
Submitted:
20 June 2025
Posted:
23 June 2025
You are already at the latest version
Abstract
Cancer progression is a multistep process driving by oncogenic forces and promoted by the close interaction between neoplastic cells and the surrounding microenviroment as well as the pre-metastatic niche. In this perspective the context of chronic arteriopathy represents a specific setting which can be associated with the arousal of lung cancer being and most often the both diseases share smoke as common risk factor. Within respect to the arterial disease we focused on the role of aneurysma dilations and on its impact on blood dynamics in cancer. Through a physical approach we defined a mathematical model which identifies altered viscosity as the physical variable linking cancer to aneurysm-related rheology. To further validate this theroretic approach an extensive screening of 976 patients carried diagnosis of cancer and arteriopaty from 2018 to 2024 was performed. From them a population of 120 cancer patients with concomitant aneurysmal disease was selected. The study cohort was subdivided based on primary site of origin into 3 groups: lung cancer (39 cases), other solid organ cancer (66 cases) and hematologic neoplasms (15 cases). Exaustive demographic, clinical and biologic data were available for each case. A close male gender-specificity was documented (83.3% of cases) as well as significant exposure to cigarette smoke. Quite surprisingly a reduced metastatic potential was reported in in all cancer types.
Keywords:
cancer
; metastases
; aneurysms
; COPD
1. Introduction
1.1. Biologic Hints in Lung Cancer Distant Spreading
Lung cancer (LC) most often presents with metastatic lesions at diagnosis [1,2,3]. Metastatic dissemination strongly affects patients’ survival and quality of life. Indeed primary tumor resection improves survival even in case of single metastases with preferential site og growth in brain or bones if compared to liver or lung [4,5]. Moreover, the recent implementation of peri- and post-operative targeted and immunotherapy has signicantly improved LC patients’s outcome [6,7]. On the other hand, the lung is a preferential site for growth of malignant nodules from distant organs and a proper diagnostic work-up to assess the primary origin is mandatory in case of synchronous or metacronosus parenchymal lesions [8]. It is, thus, mandatory to determine the biologic features leading to LC early spreading. Although a deep analysis of the biologic programmes which are implicated in metastatic progression goes beyomd the scope of this work, it should be reported that it is a highly complex and multistep process encompassing the aberrant activation of epithelial-to-mesenchymal transition (EMT), angiogenesis, and lymphangiogenesis and that involves a dynamic crosstalk between tumor microenvironment, that of the pre-metastatic niche and LC stem cells (LCSCs) [9,10,11]. These factors are largely influenced by numerous genes and non-coding RNAs (ncRNAs) as well as epigenetic mechanisms [for a review see [12,13,14,15,16]. The lung cancer microenvironment consists of lung cancer cells, stromal cells (fibroblasts, immune cells, vascular cells and endothelial cells), and the extracellular matrix (ECM), all of which create a supportive niche for tumor growth and progression [17]. The peri-tumor microenvironment can promote proliferation of transformed cells and acidity, hypoxia and inflammation are the three main pro-metastatic required environmental features of this process [18]. For what concern hypoxia the more aggressive tumor cells are the ones that were exposed to oxygen deprivation and the exosomes, namely the extracellular vescicles which contains proteins, lipids and nucleic acids, related to NSCLC may contribute to metastasis under hypoxia [19]. The exosomes interact with the LC microenvironment to mediate angiogenesis, EMT transformation, immune regulation, and other processes, playing a key role in the LC occurrence and progression [20,21,22]. Chronic inflammation create a favorite environment for the invasion of cancer cells. There are more transducers involved, among them interleukin 1B (a pro inflammatory cytokine) and IL 6 (which boost STAT1 - activator of transcription 1 are known to strengthen metastasis [23]. Exosomes that originates from cancer cells of the lung release microRNA 210 (miR-210) that induces cancer’s fibroblasts (CAF s) which are correlated to the increase the progression of the lung cancer. MiR-210 induces angiogenesis factors (FGF2 and VEGF) facilitating the process of metastatization via JAKSTAT3 pathway [24]. Cancer cells invasive capacity relies on the formation of blood vessels and lymphatics. Angiogenesis and lymphangiogenesis not only supply the nutrients required by tumor cells but also create pathways for their metastasis. Among the vascular endothelial growth factor (VEGF) family, VEGF-A primarily mediates angiogenesis, whereas VEGF-C and VEGF-D are associated with lymphatic metastasis [25]. Ovarell, although a relevant amount of literature describes the molecular and genetic drivers of distant spreading, fewer data are till now available regarding the complex interplay between invasive clones and the context in which the move and how it could really affect cells fate. Thus the aim of this work, which if focused on the evaluation of the role on blood flow - in which metastastic cells are immersed and are floating - of the altered biomechanis and dynamics related to arteriopathy, such as aneurysmatic dilations, which most often affect smoker patients whith lung cancer.
1.2. Vascular Pathophysiology
The main physical characteristics of the arteriar wall affect its compliance and distensibility [26]. Bigger vessels stiffness may vary owing to modifications in the makeup of the wall that lead to changes in the elastic structure. Thus, vascular aneurysms have a multifactorial pathogenesis, essentially characterized by elastin and collagen degradation at wall level, apoptosis of vascular smooth muscle cells, and infiltration of leukocytes into the aneurysmal tissue [27]. Furthermore, vascular inflammation is the key process underlying vascular diseases onset and progression. Arterial vessel rupture is a devastating complication that occurs when the local wall stress exceeds the wall strength, resulting in intra-abdominal hemorrhage with mortality of 85% [28]. The disease is usually asymptomatic but leads to high mortality due to the risk of artery rupture [29]. In aneurysmatic dilation the reorientation of adventitial fibers in the circumferential direction alters the anisotropic properties of the vessel and likely contributes to diminished compliance. Patients with aneurysm of abdominal aorta have decreased wall distensibility as estimated by the pulse wave velocity (PWV) compared with age- and sex-matched patients without it [30]. This factor suggests an increased stiffness of the arterial tree. With increased wall stiffness, there is increased velocity of the forward pulse wave, and peripherally reflected arterial waves reach the heart in early systole, rather than diastole, causing increased systolic blood pressure, lower diastolic blood pressure, augmentation of the cardiac workload, and decreased coronary perfusion pressure. Propagation of the pulse wave through the arterial tree depends on the physical properties of the blood, which are relatively invariable, and the characteristics of the arterial wall, including its stiffness and geometry. Indeed, the term stiffness refer to the structural stiffness of the aorta, largely driven by the change in geometric effects accompanying changes in compliance, as well as the material stiffness, which describes the intrinsic properties of the arterial wall.
1.3. The Interplay Between Smoke, Cholesterol, Cancer and Vessels
Tobacco smoke is among the key risk factord for both cardio-vascular disease and cancer onset [31]. There is a close relation between cancer development and the number of cigarettes/day smoked, with the duration of the habit in years, the depth with which the smoke is inhaled, he tar and nicotine content of cigarettes smoked. The relative risk of smokers of getting bronchogenic carcinoma is about 14 times higher than that of non-smokers, while for heavy smokers (for those who consume more than 25 cigarettes/day), this risk rises to 30 times. For those who stop smoking the risk progressively reduces over the following 7-10 years, after which it returns to overlap that of non-smokers. Exposure to passive smoking is also a risk factor for the development of lung cancer, particularly if it occurred at a young age (under 25 years of age). Smoking has a direct carcinogenic effect (genotoxic damage) due to the a number of substances produced during combustion. Among the components of cigarette smoke, the main carcinogenic action is attributed to polycyclic aromatic hydrocarbons, indirect carcinogens that require transformation into active intermediates by microsomal enzymes present at the bronchial cell level [32,33,34,35,36]. Moreover, exposure to nicotine is associated to cancer cell proliferation and increased angionesis and tumor vascularization [37]. Smoking-related effects associated to aneursysmatic vascular dilation hare the following) smoke-induce activation of circulating markers among which tissue plasminogen activator (tPA). The latter is implicated in elastolysis [38]. The effect is higly augmented, significantly more than that induced by atherosclerosis, when skoking habit is associated to genetic germline variants, mainly those affecting the 3.12.3 chromosome. It is also coincevalble that smoke could exert epigenetic modulation of histone acetylation involved in cardiovascular diseases and remodelling [39]. It should be also remarked that a significant association exists between smoke, atherosclerosis and aneurysm formation [40,41]. In detail HDL cholesterol levels have been linked to the inflammatory-mediated matrix alteration involved in the development of admonival aortic aneurysms [42,43] . Moreover, most recent data point out that PD-1 (programmed death -1) and its ligand PDL-1 is overexpressed in smoke-related cancers as well as in aneurysmatic arteries [44]. Thus, immunecheck point inhibition relies on a strong rationale mainly in the LC population which carries smoke-related vascular inflammation and aneurysms formation and progression [45,46,47].
2. Methods
We here aim at analysing the fluid-dynamics of metastatic cells moving into smoking-related pathologic blood vessels to describe a real-life setting for cancer distant spreading. To reach this goal we developed a integrated approach based on theoretical application of physical laws as well as on the analysis of patients’ dataset.
2.1. Modelling
Despite the biological uniqueness of the circulatory system, the elemnetary principles that regulate it are based on the fluid dynamics laws [48,49]. Blood is composed of two main elements, namely the plasma and cellular elements (red and white cells and platelets). Within respect to fluid dynamics the plasma can be assumend as a Newtonian fluid, whereas the whole blood shows non-Newtonian behaviour [50]. The main differences with the Newtonian model for blood are found above all at low velocities in the recirculation zones and in secondary flows. Overall blood dyminc properties cannot be fully described by the Navier-Stokes equations which describe a linear viscous fluid. Here we aim at integrating the already available knowledge on hemodynamics into the dual pathologic context represented by vasculopathy - mainly with artery wall pathology - and cancer to generate a formal theory to recapitulate real life disease onset and progression.
2.2. Patients Identification and Selection
To further analyse the metastatic pattern in case of cancer associated with aneurysmatic dilations, we retrospectively investigated a consequent serie of 976 patients diagnosed with cancer and arteriopathy between January 2018 and December 2024 at the IRCCS San Matteo Hospital Foundation. Of them, we selected the 120 patients affected by cancer and aneurysms. Exhaustive demographic and clinical data are detailed in Table 1. This is not a clinical trial. Informed consent from each patient was routinely collected at hospital admission in accordance with standard hospital procedures. Patient data were collected through consultation of operating directories; pneumological and vascular surgery reports and discharge letters.
2.3. Statistical Analysis
Statistical analysis was carried out using the Excel add-in package. The continuous variables were expressed as the mean value ± the standard deviation (SD), and the latter was compared using the Student’s t-test for independent variables. The nominal variables were compared using χ2 tests. The Kaplan–Meier method was used to generate the cumulative survival curves, and the log-rank test was used to calculate the differences between the curves. A p-value < 0.05 was considered statistically significant. The entire dataset was then tested using the JMP partition algorithm (JMP-Statistical Discoveries, from SAS; website at www.jmp.com), which can search for all possible subdivisions of the best predictors of response/outcome and event probability distribution.
3. Results
3.1. Definition of a Mathematical Model
A fluid is defined as Newtonian if the tangential stress τ is directly proportional to the shear rate ƴ; otherwise a fluid that does not have these characteristics is called non-Newtonian. In cancer blood viscosity (µ) is known to be increased if compared to physiologic conditions [51,52,53,54,55,56] based on several mechanisms. Red blood aggregation [57] is aberrantly increased through a direct interaction with tumor cells mediated by molecules such as galectin-4 [58], vascular endothelial growth factor (VEGF), elastin-derived peptides (EDPs), sialic acid (TSA) [59]. Moreover blood viscosity positively correlates with the cancer stage [60] and it is exploited by metastatic cells to enhance their invasive capacity [61,62,63]. Indeed, genetic activation of invasive growth program mediates thrombosis [64,65] and platelets activation [66] ultimately leading to the development of intravascular scaffolds able to promote cell motile phenotype and scattering [67]. Within respect to arterial aneurysms, there are essentially two types, namely the fusiform ones which are dilations that involve the entire circumference of the artery and the saccular ones which are swellings that involve only one side of the aortic wall. The maximum stress increases with the diameter of the aneurysm and with the reduction of the thickness of the vessel. This stress is strongly linked to the pressure curve. The geometric irregularities provide an amplification of the stresses on the aneurysm wall. Regarding the flow stream into a tube of a defined length (L), it should be underlined that a flow of a fluid can be defined as laminar or turbulent based on the value of the adimensional parameter called Reyonold number (Re= ƴ L/µ) [68]. Turbulent flows are composed of vortices and re-circulations of very different scales which, based on the flow profile, form, disintegrate and combine with each other. Dean number is basically just Reynolds number modified to add in the variables of the pipe the fluid is flowing through. Dean number (De) is a dimensionless number, which describes the relative importance of inertial forces to centrifugal forces to curved flows. At low numbers, the flow is characterized by a stable, axisymmetric vortex core, while at high numbers, the flow becomes unstable and develops a complex secondary flow structure. In other words, low De correspond to laminar flow, whereas high De describes turbulent regimes. The viscosity is a physical quantity that defines the internal friction of a fluid, in other words it is the set of friction forces that are generated between the individual layers of fluid. The coefficient of viscosity η is the ratio (defined by Newton) between the shear stress τ and the shear rate γ. Moreover, the shear stress expresses the ratio between the force applied to a flui d layer in the direction of flow (F) and its area (A). Thus: η = τ/γ = F/A. In other words, the more viscous is the fluid, the greater is the force required. When this comcept is applied to blood, it should be noted that blood is a complex suspension where the red blood cells and other corpuscular elements are immersed in plasma, a colloidal solution. Into the blood the ration between the shear stress τ and the shear rate γ is not constant as in ideal fluids. For instances, in those vessels of smallest caliber the speed is significantly reduced, the viscosity values vary and it is only due to the rheological properties that the formation of thrombosis is prevented. Reference is commonly made to well-defined viscosity values that correspond to the shear stress of large arteries. Plasma alone can be considered, with a fair amount of approximation, a normal viscous liquid, that is, obeing the Poiseuille formula in a laminar regimem. Whole blood is not a Newtonian fluid, being characterized by an increase in viscosity at low shear rates, but for high deformation rates the viscosity of blood stabilizes at about 3.4 mPa×s (with a range of 2.2 – 4.5) in fact, for high deformation rates, red blood cells are deformed and their aggregates dispersed. These characteristics allow us to consider blood as an approximately Newtonian liquid in the case of flows inside large vessels. The main differences with the Newtonian model for blood are found above all at low velocities in the recirculation zones and in secondary flows. With these approximations, the fluid dynamics of blood can be described by the Navier Stoks equations (system of differential equations) that describe a linear viscous fluid. From these, the Poiseuille equation describes the relationship between pressure drop and flow output can be derived as follows: Δp = 8ηLQ/ πR4= 8π LQ/S2 and Q= πR4/8ηLΔp where Δp is the difference of pressure between the two extremes, L: length of vessel, η: fluid viscosity; Q: flow output/unit of time , R: vessel radius; S: vessel section. The viscosity of plasma is approximately 1 ½ times the viscosity of water and does not depend much on the concentration of proteins. Plasma viscosity is a function of temperature only. Blood viscosity is mainly influenced by plasma viscosity, temperature, hematocrit and the deformability of red blood cells. Indeed, the increase in red blood cells in the plasma, and therefore of the hematocrit, disturbs the flow lines, progressively increasing their viscosity. A non-Newtonian fluid and is described with the same equation by replacing the viscosity with the apparent viscosity. The apparent viscosity is not constant and is no longer a thermophysical property of the fluid, but depends on the flow field. One of the most used to describe the apparent viscosity of blood is the “Carreau-Yasuda model” [69,70,71] which allowing to describe the pseudo-plastic behavior for a wide range of shear rates. These are a class of more realistic models as they include not only shear thinning but also the Newtonian plateau at low and high shear rates. Blood viscosity is known to be directly influenced by acute or chronic pathological conditions.
In Newtonian fluids, which characterize vessels featuring diameter > 100 , viscosity is a function of plasma features whereas the cellular-related effect is negligible. However, it is known that - in case of cancer - extracellular fluid viscosity is altered and cooperates in tumor dissemination [72]. In smaller vasculature (diameter < 30 ) the cellular-related effects on viscosity become predominant in basal conditions and extremely significant in malignant contexts according to the biologic reasons above discussed. Thus, viscosity, a key parameter in circulation dynamics, is highly influenced by cancer and in most instances, hyper-viscosity is exploited by cancer clones to disseminate. Flows in curved tubes, as in aneurismatic arterial tracts, are characterized by strong secondary velocities that manifest themselves as counter-rotating vortices, called Dean cells, produced by a centrifugal instability [73]. Into an aneurysmatic cavity the flow topology is shown to be a function of De under pulsatile stream [74] and the vortex inside it progress through the same cycle. Notably De is related to blood viscosity and influenced by the concomitant occurrence of cancer. Overall a relantioship between the two conditions (cancers + aneurysms) can be postulated (Figure 1).
3.2. Population Characteristics and Clinical Analysis
To validate the study hypothesis a consecutive series of 120 patients affected by both cancer and aneurysms has been selected and analyze. The median age of cancer diagnosis was 72.88 years. Twenty out of the 120 cases, were females, whereas the vast majoiry of cases (83.3%) were males. Details on primary site of cancer origin, histotype and disease stage are detailed in Figure 2A-C. The vast majority of cases were active or past smokers and only 18 patients (15%) were never smokers: of the 11 were females (61.11%) mainly affected by breast cancer (7 cases) and gynecological tumors (3 cases). Two patients carried two different primary cancers: a case of concomitant diagnosis of lung and prostate cancers and another one of breast and endometrial cancer. We then focused on three distinct cancer population, namely those affected by lung cancer (39 cases, 32.5%), other cancers with different site of primary origin (66 patients, 55% of cases) and hematologic malingnancies (15 cases, 12.5%). The vast majoiry of patients carried inflammatory intra-addominal aneurysm (IAAA), whereas in sime instances aneurysmal disease involved two or more other arterial district (Figure 2D); 43.8% of cases underwent endovascular surgical repair which occurred after tumor onset (Figure 1E) Within respect to LC the vast majority of diagnoses (36 cases) were non-small cell lung cancer (NSCLC) and three cases of small cell lung cancer (SCLC). Regarding the NSCLC histotypes, 23 cases (63.88%) were adenocarcinoma (ADC) and 14 (36.11%) squamous cell cancers (SCC). In 20 out of the 36 cases, the PD-L1 TPS score was available and overall expressed with significanlt higher levels 50% in 10 cases, 5- 50in 5 cases, and 1% in 5 cases; the overall median expression wa of 30.03 (Figure 2F). All LC patients were current or previous smokers and arterial aneurysms were known beferore LC detection. Quite suprinsingly of all epithelial solid cancers - irrespective of the primary site of origin - only 14 cases (13.3%) featured a metastatic disease at time of dignosis and in only 4 patients (3.8%) the sites of secondary growth were more than two. Six out of 39 LC featured TNM stage IV disease but only 3 cases (7.6% of diagnosis) carried extrathoracic secondary lesions. Of them two cases of SCLC (bone metastases) and liver metastases in 1 NSCLC. We then moved to check the biochemical asset of each analyzed case. In detail we focus on the most relevant variable involved in inflammation and atheroschelosis. For all enrollered cases the value of PLT and serum total cholesterol were available, with an average value of 216.4 and 141 mg/dL respectively. The average value of cholesterol HDL was 46.33 mg/dL. No significant variations could be documented between baseline and the time of cancer diagnosis For 25 cases the serum LDL value wav available with an average level of 74.64 mg/dL. Overall the level of serum C-reactive protein (CRP), a systemic marker of inflammation, at time of cancer diagnosis was, unespectedly, low with an average value of 1.22. Within respect to respiratory function, in 41 out of the 120 cases a diagnosis of COPD was reached; in the remaining 79 cases a spirometry wasn’t performed even in case of inveterate smoking habit (Figure 3). These observations were then compared to the consequent unselected thoracic cancer population diagnosed and followed in our Institution in the same time interval. As expected, male patients reprent the 70.69% of cases. Notably the vast majority of tumors were adenocarcinomas (60.65%) and the prevalence of metastatic disease at diagnosis was of 48.27%. The differences in metastatic spreading observed in the cohort in study and in the unselected thoracic cancer population are statistically significant being the χ2 27.022. and the p-value is < 0.00001 (significant at p < .05).The primary site of origin was the lung (being NSCLC 75.48% and SCLC 5.74% of diagnosis) whereas in about 10% of cases lung lesions revealed as secondary masses from other organs (most often breast - 4% of cases). To further strengthen the study findings we retrospectively evaluated the incidence of cancer diagnosis among unselected patiens hospitalized in Vascular Surgery Unit and includes in the analys all cases of aneurysms (abdominal, thoracic and iliac aorta) treated from the 1st January 2024 to the 31st Januart 2025, excluding operations performed for any complications (e.g.,endoleak). Overall 171 cases were evalualted and the 15.78% of them were females. The occurrence of cancer was reported in 21.63% of cases and the majority of them (59.45%) carried an early stage disease. Lung cancer represented about 30% of diagnosis and metastatic dissemination was detectable in 50% of cases., although the limited number of cases cannot be enough to evaluate a statistical siginificance. Within respect to metastatic cancer in unselected cancer population the χ2 is 17.1487, p-value 0.000035 (significant at p < 0.05).
3.3. Results from Partition Analysis
In order to deeper investigate the study findings, the analysis of predictiors was performed to search the possible splits associated with tumor evolution and to dientify the most important factors that predict the outcome se the resulting tree to identify markers of translational relevance. The dataset, unselected for artriopathy, gender and smoke, was tested coherently and the age of diagnosis of cancer lower than 67 and the level of total cholesterol (175 mg/dl), followed,- as expected - by histotype, emerged as most relevant factors associated to tumor progression (number of distant metastases) (Figure 4A). When introducing arterial disease as variable, it behaves as the most relevant predictor (Figure 4B), followed by tumor intrinsic biology (associated to histotype) and biochemical asset and smoking habit. When partition analysisis applied to the whole dataset (Figure 4C) arteriopathy and platelet are the most powerful phenotype determinants (reduced metastatic pattern).
4. Discussion
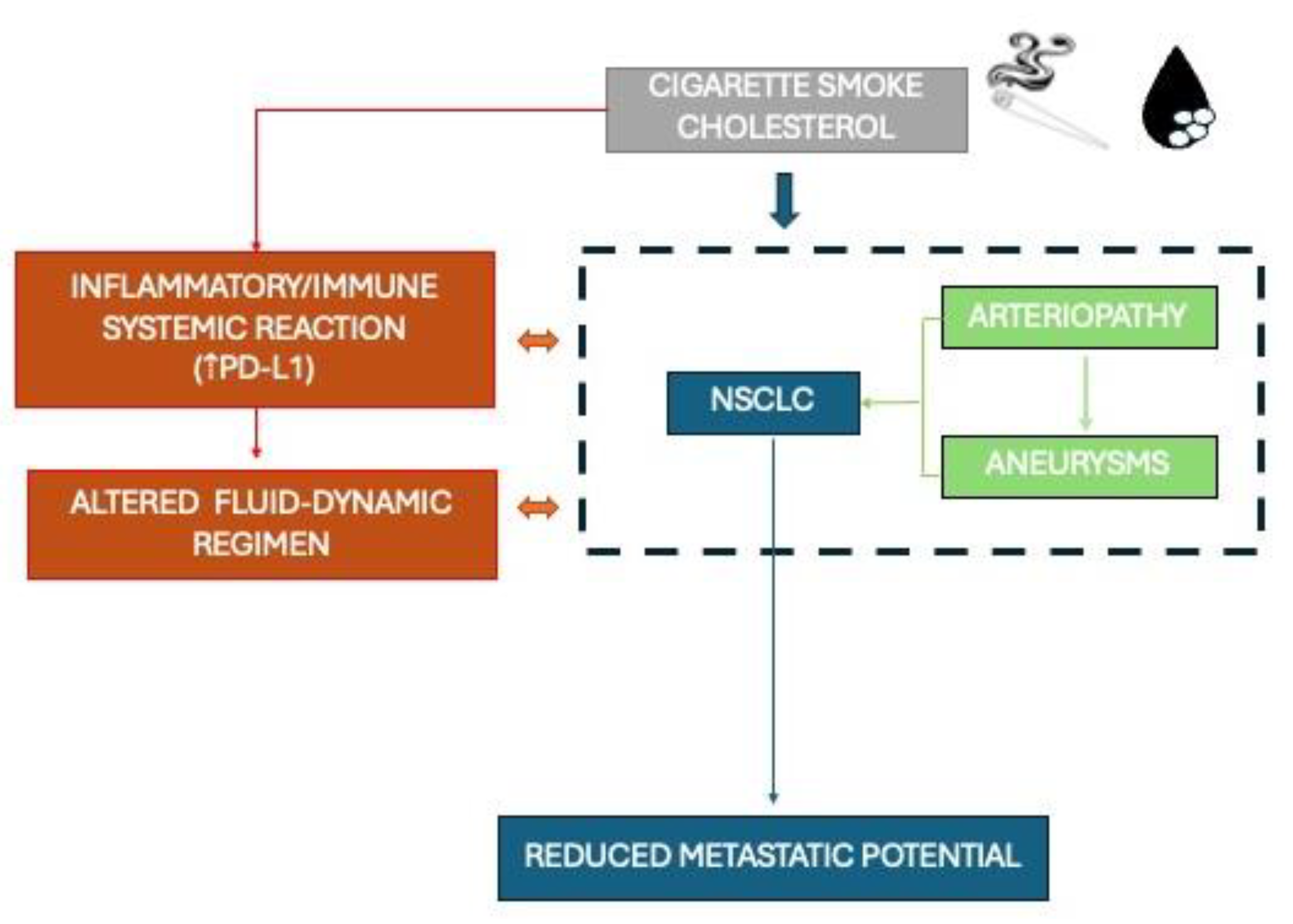
We here demonstrate that chronic periphery arterioathy disease (PAD) is implicated in modulating, and quite unespectedly impairing, the invasive behaviour of malignant cells by altering blood rheology and sustaining the pathologic immune-inflammatory reaction (Figure 5). Although being a retrospective study, the initial hypothesis according to which inflammation is associated to malignat invasive phenotype is not confirmed by the results of this work based on both theoric and statistical approaches. The mathematical model identified here pointed out blood viscosity as the most crucial variable in determing tumor spreading based on a formula which links cancer-related hypercoagulability and altered rheology and vortexes. The first implicaton of this model is to focus on the role of antiaggregant drugs in cancer patienst also affected by PAD [75,76,77,78]. Viscosity, in the cohort analysed, is not influenced by platelets which are normally represented, but possibly reflects the peculiar inflammatory status which characterizes this complex conditions. Indeed, when available, it should be possible to show that tumors express significantly high levels of PD-L1, whereas biochemical inflammatory markers (reactive protein C), total cholesterol, HDL, LDL and the LDL/HDL ratio weren’t risen as usually expected [79,80,81]. It is coincevable that chronic exposure to cigarette smoke should modulate the tumor and systemic microenvironment. Smoking habit, matched with patient’s age and total cholesterol level, could potentially exert a protective effect on tumor metastatic potential (14 % observed vs 30% expected in lung cancer based on published data). Smoking exposure not always correspond to COPD diagnosis and it should be remarked that, in some instances, spirometry test was never performed and that consequently bronchodilation therapy was assessed only in limited fraction of cases. This is a critical point that limits the conclusion of this work since the role of triple therapy against COPD is worth to be taken under consideration in this atypical immune-inflammatory cancer context. Finally, within the limits of the patients series analysed, cancer anssociated with PAD is clearly a gender-related disease with a substantial prevalence of males, mainly affecting the 7th decade of life.
5. Conclusions
Although being a retrospective analysis, the most relevant conclusion of this study is that tumors aroused in a context of pherypheral arteriopathy and aneurysmal disease featured a reduced metastatic potential if compared to a general cancer population. This condition is specifically modulated by blood viscosity, based on patient’s age, smoking habit and cholesterol and emerges as a male-clustered pathologic entity. The preliminary findings of this study support a strong rationale to a deepest investigation of the role of antiaggregants and inhaled steroids in modulating viscosity on one hand and immune-inflammatory tumor microenvironment on the other, as therapeutic treshold should be revised also in the light of their effects on cancer cell sprading capacity. Moreover, this approach will pave the way to simulation study of trans-vascular fate of drug-loaded/engineered nanoparticles in pathologic and more accurate settings.
Support Statement
Ricerca corrente 5x1000-2020 (cod. 090000X121—progetto 08050122) to G.M. Stella.
Conflicts of Interest
The authors have nothing to disclose.
References
- Xie S, Wu Z, Qi Y, Wu B, Zhu X. The metastasizing mechanisms of lung cancer: Recent advances and therapeutic challenges. Biomed Pharmacother. 2021, 138, 111450. [Google Scholar] [CrossRef]
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021, 398, 535–554. [Google Scholar] [CrossRef] [PubMed]
- Xie T, Qiu BM, Luo J, Diao YF, Hu LW, Liu XL, Shen Y. Distant metastasis patterns among lung cancer subtypes and impact of primary tumor resection on survival in metastatic lung cancer using SEER database. Sci Rep. 2024, 14, 22445. [Google Scholar] [CrossRef]
- Fu F, Chen Z, Chen H. Treating lung cancer: defining surgical curative time window. Cell Res. 2023, 33, 649–650. [Google Scholar] [CrossRef]
- La’ah AS, Chiou SH. Cutting-Edge Therapies for Lung Cancer. Cells. 2024, 13, 436. [Google Scholar] [CrossRef]
- Lin SD, Tong CY, Huang DD, Rossi A, Adachi H, Miao M, Zheng WX, Guo J. The time-to-surgery interval and its effect on pathological response after neoadjuvant chemoimmunotherapy in non-small cell lung cancer: a retrospective cohort study. Transl Lung Cancer Res. 2024, 13, 2761–2772. [Google Scholar] [CrossRef]
- Stella GM, Kolling S, Benvenuti S, Bortolotto C. Lung-Seeking Metastases. Cancers (Basel). 2019, 11, 1010. [Google Scholar] [CrossRef]
- Lundin A, Driscoll B. Lung cancer stem cells: progress and prospects. Cancer Lett. 2013, 338, 89–93. [Google Scholar] [CrossRef]
- Chu X, Tian W, Ning J, Xiao G, Zhou Y, Wang Z, Zhai Z, Tanzhu G, Yang J, Zhou R. Cancer stem cells: advances in knowledge and implications for cancer therapy. Signal Transduct Target Ther. 2024, 9, 170. [Google Scholar] [CrossRef]
- Zhou Q, Zu L, Li L, Chen X, Chen X, Li Y, Liu H, Sun Z. [Screening and establishment of human lung cancer cell lines with organ-specific metastasis potential]. Zhongguo Fei Ai Za Zhi. 2014, 17, 175–182. [Google Scholar] [CrossRef]
- Nguyen DX, Massagué J. Genetic determinants of cancer metastasis. Nat Rev Genet. 2007, 8, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Patel SA, Rodrigues P, Wesolowski L, Vanharanta S. Genomic control of metastasis. Br J Cancer. 2021, 124, 3–12. [Google Scholar] [CrossRef]
- Fares J, Fares MY, Khachfe HH, Salhab HA, Fares Y. Molecular principles of metastasis: a hallmark of cancer revisited. Signal Transduct Target Ther. 2020, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Lusby R, Demirdizen E, Inayatullah M, Kundu P, Maiques O, Zhang Z, Terp MG, Sanz-Moreno V, Tiwari VK. Pan-cancer drivers of metastasis. Mol Cancer. 2025, 24, 2. [Google Scholar] [CrossRef]
- Guo B, Li D, Du L, Zhu X. piRNAs: biogenesis and their potential roles in cancer. Cancer Metastasis Rev. 2020, 39, 567–575. [Google Scholar] [CrossRef]
- Xie S, Wu Z, Qi Y, Wu B, Zhu X. The metastasizing mechanisms of lung cancer: Recent advances and therapeutic challenges. Biomed Pharmacother. 2021, 138, 111450. [Google Scholar] [CrossRef]
- Minervini G, Pennuto M, Tosatto SCE. The pVHL neglected functions, a tale of hypoxia-dependent and -independent regulations in cancer. Open Biol. 2020, 10, 200109. [Google Scholar] [CrossRef]
- Godet I, Shin YJ, Ju JA, Ye IC, Wang G, Gilkes DM. Fate-mapping post-hypoxic tumor cells reveals a ROS-resistant phenotype that promotes metastasis. Nat Commun. 2019, 10, 4862. [Google Scholar] [CrossRef]
- Jiang C, Zhang N, Hu X, Wang H. Tumor-associated exosomes promote lung cancer metastasis through multiple mechanisms. Mol Cancer. 2021, 20, 117. [Google Scholar] [CrossRef]
- Mathieu M, Martin-Jaular L, Lavieu G, Théry C. Specificities of secretion and uptake of exosomes and other extracellular vesicles for cell-to-cell communication. Nat Cell Biol. 2019, 21, 9–17. [Google Scholar] [CrossRef]
- Wang L, Cao L, Wang H, Liu B, Zhang Q, Meng Z, Wu X, Zhou Q, Xu K. Cancer-associated fibroblasts enhance metastatic potential of lung cancer cells through IL-6/STAT3 signaling pathway. Oncotarget. 2017, 8, 76116–76128. [Google Scholar] [CrossRef]
- Li R, Ong SL, Tran LM, Jing Z, Liu B, Park SJ, Huang ZL, Walser TC, Heinrich EL, Lee G, Salehi-Rad R, Crosson WP, Pagano PC, Paul MK, Xu S, Herschman H, Krysan K, Dubinett S. Chronic IL-1β-induced inflammation regulates epithelial-to-mesenchymal transition memory phenotypes via epigenetic modifications in non-small cell lung cancer. Sci Rep. 2020, 10, 377, Erratum in: Sci Rep. 2020 Mar 4;10(1):4386. [Google Scholar] [CrossRef] [PubMed]
- Fan J, Xu G, Chang Z, Zhu L, Yao J. miR-210 transferred by lung cancer cell-derived exosomes may act as proangiogenic factor in cancer-associated fibroblasts by modulating JAK2/STAT3 pathway. Clin Sci (Lond). 2020, 134, 807–825, . Erratum in: Clin Sci (Lond). 2020, 134, 1801-1804. 10.1042/CS-20200039_COR. [CrossRef]
- Guo X, Zhu X, Zhao L, Li X, Cheng D, Feng K. Tumor-associated calcium signal transducer 2 regulates neovascularization of non-small-cell lung cancer via activating ERK1/2 signaling pathway. Tumour Biol. 2017, 39, 1010428317694324. [Google Scholar] [CrossRef]
- Thaxton C, Kano M, Mendes-Pinto D, Navarro TP, Nishibe T, Dardik A. Implications of preoperative arterial stiffness for patients treated with endovascular repair of abdominal aortic aneurysms. JVS Vasc Sci. 2024, 5, 100209. [Google Scholar] [CrossRef] [PubMed]
- Costa D, Andreucci M, Ielapi N, Serraino GF, Mastroroberto P, Bracale UM, Serra R. Vascular Biology of Arterial Aneurysms. Ann Vasc Surg. 2023, 94, 378–389. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen JJM, Meijer M, de Vries FBG, Reijnen MMPJ, Holewijn S, Thijssen DHJ. A systematic review summarizing local vascular characteristics of aneurysm wall to predict for progression and rupture risk of abdominal aortic aneurysms. J Vasc Surg. 2023, 77, 288–298.e2. [Google Scholar] [CrossRef] [PubMed]
- Signal Transduction and Targeted Therapy 2023, 8, 55. 8. [CrossRef]
- Thaxton C, Kano M, Mendes-Pinto D, Navarro TP, Nishibe T, Dardik A. Implications of preoperative arterial stiffness for patients treated with endovascular repair of abdominal aortic aneurysms. JVS Vasc Sci. 2024, 5, 100209. [Google Scholar] [CrossRef]
- Danaei G, Vander Hoorn S, Lopez AD, Murray CJ, Ezzati M. Causes of cancer in the world: comparative risk assessment of nine behavioural and environmental risk factors. Lancet 2005, 366, 1784–1793. [Google Scholar] [CrossRef]
- Crispo A, Brennan P, Jöckel KH, Schaffrath-Rosario A, Wichmann HE, Nyberg F, Simonato L, Merletti F, Forastiere F, Boffetta P, Darby S. The cumulative risk of lung cancer among current, ex- and never-smokers in European men. Br J Cancer. 2004, 91, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Asomaning K, Miller DP, Liu G, Wain JC, Lynch TJ, Su L, Christiani DC. Second hand smoke, age of exposure and lung cancer risk. Lung Cancer. 2008, 61, 13–20. [Google Scholar] [CrossRef]
- Moorthy B, Chu C, Carlin DJ. Polycyclic aromatic hydrocarbons: from metabolism to lung cancer. Toxicol Sci. 2015, 145, 5–15. [Google Scholar] [CrossRef]
- oldman R, Enewold L, Pellizzari E, Beach JB, Bowman ED, Krishnan SS, Shields PG. Smoking increases carcinogenic polycyclic aromatic hydrocarbons in human lung tissue. Cancer Res. 2001, 61, 6367–6371. [Google Scholar]
- Martey CA, Baglole CJ, Gasiewicz TA, Sime PJ, Phipps RP. The aryl hydrocarbon receptor is a regulator of cigarette smoke induction of the cyclooxygenase and prostaglandin pathways in human lung fibroblasts. Am J Physiol Lung Cell Mol Physiol. 2005, 289, L391–L399. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta P, Rizwani W, Pillai S, Kinkade R, Kovacs M, Rastogi S, Banerjee S, Carless M, Kim E, Coppola D, Haura E, Chellappan S. Nicotine induces cell proliferation, invasion and epithelial-mesenchymal transition in a variety of human cancer cell lines. Int J Cancer. 2009, 124, 36–45. [Google Scholar] [CrossRef]
- Lindholt J, Jorgensen B, Shi G-P, Henneberg EW. Relationships between activators and inhibitors of plasminogen, and the progression of small abdominal aortic aneurysms. Eur J Vasc Endovas Surg. 2003, 25, 546–551. [Google Scholar] [CrossRef]
- Krishna SM, Dear AE, Norman PE, Golledge J. Genetic and epigenetic mechanisms and their possible role in abdominal aortic aneurysm. Atherosclerosis. 2010, 212, 16–29. [Google Scholar] [CrossRef]
- Lee AJ, Fowkes FG, Carson MN, Leng GC, Allan PL. Smoking, atherosclerosis and risk of abdominal aortic aneurysm. Eur Heart J. 1997, 18, 671–676. [Google Scholar] [CrossRef]
- Peng Z, Qiu P, Guo H, Zhu C, Zheng J, Pu H, Liu Y, Wei W, Li C, Yang X, Ye K, Wang R, Lu X, Zhou Z. Association between high-density lipoprotein cholesterol and risk of abdominal aortic aneurysm among males and females aged 60 years and over. J Vasc Surg. 2025, 81, 894–904.e6. [Google Scholar] [CrossRef]
- Hobbs SD, Claridge MW, Quick CR, Day NE, Bradbury AW, Wilmink AB. LDL cholesterol is associated with small abdominal aortic aneurysms. Eur J Vasc Endovasc Surg. 2003, 26, 618–622. [Google Scholar] [CrossRef]
- Weng LC, Roetker NS, Lutsey PL, Alonso A, Guan W, Pankow JS, Folsom AR, Steffen LM, Pankratz N, Tang W. Evaluation of the relationship between plasma lipids and abdominal aortic aneurysm: A Mendelian randomization study. PLoS One. 2018, 13, e0195719. [Google Scholar] [CrossRef]
- Sun P, Zhang L, Gu Y, Wei S, Wang Z, Li M, Wang W, Wang Z, Bai H. Immune checkpoint programmed death-1 mediates abdominal aortic aneurysm and pseudoaneurysm progression. Biomed Pharmacother. 2021, 142, 111955. [Google Scholar] [CrossRef]
- Bai H, Wang Z, Li M, Sun P, Wei S, Wang W, Wang Z, Xing Y, Li J, Dardik A. Inhibition of programmed death-1 decreases neointimal hyperplasia after patch angioplasty. J Biomed Mater Res B Appl Biomater. 2021, 109, 269–278. [Google Scholar] [CrossRef]
- Sun P, Zhang L, Gu Y, Wei S, Wang Z, Li M, Wang W, Wang Z, Bai H. Immune checkpoint programmed death-1 mediates abdominal aortic aneurysm and pseudoaneurysm progression. Biomed Pharmacother. 2021, 142, 111955. [Google Scholar] [CrossRef]
- Márquez-Sánchez AC, Koltsova EK. Immune and inflammatory mechanisms of abdominal aortic aneurysm. Front Immunol. 2022, 13, 989933. [Google Scholar] [CrossRef]
- D’Arienzo MP, Rarità L. Dynamics of Blood Flows in the Cardiocirculatory System. Computation. 2024, 12, 194. [Google Scholar] [CrossRef]
- Numata S, Itatani K, Kanda K, Doi K, Yamazaki S, Morimoto K, Manabe K, Ikemoto K, Yaku H. Blood flow analysis of the aortic arch using computational fluid dynamics. Eur J Cardiothorac Surg. 2016, 49, 1578–1585. [Google Scholar] [CrossRef]
- Lynch S, Nama N, Figueroa CA. Effects of non-Newtonian viscosity on arterial and venous flow and transport. Sci Rep. 2022, 12, 20568. [Google Scholar] [CrossRef]
- Han JW, Sung PS, Jang JW, Choi JY, Yoon SK. Whole blood viscosity is associated with extrahepatic metastases and survival in patients with hepatocellular carcinoma. PLoS One. 2021, 16, e0260311. [Google Scholar] [CrossRef]
- Khan, M. M. , Puniyani, R. R., Huilgol, N. G., Hussain, M. A., & Ranade, G. G. Hemorheological profiles in cancer patients. Clinical Hemorheology and Microcirculation 1995, 15, 37–44. [Google Scholar]
- Hu, De-en, Jing-chao Ruan, and Pei-qing Wang. “Hemorheological changes in cancer.” Clinical Hemorheology and Microcirculation 8.6 (1988): 945-956.
- Dintenfass, L. Haemorheology of cancer metastases: An example of malignant melanoma. Survival times and abnormality of blood viscosity factors 1. Clin Hemorheol Micro. 1982, 2, 259–271. [Google Scholar]
- Wirtz D, Konstantopoulos K, Searson PC. The physics of cancer: the role of physical interactions and mechanical forces in metastasis. Nature Reviews Cancer. 2011, 11, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Follain G, Herrmann D, Harlepp S, Hyenne V, Osmani N, Warren SC, et al. Fluids and their mechanics in tumour transit: shaping metastasis. Nature Reviews Cancer. 2020, 20, 107–124. [Google Scholar] [CrossRef] [PubMed]
- von Tempelhoff GF, Heilmann L, Hommel G, Pollow K. Impact of rheological variables in cancer. Semin Thromb Hemost. 2003, 29, 499–513. [Google Scholar] [CrossRef]
- Helwa R, Heller A, Knappskog S, Bauer AS. Tumor cells interact with red blood cells via galectin-4 - a short report. Cell Oncol (Dordr). 2017, 40, 401–409. [Google Scholar] [CrossRef]
- Wiewiora M, Jopek J, Świętochowska E, Sławomir G, Piecuch J, Gąska M, Piecuch J. Blood-based protein biomarkers and red blood cell aggregation in pancreatic cancer. Clin Hemorheol Microcirc. 2023, 85, 371–383. [Google Scholar] [CrossRef]
- von Tempelhoff GF, Nieman F, Heilmann L, Hommel G. Association between blood rheology, thrombosis and cancer survival in patients with gynecologic malignancy. Clin Hemorheol Micro. 2000, 22, 107–130. [Google Scholar] [PubMed]
- Font-Clos F, Zapperi S, La Porta CAM. Blood Flow Contributions to Cancer Metastasis. iScience. 2020, 23, 101073. [Google Scholar] [CrossRef]
- Cancer cells move and spread faster in thicker extracellular fluids. Nature. 2022. [CrossRef]
- Bera K, Kiepas A, Godet I, Li Y, Mehta P, Ifemembi B, Paul CD, Sen A, Serra SA, Stoletov K, Tao J, Shatkin G, Lee SJ, Zhang Y, Boen A, Mistriotis P, Gilkes DM, Lewis JD, Fan CM, Feinberg AP, Valverde MA, Sun SX, Konstantopoulos K. Extracellular fluid viscosity enhances cell migration and cancer dissemination. Nature. 2022, 611, 365–373. [Google Scholar] [CrossRef]
- Boccaccio C, Comoglio PM. Genetic link between cancer and thrombosis. J Clin Oncol. 2009, 27, 4827–4833. [Google Scholar] [CrossRef]
- Boccaccio C, Sabatino G, Medico E, Girolami F, Follenzi A, Reato G, Sottile A, Naldini L, Comoglio PM. The MET oncogene drives a genetic programme linking cancer to haemostasis. Nature. 2005, 434, 396–400. [Google Scholar] [CrossRef]
- Li R, Ren M, Chen N, Luo M, Deng X, Xia J, Yu G, Liu J, He B, Zhang X, Zhang Z, Zhang X, Ran B, Wu J. Presence of intratumoral platelets is associated with tumor vessel structure and metastasis. BMC Cancer. 2014, 14, 167. [Google Scholar] [CrossRef]
- Stella GM, Benvenuti S, Gentile A, Comoglio PM. MET Activation and Physical Dynamics of the Metastatic Process: The Paradigm of Cancers of Unknown Primary Origin. EBioMedicine. 2017, 24, 34–42. [Google Scholar] [CrossRef]
- Saldana M, Gallegos S, Gálvez E, Castillo J, Salinas-Rodríguez E, Cerecedo-Sáenz E, Hernández-Ávila J, Navarra A, Toro N. The Reynolds Number: A Journey from Its Origin to Modern Applications. Fluids. 2024, 9, 299. [Google Scholar] [CrossRef]
- Coclite A, Coclite GM, De Tommasi D. Capsules Rheology in Carreau-Yasuda Fluids. Nanomaterials (Basel). 2020, 10, 2190. [Google Scholar] [CrossRef]
- Chen J, Lu XY. Numerical investigation of the non-Newtonian pulsatile blood flow in a bifurcation model with a non-planar branch. J Biomech. 2006, 39, 818–832. [Google Scholar] [CrossRef]
- Wang QQ, Ping BH, Xu QB, Wang W. Rheological effects of blood in a nonplanar distal end-to-side anastomosis. J Biomech Eng. 2008, 130, 051009. [Google Scholar] [CrossRef]
- Bera K, Kiepas A, Godet I, Li Y, Mehta P, Ifemembi B, Paul CD, Sen A, Serra SA, Stoletov K, Tao J, Shatkin G, Lee SJ, Zhang Y, Boen A, Mistriotis P, Gilkes DM, Lewis JD, Fan CM, Feinberg AP, Valverde MA, Sun SX, Konstantopoulos K. Extracellular fluid viscosity enhances cell migration and cancer dissemination. Nature. 2022, 611, 365–373. [Google Scholar] [CrossRef]
- Gomaa A, Gamal Y, Abdelmagied MM. Enhancement of thermofluid characteristics via a triple-helical tube heat exchanger. Sci Rep. 2025, 15, 6978. [Google Scholar] [CrossRef]
- Rajah G, Narayanan S, Rangel-Castilla L. Update on flow diverters for the endovascular management of cerebral aneurysms. Neurosurg Focus. 2017, E2. [Google Scholar] [CrossRef]
- Tao DL, Tassi Yunga S, Williams CD, McCarty OJT. Aspirin and antiplatelet treatments in cancer. Blood. 2021, 137, 3201–3211. [Google Scholar] [CrossRef]
- Wang X, Zhao S, Wang Z, Gao T. Platelets involved tumor cell EMT during circulation: communications and interventions. Cell Commun Signal. 2022, 20, 82. [Google Scholar] [CrossRef]
- Tavares V, Savva-Bordalo J, Rei M, Liz-Pimenta J, Assis J, Pereira D, Medeiros R. Haemostatic Gene Expression in Cancer-Related Immunothrombosis: Contribution for Venous Thromboembolism and Ovarian Tumour Behaviour. Cancers (Basel). 2024, 16, 2356. [Google Scholar] [CrossRef]
- Garcia-Leon MJ, Liboni C, Mittelheisser V, Bochler L, Follain G, Mouriaux C, Busnelli I, Larnicol A, Colin F, Peralta M, Osmani N, Gensbittel V, Bourdon C, Samaniego R, Pichot A, Paul N, Molitor A, Carapito R, Jandrot-Perrus M, Lefebvre O, Mangin PH, Goetz JG. Platelets favor the outgrowth of established metastases. Nat Commun. 2024, 15, 3297. [Google Scholar] [CrossRef]
- Potempa LA, Rajab IM, Olson ME, Hart PC. C-Reactive Protein and Cancer: Interpreting the Differential Bioactivities of Its Pentameric and Monomeric, Modified Isoforms. Front Immunol. 2021, 12, 744129. [Google Scholar] [CrossRef]
- Hart PC, Rajab IM, Alebraheem M, Potempa LA. C-Reactive Protein and Cancer-Diagnostic and Therapeutic Insights. Front Immunol. 2020, 11, 595835. [Google Scholar] [CrossRef]
- Sun T, Chen M, Shen H, PingYin, Fan L, Chen X, Wu J, Xu Z, Zhang J. Predictive value of LDL/HDL ratio in coronary atherosclerotic heart disease. BMC Cardiovasc Disord. 2022, 22, 273. [Google Scholar] [CrossRef]
Figure 1.
The formula describing the invasive pattern of cancer relies on a rheologic parameter, namely blood viscosity which, in malignant setting, isaltered independently from the fluid regimen and also impact locally on rotating vortexes.
Figure 1.
The formula describing the invasive pattern of cancer relies on a rheologic parameter, namely blood viscosity which, in malignant setting, isaltered independently from the fluid regimen and also impact locally on rotating vortexes.
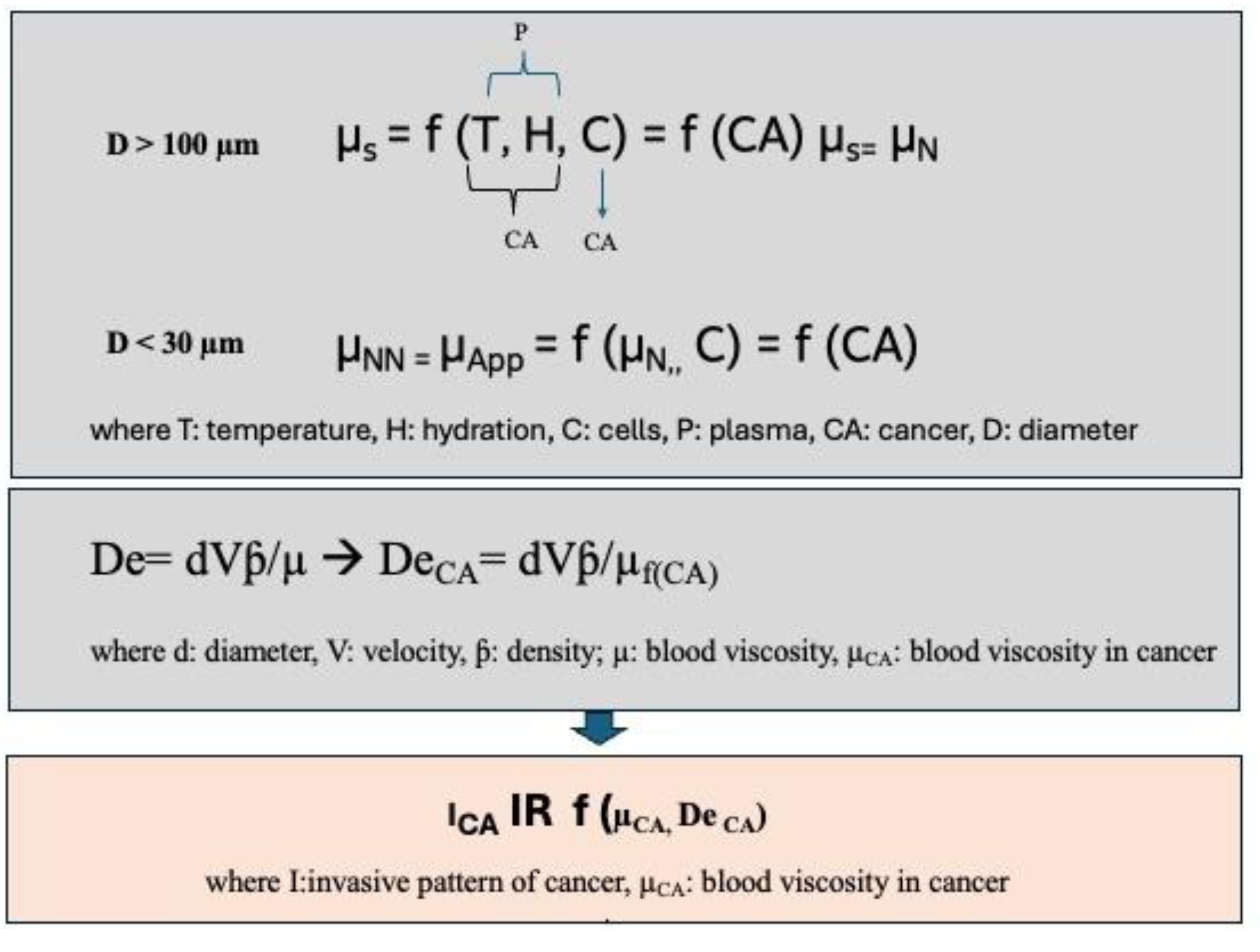
Figure 2.
Detail of the population enrolled. A-C) Primary site of cancer origin, histotype and stage (TNM 8 ed) of the cases evaluated; D-E) detail on arteriopathy and surgical approach; D) data on metastatic sites and PDL1expression referred to NSCLC. MM: multiple myeloma, NHL: non-Hodgking Lymphoma, CRC: colorectal cancer, MPM: malignant pleural mesothelioma, HNCAR: head and neck carcinoma, uro-CARC:urothelial carcinoma; PADC: pancreatic adenocarcinoma; RCC: renal cell carcinoma; Ductal: ductal breast cancer; CADC: cervical adenocarcinoma; mel: melanoma; IAAA: inflammatory intra-addominal aneurysm; CAR: carotid disease; PAD: peripheral artery disease; TAAA: thoracic abminal aneurysm; TPAU: penetrating thoracic aortic ulcer; SA: splenic artery aneurysm; CIA: common iliac arteriopathy; DTAA: descending thoracic aortic aneurysm; EVAR: endovascular repair surgery;TEVAR: thoracic aortic endovascular repair surgery; OVAS: open vascular surgery.
Figure 2.
Detail of the population enrolled. A-C) Primary site of cancer origin, histotype and stage (TNM 8 ed) of the cases evaluated; D-E) detail on arteriopathy and surgical approach; D) data on metastatic sites and PDL1expression referred to NSCLC. MM: multiple myeloma, NHL: non-Hodgking Lymphoma, CRC: colorectal cancer, MPM: malignant pleural mesothelioma, HNCAR: head and neck carcinoma, uro-CARC:urothelial carcinoma; PADC: pancreatic adenocarcinoma; RCC: renal cell carcinoma; Ductal: ductal breast cancer; CADC: cervical adenocarcinoma; mel: melanoma; IAAA: inflammatory intra-addominal aneurysm; CAR: carotid disease; PAD: peripheral artery disease; TAAA: thoracic abminal aneurysm; TPAU: penetrating thoracic aortic ulcer; SA: splenic artery aneurysm; CIA: common iliac arteriopathy; DTAA: descending thoracic aortic aneurysm; EVAR: endovascular repair surgery;TEVAR: thoracic aortic endovascular repair surgery; OVAS: open vascular surgery.
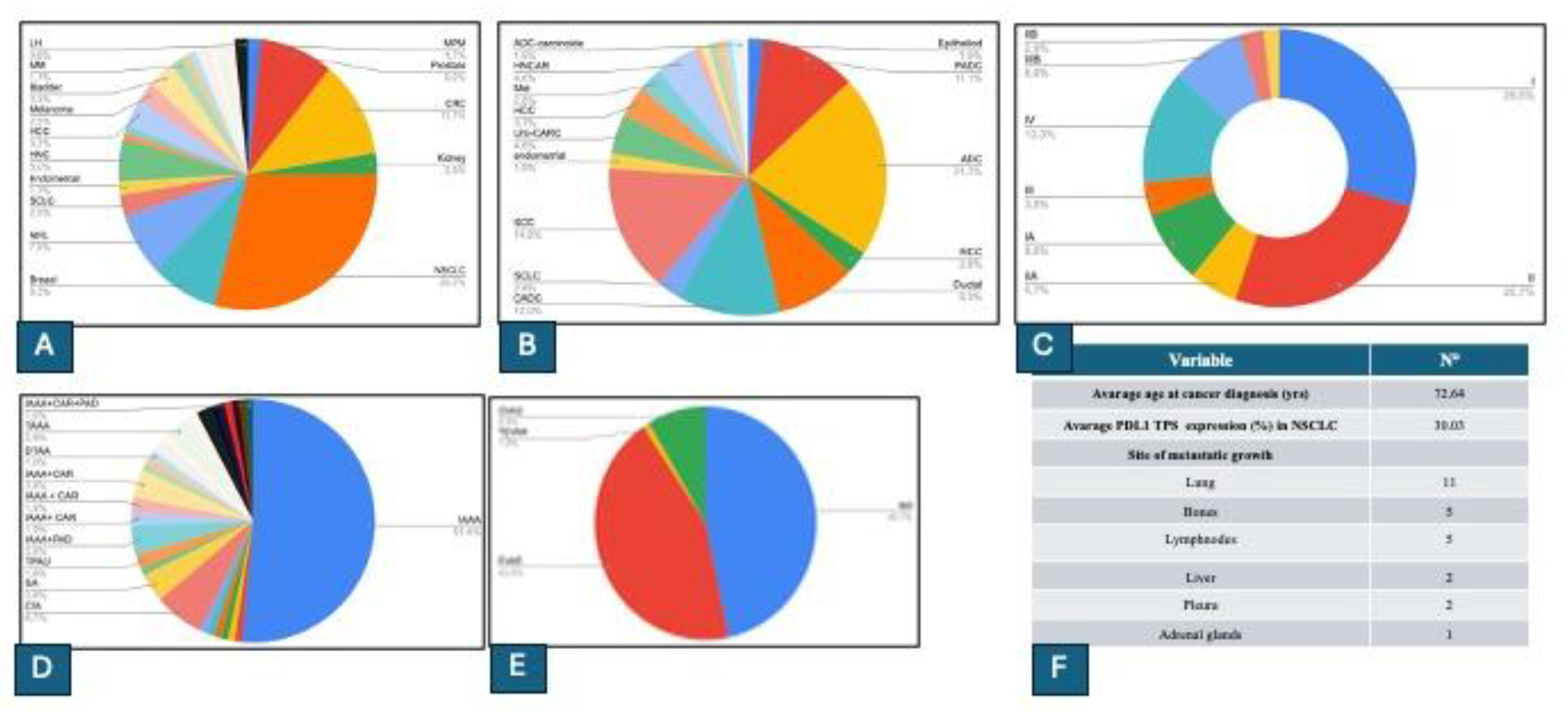
Figure 3.
Study design and demographic, clinical and biochemical features of the population evaluated.
Figure 3.
Study design and demographic, clinical and biochemical features of the population evaluated.
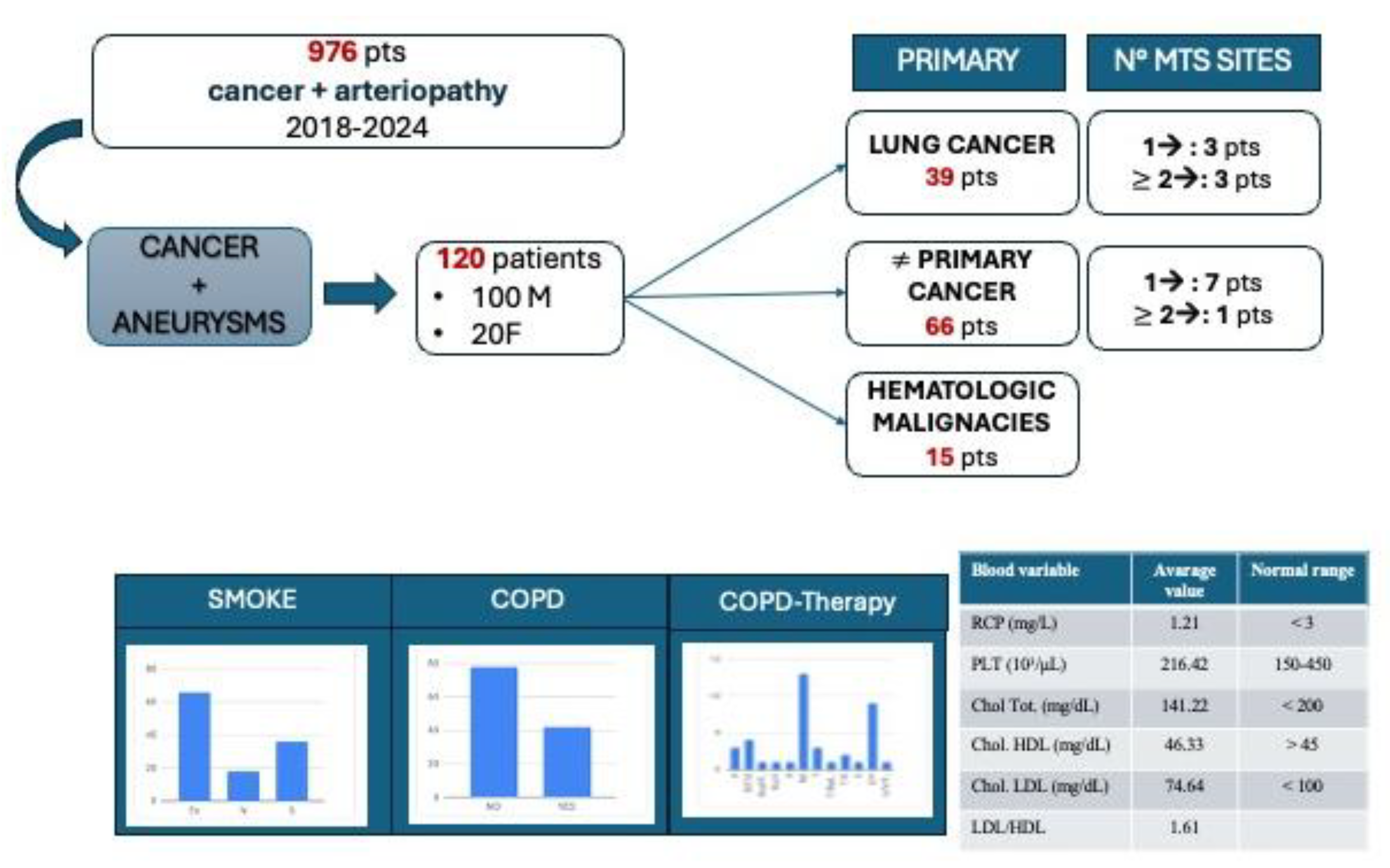
Figure 4.
Results from partition analysis applied to the whole dataset. A). Partion analysis for metastastic dissemination (excluded gender and smoke, unselected by arteriopathy) pointing out that the most relevant predictors are the patient’s age at cancer diagnosis, the level of total cholesterol and the primary tissue/organ of origin. B) Predictors screeing underlines that arteriopathy is the most relevant variable associated to outcome ( number of metastases/stage). C) Partion analysis for metastastic dissemination including data on arteriopathy and confirming that arterial disease is the first split, followed by platelet level.
Figure 4.
Results from partition analysis applied to the whole dataset. A). Partion analysis for metastastic dissemination (excluded gender and smoke, unselected by arteriopathy) pointing out that the most relevant predictors are the patient’s age at cancer diagnosis, the level of total cholesterol and the primary tissue/organ of origin. B) Predictors screeing underlines that arteriopathy is the most relevant variable associated to outcome ( number of metastases/stage). C) Partion analysis for metastastic dissemination including data on arteriopathy and confirming that arterial disease is the first split, followed by platelet level.

Figure 5.
Pathogenic mechanism of NSCLC progression in case of PAD.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



