Submitted:
21 June 2025
Posted:
24 June 2025
Read the latest preprint version here
Abstract
Background: The dietary habits of healthcare professionals, particularly dentists, are frequently compromised by demanding work schedules and occupational stress. These factors contribute to poor dietary choices, irregular eating patterns, and inadequate nutrient intake, negatively impacting both general and oral health. Methods: This comprehensive review analyzed literature on dietary habits, nutrition education, work environments, and oral health outcomes among healthcare professionals, with a particular focus on dentists. A systematic search of PubMed, Scopus, and the Cochrane Library was conducted using MeSH terms and keywords including "Dentists," "Dentistry," "Oral Health," "Diet," "Nutrition," "Nutrition Education," "Work Environ-ment," "Occupational Stress," "Physical Activity," and "Well-being." Studies published in English from 2010 to 2024 were included. Screening, quality assessment, and data extraction followed predefined criteria, and findings were narratively synthesized. Results: Of 617 articles screened, 27 met inclusion criteria. The findings demonstrate that occupational stress and poor workplace environments contribute to unhealthy dietary behaviors, which are linked to increased risks of oral disease, burnout, and poor overall well-being. Conversely, balanced nutrition, structured wellness routines, and interprofessional education were associated with improved oral and systemic health outcomes, including better oral hygiene, lower BMI, improved cardiometabolic markers, and enhanced mental health. Conclusions: Systemic integration of nutrition education into dental training, institutional policies promoting healthy workplace environments, and interprofessional collaboration are essential to support dentists’ well-being and clinical practice. Targeted interventions addressing the specific challenges of dental professionals, particularly those related to shift work and stress, are needed. Further longitudinal and interventional research is required to guide evidence-based strategies that improve both personal health and professional performance in dental practice.
Keywords:
healthcare professionals
; dentists
; oral health
; nutrition
; dietary habits
; work environment
; occupational stress
; mental well-being
; shift work
; health promotion
1. Introduction
Healthcare professionals, including dentists, play a crucial role in promoting public health by delivering both preventive and therapeutic services [1,2]. Their responsibilities extend beyond clinical care to encompass patient education, particularly in encouraging healthier lifestyle choices [3,4,5]. However, despite their expertise in health promotion, many healthcare professionals struggle to maintain optimal dietary habits due to the demands of their work environments [6]. Factors such as long working hours, high stress levels, and irregular schedules frequently disrupt eating patterns, contributing to unhealthy food choices, missed meals, and inadequate nutrient intake [1,7]. Among dentists, these challenges are further exacerbated by the limited availability of nutritious food options during clinical hours, resulting in increased reliance on quick, processed meals [6,8].
Further, poor dietary habits among healthcare professionals have wide-ranging implications for their physical and mental health [3]. Unhealthy eating behaviors, including frequent consumption of fast food and sugary snacks, are associated with an elevated risk of chronic conditions such as obesity, cardiovascular disease, and type 2 diabetes [3,9]. These patterns not only undermine personal well-being but can also impair professional performance [10]. Inadequate hydration and unbalanced meals during work shifts have been linked to cognitive fatigue, diminished alertness, and impaired decision-making, factors that compromise both patient safety and care quality [10,11]. There is a critical need for systemic interventions that support the nutrition and overall well-being of healthcare workers [10,12].
For dental professionals, the relationship between dietary habits and clinical practice is particularly significant, as nutrition directly influences oral health outcomes [13]. Nutritional deficiencies or imbalances are strongly linked to dental caries, periodontal disease, and other oral conditions, which may in turn affect clinical performance and dentists’ credibility as role models for healthy living [13,14]. The intersection of general and oral health highlights the importance of integrating nutritional counseling into dental practice [15]. Yet current evidence reveals a gap: relatively few dentists incorporate dietary advice into routine care [16]. Enhanced collaboration between dietitians and dentists could help address this gap and promote a more comprehensive approach to both oral and systemic health [15].
Globally, healthcare professionals face a variety of individual and systemic barriers to maintaining healthy dietary habits [3]. One prominent challenge is a lack of knowledge regarding evidence-based nutritional guidelines, often due to limited nutrition education in medical and dental training [17]. Many healthcare professionals report low confidence in their nutrition knowledge, contributing to inconsistent dietary practices [18,19]. Additionally, workplace environments often fail to support healthy eating, offering limited nutritious options and insufficient time for meal breaks [20,21]. These systemic shortcomings contribute to a workplace culture in which poor dietary habits are normalized [3]. Of course, these challenges affect not only physical health but also mental well-being [22]. High stress levels and demanding schedules contribute to emotional eating, characterized by consumption of high-calorie, nutrient-poor foods as a coping mechanism [23]. Emotional eating has been linked to burnout and job dissatisfaction, further underlining the interconnectedness of nutrition and professional well-being [22]. Among dentists, this issue is especially pronounced, given the profession’s demands for precision and extensive patient interaction [8].
Shift work is another factor that profoundly influences healthcare professionals’ dietary habits [7]. Irregular hours disrupt circadian rhythms, adversely affecting meal timing and dietary quality [24,25]. Shift workers often consume energy-dense foods during night shifts and skip breakfast, a pattern associated with metabolic disorders and weight gain [3,9]. Dentists working in hospital or emergency settings face similar disruptions, making it difficult to maintain balanced diets [7]. Addressing these challenges requires policies that support regular meal breaks and access to healthy food options even during unconventional hours [7,22].
Cultural and societal factors also shape healthcare professionals’ dietary behaviors [25]. In some regions, traditional dietary practices may conflict with modern nutrition guidelines [15]. Additionally, the social expectation that healthcare professionals serve as role models can produce guilt and reluctance to seek support for dietary improvement [26].
Integrating nutrition education into medical and dental curricula is a promising strategy to improve healthcare professionals’ dietary habits [25]. Formal nutrition training is associated with healthier eating behaviors among clinicians and greater confidence in providing dietary counseling to patients [15,16]. For dentists, enhancing knowledge of the diet-oral health relationships can translate into more effective care and improved outcomes [13]. In addition, continuing education and practical training workshops can help close existing knowledge gaps and reinforce healthy habits [16]. Workplace interventions also offer considerable potential to improve healthcare professionals’ nutrition [27]. Providing healthy meal options, allocating protected meal times, and enhancing a supportive culture can positively influence dietary behaviors [10,27]. Peer support groups and wellness initiatives may further encourage positive changes [23]. When combined with policy-level reforms, these strategies can cultivate a sustainable framework to enhance healthcare professionals’ health and performance [27].
This comprehensive review addresses the current lack of research on the relationship between dietary habits and oral health among dentists. While the nutrition of healthcare professionals has been studied in general, the unique challenges dentists face, including irregular schedules, elevated stress, and demanding workloads, have been relatively overlooked [14]. These factors contribute to suboptimal dietary behaviors that can adversely affect both general and oral health. This review also explores the limited integration of nutritional counseling into dental practice, highlighting the need for enhanced nutrition education and greater interdisciplinary collaboration with dietitians. Furthermore, the review identifies a gap in understanding how occupational stress influences dentists’ dietary behaviors, as well as a lack of longitudinal research on the long-term health and professional consequences of poor nutrition. Addressing these gaps can help inform targeted interventions to support dentists’ well-being and ultimately improve patient care.
2. Materials and Methods
The methodology employed a comprehensive search strategy using databases such as PubMed, Scopus, and Cochrane, with a focus on quantitative and systematic studies to examine how the pandemic has influenced the health and work-life conditions of dental professionals [28]. Quality assessment, data extraction, and statistical analysis were conducted following established protocols, including the Newcastle-Ottawa Scale and SPSS tools (IBM, 2022)[29]. The search process was also aligned with the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) (https://www.prisma-statement.org/). Inclusion and exclusion criteria were carefully defined to ensure the selection of relevant studies for this review. Eligible studies were those published between 2005 and 2024, written in English, focusing on the impact of nutrition and oral health on healthcare professionals, specifically dentists. This timeframe was chosen to capture developments in research methodologies and the growing awareness of the role of diet in oral and overall health over the past two decades. Studies in English were prioritized to maintain accessibility for the review team. Also, to create a good dataset, the review included cross-sectional studies, case-control studies, and systematic reviews. Studies were excluded if they did not focus on healthcare professionals or dentists, did not consider the significance of nutrition and oral health as a primary factor, or were review articles without original data.
Flowchart and Study Selection Process
The review process involved a comprehensive evaluation of the methodological patterns of the selected studies to confirm their adherence to high scientific standards, thereby strengthening the reliability and validity of the results [28]. During screening, studies were excluded based on the following criteria: (1) irrelevant population (non-dental professionals or unrelated occupational groups); (2) intervention mismatch (absence of dietary, nutritional, or workplace-based components); (3) inadequate outcomes (lack of data on health resilience, well-being, performance, or nutritional behaviors); (4) study type (non-original research or unavailable full text); and (5) duplicate record [30].
The following flowchart illustrates the systematic process of identifying, screening, and selecting studies for inclusion in a review. It outlines each stage, from the initial identification of records from databases and registers to the final inclusion of eligible studies. Key steps include the removal of duplicates, screening for relevance, retrieval of full-text reports, and the assessment of eligibility based on predefined criteria. This flowchart provides a clear and transparent overview of the methodology, ensuring the reproducibility and reliability of the study selection process. In the final selection phase, 64 studies were excluded after a thorough review, resulting in 27 studies being included in the systematic review (Figure 1). This quantitative breakdown underlines the systematic approach taken in the selection process, ensuring the inclusion of high-quality and relevant evidence.
3. Results
The bar chart highlights the increasing number of publications over the years focusing on the dietary habits of healthcare workers (Figure 2). The steady rise in research reflects a growing recognition of the critical role diet plays in the overall and oral health and well-being of this population. Peaks in publication activity, such as in 2019, 2021, and 2024, align with global events like the COVID-19 pandemic, which likely amplified concerns about healthcare workers’ eating habits due to heightened stress, irregular schedules, and night shifts. The data reveals key issues such as the prevalence of unhealthy eating behaviors, including irregular meals and high sugar or fat consumption, and their impact on physical and mental health. This trend in publications highlights an urgent need to address dietary challenges among healthcare workers through targeted interventions, such as workplace nutrition programs and healthier food options, to promote better health outcomes and enhance their resilience in demanding work environments.
In Table 1, we present the analysis of the articles selected for our systematic review.
Type of Study and Study Design
The majority of studies included in this review are observational, with cross-sectional surveys being the most prevalent design. Cross-sectional approaches, as seen in studies by Ahmad et al. (2015), Waqas et al. (2015), Bouillon-Minois et al. (2022), and Tantimahanon et al. (2024), are commonly used to capture a snapshot of dietary habits, mental well-being, or the effects of work patterns (e.g., shift work) among healthcare professionals at a single point in time [8,25,43,44]. This design is efficient for identifying associations across large populations but does not establish causal relationships. Systematic reviews, such as those conducted by Tohary et al. (2022) and Souza et al. (2019), provide a broader synthesis of evidence regarding the links between diet, nutrition, and oral health or work conditions [14,37]. However, they depend on the quality and consistency of primary studies, which may introduce bias. In addition to these, some position papers and expert reports (e.g., Van Horn et al. (2019); Touger-Decker et al. (2019)) offer frameworks and recommendations for advancing nutrition education and interprofessional collaboration [39,40]. Though not empirical studies, these publications contribute valuable guidance for curriculum development and policy reform. Overall, the dominance of cross-sectional and observational designs across the reviewed articles reports on a strong descriptive focus in this research field, providing important insight into current practices and gaps, while highlighting the need for more longitudinal and intervention-based studies to better inform evidence-based strategies.
Population and Sample Size
The studies included in this review examined a diverse range of healthcare professionals across various countries and settings, including doctors, nurses, dentists, dietitians, and allied health workers. This diversity provides insight into how professional roles, work environments, and cultural contexts influence dietary habits, physical activity, mental health, and occupational stress. To be more specific, sample sizes varied considerably across studies. Larger studies, such as Waqas et al. (2015) (1,190 participants), Mota et al. (2021) (710 healthcare workers), and Tantimahanon et al. (2024) (842 dental professionals), offered stronger findings and increased generalizability [8,35,44]. In contrast, smaller studies like Hobby et al. (2024) (22 participants) and Bouillon-Minois et al. (2022) (184 emergency healthcare workers) had limited statistical power and generalizability [19,25]. Also, many studies reported gender imbalances. For example, Mota et al. (2021) noted that 80.8% of participants were female, a common trend in healthcare workforce studies. Such imbalances may affect interpretations of gender-related health behaviors [35]. Further, sampling methods also varied, with many studies relying on convenience sampling and self-reported data, which introduce potential selection and response biases [7,34,35]. More structured sampling approaches were used in studies like Tantimahanon et al. (2024) (multi-center survey) and Crespo-Escobar et al. (2024) (diverse participant pool), improving representativeness [8,15]. In addition, cultural and regional differences further affect generalizability across studies. For example, findings from studies conducted in Asia, Europe, and North America reflect varying healthcare systems and dietary practices [7,14,25,39]. In summary, while the reviewed studies encompass a broad range of healthcare populations and settings, the variability in sample sizes, gender distribution, and sampling methods must be considered when interpreting the results and their applicability to different contexts.
Data Collection Methods
The studies in this review employed a variety of data collection methods, primarily determined by study design and population characteristics. Most cross-sectional and observational studies relied on self-administered surveys or questionnaires to gather data on dietary habits, physical activity, mental well-being, and occupational stressors [7,12,14,35]. These instruments were often distributed electronically (e.g., via online platforms) or through healthcare institutions, allowing efficient access to large, geographically dispersed populations of healthcare workers.
The primary strength of survey-based data collection is its cost-effectiveness and ability to capture a broad range of behaviors and self-reported outcomes. However, these methods also carry limitations, notably recall bias, social desirability bias, and limited accuracy in reporting dietary or activity patterns [15,19,35]. Variability in question wording and participant interpretation can further impact data reliability [43,44]. Further, qualitative approaches, including interviews and focus groups, were used in studies like Hobby et al. (2024), which explored healthcare professionals’ perceptions of how personal diet influences nutrition care provision [19]. These methods provide rich, detailed insights into attitudes and behaviors but are limited by small sample sizes and potential researcher bias during data collection and interpretation. A smaller number of studies used direct observational methods. For example, Bouillon-Minois et al. (2022) employed a prospective observational design to record the actual food and water intake of healthcare workers during shift work [14]. This method offers more objective data on behaviors, reducing reliance on self-report, but can still be influenced by observer effects (e.g., Hawthorne effect). Finally, systematic reviews and secondary data analyses integrated findings from multiple primary studies to provide broader evidence on diet, nutrition, and oral health [13,14]. While such methods enhance statistical power and contribute to evidence synthesis, they are constrained by the quality and heterogeneity of the included studies [15]. In conclusion, while most studies in this review relied on surveys for feasibility and reach, the use of diverse data collection methods, both quantitative and qualitative, provided complementary insights into healthcare professionals’ health behaviors and outcomes.
Statistical Methodology, Analyses, and Recommendations
The studies reviewed employed a range of statistical methods suited to their observational and cross-sectional designs. Descriptive statistics, means, standard deviations, and percentages, were commonly used to summarize demographic characteristics and self-reported behaviors [14,35,43]. These provided a general overview of dietary habits, physical activity, and mental well-being among healthcare professionals but do not permit causal inferences [15,16]. Also, inferential statistics were used in many studies to explore relationships between variables. Chi-square tests and t-tests were commonly employed to assess associations between categorical variables or to compare outcomes across groups [14,44]. Regression analyses (both univariate and multivariate) were frequently used to control for potential confounders and to identify predictors of behaviors such as dietary patterns and burnout [7,19]. For example, Tantimahanon et al. (2024) used correlation analyses to demonstrate significant relationships between nutrition knowledge and healthier eating behaviors [8]. However, the predominance of cross-sectional designs limits the ability to establish causality or temporal relationships between variables. Many studies, including those by Mota et al. (2021), Gilbert et al. (2023), and Souza et al. (2019), emphasized the need for longitudinal research to better understand how dietary behaviors and health outcomes evolve [7,35,37]. Also, sample size limitations were noted in several studies, which may have reduced statistical power and the ability to detect smaller effects [14,44]. Additionally, the widespread reliance on self-reported data introduced potential biases such as recall error and social desirability [19,35].
To address these limitations, several authors recommend the use of objective measures (e.g., biomarkers, direct observation) to supplement self-reports [7], as well as the inclusion of more diverse and representative populations [15,44]. Furthermore, Bouillon-Minois et al. (2022) stress the importance of designing targeted interventions that consider the specific constraints of healthcare settings, such as shift work, time pressures, and access to healthy food options [14]. Conclusively, while the statistical methods employed were appropriate for descriptive and associative purposes, there remains a clear need for stronger longitudinal and intervention-based studies to advance this field.
Limitations Reported
The studies included in this review, while informative, share several common limitations related to their predominantly observational and cross-sectional designs. A major concern across many studies is the reliance on self-reported data, which can introduce both recall bias and social desirability bias potentially leading to underreporting of negative behaviors and overreporting of positive ones [7,34,35]. Several studies also noted issues related to non-random sampling. For example, Ahmad et al. (2015) and Mota et al. (2021) used convenience sampling, which limits the generalizability of findings beyond the study population [35,43]. Furthermore, many studies lacked formal power calculations or stratified sampling, reducing the ability to detect smaller effects or accurately representing broader healthcare professional populations [14,44]. Another key limitation is the inability to infer causality, as cross-sectional designs only capture data at a single point in time [14,35]. This restricts conclusions about the directionality of associations between variables such as dietary behaviors and mental well-being. In summary, while the reviewed studies contribute valuable insights into the health behaviors of healthcare professionals, their findings must be interpreted in light of methodological constraints, particularly the challenges associated with self-reported data, sampling biases, and limitations in causal inference.
Comparative and Cross-Cultural Analysis
A cross-cultural comparison of healthcare professionals’ health behaviors reveals both shared challenges and regional differences shaped by cultural and socioeconomic contexts. Across all regions, work-related stress, long hours, and irregular shifts negatively affect dietary habits, physical activity, and mental well-being [7,44]. Studies from Western countries such as the US and UK emphasize barriers like long working hours, limited access to healthy food, and workplace stress, which contribute to poor dietary choices and mental health outcomes [7,42]. In contrast, research from Pakistan and Saudi Arabia highlights the influence of socioeconomic factors, traditional dietary practices, and limited preventive health infrastructure, with healthcare professionals reporting poorer diet quality and greater mental health challenges [38,44]. Further, in Brazil and Thailand, the COVID-19 pandemic significantly impacted healthcare workers’ behaviors, leading to increased stress, higher intake of carbohydrates and alcohol, and changes in physical activity as coping mechanisms [8,35]. To add more, a key distinction between higher-income and lower-income countries is in the availability of structured workplace wellness programs. In high-income settings, there is greater emphasis on preventive health promotion, though barriers such as stress and time constraints remain [42]. In lower-income countries, limited healthcare resources often result in greater focus on treatment rather than prevention [38,44]. In sum, while healthcare professionals worldwide face similar occupational stressors affecting health behaviors, cultural norms, economic resources, and healthcare infrastructure shape both the risks and opportunities for intervention. These findings underline the importance of locally tailored strategies that consider regional contexts to promote sustainable health improvements among healthcare workers [7,35].
Overall Implications
The findings from this review highlight significant challenges in maintaining healthy lifestyles among healthcare professionals across diverse settings. Long working hours, high job stress, irregular shifts, and emotional exhaustion contribute to poor dietary habits, insufficient physical activity, and increased mental health risks, ultimately affecting both healthcare workers’ well-being and the quality of patient care [7,38,44]. There is a clear need for structured, workplace-based interventions that address both physical and mental health. Creating supportive environments, through access to healthy food, opportunities for physical activity, and comprehensive mental health resources, is essential for reducing burnout and promoting healthier behaviors [8,15]. Effective programs should integrate exercise facilities, nutritious cafeteria options, and accessible psychological support services [19,42]. Further, wellness initiatives such as mindfulness programs, flexible work schedules, and stigma-free mental health resources can enhance occupational health outcomes [23]. At the policy level, institutional and governmental reforms are needed to prioritize preventive health strategies, shifting from reactive care to a proactive approach [8]. This includes establishing national guidelines for workplace wellness and incentivizing healthy behaviors [14]. To add more on this, tailored, culturally sensitive interventions are also necessary. In low- and middle-income countries, barriers such as limited resources and socioeconomic constraints require targeted solutions, such as subsidized healthy foods, community-based education, and mHealth (mobile health) tools to extend reach and impact [13,35,43]. Additionally, gender roles, religious practices, and community norms must be considered when designing interventions [12,38]. We should finally mention that the COVID-19 pandemic has exaggerated these challenges, with healthcare workers reporting worsened dietary habits, reduced physical activity, and heightened stress during this period [35]. This underlines the urgent need for long-term policies that enhance the healthcare workforce resilience and safeguard their health. Conclusively, protecting the well-being of healthcare professionals is vital to maintaining an effective healthcare system. Sustainable, multi-level interventions addressing both short- and long-term needs, are essential to promote the health, performance, and resilience of this critical workforce [7,8].
4. Discussion
Healthcare professionals, particularly dentists, occupy a unique position in promoting both general and oral health through clinical practice and patient education [46]. However, their own dietary habits and lifestyle behaviors are often influenced by occupational stressors, irregular work schedules, and high demands, which may undermine their ability to serve as effective role models and contribute to suboptimal personal health outcomes [47]. Given the growing body of evidence linking diet, nutrition, and lifestyle factors to both systemic and oral diseases, including chronic conditions and dental pathologies, addressing these gaps within dental education and practice is increasingly vital. This review seeks to integrate insights from the current literature and international guidelines to propose actionable pathways for improving nutrition-related knowledge, daily practices, competencies, and interprofessional collaboration within the dental field.
Current Gaps in Nutrition Education Among Clinicians
A consistent finding across the reviewed literature is the significant gap in nutrition and oral health education for dental professionals. Despite international guidance from WHO and FAO on the role of reduced free sugar intake and healthy diets in preventing oral diseases [48,49], and recommendations in UK policy documents promoting dietary counseling in dental care [50], most undergraduate and postgraduate dental curricula still provide limited nutrition education and lack structured competencies to support effective nutrition counseling [39,40]. Surveys reveal that many dentists lack both confidence and adequate preparation to deliver dietary advice, often influenced by personal dietary behaviors and workplace stressors that reduce their readiness to engage in nutrition promotion [8,19,38,43]. Poor dietary habits are frequently reported among dental professionals themselves, shaped by long shifts, irregular schedules, and limited healthy food options at work [8,35].
In addition to gaps in education, interprofessional collaboration between dentists and nutrition professionals remains limited. Despite evidence that such collaboration improves patient outcomes, referrals to dietitians are rare, and few dental practitioners routinely engage in coordinated care [15,16]. Reviews confirm that many dentists do not systematically address dietary factors in patient care, even though diet is a key contributor to caries and periodontal disease progression [13,14]. It is also highlighted that despite well-established links between nutrition and oral diseases, dietary counseling is not a routine component of dental care [45,51,52]. Furthermore, variable levels of nutrition-related knowledge are evident across healthcare workers, with dentists not always demonstrating superior competencies compared to peers in other professions [34,38,53].
The lack of clear national or institutional mandates further emphasizes this educational gap. While frameworks for competency-based nutrition education have been proposed, implementation across dental programs remains inconsistent [39,40]. Without systematic educational reform and policy-driven integration of nutrition competencies, dentists will remain underprepared to deliver effective nutrition guidance as part of oral healthcare delivery [52,54].
Proposed Competency-Based Curriculum
Calls for reforming dental education to include structured, competency-based nutrition training are widespread in the literature. Although diet is recognized as a key factor in both preventing and managing oral diseases, many dental programs around the world still offer only limited and inconsistent coverage of nutrition-related content [52,54]. To address this gap, there is growing support for competency-based approaches that ensure graduates are prepared to assess dietary behaviors, provide effective counseling, and collaborate with nutrition professionals in clinical care [55]. A key step forward is to establish formal nutrition competencies for dental graduates, ensuring they can confidently assess dietary behaviors, provide individualized counseling, and collaborate effectively with dietitians and other healthcare professionals [55]. Current curricula often provide fragmented or outdated nutrition content, without experiential learning that grows real-world clinical skills [52,54]. To address this problem, curricula should be restructured to include practical training in nutrition screening and dietary assessment tools; case-based learning focused on nutrition-related oral health conditions (such as caries, periodontitis, and erosion); and role-play or simulated patient encounters that develop students’ communication and counseling skills [45,54].
Moreover, integrating interprofessional education is crucial. Evidence indicates that closer collaboration between dental professionals and dietitians results in improved patient outcomes [16,51]. Dental education programs should actively promote interprofessional learning opportunities, such as joint modules with nutrition and dietetics students, interdisciplinary clinical rotations, and shared workshops on patient-centered care [51,54,56]. Without such collaboration, dental graduates risk entering practice without the skills or networks needed to support comprehensive nutrition-related care [16]. In addition to technical competencies, curricula should also address the psychosocial and behavioral aspects of dietary counseling. As studies show, many healthcare professionals’ personal dietary habits influence their confidence and motivation to provide nutrition advice [1,19,57]. Education should therefore aim to enhance dental students’ personal awareness and self-efficacy regarding healthy eating, as this will strengthen their role-modeling capacity and professional identity [58].
Finally, national and international coordination is needed to drive consistency across programs. Recent expert consensus statements recommend establishing national nutrition competency frameworks and accreditation standards to ensure that nutrition education is no longer optional or variable but becomes an essential element of dental training [39,55]. Without such policy alignment, progress will remain fragmented and uneven across institutions [40,54]. As we can conclude, competency-based reforms should include: 1) clearly defined nutrition learning outcomes; 2) practical and experiential learning activities; 3) interprofessional education; 4) strategies to enhance personal and professional self-efficacy; and 5) national coordination of curriculum standards. Implementing these changes will enable dentists to play a more effective role in promoting nutrition for oral and systemic health, both within clinical practice and as public health advocates [39,51,52,53,54,55].
Interprofessional Coordination and Collaboration
A recurring recommendation across the reviewed literature is the need to strengthen interprofessional coordination and collaboration between dentists, dietitians, physicians, and other healthcare professionals. Such collaboration is essential for delivering patient-centered care that integrates nutrition and oral health promotion [39,40,51]. In this sense, multiple studies emphasize that isolated efforts by individual practitioners are insufficient to address the complex nutritional needs of patients [39]. There is a growing consensus that interprofessional education (IPE) frameworks are required, bringing together students and clinicians from dental, medical, and nutrition disciplines to build shared competencies and a common language for collaborative care [39,59]. Institutional reforms, including the development of national coordination centers, are also recommended to support joint curricula, interprofessional clinical experiences, and continuing education [39,55].
Evidence shows that bridging traditional silos between dietetics and dentistry demands deliberate action [60]. Collaborative care models should position dental professionals to work closely with dietitians, providing nutrition screening, counseling, and appropriate referrals tailored to patients’ oral and systemic health needs [40,51]. However, current practice is hampered by fragmented care systems. Reviews show that systematic referral pathways between dentists and dietitians are lacking, and few dental settings offer integrated nutrition services [19,51]. To address this, healthcare systems must establish clear protocols for interdisciplinary referrals and team-based care [61].
But in addition to curricular reform, enhancing effective collaboration requires a shift in clinical culture and institutional priorities [45,62]. Embedding nutrition into standard dental care workflows, providing regular cross-disciplinary professional development, and encouraging shared case management will enhance both clinician confidence and competence in collaborative care [19,51]. Further, practical models of IPE have demonstrated success. For example, Noorullah et al. (2025) describe an innovative IPE experience where dental, dietetic, and medical students participate in joint clinical sessions and interprofessional seminars. This approach improved students’ understanding of each other’s roles, enhanced communication skills, and cultivated a collaborative mindset, with positive impacts on patient care [59]. Expanding such IPE models into mainstream dental education is supposed to be a critical next step [54,59]. This requires coordinated action by educational institutions, healthcare organizations, and professional bodies to: embed interprofessional learning in all levels of education; establish clear referral pathways and collaborative care protocols; and design clinical environments that value and reward team-based approaches to nutrition and oral health promotion [19,39,40,59].
Institutional and Policy Recommendations
To embed nutrition fully into dental education and clinical care, changes at both institutional and policy levels are essential. Current gaps in training and practice will not close without deliberate action from accrediting bodies, licensing authorities, professional organizations, and healthcare institutions [39,40,63]. One key priority is the formal inclusion of nutrition competencies in accreditation and licensure standards. Without such requirements, nutrition education risks remaining optional or inconsistent across dental schools [39,64]. National accreditation bodies and dental licensing organizations should mandate that dental graduates demonstrate competence in nutrition care, covering dietary assessment, patient counseling, interprofessional collaboration, and referral practices [40]. These competencies should also be built into requirements for ongoing professional certification and continuing education [39]. Continuing education itself plays a critical role in keeping practicing clinicians up to date. The expansion of interdisciplinary CPD programs, bringing together dietitians, dentists, and other healthcare providers, can improve knowledge, enhance collaboration, and support a more integrated approach to patient care [19,65]. Professional bodies should promote such interdisciplinary learning as a standard component of dental continuing education [66].
Institutional support for nutrition care must also move beyond education alone. Dental schools and clinical settings should incorporate nutrition into routine workflows, for example, through screening protocols, referral pathways to dietitians, and standard patient education tools [45,46,67]. Without this practical integration, theoretical knowledge may fail to translate into clinical action[67,68].
Another dimension often overlooked is the personal health and well-being of dental professionals themselves. Studies show that poor workplace environments, including lack of access to nutritious food, insufficient meal breaks, and high stress, can undermine clinicians’ ability to serve as effective role models for their patients [19,69]. Institutions should therefore implement policies to improve workplace nutrition environments, such as providing healthy food options, ensuring protected time for meals, and promoting wellness initiatives that support healthcare providers’ own dietary and lifestyle behaviors [39,40,70].
Ultimately, driving sustainable change will require alignment across education, regulation, and institutional culture [71]. This includes embedding nutrition competencies into accreditation and licensure; expanding interdisciplinary continuing education; ensuring practical integration into clinical care pathways; and promoting institutional environments that support healthy behaviors among both patients and providers [19,39,40,70]. Coordinated policy reforms at these levels will be crucial to achieving long-term improvements in nutrition-informed dental care [72].
Role of National Coordination Centers
Achieving consistent and sustainable integration of nutrition education across healthcare professions, including dentistry, requires leadership at the national level. Several authors emphasize that fragmented institutional efforts are insufficient to drive the systemic change needed [19,73]. The creation of national coordination centers is proposed as a mechanism to align curriculum standards, develop shared competencies, and promote interprofessional collaboration [39]. Such centers would act as central hubs, bringing together academic institutions, accrediting bodies, and professional organizations to ensure that nutrition competencies are embedded in education, licensure, and clinical practice across healthcare disciplines [40]. They would also help address current disparities between programs and regions, supporting faculty development, resource sharing, and best-practice dissemination [19]. Without national or regional leadership, variations in educational quality and practice standards will persist, undermining efforts to make nutrition counseling a routine part of dental care [51,52]. Coordinated action is needed to ensure that nutrition becomes an integral and standardized component of healthcare training at all levels [19,39,40,74].
Enhancing Dentists’ Own Oral Health Through Integrated Nutrition Education and Practice
Implementing the proposed reforms, competency-based curricula, interprofessional collaboration, institutional policy changes, and national coordination, will not only improve patient care but can also produce significant benefits for the oral health and overall well-being of dentists themselves [75]. Many studies show that dental professionals frequently experience work-related stress, irregular schedules, poor dietary habits, and limited access to nutritious food at work [8,19,39,40,74,75,76]. These factors contribute to increased risks of dental caries, periodontal disease, and other oral health issues among dentists [77]. So, incorporating nutrition education throughout dental training can help future dentists better understand the impact of their own dietary choices on both oral and overall health [8,51]. Practical learning experiences, reflective practice, and wellness-centered curricula can further encourage dentists to develop healthier personal habits and sustain motivation for self-care [39,58,78].
Institutional policies that support healthy workplace environments, including access to nutritious meals and protected meal breaks, will further enable dental professionals to maintain good oral hygiene and balanced diets during demanding work schedules [39,45,79]. In turn, improved nutrition can help reduce inflammation, strengthen the oral microbiome, and support immune function, all of which contribute to lower risk of periodontal disease and other oral conditions for dentists too [80]. Moreover, cultivating a professional culture that promotes self-care and values nutrition as a component of clinical excellence will empower dentists to serve as authentic role models for patients and colleagues [78,81]. As personal oral health improves, so too will professional identity, job satisfaction, and long-term career sustainability [53,82]. Conclusively, the collective implementation of these recommendations offers a valuable opportunity to enhance dentists’ oral health, strengthen their resilience to occupational stress, and reinforce their role as trusted advocates for preventive oral healthcare [83].
Strengths and Limitations of the Study
This review addresses an often overlooked aspect of healthcare: the connection between nutrition and the oral health of healthcare professionals [19]. Drawing on data from diverse regions and professional groups, the findings provide valuable insights into how personal dietary behaviors affect both practitioner well-being and clinical practice [7,8]. However, several limitations must be acknowledged. Many included studies relied on self-reported dietary data, which is susceptible to recall and reporting bias [44]. The cross-sectional design of most studies also limits the ability to infer causality between diet and oral health outcomes [21]. Additionally, smaller sample sizes in some studies may reduce the generalizability of findings across all healthcare settings [84]. Finally, the influence of socioeconomic factors, workplace environments, and institutional policies was not consistently controlled across studies, which may have affected results [85]. Future research should prioritize longitudinal designs and intervention studies to evaluate how systemic workplace strategies can improve healthcare professionals’ dietary behaviors and oral health over time [86,87]. Such efforts are key to supporting healthier habits, reducing oral disease risk, and enhancing both personal well-being and professional performance in the healthcare workforce [88].
Future Research Directions
Future research should prioritize longitudinal studies to clarify the causal links between nutrition, mental well-being, oral health, and job performance among healthcare professionals [7,87]. Randomized controlled trials are needed to evaluate the effectiveness of targeted dietary interventions, such as increasing intake of omega-3 fatty acids, fruits, and vegetables, on reducing stress, improving physical health, and managing common conditions like obesity and hypertension [87,89]. Given the well-established impact of shift work on diet quality, research should also examine workplace strategies such as healthier food options during night shifts and tailored counseling for reducing these effects [25,84]. Additionally, studies should explore how organizational culture and policies influence dietary behaviors, particularly through access to healthy meals, nutrition counseling, and support for physical activity [7]. Understanding the role of socioeconomic and cultural factors is equally important for designing interventions that reflect the diverse realities of healthcare settings across regions [22,44]. Finally, further investigation is needed into how integrating nutrition education into dental and medical curricula can enhance both personal and patient care outcomes, helping to close current gaps in the complex relationship between diet, mental health, and oral health in healthcare professionals [90,91,92].
5. Conclusions
Integrating nutrition into dental education and practice is essential for improving both the oral and overall health of dental professionals. Poor dietary habits, shaped by demanding work conditions, contribute to stress, burnout, and oral disease risk. Systemic changes in education, institutional policies, and workplace environments are needed to support healthier behaviors. Future research should focus on long-term interventions and address cultural, organizational, and professional factors to promote sustainable improvements in dentists’ well-being, oral health and clinical practice.
Author Contributions
Conceptualization, M.A.; methodology, M.A.; software, M.A.; validation, T.K. and M.A.; formal analysis, T.K. and M.A.; investigation, T.K. and M.A.; resources, M.A.; data curation, T.K. and M.A.; writing—original draft preparation, T.K. and M.A.; writing—review and editing, T.K. and M.A.; visualization, M.A.; supervision, M.A.; project administration, M.A.; funding acquisition, T.K. and M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Yaman, G. B., & Hocaoğlu, Ç. (2022). Examination of eating and nutritional habits in health care workers during the COVID-19 pandemic. Nutrition, 105, 111839. [CrossRef]
- Slavkin HC, Dubois PA, Kleinman DV, Fuccillo R. Science-Informed Health Policies for Oral and Systemic Health. J Healthc Leadersh. 2023 Mar 16;15:43-57. [CrossRef]
- Schneider, A., Bak, M., Mahoney, C., Hoyle, L., Kelly, M., Atherton, I. M., & Kyle, R. G. (2019). Health-related behaviours of nurses and other healthcare professionals: A cross-sectional study using the Scottish Health Survey. Journal of Advanced Nursing, 75(6), 1239–1251. [CrossRef]
- Antoniadou, M.; Varzakas, T. Diet and Oral Health Coaching Methods and Models for the Independent Elderly. Appl. Sci. 2020, 10, 4021. [Google Scholar] [CrossRef]
- Mills A, Berlin-Broner Y, Levin L. Improving Patient Well-Being as a Broader Perspective in Dentistry. Int Dent J. 2023 Dec;73(6):785-792. [CrossRef] [PubMed] [PubMed Central]
- Gaffar, B., Farooqi, F. A., Nazir, M. A., Bakhurji, E., Al-Khalifa, K. S., Alhareky, M., & Virtanen, J. I. (2022). Oral health-related interdisciplinary practices among healthcare professionals in Saudi Arabia: Does integrated care exist? BMC Oral Health, 22(1), 75. [CrossRef]
- Gilbert, A., Eyler, A., Cesarone, G., Harris, J., Hayibor, L., & Evanoff, B. (2023). Exploring university and healthcare workers’ physical activity, diet, and well-being during the COVID-19 pandemic. SAGE Open Medicine, 11, 21650799221147814. [CrossRef]
- Tantimahanon, A., Sipiyaruk, K., & Tantipoj, C. (2024). Determinants of dietary behaviors among dental professionals: Insights across educational levels. BMC Oral Health, 24, Article 724. [CrossRef]
- Canuto, R., Garcez, A., Spritzer, P. M., & Olinto, M. T. A. (2021). Associations of perceived stress and salivary cortisol with the snack and fast-food dietary pattern in women shift workers. Stress, 24(6), 763–771. [CrossRef]
- Abouelezz, N. F., Ahmed, W. S. E., Elhussieny, D. M., Ahmed, G. S., & Zaky, M. S. M. E. (2024). Dietary habits and perceived barriers of healthy eating among healthcare workers in a tertiary hospital in Egypt: A cross-sectional study. QJM: An International Journal of Medicine, 117(Supplement_2), hcae175.884. [CrossRef]
- El-Sharkawy, A. M., Bragg, D., Watson, P., Neal, K., Sahota, O., Maughan, R. J., & Lobo, D. N. (2016). Hydration amongst nurses and doctors on-call (the HANDS on prospective cohort study). Clinical Nutrition, 35(4), 935–942. [CrossRef]
- Utter J, McCray S, Denny S. Eating Behaviours Among Healthcare Workers and Their Relationships With Work-Related Burnout. American Journal of Lifestyle Medicine. 2023;0(0). [CrossRef]
- Dimopoulou, M., Antoniadou, M., Amargianitakis, M., Gortzi, O., Androutsos, O., & Varzakas, T. (2023). Nutritional factors associated with dental caries across the lifespan: A review. Applied Sciences, 13(24), 13254. [CrossRef]
- Tohary, I. A., Jan, A. S., Alotaibi, M. A., Alosaimi, T. B., Alotaibi, A. E. A., Alshayb, A. A., Sadig, J. A. A., Tumayhi, H. Y. A., Rubayyi, S. H., Amri, S. A., & Almutairi, H. T. (2022). The impact of diet and nutrition on oral health: A systematic review. Migration Letters, 19(S5), 338–346. https://www.migrationletters.com.
- Crespo-Escobar, P., Vázquez-Polo, M., van der Hofstadt, M., Nuñez, C., Montoro-Huguet, M. A., Churruca, I., & Simón, E. (2024). Knowledge gaps in gluten-free diet awareness among patients and healthcare professionals: A call for enhanced nutritional education. Nutrients, 16(15), 2512. [CrossRef]
- Lieffers, J. R., Vanzan, A. G. T., & de Mello, J. R. (2021). Nutrition care practices of dietitians and oral health professionals for oral health conditions: A scoping review. Nutrients, 13(10), 3588. [CrossRef]
- Thircuir, S., Chen, N. N., & Madsen, K. A. (2023). Addressing the gap of nutrition in medical education: Experiences and expectations of medical students and residents in France and the United States. Nutrients, 15(24), 5054. [CrossRef]
- Lahiouel, A., Kellett, J., Isbel, S., & D’Cunha, N. M. (2023). An exploratory study of nutrition knowledge and challenges faced by informal carers of community-dwelling people with dementia: Online survey and thematic analysis. Geriatrics (Basel), 8(4), 77. [CrossRef]
- Hobby, J., Parkinson, J., & Ball, L. (2024). Exploring health professionals’ perceptions of how their own diet influences their self-efficacy in providing nutrition care. Psychology & Health, 39(2), 252–267. [CrossRef]
- Torquati, L., Pavey, T., Kolbe-Alexander, T., & Leveritt, M. (2017). Promoting diet and physical activity in nurses. American Journal of Health Promotion, 31(1), 19–27. [CrossRef]
- Ahmad, W., Waqas, A., Saleem, H. A., & Naveed, S. (2017). Exploring diet, exercise, chronic illnesses, occupational stressors and mental well-being of healthcare professionals in Punjab, Pakistan. BMC Research Notes, 10(1), 745. [CrossRef]
- Chui, H., Bryant, E., Sarabia, C., Maskeen, S., & Stewart-Knox, B. (2019). Burnout, eating behaviour traits and dietary patterns. British Food Journal. [CrossRef]
- Sert, E., & Kendirkiran, G. (2024). Effects of emotional eating behaviour and burnout levels of nurses on job performance: A cross-sectional descriptive study. SAGE Open Nursing. Advance online publication. [CrossRef]
- Hulsegge, G., Boer, J. M., van der Beek, A. J., Verschuren, W. M., Sluijs, I., Vermeulen, R., & Proper, K. I. (2016). Shift workers have a similar diet quality but higher energy intake than day workers. Scandinavian Journal of Work, Environment & Health, 42(6), 459–468. [CrossRef]
- Bouillon-Minois, J.-B., Thivel, D., Croizier, C., Ajebo, É., Cambier, S., Boudet, G., Adeyemi, O. J., Ugbolue, U. C., Bagheri, R., Vallet, G. T., Schmidt, J., Trousselard, M., & Dutheil, F. (2022). The negative impact of night shifts on diet in emergency healthcare workers. Nutrients, 14(4), 829. [CrossRef]
- Tejoyuwono, A. (2020). Health lecturers and students’ views about healthcare workers as healthy lifestyle role models: A qualitative study. Indonesian Journal of Nursing Practices, 4, Article 1105. [CrossRef]
- Torquati, L., Pavey, T., & Leveritt, M. (2017). Promoting diet and physical activity in nurses: A systematic review. American Journal of Health Promotion, 31(1), 19–27. [CrossRef]
- Schiavo, J. H. (2019). PROSPERO: An international register of systematic review protocols. Medical Reference Services Quarterly, 38(2), 171-180. [CrossRef]
- IBM Corp. (2022). IBM SPSS Statistics for Windows, Version 28.0. IBM Corp.
- Mamun, A.A.; Mahmudiono, T.; Yudhastuti, R.; Triatmaja, N.T.; Chen, H.-L. Effectiveness of Food-Based Intervention to Improve the Linear Growth of Children under Five: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2430. [Google Scholar] [CrossRef] [PubMed]
- Znyk, M., & Kaleta, D. (2024). Unhealthy eating habits and determinants of diet quality in primary healthcare professionals in Poland: A cross-sectional study. Nutrients, 16(19), Article 3367. [CrossRef]
- Chen, M., Xu, X., Liu, Y., Yao, Y., Zhang, P., Liu, J., Zhang, Q., Li, R., Li, H., Liu, Y., & Chen, W. (2023). Association of eating habits with health perception and diseases among Chinese physicians: A cross-sectional study. Frontiers in Nutrition, 10. [CrossRef]
- Wolska, A., Stasiewicz, B., Kaźmierczak-Siedlecka, K., Ziętek, M., Solek-Pastuszka, J., Drozd, A., Palma, J., & Stachowska, E. (2022). Unhealthy food choices among healthcare shift workers: A cross-sectional study. Nutrients, 14(20), Article 4327. [CrossRef]
- Mehrotra, A., Mehrotra, A., Babu, A. K., Ji, P., Mapare, S. A., & Pawar, R. O. (2021). Oral health knowledge, attitude, and practices among healthcare professionals: A questionnaire-based survey. Journal of Pharmacy & BioAllied Sciences, 13(Suppl 2), S1452–S1457. [CrossRef]
- Mota, I. A., de Oliveira Sobrinho, G. D., Morais, I. P. S., & Dantas, T. F. (2021). Impact of COVID-19 on eating habits, physical activity, and sleep in Brazilian healthcare professionals. Arquivos de Neuro-Psiquiatria, 79(5), [page numbers if available]. [CrossRef]
- Portero de la Cruz, S., Cebrino, J., Herruzo, J., & Vaquero-Abellán, M. (2020). A multicenter study into burnout, perceived stress, job satisfaction, coping strategies, and general health among emergency department nursing staff. Journal of Clinical Medicine, 9(4), 1007. [CrossRef]
- Souza, R. V., Sarmento, R. A., de Almeida, J. C., & Canuto, R. (2018). The effect of shift work on eating habits: A systematic review. Scandinavian Journal of Work, Environment & Health, 45(1). [CrossRef]
- Almoteb, M. M., Alalyani, S. S., Gowdar, I. M., Penumatsa, N. V., Siddiqui, M. A. M., & Sharanesha, R. B. (2019). Oral hygiene status and practices among healthcare workers: A cross-sectional study. Journal of International Oral Health, 11(5), 268–273. [CrossRef]
- Van Horn L, Lenders CM, Pratt CA, Beech B, Carney PA, Dietz W, DiMaria-Ghalili R, Harlan T, Hash R, Kohlmeier M, Kolasa K, Krebs NF, Kushner RF, Lieh-Lai M, Lindsley J, Meacham S, Nicastro H, Nowson C, Palmer C, Paniagua M, Philips E, Ray S, Rose S, Salive M, Schofield M, Thompson K, Trilk JL, Twillman G, White JD, Zappalà G, Vargas A, Lynch C. Advancing Nutrition Education, Training, and Research for Medical Students, Residents, Fellows, Attending Physicians, and Other Clinicians: Building Competencies and Interdisciplinary Coordination. Adv Nutr. 2019 Nov 1;10(6):1181-1200. [CrossRef]
- Touger-Decker, Riva et al.Position of the Academy of Nutrition and Dietetics: Oral Health and Nutrition. Journal of the Academy of Nutrition and Dietetics, Volume 113, Issue 5, 693 – 701.
- Ab-Murat, N., Mason, L., Abdul Kadir, R., & Yusoff, N. (2018). Self-perceived mental well-being amongst Malaysian dentists. Journal of Workplace Behavioral Health, 24(2), 233–239. [CrossRef]
- Orgel, R., & Cavender, M. A. (2018). Healthy living for healthcare workers: It is time to set an example. European Journal of Preventive Cardiology, 25(5), 485–487. [CrossRef]
- Ahmad, W., Taggart, F., Shafique, M. S., Muzafar, Y., Abidi, S., Ghani, N., Malik, Z., Zahid, T., Waqas, A., & Ghaffar, N. (2015). Diet, exercise and mental-wellbeing of healthcare professionals (doctors, dentists and nurses) in Pakistan. PeerJ, 3, e1250. [CrossRef]
- Waqas, A., Ahmad, W., Haddad, M., Taggart, F. M., Muhammad, Z., Bukhari, M. H., Sami, S. A., Batool, S. M., Najeeb, F., Hanif, A., Rizvi, Z. A., & Ejaz, S. (2015). Measuring the well-being of healthcare professionals in the Punjab: A psychometric evaluation of the Warwick-Edinburgh Mental Well-being Scale in a Pakistani population. PeerJ, 3, e1264. [CrossRef]
- Taylor M. Oral health and nutrition guidance for professionals June 2012. Accessed on 21 June from https://www.scottishdental.nhs.scot/wp-content/uploads/2014/10/OralHealthAndNutritionGuidance.pdf.
- Shmarina, E., Ericson, D., Götrick, B. et al. Dental professionals’ perception of their role in the practice of oral health promotion: a qualitative interview study. BMC Oral Health 23, 43 (2023). [CrossRef]
- Escoto KH, Laska MN, Larson N, Neumark-Sztainer D, Hannan PJ. Work hours and perceived time barriers to healthful eating among young adults. Am J Health Behav. 2012 Nov;36(6):786-96. [CrossRef]
- WHO Technical Report Series, 916. Diet, nutrition and the prevention of chronic diseases. Accessed on 21 june from https://iris.who.int/bitstream/handle/10665/42665/WHO_TRS_916.pdf.
- Wilson T, Temple NJ, Bray GA. Nutrition Guide for Physicians and Related Healthcare Professions. Nutrition and Health (NH) series. Springer nature link.2022.
- Public health England. Delivering better oral health: an evidence-based toolkit for prevention Third edition, 2017. Accessed on 21 june from https://www.bsperio.org.uk/assets/downloads/Delivering_better_oral_health.pdf.
- Kaye J, Lee S, Chinn CH. The need for effective interprofessional collaboration between nutrition and dentistry. Front Public Health. 2025 Feb 26;13:1534525. [CrossRef]
- Kataoka M, Adam LA, Ball LE, Crowley J, McLean RM. Nutrition Education and Practice in University Dental and Oral Health Programmes and Curricula: A Scoping Review. Eur J Dent Educ. 2025, 29(1), 64-83. [CrossRef]
- Antoniadou, M.; Mangoulia, P.; Myrianthefs, P. Quality of Life and Wellbeing Parameters of Academic Dental and Nursing Personnel vs. Quality of Services. Healthcare 2023, 11, 2792. [Google Scholar] [CrossRef]
- Fernández CE, Torre MJ, Vargas CJ, Aravena CA, Santander J, Marshall TA. Diet and Nutrition Integration in Dental Education: A Scoping Review. Eur J Dent Educ. 2025 Jun 5. [CrossRef]
- Eisenberg DM, Cole A, Maile EJ, et al. Proposed Nutrition Competencies for Medical Students and Physician Trainees: A Consensus Statement. JAMA Netw Open. 2024;7(9):e2435425. [CrossRef]
- 56. CareQuest Institute for Oral Health. Transforming Oral Health Care Through Interprofessional Education: Use Cases. Boston, MA: April 2025. accessed 21 june from https://www.carequest.org/system/files/CareQuest_Institute_IPE-UseCases_4.1.25_Final.pdf. [CrossRef]
- Antoniadou M, Varzakas T. Breaking the vicious circle of diet, malnutrition and oral health for the independent elderly. Crit Rev Food Sci Nutr. 2021, 61(19), 3233-3255. [CrossRef]
- Ehsan F, Iqbal S, Younis MA, Khalid M. An educational intervention to enhance self-care practices among 1st year dental students- a mixed method study design. BMC Med Educ. 2024, 14, 24(1):1304. [CrossRef]
- Noorullah K, Oshita SE, McNeil AT, Ijaz A, Iqbal L, Tomar SL, Smith PD, Bilal S. Bridging Nutrition and Dentistry: An Interprofessional Education (IPE) Experience Model. J Multidiscip Healthc. 2025 May 31;18:3039-3049. [CrossRef]
- Boak R, Palermo C, Beck EJ, Pelly F, Wall C, Gallegos D. Five Actions to Strengthen the Nutrition and Dietetics Profession Into the Future: Perspectives From Australia and New Zealand. J Hum Nutr Diet. 2025 Jun;38(3):e70064. [CrossRef]
- Bendowska A, Baum E. The Significance of Cooperation in Interdisciplinary Health Care Teams as Perceived by Polish Medical Students. Int J Environ Res Public Health. 2023, 5, 20(2):954. [CrossRef]
- Rosen MA, DiazGranados D, Dietz AS, Benishek LE, Thompson D, Pronovost PJ, Weaver SJ. Teamwork in healthcare: Key discoveries enabling safer, high-quality care. Am Psychol. 2018 May-Jun;73(4):433-450. [CrossRef]
- Blanchard, M. Closing the gap between medical knowledge and patient outcomes through new training infrastacture. Trans Am Clin Climatol Assoc. 2023, 133, 119–135. [Google Scholar] [PubMed]
- DiMaria-Ghalili RA, Mirtallo JM, Tobin BW, Hark L, Van Horn L, Palmer CA. Challenges and opportunities for nutrition education and training in the health care professions: intraprofessional and interprofessional call to action. Am J Clin Nutr. 2014, 99(5 Suppl):1184S-93S. [CrossRef]
- Forsetlund L, O’Brien MA, Forsén L, Reinar LM, Okwen MP, Horsley T, Rose CJ. Continuing education meetings and workshops: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2021, 15;9(9):CD003030. [CrossRef]
- Nasseripour, M.; Agouropoulos, A.; Van Harten, M.T.; Correia, M.; Sabri, N.; Rollman, A. Current State of Professionalism Curriculum in Oral Health Education. Eur J Dent Educ. 2025, 29(1), 92–103. [Google Scholar] [CrossRef] [PubMed]
- Eyemienbai, E.J.; Logue, D.; McMonagle, G.; Doherty, R.; Ryan, L.; Keaver, L. Enhancing Nutrition Care in Primary Healthcare: Exploring Practices, Barriers, and Multidisciplinary Solutions in Ireland. Int. J. Environ. Res. Public Health 2025, 22, 771. [Google Scholar] [CrossRef] [PubMed]
- Hashemiparast M, Negarandeh R, Theofanidis D. Exploring the barriers of utilizing theoretical knowledge in clinical settings: A qualitative study. Int J Nurs Sci. 2019, 12, 6(4):399-405. [CrossRef]
- Ejiohuo O, Onyeaka H, Unegbu KC, Chikezie OG, Odeyemi OA, Lawal A, Odeyemi OA. Nourishing the Mind: How Food Security Influences Mental Wellbeing. Nutrients. 2024 Feb 9;16(4):501. [CrossRef]
- Re B, Alessandro Zardini, Francesca Sanguineti, Pietro Previtali. Healthy eating initiatives in the workplace: a configurational approach. https://www.emerald.com/insight/0007-070X.htm Accessed on 21 june from https://www.emerald.com/insight/content/doi/10.1108/bfj-10-2024-1080/full/pdf.
- Abo-Khalil, AG. Integrating sustainability into higher education challenges and opportunities for universities worldwide. Heliyon 2024, 10, e29946. [Google Scholar] [CrossRef] [PubMed]
- Hollaar, V.R.Y.; Naumann, E.; Haverkort, E.B.; Jerković-Ćosić, K.; Kok, W.E.; de van der Schueren, M.A.E. Success factors and barriers in interprofessional collaboration between dental hygienists and dietitians in community-dwelling older people: Focus group interviews. international journal of dental hygiene. 2023, 22, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Antoniadou, M.; Antoniadis, R. A Systemic Model for Resilience and Time Management in Healthcare Academia: Application in a Dental University Setting. Appl. Sci. 2024, 14, 4918. [Google Scholar] [CrossRef]
- Kris-Etherton, P. M., Petersen, K. S., Hibbeln, J. R., Hurley, D., Kolick, V., Peoples, S., Rodriguez, N., & Woodward-Lopez, G. (2021). Nutrition and behavioral health disorders: Depression and anxiety. Nutrition Reviews, 79(3), 247–260. [CrossRef]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Committee on Implementing High-Quality Primary Care; Robinson SK, Meisnere M, Phillips RL Jr., et al., editors. Implementing High-Quality Primary Care: Rebuilding the Foundation of Health Care. Washington (DC): National Academies Press (US); 2021 May 4. 6, Designing Interprofessional Teams and Preparing the Future Primary Care Workforce. Available online: https://www.ncbi.nlm.nih.gov/books/NBK571818/.
- Μangoulia, P.; Kanellopoulou, A.; Manta, G.; Chrysochoou, G.; Dimitriou, E.; Kalogerakou, T.; Antoniadou, M. Exploring the Levels of Stress, Anxiety, Depression, Resilience, Hope, and Spiritual Well-Being Among Greek Dentistry and Nursing Students in Response to Academic Responsibilities Two Years After the COVID-19 Pandemic. Healthcare 2025, 13, 54. [Google Scholar] [CrossRef] [PubMed]
- Elsahoryi NA, Ghada A. Maghaireh, Fwziah Jammal Hammad. Understanding dental caries in adults: A cross-sectional examination of risk factors and dietary behaviors. Clinical Nutrition Open Science, 2024, 57, 163-176. [CrossRef]
- Antoniadou, M. Leadership and Managerial Skills in Dentistry: Characteristics and Challenges Based on a Preliminary Case Study. Dent. J. 2022, 10, 146. [Google Scholar] [CrossRef] [PubMed]
- Oral Health in America: Advances and Challenges [Internet]. Bethesda (MD): National Institute of Dental and Craniofacial Research(US); 2021 Dec. Section 4, Oral Health Workforce, Education, Practice and Integration. Available online: https://www.ncbi.nlm.nih.gov/books/NBK578298/.
- Varzakas, T.; Antoniadou, M. A Holistic Approach for Ethics and Sustainability in the Food Chain: The Gateway to Oral and Systemic Health. Foods 2024, 13, 1224. [Google Scholar] [CrossRef] [PubMed]
- Bornman, J.; Louw, B. Leadership Development Strategies in Interprofessional Healthcare Collaboration: A Rapid Review. J Healthc Leadersh. 2023, 23, 15:175–192. [Google Scholar] [CrossRef] [PubMed]
- Antoniadou, M. Quality of Life and Satisfaction from Career and Work–Life Integration of Greek Dentists before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 9865. [Google Scholar] [CrossRef] [PubMed]
- Glick, M., Urquhart, O., Bhosale, A.S. et al. A unified voice to drive global improvements in oral health. BMC Global Public Health 2023, 1, 19. [CrossRef]
- World Health Organization (WHO). Prevention and Treatment of Dental Caries with Mercury-Free Products and Minimal Intervention: WHO Oral Health Briefing Note Series; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Kalogerakou, T, Antoniadou, M. The role of dietary antioxidants, food supplements, and functional foods for energy enhancement in healthcare professionals. Antioxidants, 2024, 13(12), 1508. [CrossRef]
- World Health Organization (WHO). Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030; Regional summary of the African Region; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Sarris, J., Logan, A. C., Akbaraly, T. N., Amminger, G. P., Balanzá-Martínez, V., Freeman, M. P., Hibbeln, J., Matsuoka, Y., Mischoulon, D., Mizoue, T., Nanri, A., Nishi, D., Ramsey, D., Rucklidge, J. J., Sanchez-Villegas, A., Scholey, A., Su, K.-P., Jacka, F. N., & International Society for Nutritional Psychiatry Research. Nutritional medicine as mainstream in psychiatry. The Lancet Psychiatry, 2015, 2(3), 271–274. [CrossRef]
- Gondivkar, S. M., Gadbail, A. R., Gondivkar, R. S., Sarode, S. C., Sarode, G. S., Patil, S., Awan, K. H. Nutrition and oral health. Disease-a-Month, 2019, 65(6), 147–154. [CrossRef]
- Papadaki, A., Nolen-Doerr, E., Mantzoros, C. S. The effect of the Mediterranean diet on metabolic health: A systematic review and meta-analysis of controlled trials in adults. Nutrients, 2020, 12(11), 3342. [CrossRef]
- Antoniadou, M. Quality of Life and Satisfaction from Career and Work–Life Integration of Greek Dentists before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 9865. [Google Scholar] [CrossRef] [PubMed]
- Antoniadou, M. Estimation of Factors Affecting Burnout in Greek Dentists before and during the COVID-19 Pandemic. Dent. J. 2022, 10, 108. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, K. P., Ezerins, M. E., Rosen, C. C., Gabriel, A. S., Patel, C., Lim, G. J. H. Socioeconomic Status and Employee Well-Being: An Intersectional and Resource-Based View of Health Inequalities at Work. Journal of Management, 2025, 51(6), 2549-2588. [CrossRef]
Figure 1.
PRISMA Flowchart for the results of the search strategies.
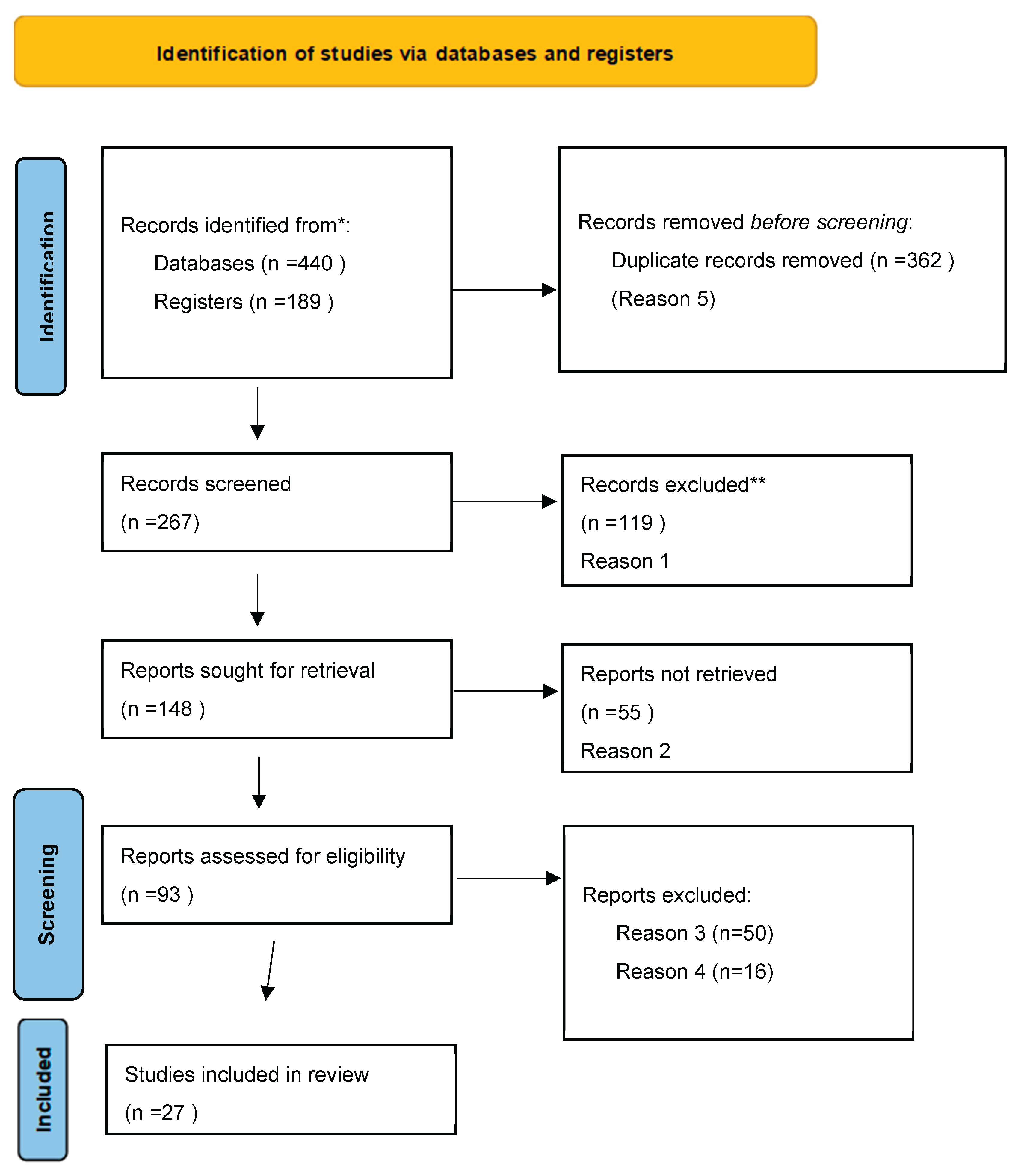
Figure 2.
Chart displaying the number of publications per year.
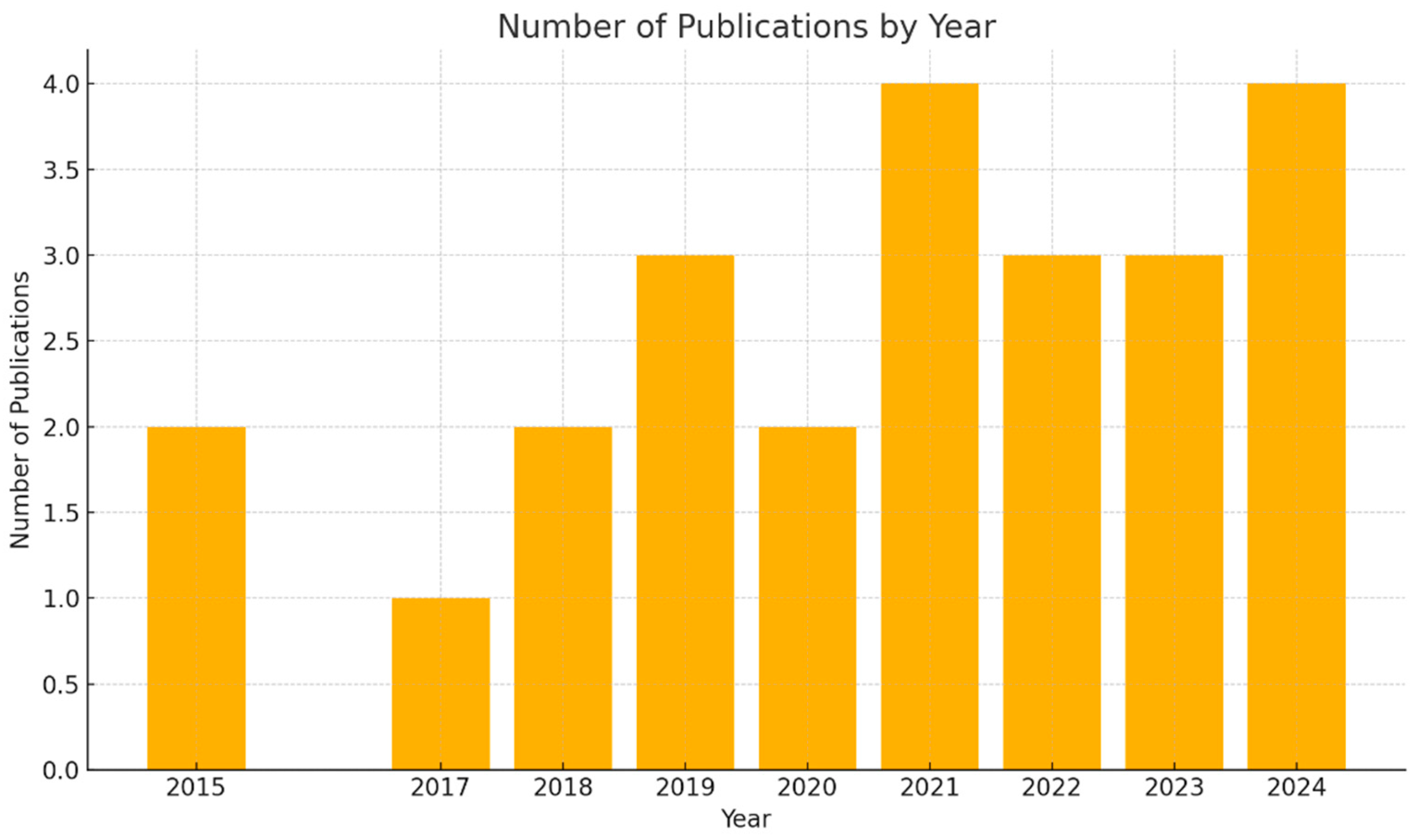

Table 1.
Studies included in this systematic review.
| Authors | Type of study- Single/multi center | Population | Exposure | Comparators | Funding and Confilct | statistical significance | Limitations | Ethics approval | Sample calulation | Confounders | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1.Tantimahanon et al., (2024), [8]. |
Cross-sectional (multi-center) | Dental professionals (UG, PG, DT; n=842) | Dietary behaviors | Knowledge, attitude, alcohol consumption | No conflicts mentioned; funded by Mahidol University | Significant correlation (P < 0.001 for all groups) | Self-reported survey may lead to response bias. Age range primarily under 30, limiting generalizability. | Approved by Mahidol University IRB (MU-DT/PY-IRB 2023/004.1701) | Calculated using formula for finite population (CI 95%, margin error 6%) | Stress, socioeconomic factors, living environment | Attitude was the strongest determinant. Alcohol consumption negatively associated with healthy behaviors. |
| 2. Crespo-Escobar et al. (2024)[15] | Cross-sectional, multi-center | CeD patients (n=2,437); HCPs (n=346); Relatives (n=1,294) | Knowledge and adherence to GFD | Knowledge gaps in GFD; adherence in CeD | Not disclosed | Significant differences in knowledge sources and quality of GFD information provision (p < 0.05) | Self-report bias; focus on Spain; overrepresentation of association members; limited dietitian availability in public healthcare; cultural specificity of findings. | Approved by the Ethics Committee of UPV/EHU | Sampling via snowball method, no formal sample calculation. | Sociodemographic data, professional role, patient association membership | Knowledge gaps in GFD adherence among CeD patients and HCPs; limited time in consultations; reliance on unreliable sources (e.g., Internet). |
| 3.Hobby et al. (2024)[19]. | Cross-sectional qualitative design | 22 health professionals (including dietitians) | Perceptions of how personal diet influences self-efficacy in providing nutrition care | Not applicable | Not reported | Not applicable | Small sample size; findings may not be generalizable due to recruitment through media channels; self-reported data may introduce bias | Approved | Not applicable | Social environment, personal experiences | Health professionals perceive personal dietary habits strongly influence their self-efficacy in providing nutrition care. Strategies supporting healthier diets may enhance care quality. |
| 4.Znyk & Kaleta (2024)[31]. | Cross-sectional study | 161 doctors and 331 nurses in Poland | Eating habits and diet quality during shifts | General population; different work conditions | Not reported | Univariate logistic regression showed significant determinants of diet (p < 0.05) | Self-reported data may introduce recall bias; cross-sectional design; no questions about income; small sample size; conducted during COVID-19 pandemic, potentially affecting habits. | Approved | Not applicable | Work experience, number of patients, BMI, smoking | Unhealthy eating habits affected 25.8% of healthcare workers, linked to smoking, work experience, and patient load. Nurses exhibited higher prevalence of unhealthy habits. |
| 5.Dimopoulou et al (2023)[13] | Narrative review (single centralized author group, not empirical; no study centers) | General human populations across lifespan (children to older adults), aggregated from various studies | Nutritional factors: dietary sugar, frequency of intake, macro/micronutrient patterns linked to dental caries | Varied across included studies (e.g., high vs. low sugar intake; frequent vs. infrequent snacking; nutrient-rich vs. nutrient-poor diets) | Not reported in article; no conflicts declared | Not applicable (review synthesis; no original hypothesis testing) | Heterogeneity of included studies (designs, populations, methods) - Potential publication bias - Narrative synthesis (no meta-analysis) - Quality and validity of primary studies vary |
Not applicable (literature review; no new human or animal research) | Not applicable | Confounders reported variably in included studies (e.g., socioeconomic status, oral hygiene, fluoride exposure), but no uniform adjustment in this review | Associations between nutrition-related variables (sugar intake, snacking frequency, nutrient deficiencies) and dental caries incidence across age groups |
| 6.Chen et al. (2023) [32] | Cross-sectional study | In-service physicians in mainland China | Eating habits (e.g., eating out, irregular meals, eating too fast) | Physicians with healthier eating habits | Not reported | Significant associations between unhealthy eating habits and suboptimal health/disease occurrence (p < 0.05) | Convenience sampling; self-reported data may introduce recall bias; cross-sectional design limits causal inference. | Approved | Not applicable | Sociodemographic characteristics, BMI classification | High prevalence of unhealthy eating habits linked to increased rates of suboptimal health, obesity, and metabolic diseases among physicians. Eating too fast and eating out were common. |
| 7.Utter et al. (2023)[12] | Cross-sectional study, single center (large healthcare organization in South-East Queensland, Australia) | 501 healthcare workers (varied roles) | Dietary behaviors (overall diet quality, fruit/vegetable intake, family shared meals) | Different levels of dietary indicators (e.g., high vs low diet quality) | Not specified | Significant inverse relationship: healthier diet associated with lower burnout (adjusted for covariates) | Cross-sectional design (no causality); self-reported data; single site; no sample size calculation reported | Not explicitly stated (likely approved by institutional ethics board) | Not reported | Age, gender, role, employment level | Burnout levels; dietary behavior indicators |
| 8.Sert & Kendirkiran (2023) [23] | Cross-sectional descriptive study | 255 nurses working in Istanbul | Emotional eating behavior, burnout levels, and their effect on job performance | Nurses with different experience levels and job satisfaction levels | Not reported | Significant positive relationship between burnout, emotional eating, and job performance | Small sample size; single hospital study may not generalize findings; self-reported scales may introduce bias | Approved | Not detailed | Work environment factors, job satisfaction, and intensive care exposure | Burnout and emotional eating behavior negatively affect job performance. Recommendations include stress management training, psychiatric support, and organizational changes to improve nurses’ emotional and physical well-being. |
| 9.Gilbert et al. (2023) [7] | Observational (multi-wave) | University and medical center staff (n=1,994 wave 1; 1,426 wave 2; 1,363 wave 3) | Physical activity and diet during COVID-19 | Mental well-being, depression, anxiety, stress | Not specified | Maintained or increased physical activity and a healthy diet were significantly associated with reduced risk of worse mental health outcomes (ORs 0.44–0.76). | Self-reported data, potential recall bias, no pre-pandemic data, generalizability limited to one employer. | Approved by Washington University IRB | No specific sample calculation described; participation across three waves | Clinical role, age, gender, race, income, ethnicity | Maintaining/increasing PA and diet correlated with better mental health outcomes (e.g., reduced anxiety, stress). |
| 10.Tohary et al. (2022), [14] | Systematic review | Various studies on oral health | Diet and nutrition’s impact on oral health | Sugary diets, processed foods, nutrient-rich diets | Not specified | Not applicable | Relied on secondary data, potential biases in source studies, observational nature of included research | Not applicable | No specific sample calculation described. | Various dietary patterns and nutrient deficiencies | A balanced diet with essential nutrients supports oral health. High sugar and processed food consumption linked to oral diseases like caries. |
| 11.Bouillon-Minois et al. (2022),[25] | Prospective observational | 184 emergency HCWs | Night shifts on food and water intake | Day shifts as baseline | Not stated | Calorie intake decreased by 206 kcal (p=0.049) and water consumption by 243 mL (p=0.010). | Small sample size, limited to emergency HCWs; self-reported food intake data; no long-term follow-up | Yes | Not reported | Time of day, shift duration | Night shifts reduced caloric intake by 14.7%, water consumption by 16.7%, carbohydrates by 8.7%, proteins by 17.6%, and lipids by 18.7%; increased periods without eating or drinking. |
| 12.Wolska et al. (2022)[33] | Cross-sectional study | 445 healthcare workers | Shift work and dietary patterns | Daily work | Not reported | Significant differences in dietary patterns and fat intake among shift workers (p < 0.05) | Regional sample; self-reported dietary data using FFQ; cross-sectional design limits causal relationships | Approved | Not applicable | Mealtime consistency, Polish-aMED® score, dietary fat intake | Shift workers showed 2x higher odds of adherence to ‘Meat/fats/alcohol/fish’ pattern; lower adherence to ‘Pro-healthy’ dietary patterns and consistency in mealtime; higher fat intake. |
| 13.Mehrotra et al. (2021)[34] | Cross-sectional survey | 473 HCWs (doctors, nurses, pharmacists, interns, technicians) | Oral health knowledge, attitudes, and practices | Comparison across HCW categories | Not stated | Significant differences in oral health knowledge among HCW categories (P < 0.05) | Self-reported data; limited sample size; cross-sectional design | Yes | Not applicable | Demographics, profession, gender | Positive attitude towards professional dental care across all HCWs; significant variation in knowledge and practices based on profession. |
| 14.Mota et al. (2021, Brazil)[35] | Cross-sectional study | 710 Brazilian HCWs (predominantly women, aged 30-40, mostly physicians) | Impact of COVID-19 on eating habits, physical activity, and sleep | General population data for comparison | Not stated | Significant changes in sleep, diet, and physical activity patterns among HCWs | Self-reported data; potential recall bias; limited generalizability to HCWs outside Brazil | Yes | Not reported | Gender, age, professional role | Sleep-related complaints (66%); increase in carbohydrate and alcohol intake (24.5% and 27%, respectively); reduced physical activity (81.8%); self-medication for insomnia (60.3%). |
| 15.Lieffers et al., (2021),[16] | Scoping Review | Oral health professionals and dietitians in high-income countries | Nutrition care practices for oral health conditions | Nutrition care practices for oral health conditions | No conflicts reported, various funding sources | Not applicable | Limited data on dietitians; lack of detail on care provided; language restrictions (English only) | Not applicable | Not applicable | Not applicable | Identified gaps in literature; recommendations for future research on collaboration and practices |
| 16.Portero de la Cruz et al. (2020))[36] | Cross-sectional study | 171 emergency nurses | Burnout, perceived stress, diet, job satisfaction | Not applicable | No conflict of interest | Lack of physical exercise, gender, and years worked were significant predictors of burnout | Single region; potential reporting bias due to self-reported measures; cross-sectional design limits causal inference | Approved | Not applicable | Gender, years of experience, coping strategies, anxiety | Prevalence of high burnout: 8.19%. Moderate perceived stress and job satisfaction; frequent social dysfunction and somatic symptoms; problem-focused coping is commonly used. |
| 17.Souza et al. (2019)[37] | Systematic review | 33 observational studies | Shift work and its impact on eating habits | Day workers or other non-shift workers | Not reported | High risk of bias in most studies reviewed | Quality scores <70%; high bias in comparability, sample selection, and non-response; limited longitudinal data | Not applicable | Not applicable | Time of exposure, duration of workday, sleep patterns | Shift work is associated with irregular meal patterns, meal skipping, and increased consumption of unhealthy foods like saturated fats and soft drinks. Longitudinal studies are needed for causal inferences. |
| 18.Schneider et al. (2019)[3] | Secondary analysis of cross-sectional data | 18,820 participants (471 nurses, 433 healthcare professionals, 813 care workers, 17,103 non-healthcare workers) | Health-related behaviours: smoking, alcohol, physical activity, fruit/vegetable intake | General working population in Scotland | Not reported | Significant differences found in smoking, physical activity, and fruit/vegetable intake; no significant differences in alcohol consumption | Small sample size for certain subgroups (e.g., nurses); self-reported behaviours may introduce bias | Not reported | Not reported | Age, occupation group | Nurses reported better health-related behaviours (except alcohol consumption) compared to the general population. Other healthcare professionals exhibited the best behaviours overall. |
| 19.Almoteb et al. (2019)[38] | Cross-sectional study | 431 HCWs (doctors, nurses, pharmacists, technicians) | Oral hygiene status, practices, and knowledge | Comparison of doctors vs. others | Not stated | Significant differences in oral hygiene practices among HCWs (P < 0.05) | Limited to one hospital; cross-sectional design; lack of WHO oral hygiene pro forma | Yes (PSAU/CDS/430400428/2016) | Based on formula | Age, gender, profession | Fair oral hygiene status observed; doctors demonstrated better interdental aid usage; need for improved oral health education and integration into medical training. |
| 20. Van Horn et al 2019[39] | Expert workshop–based position/report; synthesizes existing education initiatives; multi-institutional/disciplinary representation | Medical students, residents, fellows, attending physicians, and other clinicians in the U.S. (and collaborators internationally) | Nutrition education frameworks, competency-based curriculum, interprofessional coordination | Pre-workshop baseline of medical nutrition training vs. proposed competency-based updates; integrated models vs. traditional curricula | Supported by NIH (NHLBI, Office of Dietary Supplements, Office of Disease Prevention) and American Society for Nutrition; | Not applicable (informal consensus report; no primary data testing) | Not empirical; consensus may reflect workshop attendees’ views; lacks direct outcome data; U.S.-centric; potential bias from funding stakeholders | Not required for workshop synthesis | Not applicable | Not applicable (conceptual framework rather than an experimental design) | Recommendations/frameworks: competency-based nutrition education, national coordination center, interprofessional collaboration models, accreditation integration |
| 21. Touger-Decker et al (2019) [40] | Practice guideline/position paper (single committee-authored; not empirical research) | Dietitians, nutritionists, and oral health professionals—recommendation target; broader public indirectly | Integration of nutrition and oral health—screening, education, referrals, medical nutrition therapy | Best-practice integrated nutrition–oral health services vs. non-integrated or standard care | Endorsed and published by Academy of Nutrition and Dietetics/Elsevier; no industry funding or conflicts disclosed | Not applicable (consensus guideline; no original data or statistical testing) | Position based on existing literature and expert consensus; may be influenced by publication bias; not a systematic review | Not required (non-research guideline development) | Not applicable | Not applicable (guideline synthesis, not primary research) | Recommendations for joint nutrition–oral health care practices, education, interprofessional collaboration, and research integration |
| 22.Ab-Murat et al., (2018)[41] | Cross-sectional survey | Malaysian dentists (81% response rate) | Mental well-being assessed through self-administered questionnaire using a conceptual framework | Not disclosed | - Positive mental well-being higher in those >40 years, married, and with children (P < 0.05) | ~2.5 (as of publication year) | Limited to Malaysian dentists - Self-reported data may introduce bias - No detailed funding disclosure - Lacks longitudinal analysis |
Approved, details not specified | Sample size not explicitly calculated | Age, marital status, parental status | - 61.7% reported positive mental well-being |
| 23.Orgel & Cavender (2018)[42] | Editorial commentary on survey | 1158 NHS staff | Lifestyle and cardiovascular health | General population benchmarks | Not stated | Rates of healthy diet and physical activity marginally better than public; significant room for improvement | Low response rate (13%); self-reported data; focus on cross-sectional findings | Not applicable | Not applicable | Fatigue, workplace environment | Poor diet (1 in 6 met recommendations; 5 in 6 consumed high sugar/fat), low physical activity (50%), and workplace barriers hinder health. Recommendations: subsidized healthy food, gym access, and behavioral counseling to improve HCWs’ health and reduce public risks. |
| 24.Torquati et al. (2017)[27] | Systematic review | Nurses/student nurses in healthcare | Interventions promoting diet and PA | Nurses with no or standard PA/diet interventions | Not reported | Promising but inconsistent effects on PA and diet outcomes in nurses. | Small sample sizes; low to moderate study quality; limited measurement of dietary outcomes; lack of objective measures. | Not applicable | Not applicable | Participant motivation, baseline health behaviors | Positive outcomes in PA (structured exercise, goal setting); dietary changes reported in few studies. Improved body composition in two studies without significant diet/PA changes. |
| 25.Ahmad et al. (2015)[43] | Cross-sectional | Healthcare professionals (N = 1,190; doctors, nurses, dentists in Punjab, Pakistan) | Dietary habits, exercise, mental well-being | Comparison with recommended guidelines (USDA, AHA, WEMWBS) | Not disclosed | Significant associations for diet, exercise, and mental well-being factors (p < 0.05) | Convenience sampling, limited to Punjab, Pakistan; self-reported BMI; no occupational stress scale; reliance on non-local guidelines (USDA); underrepresentation of dentists | Approved by CMH Lahore Medical and Dental College Ethical Review Committee | Sample size based on effect sizes; no a priori power calculation. | Sociodemographic factors, income, profession, occupational stressors | HCPs in Pakistan have poor adherence to dietary, exercise, and mental well-being guidelines, impacting both personal and professional outcomes. |
| 26.Waqas Ahmad et al., (2015)[44] | Cross-sectional | Healthcare professionals (N = 1,319; doctors, nurses, dentists, pharmacists, physiotherapists in Punjab, Pakistan) | Diet, exercise, mental well-being, chronic illnesses, occupational stressors | Comparison with global and USDA dietary standards, AHA exercise guidelines, WEMWBS mental well-being scores | Not disclosed | Identified significant predictors of mental well-being (p < 0.05) | Convenience sampling, restricted to Punjab, no validated occupational stress scale; BMI based on self-reported data; limited generalizability to Pakistan. | Ethical approval obtained, but WEMWBS not translated into Urdu | Not calculated; convenience sampling used with 87.35% response rate | Sociodemographic factors, household income, career satisfaction | HCPs in Punjab exhibit suboptimal dietary and exercise habits, moderate mental well-being, and high occupational stress levels affecting both personal and professional health. |
| 27.Taylor, M. (2012)[45] | Clinical guidance document developed by Oral Health & Nutrition Reference Group; not empirical research; single-author group | Healthcare professionals (dentists and oral health teams) in Scotland; recommendations tailored to general population, especially children under 5 | Use of dietary strategies and oral health advice (impact of fermentable carbohydrates, nutrient quality, frequency of eating) | Not applicable — guidance compares best-practice dietary/oral hygiene recommendations to standard or baseline practices | Developed under NHS Health Scotland; no conflicts of interest reported | Not applicable (guidance, not original research) | Based on expert consensus and existing evidence; no new data; may not reflect all global contexts; guidance publication date (2012) may limit current relevance | Not required (guidance document, not human subjects research) | Not applicable | Not applicable; recommendations inherently account for common dietary/oral health factors | Evidence-based oral health and nutrition advice aimed at reducing caries risk, promoting healthy diet frequency and content, supporting professional oral health counselling practices |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



