Submitted:
27 June 2025
Posted:
27 June 2025
You are already at the latest version
Abstract
Background: Anemia during pregnancy remains a significant public health concern, especially in low- and middle-income countries. It contributes to adverse maternal and fetal outcomes and is influenced by multiple socioeconomic, dietary, and obstetric factors. This study aimed to assess the prevalence of anemia and its associated risk factors among pregnant women attending antenatal care in Meerut City. Methods: A cross-sectional study was conducted among 210 pregnant women attending antenatal care services at an Urban Primary Health Center (UPHC) in Meerut City. Data on sociodemographic characteristics, obstetric history, dietary habits, knowledge regarding anemia, and supplementation adherence were collected using a pre-tested semi-structured questionnaire. Hemoglobin levels were measured to classify anemia severity. Bivariate analysis identified factors associated with anemia, and variables with p < 0.10 were included in a multivariable logistic regression model. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated. Statistical significance was set at p < 0.05. Results: Out of the total 210 respondents, the overall prevalence of anemia among pregnant women was 63.8%, with 28.6% having mild anemia, 31.4% moderate anemia, and 3.8% severe anemia. Anemia was significantly more prevalent among women from low-income households (p < 0.001), those with lower educational attainment (p = 0.002), poor dietary intake (p < 0.001), and limited knowledge of anemia and its sources (p = 0.000). A significant proportion (83.3%) of anemic women rarely consumed iron-rich foods such as meat, beans, and green leafy vegetables. Multivariable logistic regression analysis identified low household income (AOR = 2.7; 95% CI: 1.4–5.3; p = 0.003) and poor dietary intake (AOR = 3.5; 95% CI: 1.8–6.7; p < 0.001) as independent predictors of anemia after adjusting for age, parity, and gestational age. Conclusion: Anemia remains highly prevalent among pregnant women in this urban setting, primarily driven by low socioeconomic status, poor dietary diversity, and suboptimal nutritional practices. Strengthening antenatal care services with a focus on poverty alleviation, nutritional counseling, early antenatal care initiation, and enhanced iron and folic acid supplementation adherence is critical to reducing anemia burden and improving maternal and neonatal health outcomes.The study highlights a high burden of anemia among pregnant women in Meerut City, with nutritional inadequacy and economic deprivation being the major contributing factors. These findings emphasize the urgent need for integrated antenatal interventions focusing on improving maternal nutrition, dietary counselling, and addressing underlying socioeconomic inequalities. Strengthening existing national programs such as Anemia Mukt Bharat with local-level nutritional surveillance and community-based education can play a pivotal role in reducing the anemia burden among pregnant women in urban India. Keywords: Maternal anemia, Nutritional status, Socioeconomic status, Dietary diversity, Iron intake, Maternal health, Urban population in India, North India
Keywords:
Maternal anemia
; Nutritional status
; Socioeconomic status
; Dietary Diversity
; Iron intake
; Maternal health
; Urban population in India
; North India
1. Introduction
Anemia during pregnancy is a widespread public health issue, particularly in developing countries like India, where it contributes significantly to maternal and fetal morbidity and mortality. Characterized by a reduced concentration of hemoglobin in the blood, anemia impairs the oxygen-carrying capacity of red blood cells, which is crucial for maintaining maternal and fetal health. According to the World Health Organization (WHO), anemia affects approximately 40% of pregnant women globally, with an even higher burden in South Asia. In India, the National Family Health Survey (NFHS-5) reported that more than 50% of pregnant women are anemic, underscoring the urgency of addressing this condition as a national priority.
The causes of anemia in pregnancy are multifactorial, with iron deficiency being the most common contributor. However, nutritional inadequacies, poor dietary habits, recurrent infections, and limited access to health services also play a critical role. In addition to biological and health-related factors, the socioeconomic context of a woman significantly influences her vulnerability to anemia. Low-income households often lack access to nutritious food, healthcare, and education, which exacerbates the risk of anemia during pregnancy. Thus, the interplay between nutrition and economic status becomes a crucial determinant in the prevalence and severity of anemia among expectant mothers.
Meerut City, a rapidly urbanizing region in western Uttar Pradesh, presents a unique demographic profile characterized by socioeconomic diversity, nutritional transition, and varying access to antenatal care services. Despite its proximity to the National Capital Region (NCR), significant disparities in maternal health indicators persist. Limited research has been conducted to explore how both nutritional and economic determinants contribute to anemia in pregnant women in this specific urban setting.
Understanding the prevalence of anemia in this region, alongside the contributing nutritional and economic factors, is essential for informing targeted interventions. Nutritional education, supplementation programs, and economic empowerment initiatives can significantly reduce the incidence of anemia if appropriately tailored to the local context. Furthermore, identifying vulnerable groups within the urban population can help policymakers design more effective and equitable health strategies.
This study aims to assess the prevalence of anemia among pregnant women in Meerut City and examine how their nutritional status and economic position contribute to this condition. By exploring these associations, the research seeks to provide evidence-based recommendations that can guide public health policy, improve maternal health outcomes, and reduce the burden of anemia in similar urban contexts.
2. Background of the Study
Anemia in pregnancy remains a critical concern globally and is especially prevalent in South Asia, where nutritional deficiencies and socioeconomic inequities converge to impact maternal health. The World Health Organization (WHO) identifies anemia—primarily iron deficiency anemia—as a major contributor to adverse pregnancy outcomes including preterm birth, low birth weight, and maternal mortality.
Several cross-sectional studies have consistently reported high anemia prevalence among pregnant women across diverse settings. For example, Abriha et al. (2014) in Ethiopia and Tibambuya et al. (2019) in Ghana found anemia rates exceeding 40%, largely attributed to poor dietary intake and low socioeconomic status. Similarly, in India, Kumari et al. (2019) observed that maternal anemia significantly increased the risk of adverse birth outcomes such as low birth weight and preterm delivery.
In urban settings, dietary habits play a pivotal role in anemia prevalence. Grover et al. (2020) linked anemia in urban Haryana to low consumption of iron-rich foods and poor dietary diversity. Similarly, Diamond-Smith et al. (2016) highlighted that persistent anemia among poor pregnant women in Chandigarh stemmed from both nutritional deficits and limited access to quality health care services.
The impact of economic status is equally profound. Sappani et al. (2023) demonstrated that severe and moderate anemia among Indian women of reproductive age was significantly associated with poverty, lack of education, and limited autonomy. Pathak et al. (1999) and Kapil et al. (1999) reported that anemia prevalence was disproportionately higher among women living in urban slums compared to the general population, with inadequate iron intake and poor sanitation being key factors.
More recent findings by Chakrabarti et al. (2018) and Samuel et al. (2013) suggest that even in urban and semi-urban contexts, consumption of foods containing iron absorption inhibitors (like phytates and tannins) further compounds the problem, despite supplementation programs. Mithra et al. (2013) and Vindhya et al. (2019) further noted low compliance with iron-folic acid (IFA) supplementation, especially among women with lower literacy and financial instability.
Collectively, these studies underscore that anemia among pregnant women is not solely a nutritional issue, but rather a complex condition influenced by a range of dietary, economic, cultural, and health system-related factors. However, there is limited evidence from cities like Meerut in western Uttar Pradesh, where urbanization, poverty pockets, and evolving dietary habits present a distinct context. This study aims to bridge that gap by examining both nutritional and economic determinants of anemia among pregnant women in Meerut City.
3. Methodology
This research study was conducted with the aim of assessing the prevalence of anemia among pregnant women in Meerut City, Uttar Pradesh, and examining the relationship between their nutritional status, economic position, and the occurrence of anemia. A systematic and comprehensive methodological approach was adopted to ensure the reliability, validity, and generalizability of the findings.
Study Design and Setting
This community-based cross-sectional study was conducted in Meerut City, western Uttar Pradesh, India. Meerut comprises 28 Government Urban Primary Health Centres (UPHCs) that provide antenatal care to women in urban and peri- areas. Data collection took place from April to June 2025.
Study Population and Sample Size
The target population was all pregnant women registered for antenatal care at the 28 UPHCs during the study period. A total sample of 210 pregnant women was determined sufficient to detect a 50% anemia prevalence with 95% confidence and 7% margin of error, accounting for a 10% nonresponse rate.
Sampling Procedure
A multistage stratified random sampling approach was used:
- Stratification: All 28 UPHCs were included to ensure representativeness of the city’s geographic zones.
- Allocation: The 210 participants were proportionately allocated to each UPHC based on the number of antenatal registrations in the preceding month.
- Participant Selection: From each UPHC, pregnant women were selected randomly from the ANC register using a simple random sampling method (lottery method or random number table), until the assigned number of participants for that center was reached.
- ➢
- Inclusion and Exclusion Criteria
Inclusion:
- Pregnant women of any gestational age
- Registered for ANC at one of the 28 UPHCs
- Resident of Meerut City for ≥ 6 months
- Provided written informed consent
Exclusion:
- Known chronic diseases unrelated to anemia (e.g., renal failure, malignancy)
- Blood transfusion within the last month
- Inability to participate due to severe illness or communication barriers
Data Collection
- A pre-tested, structured questionnaire was administered through face-to-face interviews in the local language (Hindi) by trained female field investigators. The questionnaire had the following sections:
- Demographic details: age, marital status, parity, education, occupation, religion.
- Socioeconomic status: family income, housing conditions, and asset ownership.
- Obstetric history: gestational age, previous pregnancies, birth intervals, miscarriage history.
- Nutritional habits: daily meal patterns, food group intake, iron-rich food consumption, and supplement usage.
- Health services utilization: number of antenatal visits, iron-folic acid tablet distribution and consumption.
- Hemoglobin values were extracted from each woman’s ANC record, reflecting in routine visits register hemoglobin meter testing recently conducted at the UPHC. Anemia was classified as per WHO criteria:
- Mild: 10.0–10.9 g/dL
- Moderate: 7.0–9.9 g/dL
- Severe: < 7.0 g/dL
Ethical Considerations
Ethical clearance was obtained from the Institutional Ethics Committee of Swami Vivekananda Subharti University Meerut, Uttar Pradesh, India all participants were informed about the objectives and procedures of the study, and written informed consent was obtained prior to data collection. Participation was entirely voluntary, and confidentiality of responses was strictly maintained. No invasive procedures were performed solely for the research purpose.
Statistical Analysis
Data were entered and analyzed using advance excel & JASP (Jeffreys's Amazing Statistics Program) is a free and open-source statistical software program
- Descriptive statistics: Means (± SD) for continuous variables; frequencies (%) for categorical variables.
- Bivariate analysis: Chi-square tests assessed associations between anemia status and categorical factors (socioeconomic and dietary variables).
- Multivariable logistic regression: Variables significant at p < 0.10 in bivariate analysis were entered into the model to identify independent predictors of anemia, adjusting for age, parity, and gestational age. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported.Statistical significance: Set at p < 0.05 for all tests.
4. Results
Figure 1.
Level of Anemia among Pregnant Women. The pie chart represents the distribution of anemia severity among pregnant women based on hemoglobin levels: Normal (≥11 g/dL), Mild anemia (10–10.9 g/dL), Moderate anemia (7–9.9 g/dL), and Severe anemia (<7 g/dL).
Figure 1.
Level of Anemia among Pregnant Women. The pie chart represents the distribution of anemia severity among pregnant women based on hemoglobin levels: Normal (≥11 g/dL), Mild anemia (10–10.9 g/dL), Moderate anemia (7–9.9 g/dL), and Severe anemia (<7 g/dL).
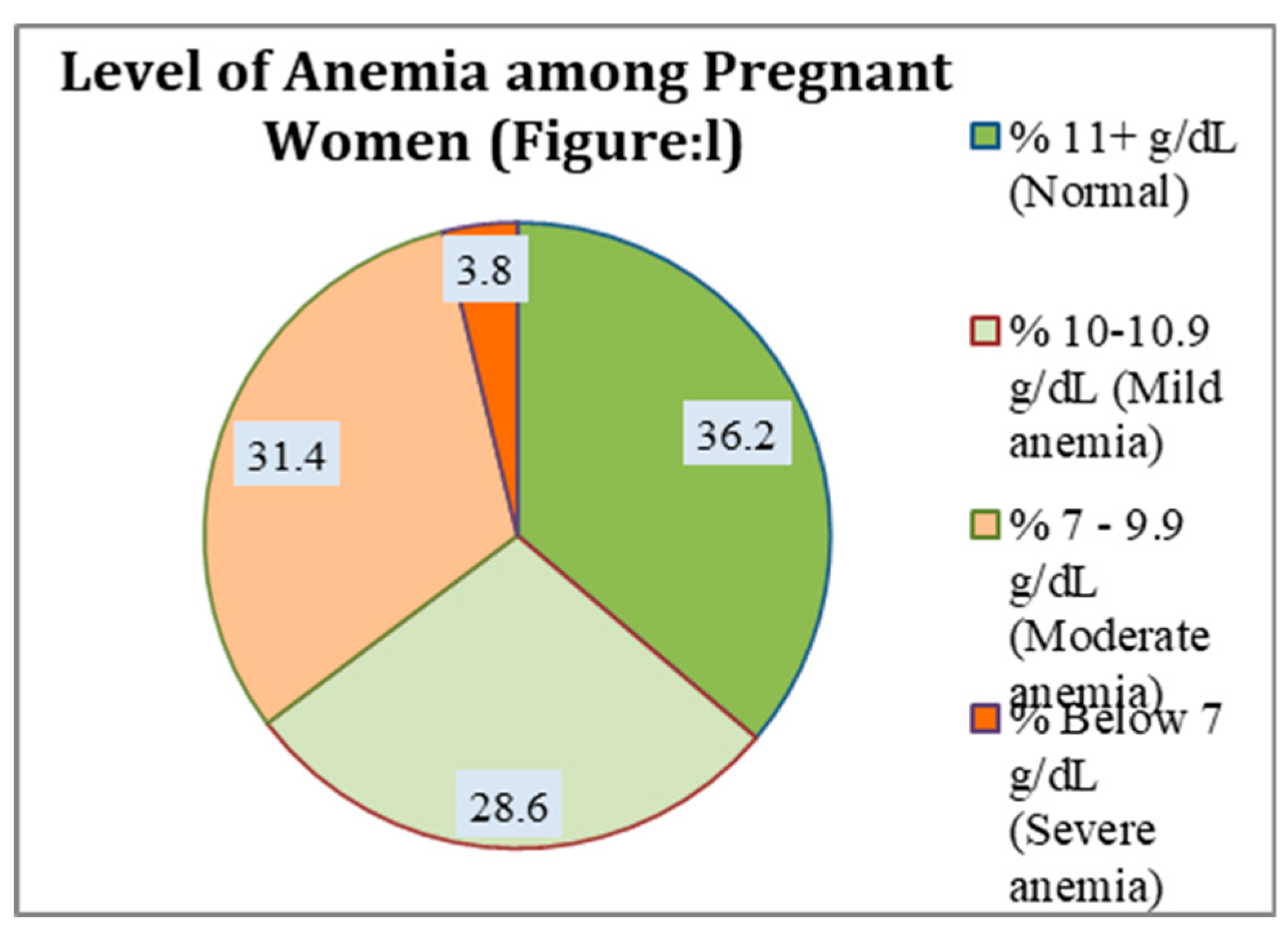
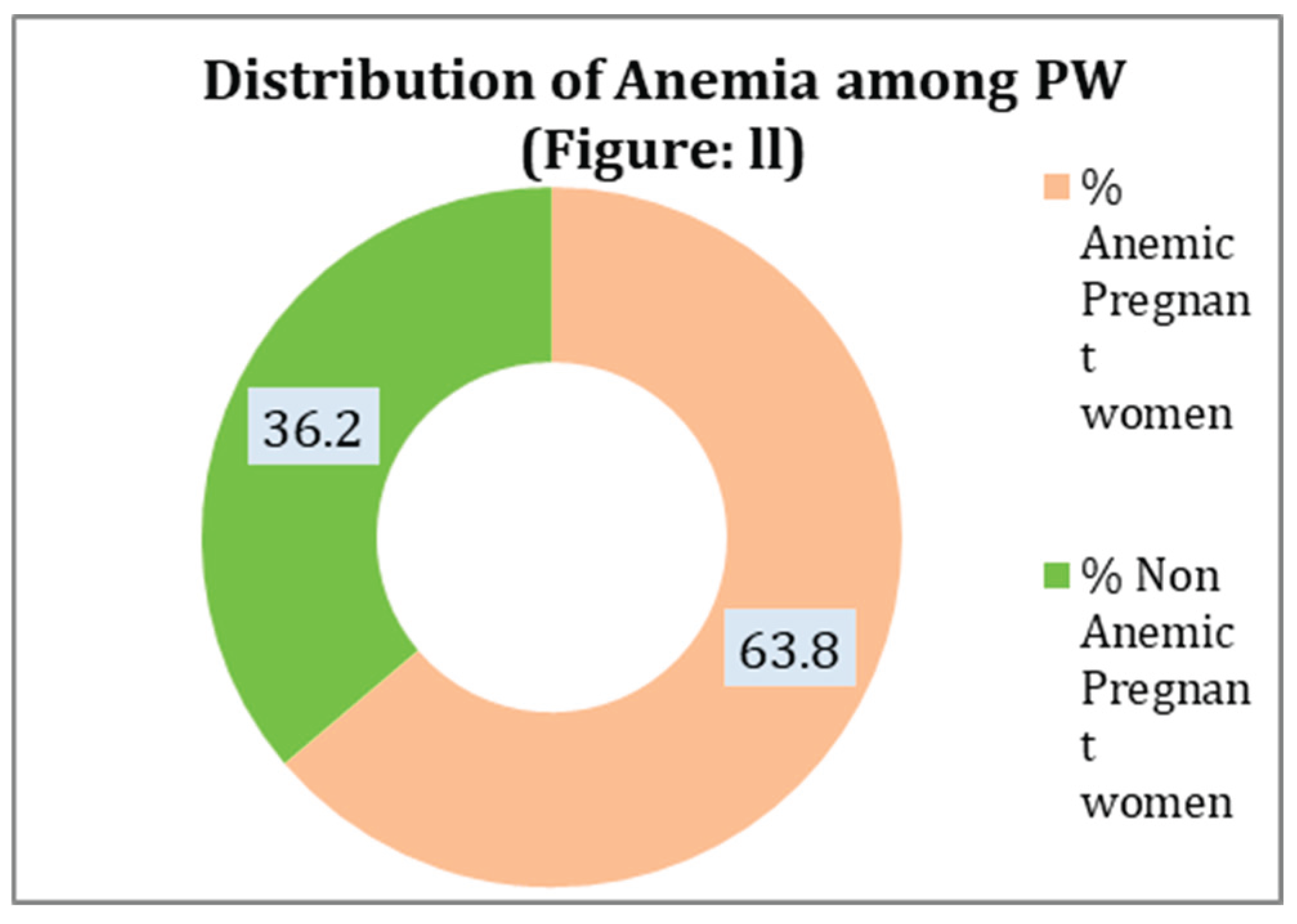
Figure 2.
Distribution of Anemia among Pregnant Women (PW). The donut chart shows the overall proportion of anemic (63.8%) and non-anemic (36.2%) pregnant women in the study population.
Figure 2.
Distribution of Anemia among Pregnant Women (PW). The donut chart shows the overall proportion of anemic (63.8%) and non-anemic (36.2%) pregnant women in the study population.

| The socio-demographic characteristics of expectant mothers (n = 210) | |||
| Variables | Anemic PW - 134 ( %) | Non Anemic PW - 76 (%) | Total - 210(%) |
| Women's age group who are pregnant | |||
| ≤ 20 | 9 (6.7) | 3 (3.9) | 12 (5.7) |
| Age 21-25 | 46 (34.3) | 31 (40.8) | 77 (36.7) |
| Age 26 -30 | 56 (41.8) | 33 (43.4) | 89 (42.4) |
| Age 31 -35 | 19 (14.2) | 7 (9.2) | 26 (12.4) |
| Age >35 | 4 (3.0) | 2 (2.6) | 6 (2.9) |
| Monthly household income | |||
| Low | 84 (62.7) | 10 (13.2) | 94 (44.8) |
| Medium | 39 (29.1) | 38 (50.0) | 77 (36.7) |
| High | 11 (8.2) | 28 (36.8) | 39 (18.6) |
| Pregnant women's educational attainment | |||
| No formal Education | 23 (17.2) | 7 (9.2) | 30 (14.3) |
| Primary & Middle (1-8) | 67 (50.0) | 28 (36.8) | 95 (45.2) |
| Secondary & Higher Secondary (9-12) | 37 (27.6) | 26 (34.2) | 63 (30.0) |
| UG & PG | 7 (5.2) | 15 (19.7) | 22 (10.5) |
| Religion of Pregnant women | |||
| Hindu & Other | 68 (50.7) | 45 (59.2) | 113 (53.8) |
| Muslim | 66 (49.3) | 31 (40.8) | 97 (46.2) |
| Category of Religion | |||
| General | 60 (44.8) | 33 (43.4) | 93 (44.3) |
| OBC | 53 (39.6) | 34 (44.7) | 87 (41.4) |
| SC | 21 (15.7) | 9 (11.8) | 30 (14.3) |
| Basic Amenities Are Available (Electricity, clean drinking water, sanitary amenities, television, air conditioning, laptop or computer, and automobile transportation) | |||
| Low | 40 (29.9) | 19 (25.0) | 59 (28.1) |
| Medium | 76 (56.7) | 20 (26.3) | 96 (45.7) |
| Normal | 18 (13.4) | 37 (48.7) | 55 (26.2) |
| Entertainment Activities (Watch TV, Go to the Movies, and Read the News) | |||
| Low | 73 (54.5) | 11 (14.5) | 84 (40.0) |
| Moderate | 34 (25.4) | 21 (27.6) | 55 (26.2) |
| High | 27 (20.1) | 44 (57.9) | 71 (33.8) |
| Size of the family | |||
| 3-5 | 16 (11.9) | 17 (22.4) | 33 (15.7) |
| More than 5 | 118 (88.1) | 59 (77.6) | 177 (84.3) |
| Obstetrics features of ANC participants at UPHC Meerut City town, March–June 2025 (N=210) | |||
| Variables | Anemic PW - 134 ( %) | Non Anemic PW - 76 (%) | Total - 210(%) |
| Gestational Age of Pregnant women | |||
| First Trimester | 3 (2.2) | 5 (6.6) | 8 (3.8) |
| Second trimester (13-26 weeks) | 36 (26.9) | 33 (43.4) | 69 (32.9) |
| Third trimester (27+ weeks) | 95 (70.9) | 38 (50.0) | 133 (63.3) |
| For this pregnancy, begin your first ANC visit | |||
| Before 12 weeks | 5 (3.7) | 7 (9.2) | 12 (5.7) |
| 12–20 weeks | 129 (96.3) | 68 (89.5) | 197 (93.8) |
| 21–28 weeks | 0 (0.0) | 1 (1.3) | 1 (0.5) |
| Women in Pregnancy Gravida | |||
| 1 | 25 (18.7) | 19 (25.0) | 44 (21.0) |
| 2 | 54 (40.3) | 34 (44.7) | 88 (41.9) |
| 3 | 42 (31.3) | 16 (21.1) | 58 (27.6) |
| 4 | 13 (9.7) | 7 (9.2) | 20 (9.5) |
| The parity of pregnant women | |||
| 0 | 45 (33.6) | 27 (35.5) | 72 (34.3) |
| 1 | 53 (39.6) | 33 (43.4) | 86 (41.0) |
| 2 | 27 (20.1) | 12 (15.8) | 39 (18.6) |
| 3 | 9 (6.7) | 4 (5.3) | 13 (6.2) |
| Birth Gap from the previous to the present | |||
| Primigravida | 31 (23.1) | 27 (35.5) | 58 (27.6) |
| <2 | 72 (53.7) | 28 (36.8) | 100 (47.6) |
| >2 | 31 (23.1) | 21 (27.6) | 52 (24.8) |
| Live Children in the Present | |||
| 0 | 30 (22.4) | 28 (36.8) | 58 (27.6) |
| 1 | 60 (44.8) | 30 (39.5) | 90 (42.9) |
| 2 | 37 (27.6) | 15 (19.7) | 52 (24.8) |
| 3 | 7 (5.2) | 3 (3.9) | 10 (4.8) |
| Dietary Habit ,Anemia and its awareness | |||
| Variables | Anemic PW - 134 ( %) | Non Anemic PW - 76 (%) | Total - 210(%) |
| Daily diet include :- Fruits, Vegetables, Dairy products, Protein (meat, fish, eggs),Junk Food (Noodles, bread, pasta) | |||
| Low | 87 (64.9) | 10 (13.2) | 97 (46.2) |
| Medium | 41 (30.6) | 37 (48.7) | 78 (37.1) |
| Normal | 6 (4.5) | 29 (38.2) | 35 (16.7) |
| Do you face financial constraints in purchasing nutritious food? | |||
| Yes | 104 (77.6) | 43 (56.6) | 147 (70.0) |
| No | 30 (22.4) | 33 (43.4) | 63 (30.0) |
| Consume foods high in iron, such as meat, beans, and green leafy vegetables | |||
| Daily | 5 (3.7) | 9 (11.8) | 14 (6.7) |
| 2-3 times/week | 9 (6.7) | 12 (15.8) | 21 (10.0) |
| Rarely | 120 (89.6) | 55 (72.4) | 175 (83.3) |
| Do you know how important it is to eat a balanced diet when pregnant? | |||
| Yes | 116 (86.6) | 69 (90.8) | 185 (88.1) |
| No | 18 (13.4) | 7 (9.2) | 25 (11.9) |
| How is your Iron/FA intake? | |||
| Daily | 36 (26.9) | 19 (25.0) | 55 (26.2) |
| Once in a week | 16 (11.9) | 13 (17.1) | 29 (13.8) |
| Sometime | 82 (61.2) | 44 (57.9) | 126 (60.0) |
| Do you follow a special diet during pregnancy | |||
| Yes | 19 (14.2) | 60 (78.9) | 79 (37.6) |
| No | 115 (85.8) | 16 (21.1) | 131 (62.4) |
| Knowledge of Anemia and Its Sources | |||
| High | 29 (21.6) | 35 (46.1) | 64 (30.5) |
| Moderate | 58 (43.3) | 18 (23.7) | 76 (36.2) |
| Low | 47 (35.1) | 23 (30.3) | 70 (33.3) |
| Factors associated with Prevalence of Anemia among pregnant women | |||||
| Variables | Anemic PW - 134 (%) | Non Anemic PW - 76 (%) | Total - 210(%) | Chi Square P-Value | Logistic Regression p-value |
| Household monthly Income | |||||
| Low | 84 (62.7) | 10 (13.2) | 94 (44.8) | 0.000* | 0.003** |
| Medium | 39 (29.1) | 38 (50.0) | 77 (36.7) | ||
| High | 11 (8.2) | 28 (36.8) | 39 (18.6) | ||
| Daily diet include :- Fruits, Vegetables, Dairy products, Protein (meat, fish, eggs),Junk Food (Noodles, bread, pasta) | |||||
| Low | 87 (64.9) | 10 (13.2) | 97 (46.2) | 0.000* | <0.001** |
| Medium | 41 (30.6) | 37 (48.7) | 78 (37.1) | ||
| Normal | 6 (4.5) | 29 (38.2) | 35 (16.7) | ||
| Knowledge of Anemia and Its Sources | |||||
| High | 29 (21.6) | 35 (46.1) | 64 (30.5) | 0.000* | 0.187*** |
| Moderate | 58 (43.3) | 18 (23.7) | 76 (36.2) | ||
| Low | 47 (35.1) | 23 (30.3) | 70 (33.3) | ||
| Pregnant women's educational attainment | |||||
| No formal Education | 23 (17.2) | 7 (9.2) | 30 (14.3) | 0.002* | 0.116*** |
| Primary & Middle (1-8) | 67 (50.0) | 28 (36.8) | 95 (45.2) | ||
| Secondary & Higher Secondary (9-12) | 37 (27.6) | 26 (34.2) | 63 (30.0) | ||
| UG & PG | 7 (5.2) | 15 (19.7) | 22 (10.5) | ||
* The result Chi-square is significant at p < .05, ** Logistic Regression p-value is significant at <.05 & *** p-value is not significant at <.05.
- ➢
- Interpretation of Key Findings:
The present study examined the sociodemographic, obstetric, dietary, and awareness-related factors associated with anemia among 210 pregnant women attending antenatal care at UPHC Meerut City, India. A high prevalence of anemia was observed among pregnant women with various interrelated risk factors identified.
Sociodemographic analysis revealed that most anemic women were in the age group of 26-30 years (41.8%), with a majority (62.7%) from low-income households, compared to only 13.2% of non-anemic women in the same income group, indicating a significant association between lower socioeconomic status and anemia. Educational attainment was also strongly linked; 17.2% of anemic women had no formal education, and 50% had only primary or middle school education, while higher educational levels were more prevalent among non-anemic women. Religious and caste-wise distribution showed comparable representation; however, social determinants such as low income and education likely contributed indirectly to anemia prevalence. Access to basic amenities was limited among anemic women, with 29.9% lacking adequate utilities, and entertainment activities were also minimal, reflecting broader socio-environmental deprivation.
Obstetric characteristics further highlighted that the majority of women (63.3%) initiated their first ANC visit in the second trimester or later, with 70.9% of anemic women presenting in the third trimester, indicating delayed healthcare engagement. Higher gravidity and parity were also associated with anemia, with 31.3% of anemic women being in their third pregnancy and 27% already having two living children. Short birth intervals (<2 years) were more common among anemic women (53.7%), suggesting that closely spaced pregnancies may contribute to nutritional depletion and higher anemia risk.
Dietary habits demonstrated a clear relationship with anemia. A significant proportion of anemic women (64.9%) reported poor dietary quality, with insufficient intake of fruits, vegetables, dairy products, proteins, and over-reliance on junk food. Financial barriers were substantial, with 77.6% of anemic women reporting economic constraints in purchasing nutritious food. Consumption of iron-rich foods was notably low; 89.6% of anemic women rarely consumed such foods. Despite good awareness regarding the importance of a balanced diet (86.6%), practical implementation was poor, as reflected in low adherence to daily iron and folic acid supplementation (only 26.9% daily intake among anemic women). Moreover, a majority of non-anemic women (78.9%) reported following a special diet during pregnancy, while 85.8% of anemic women did not, indicating that proactive dietary management may have a protective effect. Knowledge of anemia and its sources was moderate to low in most anemic women, with only 21.6% demonstrating high knowledge.
Multivariate analysis confirmed that low household income (p=0.003) and poor dietary quality (p<0.001) were strong independent predictors of anemia. While lower knowledge levels and lower education were associated with anemia in univariate analysis, they did not remain significant in multivariate regression, indicating that socioeconomic status and dietary habits may have a more direct influence on anemia risk.
Collectively, these findings underscore the complex interplay between socioeconomic deprivation, poor dietary habits, delayed antenatal care initiation, high parity, short interpregnancy intervals, and inadequate nutritional management as key contributors to anemia among pregnant women in this setting. Interventions focusing on improving household income, enhancing dietary quality, promoting timely ANC engagement, encouraging adequate birth spacing, and strengthening nutritional education and supplementation adherence are crucial for the effective prevention and control of anemia during pregnancy.
Summary and Conclusion
This study highlights a high burden of anemia among pregnant women attending antenatal care in Meerut City, with multifactorial determinants contributing to its prevalence. The findings demonstrate that low household income, poor dietary habits, financial constraints in purchasing nutritious food, delayed initiation of antenatal care, high parity, short birth intervals, and suboptimal adherence to iron and folic acid supplementation are significantly associated with anemia. While knowledge and awareness regarding the importance of a balanced diet were generally adequate, practical application in dietary behavior and supplementation compliance was limited among anemic women. Multivariate analysis identified low socioeconomic status and inadequate dietary intake as the most significant independent predictors of anemia.
The results emphasize the urgent need for comprehensive, multi-sectoral strategies that address the underlying social determinants of health, including poverty alleviation, nutritional education, dietary support programs, improved access to affordable nutritious foods, early and regular antenatal care, and effective counseling on adherence to iron and folic acid supplementation. Strengthening these interventions is essential for reducing the burden of anemia, improving maternal and fetal outcomes, and advancing maternal health goals.
5. Discussion
This study investigated the multifactorial determinants of anemia among pregnant women attending antenatal care services at UPHC Meerut City. The findings revealed a high prevalence of anemia, with significant associations observed across sociodemographic, obstetric, dietary, and behavioral domains.
Sociodemographic analysis indicated that anemia was disproportionately prevalent among women from lower-income households with limited educational attainment and restricted access to basic amenities. Financial constraints likely limit the ability to procure diverse, nutrient-rich foods, directly contributing to nutritional anemia. These findings are consistent with prior studies that have identified low socioeconomic status as a significant risk factor for maternal anemia.
Obstetric characteristics further influenced anemia risk. The majority of anemic women initiated antenatal care in the second or third trimester, delaying timely identification and management of anemia. Higher gravidity, increased parity, and short birth intervals were commonly observed among anemic women, suggesting cumulative nutritional depletion over successive pregnancies. These patterns underscore the need for family planning services and public health education promoting adequate birth spacing and early antenatal care enrollment.
Dietary practices were strongly associated with anemia status. Despite adequate general awareness of the importance of balanced nutrition during pregnancy, many anemic women reported poor dietary quality, characterized by insufficient intake of iron-rich foods and overconsumption of nutrient-poor options. Financial barriers, limited dietary diversity, and inconsistent adherence to iron and folic acid supplementation exacerbated their vulnerability. In contrast, non-anemic women more frequently adopted special pregnancy diets and adhered to supplementation regimens, demonstrating the protective effect of effective nutritional management.
Although knowledge about anemia and its dietary sources was statistically associated with anemia status in univariate analysis, it did not retain significance in multivariate regression. This suggests that knowledge alone may be insufficient to drive behavior change in the presence of socioeconomic and systemic barriers.
These findings highlight the complex interplay of social determinants, obstetric history, dietary habits, and health behaviors in the etiology of anemia during pregnancy. Comprehensive and integrated interventions are necessary to address these intersecting risk factors and reduce anemia prevalence effectively.
6. Conclusion
Anemia remains highly prevalent among pregnant women in this urban setting, primarily driven by low socioeconomic status, poor dietary diversity, and suboptimal nutritional practices. Strengthening antenatal care services with a focus on poverty alleviation, nutritional counseling, early antenatal care initiation, and enhanced iron and folic acid supplementation adherence is critical to reducing anemia burden and improving maternal and neonatal health outcomes.The study highlights a high burden of anemia among pregnant women in Meerut City, with nutritional inadequacy and economic deprivation being the major contributing factors. These findings emphasize the urgent need for integrated antenatal interventions focusing on improving maternal nutrition, dietary counselling, and addressing underlying socioeconomic inequalities. Strengthening existing national programs such as Anemia Mukt Bharat with local-level nutritional surveillance and community-based education can play a pivotal role in reducing the anemia burden among pregnant women in urban India.
Conflict of interest
The authors declare no conflict of interest regarding the publication of this article.
Source of funding
This research received no external funding.
Data availability statement
This is a review article and does not include any primary data. All data discussed are from previously published studies cited in the reference list.
Transparency statement
The corresponding author (Dr. Prem Kumar) affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
References
- Abriha, A., Yesuf, M.E. & Wassie, M.M. Prevalence and associated factors of anemia among pregnant women of Mekelle town: a cross sectional study. BMC Res Notes 7, 888 (2014).
- Tibambuya BA, Ganle JK, Ibrahim M. Anaemia at antenatal care initiation and associated factors among pregnant women in West Gonja District, Ghana: a cross-sectional study. Pan Afr Med J. 2019 Aug 27;33:325. [CrossRef] [PubMed] [PubMed Central]
- Anlaakuu P, Anto F. Anaemia in pregnancy and associated factors: a cross sectional study of antenatal attendants at the Sunyani Municipal Hospital, Ghana. BMC Res Notes. 2017 Aug 11;10(1):402.
- Adjei-Gyamfi S, Asirifi A, Peprah W, Abbey DA, Hamenoo KW, Zakaria MS, Mohammed O, Aryee PA. Anaemia at 36 weeks of pregnancy: Prevalence and determinants among antenatal women attending peri-urban facilities in a developing country, Ghana. PLOS Glob Public Health. 2024 Sep 5;4(9):e0003631. [CrossRef] [PubMed] [PubMed Central]
- Kumari S, Garg N, Kumar A, Guru PKI, Ansari S, Anwar S, Singh KP, Kumari P, Mishra PK, Gupta BK, Nehar S, Sharma AK, Raziuddin M, Sohail M. Maternal and severe anaemia in delivering women is associated with risk of preterm and low birth weight: A cross sectional study from Jharkhand, India. One Health. 2019 Aug 19;8:100098. [CrossRef] [PubMed] [PubMed Central]
- Baig-Ansari N, Badruddin SH, Karmaliani R, Harris H, Jehan I, Pasha O, Moss N, McClure EM, Goldenberg RL. Anemia prevalence and risk factors in pregnant women in an urban area of Pakistan. Food Nutr Bull. 2008 Jun;29(2):132-9. [CrossRef] [PubMed] [PubMed Central]
- Sappani M, Mani T, Asirvatham ES, Joy M, Babu M, Jeyaseelan L. Trends in prevalence and determinants of severe and moderate anaemia among women of reproductive age during the last 15 years in India. PLoS One. 2023 Jun 1;18(6):e0286464. [CrossRef] [PubMed] [PubMed Central]
- Perumal V. Reproductive risk factors assessment for anaemia among pregnant women in India using a multinomial logistic regression model. Trop Med Int Health. 2014 Jul;19(7):841-51. Epub 2014 Apr 7. 2014. [CrossRef] [PubMed]
- Tirore LL, Mulugeta A, Belachew AB, Gebrehaweria M, Sahilemichael A, Erkalo D, Atsbha R. Factors associated with anaemia among women of reproductive age in Ethiopia: Multilevel ordinal logistic regression analysis. Matern Child Nutr. 2021 Jan;17(1):e13063. Epub 2020 Aug 5. [CrossRef] [PubMed] [PubMed Central]
- Ara G, Hassan R, Haque MA, Boitchi AB, Ali SD, Kabir KS, Mahmud RI, Islam KA, Rahman H, Islam Z. Anaemia among adolescent girls, pregnant and lactating women in the southern rural region of Bangladesh: Prevalence and risk factors. PLoS One. 2024 Jul 10;19(7):e0306183. [CrossRef] [PubMed] [PubMed Central]
- Grover K, Kumar T, Doda A, Bhutani R, Yadav S, Kaushal P, Kapoor R, Sharma S. Prevalence of anaemia and its association with dietary habits among pregnant women in the urban area of Haryana. J Family Med Prim Care. 2020 Feb 28;9(2):783-787. [CrossRef] [PubMed] [PubMed Central]
- Diamond-Smith NG, Gupta M, Kaur M, Kumar R. Determinants of Persistent Anemia in Poor, Urban Pregnant Women of Chandigarh City, North India: A Mixed Method Approach. Food Nutr Bull. 2016 Jun;37(2):132-43. Epub 2016 Mar 23. [CrossRef] [PubMed]
- Mithra P, Unnikrishnan B, Rekha T, Nithin K, Mohan K, Kulkarni V, Kulkarni V, Agarwal D. Compliance with iron-folic acid (IFA) therapy among pregnant women in an urban area of south India. Afr Health Sci. 2013 Dec;13(4):880-5. [CrossRef] [PubMed] [PubMed Central]
- Perumal V. Reproductive risk factors assessment for anaemia among pregnant women in India using a multinomial logistic regression model. Trop Med Int Health. 2014 Jul;19(7):841-51. Epub 2014 Apr 7. [CrossRef] [PubMed]
- Kapil U, Pathak P, Tandon M, Singh C, Pradhan R, Dwivedi SN. Micronutrient deficiency disorders amongst pregnant women in three urban slum communities of Delhi. Indian Pediatr. 1999 Oct;36(10):983-9. [PubMed]
- Pathak P, Tandon M, Kapil U, Singh C. Prevalence of iron deficiency anemia amongst pregnant women in urban slum communities of Delhi. Indian Pediatr. 1999 Mar;36(3):322-3. [PubMed]
- Chotnopparatpattara P, Limpongsanurak S, Charnngam P. The prevalence and risk factors of anemia in pregnant women. J Med Assoc Thai. 2003 Nov;86(11):1001-7. [PubMed]
- Alper BS, Kimber R, Reddy AK. Using ferritin levels to determine iron-deficiency anemia in pregnancy. J Fam Pract. 2000 Sep;49(9):829-32. [PubMed]
- 19. Gayathri S, Manikandanesan S, Venkatachalam J, Gokul S, Yashodha A, Premarajan KC. Coverage of and compliance to iron supplementation under the National Iron Plus Initiative among reproductive age-group women in urban Puducherry - a cross-sectional study. Int J Adolesc Med Health. 2019 Apr 11;33(2). [CrossRef] [PubMed]
- Samuel TM, Thomas T, Finkelstein J, Bosch R, Rajendran R, Virtanen SM, Srinivasan K, Kurpad AV, Duggan C. Correlates of anaemia in pregnant urban South Indian women: a possible role of dietary intake of nutrients that inhibit iron absorption. Public Health Nutr. 2013 Feb;16(2):316-24. Epub 2012 May 11. [CrossRef] [PubMed] [PubMed Central]
- Vindhya J, Nath A, Murthy GVS, Metgud C, Sheeba B, Shubhashree V, Srinivas P. Prevalence and risk factors of anemia among pregnant women attending a public-sector hospital in Bangalore, South India. J Family Med Prim Care. 2019 Jan;8(1):37-43. [CrossRef] [PubMed] [PubMed Central]
- Pathak P, Tandon M, Kapil U, Singh C. Prevalence of iron deficiency anemia amongst pregnant women in urban slum communities of Delhi. Indian Pediatr. 1999 Mar;36(3):322-3. [PubMed]
- Chakrabarti S, George N, Majumder M, Raykar N, Scott S. Identifying sociodemographic, programmatic and dietary drivers of anaemia reduction in pregnant Indian women over 10 years. Public Health Nutr. 2018 Sep;21(13):2424-2433. Epub 2018 Apr 12. [CrossRef] [PubMed] [PubMed Central]
- Kaur M, Chauhan A, Manzar MD, Rajput MM. Maternal Anaemia and Neonatal Outcome: A Prospective Study on Urban Pregnant Women. J Clin Diagn Res. 2015 Dec;9(12):QC04-8. Epub 2015 Dec 1. [CrossRef] [PubMed] [PubMed Central]
- Thasneem NB, Kaimal RS, Thengu Murichathil AH. Study of sociodemographic factors and perceptions of women in the reproductive age group with anaemia - A hospital-based cross-sectional study in South India. J Family Med Prim Care. 2025 Apr;14(4):1338-1345. Epub 2025 Apr 25. [CrossRef] [PubMed] [PubMed Central]
- Perumal V. Reproductive risk factors assessment for anaemia among pregnant women in India using a multinomial logistic regression model. Trop Med Int Health. 2014 Jul;19(7):841-51. Epub 2014 Apr 7. [CrossRef] [PubMed]
- Ghosal J, Bal M, Ranjit M, Das A, Behera MR, Satpathy SK, Dutta A, Pati S. To what extent classic socio-economic determinants explain trends of anaemia in tribal and non-tribal women of reproductive age in India? Findings from four National Family Heath Surveys (1998-2021). BMC Public Health. 2023 May 11;23(1):856. [CrossRef] [PubMed] [PubMed Central]
- Dutta PK, Urmil AC, Gund SS, Dutta M. Utilisation of health services by "high risk" pregnant women in a semi urban community of Pune -- an analytical study. Indian J Matern Child Health. 1990 Jan-Mar;1(1):15-9. [PubMed]
- Thasneem NB, Kaimal RS, Thengu Murichathil AH. Study of sociodemographic factors and perceptions of women in the reproductive age group with anaemia - A hospital-based cross-sectional study in South India. J Family Med Prim Care. 2025 Apr;14(4):1338-1345. Epub 2025 Apr 25. [CrossRef] [PubMed] [PubMed Central]
- Larson LM, Thomas T, Kurpad AV, Martorell R, Hoddinott J, Adebiyi VO, Swaminathan S, Neufeld LM. Predictors of anaemia in mothers and children in Uttar Pradesh, India. Public Health Nutr. 2024 Jan 8;27(1):e30. 2024. [CrossRef] [PubMed] [PubMed Central]
- Dwarkanath P, Vasudevan A, Thomas T, Anand SS, Desai D, Gupta M, Menezes G, Kurpad AV, Srinivasan K. Socio-economic, environmental and nutritional characteristics of urban and rural South Indian women in early pregnancy: findings from the South Asian Birth Cohort (START). Public Health Nutr. 2018 Jun;21(8):1554-1564. Epub 2018 Feb 5. [CrossRef] [PubMed] [PubMed Central]
- Perumal V. Reproductive risk factors assessment for anaemia among pregnant women in India using a multinomial logistic regression model. Trop Med Int Health. 2014 Jul;19(7):841-51. Epub 2014 Apr 7. [CrossRef] [PubMed]
- Abdallah F, John SE, Hancy A, Paulo HA, Sanga A, Noor R, Lankoande F, Chimanya K, Masumo RM, Leyna GH. Prevalence and factors associated with anaemia among pregnant women attending reproductive and child health clinics in Mbeya region, Tanzania. PLOS Glob Public Health. 2022 Oct 5;2(10):e0000280. [CrossRef] [PubMed] [PubMed Central]
- Derso T, Abera Z, Tariku A. Magnitude and associated factors of anemia among pregnant women in Dera District: a cross-sectional study in northwest Ethiopia. BMC Res Notes. 2017 Aug 1;10(1):359. [CrossRef] [PubMed] [PubMed Central]
- Aziz Ali S, Abbasi Z, Feroz A, Hambidge KM, Krebs NF, Westcott JE, Saleem S. Factors associated with anemia among women of the reproductive age group in Thatta district: study protocol. Reprod Health. 2019 Mar 18;16(1):34. [CrossRef] [PubMed] [PubMed Central]
- Mankelkl G, Kinfe B. Sociodemographic factors associated with anemia among reproductive age women in Mali; evidenced by Mali malaria indicator survey 2021: spatial and multilevel mixed effect model analysis. BMC Womens Health. 2023 May 27;23(1):291. [CrossRef] [PubMed] [PubMed Central]
- Kare AP, Gujo AB. Anemia among Pregnant Women Attending Ante Natal Care Clinic in Adare General Hospital, Southern Ethiopia: Prevalence and Associated Factors. Health Serv Insights. 2021 Jul 29;14:11786329211036303. [CrossRef] [PubMed] [PubMed Central]
- Ouzennou N, Amor H, Baali A. Socio-economic, cultural and demographic profile of a group of Moroccan anaemic pregnant women. Afr Health Sci. 2019 Sep;19(3):2654-2659. 2019. [CrossRef] [PubMed] [PubMed Central]
- Lebso M, Anato A, Loha E. Prevalence of anemia and associated factors among pregnant women in Southern Ethiopia: A community based cross-sectional study. PLoS One. 2017 Dec 11;12(12):e0188783. [CrossRef] [PubMed] [PubMed Central]
- Gedefaw L, Ayele A, Asres Y, Mossie A. Anemia and Associated Factors Among Pregnant Women Attending Antenatal Care Clinic in Wolayita Sodo Town, Southern Ethiopia. Ethiop J Health Sci. 2015 Apr;25(2):155-62. [CrossRef] [PubMed] [PubMed Central]
- Abriha A, Yesuf ME, Wassie MM. Prevalence and associated factors of anemia among pregnant women of Mekelle town: a cross sectional study. BMC Res Notes. 2014 Dec 9;7:888. [CrossRef] [PubMed] [PubMed Central]
- Ouzennou N, Tikert K, Belkedim G, Jarhmouti FE, Baali A. Prévalence et déterminants sociaux de l'anémie chez les femmes enceintes dans la Province d'Essaouira, Maroc [Prevalence and social determinants of anemia in pregnant women in Essaouira Province, Morocco]. Sante Publique. 2018 September-October;30(5):737-745. [CrossRef] [PubMed]
- Azzam A, Khaled H, Alrefaey AK, Basil A, Ibrahim S, Elsayed MS, Khattab M, Nabil N, Abdalwanees E, Halim HWA. Anemia in pregnancy: a systematic review and meta-analysis of prevalence, determinants, and health impacts in Egypt. BMC Pregnancy Childbirth. 2025 Jan 14;25(1):29. [CrossRef] [PubMed] [PubMed Central]
- Eweis M, Farid EZ, El-Malky N, Abdel-Rasheed M, Salem S, Shawky S. Prevalence and determinants of anemia during the third trimester of pregnancy. Clin Nutr ESPEN. 2021 Aug;44:194-199. Epub 2021 Jul 2. [CrossRef] [PubMed]
- Workicho A, Belachew T, Ghosh S, Kershaw M, Lachat C, Kolsteren P. Burden and determinants of undernutrition among young pregnant women in Ethiopia. Matern Child Nutr. 2019 Jul;15(3):e12751. Epub 2018 Dec 11. [CrossRef] [PubMed] [PubMed Central]
- Diddana TZ. Factors associated with dietary practice and nutritional status of pregnant women in Dessie town, northeastern Ethiopia: a community-based cross-sectional study. BMC Pregnancy Childbirth. 2019 Dec 23;19(1):517. [CrossRef] [PubMed] [PubMed Central]
- Gebremichael MA, Belachew Lema T. Dietary Diversity, Nutritional Status, and Associated Factors Among Pregnant Women in Their First Trimester of Pregnancy in Ambo District, Western Ethiopia. Nutr Metab Insights. 2023 Aug 22;16:11786388231190515. [CrossRef] [PubMed] [PubMed Central]
- Muze M, Yesse M, Kedir S, Mustefa A. Prevalence and associated factors of undernutrition among pregnant women visiting ANC clinics in Silte zone, Southern Ethiopia. BMC Pregnancy Childbirth. 2020 Nov 19;20(1):707. [CrossRef] [PubMed] [PubMed Central]
- Ahmed A, Mohammed A, Ateye MD, Abdusamed S. Prevalence of undernutrition and associated factors among adolescent pregnant women in Dolo-Ado town, Somali region, Ethiopia. BMC Pregnancy Childbirth. 2025 Jan 31;25(1):105. [CrossRef] [PubMed] [PubMed Central]
- Vindhya J, Nath A, Murthy GVS, Metgud C, Sheeba B, Shubhashree V, Srinivas P. Prevalence and risk factors of anemia among pregnant women attending a public-sector hospital in Bangalore, South India. J Family Med Prim Care. 2019 Jan;8(1):37-43. [CrossRef] [PubMed] [PubMed Central]
- Nair MS, Raphael L, Chandran P. Prevalence of anaemia and associated factors among antenatal women in rural Kozhikode, Kerala. J Family Med Prim Care. 2022 May;11(5):1851-1857. Epub 2022 May 14. [CrossRef] [PubMed] [PubMed Central]
- Bharati P, Som S, Chakrabarty S, Bharati S, Pal M. Prevalence of anemia and its determinants among nonpregnant and pregnant women in India. Asia Pac J Public Health. 2008;20(4):347-59. [CrossRef] [PubMed]
- Jin Y, Talegawkar SA, Sedlander E, DiPietro L, Parida M, Ganjoo R, Aluc A, Rimal R. Dietary Diversity and Its Associations with Anemia among Women of Reproductive Age in Rural Odisha, India. Ecol Food Nutr. 2022 May-Jun;61(3):304-318. Epub 2021 Oct 13. [CrossRef] [PubMed]
- Pathak P, Kapil U, Kapoor SK, Saxena R, Kumar A, Gupta N, Dwivedi SN, Singh R, Singh P. Prevalence of multiple micronutrient deficiencies amongst pregnant women in a rural area of Haryana. Indian J Pediatr. 2004 Nov;71(11):1007-14. [CrossRef] [PubMed]
- Debnath A, Debbarma A, Debbarma SK, Bhattacharjya H. Proportion of anaemia and factors associated with it among the attendees of the antenatal clinic in a teaching institute of northeast India. J Family Med Prim Care. 2021 Jan;10(1):283-288. Epub 2021 Jan 30. [CrossRef] [PubMed] [PubMed Central]
- Ghosh P, Dasgupta A, Paul B, Roy S, Biswas A, Yadav A. A cross-sectional study on prevalence and determinants of anemia among women of reproductive age in a rural community of West Bengal. J Family Med Prim Care. 2020 Nov 30;9(11):5547-5553. [CrossRef] [PubMed] [PubMed Central]
- Bobdey S, Sinha S. Prevalence of anemia among women: A pilot study. Med J Armed Forces India. 2012 Oct;68(4):407-9. https://doi.org/10.1016/j.mjafi.2012.04.019. Epub 2012 Aug 22. Epub 2012 Aug 22. [CrossRef] [PubMed] [PubMed Central]
- Mehrotra M, Yadav S, Deshpande A, Mehrotra H. A study of the prevalence of anemia and associated sociodemographic factors in pregnant women in Port Blair, Andaman and Nicobar Islands. J Family Med Prim Care. 2018 Nov-Dec;7(6):1288-1293. [CrossRef] [PubMed] [PubMed Central]
- Pradhan S, Karna T, Singha D, Bhatta P, Rath K, Behera A. Prevalence and risk factor of anemia among pregnant women admitted in antenatal ward in PBMH Bhubaneswar, Odisha. J Family Med Prim Care. 2023 Nov;12(11):2875-2879. Epub 2023 Nov 21. [CrossRef] [PubMed] [PubMed Central]
- Samuel TM, Thomas T, Finkelstein J, Bosch R, Rajendran R, Virtanen SM, Srinivasan K, Kurpad AV, Duggan C. Correlates of anaemia in pregnant urban South Indian women: a possible role of dietary intake of nutrients that inhibit iron absorption. Public Health Nutr. 2013 Feb;16(2):316-24. Epub 2012 May 11. [CrossRef] [PubMed] [PubMed Central]
- Sharma N, Kishore J, Gupta M, Singla H, Dayma R, Sharma JB. The Minimum Dietary Diversity for Women (MDD-W) Score: Its Association With the Prevalence and Severity of Anemia in Pregnancy. Cureus. 2024 Aug 5;16(8):e66248. [CrossRef] [PubMed] [PubMed Central]
- Lukose A, Ramthal A, Thomas T, Bosch R, Kurpad AV, Duggan C, Srinivasan K. Nutritional factors associated with antenatal depressive symptoms in the early stage of pregnancy among urban South Indian women. Matern Child Health J. 2014 Jan;18(1):161-170. [CrossRef] [PubMed]
- Kalaivani K. Prevalence & consequences of anaemia in pregnancy. Indian J Med Res. 2009 Nov;130(5):627-33. [PubMed]
- Thasneem NB, Kaimal RS, Thengu Murichathil AH. Study of sociodemographic factors and perceptions of women in the reproductive age group with anaemia - A hospital-based cross-sectional study in South India. J Family Med Prim Care. 2025 Apr;14(4):1338-1345. Epub 2025 Apr 25. [CrossRef] [PubMed] [PubMed Central]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



