
Submitted:
29 November 2025
Posted:
01 December 2025
You are already at the latest version
Abstract
Background: Therapeutic applications of saline solutions in oral healthcare range from mineral waters to standardized sodium chloride preparations. Despite widespread traditional use, their scientific foundation remains inadequately characterized. This scoping review aimed to map the available evidence for saline interventions in oral healthcare and identify research gaps. Methods: Following JBI methodology and PRISMA-ScR guidelines, four electronic databases (PubMed, Scopus, Web of Science, Cochrane Library) were systematically searched for publications from 2000 to 2025. Studies were classified along a spectrum from geological mineral waters to artificial preparations. Narrative synthesis was employed with systematic gap identification. Results: Seventeen studies met inclusion criteria, with a median sample size of 41 participants and median follow-up of 4 weeks. Evidence distribution revealed concentration on hypersaline Dead Sea derivatives (n=7, 41%) and European thermal waters (n=6, 35%), with limited representation of marine-derived (n=1, 6%) and simple saline solutions (n=3, 18%). Reported outcomes included periodontal parameters, xerostomia symptoms, viral load, mucositis severity, and dentin hypersensitivity, with variable methodological quality across studies. Heterogeneity in interventions, comparators, and outcome measures precluded direct comparisons. Conclusions: The current evidence base for salt-based oral interventions remains limited and methodologically heterogeneous. While preliminary findings suggest potential applications across multiple clinical domains, small sample sizes, short follow-up periods, and inconsistent outcome measures preclude definitive recommendations. Standardized protocols and adequately powered trials are needed before evidence-based clinical integration.
Keywords:
thermal water
; mineral water
; saline solution
; oral health
1. Introduction
Chlorhexidine-based mouthwashes remain the gold standard for chemical plaque control, demonstrating consistent efficacy in reducing bacterial adhesion and gingival inflammation [1,2]. However, accumulating evidence documents clinically relevant adverse effects, including extrinsic dental staining, supragingival calculus formation, taste alteration, and hypersensitivity reactions, which limit long-term patient compliance [3,4]. Furthermore, emerging research indicates that broad-spectrum antimicrobial agents may induce dysbiotic shifts in the oral microbiome, with potential downstream consequences including impaired enterosalivary nitrate-nitrite-nitric oxide pathway function and associated cardiovascular implications [5,6]. These concerns have stimulated renewed interest in alternative antimicrobial and anti-inflammatory approaches, among which saline-based interventions warrant systematic investigation given their extensive ethnopharmacological history and favorable safety profile [7,8]. The term "saline-based interventions" encompasses a compositionally heterogeneous spectrum ranging from geologically complex mineral waters to standardized sodium chloride preparations. Natural thermal and mineral waters acquire distinctive ionic signatures through prolonged hydrothermal circulation within specific geological formations, yielding solutions characterized by variable concentrations of dissolved minerals, trace elements, and potentially bioactive compounds [9,10]. Hypersaline environments exemplified by the Dead Sea basin, with total dissolved solids exceeding 340 g/L, present extreme ionic compositions—notably elevated magnesium, potassium, and bromide concentrations—hypothesized to exert therapeutic effects through osmotic bacterial stress, enhanced epithelial penetration, and anti-inflammatory mineral activity [11,12]. European thermal medicine centers, particularly in France (Avène, La Roche-Posay), Italy (Salsomaggiore, Saturnia), and Germany (Baden-Baden), have maintained structured therapeutic protocols for centuries, with documented efficacy in dermatological and rheumatological applications [13,14]. Nevertheless, systematic investigation of oral health applications remains notably limited. Marine-derived preparations occupy an intermediate position along this compositional spectrum, offering the reproducibility of standard seawater salinity (approximately 35 g/L total dissolved solids) with naturally occurring trace element profiles less variable than those of geologically constrained thermal sources [15]. Simple saline solutions represent the opposite pole: standardized sodium chloride concentrations eliminating compositional variability while preserving fundamental osmotic mechanisms of bacterial inhibition and wound healing promotion [16,17]. This latter category holds particular relevance for resource-limited settings where commercial antimicrobial formulations remain economically inaccessible. Despite centuries of empirical application across diverse cultural contexts, the scientific evidence base for salt-based oral interventions remains inadequately characterized. While the balneotherapy literature addressing systemic and dermatological applications is extensive, comparatively few controlled studies have evaluated oral health outcomes specifically. Prior reviews have typically addressed isolated intervention categories or specific clinical conditions without systematic mapping across the full intervention spectrum. The heterogeneous nature of this literature—encompassing diverse water sources, delivery modalities, clinical populations, and outcome measures—renders conventional systematic review methodology with quantitative synthesis premature. This scoping review aimed to: (1) systematically map the extent and nature of research evidence concerning salt-based interventions for oral health applications; (2) characterize study populations, intervention types, comparators, and outcomes assessed; and (3) identify gaps in the existing literature to inform priorities for future primary research.
2. Materials and Methods
2.1. Search Strategy
A systematic search was conducted across four electronic databases: PubMed/MEDLINE, Scopus, Web of Science Core Collection, and Cochrane Library. The initial search was performed in October 2024 and updated on November 2025 to capture recent publications. Searches were limited to publications from January 2000 to December 2025 and to studies published in English, Italian, French, German, Spanish, or Portuguese.
The search strategy was developed in consultation with a medical librarian and combined controlled vocabulary (MeSH terms, Emtree) with free-text terms. No filters for study design were applied to maximize sensitivity. The complete search strategies for all databases are provided in Supplementary Table S1. The PubMed search strategy was as follows:
(("thermal water*"[tiab] OR "mineral water*"[tiab] OR "spa water*"[tiab] OR "balneotherapy"[tiab] OR "Dead Sea"[tiab] OR "saline solution*"[tiab] OR "salt water"[tiab] OR "saltwater"[tiab] OR "sodium chloride solution*"[tiab] OR "hypertonic saline"[tiab] OR "marine water"[tiab] OR "seawater"[tiab] OR "sea water"[tiab]) AND ("oral health"[tiab] OR "oral hygiene"[tiab] OR "periodontal"[tiab] OR "periodontitis"[tiab] OR "gingivitis"[tiab] OR "gingival"[tiab] OR "mouthwash*"[tiab] OR "mouth rinse*"[tiab] OR "mouthrinse*"[tiab] OR "oral rinse*"[tiab] OR "dental"[tiab] OR "oral mucosa"[tiab] OR "stomatitis"[tiab] OR "mucositis"[tiab] OR "plaque"[tiab] OR "caries"[tiab]))
This strategy was adapted for each database according to platform-specific syntax requirements. Grey literature was searched through ClinicalTrials.gov, WHO International Clinical Trials Registry Platform (ICTRP), and OpenGrey. Reference lists of included studies and relevant reviews were hand-searched to identify additional eligible publications. Conference abstracts were excluded due to insufficient methodological detail for quality assessment.
2.2. Eligibility Criteria
Eligibility criteria were defined using the Population, Concept, Context (PCC) framework recommended for scoping reviews.
Population: Human participants of any age, including healthy individuals and those with oral or systemic conditions. In vitro and animal studies were excluded unless they included a human clinical component.
Concept: Interventions using salt-based or mineral-rich water solutions for oral health purposes. This included hypersaline waters (Dead Sea derivatives), thermal mineral waters, marine-derived solutions, simple saline solutions, and sea salt formulations. Interventions could be administered as mouthwashes, rinses, sprays, irrigations, toothpastes, or gels. Studies examining sodium chloride solely as a vehicle or negative control without therapeutic intent were excluded.
Context: Any clinical, community, or home-based setting. No geographic restrictions were applied.
Additional inclusion criteria were: (1) original research reporting primary data; (2) assessment of at least one oral health outcome (clinical, microbiological, patient-reported, or biochemical); and (3) publication in a peer-reviewed journal. Exclusion criteria were: (1) narrative reviews, editorials, case reports, and expert opinions; (2) studies examining systemic effects of salt intake without oral health outcomes; and (3) studies where the salt-based intervention could not be isolated from other active components.
2.3. Study Selection
Study selection followed a two-stage process. In the first stage, two reviewers (EF, BS) independently screened titles and abstracts using Rayyan systematic review software [18]. Studies deemed potentially relevant by either reviewer proceeded to full-text assessment. In the second stage, the same two reviewers independently evaluated full-text articles against pre-specified eligibility criteria. At both stages, reviewers met regularly to discuss uncertainties and resolve discrepancies through consensus. When agreement could not be reached, a third reviewer (GM) made the final determination. Reasons for exclusion at the full-text stage were documented systematically and are presented in the PRISMA flow diagram (Figure 1).
2.4. Data Extraction
Data extraction was performed independently by two reviewers (EF, BS) using a standardized extraction form developed a priori (Supplementary Table S2). The form was piloted on three randomly selected studies and refined to improve clarity and consistency. Extracted data included: bibliographic information, study design, setting, population characteristics, intervention details (water type, mineral composition when reported, concentration, application method, frequency, and duration), comparator, outcomes assessed, follow-up duration, and key findings. Discrepancies in extracted data were resolved through consensus discussion, with arbitration by a third reviewer (GB) when necessary. Given the descriptive nature of scoping reviews, study authors were not contacted for missing or unclear data.
2.5. Data Synthesis
Given the heterogeneity in study designs, populations, interventions, and outcomes, quantitative meta-analysis was not appropriate. Data were synthesized narratively following Synthesis Without Meta-analysis (SWiM) guidelines. Studies were grouped by intervention category (hypersaline/Dead Sea, thermal waters, marine-derived, simple saline, sea salt formulations) and outcome domain. Results are presented using descriptive statistics (frequencies, percentages, medians, ranges) and tabular summaries. The evidence map illustrates the distribution of studies across intervention types and outcome categories.
3. Results
3.1. Study Selection and Characteristics
The systematic search identified 915 records across four databases: PubMed (n=342), Scopus (n=287), Web of Science (n=198), and Cochrane Library (n=45). An additional 43 records were identified through grey literature searches (n=23), citation searching (n=12), and hand searching (n=8). After removing 228 duplicates, 687 unique records underwent title and abstract screening, of which 598 were excluded as clearly irrelevant. Full-text assessment of 83 articles resulted in exclusion of 66 studies, leaving 17 studies that met all eligibility criteria (Figure 1). The included studies were published between 2007 and 2024 across nine countries. Sample sizes ranged from 10 to 93 participants (median 41), and follow-up periods ranged from 5 days to 3 months (median 4 weeks). Study designs included randomized controlled trials (n=9), quasi-experimental studies (n=4), prospective cohort studies (n=2), and cross-sectional studies (n=2). Studies were classified into five intervention categories: hypersaline Dead Sea derivatives (n=7, 41%), thermal mineral waters (n=5, 29%), simple saline solutions (n=3, 18%), sea salt formulations (n=2, 12%), and marine-derived solutions (n=1, 6%). All thermal water studies except one investigated Castéra-Verduzan thermal water (France). Detailed study characteristics are presented in Table 1; distribution by intervention category is summarized in Table 2.
3.2. Outcomes and Comparators
Six outcome domains were identified: periodontal parameters (n=9), xerostomia/salivary function (n=4), antimicrobial/antiviral effects (n=4), mucositis (n=1), dentin hypersensitivity (n=1), and whitening/remineralization (n=2). Fourteen different assessment instruments were used, precluding quantitative synthesis. Chlorhexidine was the most common comparator (n=6), followed by placebo/sham (n=5), no treatment (n=3), and other active comparators (n=2). Three studies compared different formulations without external controls.
3.3. Findings by Intervention Category
3.3.1. Hypersaline Dead Sea Derivatives
Seven studies reported mixed findings. Positive outcomes included significant viral load reductions (HSV-1, HCMV, EBV; p<0.001) [21], bacterial toxin neutralization (leukotoxin −84%, endotoxin −40%) [22], periodontal improvements equivalent to chlorhexidine [23], and reduced radiation-induced mucositis severity [26]. However, Dead Sea products showed no advantage over conventional systems for tooth whitening [20] or enamel remineralization [25].
3.3.2. Thermal Mineral Waters
Five studies showed inconsistent results for xerostomia: Alpöz et al. [28] found no difference versus placebo (with placebo performing better for some symptoms), while Skrinjar et al. [29] reported the highest quality-of-life effect size (0.52) for Buccotherm®. Toumassian et al. [30] demonstrated increased salivary mineralizing potential after 3 months. For gingivitis, Novozhilova et al. [31]—the only registered trial (NCT05623761)—reported significant gingival and bleeding improvements.
3.3.3. Simple Saline Solutions
3.3.4. Marine-Derived and Sea Salt Formulations
4. Discussion
This scoping review systematically mapped the available evidence on salt-based interventions for oral health. The findings reveal a nascent but heterogeneous evidence base characterized by geographic concentration, methodological limitations, and inconsistent results across similar interventions. The findings should be contextualized within the broader balneotherapy literature. Falagas et al. [7], evaluating randomized controlled trials of balneotherapy across medical conditions, identified methodological limitations similar to those observed here: small sample sizes, inadequate blinding, and heterogeneous outcome measures.
Fioravanti et al. [36] noted that while balneotherapy evidence is most robust for rheumatological and dermatological applications, other therapeutic domains remain understudied. This pattern is confirmed by Verhagen et al. [42], whose review of thermal waters in chronic skin diseases identified substantially more controlled trials than the present review found for oral health applications—suggesting that oral health represents a particularly neglected domain within thermal medicine research despite shared mechanistic rationales. To our knowledge, this represents the first scoping review to systematically map salt-based oral health interventions across the full compositional spectrum from geological mineral waters to artificial saline preparations.
Previous reviews have addressed isolated intervention types—such as thermal waters for dermatological conditions [42] or balneotherapy for osteoarthritis [42]—without comprehensive mapping of salt-based approaches specifically for oral health outcomes. The predominance of Dead Sea derivative research (41% of included studies) reflects established research infrastructure in Israel and commercial interest in hypersaline mineral products rather than inherent therapeutic superiority.
Findings within this category were notably mixed: while Nowzari et al. [21,22] reported significant antiviral effects and bacterial toxin neutralization, and Matceyevsky et al. [26] demonstrated reduced radiation-induced mucositis severity, other studies found no advantage for tooth whitening [20] or enamel remineralization [25]. This pattern suggests that Dead Sea derivatives may offer therapeutic potential for specific applications—particularly infection control and mucositis prophylaxis—while lacking broad-spectrum oral health benefits. The mechanistic basis for observed antiviral effects warrants further investigation, as reduction of oral herpesvirus loads could have implications for periodontal disease progression given established associations between viral reactivation and periodontitis [52]. Thermal water studies presented a particularly instructive pattern of contradictory findings. For xerostomia management, Alpöz et al. [28] found no significant difference between Buccotherm® spray and placebo, with placebo actually performing better for mastication, swallowing, and speech symptoms. In contrast, Skrinjar et al. [29] reported the highest quality-of-life effect size (0.52) for the same product compared to alternative treatments. These discrepant findings may reflect differences in study design (crossover versus parallel-group), outcome measures (VAS symptoms versus OHIP-14), or population characteristics (xerostomia etiology). Notably, Novozhilova et al. [31]—the only registered trial among thermal water studies—demonstrated significant improvements in gingival indices and bleeding reduction, with enhanced dentin hypersensitivity outcomes when fluoride was added. Toumassian et al. [30] reported increased salivary mineralizing potential following three months of thermal water product use in post-COVID patients, though the absence of a placebo control limits causal interpretation. Critically, four of five thermal water studies investigated products from a single source (Castéra-Verduzan, France), limiting generalizability to the broader category of European thermal waters.
This concentration is notable given the extensive thermal medicine infrastructure in Germany, Italy, and other European countries with documented efficacy in dermatological applications [43,46], yet virtually no published research on oral health outcomes. Silva et al. [27], investigating Portuguese Amarante thermal sulfur water, represents the sole exception and reported modest improvements in oral mucosal disease symptoms. The comparison with chlorhexidine efficacy provides important clinical context. Corte et al. [40], in their systematic review of chlorhexidine mouthrinses, documented consistent plaque and gingivitis reduction—establishing the benchmark against which alternative interventions must be evaluated. Simple saline solutions demonstrated the most consistent findings across included studies relative to this standard. Collins et al. [32] found saltwater rinse equivalent to chlorhexidine 0.12% following periodontal surgery, with no significant difference in gingival index reduction at 12 weeks. Aravinth et al. [33] reported comparable antimicrobial effects between salt water and chlorhexidine in schoolchildren. Fotso et al. [34] additionally demonstrated concentration-dependent antibacterial duration, with 5.8% saline matching chlorhexidine efficacy at 5 hours post-application.
These findings carry substantial implications for resource-limited settings where commercial antimicrobial formulations remain economically inaccessible. Moreover, growing concerns regarding chlorhexidine-induced microbiome disruption [5] and potential cardiovascular implications through enterosalivary pathway interference [6] suggest that simple saline solutions merit consideration as alternatives with more favorable safety profiles. However, the small sample sizes and short follow-up periods of included studies preclude definitive recommendations for clinical substitution. The marine-derived and sea salt formulation categories each contained too few studies for meaningful synthesis. The single marine-derived rinse study by Calvo-Guirado et al. [24] reported superior periodontal outcomes versus chlorhexidine 0.2% and saline controls, but this finding requires replication before clinical interpretation. Sea salt formulations showed mixed results: Hoover et al. [35] found no significant differences in plaque or bleeding compared to standard oral hygiene, while Corte et al. [36] reported significant S. mutans reduction versus placebo. However, these formulations combine salt with additional active ingredients (xylitol, lysozyme), precluding attribution of effects to the salt component specifically. Several methodological limitations characterized the included evidence base. First, 71% of studies enrolled fewer than 50 participants, limiting statistical power and precision of effect estimates. Second, only two studies exceeded four weeks follow-up, precluding assessment of sustained efficacy or long-term safety. Third, inadequate blinding was common—particularly problematic given the distinctive taste and appearance of many salt-based interventions. Fourth, outcome heterogeneity was substantial, with 14 different assessment instruments across 17 studies preventing quantitative synthesis. Finally, mineral composition was adequately reported in only four studies, limiting mechanistic interpretation and replication potential.
This scoping review has limitations inherent to its methodology. The restriction to peer-reviewed publications may have excluded relevant grey literature and introduced publication bias. The concentration of thermal water evidence from a single commercial source (Buccotherm®) may reflect publication bias toward industry-sponsored research.
Consistent with scoping review methodology and PRISMA-ScR guidelines [19], formal quality assessment was not performed, limiting interpretation of finding reliability. The heterogeneity of interventions, populations, and outcomes precluded quantitative synthesis, and narrative approaches carry inherent subjectivity in evidence interpretation. Future research priorities emerging from this evidence map include: (1) systematic investigation of European thermal waters beyond Castéra-Verduzan, utilizing standardized protocols and validated outcome measures; (2) adequately powered trials with extended follow-up periods (minimum 3–6 months) to assess sustained efficacy and safety; (3) head-to-head comparisons between intervention categories using common outcome measures to enable meta-analysis; (4) mechanistic studies characterizing the mineral composition requirements for therapeutic effects; and (5) investigation in underrepresented populations, particularly immunocompromised patients where preliminary mucositis findings suggest potential benefit [26]. Development of consensus core outcome sets for salt-based oral intervention trials would facilitate future evidence synthesis and clinical translation.
5. Conclusions
While preliminary findings suggest potential therapeutic applications—particularly for Dead Sea derivatives in periodontal care and mucositis prophylaxis—the limited number of studies, small sample sizes, and methodological heterogeneity preclude definitive clinical recommendations. Key research priorities include systematic investigation of European thermal waters using standardized protocols, larger adequately-powered trials with extended follow-up, and development of consensus outcome measures. Until higher-quality evidence emerges, salt-based interventions should be considered experimental adjuncts requiring further validation before clinical implementation.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1. Complete Database Search Strategies; Table S2: Studies Excluded at Full-Text Screening with Reasons.
Author Contributions
Conceptualization, E.F. and B.S.; methodology, E.F.; software, B.R.; validation, G.B., G.M. and M.S.; formal analysis, E.F., M.S.; investigation B.S., G.M.; resources, G.M.; data curation, B.S.; writing—original draft preparation, E.F., B, S., G.B; writing—review and editing, E.F., B.S., G.M; visualization, B.R., M.S.; supervision, B.S.; project administration, E.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BI | Bleeding Index |
| CMC | Carboxymethylcellulose |
| DH | Dentin Hypersensitivity |
| EBV | Epstein-Barr Virus |
| HCMV | Human Cytomegalovirus |
| HSV-1 | Herpes Simplex Virus Type 1 |
| JBI | Joanna Briggs Institute |
| MGI | Modified Gingival Index |
| NIH | National Institutes of Health |
| OHIP-14 | Oral Health Impact Profile 14 |
| OMD | Oral Mucosal Disease |
| OSF | Open Science Framework |
| PRISMA-ScR | Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews |
| QoL | Quality of Life |
| VAS | Visual Analog Scale |
References
- Marinho, A.C.S.; Martins, E.N.; Ribeiro, S.F.; Pereira, J.A. Antimicrobial activity of essential oil-based mouthwashes against oral pathogenic bacteria. Int. J. Dent. 2019, 2019, 3878408. [Google Scholar] [CrossRef]
- Sharma, N.C.; Charles, C.H.; Qaqish, J.G.; Galustians, H.J.; Zhao, Q.; Kumar, L.D. Comparative effectiveness of an essential oil mouthrinse and dental floss in controlling interproximal gingivitis and plaque. Am. J. Dent. 2002, 15, 351–355. [Google Scholar] [PubMed]
- Farah, C.S.; McIntosh, L.; McCullough, M.J. Mouthwashes. Aust. Prescr. 2009, 32, 162–164. [Google Scholar] [CrossRef]
- Santos, G.O.; Vasconcelos, C.C.; Lopes, A.J.; Cartágenes, M.S.; Filho, A.K.; do Nascimento, F.R.; Ramos, R.M.; Pires, E.R.; de Andrade, M.S.; Rocha, F.A.; et al. Candida infections and therapeutic strategies: mechanisms of action for traditional and alternative agents. Front. Microbiol. 2018, 9, 1351. [Google Scholar] [CrossRef]
- Bescos, R.; Ashworth, A.; Cutler, C.; Brookes, Z.L.S.; Belfield, L.; Rodiles, A.; Casas-Agustench, P.; Farnham, G.; Liddle, L.; Burleigh, M.; White, D.; Easton, C.; Hickson, M. Effects of Chlorhexidine mouthwash on the oral microbiome. Sci. Rep. 2020, 10, 5254. [Google Scholar] [CrossRef]
- Kapil, V.; Haydar, S.M.; Pearl, V.; Lundberg, J.O.; Weitzberg, E.; Ahluwalia, A. Physiological role for nitrate-reducing oral bacteria in blood pressure control. Free Radic. Biol. Med. 2013, 55, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Zarkadoulia, E.; Rafailidis, P.I. The therapeutic effect of balneotherapy: evaluation of the evidence from randomised controlled trials. Int. J. Clin. Pract. 2009, 63, 1068–1084. [Google Scholar] [CrossRef]
- Collins, J.R.; Veras, K.; Hernández, M.; Hou, W.; Hong, H.; Romanos, G.E. Anti-inflammatory effect of salt water and chlorhexidine 0.12% mouthrinse after periodontal surgery: A randomized prospective clinical study. Clin. Oral Investig. 2021, 25, 4349–4357. [Google Scholar] [CrossRef]
- Rodriguez, P.; Cionca, N.; Benic, G.I.; Bornstein, M.M. Interventions for preventing oral mucositis in patients receiving cancer treatment. Cochrane Database Syst. Rev. 2015, 12, CD000978. [Google Scholar] [CrossRef]
- Seité, S. Thermal waters as cosmeceuticals: La Roche-Posay thermal spring water example. Clin. Cosmet. Investig. Dermatol 2013, 6, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Marini, I.; Checchi, L.; Vecchiet, F. Intraoral distribution and antimicrobial activity of a chlorhexidine mouthrinse in orthodontic patients. Oral Health Prev. Dent. 2014, 12, 37–44. [Google Scholar] [CrossRef]
- Michel, J.L.; Josue, A.; Ko, G.J.; Campbell, K.; Velazquez-Kronen, R.; Seabrook, J.A.; Matsui, D.; et al. Efficacy of sea salt rinse in street children of Manila, Philippines. Int. J. Pediatr. 2013, 2013, 928971. [Google Scholar] [CrossRef]
- Wood, J.M. Bacterial responses to osmotic challenges. J. Gen. Physiol. 2015, 145, 381–388. [Google Scholar] [CrossRef]
- Butcher, L.D.; den Hartog, G.; Ernst, P.B.; Crowe, S.E. Oxidative stress resulting from helicobacter pylori infection contributes to gastric carcinogenesis. Cell. Mol. Gastroenterol. Hepatol. 2017, 3, 316–322. [Google Scholar] [CrossRef]
- Ghersetich, I.; Freedman, D.; Lotti, T. Balneology today. J. Eur. Acad. Dermatol. Venereol. 2000, 14, 346–348. [Google Scholar] [CrossRef]
- Giggenbach, W.F. Isotopic composition of geothermal water and steam discharges. In Application of Geochemistry in Geothermal Reservoir Development; D'Amore, F., Ed.; UNITAR/UNDP: New York, NY, USA, 1991; pp. 253–273. [Google Scholar]
- Fournier, R.O.; Truesdell, A.H. An empirical Na-K-Ca geothermometer for natural waters. Geochim. Cosmochim. Acta 1973, 37, 1255–1275. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; et al. Rayyan—a web and mobile app for systematic reviews. Syst Rev 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Gurich, N.; Anastasia, M.K.; Grender, J.; Sagel, P. Tooth color change and tolerability evaluation of a hydrogen peroxide whitening strip compared to a strip, paste, and rinse regimen containing plant-based oils and Dead Sea salt. Am. J. Dent. 2023, 36, 151–155. [Google Scholar] [PubMed]
- Nowzari, H.; Wilder-Smith, P. Effects of mouthwash on oral cytomegalovirus, Epstein-Barr virus, herpes simplex virus type-1. Adv Clin Med Res 2022, 3, 44. [Google Scholar] [CrossRef]
- Nowzari, H.; Tuan, M.C.; Jorgensen, M.; Michel, M.G.; Michel, J.F. Dead sea salt solution: composition, lack of cytotoxicity and in vitro efficacy against oral leukotoxins, endotoxins and glucan sucrose. Insights Biol. Med. 2022, 6, 009–014. [Google Scholar] [CrossRef]
- Rodriguez, P.; Ajdaharian, J. Effects of a novel mouthwash on plaque presence and gingival health. Dentistry 2017, 7, 460. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Fernández Domínguez, M.; Aragoneses, J.M.; Martínez González, J.M.; Fernández-Boderau, E.; Garcés-Villalá, M.A.; Romanos, G.E.; Delgado-Ruiz, R. Evaluation of new seawater-based mouthrinse versus chlorhexidine 0.2% reducing plaque and gingivitis indexes. A randomized controlled pilot study. Appl. Sci. 2020, 10, 982. [Google Scholar] [CrossRef]
- Ajdaharian, J.; Takesh, T.; Anbarani, A.; Ho, J.; Wilder-Smith, P. Effects of a novel mouthwash on dental remineralization. Dentistry (Sunnyvale) 2017, 7, 432. [Google Scholar] [CrossRef]
- Matceyevsky, D.; Gotfrid, J.; Amsili, S.; Okamoto, A.; Ferreira, S.M.; Lipp, M.; Liebermann, A. Prophylactic Dead Sea mineral products for radiation-induced oral and skin mucositis in cancer patients receiving head and neck radiotherapy. Support. Care Cancer 2007, 15, 1303–1309. [Google Scholar]
- Silva, P.; Couto, P.; Viana, A.; Silva, F.; Correia, M.J. Unravelling the benefits of thermal waters enhancing oral health: a pilot study. BMC Oral Health 2024, 24, 1502. [Google Scholar] [CrossRef]
- Alpöz, E; Çankaya, H; Güneri, P; Epstein, JB; Boyacioglu, H; Kabasakal, Y; Ocakci, PT. Impact of Buccotherm® on xerostomia: a single blind study. Spec Care Dentist 2015, 35, 1–7. [Google Scholar] [CrossRef]
- Skrinjar, I; Vucicevic Boras, V; Bakale, I; Andabak Rogulj, A; Brailo, V; Vidovic Juras, D; Alajbeg, I; Vrdoljak, DV. Comparison between three different saliva substitutes in patients with hyposalivation. Clin Oral Investig. 2015, 19, 753–7. [Google Scholar] [CrossRef] [PubMed]
- Toumassian, M.G.; Toumassian, S.G.; Satygo, E.A. Efficacy of oral hygiene products based on hydrothermal water from Castéra-Verduzan in patients with post-COVID syndrome. Klin. Stomatol. 2022, 25, 82–87. (In Russian) [Google Scholar] [CrossRef]
- Novozhilova, N; Andreeva, E; Polyakova, M; Makeeva, I; Sokhova, I; Doroshina, V; Zaytsev, A; Babina, K. Antigingivitis, Desensitizing, and Antiplaque Effects of Alkaline Toothpastes: A Randomized Clinical Trial. Dent J 2023, 11, 96. [Google Scholar] [CrossRef]
- Collins, J.R.; Veras, K.; Hernández, M.; Hou, W.; Hong, H.; Romanos, G.E. Anti-inflammatory effect of salt water and chlorhexidine 0.12% mouthrinse after periodontal surgery: A randomized prospective clinical study. Clin. Oral Investig. 2021, 25, 4349–4357. [Google Scholar] [CrossRef]
- Aravinth, V.; Aswath Narayanan, M.; Ramesh Kumar, S.; Selvamary, A.; Sujatha, V. Salt water rinse: A cost effective mouth wash. J. Clin. Diagn. Res. 2017, 11, ZC01–ZC03. [Google Scholar]
- Fotso, M.; Leuschke, J.; Kristensen, S.; Jiskoot, W.; Bjørge, I.M.; Christensen, B.E. Cross-over clinical trial on antimicrobial effect of homemade saline solutions at different concentrations versus 0.1% chlorhexidine. Int. J. Dent. Hyg. 2022, 20, 156–164. [Google Scholar]
- Hoover, J.; Tovar, E.; Zlatnik, T.; Karunanayake, C. Efficacy of a rinse containing sea salt and lysozyme on biofilm and gingival health in a group of young adults: A pilot study. Int. J. Dent. Hyg. 2017, 15, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Corte, A.; Grasso, N.; Zullo, S.; D'Andrea, G.; Mancini, A.; Castagna, G.; Mariani, P. Efficacy of sea salt-based mouthwash and xylitol in improving oral hygiene among adolescent population: A pilot study. Healthcare 2020, 8, 574. [Google Scholar] [CrossRef]
- Kumar, L.; Chhibber, S.; Harjai, K. Natural Anti-biofilm Agents: Strategies to Control Biofilm-Forming Pathogens. Front. Microbiol. 2020, 11, 566325. [Google Scholar] [CrossRef]
- Roy, R.; Tiwari, M.; Donelli, G.; Tiwari, V. Strategies for combating bacterial biofilms: A focus on anti-biofilm agents and their mechanisms of action. Virulence 2018, 9, 522–554. [Google Scholar] [CrossRef]
- Abu-Ghazaleh, S.; Dardas, M.; Shehadeh, M.; Al-Haddad, M.; Darwich, A.; Al-Omari, I.K. Antimicrobial activity of Bacillus persicus 24-DSM isolated from Dead Sea mud. BMC Microbiol. 2018, 18, 203. [Google Scholar] [CrossRef]
- Van Strydonck, D.A.; Slot, D.E.; Van der Velden, U.; Van der Weijden, F. Effect of a chlorhexidine mouthrinse on plaque, gingival inflammation and staining in gingivitis patients: a systematic review. J. Clin. Periodontol. 2012, 39, 1042–1055. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, A.; Karagulle, M.; Bender, T.; Karagülle, M.Z. Balneotherapy in medicine: A review. Environ. Health Prev. Med. 2017, 22, 17. [Google Scholar] [CrossRef]
- Verhagen, A.P.; Bierma-Zeinstra, S.M.; Boers, M.; Cardoso, J.R.; Lambeck, J.; de Bie, R.; de Vet, H.C. Balneotherapy for osteoarthritis. Cochrane Database Syst. Rev. 2015, 4, CD006864. [Google Scholar] [CrossRef]
- Dubois, O.; Nouveau, S.; Jourdan, E.; Bastien, P.; Macé, S. Clinical efficacy of La Roche-Posay thermal spring water coordinated with dermatological treatments in atopic dermatitis. Eur. J. Dermatol 2018, 28, 585–592. [Google Scholar] [CrossRef]
- Karagülle, M.; Karagülle, M.Z.; Karagülle, O.; Dönmez, A.; Turan, M. A 10-day course of SPA therapy is beneficial for people with severe knee osteoarthritis. A 24-week randomised, controlled pilot study. Clin. Rheumatol. 2007, 26, 2063–2071. [Google Scholar] [CrossRef]
- Pinton, J.; Friden, H.; Kettaneh-Wold, N.; Hussain, H.; Faergemann, J.; Larkö, O. Clinical and biological effects of balneotherapy with selenium-rich spa water in patients with psoriasis vulgaris. Br. J. Dermatol 1995, 133, 344–347. [Google Scholar] [CrossRef]
- Cacciapuoti, S.; Luciano, M.A.; Megna, M.; Annunziata, M.C.; Napolitano, M.; Patruno, C.; Scala, E.; Colicchio, R.; Pagliuca, C.; Salvatore, P.; Fabbrocini, G. The Role of Thermal Water in Chronic Skin Diseases Management: A Review of the Literature. J. Clin. Med. 2020, 9, 3047. [Google Scholar] [CrossRef]
- Oren, A.; Garrity, G.M.; Parker, C.T.; Chuvochina, M.; Trujillo, M.E. Lists of names of prokaryotic candidatus taxa. Int. J. Syst. Evol. Microbiol. 2020, 70, 3956–4000. [Google Scholar] [CrossRef]
- Mosaddad, S.A.; Hussain, A.; Tebyaniyan, H. Green alternatives as antimicrobial agents in mitigating periodontal diseases: A narrative review. Microorganisms 2023, 11, 1269. [Google Scholar] [CrossRef] [PubMed]
- Michel, J.L.; Josue, A.; Ko, G.J.; Campbell, K.; Velazquez-Kronen, R.; Seabrook, J.A.; Matsui, D. Efficacy of sea salt rinse in street children of Manila, Philippines. Int. J. Pediatr. 2013, 2013, 928971. [Google Scholar] [CrossRef]
- Klompas, M.; Speck, K.; Howell, M.D.; Greene, L.R.; Berenholtz, S.M. Reappraisal of routine oral care with chlorhexidine gluconate for patients receiving mechanical ventilation: systematic review and meta-analysis. JAMA Intern. Med. 2014, 174, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Nathan, C.; Brukner, M.; Bonomo, R.A. Rethinking oral antiseptics. Antimicrob. Agents Chemother. 2021, 65, e02718-20. [Google Scholar] [CrossRef]
- Slots, J.; Slots, H. Periodontal herpes virus morbidity and treatment. Periodontol. 2000 2019, 79, 210–220. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S. From focal sepsis to periodontal medicine: a century of exploring the role of the oral microbiome in systemic disease. J. Physiol. 2017, 595, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Kümmerer, K. Antibiotics in the aquatic environment—a review—part I. Chemosphere 2009, 75, 417–434. [Google Scholar] [CrossRef] [PubMed]
- Fischbach, M.A.; Walsh, C.T. Antibiotics for emerging pathogens. Science 2009, 325, 1089–1093. [Google Scholar] [CrossRef]
- Newman, D.J.; Cragg, G.M. Natural products as sources of new drugs over the nearly four decades from 01/1981 to 09/2019. J. Nat. Prod. 2020, 83, 770–803. [Google Scholar] [CrossRef]
Figure 1.
PRISMA-ScR flow diagram showing study selection process for salt-based oral health interventions.
Figure 1.
PRISMA-ScR flow diagram showing study selection process for salt-based oral health interventions.
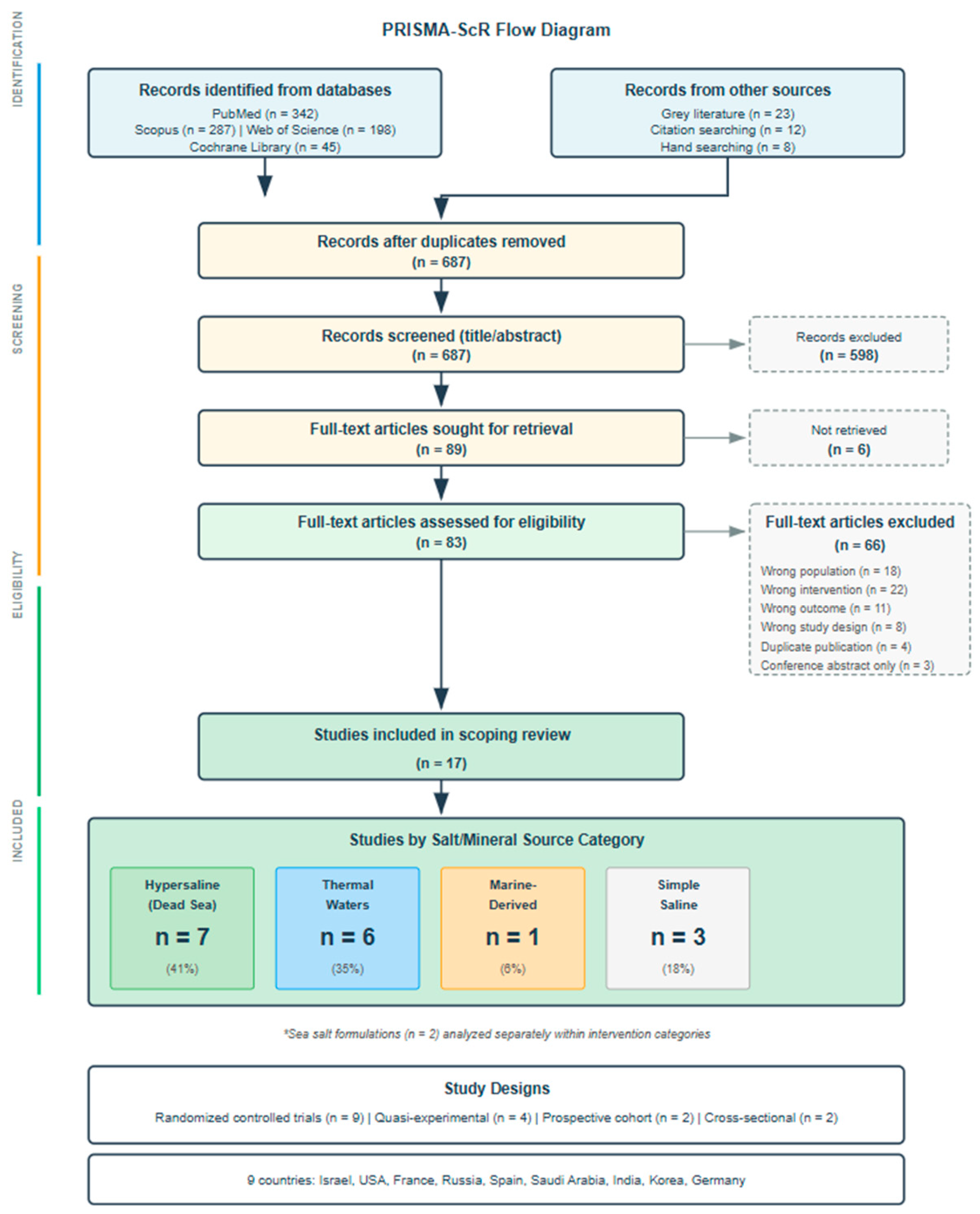

Table 1.
Characteristics of Included Studies.
| Author | Water Type | Study Design | Population/Sample | Intervention | Control | Outcomes | Key Findings |
|---|---|---|---|---|---|---|---|
| HYPERSALINE WATER STUDIES (DEAD SEA REGION) | |||||||
| Gurich et al. [20] |
Hypersaline Dead Sea derivatives |
Parallel-group double-blind RCT | 50 adults (18-62 years) |
Natural whitening regimen with Dead Sea salt-based products (strips, toothpaste, mouthwash) | Conventional peroxide-based whitening system |
Objective tooth color assessment at 7, 10, and 14 days |
Natural Dead Sea regimen failed to achieve significant color improvement, while conventional treatment produced measurable whitening |
| Nowzari et al., 2022a [21] |
Hypersaline Dead Sea derivatives | Double-blind controlled trial |
30 adults (25-35 years) with gingivitis and detectable oral viruses | Oral rinse containing Dead Sea salts used twice daily over 8-week period |
Control rinse (distilled water) |
Salivary detection of herpes viruses (HSV-1, HCMV, EBV) | Dead Sea salt rinse significantly decreased viral loads compared to control group for all measured viruses (p < 0.001) |
| Nowzari et al., 2022b [22] |
Hypersaline Dead Sea derivatives | Laboratory efficacy study |
Mouse fibroblast cell cultures | Dead Sea salt solution exposure at therapeutic concentrations | Standard culture conditions | Cell viability and bacterial toxin neutralization | Salt solution demonstrated safety (no cytotoxicity) and substantial reduction of oral pathogen byproducts: leukotoxin (-84%), endotoxin (-40%), glucan enzyme (-90%) |
| Rodriguez & Ajdaharian [23] |
Hypersaline Dead Sea derivatives |
Three-arm controlled trial | 10 healthy volunteers | Commercial Dead Sea salt mouthwash (Oral Essentials brand) | Active control (chlorhexidine) and negative control (no rinse) | Standard periodontal indices (plaque, gingivitis, bleeding) | Both active rinses equally effective in reducing periodontal inflammation compared to no treatment; no statistical difference between Dead Sea and |
| Calvo-Guirado et al. [24] |
Natural seawater (moderate salinity) | Crossover design RCT |
93 dental students (19-42 years) | Marine-derived oral rinse (SEA 4 Encias brand) | Reference standard (0.2% chlorhexidine) and neutral control (saline) | Periodontal clinical parameters over 4-week trial | Marine rinse outperformed both chlorhexidine and saline controls in reducing plaque accumulation and gingival inflammation scores |
| Ajdaharian et al. [25] |
Hypersaline Dead Sea derivatives | Crossover enamel study |
10 participants providing 300 tooth samples | Experimental sensitivity rinse with Dead Sea components and plant extracts | Commercial fluoride rinse (Sensodyne) and no-rinse control | Enamel surface microhardness recovery after demineralization | No therapeutic advantage observed for Dead Sea formulation; all groups showed equivalent enamel remineralization over 5-day exposure period |
| Matceyevsky et al. [26] |
Hypersaline Dead Sea minerals | Prospective cohort study |
54 cancer patients receiving head/neck radiotherapy | Prophylactic Dead Sea mineral products (oral rinse + topical cream) | Conventional supportive care | Radiation-induced oral and skin mucositis severity grading | Dead Sea mineral therapy significantly reduced severe mucositis incidence and prevented treatment interruptions compared to standard management |
| THERMAL WATER STUDIES | |||||||
| Silva et al., [27] | Thermal sulfur water | Observational, longitudinal, comparative study |
90 thermalists randomly allocated to groups | Thermal sulfuric natural mineral water of Amarante Thermal baths via gargles and oral showers for 14 days | Saline solution | Plaque index, gingival bleeding index, periodontal probing depth, oral mucosa disease symptoms | TW_TA group showed greater reduction in pain frequency (35.5% vs 28.9% "rarely" experiencing pain). Positive evolution in both groups for OMD symptoms |
| Alpöz et al. [28] | Thermal water (Castéra-Verduzan, France) | Single-blind crossover study | 20 xerostomia patients (17 women, 3 men; age 43-75 years, mean 51.5) | Buccotherm® spray 6 times daily for 14 days | Placebo (diluted tea solution with similar appearance) | Subjective xerostomia symptoms via VAS (10 items including dry mouth, difficulty swallowing, speech) | No significant difference between thermal water spray and placebo for overall xerostomia relief. Placebo showed lower VAS scores than thermal water for several symptoms (mastication p=0.006, swallowing p=0.00, speech p=0.003) |
| Skrinjar et al. [29] | Thermal water (Castéra-Verduzan, France) | Open-label randomized controlled trial | 60 drug-induced hyposalivation patients (45 women, 15 men; age 45-73 years, mean 64) | Buccotherm® spray (n=30) vs Xeros® mouthwash (n=15) vs marshmallow root (n=15); 4 times daily for 2 weeks | Three-arm comparison | Quality of life (OHIP-14), dry mouth intensity (VAS) | Buccotherm® showed highest effect size on QoL (0.52) compared to Xeros® (0.33) and marshmallow root (0.26). All three reduced VAS scores significantly (p<0.05) with no between-group difference |
| Toumassian et al. [30] | Thermal water (Castéra-Verduzan, France) | Prospective comparative study | 80 post-COVID syndrome patients (dental students; mean age 21.5 years) | Group I (n=46): Buccotherm® toothpaste + mouthwash; Group II (n=34): toothpaste + mouthwash + spray 3x/day; 3-month duration | Between-group comparison (no placebo) | Salivation rate, viscosity, pH, mineralizing potential, calcium and magnesium concentration | Mineralizing potential increased significantly in both groups (Group I: 1.31→2.27; Group II: 1.28→2.87, p<0.05). Group II showed greater improvement in salivation rate and mineral concentration |
| Novozhilova et al. [31] | Thermal water (Castéra-Verduzan, France) | Double-blind parallel-group RCT | 82 patients aged 20-25 years with gingivitis and dentin hypersensitivity | Toothpaste containing 46% Castéra-Verduzan thermal water (pH 8.8): Group TW (fluoride-free, n=41) vs Group TWF (with 1450 ppm NaF, n=41); twice daily for 4 weeks | Between-group comparison | Modified Gingival Index, Bleeding Index, VAS and Schiff Scale for dentin hypersensitivity, Rustogi Modified Navy Plaque Index, salivary pH | Significant improvement in gingival condition (MGI effect sizes: TW=0.99, TWF=1.71) and bleeding (BI effect sizes: TW=3.17, TWF=2.64). Dentin hypersensitivity decreased more in TWF group (VAS effect size=3.28). Plaque index improved in both groups |
| SIMPLE SALINE SOLUTION STUDIES | |||||||
| Collins et al. [32] |
Simple saline solution (artificial) | Randomized prospective double-blind study | 37 chronic periodontitis patients | Saltwater mouth rinse following open flap debridement | 0.12% chlorhexidine mouth rinse | Gingival Index, post-operative pain, mouth rinse satisfaction, matrix metalloproteinase activity | Significant decrease in GI from baseline to week 1/12 in both groups. No significant difference between groups. Saltwater as efficient as chlorhexidine |
| Aravinth et al. [33] |
Simple saline solution (artificial) | School-based randomized controlled trial | School children | Salt water rinse | Chlorhexidine mouth rinse | Dental plaque and oral microbial count | Salt water rinse effective as adjunct to routine mechanical plaque control. Comparable antimicrobial effects to chlorhexidine |
| Fotso et al. [34] | Simple saline solutions (artificial) | Cross-over clinical trial | 10 participants (240 saliva samples) | Homemade saline solutions at different concentrations (2%, 5.8%, 23%) | 0.1% chlorhexidine | Oral flora reduction and duration of effect | 2% saline: 3h antibacterial effect. 5.8% saline: 5h effect (same as chlorhexidine). 23% saline: 7h effect but irritating taste |
| SEA SALT FORMULATION STUDIES | |||||||
| Hoover et al. [35] |
Sea salt formulation | Pilot study | 30 dental students aged 20-26 years | Sea salt, xylitol, and lysozyme mouth rinse for 30 days | Standard oral hygiene only | Turesky plaque index, gingival bleeding on probing | No statistically significant differences in overall plaque and gingivitis reduction between groups |
| Corte et al., [36] | Sea salt formulation |
Randomized, double-blinded, placebo-controlled study |
20 healthy adolescents | Combined mouth rinse with sea salt, xylitol, lysozyme, and menthol (H2Ocean) | Placebo rinse (mint-flavored water) | Plaque index, S. mutans levels | Sea salt-based mouthwash reduced bacterial levels of S. mutans significantly vs placebo |
* Abbreviations: BOP, bleeding on probing; CHX, chlorhexidine; Cross-sect, cross-sectional; DH, dentin hypersensitivity; DMFT, decayed/missing/filled teeth; F, fluoride; GI, gingival index; KNHANES, Korea National Health and Nutrition Examination Survey; MGI, modified gingival index; OR, odds ratio; PI, plaque index; PPD, probing pocket depth; QoL, quality of life; Quasi-exp, quasi-experimental; RCT, randomized controlled trial; VAS, visual analog scale. Notes: All thermal water studies used Castéra-Verduzan thermal water (France) as the mineral source.
Table 2.
Distribution of included studies by intervention category.
| Intervention Category | Studies (n) | Percentage Countries | Countries |
| Hypersaline Dead Sea derivatives | 7 | 41% | Israel, USA |
| Thermal/mineral waters | 6 | 35% | France, Portugal, Turkey, Croatia, Russia |
| Marine-derived solutions | 1 | 6% | Spain |
| Simple saline solutions | 3 | 18% | USA, Cameroon, India |
1 Tables may have a footer.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



