Submitted:
11 June 2025
Posted:
11 June 2025
You are already at the latest version
Abstract
The increasing incidence of Streptococcus suis (S. suis)-associated meningitis, which is significantly associated with sudden deafness, necessitates further investigation into its clinical characteristics and outcomes. To evaluate the clinical features and outcomes of S. suis-associated meningitis in a tertiary hospital in Bali, Indonesia, this cross-sectional study reviewed the medical records of patients diagnosed with suspected S. suis-associated meningitis from 2022 to 2024. The diagnosis of meningitis was based on the presence of fever, headache, neck stiffness, and altered mental status. Blood cultures were performed to confirm S. suis-associated meningitis. The diagnosis was confirmed when a blood culture was positive for S. suis and was probable based on a history of consuming raw pork. Both cases were categorized as S. suis-associated meningitis. Out of 67 patients, 34 (50.7%) presented with deafness. Common symptoms of meningitis include fever (100%), neck stiffness (100%), and severe headache (28.4%). Blood cultures revealed S. suis in 10.5% of cases. The total number of S. suis-associated meningitis cases was 31 out of 67 (46.3%), comprising probable cases (30, 44.8%) and confirmed cases (7, 10.4%). S. suis bacteremia caused deafness in 85.7% of cases. This study found no significant association between raw pork consumption and deafness (p = 0.151; odds ratio = 1.538, 95% CI = 0.584-4.055). The overall case fatality rate was 4.5%, with a 1.5% mortality rate among patients with confirmed S. suis-associated meningitis. The most common complications noted in this study were septic shock and sudden deafness. Increased awareness and preventive measures regarding pig-related exposure are crucial for managing this emerging public health threat.
Keywords:
meningitis
; sudden deafness
; zoonotic
; bacteremia
; S. suis
1. Introduction
S. suis-associated meningitis is a significant zoonotic disease caused by Streptococcus suis, which is particularly prevalent in regions with close human–pig interactions. This Gram-positive bacterium is a common pathogen in pigs and is transmitted to humans through direct contact with pigs or pork products [1]. The disease is primarily diagnosed in rural areas and among individuals with occupational exposure [2,3]. As the leading cause of bacterial meningitis in adults, particularly in areas where close contact between humans and pigs is common, the incidence of S. suis-associated meningitis is reported to be increasing in Southeast Asian countries, including Vietnam, Thailand, Hong Kong, China, and Japan [4]. Cases of this type of meningitis have also been identified in Europe, North America, South America, Oceania, and Africa [5,6,7,8]. The reported annual incidence of S. suis meningitis in Thailand is alarmingly high, reaching between 0 and 0.381 cases per 100,000 individuals [9]. In Vietnam, the estimated annual incidence rate is approximately 0.25 to 0.32 cases per 100,000 population [10]. Hong Kong reports a yearly incidence of 0.09 cases per 100,000 people, underscoring the persistent threat posed by this infection [11]. Furthermore, between 2011 and 2014, China's estimated annual incidence rate of S. suis infections in humans ranged from 0.249 to 0.324 cases per 100,000 population, highlighting a notable public health issue that warrants attention [10]. These statistics underscore a pressing need for heightened awareness and proactive measures to combat this infectious disease in Southeast Asia.
Streptococcus suis is an encapsulated, facultative anaerobic bacterium. It is primarily found in pigs but can also cause severe zoonotic infections in humans. Its pathogenicity is linked to structural components like capsular polysaccharides (CPS), surface proteins, and cell wall elements. Key virulence factors include the capsular polysaccharides, the toxin suilysin, biofilm formation, and genes related to immune evasion, metabolism, and stress responses. [12,13,14]. S. suis comprises 29 serotypes, classified according to their capsular polysaccharide (CPS) composition [15]. In pigs, S. suis infection begins with colonization of the respiratory or oral mucosa, where it must compete with the normal microflora and resist local mucosal immunity. The bacteria adhere to and breach the mucosal epithelial cell barrier, enabling them to invade deeper tissues and enter the bloodstream. The pathogen’s virulence factors and encapsulation allow S. suis to evade the immune system by interfering with phagocytosis and modulating dendritic cells, resulting in exaggerated production and neutrophil recruitment. The pathogen can adhere to and invade brain microvascular endothelial cells through specific virulence factors, such as serine-rich glycoproteins, which interact with the vimentin receptor. S. suis infection induces inflammasome activation, leading to the secretion of pro-inflammatory cytokines and the disruption of blood–brain barrier and tight junction proteins, facilitating the pathogen's invasion into the central nervous system [16,17]. The infection can have various clinical manifestations, including fever, chills, headache, decreased appetite, generalized pain, signs of meningitis, sepsis, irreversible hearing loss, toxic shock syndrome, arthritis, endocarditis, skin manifestations, and vestibular dysfunction [18,19,20].
Key risk factors for contracting this infection include consuming raw or undercooked pork, such as undercooked pig blood or intestine, and handling sick or dead pigs. [15,21]. Since 2014, cases of S. suis-associated meningitis have been reported to increase in Bali, Indonesia, where pig farms are densely concentrated [22]. During ceremonies, the Balinese often serve high-risk dishes, including raw pig blood, undercooked suckling pig, or pig intestine [23].
Despite its prevalence in certain regions, S. suis infections are frequently underreported due to diagnostic challenges and a lack of awareness [24]. This study presents the clinical characteristics of meningitis cases in which patients experienced sudden deafness related to S. suis, as observed in a tertiary hospital with limited resources.
2. Methods
2.1. Ethical Consideration
The study protocol was reviewed and approved by the Research Ethics Committee of Sanjiwani Hospital, Bali (document number 420/40268/RSU). This study is a retrospective analysis of medical records from the hospital; therefore, informed consent was not required.
2.2. Study Design
This study is a retrospective analysis of the medical records of patients diagnosed with suspected S. suis-associated meningitis between 2022 and 2024 who were admitted to Sanjiwani Hospital, a tertiary referral hospital in Bali with 241 beds. The inclusion criteria for this study were primarily based on clinical diagnosis and comprised adult patients aged 18 years or older who had been diagnosed with suspected S. suis-associated meningitis. The clinical diagnosis of meningitis was determined by the presence of the classic triad: fever, neck stiffness, and altered mental status or headache [25]. Incomplete medical record data were excluded from the study. In this study, cases were defined as confirmed S. suis-associated meningitis if the patient had a positive S. suis culture, and probable S. suis infection if the patient had a history of consuming raw pork. Meningitis cases refer to all instances formerly diagnosed with suspected S. suis-associated meningitis.
2.3. Laboratory and Imaging Investigation
At the tertiary hospital, lumbar puncture to obtain cerebrospinal fluid (CSF) is often deferred due to concerns about the risk of cerebral herniation. Additionally, the high cost of CSF analysis prevented it from being performed routinely to confirm the cause of meningitis. As the number of cases of probable S. suis-related meningitis is increasing, the hospital has implemented a non-invasive diagnostic tool, blood culture, for meningitis cases, including those with or without sudden deafness.
Blood samples from patients exhibiting clinical signs of meningitis were introduced onto 5% defibrinated sheep blood agar plates (DSBAPs) and incubated in 5% CO2 at 37°C for 18–24 hours [26]. According to the Clinical and Laboratory Standards Institute guidelines, the resulting colonies were isolated for identification and drug susceptibility testing using a fully automatic VITEK 2 COMPACT system [27]. Selected colonies were cultured in tryptic soy broth, incubated at 37°C for 18–24 hours, and preserved at –80°C in 50% glycerol. Next, the S. suis isolates were cultured on DSBAPs and incubated in 5% CO2 at 37°C for 18–24 h for further analysis.
The imaging approach used in this study was head computed tomography (CT), although CT is not sensitive to detecting meningitis.
2.4. Statistical Analysis
SPSS Version 25 (SPSS Inc., Chicago, IL) was used to analyze the collected statistical data. A probability value of p ≤ 0.05 was considered statistically significant. Numerical data were compared using the independent-samples t-test or the Mann–Whitney test, depending on their distribution. The Chi-Square test was used for categorical data.
3. Results
We identified 74 cases of suspected S. suis-associated meningitis, referred to as meningitis cases, from the hospital medical records of patients admitted between 2022 and 2024. Of these, 67 cases had complete data for analysis (Table 1). The first patients with meningitis to present with sudden deafness were admitted in April 2022. Among the 67 cases, 34 patients presented with deafness, representing 50.7%. There were 30 cases of probable S. suis-associated meningitis (44.8%) and 7 cases of confirmed S. suis-associated meningitis (10.4%) (Table 1). Therefore, the overall number of S. suis-associated meningitis cases was 31 out of 67 (46.3%), with one culture-positive patient who had no history of consuming raw pork. Statistical analysis revealed no significant association between raw pork consumption and the presentation of deafness (p=0.151; odds ratio =1.538, 95% CI=0.584-4.055).
All samples exhibited fever and neck stiffness, with both systems present in 100% of cases. Among the subjects with clinical meningitis presenting with sudden deafness, only 56.7% reported consuming raw pork blood. The chief complaints of the subjects included a decrease in consciousness (52.2%), severe headache (28.4%), fever (13.4%), altered mental status (4%), convulsion (1.5%), and loss of hearing (1%). Three subjects (4.5%) experienced both septic arthritis and deafness. Septic shock occurred in 11 subjects (16.4%), 3 of whom (4.5%) died. In total, septic shock complications occurred in 3 patients in the group with meningitis and sudden deafness (4.5%). Among these subjects with clinical meningitis and sudden deafness, mortality due to septic shock was 1 (1.5%). Consequently, the mortality rate for S. suis-associated meningitis was also 1 (1.5%).
The first suspected cases of S. suis-associated meningitis patients presenting with sudden deafness were reported in April 2022 (Figure 1). Most meningitis cases were reported in 2024. In 2022, the total number of cases with sudden deafness was 6 (9%), followed by 4 (6%) in 2023 and an enormous increase to 24 (35.8%) in 2024. The highest number of cases of meningitis with sudden deafness was reported in January and February 2024.
This study did not evaluate the CSF analysis or CSF culture results. The only non-invasive tool to support the diagnosis of S. suis-associated meningitis was blood culture, which was performed selectively due to cost considerations. The identification of S. suis in the blood of patients with clinical meningitis was confirmed with the diagnosis of S. suis-associated meningitis [28]. The blood culture results are described in Figure 2. Blood culture was performed in only 10 patients, revealing S. suis bacteremia in 7 out of 67 (10.4%) cases. Additionally, 1 case (1.5%) was positive for Staphylococcus bacteremia, while 2 out of 67 (3%) exhibited no growth. In this study, S. suis bacteremia caused six cases (85.7%) of sudden deafness, with 83.3% occurring in males.
The main results of the computed tomography (CT) scans were typical, with 58.9 % showing no signs of meningeal enhancement. Others reveal meningeal enhancement or nonspecific findings such as hypodense lesions. The laboratory findings are summarized in Table 2. No significant differences were observed in laboratory results between those presenting with meningitis and sudden deafness and those without sudden deafness except for the mean WBC count, which was higher in the group with sudden deafness (14.3 vs. 10.9 × 10^3/mL, p = 0.039).
All patients were treated with 2 grams of intravenous ceftriaxone every 12 hours for 10 to 14 days, in addition to dexamethasone at a dose of 10 mg intravenously every six hours for four days. Among the 67 patients with meningitis, 95.5% survived, resulting in an overall mortality rate of 4.5%.
4. Discussion
The diagnosis of S. suis-related meningitis does not rely on detecting S. suis in the cerebrospinal fluid (CSF); the presence of S. suis bacteremia can also confirm the diagnosis [10,28]. The consumption of raw pork in Bali is concerning, particularly given the discovery of bacteremia related to S. suis. However, the current study found no significant association between raw pork consumption and meningitis with sudden deafness, yielding an odds ratio of 1.538 with a wide confidence interval that suggests non-significance. Despite the lack of statistical significance, the elevated odds ratio indicates a potential risk and warrants further investigation, particularly given the small sample size of 67 participants.
The odds ratio for acquiring an S. suis infection after consuming raw pork was 4.63 (95% CI 2.94–7.29). In comparison, the odds ratio for infection following exposure to a pig was 4.01 (95% CI 2.61–6.15), and the odds ratio for consuming pork was 3.03 (95% CI 1.61–5.68) [2]. Furthermore, a study conducted in Bali between 2014 and 2017 reported that the incidence of S. suis-associated meningitis reached 62% [22].
Among the cases with S. suis bacteremia, a significant majority of patients—83.8%—were male. This result aligns with previous studies indicating that males constitute a predominant percentage of S. suis-associated meningitis cases, accounting for as much as 88% [21]. The higher incidence of meningitis in males may be attributed to various factors, including hormonal, biological, and behavioral differences. Testosterone, for instance, can modulate immune responses, potentially increasing susceptibility to infections [29]. Furthermore, cultural practices in Bali dictate that only males prepare pork, exposing them to greater risk via undercooked or raw pork products [23].
Clinical manifestations of meningitis typically include headaches, neck stiffness, vomiting, and fever [30]. In adults, common symptoms include neck stiffness, fever, and altered mental state [25]. This study reported that all subjects presented with fever and signs of meningism, alongside other symptoms such as convulsions, ataxia, and severe headaches. These clinical presentations underscore the need for rapid diagnosis and treatment to mitigate bacterial mortality.
Laboratory findings are crucial in diagnosing bacterial meningitis, with elevated white blood cell (WBC) counts indicating an inflammatory response to bacterial infection. The analysis revealed a significant median difference in WBC levels between cases associated with sudden deafness and those without. In one reported case of S. suis meningitis, the WBC count was exceptionally high at 27.28 × 10^9/L, with 94.20% neutrophils [31]. This elevation in WBCs is linked to the host's inflammatory response to S. suis, which stimulates macrophages to secrete pro-inflammatory cytokines such as IL-1β, TNF-α, IL-6, and IL-8, which are essential for recruiting and activating leukocyte populations [32]. Indeed, the capsular material of S. suis significantly excites the generation of prostaglandin E2 and matrix metalloproteinase 9 in macrophages, contributing to tissue destruction and blood–brain barrier disruption [33].
The diagnosis of meningitis in this study was based on the classic triad of fever, neck rigidity, and altered mental state or headache. However, the high mortality rate of bacterial meningitis, ranging from 10% to 20% in developed countries, underscores the need for robust diagnostic systems to enable timely treatment. The sensitivity of clinical judgment in diagnosing bacterial meningitis varies, with the classic triad exhibiting a sensitivity of only 40% to 50% [34].
In this study, blood cultures were performed in only 10 cases, resulting in a 70% identification rate for S. suis, while 10% identified Staphylococcus spp., and no growth was observed in 20%. The misidentification of S. suis as viridans streptococci has been documented elsewhere, with follow-up investigations confirming that a significant percentage of viridans cases were S. suis [35]. Other studies have confirmed S. suis-associated meningitis through blood culture, cerebrospinal fluid (CSF) culture, real-time polymerase chain reaction (RT-PCR), or a combination of these methods [28].
CSF analysis plays a crucial role in diagnosing bacterial meningitis, focusing on cytochemical characteristics such as the white blood cell (WBC) count, protein concentration, and glucose levels. An elevated WBC count exceeding 10 cells/µL in the CSF is a standard threshold for diagnosis [36]. A predominance of neutrophils suggests bacterial meningitis, whereas lymphocyte dominance indicates a viral infection. A CSF glucose level below 60 mg/dL or a CSF/serum glucose ratio of less than 0.44 generally indicates bacterial meningitis [37]. Elevated protein levels are also typically observed in bacterial cases, while a CSF lactate level exceeding 30 mg/dL indicates bacterial meningitis [38,39]. These findings underscore the utility of CSF analysis as a practical tool in resource-limited settings where advanced diagnostic facilities may not be available. Further analysis of CSF includes Gram staining, culture, and/or sensitivity testing. Gram staining may detect bacteria in 50-80% of cases, while culture yields a positive result in more than 80%; however, a study reported low sensitivity in CSF cultures [40]. Accurately identifying the causative organism without cultural evidence becomes challenging, potentially leading to incorrect diagnoses or ineffective treatments.
Given the importance of CSF analysis, the absence of such assessments and RT-PCR testing in this study introduces several confounding factors. Without comprehensive CSF analysis, accurately confirming meningitis becomes challenging, potentially leading to the misclassification of other conditions. The symptoms of meningitis can overlap with those of various illnesses, complicating the clinical picture. Additionally, without conclusive CSF investigations, it is not easy to assess the impact of co-infections or other pathogens that may contribute to clinical outcomes.
The complications associated with S. suis-associated meningitis observed in this study included septic shock, arthritis, and sudden deafness. Previous research has documented additional complications, such as renal or liver involvement, acute respiratory distress syndrome, endophthalmitis, spinal abscess, and skin rashes [28]. Hearing loss and vestibular dysfunction are common sequelae, with one study reporting that up to 75% of subjects with S. suis meningitis experienced hearing loss [10,41]. The primary mechanism linking S. suis meningitis to hearing loss is related to suppurative labyrinthitis, which can lead to damage to the cochlea and auditory nerve. High bacterial loads can increase the permeability of the blood–labyrinth barrier, allowing bacteria and inflammatory cells to enter the cochlea and causing direct damage to the inner ear's sensory cells [42].
This study's case fatality rate (CFR) for S. suis-associated meningitis was 1.5%. In contrast, previous studies in Bali reported a CFR of 11.4% among confirmed cases. In regions like Togo, within the African meningitis belt, the CFR was reported at 7%, highlighting the variability in outcomes depending on geographic and healthcare factors [5]. An elevated CFR associated with S. suis infection can be attributed to rapid disease progression and nonspecific early symptoms, complicating timely diagnosis and treatment [43,44]. The inflammatory response induced by S. suis, including the generation of IL-17A, can lead to significant tissue damage and disruption of the blood–brain barrier, facilitating nervous system infection [45].
Although the results did not indicate a significant association between raw pork consumption and S. suis infection, they are important in underscoring the public health risks in regions with cultural practices involving undercooked pork. We advocate for improved diagnostic approaches and effective public health strategies to mitigate the rising incidence of S. suis infections, particularly in high-risk populations. By fostering a deeper understanding of the clinical manifestations and risks associated with this infection, this study aims to contribute to better health outcomes and prevention efforts in affected communities.
5. Study Limitation
Since this study is retrospective, its limitations primarily stem from a lack of critical data, such as CSF analysis and culture results, as well as the availability of other tools to detect S. suis using RT-PCR. As it is retrospective, the study relies on the accuracy and completeness of the data in the medical record, which may introduce bias. Gaps in analysis could arise from crucial missing data regarding patient demographics, clinical specifics, or treatment outcomes. If the data were not complete, subjects were excluded. Furthermore, a small sample size may limit the generalizability of the findings to the population. We included all subjects diagnosed with suspected S. suis-associated meningitis during the designated study period for whom data were complete . Variability in data recording might result from disparate healthcare practitioners recording information differently. This potential bias could make interpreting and analyzing the data more challenging. However, the medical record team at our teaching hospital has remained consistent, ensuring a uniform approach to the record-keeping system.
The generalizability of our study is limited due to demographic and geographic factors. The study population predominantly consists of an adult age group, which may restrict the applicability of the findings to other age groups that exhibit different immune responses and clinical presentations. Additionally, the geographic limitations of the current study, where the risk factors for S. suis infection, such as a dense pig population and specific cultural attitudes, are prevalent, may also influence the results.
6. Conclusion
Although the statistical analysis is not significant, the high incidence of S. suis bacteremia among cultured subjects indicates that this study has substantial public health implications for Bali. The region's high pig density increases the risk of infection. Implementing preventive measures, such as safe pig slaughtering and proper cooking practices, can help reduce S. suis infections.
Future research should focus on diverse subpopulations; prospective cohort studies could be conducted to gain a deeper understanding of the condition. This approach will enhance the quality and completeness of the dataset, enabling more accurate outcome assessments. It will also facilitate the use of advanced diagnostic methods, such as next-generation sequencing and improved serological tests, including cerebrospinal fluid (CSF) analysis and reverse transcription–polymerase chain reaction (RT-PCR) testing.
Moreover, additional studies should explore the relationship between dietary practices and infection rates to inform public health strategies. By developing a comprehensive understanding of the epidemiology and risk factors associated with S. suis, we can address this emerging public health threat more effectively.
Author Contributions
Conceptualization: SM; data curation: TIP, RKD; formal analysis: AGP; methodology: SLD; supervision: SM; writing—original draft: SM, KS; writing—review and editing: SM.
Funding
No funding source is available to declare.
Institutional Review Board Statement
The study protocol was reviewed and approved by the Research Ethics Committee of Sanjiwani Hospital, Bali (document number 420/40268/RSU, on 19 October 2024).
Informed Consent Statement
This study was a retrospective analysis of medical records from the hospital; therefore, informed consent was not required.
Data Availability Statement
The data presented in this study are available.
Acknowledgments
We gratefully acknowledge all participants of the study.
Conflicts of Interest
The authors declare no competing interests.
References
- S. T. Hlebowicz M, Jakubowski P, “Streptococcus suis Meningitis: Epidemiology, Clinical Presentation and Treatment,” Vector Borne Zoonotic Dis, vol. 19, no. 8, pp. 557–562, 2019.
- A. Rayanakorn, B. H. Goh, L. H. Lee, T. M. Khan, and S. Saokaew, “Risk factors for Streptococcus suis infection: A systematic review and meta-analysis,” Sci. Rep., vol. 8, no. 1, pp. 1–9, 2018. [CrossRef]
- C. Neila-Ibáñez et al., “Risk factors associated with Streptococcus suis cases on pig farms in Spain,” Vet. Rec., vol. 193, no. 5, p. no, 2023. [CrossRef]
- A. van Samkar, M. C. Brouwer, C. Schultsz, A. van der Ende, and D. van de Beek, “Streptococcus suis Meningitis: A Systematic Review and Meta-analysis,” PLoS Negl. Trop. Dis., vol. 9, no. 10, pp. 1–10, 2015. [CrossRef]
- H. Tall et al., “Identification of Streptococcus suis Meningitis through Population-Based Surveillance, Togo, 2010–2014,” Emerg. Infect. Dis., vol. 22, no. 7, pp. 1262–1264, Jul. 2016. [CrossRef]
- K. Rieckmann, S.-M. Pendzialek, T. Vahlenkamp, and C. G. Baums, “A critical review speculating on the protective efficacies of autogenous Streptococcus suis bacterins as used in Europe,” Porc. Heal. Manag., vol. 6, no. 1, p. 12, Dec. 2020. [CrossRef]
- D. van de Beek, L. Spanjaard, and J. de Gans, “Streptococcus suis meningitis in the Netherlands,” J. Infect., vol. 57, no. 2, pp. 158–161, Aug. 2008. [CrossRef]
- J. Dutkiewicz et al., “Streptococcus suis: a re-emerging pathogen associated with occupational exposure to pigs or pork products. Part I – Epidemiology,” Ann. Agric. Environ. Med., vol. 24, no. 4, pp. 683–695, Dec. 2017. [CrossRef]
- P. Praphasiri et al., “Streptococcus suis Infection in Hospitalized Patients, Nakhon Phanom Province, Thailand,” Emerg. Infect. Dis., vol. 21, no. 2, pp. 345–348, Feb. 2015. [CrossRef]
- V. T. L. Huong et al., “Epidemiology, Clinical Manifestations, and Outcomes of Streptococcus suis Infection in Humans,” Emerg. Infect. Dis., vol. 20, no. 7, Jul. 2014. [CrossRef]
- E. MA et al., “Streptococcus suis infection in Hong Kong: an emerging infectious disease?,” Epidemiol. Infect., vol. 136, no. 12, pp. 1691–1697, Dec. 2008. [CrossRef]
- J. Arenas et al., “In vivo transcriptomes of Streptococcus suis reveal genes required for niche-specific adaptation and pathogenesis,” Virulence, vol. 10, no. 1, pp. 334–351, Jan. 2019. [CrossRef]
- G. Li et al., “Inhibition of suilysin activity and inflammation by myricetin attenuates Streptococcus suis virulence,” Life Sci., vol. 223, pp. 62–68, Apr. 2019. [CrossRef]
- Y. Zhu et al., “Comparative genetic analyses provide clues about capsule switching in Streptococcus suis 2 strains with different virulence levels and genetic backgrounds,” Microbiol. Res., vol. 250, p. 126814, Sep. 2021. [CrossRef]
- A. Kerdsin, M. Segura, N. Fittipaldi, and M. Gottschalk, “Sociocultural Factors Influencing Human Streptococcus suis Disease in Southeast Asia,” Foods, vol. 11, no. 9, p. 1190, Apr. 2022. [CrossRef]
- C. Zheng, M. Wei, M. Jia, and M. Cao, “Involvement of Various Enzymes in the Physiology and Pathogenesis of Streptococcus suis,” Vet. Sci., vol. 7, no. 4, p. 143, Sep. 2020. [CrossRef]
- J.-P. Auger, S. Payen, D. Roy, A. Dumesnil, M. Segura, and M. Gottschalk, “Interactions of Streptococcus suis serotype 9 with host cells and role of the capsular polysaccharide: Comparison with serotypes 2 and 14,” PLoS One, vol. 14, no. 10, p. e0223864, Oct. 2019. [CrossRef]
- A. M. Domado and J. Itable, “Streptococcus suis: Bacteremia presenting with fever, rashes, arthritis and neurologic deficits,” Androl. Gynecol. Curr. Res., vol. 05, no. 03, 2017. [CrossRef]
- K. Li et al., “Meningitis and sepsis caused by Streptococcus suis in an elderly woman: A CARE-compliant case report,” Medicine (Baltimore)., vol. 102, no. 43, p. e35780, Oct. 2023. [CrossRef]
- N. He, H. Li, and X. Zhang, “Human Streptococcus suis Infection,” in Radiology of Infectious Diseases: Volume 2, Dordrecht: Springer Netherlands, 2015, pp. 113–119. [CrossRef]
- D. T. N. Ho et al., “Risk Factors of Streptococcus suis Infection in Vietnam. A Case-Control Study,” PLoS One, vol. 6, no. 3, p. e17604, Mar. 2011. [CrossRef]
- N. M. Susilawathi et al., “Streptococcus suis –Associated Meningitis, Bali, Indonesia, 2014–2017,” Emerg. Infect. Dis., vol. 25, no. 12, pp. 2235–2242, Dec. 2019. [CrossRef]
- I. A. Aryasa et al., “<em>Streptococcus suis</em> meningitis related to processing and consuming raw pork during Balinese tradition, <em>Mebat</em>,” Med. J. Indones., vol. 29, no. 1, pp. 88–92, Mar. 2020. [CrossRef]
- N. M. A. Tarini et al., “Misidentification of S. suis as a Zoonotic Agent,” Open Access Maced. J. Med. Sci., vol. 7, no. 14, pp. 2309–2312, Jul. 2019. [CrossRef]
- M. Scarborough and G. E. Thwaites, “The diagnosis and management of acute bacterial meningitis in resource-poor settings,” Lancet Neurol., vol. 7, no. 7, pp. 637–648, Jul. 2008. [CrossRef]
- S. K. Lehman DC, Mahon CR, Textbook of diagnostic microbiology. 2016.
- Clinical and Laboratory Standards Institute, Performance standards for antimicrobial susceptibility testing; twenty-fifth informational supplement (M100-S27). Wayne (PA): The Institute, 2017.
- H. F. L. Wertheim et al., “Streptococcus suis, an Important Cause of Adult Bacterial Meningitis in Northern Vietnam,” PLoS One, vol. 4, no. 6, p. e5973, Jun. 2009. [CrossRef]
- T. Lakshmikanth et al., “Immune system adaptation during gender-affirming testosterone treatment,” Nature, vol. 633, no. 8028, pp. 155–164, Sep. 2024. [CrossRef]
- R. R. Sharma and A. Sharma, “Meningitis: Current Understanding and Management,” in The Microbiology of Central Nervous System Infections, Elsevier, 2018, pp. 3–27. [CrossRef]
- Y. Liu, Z. Kou, X. Wang, S. Chen, R. Li, and Q. Wang, “Case report: One human Streptococcus suis infection in Shandong Province, China,” Medicine (Baltimore)., vol. 102, no. 14, p. e33491, Apr. 2023. [CrossRef]
- S. Tanabe, M. Gottschalk, and D. Grenier, “Hemoglobin and Streptococcus suis cell wall act in synergy to potentiate the inflammatory response of monocyte-derived macrophages,” Innate Immun., vol. 14, no. 6, pp. 357–363, Dec. 2008. [CrossRef]
- M.-C. Jobin, M. Gottschalk, and D. Grenier, “Upregulation of prostaglandin E2 and matrix metalloproteinase 9 production by human macrophage-like cells: Synergistic effect of capsular material and cell wall from Streptococcus suis,” Microb. Pathog., vol. 40, no. 1, pp. 29–34, Jan. 2006. [CrossRef]
- A. Viallon, E. Bothelo-Nevers, and F. Zeni, “Clinical decision rules for acute bacterial meningitis: current insights,” Open Access Emerg. Med., p. 7, Apr. 2016. [CrossRef]
- A. Fongcom, S. Pruksakorn, P. Netsirisawan, R. Pongprasert, and P. Onsibud, “Streptococcus suis infection: a prospective study in northern Thailand.,” Southeast Asian J. Trop. Med. Public Health, vol. 40, no. 3, pp. 511–517, May 2009.
- I. M. Lucke et al., “Elevated leukocyte count in cerebrospinal fluid of patients with chronic inflammatory demyelinating polyneuropathy,” J. Peripher. Nerv. Syst., vol. 23, no. 1, pp. 49–54, Mar. 2018. [CrossRef]
- M. Zeinalizadeh, M. Shadkam, P. Afarinesh Khaki, A. Abdollahi, M. Douraghi, and M. Salehi, “Cerebrospinal Fluid Analysis in Patients with Post-neurosurgical Procedures: Meningitis vs. Non-meningitis,” Iran. J. Pathol., vol. 19, no. 3, pp. 342–347, Jul. 2024. [CrossRef]
- C. O’Leary et al., “Predictive performance of cerebrospinal fluid parameters for diagnosis of meningitis in infants: a cohort study,” Arch. Dis. Child., vol. 110, pp. 209–215, 2025. [CrossRef]
- R. B. Domingues, G. B. P. Fernandes, F. B. V. de M. Leite, and C. Senne, “Performance of lactate in discriminating bacterial meningitis from enteroviral meningitis,” Rev. Inst. Med. Trop. Sao Paulo, vol. 61, 2019. [CrossRef]
- L. Manning, M. Laman, T. Mare, I. Hwaiwhanje, P. Siba, and T. M. E. Davis, “Accuracy of cerebrospinal leucocyte count, protein and culture for the diagnosis of acute bacterial meningitis: a comparative study using <scp>B</scp> ayesian latent class analysis,” Trop. Med. Int. Heal., vol. 19, no. 12, pp. 1520–1524, Dec. 2014. [CrossRef]
- A. Kerdsin, “Human Streptococcus suis Infections in Thailand: Epidemiology, Clinical Features, Genotypes, and Susceptibility,” Trop. Med. Infect. Dis., vol. 7, p. 359, 2022. [CrossRef]
- M. C. Domínguez-Punaro, U. Koedel, T. Hoegen, C. Demel, M. Klein, and M. Gottschalk, “Severe cochlear inflammation and vestibular syndrome in an experimental model of Streptococcus suis infection in mice,” Eur. J. Clin. Microbiol. Infect. Dis., vol. 31, no. 9, pp. 2391–2400, Sep. 2012. [CrossRef]
- X. Xia, X. Wang, X. Wei, J. Jiang, and J. Hu, “Methods for the detection and characterization of Streptococcus suis: from conventional bacterial culture methods to immunosensors,” Antonie Van Leeuwenhoek, vol. 111, no. 12, pp. 2233–2247, Dec. 2018. [CrossRef]
- Z. Ágoston, G. Terhes, P. Hannauer, M. Gajdács, and E. Urbán, “Fatal case of bacteremia caused by Streptococcus suis in a splenectomized man and a review of the European literature,” Acta Microbiol. Immunol. Hung., vol. 67, no. 3, pp. 148–155, Oct. 2020. [CrossRef]
- L. Xu et al., “Interleukin-17A Contributed to the Damage of Blood-CNS Barriers During Streptococcus suis Meningitis,” Mol. Neurobiol., vol. 59, no. 4, pp. 2116–2128, Apr. 2022. [CrossRef]
Figure 1.
Seasonal patterns of suspected S. suis-associated meningitis cases in tertiary hospital.

Figure 2.
Blood culture results. NA: not assessed.
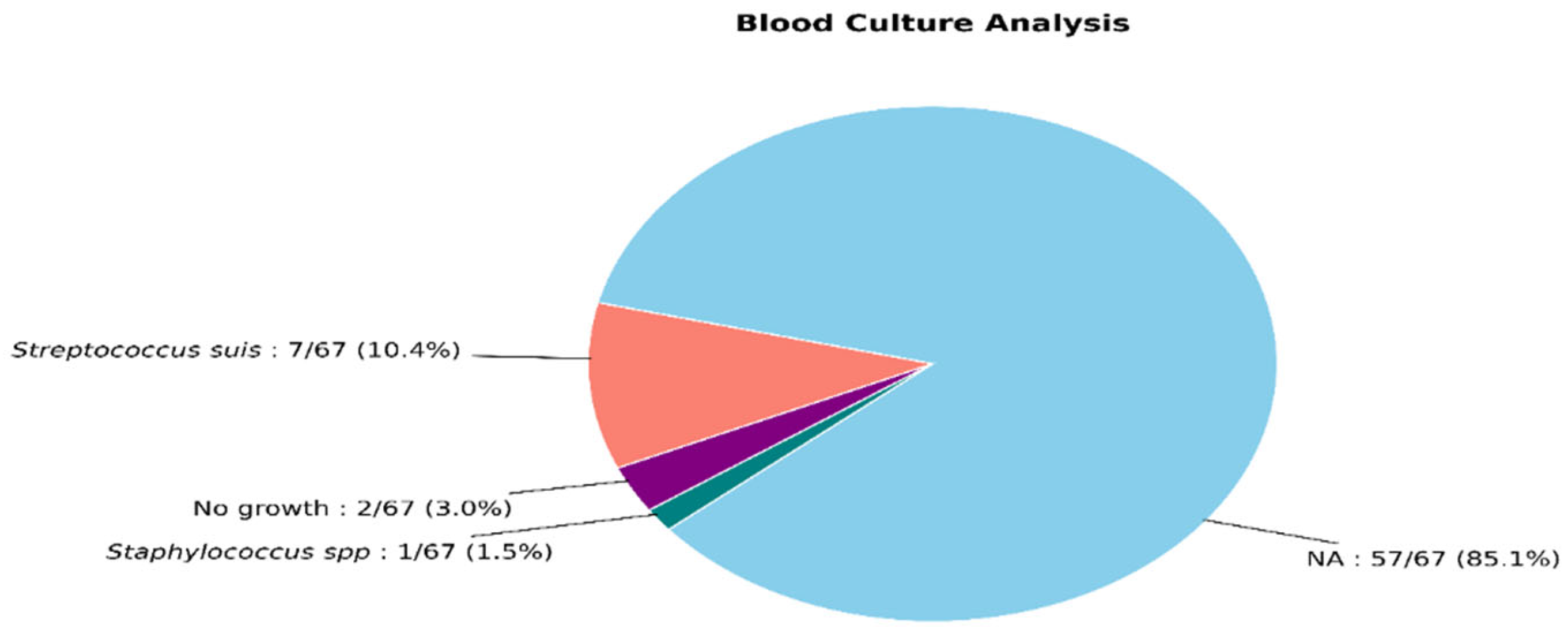

Table 1.
Demographic and clinical characteristics of subjects.
| Variables |
Total (N =67) |
Meningitis with sudden deafness (N=34) |
Meningitis without sudden deafness (N=33) |
p |
| Sex, N, (%) Male Female |
52 (77.7) 15 (22.4) |
27 (51.9) 7 (46.7) |
25 (48.1) 8 (53.3) |
0.474# |
| Age, (year), mean ±SD | 53.8 (14.9) | 53.7 (16.9) | 53.8 (12.9) | 0.965$ |
| Fever onset (day), mean ±SD | 2.8 (1.4) | 2.9 (1.6) | 2.6 (1.3) | 0.335$ |
| Length of stay (days), mean ±SD | 11.4 (3.8) | 11.4 (3.4) | 11.4 (4.3) | 0.044$ |
| Raw pork consumption, N (%) | 30 (44.8) | 17 (56.7) | 13 (43.3) | 0.151# |
| Sign and symptoms, N, (%) Headache Convulsion Ataxia Vomiting Hemiparesis Neck rigidity Mental state disturbance Septic arthritis |
66 (98.5) 8 (11.9) 4 (58.1) 63 (94) 6 (9) 67 (100) 43 (64.2) 9 (13.4) |
33 (50) 4 (50) 2 (50) 31 (49.2) 2 (33.3) 34 (50.7) 19 (44.2) 4 (44.4) |
33 (50) 4 (50) 2 (50) 32 (58.8) 4 (66.7) 33 (49.3) 24 (55.8) 5 (55.6) |
0.507* 0.628* 0.682* 0.318* 0.322* NA 0.151# 0.480* |
| ICU treatment | 3 ( 4.5) | 0 | 3 (100) | 0.114* |
| Outcome Survival |
64 (95.5) |
33 (51.6) |
31 (48.4) |
0.489* |
$The independent t-test was used to compare the groups. # The chi-square test was used to compare the groups. *Fisher’s exact test; significance value at p < 0.05. NA: not assessed.
Table 2.
Laboratory results of the subjects at admission.
|
Total (N=67) |
Meningitis with sudden deafness (N=34) |
Meningitis without sudden deafness (N=33) |
p | |
| CBC at admission Hemoglobin (g/dL) Hematocrit (%) Leucocyte (x103/mL) Thrombocyte (x103/mL) |
13.3 (1.7)a 39.2 (5)a 13.6 (6.2)a 305 (125.3)a |
13.3 ± 1.9a 39.2 ± 5.7a 14.3 (7-38.2)b 302.9 ±130.1a |
13.3 ± 1.5a 39.2 ± 4.3a 10.9 (5.3-26.3)b 307.2 ± 122a |
NA NA 0.039# 0.892* |
| AST, IU/L | 47.6 (48)a | 37.5 (11-330)b | 33 (4-133)b | 0.261# |
| ALT, IU/L | 45.9 (37)a | 36 (19-224)b | 32 (13-85)b | 0.961 |
| BUN, mg/dL | 51 (9-211)a | 36.2 (22.9-188.2)b | 34.2 (16.1-65.2)b | 0.363# |
| SC, mg/dL | 41 (23.5)a | 0.7 (0.2-4.5)b | 0.7 (0.3-1.2)b | NA |
| Blood sugar, mg/dL | 138.2 (47.3)a | 125 (93-199)b | 123 (84-454)b | 0.337# |
Note: a data presented as mean (±SD), b data presented as median (minimum–maximum). *independent t-test. #Mann—Whitney test. Values are significant at p < 0.05. NA: not assessed.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



