Submitted:
17 June 2025
Posted:
18 June 2025
You are already at the latest version
Abstract
Background: The suitability of minimally invasive adrenalectomy (MIA) for adrenal tumors ≥6 cm remains debated due to technical challenges and oncological concerns. This study aimed to assess the safety and feasibility of MIA for large adrenal tumors by comparing surgical outcomes with smaller tumors. Methods: This retrospective cohort study included 269 patients who underwent MIA (2013–2023), divided into two groups: Group A (< 6 cm, n=197) and Group B (≥6 cm, n=72). The primary endpoint was the postoperative complication rate; secondary endpoints included conversion to open surgery and postoperative length of stay (LOS). Results: Multivariate analysis identified no factors associated with postoperative complications, whereas tumor size ≥6 cm was associated with conversion to open surgery (p=0.031). Bilateral procedures and a higher Charlson comorbidity index were associated with longer LOS (p< 0.001 and p=0.015, respectively). Conclusion: MIA is a safe and feasible approach for tumors ≥6 cm, despite being associated with a higher conversion rate.
Keywords:
adrenalectomy
; laparoscopic adrenalectomy
; retroperitoneoscopic
; large adrenal tumors
; surgical outcomes
Introduction
Currently, laparoscopic adrenalectomy (LA) is recognized as the standard treatment for small adrenal tumors, following its introduction by Gagner et al. [1] and Higashihara et al. [2] in 1992. The advantages of LA compared to open adrenalectomy include reduced postoperative pain, shorter hospital stays, and superior cosmetic outcomes [3,4,5,6,7,8,9,10].
The suitability of minimally invasive adrenalectomy (MIA) for large adrenal tumors remains a subject of ongoing debate in the literature [11,12,13,14,15], primarily due to technical difficulties and oncological considerations. Nonetheless, some authors argue that tumor size alone should not constitute an absolute contraindication for a minimally invasive approach [10,13].
There is no clear definition of the size of a large adrenal tumor [13]. However, the European Society of Endocrinology Clinical Practice Guidelines recommends laparoscopic surgery for adrenal tumors smaller than 6 cm without local invasion, while advocating an individualized surgical strategy for tumors exceeding 6 cm [16].
This study aims to compare the surgical outcomes of patients undergoing MIA for tumors ≥ 6 cm in size with those for tumors < 6 cm.
Material and Methods
Study Design and Population
This retrospective cohort study included all consecutive patients who underwent MIA at our Institution from January 2013 to December 2023. Patients who underwent open adrenalectomy have been excluded. A prospectively designed database was used for data collection and analysis. Patients were divided into two groups based on the tumor size: Group A included patients with tumor < 6 cm, while Group B included patients with tumor ≥ 6 cm. A flowchart of enrolled patients is described in Figure 1.
Demographics and baseline patients’ characteristics included age, body mass index (BMI), gender, presence of comorbidities, prior abdominal surgery, hormonal hypersecretion, Charlson comorbidity index [17], American Society of Anesthesiologists (ASA) score [18], tumor location, surgical approach, associated surgeries, underlying genetic conditions, tumor size (in case of bilateral surgery, the largest diameter was considered), and histologic diagnosis. For analysis, histologic diagnoses were categorized into: cortical adenoma and cortical cyst, pheochromocytoma, myelolipoma, adrenal malignancies (including adrenal cortical carcinoma, angiosarcoma, and adrenal metastases), and others (including lymphoma, ganglioneuroma, angiomyolipoma, hemangioma, lymphangioma, and fibrous solitary tumor).
Moreover, we collected data regarding operative time (defined from the skin incision to the skin closure), conversion to open, reason for conversion, intraoperative complications, blood transfusion, postoperative length of hospital stay (defined as the days from the surgical operation to the discharge; LOS), postoperative complication rate, Clavien-Dindo Classification [19], Comprehensive Complication Index (CCI) [20], readmission at 30 days, mortality. The manuscript has been structured according to the Strengthening The Report Of Cohort Studies in Surgery (STROCCS) 2024 guideline [21].
The primary endpoint of this study was the rate of postoperative complications. Secondary endpoints were the conversion rate and the LOS.
This study has been approved by the Internal Review Board (IRB) (IRB code: 27924).
Statistical Analysis
Continuous quantitative data were expressed as mean ± standard deviation (SD) and compared using Student’s t test or Mann-Whitney test, when appropriate. Categorical qualitative data were expressed as numbers and percentages and compared using the χ² test (or Fisher’s exact test, when appropriate). Logistic and linear regression analyses were used to identify factors independently associated with postoperative complications, conversion to open surgery, and LOS. For linear and logistic regression modeling, tumor location was coded as a binary variable, with categories “unilateral” and “bilateral”. Factors with p-value < 0.10 at univariate analysis were included in multivariate analysis models. Multivariable analyses were presented as odds ratios (OR), when appropriate, coefficients, and p-value (95% confidence interval; CI).
All analyses were carried out with SPSS v.28 (IBM Corp., Armonk, NY, USA).
Results
Characteristics of the Study Population
Overall, 269 patients have been enrolled; in particular, 197 (73.2%) were included in Group A, while 72 (26.8%) were included in Group B. At univariate analysis, no difference between Group A and Group B was documented in terms of age (52 ± 13.6 vs. 55.5 ± 13.5 years, respectively; p=0.058), BMI (27.6 ± 6.8 vs. 27.9 ± 6.7 Kg/m2, respectively; p=0.795), presence of comorbidities (91.4% vs. 93.1%, respectively; p=0.655), prior abdominal surgery (47.2% vs. 38.9%, respectively; p=0.224), tumor location (p=0.055), and underlying genetic mutation (6.1% vs. 9.7%, respectively; p=0.303). On the other hand, at univariate analysis a statistical significant difference was documented in terms of gender (p=0.018), Charlson comorbidity index (1.9 ± 1.8 vs. 2.4 ± 2.0, respectively; p=0.049), ASA score (p<0.001), hormonal hypersecretion (60.4% vs. 41.7%; p=0.006), surgical approach (p<0.001), histologic diagnosis (p<0.001), and tumor size (3.6 ± 1.3 vs. 7.6 ± 1.8 cm, respectively; p<0.001). These data are summarized in Table 1.
Intraoperative and Postoperative Outcomes
At univariate analysis no statistically significant difference was documented in terms of associated operations (11.7% vs. 9.7%, respectively; p=0.652), conversion to open surgery (2.5% vs. 8.3%; p=0.075), reason for conversion to open surgery (p=0.143), intra-operative complications (1% vs. 2.8%, respectively; p=0.646), blood transfusion (1% vs. 4.2%, respectively; p=0.236), need for postoperative ICU (53.8% vs. 58.3%, respectively; p=0.508), length of postoperative ICU stay (1 ± 0.2 vs. 1.1 ± 0.4 days, respectively; p=0.406), LOS (3.1 ± 1.7 vs. 3.5 ± 2.3 days, respectively; p=0.112), postoperative complications rate (9.6% vs. 11.1%, respectively; p=0.723), Clavien-Dindo classification (p=0.975), CCI (2 ± 6.7 vs. 2.1 ± 6.1, respectively; p=0.857), readmission at 30 days (2% vs. 1.4%, respectively; p=0.730). A statistically significant difference was documented in terms of operative times between Group A and Group B (97.8 vs. 120 min, respectively; p=0.002). These data are summarized in Table 2.
Diagnostic Workup and Oncological Outcomes of ACC Patients
In 6 (2.2%) patients, histological diagnosis reveals adrenal cortical carcinoma (ACC), 4 (2%) included in Group A and 2 (2.8%) in Group B. All patients underwent pre-operative CT scan, 2 (33.3%) of them also underwent MRI, and 1 (16.7%) also underwent MRI and PET scan. At pre-operative imaging, 5 (83.3%) cases presented regular margins without necrosis area, while 1 (16.7%) presented irregular margins with a heterogeneous intraparenchymal area consistent with necrosis. All cases presented without adjacent organs infiltration. ACC was incidentally identified through histological examination in all cases except one (16.7%), where a preoperative suspicion had already been raised due to high PET uptake and CT-scan features. The mean Hounsfield Unit of ACCs was 37. Three (50%) cases were non-functioning, whereas 2 (33%) exhibited cortisol hypersecretion and 1 (16.7%) demonstrated combined catecholamine and androgen hypersecretion. No capsular disruption was documented either intraoperatively or at histopathological examination. Moreover, an R0 resection was achieved in all cases.
Recurrence occurred in 2 (33.3%) patients, one per group, after a mean follow-up of 35 ± 21.1 months. The Group A ACC patient had recurrence in the retroperitoneum and ipsilateral kidney and is currently under treatment with mitotane with a good disease control; conversely, the Group B ACC patient had recurrence in the retroperitoneum, treated surgically, and thereafter in the liver, treated by cryoablation, and the disease is controlled at the last follow-up. The mean disease-free survival was 27 ± 14.8 months. No adrenal disease-related death occurred in the whole case series.
Multivariate Analyses
In logistic regression analysis, no factors were associated with postoperative complications (Table 3), while tumor size ≥ 6 cm was significantly associated with conversion to open surgery (p=0.031) (Table 4).
In linear regression analysis, Charlson comorbidity index and bilateral procedures were significantly associated with longer LOS (p=0.015 and <0.001, respectively) (Table 5).
Discussion
Although it is well-known that MIA represents the best surgical option for small adrenal tumors, its role for large adrenal lesions is historically considered a debated topic. Nonetheless, the cut-off of 6 cm is not based on good clinical evidence [16]. The primary challenge lies in the need for extensive tumor manipulation during surgery and difficulties in tumor handling. Furthermore, tumor size has traditionally been considered a critical factor in estimating malignancy, with the prevailing belief that malignant adrenal tumors are best managed through open surgery to reduce the risk of tumor spillage and capsule rupture [22,23]. However, these concerns have been progressively addressed over time. Advances in perioperative management, a deeper understanding of adrenal disease pathophysiology, and significant improvements in laparoscopic techniques, particularly those enhancing visualization and minimizing gland manipulation, have rendered tumor size no longer an absolute contraindication to laparoscopic surgery in appropriately selected patients [24,25,26].
In the present study, we reported our 10-year experience on 269 adrenalectomy patients treated with a minimally invasive approach. The two groups include a wide range of pre-operative diagnoses. Our results reveal comparable outcomes in terms of safety for adrenal tumors < or ≥ 6 cm, with no difference regarding intra- and post-operative complications. These findings demonstrate the reliability of minimally invasive surgery for approaching large adrenal masses in experienced hands.
Our results mirror previous published studies, which documented the safety of MIA regardless of tumor size when performed by skilled surgeons [25,27,28,29]. Conversely, some authors [26,30,31] documented a higher rate of post-operative complications for large adrenal tumors, although they reported that these are generally low and that 6 cm should not be considered the upper limit for performing MIA in high-volume Institutions.
Our study reveals that large adrenal tumors are associated with a higher rate of conversion to open surgery in multivariate analysis. This is likely due to difficulties in handling large adrenal masses and their higher likelihood of bleeding, but these issues can be considered regardless of the surgical approach [14,25]. Indeed, it is questionable to routinely refer large adrenal masses to open surgery since conventional adrenalectomy is not easier than MIA. Moreover, our conversion rate for large adrenal masses is relatively low (8.3%), and our findings are in line with previous studies (6.7 – 14.6%) [14,25,30]. Notably, 4 out of 6 conversions in Group B occurred for right-sided adrenal tumors: this may be due to the retrocaval growth of large adrenal masses, which may have made the dissection challenging.
Our study documented a longer operative time associated with adrenal lesions ≥ 6 cm, aligning with existing literature [14,25,30]. This is likely related to more demanding dissection of large adrenal masses, which may dislocate surrounding structures. Tiberio et al. reported a significant increase in intra-operative complications and hospital stay for adrenalectomies lasting more than 140 min [32]. However, the mean operative time in both groups is lower than the cut-off reported by Tiberio et al. [32], and we hypothesized that our difference in operative time between groups, although statistically significant, may be clinically negligible. Besides, it is noteworthy to underline that almost 10% of patients per group underwent associated operations along with adrenalectomy, prolonging the overall duration of the intervention.
We found that large adrenal masses are not associated with prolonged LOS, confirming previous findings [25,26,33]. Conversely, we documented that the Charlson comorbidity index and bilateral procedures are related to longer LOS. These findings are somewhat intuitive, as patients with greater comorbidities and those who experienced iatrogenic adrenal insufficiency are usually associated with longer hospitalization [31].
The major concern regarding minimally invasive treatment of adrenal lesions is related to the increasing risk of malignancy according to size. The NIH consensus statement reported that the rate of incidental adrenal cortical carcinoma is 2% for lesions smaller than 4 cm, 6% for tumors sized between 41 and 60 mm, and 25% for tumors larger than 6 cm [34]. Thus, there are controversies in handling large adrenal masses due to the fear of tumor capsule disruption and tumor spillage, leading to tumor recurrence. Nonetheless, these complications may occur even during open adrenalectomy; thus, the surgical approach should not be considered a contraindication, but is the surgeon’s skills determine the safety of the resection. Moreover, an accurate pre-operative workup may raise the suspicion of adrenal cortical carcinoma, either for the radiological characteristics of the tumor itself or for the presence of organ invasiveness or lymph node metastasis. Furthermore, intraoperative findings could guide the surgeons regarding the suspicion of a malignant lesion. Our study was not focused on the oncological safety of MIA for malignant adrenal lesions and its comparison with open adrenalectomy. Notwithstanding, since the incidence of ACC in Group B was less than 3%, opting for an open approach for all adrenal masses larger than 6 cm would preclude the vast majority of patients from the benefits of MIA, in particular, faster recovery, less estimated blood loss, and LOS [35]. However, in the present study, we described 6 ACCs, 4 with tumors sized < 6 cm and 2 sized ≥ 6 cm. All but one diagnoses were incidental, and surgery without capsule disruption led to an R0 resection in all cases. Nonetheless, recurrence occurs in 2 patients, one included in Group A (local relapse) and 1 in Group B (local relapse and liver metastasis). After a mean follow-up of 35 months, all patients are still alive. Besides, although the issue is still highly debated [22,23,36], Machado et al. reported in a systematic review no difference in terms of local recurrence, positive resection margins, peritoneal carcinomatosis, and time to recurrence between laparoscopic and open adrenalectomy. The authors concluded that a poor outcome is more likely related to inadequate surgery rather than the chosen approach [37]. Similar findings are reported by other authors [24,38,39].
The primary limitation of the present study is its retrospective design, which may have introduced selection bias. Additionally, the study cohort includes patients with various adrenal histologies and lacks a specific oncological comparison with open adrenalectomy in patients with ACC. Finally, as this study reflects the experience of a high-volume institution, the findings may not be generalizable to other settings.
Conclusion
In conclusion, MIA for large adrenal tumors (≥ 6 cm) is safe and technically feasible in experienced hands, although it is associated with longer operative time and a higher conversion rate. Nonetheless, these findings should not overshadow the benefits of MIA for these patients. We believe that MIA should remain the first-line approach for adrenal masses without signs of local invasion, regardless of tumor size. However, careful patient selection is key to achieving optimal outcomes.
Author Contributions
Conceptualization, Leonardo Rossi and Gabriele Materazzi; Data curation, Leonardo Rossi, Chiara Becucci, Ortensia Della Posta and Luisa Sacco; Formal analysis, Leonardo Rossi and Ortensia Della Posta; Investigation, Leonardo Rossi and Luisa Sacco; Methodology, Leonardo Rossi, Piermarco Papini, Mattia Cammarata, Carlo Ambrosini and Gabriele Materazzi; Supervision, Carlo Ambrosini and Gabriele Materazzi; Validation, Mattia Cammarata, Carlo Ambrosini and Gabriele Materazzi; Writing – original draft, Leonardo Rossi; Writing – review & editing, Piermarco Papini and Francesca Palma.
Funding
No direct or indirect financial support was received.
Institutional Review Board Statement
All procedures performed in this study were in accordance with the 1964 Helsinki Declaration and its later amendments. Ethical approval was obtained from the local ethics committee (Comitato Etico Regione Toscana - AREA VASTA NORD OVEST).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Data Availability Statement
The data that support the findings of this study are available from the. corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gagner M, Lacroix A, Bolté E. Laparoscopic adrenalectomy in Cushing’s syndrome and pheochromocytoma. N Engl J Med. 1992 Oct 1;327(14):1033. [CrossRef]
- Higashihara E, Tanaka Y, Horie S, Aruga S, Nutahara K, Homma Y, et al. [A case report of laparoscopic adrenalectomy]. Nihon Hinyokika Gakkai Zasshi Jpn J Urol. 1992 Jul;83(7):1130–3.
- Heger P, Probst P, Hüttner FJ, Gooßen K, Proctor T, Müller-Stich BP, et al. Evaluation of Open and Minimally Invasive Adrenalectomy: A Systematic Review and Network Meta-analysis. World J Surg. 2017 Nov;41(11):2746–57. [CrossRef]
- Pogorzelski R, Toutounchi S, Krajewska E, Fiszer P, Kącka A, Piotrowski M, et al. The usefulness of laparoscopic adrenalectomy in the treatment of adrenal neoplasms - a single-centre experience. Endokrynol Pol. 2017;68(4):407–10. [CrossRef]
- Li J, Wang Y, Chang X, Han Z. Laparoscopic adrenalectomy (LA) vs open adrenalectomy (OA) for pheochromocytoma (PHEO): A systematic review and meta-analysis. Eur J Surg Oncol J Eur Soc Surg Oncol Br Assoc Surg Oncol. 2020 Jun;46(6):991–8. [CrossRef]
- Shen WT, Lim RC, Siperstein AE, Clark OH, Schecter WP, Hunt TK, et al. Laparoscopic vs open adrenalectomy for the treatment of primary hyperaldosteronism. Arch Surg Chic Ill 1960. 1999 Jun;134(6):628–31; discussion 631-632. [CrossRef]
- Hazzan D, Shiloni E, Golijanin D, Jurim O, Gross D, Reissman P. Laparoscopic vs open adrenalectomy for benign adrenal neoplasm. Surg Endosc. 2001 Nov;15(11):1356–8. [CrossRef]
- Materazzi G, Rossi L. Robot-assisted adrenalectomy: state of the art. Updat Surg. 2021 Jun;73(3):1131–46. [CrossRef]
- Guazzoni G, Montorsi F, Bocciardi A, Da Pozzo L, Rigatti P, Lanzi R, et al. Transperitoneal laparoscopic versus open adrenalectomy for benign hyperfunctioning adrenal tumors: a comparative study. J Urol. 1995 May;153(5):1597–600. [CrossRef]
- Zografos GN, Farfaras A, Vasiliadis G, Pappa T, Aggeli C, Vassilatou E, et al. Laparoscopic resection of large adrenal tumors. JSLS. 2010;14(3):364–8. [CrossRef]
- Dalvi AN, Thapar PM, Thapar VB, Rege SA, Deshpande AA. Laparoscopic adrenalectomy for large tumours: Single team experience. J Minimal Access Surg. 2012 Oct;8(4):125–8. [CrossRef]
- Hobart MG, Gill IS, Schweizer D, Sung GT, Bravo EL. Laparoscopic adrenalectomy for large-volume (> or = 5 cm) adrenal masses. J Endourol. 2000 Mar;14(2):149–54. [CrossRef]
- MacGillivray DC, Whalen GF, Malchoff CD, Oppenheim DS, Shichman SJ. Laparoscopic resection of large adrenal tumors. Ann Surg Oncol. 2002 Jun;9(5):480–5.
- Natkaniec M, Pędziwiatr M, Wierdak M, Major P, Migaczewski M, Matłok M, et al. Laparoscopic Transperitoneal Lateral Adrenalectomy for Large Adrenal Tumors. Urol Int. 2016;97(2):165–72. [CrossRef]
- Parente A, Verhoeff K, Wang Y, Wang N, Wang Z, Śledziński M, et al. Robotic and Laparoscopic Adrenalectomy for Pheochromocytoma: An International Multicenter Study. Eur Urol Focus. 2024 Sep 14;S2405-4569(24)00168-8. [CrossRef]
- Fassnacht M, Tsagarakis S, Terzolo M, Tabarin A, Sahdev A, Newell-Price J, et al. European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2023 Jul 20;189(1):G1–42. [CrossRef]
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83. [CrossRef]
- Daabiss, M. American Society of Anaesthesiologists physical status classification. Indian J Anaesth. 2011 Mar;55(2):111–5. [CrossRef]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004 Aug;240(2):205–13.
- Slankamenac K, Graf R, Barkun J, Puhan MA, Clavien PA. The comprehensive complication index: a novel continuous scale to measure surgical morbidity. Ann Surg. 2013 Jul;258(1):1–7.
- Rashid R, Sohrabi C, Kerwan A, Franchi T, Mathew G, Nicola M, et al. The STROCSS 2024 guideline: strengthening the reporting of cohort, cross-sectional, and case-control studies in surgery. Int J Surg Lond Engl. 2024 Jun 1;110(6):3151–65. [CrossRef]
- Miller BS, Gauger PG, Hammer GD, Doherty GM. Resection of adrenocortical carcinoma is less complete and local recurrence occurs sooner and more often after laparoscopic adrenalectomy than after open adrenalectomy. Surgery. 2012 Dec;152(6):1150–7. [CrossRef]
- Wu K, Liu Z, Liang J, Tang Y, Zou Z, Zhou C, et al. Laparoscopic versus open adrenalectomy for localized (stage 1/2) adrenocortical carcinoma: Experience at a single, high-volumecenter. Surgery. 2018 Dec;164(6):1325–9.
- Donatini G, Caiazzo R, Do Cao C, Aubert S, Zerrweck C, El-Kathib Z, et al. Long-term survival after adrenalectomy for stage I/II adrenocortical carcinoma (ACC): a retrospective comparative cohort study of laparoscopic versus open approach. Ann Surg Oncol. 2014 Jan;21(1):284–91. [CrossRef]
- Balla A, Palmieri L, Meoli F, Corallino D, Ortenzi M, Ursi P, et al. Are Adrenal Lesions of 6 cm or More in Diameter a Contraindication to Laparoscopic Adrenalectomy? A Case-Control Study. World J Surg. 2020 Mar;44(3):810–8.
- Cicek MC, Gunseren KO, Senol K, Vuruskan H, Yavascaoglu I. Is 6 cm Diameter an Upper Limit for Adrenal Tumors to Perform Laparoscopic Adrenalectomy? J Laparoendosc Adv Surg Tech A. 2021 Mar;31(3):301–5.
- Agrusa A, Romano G, Frazzetta G, Chianetta D, Sorce V, Di Buono G, et al. Laparoscopic adrenalectomy for large adrenal masses: single team experience. Int J Surg Lond Engl. 2014;12 Suppl 1:S72-74. [CrossRef]
- Feo CV, Portinari M, Maestroni U, Del Rio P, Severi S, Viani L, et al. Applicability of laparoscopic approach to the resection of large adrenal tumours: a retrospective cohort study on 200 patients. Surg Endosc. 2016 Aug;30(8):3532–40. [CrossRef]
- Sharma R, Ganpule A, Veeramani M, Sabnis RB, Desai M. Laparoscopic management of adrenal lesions larger than 5 cm in diameter. Urol J. 2009;6(4):254–9.
- Prakobpon T, Santi-Ngamkun A, Usawachintachit M, Ratchanon S, Sowanthip D, Panumatrassamee K. Laparoscopic transperitoneal adrenalectomy in the large adrenal tumor from single center experience. BMC Surg. 2021 Feb 1;21(1):68. [CrossRef]
- Chen Y, Scholten A, Chomsky-Higgins K, Nwaogu I, Gosnell JE, Seib C, et al. Risk Factors Associated With Perioperative Complications and Prolonged Length of Stay After Laparoscopic Adrenalectomy. JAMA Surg. 2018 Nov 1;153(11):1036–41. [CrossRef]
- Tiberio GAM, Solaini L, Arru L, Merigo G, Baiocchi GL, Giulini SM. Factors influencing outcomes in laparoscopic adrenal surgery. Langenbecks Arch Surg. 2013 Jun;398(5):735–43. [CrossRef]
- Parnaby CN, Chong PS, Chisholm L, Farrow J, Connell JM, O’ Dwyer PJ. The role of laparoscopic adrenalectomy for adrenal tumours of 6 cm or greater. Surg Endosc. 2008 Mar;22(3):617–21. ttps://doi.org/10.1007/s00464-007-9709-7.
- NIH state-of-the-science statement on management of the clinically inapparent adrenal mass (‘incidentaloma’). NIH Consens State Sci Statements. 2002 Feb 4;19(2):1–25.
- Gan L, Meng C, Li K, Lei Peng null, Li J, Wu J, et al. Safety and effectiveness of minimally invasive adrenalectomy versus open adrenalectomy in patients with large adrenal tumors (≥5 cm): A meta-analysis and systematic review. Int J Surg Lond Engl. 2022 Aug;104:106779. [CrossRef]
- Cooper AB, Habra MA, Grubbs EG, Bednarski BK, Ying AK, Perrier ND, et al. Does laparoscopic adrenalectomy jeopardize oncologic outcomes for patients with adrenocortical carcinoma? Surg Endosc. 2013 Nov;27(11):4026–32. [CrossRef]
- Machado NO, Al Qadhi H, Al Wahaibi K, Rizvi SG. Laparoscopic Adrenalectomy for Large Adrenocortical Carcinoma. JSLS. 2015;19(3):e2015.00036. [CrossRef]
- Brix D, Allolio B, Fenske W, Agha A, Dralle H, Jurowich C, et al. Laparoscopic versus open adrenalectomy for adrenocortical carcinoma: surgical and oncologic outcome in 152 patients. Eur Urol. 2010 Oct;58(4):609–15. [CrossRef]
- Lombardi CP, Raffaelli M, De Crea C, Boniardi M, De Toma G, Marzano LA, et al. Open versus endoscopic adrenalectomy in the treatment of localized (stage I/II) adrenocortical carcinoma: results of a multiinstitutional Italian survey. Surgery. 2012 Dec;152(6):1158–64. [CrossRef]
Figure 1.
Study flow chart of patients enrollment.
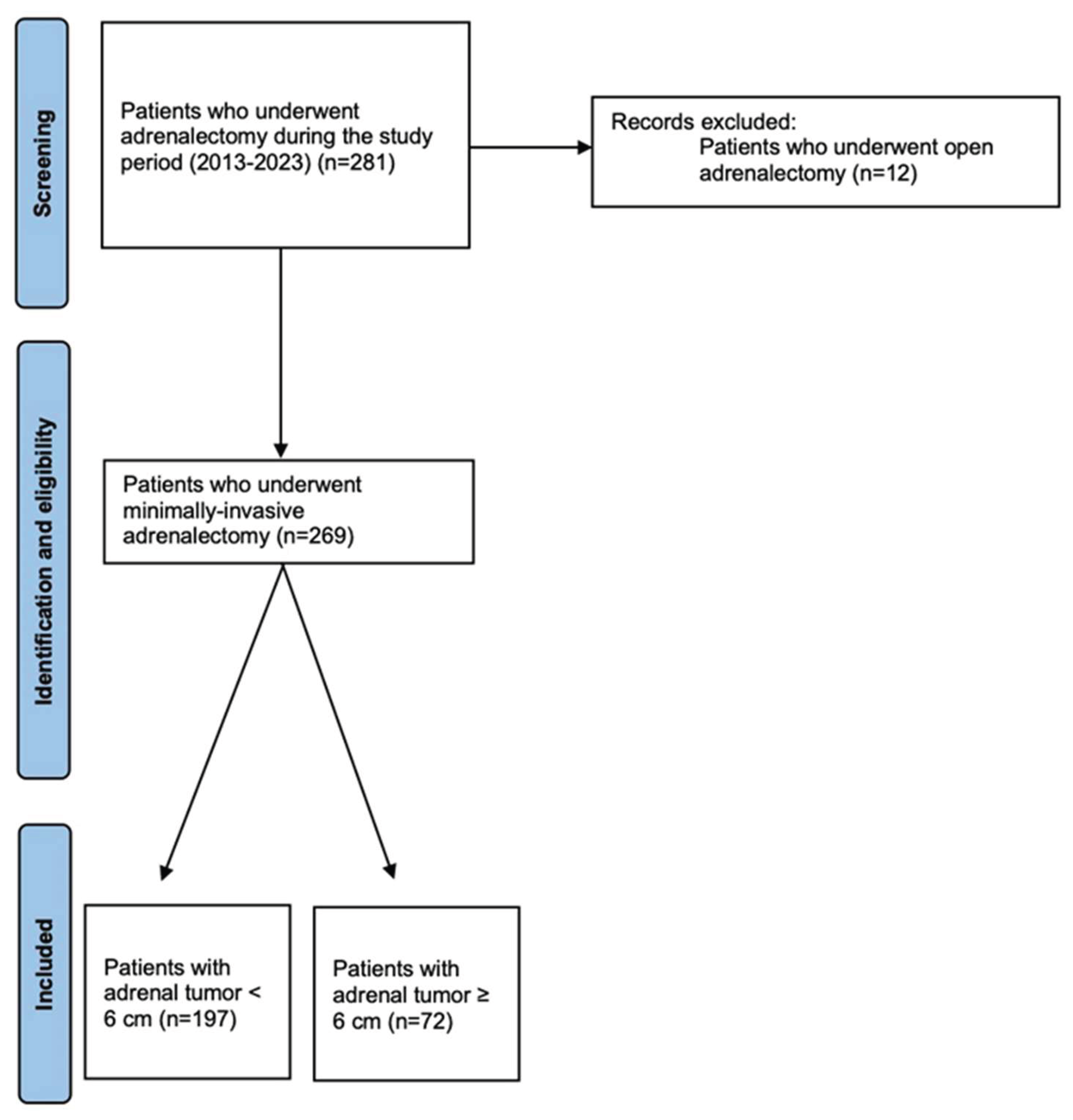

Table 1.
Univariate analysis of baseline, preoperative, and histologic characteristics of the study groups.
Table 1.
Univariate analysis of baseline, preoperative, and histologic characteristics of the study groups.
| Parameter | Group A (< 6 cm) N=197 (73.2%) |
Group B (≥ 6 cm) N=72 (26.8%) |
p value |
|---|---|---|---|
| Age, mean ± SD (years) | 52 ± 13.6 | 55.5 ± 13.5 | 0.058 |
| BMI, mean ± SD (kg/m2) | 27.6 ± 6.8 | 27.9 ± 6.7 | 0.795 |
| Female, n. (%) Male, n. (%) |
75 (38.1) 123 (61.9) |
38 (54.2) 41(45.8) |
0.018 |
| Comorbidity, n. (%) | 180 (91.4) | 67 (93.1) | 0.655 |
| Charlson Comorbidity Index, mean ± SD | 1.9 ± 1.8 | 2.4 ± 2.0 | 0.049 |
| ASA score n. (%) 1 2 3 4 |
1 (0.5) 113 (56.3) 82 (42.1) 2 (1) |
5 (6.9) 26 (34.7) 48 (58.3) 0 (0) |
<0.001 |
| Prior abdominal surgery, n. (%) | 93 (47.2) | 28 (38.9) | 0.224 |
| Hormonal hypersecretion, n (%) Catecholamine, n (%) Aldosterone, n (%) Cortisol, n (%) Cortisol + Aldosterone, n (%) Catecholamine + Androgen, n (%) |
131 (66.5) 51 (25.9) 38 (19.3) 41 (20.8) 1 (0.5) 0 |
30 (41.7) 19 (26.4) 2 (2.8) 9 (12.5) 0 1 (1.4) |
<0.001 |
| Surgical approach Transperitoneal, n. (%) Retroperitoneal, n. (%) Robotic transperitoneal, n. (%) |
149 (75.6) 43 (21.8) 5 (2.5) |
69 (95.8) 1 (1.4) 2 (2.8) |
<0.001 |
| Tumor location: Right, n. (%) Left, n. (%) Bilateral, n. (%) |
95 (48.2) 95 (48.2) 7 (3.6) |
45 (62.5) 23 (31.9) 4 (5.6) |
0.055 |
| Genetic mutation, n. (%) 21-OHD, n. (%) MEN2A, n. (%) MEN2B, n. (%) NF1, n. (%) VHL, n. (%) Maffucci syndrome, n. (%) |
12 (6.1) 0 (0) 5 (2.5) 2 (1) 3 (1.5) 2 (1) 0 (0) |
7 (9.7) 1 (1.4) 4 (5.6) 0 (0) 1 (1.4) 0 (0) 1 (1.4) |
0.303 |
| Tumor size (major lesion), mean ± SD (cm) | 3.6 ± 1.3 | 7.6 ± 1.8 | <0.001 |
| Histology Cortical adenoma or cyst, n. (%) With AMH, n (%) Pheochromocytoma, n. (%) Adrenal malignancies, n. (%) ACC, n.(%) Angiosarcoma, n. (%) Adrenal metastasis, n. (%) Myelolipoma, n. (%) Others, n. (%) Lymphoma, n. (%) Ganglioneuroma, n. (%) Angiomyolipoma, n. (%) Hemangioma, n. (%) Lymphangioma, n. (%) Fibrous solitary tumor, n. (%) |
131 (66.5) 6 (4.6) 45 (22.8) 10 (5.1) 4 (2) 0 6 (3) 1 (0.5) 10 (5.1) 0 3 (1.5) 1 (0.5) 1 (0.5) 3 (1.5) 2 (1) |
28 (38.9) 2 (2.8) 17 (23.6) 9 (12.5) 2 (2.8) 1 (1.4) 6 (8.3) 14 (19.4) 4 (5.6) 2 (2.8) 2 (2.8) 0 0 0 0 |
<0.001 |
SD: standard deviation; ASA: American Society of Anesthesiologists; BMI: body mass index; 21-OHD: 21-hydroxylases deficiency; MEN2A: multiple endocrine neoplasia type 2A; MEN2B: multiple endocrine neoplasia type 2B; NF1: neurofibromatosis type 1; VHL: von Hippel-Lindau disease; ACC: adrenal cortical carcinoma; AMH: adrenal medullary hyperplasia.
Table 2.
Univariate analysis of operative and postoperative outcomes of the study groups.
| Parameter | Group A (< 6 cm) N=197 (73.2%) |
Group B (≥ 6 cm) N=72 (28.8%) |
p value |
|---|---|---|---|
| Operative time, mean ± SD (min) | 97.8 ± 50.5 | 120 ± 56.2 | 0.002 |
| Associated surgeries, n. (%) | 23 (11.7) | 7 (9.7) | 0.652 |
| Conversion to open, n. (%) | 5 (2.5) | 6 (8.3) | 0.075 |
| Reason for conversion Technical difficulties, n. (%) Hemodynamic instability, n. (%) Others, n. (%) |
1 (0.5) 0 (0) 4 (2) |
4 (5.6) 2 (2.8) 0 (0) |
0.143 |
| Intra-operative complications No complications, n. (%) Hemorrhage, n. (%) Iatrogenic damage, n. (%) Others, n. (%) |
2 (1%) 195 (99.0) 0 (0) 1 (0.5) 1 (0.5) |
2 (2.8%) 70 (97.2) 1 (1.4) 0 (0) 1 (1.4) |
0.646 |
| Blood transfusions, n. (%) | 2 (1.0) | 3 (4.2) | 0.236 |
| Post-operative ICU, n. (%) | 106 (53.8) | 42 (58.3) | 0.508 |
| Length of ICU stay, mean ± SD (days) | 1 ± 0.2 | 1.1 ± 0.4 | 0.406 |
| Length of hospital stay, mean ± SD (days) | 3.1 ± 1.7 | 3.5 ± 2.3 | 0.112 |
| Postoperative complications, n. (%) | 19 (9.6) | 8 (11.1) | 0.723 |
| Clavien-Dindo classification Grade 1, n. (%) Grade 2, n. (%) Grade 3a, n. (%) Grade 4a, n. (%) |
6 (3) 10 (5.1) 1 (0.5) 2 (1) |
2 (2.8) 6 (8.3) 0 0 |
0.975 |
| Comprehensive Complications Index, mean ± SD | 2.0 ± 6.7 | 2.1 ± 6.1 | 0.857 |
| Readmission at 30 days, n. (%) | 4 (2) | 1 (1.4) | 0.730 |
| Adrenal-related mortality, n (%) | 0 | 0 | NA |
SD: standard deviation; ICU: intensive care unit; NA: not available.
Table 3.
Logistic regression analysis of factors associated with postoperative complications.
| Parameter | Coefficient | p-value | Odds Ratio | 95% CI | |
|---|---|---|---|---|---|
| Inferior | Superior | ||||
| Tumor size ≥ 6 cm | 0.149 | 0.768 | 1.161 | 0.432 | 3.117 |
| Age | -0.027 | 0.197 | 0.973 | 0.934 | 1.014 |
| Gender | 0.091 | 0.838 | 0.745 | 0.455 | 2.637 |
| ASA score | 0.525 | 0.240 | 1.691 | 0.704 | 4.063 |
| Charlson comorbidity index | 0.282 | 0.056 | 1.326 | 0.993 | 1.771 |
| Hormonal Hypersecretion |
0.378 | 0.426 | 1.459 | 0.575 | 3.701 |
| Tumor location (unilateral or bilateral) |
-0.223 | 0.851 | 0.800 | 0.078 | 8.162 |
| Surgical approach | -0.064 | 0.841 | 0.938 | 0.503 | 1.749 |
| Histology | 0.091 | 0.658 | 1.096 | 0.731 | 1.642 |
ASA: American Society of Anesthesiologists; CI: confidence interval.
Table 4.
Logistic regression analysis of factors associated with conversion rate.
| Parameter | Coefficient | p-value | Odds Ratio | 95% CI | |
|---|---|---|---|---|---|
| Inferior | Superior | ||||
| Tumor size ≥ 6 cm | 1.758 | 0.031 | 5.800 | 1.177 | 28.595 |
| Age | 0.008 | 0.842 | 1.008 | 0.928 | 1.096 |
| Gender | 0.855 | 0.266 | 2.351 | 0.522 | 10.587 |
| ASA score | 1.662 | 0.057 | 5.271 | 0.950 | 29.253 |
| Charlson comorbidity index | 0.022 | 0.930 | 1.023 | 0.620 | 1.688 |
| Hormonal Hypersecretion |
-0.388 | 0.632 | 0.678 | 0.138 | 3.327 |
| Tumor location (unilateral or bilateral) |
0.853 | 0.526 | 2.346 | 0.168 | 32.808 |
| Surgical approach | 0.184 | 0.772 | 1.202 | 0.347 | 4.157 |
| Histology | 0.029 | 0.927 | 1.030 | 0.548 | 1.935 |
ASA: American Society of Anesthesiologists; CI: confidence interval.
Table 5.
Linear regression analysis of factors associated with LOS.
| Parameter | Coefficient | p-value | 95% CI | |
|---|---|---|---|---|
| Inferior | Superior | |||
| Tumor size ≥ 6 cm | 0.248 | 0.344 | -0.268 | 0.764 |
| Age | -0.011 | 0.332 | -0.034 | 0.011 |
| Gender | 0.203 | 0.378 | -0.251 | 0.657 |
| ASA score | 0.416 | 0.062 | -0.021 | 0.853 |
| Charlson comorbidity index | 0.211 | 0.015 | 0.041 | 0.381 |
| Hormonal Hypersecretion |
-0.276 | 0.239 | -0.737 | 0.185 |
| Tumor location (unilateral or bilateral) | 3.231 | <0.001 | 2.037 | 4.424 |
| Surgical approach | -0.193 | 0.207 | -0.494 | 0.108 |
| Histology | 0.051 | 0.630 | -0.157 | 0.259 |
ASA: American Society of Anesthesiologists; CI: confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



