Submitted:
03 July 2025
Posted:
04 July 2025
You are already at the latest version
Abstract
Virtual Reality (VR) is a useful educational tool in healthcare, allowing students to practise and improve practical skills. In speech and language therapy (SLT), the need to revise academic curricula to adapt them to university contexts and integrate them with advanced clinical practices, has highlighted the need to analyse the use of VR in this sector. The objective of this scoping review was to investigate whether research has considered using VR to support SLT students' training and highlight potential gaps in the literature. The study followed the JBI methodology for scoping reviews and was reported according to PRISMA-ScR guidelines. In May 2025, databases in healthcare, computer science, and education were searched, along with other sources. No constraints were applied and all study types were considered. Fourteen studies were included in the review and analysed under four core subjects: VR technology, SLT context, training purposes and main outcomes and assessment methods. VR is still in its early stages in SLT education. While simulation is becoming more common, most VR tools are non-immersive or semi-immersive, with few fully immersive ones. Some recent studies suggest VR supports students' communication, interdisciplinary and clinical skills. Overall, VR is well accepted and supports experiential and skills-based learning.
Keywords:
Virtual Reality
; VR
; Speech Therapy
; Speech and Language Therapy Training
; Speech and Language Pathology Training
; SLP
; Students
; Clinical practices
; Practical skills
; Clinical skills
1. Introduction
1.1. Background
In recent decades, the world’s demographic structure has undergone significant changes, characterised by population growth and progressive ageing [1]. Ageing represents a new challenge as patients’ clinical situations become more complex. Most countries worldwide are experiencing a shortage of health workers, which is expected to worsen in future [2,3,4]. Therefore, innovative care procedures and highly qualified healthcare professionals are needed to meet patient needs.
In addition, the professional political conditions of the health professionals is undergoing a significant transformation, promoting the transition from a vocational training model to a university-level education, focusing on scientific knowledge, research, and evidence-based practice. This change in education is driven by the necessity to enhance professionalism of practitioners and improve the quality of care, contributing to enhanced patient outcomes and ensuring alignment with international standards in healthcare education and practice [4,5]. These needs lead to the rethinking of the academic curricula of health professionals to meet the educational requirements of the university system, while ensuring the acquisition of the practical and clinical skills.
Traditionally, practical skills are acquired during training through direct experience in the field, working alongside professionals and performing therapeutic activities on real patients under supervision. However, direct “hands-on” learning has both ethical and organisational limitations, especially when it comes to inexperienced students.
To address these critical issues, the World Health Organisation has recommended the use of reality simulation-based tools [3], recognising the pedagogical value of safe and controlled environments in which students can practise without the risk of accidentally harming patients. Several studies have highlighted the efficacy of simulation-based education compared to traditional learning methods [6] and demonstrated how integrating advanced technologies with traditional learning approaches enhances the acquisition of skills and the training of healthcare professionals [7,8]. Furthermore, the advent of the COVD-19 pandemic made it necessary to develop new distance learning techniques, both to protect patients and students, and to continue to provide students with adequate and comprehensive training. This has fostered the development of simulation-based technologies, such as virtual reality (VR), in healthcare education and training.
1.1.1. Training in Speech Therapy
As every healthcare field, speech therapy (ST), also known as speech-language pathology (SLP), is facing the problems previously described. In recent years, the ageing of the population and increasing number of people who have experienced serious health problems, e.g. brain strokes, head and neck cancer, progressive neurologic diseases [9], have led to a significant increase in the number of patients suffering from communication (i.e. apraxia) and swallowing (i.e. dysphagia) disorders.
Recent advancements in the speech therapy field, both from the educational and technical point of view, are resulting in significant improvements in treatment outcomes. In fact, in addition to the shifting from the vocational to the university education, the introduction of techniques previously handled by other professionals into the training of speech therapists, such as Flexible Endoscopic Evaluation of Swallowing (FEES), highlights the need for an update of the academic curricula. Moreover, the arise of new techniques as the transcranial Direct Current Stimulation (tDCS) and the necessity of practicing complex procedures as Tracheostomy Tube Management, also known as Tracheal Cannula Management (TTM and TCM, respectively), provide the opportunity to reshape the speech therapy curricula.
Moreover, belonging to the healthcare sector, ST also requires students to achieve a certain amount of hours in order to obtain their professional certificate. As a matter of example, in Germany, 1900 hours of clinical practice are required, according to LogAPrO, 1980 [10], while in the USA, students are required to complete 375 hours of direct clinical placements with patients in order to be certified to practise [11]. In order to provide students with the necessary amount of clinical practice, to reduce the workload of clinical placements settings and to address the shortage of licensed clinical educators, some national entities have started recommending the introduction of simulation-based training in speech and language therapy programmes. Indeed, since January 2023, ASHA allows students enrolled in the graduate program to gain up to 75 direct contact hours through clinical simulation [12]. In Australia, initial efforts to integrate simulation-based learning into speech pathology courses can be found in the project led by Dr. A. Hill, within which a Simulation-based Learning Program was developed between 2014 and 2018 [13].
Clinical simulations comprehend several kinds of situations aiming at representing the reality to let students deal with real-life contexts. Clinical simulations can be categorised into “levels according to how closely the simulation replicates the real-world
experience in terms of physical, environmental and psychological elements” [14](p.6). The Council of Academic Programs in Communication Sciences and Disorders (CAPCSD) has identified five categories of healthcare simulation, ranging in levels of fidelity: standardized patients, task trainers, manikins, computer-based (gaming), and immersive virtual reality [14].
The current scoping review aims at mapping the use of VR (non-immersive, semi-immersive and immersive), hence, among the simulation types individuated by CAPCSD, here only computer-based simulations and immersive virtual reality-based tools are considered relevant.
1.1.2. Virtual Reality-based Simulation
Among the categories of simulation identified by the CAPCSD, the authors of the current review decided to focus on both VR and computer-based kinds of simulations. Since the title of the review refers to VR, the choice of considering the first category may appear obvious. In contrast, the decision to include computer-based systems may seem less intuitive. However, this choice is justified by the broad definition of virtual reality, which encompassess several kinds of systems from the least immersive ones to the most immersive ones.
VR can be categorized according to several factors such as immersion, presence and interactivity. In the current review, VR was categorised according to the level of immersion the technology was able to provide. Indeed, VR can provide different degrees of immersion which is the capacity of the technology of “delivering inclusive, extensive, surrounding and vivid illusion of reality to the senses of a human participant”[15](p.3).
For this paper, VR has been divided into three macro categories: immersive VR, semi-immersive VR and non-immersive VR. In this context, we refer to immersive VR when the technology is able to “surround”, i.e. through the use of head-mounted displays (HMDs) or CAVE systems [15]. On the contrary, we categorized as “non immersive VR” the desktop-based systems, which can be interacted through the use of mouse and keyboard, such as Virtual Patients. Systems that implement intermediate shades of immersiveness will be categorized as semi-immersive VR, these may include the use of larger screens to provide the user with a higher sense of presence.
Given this explanation, taking into account computer-based tools too aligns with the current conceptual framework of VR and ensures a comprehensive mapping of its applications in speech therapy education.
Virtual reality has been demonstrated to offer immersive, interactive learning environments that promote the acquisition of theoretical knowledge while increasing student engagement and motivation [16]. By simulating a wide range of clinical scenarios, including rare or complex cases, VR allows students to develop and refine practical skills through unlimited, self-paced repetition in a controlled setting [8]. This flexibility fosters expertise acquisition without the ethical or logistical challenges associated with treating real patients, thereby reducing stress and enhancing students’ confidence and awareness [6].
1.2. Rationale
Some studies investigated the use of VR systems in the context of medical education and clinical care [17] or in the field of communication disabilities [18] but none focused on the evaluation of these systems specifically for speech therapists’ skills training of clinical procedures. Considering the current orientation towards the simulation-based clinical training in ST, as well as the numerous studies and projects successfully developed using different simulation tools [19,20,21], the integration of virtual reality into speech pathology training programmes seems to be a promising strategy to improve clinical preparedness and support the development of essential professional skills. In the absence of dedicated reviews on this topic, in order to support the above assertion, our research team decided to conduct a scoping review to understand and analyse in a clear and structured manner whether and how virtual reality has already been considered as an educational and training tool for speech therapy students.
1.3. Objectives
The objective of this scoping review is to investigate whether extant research has considered the use of Virtual Reality as a tool to support the training of speech therapy and language pathology students to improve their practical skills and prepare them to perform clinical procedures. The aim of this study is to provide a comprehensive mapping of the integration of this technology within the domain of speech therapy, with a view to highlighting potential gaps in the current literature. In order to achieve these objectives, the following research questions guided the scoping review:
- How is virtual reality being used in the education and clinical training of speech-language pathology students?
- What are the educational, technological, and methodological characteristics of VR-based interventions in speech-language pathology training?
- What outcomes and benefits are reported in the literature regarding the use of VR in the training of speech-language pathology students? How are these assessed?
2. Materials and Methods
This scoping review was conducted in accordance with the Joanna Briggs Institute Manual for Evidence Synthesis’s Methodology for Scoping Reviews [22] and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping reviews (PRISMA-ScR) guidelines [23].
2.1. Protocol and Registration
A preliminary search of PubMed, PubMed Central, ScienceDirect, EBSCOHost, the Cochrane Database of Systematic Reviews, PROSPERO and JBI Evidence Synthesis was conducted and no protocol addressing our subject of interest was identified. Therefore, our team developed a protocol that was followed to conduct the review, which has not been published but is available in Appendix A.
2.2. Eligibility Criteria
In order to perform a comprehensive literature search, the eligibility criteria were kept as broad as possible. Indeed, the search was not constrained by temporal or linguistic limitations. The opportunity for such freedom was determined by two factors. Firstly, the novelty of the topic under consideration, as virtual reality is a relatively recent technology that naturally limits the search over time. Secondly, the resources available nowadays, such as online translators and artificial intelligence aided tools, enable the possibility to consult and include sources in a wide range of languages. Additionally, sources in any publication status were considered and no restrictions regarding the study design were applied to provide a reliable map of the available literature. To provide a complete overview of the sources, the typology of study has been made available within the results of this study.
The records retrieved from the search were considered as eligible for the inclusion in the current review if they met all the following criteria:
- The study was targeted to students or trainees in speech therapy and language pathology field;
- The study involved the use of virtual reality (including immersive, semi-immersive, and non-immersive formats) or, it assessed or evaluated the use of the VR technology;
- The purpose was the education and/or training of students.
2.3. Information Sources
A comprehensive search of the relevant literature was conducted, covering a range of sources including specialised databases, archives, registers, grey literature websites and artificial intelligence (AI)-driven platforms.
The interdisciplinary nature of the topic under consideration necessitated the consideration of specific databases from the healthcare field, addressing the speech therapy sector; the computer science field, addressing virtual reality technology; and the educational sector. The following academic databases and research engines were queried: ACM Digital Library, Cochrane Library, EBSCOhost, IEEE Xplore, PubMed, PubMed Central, ScienceDirect, SpeechBite and Wiley. The PROSPERO register was interrogated to identify ongoing studies and minimise bias risks of our search.
In addition to structured database searches, Google Scholar was consulted to identify grey literature and the AI research assistant Elicit [24] was used to find further records. We also performed snowballing by manually screening the reference lists of the included articles and reviewing related studies suggested by search engines and online platforms (e.g. Google Scholar, PubMed, etc…), which appeared as “related articles” or algorithm-based recommendations. These were screened manually for relevance and inclusion criteria.
A preliminary search was initiated at the beginning of April 2025, followed by the main investigation in May 2025, which was concluded on 20 May 2025. During this period, information sources were consulted repeatedly in order to refine the search strategies and adapt them to each research system, while maintaining consistency with the guiding research questions.
2.4. Search
A preliminary exploratory search was carried out before the final search. This process allowed the team to identify relevant terminology and try out different keyword combinations among the previously listed databases. The final keywords, listed in Table 1, were chosen based on insights gained during this preliminary phase. In order to avoid the potential loss of pertinent terminology, word roots were employed to encompass their potential variations wherever applicable. As a matter of example, the word “student*” was searched to include publications containing both the terms “student” and “students”.
During the search, keywords were combined using Boolean operators, and the search symbols specified by each database’s interface were employed. Where feasible, the keyword search was conducted by applying filters to restrict the search to the fields of title, abstract and keywords. The complete search strategy used for each database is provided in Appendix B.
2.4.1. Exceptions
Although the search strategy illustrated above was applied to most of the information resources, with the appropriate minor modifications, it was necessary to make more substantial modifications to the search strategy for some source of information. The current paragraph offers an overview of the strategies employed for the exceptions previously mentioned.
The SpeechBite database search strategy differed from the others due to the keywords utilised. Indeed, given the database’s specialisation in the domain of speech therapy, it was unnecessary to specify the target population. In addition, the context-related keywords “VR” and “virtual reality” were selected for the site’s advanced search system, which requires the use of one or two keywords.
The Science Direct database search procedure slightly differed from the others. Indeed, the search was performed three times via three distinct queries, owing to the search engine’s capacity constraints regarding the utilisation of no more than eight logical operators in a single query.
The search across Google Scholar was conducted in a slightly different way. Firstly, it is important to note that on Google Scholar, keywords entered can only be searched for in the titles of the records or anywhere in their text. After some initial trials, it was determined that restricting the keyword search to the title would have been too restrictive, as only a few records appeared. Consequently, it was decided to search for keywords across the entire text. However, this resulted in the query providing too many results, so to reduce the number of records resulting from the search, some terms were excluded from the search process. The platform was requested to remove records containing the following terms: “child”, “children”, “deaf”, “autism” and “rehabilitation”. These terms were selected because they frequently occurred in the titles of studies identified by Google Scholar that were not relevant to the present study. The elimination of these terms resulted in a substantial reduction in the number of results obtained. Nevertheless, the number of articles was still significant, so a manual selection process was implemented based only on the relevance of the titles. The searching process for Google Scholar is provided in Appendix C.
The research on Elicit followed a completely different process to previous studies. In fact, Elicit is not a traditional database, but rather an artificial intelligence-based platform designed to support the writing of scientific reviews. Its main functionalities include the ability to identify relevant studies based on research questions, facilitating the identification, synthesis and organisation of evidence in a targeted and efficient manner. The search questions reported above were therefore entered into Elicit, which was asked to find studies that could help address them. The search on Elicit was performed three times and 500 studies were found each time. For each iteration, artificial intelligence was used to screen the articles in detail, categorising them according to the target population, context and concept (see Table 1), and to detect the most relevant records. The three searches returned 12, 16 and 31 records, respectively. These resulting records were subsequently manually subjected to the evidence selection according to the process described in section 2.5.
2.5. Selection of Sources of Evidence
All the records resulting from the search were imported into Zotero to identify and remove duplicates. Once the duplicates had been removed, a two-step screening process was initiated. Firstly, a title and abstract screening was conducted, followed by a full-text screening, in order to identify the studies to consider for the review.
The title and abstract screening was performed by two independent reviewers, one specialised in the speech and language pathology sector (EH) and one specialised in the computer science field (FG). In case the reviewers both agreed that an article met the eligibility criteria, it was included and progressed to the next step of the review. Conversely, if both agreed that the article did not meet the criteria, it was excluded from the study. In cases of disagreement between the two reviewers regarding an article’s eligibility or, in the event that the initial title and abstract screening did not clearly indicate whether all three inclusion criteria were met, the study was deemed eligible for full-text screening as well.
The records considered eligible for the full-text screening process underwent independent review by three reviewers. As part of the full-text screening process, one researcher (FG) reviewed all of the studies to ensure consistency. Two additional reviewers, an expert of the speech therapy field (MW) and one expert of the computer science field (WM), each independently screened half of the total studies. During the second phase, the full-text screening, each article was read in its entirety in order to verify whether it met all the eligibility criteria for inclusion in the review. In cases where there were divergent opinions regarding the inclusion of the study in the review, a discussion was held. If no solution was found, the third reviewer was consulted. After this stage, the articles considered relevant to the research objectives were included in the study categorized according to predefined thematic and methodological criteria.
2.6. Data Charting Process
Relevant data were extracted from each record during the full-text screening process. Each reviewer (MW, WM and FG) independently took notes on the points of interest of each study, which FG then summarised in an Excel file. The data extraction template can be found in Appendix D.
2.7. Data Items
The extracted data included the title, author(s), publication year, country, language, study type (i.e. design), VR type (i.e. non-immersive, semi-immersive or immersive), VR characteristics (tool used for the VR implementation), the population addressed by the study (e.g. Bachelor’s or Master’s students specialising in speech and language pathology and eventual sub-field), the educational and/or training purpose (e.g. enhancement of communication skills, development of interviewing capacity, etc…), and the main results and findings of the study with the evaluation method used (i.e. direct assessment, interviews or trial-based perspectives).
2.8. Critical Appraisal of Individual Sources of Evidence
As this was a scoping review conducted in order to map the literature on our topic as comprehensively as possible, a critical appraisal of individual sources of evidence included was not conducted.
2.9. Synthesis of Results
The extracted data from the records were synthesised during the data charting process (paragraph 2.6) and are reported here through descriptive and thematic analyses. Where applicable, data are presented in tables, diagrams and flowcharts and accompanied by a narrative description to provide a comprehensive overview of the results.
3. Results
3.1. Selection of Sources of Evidence
The identification, screening and inclusion processes are shown in Figure 1. The database search produced a total of 174 records. Of these, 79 were retrieved through databases and registers, while the remaining 95 were found via other methods, such as grey literature (36) and AI-aided tools (59). After removing duplicates (57), 117 records underwent title and abstract screening. Of these, 75 were deemed ineligible for full-text screening. The remaining 42 were screened in full by the reviewers. In parallel, whenever a related article was suggested or an interesting citation was identified (through snowballing), the article was also screened in terms of its title and abstract. If it was eligible for full-text screening, it was read in full. Twenty-six records were identified in this way and fully reviewed. Therefore, a total of 68 records underwent full-text screening by the reviewers. The reviewers reached a consensus on the eligibility of the articles in the majority of the cases, with a total of four articles resulting in divergent opinions. A consensus was reached by the reviewers regarding the inclusion or exclusion of the record for these four articles. In the course of the study, three of these were included, while one was excluded. Of the 68 records reviewed, 42 were defined as ineligible for the review, 12 were not retrieved and 14 were deemed appropriate for the review and were included and analysed.
3.2. Characteristics of Sources of Evidence
The included studies characteristics are summarized in Table 2.
The included studies were published between 2006 and 2025, and were primarily conducted in the USA (n = 7, 50%) and Australia (n = 3, 21,4%). Despite being published in different countries, including non-English-speaking countries, all the included articles are in English (n = 14, 100%). Figure 2 shows the geographical distribution of the included studies.
Overall, a positive trend has been observed in the utilisation of VR in the domain of speech therapy training in recent years. Figure 3 shows the number of articles published per year and country of the authors’ institutions.
The typology of records included is broad. The included records are predominantly constituted of mixed-methods studies (n = 4, 28,6%), descriptive studies (n = 4, 28,6%), and experimental studies (n = 4, 28,6%). A further series of studies was identified, including pilot studies (n = 2, 14,3%), qualitative studies (n = 2, 14,3%), randomised controlled trials (n = 2, 14,3%), observational studies (n = 1, 7,1%), and design-based studies (n = 1, 7,1%). It is worth highlighting that the total sum exceeds 14, as some of the articles implement more than one typology. Moreover, in consideration of the objective of the present research, which is to map the present state of the literature, the following sources were included: journal articles, peer-reviewed publications, poster presentations and master theses.
3.3. Critical Appraisal Within Sources of Evidence
A critical appraisal of the sources of evidence was not performed.
3.4. Results of Individual Sources of Evidence
A range of outcomes has been reported in studies examining the use of VR in speech therapy training. The studies included in this analysis are consistent with the established criteria for the search, and each of them combines the three key focus points (virtual reality, population and training purposes) in a different way. The subsequent table (Table 3) provides a concise overview of the primary conclusions derived from each record that was covered in the review.
3.5. Synthesis of Results
On the basis of the purpose of our scoping review, the findings have been analysed under four major cores: (1) VR type and characteristics, (2) population, (3) training purposes (and sub-field of application), and (4) main outcomes and assessment methods.
3.5.1. Virtual Reality - Type and Characteristics
As outlined in the eligibility criteria that were applied in the selection of studies for inclusion, the focus was exclusively on studies that incorporated VR as a technological element. In the current review, VR was categorised according to the level of immersion the technology was able to provide. Indeed, VR can provide different degrees of immersion which is the capacity of the technology of “delivering inclusive, extensive, surrounding and vivid illusion of reality to the senses of a human participant”[15](p.3).
For this paper, VR has been divided into three macro categories: immersive VR, semi-immersive VR and non-immersive VR. In this context, we refer to immersive VR when the technology is able to “surround”, i.e. through the use of head-mounted displays (HMDs) or CAVE systems [15]. On the contrary, we categorized as “non immersive VR” the desktop-based systems, which can be interacted through the use of mouse and keyboard, such as Virtual Patients. Systems that implement intermediate shades of immersiveness will be categorized as semi-immersive VR, these may include the use of larger screens to provide the user with a higher sense of presence.
The simple categorization “VR” has been used to identify the studies in which the kind of virtual reality used was not specified. From now on, VR references will target the general use of VR, unless it is specified otherwise.
Some of the included studies also take into account or evaluate other technologies such as AR or MR that are not outlined here. Figure 4 and Figure 5 represent the VR types of the included studies and their characteristics, respectively.
In the included studies, 6 (42.9%) [26,27,30,31,32,33] of them implemented a non-immersive VR simulation. The primary objective of these studies is to furnish SLP students with screen-based simulations and the opportunity to interact with virtual patients to foster conversation, train communication [27,29,33], interpersonal [27,29], interviewing [26,32] and reasoning [26] skills.
Immersive VR systems were analysed in 5 (35,7%) [25,28,35,36,37] studies. These systems aim to immerse the user into a realistic environment within which the user can move and interact with the objects with physical body movements, providing them with a high sense of presence.
As early as 2006, the Virtual Immersion Center for Simulation Research (VICSR) expressed itself on the potential of providing computerised training in a safe, controlled, learner-centred environment for the field of speech language pathology that could promote transfer of skills into real world settings [25]. Indeed, the VICSR aimed at developing an immersive virtual reality CAVE able to provide speech pathology students with a simulation environment to practice real life scenarios.
Later on, other studies investigated the use of a more recent technology, i.e. Head Mounted Display (HMD). In 2018, Moradi et al. [28] investigated the use of a system composed of 3D glasses with an additional monitor and a pair of gloves while others proposed to use the Oculus Quest 1 [36] and the Meta Quest 3 [37].
The study conducted by Towson et al. [29] was classified as semi-immersive since it involves the use of a real-time mixed reality simulator, TechLivE, as well as a “large television screen, which features a virtual conference room and one adult avatar. There is a desk and chair in front of the screen in which the participant sits, with additional chairs around the perimeter of the room for observers.” [29](p.5).
3.5.2. Population
As outlined in the eligibility criteria that were applied in the selection of studies for inclusion, the focus was exclusively on studies that were targeting the population of speech and language pathology students. The selected studies involved students from both the graduate and undergraduate courses, who were enrolled in different academic years. Figure 6 represents the target population of the included studies.
All studies considered have speech therapy students as their target population. The target population is characterised by homogeneity with regard to undergraduate and graduate students. Rondon-Melo & Andrade [31] concentrate their study on hearing sciences students, given that Speech-Language and Hearing Sciences (SLHS) students are enrolled in a unique course. In addition to conducting these studies to verify the effectiveness of VR in academic curricula, some researchers have addressed their search to clinical educators to assess their point of view regarding this innovation [27]. Xonbabayeva Madinabonu Asqarjon kizi also conducted a structured survey among both SLP and educators to assess the use and effectiveness of ICT in the SLP training programs [38]. Finally, the study conducted by Williams [25] also presents its technology as a valid tool for training patients with communication disorders, as well as a positive educational tool for training students.
3.5.3. Training Purposes (and Sub-Fields of Application)
As outlined in the eligibility criteria that were applied in the selection of studies for inclusion, the focus was exclusively on studies that aimed at providing or enhancing SLP students’ skills. Five main kinds of skills emerged: (1) communication and interpersonal collaborative skills, (2) clinical interviewing or reasoning skills, (3) performance knowledge, (4) clinical skills and (5) person-centered care intervention and awareness. Figure 7 illustrates the training purposes of the included studies.
Among the included studies, 3 (21,4%) [27,29,33] addressed the communication and interpersonal collaborative skills training being a core capacity for speech therapists. Indeed, communication is fundamental to understand patients’ necessities and to exchange information with different stakeholders, i.e. patients’ families and other clinicians. Two studies (14,3%) [26,32], focused on clinical interviewing or clinical reasoning processes aimed at enhancing students’ capacity of investigating and diagnosing the correct disease and to find the correct therapy to treat the patient.
Other two studies (14,3%) faced the thematic of the performance knowledge [30,31]. In 2019, Carter et al. [30] utilised the non-immersive SimuCase platform to facilitate students in practising with virtual patients, with the objective of enhancing their performance in the domain of paediatric language disorders. In the same year, Rondon-Melo et al. [31] conducted an experiment comparing the level of knowledge students gained from three different educational methods on the subject of the anatomy and physiology of the orofacial myofunctional system.
Two studies (14,3%) highlight the importance for students to understand the importance of delivering person-centered care to patients [34,35]. Blaydes et al. and Deman et al., independently, describe in their studies how letting students feel what patients do experience in everyday life is helpful to foster empathy and, therefore, being more focused on delivering a patient-centered care therapy and cure.
A total of five studies (35,7%) focused on training and enhancing the clinical skills of students [25,28,36,37,38]. These studies aimed at using VR as a tool to train speech-therapy specific procedures whose knowledge is fundamental but which are difficult to train prior to clinical placements. Already in 2006, thought about providing a simulated environment (i.e. CAVE) to students to let them train clinical procedures related to communication diseases [25]. Later, in 2018, Moradi et al. [28] described an immersive VR-based technology to let students train with oral organs assessment. In 2023, Kelly at al. [36] described the positive perspectives of SLP students regarding training Oral Musculature Assessment (OMA) through the use of the Oculus Quest 1. The most recent studies, conducted in 2025, also propose the training of practical skills [38] and of specific speech therapy clinical skills related to complex techniques such as TTM, FEES and tDCS [37].
The majority of the included studies, in addition to focusing on the type of skill to be trained, consider a particular clinical practice and/or clinical condition as an example. The following subfields emerge from the analysis of the extant studies: dysphagia, dementia, OMA, communication disorders, FEES, TTM, tDCS, oral organs assessment, stuttering-related anxiety and stuttering.
3.5.4. Main Outcomes and Assessment Methods
The included studies reported a range of outcomes related to the effectiveness of VR-based training in the field of speech therapy. These outcomes were assessed in different ways, based on the necessities of each study.
Overall, the studies reported positive results both in terms of soft skills and hard skills. In line with the prediction that Williams made in 2006 in his study, VR systems foster the increase of competencies [25,26,27,33,38] and skills transfer [25]. Different studies assessed the acquisition and enhancement of skills [30,38] and, therefore, enhancements in the performance [28,29]. Additionally, also improvements in reasoning, empathy [26,34] and confidence [27,38]. Deman et al. [35], stated that students reported fear and physiological fear due to the aim of the VR experience to let users feel the anxiety usually proven by people who stutter.
The VR is generally well accepted and considered as a valid tool to simulate real-life situations that are difficult to face and to train with before clinical placements. Indeed, the included studies report high acceptability [29], positive reaction of students’ intrinsic and extrinsic value for the training experience [36] and positive feedback [26].
The studies used both qualitative and quantitative evaluation methods to evaluate the VR under several aspects in the context of ST training. Some authors preferred to evaluate their systems using standard questionnaires and/or standardized minimum requirements scales, some examples are: International Classification of Functioning Disability and Health (ICF) [32] Situation - Background - Assessment - Recommendation - Communication (SBAR-C) [29]; Communication Competence in Interpersonal Settings (CCIS) and Patient Relationship Questionnaire (PRQ) [33]; usability, presence, acceptance, user experience questionnaires [37]; Standardized Clinical Skills Inventory (SCSI) and Critical Thinking in Clinical Skill Development (CTCSD) [30]. Additionally, qualitative interviews to SLP students and educators were carried on to record their considerations regarding the use of VR in ST training [26,27,32,36,38].
4. Discussion
4.1. Summary of Evidence
The number of records found that regard the use of VR in SLP training is limited, with only fourteen studies retrieved during the review process. As stated in several studies [18,28,36], there is a lack of search for simulation-based systems for SLP students, and this is clearly reflected in the VR context too. This paucity of records suggests that the topic is still in its infancy, with VR-based systems representing a new potential subject of search within speech therapy.
In speech therapy education and training, the use of simulation has increased significantly over time, with numerous studies evaluating its effectiveness in enhancing students’ learning outcomes and clinical readiness [28,29,30,33,34,39]. Despite the absence of constraints in the current review, the included studies span a period of almost 20 years, with only one study published in 2006 and the others in the last nine years. This trend may suggest that, already in 2006, the potential of this technology was emerging but only in the last few years, the wide range of applications that VR has and the positive outcomes reported in education and training contexts, caught the attention of the SLP field. Indeed, this field has been undergoing significant changes in terms of university curricula, reflecting the evolving demands of clinical practice and the integration of simulation-based educational technologies.
During the screening process conducted for this review, various forms of simulation were identified, including the use of mannequins, virtual learning environments (VLEs), standardized patients, role-playing activities, and computer-based scenarios. However, the studies specifically focusing on VR are few. Although the limited number of studies, our team identified some common features and emerging patterns across the included research.
Analysing the data, it emerges that, in most cases, non-immersive and semi-immersive VR are primarily employed to train communication, interpersonal and collaborative skills while immersive VR is used to develop practical and clinical skills. Moreover, while the purpose of training the first kind of systems is more homogeneous, the skills that immersive VR applications aim to train are practical and procedure-specific.
On the one hand, the first kind of systems often feature virtual patients or avatars that simulate realistic clinical scenarios, allowing users to engage in interview-based interactions (mainly chat-based) and practice clinical reasoning in a structured yet flexible and controlled environment. These have resulted in being effective for students in practicing dialogues with patients while investigating the diagnosis and reasoning on the following steps to perform. In addition to the enhancement of these soft skills, VR turned out to be a useful tool to improve awareness with regard to patients’ clinical situations and foster empathy towards them, allowing for a more dedicated approach. the patient’s conditions.
On the other hand, immersive VR systems have been investigated for training procedures that usually require a direct hands-on approach toward the patient. Except for the cave-based immersive system [25], which provides an environment where to practice communicative skills, and the system described by Deman [35], which aims at letting the users experience stuttering-related social anxiety, the other three studies describe systems focusing on very specific and different topics. Indeed, these tools provide specific scenarios to gain practical experience in specific clinical procedures, i.e. oral functional assessment [28], FEES, TTM and tDCS [37], and OMA [36]. It is worth to note that only Moradi and colleagues [28] managed to assess the effectiveness of the system, registering an increase of student’s score through independent-T test while Kelly et al. [36] qualitatively assessed the perspectives of VR-OMA across ST students. The project carried on by Gentile et al. [37] is still in its prototype phase and has not been tested yet. To the best of authors’ knowledge, these observations led to the thought that recent technologies effectiveness, i.e. Oculus Quest 1 and Meta Quest 3, have not been tested yet in ST training contexts therefore highlighting a gap in the literature. Given Moradi’s opinion assessing that “Virtual Reality technology results in increase in attention, concentration, and motivation” and that “Virtual Reality structure is so flexible in training and lets the students know this technology in different situations and sometimes new situations to choose, each one can be a type of learning.” [28](p. 89), the authors of this review believe that it is worth investigating this sector.
Additionally, SLP related studies [41,42], which were not included in the review due to inclusion and exclusion criteria restrictions, highlight the effectiveness of VR training systems for professionals and providers. This may suggest that the inclusion of such tools into the SLP student’s training could have positive effects on future speech therapists, if adequately adapted to educational contexts.
Future search may investigate the outcomes derived from the use of immersive, new and cutting-edge VR training systems in ST training and define a framework for the development of specific scenarios to train with.
Additional Considerations
The included studies were conducted in various countries, with a particularly high concentration in the USA and Australia. A deeper insight of the data reveals a rise in interest in the use of VR for ST education and training, with a significant increase observed beginning in 2016 for the USA and in 2018 for Australia. This increase may be associated with institutional support and guidance provided by national associations such as ASHA in the USA and SPA in Australia. Indeed, both ASHA and SPA have actively supported the integration of simulation-based training in ST curricula. In the USA, up to 75 hours of mandatory practicum can be delivered through simulation based systems while, in Australia, an inter-university research was carried out to develop simulation-integrated curricula. These suggestions and recommendations at national level probably fostered the interest of universities in conducting research in this direction.
In Europe, research in this area remains limited, which may be due to the decentralized nature of professional regulation and the absence of guidelines from a pan-European body such as the European Speech and Language Therapy Association (ESLA). To the best of the authors’ knowledge, there are no specific guidelines or recommendations for simulation-based learning in the field of speech and language therapy. Within the European context, the authors are aware of more general recommendations, such as the “SimNAT Pflege Leitlinie Simulation als Lehr-Lernmethode.”
4.2. Limitations
Although the intention was to make this review a faithful representation of the current literature by conducting unrestricted research, the authors acknowledge its limitations.
Firstly, some potentially relevant articles may not have been identified due to limited academic access to certain databases and subscription-based journals, which could have affected the comprehensiveness of the review. Secondly, although Google Scholar was used as an additional information source, some relevant articles may not have been retrieved due to the constraints introduced in the query. Indeed, because of the large number of studies retrieved (15800) using the query used for other databases, some restrictions were imposed on the search. Some recurrent words referring to irrelevant topics such as “rehabilitation” were excluded from the search to reduce the number of records to be screened. Future studies in this context could broaden this search even more, including all the sources we weren’t able to access.
Additionally, during the keyword search, particularly the preliminary search, it was observed that the duties of speech therapists sometimes overlap with those of other healthcare professionals. Moreover, this overlap is difficult to delineate since speech therapy regulations differ from country to country. As a result, some speech therapy-related practices may have been developed and studied under other allied health disciplines, and thus may not have been identified using our search keywords. Future research could expand the scope to investigate the use of VR technology in the training of speech therapy allied professions or for speech-therapy specific procedures.
5. Conclusions
The importance of practice-based learning to promote the acquisition of skills, situated learning approach, and the potential of immersive virtual reality to support this learning paradigm have been known for more than two decades. Several reviews assessed the lack of VR systems for specific healthcare fields [40] and, more specifically in the field of speech therapy [34,43]. Indeed, only 14 studies were found relevant in the context of ST training through a VR-based tool. VR in speech therapy training is generally used to enhance communication competencies of ST students towards different stakeholders, improve their empathy and awareness regarding the importance of providing patient-centered care and foster the acquisition of clinical and practical skills. Most of the studies included focus on the effects of non-immersive VR while, regarding the use of immersive VR-based tools there are no concrete results yet, except from the positive perspectives of students regarding their integration into curricula [36] and the literature-based evidence provided by other healthcare fields [34]. Overall, the results reported by the included studies generally indicate the positive impact of VR in the domain of speech therapy training.
In conclusion, this scoping review provides a general overview of the utilisation of VR in the training context of speech therapy. Despite the paucity of literature in this field, a lack of studies and applications based on immersive virtual reality to train future speech therapists has been identified. This analysis has the potential to pave the way for future research and studies regarding the inclusion of immersive virtual reality in the domain of speech therapy training to facilitate the acquisition of practical skills for specific-oriented ST clinical procedures.
Author Contributions
Conceptualization, F.G., M.W. and W.M.; methodology, F.G., M.W. and W.M.; software, F.G.; data curation, F.G.; analysis, F.G., E.H., M.W.and W.M.; writing-original draft preparation, F.G.; writing-review and editing, F.G., M.W. and W.M.; visualisation, F.G.; supervision, M.W. and W.M.; funding acquisition, M.W. and W.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Pädagogische Hochschule Weingarten, Landesgraduiertenförderungsgesetz (LGFG) Grant and Starting Grant VRLogo.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
The author(s) would like to thank all those who contributed indirectly to the development of this work through inspiring discussions, critical thinking, or the broader academic environment.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| VR | Virtual Reality |
| ST | Speech Therapy |
| SLT | Speech and Language Therapy |
| SLP | Speech and Language Pathology |
| FEES | Flexible Endoscopic Evaluation of Swallowing |
| tDCS | Transcranial Direct Current Stimulation |
| TTM | Tracheostomy Tube Management |
| TCM | Tracheal Cannula Management |
| CFCC | Council for Clinical Certification in Audiology and Speech-Language Pathology |
| ASHA | American Speech-Language-Hearing Association |
| CAPCSD | Council of Academic Programs in Communication Sciences and Disorders |
| VICSR | Virtual Immersion Center for Simulation Research |
| HMD | Head Mounted Display |
| SLHS | Speech-Language and Hearing Sciences |
| OMA | Oral Musculature Assessment |
Appendix A
A.1. Title
Virtual Reality in Speech Therapy students’ Training: a Scoping Review Protocol
A.2. Abstract
Background: Virtual reality (VR) has been demonstrated to be a useful educational tool, particularly in healthcare, as it allows students to practise and improve their practical skills. In the field of speech therapy (ST), the necessity to revise academic curricula has been highlighted, both to adapt them to university contexts and to align them with international standards and recommendations. Furthermore, there is a need to integrate them with the most advanced clinical practices. In order to address these issues, it is worth analysing the use of VR in this field.
Objective: The objective of this paper is to provide a protocol to be used as a guideline to conduct a scoping review to investigate whether research has considered using VR to support speech and language therapy students’ training. The aim is to map the technology’s use within logopedics and highlight gaps in the literature.
Methods and analysis: The proposed scoping review will be conducted in accordance with the Joanna Briggs Institute’s methodology for conducting scoping reviews. The study will be reported in line with the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines. The data will be searched across databases and grey literature platforms; additional records will be identified through AI-aided tools and reviewed manually. The screening and analysis processes will be performed through the utilisation of forms and tables recommended by the PRISMA-ScR guidelines.
Ethics and dissemination: As this scoping review will involve analysis of publicly available data, ethical approval is not required. The findings of this review will be submitted for peer-reviewed publications and for presentation at relevant academic conferences.
Registration: The current protocol has not been published.
A.3. Keywords
Clinical procedures; practical skills; speech-language pathology; university curriculum; VR.
A.4. Introduction
A.4.1. Background
In recent decades, demographic shifts characterised by population growth and ageing have made clinical care more complex. At the same time, many countries are experiencing a shortage of healthcare workers (OECD, 2025; WHO, 2013; WHO, 2016). These trends highlight the need for innovative care models and well-trained professionals who are equipped to manage complex patient needs. Consequently, healthcare education is evolving from vocational training to university-level programmes that focus on scientific knowledge, research and evidence-based practice. This shift aims to enhance the professionalism of practitioners and care quality, and align healthcare education and practice at international level (Eurydice, 2024; WHO, 2016). Consequently, academic curricula are being redesigned to balance theoretical learning with hands-on clinical skills development. Traditionally, practical skills have been acquired through supervised clinical experience. However, this approach poses ethical and logistical challenges, particularly for beginners. Therefore, the WHO (2013) has promoted simulation-based learning as a valid support, offering a safe environment in which students can practise without endangering patients.
A.4.2. Rationale
As occurs in other healthcare fields, speech therapy is facing increasing demands due to population ageing and the rise in conditions such as stroke, head and neck cancer, and neurodegenerative diseases, resulting in a greater number of patients with communication and swallowing disorders (Christmas & Rogus-Pulia, 2019). Advancements in both education and technology are enhancing treatment outcomes and reshaping training needs. The transition to university-level education and the emergence of both established techniques and new procedures, such as Flexible Endoscopic Evaluation of Swallowing (FEES), transcranial Direct Current stimulation (tDCS) and Tracheostomy Tube Management (TTM), highlight the need to update academic curricula.
Considering the current orientation towards simulation-based healthcare education, the integration of virtual reality in speech therapy training programs could represent a valid strategy for promoting skill acquisition and enhancing clinical preparation. In fact, virtual reality represents a valuable educational tool, able to promote the learning of theoretical knowledge while fostering student engagement. It also supports the acquisition and refinement of practical skills by allowing learners to immerse themselves in varied clinical scenarios and repeat procedures without limitation. Moreover, VR enables training in realistic, simulated environments without ethical concerns, eliminating the risk of harming patients or over-stressing students.
A.4.3. Objectives
A preliminary search of PubMed, PubMed Central, ScienceDirect, EBSCOHost, the Cochrane Database of Systematic Reviews, PROSPERO and JBI Evidence Synthesis was conducted and just one review was identified that relatively addressed the subject of interest. In 2022, Nagdee and colleagues (Nagdee et al., 2022) conducted a scoping review with the aim of collecting information regarding the use of simulations as a mode of clinical training in healthcare professions (HCPs). The study found a gap in the evidence regarding the utility of simulation in the clinical training of speech-language pathology and audiology professions.
However, it should be considered that the research conducted by Nagdee and colleagues was more general in scope, covering health disciplines as a whole. In contrast, our scoping review focuses on the field of speech therapy and its clinical practices. In addition, our scoping review is conducted three years after the previous one, a sufficient timeframe for the development of new technologies and a change in the educational landscape of speech therapy.
Consequently, the objective of this paper is to provide a protocol to ease the process of conducting a scoping review to map the current literature and provide a comprehensive overview of the current state-of-the-art regarding the use of VR for the training of speech and language therapy students. The review also aims at identifying gaps in the existing literature and propose potential opportunities for future research.
A.5. Review Questions
The proposed scoping review’s objective is to explore and synthesize existing literature on the use of virtual reality in the education and training of speech and language therapy students. In accordance to this objective, the research question guiding the review was developed through the aid of the PCC mnemonic (i.e. Population, Concept, Context) recommended by the Joanna Briggs Institute Manual for Evidence Synthesis (Peters et al., 2020).
The review seeks to address the following research questions:
- How is virtual reality being used in the education and clinical training of speech-language pathology students?
- What are the educational, technological, and methodological characteristics of VR-based interventions in speech-language pathology training?
- What outcomes and benefits are reported in the literature regarding the use of VR in the training of speech-language pathology students? How are these assessed?
A.6. Inclusion criteria
As well as for the development of the research questions, the PCC mnemonic has also been utilised to identify the inclusion criteria and hence, to determine the exclusion ones.
A.6.1. Population
This scoping review will take into account studies referring to speech and language pathology students. Both university-level and vocational education students will be included. Since within their courses, students are required to achieve a certain amount of hands-on clinical practice and therefore, they have to attend a practicum, trainees, interns and apprentices will be also considered.
In accordance with the objectives of this scoping review, studies that include students from other disciplines, such as medicine, surgery and the general healthcare sector, as a reference population will be excluded from the review. Studies that refer to a group of students from disciplines related to speech-language pathology and/or that share its clinical techniques (e.g. otolaryngology, pulmonology, respiratory nursing) will only be considered if judged relevant. The research team will assess the relevance of the selected studies with respect to the other inclusion and exclusion criteria. In the case of a positive judgement, the studies will be included in the scoping review, with the appropriate adjustments and explanations.
A.6.2. Concept
The central concept of this scoping review is the use of virtual reality as an educational tool for the training of speech and language therapy students and for skills acquisition. VR comprehends a wide range of simulations able to present a fictitious environment as a real one. It can be divided into three main categories: non-immersive, semi-immersive and immersive. In the context of this review, all types of VR will be taken into account in order to have a better understanding on the utilisation of this technology. The kind of VR used in each study included will be categorised and described.
A.6.3. Context
The proposed scoping review will consider studies within the educational and training settings within the speech and language therapy field. The main point of interest of this search is the students’ clinical and practical skills acquisition and training of their hands-on abilities. Studies from any geographical location will be considered, without restrictions on cultural or institutional setting, in order to capture the broadest possible understanding of how VR is applied in speech-language pathology training across diverse educational landscapes.
Studies referring to the use of VR of speech and language therapy for more “general” educational purposes, will not be excluded a priori but will be screened and taken into account if considered relevant.
A.6.4. Types of sources
The scoping review will take into account all types of sources that provide relevant information on the use of virtual reality in the training of speech and language therapy students. Eligible sources will include all kinds of research studies (quantitative, qualitative, and mixed methods), reviews (scoping, systematic, meta-analysis), theoretical papers, conference proceedings, as well as grey literature.
No restrictions will be applied regarding study design, publication type, language, or year of publication. The objective of this approach is to provide a comprehensive overview of the currently available data on this topic.
A.7. Methods
The proposed scoping review will be conducted in accordance with the Joanna Briggs Institute’s methodology for scoping reviews and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews, i.e. PRISMA-ScR, guidelines (Tricco et al., 2018).
A.7.1. Search strategy
The proposed search strategy is designed to identify as many resources as possible on the subject matter. The interdisciplinary nature of the topic, which combines speech therapy (a health discipline) with virtual reality (one of today’s most cutting-edge technologies) and the educational and training context, necessitates the conducting of research on databases specialising in each of the three fields. Therefore, the following academic databases and search engines will be consulted: ACM Digital Library, Cochrane Library, EBSCOhost, IEEE Xplore, PubMed, PubMed Central, ScienceDirect, SpeechBite and Wiley. Grey literature, retrieved via Google Scholar, will also be taken into account. The PROSPERO register will also be consulted to detect ongoing studies and avoid bias risks. Moreover, AI-aided tools, such as Elicit (https://elicit.com/) will be used to identify additional records to analyse.
All source types will be included, such as descriptive, observational, experimental, quasi-experimental, interventional, mixed methods, qualitative, quantitative, and review studies, as well as other relevant empirical or secondary research designs. No time nor language constraints will be imposed. In order to undertake the search, it is first necessary to determine the keywords that will be used to scour the databases. These will be identified using the PCC mnemonic, then adapted and combined according to the characteristics of each interface to create appropriate queries. At this stage, the search will be limited to the titles, abstracts, and keywords of the articles. As no language filter will be imposed during the search, articles found in non-English will be translated with the help of online translators. The studies detected by the AI research assistant will also be taken into account.
In case a shortage of studies is detected, the few that are found will be subjected to the snowball process. This involves analysing their reference lists to identify other possible studies that are relevant to the scoping review.
A.7.2. Study/Source of evidence selection
Following the search, all identified sources will be collated and uploaded into Zotero (https://www.zotero.org/) and duplicates removed. It is important to note that studies identified by the AI-based research assistant, Elicit, will also be imported into Zotero and undergo the same manual verification process as other sources.
The source of evidence selection will undergo a two-step screening process:
- Title and abstract screening.
- Full text review.
The identification of eligible studies will be based on the criteria determined through the PCC framework. In the event of any doubt regarding the eligibility of a study, it will proceed to the subsequent stage of the process, which consists of a comprehensive review to establish its relevance.
The title and abstract screening will be conducted by two independent reviewers. In the event of a discrepancy regarding the eligibility of a source for the second-step screening, the source will be subjected to the full-text screening process to ensure that any potential ambiguities are resolved. As well as the first step, the full-text screening will be conducted by two independent reviewers. In the event of a divergence of opinion regarding the inclusion or exclusion of a source from the review, the reviewers will engage in a constructive dialogue to reach a consensus. Should this prove unsuccessful, a third reviewer will be consulted.
The study of the evidence selection process will be fully reported in the final scoping review through the dedicated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines flow diagram (Page et al., 2021) presented in Figure A1. If considered appropriate, modifications will be made to the PRISMA flowchart in accordance with the exact methodology followed and any changes will be explained and justified in the final scoping review.
Figure A1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources.
Figure A1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources.
A.7.3. Data extraction
The data extraction process will be guided by the standardized data extraction tool developed by the Joanna Briggs Institute for scoping reviews (Peters et al., 2020). If considered appropriate, modifications will be made to the data extraction tool in accordance with the findings and any changes will be explained and justified in the final scoping review.
A.7.4. Data analysis and presentation
The findings of the scoping review will be reported following the PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews) Checklist to ensure transparent and comprehensive reporting (Tricco et al., 2018). The data will be presented in tabular or diagrammatic form and accompanied by a narrative description and accurate analysis. Furthermore, when relevant, graphics will be presented to provide a comprehensive data visualisation.
Appendix B
Search Strategy for ACM Digital Library, Cochrane Library, EBSCOhost, IEEE Xplore, PubMed, Science Direct, SpeechBite and Wiley databases and for the PubMed Central Archive. The search was conducted in May 2025.

Table 1.
Search strategy table.
| Database | Query | Filter | Identified articles |
|---|---|---|---|
| ACM Digital Library | ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student*) ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student* OR educat*) |
title OR publication title OR abstract OR keywords | 0 0 |
| Cochrane Library | (("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student*)):ti,ab,kw (("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student* OR educat*)):ti,ab,kw |
title OR publication title OR abstract OR keywords | 1 3 |
| EBSCOhost | ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student*) ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student* OR educat*) |
- | 3 7 |
| IEEE Xplore | "Publication Title":("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student*) OR "Abstract":("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student*) OR "Author Keywords":("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student*) "Publication Title":("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student* OR educat*) OR "Abstract":("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student* OR educat*) OR "Author Keywords":("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student* OR educat*) |
publication title OR abstract OR author keywords |
0 0 |
| PROSPERO | ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student* OR educat*) | - | 7 |
| PubMed | ("speech therapy"[Title/Abstract] OR "speech-language therapy"[Title/Abstract] OR "SLT"[Title/Abstract] OR "speech pathology"[Title/Abstract] OR "speech-language pathology"[Title/Abstract] OR "SLP"[Title/Abstract] OR logop*[Title/Abstract]) AND ("VR"[Title/Abstract] OR "virtual reality"[Title/Abstract]) AND (training*[Title/Abstract]) AND (student*[Title/Abstract]) ("speech therapy"[Title/Abstract] OR "speech-language therapy"[Title/Abstract] OR "SLT"[Title/Abstract] OR "speech pathology"[Title/Abstract] OR "speech-language pathology"[Title/Abstract] OR "SLP"[Title/Abstract] OR logop*[Title/Abstract]) AND ("VR"[Title/Abstract] OR "virtual reality"[Title/Abstract]) AND (training*[Title/Abstract]) AND (student*[Title/Abstract] OR educat*[Title/Abstract]) |
title OR abstract | 2 6 |
| PubMed Central | (("speech therapy"[Abstract] OR "speech-language therapy"[Abstract] OR "SLT"[Abstract] OR "speech pathology"[Abstract] OR "speech-language pathology"[Abstract] OR "SLP"[Abstract] OR logop*[Abstract]) AND ("VR"[Abstract] OR "virtual reality"[Abstract]) AND (training*[Abstract]) AND (student*[Abstract])) OR (("speech therapy"[Title] OR "speech-language therapy"[Title] OR "SLT"[Title] OR "speech pathology"[Title] OR "speech-language pathology"[Title] OR "SLP"[Title] OR logop*[Title]) AND ("VR"[Title] OR "virtual reality"[Title]) AND (training*[Title]) AND (student*[Title])) (("speech therapy"[Abstract] OR "speech-language therapy"[Abstract] OR "SLT"[Abstract] OR "speech pathology"[Abstract] OR "speech-language pathology"[Abstract] OR "SLP"[Abstract] OR logop*[Abstract]) AND ("VR"[Abstract] OR "virtual reality"[Abstract]) AND (training*[Abstract]) AND (student*[Abstract] OR eduact*[Abstract])) OR (("speech therapy"[Title] OR "speech-language therapy"[Title] OR "SLT"[Title] OR "speech pathology"[Title] OR "speech-language pathology"[Title] OR "SLP"[Title] OR logop*[Title]) AND ("VR"[Title] OR "virtual reality"[Title]) AND (training*[Title]) AND (student*[Title] OR educat*[Title])) |
title OR abstract |
3 3 |
| Science Direct | "(speech language therapy OR ""SLT"" OR speech language pathology OR ""SLP"" OR logop) AND (""VR"" OR ""virtual reality"") AND (training) AND (student) (speech language therapy OR ""SLT"" OR speech language pathology OR ""SLP"" OR logop) AND (""virtual reality"") AND (training) AND (student)" (speech language therapy OR "SLT" OR speech language pathology OR "SLP" OR logop) AND ("virtual reality") AND (training) AND (student OR education) |
title OR abstract OR specified keywords | 2 2 3 |
| SpeechBite | "virtual reality" | - | 16 |
| Wiley | ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student*) ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logop*) AND ("VR" OR "virtual reality") AND (training*) AND (student* OR educat*) |
title OR abstract OR keywords | 17 4 |
Appendix C
Search Strategy for Google Scholar. The search was conducted in May 2025.
Table 1.
Google Scholar search strategy table.
| Query | Identified articles |
|---|---|
| allintitle: ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") AND (training OR trainings) AND (student OR students) -child -children -deaf -autism -rehabilitation | 0 |
| allintitle: ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") AND (training OR trainings) AND (student OR students) | 0 |
| allintitle: ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") AND (training OR trainings) -child -children -deaf -autism -rehabilitation | 1* |
| allintitle: ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") AND (training OR trainings) | 1* |
| allintitle: ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") AND (student OR students) | 0 |
| allintitle: ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") -child -children -deaf -autism -rehabilitation | 4* |
| allintitle: ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") | 5* |
| allintitle: ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") AND (education OR educational) | 1* |
| ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") AND (training OR trainings) AND (student OR students OR education OR educational) | 15800 |
| ("speech therapy" OR "speech-language therapy" OR "SLT" OR "speech pathology" OR "speech-language pathology" OR "SLP" OR logopedie OR logopaedie OR logopedics OR logopaedics) AND (VR OR "virtual reality") AND (training OR trainings) AND (student OR students OR education OR educational) -child -children -deaf -autism -rehabilitation | 2910* |
*Of these records, the titles were read. It was only the titles that were considered to be relevant that were subsequently manually subjected to the evidence selection process described in the following section.
Appendix D
Data Charting Table to extract data from included articles.
Table 1.
Data Charting Table to extract data from included articles.
| Title & Reference | Year | Country | Language | Study type | VR type | VR characteristics | Population | Training purposes (and sub-field) |
Main outcomes and assessment |
|---|---|---|---|---|---|---|---|---|---|
References
- World Health Organization. Ageing and health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 28 May 2025).
- OECD. What Do We Know about Young People’s Interest in Health Careers?; OECD Publishing, 2025. [CrossRef]
- World Health Organization. Transforming and Scaling up Health Professionals’ Education and Training: World Health Organization Guidelines 2013; World Health Organization: Geneva, 2013.
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030; World Health Organization: Geneva, 2016.
- The European Higher Education Area in 2024: Bologna Process Implementation Report; European Education and Culture Executive Agency, Ed.; Publications Office: Luxembourg, 2024. [CrossRef]
- McGaghie, W. C.; Issenberg, S. B.; Barsuk, J. H.; Wayne, D. B. A Critical Review of Simulation-Based Mastery Learning with Translational Outcomes. Med Educ 2014, 48 (4), 375–385. [CrossRef]
- Sung, H.; Kim, M.; Park, J.; Shin, N.; Han, Y. Effectiveness of Virtual Reality in Healthcare Education: Systematic Review and Meta-Analysis. Sustainability 2024, 16 (19), 8520. [CrossRef]
- Kyaw, B. M.; Saxena, N.; Posadzki, P.; Vseteckova, J.; Nikolaou, C. K.; George, P. P.; Divakar, U.; Masiello, I.; Kononowicz, A. A.; Zary, N.; Tudor Car, L. Virtual Reality for Health Professions Education: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. J Med Internet Res 2019, 21 (1), e12959. [CrossRef]
- Christmas, C.; Rogus-Pulia, N. Swallowing Disorders in the Older Population. J American Geriatrics Society 2019, 67 (12), 2643–2649. [CrossRef]
- Springer, L.; Zückner, H. Empfehlende Ausbildungsrichtlinie für die staatlich anerkannten Logopädieschulen in NRW. 16 Aug 2006.
- Council for Clinical Certification in Audiology and Speech-Language Pathology of the American Speech-Language-Hearing Association. 2020 Standards for the Certificate of Clinical Competence in Speech-Language Pathology; American Speech-Language-Hearing Association, 2018. https://www.asha.org/certification/2020-SLP-Certification-Standards.
- American Speech-Language-Hearing Association. 2020 Standards for Certification of the Practice of Speech-Language Pathology. Available online: https://www.asha.org/certification/2020-slp-certification-standards/?srsltid=AfmBOorFKk7aftWeRQ0iWAasSV3KNTgwxUxORZHRVKC_E_aMM3V1r9d_#5 (accessed on 17 June 2025).
- Speech Pathology Australia. Simulation-Based Learning Program. Available online: https://www.speechpathologyaustralia.org.au/Public/Public/About-Us/Ethics-and-standards/Simulation-based-learning-program.aspx?hkey=f0d1f1f5-c9f7-4806-9f18-1e3993ce09c0 (accessed on 17 June 2025).
- Council of Academic Programs in Communication Sciences and Disorders. Best Practices in Healthcare Simulations in Communication Sciences and Disorders. March 2019. Available online: https://growthzonesitesprod.azureedge.net/wp-content/uploads/sites/1023/2020/03/Best-Practices-in-CSD.pdf (accessed on: 17 June 2025).
- Slater, M.; Wilbur, S. A Framework for Immersive Virtual Environments (FIVE): Speculations on the Role of Presence in Virtual Environments. Presence: Teleoperators & Virtual Environments 1997, 6 (6), 603–616. [CrossRef]
- Using Immersive Technologies to Enhance Student Learning Outcomes in Clinical Sciences Education and Training; 2023. [CrossRef]
- Dhar, E.; Upadhyay, U.; Huang, Y.; Uddin, M.; Manias, G.; Kyriazis, D.; Wajid, U.; AlShawaf, H.; Syed Abdul, S. A Scoping Review to Assess the Effects of Virtual Reality in Medical Education and Clinical Care. DIGITAL HEALTH 2023, 9, 20552076231158022. [CrossRef]
- Bryant, L.; Brunner, M.; Hemsley, B. A Review of Virtual Reality Technologies in the Field of Communication Disability: Implications for Practice and Research. Disability and Rehabilitation: Assistive Technology 2020, 15 (4), 365–372. [CrossRef]
- Rose, T. A.; Copley, A.; Scarinci, N. A. Benefits of Providing an Acute Simulated Learning Environment to Speech Pathology Students: An Exploratory Study. FoHPE 2017, 18 (3), 44–59. [CrossRef]
- Hemmerich, A.; Hoepner, J. Using Video Simulations for Assessing Clinical Skills in Speech-Language Pathology Students. JoTLT 2022, 11 (1). [CrossRef]
- Petrich, T.; Mills, B.; Lewis, A.; Hansen, S.; Brogan, E.; Ciccone, N. Utilisation of Simulation-Based Learning to Decrease Student Anxiety and Increase Readiness for Clinical Placements for Speech-Language Pathology Students. International Journal of Speech-Language Pathology 2024, 26 (3), 380–389. [CrossRef]
- Peters, M. D.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A. C.; Khalil, H. Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Lockwood, C., Porritt, K., Pilla, B., Jordan, Z., Eds.; JBI, 2024. [CrossRef]
- Tricco, A. C.; Lillie, E.; Zarin, W.; O’Brien, K. K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M. D. J.; Horsley, T.; Weeks, L.; Hempel, S.; Akl, E. A.; Chang, C.; McGowan, J.; Stewart, L.; Hartling, L.; Aldcroft, A.; Wilson, M. G.; Garritty, C.; Lewin, S.; Godfrey, C. M.; Macdonald, M. T.; Langlois, E. V.; Soares-Weiser, K.; Moriarty, J.; Clifford, T.; Tunçalp, Ö.; Straus, S. E. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169 (7), 467–473. [CrossRef]
- Elicit. Available online: https://elicit.com/ (accessed on 28 June 2025).
- Williams, S. L. The Virtual Immersion Center for Simulation Research: Interactive Simulation Technology for Communication Disorders. 2006.
- Sia, I.; Halan, S.; Lok, B.; Crary, M. A. Virtual Patient Simulation Training in Graduate Dysphagia Management Education—A Research-Led Enhancement Targeting Development of Clinical Interviewing and Clinical Reasoning Skills. Perspect ASHA SIGs 2016, 1 (13), 130–139. [CrossRef]
- Banszki, F.; Beilby, J.; Quail, M.; Allen, P.; Brundage, S.; Spitalnick, J. A Clinical Educator’s Experience Using a Virtual Patient to Teach Communication and Interpersonal Skills. AJET 2018, 34 (3). [CrossRef]
- Moradi, N.; Rahimifar, P.; Soltani, M.; Shaterzadeh-Yazdi, M. J.; Hosseini Bidokhti, M. Oral Functional Assessment Training in Speech Therapy Students Using Virtual Reality (VR). Int. J. Musculoskelet. Pain Prev. 2018, 3 (3), 87–89.
- University of Central Florida; Towson Ph.D., Ccc-Slp, J. A.; Taylor Ph.D., M. S.; University of Central Florida; Pt, Dpt, Pc S, J. T.; University of Central Florida; Paul Ph.D., Bcba, C.; Georgia State University; Pabian Pt, Dpt, Sc S, Oc S, P.; University of Central Florida; Zraick Ph.D., Ccc-Slp, R. I.; University of Central Florida. Impact of Virtual Simulation and Coaching on the Interpersonal Collaborative Communication Skills of Speech-Language Pathology Students: A Pilot Study. TLCSD 2018, 2 (2). [CrossRef]
- Carter, M. D. The Effects of Computer-Based Simulations on Speech-Language Pathology Student Performance. Journal of Communication Disorders 2019, 77, 44–55. [CrossRef]
- Rondon-Melo, S.; Andrade, C. R. F. D. Efeitos Do Uso de Diferentes Tecnologias Educacionais Na Aprendizagem Conceitual Sobre o Sistema Miofuncional Orofacial. Audiol., Commun. Res. 2019, 24, e2050. [CrossRef]
- Miles, A.; Hayden, S.; Carnell, S.; Halan, S.; Lok, B. What Do Speech Pathology Students Gain from Virtual Patient Interviewing? A WHO International Classification of Functioning Disability and Health (ICF) Analysis. BMJ STEL 2020, bmjstel-2020-000616. [CrossRef]
- Robinson, K. E.; Allen, P. J.; Quail, M.; Beilby, J. Virtual Patient Clinical Placements Improve Student Communication Competence. Interactive Learning Environments 2020, 28 (6), 795–805. [CrossRef]
- Blaydes, M. S. Effects of a Virtual Reality Dementia Experience on Graduate Communication Disorders Students’ Future Clinical Practice. https://encompass.eku.edu/etd/687/.
- Deman, H.; Boets, B.; Hermans, D.; Rombouts, E. Virtual Reality and Stuttering: A Tool for Experiential Learning in Preservice Speech Therapy Education. https://lirias.kuleuven.be/3711926.
- Kelly, B.; Walters, J.; Unicomb, R. Speech Pathology Student Perspectives on Virtual Reality to Learn a Clinical Skill. TeachingandLearninginCommunicationSciences&Disorders 2023, 7(1). [CrossRef]
- Gentile, F.; Wanke, M.; Mueller, W. Virtual Reality in Speech Therapy Training: Scenarios and Prototyping. In Proceedings of INTED2025 Conference; IATED: Valencia, Spain, 3-5 March 2025.
- THE USE OF INFORMATION AND COMMUNICATION TECHNOLOGIES IN PREPARING FUTURE SPEECH THERAPISTS FOR PROFESSIONAL PRACTICE | International Multidisciplinary Journal for Research & Development. https://www.ijmrd.in/index.php/imjrd/article/view/2724 (accessed 2025-05-27).
- MacBean, N.; Theodoros, D.; Davidson, B.; Hill, A. E. Simulated Learning Environments in Speech-Language Pathology: An Australian Response. International Journal of Speech-Language Pathology 2013, 15 (3), 345–357. [CrossRef]
- Jiang, H.; Vimalesvaran, S.; Wang, J. K.; Lim, K. B.; Mogali, S. R.; Car, L. T. Virtual Reality in Medical Students’ Education: Scoping Review. JMIR Med. Educ. 2022, 8 (1), e34860. [CrossRef]
- Hood, R. J.; Maltby, S.; Keynes, A.; Kluge, M. G.; Nalivaiko, E.; Ryan, A.; Cox, M.; Parsons, M. W.; Paul, C. L.; Garcia-Esperon, C.; Spratt, N. J.; Levi, C. R.; Walker, F. R. Development and Pilot Implementation of TACTICS VR: A Virtual Reality-Based Stroke Management Workflow Training Application and Training Framework. Front. Neurol. 2021, 12, 665808. [CrossRef]
- Chiang, D. H.; Huang, C. C.; Cheng, S. C.; Cheng, J. C.; Wu, C. H.; Huang, S. S.; Yang, Y. Y.; Yang, L. Y.; Kao, S. Y.; Chen, C. H.; Shulruf, B.; Lee, F. Y. Immersive Virtual Reality (VR) Training Increases the Self-Efficacy of In-Hospital Healthcare Providers and Patient Families Regarding Tracheostomy-Related Knowledge and Care Skills: A Prospective Pre-Post Study. Medicine 2022, 101 (2), e28570. [CrossRef]
- Overby, M. Stakeholders’ Qualitative Perspectives of Effective Tele-Practice Pedagogy in Speech–Language Pathology. Int. J. Language Communication Disorders. 2018, 53 (1), 101–112.
- Page, M. J.; McKenzie, J. E.; Bossuyt, P. M.; Boutron, I.; Hoffmann, T. C.; Mulrow, C. D.; Moher, D. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [CrossRef]
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources adapted according to our research process. The original flowchart was adapted to reflect the research process followed. *pre-screening: this screening was only applied to Google Scholar (title-based screening) and Elicit (automatic screening performed by the program). This process is fully described in paragraph 2.4 (Exceptions). **suggested resources: these are the ones suggested by search engines and online platforms (e.g., Google Scholar, PubMed), which appeared as ‘related articles’ or algorithm-based recommendations.
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources adapted according to our research process. The original flowchart was adapted to reflect the research process followed. *pre-screening: this screening was only applied to Google Scholar (title-based screening) and Elicit (automatic screening performed by the program). This process is fully described in paragraph 2.4 (Exceptions). **suggested resources: these are the ones suggested by search engines and online platforms (e.g., Google Scholar, PubMed), which appeared as ‘related articles’ or algorithm-based recommendations.
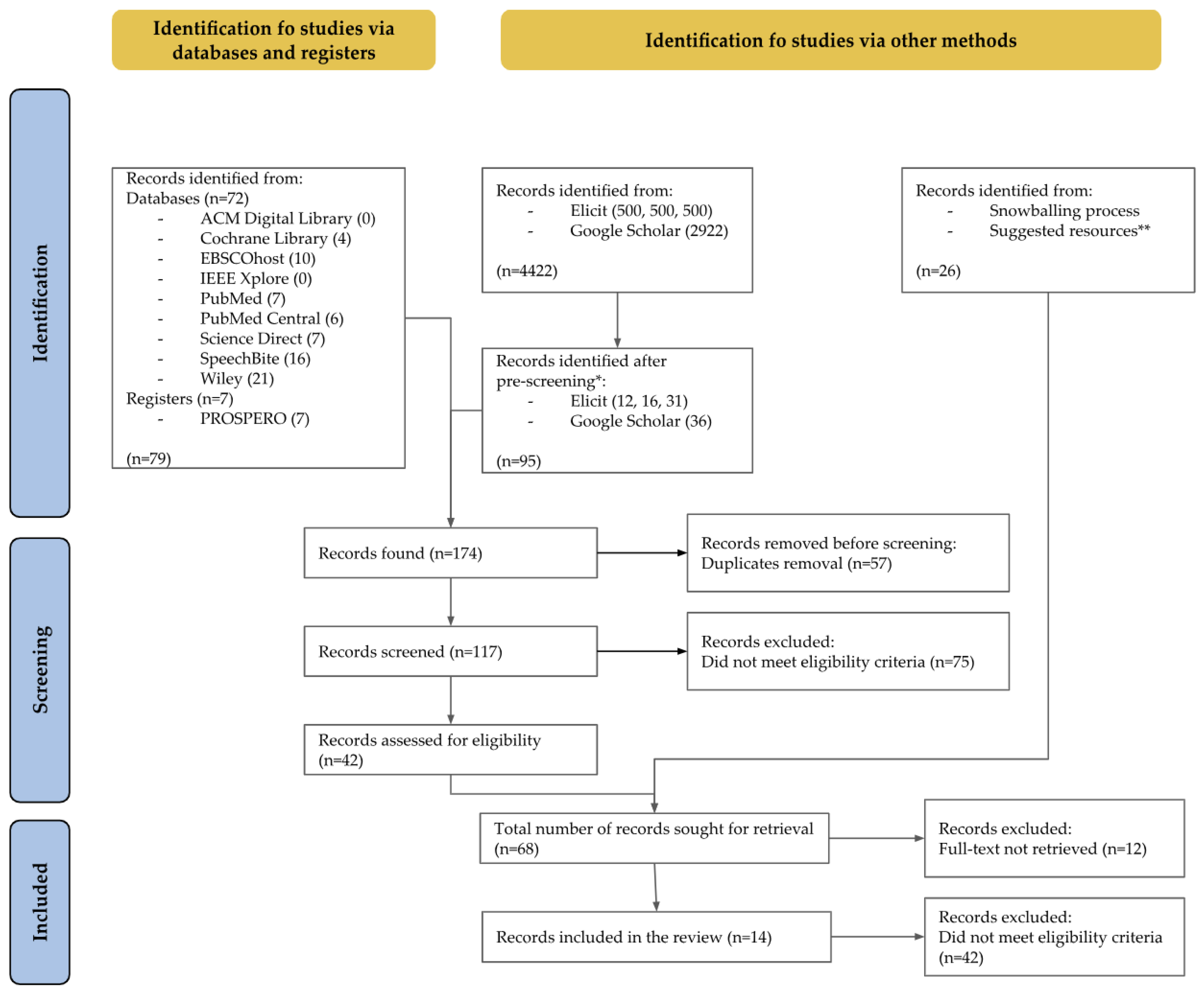
Figure 2.
Geographical distribution of the included studies. Please note: the graph’s total number of articles is higher than the included number because some studies were done by two countries.
Figure 2.
Geographical distribution of the included studies. Please note: the graph’s total number of articles is higher than the included number because some studies were done by two countries.
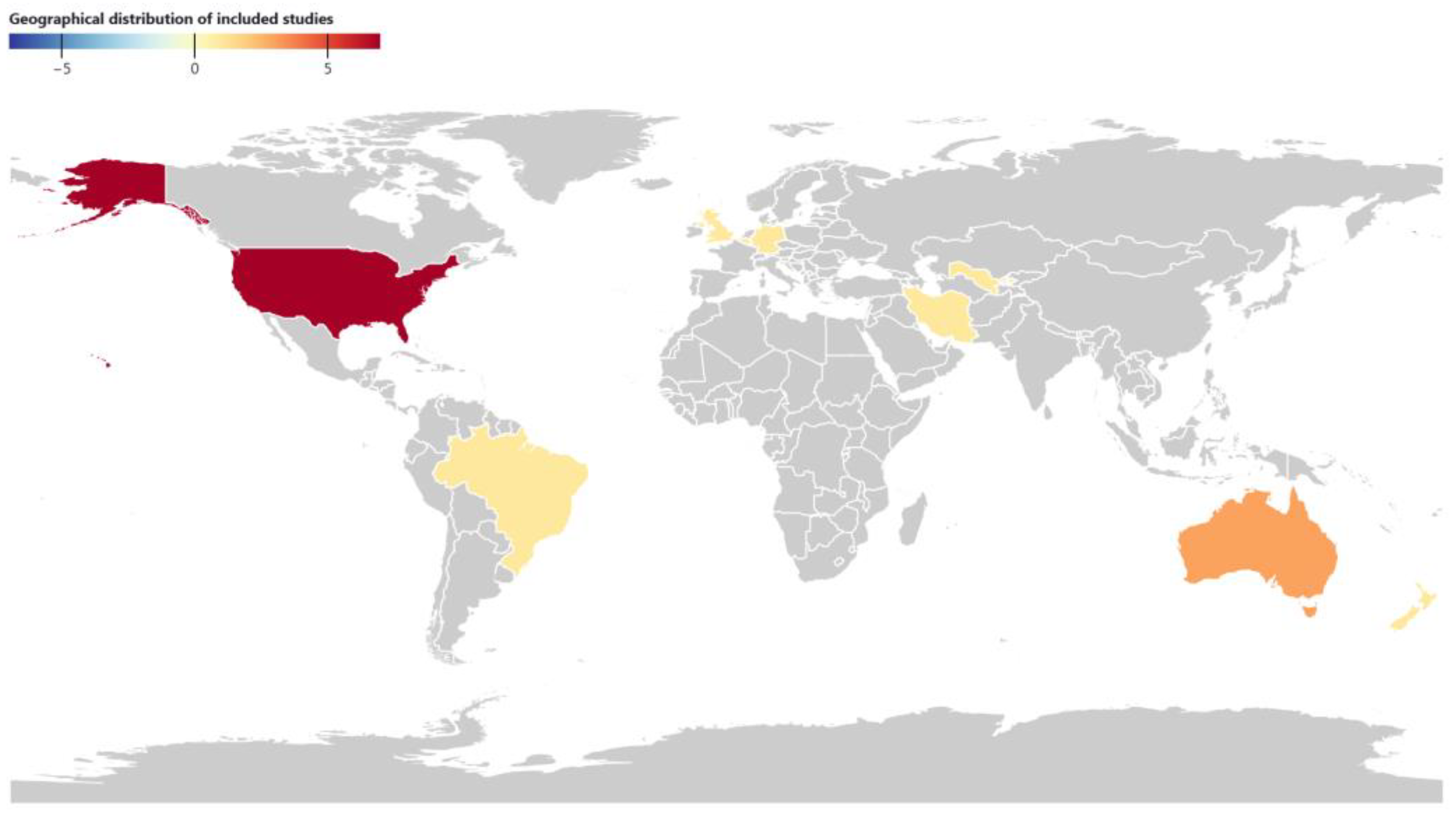
Figure 3.
Number of articles published per year and country of the authors’ institutions. Please note: the graph’s total number of articles is higher than the included number because some studies were done by two countries.
Figure 3.
Number of articles published per year and country of the authors’ institutions. Please note: the graph’s total number of articles is higher than the included number because some studies were done by two countries.
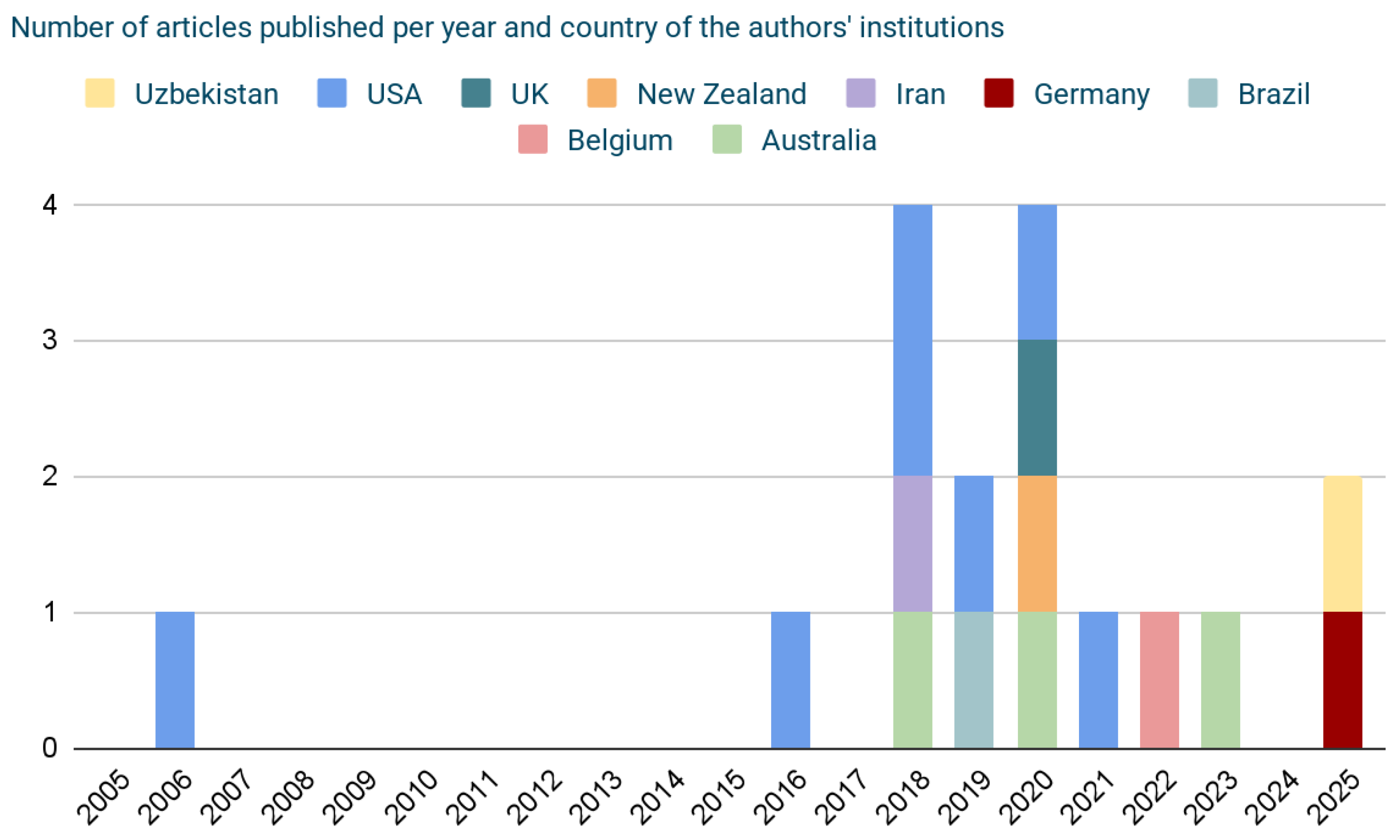
Figure 4.
VR types of the included studies.

Figure 5.
VR characteristics of the included studies.
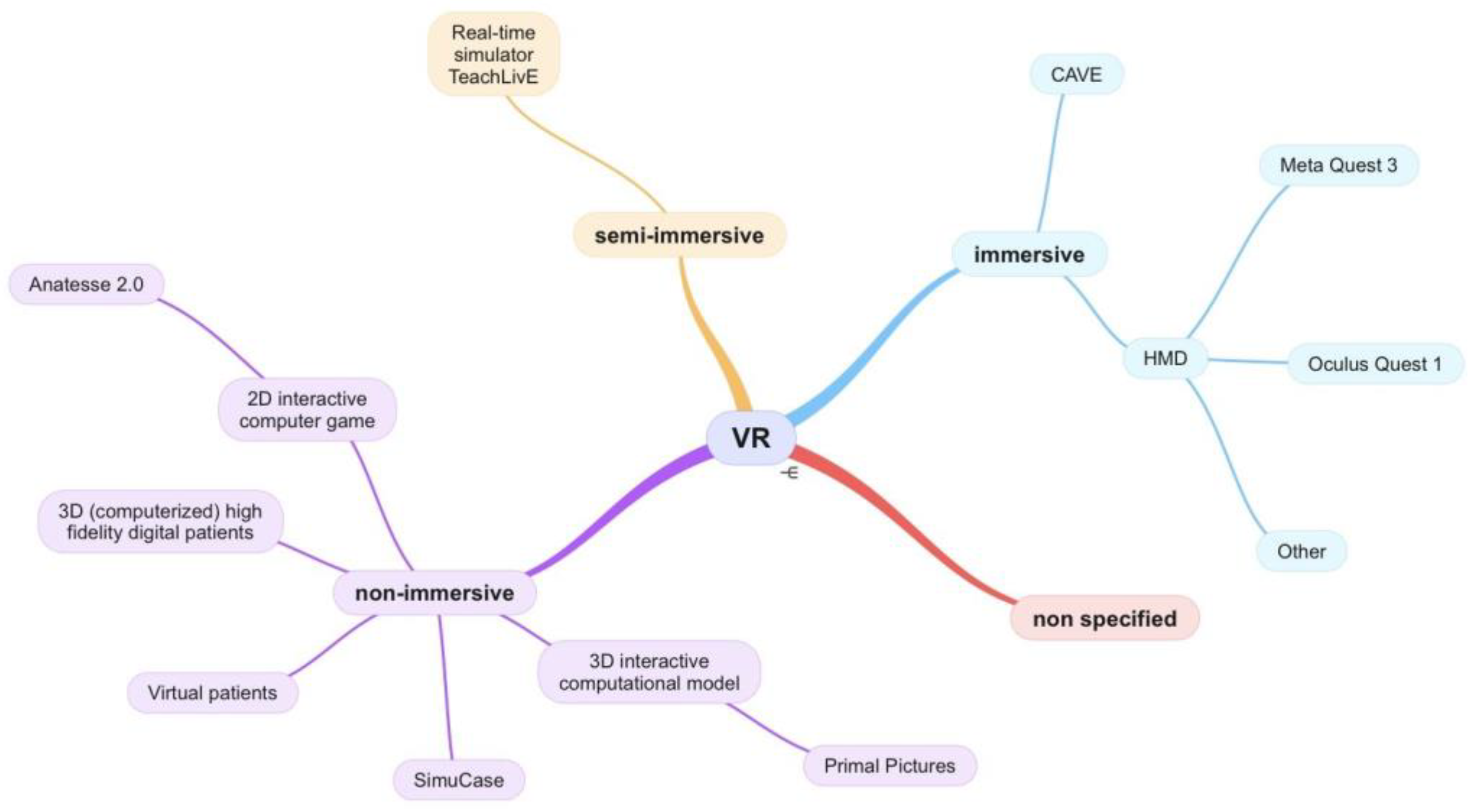
Figure 6.
Target population of the included studies.
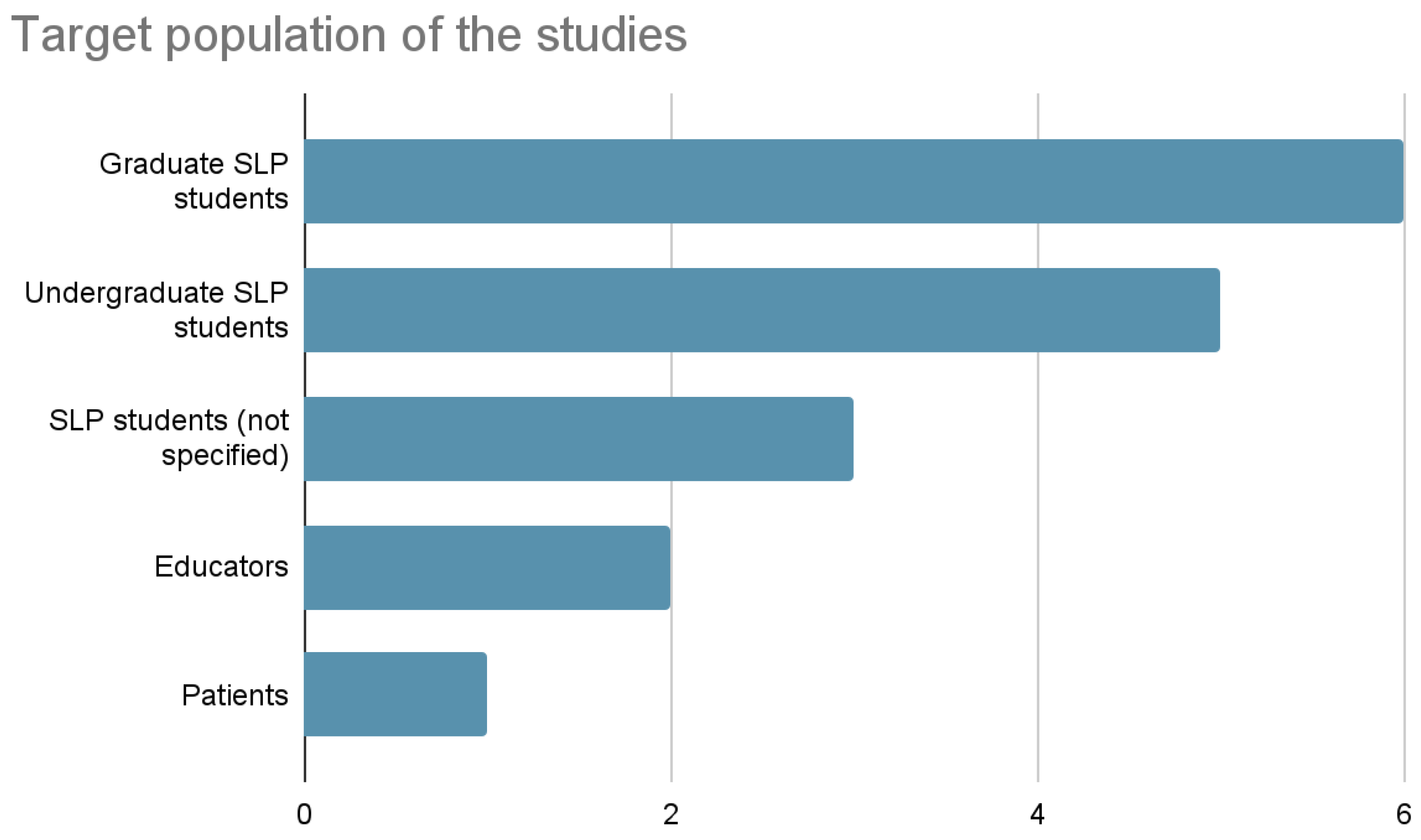
Figure 7.
Training purposes of the included studies.
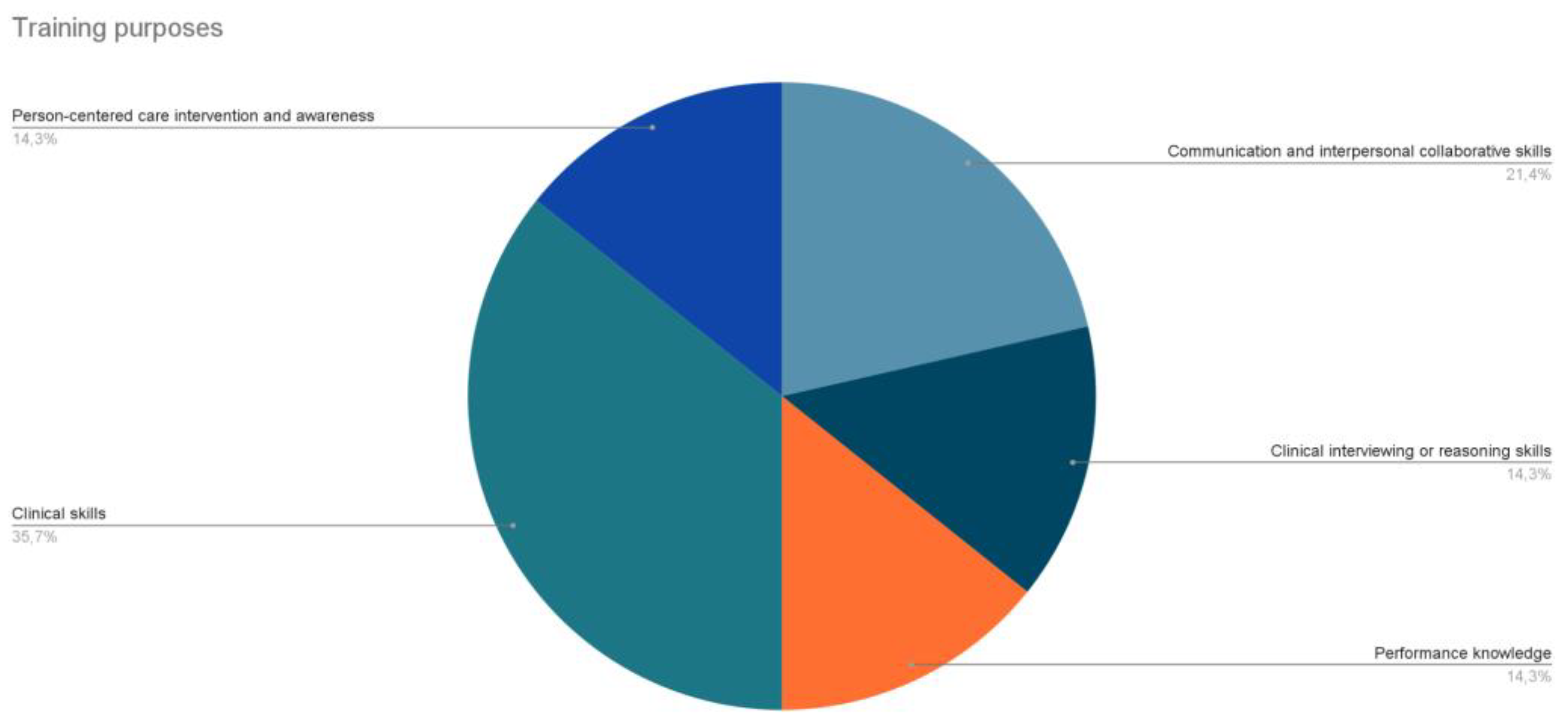
Table 1.
List of keywords used according to the PCC framework.
| Focus | Keywords |
|---|---|
| Population | speech therapy, speech-language therapy, SLT, speech pathology, speech-language pathology, SLP, logop* (i.e. logopedie, logopaedie, logopedics, logopaedics), student* (i.e. student, students) |
| Concept | VR, virtual reality |
| Context | training* (i.e. training, trainings), educat* (i.e. education, educational) |
Table 2.
Data extraction of study characteristics.
| Title and Reference | Year | Country | Language | Study type |
|---|---|---|---|---|
| The Virtual Immersion Center for Simulation Research: Interactive Simulation Technology for Communication Disorders [25] | 2006 | USA (Ohio) | en | Pilot |
| Virtual Patient Simulation Training in Graduate Dysphagia Management Education—A Research-Led Enhancement Targeting Development of Clinical Interviewing and Clinical Reasoning Skills [26] | 2016 | USA (Florida) | en | Mixed methods |
| A Clinical Educator’s Experience Using a Virtual Patient to Teach Communication and Interpersonal Skills [27] | 2018 | USA (Georgia) Australia |
en | Qualitative |
| Oral Functional Assessment Training in Speech Therapy Students Using Virtual Reality (VR) [28] | 2018 | Iran | en | Descriptive |
| Impact of Virtual Simulation and Coaching on the Interpersonal Collaborative Communication Skills of Speech-Language Pathology Students: A Pilot Study [29] | 2018 | USA (Florida) | en | Pilot, Experimental |
| The Effects of Computer-Based Simulations on Speech-Language Pathology Student Performance [30] | 2019 | USA (Georgia) | en | Experimental |
| Efeitos Do Uso de Diferentes Tecnologias Educacionais Na Aprendizagem Conceitual Sobre o Sistema Miofuncional Orofacial [31] | 2019 | Brazil | en | Controlled randomized trial, Experimental |
| What Do Speech Pathology Students Gain from Virtual Patient Interviewing? A WHO International Classification of Functioning Disability and Health (ICF) Analysis [32] | 2020 | USA (Florida) New Zealand |
en | Observational, Descriptive |
| Virtual Patient Clinical Placements Improve Student Communication Competence [33] | 2020 | Australia UK |
en | Experimental |
| Effects of a Virtual Reality Dementia Experience on Graduate Communication Disorders Students’ Future Clinical Practice [34] | 2021 | USA (Kentucky) | en | Mixed methods (MA thesis) |
| Virtual Reality and Stuttering: A Tool for Experiential Learning in Preservice Speech Therapy Education [35] | 2022 | Belgium | en | Descriptive, Controlled randomized trial (poster presentation) |
| Speech Pathology Student Perspectives on Virtual Reality to Learn a Clinical Skill [36] | 2023 | Australia | en | Qualitative |
| Virtual Reality in Speech Therapy Training: Scenarios and Prototyping [37] | 2025 | Germany | en | Mixed methods, Design-based research |
| The Use of Information and Communication Technologies in Preparing Future Speech Therapists for Professional Practice [38] | 2025 | Uzbekistan | en | Mixed methods, Descriptive |
Table 3.
Results of individual sources of evidence.
| Author(s) and Reference | VR type | VR characteristics | Population | Training purposes (and sub-fields) | Main outcomes and assessment methods |
|---|---|---|---|---|---|
| (Williams, 2006) [25] | Immersive VR | CAVE projection-based technology |
Graduate SLP (and patients with communication disorders) | clinical skills (communication disorders) |
predicts increased competency and transfer of skills |
| (Sia et al., 2016) [26] | Non immersive VR | Virtual Patients (VPP); immersive VP simulation | Graduate SLP | clinical interviewing and clinical reasoning skills (stuttering) |
improvement of diagnosis competencies, reasoning and empathy; positive feedback |
| (Banszki et al., 2018)[27] | Non immersive VR | Virtual Patients; immersive VP simulation | Undergraduate (3rd year); CE point of view | communication and interpersonal skills | improvement of CE confidence and pedagogical skills as educator |
| (Moradi et al., 2018)[28] | Immersive VR | 3D glasses + monitor + gloves | SLP students (5th term) | oral organs assessment training | increase of students’ scores |
| (Towson et al., 2018) [29] | Semi immersive VR | mixed reality real-time simulator TeachLivE | Graduate SLP (3rd semester) | interpersonal collaborative communication skills when delivering information regarding a singular patient to different stakeholders | performance enhancement (2nd attempt);collaborative communication (Situation- Background- Assessment- Recommendation- Communication [SBAR-C]), high acceptability |
| (Carter, 2019) [30] | Non immersive VR | Virtual Patients; SimuCase; immersive VP simulation | Graduate SLP (2nd semester) | performances in the pediatric language disorders | improved clinical skills, high levels of improvement on the SCSI and CTCSD |
| (Rondon-Melo & Andrade, 2019) [31] | Non immersive VR | 2D interactive computer game (Anatesse 2.0); interactive 3D computational model (Primal Pictures) | Undergraduate students in Speech-Language and Hearing Sciences (SLHS) | anatomy and physiology of the orofacial myofunctional system | students’ performance in the knowledge assessment was similar, regardless of the learning method applied |
| (Miles et al., 2020) [32] | Non immersive VR | Virtual Patients | Graduate final year | interviewing skills using WHO-ICF (dysphagia) |
ICF respected, matching health literacy; VP interviews and findings as assessment |
| (Robinson et al., 2020) [33] | Non immersive VR | 3D (computerised) high fidelity digital patients; immersive VP simulation | Undergraduate SLP (2nd year) | communication skills (dementia) |
improved communication competence; CCIS, PRQ questionnaires as assessment |
| (Blaydes, 2021) [34] | VR (non specified) | non specified | Graduate SLP (2nd year) | understanding the importance of providing person-centered care (dementia) |
small margin for score improvement; increased levels of empathy |
| (Deman et al., 2022) [35] | Immersive VR | not specified | BA SLP students | understanding stuttering-related anxiety | students reported fear and physiological fear responses |
| (Kelly et al., 2023) [36] | Immersive VR | VR-OMA application; Oculus Quest 1 | Undergraduate SLP (2nd year) | clinical skills (oral musculature assessment) |
positive reaction of students’ intrinsic and extrinsic value for the training experience |
| (Gentile et al., 2025) [37] | Immersive VR | Meta Quest 3 applications implementing different scenarios | SLP | clinical skills (FEES, TTM, tDCS) |
prototype development to be assessed through usability, presence, acceptance, user experience |
| (Xonbabayeva Madinabonu Asqarjon kizi, 2025) [38] | VR (non specified) | not specified | SLP students and educators | practical skills | enhanced understanding, skill acquisition, confidence and competence; interviews assessment |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



