraj, S.R.; Prasad, C.P.; Eranimose, B.; Jagadeesh, S. Safety assessment of lutein and zeaxanthin supplementation and its effects on blood glucose levels, kidney functions, liver functions, and bone health – randomized, double-blind, placebo-controlled clinical study. MedRxiv 2023. [Google Scholar] [CrossRef]
- Mounien, L.; Tourniaire, F.; Landrier, J.F. Anti-obesity effect of carotenoids: Direct impact on adipose tissue and adipose tissue-driven indirect effects. Nutrients 2019, 11, 1562. [Google Scholar] [CrossRef]
- Yao, N.; Yan, S.; Guo, Y.; Wang, H.; Li, X.; Wang, L.; Hi, W.; Li, B.; Cui, W. The association between carotenoids and subjects with overweight or obesity: a systematic review and meta-analysis. Food Funct. 2021, 12, 4768–4782. [Google Scholar] [CrossRef] [PubMed]
- Hahemi, D.; Fard, M.V.; Mohammadhasani, K.; Barati MNattagh-Eshtivani, E. Carotenoids improve obesity and fatty liver disease via gut microbiome: A narrative review. Food Sci Nutr. 2025, 13, e70092. [Google Scholar] [CrossRef]
- Eroglu, A.; Al’ Abr, A.L.; Kopec, R.E.; Crook, N.; Bohn, T. Carotenoids and their health benefits as derived via interactions with gut microbiota. Adv. Nutr. 2023, 14, 238–255. [Google Scholar] [CrossRef]
- Schmidt, K.; Haddad, E.N.; Sugino, K.Y.; Vevang, K.R.; Peterson, L.A.; Korathar, R.; Gross, M.D.; Kerver, J.M.; Comstock, S.S. Dietary and plasma carotenoids are positively associated with alpha diversity in the fetal microbiota of pregnant women. J Food Sci. 2021, 86, 602–613. [Google Scholar] [CrossRef]
- Rocha, H.R.; Coelho, M.C.; Gomes, A.M.; Pintado, M.E. Carotenoids diet: Digestion, gut microbiota modulation, and inflammatory diseases. Nutrients 2023, 15, 2265. [Google Scholar] [CrossRef] [PubMed]
- Meneguelli, T.S.; Mishima, M.D.V.; Hermsdorff, H.H.M.; Martino, H.S.D.; Bressan, J.; Tako, E. Effect of carotenoids on gut health and inflammatory status: A systematic review of in vivo animal studies. Crit Rev Food Sci Nutr. 2024, 64, 11206–11221. [Google Scholar] [CrossRef]
- Bernabeu, M.; Gharibzahedi, S.M.T.; Ganaie, A.A.; Mach, M.A.; Dar, B.N.; CAstagnini, J.M.; Garcia-Bonillo, C.; Melendez-Martinez, A.J.; Altintas, Z.; Barba, F.J. The potential modulation of gut microbiota and oxidative stress by dietary carotenoid pigments. Crit Rev Food Sci Nutr. 2024, 64, 12555–12573. [Google Scholar] [CrossRef]
- Kumar, S.; Mukherjee, R.; Gaur, P.; Leal, E.; Lyu, X.; Ahmad, S.; Puri, P.; Chang, C.-M.; Raj, V.S.; Pandey, R.P. Unveiling roles of beneficial gut bacteria and optimal diets for health. Front Microbiol. 2025, 16, 1527755. [Google Scholar] [CrossRef]
- Tanaka, T.; Shnimizu, M.; Moriwaki, H. Cancer chemoprevention by carotenoids. Molecules 2012, 17, 3202–3242. [Google Scholar] [CrossRef] [PubMed]
- Rowles, J.L.; Erdman, J.W., Jr. Carotenoids and their role in cancer prevention. Biochim Biophys Acata Mol Cell Biol Lipids 2020, 1865, 158613. [Google Scholar] [CrossRef]
- Dulinska-Litewka, J.; Sharoni, Y.; Halubiec, P.; Lazarczyk, A.; Szafranski, O.; McCubrey Gasiorkiewicz, B.; Laidler, P.; Bohn, T. Recent progress in discovering the role of carotenoids and their metabolites in prostatic physiology and pathology with a focus on prostate cancer- A review- Part 1: Molecular mechanisms of carotenoid action. Antioxidants 2021, 10, 319. [Google Scholar] [CrossRef] [PubMed]
- Shafiq, M.A.; Gull, R.; Nazik, G. Dietary Carotenoids and their multifaceted roles in cancer prevention. J Health Rehab Res. 2024, 4. [Google Scholar] [CrossRef]
- Baeza-Morales, A.; Medina-Garcia, M.; Martinez-Peinado, P.; Pascual-Garica, S.; Pujalte-Satorre, C.; Lopez-Jaen, A.B.; Martinez-Espinosa, R.M.; Sempere-Ortells, J.M. The antitumour mechanisms of carotenoids: A comprehensive review. Antioxidants 2024, 13, 1060. [Google Scholar] [CrossRef]
- Dehnavi, M.K.; Ebrahimpour-Koujan, S.; Lotfi, K.; Azadbakht, L. The association between circulating carotenoids and risk of breast cancer: A systematic review and dose-response meta-analysis of prospective studies. Adv Nutr. 2024, 15, 100135. [Google Scholar] [CrossRef] [PubMed]
- Shin, J. Song M-H, Oh J-W, Keum Y-S, Saini RK. Pro-oxidant actions of carotenoids in trigging apoptosis of cancer cells: A review of emerging evidence. Antioxidants 2020, 9, 532. [Google Scholar] [CrossRef]
- Belludi, A.S.; Verma, S.; Banthia, R.; Bhusari, P.; Parwani, S.; Kedia, S.; Saiprasad, S.V. Effect of lycopene in the treatment of periodontal disease: A clinical study. J Comp Dental Prac. 2013, 14, 1054–1059. [Google Scholar] [CrossRef]
- Varela-Lopez, A.; Battino, M.; Bullon PQuiles, J.L. Dietary antioxidants for chronic periodontitis prevention and its treatment: a review on current evidences from animal and human studies. Ars Pharmaceutica 2015, 56, 131–140. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Almas, K. The role of nutrition in periodontal health: An update. Nutrients 2016, 8, 530. [Google Scholar] [CrossRef]
- Kaur, G.; Kathariya, R.; Bansal, S.; Singh, A.; Shahakar, D. Dietary antioxidants and their indispensable role in periodontal health. J Food Drug Analysis 2016, 24, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Lambert, J.; Bush, H.; Huja, P.E.; Basu, A. Serum nutrient levels and aging effects on periodontitis. Nutrients 2018, 10, 1986. [Google Scholar] [CrossRef]
- Naruishi, K. Carotenoids and periodontal infection. Nutrients 2020, 12, 269. [Google Scholar] [CrossRef]
- Li, F.; Wang, G.; Zhang, Y. Association between carotenoid intake and periodontitis in diabetic patients. J Nutr Sci. 2024, 13, e11. [Google Scholar] [CrossRef]
- Kaur, G.; Dhillon, S.; Aulakh, N. Lycopene and oral health: A comprehensive review. Med Res Pub. 2025. Available online: https://www.medicalandresearch.com/current_issue/2485#:~:text=Recent%20studies%20suggest%20that%20lycopene,dental%20hygiene%20and%20preventive%20dentistry (accessed on 16 June 2025).
- Semba, R.D.; Varadhan, R.; Bartali, B.; Ferrucci, L.; Ricks, M.O.; Blaum, C.; Fried, L.P. Low serum carotenoids and development of severe walking disability among older women living in the community: the Women’s Health and Aging Study I. Age Ageing 2007, 36, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Lauretani, F.; Ferrucci, L. Carotenoids as protection against sarcopenia in older adults. Arch Biochm Biophys. 2007, 458, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Lauretani, F.; Semba, R.D.; Bandinelli, S.; Dayhoff-Brannigan, M.; Giacomini, V.; Corsi, A.M.; Guralnik, J.M.; Ferrucci, L. Low plasma carotenoids and skeletal muscle strength decline over six years. J Gerontol A Biol Sci Med Sci. 2008, 63, 376–383. [Google Scholar] [CrossRef]
- Jeong, D.; Park, S.; Kim, H.; Kwon, O. Association of carotenoids concentrations in blood with physical performance in Korean adolescents: The 2018 national fitness award project. Nutrients 2020, 12, 1821. [Google Scholar] [CrossRef]
- Welch, A.A.; Jennings, A.; Kelaiditi, E.; Skinner, J.; Steves, C.J. Cross-sectional associations between dietary antioxidant vitamin C, E and carotenoids intakes and sarcopenia indices in women aged 18-79 years. Calcif Tissue Int. 2020, 206, 331–342. [Google Scholar] [CrossRef]
- Sahni, S.; Dufour, A.B.; Fielding, R.A.; Newman, A.B.; Kiel, D.P.; Hannan, M.T.; Jacques, P.F. Total carotenoid intake is associated with reduced loss of grip strength and gait speed over time in adults: The Framingham Offspring Study. Am J Clin Nutr. 2021, 113, 437–445. [Google Scholar] [CrossRef]
- Bartali, B.; Semba, R.D. Carotenoids and healthy aging: the fascination continues. Am J Clin Nutr. 2021, 113, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.H.; Duggan, E.; Davis, J.; O’Halloran, A.M.; Knight, S.P.; Kenny, R.A.; McCarthy, S.N.; Romero-Ortuno, R. Plasma lutein and zeaxanthin concentrations associated with musculoskeletal health and incident frailty in The Irish Longitudinal Study on Aging (TILDA). Exp Geronotol. 2023, 171, 112013. [Google Scholar] [CrossRef]
- Tarshish, E.; Hermoni, K.; Muizzudin, N. Effect of Lumenato a tomato derived oral supplement on improving skin barrier strength. Skin Res Tech. 2023, 29, e13504. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, C.; Yuan, J.; Du, Y.; Zeng, J.; Sun, Y.; Wu, Y.; Gao, X.-H.; Chen, H.-D. Effects of oral carotenoids on oxidative stress: A systematic review and meta-analysis of studies in the recent 20 years. Front. Nutr. 2022, 9, 754707. [Google Scholar] [CrossRef] [PubMed]
- Ermakov, I.V.; Ermakova, M.; Sharifzadeh, M.; Gorusupudi, A.; Farnsworth, K.; Bernstein, P.S.; Stookey, J.; Evans, J.; Arana, T.; Tao-Lew, L.; Isman, C.; Clayton, A.; Obana, A.; Whigham, L.; Redelfs, A.H.; Jahns, L.; Gellerman, W. Optical assessment of skin carotenoid status as a biomarker of vegetable and fruit intake. Arch Biochem Biophys. 2018, 646, 46–54. [Google Scholar] [CrossRef]
- Radtke, M.D.; Pitts, S.J.; Jahns, L.; Firnhaber, G.; Loofbourrow, B.M.; Zeng, A.; Scherr, R.E. Criterion-related validity of spectroscopy-based skin carotenoid measurements as a proxy for fruit and vegetable intake: A systematic review. Adv Nutr. 2020, 11, 1282–1299. [Google Scholar] [CrossRef]
- Radtke, M.D.; Poe, M.; Stookey, J.; Pitts, S.J.; Moran, N.E.; Landry, M.J.; Rubin, L.P.; Stage, V.C.; Scherr, R.E. Recommendations for the use of the Veggie Meter® for spectroscopy-based skin carotenoid measurements in the research setting. Res Method Study Design. 2021, 5, nzab104. [Google Scholar] [CrossRef]
- Radtke, M.; Pitts, S.J.; Jahns, L.; Firnhaber, G.; Loofbourrow, B.; Zeng, A.; Scherr, R. Examining the validity of spectroscopy-based skin carotenoid measurements as a proxy for fruit and vegetable consumption. Curr Dev Nutr. 2020, 4, nzaa041_029. [Google Scholar] [CrossRef]
- Hwang, J.-E.; Park, J.-Y.; Jung, M.H.; Eom, K.; Moon, H.S.; Joung, H.; Kim, Y.J. Evaluation of a commercial device based on reflection spectroscopy as an alternative to resonance Ramman spectroscopy in measuring skin carotenoid levels: Randomized control trials. Sensors 2023, 23, 7654. [Google Scholar] [CrossRef]
- Hasin, S.; Dev, D.A.; Swindle, T.; Sisson, S.B.; Pitts, S.J.; Purkait, T.; Clifton, S.C.; Dixon, J.; Stage, V.C. Systemic review of reflection spectroscopy-based skin carotenoid assessment in children. Nutrients 2023, 15, 1315. [Google Scholar] [CrossRef]
- Veggie Meter – Longevity Link Corporation, website. Available online: http://www.longevitylinkcorporation.com/ (accessed on 21 June 2025).
- Obana A, Measurement of skin carotenoids and their association with diseases: A narrative review. BBA Mole Cell Biol Lipids 2025, 1870, 159612. [CrossRef]
- Ahn, S.; Hwang, J.-E.; Kim, Y.J.; Eom, K.; Jung, M.H.; Moon, H.S.; Han, D.; Park, J.M.; Oh, S.U.; Park, J.-H.; Joung, H. Examination of the utility of skin carotenoid status in estimating intakes of carotenoids and fruits and vegetables: A randomized, parallel-group, controlled feeding trial. Nutrition 2024, 119, 112304. [Google Scholar] [CrossRef]
- Udensi, J.; Loughman, J.; Loskutova, E.; Byrne, H.J. Raman spectroscopy of carotenoid compounds for clinical applications- A review. Molecules 2022, 27, 9017. [Google Scholar] [CrossRef] [PubMed]
- Nu Skin RRS technology BioPhontic S3 Scanner website. Available online: https://www.nuskin.com/content/nuskin/en_US/products/pharmanex/scanner/s3_score.html (accessed on 21 June 2025).
- Sharifzadeh, M. Accurate quantification of carotenoids in human skin: Correcting for melanin and hemoglobin interference. Wor Jour Clin Der. 2025, 2, 01–12. [Google Scholar]
- Soulat, J.; Andueza, D.; Graulet, B.; Girard, C.L.; Labonne, C.; Ait-Kaddour, A.; Martin, B.; Ferlay, A. Foods. 2020, 9, 592. [Google Scholar] [PubMed]
- Lassale, C.; Gaye, B. Addressing global micronutrient inadequacies: enhancing global data representation. Lancet 2024, 12, e1561–e1562. [Google Scholar] [CrossRef]
- Kim, Y.-I.; Choi, Y.; Park, J. The role of continuous glucose monitoring in physical activity and nutrition management: perspectives on present and possible uses. Physical Activity Nutr. 2023, 27, 44–51. [Google Scholar] [CrossRef]
- Klonoff, D.C.; Nguyen, K.T.; Xu, N.Y.; Gutierrez, A.; Espinoza, J.C.; Vidmar, A.P. Use of continuous glucose monitors by people without diabetes: An idea whose time has come? J. Diabetes Sci. Technol. 2023, 17, 1686–1697. [Google Scholar] [CrossRef]
- Ehrhardt, N.; Al Zaghal, E. Continuous glucose monitoring as a behavior modification tool. Clin Diabetes 2020, 38, 126–131. [Google Scholar] [CrossRef]
- Kruas, W.E.; Janz, K.F.; Powell KECampbell, W.W.; Jakicic, J.M.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L. Daily step counts for measuring physical activity exposure and its relation to health. Med Sci Sports Exerc. 2019, 51, 1206–1212. [Google Scholar] [CrossRef]
- Paluch, A.E.; Gabriel, K.P.; Fulton, J.E.; Lewis, C.E.; Schreiner, P.J.; Sternfeld, B.; Sidney, S.; Siddique, J.; Whitaker, K.M.; Carnethon, M.R. Steps per day and all-cause mortality in middle-aged adults in the coronary artier risk development in young adults study. JAMA Network Open 2021, 4, e21224516. [Google Scholar] [CrossRef]
- del Pozo Cruz, B.; Ahmadi, M.N.; Lee, I.-M.; Stamatakis, E. Prospective associations of daily step counts and intensity with cancer and cardiovascular disease incidence and mortality and all-cause mortality. JAMA Intern Med. 2022, 182, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Robbins, R.; Sexis, A.; Masters, L.M.; Chanko, N.; Diaby, F.; Vieira, D.; Jean-Louis, G. Sleep tracking: A systematic review of the research using commercially available technology. Curr Sleep Med Res. 2019, 5, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Seid, A.; Fufa, D.D.; Biew, Z.W. The use of internet-based smartphone apps consistently improved consumer’s healthy eating behaviors: a systematic review of randomized controlled trials. Front Digital Health. 2024, 6, 1282570. [Google Scholar] [CrossRef] [PubMed]
- Knaggs, H.; Hester, S.N.; Gibb, T.; Riggs, M.; Ferguson, S.; Major, R.; Fisk, N. Global, gender, and age variation in skin carotenoid scores (SCS) quantified by spectroscopy reflects a measure of health and wellness. 2025 10th International Conference on Health & Nutrition, Chicago, IL, USA, Integrative Nutrition. in press.
- Major, R.; Hester, S.; Gibb, T.; Riggs, M.; Ferguson, S.; Knaggs, H.; Fisk, N. The correlation between skin carotenoid scores and specific diet and lifestyle choices. 2025 10th International Conference on Health and Nutrition, Chicago, IL, USA, Integrative Nutrition. in press.
- Faffetti, E.; Mondino, E.; Di Baldassarre, G. COVID-19 vaccine hesitancy in Sweden and Italy: The role of trust in authorities. Scandinavian J Pub Health 2022, 50, 803–809. [Google Scholar] [CrossRef]
- Stahl, W.; Heinrich, U.; Jungman, H.; von Laar, J.; Schietzel, M.; Sies, H.; Tronnier, H. Increased dermal carotenoids levels assessed by noninvasive reflection spectrophotometry correlate with serum levels in women ingesting betatene. Nutr Metab. 1998, 128, 903–907. [Google Scholar] [CrossRef]
- Streker, M.; Proksch, E.; Kattenstroth, J.-C.; Poeggeler, B.; Lemmnitz, G. Comparative assessment of nutraceuticals for supporting skin health. Nutraceuticals 2025, 5, 13. [Google Scholar] [CrossRef]
- Shanaida, M.; Mykailenko, O.; Lysiuk, R.; Hudz Balwierz, R.; Shulhai, A.; Shapovalova, N.; Shanaida, V.; Bjorklund, G. Carotenoids for antiaging: Nutraceutical, pharmaceutical, and cosmeceutical applications. Pharmaceuticals 2025, 18, 403. [Google Scholar] [CrossRef]
- Babar, M.; Buzdar, J.A.; Zaheer, Z.; Nizam-ud-din, N.; Mustafa, G.; Khan, B.A.; Hanif, M.; Asghar, T.; Qadeer, A. Carotenoids as a nutraceutical and health-promoting dietary supplement for human and animals: an update review. Trad Med Res. 2025, 10, 14. [Google Scholar] [CrossRef]
- Ibrahim, M.; Singh, H.; Fahim, M.; Khan, S.; Khan, J.; Arun, J.K.; Mishra, A.K.; Virmani, T.; Sharma, A.; Kumar, G.; Gugulothu, D.; Chopra, S.; Chopra, H. Nutraceutical interventions for mitigating skin ageing: Analysis of mechanism and efficacy. Curr Pharm Design. 2025, 31, 2385–2401. [Google Scholar] [CrossRef]
- Hester, S.N.; Major, R.A.; Gibb, T.; Riggs, M.; Ferguson, S.; Fisk, N.; Knaggs, H. Use of spectroscopy to validate effects of a multivitamin on nutrient status. Am. Soc. Nutr. 2025, Orlando, Florida, USA, Curr Dev Nutr. 2025, in press.
- Black, H.S.; Boehm, F.; Edge, R.; Truscott, T.G. The benefits and risks of certain dietary carotenoids that exhibit both anti- and pro-oxidative mechanisms- A comprehensive review. Antioxidants 2020, 9, 264. [Google Scholar] [CrossRef] [PubMed]
- Grand View Research. Carotenoids Market Size, Share & Trends Analysis Report By Product, By Application (Food, Supplements, Feed, Pharmaceuticals, Cosmetics), By Source, By Region, And Segment Forecasts, 2024 – 2030. https://www.grandviewresearch.com/industry-analysis/carotenoids-market. Accessed 20 JUN 2025.
- Harlem World, 3 March 2025. The future of wearable tech: From fitness trackers to smart clothing. https://www.harlemworldmagazine.com/the-future-of-wearable-tech-from-fitness-trackers-to-smart-clothing/#:~:text=The%20future%20of%20wearable%20tech%20is%20filled%20with%20exciting%20possibilities,we%20have%20yet%20to%20imagine. Accessed 20 JUN 2025.
- Kolasinac, S.M.; Pecinar, I.; Gajic, R.; Mutavizic, D.; Stevanovic, Z.P.D. Raman spectroscopy in the characterization of food carotenoids: Challenges and prospects. Foods 2025, 14, 953. [Google Scholar] [CrossRef] [PubMed]
- Ashokkumar, V.; Flora, G.; Sevannan, M.; Sripriya, R.; Chen, W.H.; Park, J.-H.; Banu, J.R.; Kumar, G. Technological advances in the production of carotenoids and their applications – A critical review. Bioscource Tech. 2023, 367, 128215. [Google Scholar] [CrossRef] [PubMed]
- Budzianowska, A.; Banas, K.; Budzianowski, J.; Kikowsaka, M. Antioxidants to defend healthy and youthful skin – current trends and future directions in cosmetology. Applied Sci. 2025, 15, 2571. [Google Scholar] [CrossRef]
- Afzaal, M.; Imran, A.; Iqbal, S.S.; Nawaz, S.; Batool, A.; Abbasie, N.A.; Iftikhar, T.; Nawaz, R.; Ali, A.A.; Sharif, N.T.; Zahra, M. Potential microalgae-derived antioxidants as human health supplements nutritional evaluation and benefits. Alge BioTech Biomed Nutr Appl. 2025, 200, 131–144. [Google Scholar] [CrossRef]
- Sharma, S.; Dedha, A.; Gupta, M.M.; Singh, N.; Gautan, A.; Kumari, A. Green and sustainable technologies for extraction of carotenoids from natural sources: a comprehensive review. Preparative Biochem Biotech. 2025, 55, 245–277. [Google Scholar] [CrossRef]
- Song, J. Zhu Y, Liu J. Construction of nutrient delivery system for carotenoids and their antioxidant and anti-inflammatory activities. Front. Nutr. 2025, 11, 1539429. [Google Scholar] [CrossRef]
- Valacchi, G.; Percorelli, A. Role of scavenger receptor B1 (SR-B1) in improving food benefits for human health. Annu Rev Food Sci Technol. 2025, 16, 403–432. [Google Scholar] [CrossRef]
Figure 1.
A. Carotene Structure and B. Xanthophyll-like Structure. This classification is based on the chemical structures containing only carbon and hydrogen atom (A) or the presence or absence of oxygen atoms (B). Chemical structures modified from PubChem: pubchem.ncbi.nlm.nih.gov.
Figure 1.
A. Carotene Structure and B. Xanthophyll-like Structure. This classification is based on the chemical structures containing only carbon and hydrogen atom (A) or the presence or absence of oxygen atoms (B). Chemical structures modified from PubChem: pubchem.ncbi.nlm.nih.gov.

Figure 2.
Structures of the Six Major Carotenoids Found in Human Blood, Skin and Tissues. Adapted and modified from Terao [20], license under CC BY 3.0.
Figure 2.
Structures of the Six Major Carotenoids Found in Human Blood, Skin and Tissues. Adapted and modified from Terao [20], license under CC BY 3.0.
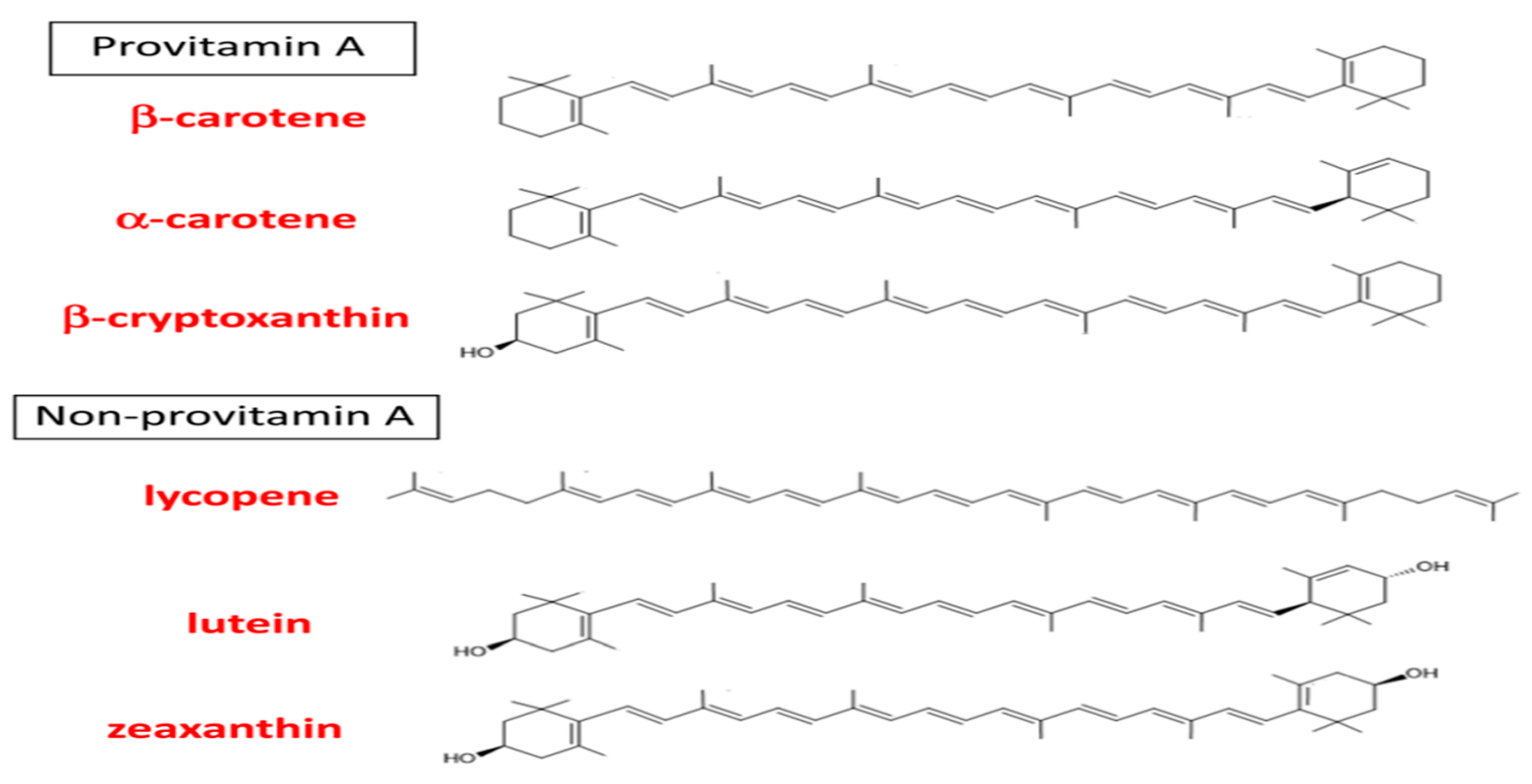
Figure 3.
Carotenoids represent a pleiotropic factor in the hallmark of aging that can enhance healthspan. This figure displays the multi-factor influences of carotenoids in health and disease. Reactive Oxygen Species = ROS.
Figure 3.
Carotenoids represent a pleiotropic factor in the hallmark of aging that can enhance healthspan. This figure displays the multi-factor influences of carotenoids in health and disease. Reactive Oxygen Species = ROS.
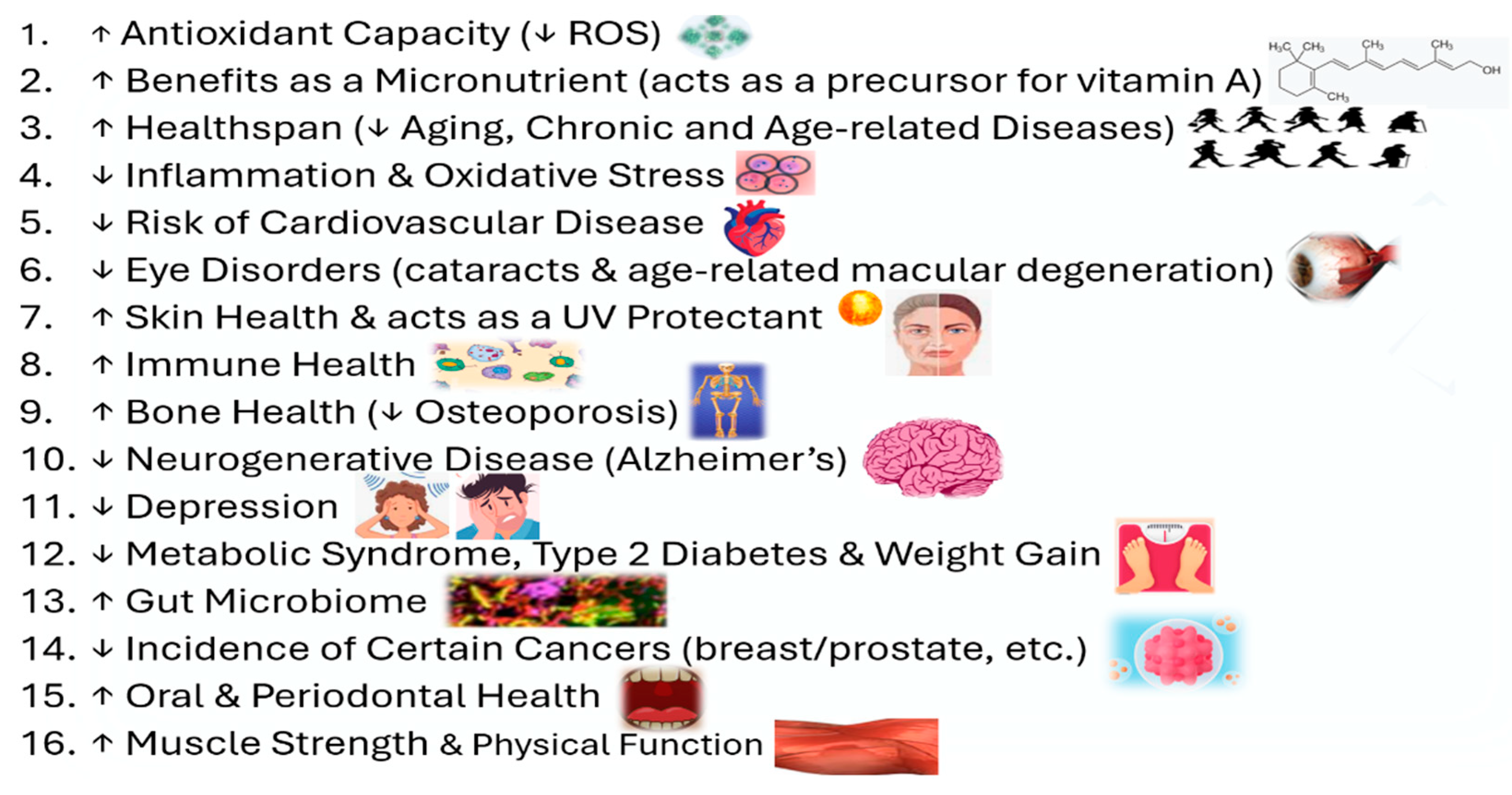
Figure 4.
Veggie Meter example display, showing the overall skin carotenoid score (red pointer-indicator) and in the right-hand panel a comparison (red bar) to a reference population histogram indicating the general population. Adapted and modified from Radtke et al. [166], license under CC BY 4.0.
Figure 4.
Veggie Meter example display, showing the overall skin carotenoid score (red pointer-indicator) and in the right-hand panel a comparison (red bar) to a reference population histogram indicating the general population. Adapted and modified from Radtke et al. [166], license under CC BY 4.0.
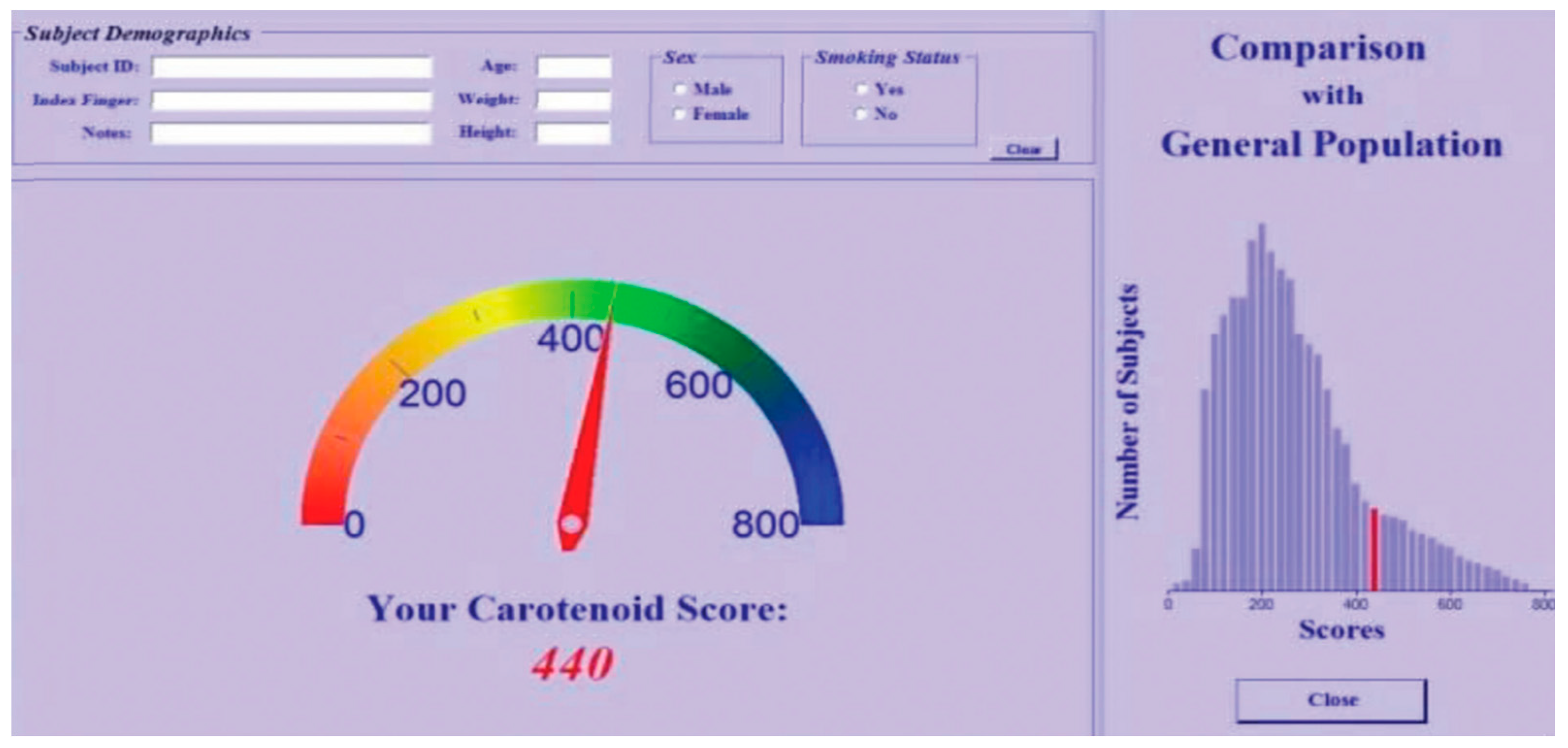
Figure 5.
Example of skin carotenoid (color-coded) ranges with a NuSkin BioPhotonic S3 Scanner® used with permission. Remarkably, more than 75 publications over 20 years have utilized NuSkin’s BioPhotonic Scanner®.
Figure 5.
Example of skin carotenoid (color-coded) ranges with a NuSkin BioPhotonic S3 Scanner® used with permission. Remarkably, more than 75 publications over 20 years have utilized NuSkin’s BioPhotonic Scanner®.
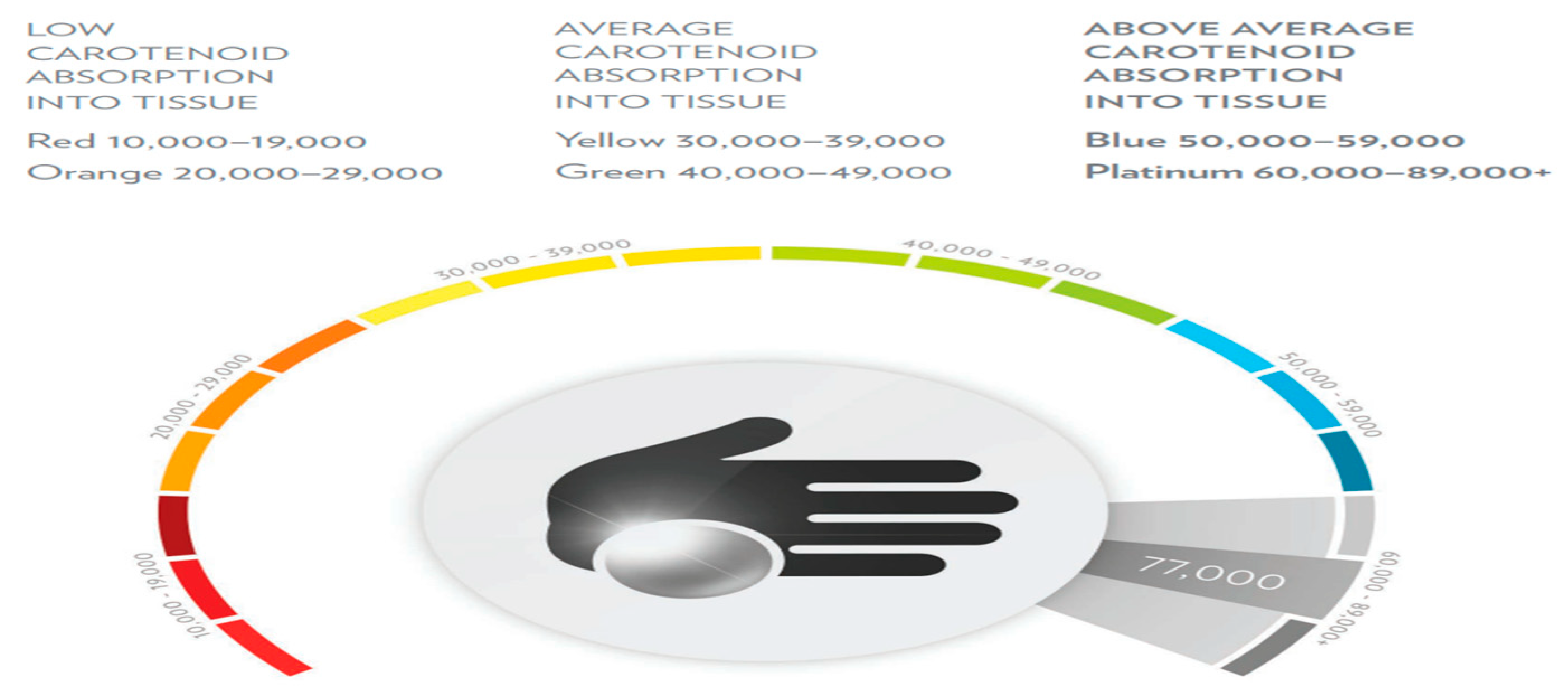
Figure 6.
A. Global Skin Carotenoid Scores by Age (from before 1 year of age = 0 to 100 years of age). Figure 6B. Total Data Collected from 2002 to 2025 Representing 21.27 Million Scans.
Figure 6.
A. Global Skin Carotenoid Scores by Age (from before 1 year of age = 0 to 100 years of age). Figure 6B. Total Data Collected from 2002 to 2025 Representing 21.27 Million Scans.
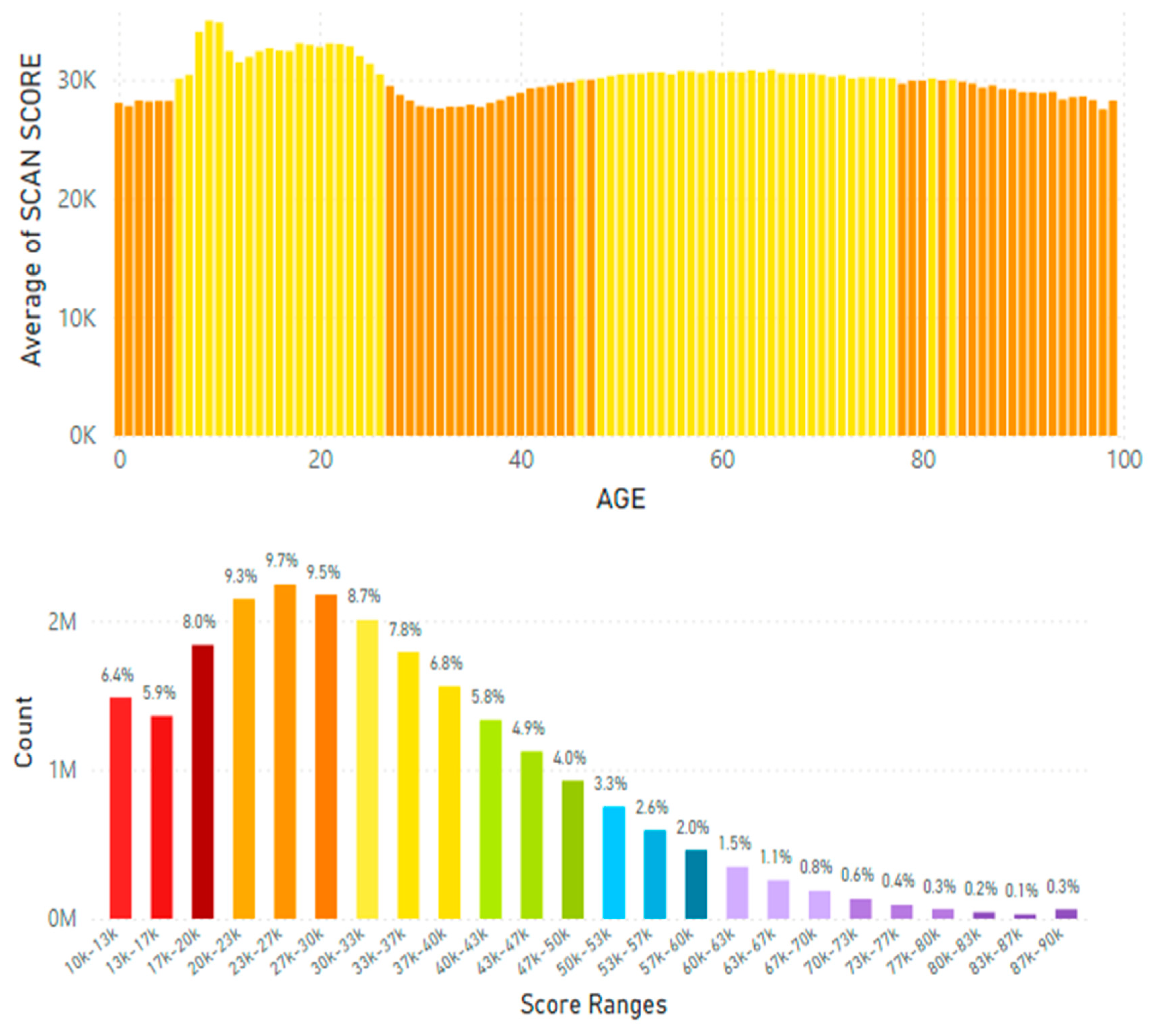
Figure 8.
A. Japanese Carotenoid Scores by Age (from before 1 year of age = 0 to 100 years of age). Figure 8B. Japanese Average Skin Carotenoid Score = 36.18 K RIU from 2.29 million scans. (See Figure 6B for more information about this histogram information.).
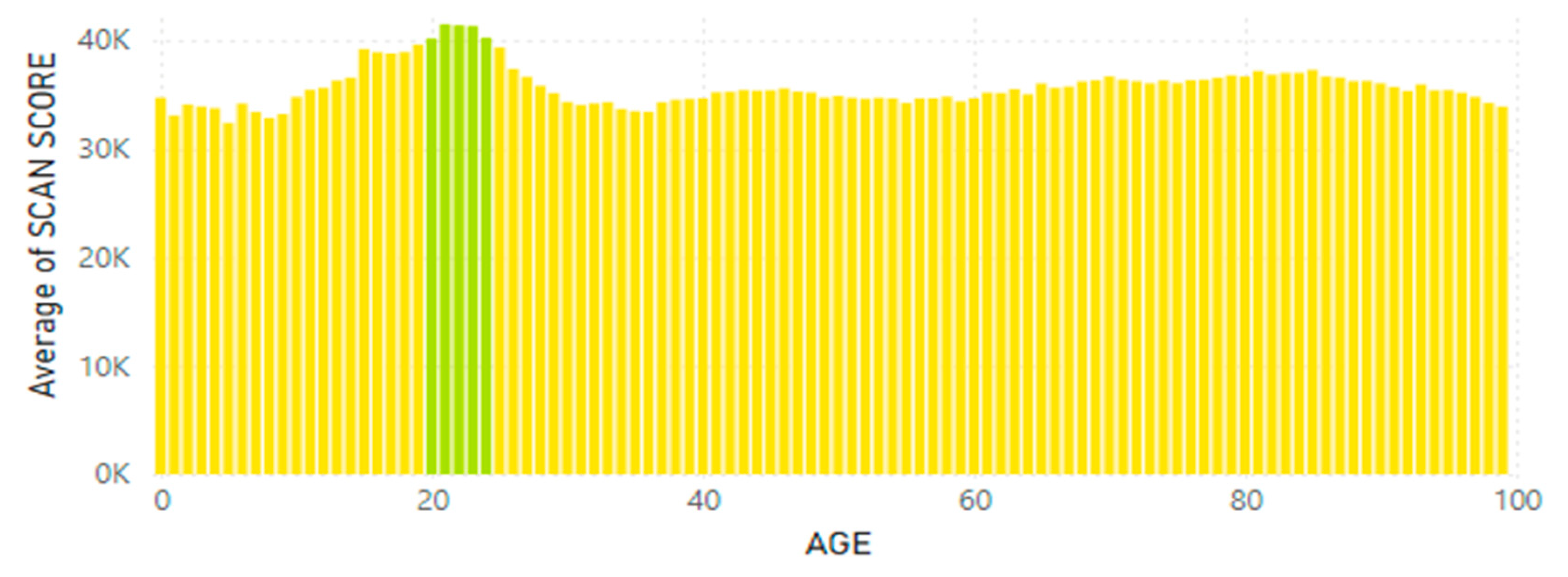
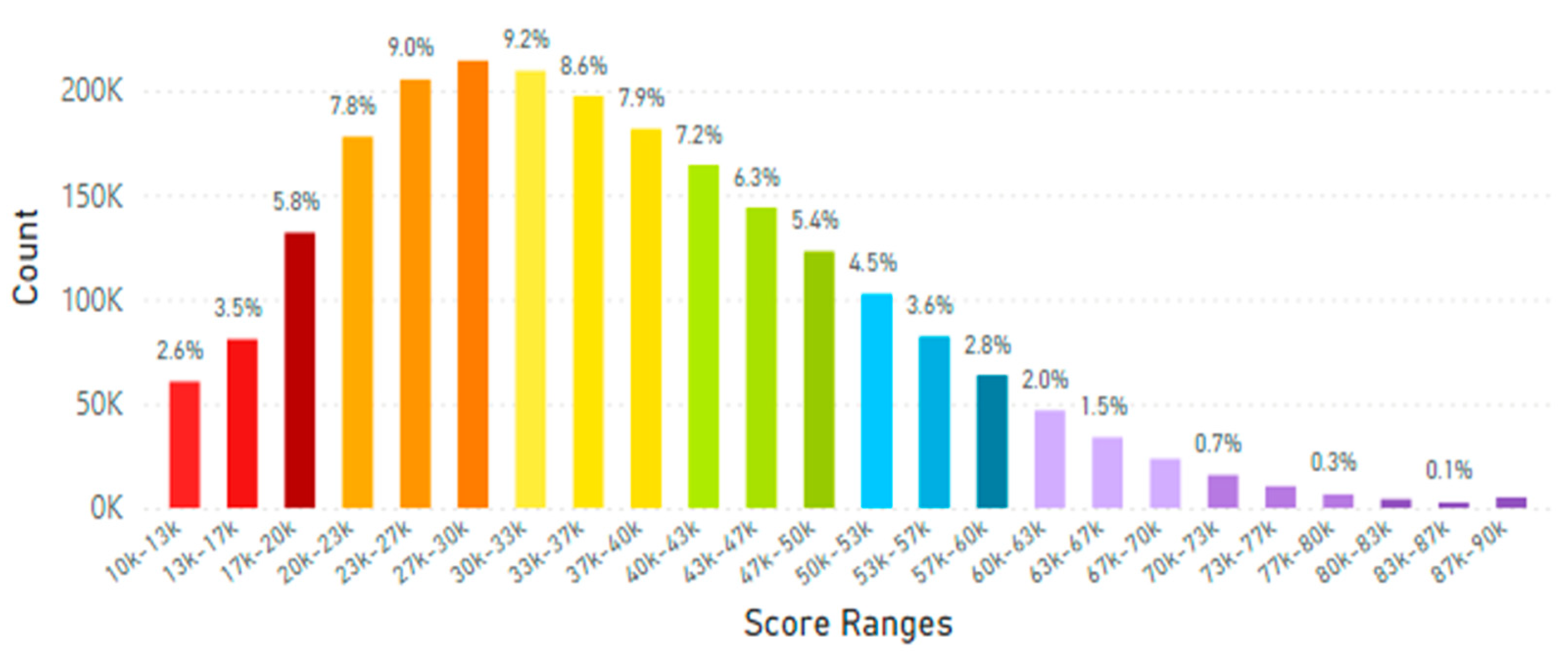
Figure 9.
A. Skin Carotenoid Scores From Mainland China by Age (from before 1 year of age = 0 to 100 years of age). Figure 9B. Mainland China Average Skin Carotenoid Score = 32.23K RIU from 3.99 million scans. (See Figure 6B legend for additional information about this histogram.).
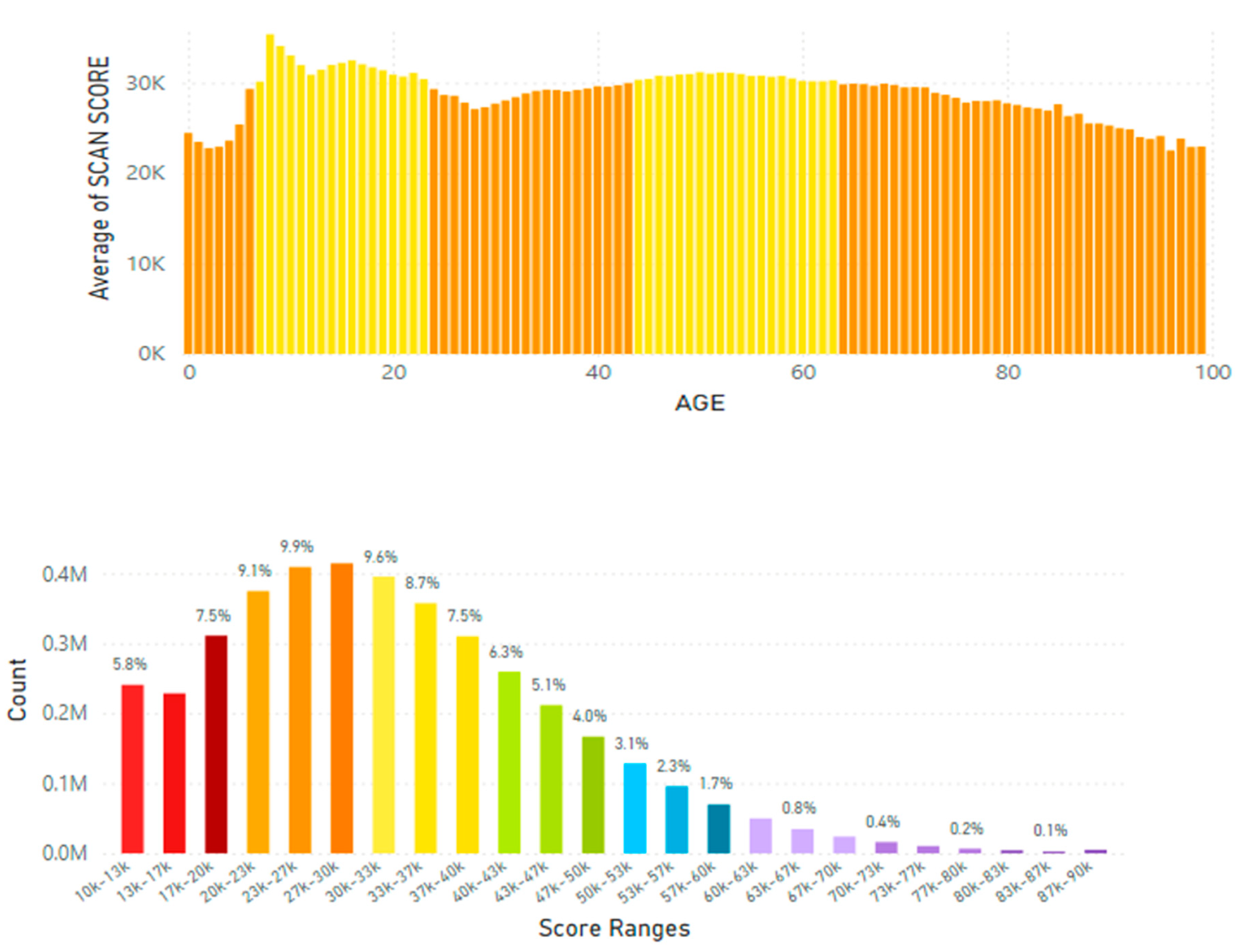
Figure 10.
A. Taiwan Carotenoid Skin Score by Age (from before 1 year of age = 0) to 100 years old). Figure 10B. The Average Skin Carotenoid Score in Tiawan was 28.85K RIU from 1.73 million scans. (See Figure 6B legend for additional information about this histogram.).
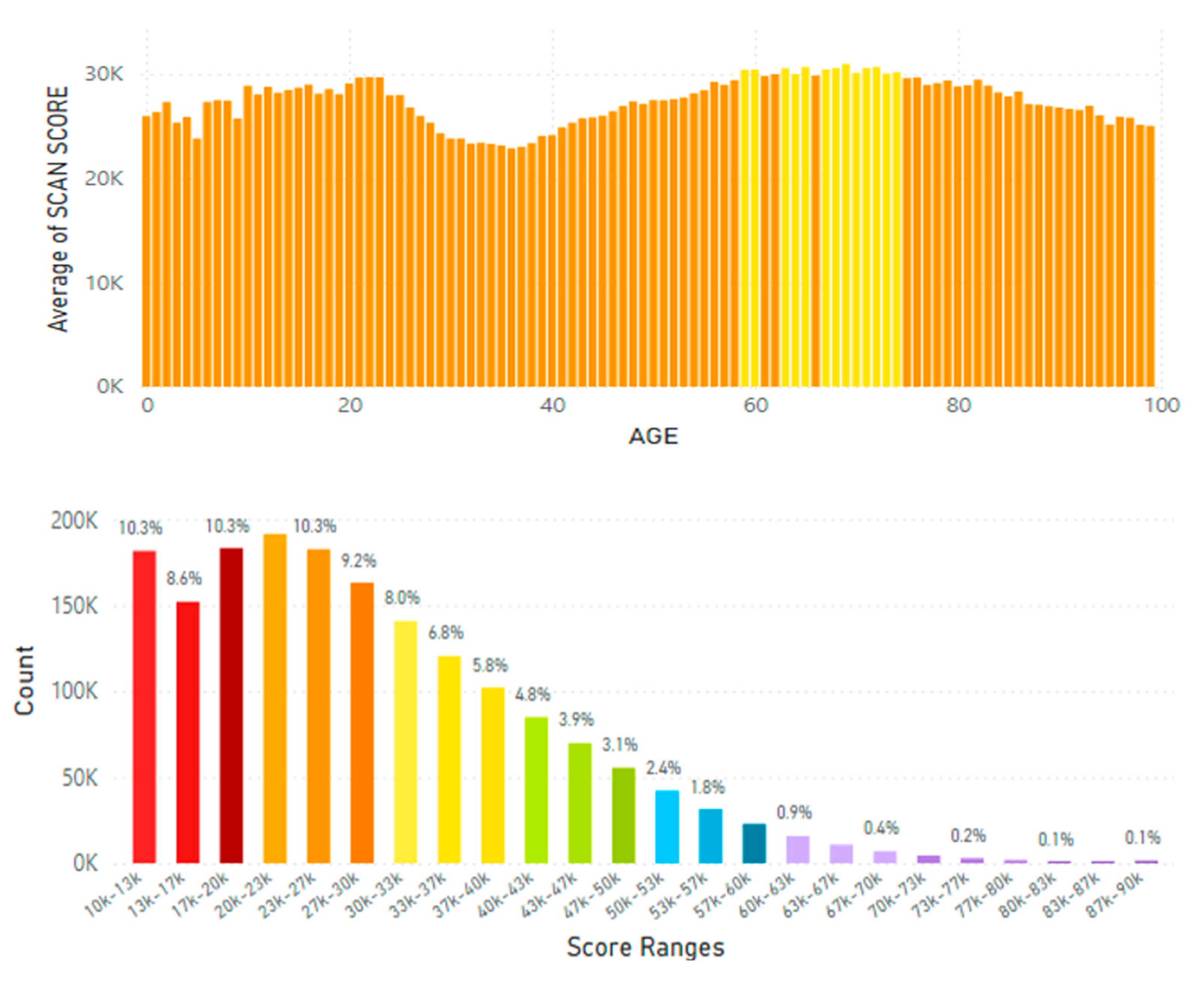
Figure 11.
A. Skin Carotenoid Scores in the Southeastern Asia by Age (from before 1 year of age = 0 to 100 years of age). Figure 11B. The Average Skin Carotenoid Score in Southeastern Asia was 27.70K RIU from 2.92 million scans. (See Figure 6B legend for additional information about this histogram.).
Figure 11.
A. Skin Carotenoid Scores in the Southeastern Asia by Age (from before 1 year of age = 0 to 100 years of age). Figure 11B. The Average Skin Carotenoid Score in Southeastern Asia was 27.70K RIU from 2.92 million scans. (See Figure 6B legend for additional information about this histogram.).
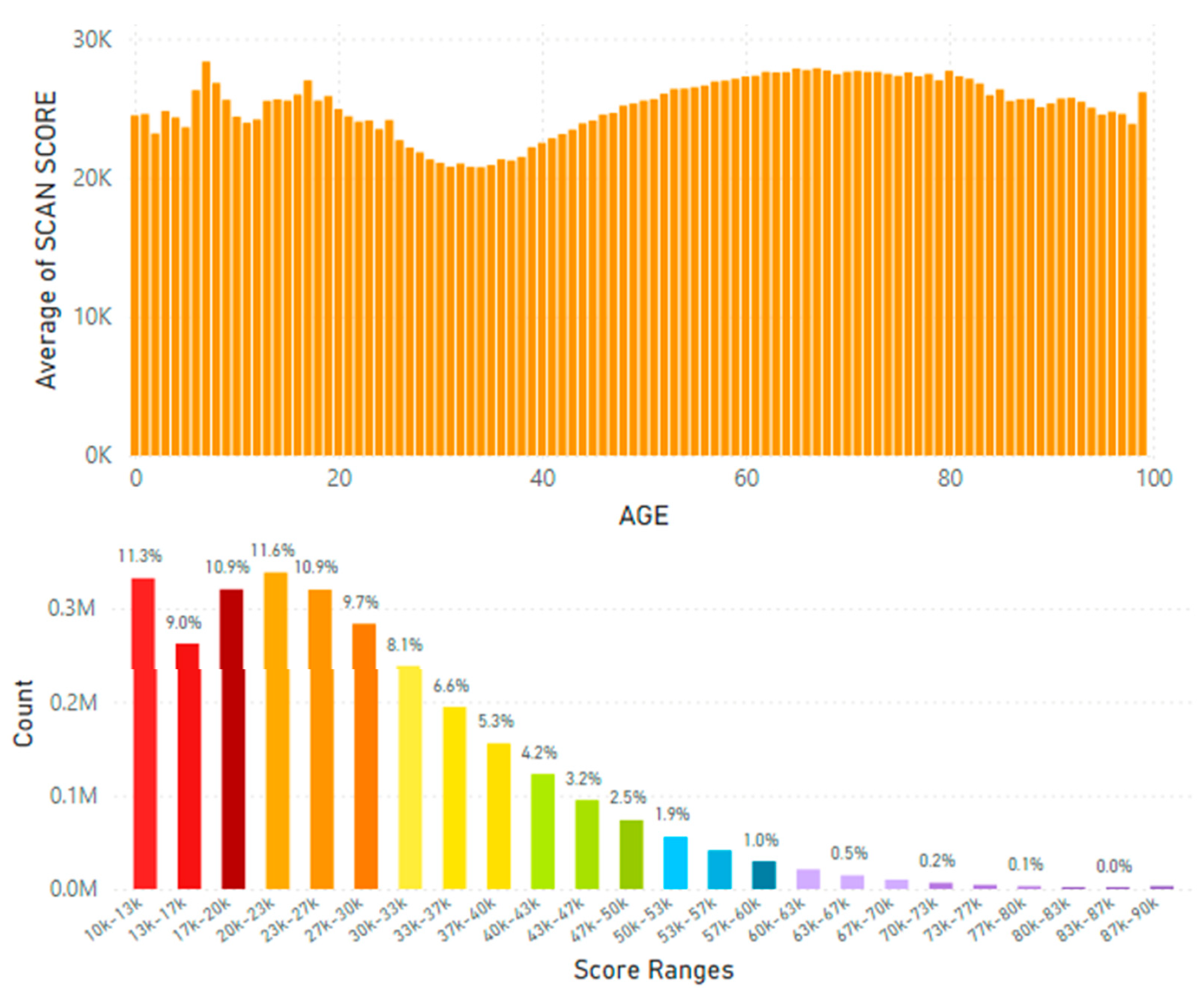
Figure 12.
A (left panels). The Philippine and Indonesia Figure 12B (right panels). The Average Skin Carotenoid Carotenoid Skin Scores by Age (from before 1 year of Score in the Philippines was 20.65K RIU from 204,500 Age = 0 to 100 years old). scans; in Indonesia was 25.29K RIU from 487,430 scans. (See Figure 6B legend for additional information about this histogram).
Figure 12.
A (left panels). The Philippine and Indonesia Figure 12B (right panels). The Average Skin Carotenoid Carotenoid Skin Scores by Age (from before 1 year of Score in the Philippines was 20.65K RIU from 204,500 Age = 0 to 100 years old). scans; in Indonesia was 25.29K RIU from 487,430 scans. (See Figure 6B legend for additional information about this histogram).
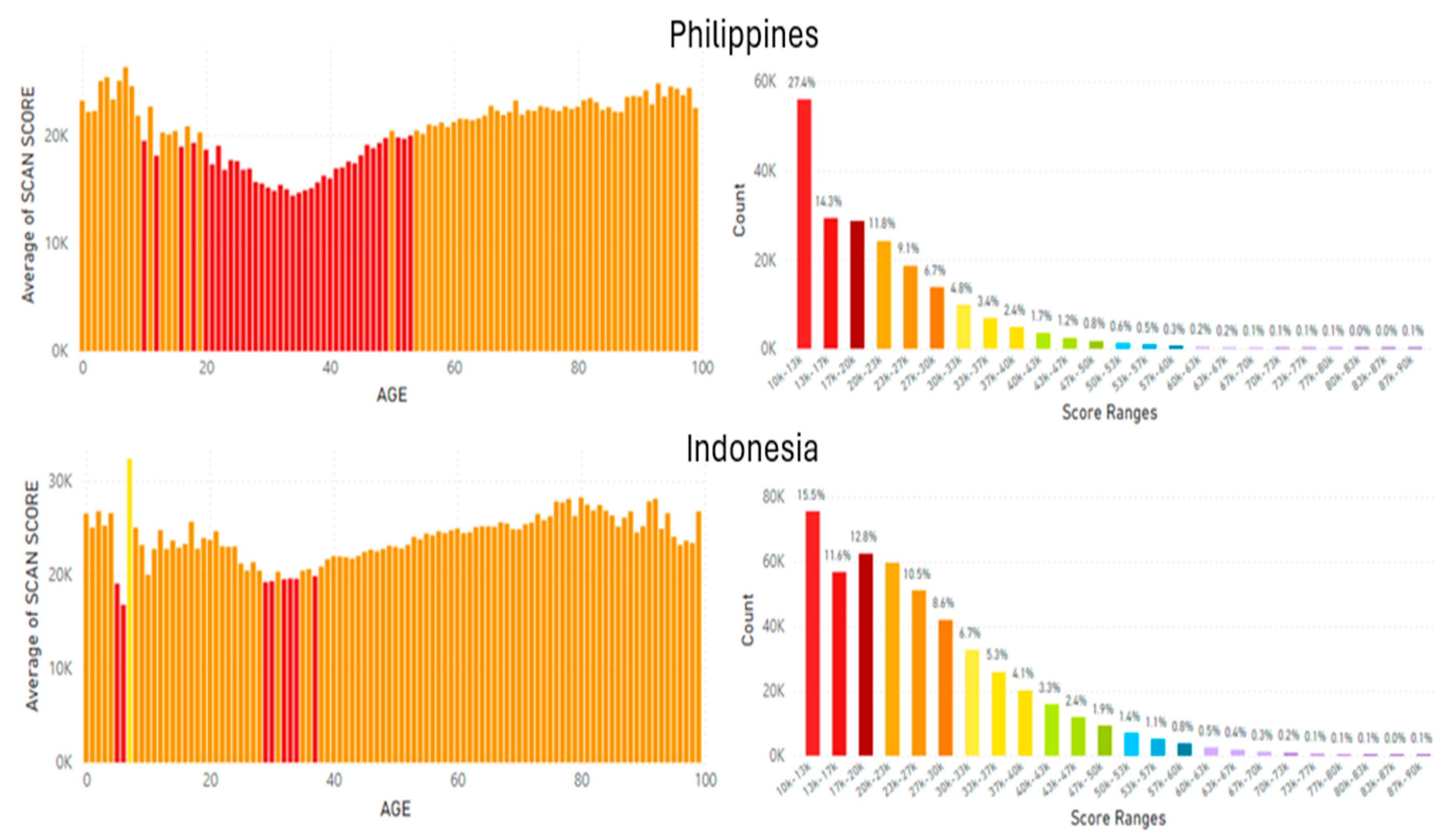
Figure 13.
A. Thailand Carotenoid Scores by Age (from before 1 year of age = 0 to 100 years of age).Figure 13B. Thailand Average Skin Carotenoid Score = 29.16K RIU from 705,790 scans. (See Figure 6B legend for additional information about this histogram.).
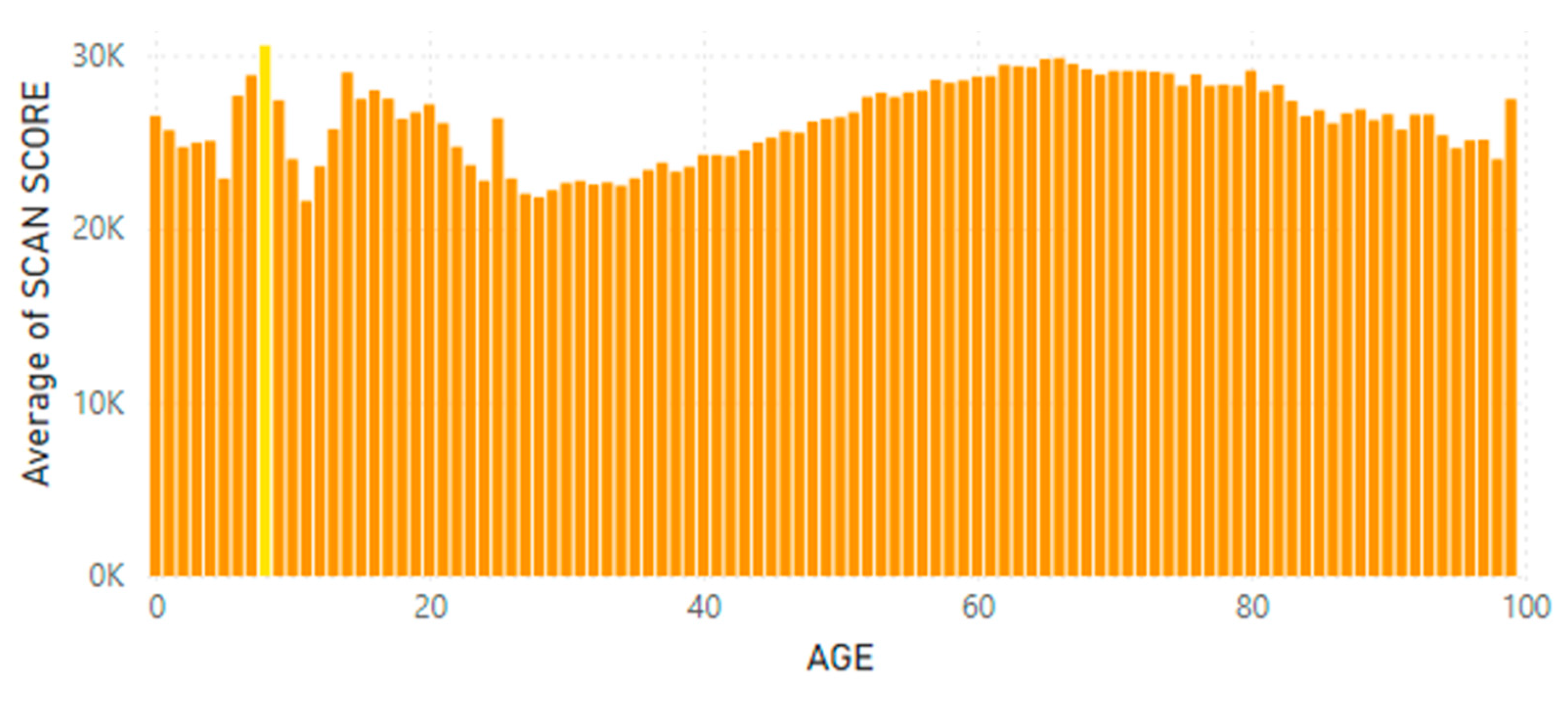
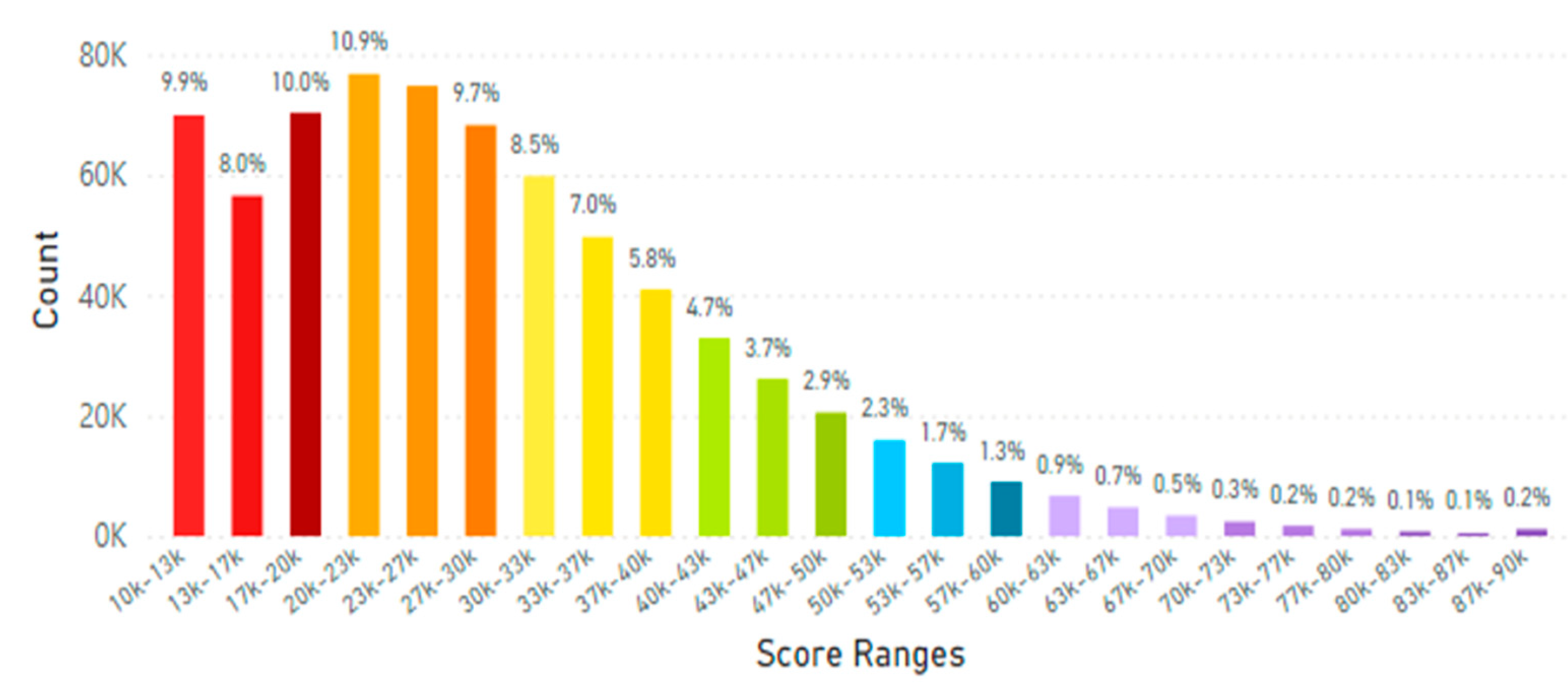
Figure 14.
A. Australia and New Zealand Skin Carotenoid Scores by Age (from before 1 year of age = 0 to 100 years of age).Figure 14B. Australia and New Zealand Average Skin Carotenoid Score = 28.90K RIU from 3.48 million scans. (See Figure 6B for additional information about this histogram.).
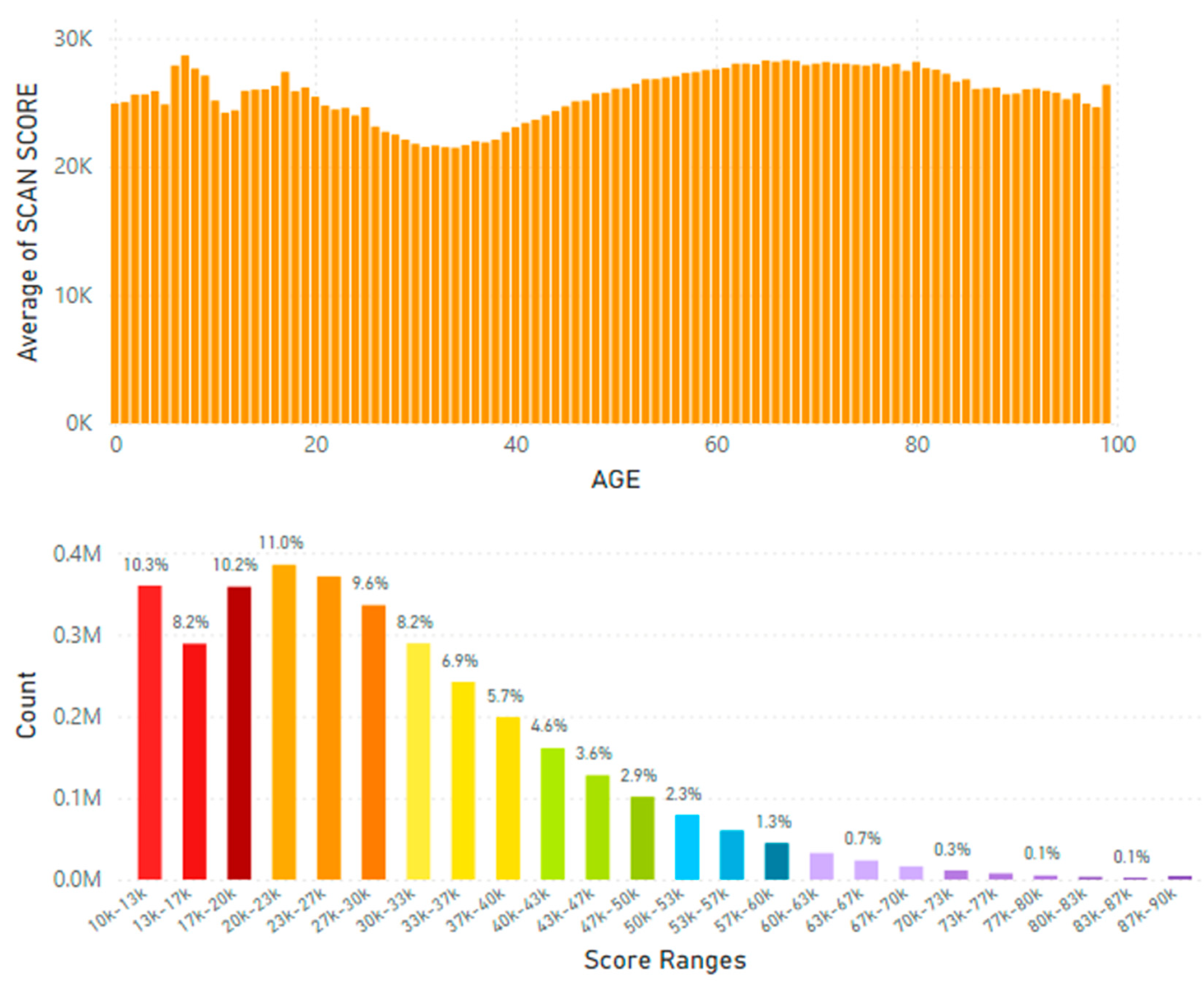
Figure 15.
A. Skin Carotenoid Scores from Europe and Africa by Age (from before 1 year of age = 0 to 100 years of age).Figure 15B. The Europe Average Skin Carotenoid Score = 34.50K RIU from 3.18 million scans. (See Figure 6B legend for additional information about this histogram.).
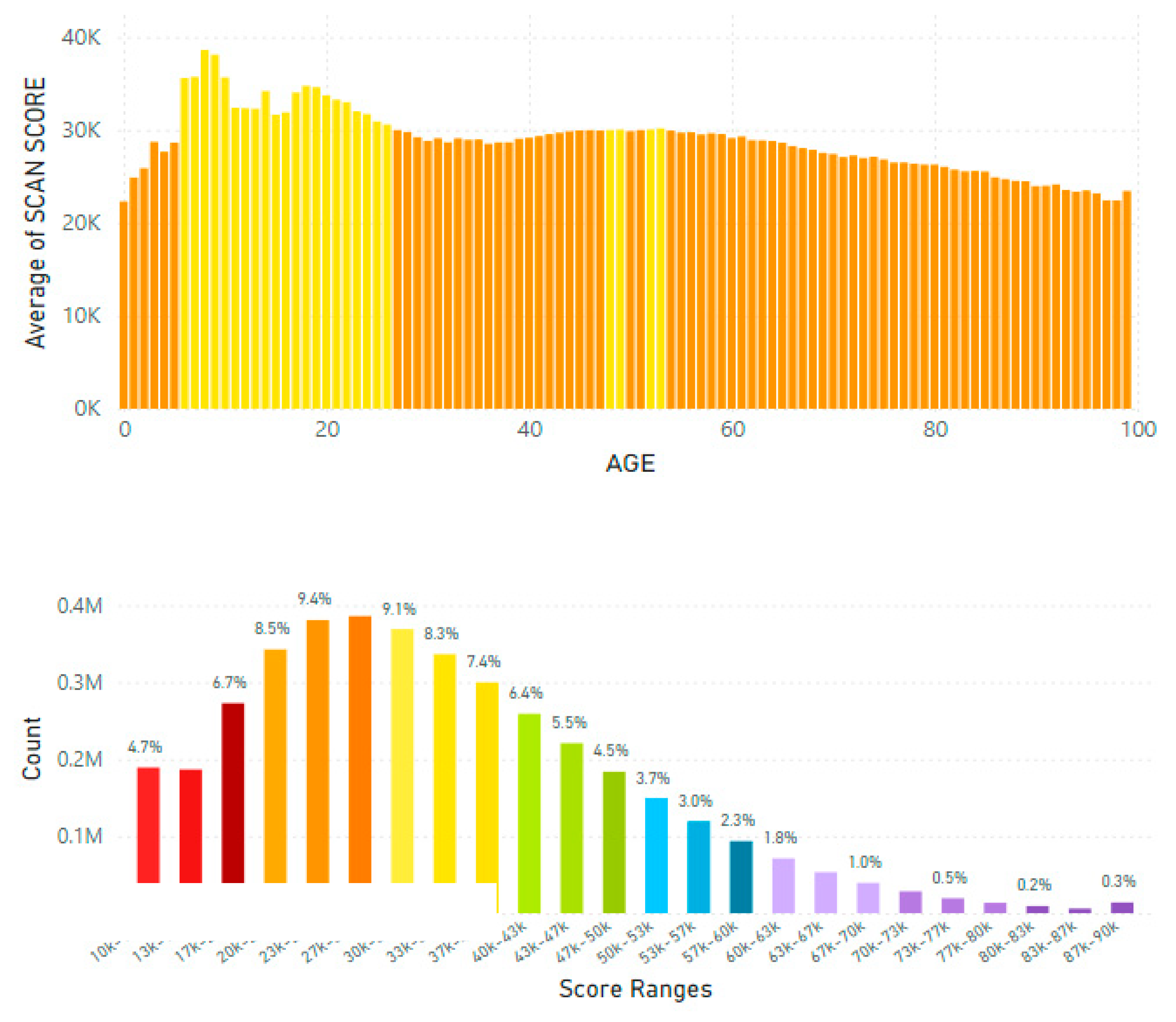
Figure 16.
A. Skin Carotenoid Scores from the United Kingdom by Age (from before 1 year of age = 0 to 100 years of age).Figure 16B. United Kingdom Average Skin Carotenoid Score = 36.68K RIU from 104,990 scans. (See Figure 6B legend for additional information about this histogram.).
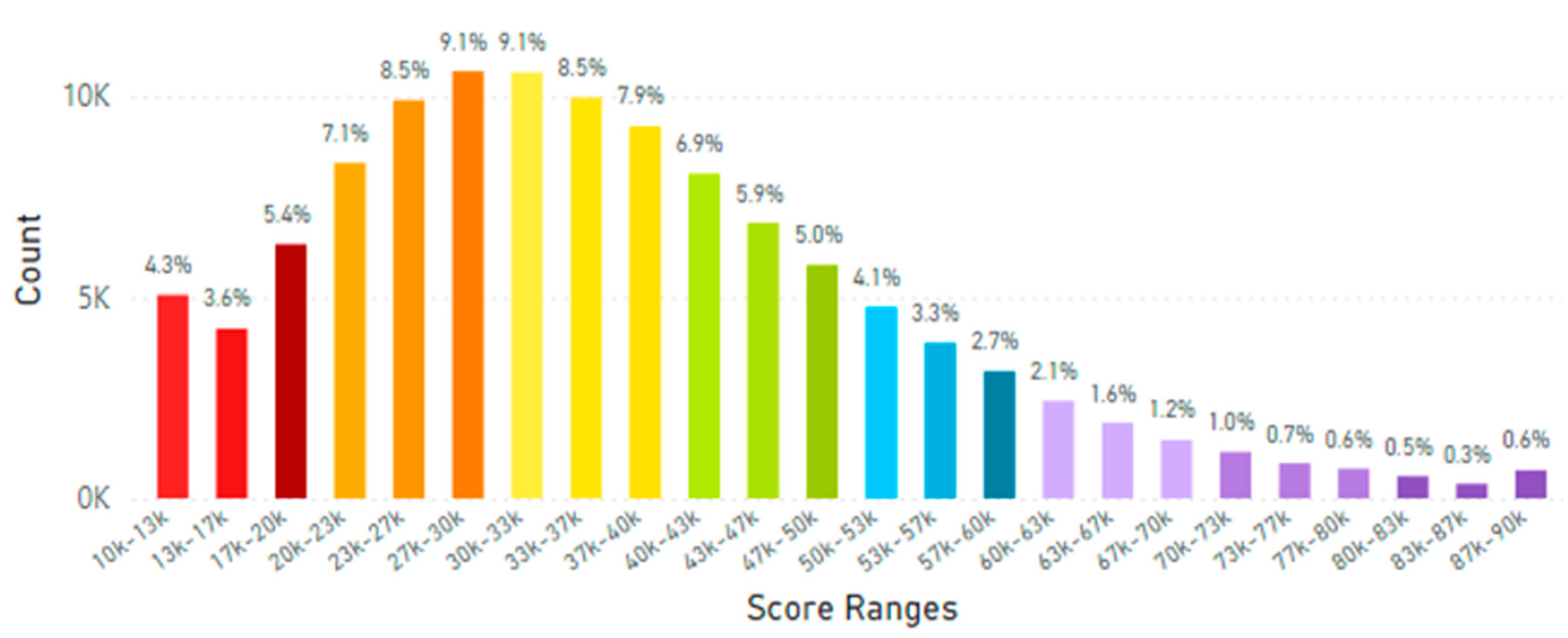
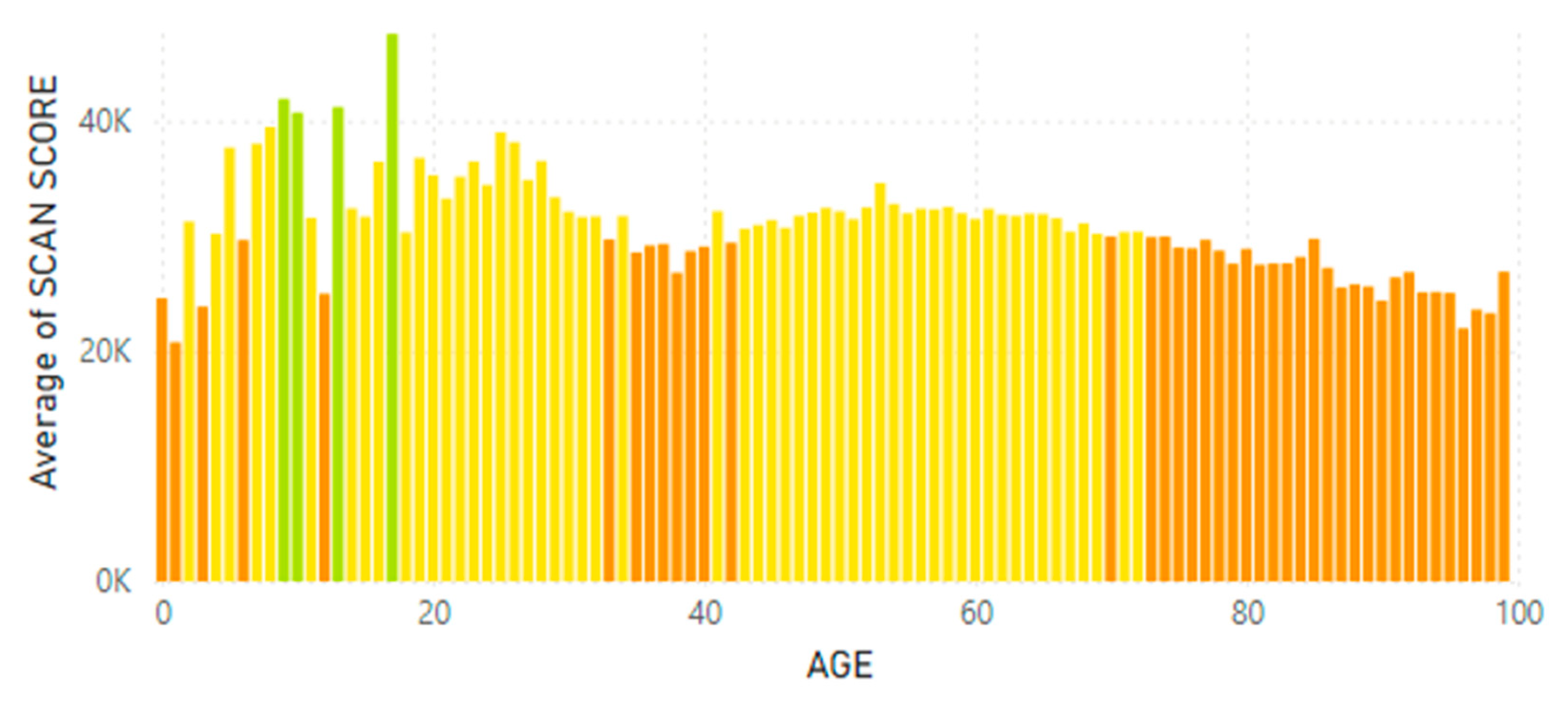
Figure 17.
A. Skin Carotenoid Scores From France and Germany by Age (from before 1 year of age = 0 to 100 years of age). Figure 17B. France and Germany Average Skin Carotenoid Score = 42.68K RIU from 155,700 scans. (See Figure 6B legend for additional information about this histogram.).
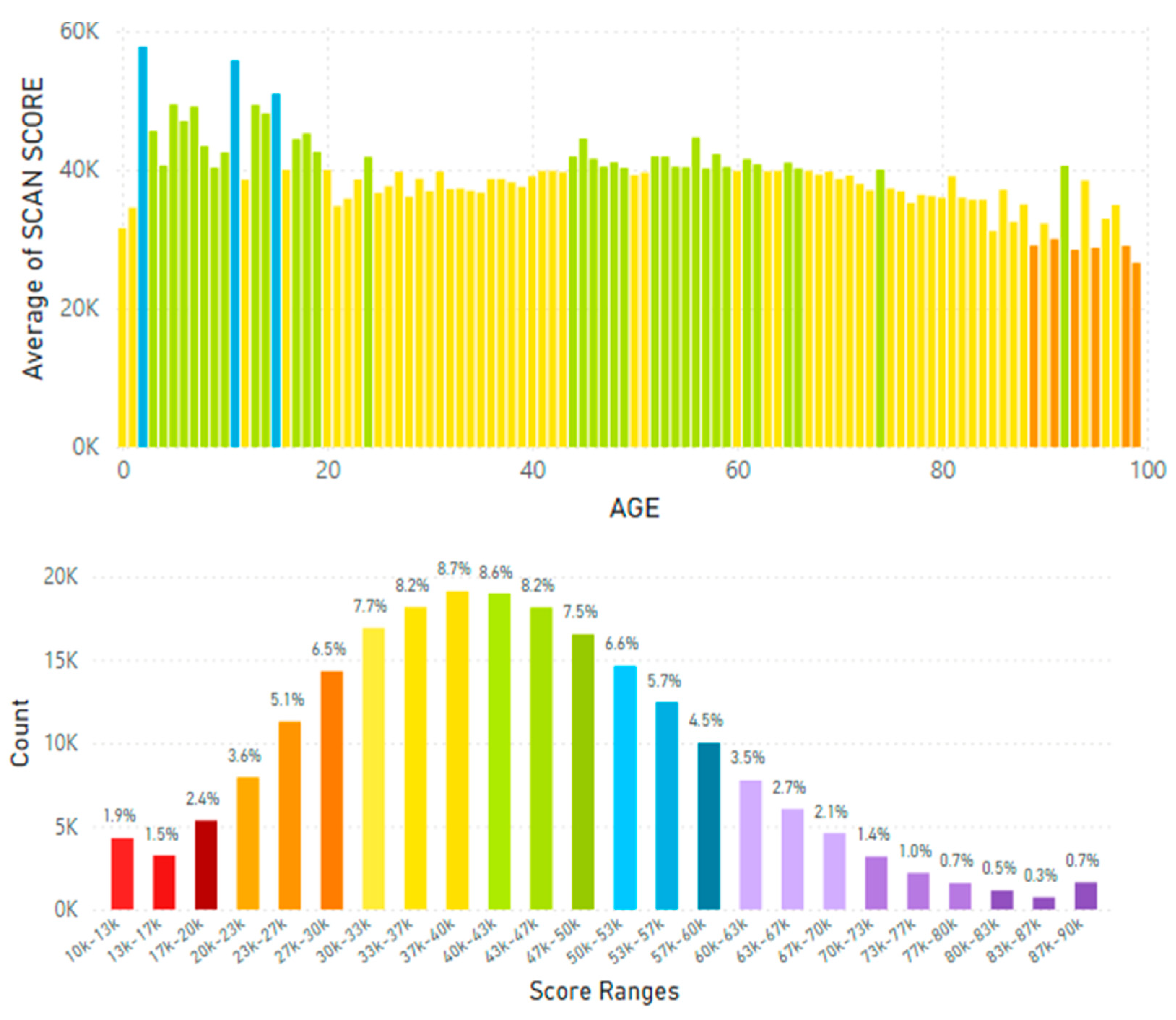
Figure 18.
A. European Skin Carotenoid Scores during the Pandemic (April 2020 to January 2025) by Age.Figure 18B. European Average Skin Carotenoid Scores = 44.34K RIU from 392,600 scans during the Pandemic. (See Figure 6B legend for additional information about this histogram.).
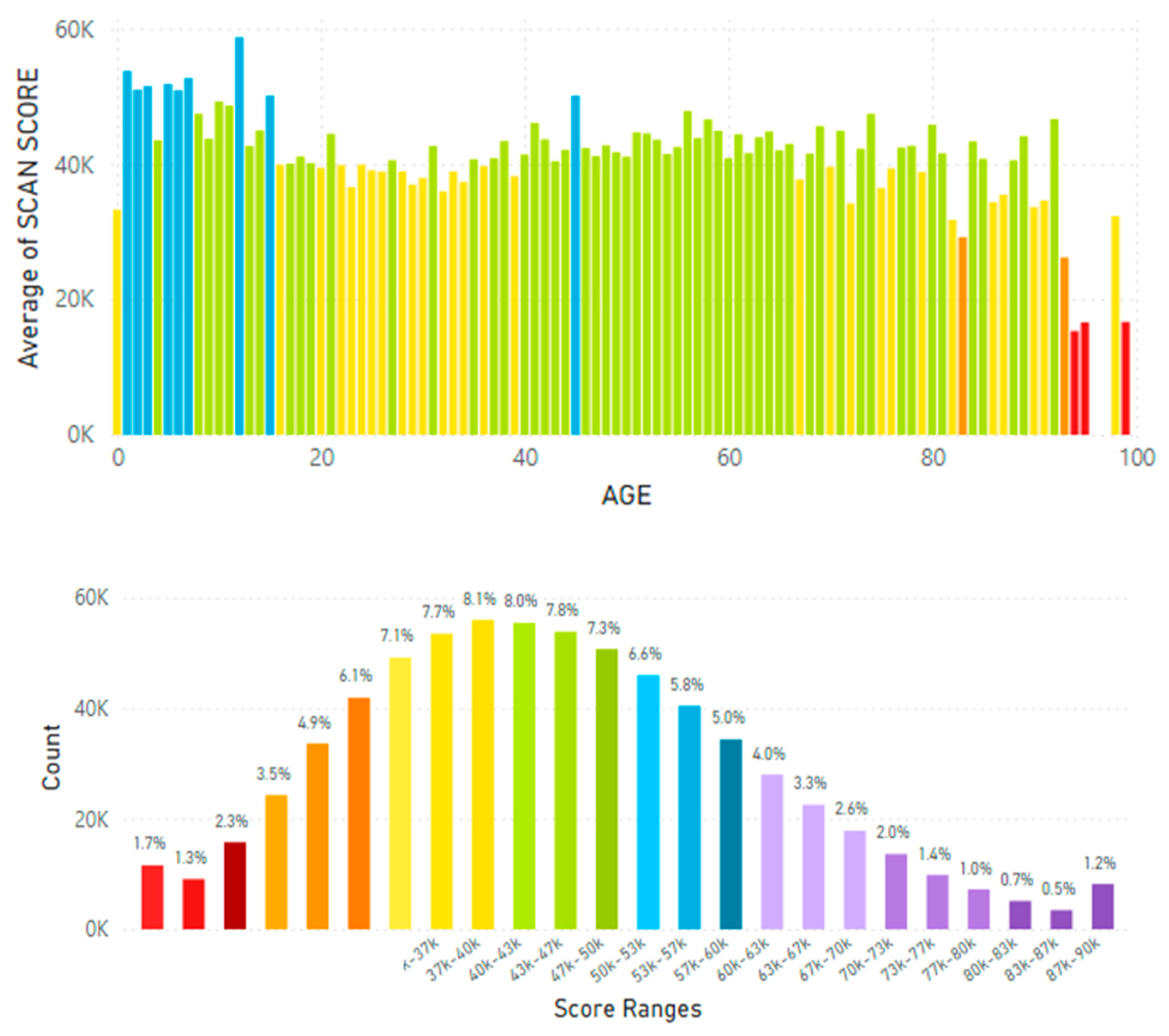
Figure 19.
A. North America (Canada and The United States of America) Skin Carotenoid Scores by Age (from before 1 year of age = 0 to 100 years of age).Figure 19B. North America (Canada and The United States of America) Average Skin Carotenoid Score = 33.00K RIU from 4.89 million scans. (See Figure 6B legend for additional information about this histogram.).
Figure 19.
A. North America (Canada and The United States of America) Skin Carotenoid Scores by Age (from before 1 year of age = 0 to 100 years of age).Figure 19B. North America (Canada and The United States of America) Average Skin Carotenoid Score = 33.00K RIU from 4.89 million scans. (See Figure 6B legend for additional information about this histogram.).
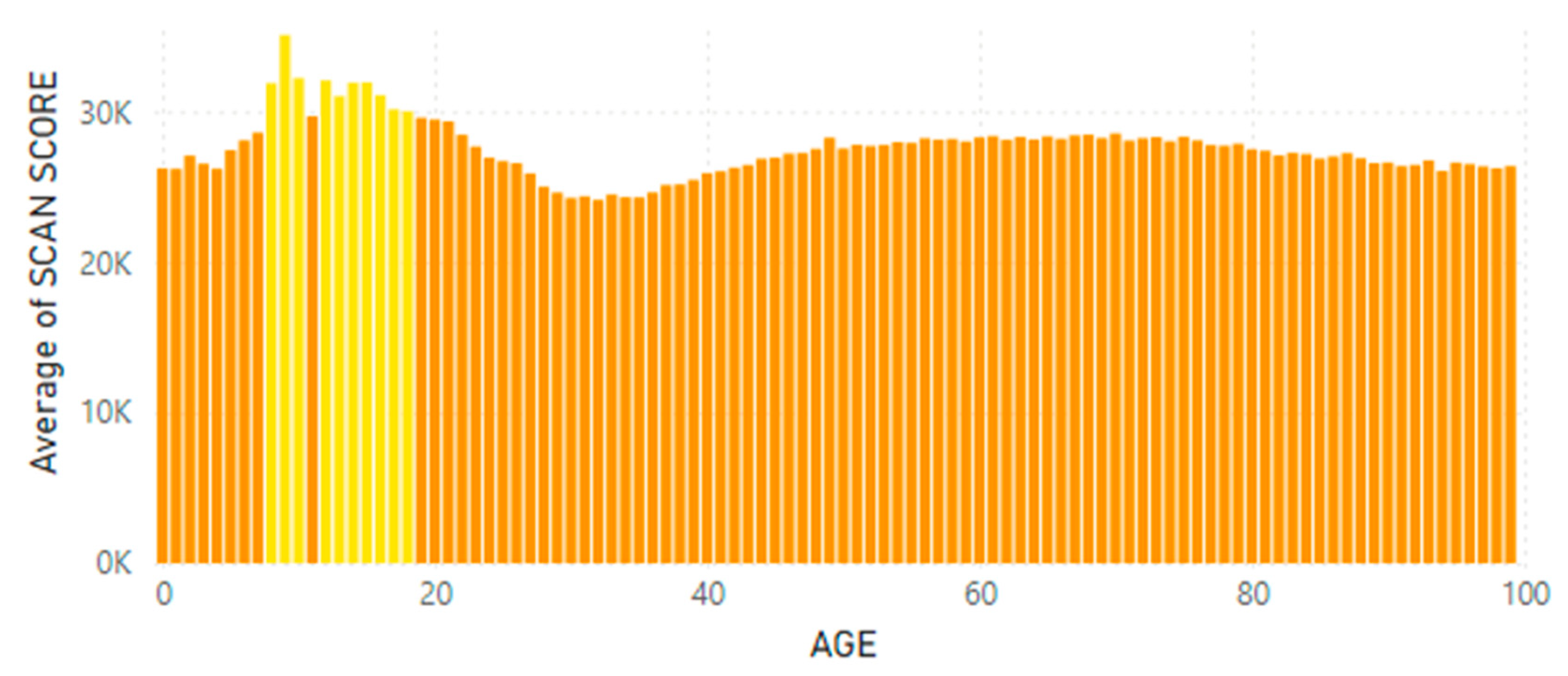
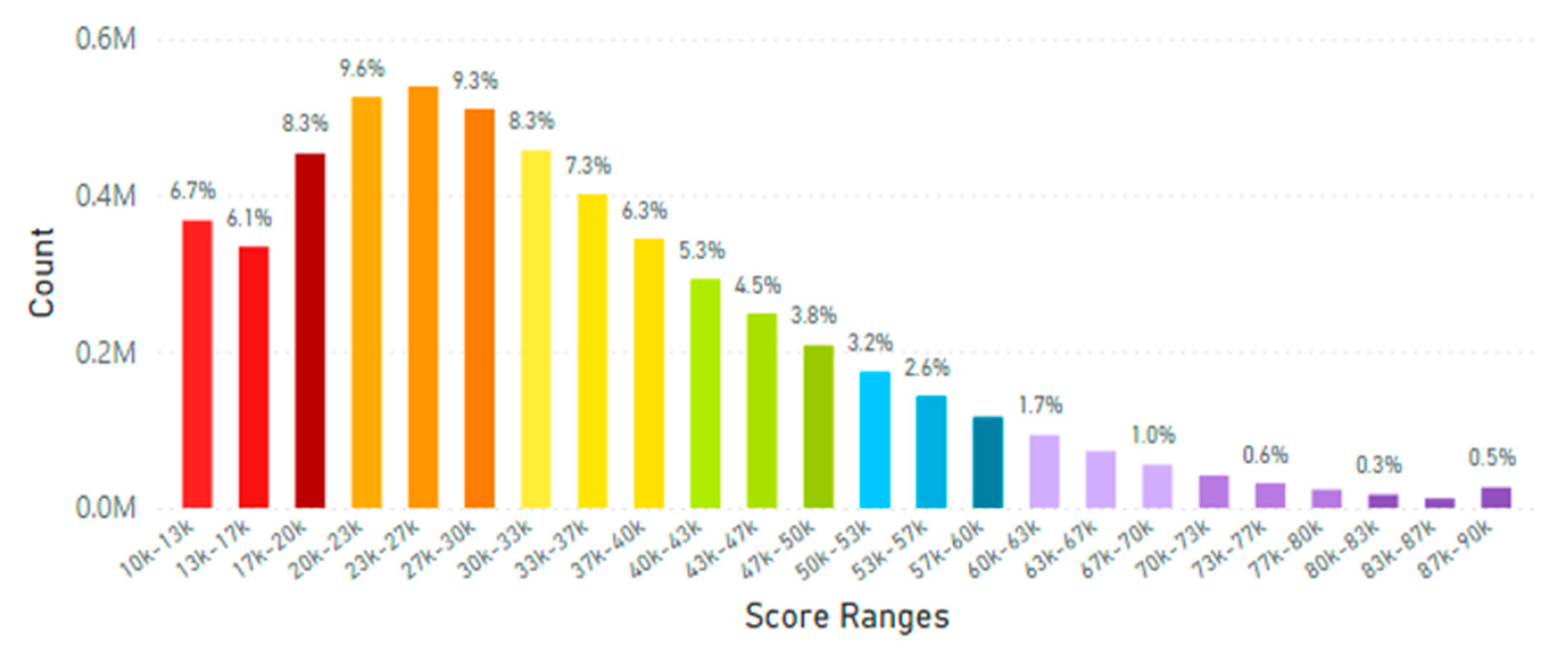
Figure 20.
A. Skin Carotenoid Scores from Latin America by Age (from before 1 year of age = 0 to 100 years of age).Figure 20B. Latin America Average Skin Carotenoid Score = 32.39K RIU from 306,490 scans. (See Figure 6B legend for additional information about this histogram.).
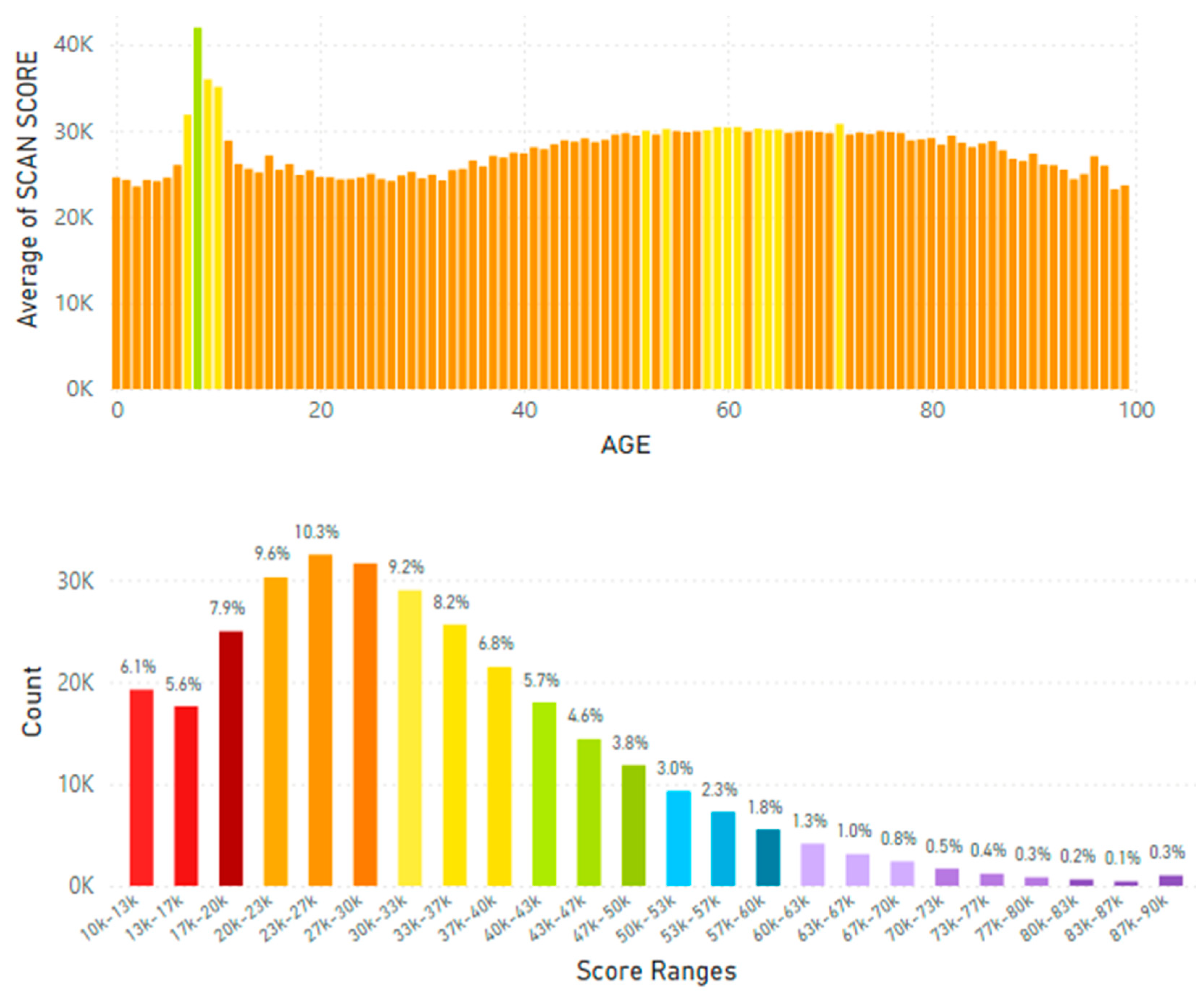
Figure 21.
Left-panel RRS Skin Carotenoid Levels. Right-panel RS Skin Carotenoid Levels. * = signficantly increased skin carotenoid levels compared to placebo-control values.
Figure 21.
Left-panel RRS Skin Carotenoid Levels. Right-panel RS Skin Carotenoid Levels. * = signficantly increased skin carotenoid levels compared to placebo-control values.
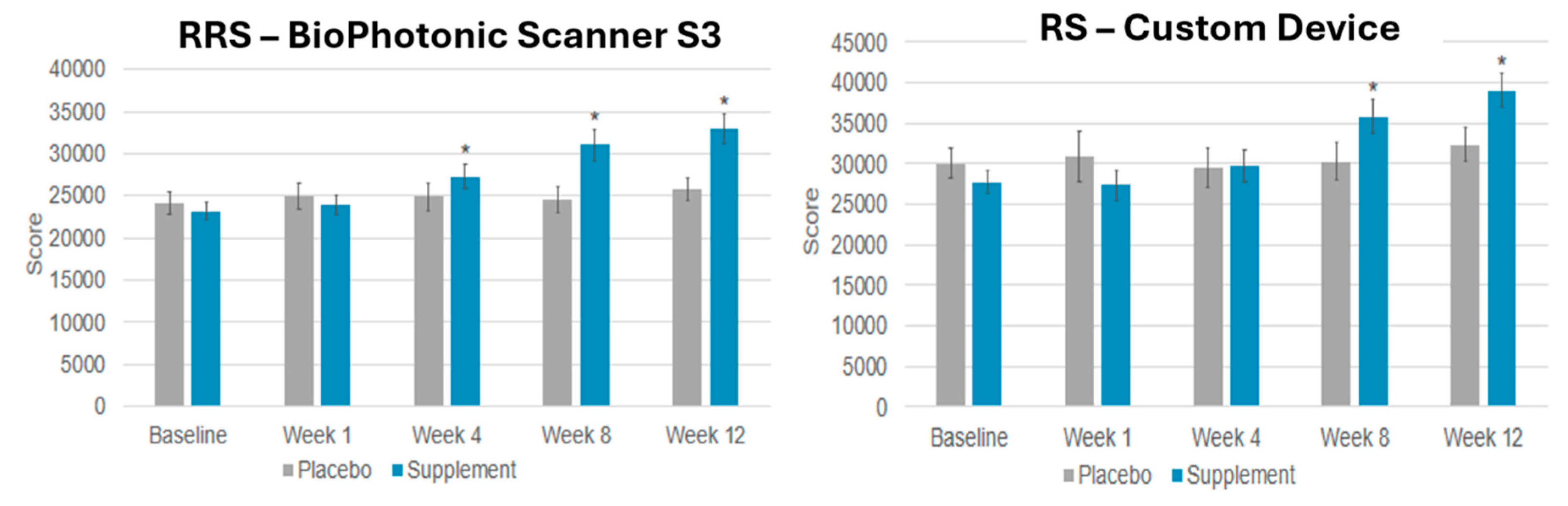
Figure 22.
Global Skin Carotenoid Scores Correlated with Fruit and Vegetable (F&V) Daily Intake or with Individuals Taking the Nutraceutical Supplement (Life Pak) twice daily. Life Pak contains vitamins, minerals, carotenoids and phytonutrients.
Figure 22.
Global Skin Carotenoid Scores Correlated with Fruit and Vegetable (F&V) Daily Intake or with Individuals Taking the Nutraceutical Supplement (Life Pak) twice daily. Life Pak contains vitamins, minerals, carotenoids and phytonutrients.
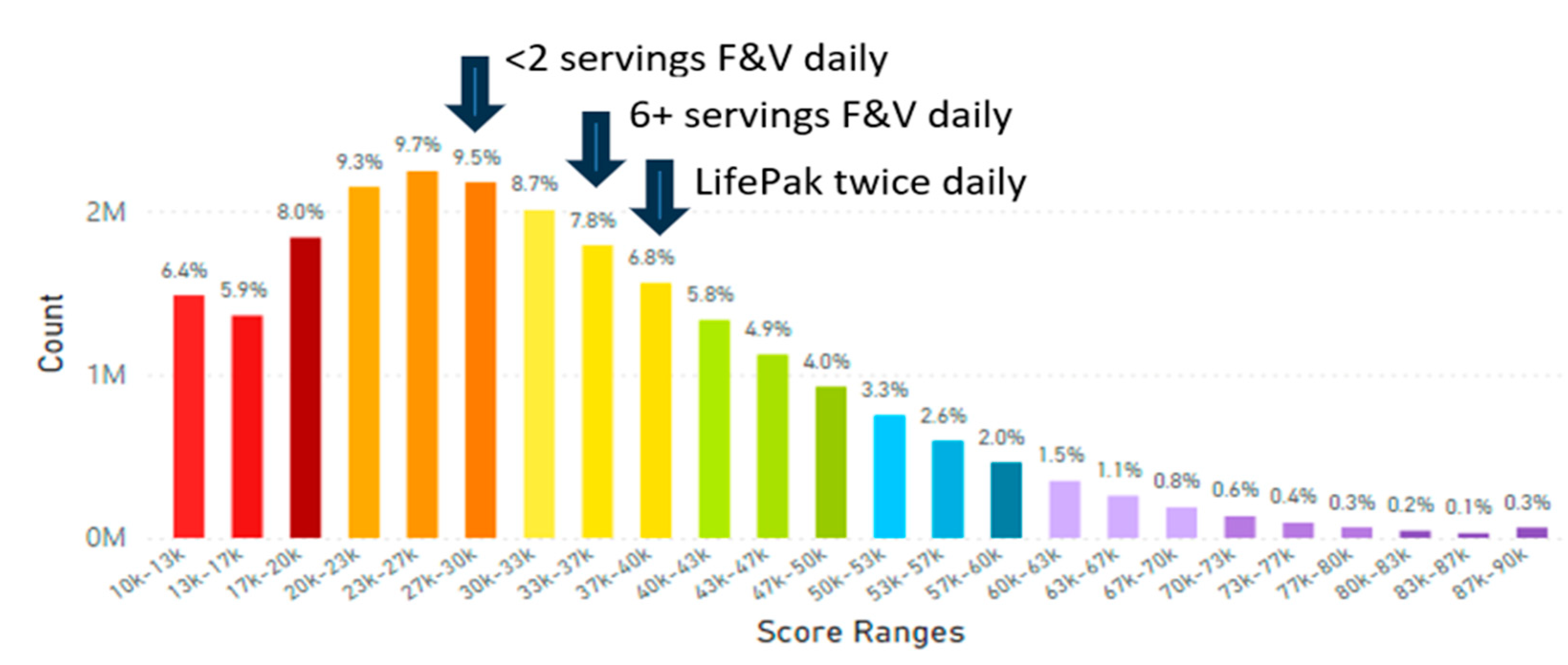
Figure 23.
The Importance of Carotenoids in Well-being to Enhance Human Healthspan by Knowing Skin Carotenoid Levels.
Figure 23.
The Importance of Carotenoids in Well-being to Enhance Human Healthspan by Knowing Skin Carotenoid Levels.
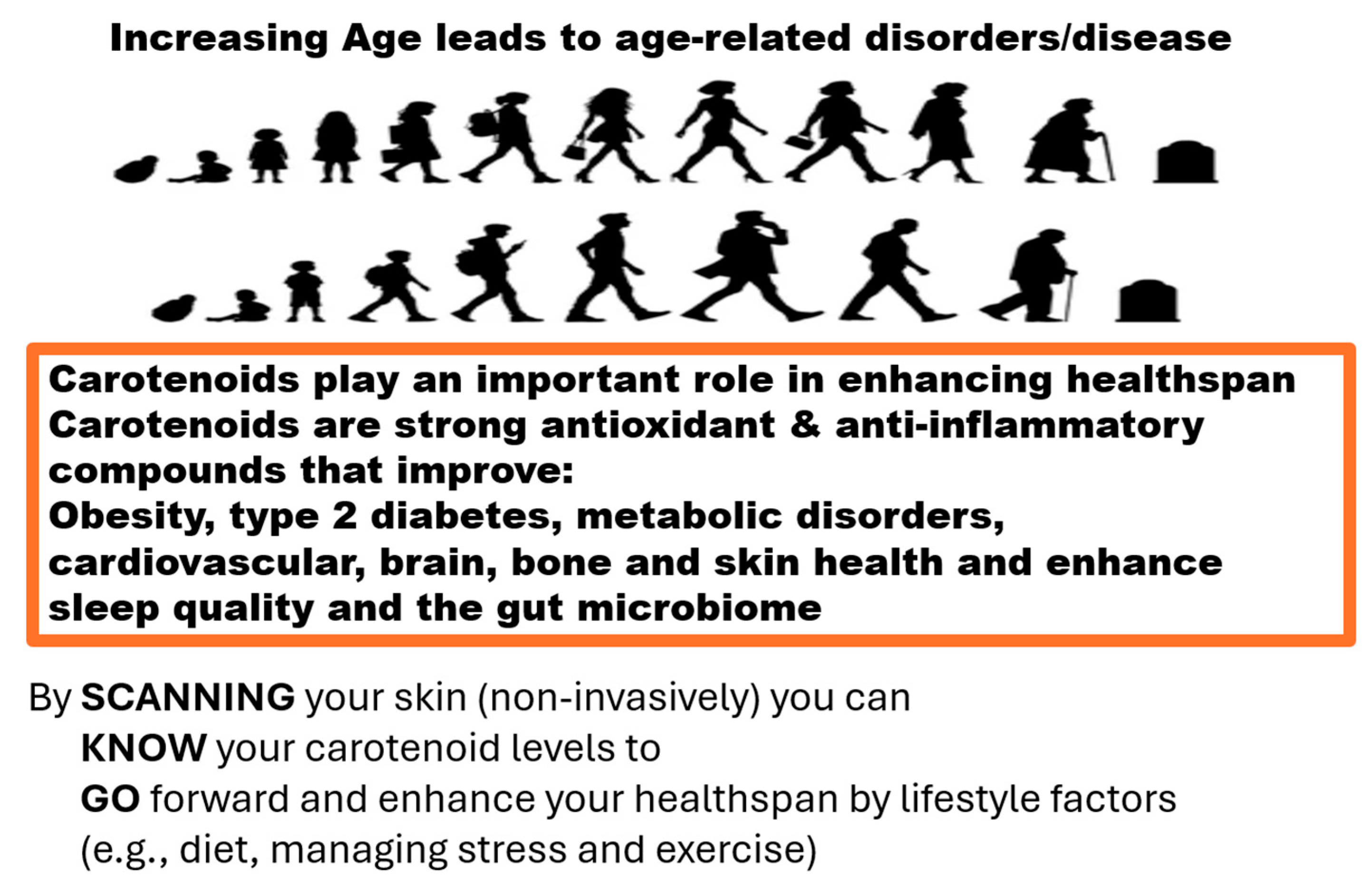

Table 1.
Skin Carotenoid Scores From the Nordic Countries and Russia.
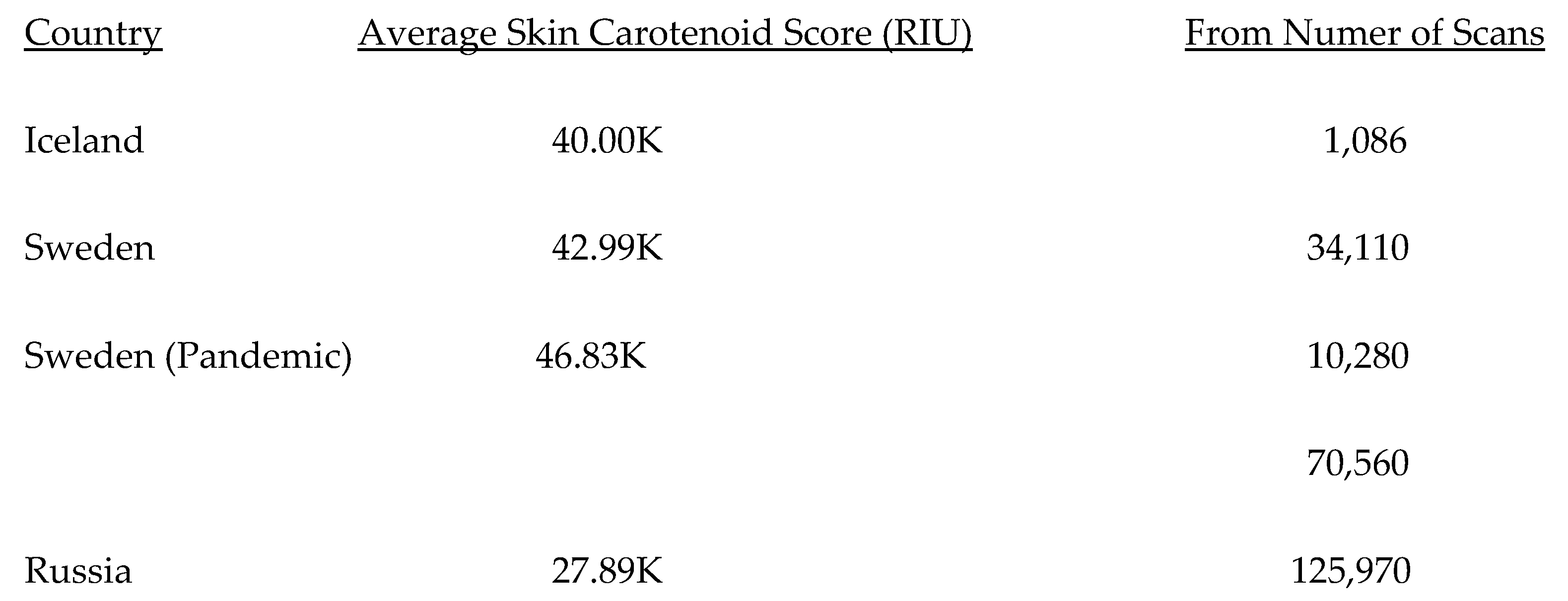
Table 2.
Global Average Skin Carotenoid Scores (RIU) by Ethinicity.
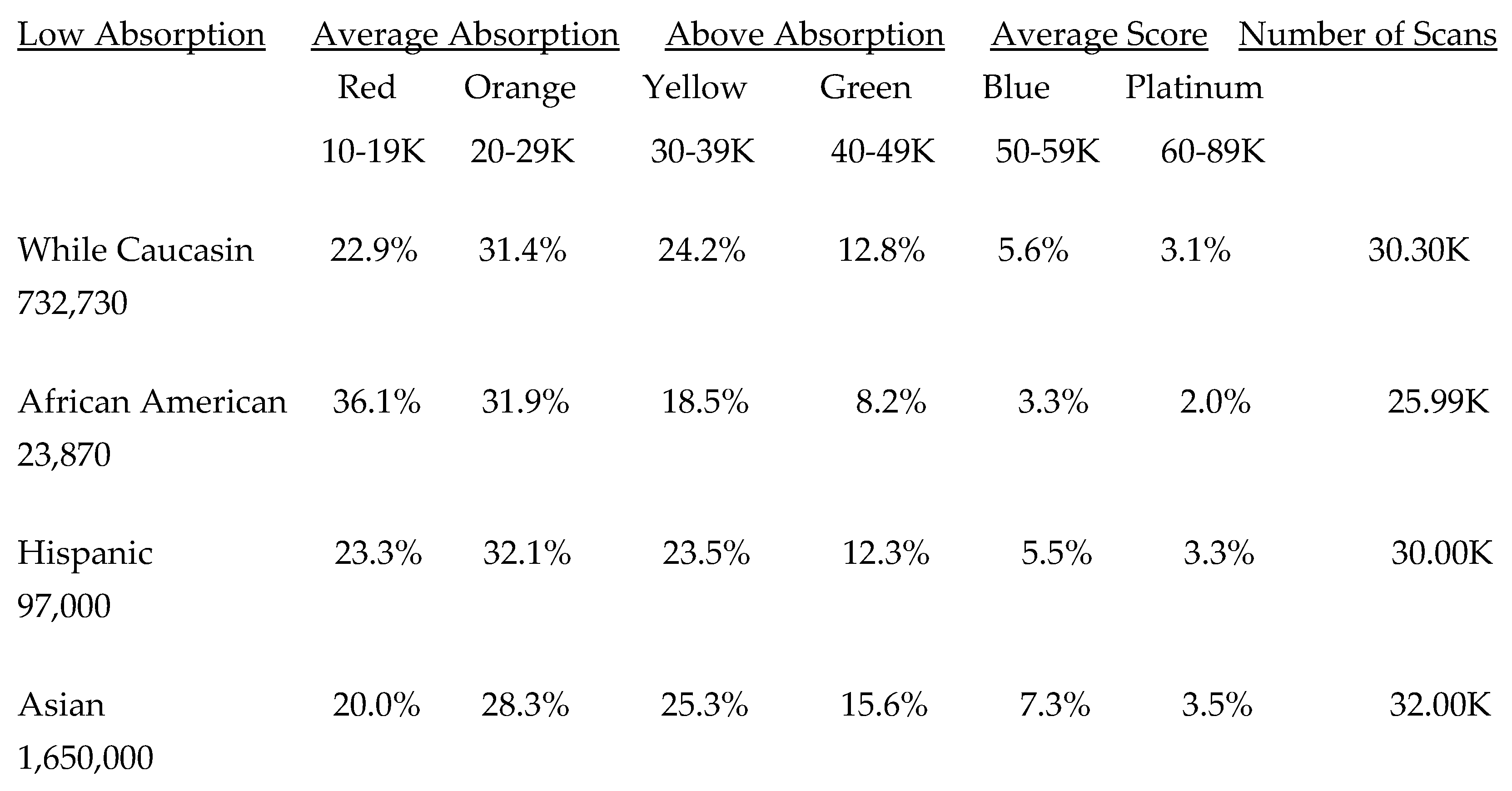
Low Absorption = Low Carotenoid Absorption into Tissue; Average Absorption = Average Carotenoid Absorption into Tissue and Above Asborption = Above Carotenoid Absorption into Tissue. The percentages displayed above fall within a specific range under the color-coded absorption labels. RIU = Raman Intensity Units.
Table 3.
Global Ranking of the Average Skin Carotenoid Scores in Different Countries/Regions and During the Pandemic.
Table 3.
Global Ranking of the Average Skin Carotenoid Scores in Different Countries/Regions and During the Pandemic.
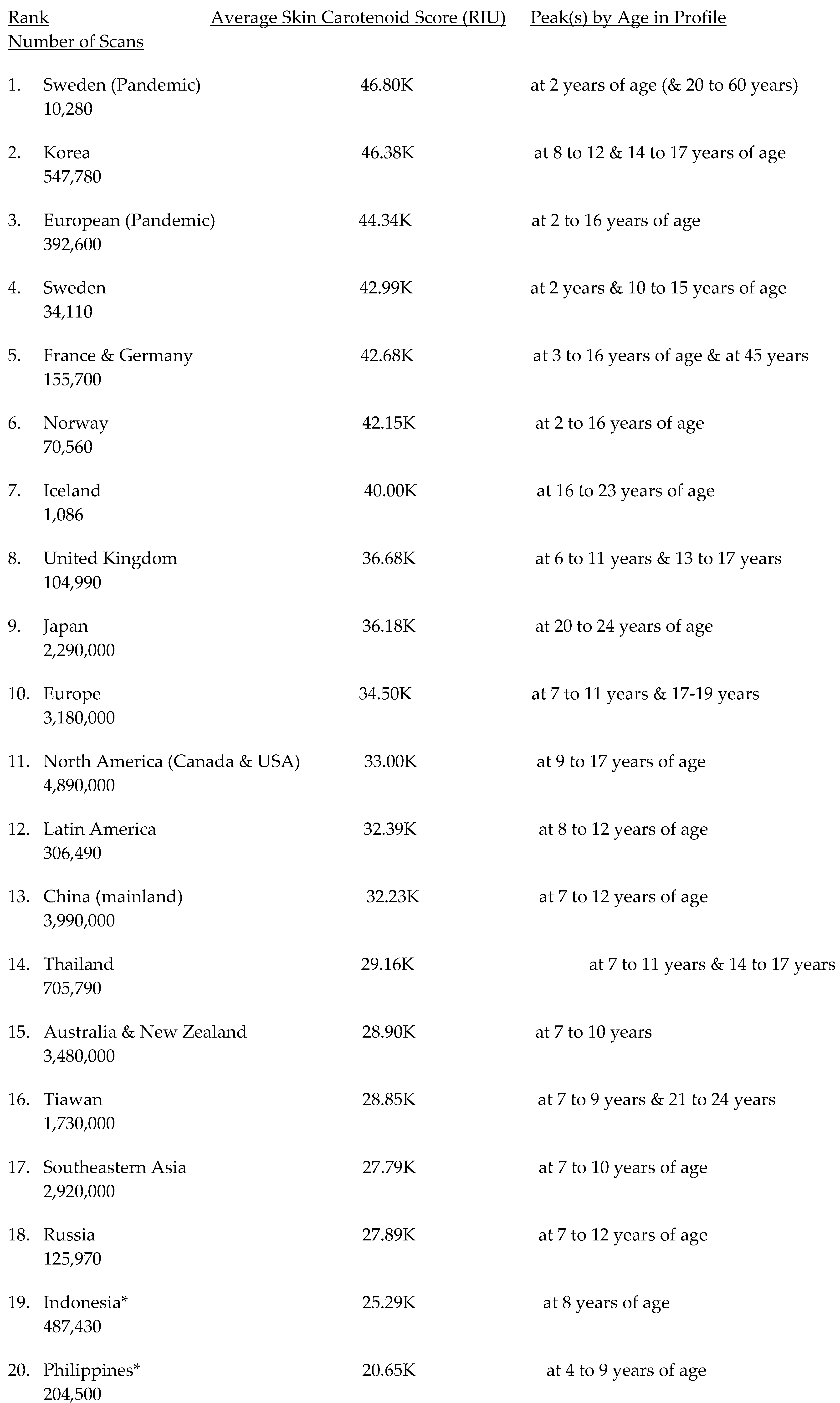
USA = United States of America. The average skin carotenoid scores correspond to the range of values for pigment absorption. For example, 10-19K RIU and 20-29K RIU indicate low absorption of cartenoids into tissues; 30-39K RIU and 40-49K RIU indicated average absorption into tissues; and 50-59K RIU and 60-89K RIU indicate above average absorption of carotenoids into tissues. * indicates for the age distribution for Indonesia and the Philippines in individuals 25 to 40 years old displayed particularly low skin carotenoid levels and the risk of carotenoid deficiency may be high. RIU = Raman Intensity Units.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



