
Submitted:
02 July 2025
Posted:
03 July 2025
You are already at the latest version
Abstract
Routine collection of Patient-Reported Outcomes (PRO) can enhance patient-pharmacist communication and identify medication-related concerns. This study aims to (1) explore patients’ experiences with RxTalk™, an electronic PRO tool; (2) describe the influence of RxTalk™ on patients’ attributes and the dynamics of communication; (3) identify suggestions for future improvements. This study is part of a pilot randomized controlled trial in which patients completed questions on RxTalk™ in the pharmacy before they spoke with the pharmacist. Patients’ interaction with pharmacists was tape-recorded and analyzed, and phone interviews were conducted with patients within one week. We integrated data from RxTalk™, observations, taped encounters, and interviews to provide a thicker description of patients’ experiences with RxTalk™ and its impact on their communication behavior. 70% of patients found RxTalk™ easy to use, and 59% perceived RxTalk™ as very useful to extremely useful. Triangulated findings show that RxTalk™ met patients’ social and informational needs, improved their communication skills, and cultivated a sense of privacy to share concerns. Furthermore, RxTalk™ validated the appropriateness of reporting any health and medication concerns. Given that patients had a positive experience with RxTalk™, pharmacists should consider integrating PRO tools into their daily services to improve patient interactions and quality of care.
Keywords:
patient reported outcomes
; PRO
; patient-pharmacist communication
; patient-centered communication
; community pharmacy
; digital health interventions
; medication adherence
; medication problems
1. Background
Patient-reported outcomes (PRO) are patients’ reports of how they feel, think, and function with regard to their health without the interpretation of clinicians [1]. The collection of PRO in healthcare settings is associated with better symptom monitoring, shared decision-making, and tailored patient care [2]. Acknowledging the value of routine collection of PRO, regulatory and federal agencies such as the Agency for Healthcare Quality and Research and The Office of the National Coordinator for Health Information Technology consider research related to patient-generated health data among their top priorities [3,4].
As community pharmacists are at the forefront of the healthcare system and have more frequent interactions with patients, using electronic PRO tools in pharmacies holds a significant advantage for both patients and pharmacists. In the fast-paced pharmacy environment, patients can share their medication experiences efficiently and be more involved in the counseling [5]. PRO tools can support pharmacists’ roles through early identification and management of medication-related problems, eventually leading to improved medication adherence and health outcomes. Additionally, they can overcome barriers to effective patient-pharmacist interaction, such as limited time and lack of privacy [6]. Although the utilization of PRO to guide the management and monitoring of health conditions is not new in pharmacy-related research, little research has evaluated how integrating PRO into medication consultations can influence the interaction between patients and pharmacists [7-9].
Using a randomized controlled design, we explored the impact of RxTalk™, a tablet-based PRO tool, on patient-pharmacist interaction in a community pharmacy setting that wished to try out a new service to improve the quality of pharmacy consultations [10]. Patients in the intervention group used RxTalk™ before medication consultations, while those in the control group received standard care and did not use RxTalk™. After intervention patients completed the questions in RxTalk™, the researcher copied key information from RxTalk™ into a paper-based summary sheet, including patients’ PRO scores and types of health and/or medication concerns. Both patients and pharmacists received a copy of the summary sheet and were encouraged to use it during consultation. Their consultation was then audio recorded. These audio recordings documented that during the consultation with pharmacists, patients who used RxTalkTM were more engaged and expressed significantly more concerns compared to the control group [10].
Since the examination of real-world medication consultations through audio-recording conversations is relatively limited in pharmacy literature [6], this study offers an additional novel opportunity to explore the mechanism underlying the intervention’s impact on promoting patient engagement and expressing concerns. Guided by communication theories and using multiple data sources, a second set of analyses was done in this paper to help further our understanding of why RxTalk was effective. These analyses could inform the development and refinement of future electronic tools to collect PROs that are easy to use, meet patients’ needs, and help pharmacists provide better care.
Thus, our study aims in this paper are to (1) explore patients’ perceptions of RxTalk™ and describe their responses in the tool, (2) describe the influence of RxTalk™ on patients’ attributes and the dynamics of communication, and (3) solicit patients’ suggestions for future improvements.
2. Materials and Methods
2.1. Intervention Description
RxTalk™ was developed using Qualtrics© 2023 (Qualtrics, Provo, UT). It includes an adaptive questionnaire that tailors questions to each participant based on their responses to previous questions. RxTalk™ assesses the patient’s goals for the pharmacy visit, as well as their health and medication concerns. It also asks about the medication the patient wishes to discuss with their pharmacist, followed by two validated PRO measures related to medication adherence: the Brief Medication Questionnaire (BMQ) [11] and the Merck Adherence Estimator [12]. A third PRO measure included in RxTalk™ is the Global Health Rating, which assesses patients’ overall perception of their health [13]. The tool ends with a question that encourages patients to report any additional questions/concerns about their health conditions. A full description of the intervention is published elsewhere [10].
2.2. Study Design
This study employs a multi-method approach, utilizing data collected from RxTalk™ users in the intervention group of the pilot randomized controlled trial [10]. Multi-method studies offer numerous advantages for program evaluation, such as providing a comprehensive and richer understanding of the program under investigation, overcoming the weaknesses inherent in single-method studies, and allowing the triangulation of findings [14]. Data were collected from one community pharmacy between March and May 2023. Patients enrolled in the study were adults with at least one chronic illness that requires routine prescription medication(s).
2.3. Theoretical Framework and Constructs
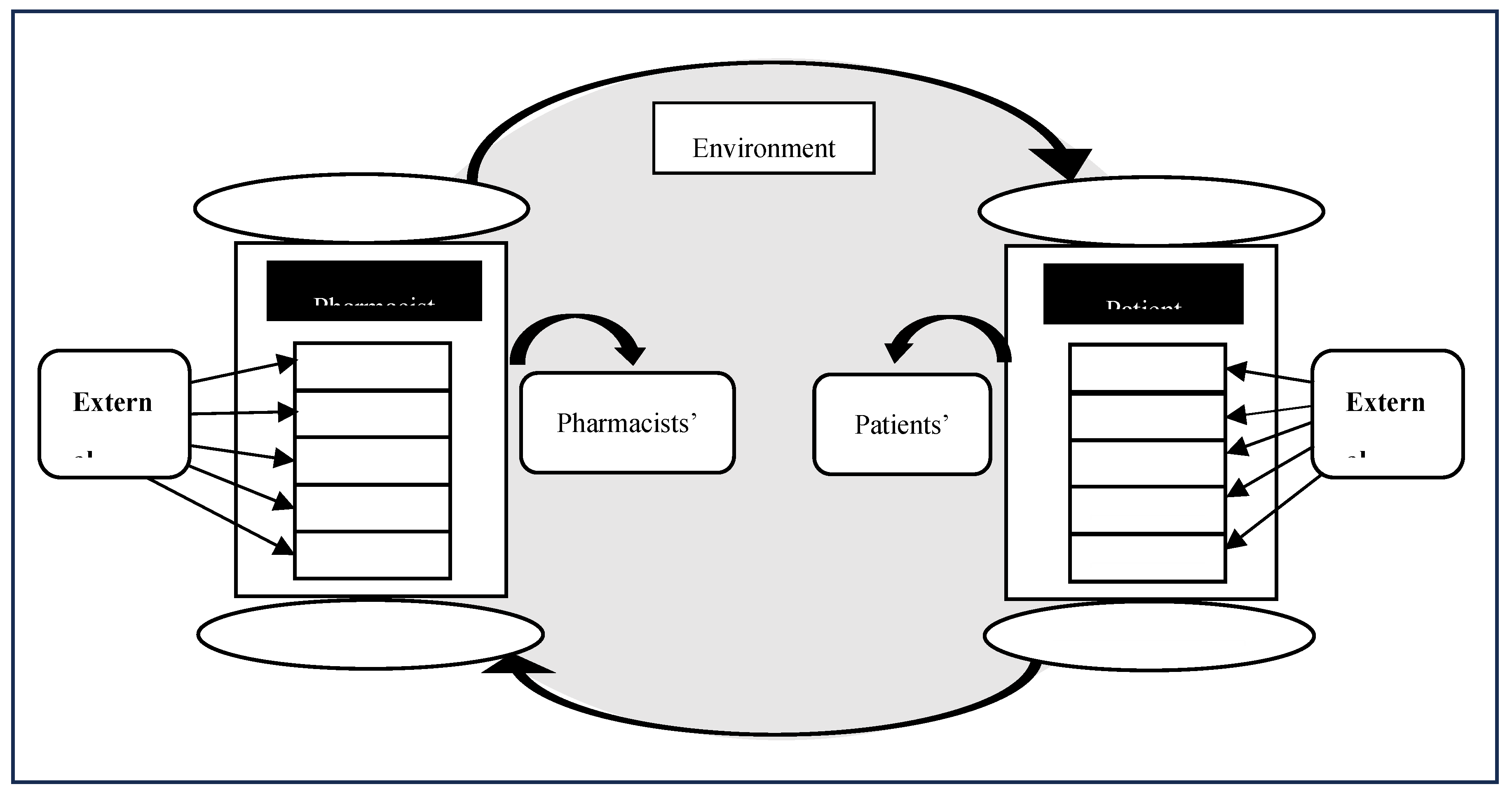
The Conceptual Framework for Patient-Provider Communication (PPC) guided our data collection, analysis, and interpretation (Figure 1). According to PPC, communication is a multidimensional process that includes relationship and content and occurs in a complex environment [15]. The success of communication between patients and clinicians depends on enabling both parties to address their goals through conveying and interpreting messages. The model also emphasizes the role of participants’ attributes such as needs, beliefs, values, skills, and emotions in the communication process. Individuals’ needs include basic human needs and secondary needs (e.g. need for validation). Participants’ values encompass principles and standards that guide their behavior. Skills include participants’ ability to communicate, and beliefs are their perceptions of the world and specifics of a situation. Emotions can have either a negative or a positive valence.
Figure 1.
Conceptual framework of patient-pharmacist communication [15]
Figure 1.
Conceptual framework of patient-pharmacist communication [15]
2.4. Data sources and Analysis
Data used in this study were collected and analyzed using different methods and analytical techniques described in Table 1. All consultations were audio-recorded on the day of enrollment using an encrypted audio recorder placed on the counter. Two coders (BQ and BC) coded the interactions using a validated tool after establishing interrater reliability [16]. Coding focused on identifying utterances that describe active patient participation, including question-asking, concern expression, and assertive statements. Additionally, we identified the type of health and medication concerns that were shared by patients in the consultation to compare them to patients’ responses in RxTalk™.
Semi-structured interviews were conducted with patients over the phone within one week of enrollment and visit. The interviews were audiorecorded and transcribed verbatim and deidentified for later analysis by the lead researcher (BQ). Analysis was aided by qualitative analysis software (NVivo, 2020) [17]. Two coders (BQ and SM) coded the interview transcripts using a hybrid approach of inductive and deductive coding. First, the lead researcher conducted a first pass on all interviews to familiarize herself with the data. Then, a few transcripts were read word by word. Statements that described information related to areas of interest and constructs of PPC were highlighted and used to create preliminary codes and develop the initial draft of the codebook. The lead researcher then coded the remaining transcripts in addition to recoding the former transcripts using the codebook. The codes were later sorted into categories based on how they were related. The second coder analyzed the transcripts independently using the codebook, and weekly meetings were conducted to discuss any discrepancies in coding until a consensus was reached.
When available, findings related to patients’ experiences with RxTalk™ were integrated from different data sources to provide a more comprehensive and thicker description. For example, ease of use was determined by integrating researcher observations and interview questions about usability [18].
3. Results
3.1. Baseline Characteristics and RxTalk™ Data
Thirty patients used RxTalk™ as part of the RCT intervention group, and 27 (90%) completed all study activities. All study patients were white, and the majority were females (73.3%) with a mean (SD) age of 54.9 (15.8). Eleven patients had a high school diploma or less (40.7%), and the remainder had some college or higher 16 (59.3%); education data was missing for 3 patients who were lost to follow-up. Most patients were picking up refill prescriptions 21 (70%) when they enrolled in the study.
Half of the patients had hypertension, 43% had chronic pain, 26.7% had mental health conditions, and 20% had diabetes.
In RxTalk™, the patient questionnaire was designed to be adaptive and allowed users to skip questions. Based on that, patients got different screens based on their answers. It first identified patients’ medical conditions and then prompted them to select the condition with the most concerns, if any. Among the 30 patients, 22(73.3%) reported medical condition concerns: 9(40.9%) feared their condition was uncontrolled, and 7(31.8%) cited symptoms or side effects concerns. Patients who indicated that they have “No concerns about their medical condition” were asked specifically about medication issues. This stepwise approach helped capture concerns primarily tied to medications. In total, 8 (30%) patients struggled with side effects, adherence, or other medication-related problems. Finally, when asked to select a medication to complete PRO measures and discuss with the pharmacist, 70% of patients selected medications taken for more than 6 months. Four patients were excluded from the latter adherence analysis since they selected a new medication. Of the 26 remaining patients, 23.1% were nonadherent to their medications according to the BMQ. However, responses to the Merck adherence estimator show that 60% of patients were at moderate to high risk of intentional nonadherence to their medications. Only 6.6% of patients perceived their health as excellent. A full summary of patients’ responses to RxTalk™ can be found in Table 2.
3.2. Perceptions of the RxTalk™ Tool
Twenty-seven (90 %) of patients who used RxTalk™ completed the phone interviews. Patients’ responses to Likert scale usability questions and relevant quotes from probing questions are summarized in Table 3. Types of problems observed while patients used RxTalk™ are described in Table 4.
Most interviewed patients (70.4%) perceived RxTalk™ as easy to use compared to only 2 (7.4%) who perceived it as hard (Table 3). Observational data suggest that 17/30(56.7%) patients required assistance or had minor issues while using RxTalk™ (Table 4). During interviews, many patients appreciated the opportunity to answer questions electronically compared to paper and pencil surveys. Being comfortable with technology, availability of researcher support/assistance, and the simplicity of the tool made the experience easy for patients. Moreover, having to wait for a prescription to get ready facilitated the acceptance of RxTalk™. On the other hand, lack of familiarity with tablet computers, difficulty remembering the name of medications, and the need to reflect on health/medication problems before giving an answer affected patients’ perceptions of RxTalk™ usability.
In terms of future use of RxTalk™, only 11% said they were slightly or not likely to use it in the next 3 months. Many patients recognized RxTalk’s potential to facilitate communication with pharmacists and set the agenda for consultations, noting that these features would encourage them to use the tool again in the future. The small number of patients who had low intention to use RxTalk™ in the future, cited their preference for direct interaction with pharmacists or no perceived need for using RxTalk™ in the absence of health/medication concerns.
3.3. RxTalk™ and the Communication Dynamics
To explore the mechanism by which RxTalk™ influenced patients’ communication behavior of expressing more concerns to pharmacists than did the control group, we examined patients’ goals and expectations, attributes (needs, beliefs, values, skills, and emotions), and perception of the communication context as defined by the PPC framework.
3.3.1. Goals and Expectations
Only 3 patients (10%) reported in RxTalk™ that one of the goals of their current pharmacy visit was to seek consultations on their medications. Despite this, many patients expressed concerns about their health/medications during their subsequent taped encounters, as seen in our previous paper, where significantly more concerns were expressed by RxTalk™ users than by the control group. [10] This suggests that RxTalk™ not only altered patients’ goals, but it also furthered them. For example, one patient (PT47) indicated in RxTalk™ that the goal of her pharmacy visit was limited to picking up prescriptions. However, in the interview, she admitted that she had issues with her medications and was satisfied with the pharmacist's consultation and recommendations.
“He answered all my questions in a satisfactory manner and gave me a couple of suggestions to discuss with my doctor.” PT47
3.3.2. Patient Reflection and Skills to Express Concerns
Patients voiced that answering questions in RxTalk™ prompted them to reflect on their health and medication concerns, bringing these issues to the forefront of their minds. Consequently, they felt more prepared and ready to discuss them in consultations. This suggests that RxTalk™ helped equip patients with the skills and the language that they needed to express their concerns. Also, it reduced the amount of information needed to explain their medication and health-related issues.
“and I thought since you had asked the question, was there one medication that I was concerned about, that kind of then move to the forefront of my mind, that well maybe I can ask him about these things.” PT30
“it made it easier than me having to explain it all to the pharmacist after I filled out the survey.” PT24
3.3.3. Cued Pharmacist to Patient Needs
Patients perceived the summary sheet favorably, articulating that it helped pharmacists become aware of their agenda for that visit and deliver more tailored consultations. This suggests that RxTalk™ improved pharmacists' skills to identify patients’ highest concerns. This has the potential to streamline consultations and reduce the workload for pharmacists during busy hours.
“I think it prepares them when they call you up to pick up your medicine to go over the one thing or two things that you were specific in wanting to know” PT3
Interviewer: “So do you feel that there are certain situations that make you more likely to use it in the future versus other situations?”
Patient: “When it does get crowded, plus, sometimes, even if it's not crowded, they do get a lot of calls. There's a lot of times when someone can't be there.” PT43
3.3.4. Needs
Using RxTalk™ fulfilled patients’ need to connect and feel cared for. They appreciated the opportunity to “talk to the pharmacist” after using RxTalk™, which is not commonly done during refill medication pickup.
“That we got to sit there, talk face to face. Usually, I just go in there and get my medicine and come right back out.” PT26
In addition to relational needs, the personalized consultation that patients received after using RxTalk™ addressed their informational needs and helped them get answers to questions that they never thought to ask any of their other healthcare providers.
“It answered questions that I had for 30 years and just never bothered to ask” PT39
3.3.5. Preferences and Values
Patients’ interviews indicate that RxTalk™ lowered the threshold for sharing concerns and validated the appropriateness of discussing any medication-related issue patients might be experiencing, even if they were minor.
“I think if it would have been a really strong concern, I would have called and talked to them or talked to him at a time when he was, you know, giving me, when I was buying other medicines.” PT30
In the same vein, taped encounters demonstrate that issues that are sensitive for patients to raise, such as mental health, were discussed openly in 6 (20%) of the encounters. The tapes also indicate that patients selected and discussed medications picked up from other pharmacies in 3 (10%) of the taped encounters, as the pharmacist was heard saying the medication was not found in the patients’ profiles. This suggests that the RxTalk™ helped patients overcome their values and beliefs of only discussing medications that are picked up from that pharmacy.
3.3.6. Emotions
A few patients reported that engaging in direct conversations with pharmacists could induce anxiety, particularly if they perceived the pharmacists as busy and not open to interruptions during their work. However, completing the questions in RxTalk™ contributed to alleviating these patients' concerns and fostered their confidence in voicing their concerns and questions through the tablet.
“It's easier to write the answers sometimes on the computer or the tablet because you can be nervous sometimes without asking the pharmacist, especially if they're busy.” PT5
3.3.7. Environmental/ Contextual Factors
Most of the patients, 19 (70.4%), reported that they had a positive experience completing the RxTalk™ questions in the pharmacy's waiting room. The remaining patients, 8 (29.6%), had a negative perception of the limited space and inconvenience in the pharmacy.
“It was probably a pretty good way to do it while I was waiting in order just to fill it out.”PT53
Since the pharmacy had limited privacy and was located in a close-knit community, patients appreciated the ability to type in their concerns and sensitive information without being heard by others. The privacy feature was especially useful for patients employed at the hospital when the pharmacy was crowded and there was a high risk of losing privacy.
“I guess the thing, the privacy, part of it. That I'm able to ask that question, and you know it would have been fine if he was able to respond on it that way”.PT30
3.4. Suggestions for Improvement
3.4.1. RxTalk™ Features
Patients gave a few suggestions about improving the design and content of RxTalk™. Comments included adding more instructions, including a text box under health/medication concerns, to provide more contextual information. Additionally, patients suggested integrating a risk assessment system within RxTalk™, which flags patients who require prompt attention by pharmacists and filters out those with no issues or real concerns.
3.4.2. Setting for Using RxTalk™
For future use, only 8 patients (29.6%) suggested using RxTalk™ in the same way it was used in the study, in the pharmacy waiting area. Most patients, 14 (51.9%), preferred to use it remotely at home using a link sent to their phones or personal computers. Other suggestions included completing the questions in the pharmacy away from traffic, inside patients’ cars in the parking lot, ahead of medication review appointments, or securing the tablet on a kiosk in the pharmacy for better convenience and privacy.
3.4.3. Feedback from Pharmacists
Seventeen patients (63%) expressed their appreciation for receiving feedback through face-to-face interaction with pharmacists to allow bidirectional communication. Some patients were also open to other ways of asynchronous communication for receiving pharmacist feedback, such as text messages, email, pharmacy app, or RxTalk™ itself. One patient suggested having a written document with the pharmacist’s recommendation following the consultation. Lastly, a few patients expressed interest in receiving a phone call from their pharmacist to discuss issues that were recalled later.
4. Discussion
4.1. Discussion
This study is among the first theoretically driven, in-depth evaluations of the experiences of patients with chronic medical conditions with an electronic PRO tool in a community pharmacy setting. One of the strengths of this study is the utilization of multiple data sources to explore how an interaction with an electronic pre-consultation tool can shape patients’ communication with pharmacists. Having RxTalk™ collect PRO data about patients was perceived positively as the tool was quick and straightforward to use, and it gave pharmacists insights into their questions and concerns. The prompt integration of patients’ responses in RxTalk™ into the consultation helped patients see the value of RxTalk™ and how their data was being used by pharmacists, which improved its acceptability. The finding that most patients found RxTalk™ easy and useful becomes even more significant considering that in this rural setting, 40% of the study sample had high school education or less, and many patients expressed a lack of comfort with technology. This suggests that using simple tools, such as survey software loaded onto a touch screen device, has the potential to successfully monitor medication use in rural underserved areas to augment limited staffing resources.
Demonstrating that an intervention is effective is not adequate without exploring how it works, why it works, and under which conditions [10]. The Conceptual Framework for Patient-Provider Communication constructs proved helpful to explore how RxTalk™ influenced patients’ interaction with pharmacists. It helped explain how the PRO assessment tool could influence a complex behavior, such as patient communication about their concerns [19]. Having the written summary for both patient and provider was a key element to cue both the patient and pharmacist during their encounter that a dialogue was expected about patient concerns. Additionally, having RxTalk™ ask a brief set of questions about concerns and behaviors helped patients reflect on and identify their concerns. It gave them language to share these concerns with the pharmacist and validated the appropriateness of discussing long-standing issues and problems not related to the visit. Pharmacists’ perceptions of RxTalk™ and how it influenced and informed their interactions with patients, compared to standard consultations also was positive and will be described in detail in a different paper.
Most patients in this study identified concerns in RxTalk™ with medications they had taken for more than 6 months. This underscores the importance of shifting the focus from simply counseling on new prescriptions to including refill prescriptions. Tools such as RxTalk™ could identify which patients have concerns about refill medications. As adherence decreases over time [20] and adverse effects are prevalent [21], RxTalk™ can help uncover issues through medication use assessment and create more interaction opportunities between patients and pharmacists. This can potentially improve health outcomes for patients with chronic medical conditions. Patients reporting medications refilled from other pharmacy sites in RxTalk™, such as chain pharmacies and mail orders, was an unexpected finding. This highlights that PRO tools can reduce fragmentation in care and contribute to medication reconciliation, especially when implemented in a pharmacy site with strong patient loyalty. This finding will be considered when redesigning RxTalk™ in future studies.
As the management of privacy can be challenging in the busy pharmacy environment [22], RxTalk™ was deemed valuable when patients had concerns about diseases with sensitive connotations like mental health issues and chronic pain, which were discussed in one-third of the encounters. Given the low frequency of the discussions of these conditions in pharmacy consultations, these findings suggest that RxTalk™ helped normalize the dialogue about sensitive conditions and provided a safer, private space for sharing the context of these problems [23,24].
The researcher’s assistance was essential for the successful implementation of RxTalk™. While comprehension issues can be resolved by improving the instructions in future iterations of RxTalk™, technical issues need special consideration. Assigning one pharmacy personnel as a technical support person would encourage patients’ adoption and ensure a seamless experience, especially for older adults and those with limited experience with technology. This aligns with the recommendations from another similar study in clinics, which showed that individual assistance facilitated the uptake and adoption of digital tools [25,26].
This study has several limitations. The study was conducted in a rural setting with a relatively small sample, which limits the generalizability of patients’ experience with RxTalk™ to urban and metropolitan settings. Also, since sampling was not random, it is possible that patients who joined the study were more likely to be receptive to using technology compared to those who didn’t. However, many patients expressed a lack of comfort with technology at the start of using RxTalk™, which reduces the possibility of this risk. Lastly, future studies should invite patients in the control group to use RxTalk™ as a wait list control to make an in-depth comparison between the two groups and rule out any possible confounders.
4.2. Practice Implications
Pharmacies can adopt several strategies to facilitate the integration of PRO tools in their settings and provide tailored consultation to their patients. The reluctance of some patients to use the tool can be addressed by sending pre-visit text messages to patients to inform them about the PRO service, which can alter their expectations of the visit and its duration. The pharmacy team should also introduce the tool using a carefully crafted message emphasizing the importance of monitoring medication use, efficacy, and side effects [27]. For better efficiency, the pharmacy team can utilize a risk-based approach and target at-risk populations such as older adults, patients with polypharmacy or multiple comorbidities, and those with refill gaps in the pharmacy dispensing system [28]. Patients who are typically reserved or hesitant in their communication can also benefit from using such tools [29].
Patients’ preference to complete the PRO assessment remotely before the pharmacy visit can be further explored in areas with better internet connectivity to identify the opportunities, challenges, and overall patient experiences. Studies examining the integration of PRO with patient portals (MyChart; Epic Systems) have demonstrated that patients completing PRO assessments in the comfort of their homes was feasible, well accepted, and contributed to higher contextualization of care [26,30]. Additionally, pharmacies can capitalize on patients’ comfort with existing infrastructure, such as their pharmacy app for patient targeting and PRO collection.
4.3. Conclusion
Using RxTalk™ was perceived positively by patients as it prepared them for the consultation and gave pharmacists insights into their concerns. To expand evidence on the feasibility and acceptability of RxTalk™, future research needs to explore patient experiences in other pharmacy settings, urban locations and include different types of encounters, such as drive-thru visits and videoconferencing consultations.
Author statement
BQ Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Validation; Visualization; Roles/Writing - original draft; and Writing - review & editing; SA: Formal analysis, Writing - review & editing; BC: Conceptualization, Methodology; Project administration; Resources; Validation; Supervision, Writing - review & editing
Supplementary Materials
The following supporting information can be downloaded at: XXXX (Appendix 1. Phone interview protocol)
Funding
This study was funded by the Sonderegger Research Award at the University of Wisconsin-Madison.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of The University of Wisconsin-Madison (2022–1431).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data can be provided by the corresponding author upon request.
Acknowledgement
We gratefully acknowledge the insightful feedback and support provided by Dr. Olufunmilola Abraham and Dr. Olayinka Shiyanbola, which greatly enhanced the quality of this work. We also extend our appreciation to Dr. Jennifer Dykema, Faculty Director of the University of Wisconsin Survey Center, for her invaluable input and assistance with the survey design in Qualtrics.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rothman, M.L.; Beltran, P.; Cappelleri, J.C.; Lipscomb, J.; Teschendorf, B. Patient-Reported Outcomes: Conceptual Issues. Value Heal. 2007, 10, S66–S75. [Google Scholar] [CrossRef]
- Calvert, M.; Kyte, D.; Price, G.; Valderas, J.M.; Hjollund, N.H. Maximising the impact of patient reported outcome assessment for patients and society. BMJ 2019, 364, k5267. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality. Current Priorities: Patient-generated Health Data. https://digital.ahrq.gov/program-overview/directors-corner#current.
- The Office of the National Coordinator for Health Information Technology. National Health IT Priorities for Research: A Policy and Development Agenda. https://www.healthit.gov/topic/scientific-initiatives/national-health-it-priorities-research-policy-and-development-agenda.
- Greenhalgh, J. The applications of PROs in clinical practice: what are they, do they work, and why? Qual. Life Res. 2009, 18, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Qudah, B.; Thakur, T.; Chewning, B. Factors influencing patient participation in medication counseling at the community pharmacy: A systematic review. Res. Soc. Adm. Pharm. 2021, 17, 1863–1876. [Google Scholar] [CrossRef]
- Marra, C.A.; Cibere, J.; Grubisic, M.; Grindrod, K.A.; Gastonguay, L.; Thomas, J.M.; Embley, P.; Colley, L.; Tsuyuki, R.T.; Khan, K.M.; et al. Pharmacist-initiated intervention trial in osteoarthritis: A multidisciplinary intervention for knee osteoarthritis. Arthritis Care Res. 2012, 64, 1837–1845. [Google Scholar] [CrossRef]
- Zuckerman, A.D.; Banks, A.M.; Wawrzyniak, J.; Rightmier, E.; Simonson, D.; Zagel, A.L.; Turco, E.; Blevins, A.; DeClercq, J.; Choi, L. Patient-reported outcomes and pharmacist actions in patients with multiple sclerosis managed by health-system specialty pharmacies. Am. J. Heal. Pharm. 2023, 80, 1650–1661. [Google Scholar] [CrossRef] [PubMed]
- Lemanska, A.; Poole, K.; Manders, R.; Marshall, J.; Nazar, Z.; Noble, K.; Saxton, J.M.; Turner, L.; Warner, G.; Griffin, B.A.; et al. Patient activation and patient-reported outcomes of men from a community pharmacy lifestyle intervention after prostate cancer treatment. Support. Care Cancer 2022, 30, 347–358. [Google Scholar] [CrossRef]
- Qudah, B.; Chewning, B. Exploring the impact of a digital health tool on patients’ interaction with community pharmacists: A pilot randomized controlled study. Res. Soc. Adm. Pharm. 2024, 20, 986–994. [Google Scholar] [CrossRef]
- Svarstad, B.L.; A Chewning, B.; Sleath, B.L.; Claesson, C. The brief medication questionnaire: A tool for screening patient adherence and barriers to adherence. Patient Educ. Couns. 1999, 37, 113–124. [Google Scholar] [CrossRef]
- CA. M. The Adherence Estimator: a brief, proximal screener for patient propensity to adhere to prescription medications for chronic disease.. Curr Med Res Opin 2009;25:215-38.
- McHorney, C.A. The Adherence Estimator: a brief, proximal screener for patient propensity to adhere to prescription medications for chronic disease. Curr. Med Res. Opin. 2009, 25, 215–238. [Google Scholar] [CrossRef]
- Odendaal, W.; Atkins, S.; Lewin, S. Multiple and mixed methods in formative evaluation: Is more better? Reflections from a South African study. BMC Med Res. Methodol. 2016, 16, 173. [Google Scholar] [CrossRef]
- Feldman-Stewart, D.; Brundage, M.D. A conceptual framework for patient–provider communication: a tool in the PRO research tool box. Qual. Life Res. 2008, 18, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Street Jr RL, Millay B. Analyzing patient participation in medical encounters. Health Commun, 2001;13(1):61-73.
- QSR International. NVivo Version 12, 2019, QSR International. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on day month year).
- Amin, M.E.K.; Nørgaard, L.S.; Cavaco, A.M.; Witry, M.J.; Hillman, L.; Cernasev, A.; Desselle, S.P. Establishing trustworthiness and authenticity in qualitative pharmacy research. Res. Soc. Adm. Pharm. 2020, 16, 1472–1482. [Google Scholar] [CrossRef] [PubMed]
- Feldman-Stewart, D.; Brundage, M.D.; Tishelman, C. A conceptual framework for patient–professional communication: an application to the cancer context. Psycho-Oncology 2005, 14, 801–809. [Google Scholar] [CrossRef]
- Krousel-Wood M, Joyce C, Holt E, et al. Predictors of decline in medication adherence: results from the cohort study of medication adherence among older adults. J. Hypertens, 2011;58(5):804-10.
- Thomsen, L.A.; Winterstein, A.G.; S⊘Ndergaard, B.; Haugb⊘Lle, L.S.; Melander, A. Systematic Review of the Incidence and Characteristics of Preventable Adverse Drug Events in Ambulatory Care. Ann. Pharmacother. 2007, 41, 1411–1426. [Google Scholar] [CrossRef] [PubMed]
- Hattingh, H.L.; Emmerton, L.; Tin, P.N.C.; Green, C. Utilization of community pharmacy space to enhance privacy: a qualitative study. Heal. Expect. 2016, 19, 1098–1110. [Google Scholar] [CrossRef]
- Vinay Phokeo, M.Sc., B. Sc.Phm.,, Beth Sproule, Pharm.D., B.Sc.Phm., and, Lalitha Raman-Wilms, Pharm.D., B.Sc.Phm. Community Pharmacists' Attitudes Toward and Professional Interactions With Users of Psychiatric Medication. Psychiatr Serv, 2004;55(12):1434-1436.
- Gardner, D.M.; Murphy, A.L.; Woodman, A.K.; Connelly, S. Community pharmacy services for antidepressant users. Int. J. Pharm. Pr. 2001, 9, 217–224. [Google Scholar] [CrossRef]
- Grossman, L.V.; Creber, R.M.M.; Ancker, J.S.; Ryan, B.; Polubriaginof, F.; Qian, M.; Alarcon, I.; Restaino, S.; Bakken, S.; Hripcsak, G.; et al. Technology Access, Technical Assistance, and Disparities in Inpatient Portal Use. Appl. Clin. Informatics 2019, 10, 040–050. [Google Scholar] [CrossRef]
- Holt, J.M.; Spanbauer, C.; Cusatis, R.; Winn, A.N.; Talsma, A.; Asan, O.; Somai, M.; Hanson, R.; Moore, J.; Makoul, G.; et al. Real-world implementation evaluation of an electronic health record-integrated consumer informatics tool that collects patient-generated contextual data. Int. J. Med Informatics 2022, 165, 104810. [Google Scholar] [CrossRef]
- Steinman, M.A.; Handler, S.M.; Gurwitz, J.H.; Schiff, G.D.; Covinsky, K.E. Beyond the Prescription: Medication Monitoring and Adverse Drug Events in Older Adults. J. Am. Geriatr. Soc. 2011, 59, 1513–1520. [Google Scholar] [CrossRef]
- Lazarou, J.; Pomeranz, B.H.; Corey, P.N. Incidence of Adverse Drug Reactions in Hospitalized Patients: A Meta-Analysis of Prospective Studies. Surv. Anesthesiol. 1999, 43, 53–54. [Google Scholar] [CrossRef]
- Chewning, B.; Schommer, J.C. Increasing Clients' Knowledge of Community Pharmacists' Roles. Pharm. Res. 1996, 13, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Recinos, P.F.; Dunphy, C.J.; Thompson, N.; Schuschu, J.; Urchek, J.L.; Katzan, I.L. Patient Satisfaction with Collection of Patient-Reported Outcome Measures in Routine Care. Adv. Ther. 2017, 34, 452–465. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Data sources and analytic techniques.
| Method | Type of data collected | Analytic technique | Coders |
| Responses in RxTalk™ | Goals of the pharmacy visit, medical conditions, health concerns, medication concerns, name of medication for PRO questions, medication dosing schedule, adherence barrier measures (BMQ [11] , Merck adherence estimator [12] and Global Health scale [13]), additional questions or concerns for pharmacists | Descriptive -frequencies and percentages |
|
| Audio-recorded pharmacy consultations | Names of medications/conditions and medication use barriers discussed during consultations were extracted from the recordings to explore the nature of topics, questions, and concerns raised by patients and pharmacists. |
Descriptive - frequencies and percentages |
One coder (BQ) |
| Observations | Questions and problems encountered by patients while using RxTalk™ were recorded using an observation checklist, which classified issues into technical issues and comprehension issues | Descriptive - Frequencies and percentages |
One coder (BQ) |
| Interviews | Patients’ perceptions of RxTalk™ in terms of usefulness, ease of use, perceived risk, and intention to use RxTalk™ in the future were collected using Likert-scale interview questions followed by open-ended probes. Patients’ perception of the consultation was also sought. Further information about the interview guide can be found in Appendix 1. |
Descriptive - Frequencies and percentages (for Likert-scale questions). Hybrid inductive and deductive content analysis (for open-ended questions) |
Two coders (BQ & SM) |
Table 2.
Patients’ responses in RxTalk™.
| RxTalk™ questions | Frequency (%) (n=30) |
|
Goals of pharmacy visit (select all that apply) Medication pickup Get consultation Medication review |
28 (93.3%) 3 (10%) 3 (10%) |
|
Patients’ medical conditions (select all that apply) Hypertension Chronic pain High Cholesterol Mental health Diabetes Other∗ |
15 (50%) 13 (43.3%) 8 (26.7%) 8 (26.7%) 6 (20%) 10 (33.3%) |
|
Conditions with questions/concerns (Total) ∗∗ Chronic pain Diabetes Hypertension Mental health High cholesterol Other No concerns/missing |
7 (23.3%) 6 (20%) 5 (16.7%) 5 (16.7%) 2 (6.7%) 7 (23.3%) 3 (10%) |
|
Type of medical condition concerns† (select all that apply) Uncontrolled condition Symptoms or side effects Following diet Concerns about medications Other None |
9 (40.9%) 7 (31.8%) 6 (27.3%) 8 (36.4%) 2 (9%) 1 (4.5%) |
|
Type of medication concerns †† (select all that apply) Side effects Medication not working Remembering to take medication Other |
5 (62.5%) 2 (25%) 3 (37.5%) 1 (12.5%) |
|
Duration of taking the selected medication Less than 1 month 3-6 months More than 6 months |
8 (26.7%) 1 (3.3%) 21 (70%) |
|
Global health rating Excellent Very good Good Fair |
2 (6.7%) 6 (20%) 11 (36.7%) 11 (36.7%) |
|
BMQ - Adherent? α Yes No |
20 (76.9%) 6 (23.1%) |
|
Merck estimator Low risk Moderate risk High risk |
12 (40%) 10 (33.3%) 8 (26.7%) |
∗ Others include asthma, memory problems, prostate, hypothyroidism, migraine, and osteoporosis ∗∗The numbers reflect all conditions selected by patients after going through the 3 questions about conditions that patients had questions or concerns about. †Out of the 22 patients who were presented with this question ††Out of 9 patients who were presented with this question, there was one missing entry α4 patients were excluded since they selected new prescriptions. Adherence was determined by comparing patients’ responses to BMQ questions to their responses to the question about the regimen recommended by the prescribing clinician. Also, patients reporting missing their medication ≥ 1 time, in the 4th item of BMQ, were considered nonadherent.
Table 3.
Patients’ perception of RxTalk™ elicited during phone interviews.
| Perception of RxTalk™ (n=27) | Frequency (%) | Representative quotes | |
|
Attitude Positive Neutral Negative |
22 (77.8%) 3 (11.1%) 2 (7.4%) |
Positive “Very easy to use, not a lot of questions, but it did get to the point of what you were seeking.”PT46 Negative “ I don’t see the purpose of having to fill that out just to have a consult with the pharmacists” PT21 |
|
|
Usefulness Extremely useful Very useful Somewhat useful Slightly useful Not at all useful |
4 (14.8%) 12 (44.4%) 7 (25.9%) 3 (11.1%) 1 (3.7%) |
Useful “Information wise, you know, I just feel that I get the whole picture of what was going on that way.” PT1 Not that useful “If I'm going into the pharmacy, I just want to go pick up my medicine. I don't have to use the iPad in there.” PT7 |
|
|
Ease of use Easy Hard Neither easy nor hard |
19 (70.4%) 2 (7.41%) 6 (22.2%) |
Easy “Everything was pretty clear, and I didn't have to ask any questions. I understood what the questions were and, you know, how to answer those questions.” PT43 Hard “I don't know if it’s so much more using the tablet or if it actually made me kinda have to think of what I've been taking for medications to be able to put in there.” PT23 |
|
|
Intention to use RxTalk™ after 3 months Extremely likely Very likely Somewhat likely Slightly likely Not at all likely |
4 (14.8%) 9 (33.3%) 11 (40.7%) 2 (7.4%) 1 (3.7%) |
High intention “I like using technology for stuff like this, I guess.” PT53 Low intention “If I had any major concerns, the tablet would be helpful. But you know when I go in, just pick up my thyroid med, I wouldn't necessarily need to use it.” PT48 |
|
Table 4.
Problems encountered by patients while using RxTalk™.
| Type of usability problem |
Frequency (%) (n=30) |
|
Technical difficulties Navigating screens Filling information/clicking on responses |
7 (23.3%) 7 (23.3%) |
|
Comprehension problems Selecting appropriate answer Knowing name or spelling of medication Understanding the questions/instructions |
11 (36.7%) 6 (20%) 3 (10%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



