
Submitted:
19 March 2025
Posted:
20 March 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The declaration of COVID-19 as a pandemic by the World Health Organization in 2020 led to the widespread suspension of clinical practices worldwide, including dentistry. This study aims to evaluate the impact of these restrictions on oral health and dietary habits. Methods: A retrospective cross-sectional study was conducted at Egas Moniz University Clinic (Lisbon Metropolitan Area), covering the period from June 2019 to June 2021. A total of 3,380 participants were included and categorized into two cohorts: pre- and post-COVID-19 restrictions. Data was collected through a structured questionnaire assessing oral health behaviors and dietary habits. Results: Out of 3,469 incoming patients, 3,380 met the inclusion criteria. Statistically significant post-lockdown changes were observed in body mass index, smoking status, oral hygiene behaviors, and specific dietary patterns such as tobacco and honey consumption, there was a decreased use of dental floss, mouthwash and altered tooth brushing frequency. Conclusions: COVID-19-related restrictions had an unequal impact on oral health and dietary behaviors in the studied population, highlighting the need for targeted public health strategies to mitigate the effects of such disruptions on vulnerable groups.
Keywords:
Covid-19
; Oral health
; Oral health habits
; dietary habits
; pandemic
; covid restrictions
1. Introduction
In 2020, the World Health Organization (WHO) declared COVID-19 a pandemic [1]. The uncertainty regarding the transmission of the coronavirus and concerns about its spread led health authorities worldwide to suspend certain clinical practices, including dentistry [2]. This pandemic response changed how dental care was delivered. Many dental offices and healthcare institutions, adapting to social isolation measures new treatment protocols. During this period, they could only provide urgent and emergency care [3,4].
The COVID-19 pandemic changed daily routines and eating habits worldwide. Remote work, more reliance on home-delivered fast food, and delayed dental visits have raised the risk of oral health problems [5].
As a result, patient care underwent significant changes, with uncertain consequences for oral hygiene and oral health complications [6,7]. In this context, dental clinics play a vital role in reinforcing proper oral hygiene practices. Routine check-ups allow clinics to teach patients about effective brushing and flossing techniques that are often overlooked in daily routines. This education helps reduce the negative impacts of limited access to dental care [7].
The pandemic, especially during the periods of lockdown, significantly affected emotional well-being of many people [5]. People frequently turn to unhealthy activities as coping techniques while under stress [8,9]. Spending extensive periods at home during lockdown, often accompanied by stress and boredom, led people to smoke more frequently [10,11] and increase their intake of meals, snacks, and comfort foods—typically high in sugar [12,13,14,15]. On the other hand, the additional time available at home should help individuals to devote greater attention and care to their oral hygiene routines, potentially benefiting their oral health, even if this were not verified.
Thus, a significant shift in dietary habits can be observed, characterized by increased consumption of sugary foods and a decline in oral hygiene practices. These behavioral changes may contribute to a higher incidence of oral health issues, including an increased prevalence of dental caries [16].
Nevertheless, despite this context, the impact of the COVID-19 pandemic on oral health habits remains poorly explored. Therefore, we conducted a retrospective analysis of a sample of first-time patients attending a reference dental clinic at a Portuguese university, aiming to understand the effects of pandemic-related restrictions on their oral health and dietary habits. The null hypothesis (H0) tested in this study is that the restrictions imposed during the COVID-19 pandemic had no significant impact on oral health or dietary behaviors.
2. Materials and Methods
This study adhered to the STROBE guidelines for the reporting of observational studies in epidemiology [17] and complied with the ethical principles outlined in the Declaration of Helsinki (1975), last revised in 2024. Ethical approval was granted by the Institutional Review Board (or Ethics Committee) of Egas Moniz (ID no. 898, issued on 24 September 2020). During the initial appointment, all participants provided written informed consent.
2.1. Study Setting and Participants
This study was designed as a retrospective analysis of responses obtained from a questionnaire filled out by new patients during their first consultation, using a comprehensive database of patients who attended the clinic between June 2019 and June 2021. The questionnaire followed the guidelines set out in the World Health Organization’s (WHO) Oral Health Surveys: Basic Methods (5th Edition).
The initial questionnaire collected essential demographic data, such as age, sex, educational level, employment status, medical history, medication use, smoking habits, and oral hygiene practices. Inclusion criteria require participants to be aged 18 years or older and provide written informed consent. Total edentulism was an exclusion criterion.
Participants were divided into two distinct groups based on the period during which they completed the questionnaire: Group 1 (BCR) – before COVID-19 restrictions (June 2019 to early March 2020), and Group 2 (ACR) – after COVID-19 restrictions (May 2020 to June 2021).
2.2. Dependent Variables
Oral hygiene habits were assessed based on the frequency of tooth brushing (2–3 times daily, once per day, 2–6 times per week, or never), the choice between a manual and an electric toothbrush, as well as the use of dental floss and mouthwash.
Additionally, dietary habits were examined, including the consumption of fresh fruit, biscuits, cakes, sweets or candies, lemonade or other soft drinks, coffee with sugar, and tea with sugar. The frequency of consumption was categorized as several times a day, daily, several times a week, once a week, several times a month, or rarely/never.
2.3. Independent Variables
Sociodemographic data was collected through a self-administered questionnaire completed before the clinical assessment to minimize potential response bias.
The independent variables included key indicators related to health determinants and sociodemographic characteristics, specifically age, gender, educational attainment, smoking habits, and body mass index (BMI). Gender was categorized as male or female. Age was recorded as a continuous variable (in years) and later classified into four categories: 18–24, 25–44, 45–64, and ≥65 years. Educational attainment was categorized following the guidelines provided by the International Standard Classification of Education (ISCED, updated in 2011). This classification methodology aligns with previous studies evaluating similar variables [18,19,20].
2.4. Statistical Analysis
Data analysis was conducted using IBM SPSS Statistics version 28.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were computed to summarize demographic and clinical data. Inferential analysis was performed using independent samples t-tests to evaluate differences between the two groups (before and after COVID-19 restrictions) regarding various variables. Statistical significance was set at a p-value lower than 0.05 (p < 0.05).
3. Results
3.1. Participants inclusion and characteristics
Out of a total of 3,469 incoming patients, 3,380 (97.4%) met the eligibility criteria, whereas 89 individuals were excluded from the study. Reasons for exclusion included being under 18 years of age (n=44; 1.3%) or being edentulous (n=45; 1.3%) (Figure 1)
Table 1 provides a detailed sociodemographic, health, and behavioral characterization of 3,380 participants, categorized into two distinct groups: pre-lockdown (n = 2,278) and post-lockdown (n = 1,102). Overall, females represented 59.4% of participants, decreasing slightly from 60.1% pre-lockdown to 56.8% post-lockdown. Conversely, males accounted for 40.6%, showing an increase from 39.9% pre-lockdown to 43.2% post-lockdown.
The mean age of participants was 43.21 years, with a minor decline from 43.36 years pre-lockdown to 42.90 years post-lockdown. Age distribution revealed that 21.3% were in the 18–24 years category, 32.4% were aged 25–44 years, 32.2% belonged to the 45–64 years group, and 14.2% were 65 years or older.
Regarding education levels, participants without formal education comprised 22.4%, showing a reduction from 24.1% pre-lockdown to 18.7% post-lockdown. Elementary education was reported by 37.4%, slightly decreasing from 37.7% pre-lockdown to 36.8% post-lockdown. Middle-level education was indicated by 26.9% of participants overall. Higher education notably increased from 0.7% pre-lockdown to 8.7% post-lockdown, with an overall percentage of 3.3%.
In terms of Body Mass Index (BMI), 3.6% of participants had a BMI below 18.5 kg/m2. The majority (46.1%) had a BMI within the normal range (18.5–24.9 kg/m2), increasing from 44.5% pre-lockdown to 49.5% post-lockdown. Those classified as overweight (25.0–29.9 kg/m2) represented 34.1%, with minimal variation between periods. Participants classified with obesity (BMI ≥ 30.0 kg/m2) accounted for 16.2% overall, decreasing from 17.3% pre-lockdown to 14.0% post-lockdown.
Lastly, 79.2% of the participants reported being non-smokers. However, there was a notable increase in active smokers from 18.0% pre-lockdown to 26.6% post-lockdown.
Table 2 summarizes oral hygiene practices of the 3,380 participants, divided into pre-lockdown (n = 2,278) and post-lockdown (n = 1,102) groups. The majority (88.6%) of participants used manual toothbrushes, with minimal variation between periods (88.5% pre-lockdown vs. 88.6% post-lockdown). Electric toothbrush usage was relatively low, representing 10.9% overall, with a slight increase from 10.8% pre-lockdown to 11.1% post-lockdown.
Regarding tooth brushing frequency, 75.6% brushed their teeth 2–3 times daily overall, although this percentage significantly decreased from 81.2% pre-lockdown to 64.2% post-lockdown. Participants brushing once daily accounted for 15.0%, slightly declining from 15.5% pre-lockdown to 14.1% post-lockdown. Notably, those brushing 2–6 times weekly increased substantially from 1.9% pre-lockdown to 18.5% post-lockdown, with an overall average of 7.3%. Participants who never brushed their teeth constituted 2.1%, rising from 1.5% pre-lockdown to 3.2% post-lockdown.
Dental floss was not commonly used, with 65.8% of participants reporting no flossing, increasing from 62.0% pre-lockdown to 73.7% post-lockdown. Correspondingly, dental floss use decreased from 38.0% pre-lockdown to 26.3% post-lockdown, with an overall usage of 34.2%.
Mouthwash use was reported by 43.1% of participants overall, with a decrease from 44.5% pre-lockdown to 40.1% post-lockdown. Conversely, those not using mouthwash increased slightly from 55.5% pre-lockdown to 59.9% post-lockdown, totaling 56.9% overall.
Table 3 provides descriptive data regarding the dietary habits of the 3,380 participants.
Fresh fruit consumption was frequent among participants, with 44.7% reporting consumption several times a day, increasing slightly from 43.8% pre-lockdown to 46.7% post-lockdown. Daily fruit consumption remained stable around 30.5%. A small percentage (3.8%) seldom or never consumed fresh fruit.
Regarding biscuits and cakes, 44.1% of participants reported weekly consumption, with little variation between periods. Daily consumption decreased slightly from 18.8% pre-lockdown to 15.6% post-lockdown. Conversely, those seldom or never consuming biscuits and cakes increased from 26.9% pre-lockdown to 29.7% post-lockdown.
Daily honey consumption showed a small increase from 7.0% pre-lockdown to 9.1% post-lockdown and once a week consumption increased from 19,4% pre-lockdown to 21,1% pós-lockdown.
Sweets or candies had weekly consumption reported by 44.1% of participants overall, increasing slightly post-lockdown (45.6%) compared to pre-lockdown (43.4%). Daily intake decreased from 13.2% pre-lockdown to 12.3% post-lockdown, while occasional consumption (several times a month) slightly increased post-lockdown.
The majority (54.6%) of participants reported seldom or never consumed lemonade or soft drinks, with little variation between pre-lockdown (54.3%) and post-lockdown (55.1%). Daily consumption decreased from 10.2% pre-lockdown to 8.5% post-lockdown.
78.1% of participants rarely or never added sugar to their tea. Regular tea consumption (daily or several times daily) was stable at around 9.8% overall, with minimal variation between the two periods.
Coffee with sugar was consumed several times a day by 21.0% of participants overall, decreasing from 22.5% pre-lockdown to 18.1% post-lockdown. Notably, the percentage of participants who seldom or never drank coffee with sugar decreased from 54.0% pre-lockdown to 47.7% post-lockdown. Additionally, there was a substantial increase in missing or non-responses post-lockdown (16.2%).
Table 4 clearly summarizes the results of independent samples t-tests comparing oral health and dietary habits between pre-lockdown (n = 2,278) and post-lockdown (n = 1,102) groups.
Significant differences (p < 0.05) are observed in BMI, active smoking, honey/jam consumption, coffee with sugar consumption, dental floss usage, mouthwash usage, and tooth brushing frequency, indicating notable changes in these behaviors post-lockdown.
4. Discussion
This retrospective study assessed oral health habits and behaviors in a Portuguese adult population using self-reported questionnaires completed during initial dental consultations. The main goal was to evaluate how oral health habits were affected by the COVID-19-induced lockdown by comparing self-reported practices and attitudes before and after this period across various demographic and behavioral factors.
During the COVID-19 pandemic, restrictive policies such as lockdowns, social distancing, and isolation significantly impacted daily routines, mental health, economic stability, and lifestyle habits, potentially influencing smoking behaviors and patterns among individuals [21].
The implementation of lockdown measures significantly impacted lifestyle behaviors, including smoking habits. Evidence from recent studies indicates that social isolation and psychological stress associated with home confinement led to increased tobacco consumption [21,22,23]. In Italy, a web-based cross-sectional study conducted during the lockdown revealed that approximately 30% of smokers increased their cigarette consumption by an average of 5.6 cigarettes per day, while a small proportion (0.6%) of former smokers resumed smoking [22]. This shift towards increased smoking aligns with a systematic review and meta-analysis showing that, despite varied individual responses, a considerable number of smokers globally reported heightened tobacco use during the pandemic period [23].
Furthermore, the COVID-19 lockdown conditions not only increased smoking frequency among existing smokers but also influenced smoking initiation, particularly among vulnerable groups. A cross-sectional study in Jordan documented that 22.4% of smokers started smoking during the year of the pandemic lockdown, with young adults and females significantly more likely to begin smoking in response to the stress factors related to COVID-19 restrictions [21]. Similarly, in Portugal, individuals experiencing sustained high levels of stress, anxiety, and depression during lockdown were more likely to be smokers, suggesting tobacco use as a coping mechanism during pandemic-related restrictions [24]. The pandemic thus exacerbated unhealthy lifestyle choices, highlighting the critical need for targeted public health interventions to address increased tobacco use resulting from pandemic-related stress and social isolation.
Despite the observed mean reduction in honey consumption from the pre-lockdown to the post-lockdown group in our data, recent literature reports contrasting findings. Studies suggest that the COVID-19 pandemic has led to an increased interest in honey consumption, particularly organic honey, due to heightened consumer awareness regarding health, food safety, and sustainability [25,26]. Consumers viewed honey as a genuine, natural, and health-promoting product, integrating it more frequently into their diets to support immune function and overall well-being during and following the pandemic period. Thus, while our observations highlight a decline, existing research underscores continued and potentially enhanced appeal of honey as a beneficial food in the context of COVID-19 [27].
Our findings indicate a decrease in coffee consumption, particularly coffee with sugar, after the COVID-19 pandemic restrictions. However, other studies have shown different trends. Some research suggests that coffee consumption increased during the pandemic, possibly due to changes in daily routines and higher stress levels from social isolation [28,29,30]. In Portugal, the COVID-19 lockdown led 8.7% of people to report an increased need for stimulant drinks, primarily coffee, suggesting its role as a coping strategy in stressful times [31]. In contrast, other authors found that although spending on coffee declined, the daily amount consumed slightly increased [30]. These contrasting findings highlight the complexity of consumption behavior shifts caused by the pandemic, underscoring the importance of considering broader psychosocial and economic factors when interpreting changes in dietary habits.
Regarding oral hygiene practices, dental floss usage significantly declined by 12% (p<0.001), while mouthwash usage also decreased slightly yet significantly (p=0.015). However, tooth brushing frequency significantly improved (from 0.24 to 0.62, p<0.001). These findings suggest varied impacts of the COVID-19 lockdown on dietary habits and oral health behaviors, reinforcing previous research highlighting the influence of the pandemic on lifestyle choices [6,32]. Similar trends were observed in other studies [33], who reported increased self-reported oral health care issues such as dental plaque accumulation and tooth discoloration due to poor oral hygiene and altered dietary patterns during the lockdown period. Other studies further supported these findings, noting that dietary habits, particularly increased consumption of sweets and snacks, negatively affected oral health during confinement [34]. Additionally, a systematic review emphasized that reduced access to routine dental care and increased stress led to decreased oral hygiene practices, further exacerbating oral health problems during the COVID-19 pandemic [35].
Strenghts and Limitations
When evaluating our study, it is essential to acknowledge both its strengths and its limitations. One notable limitation is the observational nature of the study design, which does not allow for the establishment of causal relationships. Furthermore, the data were collected through a self-administered questionnaire completed by the patients themselves. This means that the responses may not fully reflect the clinical reality, as they rely on the accuracy and honesty self-reporting of the participants.
Nevertheless, the large sample size represents a major strength, enhancing the reliability and generalizability of the findings. Additionally, it is important to consider that changes in dental procedures due to the disruption of clinical activity during the COVID-19 pandemic posed further constraints to the study.
5. Conclusions
Considering the results and the characteristics of the studied population, we reject the null hypothesis of this study. Our findings indicate that the restrictions imposed during the COVID-19 pandemic had an unequal impact on oral health and dietary habits within this population. Statistically significant changes were observed in oral health-related behaviors and specific dietary patterns, including an increased consumption of tobacco and intake of coffee with sugar, alongside a marked reduction in tooth brushing frequency, flossing and use of mouthwash. These results highlight the importance of developing more nuanced and targeted strategies to better understand and address disparities in oral health outcomes, particularly in the context of lifestyle disruptions brought about by the pandemic.
Author Contributions
Conceptualization, E.G., R.C., T.D., M.N.; A.J., C.S.; Methodology, E.G., R.C, and T.D.; Validation, J.J.M; Formal analysis, E.G.; Investigation, E.G. R.C, and T.D; Resources, E.G.; Data curation, E.G.; Writing—original draft preparation, E.G., R.C, and T.D; Writing— Review and Editing, E.G., R.C., T.D., and J.J.M. Visualization, E.G.; Supervision, E.G. and J.J.M.; Project administration, E.G.;. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (or Ethics Committee) of Egas Moniz (ID no. 898 on September 24, 2020).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the study.
Data Availability Statement
The entirety of the data compiled and examined throughout this study can be found within this document. Any additional queries should be directed towards the author in charge of correspondence.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Al-Halabi, M.; Salami, A.; Alnuaimi, E.; Kowash, M.; Hussein, I. Assessment of paediatric dental guidelines and caries management alternatives in the post COVID-19 period. A critical review and clinical recommendations. European Archives of Paediatric Dentistry 2020, 21, 543–556. [Google Scholar] [CrossRef]
- Souza, T.F.d.; Martins, M.L.; Jural, L.A.; Maciel, I.P.; Magno, M.B.; Coqueiro, R.d.S.; Pithon, M.M.; Leal, S.C.; Fonseca-Gonçalves, A.; Maia, L.C. Did the Use of Minimum Interventions for Caries Management Change during the COVID-19 Pandemic? A Cross-Sectional Study. Caries Research 2023, 57, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Bekes, K.; Ritschl, V.; Stamm, T. COVID-19 pandemic and its impact on pediatric dentistry in Austria: Knowledge, perception and attitude among pediatric dentists in a cross-sectional survey. Journal of Multidisciplinary Healthcare 2021, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Cărămidă, M.; Dumitrache, M.A.; Țâncu, A.M.C.; Ilici, R.R.; Ilinca, R.; Sfeatcu, R. Oral Habits during the Lockdown from the SARS-CoV-2 Pandemic in the Romanian Population. Medicina 2022, 58, 387. [Google Scholar] [CrossRef]
- Guerreiro, E.; Botelho, J.; Machado, V.; Proença, L.; Mendes, J.J.; Manso, A.C. Caries Experience before and after COVID-19 Restrictions: An Observational Study. Journal of Clinical Medicine 2024, 13, 1164. [Google Scholar] [CrossRef]
- Wdowiak-Szymanik, A.; Wdowiak, A.; Szymanik, P.; Grocholewicz, K. Pandemic COVID-19 influence on adult’s oral hygiene, dietary habits and caries disease—literature review. International journal of environmental research and public health 2022, 19, 12744. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Ng, D.M.; Jeffery, R.W. Relationships between perceived stress and health behaviors in a sample of working adults. Health psychology 2003, 22, 638. [Google Scholar] [CrossRef]
- Nichter, M.; Nichter, M.; Carkoglu, A.; Tobacco Etiology Research, N. Reconsidering stress and smoking: a qualitative study among college students. Tob Control 2007, 16, 211–214. [Google Scholar] [CrossRef]
- Fidler, J.A.; West, R. Self-perceived smoking motives and their correlates in a general population sample. Nicotine & Tobacco Research 2009, 11, 1182–1188. [Google Scholar]
- Evers, C.; Dingemans, A.; Junghans, A.F.; Boevé, A. Feeling bad or feeling good, does emotion affect your consumption of food? A meta-analysis of the experimental evidence. Neuroscience & Biobehavioral Reviews 2018, 92, 195–208. [Google Scholar]
- Yılmaz, C.; Gökmen, V. Neuroactive compounds in foods: Occurrence, mechanism and potential health effects. Food Research International 2020, 128, 108744. [Google Scholar] [CrossRef]
- Rodríguez-Martín, B.C.; Meule, A. Food craving: new contributions on its assessment, moderators, and consequences. 2015, 6, 21. [Google Scholar] [CrossRef]
- Havermans, R.C.; Vancleef, L.; Kalamatianos, A.; Nederkoorn, C. Eating and inflicting pain out of boredom. Appetite 2015, 85, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, Y.; Isumi, A.; Fujiwara, T. Impacts of the COVID-19 pandemic exposure on child dental caries: difference-in-differences analysis. Caries Research 2022, 56, 546–554. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J Anaesth 2019, 13, S31–S34. [Google Scholar] [CrossRef]
- Guerreiro, E.; Botelho, J.; Machado, V.; Proença, L.; Mendes, J.J.; Manso, A.C. Caries experience and risk indicators in a Portuguese Population: a cross-sectional study. International Journal of Environmental Research and Public Health 2023, 20, 2511. [Google Scholar] [CrossRef]
- Mendes, J.J.; Viana, J.; Cruz, F.; Garrido, L.; Jessen, I.; Rodrigues, J.; Proença, L.; Delgado, A.S.; Machado, V.; Botelho, J. Radiographically screened periodontitis is associated with deteriorated oral-health quality of life: A cross-sectional study. Plos one 2022, 17, e0269934. [Google Scholar] [CrossRef]
- Schneider, S.L. The international standard classification of education 2011. In Class and stratification analysis; Emerald Group Publishing Limited, 2013; Volume 30, pp. 365–379. [Google Scholar]
- Khamees, A.; Awadi, S.; Rawashdeh, S.; Talafha, M.; Alzoubi, M.; Almdallal, W.; Al-Eitan, S.; Saeed, A.; Al-Zoubi, R.M.; Al-Zoubi, M.S. The impact of COVID-19 pandemic lockdown on smoking habits and lifestyle: A cross-sectional study. Health Sci Rep 2023, 6, e1392. [Google Scholar] [CrossRef]
- Ferrante, G.; Camussi, E.; Piccinelli, C.; Senore, C.; Armaroli, P.; Ortale, A.; Garena, F.; Giordano, L. Did social isolation during the SARS-CoV-2 epidemic have an impact on the lifestyles of citizens? Epidemiol Prev 2020, 44, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.R.; Evripidou, K.; Siargkas, A.; Breda, J.; Chourdakis, M. Impact of COVID-19 lockdown on smoking and vaping: systematic review and meta-analysis. Public Health 2023, 218, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.; Ferreira, S.; Moreira, P.; Machado-Sousa, M.; Couto, B.; Raposo-Lima, C.; Costa, P.; Morgado, P.; Picó-Pérez, M. Stress, anxiety, and depression trajectories during the "first wave" of the COVID-19 pandemic: what drives resilient, adaptive and maladaptive responses in the Portuguese population? Front Public Health 2024, 12, 1333997. [Google Scholar] [CrossRef]
- Murmura, F.; Liberatore, L.; Musso, F.; Bravi, L.; Pierli, G. Organic Honey - Comparison of Generational Behaviour and Consumption Trends After Covid-19. Journal of Food Products Marketing 2024, 30, 67–88. [Google Scholar] [CrossRef]
- Sedik, P.; Hudecova, M.; Predanocyova, K. Exploring Consumers' Preferences and Attitudes to Honey: Generation Approach in Slovakia. Foods 2023, 12. [Google Scholar] [CrossRef]
- Attia, Y.A.; Giorgio, G.M.; Addeo, N.F.; Asiry, K.A.; Piccolo, G.; Nizza, A.; Di Meo, C.; Alanazi, N.A.; Al-Qurashi, A.D.; El-Hack, M.E.A.; et al. COVID-19 pandemic: impacts on bees, beekeeping, and potential role of bee products as antiviral agents and immune enhancers. Environ Sci Pollut Res Int 2022, 29, 9592–9605. [Google Scholar] [CrossRef] [PubMed]
- Castellana, F.; De Nucci, S.; De Pergola, G.; Di Chito, M.; Lisco, G.; Triggiani, V.; Sardone, R.; Zupo, R. Trends in Coffee and Tea Consumption during the COVID-19 Pandemic. Foods 2021, 10. [Google Scholar] [CrossRef]
- Cummings, J.R.; Ackerman, J.M.; Wolfson, J.A.; Gearhardt, A.N. COVID-19 stress and eating and drinking behaviors in the United States during the early stages of the pandemic. Appetite 2021, 162, 105163. [Google Scholar] [CrossRef]
- Thubsang, A.; Thiwongwiang, C.; Wisetdee, C.; Chompoonuch, J.; Anson, M.; Phalamat, S.; Arreeras, T. COVID-19 pandemic affected on coffee beverage decision and consumers’ behavior. In Proceedings of the 2022 International Conference on Decision Aid Sciences and Applications (DASA); 2022; pp. 976–980. [Google Scholar]
- Fernandes, S.; Sosa-Napolskij, M.; Lobo, G.; Silva, I. Impact of the COVID-19 pandemic in the Portuguese population: Consumption of alcohol, stimulant drinks, illegal substances, and pharmaceuticals. PLoS One 2021, 16, e0260322. [Google Scholar] [CrossRef]
- Costa, A.L.; Pereira, J.L.; Franco, L.; Guinot, F. COVID-19 lockdown: impact on oral health-related behaviors and practices of Portuguese and Spanish children. International Journal of Environmental Research and Public Health 2022, 19, 16004. [Google Scholar] [CrossRef]
- Paszynska, E.; Cofta, S.; Hernik, A.; Otulakowska-Skrzynska, J.; Springer, D.; Roszak, M.; Sidor, A.; Rzymski, P. Self-Reported Dietary Choices and Oral Health Care Needs during COVID-19 Quarantine: A Cross-Sectional Study. Nutrients 2022, 14, 313. [Google Scholar] [CrossRef] [PubMed]
- Skotnicka, M.; Karwowska, K.; Kłobukowski, F.; Wasilewska, E.; Małgorzewicz, S. Dietary Habits before and during the COVID-19 Epidemic in Selected European Countries. Nutrients 2021, 13, 1690. [Google Scholar] [CrossRef] [PubMed]
- Maestre, A.; Sospedra, I.; Martínez-Sanz, J.M.; Gutierrez-Hervas, A.; Fernández-Saez, J.; Hurtado-Sánchez, J.A.; Norte, A. Assessment of Spanish food consumption patterns during COVID-19 home confinement. Nutrients 2021, 13, 4122. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
Figure 1.
Participants inclusion.
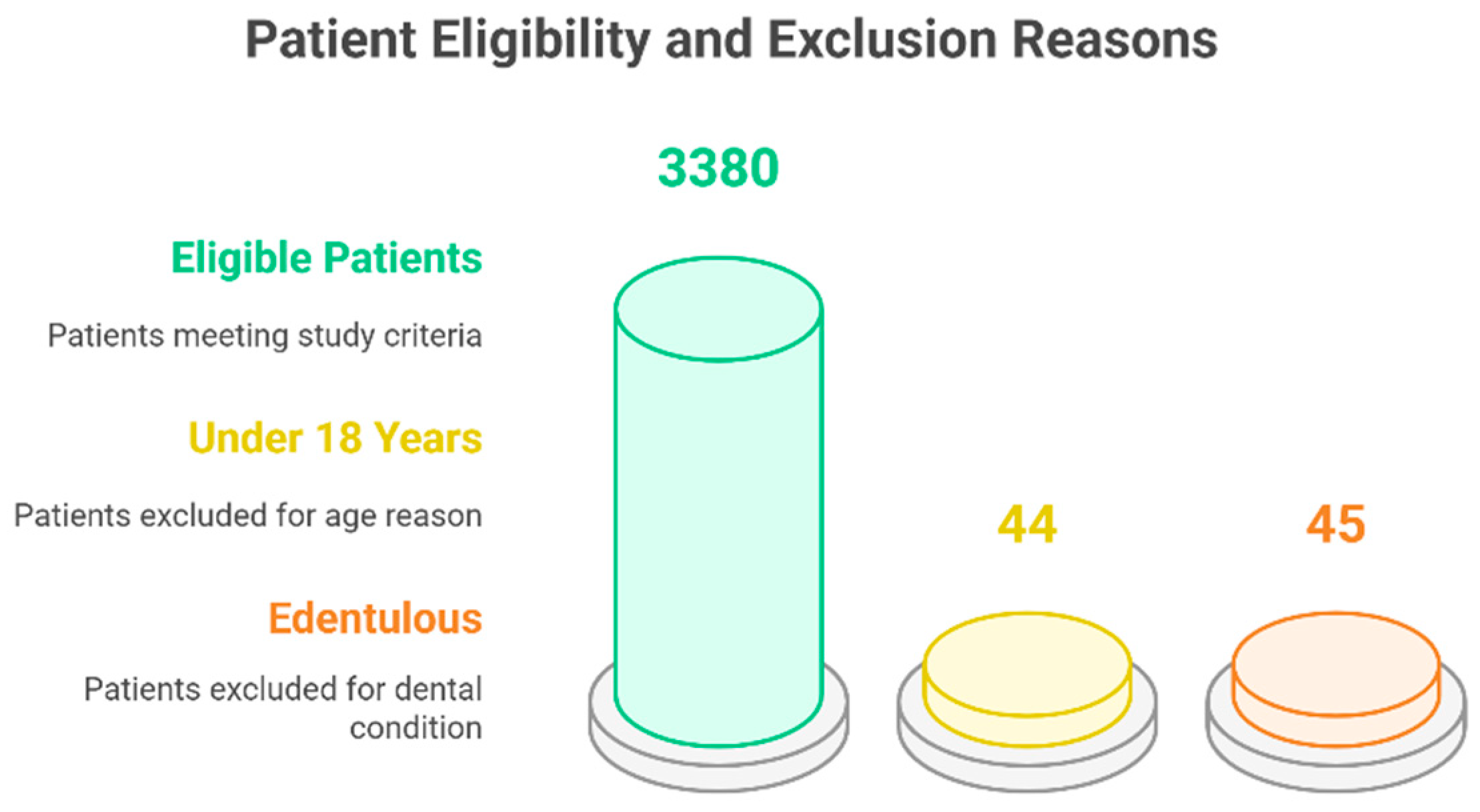

Table 1.
Sociodemographic, health, and behavior characterization of the participants (n = 3,380).
| Variable | Total (n = 3,380) | Pre-lockdown (n =2,278 ) | Post-lockdown (n=1,102) |
| Sex, % (n) | |||
| Female | 59.4 (2,007) | 60.1 (1,369) | 56.8 (476) |
| Male | 40.6 (1,373) | 39.9 (909) | 43.2 (362) |
| Age, mean | 43.21 | 43.36 | 42.90 |
| Age interval (years), % (n) | |||
| 18-24 | 21.3 (719) | 21.2 (484) | 21.3 (235) |
| 25-44 | 32.4 (1,094) | 32.3 (736) | 32.5 (358) |
| 45-64 | 32.2 (1,088) | 31.9 (727) | 32.8 (361) |
| ≥65 | 14.2 (479) | 14.5 (331) | 13.4 (148) |
| Education, % (n) | |||
| No studies | 22.4 (756) | 24.1 (550) | 18.7 (206) |
| Elementary | 37.4 (1,265) | 37.7 (859) | 36.8 (406) |
| Middle | 26.9 (1,247) | 37.4 (853) | 35.8 (394) |
| Higher | 3.3 (112) | 0.7 (16) | 8.7 (96) |
| BMI (Kg/m2) % (n) | |||
| < 18,5 | 3.6 (120) | 3.8 (86) | 3.1 (34) |
| 18.5-24.9 | 46.1 (1,558) | 44.5 (1,013) | 49.5 (545) |
| 25.0-29.9 | 34.1 (1,153) | 34.4 (784) | 33.5 (369) |
| ≥ 30.0 | 16.2 (549) | 17.3 (35) | 14.0 (154) |
| Active Smoker % (n) | |||
| No | 79.2 (2,678) | 82.0 (1,869) | 73.4 (809) |
| Yes | 20.8 (702) | 18.0 (409) | 26.6 (293) |
Abbreviations: BMI—Body Mass Index; n—number of participants.
Table 2.
Oral health care and self-reported perception about oral health condition descriptive data (n = 3,380).
Table 2.
Oral health care and self-reported perception about oral health condition descriptive data (n = 3,380).
| Variable | Total (n = 3,380) | Pre-lockdown (n =2,278 ) | Post-lockdown (n=1,102) |
| Type of toothbrush, % (n) | |||
| Manual | 88.6 (2,993) | 88.5 (2,017) | 88.6 (976) |
| Electric | 10.9 (368) | 10.8 (246) | 11.1 (122) |
| Toothbrush frequency % (n) | |||
| 2–3 times/daily | 75.6 (2,555) | 81.2 (1,847) | 64.2 (708) |
| 1 time/daily | 15.0 (507) | 15.5 (352) | 14.1 (155) |
| 2–6 times/weekly | 7.3 (248) | 1.9 (44) | 18.5 (204) |
| Never | 2.1 (70) | 1.5 (35) | 3.2 (35) |
| Dental Floss usage, % (n) | |||
| No | 65.8 (2,225) | 62.0 (1,413) | 73.7 (812) |
| Yes | 34.2 (1,155) | 38.0 (865) | 26.3 (290) |
| Mouth wash usage, % (n) | |||
| No | 56.9 (1,924) | 55.5 (1,264) | 59.9 (660) |
| Yes | 43.1 (1,456) | 44.5 (1,014) | 40.1 (442) |
Table 3.
Descriptive data on dietary habits consumption (n = 3,380).
| Variable | Total (n = 3,380) | Pre-lockdown (n =2,278 ) | Post-lockdown (n=1,102) |
| Fresh fruit % (n) | |||
| Several times a day | 44.7 (1,512) | 43.8 (997) | 46.7 (515) |
| Every day | 30.5 (1,031) | 30.4 (693) | 30.7 (338) |
| Once a week | 18.3 (618) | 19.1 (435) | 16.6 (183) |
| Several times a month | 2.7 (90) | 2.7 (61) | 2.6 (29) |
| Seldom/never | 3.8 (129) | 4.0 (92) | 3.4 (37) |
| Biscuits and cakes % (n) | |||
| Not know/not answer | 0.1 (3) | 0 (0) | 0.3 (3) |
| Several times a day | 6.3 (213) | 5.9 (134) | 7.2 (79) |
| Every day | 17.8 (600) | 18.8 (428) | 15.6 (172) |
| Once a week | 44.1 (1,490) | 44.2 (1,007) | 43.8 (483) |
| Several times a month | 4.0 (135) | 4.3 (97) | 3.4 (38) |
| Seldom/never | 27.8 (939) | 26.9 (612) | 29.7 (327) |
| Jam or Honey % (n) | |||
| Not know/not answer | 0.1 (3) | 0 (0) | 0.3 (3) |
| Several times a day | 1.1 (37) | 1.2 (28) | 0.8 (9) |
| Every day | 7.7 (260) | 7.0 (160) | 9.1 (100) |
| Once a week | 19.9 (673) | 19.4 (441) | 21.1 (232) |
| Several times a month | 2.0 (67) | 2.0 (46) | 1.9 (21) |
| Seldom/never | 69.2 (2,340) | 70.4 (1,603) | 66.9 (737) |
| Sweets/candies, % (n) | |||
| Not know/not answer | 0.1 (2) | 0 (0) | 0.2 (2) |
| Several times a day | 5.6 (190) | 5.4 (122) | 6.2 (68) |
| Every day | 12.9 (436) | 13.2 (300) | 12.3 (136) |
| Once a week | 44.1 (1,490) | 43.4 (988) | 45.6 (502) |
| Several times a month | 3.6 (123) | 3.5 (79) | 4.0 (44) |
| Seldom/never | 33.7 (1,139) | 34.6 (789) | 31.8 (350) |
| Lemonade or soft drinks, % (n) | |||
| Not know/not answer | 0.1 (3) | 0 (0) | 0.3 (3) |
| Several times a day | 6.4 (216) | 6.2 (141) | 6.8 (75) |
| Every day | 9.7 (327) | 10.2 (233) | 8.5 (94) |
| Once a week | 26.0 (878) | 25.9 (591) | 26.0 (287) |
| Several times a month | 3.3 (111) | 3.3 (75) | 3.3 (36) |
| Seldom/never | 54.6 (1,845) | 54.3 (1,238) | 55.1 (607) |
| Tea with sugar, % (n) | |||
| Not know/not answer | 0.2 (6) | 0 (0) | 0.35 (6) |
| Several times a day | 2.8 (95) | 2.8 (64) | 2.8 (31) |
| Every day | 7.0 (237) | 7.1 (161) | 6.9 (76) |
| Once a week | 10.4 (352) | 10.7 (244) | 9.8 (108) |
| Several times a month | 1.5 (51) | 1.2 (27) | 2.2 (24) |
| Seldom/never | 78.1 (2,639) | 78.2 (1,782) | 77.8 (857) |
| Coffee with sugar, % (n) | |||
| Not know/not answer | 5.3 (178) | 0 (0) | 16.2 (178) |
| Several times a day | 21.0 (711) | 22.5 (512) | 18.1 (199) |
| Every day | 15.2 (513) | 16.3 (372) | 12.8 (141) |
| Once a week | 5.3 (180) | 6.0 (136) | 4.0 (44) |
| Several times a month | 1.3 (43) | 1.3 (29) | 1.3 (14) |
| Seldom/never | 51.9 (1,755) | 54.0 (1,229) | 47.7 (526) |
Table 4.
Results of independent samples t-tests comparing oral health and dietary habits before (n = 2,278) and after lockdown (n = 1,102). Total n = 3,380.
Table 4.
Results of independent samples t-tests comparing oral health and dietary habits before (n = 2,278) and after lockdown (n = 1,102). Total n = 3,380.
| Variable | Mean (Pre-lockdown) |
Mean (Post-lockdown) |
p-value | Significant Difference |
|---|---|---|---|---|
| BMI | 1.65 | 1.58 | 0.007 | Yes |
| Active smoker | 0.18 | 0.27 | <0.001 | Yes |
| Gum bleeding | 0.39 | 0.48 | 0.367 | No |
| Dental mobility | 0.26 | 0.24 | 0.167 | No |
| Fresh fruit consumption | 2.32 | 2.24 | 0.076 | No |
| Biscuits | 3.90 | 4.01 | 0.152 | No |
| Honey/Jam | 5.19 | 5.06 | 0.013 | Yes |
| Candy chewing | 5.39 | 5.46 | 0.199 | No |
| Sweets | 4.23 | 4.17 | 0.199 | No |
| Soft drinks | 4.69 | 4.73 | 0.247 | No |
| Tea with sugar | 5.31 | 5.29 | 0.772 | No |
| Coffee with sugar | 4.15 | 3.58 | <0.001 | Yes |
| Manual toothbrush | 0.89 | 0.89 | 0.984 | No |
| Electric toothbrush | 0.11 | 0.11 | 0.406 | No |
| Dental floss usage | 0.38 | 0.26 | <0.001 | Yes |
| Interdental brush | 0.08 | 0.06 | 0.812 | No |
| Mouthwash usage | 0.45 | 0.40 | 0.015 | Yes |
| Tooth brushing frequency | 0.24 | 0.62 | <0.001 | Yes |
| Teeth self-perception | 3.65 | 3.42 | 0.713 | No |
| Gum self-perception | 3.46 | 3.16 | 0.422 | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



