
Submitted:
25 March 2025
Posted:
25 March 2025
You are already at the latest version
Abstract
Background/Objectives: In the present study, we aimed to analyze the temporal trends in the prevalence of adrenal tumors diagnosed over a 22 years’ period (2001-2022) in a university hospital in Romania. Additionally, our goal was to highlight and illustrate the demographic and histo-pathological features of these rare tumors within our population. Methods: We performed a retrospective review of 116 cases of adrenal lesions registered in our institution. Data was analyzed in a comparative way, by dividing the study period into two equal 11 years’ time-intervals: 2001-2011 vs. 2012-2022. Results: Within our study population, the most common lesions were adenomas (31.9%), followed by pheochromocytomas (24.1%), and adrenal cortical carcinomas (11.2%); other lesions (eg. cysts, myeloliopma, etc.) were rare. Adrenal surgeries increased by 36% in the last 11 years (n=49 cases in 2001-2011 vs. n=67 cases in 2012-2022, p=0.095). The prevalence of adrenal adenomas almost doubled in the second study period (38.8% vs. 22.4%, p=0.014). Pheochromocytomas remained constant, revealing a similar prevalence (around 24%) in both time periods. Carcinomas’ prevalence was lower in 2012-2022 compared to 2001-2011 (7.4% vs. 16.3%, p=0.405). Conclusion: Our study demonstrated an increased prevalence of adrenal tumors in our institution over the last 11 years (2011-2022) compared to the previous period (2001- 2011). Adrenal cortical adenomas were the most common tumors, with a prevalence that was almost double between 2011-2022 vs. 2001-2011. They were followed by pheochromocytomas, which showed a constant prevalence, and by cortical carcinomas whose prevalence has decreased over the past decade in our institution.
Keywords:
adrenals
; adrenal adenoma
; adrenal carcinoma
; pheochromocytoma
; prevalence trend
1. Introduction
Before the development of imaging techniques adrenal tumors were considered extremely rare. Their diagnosis was established late, only when local compressive symptoms or associated hormonal excess were documented [1]. The accessibility to high-performance diagnostic imaging tools has significantly improved medical diagnosis and patient care, but has brought a new challenge in the management of incidentally discovered adrenal tumors.
Before 2000s, studies based on CT (computer tomography) scans have reported a low frequency of adrenal tumors (0.3-3.4%), most probably because of low-resolution imaging technology that often failed to detect small lesions. However, later on, when new high-resolution CT techniques were used, the prevalence of adrenal tumors increased, ranging from 1-5.1% [1]. It is well known that these tumors become more prevalent with age: from 4–7% among people older than 40 years old, to 5–10% in individuals older than 70 years [2,3,4,5].
Autopsy studies have shown a general prevalence of 1.7 to 3.6% for adrenal tumors, with higher rates in patients over 50 years old (5-7%) and significantly lower rates in children (0.15-0.36%) [5].
When dealing with an adrenal tumor, two critical concerns arise: the likelihood of malignancy and the evaluation of its hormone secretion activity. Most adrenal tumors are usually small benign nonfunctional adrenocortical adenomas [6], that don’t cause symptoms or require treatment [4]. Adrenocortical hormone-active tumors, on the other hand, are associated with endocrine syndromes resulting from the secretion of cortisol, aldosterone, sex hormones or their precursors.
Endogenous Cushing's syndrome is a rare condition, with an incidence of 0.7–2.4 cases per million population per year [7] associated with adrenal tumors that secrete excessive amounts of cortisol, leading to multiple comorbidities [8].
Conn's syndrome is characterized by excessive aldosterone production, accounting for approximately 20% of cases of resistant hypertension [9]; it is related to a wide range of pathologies, including bilateral adenomas, unilateral hyperplasia, micronodules, and microscopic aldosterone-producing cell clusters [10].
Excessive androgen production due to adrenal cortex tumors is extremely rare, with some studies reporting incidence rates of approximately 0.02 cases per million population per year [11,12]. These tumors are more likely to be malignant [12].
With regard to adrenal cancer, its diagnosis and, even more, its management are extremely challenging in day practice because of its high potential for aggressive behavior and risk of distant metastasis. Its incidence is estimated at 0.72 cases per million population per year, accounting for 0.2% of all cancer deaths in the United States [13,14,15]. In some clinical and surgical studies, adrenocortical carcinoma has been found to account for about 8-11% of all adrenal tumors [16,17]. The overall 5-year survival rates for adrenal carcinoma range from 35% to 58% [18].
Pheochromocytomas are neuroendocrine neoplasms of chromaffin tissue originating from the adrenal medulla. The excess secretion of catecholamines that characterizes these tumors can lead to a wide range of severe symptoms that significantly impact the patient’s quality of life. The incidence of pheochromocytoma in The United States is about 2-8 per million per year [19,20].
This wide array of adrenal neoplasms, ranging from asymptomatic adenomas to fatal carcinomas, raises challenges due to the diverse clinical presentations, imaging characteristics, histopathological findings, prognosis, and treatment strategies, and has increasingly become a focus of attention in recent years.
In the present study, we aimed to assess the temporal trends in the prevalence of adrenal tumors diagnosed over a 22-year period in university hospital in Romania (2001-2022). Additionally, our study aimed to highlight and illustrate the demographic and histopathological features of these rare tumors within our population.
2. Materials and Methods
2.1. Database and Study Design
We performed a 22-years retrospective study including all patients who underwent adrenal surgery and who were registered in the Pathology Department, Emergency County Hospital, Târgu-Mureș, Romania, between January 2001 and December 2022. The Ethics Committee of the Târgu-Mureş Emergency County Hospital approved the study (Letter of approval no.4467/16.02.2023).
2.2. Pathological Data and Study Groups
All patients who underwent adrenal surgery (open or laparoscopic adrenalectomy) between January 2001 and December 2022 were included in the study. Patient demographics (age, gender) year of diagnosis, clinical diagnosis and pathological data (complete histopathological diagnosis, tumor histology, etc.) were all retrieved from institutional database registries and pathological reports.
The histopathological diagnosis for adrenal tumors was set according to World Health Organization (WHO) Classification of Tumors of Endocrine Organs, 2nd (2000), 3rd (2004) and 4th (2017) editions, respectively [21,22,23]. Adrenal tumors originating from the cortical region encompassed both benign (adenomas, cysts, myelolipomas, hemangiomas, and nodular hyperplasia) and malignant (cortical carcinomas) tumors. Tumors of the adrenal medulla included: pheochomocytomas, benign ganglioneuromas and malignant ganglioneuroblastomas. The 4th edition of the WHO Classification of Endocrine Tumors (2017) states that all pheochromocytomas are considered to have metastatic potential, thus, they are no longer regarded as benign or malignant and long-term follow-up of these patients is recommended. Other rare tumors included adrenal lymphomas and metastasis. We focused our analysis on the most common adrenal tumors: adenomas, pheochromocytomas and cortical carcinomas.
2.3. Statistical Analysis
Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS, version 22, Chicago, IL, USA), Excel 2021, and Minitab Statistics Software 20.3 (2021) programs. Descriptive statistical analyses were done. The data were expressed as nominal or quantitative variables. Numbers and percentages were used to express nominal variables. The frequencies of the nominal variables were compared using the Chi-squared test. The normal distribution of continuous variables was assessed using the Kolmogorov–Smirnov test or histograms. The distributed continuous variables were expressed as mean +/− standard deviation (SD). The ANOVA test was used to compare several mean values. We analyzed the data in comparison by dividing the study period into two equal 11 years’ time-intervals: from January 2001 to December 2011 versus January 2012 to December 2022. The level of statistical significance was set at p < 0.05 and confidence intervals were set at 95%.
3. Results
3.1. Patient Characteristics
A total of 116 patients underwent adrenalectomy and were registered in the Department of Pathology, Târgu-Mureș Emergency County Hospital, Romania, from January 2001 to December 2022. The mean age at diagnosis was 52.78 ± 14.21 years (range 3-78); more than half of the patients were women (n=64, 55.2%). The mean age at diagnosis was 52.35 ±11.55 years for women (range 14-72) and 53.30 ± 16.98 years for men (range 3-78).
With regard to the site of origin, cortical lesions were the most prevalent (n=71, 61.2%), followed by medullar lesions (n=31, 26.7%) and other tumors types, herein including metastatic tumors (n=14, 12.1%),Table 1.
Demographic characteristics of the patients included in the study are illustrated in Table 1. The ages of patients undergoing adrenalectomies ranged widely from 3 to 78 years. The youngest patients were two infants, aged 3 and 5 years-old, both diagnosed with ganglioneuroblastoma. Another very young patient was a 10-year-old boy with the diagnosis of pheochromocytoma. Most of the adrenal tumors in our study occurred in patients found in 6th life decade (50-59 years-old), Figure 1.
Although adrenal tumors generally appeared to be slightly more common in women, with a Women/Men (W/M) ratio of 64/52, it is worth noting that this ratio varied depending on the specific tumor type. The most significant W/M ratio disparity was observed with regard to the prevalence of cysts (8/0), myelolipomas (5/1) and adenomas (27/10). In case of pheochromocytomas, an equal gender distribution was observed. By contrast, carcinomas occurred more frequently in men (W/M= 5/8) and men were typically older than women (57.22 years versus 45.60 years) with the same diagnosis, Table 1.
3.2. Pathological Data
Table 1 summarizes the prevalence of different histopathological types of adrenal tumors, included in the study. With regard to the site of origin, cortical lesions were the most prevalent (n=71, 61.2%), followed by medullar lesions (n=31, 26.7%) and other tumors types, herein including metastatic tumors (n=14, 12.1%).
In 49.13% (n=57) of the cases, a final diagnosis of malignancy was established (herein including cortical carcinomas, pheochromocytomas, neuroblastomas, lymphomas, and metastatic tumors), while the remaining cases (n=59, 50.87%) were classified as benign (herein comprising adenoma, adrenal cyst, myelolipoma, hemangioma, nodular hyperplasia, and ganglioneuroma).
Figure 2 illustrates the prevalence of adrenal tumors according to the pathological type in our study population. The most common three adrenal tumor types, accounting for nearly 70% of all the cases in our study were: (1) adenomas (31.9%), (2) pheochromocytomas (24.1%), and (3) adrenal cortical carcinomas (11.2%).
In our study group, adrenal tumors were more frequently found on the left side (Left/Right ratio: 64/49). Metastatic tumors were equally distributed either in the left or the right adrenal gland. Half of the metastatic tumors (n=6 cases), were adenocarcinomas with different primary origin, while three cases corresponded to pulmonary squamous cell carcinomas. The remaining metastatic tumor cases (n=3 cases) corresponded to one case of undifferentiated carcinoma, one melanoma case, and one clear cell renal carcinoma case.
3.2. Time Trend Prevalence of Adrenal Tumors in Our Study Population
We further analyzed the time trends of adrenal tumor prevalence in our institution from 2001 to 2022, comparing two 11-year intervals: 2001-2011 and 2012-2022.
Between 2012 and 2022, the number of adrenal surgeries increased by 36.7% (67 cases) compared to the period 2001-2011 (49 cases), (p=0.095), Figure 3. With regard to adenomas, pheochromocytomas and adrenal cortical carcinomas (the three most common adrenal tumor types), the most significant change was noticed in case of adenomas, where the prevalence rate doubled during the second study period (2012–2022), with 26 (38.8%) cases compared to 11 (22.4%) cases in the previous period (2001–2011), p=0.014, Figure 4.
Pheochromocytomas revealed an almost equal frequency across the two study periods (12 cases, 24.4% versus 16 cases, 23.8%), with no significant changes in the occurrence rate, p=0.450, Figure 4. As for adrenal carcinomas, there was a slight decrease in the number of cases in the second period (2012–2022) with 5 cases (7.4%), compared to 8 cases (16.3%) in the first period (2001–2011), although the change was not statistically significant p=0.405, Figure 4. Two cases of adrenal carcinoma presented metastases at the time of diagnosis: in the kidney (the case of a 74-year-old man) and in the ovary (the case of a 20-year-old woman).
*The Chi-Square Goodness-of-Fit test evaluates whether the observed distribution of adenomas (A), pheochromocytomas (B), carcinomas (C) and all adrenal tumors significantly differ from the expected distribution, across the two-time intervals (T1: 2001-2011 and T2: 2012-2022). p-value < 0.05, indicates that the difference between observed and expected counts is statistically significant. The larger the Chi-Square (χ²) value, the more significant the test.
Figure 5 shows the annual rate of adenomas, pheochromocytomas and carcinomas diagnosed in our institution over the study period (2001-2022), with respect to the total number of cases. In the last 11 years (2012-2022), compared to the previous period (2001-2011), there has been an increase in the total number of adrenal tumors registered in our department. This increase was primarily due to a more common identification of adrenal adenomas, as the prevalence of pheochromocytomas remained unchanged and carcinomas exhibited a slight downward trend, although not statistically significant, continuing to be rare tumors. One notable observation is the significant decrease in the number of adrenal tumor cases in 2020, the year of COVID-19 (Coronavirus Disease 2019) pandemic, when only 3 cases were registered, compared to 7 cases in the previous year, 2019.
*The graph shows the annual rate of diagnosed adrenal tumors, including adenomas, pheochromocytomas, and carcinomas, from 2001 to 2022, along with the total number of cases. The total number of adrenal tumors, represented by the blue line, exhibits an upward trend, indicating a general increase in diagnoses over time. Although there are fluctuations, the overall trajectory suggests a rising prevalence of adrenal tumors in recent years. Adenomas, represented by the red line, display a clear increasing trend, suggesting that these tumors have become more common over time. Pheochromocytomas, shown in purple, exhibit a mild increase, but the growth rate is less pronounced compared to adenomas. Carcinomas, represented by the green line, appear relatively stable or slightly decreasing.
4. Discussion
In the present study we aimed to assess the temporal trends in the prevalence of adrenal tumors diagnosed over a 22-year period in university hospital in Romania (2001-2022). Additionally, our objective was to highlight and illustrate clinicopathological characteristics of these tumors in our population.
Adrenal tumors are rare entities, accounting for approximately 5% of all tumors in the adult population [24]. Our study, covering a large period of time (22 years) included 116 patients who underwent adrenal surgery and were registered in our institution (Department of Pathology, Târgu-Mureș Emergency County Hospital, Romania) between 2002 and 2022. Our data revealed a 36.7% increase in the prevalence of adrenal tumors in the last 11 years (2012-2022), compared to the previous period (2001-2011). Our results are in accordance with published data from the literature.
A large study conducted in Minnesota, United States, based on medical records confirming the diagnosis of adrenal tumors, found a tenfold increase in the incidence of these tumors over a 23-year period (1995-2017) [5]. Similarly, a 10-year study in Iran, which analyzed adrenal surgical specimens, reported an increase in the incidence of adrenal tumors from 3 cases in 2004 to 21 cases in 2014 [25]. The increase in the number of adrenal tumors can be partly attributed to improved detection, thanks to the widespread availability of advanced imaging technologies, which allow physicians to diagnose these tumors even when they are clinically silent [2]. Our data showed that the most frequent adrenal pathology was represented by cortical adenomas, which doubled between 20112-2022 compared to 2001-2011, (26 cases versus 11 cases), supporting the upward curve of adrenal lesions.
The second most common tumor in our study was pheochromocytoma (24.1%); its prevalence was similar in the last 11 years (2012-2022), compared to the previous period (2001-2011) (23.8% versus 24.4%). An extensive systematic review of 12 studies, which included 4060 cases of pheochromocytoma diagnosed between 1949 and 2019, highlighted a significant increase in pheochromocytomas’ incidence over time, from 0.19/100,000/year in studies performed before 2000 to 0.58/100,000/year in the studies after 2010 [26].
By contrast, the study performed Ebbehoj et al. reported a slight decrease in the frequency of pheochromocytoma cases in Olmsted County, Minnesota, from 2.2% during the period 1995-2002 to 1.0% in the period 2011-2017 [5]. In Denmark, however, there was a 4.8-fold increase in pheochromocytoma cases from 1977 to 2015. This rise was attributed to a new group of older patients with smaller, incidentally discovered tumors, and atypically presenting with few or no paroxysmal symptoms [27].
The diagnostic methods when dealing with pheochromocytoma cases have largely evolved over time, and this aspect must be considered when comparing literature data revealing heterogeneous observations. Before 1986, about half of the patients were diagnosed based on symptoms, investigations for potential secondary hypertension, and a quarter through autopsy findings [26,27]. The increased detection rate in some studies can be attributed not only to advances in medical imaging, but also to improvements in biochemical testing, metanephrine/normetanephrine measurements being now widely available. The recently improved recognition of high germline mutation rates in pheochromocytoma patients, coupled with genetic testing and surveillance of family members at risk, might explain the increased frequency of pheochromocytoma in some studies. We also need to consider geographic disparities, variations in access to screening, economic factors, and the presence of founder mutations, all of which contribute to differing epidemiological trends.
An interesting result highlighted by our data is with regard to the time trend prevalence of adrenal carcinoma cases. Our study showed a decline in the prevalence of adrenal carcinomas over the last 11 years (n=5 cases, 7.4%), compared to the previous period (n=8 cases, 16.3%), although this change was not statistically significant (p=0.405). Literature data regarding the incidence of adrenal carcinomas is sparse and controversial.
A comprehensive study in the United States reported an overall age-adjusted incidence of adrenal carcinomas of 1.02 per 1.000.000 inhabitants per year, that did not change significantly between 1973 and 2014 [28]. Conversely, a study from Netherlands covering the period from 1993 to 2010 observed a decreasing overall incidence rate of adrenal carcinoma, from 1.3 per million person-years in 1993 to 1.0 per million person-years in 2010 [29]. Meanwhile, in Denmark, the incidence rate between 2003 and 2019 was reported at 1.4 per million per year. Notably, the incidence rate ratio significantly increased in women by 1.06 [95% confidence interval (CI): 1.02-1.12] per year, while no such trend was observed in men [30]. The data may exhibit heterogeneity, partly attributable to the different timeframes across the studies, which likely contributed to variations in the population’s access to and utilization of advanced diagnostic imaging techniques, thereby influencing the results.
In 2020, the incidence of adrenal tumors notably decreased, with only 3 cases reported compared to 7 cases in 2019. This decline is likely attributable to the impact of the COVID-19 pandemic, declared by the WHO on March 11, 2020 [31]. The crisis resulted in reduced healthcare access, limited imaging evaluations, the implementation of social distancing measures, the shift to telemedicine, and delays in elective surgeries, all of which likely contributed to the lower number of cases observed that year [32,33].
Regarding demographic data, our study shows that adrenal tumors are more common in adults, in the 6th decade of life. In the study performed by Ebbehoj et al. (1995-2017), the mean age of the patients with adrenal tumors diagnosed between was 62 years [5]. By contrast, in a study performed in Iran, the patients were significantly younger, with a mean age of 37.7 years. These results can be attributed to the higher proportion of neuroblastoma cases included in their study [25].
The pheochromocytoma patients included in our study had a mean age at diagnosis of 51.11 years, which aligns with the mean ages reported in other studies, where values range from 43 to 56.2 years [6,25]. Interestingly, Berends observed a gradual increase in the age of patients diagnosed with pheochromocytoma, with the average age rising from 45 years in 1995 to 55 years by 2015 [34].
In our study, we did not identify any cases of adrenal carcinoma in the pediatric population, and women were much younger (45 years) than men with this pathology (57 years). This finding aligns with literature reports that place the average age of carcinoma diagnosis between 46 and 56 years-old [15,28,29].
The youngest patients in the study were two pediatric cases (age 3 and 5, respectively), both diagnosed with neuroblastoma. Neuroblastoma accounts for approximately 10% of all pediatric cancers and typically affects children within the first 5 years of life [35].
In line to literature data, most of patients with adrenal lesions in our study were women (55.2%) [6,14,15,25,28,29]. By contrast, adrenal carcinomas occurred more frequently in men in our study (W:M ratio is 5:8). The risk factors influencing the gender distribution of adrenal carcinoma are not well-established. Heavy smoking in men, and the use of contraceptives in women, particularly before the age of 25, have been suggested as potential risk factors [15,36].
Consistent with other research, adrenal lesions were predominantly found on the left side (n=67 versus n= 49) [5,19].
The adrenal gland is a frequent site of metastases in various number of malignant tumors. In nononcological and unselected populations, the prevalence of adrenal metastases is 0–21 % while in oncological patients, the prevalence is referred to be higher, of 32-72% [37]. Cancer of the lung, breast, ovary, and malignant melanoma are the most common primary cancers that metastasize to the adrenal glands [37]. Our data showed a 10.2% proportion of metastasis among all adrenal tumors, similar to previously reported series [38,39]. Apart from two cases: one case of renal carcinoma and another one of squamous pulmonary carcinoma, for the other remaining cases the primary tumor was unknown at the time of surgery.
5. Conclusions
Adrenal tumors are rare entities in routine pathologic activity. Nevertheless, our study demonstrated an increased prevalence of these tumors in our institution over the last 11 years (2011-2022) compared to the previous period (2001-2011). These results are largely attributed to the increased detection and diagnosis of adrenal cortical adenomas, whose prevalence almost doubled between 2011-2022 versus 2001-2011. The widespread use of advanced imaging technologies in recent years could have significantly contributed to the detection of these tumors, even when they are asymptomatic.
Adrenal cortical adenomas were followed in prevalence by pheochromocytomas, cortical carcinomas and adrenal metastasis, whereas other tumors were rare. Pheochromocytomas’ frequency remained constant over the last 22 years, while cortical carcinoma continues to be a rare condition, whose prevalence has decreased over the past decade in our institution.
Author Contributions
Conceptualization, RC, ANB and AB; Methodology, RC, ANB and AB; Software: SM; Validation, RC, ANB and AB; Formal analysis: SM; Investigation: RC and SM; Resources: RC, ANB, and AB; Data Curation: RC, ANB, and SM; Writing – Orig-inal Draft Preparation: RC; Writing – Review &Editing: ANB and AB; Visualization: ANB; Su-pervision: AB; Project Administration, RC; Funding Acquisition, RC.
Funding
This research was funded by the George Emil Palade University of Medicine, Pharmacy, Science and Technology of Târgu-Mureș, Research Grant No. 164/10/10.01.2023.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the Emergency County Hospital, Târgu-Mureş, Romania (Letter of Approval no.4467/16.02.2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions (personal data protection of the patients included in the study).
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Sherlock, M.; Scarsbrook, A.; Abbas, A.; Fraser, S.; Limumpornpetch, P.; Dineen, R.; Stewart, P.M. Adrenal Incidentaloma. Endocr Rev 2020, 41. [Google Scholar] [CrossRef] [PubMed]
- Bovio, S.; Cataldi, A.; Reimondo, G.; Sperone, P.; Novello, S.; Berruti, A.; Borasio, P.; Fava, C.; Dogliotti, L.; Scagliotti, G. V.; et al. Prevalence of Adrenal Incidentaloma in a Contemporary Computerized Tomography Series. J Endocrinol Invest 2006, 29. [Google Scholar] [CrossRef] [PubMed]
- Reimondo, G.; Castellano, E.; Grosso, M.; Priotto, R.; Puglisi, S.; Pia, A.; Pellegrino, M.; Borretta, G.; Terzolo, M. Adrenal Incidentalomas Are Tied to Increased Risk of Diabetes: Findings from a Prospective Study. Journal of Clinical Endocrinology and Metabolism 2020, 105. [Google Scholar] [CrossRef] [PubMed]
- Song, J.H.; Chaudhry, F.S.; Mayo-Smith, W.W. The Incidental Adrenal Mass on CT: Prevalence of Adrenal Disease in 1,049 Consecutive Adrenal Masses in Patients with No Known Malignancy. American Journal of Roentgenology 2008, 190. [Google Scholar] [CrossRef]
- Ebbehoj, A.; Li, D.; Kaur, R.J.; Zhang, C.; Singh, S.; Li, T.; Atkinson, E.; Achenbach, S.; Khosla, S.; Arlt, W.; et al. Epidemiology of Adrenal Tumors - a Population-Based Study in Olmsted County, Minnesota. Lancet Diabetes Endocrinol 2020, 8. [Google Scholar] [CrossRef]
- Li, L.; Dou, J.; Gu, W.; Yang, G.; Du, J.; Yang, L.; Zang, L.; Wang, X.; Jin, N.; Ouyang, J.; et al. Clinical Analysis of 4 049 Hospitalized Cases of Adrenal Lesions. Zhonghua Yi Xue Za Zhi 2014, 94. [Google Scholar]
- Sharma, S.T.; Nieman, L.K.; Feelders, R.A. Cushing’s Syndrome: Epidemiology and Developments in Disease Management. Clin Epidemiol 2015, 7. [Google Scholar] [CrossRef]
- Savas, M.; Mehta, S.; Agrawal, N.; Van Rossum, E.F.C.; Feelders, R.A. Approach to the Patient: Diagnosis of Cushing Syndrome. Journal of Clinical Endocrinology and Metabolism 2022, 107. [Google Scholar] [CrossRef]
- Pillai, K.; Fares, A.; Dargham, S.; Al Suwaidi, J.; Jayyousi, A.; Abi Khalil, C. Primary Hyperaldosteronism Is Associated with Increased Mortality and Morbidity in Patients with Hypertension and Diabetes. Front Endocrinol (Lausanne) 2023, 14. [Google Scholar] [CrossRef]
- Hundemer, G.L.; Vaidya, A. Primary Aldosteronism Diagnosis and Management: A Clinical Approach. Endocrinol Metab Clin North Am 2019, 48. [Google Scholar]
- Vimal, R.K.Y.S.K.K.N.K.C.Y.T. Virilizing Adrenal Tumor: Case Report. IOSR Journal of Dental and Medical Sciences 2019, 18, 76–77. [Google Scholar]
- Sciarra, F.; Tosti-Croce, C.; Toscano, V. Androgen-Secreting Adrenal Tumors. Minerva Endocrinol 1995, 20. [Google Scholar]
- Kebebew, E.; Reiff, E.; Duh, Q.Y.; Clark, O.H.; McMillan, A. Extent of Disease at Presentation and Outcome for Adrenocortical Carcinoma: Have We Made Progress? World J Surg 2006, 30. [Google Scholar] [CrossRef]
- Allolio, B.; Fassnacht, M. Clinical Review: Adrenocortical Carcinoma: Clinical Update. Journal of Clinical Endocrinology and Metabolism 2006, 91. [Google Scholar]
- Else, T.; Kim, A.C.; Sabolch, A.; Raymond, V.M.; Kandathil, A.; Caoili, E.M.; Jolly, S.; Miller, B.S.; Giordano, T.J.; Hammer, G.D. Adrenocortical Carcinoma. Endocr Rev 2014, 35. [Google Scholar] [CrossRef]
- Libé, R.; Huillard, O. Adrenocortical Carcinoma: Diagnosis, Prognostic Classification and Treatment of Localized and Advanced Disease. Cancer Treat Res Commun 2023, 37. [Google Scholar] [CrossRef]
- Fassnacht, M.; Arlt, W.; Bancos, I.; Dralle, H.; Newell-Price, J.; Sahdev, A.; Tabarin, A.; Terzolo, M.; Tsagarakis, S.; Dekkers, O.M. Management of Adrenal Incidentalomas: European Society of Endocrinology Clinical Practice Guideline in Collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol 2016, 175. [Google Scholar] [CrossRef]
- Low, G.; Sahi, K. Clinical and Imaging Overview of Functional Adrenal Neoplasms. International Journal of Urology 2012, 19. [Google Scholar] [CrossRef]
- Huang, B.L.; Liu, Q.; Teng, Y.Y.; Peng, S.Q.; Liu, Z.; Li, M.L.; Liang, J.Y.; Zhang, Y.; Wang, M. Global Trends and Current Status in Pheochromocytoma: A Bibliometric Analysis of Publications in the Last 20 Years. Front Endocrinol (Lausanne) 2023, 14. [Google Scholar] [CrossRef]
- Conzo, G.; Pasquali, D.; Colantuoni, V.; Circelli, L.; Tartaglia, E.; Gambardella, C.; Napolitano, S.; Mauriello, C.; Avenia, N.; Santini, L.; et al. Current Concepts of Pheochromocytoma. International Journal of Surgery 2014, 12. [Google Scholar] [CrossRef]
- Kleihues, P.; Sobin, L.H. World Health Organization Classification of Tumors. Cancer 2000, 88. [Google Scholar] [CrossRef]
- DeLellis, RA. , Lloyd RV., Heitz PU., E.C. WHO Classification of Tumors Pathology and Genetics of Tumors of Endocrine Organs.
- Juan Rosai, R.Y.O.G.K.R.V.L. 2017.
- Ebbehoj, A.; Kaur, R.J.; Li, D.; Singh, S.; Zhang, C.; Atkinson, E.J.; Achenbach, S.J.; Rocca, W.A.; Khosla, S.; Bancos, I. SAT-176 Epidemiology of Adrenal Tumors: A Population Based Study of 1287 Patients. J Endocr Soc 2020, 4. [Google Scholar] [CrossRef]
- Zahir, S.T.; Aalipour, E.; Barand, P.; Kaboodsaz, M. Clinicopathological Features of Adrenal Tumors: A Ten-Year Study in Yazd, Iran. Asian Pacific Journal of Cancer Prevention 2015, 16. [Google Scholar] [CrossRef]
- Al Subhi, A.R.; Boyle, V.; Elston, M.S. Systematic Review: Incidence of Pheochromocytoma and Paraganglioma over 70 Years. J Endocr Soc 2022, 6. [Google Scholar] [CrossRef] [PubMed]
- Ebbehoj, A.; Stochholm, K.; Jacobsen, S.F.; Trolle, C.; Jepsen, P.; Robaczyk, M.G.; Rasmussen, Å.K.; Feldt-Rasmussen, U.; Thomsen, R.W.; Søndergaard, E.; et al. Incidence and Clinical Presentation of Pheochromocytoma and Sympathetic Paraganglioma: A Population-Based Study. Journal of Clinical Endocrinology and Metabolism 2021, 106. [Google Scholar] [CrossRef]
- Sharma, E.; Dahal, S.; Sharma, P.; Bhandari, A.; Gupta, V.; Amgai, B.; Dahal, S. The Characteristics and Trends in Adrenocortical Carcinoma: A United States Population Based Study. J Clin Med Res 2018, 10. [Google Scholar] [CrossRef]
- Kerkhofs, T.M.A.; Verhoeven, R.H.A.; Van Der Zwan, J.M.; Dieleman, J.; Kerstens, M.N.; Links, T.P.; Van De Poll-Franse, L. V.; Haak, H.R. Adrenocortical Carcinoma: A Population-Based Study on Incidence and Survival in the Netherlands since 1993. Eur J Cancer 2013, 49. [Google Scholar] [CrossRef]
- Pedersen, J.; Jarløv, A.E.; Rasmussen, Å.K.; Stochholm, K. Incidence, Treatment, and Survival of Adrenocortical Carcinoma in Denmark 2003-2019. J Endocr Soc 2024, 8. [Google Scholar] [CrossRef]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomedica 2020, 91. [Google Scholar]
- Zhang, Y.N.; Chen, Y.; Wang, Y.; Li, F.; Pender, M.; Wang, N.; Yan, F.; Ying, X.H.; Tang, S.L.; Fu, C.W. Reduction in Healthcare Services during the COVID-19 Pandemic in China. BMJ Glob Health 2020, 5. [Google Scholar] [CrossRef]
- Pujolar, G.; Oliver-Anglès, A.; Vargas, I.; Vázquez, M.L. Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review. Int J Environ Res Public Health 2022, 19. [Google Scholar]
- Berends, A.M.A.; Buitenwerf, E.; de Krijger, R.R.; Veeger, N.J.G.M.; van der Horst-Schrivers, A.N.A.; Links, T.P.; Kerstens, M.N. Incidence of Pheochromocytoma and Sympathetic Paraganglioma in the Netherlands: A Nationwide Study and Systematic Review. Eur J Intern Med 2018, 51. [Google Scholar] [CrossRef]
- Ponzoni, M.; Bachetti, T.; Corrias, M.V.; Brignole, C.; Pastorino, F.; Calarco, E.; Bensa, V.; Giusto, E.; Ceccherini, I.; Perri, P. Recent Advances in the Developmental Origin of Neuroblastoma: An Overview. Journal of Experimental and Clinical Cancer Research 2022, 41. [Google Scholar] [CrossRef] [PubMed]
- Hsing, A.W.; Nam, J.M.; Co Chien, H.T.; McLaughlin, J.K.; Fraumeni, J.F. Risk Factors for Adrenal Cancer: An Exploratory Study. Int J Cancer 1996, 65. [Google Scholar] [CrossRef]
- Wagnerova, H.; Lazurova, I.; Felsoci, M. Adrenal Metastases. Bratislava Medical Journal 2013, 114. [Google Scholar] [CrossRef]
- Samsel, R.; Cichocki, A.; Roszkowska-Purska, K.; Papierska, L.; Koalasinska-Cwikla, A.; Karpeta, E.; Ostrowski, T.; Nowak, K. Adrenal Metastases-Long-Term Results of Surgical Treatment, Single-Centre Experience. Wspolczesna Onkologia 2020, 24. [Google Scholar] [CrossRef]
- Kälviäinen-Mejía, H.K.; Sancho-Pardo, P.; Miguelena-Bobadilla, J.M.; Casamayor-Franco, M.C.; Dobón-Rascón, M.A. Surgery of the Adrenal Metastases. Cirugia y Cirujanos (English Edition) 2021, 89. [Google Scholar] [CrossRef]
Figure 1.
The age of the patients included in the study in relation to the type of adrenal pathology. *Most patients were diagnosed in the age range of 50-60 years. The extreme ages in our study are represented by a 78-year-old patient with adrenal adenoma and two patients aged 3 and 5 years with ganglioneuroblastomas.
Figure 1.
The age of the patients included in the study in relation to the type of adrenal pathology. *Most patients were diagnosed in the age range of 50-60 years. The extreme ages in our study are represented by a 78-year-old patient with adrenal adenoma and two patients aged 3 and 5 years with ganglioneuroblastomas.
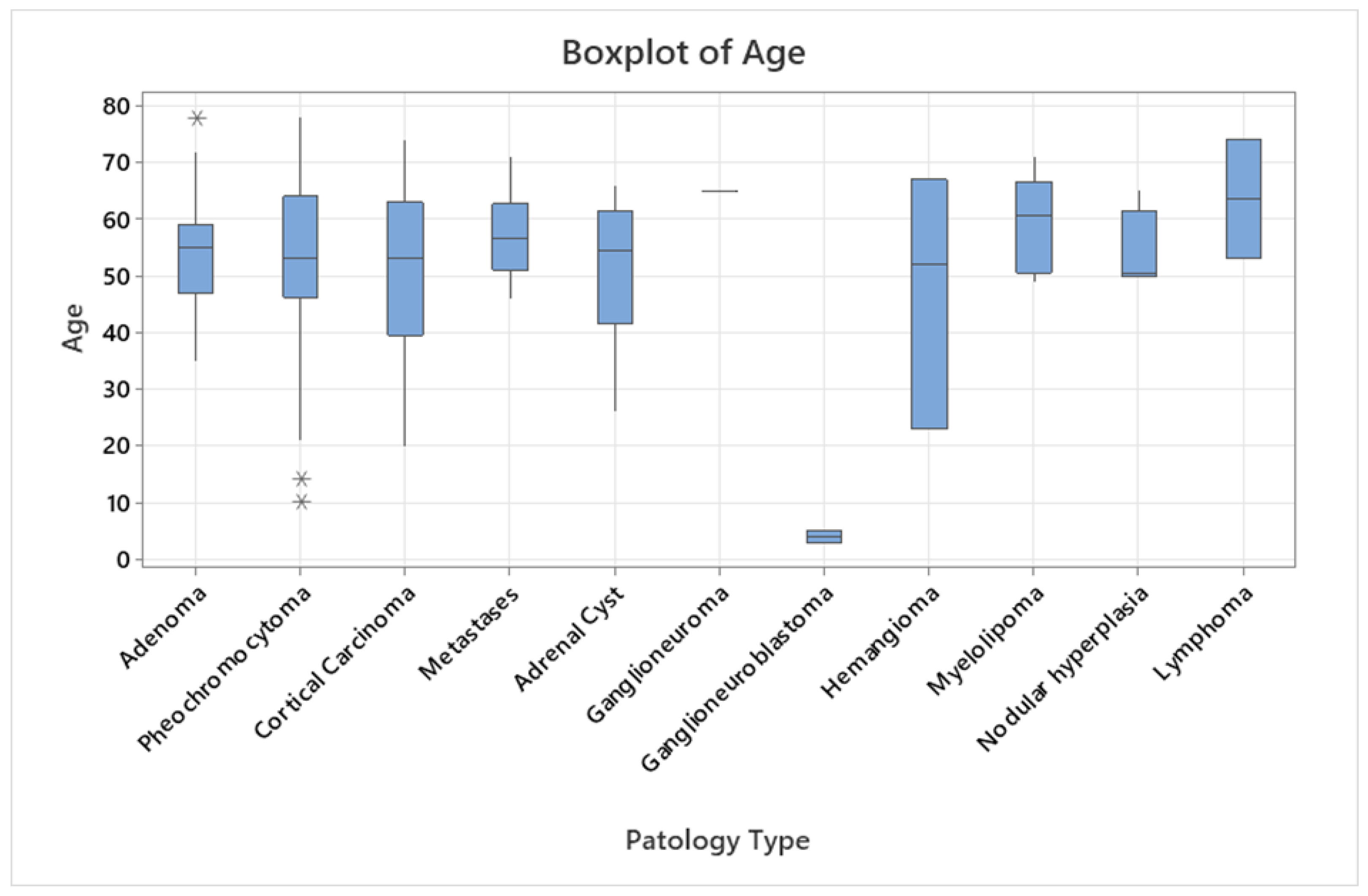
Figure 2.
The prevalence of adrenal tumors according to the pathological type. * The Pareto chart illustrates the prevalence of adrenal tumors by pathological type, showing both absolute frequency (bars) and cumulative percentage (line). Adenomas are the most common tumors, accounting for 31.9% (37 cases), followed by pheochromocytomas (24.1%, 28 cases) and cortical carcinomas (11.2%, 13 cases). These three types make up 67.2% of all cases, highlighting their dominance. Other types, such as metastases, adrenal cysts, myelolipomas, and nodular hyperplasia, are less frequent.
Figure 2.
The prevalence of adrenal tumors according to the pathological type. * The Pareto chart illustrates the prevalence of adrenal tumors by pathological type, showing both absolute frequency (bars) and cumulative percentage (line). Adenomas are the most common tumors, accounting for 31.9% (37 cases), followed by pheochromocytomas (24.1%, 28 cases) and cortical carcinomas (11.2%, 13 cases). These three types make up 67.2% of all cases, highlighting their dominance. Other types, such as metastases, adrenal cysts, myelolipomas, and nodular hyperplasia, are less frequent.
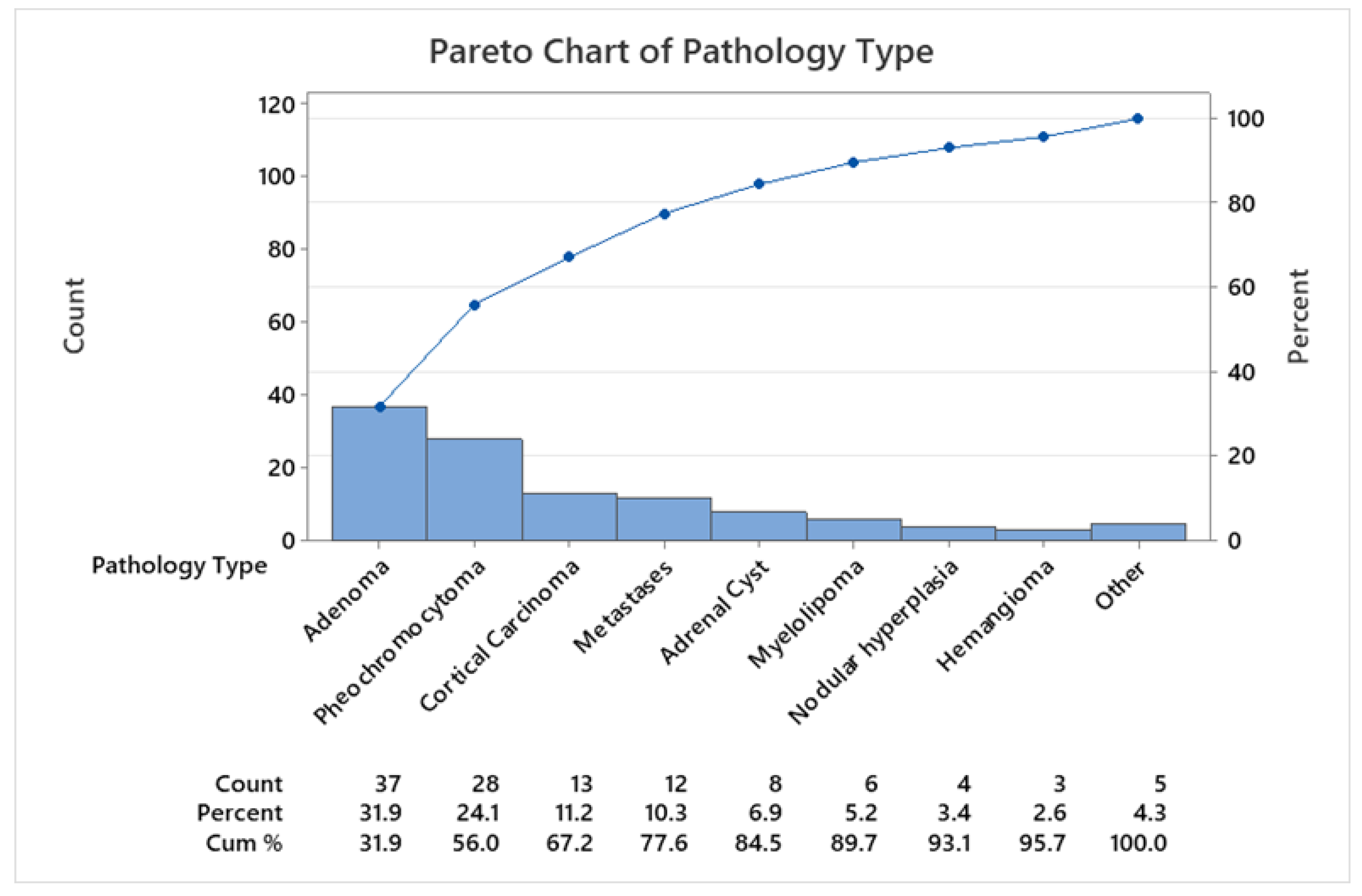
Figure 3.
The proportion of each histological type of adrenal tumor in comparison between 2001-2011 (T1) versus 2012-2022 (T2). There is a 36.7% increase in the number of all adrenal tumors during the T2 period (n=67) compared to the T1 period (n=49).
Figure 3.
The proportion of each histological type of adrenal tumor in comparison between 2001-2011 (T1) versus 2012-2022 (T2). There is a 36.7% increase in the number of all adrenal tumors during the T2 period (n=67) compared to the T1 period (n=49).
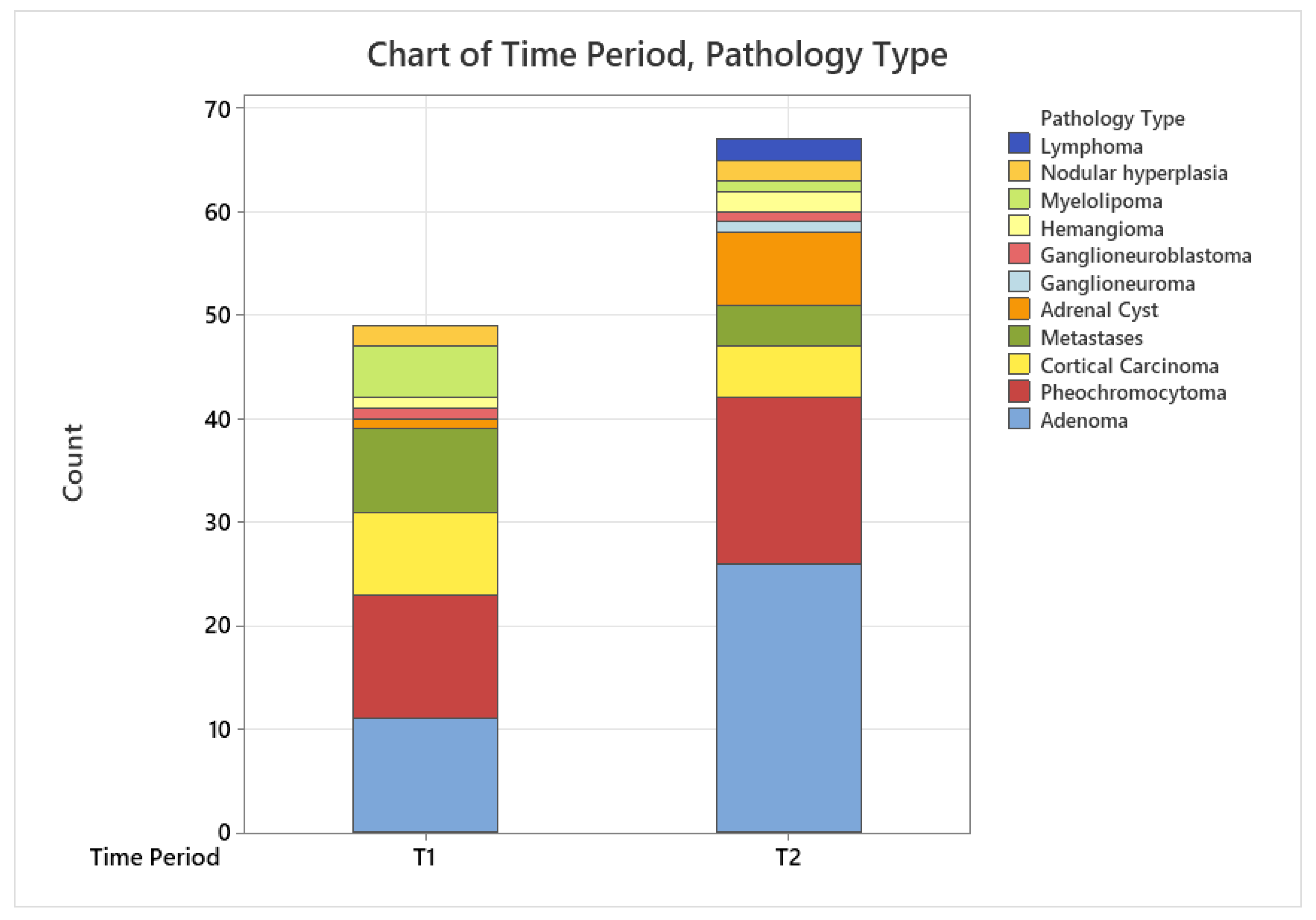
Figure 4.
Prevalence of adenomas (A), pheocromocytomas (B) and carcinomas (C) in comparison between 2001-2011 (T1) versus 2012-2022 (T2).
Figure 4.
Prevalence of adenomas (A), pheocromocytomas (B) and carcinomas (C) in comparison between 2001-2011 (T1) versus 2012-2022 (T2).
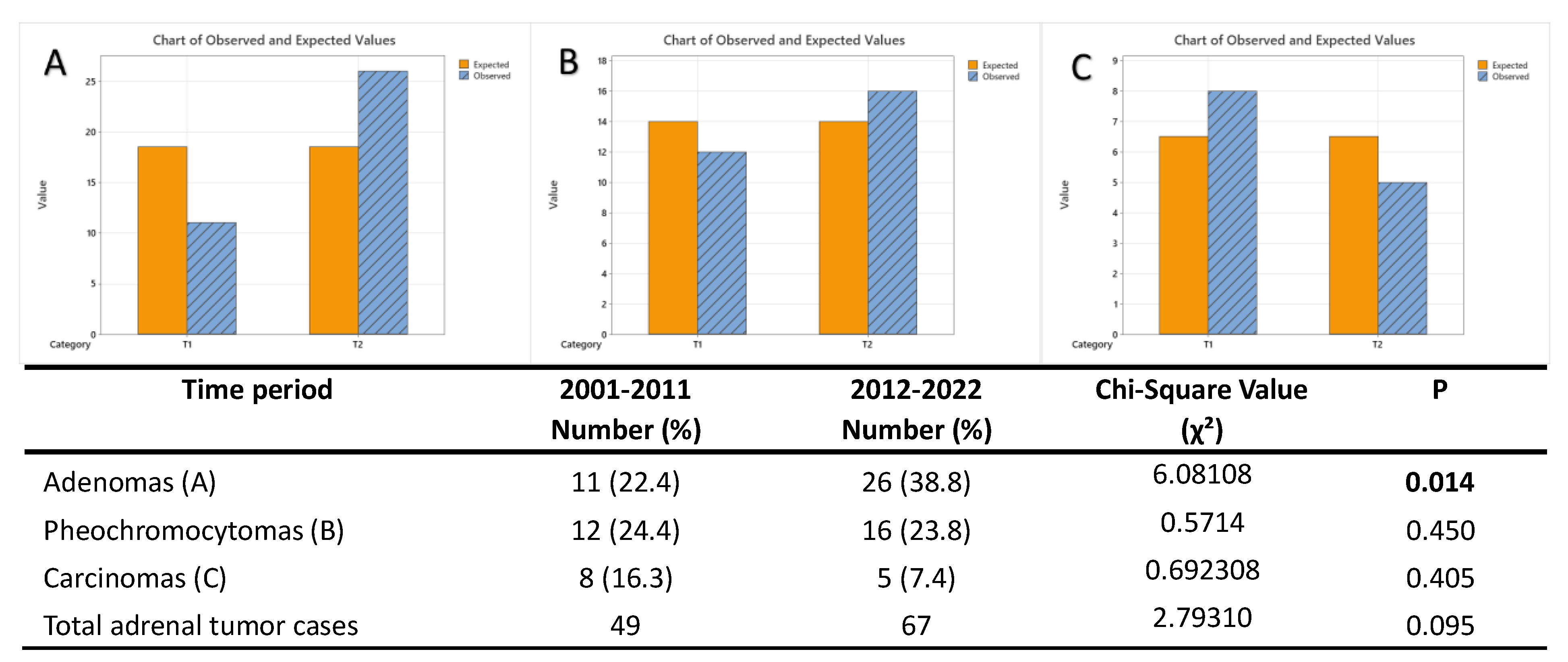
Figure 5.
Annual rate of adenomas (red line), pheochromocytomas (purple line) and carcinomas (green line) diagnosed in our institution over the study period (2001-2022), with respect to the total number of cases (blue line).
Figure 5.
Annual rate of adenomas (red line), pheochromocytomas (purple line) and carcinomas (green line) diagnosed in our institution over the study period (2001-2022), with respect to the total number of cases (blue line).
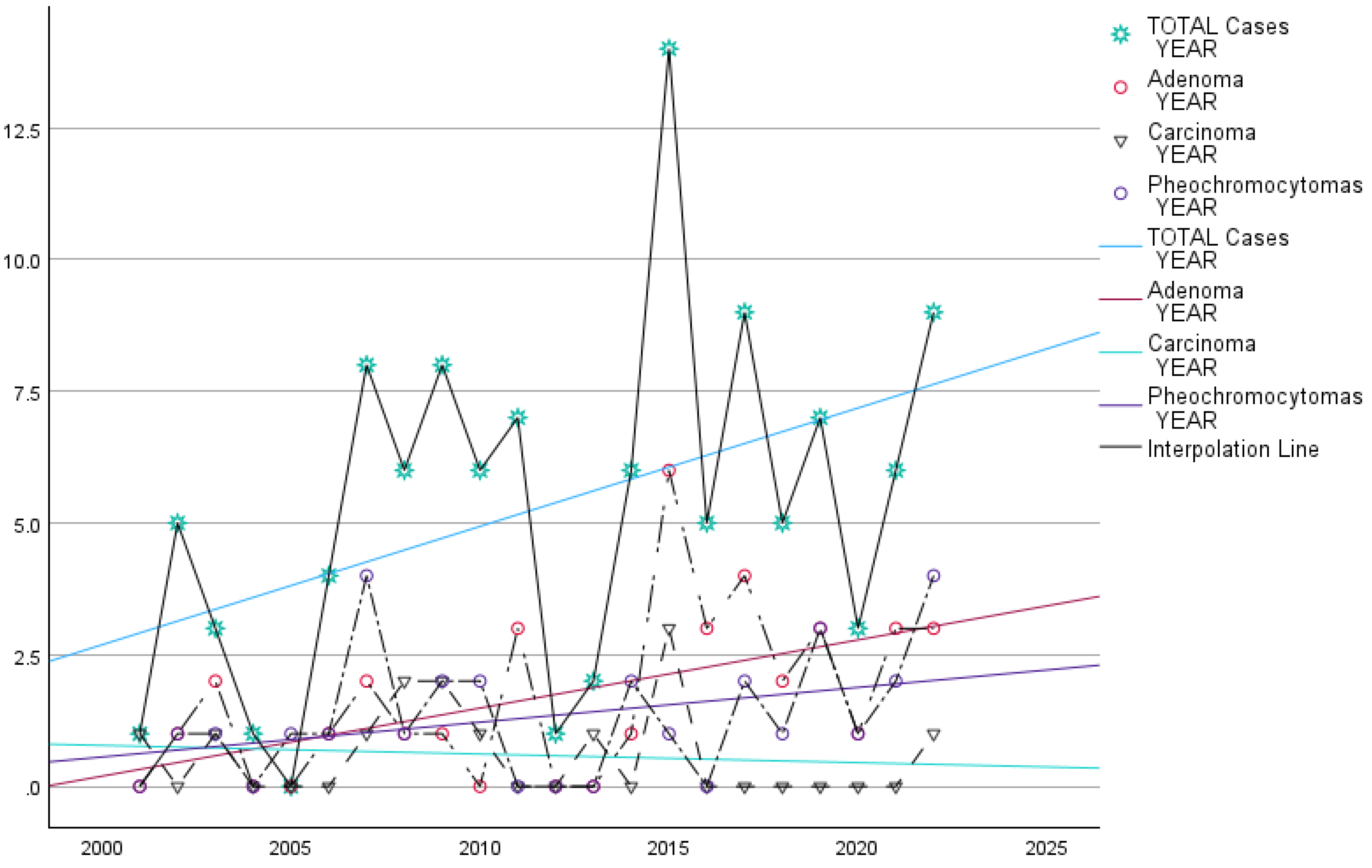

Table 1.
Demographic and clinical characteristics of patients diagnoses with different histopathological types of adrenal tumors between 2001-2022.
Table 1.
Demographic and clinical characteristics of patients diagnoses with different histopathological types of adrenal tumors between 2001-2022.
| Patology Type | Number (%) | Age (years) Mean ±SD* |
Age (years) Range |
Women/ Men |
Women age Mean ±SD | Men age Mean ±SD | Laterality Left/Right |
|---|---|---|---|---|---|---|---|
| Cortical tumors | 71 (61.2) | 53.43±11.40 | 20-78 | 46/25 | 51.95±10.79 | 56.16±12.19 | 45/26 |
| Adenoma | 37 (31.9) | 53.68 ±9.40 | 35- 78 | 27/10 | 52.33±9.15 | 57.30±9.54 | 24/13 |
| Adrenal cyst | 8 (6.9) | 51.63 ±13.33 | 26- 66 | 8/0 | 51.63±13.33 | - | 6/2 |
| Myelolipoma | 6 (5.2) | 59.50 ±8.80 | 49- 71 | 5/1 | 57.20±7.56 | 71 | 2/4 |
| Hemangioma | 3 (2.6) | 47.33 ±22.36 | 23- 67 | 0/3 | - | 47.33±22.36 | 2/1 |
| Nodular hyperplasia | 4 (3.4) | 54.00 ±7.35 | 50- 65 | 1/3 | 50 | 55.33±8.38 | 2/2 |
| Cortical carcinoma | 13 (11.2) | 52.31 ±15.12 | 20- 74 | 5/8 | 45.60±16.60 | 57.22±12.13 | 9/4 |
| Medullar tumors | 31 (26.7) | 48.51±20.27 | 3-78 | 14/17 | 52.71±15.07 | 45.05±23.62 | 16/15 |
| Pheochromocytoma | 28 (24.1) | 51.11 ±17.12 | 10- 78 | 14/14 | 52.71±15.07 | 49.50±19.38 | 15/13 |
| Ganglioneuroma | 1 (0.9) | 65.00 | - | 0/1 | - | 65 | 0/1 |
| Ganglioneuroblastoma | 2 (1.7) | 4.00 ±1.41 | 3- 5 | 0/2 | - | 4.00±1.00 | 1/1 |
| Others | 14 (12.1) | 58.21±8.32 | 46-74 | 4/10 | 55.75±7.50 | 59.2±8.80 | 6/8 |
| Metastases | 12 (10.4) | 57.33 ±7.48 | 46- 71 | 4/8 | 55.75±7.50 | 59.88±9.04 | 6/6 |
| Lymphoma | 2 (1.7) | 63.50 ±14.84 | 53- 74 | 0/2 | - | 63.50±14.84 | 0/2 |
| Total | 116 (100) | 52.78 ± 14.21 | 3- 78 | 64/52 | 52.35±11.55 | 53.30± 16.98 | 67/49 |
*SD: standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



