
Submitted:
09 June 2025
Posted:
09 June 2025
You are already at the latest version
Abstract
The management of end-stage kidney disease (ESKD) poses a substantial clinical and economic challenge, characterized by a growing patient burden, rising healthcare costs, and persistent unmet needs to enhance survival outcomes and quality of life. Background/Objectives: Conventional high-flux hemodialysis (HD) remains the dominant form of renal replacement therapy for ESKD but is still associated with substantial morbidity and mortality. High-volume post-dilution online hemodiafiltration (HVHDF) offers a promising alternative by enhancing convective removal of uremic toxins. Methods: We conducted a narrative review of randomized controlled trials, meta-analyses, real-world cohort studies, and registry analyses published between 2010 and 2024. Evidence was categorized into short-term, medium-term, and long-term outcomes, including hemodynamic stability, inflammation, anemia, infection risk, cardiovascular events, cognitive decline, quality of life, and survival. Results: HVHDF improves short-term outcomes by enhancing toxin clearance, stabilizing blood pressure, reducing inflammation and oxidative stress, and improving anemia management. Medium-term benefits include improved nutritional status, reduced hospitalizations related to infections, and improved neurological and immune function. Long-term data from major trials (e.g., ESHOL, CONVINCE) and large real-world studies show consistent reductions in all-cause and cardiovascular mortality, particularly with convection volumes ≥23 L/session. A clear dose-response relationship supports the clinical relevance of convection volume targets. HVHDF has also shown benefits in preserving cognitive function and enhancing health-related quality of life. Conclusions: Strong and converging evidence supports HVHDF as a superior dialysis modality. Given its survival benefits, better tolerance, and broader impact on patient outcomes, HVHDF should be considered the new standard of care in dialysis, especially in light of the recent regulatory approval of the machine that provides the ability to perform HDF in the United States.
Keywords:
Hemodiafiltration
; Clinical Outcomes
; convection volume
; anemia
; inflammation
; cognitive function
1. Introduction
Conventional hemodialysis (HD) remains the most commonly used renal replacement therapy (RRT) for patients with end-stage kidney disease (ESKD). Despite advances, conventional hemodialysis (HD) remains associated with persistently high morbidity and mortality. According to the United States Renal Data System 2024 Annual Data Report, the all-cause mortality rate among HD patients in 2022 was 145.6 per 1000 person-years, nearly unchanged from 2012 [1]. In response to these limitations, online post-dilution hemodiafiltration (HDF) and, more recently, high-volume hemodiafiltration (HVHDF) have emerged as promising alternatives [2,3,4,5]. By enhancing the clearance of middle- and large-molecular-weight uremic toxins and improving treatment tolerance, HVHDF has been associated with better clinical outcomes. Over two decades of comparative research have confirmed that HDF—particularly with convection volumes of≥23 L/session—delivers meaningful clinical advantages [2,3,6,7]. Recent reviews have summarized these benefits (Table 1) [8,9,10,11,12]. This manuscript provides a critical synthesis of the clinical evidence supporting HDF, specifically focusing on HVHDF. Outcomes are reviewed across three temporal dimensions: Short-term, medium-term, and long-term outcomes, to deliver a comprehensive, evidence-based perspective supporting the broader adoption of HVHDF in clinical practice. Its increasing uptake in Europe and recent regulatory approval in the United States underscore its growing clinical relevance.
2. Materials and Methods
This review presents a structured narrative synthesis of clinical outcomes associated with online HDF compared to conventional high-flux hemodialysis, focusing on adult patients with ESKD. It includes a critical appraisal of peer-reviewed published articles on randomized controlled trials (RCTs), meta-analyses and individual patient data (IPD) meta-analyses, registry studies, and large-scale real-world evidence (RWE). Outcomes were stratified into three domains: Short-term intermediate outcomes, medium-term clinical endpoints, and long-term hard outcomes. A targeted literature search was conducted using PubMed/MEDLINE, Embase, and Cochrane Library databases to identify English-language articles published between January 2010 and December 2024. Search terms included: “hemodiafiltration,” “high-flux hemodialysis,” “convection volume,” “mortality,” “anemia,” “inflammation,” and “quality of life.” Additional references were identified through citation tracking and expert consultation. Eligible studies included RCTs, Individual patient data (IPD) meta-analyses, registry-based observational studies and real-world cohort analyses reporting clinical outcomes (morbidity, mortality, quality of life, or biochemical parameters). Exclusion criteria were non-comparative case series, pediatric populations, and studies lacking defined treatment parameters (e.g., undefined convection volumes).
3. Short-Term Intermediate Outcomes
HDF offers several physiological and biochemical advantages over conventional HD, particularly in terms of solute clearance efficiency.
3.1. Enhanced Toxin Clearance
Enhanced toxin clearance: In 2003, the European Uremic Toxins working group classified uremic toxins based into three categories based on physicochemical properties affecting dialytic removal [13,14,15]: Small water-soluble compounds (WSCs, <500 Da), Middle molecular weight substances (MMWs, 0.5–40 kDa), and Protein-bound uremic toxins (PBUTs). By combining diffusion and convection, HVHDF enhances clearance across all solute classes, notably: small solutes (e.g., urea, creatinine, and phosphate): HVHDF enhances urea (60 Da) removal with efficacy proportional to substitution volume [16,17,18,19,20,21]. The DOPPS study showed superior Kt/V urea in patients receiving 15–24.9 L/session of substitution fluid versus those on standard HD [17]. Optimized HVHDF prescription, utilizing automated ultrafiltration and substitution control, achieves higher clearances of small- and middle-molecule clearance without increasing dialysis fluid consumption thus improving both efficiency and environmental sustainability [22]. Phosphate (95 Da): Clearance is increased by 15–20%, potentially reducing phosphate binder use [23,24,25,26,27,28,29]. However, the impact on predialysis serum phosphate is modest (<15%) influenced by rebound kinetics and improved appetite in HDF-treated patients [10,28,30,31]. Middle and large molecule clearance: HVHDF significantly enhances the removal of MMWs such as β2-microglobulin (β2M) and tends to improve the elimination of protein-bound uremic toxins (PBUTs), which are poorly removed by HD but are associated with inflammation and cardiovascular risk. Table 2 summarizes representative of MMWs toxins and PBTUs, for which increased clearance with HDF vs high flux has been demonstrated, along with their clinical relevance.
3.2. Improved Hemodynamic Stability
Efforts to enhance outcomes in chronic dialysis patients increasingly emphasize reducing intradialytic and peridialytic hemodynamic instability. Intradialytic hypotension (IDH), which was once considered benign, is now recognized as a serious clinical event. Both symptomatic and subclinical IDH episodes contribute to myocardial stunning, hypoperfusion of vital organs (e.g., brain, gut, and kidneys), and are associated with: symptomatic distress, reduced dialysis efficacy, increased vascular access thrombosis, loss of residual kidney function, cardiovascular events, and higher mortality risks [61]. These adverse outcomes result largely from repeated organ hypoperfusion and cumulative tissue and organ injury [62,63,64].
Numerous studies, including several RCTs, show that HVHDF is associated with a lower incidence of IDH compared to conventional HD, independently of sodium balance effects [31,65,66,67,68,69]. HDF addresses multiple mechanisms contributing to hemodynamic instability [70,71]: (a) Sodium handling and the Gibbs–Donnan effect: High convective transport during HVHDF, balanced by online substitution fluid, induces a mild hypertonic gradient. Albumin binding and Donnan effect reduce sodium concentration in the ultrafiltrate, raising plasma osmolality and enhancing plasma vascular refilling from the interstitial space. This supports effective volemia and stabilizes blood pressure during dialysis [70,72,73]. Despite large substitution volumes, sodium mass balance is well preserved [74] , with no evidence of fluid overload or dysnatremia [68]. In a multicenter cohort study, Chazot et al. confirmed that there is no increased risk of volume overload with post-dilution HVHDF [75]. However, improved sodium balance alone does not explain the hemodynamic benefits observed with HDF compared to high-flux HD [9,76]. (b) Endothelial effects of substitution fluid: The use of isotonic bicarbonate-buffered substitution fluid, with superior hemocompatibility, may stabilize endothelial function, support vascular tone, and facilitate plasma refilling, thereby contributing to improved hemodynamic stability [8,77,78]. (c) Thermal balance: Heat loss from the extracorporeal circuit causes mild core cooling, which has been linked to better blood pressure stability during dialysis [67,79]. This benefit diminishes under isothermic conditions, suggesting additional mechanisms, particularly endothelial modulation, are involved [80]. (d) Inflammatory modulation: Ultrapure dialysate and sterile substitution fluid reduce systemic inflammation more effectively than high-flux HD [57,81,82]. While inflammation is implicated in intradialytic hypotension (IDH), the direct causal relationship remains speculative. (e) Supportive and indirect factors: HVHDF is associated with improved anemia management [83,84,85], better nutritional status [85,86], enhanced physical functioning [87], [86,88,89,90] and preservation of residual kidney function [91]. These benefits may indirectly enhance cardiovascular resilience and overall hemodynamic tolerance.
Supporting evidence from recent studies. While early RCTs showed mixed results, as highlighted by the European Dialysis (EuDial) Working Group, newer studies and analyses with better methodology suggest a protective effect of HDF on IDH [92,93]. These limitations have been addressed in a recent study using real-world data. Target emulated study (Zoccali et al.): using real-world data from 4,072 incident HD patients, the study showed HDF modifies the relationship between dialysis and IDH risk, acting as a mitigating factor, despite not being explicitly designed to assess IDH [92]. The HOLLANT study showed that HVHDF significantly reduced IDH compared to conventional HD, providing better intradialytic blood pressure stability [93]. Italian Convective Study (Locatelli et al,): HDF reduced symptomatic IDH by 51% (p<0.001), outperforming hemofiltration and HD. Predialysis systolic blood pressure increased significantly in HDF patients, reflecting enhanced vascular stability [11,12,65]. In brief, HVHDF improves intradialytic hemodynamic stability through multiple complementary mechanisms: osmotic-driven plasma refilling, endothelial effects, thermal balance modulation, and reduced inflammation. Recent well-controlled studies increasingly support its role in preventing IDH, systemic stress, and enhancing cardiovascular protection.
3.3. Reduction of Intradialytic Cramps
Intradialytic muscle cramps are a frequent and distressing complication of HD, affecting 33–86% of patients with ESKD and occurring in 5–20% of sessions [94,95,96]. These painful events arise toward the end of a session, potentially leading to premature termination, compromised dialysis adequacy, and diminished quality of life [97]. The pathophysiology is multifactorial and not fully elucidated, but key contributors include Intradialytic hypotension (IDH), excessive ultrafiltration rates (UFRs), inaccurate dry weight assessment, altered plasma osmolality and perfusion, electrolyte imbalances [98,99,100,101]. Additional contributors may include vitamin deficiencies, elevated serum leptin, and increased intact parathyroid hormone (iPTH) levels [102]. HDF has been associated with a lower incidence of muscle cramps in select patient populations. Both observational and interventional studies, such as those by Karkar et al. and Morena et al., reported a significant reduction in cramp frequency among adult and elderly HDF patients undergoing HVHDF [43,68]. Despite these encouraging findings, the current evidence base is limited, and further well-designed studies are needed to confirm HVHDF’s superiority in cramp prevention.
3.4. Reduction in Inflammation and Oxidative Stress
Each HD session exposes the patient’s blood to the extracorporeal circuit, triggering the endothelial barrier and initiating a cascade of mechanical and biochemical triggers that contribute to enhancing oxidative stress and systemic inflammation. This process begins with vascular access puncture and is sustained by blood-membrane interaction, which activates coagulation and immune pathways, including complement activation, contributing to systemic inflammatory responses and oxidative damage [103,104]. HVHDF has shown superior anti-inflammatory effects compared to conventional HD, due to: use of ultrapure dialysate, biocompatible membranes, improved hemodynamic stability, enhanced anemia management, and superior clearance of middle and large molecular weight solutes, including cytokines and other inflammatory mediators [57,81,82]. HVHDF significantly reduces systemic inflammatory markers, including C-reactive protein (CRP), interleukin-6 (IL-6), tumor necrosis factor-alpha, soluble CD40 ligand, pentraxin, advanced glycation end products, and complement activation products [15,23,34,49,57,81,82,105,106,107,108,109]. Additionally, HVHDF downregulates proinflammatory monocyte subsets (CD14+/CD16+) and reduces dendritic cell maturation, effects particularly pronounced in diabetic patients, possibly due to improved autonomic regulation and reduced sympathetic activation [110,111]Although large-scale head-to-head trials remain limited, HDF's anti-inflammatory and antioxidative effects likely contribute to its documented cardiovascular and survival benefits, supporting its preferential use in patients with a high inflammatory burden.
3.5. Improved Anemia Management
HVHDF offers significant advantages in optimizing anemia management in patients with ESKD, surpassing conventional HD through a multifactorial approach [12] that include: Enhanced removal of middle and large molecular weight uremic toxins; reduced systemic inflammation and oxidative stress; improved iron metabolism; more efficient phosphate control; prolonged red blood cell survival. HDF offers a multifaceted approach to improving treatment outcomes and reducing dependence on pharmacological interventions more efficiently than conventional HD [18,112,113,114,115,116,117]. HDF effectively clears larger uremic molecules, which are known to inhibit erythroid progenitor cells. HDF promotes more efficient erythropoiesis by clearing uremic toxins that inhibit erythroid progenitor proliferation [118,119,120], including burst-forming unit–erythroid (BFU-E) suppression factors [121]. Simultaneously, HDF reduces systemic inflammation by lowering circulating interleukin-6 and C-reactive protein levels, decreasing hepcidin synthesis [122,123]. The resulting hepcidin suppression enhances iron mobilization and utilization, reducing functional iron deficiency and the need for both erythropoiesis-stimulating agents (ESAs) and intravenous iron and supporting a more sustained hematological response [124,125]. Clinical evidence, including the REDERT trial and large cohort analyses, confirms that patients on HVHDF demonstrate lower ESA resistance indices and reduced hepcidin levels compared to those on conventional HD [83,84]. This supports a mechanistic link between improved iron metabolism and reduced pharmacologic dependency.
Additional benefits of HDF include more effective phosphate removal, leading to better control of secondary hyperparathyroidism, a known contributor to ESA resistance and bone marrow suppression. Moreover, HDF has been shown to prolong red blood cell (RBC) survival, thereby stabilizing hemoglobin levels and reducing hemolysis-associated anemia [126,127].
The combined use of HDF with long-acting intravenous ESAs seems to benefit anemia management by reducing the Erythropoietin Resistance Index [8]. However, large-scale RCTs are needed to conclusively determine the magnitude of HDF’s benefit for anemia in ESKD. Overall, HVHDF appears particularly advantageous for patients with inflammation-related ESA resistance, positioning it as a preferred modality for optimizing anemia management in ESKD patients [12].
3.6. Preservation of Residual Kidney Function
HVHDF may better preserve residual kidney function compared to conventional HD, primarily through improved hemodynamic stability and reduction of micro-inflammation [91,128]. The use of ultrapure dialysate and biocompatible membranes has been associated with sustained urine output, with outcomes potentially comparable to those seen in peritoneal dialysis. However, while physiologically plausible, this benefit remains theoretical, as robust confirmation from large-scale RCTs or observational studies is still lacking. Further research is needed to determine the long-term effects of HDF's on residual kidney function.
3.7. Reduction in Skin Hyperpigmentation
Online HDF has been associated with a significant decrease in skin hyperpigmentation among patients with ESKD, likely due to its superior clearance of β2-microglobulin and other pigmentary middle-molecular-weight toxins (e.g., melanin). Lin et al. reported improved skin pigmentation in ESKD patients with increased and more frequent HDF, though without objective colorimetric assessment [129]. Moon et al. subsequently demonstrated that HDF significantly reduced skin pigmentation compared to low-flux HD, identifying HDF as an independent predictor of decreased melanin index in the forehead region [130]. Shibata et al. confirmed that HD patients exhibited darker skin than healthy controls, and those on online HDF experienced notable skin lightening, coinciding with a reduction in β2M levels [131]. These findings suggest that MMW accumulation contributes to uremic skin changes and that HDF offers a dermatological benefit beyond traditional uremia management.
4. Middle-Term Intermediate Outcomes
Over the course of months to years, HDF demonstrates sustained clinical benefits, improving patient well-being and reducing dialysis-related complications.
4.1. ß2-Microglobulin Amyloidosis and Joint Symptoms Control
HDF offers superior removal and lower circulating levels of β2M compared to conventional hemodialysis, especially when high convection volumes are delivered [36,37,38,39,40,41]. This enhanced clearance is associated with a reduced risk of dialysis-related amyloidosis (DRA), manifesting as carpal tunnel syndrome, bone cysts, and joint pain [11,132]. Since β2M clearance increases with convection volume [37,133], HVHDF remains the most effective modality for its removal. Importantly, DRA also contributes to systemic complications, including cardiovascular disease and autonomic dysfunction [39,134,135]. The combined use of ultrapure dialysate, biocompatible membranes, and effective convective clearance facilitates these improvements [11,136]. HVHDF is particularly indicated in patients with β2M levels above 27 mg/L or symptomatic DRA [10]. Clinical improvement in joint mobility and pain relief is frequently reported after switching from HD to HVHDF [10,137], supporting its utility of HVHDF in advanced amyloidosis and improving quality of life.
4.2. Improved Nutritional Status
HVHDF is consistently associated with better nutritional outcomes in ESKD patients. Observational studies show increased appetite, higher protein intake, and preservation of lean body mass [11,85,138]. Compared to high-flux HD, patients on HVHDF show improved body cell mass and nutritional markers [85,86]. A key mechanism is the superior clearance of pro-inflammatory and anorexigenic middle molecules, particularly leptin, which is elevated in dialysis patients and contributes to appetite suppression and inflammation [44,45,139]. By mitigating the Malnutrition-Inflammation Complex Syndrome (MICS), characterized by protein-energy wasting, inflammation, and elevated IL-6, TNF-α, and IL-1β. By interrupting this cycle, HVHDF supports the better maintenance of serum albumin and prealbumin levels, reduces muscle catabolism, and improves functional capacity, especially in patients with inflammatory cachexia [140,141].[142]. Although HVHDF may induce mild losses of amino acids, water-soluble vitamins, and micronutrients, these can typically be corrected with oral supplementation [11,143,144].
4.3. Reduced Infection Risk
Infectious complications are a leading cause of morbidity and the second most common cause of death in ESKD patients after cardiovascular disease [145,146]. This elevated risk stems from uremia-induced immune dysfunction, characterized by impaired innate and adaptive immunity due to the accumulation of middle and large-molecular-weight uremic toxins [141,142,147,148,149]. Additional factors include advanced age, diabetes, central venous catheter use, hypoalbuminemia, comorbidities, inadequate hygiene practices, and latent disease [150,151,152,153,154,155]. HVHDF offers a promising strategy to reduce infection risk by enhancing the clearance of immune-impairing uremic toxins [53]. Its superior hemodynamic stability may also reduce episodes of intestinal ischemia and bacterial translocation, an underrecognized pathway for systemic infection in dialysis patients [7]. [156] [157]. HVHDF is associated with stronger vaccine-induced immune responses than conventional HD. Studies show more sustained seroprotection and higher lymphocyte proliferation in response to influenza A vaccination [10,158] and higher, more durable antibody titers after SARS-CoV-2 vaccination [10,159,160,161,162]. Robust clinical data support these immunological benefits. The ESHOL study demonstrated a 55% reduction in infection-related mortality and a 22% reduction in infection-related hospitalizations in HVHDF group compared to high-flux HD [10,31]. Similarly, the CONVINCE trial showed a lower hazard ratio for infection-related death in patients treated with HVHDF (HR 0.69; 95% CI, 0.49–0.96), including COVID-19 related deaths [2]. A meta-analysis by Vernooij et al., pooling data from five randomized controlled trials (n = 4153 patients), reported that patients receiving convection volumes ≥23 L/session had a 49% lower risk of infection-related mortality compared to HD (adjusted HR 0.51; 95% CI, 0.28–0.93) [3].
4.4. Cardiovascular Benefits
Growing evidence supports the role of HVHDF in reducing all-cause mortality and cardiovascular mortality in ESKD patients [8]. The pathogenesis of cardiovascular disease in this population is driven by chronic inflammation, oxidative stress, and the retention of uremic toxins, which accelerates vascular aging, promotes arterial stiffness, impairs endothelial function, and contributes to vascular calcification [8]. HVHDF mitigates these mechanisms through both direct and indirect effects: Direct cardiovascular effects include reduced intradialytic hypotension, enhanced hemodynamic stability (independent of sodium balance), improved cardiac remodeling, and attenuated left ventricular hypertrophy [57,65,66,67,74,76,163]. HVHDF also improves endothelial function, reduces arterial stiffness, slows the progression of atherosclerosis, and lowers systemic inflammation and oxidative stress [81,82,164,165,166,167]. Moreover, HVHDF may lower sympathetic overactivity and reduce arrhythmogenic risk [168,169]. Indirect effects contributing to cardiovascular health include better anemia control [83,84,85], improved nutritional status [85,86], increased physical activity [87], enhanced quality of life [86,88,89,90] and preservation of residual kidney function [91].
4.4. Peripheral Neuropathy Improvements
Peripheral neuropathy is the most common long-term neurological complication in ESKD, typically presenting as symmetrical, distal sensorimotor neuropathy predominantly affecting the lower limbs. Symptoms include paresthesia, sensory loss, reduced reflexes, muscle weakness, insomnia, irritability, pruritus, and restless legs syndrome (RLS) [170,171,172,173]. The pathogenesis involves the accumulation of neurotoxic middle molecules, such as indoxyl sulfate, p-cresyl sulfate, β2-microglobulin, PTH, along with [174,175,176] oxidative stress [176], leading to demyelination and axonal degeneration. Risk factors include prolonged dialysis duration, suboptimal dialysis dose, diabetes, micronutrient deficiencies, and advanced age. Preliminary evidence suggests that HVHDF may slow the neuropathy progression by enhancing the clearance of neurotoxic middle MW toxins [177]. Patients transitioning from HD to HDF have reported improvements in pruritus [88,178,179] and RLS symptoms. In a report by Sakurai et al., two patients with refractory RLS experienced marked improvement with HVHDF, which correlated with achieving an α1-microglobulin (α1-MG) removal rate ≥ 40%. [56]. Notably, symptoms recurred upon switching back to conventional HD or when the α1-MG clearance declined [56], suggesting that α1-MG may serve as a therapeutic target marker in RLS management and that HVHDF may offer a promising non-pharmacologic therapy in these cases. However, the FINESSE RCT conducted in Australia did not confirm these findings, which reported no significant differences in neuropathy progression between HDF and HD [180]. Nonetheless, methodological limitations (nerve conduction measurements) and potential biases may have influenced the outcomes. While symptomatic relief is achievable with HVHDF, particularly for pruritus and RLS, structural nerve damage from longstanding uremia remains largely irreversible [180], underscoring the importance of early intervention and the start of HVHDF.
4.5. Cognitive and Quality of Life Benefits
Cognitive impairment and reduced health-related quality of life (HRQoL) are highly prevalent yet frequently underrecognized complications in the dialysis population [181]. Cognitive defects span memory, executive function, attention, visuospatial skills, emotional well-being, social engagement, and physical performance. (176). Prevalence estimates vary, but moderate to severe impairments affect up to 70% of patients over 55 years old receiving HD, and significant deficits can occur at any age [182,183,184]. The etiology is multifactorial, involving traditional risk factors (e.g., aging, depression, vascular disease), ESKD-related contributors (e.g., chronic inflammation, oxidative stress, mineral bone disorders, anemia), and dialysis-specific mechanisms such as recurrent intradialytic hypotension, cerebral hypoperfusion, and the accumulation of neurotoxic solutes [185,186,187,188,189,190,191,192,193,194,195,196]. These synergistic insults lead to cerebral ischemia, white matter damage, and progressive neurocognitive decline. HVHDF may mitigate these effects by improving intradialytic hemodynamic stability, enhancing clearance of neurotoxic middle-molecular-weight molecules, and reducing systemic inflammation and oxidative stress. The CONVINCE trial demonstrated a significantly slower rate of cognitive decline in patients treated with HVHDF compared to those receiving high-flux HD [4], with the greatest preservation seen in cognitive function scores. These findings suggest a potential neuroprotective role of HVHDF. Beyond cognition, HVHDF has shown positive impacts on broader quality of life measures. The HDFit trial reported increased physical activity, reflected by higher daily step counts, among patients on HDF, although no change was noted in sleep duration [87,197]. In CONVINCE, HRQoL was assessed using the PROMIS® across eight domains, including physical and cognitive function, fatigue, pain interference, and social participation [2,4]. While cognitive function declined in both treatment arms over time, the decline was significantly attenuated in the HVHDF group. In addition to cognitive outcomes, improvements were noted in physical function, social participation, and pain interference. These findings are further supported by the EUDIAL, which recognizes HVHDF as potentially superior to high-flux HD for cognitive preservation [7].
Taken together, these data highlight that HVHDF improves survival and physiological parameters and helps preserve cognitive function, physical independence, and overall well-being in patients with ESKD.
5. Long-term outcomes
While the short—and medium-term benefits of HDF are important from the patient perspective, the cumulative physiological advantages of HVHDF translate into superior long-term outcomes compared to High-Flow HD (Figure 1).
5.1. Randomized Controlled Trials
Numerous RCTs, meta-analyses, and RWE studies have evaluated the effect of HDF/HVHDF on all-cause mortality compared to conventional HD. While RCTs remain the gold standard for establishing causal efficacy, their generalizability is often limited by strict inclusion criteria, protocol standardization, and intensive monitoring, conditions that do not reflect the complexity of routine ESKD care [198,199,200,201,202,203,204]. In contrast, RWE, derived from observational cohorts, registries, and clinical databases, provides valuable complementary insights. As emphasized by Canaud et al., RWE is essential for assessing treatment effectiveness, scalability, and safety in real-world practice [11]. This is particularly relevant in ESKD, where patient heterogeneity, comorbidities, and care variability complicate the application of RCT findings to daily nephrology [11,12]. Integrating both RCT and RWE is thus essential for a comprehensive assessment of HDF's clinical value. Recent evidence demonstrates that HDF, when delivered with high convection volumes (>23 L/session), improves survival compared to High Flux HD. In 2025, the EuDial published a consensus statement synthesizing findings from systematic reviews and expert evaluations of both adult and pediatric populations [7]. The panels issued 22 consensus statements addressing survival, cardiovascular events, health-related quality of life, and biochemical markers. A key conclusion statement is that HVHDF is associated with reduced all-cause and cardiovascular mortality, particularly in patients with favorable clinical profiles and reliable vascular access. The benefit is most consistently observed in patients dialyzed via arteriovenous fistula, underscoring the importance of both patient selection and optimized convection dosing [7].
The mortality benefit of post-dilution HDF has been evaluated in six major European RCTs, Italian Convective Study, CONTRAST, Turkish, ESHOL, FRENCHIE, and CONVINCE, with outcomes largely influenced by the level of convection volume achieved. [2,31,65,68,205,206] (Table 3).
While the CONTRAST (2010) and Turkish (2013) trials did not demonstrate an overall survival advantage of HDF compared to conventional HD, both reported significant mortality reductions in subgroup analyses, achieving higher convection volume. In CONTRAST, patients receiving > 21.9 L/session had a 38% lower risk of death (HR = 0.62; 95% CI: 0.41–0.83)[205]. Similarly, the Turkish trial reported a 29% mortality reduction for those with substitution volumes > 17.4 L/session (HR = 0.71; 95% CI: 0.07–0.71; p = 0.01) [206]. The ESHOL trial (2013), a multicenter, open-label RCT, provided robust evidence supporting the survival benefit of post-dilution HVHDF. Among 906 prevalent ESKD patients, HDF reduced all-cause mortality by 30% (HR = 0.70; 95% CI: 0.53–0.92; p = 0.01) and cardiovascular mortality by 33% (HR = 0.67; 95% CI: 0.44–1.02; p = 0.06) [31]. Post hoc analyses revealed a dose-response relationship: patients achieving 23–25 L/session had a 40% lower mortality (HR = 0.60; 95% CI: 0.39–0.90), while those exceeding 25 L/session saw a 45% reduction (HR = 0.55; 95% CI: 0.34–0.84) [31]. By contrast, the FRENCHIE trial (2017) found no significant difference in mortality between HD and post-dilution HDF groups, likely due to lower achieved convection volumes compared to ESHOL [68]. The CONVINCE trial (2023), a large, multicenter RCT funded by the European Union’s Horizon 2020 program, enrolled 1,360 ESKD patients from 61 dialysis centers across eight European countries (Spain, Romania, Germany, Portugal, France, Hungary, the Netherlands, and the UK) [2]. Patients randomized to post-dilution HVHDF (≥ 23 L/session) experienced a 23% reduction in all-cause mortality (HR = 0.77; 95% CI: 0.65–0.93) after a median follow-up of 30 months, while also achieving higher dialysis dose (spKt/V) compared to the HD group [2]. Notably, HVHDF was associated with significant improvements in health-related quality of life [4].
The ongoing “High-Volume Hemodiafiltration vs. High-Flux Hemodialysis Registry Trial (H4RT in the UK is designed further to assess the clinical benefits of HVHDF versus HD [207]. This registry-based RCT targets convection volumes > 23 L per session in post-dilution mode [207], with results expected by 2026.
5.2. Meta-analyses: Expanding the Case for HVHDF
Before 2016, several meta-analyses assessed convective dialysis techniques, but lacked a specific focus on HDF [11]. Instead, they broadly compared convection-based therapies, including hemofiltration (diafiltration), acetate-free biofiltration (AFB), and paired filtration dialysis (PFD), and provided limited insights into the impact of convective volume on outcomes [69,164,169,208] .European Pooling Project (2016). The first major meta-analysis targeting HDF was the European Pooling Project, an individual patient data (IPD) meta-analysis, combining data from four randomized controlled trials (CONTRAST, Turkish, ESHOL, and FRENCHIE; N = 2,793) comparing post-dilution HDF (n = 1,400) with conventional HD (n = 1,393) to assess long-term clinical outcomes [6]. Over a median follow-up of 2.5 years, patients receiving >23 L per 1.73 m² body surface area per session experienced a 22% reduction in all-cause mortality (HR = 0.78; 95% CI: 0.62–0.98) and a 31% reduction in cardiovascular mortality (HR = 0.69; 95% CI: 0.47–1.00), after adjustment for key covariates [6]. Comprehensive IPD meta-analysis by Vernooij et al. (2024). More recently, Vernooij et al. conducted an updated a pooled IPD analysis of five European RCTs (CONTRAST, Turkish, ESHOL, FRENCHIE, and CONVINCE; N =4,153; 2,083 HDF; 2,070 HD) [3]. HVHDF was associated with a 16% reduction in all-cause mortality (HR=0.84 (95% CI: 0.74–0.95) and a 22% reduction in cardiovascular mortality (HR = 0.78; 95% CI: 0.64–0.96) [3]. Subgroup analyses suggested enhanced survival in patients aged ≥65 years, those without diabetes or cardiovascular disease, and individuals with dialysis vintage ≥30 months. Conversely, no significant mortality benefit was observed in younger patients (<65 years), those with diabetes, or patients with biochemical markers of malnutrition (e.g., serum albumin levels < 4.0 g/dL). Although no significant interaction was found, a clear dose-response relationship emerged: greater convection volume was associated with lower mortality risk [3].
5.3. Reinforcement from Real World Evidence. Dose-response across observational studies
Several RWE studies corroborate the survival benefit of HDF seen in RCTs and meta-analyses, consistently showing a dose-response association between substitution/convective volume and relative survival rate [17,209,210,211,212,213,214,215,216,217]. Benefits are most pronounced when substitution/convective volumes exceed 21/23 L per session, respectively, and have exhibited the most favorable effect on mortality outcomes [209,210,211,212,213,218].
In 2006, the DOPPS Study, first reported improved survival with substitution volumes greater than 15L [17]. The French National Registry showed reduced all-cause (HR = 0.84) and cardiovascular mortality (HR = 0.73) in HDF patients [219]. The Australia and New Zealand Dialysis and Transplant Registry (ANZDATA) reported similar findings; HR for all-cause was 0.79 in Australia and 0.88 in New Zealand, with cardiovascular mortality significantly lower in the Australian HDF cohort (HR 0.78) [214]. The Japanese Society for Dialysis Therapy (JSDT) registry supports these results, indicating that predilution HDF was associated with a reduction in all-cause mortality (HR 0.83), particularly when high-volume convective doses were employed [215]. In Latin America, propensity score-matched cohort studies from Brazil and Colombia demonstrated substantial mortality reductions (HR =0.71 and O.45, respectively) among HDF-treated patients [220,221].
Large-scale contemporary RWE: Zhang et al (2025). A landmark RWE by Zhang et al. assessed the real-world effectiveness of HVHDF compared to high-flux HD on 85,117 adult patients treated in FMC NephroCare clinics across 23 countries between 2019 and 2022 (Bosnia and Herzegovina, Croatia, Czech Republic, Estonia, Finland, France, Hungary, Italy, Kazakhstan, Kyrgyzstan, Netherlands, Poland, Portugal, Romania, Russia, Serbia, Slovakia, Slovenia, South Africa, Spain, Sweden, Turkey, and Ukraine) [222]. The analysis confirmed a 22% reduction in all-cause mortality with HDF versus HD; a 30% mortality reduction for those receiving HVHDF (≥ 23 L convection volume per session); a 31% lower risk of cardiovascular mortality for HDF [222]. Consistent benefits across subgroups regardless of age, dialysis vintage, diabetes, or cardiovascular disease status [222]. Sustained survival advantage during the COVID-19 pandemic, regardless of infection status [222]. Robustness of findings confirmed via sensitivity analyses, adjusting for demographics, clinical parameters, and country-level variation [222].
The growing body of evidence from RCTs, IPD meta-analyses, and real-world studies consistently supports the mortality benefit of HVHDF, particularly when adequate convection volumes are delivered [17,209,210,211,212,213,214,215,216,217]. A grade, dose response relationship between convection volume and survival underscores the clinical importance of achieving high convective efficiency in routine practice [209,210,211,212,213,218].
6. Conclusion
Post-dilution HVHDF represents a significant advancement in renal replacement therapy, consistently demonstrating superior outcomes compared to high-flux HD. When delivered with adequate convection volumes (≥23 L/session), HVHDF is associated with significant reductions in all-cause and cardiovascular mortality, as confirmed by recent randomized controlled trials, individual patient-level meta-analyses, and large-scale real-world evidence. Importantly, the clinical benefits of HVHDF extend beyond survival. HVHDF offers broad clinical advantages, including improved hemodynamic stability, enhanced toxin removal, inflammation control, and better anemia management, all of which contribute to a superior quality of life. These effects are dose-dependent and consistent across heterogenous patient populations, underscoring the importance of optimized delivery and automated system implementation. Given the robustness and consistency of evidence, HVHDF should be considered not merely as an alternative to high-flux HD but as a preferred standard of care. Wider implementation, especially in regions where uptake has been limited or has not yet started, will require targeted education, infrastructure, and technological support, as well as integration into outcome-driven clinical frameworks. Future efforts should focus on embedding HVHDF into personalized, value-based care models, emphasizing survival, symptom control, and patient-reported outcomes. Policymakers, payers, and advocacy groups must acknowledge HVHDF's clinical and economic value and collaborate to ensure equitable access, appropriate reimbursement models, and sustainable implementation at scale.
Author Contributions
Conceptualization S.S.; methodology B.C.; writing S.S.; review and editing S.S., F.W.M., B.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
S.S. and F.W.M. are Fresenius Medical Care employees; B.C. has no conflicts of interest.
References
- United States Renal Data System. 2024 USRDS Annual Data Report: Epidemiology of kidney disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, , 2024.
- Blankestijn, P.J.; Vernooij, R.W.M.; Hockham, C.; Strippoli, G.F.M.; Canaud, B.; Hegbrant, J.; Barth, C.; Covic, A.; Cromm, K.; Cucui, A.; et al. Effect of Hemodiafiltration or Hemodialysis on Mortality in Kidney Failure. N Engl J Med 2023, 389, 700-709. [CrossRef]
- Vernooij, R.W.M.; Hockham, C.; Strippoli, G.; Green, S.; Hegbrant, J.; Davenport, A.; Barth, C.; Canaud, B.; Woodward, M.; Blankestijn, P.J.; et al. Haemodiafiltration versus haemodialysis for kidney failure: an individual patient data meta-analysis of randomised controlled trials. Lancet (London, England) 2024, 404, 1742-1749. [CrossRef]
- Rose, M.; Fischer, F.H.; Liegl, G.; Strippoli, G.F.M.; Hockham, C.; Vernooij, R.W.M.; Barth, C.; Canaud, B.; Covic, A.; Cromm, K.; et al. The CONVINCE randomized trial found positive effects on quality of life for patients with chronic kidney disease treated with hemodiafiltration. Kidney Int 2024, 106, 961-971. [CrossRef]
- Strippoli, G.F.M.; Green, S.C. Actioning the findings of hard endpoint clinical trials as they emerge in the realm of chronic kidney disease care: a review and a call to action. Clin Kidney J 2024, 17, sfae035. [CrossRef]
- Peters, S.A.; Bots, M.L.; Canaud, B.; Davenport, A.; Grooteman, M.P.; Kircelli, F.; Locatelli, F.; Maduell, F.; Morena, M.; Nubé, M.J.; et al. Haemodiafiltration and mortality in end-stage kidney disease patients: a pooled individual participant data analysis from four randomized controlled trials. Nephrol Dial Transplant 2016, 31, 978-984. [CrossRef]
- Battaglia, Y.; Shroff, R.; Meijers, B.; Nistor, I.; Alfano, G.; Franssen, C.; Luyckx, V.; Liakopoulos, V.; Mantovani, A.; Baciga, F.; et al. Haemodiafiltration versus high-flux haemodialysis - a Consensus Statement from the EuDial Working Group of the ERA. Nephrol Dial Transplant 2025. [CrossRef]
- Canaud, B.; Blankestijn, P.J.; Grooteman, M.P.C.; Davenport, A. Why and how high volume hemodiafiltration may reduce cardiovascular mortality in stage 5 chronic kidney disease dialysis patients? A comprehensive literature review on mechanisms involved. Semin Dial 2022, 35, 117-128. [CrossRef]
- Lang, T.; Zawada, A.M.; Theis, L.; Braun, J.; Ottillinger, B.; Kopperschmidt, P.; Gagel, A.; Kotanko, P.; Stauss-Grabo, M.; Kennedy, J.P.; et al. Hemodiafiltration: Technical and Medical Insights. Bioengineering (Basel) 2023, 10. [CrossRef]
- Pedreros-Rosales, C.; Jara, A.; Lorca, E.; Mezzano, S.; Pecoits-Filho, R.; Herrera, P. Unveiling the Clinical Benefits of High-Volume Hemodiafiltration: Optimizing the Removal of Medium-Weight Uremic Toxins and Beyond. Toxins (Basel) 2023, 15. [CrossRef]
- Canaud, B.; Strippoli, G.; Davenport, A. High-Volume Hemodiafiltration Versus High-Flux Hemodialysis: A Narrative Review for the Clinician. J Clin Med 2025, 14. [CrossRef]
- Stuard, S.; Maddux, F.W. High-Volume Hemodiafiltration: Expanding the Evidence Beyond Randomized Trials—A Critical Perspective on the 2025 EuDial Consensus. Journal of Clinical Medicine 2025, 14, 3174.
- Vanholder, R.; De Smet, R.; Glorieux, G.; Argilés, A.; Baurmeister, U.; Brunet, P.; Clark, W.; Cohen, G.; De Deyn, P.P.; Deppisch, R.; et al. Review on uremic toxins: classification, concentration, and interindividual variability. Kidney Int 2003, 63, 1934-1943. [CrossRef]
- Neirynck, N.; Vanholder, R.; Schepers, E.; Eloot, S.; Pletinck, A.; Glorieux, G. An update on uremic toxins. International urology and nephrology 2013, 45, 139-150. [CrossRef]
- Rosner, M.H.; Reis, T.; Husain-Syed, F.; Vanholder, R.; Hutchison, C.; Stenvinkel, P.; Blankestijn, P.J.; Cozzolino, M.; Juillard, L.; Kashani, K.; et al. Classification of Uremic Toxins and Their Role in Kidney Failure. Clin J Am Soc Nephrol 2021, 16, 1918-1928. [CrossRef]
- Canaud, B.; Bosc, J.Y.; Leblanc, M.; Garred, L.J.; Vo, T.; Mion, C. Evaluation of high-flux hemodiafiltration efficiency using an on-line urea monitor. Am J Kidney Dis 1998, 31, 74-80. [CrossRef]
- Canaud, B.; Bragg-Gresham, J.L.; Marshall, M.R.; Desmeules, S.; Gillespie, B.W.; Depner, T.; Klassen, P.; Port, F.K. Mortality risk for patients receiving hemodiafiltration versus hemodialysis: European results from the DOPPS. Kidney Int 2006, 69, 2087-2093. [CrossRef]
- Pedrini, L.A.; De Cristofaro, V.; Comelli, M.; Casino, F.G.; Prencipe, M.; Baroni, A.; Campolo, G.; Manzoni, C.; Coli, L.; Ruggiero, P.; et al. Long-term effects of high-efficiency on-line haemodiafiltration on uraemic toxicity. A multicentre prospective randomized study. Nephrol Dial Transplant 2011, 26, 2617-2624. [CrossRef]
- Shinzato, T.; Kobayakawa, H.; Maeda, K. Comparison of various treatment modes in terms of beta 2-microglobulin removal: hemodialysis, hemofiltration, and push/pull HDF. Artif Organs 1989, 13, 66-70. [CrossRef]
- Vanholder, R.; Meert, N.; Schepers, E.; Glorieux, G. From uremic toxin retention to removal by convection: do we know enough? Contrib Nephrol 2008, 161, 125-131. [CrossRef]
- Santoro, A.; Ferramosca, E.; Mancini, E.; Monari, C.; Varasani, M.; Sereni, L.; Wratten, M. Reverse mid-dilution: new way to remove small and middle molecules as well as phosphate with high intrafilter convective clearance. Nephrol Dial Transplant 2007, 22, 2000-2005. [CrossRef]
- Canaud, B.; Gagel, A.; Peters, A.; Maierhofer, A.; Stuard, S. Does online high-volume hemodiafiltration offer greater efficiency and sustainability compared with high-flux hemodialysis? A detailed simulation analysis anchored in real-world data. Clin Kidney J 2024, 17, sfae147. [CrossRef]
- Canaud, B. The early years of on-line HDF: how did it all start? How did we get here? Contrib Nephrol 2011, 175, 93-109. [CrossRef]
- Lornoy, W.; De Meester, J.; Becaus, I.; Billiouw, J.M.; Van Malderen, P.A.; Van Pottelberge, M. Impact of convective flow on phosphorus removal in maintenance hemodialysis patients. J Ren Nutr 2006, 16, 47-53. [CrossRef]
- Zehnder, C.; Gutzwiller, J.P.; Renggli, K. Hemodiafiltration--a new treatment option for hyperphosphatemia in hemodialysis patients. Clin Nephrol 1999, 52, 152-159.
- Penne, E.L.; van der Weerd, N.C.; van den Dorpel, M.A.; Grooteman, M.P.; Levesque, R.; Nube, M.J.; Bots, M.L.; Blankestijn, P.J.; ter Wee, P.M.; Investigators, C. Short-term effects of online hemodiafiltration on phosphate control: a result from the randomized controlled Convective Transport Study (CONTRAST). Am J Kidney Dis 2010, 55, 77-87. [CrossRef]
- Davenport, A.; Gardner, C.; Delaney, M.; Pan Thames Renal Audit, G. The effect of dialysis modality on phosphate control : haemodialysis compared to haemodiafiltration. The Pan Thames Renal Audit. Nephrol Dial Transplant 2010, 25, 897-901. [CrossRef]
- Daugirdas, J.T. Comparison of measured vs kinetic-model predicted phosphate removal during hemodialysis and hemodiafiltration. Nephrol Dial Transplant 2022, 37, 2522-2527. [CrossRef]
- Movilli, E.; Camerini, C.; Gaggia, P.; Poiatti, P.; Pola, A.; Viola, B.F.; Zubani, R.; Jeannin, G.; Cancarini, G. Effect of post-dilutional on-line haemodiafiltration on serum calcium, phosphate and parathyroid hormone concentrations in uraemic patients. Nephrol Dial Transplant 2011, 26, 4032-4037. [CrossRef]
- Ok, E.; Asci, G.; Toz, H.; Ok, E.S.; Kircelli, F.; Yilmaz, M.; Hur, E.; Demirci, M.S.; Demirci, C.; Duman, S.; et al. Mortality and cardiovascular events in online haemodiafiltration (OL-HDF) compared with high-flux dialysis: results from the Turkish OL-HDF Study. Nephrol Dial Transplant 2013, 28, 192-202. [CrossRef]
- Maduell, F.; Moreso, F.; Pons, M.; Ramos, R.; Mora-Macia, J.; Carreras, J.; Soler, J.; Torres, F.; Campistol, J.M.; Martinez-Castelao, A.; et al. High-efficiency postdilution online hemodiafiltration reduces all-cause mortality in hemodialysis patients. J Am Soc Nephrol 2013, 24, 487-497. [CrossRef]
- Moon, S.J.; Lee, J.E.; Kim, J.K.; Yoon, S.Y.; Kang, S.W.; Choi, K.H.; Ha, S.K.; Park, H.C. The relationship between hemodialysis modality and insulin resistance in non-diabetic hemodialysis patients. Blood purification 2015, 39, 224-229. [CrossRef]
- Chen, H.; Han, X.; Cui, Y.; Ye, Y.; Purrunsing, Y.; Wang, N. Parathyroid Hormone Fragments: New Targets for the Diagnosis and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder. Biomed Res Int 2018, 2018, 9619253. [CrossRef]
- Stein, G.; Franke, S.; Mahiout, A.; Schneider, S.; Sperschneider, H.; Borst, S.; Vienken, J. Influence of dialysis modalities on serum AGE levels in end-stage renal disease patients. Nephrol Dial Transplant 2001, 16, 999-1008. [CrossRef]
- Jørstad, S.; Smeby, L.C.; Balstad, T.; Widerøe, T.E. Generation and removal of anaphylatoxins during hemofiltration with five different membranes. Blood purification 1988, 6, 325-335. [CrossRef]
- Padrini, R.; Canova, C.; Conz, P.; Mancini, E.; Rizzioli, E.; Santoro, A. Convective and adsorptive removal of beta2-microglobulin during predilutional and postdilutional hemofiltration. Kidney Int 2005, 68, 2331-2337. [CrossRef]
- Lornoy, W.; Becaus, I.; Billiouw, J.M.; Sierens, L.; Van Malderen, P.; D'Haenens, P. On-line haemodiafiltration. Remarkable removal of beta2-microglobulin. Long-term clinical observations. Nephrol Dial Transplant 2000, 15 Suppl 1, 49-54. [CrossRef]
- Maduell, F.; del Pozo, C.; Garcia, H.; Sanchez, L.; Hdez-Jaras, J.; Albero, M.D.; Calvo, C.; Torregrosa, I.; Navarro, V. Change from conventional haemodiafiltration to on-line haemodiafiltration. Nephrol Dial Transplant 1999, 14, 1202-1207. [CrossRef]
- Roumelioti, M.E.; Trietley, G.; Nolin, T.D.; Ng, Y.H.; Xu, Z.; Alaini, A.; Figueroa, R.; Unruh, M.L.; Argyropoulos, C.P. Beta-2 microglobulin clearance in high-flux dialysis and convective dialysis modalities: a meta-analysis of published studies. Nephrol Dial Transplant 2018, 33, 542. [CrossRef]
- Locatelli, F.; Mastrangelo, F.; Redaelli, B.; Ronco, C.; Marcelli, D.; La Greca, G.; Orlandini, G. Effects of different membranes and dialysis technologies on patient treatment tolerance and nutritional parameters. The Italian Cooperative Dialysis Study Group. Kidney Int 1996, 50, 1293-1302. [CrossRef]
- Susantitaphong, P.; Tiranathanagul, K.; Katavetin, P.; Townamchai, N.; Praditpornsilpa, K.; Tungsanga, K.; Eiam-Ong, S. Efficacy of convective-controlled double high-flux hemodiafiltration versus on-line hemodiafiltration: 1-year prospective study. Blood purification 2010, 29, 35-43. [CrossRef]
- Ward, R.A.; Greene, T.; Hartmann, B.; Samtleben, W. Resistance to intercompartmental mass transfer limits beta2-microglobulin removal by post-dilution hemodiafiltration. Kidney Int 2006, 69, 1431-1437. [CrossRef]
- Guedes, M.; Vernooij, R.W.M.; Davenport, A.; Kuhlmann, M.K.; Aregger, F.; Pecoits-Filho, R. Clinical performance, intermediate and long-term outcomes of high-volume hemodiafiltration in patients with kidney failure. Semin Dial 2022, 35, 420-426. [CrossRef]
- Widjaja, A.; Kielstein, J.T.; Horn, R.; von zur Muhlen, A.; Kliem, V.; Brabant, G. Free serum leptin but not bound leptin concentrations are elevated in patients with end-stage renal disease. Nephrol Dial Transplant 2000, 15, 846-850. [CrossRef]
- Kim, S.; Oh, K.H.; Chin, H.J.; Na, K.Y.; Kim, Y.S.; Chae, D.W.; Ahn, C.; Han, J.S.; Kim, S.; Joo, K.W. Effective removal of leptin via hemodiafiltration with on-line endogenous reinfusion therapy. Clin Nephrol 2009, 72, 442-448. [CrossRef]
- Kuo, H.L.; Chou, C.Y.; Liu, Y.L.; Yang, Y.F.; Huang, C.C.; Lin, H.H. Reduction of pro-inflammatory cytokines through hemodiafiltration. Ren Fail 2008, 30, 796-800. [CrossRef]
- Morena, M.; Creput, C.; Bouzernidj, M.; Rodriguez, A.; Chalabi, L.; Seigneuric, B.; Lauret, C.; Bargnoux, A.S.; Dupuy, A.M.; Cristol, J.P. Randomised trial on clinical performances and biocompatibility of four high-flux hemodialyzers in two mode treatments: hemodialysis vs post dilution hemodiafiltration. Sci Rep 2019, 9, 18265. [CrossRef]
- Suzuki, S.; Moriyama, K.; Hara, Y.; Hinoue, T.; Kato, Y.; Hasegawa, D.; Kuriyama, N.; Nakamura, T.; Komatsu, S.; Yamashita, C.; et al. Comparison of myoglobin clearance in three types of blood purification modalities. Ther Apher Dial 2021, 25, 401-406. [CrossRef]
- Canaud, B.; Wizemann, V.; Pizzarelli, F.; Greenwood, R.; Schultze, G.; Weber, C.; Falkenhagen, D. Cellular interleukin-1 receptor antagonist production in patients receiving on-line haemodiafiltration therapy. Nephrol Dial Transplant 2001, 16, 2181-2187. [CrossRef]
- Krieter, D.H.; Falkenhain, S.; Chalabi, L.; Collins, G.; Lemke, H.D.; Canaud, B. Clinical cross-over comparison of mid-dilution hemodiafiltration using a novel dialyzer concept and post-dilution hemodiafiltration. Kidney Int 2005, 67, 349-356. [CrossRef]
- Bourguignon, C.; Chenine, L.; Bargnoux, A.S.; Leray-Moragues, H.; Canaud, B.; Cristol, J.P.; Morena, M. Hemodiafiltration improves free light chain removal and normalizes kappa/lambda ratio in hemodialysis patients. J Nephrol 2016, 29, 251-257. [CrossRef]
- Lukkanalikitkul, E.; Kidkaem, H.; Phonrat, M.; Prathompong, P.; Anutrakulchai, S. A randomized trial comparing medium cut-off membrane dialyzers with online hemodiafiltration for uremic toxins clearance in hemodialysis patients. Sci Rep 2025, 15, 5467. [CrossRef]
- Ward, R.A.; Schmidt, B.; Hullin, J.; Hillebrand, G.F.; Samtleben, W. A comparison of on-line hemodiafiltration and high-flux hemodialysis: a prospective clinical study. J Am Soc Nephrol 2000, 11, 2344-2350. [CrossRef]
- Ronco, C. Hemodiafiltration: Technical and Clinical Issues. Blood purification 2015, 40 Suppl 1, 2-11. [CrossRef]
- Meijers, B.K.; Van Kerckhoven, S.; Verbeke, K.; Dehaen, W.; Vanrenterghem, Y.; Hoylaerts, M.F.; Evenepoel, P. The uremic retention solute p-cresyl sulfate and markers of endothelial damage. Am J Kidney Dis 2009, 54, 891-901. [CrossRef]
- Sakurai, K.; Saito, T.; Hosoya, H.; Kurihara, Y.; Yamauchi, F. Therapeutic effect of high-efficiency online hemodiafiltration for recurrent restless legs syndrome in dialysis patients. J Artif Organs 2020, 23, 296-301. [CrossRef]
- den Hoedt, C.H.; Bots, M.L.; Grooteman, M.P.; van der Weerd, N.C.; Mazairac, A.H.; Penne, E.L.; Levesque, R.; ter Wee, P.M.; Nube, M.J.; Blankestijn, P.J.; et al. Online hemodiafiltration reduces systemic inflammation compared to low-flux hemodialysis. Kidney Int 2014, 86, 423-432. [CrossRef]
- Patrier, L.; Dupuy, A.M.; Granger Vallee, A.; Chalabi, L.; Morena, M.; Canaud, B.; Cristol, J.P. FGF-23 removal is improved by on-line high-efficiency hemodiafiltration compared to conventional high flux hemodialysis. J Nephrol 2013, 26, 342-349. [CrossRef]
- Nishizawa, Y.; Hosoda, Y.; Horimoto, A.; Omae, K.; Ito, K.; Higuchi, C.; Sakura, H.; Nitta, K.; Ogawa, T. Fibroblast growth factor 23 (FGF23) level is associated with ultrafiltration rate in patients on hemodialysis. Heart Vessels 2021, 36, 414-423. [CrossRef]
- Lima, J.D.; Guedes, M.; Rodrigues, S.D.; Florido, A.C.S.; Moreno-Amaral, A.N.; Barra, A.B.; Canziani, M.E.; Cuvello-Neto, A.; Poli-de-Figueiredo, C.E.; Pecoits-Filho, R.; et al. High-volume hemodiafiltration decreases the pre-dialysis concentrations of indoxyl sulfate and p-cresyl sulfate compared to hemodialysis: a post-hoc analysis from the HDFit randomized controlled trial. J Nephrol 2022, 35, 1449-1456. [CrossRef]
- Stuard, S.; Ridel, C.; Cioffi, M.; Trost-Rupnik, A.; Gurevich, K.; Bojic, M.; Karibayev, Y.; Mohebbi, N.; Marcinkowski, W.; Kupres, V. Hemodialysis Procedures for Stable Incident and Prevalent Patients Optimize Hemodynamic Stability, Dialysis Dose, Electrolytes, and Fluid Balance. Journal of Clinical Medicine 2024, 13, 3211.
- Bleyer, A.J.; Russell, G.B.; Satko, S.G. Sudden and cardiac death rates in hemodialysis patients. Kidney Int 1999, 55, 1553-1559. [CrossRef]
- Flythe, J.E.; Xue, H.; Lynch, K.E.; Curhan, G.C.; Brunelli, S.M. Association of mortality risk with various definitions of intradialytic hypotension. J Am Soc Nephrol 2015, 26, 724-734. [CrossRef]
- Burton, J.O.; Jefferies, H.J.; Selby, N.M.; McIntyre, C.W. Hemodialysis-induced repetitive myocardial injury results in global and segmental reduction in systolic cardiac function. Clin J Am Soc Nephrol 2009, 4, 1925-1931. [CrossRef]
- Locatelli, F.; Altieri, P.; Andrulli, S.; Bolasco, P.; Sau, G.; Pedrini, L.A.; Basile, C.; David, S.; Feriani, M.; Montagna, G.; et al. Hemofiltration and hemodiafiltration reduce intradialytic hypotension in ESRD. J Am Soc Nephrol 2010, 21, 1798-1807. [CrossRef]
- Donauer, J.; Schweiger, C.; Rumberger, B.; Krumme, B.; Bohler, J. Reduction of hypotensive side effects during online-haemodiafiltration and low temperature haemodialysis. Nephrol Dial Transplant 2003, 18, 1616-1622. [CrossRef]
- Sande, F.M.V.; Kooman, J.P.; Konings, C.J.; Leunissen, K.M.L. Thermal effects and blood pressure response during postdilution hemodiafiltration and hemodialysis: the effect of amount of replacement fluid and dialysate temperature. J Am Soc Nephrol 2001, 12, 1916-1920. [CrossRef]
- Morena, M.; Jaussent, A.; Chalabi, L.; Leray-Moragues, H.; Chenine, L.; Debure, A.; Thibaudin, D.; Azzouz, L.; Patrier, L.; Maurice, F.; et al. Treatment tolerance and patient-reported outcomes favor online hemodiafiltration compared to high-flux hemodialysis in the elderly. Kidney Int 2017, 91, 1495-1509. [CrossRef]
- Wang, A.Y.; Ninomiya, T.; Al-Kahwa, A.; Perkovic, V.; Gallagher, M.P.; Hawley, C.; Jardine, M.J. Effect of hemodiafiltration or hemofiltration compared with hemodialysis on mortality and cardiovascular disease in chronic kidney failure: a systematic review and meta-analysis of randomized trials. Am J Kidney Dis 2014, 63, 968-978. [CrossRef]
- Kawanishi, H. Is There Enough Evidence to Prove That Hemodiafiltration Is Superior? Blood purification 2018, 46, 3-6. [CrossRef]
- Sars, B.; van der Sande, F.M.; Kooman, J.P. Intradialytic Hypotension: Mechanisms and Outcome. Blood purification 2020, 49, 158-167. [CrossRef]
- Gross, M.; Gagel, A.; Maierhofer, A. The Donnan equilibrium is still valid in high-volume HDF. The International journal of artificial organs 2024, 47, 867-875. [CrossRef]
- Waniewski, J.; Pietribiasi, M.; Pstras, L. Calculation of the Gibbs-Donnan factors for multi-ion solutions with non-permeating charge on both sides of a permselective membrane. Sci Rep 2021, 11, 22150. [CrossRef]
- Rodriguez, A.; Morena, M.; Bargnoux, A.S.; Chenine, L.; Leray-Moragues, H.; Cristol, J.P.; Canaud, B. Quantitative assessment of sodium mass removal using ionic dialysance and sodium gradient as a proxy tool: Comparison of high-flux hemodialysis versus online hemodiafiltration. Artif Organs 2021, 45, E280-E292. [CrossRef]
- Chazot, C.; Deleuze, S.; Fadel, B.; Hebibi, H.; Jean, G.; Levannier, M.; Puyoo, O.; Attaf, D.; Stuard, S.; Canaud, B. Is high-volume post-dilution haemodiafiltration associated with risk of fluid volume imbalance? A national multicentre cross-sectional cohort study. Nephrology Dialysis Transplantation 2019, 34, 2089-2095. [CrossRef]
- La Milia, V.; Ravasi, C.; Carfagna, F.; Alberghini, E.; Baragetti, I.; Buzzi, L.; Ferrario, F.; Furiani, S.; Barbone, G.S.; Pontoriero, G. Sodium removal and plasma tonicity balance are not different in hemodialysis and hemodiafiltration using high-flux membranes. J Nephrol 2019, 32, 461-469. [CrossRef]
- Myburgh, J.A.; Mythen, M.G. Resuscitation fluids. N Engl J Med 2013, 369, 2462-2463. [CrossRef]
- Oberleithner, H. Vascular endothelium: a vulnerable transit zone for merciless sodium. Nephrol Dial Transplant 2014, 29, 240-246. [CrossRef]
- Daugirdas, J.T. Lower cardiovascular mortality with high-volume hemodiafiltration: a cool effect? Nephrol Dial Transplant 2016, 31, 853-856. [CrossRef]
- Maggiore, Q.; Pizzarelli, F.; Sisca, S.; Zoccali, C.; Parlongo, S.; Nicolo, F.; Creazzo, G. Blood temperature and vascular stability during hemodialysis and hemofiltration. Trans Am Soc Artif Intern Organs 1982, 28, 523-527.
- Agbas, A.; Canpolat, N.; Caliskan, S.; Yilmaz, A.; Ekmekci, H.; Mayes, M.; Aitkenhead, H.; Schaefer, F.; Sever, L.; Shroff, R. Hemodiafiltration is associated with reduced inflammation, oxidative stress and improved endothelial risk profile compared to high-flux hemodialysis in children. PLoS One 2018, 13, e0198320. [CrossRef]
- Filiopoulos, V.; Hadjiyannakos, D.; Metaxaki, P.; Sideris, V.; Takouli, L.; Anogiati, A.; Vlassopoulos, D. Inflammation and oxidative stress in patients on hemodiafiltration. Am J Nephrol 2008, 28, 949-957. [CrossRef]
- Marcelli, D.; Bayh, I.; Merello, J.I.; Ponce, P.; Heaton, A.; Kircelli, F.; Chazot, C.; Di Benedetto, A.; Marelli, C.; Ladanyi, E.; et al. Dynamics of the erythropoiesis stimulating agent resistance index in incident hemodiafiltration and high-flux hemodialysis patients. Kidney Int 2016, 90, 192-202. [CrossRef]
- Panichi, V.; Scatena, A.; Rosati, A.; Giusti, R.; Ferro, G.; Malagnino, E.; Capitanini, A.; Piluso, A.; Conti, P.; Bernabini, G.; et al. High-volume online haemodiafiltration improves erythropoiesis-stimulating agent (ESA) resistance in comparison with low-flux bicarbonate dialysis: results of the REDERT study. Nephrol Dial Transplant 2015, 30, 682-689. [CrossRef]
- Molina, P.; Vizcaino, B.; Molina, M.D.; Beltran, S.; Gonzalez-Moya, M.; Mora, A.; Castro-Alonso, C.; Kanter, J.; Avila, A.I.; Gorriz, J.L.; et al. The effect of high-volume online haemodiafiltration on nutritional status and body composition: the ProtEin Stores prEservaTion (PESET) study. Nephrol Dial Transplant 2018, 33, 1223-1235. [CrossRef]
- Aichi, M.; Kuragano, T.; Iwasaki, T.; Ookawa, S.; Masumoto, M.; Mizusaki, K.; Yahiro, M.; Kida, A.; Nanami, M. Hemodiafiltration Improves Low Levels of Health-Related Quality Of Life (Qol) and Nutritional Conditions of Hemodialysis Patients. ASAIO journal (American Society for Artificial Internal Organs : 1992) 2022, 68, 297-302. [CrossRef]
- Pecoits-Filho, R.; Larkin, J.; Poli-de-Figueiredo, C.E.; Cuvello-Neto, A.L.; Barra, A.B.L.; Goncalves, P.B.; Sheth, S.; Guedes, M.; Han, M.; Calice-Silva, V.; et al. Effect of hemodiafiltration on measured physical activity: primary results of the HDFIT randomized controlled trial. Nephrol Dial Transplant 2021, 36, 1057-1070. [CrossRef]
- Karkar, A.; Abdelrahman, M.; Locatelli, F. A Randomized Trial on Health-Related Patient Satisfaction Level with High-Efficiency Online Hemodiafiltration versus High-Flux Dialysis. Blood purification 2015, 40, 84-91. [CrossRef]
- Hazim, A.; Adarmouch, L.; Eloury, A.; Aasfara, J.; Asly, M.; Slassi, I. Hemodialysis-related headache: Still a challenge in 2020? Effect of conventional versus online hemodiafiltration from a study in Casablanca, Morocco. Artif Organs 2021, 45, 602-607. [CrossRef]
- Kantartzi, K.; Panagoutsos, S.; Mourvati, E.; Roumeliotis, A.; Leivaditis, K.; Devetzis, V.; Passadakis, P.; Vargemezis, V. Can dialysis modality influence quality of life in chronic hemodialysis patients? Low-flux hemodialysis versus high-flux hemodiafiltration: a cross-over study. Ren Fail 2013, 35, 216-221. [CrossRef]
- Vilar, E.; Fry, A.C.; Wellsted, D.; Tattersall, J.E.; Greenwood, R.N.; Farrington, K. Long-term outcomes in online hemodiafiltration and high-flux hemodialysis: a comparative analysis. Clin J Am Soc Nephrol 2009, 4, 1944-1953. [CrossRef]
- Zoccali, C.; Tripepi, G.; Carioni, P.; Fu, E.L.; Dekker, F.; Stel, V.; Jager, K.J.; Mallamaci, F.; Hymes, J.L.; Maddux, F.W.; et al. Antihypertensive Drug Treatment and the Risk for Intrahemodialysis Hypotension. Clin J Am Soc Nephrol 2024, 19, 1310-1318. [CrossRef]
- Rootjes, P.A.; Chaara, S.; de Roij van Zuijdewijn, C.L.M.; Nubé, M.J.; Wijngaarden, G.; Grooteman, M.P.C. High-Volume Hemodiafiltration and Cool Hemodialysis Have a Beneficial Effect on Intradialytic Hemodynamics: A Randomized Cross-Over Trial of Four Intermittent Dialysis Strategies. Kidney Int Rep 2022, 7, 1980-1990. [CrossRef]
- Neal, C.R.; Resnikoff, E.; Unger, A.M. Treatment of dialysis-related muscle cramps with hypertonic dextrose. Archives of internal medicine 1981, 141, 171-173.
- McGill, R.L.; Weiner, D.E. Dialysate Composition for Hemodialysis: Changes and Changing Risk. Semin Dial 2017, 30, 112-120. [CrossRef]
- Flythe, J.E.; Hilliard, T.; Castillo, G.; Ikeler, K.; Orazi, J.; Abdel-Rahman, E.; Pai, A.B.; Rivara, M.B.; St Peter, W.L.; Weisbord, S.D.; et al. Symptom Prioritization among Adults Receiving In-Center Hemodialysis: A Mixed Methods Study. Clin J Am Soc Nephrol 2018, 13, 735-745. [CrossRef]
- Punj, S.; Enaam, A.; Marquez, A.; Atkinson, A.J., Jr.; Batlle, D. A Survey on Dialysis-Related Muscle Cramping and a Hypothesis of Angiotensin II on Its Pathophysiology. Kidney Int Rep 2020, 5, 924-926. [CrossRef]
- Chillar, R.K.; Desforges, J.F. Muscular cramps during maintenance haemodialysis. Lancet (London, England) 1972, 2, 285. [CrossRef]
- Kolb, J.; Kitzler, T.M.; Tauber, T.; Morris, N.; Skrabal, F.; Kotanko, P. Proto-dialytic cardiac function relates to intra-dialytic morbid events. Nephrol Dial Transplant 2011, 26, 1645-1651. [CrossRef]
- Basile, C.; Lomonte, C. A neglected issue in dialysis practice: haemodialysate. Clin Kidney J 2015, 8, 393-399. [CrossRef]
- Beladi Mousavi, S.S.; Zeraati, A.; Moradi, S.; Mousavi, M.B. The effect of gabapentin on muscle cramps during hemodialysis: A double-blind clinical trial. Saudi J Kidney Dis Transpl 2015, 26, 1142-1148. [CrossRef]
- Noordzij, M.; Boeschoten, E.W.; Bos, W.J.; Dekker, F.W.; Bossuyt, P.M.; Krediet, R.T.; Korevaar, J.C.; Group, N.S. Disturbed mineral metabolism is associated with muscle and skin complaints in a prospective cohort of dialysis patients. Nephrol Dial Transplant 2007, 22, 2944-2949. [CrossRef]
- Campo, S.; Lacquaniti, A.; Trombetta, D.; Smeriglio, A.; Monardo, P. Immune System Dysfunction and Inflammation in Hemodialysis Patients: Two Sides of the Same Coin. J Clin Med 2022, 11. [CrossRef]
- Kokubo, K.; Kurihara, Y.; Kobayashi, K.; Tsukao, H.; Kobayashi, H. Evaluation of the Biocompatibility of Dialysis Membranes. Blood purification 2015, 40, 293-297. [CrossRef]
- Ağbaş, A.; Canpolat, N.; Çalışkan, S.; Yılmaz, A.; Ekmekçi, H.; Mayes, M.; Aitkenhead, H.; Schaefer, F.; Sever, L.; Shroff, R. Hemodiafiltration is associated with reduced inflammation, oxidative stress and improved endothelial risk profile compared to high-flux hemodialysis in children. PLoS One 2018, 13, e0198320. [CrossRef]
- Fischer, D.C.; Smith, C.; De Zan, F.; Bacchetta, J.; Bakkaloglu, S.A.; Agbas, A.; Anarat, A.; Aoun, B.; Askiti, V.; Azukaitis, K.; et al. Hemodiafiltration Is Associated With Reduced Inflammation and Increased Bone Formation Compared With Conventional Hemodialysis in Children: The HDF, Hearts and Heights (3H) Study. Kidney Int Rep 2021, 6, 2358-2370. [CrossRef]
- Santoro, A.; Mancini, E. Is hemodiafiltration the technical solution to chronic inflammation affecting hemodialysis patients? Kidney International 2014, 86, 235-237. [CrossRef]
- Cavallari, C.; Dellepiane, S.; Fonsato, V.; Medica, D.; Marengo, M.; Migliori, M.; Quercia, A.D.; Pitino, A.; Formica, M.; Panichi, V.; et al. Online Hemodiafiltration Inhibits Inflammation-Related Endothelial Dysfunction and Vascular Calcification of Uremic Patients Modulating miR-223 Expression in Plasma Extracellular Vesicles. J Immunol 2019, 202, 2372-2383. [CrossRef]
- Carracedo, J.; Merino, A.; Nogueras, S.; Carretero, D.; Berdud, I.; Ramírez, R.; Tetta, C.; Rodríguez, M.; Martín-Malo, A.; Aljama, P. On-line hemodiafiltration reduces the proinflammatory CD14+CD16+ monocyte-derived dendritic cells: A prospective, crossover study. J Am Soc Nephrol 2006, 17, 2315-2321. [CrossRef]
- Carracedo, J.; Merino, A.; Nogueras, S.; Carretero, D.; Berdud, I.; Ramirez, R.; Tetta, C.; Rodriguez, M.; Martin-Malo, A.; Aljama, P. On-line hemodiafiltration reduces the proinflammatory CD14+CD16+ monocyte-derived dendritic cells: A prospective, crossover study. J Am Soc Nephrol 2006, 17, 2315-2321. [CrossRef]
- Rama, I.; Llaudo, I.; Fontova, P.; Cerezo, G.; Soto, C.; Javierre, C.; Hueso, M.; Montero, N.; Martinez-Castelao, A.; Torras, J.; et al. Online Haemodiafiltration Improves Inflammatory State in Dialysis Patients: A Longitudinal Study. PLoS One 2016, 11, e0164969. [CrossRef]
- Panichi, V.; Tetta, C. The biological response to online hemodiafiltration. Contrib Nephrol 2007, 158, 194-200. [CrossRef]
- Canaud, B.; Chenine, L.; Henriet, D.; Leray, H. Online hemodiafiltration: a multipurpose therapy for improving quality of renal replacement therapy. Contrib Nephrol 2008, 161, 191-198. [CrossRef]
- Bowry, S.K.; Gatti, E. Impact of hemodialysis therapy on anemia of chronic kidney disease: the potential mechanisms. Blood purification 2011, 32, 210-219. [CrossRef]
- Bonforte, G.; Grillo, P.; Zerbi, S.; Surian, M. Improvement of anemia in hemodialysis patients treated by hemodiafiltration with high-volume on-line-prepared substitution fluid. Blood purification 2002, 20, 357-363. [CrossRef]
- Pedrini, L.A.; Comelli, M.; Ruggiero, P.; Feliciani, A.; Manfrini, V.; Cozzi, G.; Castellano, A.; Pezzotta, M.; Gatti, G.; Arazzi, M.; et al. Mixed hemodiafiltration reduces erythropoiesis stimulating agents requirement in dialysis patients: a prospective randomized study. J Nephrol 2020, 33, 1037-1048. [CrossRef]
- Lin, C.L.; Huang, C.C.; Yu, C.C.; Wu, C.H.; Chang, C.T.; Hsu, H.H.; Hsu, P.Y.; Yang, C.W. Improved iron utilization and reduced erythropoietin resistance by on-line hemodiafiltration. Blood purification 2002, 20, 349-356. [CrossRef]
- Macdougall, I.C. Role of uremic toxins in exacerbating anemia in renal failure. Kidney international. Supplement 2001, 78, S67-72. [CrossRef]
- Yamada, S.; Kataoka, H.; Kobayashi, H.; Ono, T.; Minakuchi, J.; Kawano, Y. Identification of an erythropoietic inhibitor from the dialysate collected in the hemodialysis with PMMA membrane (BK-F). Contrib Nephrol 1999, 125, 159-172. [CrossRef]
- Ayli, D.; Ayli, M.; Azak, A.; Yuksel, C.; Kosmaz, G.P.; Atilgan, G.; Dede, F.; Abayli, E.; Camlibel, M. The effect of high-flux hemodialysis on renal anemia. J Nephrol 2004, 17, 701-706.
- Aucella, F.; Scalzulli, R.P.; Vigilante, M.; Stallone, C. [The hemodiafiltration with endogenous reinfusion reduces the erythroid progenitor inhibition by uremic serum]. G Ital Nefrol 2004, 21 Suppl 30, S128-132.
- Allen, D.A.; Breen, C.; Yaqoob, M.M.; Macdougall, I.C. Inhibition of CFU-E colony formation in uremic patients with inflammatory disease: role of IFN-gamma and TNF-alpha. J Investig Med 1999, 47, 204-211.
- Panichi, V.; Rizza, G.M.; Paoletti, S.; Bigazzi, R.; Aloisi, M.; Barsotti, G.; Rindi, P.; Donati, G.; Antonelli, A.; Panicucci, E.; et al. Chronic inflammation and mortality in haemodialysis: effect of different renal replacement therapies. Results from the RISCAVID study. Nephrol Dial Transplant 2008, 23, 2337-2343. [CrossRef]
- Malyszko, J.; Malyszko, J.S.; Kozminski, P.; Mysliwiec, M. Type of renal replacement therapy and residual renal function may affect prohepcidin and hepcidin. Ren Fail 2009, 31, 876-883. [CrossRef]
- Bolasco, P.G.; Ghezzi, P.M.; Serra, A.; Corazza, L.; Murtas, S.; Mascia, M.; Cossu, M.; Ferrara, R.; Cogoni, G.; Cadinu, F.; et al. Hemodiafiltration with endogenous reinfusion with and without acetate-free dialysis solutions: effect on ESA requirement. Blood purification 2011, 31, 235-242. [CrossRef]
- Lutton, J.D.; Solangi, K.B.; Ibraham, N.G.; Goodman, A.I.; Levere, R.D. Inhibition of erythropoiesis in chronic renal failure: the role of parathyroid hormone. Am J Kidney Dis 1984, 3, 380-384. [CrossRef]
- Horl, W.H. The clinical consequences of secondary hyperparathyroidism: focus on clinical outcomes. Nephrol Dial Transplant 2004, 19 Suppl 5, V2-8. [CrossRef]
- Vilar, E.; Farrington, K. Emerging importance of residual renal function in end-stage renal failure. Semin Dial 2011, 24, 487-494. [CrossRef]
- Lin, C.L.; Huang, C.C.; Chang, C.T.; Wu, M.S.; Hung, C.C.; Chien, C.C.; Yang, C.W. Clinical improvement by increased frequency of on-line hemodialfiltration. Ren Fail 2001, 23, 193-206. [CrossRef]
- Moon, S.J.; Kim, D.K.; Chang, J.H.; Kim, C.H.; Kim, H.W.; Park, S.Y.; Han, S.H.; Lee, J.E.; Yoo, T.H.; Han, D.S.; et al. The impact of dialysis modality on skin hyperpigmentation in haemodialysis patients. Nephrol Dial Transplant 2009, 24, 2803-2809. [CrossRef]
- Shibata, M.; Nagai, K.; Usami, K.; Tawada, H.; Taniguchi, S. The quantitative evaluation of online haemodiafiltration effect on skin hyperpigmentation. Nephrol Dial Transplant 2011, 26, 988-992. [CrossRef]
- Locatelli, F.; Marcelli, D.; Conte, F.; Limido, A.; Malberti, F.; Spotti, D. Comparison of mortality in ESRD patients on convective and diffusive extracorporeal treatments. The Registro Lombardo Dialisi E Trapianto. Kidney Int 1999, 55, 286-293. [CrossRef]
- Cornelis, T.; van der Sande, F.M.; Eloot, S.; Cardinaels, E.; Bekers, O.; Damoiseaux, J.; Leunissen, K.M.; Kooman, J.P. Acute hemodynamic response and uremic toxin removal in conventional and extended hemodialysis and hemodiafiltration: a randomized crossover study. Am J Kidney Dis 2014, 64, 247-256. [CrossRef]
- Gal, R.; Korzets, A.; Schwartz, A.; Rath-Wolfson, L.; Gafter, U. Systemic distribution of beta 2-microglobulin-derived amyloidosis in patients who undergo long-term hemodialysis. Report of seven cases and review of the literature. Arch Pathol Lab Med 1994, 118, 718-721.
- Takayama, F.; Miyazaki, S.; Morita, T.; Hirasawa, Y.; Niwa, T. Dialysis-related amyloidosis of the heart in long-term hemodialysis patients. Kidney international. Supplement 2001, 78, S172-176. [CrossRef]
- Schiffl, H.; Lang, S.M.; Fischer, R. Ultrapure dialysis fluid slows loss of residual renal function in new dialysis patients. Nephrol Dial Transplant 2002, 17, 1814-1818. [CrossRef]
- Maeda, K.; Kobayakawa, H.; Fujita, Y.; Takai, I.; Morita, H.; Emoto, Y.; Miyazaki, T.; Shinzato, T. Effectiveness of push/pull hemodiafiltration using large-pore membrane for shoulder joint pain in long-term dialysis patients. Artif Organs 1990, 14, 321-327. [CrossRef]
- Paglialonga, F.; Monzani, A.; Prodam, F.; Smith, C.; De Zan, F.; Canpolat, N.; Agbas, A.; Bayazit, A.; Anarat, A.; Bakkaloglu, S.A.; et al. Nutritional and Anthropometric Indices in Children Receiving Haemodiafiltration vs Conventional Haemodialysis - The HDF, Heart and Height (3H) Study. J Ren Nutr 2023, 33, 17-28. [CrossRef]
- Mandolfo, S.; Borlandelli, S.; Imbasciati, E. Leptin and beta2-microglobulin kinetics with three different dialysis modalities. The International journal of artificial organs 2006, 29, 949-955. [CrossRef]
- Kalantar-Zadeh, K.; Kopple, J.D.; Humphreys, M.H.; Block, G. Comparing outcome predictability of markers of malnutrition-inflammation complex syndrome in haemodialysis patients. Nephrol Dial Transplant 2004, 19, 1507-1519. [CrossRef]
- Wolley, M.; Jardine, M.; Hutchison, C.A. Exploring the Clinical Relevance of Providing Increased Removal of Large Middle Molecules. Clin J Am Soc Nephrol 2018, 13, 805-814. [CrossRef]
- Haag-Weber, M.; Cohen, G.; Horl, W.H. Clinical significance of granulocyte-inhibiting proteins. Nephrol Dial Transplant 2000, 15 Suppl 1, 15-16. [CrossRef]
- Murtas, S.; Aquilani, R.; Iadarola, P.; Deiana, M.L.; Secci, R.; Cadeddu, M.; Bolasco, P. Differences and Effects of Metabolic Fate of Individual Amino Acid Loss in High-Efficiency Hemodialysis and Hemodiafiltration. J Ren Nutr 2020, 30, 440-451. [CrossRef]
- Bevier, A.; Novel-Catin, E.; Blond, E.; Pelletier, S.; Parant, F.; Koppe, L.; Fouque, D. Water-Soluble Vitamins and Trace Elements Losses during On-Line Hemodiafiltration. Nutrients 2022, 14. [CrossRef]
- Johansen, K.L.; Gilbertson, D.T.; Li, S.; Li, S.; Liu, J.; Roetker, N.S.; Ku, E.; Schulman, I.H.; Greer, R.C.; Chan, K.; et al. US Renal Data System 2023 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am J Kidney Dis 2024, 83, A8-A13. [CrossRef]
- Silberzweig, J.I. Reducing Infections in Outpatient Hemodialysis: The Impact of Human Factors. Am J Kidney Dis 2024, 84, 4-5. [CrossRef]
- Kato, S.; Chmielewski, M.; Honda, H.; Pecoits-Filho, R.; Matsuo, S.; Yuzawa, Y.; Tranaeus, A.; Stenvinkel, P.; Lindholm, B. Aspects of immune dysfunction in end-stage renal disease. Clin J Am Soc Nephrol 2008, 3, 1526-1533. [CrossRef]
- Vanholder, R.; Ringoir, S. Infectious morbidity and defects of phagocytic function in end-stage renal disease: a review. J Am Soc Nephrol 1993, 3, 1541-1554. [CrossRef]
- Vaziri, N.D.; Pahl, M.V.; Crum, A.; Norris, K. Effect of uremia on structure and function of immune system. J Ren Nutr 2012, 22, 149-156. [CrossRef]
- den Hoedt, C.H.; Grooteman, M.P.; Bots, M.L.; Blankestijn, P.J.; van der Tweel, I.; van der Weerd, N.C.; Penne, E.L.; Mazairac, A.H.; Levesque, R.; ter Wee, P.M.; et al. The Effect of Online Hemodiafiltration on Infections: Results from the CONvective TRAnsport STudy. PLoS One 2015, 10, e0135908. [CrossRef]
- Allon, M.; Radeva, M.; Bailey, J.; Beddhu, S.; Butterly, D.; Coyne, D.W.; Depner, T.A.; Gassman, J.J.; Kaufman, A.M.; Kaysen, G.A.; et al. The spectrum of infection-related morbidity in hospitalized haemodialysis patients. Nephrol Dial Transplant 2005, 20, 1180-1186. [CrossRef]
- Kaplowitz, L.G.; Comstock, J.A.; Landwehr, D.M.; Dalton, H.P.; Mayhall, C.G. A prospective study of infections in hemodialysis patients: patient hygiene and other risk factors for infection. Infect Control Hosp Epidemiol 1988, 9, 534-541. [CrossRef]
- Akmal, M. Hemodialysis in diabetic patients. Am J Kidney Dis 2001, 38, S195-199. [CrossRef]
- Hoen, B.; Paul-Dauphin, A.; Hestin, D.; Kessler, M. EPIBACDIAL: a multicenter prospective study of risk factors for bacteremia in chronic hemodialysis patients. J Am Soc Nephrol 1998, 9, 869-876. [CrossRef]
- Schild, A.F.; Perez, E.; Gillaspie, E.; Seaver, C.; Livingstone, J.; Thibonnier, A. Arteriovenous fistulae vs. arteriovenous grafts: a retrospective review of 1,700 consecutive vascular access cases. J Vasc Access 2008, 9, 231-235.
- Canaud, B.; Popa, C.; Leray-Moragues, H.; Morena-Carrere, M.; Cristol, J.P. "Can Gut Instinct Guide the Detection of Intestinal Bacterial Translocation in Dialysis Patients?". Kidney Int Rep 2025, 10, 12-16. [CrossRef]
- Rootjes, P.A.; Grooteman, M.P.C.; Budding, A.E.; Bontkes, H.J.; Wijngaarden, G.; Nube, M.J.; de Roij van Zuijdewijn, C.L.M. Randomized Trial Demonstrating No Translocation of Intact Intestinal Bacteria During Hemodialysis or Hemodiafiltration. Kidney Int Rep 2025, 10, 109-119. [CrossRef]
- Nongnuch, A.; Ngampongpan, W.; Srichatrapimuk, S.; Wongsa, A.; Thongpraphai, S.; Boonarkart, C.; Sanmeema, N.; Chittaganpitch, M.; Auewarakul, P.; Tassaneetrithep, B.; et al. Immune response to influenza vaccination in ESRD patients undergoing hemodialysis vs. hemodiafiltration. PLoS One 2020, 15, e0227719. [CrossRef]
- Chuva, T.; Santos, T.; Goncalves, F.; Costa, L.; Alves, E.; Neves, I.; Paiva, A.; Carvalho, B.; Sousa, T.; Ramalheiro, A.; et al. Humoral immunity against Covid-19 six months after the Pfizer BNT162b2 vaccine in hemodialysis patients: data from five dialysis units. Is there a protective role for hemodiafiltration in the Covid-19 pandemic? J Nephrol 2022, 35, 1543-1545. [CrossRef]
- Lioulios, G.; Fylaktou, A.; Asouchidou, D.; Xochelli, A.; Nikolaidou, V.; Stai, S.; Christodoulou, M.; Giamalis, P.; Tsouchnikas, I.; Papagianni, A.; et al. Effect of Lymphocyte Phenotypic Alterations on the Humoral Response to Vaccination Against SARS-COV-2 in Dialysis Patients. Ann Lab Med 2023, 43, 451-460. [CrossRef]
- Hebibi, H.; Edeas, M.; Cornillac, L.; Beaudreuil, S.; Achiche, J.; Attaf, D.; Saibi, S.; Chazot, C.; Ouaaz, F.; Canaud, B. SARS-CoV-2 mRNA Vaccine Immunogenicity in Hemodialysis Patients: Promising Vaccine Protection That May Be Hindered by Fluid Overload. Kidney and Dialysis 2022, 2, 44-56.
- Carrera, F.; Jacobson, S.H.; Costa, J.; Marques, M.; Ferrer, F. Better Anti-Spike IgG Antibody Response to SARS-CoV-2 Vaccine in Patients on Haemodiafiltration than on Haemodialysis. Blood purification 2023, 52, 600-608. [CrossRef]
- Czifra, A.; Pall, A.; Kulcsar, J.; Barta, K.; Kertesz, A.; Paragh, G.; Lorincz, I.; Jenei, Z.; Agarwal, A.; Zarjou, A.; et al. Hemodialysis and hemodiafiltration differently modulate left ventricular diastolic function. BMC Nephrol 2013, 14, 76. [CrossRef]
- Mostovaya, I.M.; Blankestijn, P.J.; Bots, M.L.; Covic, A.; Davenport, A.; Grooteman, M.P.; Hegbrant, J.; Locatelli, F.; Vanholder, R.; Nube, M.J.; et al. Clinical evidence on hemodiafiltration: a systematic review and a meta-analysis. Semin Dial 2014, 27, 119-127. [CrossRef]
- Ohtake, T.; Oka, M.; Ishioka, K.; Honda, K.; Mochida, Y.; Maesato, K.; Moriya, H.; Hidaka, S.; Kobayashi, S. Cardiovascular protective effects of on-line hemodiafiltration: comparison with conventional hemodialysis. Ther Apher Dial 2012, 16, 181-188. [CrossRef]
- Charitaki, E.; Davenport, A. Does hemodiafiltration reduce vascular stiffness measured by aortic pulse wave velocity compared with high-flux hemodialysis? Hemodialysis international. International Symposium on Home Hemodialysis 2014, 18, 391-395. [CrossRef]
- Shroff, R.; Smith, C.; Ranchin, B.; Bayazit, A.K.; Stefanidis, C.J.; Askiti, V.; Azukaitis, K.; Canpolat, N.; Agbas, A.; Aitkenhead, H.; et al. Effects of Hemodiafiltration versus Conventional Hemodialysis in Children with ESKD: The HDF, Heart and Height Study. J Am Soc Nephrol 2019, 30, 678-691. [CrossRef]
- Chang, J.W.; Yang, W.S.; Seo, J.W.; Lee, J.S.; Lee, S.K.; Park, S.K. Continuous venovenous hemodiafiltration versus hemodialysis as renal replacement therapy in patients with acute renal failure in the intensive care unit. Scand J Urol Nephrol 2004, 38, 417-421. [CrossRef]
- Nistor, I.; Palmer, S.C.; Craig, J.C.; Saglimbene, V.; Vecchio, M.; Covic, A.; Strippoli, G.F. Convective versus diffusive dialysis therapies for chronic kidney failure: an updated systematic review of randomized controlled trials. Am J Kidney Dis 2014, 63, 954-967. [CrossRef]
- Lakshman, S.G.; Ravikumar, P.; Kar, G.; Das, D.; Bhattacharjee, K.; Bhattacharjee, P. A Comparative Study of Neurological Complications in Chronic Kidney Disease with Special Reference to its Stages and Haemodialysis Status. J Clin Diagn Res 2016, 10, OC01-OC04. [CrossRef]
- Arnold, R.; Issar, T.; Krishnan, A.V.; Pussell, B.A. Neurological complications in chronic kidney disease. JRSM Cardiovasc Dis 2016, 5, 2048004016677687. [CrossRef]
- Chillon, J.M.; Massy, Z.A.; Stengel, B. Neurological complications in chronic kidney disease patients. Nephrol Dial Transplant 2016, 31, 1606-1614. [CrossRef]
- Krishnan, A.V.; Kiernan, M.C. Neurological complications of chronic kidney disease. Nat Rev Neurol 2009, 5, 542-551. [CrossRef]
- Krishnan, A.V.; Phoon, R.K.; Pussell, B.A.; Charlesworth, J.A.; Kiernan, M.C. Sensory nerve excitability and neuropathy in end stage kidney disease. J Neurol Neurosurg Psychiatry 2006, 77, 548-551. [CrossRef]
- Krishnan, A.V.; Lin, C.S.; Kiernan, M.C. Nerve excitability properties in lower-limb motor axons: evidence for a length-dependent gradient. Muscle Nerve 2004, 29, 645-655. [CrossRef]
- Camargo, C.R.S.; Schoueri, J.H.M.; Alves, B.; Veiga, G.; Fonseca, F.L.A.; Bacci, M.R. Uremic neuropathy: an overview of the current literature. Rev Assoc Med Bras (1992) 2019, 65, 469-474. [CrossRef]
- Arnold, R.; Pussell, B.A.; Pianta, T.J.; Grinius, V.; Lin, C.S.; Kiernan, M.C.; Howells, J.; Jardine, M.J.; Krishnan, A.V. Effects of hemodiafiltration and high flux hemodialysis on nerve excitability in end-stage kidney disease. PLoS One 2013, 8, e59055. [CrossRef]
- Jiang, X.; Ji, F.; Chen, Z.W.; Huang, Q.L. Comparison of high-flux hemodialysis with hemodialysis filtration in treatment of uraemic pruritus: a randomized controlled trial. International urology and nephrology 2016, 48, 1533-1541. [CrossRef]
- Arzhan, S.; Roumelioti, M.E.; Unruh, M.L. Itch and Ache on Dialysis: New Approaches to Manage Uremic Pruritus and Restless Legs. Blood purification 2020, 49, 222-227. [CrossRef]
- Kang, A.; Arnold, R.; Gallagher, M.; Snelling, P.; Green, J.; Fernando, M.; Kiernan, M.C.; Hand, S.; Grimley, K.; Burman, J.; et al. Effect of Hemodiafiltration on the Progression of Neuropathy with Kidney Failure: A Randomized Controlled Trial. Clin J Am Soc Nephrol 2021, 16, 1365-1375. [CrossRef]
- Sehgal, A.R.; Grey, S.F.; DeOreo, P.B.; Whitehouse, P.J. Prevalence, recognition, and implications of mental impairment among hemodialysis patients. American Journal of Kidney Diseases 1997, 30, 41-49. [CrossRef]
- Kurella Tamura, M.; Yaffe, K. Dementia and cognitive impairment in ESRD: diagnostic and therapeutic strategies. Kidney Int 2011, 79, 14-22. [CrossRef]
- Murray, A.M. Cognitive Impairment in the Aging Dialysis and Chronic Kidney Disease Populations: An Occult Burden. Advances in Chronic Kidney Disease 2008, 15, 123-132. [CrossRef]
- Drew, D.A.; Weiner, D.E.; Tighiouart, H.; Duncan, S.; Gupta, A.; Scott, T.; Sarnak, M.J. Cognitive Decline and Its Risk Factors in Prevalent Hemodialysis Patients. Am J Kidney Dis 2017, 69, 780-787. [CrossRef]
- Van Campenhout, A.; Golledge, J. Osteoprotegerin, vascular calcification and atherosclerosis. Atherosclerosis 2009, 204, 321-329. [CrossRef]
- Fan, S.S.; Lin, L.F.; Chen, V.C.; Hsieh, C.W.; Hsiao, H.P.; McIntyre, R.S.; Iacobucci, M.; Coles, A.S.; Tsai, D.J.; Weng, J.C.; et al. Effects of Lower Past-Year Serum Sodium and Hyponatremia on Depression Symptoms and Cognitive Impairments in Patients With Hemodialysis. Ther Apher Dial 2020, 24, 169-177. [CrossRef]
- Olczyk, P.; Kusztal, M.; Golebiowski, T.; Letachowicz, K.; Krajewska, M. Cognitive Impairment in End Stage Renal Disease Patients Undergoing Hemodialysis: Markers and Risk Factors. Int J Environ Res Public Health 2022, 19. [CrossRef]
- Hsieh, H.L.; Yang, C.M. Role of redox signaling in neuroinflammation and neurodegenerative diseases. Biomed Res Int 2013, 2013, 484613. [CrossRef]
- Kurella Tamura, M.; Wadley, V.; Yaffe, K.; McClure, L.A.; Howard, G.; Go, R.; Allman, R.M.; Warnock, D.G.; McClellan, W. Kidney function and cognitive impairment in US adults: the Reasons for Geographic and Racial Differences in Stroke (REGARDS) Study. Am J Kidney Dis 2008, 52, 227-234. [CrossRef]
- Murray, A.M.; Tupper, D.E.; Knopman, D.S.; Gilbertson, D.T.; Pederson, S.L.; Li, S.; Smith, G.E.; Hochhalter, A.K.; Collins, A.J.; Kane, R.L. Cognitive impairment in hemodialysis patients is common. Neurology 2006, 67, 216-223. [CrossRef]
- Cervellati, C.; Romani, A.; Seripa, D.; Cremonini, E.; Bosi, C.; Magon, S.; Passaro, A.; Bergamini, C.M.; Pilotto, A.; Zuliani, G. Oxidative balance, homocysteine, and uric acid levels in older patients with Late Onset Alzheimer's Disease or Vascular Dementia. J Neurol Sci 2014, 337, 156-161. [CrossRef]
- MacEwen, C.; Sutherland, S.; Daly, J.; Pugh, C.; Tarassenko, L. Relationship between Hypotension and Cerebral Ischemia during Hemodialysis. J Am Soc Nephrol 2017, 28, 2511-2520. [CrossRef]
- Casserly, I.; Topol, E.J. Convergence of atherosclerosis and Alzheimer's disease: inflammation, cholesterol, and misfolded proteins. The Lancet 2004, 363, 1139-1146. [CrossRef]
- Breteler, M.M.; van Amerongen, N.M.; van Swieten, J.C.; Claus, J.J.; Grobbee, D.E.; van Gijn, J.; Hofman, A.; van Harskamp, F. Cognitive correlates of ventricular enlargement and cerebral white matter lesions on magnetic resonance imaging. The Rotterdam Study. Stroke 1994, 25, 1109-1115. [CrossRef]
- Chai, C.; Wang, H.; Chu, Z.; Li, J.; Qian, T.; Mark Haacke, E.; Xia, S.; Shen, W. Reduced regional cerebral venous oxygen saturation is a risk factor for the cognitive impairment in hemodialysis patients: a quantitative susceptibility mapping study. Brain Imaging Behav 2020, 14, 1339-1349. [CrossRef]
- Arieff, A.I. Aluminum and the Pathogenesis of Dialysis Encephalopathy. American Journal of Kidney Diseases 1985, 6, 317-321. [CrossRef]
- Han, M.; Guedes, M.; Larkin, J.; Raimann, J.G.; Lesqueves Barra, A.B.; Canziani, M.E.F.; Cuvello Neto, A.L.; Poli-de-Figueiredo, C.E.; Kotanko, P.; Pecoits-Filho, R. Effect of Hemodiafiltration on Self-Reported Sleep Duration: Results from a Randomized Controlled Trial. Blood purification 2020, 49, 168-177. [CrossRef]
- Kim, H.S.; Lee, S.; Kim, J.H. Real-world Evidence versus Randomized Controlled Trial: Clinical Research Based on Electronic Medical Records. J Korean Med Sci 2018, 33, e213. [CrossRef]
- Skarbinski, J.; Fischer, H.; Hong, V.; Liu, L.; Yau, V.M.; Incerti, D.; Qian, L.; Ackerson, B.K.; Amsden, L.B.; Shaw, S.F.; et al. Real-World Evidence to Supplement Randomized Clinical Trials: Tocilizumab for Severe COVID-19 Pneumonia vs. a Cohort Receiving Standard of Care. Clinical pharmacology and therapeutics 2023, 114, 1073-1081. [CrossRef]
- Sheldrick, R.C. Randomized Trials vs Real-world Evidence: How Can Both Inform Decision-making? Jama 2023, 329, 1352-1353. [CrossRef]
- Franklin, J.M.; Glynn, R.J.; Suissa, S.; Schneeweiss, S. Emulation Differences vs. Biases When Calibrating Real-World Evidence Findings Against Randomized Controlled Trials. Clinical pharmacology and therapeutics 2020, 107, 735-737. [CrossRef]
- Deleuran, M.; Vestergaard, C. Real-world evidence vs. randomized control trials. Br J Dermatol 2020, 182, 275-276. [CrossRef]
- Craig, J.C.; Irwig, L.M.; Stockler, M.R. Evidence-based medicine: useful tools for decision making. Med J Aust 2001, 174, 248-253. [CrossRef]
- Strippoli, G.F.; Craig, J.C.; Schena, F.P. The number, quality, and coverage of randomized controlled trials in nephrology. J Am Soc Nephrol 2004, 15, 411-419. [CrossRef]
- Grooteman, M.P.; van den Dorpel, M.A.; Bots, M.L.; Penne, E.L.; van der Weerd, N.C.; Mazairac, A.H.; den Hoedt, C.H.; van der Tweel, I.; Lévesque, R.; Nubé, M.J.; et al. Effect of online hemodiafiltration on all-cause mortality and cardiovascular outcomes. J Am Soc Nephrol 2012, 23, 1087-1096. [CrossRef]
- Ok, E.; Asci, G.; Toz, H.; Ok, E.S.; Kircelli, F.; Yilmaz, M.; Hur, E.; Demirci, M.S.; Demirci, C.; Duman, S.; et al. Mortality and cardiovascular events in online haemodiafiltration (OL-HDF) compared with high-flux dialysis: results from the Turkish OL-HDF Study. Nephrol Dial Transplant 2013, 28, 192-202. [CrossRef]
- Caskey, F.J.; Procter, S.; MacNeill, S.J.; Wade, J.; Taylor, J.; Rooshenas, L.; Liu, Y.; Annaw, A.; Alloway, K.; Davenport, A.; et al. The high-volume haemodiafiltration vs high-flux haemodialysis registry trial (H4RT): a multi-centre, unblinded, randomised, parallel-group, superiority study to compare the effectiveness and cost-effectiveness of high-volume haemodiafiltration and high-flux haemodialysis in people with kidney failure on maintenance dialysis using linkage to routine healthcare databases for outcomes. Trials 2022, 23, 532. [CrossRef]
- Susantitaphong, P.; Siribamrungwong, M.; Jaber, B.L. Convective therapies versus low-flux hemodialysis for chronic kidney failure: a meta-analysis of randomized controlled trials. Nephrol Dial Transplant 2013, 28, 2859-2874. [CrossRef]
- Neri, L.; Gurevich, K.; Zarya, Y.; Plavinskii, S.; Bellocchio, F.; Stuard, S.; Barbieri, C.; Canaud, B. Practice Patterns and Outcomes of Online Hemodiafiltration: A Real-World Evidence Study in a Russian Dialysis Network. Blood purification 2021, 50, 309-318. [CrossRef]
- Imamović, G.; Hrvačević, R.; Kapun, S.; Marcelli, D.; Bayh, I.; Grassmann, A.; Scatizzi, L.; Maslovarić, J.; Canaud, B. Survival of incident patients on high-volume online hemodiafiltration compared to low-volume online hemodiafiltration and high-flux hemodialysis. International urology and nephrology 2014, 46, 1191-1200. [CrossRef]
- Canaud, B.; Barbieri, C.; Marcelli, D.; Bellocchio, F.; Bowry, S.; Mari, F.; Amato, C.; Gatti, E. Optimal convection volume for improving patient outcomes in an international incident dialysis cohort treated with online hemodiafiltration. Kidney Int 2015, 88, 1108-1116. [CrossRef]
- Canaud, B.; Bayh, I.; Marcelli, D.; Ponce, P.; Merello, J.I.; Gurevich, K.; Ladanyi, E.; Ok, E.; Imamovic, G.; Grassmann, A.; et al. Improved survival of incident patients with high-volume haemodiafiltration: a propensity-matched cohort study with inverse probability of censoring weighting. Nephron 2015, 129, 179-188. [CrossRef]
- Maduell, F.; Varas, J.; Ramos, R.; Martin-Malo, A.; Pérez-Garcia, R.; Berdud, I.; Moreso, F.; Canaud, B.; Stuard, S.; Gauly, A.; et al. Hemodiafiltration Reduces All-Cause and Cardiovascular Mortality in Incident Hemodialysis Patients: A Propensity-Matched Cohort Study. Am J Nephrol 2017, 46, 288-297. [CrossRef]
- See, E.J.; Hedley, J.; Agar, J.W.M.; Hawley, C.M.; Johnson, D.W.; Kelly, P.J.; Lee, V.W.; Mac, K.; Polkinghorne, K.R.; Rabindranath, K.S.; et al. Patient survival on haemodiafiltration and haemodialysis: a cohort study using the Australia and New Zealand Dialysis and Transplant Registry. Nephrol Dial Transplant 2019, 34, 326-338. [CrossRef]
- Kikuchi, K.; Hamano, T.; Wada, A.; Nakai, S.; Masakane, I. Predilution online hemodiafiltration is associated with improved survival compared with hemodialysis. Kidney Int 2019, 95, 929-938. [CrossRef]
- Mercadal, L.; Franck, J.E.; Metzger, M.; Urena Torres, P.; de Cornelissen, F.; Edet, S.; Bechade, C.; Vigneau, C.; Drueke, T.; Jacquelinet, C.; et al. Hemodiafiltration Versus Hemodialysis and Survival in Patients With ESRD: The French Renal Epidemiology and Information Network (REIN) Registry. Am J Kidney Dis 2016, 68, 247-255. [CrossRef]
- Imamovic, G.; Hrvacevic, R.; Kapun, S.; Marcelli, D.; Bayh, I.; Grassmann, A.; Scatizzi, L.; Maslovaric, J.; Canaud, B. Survival of incident patients on high-volume online hemodiafiltration compared to low-volume online hemodiafiltration and high-flux hemodialysis. International urology and nephrology 2014, 46, 1191-1200. [CrossRef]
- Jirka, T.; Cesare, S.; Di Benedetto, A.; Perera Chang, M.; Ponce, P.; Richards, N.; Tetta, C.; Vaslaky, L. Mortality risk for patients receiving hemodiafiltration versus hemodialysis. Kidney Int 2006, 70, 1524; author reply 1524-1525. [CrossRef]
- Mercadal, L.; Franck, J.E.; Metzger, M.; Urena Torres, P.; de Cornelissen, F.; Edet, S.; Béchade, C.; Vigneau, C.; Drüeke, T.; Jacquelinet, C.; et al. Hemodiafiltration Versus Hemodialysis and Survival in Patients With ESRD: The French Renal Epidemiology and Information Network (REIN) Registry. Am J Kidney Dis 2016, 68, 247-255. [CrossRef]
- Valderrama, L.A.; Barrera, L.; Cantor, E.J.; Muñoz, J.; Arango, J.; Tobon, C.; Canaud, B. Mortality in High-Flux Hemodialysis vs. High-Volume Hemodiafiltration in Colombian Clinical Practice: A Propensity Score Matching Study. Kidney and Dialysis 2022, 2, 209-220.
- da Rocha, E.P.; Kojima, C.A.; Modelli de Andrade, L.G.; Costa, D.M.; Magalhaes, A.O.; Rocha, W.F.; de Vasconcelos Junior, L.N.; Rosa, M.G.; Wagner Martins, C.S. Comparing Survival Outcomes between Hemodialysis and Hemodiafiltration Using Real-World Data from Brazil. Journal of Clinical Medicine 2024, 13, 594.
- Zhang, Y.; Winter, A.; Ferreras, B.A.; Carioni, P.; Arkossy, O.; Anger, M.; Kossmann, R.; Usvyat, L.A.; Stuard, S.; Maddux, F.W. Real-world effectiveness of hemodialysis modalities: a retrospective cohort study. BMC Nephrology 2025, 26, 1-9. [CrossRef]
Figure 1.
Mechanistic Cascade of High-Volume HDF: From Enhanced Solute Clearance to Survival Benefit in ESKD Patients *. *CV: cardiovascular; IDH: Intradialytic hypotension; ESA: Erythropoietin Stimulating Agents.
Figure 1.
Mechanistic Cascade of High-Volume HDF: From Enhanced Solute Clearance to Survival Benefit in ESKD Patients *. *CV: cardiovascular; IDH: Intradialytic hypotension; ESA: Erythropoietin Stimulating Agents.
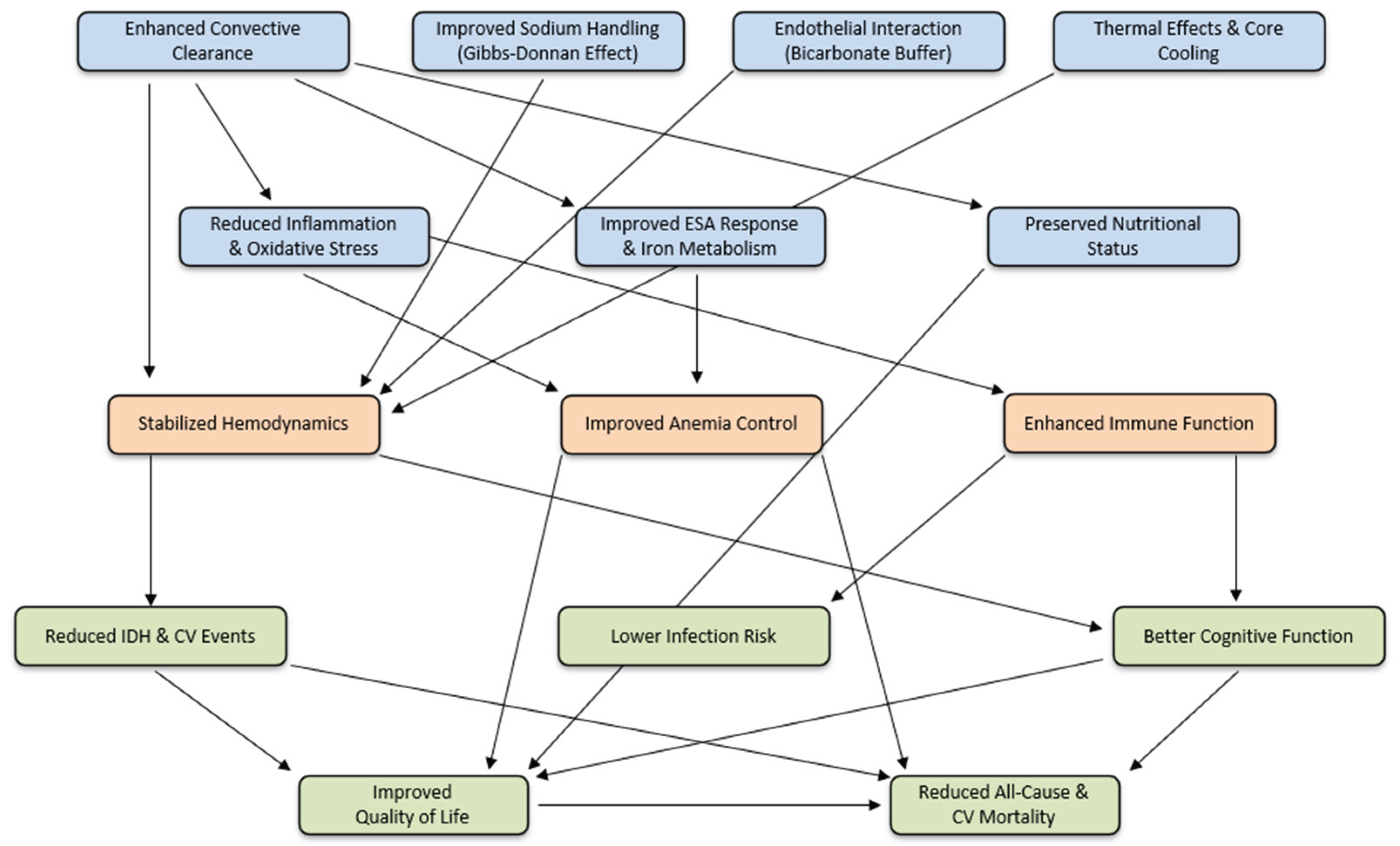

Table 1.
HDF and high-volume HDF effects on short, middle, and long-term clinical outcomes.
| Short-term Outcomes | Middle-Term Outcomes | Long-Term Outcomes |
|---|---|---|
| Enhanced toxin clearance | Reduced amyloidosis | Reduced all-cause mortality |
| Improved hemodynamic stability | Reduced joint pain | Reduced CV* mortality |
| Reduced inflammation | Improved nutritional status | |
| Reduced oxidative stress | Reduced infection risk | |
| Better anemia management | Cardiovascular benefits | |
| Residual kidney function protection | Peripheral Neuropathy Improvements: | |
| Reduced intradialytic cramps | Slow progression cognitive impairment | |
| Reduced skin hyperpigmentation | Improvement of QoL* |
* CV: Cardio-Vascular. QoL: Quality of Life.
Table 2.
HDF and high-volume HDF effects on short, middle, and long-term clinical outcomes.
| MMWs and PBTUs | MW (Da) | Clinical Relevance |
|---|---|---|
| Insulin [32] | 5,800 | Glucose metabolism |
| PTH Fragments [29,33] | 9,000 | CKD-MBD |
| AGE Products [23,34] | >10,000 | Oxidative vascular damage |
| Complement C3a/C5a [35] | 11,500 | Inflammation, immune response |
| Beta 2-Microglobulin [36,37,38,39,40,41,42,43] | 11,800 | Amyloidosis, inflammation |
| Leptin [44,45] | 16,000 | Appetite regulation |
| Tumor Necrosis Factor-alpha [46] | 17,000 | Systemic inflammation |
| Myoglobin [47,48] | 17,000 | Rhabdomyolysis marker |
| Interleukin-1 [49] | 17,000 | Inflammation, immune signaling |
| Retinol-Binding Protein [50] | 21,000 | Insulin resistance |
| Free Light Chains K/L [47,51,52] | 22,000 | Inflammation, dyscrasias |
| Beta-trace Protein [47] | 23,000 | GFR biomarker |
| Complement Factor D (Adipsin) [53] | 24,000 | Complement activation |
| Hepcidin [54,55] | 25,000 | Iron regulation |
| Alpha-1 Microglobulin [56] | 26,000 | Tubular injury, oxidative stress |
| Interleukin-6 [57] | 26,000 | Inflammation, CV risk |
| Fibroblast Growth Factor 23 [58,59] | 32,000 | CKD-MBD, vascular calcification |
| Alpha-1-Acid Glycoprotein [47] | 43,000 | Acute phase protein |
| Protein-bound p-Cresyl Sulfate [60] | 188 | Inflammation, atherosclerosis |
| Protein-bound Indoxyl Sulfate [60] | 213 | Vascular calcification, oxidative stress |
* PTH: Parathyroid Hormone. QoL: Quality of Life. AGE: Advanced Glycation End; K/L: (Kappa/Lambda).
Table 2.
This is a table. Tables should be placed in the main text near to the first time they are cited.
Table 2.
This is a table. Tables should be placed in the main text near to the first time they are cited.
| Study | Country | Sample Size (HD/HDF) | Sub/Conv Vol (L/session) | Primary Outcome | Key Findings |
|---|---|---|---|---|---|
| ICS [65] | Italy | 70/40 | Sub 30-40 (pre) | ISH | ISH ↓ 50.9% with HDF |
| CONTRAST [205] | NL-CA | 356/358 | Sub 19.8 | All-cause mortality | No difference overall, but benefit with high-volume HDF |
| Turkish [206] | Turkey | 391/391 | 17.2/19.5 | All-cause mortality + CV event | No difference overall, better survival in high-efficiency HDF |
| ESHOL [31] | Spain | 450/456 | 21.8/23.9 | All-cause mortality | 30% lower all-cause mortality in HDF |
| FRENCHIE [68] | France | 191/190 | 20/21 | Intradialytic tolerance | Better tolerance; no difference in mortality |
| CONVINCE [2] | M | 677/683 | 23.0/25.5 | All-cause mortality | HDF ↓ all-cause mortality by 23% (HR 0.77) |
* ICV: Italian Convective Study; NL: The Nederland; CA: Canada; Sub/Conv Vol: Substitution/convection Volume. ISH: intradialytic symptomatic hypotension. M: Multinational.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



