
Submitted:
03 July 2025
Posted:
10 July 2025
You are already at the latest version
Abstract
Historically, colorectal liver metastases (CRLM) have been considered a contraindication for liver transplantation (LT), given the limited organ supply and poor oncologic efficacy. Recent studies, however, have demonstrated that highly selected patients with unresectable CRLM can achieve remarkable long-term survival following LT, often surpassing outcomes seen with conventional systemic therapies. This review explores the evolving role of LT for the treatment of unresectable CRLM, examining patient selection criteria, overall survival, disease-free survival, recurrence patterns, and emerging biomarkers that may guide transplant eligibility. Additionally, we discuss innovations in organ utilization, including living donor LT and machine perfusion strategies, to expand access while mitigating ethical concerns surrounding organ allocation. As LT for CRLM transitions from experimental protocols to clinical application, this review highlights key challenges and opportunities that will shape its future role in the field of transplant oncology.
Keywords:
colorectal cancer
; colorectal liver metastases
; liver transplantation
; patient selection
; overall survival
; disease free survival
Introduction
Colorectal cancer (CRC) is the third most frequently diagnosed cancer and the third most common cause of cancer-related mortality in both men and women in the United States [1]. The 5-year survival rate for localized CRC is 91%; however, this rate decreases to 36% for patients with regional lymph node metastases and 14% in the presence of distal metastases [1]. The liver is the most common site for metastatic spread [2]. The International Hepato-Pancreato-Biliary Association (IHPBA) divide liver metastases from colorectal cancer (CRLM) into different categories based on resectability and time of diagnosis [3]. Approximately 22% of patients with CRCs have metastatic disease at diagnosis, and up to 70% of patients will develop end-stage liver disease due to progression of tumor burden or from side effects of systemic or locoregional therapies [4]. Only 20–30% of CRLM patients can be resected when diagnosed because of the anatomical constraints or the extent of the disease [5]. Patients with unresectable CRLM as illustrated in Figure 1, where almost all hepatic segments are involved, systemic therapy (ST) alone yields a 5-year overall survival (OS) rate of less than 15%, whereas hepatic resection is associated with 5- and 10-year survival rates of 42% and 25%, respectively [6]. Even after radical hepatic resections, the liver remains the most common site of recurrence, with 50-75% of patients experiencing recurrent disease in the liver [7].
Modern liver-directed therapies include histotripsy, thermal ablation, trans-arterial radioembolization, trans-arterial chemoembolization, and stereotactic body radiotherapy, in addition to surgery. These modalities are predominantly employed for palliative purposes, aiming to alleviate symptoms rather than achieving a cure. Histotripsy is an ultrasound-based, non-thermal, and non-invasive targeted therapy developed in recent years. Although our experience with histotripsy for CRLM is still limited, this new technology has shown promising results with an OS rate of 58.6%, and one-year survival rates of 73.3% in patients with hepatocellular carcinoma (HCC) and 48.6% in patients with other types of metastatic disease [8]. Multiple factors, including tumor-related characteristics (such as the number, size, and location), patient-related factors (such as frailty, comorbidities, and personal preferences), and oncological features (such as the timing of metastasis and tumor aggressiveness) influence the type of local therapy used. In the presence of poor prognostic signs, ST is generally preferred over local interventions for comprehensive disease control. Advances in ST have significantly improved outcomes by increasing curative potential in patients with resectable CRLM. Additionally, in select patients with unresectable CRLM, ST can downsize metastases and facilitate secondary interventions including hepatic resections [9].
Liver Transplantation for Unresectable Colorectal Metastatic Disease
LT is the standard treatment for patients with end-stage liver disease, selected unresectable HCCs, low-grade neuroendocrine tumors (NETs), and hilar and intra-hepatic cholangiocarcinomas within specific criteria defined by the United Network of Organ Sharing (UNOS) [10]. LT for CRLM was historically considered inappropriate due to high perioperative mortality rates, suboptimal oncologic outcomes, high recurrence rates, and ethical concerns related to the distribution of scarce donor organs. Recent advances, however, have altered this perspective. Enhanced perioperative care, optimized immunosuppression protocols, the development of novel ST agents, and increasingly favorable transplantation outcomes in other primary and secondary tumors have renewed interest in LT for carefully selected patients with CRLM.
The Milan criteria for HCC, which include either a solitary tumor measuring ≤5 cm or up to three nodules each measuring ≤3 cm, without vascular invasion or extrahepatic dissemination. Meeting these parameters has been associated with 5-year OS rates of up to 70% [11]. The Mayo protocol for perihilar cholangiocarcinoma includes tumor size ≤3 cm, the lack of intra- or extrahepatic metastases, no nodal involvement on imaging, and prior neoadjuvant therapy (chemoradiation). This approach has resulted in 5-year OS rates of up to 65% [12]. For NETs, selection criteria include well-differentiated histology, liver-only disease, low Ki-67 index (<10–20%), stable disease for at least 6 months, and the absence of extrahepatic metastases, with survival rates over 60–80% [13]. The demonstrated success of rigorous selection criteria in these malignancies has prompted the broadening of LT indications to include CRLM.
SECA Trials
The first prospective study evaluating the role of LT in CRLM was the SECA-I trial [14]. In a cohort of 21 patients, 5-year OS rate was 60%, but the study was limited by its small sample size and in the cohort recurrence rate was high with a relatively short disease-free survival (DFS). The subsequent SECA-II trial, used more stringent selection criteria, and demonstrated a more favorable 5-year OS that was 83% with a median follow-up of 36 months [15]. In a subsequent study of 12 LT recipients, Andres et al. [16] reported a 1-year OS of 83%, a 5-year OS of 50%, and a recurrence rate of 60% with DFS rates of 56% at 1 year and 38% at 5 years. Furthermore, the randomized TransMet trial demonstrated a 5-year OS rate of 57% in the LT group compared to 13% in the ST-only group [17]. These findings were further supported by a recent meta-analysis conducted by Dawood et al. [18], which demonstrated 1-, 3-, and 5-year OS rates of 95%, 77%, and 53%, respectively, with corresponding DFS rates of 51%, 33%, and 13%.
Current Outcomes and Emerging Strategies for Unresectable Colorectal Liver Metastases
Systemic chemotherapy remains the standard for unresectable CRLM, yet long-term outcomes are poor. The NORDIC VII study reported a median progression-free survival (PFS) of 8 months and overall survival (OS) of 12 months, with a 5-year OS under 9% [19], underscoring the limited efficacy of current treatments.
In resectable cases, chemotherapy offers only modest benefits. A meta-analysis by Sonbol et al. [19] showed that perioperative chemotherapy improves disease-free survival (DFS) but not OS. Similarly, Kanemitsu et al. [20] observed lower 5-year OS with adjuvant chemotherapy (69.5%) compared to surgery alone (83.0%), raising concerns about its long-term value.
Liver transplantation (LT) has emerged as a promising option for highly selected patients with unresectable CRLM, achieving survival outcomes that may surpass those of conventional therapies. In parallel, novel systemic and cell-based therapies are under investigation. Krishnan et al. [21] identified MiNK-215, a cell therapy that reshapes the tumor microenvironment by depleting stromal cells and enhancing CD8+ T cell infiltration. Its incorporation into transplant protocols could improve outcomes and reduce recurrence.
Patient Selection and Outcomes of Liver Transplantation for Unresectable Colorectal Liver Metastases
Liver transplantation (LT) and emerging systemic therapies (ST) offer promising survival benefits for colorectal liver metastases (CRLM), but outcomes hinge on careful patient selection. Identifying candidates with favorable tumor biology, treatment response, and preserved functional status is essential for therapeutic success and responsible use of scarce donor organs.
Survival outcomes after LT have improved substantially since 2005, with 5-year overall survival (OS) surpassing 65% and reaching 83% in patients meeting SECA-II criteria [15]. In contrast, ST—the standard of care for unresectable CRLM—is associated with a median OS of 24 months and a 5-year OS of ~10%, particularly in patients with ECOG 0–1, RAS/BRAF wild-type tumors, and left-sided primaries [6].
The SECA-I trial identified predictors of poor post-LT outcomes: largest lesion >5.5 cm, disease progression on ST, pre-transplant CEA >80 µg/L, and <2 years between CRC resection and LT [14]. The Fong Clinical Risk Score (FCRS)—which incorporates nodal status, interval to recurrence, metastasis burden, CEA level, and PET metabolic tumor volume (MTV)—has further refined patient selection. Patients with an Oslo score of 0 or FCRS of 1 achieved a 10-year OS of 80%. A PET-MTV <70 cm² was associated with a 5-year OS of 66.7%, compared to 26.6% in patients with MTV >70 cm² [22]. Additional adverse prognostic indicators include tumor burden score ≥9, ≥9 liver lesions, right-sided tumors, and elevated CEA levels.
The SECA-II and TransMet trials applied more stringent selection criteria. SECA-II required stable disease on first-line ST, absence of BRAF V600E mutations, ≤3 chemotherapy lines, and favorable tumor profiles, achieving a 5-year OS of 83%. In TransMet, 5-year OS was 56.6% with LT plus ST versus 12.6% with ST alone (HR 0.37; p=0.0003), underscoring the survival advantage of rigorous selection.
In 2021, the International Hepato-Pancreato-Biliary Association (IHPBA) issued guidelines recommending LT only for patients with liver-limited, unresectable disease, ≥6 months of disease control on ST, R0 resection of the primary tumor, and no evidence of locoregional recurrence [23]. Exclusion criteria include high-risk molecular features (e.g., BRAF V600E, TP53/RAS co-mutations, MSI-high status) [23]. Relative contraindications include sarcopenia, N2 lymph node involvement, and rising CEA. PET-based parameters such as MTV and total lesion glycolysis are validated prognostic markers.
A summary of key studies and selection criteria is provided in Table 1. Collectively, these data support LT as a viable option in selected patients with CRLM and emphasize the importance of structured, evidence-based selection frameworks to optimize outcomes and donor organ use.
Immunotherapy and Transplant Compatibility
Immunotherapy has transformed the treatment landscape for microsatellite instability-high (MSI-high) and mismatch repair-deficient (dMMR) CRC. In the CheckMate 142 trial, immune checkpoint inhibitors achieved 24-month progression-free survival (PFS) and overall survival (OS) rates of 74% and 79%, respectively [24]. However, their use in LT recipients remains limited due to a high risk of allograft rejection. Immune activation induced by checkpoint blockade can override maintenance immunosuppression and lead to acute or chronic rejection, often with irreversible graft loss.
Standard immunosuppressive regimens, including calcineurin inhibitors, are essential to prevent rejection but carry substantial risks, such as nephrotoxicity, secondary malignancies, and increased recurrence of certain cancers, including the primary malignancy [25]. These risks complicate the integration of immunotherapy into post-transplant care and highlight the need for alternative strategies or refined immunosuppressive protocols. Ongoing studies are investigating ways to balance immune surveillance with graft tolerance, which may eventually broaden the therapeutic window for immunotherapy in transplant recipients.
Ethical and Allocation Considerations
The use of scarce deceased donor livers for colorectal liver metastases (CRLM) presents ethical and allocation challenges. Unlike hepatocellular carcinoma (HCC), where biologically validated selection criteria such as the Milan, UCSF, and Tokyo guidelines are well established, CRLM selection primarily relies on imaging and clinical judgment. These HCC frameworks reflect the Metroticket paradigm, in which increasing tumor burden predicts lower post-transplant survival [26]. In contrast, CRLM patients often have low MELD scores, limiting their access to transplantation under the current allocation model [23].
To address these disparities, proposed solutions include MELD exception pathways, living donor liver transplantation (LDLT), and innovative hybrid approaches such as the RAPID procedure (Resection and Partial Liver Transplantation with Delayed Total Hepatectomy) [27]. These strategies can expand access while reducing dependence on the deceased donor pool. However, LDLT introduces ethical complexities regarding donor safety. Safe implementation requires a graft-to-recipient weight ratio >0.8% (potentially acceptable down to 0.6% in select cases), low hepatic steatosis, and adequate remnant liver volume for the donor [28].
Deceased donor LT remains limited by chemotherapy timing, waitlist dropout, and prolonged allocation delays [28]. Balancing equity, utility, and donor risk is critical as the field evolves toward broader application of LT for CRLM within an ethically sustainable framework.
Innovations in Organ Utilization
Expanding the donor liver pool is essential to improving access to transplantation for patients with unresectable colorectal liver metastases (CRLM), many of whom remain ineligible under current allocation models due to low MELD scores. Surgical innovations such as living donor liver transplantation (LDLT) and split-liver transplantation (split-LT) have emerged as effective alternatives. In a cohort of LDLT recipients with unresectable CRLM, Kaltenmeier et al. reported a mean recurrence-free survival of 2.2 years and an overall survival (OS) of 3 years, with low recurrence rates that were generally manageable [29]. Settmacher et al. described a novel two-stage transplantation strategy involving an initial left lateral segment graft from a living donor followed by an extended right lobe from a deceased donor. This approach achieved a 1-year OS of 85% and >90% graft regeneration by 3 months [30].
Technological advances in machine perfusion (MP) have further improved graft viability and utilization, particularly for extended-criteria donor (ECD) livers. Hypothermic oxygenated perfusion (HOPE) reduces ischemia-reperfusion injury and lowers the incidence of post-transplant complications [31]. Normothermic machine perfusion (NMP) allows functional assessment of the graft ex vivo, enhances mitochondrial activity, and facilitates safe use of marginal organs [32]. In the VITTAL trial, 70% of livers initially deemed unsuitable were successfully transplanted following NMP, with favorable short-term outcomes [33]. Emerging platforms such as MP Plus integrate adjunctive repair protocols to rehabilitate ECD grafts, while also reducing biliary complications—further extending the clinical utility of MP in challenging donor scenarios [31].
Together, these innovations offer promising avenues to overcome organ scarcity, improve equity in access, and enhance outcomes for patients undergoing liver transplantation for CRLM.
Biomarkers and Predictive Tools
Advances in molecular diagnostics are reshaping LT selection for CRLM, enabling more precise, biology-driven decision-making. While standard post-treatment surveillance relies on cross-sectional imaging and carcinoembryonic antigen (CEA) monitoring, no single biomarker has yet achieved universal adoption.
Emerging liquid biopsy platforms—including circulating tumor DNA (ctDNA), cell-free DNA (cfDNA), microRNA, and tumor-derived exosomes—offer dynamic, non-invasive assessment of tumor burden and biology. Among these, ctDNA has shown particularly strong predictive value. A meta-analysis by Wang et al. demonstrated that ctDNA positivity is significantly associated with recurrence risk (relative risk 4.65; hazard ratio 9.14) [34].
Other predictive markers include mutations in KRAS/NRAS and BRAF V600E, tumor mutational burden, and imaging-based radiomic parameters such as metabolic tumor volume (MTV) and total lesion glycolysis on PET/CT. These factors independently correlate with post-transplant outcomes [35]. Incorporating such biomarkers into composite scoring systems or machine learning algorithms may substantially refine candidate selection and improve long-term success.
Conclusion
Liver transplantation for unresectable CRLM now achieves 5-year survival outcomes comparable to hepatocellular carcinoma and far superior to systemic therapy alone. These gains depend on rigorous selection criteria that integrate anatomical, molecular, and metabolic parameters. Concurrent advances in organ preservation, surgical innovation, LDLT, and machine perfusion are broadening access to transplant. Future priorities include validating predictive models, standardizing the integration of biomarkers, and conducting prospective, multicenter trials to ensure optimal outcomes and equitable access to care.
Author Contributions
Dr. Demirors: conceptualized and designed the study, contributed to literature review, data interpretation, and manuscript drafting. All authors critically revised the manuscript for important intellectual content and approved the final version for submission. Dr. Sethi: contributed to literature review, data interpretation, and manuscript drafting. Dr. Molinari: conceptualized the study, data interpretation and manuscript editing. Dr. Abiha Abdullah: contributed to the literature review and manuscript drafting. Dr. Charbel Elias: contributed to the literature review and manuscript drafting. Frank Spitz: contributed to the literature review and manuscript drafting. Jason Mial-Anthony: contributed to the literature review and manuscript drafting. Dr. Godwin Packiaraj: contributed to the literature review and manuscript drafting. Dr. Sabin Subedi: contributed to the literature review and manuscript drafting. Dr. Shwe Han: contributed to the literature review and manuscript drafting. Dr. Timothy Fokken: contributed to the literature review and manuscript drafting.
Funding
No financial support was received for the current study.
Acknowledgments
The authors thank the staff and colleagues from the University of Pittsburgh, Starzl Transplant Institute for their support and contributions to the development of this manuscript.
Conflicts of Interest
All authors declare no conflict of interest.
Abbreviations
| CRC | colorectal cancer |
| CRLM | colorectal liver metastases |
| LT | liver transplantation |
| ST | systemic therapy |
| OS | overall survival |
| DFS | disease-free survival |
| PFS | progression-free survival |
| HCC | hepatocellular carcinoma |
| NET | neuroendocrine tumors |
| UNOS | United Network for Organ Sharing |
| SECA | Secondary Cancer |
| IHPBA | International Hepato-Pancreatic Biliary Association |
| ECOG | Eastern Cooperative Oncology Group |
| CEA | Carcinoembruonic Antigen |
| FCRS | Fong Clinical Risk Score |
| PET | Positron Emission Tomography |
| MTV | Metabolic Tumor Volume |
| MSI | Microsatellite Instability |
| dMMR | Deficient Mismatch Repair |
| MELD | Model for End-Stage Liver Disease |
| LDLT | Live Donor Liver Transplantation |
| RAPID | Resection and Partial Liver Transplantation with Delayed Total Hepatectomy |
| MP | Machine Perfusion |
| ECD | Extended-criteria Donor |
| HOPE | Hypothermic Oxygenated Perfusion |
| NMP | Normothermic Machine Perfusion |
| ctDNA | Circulating Tumor DNA |
| cfDNA | Cell-free DNA |
| HR | Hazard ratio |
| RR | Relative risk |
| UCSF | University of California San Francisco |
| VITTAL | Viability Testing and Transplantation of Marginal Livers |
References
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef]
- Zhou H, Liu Z, Wang Y, Wen X, Amador EH, Yuan L, et al. Colorectal liver metastasis: molecular mechanism and interventional therapy. Signal Transduct Target Ther. 2022, 7, 70. [Google Scholar] [CrossRef]
- Varley R, Tarazi M, Dave M, Mobarak S, Stott MC, Baltatzis M, et al. Liver Transplantation for Non-Resectable Liver Metastases from Colorectal Cancer: A Systematic Review and Meta-Analysis. World J Surg. 2021, 45, 3404–3413. [Google Scholar] [CrossRef] [PubMed]
- McFadden NR, Perry LM, Ghalambor TJ, Langan RC, Gholami S. Locoregional Liver-Directed Therapies to Treat Unresectable Colorectal Liver Metastases: A Review. Oncology (Williston Park) 2022, 36, 108–114. [Google Scholar]
- Tasoudis PT, Ziogas IA, Alexopoulos SP, Fung JJ, Tsoulfas G. Role of liver transplantation in the management of colorectal liver metastases: Challenges and opportunities. World J Clin Oncol. 2021, 12, 1193–1201. [Google Scholar] [CrossRef]
- Bachler JL, Khan GN, Wollner IS, Philip PA. Treatment of Unresectable and Resectable Stage IV Colorectal Cancer. Clinical advances in hematology & oncology: H&O 2024, 22, 455–463. [Google Scholar]
- Liu W, Liu J-M, Wang K, Wang H-W, Xing B-C. Recurrent colorectal liver metastasis patients could benefit from repeat hepatic resection. BMC surgery 2021, 21, 1–10. [Google Scholar]
- Ziemlewicz TJ, Critchfield JJ, Mendiratta-Lala M, Wiggermann P, Pech M, Serres-Creixams X, et al. The #HOPE4LIVER single-arm Pivotal Trial for Histotripsy of Primary and Metastatic Liver Tumors: 1-year Update of Clinical Outcomes. Ann Surg.
- Tang W, Ren L, Liu T, Ye Q, Wei Y, He G, et al. Bevacizumab plus mFOLFOX6 versus mFOLFOX6 alone as first-line treatment for RAS mutant unresectable colorectal liver-limited metastases: the BECOME randomized controlled trial. Journal of Clinical Oncology 2020, 38, 3175–3184. [Google Scholar] [CrossRef]
- Huang G, Song W, Zhang Y, Yu J, Lv Y, Liu K. Liver transplantation for intrahepatic cholangiocarcinoma: a propensity score-matched analysis. Scientific Reports 2023, 13, 10630. [Google Scholar] [CrossRef]
- Kulik L, Heimbach JK, Zaiem F, Almasri J, Prokop LJ, Wang Z, et al. Therapies for patients with hepatocellular carcinoma awaiting liver transplantation: a systematic review and meta-analysis. Hepatology 2018, 67, 381–400. [Google Scholar] [CrossRef]
- Goldaracena N, Gorgen A, Sapisochin G. Current status of liver transplantation for cholangiocarcinoma. Liver Transplant 2018, 24, 294–303. [Google Scholar] [CrossRef]
- Citterio D, Coppa J, Sposito C, Busset MDD, Virdis M, Pezzoli I, et al. The role of liver transplantation in the treatment of liver metastases from neuroendocrine tumors. Current Treatment Options in Oncology 2023, 24, 1651–1665. [Google Scholar] [CrossRef]
- Hagness M, Foss A, Line P-D, Scholz T, Jørgensen PF, Fosby B, et al. Liver transplantation for nonresectable liver metastases from colorectal cancer. Annals of surgery 2013, 257, 800–806. [Google Scholar] [CrossRef]
- Dueland S, Syversveen T, Solheim JM, Solberg S, Grut H, Bjørnbeth BA, et al. Survival following liver transplantation for patients with nonresectable liver-only colorectal metastases. Annals of surgery 2020, 271, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Andres A, Oldani G, Berney T, Compagnon P, Line P-D, Toso C. Transplantation for colorectal metastases: on the edge of a revolution. Translational gastroenterology and hepatology 2018, 3, 74. [Google Scholar] [CrossRef] [PubMed]
- Adam R, Piedvache C, Chiche L, Adam JP, Salamé E, Bucur P, et al. Liver transplantation plus chemotherapy versus chemotherapy alone in patients with permanently unresectable colorectal liver metastases (TransMet): results from a multicentre, open-label, prospective, randomised controlled trial. The Lancet 2024, 404, 1107–1118. [Google Scholar] [CrossRef] [PubMed]
- Dawood ZS, Brown ZJ, Munir MM, Waqar U, Rawicz-Pruszynski K, Endo Y, et al. Outcomes of liver transplant for colorectal liver metastasis: a systematic review and meta-analysis. J Gastrointest Surg 2024, 28, 1943–1950. [Google Scholar] [CrossRef]
- Schepers EJ, Hartman SJ, Whitrock JN, Quillin RC. Liver transplantation for colorectal liver metastases. Surgical Clinics 2024, 104, 227–242. [Google Scholar]
- Sonbol MB, Siddiqi R, Uson Jr PLS, Pathak S, Firwana B, Botrus G, et al. The role of systemic therapy in resectable colorectal liver metastases: systematic review and network meta-analysis. The Oncologist 2022, 27, 1034–1040. [Google Scholar] [CrossRef]
- Krishnan S, Joshi B, Keith J, Frazier R, Kalinowska B, Choi JS, et al. MiNK-215, an IL-15 armored FAP-targeting CAR iNKT cell therapy, effectively treats human organoid models of treatment-refractory MSS colorectal cancer (CRC) liver metastases. Cancer Research, 1331.
- Wu F, Cao G, Lu J, Ye S, Tang X. Correlation between 18F-FDG PET/CT metabolic parameters and microvascular invasion before liver transplantation in patients with hepatocellular carcinoma. Nuclear Medicine Communications 2024, 45, 1033–1038. [Google Scholar] [CrossRef]
- Malik AK, Mahendran B, Lochan R, White SA. Liver Transplantation for Nonresectable Colorectal Liver Metastases (CRLM). Indian Journal of Surgical Oncology 2024, 15 (Suppl. S2), 255–260. [Google Scholar] [CrossRef] [PubMed]
- Overman MJ, Gelsomino F, Aglietta M, Wong M, Miron MLL, Leonard G, et al. Nivolumab plus relatlimab in patients with previously treated microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: the phase II CheckMate 142 study. Journal for immunotherapy of cancer 2024, 12, e008689. [Google Scholar] [CrossRef] [PubMed]
- Luft, FC. Calcineurin inhibition, cardiovascular consequences, vascular resistance, and potential responses. Acta Physiologica 2024, 240, e14084. [Google Scholar] [CrossRef] [PubMed]
- Barreto SG, Strasser SI, McCaughan GW, Fink MA, Jones R, McCall J, et al. Expansion of liver transplantation criteria for hepatocellular carcinoma from Milan to UCSF in Australia and New Zealand and justification for Metroticket 2.0. Cancers 2022, 14, 2777.
- Coubeau L, Foguenne M, Marique L, Bonaccorsi Riani E, Ciccarelli O. RAPID-type auxiliary liver transplantation for unresectable colorectal liver metastases: A first-stage surgical video. Annals of surgical oncology 2025, 32, 2300–2301. [Google Scholar] [CrossRef]
- Ayoub I, Sharshar M, Shoreem H, Osman M, El-Ella KA, Uemoto S. Outcome and challenges of left-lobe living-donor liver transplantation in adults. The Egyptian Journal of Surgery 2021, 40, 1328–1337. [Google Scholar]
- Kaltenmeier C, Geller DA, Ganesh S, Tohme S, Molinari M, Tevar A, et al. Living donor liver transplantation for colorectal cancer liver metastases: Midterm outcomes at a single center in North America. American Journal of Transplantation 2024, 24, 681–687. [Google Scholar] [CrossRef]
- Settmacher U, Ali-Deeb A, Coubeau L, Cillo U, Line P-D, Guba M, et al. Auxilliary liver transplantation according to the RAPID procedure in noncirrhotic patients: technical aspects and early outcomes. Annals of Surgery 2023, 277, 305–312. [Google Scholar] [CrossRef]
- Schlegel A, Mueller M, Muller X, Eden J, Panconesi R, von Felten S, et al. A multicenter randomized-controlled trial of hypothermic oxygenated perfusion (HOPE) for human liver grafts before transplantation. Journal of hepatology 2023, 78, 783–793. [Google Scholar] [CrossRef]
- Meszaros AT, Hofmann J, Buch ML, Cardini B, Dunzendorfer-Matt T, Nardin F, et al. Mitochondrial respiration during normothermic liver machine perfusion predicts clinical outcome. EBioMedicine 2022, 85, 104311. [Google Scholar] [CrossRef]
- Mergental H, Laing RW, Kirkham AJ, Clarke G, Boteon YL, Barton D, et al. Discarded livers tested by normothermic machine perfusion in the VITTAL trial: Secondary end points and 5-year outcomes. Liver Transplant 2024, 30, 30–45. [Google Scholar] [CrossRef]
- Wang R, Zhao A, Cao N, Li Z, Zhang G, Liu F. The value of circulation tumor DNA in predicting postoperative recurrence of colorectal cancer: a meta-analysis. International Journal of Colorectal Disease, 1463.
- Stern NM, Mikalsen LTG, Dueland S, Schulz A, Line PD, Stokke C, et al. The prognostic value of [18F] FDG PET/CT texture analysis prior to transplantation for unresectable colorectal liver metastases. Clinical Physiology and Functional Imaging 2025, 45, e12908. [Google Scholar] [CrossRef]
- Smedman TM, Line PD, Hagness M, Syversveen T, Grut H, Dueland S. Liver transplantation for unresectable colorectal liver metastases in patients and donors with extended criteria (SECA-II arm D study). BJS open 2020, 4, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Toso C, Marques HP, Andres A, Sousa FC, Adam R, Kalil A, et al. Liver transplantation for colorectal liver metastasis: Survival without recurrence can be achieved. Liver Transplant 2017, 23, 1073–1076. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Alejandro R, Ruffolo LI, Sasaki K, Tomiyama K, Orloff MS, Pineda-Solis K, et al. Recipient and donor outcomes after living-donor liver transplant for unresectable colorectal liver metastases. JAMA surgery 2022, 157, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Sasaki K, Ruffolo LI, Kim MH, Fujiki M, Hashimoto K, Imaoka Y, et al. The current state of liver transplantation for colorectal liver metastases in the United States: a call for standardized reporting. Annals of Surgical Oncology 2023, 30, 2769–2777. [Google Scholar] [CrossRef]
- Solheim JM, Dueland S, Line P-D, Hagness M. Transplantation for nonresectable colorectal liver metastases: long-term follow-up of the first prospective pilot study. Annals of Surgery 2023, 278, 239–245. [Google Scholar] [CrossRef]
Figure 1.
Example of metastatic colorectal liver disease demonstrating bilobar and multifocal involvement, precluding curative hepatic resection due to insufficient future liver remnant.
Figure 1.
Example of metastatic colorectal liver disease demonstrating bilobar and multifocal involvement, precluding curative hepatic resection due to insufficient future liver remnant.
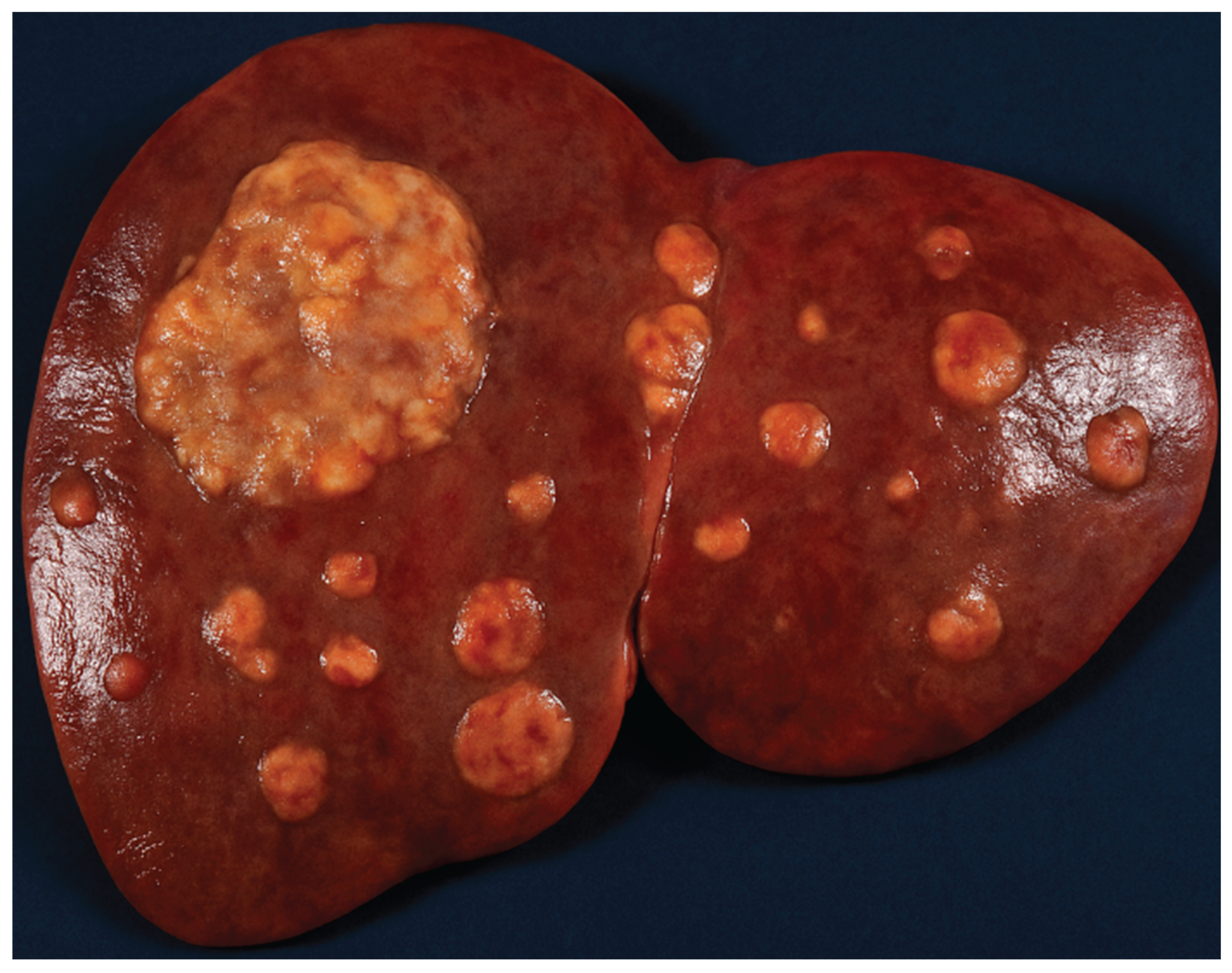

Table 1.
Comparison of Studies on Liver Transplantation in Non-resectable Colorectal Liver Metastases [14,15,17,29,36,37,38,39,40].
| Authors, Year of Publication, Reference | Time Period | Number of Patients | Study Design | Selection Criteria | Outcomes | Recurrence Rate | Comments |
|---|---|---|---|---|---|---|---|
| Hagness et al. 2013 SECA-I trial [14] | 2006-2011 | n=21 | Prospective | · Resected primary CRC · ≥ 6 weeks of pre-LT chemotherapy · Liver-only CLMs · CEA 1–2,000 µg/L · Largest tumor 28–130 mm · Metabolic tumor volume (MTV) at LT: 0–874 cm³ · No extrahepatic disease |
5-yr OS 60 % | 19 / 21 (90 %) | · No chemotherapy response requirement · Wide CEA range · Larger tumor size allowed · Excluded any extrahepatic disease |
| Dueland et al. 2020 SECA-II trial [15] | 2012–2016 | n=15 | Prospective | · Resected primary CRC · Partial response after 6 weeks pre-LT chemo · Liver-only CLMs · Negative pre-LT colonoscopy · No lesion > 10 cm · CEA 1–30 µg/L · Largest tumor 3–47 mm · Metabolic tumor volume at LT: 0–140 cm³ |
5-yr OS 83 % | 8 / 15 (53.3 %) | · Required chemotherapy response · Tighter CEA range · Smaller maximum tumor size |
| Smedman et al. 2020 SECA-III Arm D [36] |
2014–2018 | n=10 | Prospective | · Same as SECA-II (resected primary; response to 6 weeks chemo; liver-only; neg. colonoscopy; no tumor > 10 cm) · Allowed resectable lung mets · CEA 2–4,346 µg/L · MTV at LT: 0–201 cm³ |
2-yr OS 43 % | 8 / 10 (80 %) | · Included resectable lung metastases · Much higher allowable CEA range |
| Toso et al. 2017 [37] | 1995–2015 | n=12 | Retrospective | · Resected primary CRC · ≥ 1/12 had partial response to pre-LT chemo; one patient received intraoperative chemotherapy · Median CEA 16.9 µg/L · Two patients with lesions > 5 cm · Presumed liver-only disease |
5-yr OS 50 % | 6 / 12 (50 %) | · One patient received intraoperative chemotherapy · No strict size cutoff (lesions > 5 cm allowed) |
| Hernández-Alejandro et al. 2022 [38] | 2017–2021 | n=10 | Retrospective | · Followed IHPBA LT guidelines · Resected primary CRC · Median CEA 1.6–56.4 µg/L · Included KRAS-mutated cases (3 patients) · Liver-only disease; no explicit size thresholds |
1.5-yr OS 100 % | 3 / 10 (30 %) | · IHPBA consensus criteria · No size or response cutoffs · KRAS mutations allowed |
| Sasaki et al. 2023 [39] | 2017–2022 | n=46 | Retrospective | · Resected primary CRC · Unresectable liver-only metastases · No other selection criteria specified |
3-yr OS 60.4 % | 10 / 46 (22 %) | · Broad inclusion: only “liver-only” requirement |
| Kaltenmeier et al. 2023 [38] | 2019–2022 | n=10 | Retrospective | · Resected primary CRC · 6–12 wk pre-LT chemo with stable disease or partial response · Negative pre-LT colonoscopy · CEA < 100 µg/L · 5 patients had lesions > 5 cm · Liver-only disease |
1.5-yr OS 100 % | 3 / 10 (30 %) | · Required chemotherapy response · Allowed some lesions > 5 cm if chemo-responsive · Moderate CEA cutoff |
| Solheim et al. 2023 (SECA-I/II; 10-year follow-up results) [40] | 2006–2012 | n=23 | Prospective | · Unresectable liver-only CRC mets, complete radical resection of primary tumor · ECOG 0–1 · ≥ 6 weeks of chemo · No extrahepatic disease on CT/PET-CT · Exclusions: > 10 % weight loss; LT contraindications; other malignancies; BMI > 30 |
5-yr OS 75 %; 10-yr OS 50 % | 23 / 23 (100 %) | · Only unresectable liver-only requirement · Added performance & BMI/exclusion criteria |
| Adam et al. 2024 TRANSMET trial [17] | 2016–2021 | n=94 | Prospective | · Resected primary CRC · ECOG 0–1 · No local recurrence on colonoscopy within past 12 months · No extrahepatic disease · No BRAF mutations · CEA < 80 µg/L or ≥ 50 % decrease from baseline · Liver-only metastases |
5-yr OS 73 % | 28 / 47 (60 %) | · Added colonoscopy requirement · Excluded BRAF-mutated tumors · CEA < 80 µg/L or ≥ 50 % decrease from baseline criteria |
Legend: BMI, Body Mass Index; CEA, Carcinoembryonic Antigen; CLMs, Colorectal Liver Metastases; CRC, Colorectal Cancer; ECOG, Eastern Cooperative Oncology Group; IHPBA, International Hepato-Pancreato-Biliary Association; LT, Liver Transplantation; MTV, Metabolic Tumor Volume; OS, Overall Survival.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



