
Submitted:
30 May 2025
Posted:
04 June 2025
You are already at the latest version
Abstract
Background:
Tumour invasion is caused by mutations in the KRAS gene, and lung cancer is one of the world's leading causes of death.
Aim of the study:
To create monoclonal antibodies against the KRAS protein mutation in lung cancer and to produce a lipid-nanoparticle (LNP)-mRNA vaccine against various lung cancer types.
Type of the study:
Screening experimental study.
Methodology:
Using hybridoma technology, monoclonal antibodies to mutant KRAS protein were produced. The neutralising monoclonal antibodies were subsequently covalently modified to include the cell-penetrating nonapeptide arginine molecules before the antibody hinge regions. Besides, a lipid-nanoparticle-mRNA vaccine containing 10 µg mRNA of mutated forms of lung cancer KRAS protein, 10 µg mRNA of lung cancer TMEM 97 protein, and 10 µg mRNA of lung cancer TMEM 48 protein was created.
To ascertain the effectiveness of the active and passive immunization of the test vaccine and monoclonal antibodies to mutant forms of the KRAS protein, animal experiments were conducted on transgenic mice implanted with lung cancer.
To determine the pharmacokinetic and pharmacodynamic effects of the test vaccination in conjunction with the test monoclonal antibodies to mutant versions of the KRAS protein, immunogenicity testing was conducted in phase 1 randomised human clinical trials.
Results:
The protective power of monoclonal antibodies to mutant versions of lung KRAS protein and the test lung cancer LNP-mRNA vaccine was about 73% in preclinical experiments. However, it was roughly 65% in phase 1 randomised human clinical trials.
In preclinical experiments, lung cancer metastasis was impeded by around 82%, whereas in phase 1 randomised human clinical trials, it was averted by 76%.
Conclusion:
Due to the innovative invention of active-passive immunization, which included monoclonal antibodies and the lung cancer LNP-mRNA vaccine, the current trial showed promise in preventing the spread of lung cancer.
Keywords:
Monoclonal antibodies
; LNP-mRNA-Vaccine
; Lung cancer KRAS protein
; Lung cancer TMEM 97
; Lung cancer TMEM 48
Introduction
One of the leading causes of death globally is cancer.[1] In 2022, there were an estimated 20 million new cases and 9.7 million deaths worldwide.[2] An estimated 53.5 million people were still alive five years after being diagnosed with cancer.[3] One in five people will develop cancer in their lifetime, and one in nine men and one in twelve women will die from the disease.[4] There were nearly 20 million new cases and 9.7 million deaths worldwide in 2022.[5] By 2040, it is expected that there will be 29.9 million new cases of cancer annually and 15.3 million deaths from cancer.[6]
Ninety percent of deaths worldwide are caused by cancer metastases.[7]
Ninety percent of cancer causes are environmental factors.[8] Lung cancer is the most common cancer diagnosed and the leading cause of cancer death globally, both in men and women, with nearly 2.5 million cases (1 in 8 cancers)[9] and 1.8 million deaths (1 in 5 deaths).[10] The most common types of lung cancer include mesothelioma, lung nodules, non-small lung cancer, and small lung cancer.[11] Major biomarkers of lung cancer include mutations in the KRAS, TMEM 48, and TMEM 97 genes.[12]
Surgery, radiation, and chemotherapy are cancer management strategies.[13] For the lung cancer, chemotherapy had modest curative results. [14] Nowadays, there are trials underway to use targeted medicines for the treatment of lung cancer, such as monoclonal antibodies, to supplement chemotherapy and prevent the incidence of chemotherapeutic drug resistance. [15]
Nowadays, clinical studies are being conducted to manage several types of malignancies, including lung cancer using mRNA cancer vaccines. [16] The current work aimed to develop a combination therapy that included lipid nanoparticles (LNP)-mRNA therapeutic lung cancer vaccination and humanized monoclonal antibodies for successful lung cancer treatment.
Methodology
Ethical Statement
All pertinent national, institutional, and/or worldwide guidelines for the care and use of animals were followed in the current study. The ethical committee for animal handling at Cairo University (ECAHCU), the pharmacy faculty at the University of Cairo, Egypt, and the local authorities authorized all procedures used in the examination, including those involving animals, per the Weatherall report's recommendations (approval number TVV359 in date 3/7/2024). Every attempt was made to reduce the number of animals used in the study, as well as their suffering.
Source of Animal Models
A hundred male mice weighing between 40 and 50 grams were provided and authorized for legalization by the Department of Pharmacology and Toxicology at Cairo University's College of Pharmacy in Egypt.
Collection of the Samples
One hundred ml blood samples were collected from 100 lung cancer patients resident in general hospitals in different governorates in Egypt through venipuncture. Blood was collected from a vein, usually from the inside of the elbow or back of the hand. A needle was inserted into the vein, and then the blood was collected in air tight vial or a syringe. Later the blood samples were stored inside a refrigerator at 4 ̊C until processed.
Inclusion Criteria for Animal Models
Adult immune-competent male mice weighing 40-50 gm implanted with different types of lung cancers. To achieve this two hundred uL of ATCC CCL-5803 lung cancer cell line solution with catalog number NCl-H1299 (purchased from ATCC company, USA) and 200 uL of ATCC CRL-5877 lung cancer cell line solution with catalog number NCl-H1573 (purchased from ATCC company, USA) were injected subcutaneously into each mouse's flank using 24 gauge fresh needle. 45 mice were used in the present study.
Exclusion Criteria for Animal Models
Young mice Pregnant female mice and healthy mice.
Inclusion Criteria for Randomized Human Clinical Trials Phase I
Adults older than 20 years old who histologically confirmed stage I or II small or nonsmall lung cancer. ECOG lies between 0-1. Life expectancy˃ 3 months.
Exclusion Criteria for Randomized Human Clinical Trials Phase I
Pregnancy and lactation. Presence of active autoimmune disease. Lung cancer patients younger than 20 years old. Presence of uncontrolled infections. Lung cancer candidates administrating immunosuppressive drugs. Adults older than 20 years old who histologically did not confirm stage I or II small or nonsmall lung cancer.
Material
All chemical and biological components were purchased from Alnasr Pharmaceutical Company at Abo zabal Alkhanka, Qalyobia, Egypt, and Algomhoria Pharmaceutical Company at Cairo, Egypt.

Table 1.
List of instruments.
| Instrument | Model and manufacturer |
|---|---|
| Autoclaves | Tomy, japan |
| Aerobic incubator | Sanyo, Japan |
| Digital balance | Mettler Toledo, Switzerland |
| Oven | Binder, Germany |
| Deep freezer -80 ℃ | Artiko |
| Refrigerator 5 | whirlpool |
| pH meter electrode | Mettler-toledo, UK |
| Deep freezer -20 ℃ | whirlpool |
| Gyrator shaker | Corning gyrator shaker, Japan |
| 190-1100nm Ultraviolet-visible spectrophotometer | UV1600PC, China |
| Light (optical) microscope | Amscope 120X-1200X, China |
Place and Date of the Study
Between July 2024 and April 2025. This study was conducted at Cairo University's pharmacy faculty in Egypt.
Type of Study
Screening experimental study.
Methods
Production of Monoclonal Antibodies
This was performed using the hybridoma technology. The procedure was carried out according to Mitra S, Tomar PC, 2021 study. In brief, 100 ml of populations of 10 % W/V spleen cells solution from the mice immunized against a mutated form of KRAS protein antigen were mixed with 200 ml of populations of 15 % W/V MM.1S myeloma cell line solution with catalog number CRL-2974 ™ ( purchased from ATCC company, USA) in presence of 20 ml of PEG 20 as a fusing agent. Afterward, the fused cells were selected in hypoxanthine-aminopterin-thymidine (HAT) medium while, the unfused cells died and were removed using a centrifuge for the culture at 500 rpm for 5 minutes, then the supernatant containing the unfused dead cells was discarded.
Later the hybridoma cells were placed in wells and monitored for the production of monoclonal antibodies to the mutated form of KRAS protein.[17]
The monoclonal antibodies were humanized. The protocol of humanization was applied according to Slarve M et al, 2023 study.
In brief, mRNAs were extracted from the available hybridoma cells producing murine anti-KRAS antibodies recognizing KRAS-1a (FVC-1),-2b (FVC-2), and LTHIIIa. Afterwards, the cDNA was synthesized.
Recombinant fragments consisting of the variable regions of the H and L chains of the murine monoclonal antibody ligated to the constant region of the human IgG2 were incorporated into the pET28a plasmid expression vector and transfected into CHO cells. The humanized antibody specificity was detected and tested using ELISA.[18]
Arginine nonapeptide, a cell-penetrating peptide (CPP), was conjugated covalently to the monoclonal antibody through stable thioether bonds formed using thiol-based conjugation. The procedure of this conjugation involved the reduction of monoclonal antibody through dissolving the monoclonal antibody in PBS (pH 7.4) at 1-5 mg/ml, then TCEP (1-10 mM) or DTT ( 5-10 mM) was added to reduce the interchain disulfides and the mixture was incubated at 37 ̊C for 30 min. The excess reducing agent was removed using a desalting column.
Later maleimide activation of the CPP step occurred by dissolving the arginine-rich nonapeptide in PBS (pH 7.4). Then, the maleimide-activated crosslinker ( e.g., Sulfo-SMCC, BMPS) in a 2:1 molar ratio to the peptide, and the mixture was incubated at RT for 30 min. Afterwards, the maleimide-peptide was purified using HPLC.
This was followed by the conjugation reaction step through mixing the thiolated monoclonal antibody with maleimide-activated peptide at a 1:3 molar ratio. This mixture was incubated for 4 hours overnight at 4 ̊C. The unreacted maleimide groups were quenched with L-cysteine (1 mM, 15 min). The purification step was performed using.
HPLC to remove unconjugated peptide.
Antigen-binding specificity was characterized using the ELISA technique. ELISA procedure comprised coating the ELISA plate through the addition of 100 µl of the mutated form of KRAS antigen (1-5 µg/ml in PBS) to each well and the incubation overnight at 4 ̊C. This was followed by the blocking step through the addition of 200 µl of 5% W/V casein in PBS and the incubation at 37 ̊C for 1 hour. For the detection step, HRP-conjugated anti-human IgG ( for standard monoclonal antibodies) was added and the mixture was incubated for 1 hour at 37 ̊C. Later, Washing 3˟ with PBST (PBS+ 0.05% Tween-20) was performed. TMB substrate was added later and the reaction was stopped with H2SO4 (1 M). The absorbance was measured using a plate reader at 450 nm wavelength.
After ELISA was completed the conjugates were stored at 4 ̊C in PBS+ 0.02% NaN3.
Manufacture of In Vitro mRNA Lung Cancer Vaccine
Mutated forms of KRAS, TMEM 97, and TMEM 48 proteins were identified on the lung cancer cell surfaces serologically using ELISA. The cDNA of each protein was determined and registered in the GenBank on the NCBI website. In Vitro, mRNA transcription was performed using a RiboMAXTM kit with catalog number 1280 (Purchased from Promega company, USA) manufacture instructions. The procedure was followed according to the kit, 's Manufacturer's instructions. In brief, the separated DNA templates (cDNA) of the mutated forms of the previously mentioned proteins above were inserted into the transcription vector (pUC18, purchased from Invitrogen, USA) Plasmid using EcoR I cutting endonuclease enzyme type II (purchased from Merck company, USA) and ligase enzyme (purchased from Merck Company, USA); then the recombinant plasmid was linearized by restriction digestion using Hind III cutting endonuclease enzyme type II (purchased from Invitrogen company, USA). Afterward, a clean-up using the wizard® DNA clean-up system was applied to the linearized cDNA templates of the mutated proteins (KRAS, TMEM 97, and TMEM 48).
The reaction components comprising 20 µl SP6 transcription 5× buffer, 20 µl rNTPS, 50 µl linear DNA templates (cDNA) of mutated proteins, 10 µl nuclease-free water, and 10 µl SP6 RNA polymerase were assembled inside a test tube (reaction components SP6 transcription 5× buffer, rNTPS and SP6 RNA polymerase were purchased from Promega company, USA). After this, the reaction mixture was pipetted and incubated at 4 ̊C for 4 hours. Later mRNA was capped at 5-end cotranscriptionally using the capping kit with catalog number CAP-K25 (purchased from OZBIOSCIECES company, France). The capping process was followed according to the instructions of the capping kit manufacturer. Furthermore, a poly-A tail was incorporated into each mRNA strand at 3- end using a Poly(A) Tailing kit with catalog number AM1350 (purchased from InvitrogenTM company, USA). The procedure of the incorporation of a poly-A tail to each mRNA strand was completed per the Poly(A) Tailing kit manufacturer's instructions. Subsequently, mRNA transcripts were purified using the phenol/chloroform extraction technique.
The Procedure of the Purification of mRNA Transcripts
The impurities of cDNA templates were removed by 2 U DNAase I added directly and incubated at 37 ̊C for 15 min. Two microliters of 0.5 M EDTA were added at pH 8 and were incubated at 65 ̊C for 10 min to stop the reaction. mRNA transcripts of the proteins of interest were purified using the phenol/chloroform extraction technique. To 50 µl reaction mixture 85 µl of DEPC-treated water and 15 µl of 3M Na acetate were added and mixed thoroughly.
An equal volume of 1:1 phenol/chloroform mixture was extracted and then twice with an equal volume of chloroform.
The aqueous phase was collected and transferred to a new test tube.
mRNA transcripts of the test proteins were precipitated by adding 2 volumes of 70% ethanol and the pellet was incubated at -20 ̊C for at least 30 min. Later the pellet was collected by centrifugation at 400 rpm. The supernatant was removed and the pellet was rinsed with 500 µl of 70% ethyl alcohol.
The mRNA was resuspended in 20 µl of DEPC-treated water, then stored at -20 ̊C.
Encapsulation of mRNA Transcripts of the Test Proteins KRAS, TMEM 48, and TMEM 97 with Ionizable Cationic Lipid Nanoparticles (LNPs) with Particle Size 80-100 nm in Diameter
The procedure comprised mixing a lipid phase with an aqueous phase.
A lipid phase comprises lipid components. These lipid components included ionizable cationic lipid MC3, 1,2-Distearoyl-sn-glycero-3-phsphocoline (DSPC), cholesterol, and PEG-lipid DMG-PEG2000. Then the lipid components were vortexed well to dissolve completely in 70 % ethanol at appropriate molar ratios of 50:10:38.5:1.5 mol% respectively.
An aqueous phase was prepared from solubilizing 1mg/ml of purified mRNA in citrate buffer (10 mM, pH 4.0).
This was followed by quickly combining 750 µl mRNA solution with 250 µl lipid/ethanol while pipetting fast using T-mixer (T-MixerTM ColibriTM purchased from Medmix company, USA) at a flow rate of 3:1 (aqueous: ethanol). Rapid mixing was crucial to forming uniform lipid nanoparticles with particle size (80-100 nm diameter). PBS (pH 7.4) was added to the mixture to dilute the ethanol to <10% final concentration. A final encapsulation greater than 90% was obtained. Purification was performed by placing the LNPs-mRNA mixture in dialysis tubing (MWCO ~10-100 KDa). Dialysis was achieved overnight against a large volume of PBS at 4 ̊C. The particle size and zeta potential were determined using dynamic light scatter (DLS), while encapsulation efficiency was made using RiboGreen assay ( after lysing LNPs with Triton-X). The mRNA concentration was determined by measuring the optical density (absorbance) using a UV spectrophotometer at 260 nm wavelength.
Linking Cysteinyl Octapeptide Arginine Cell-Penetrating Peptide (Cys-R8 CPP) to LNPs-mRNA Cancer Suspension
This was carried out using the surface functionalization of LNPs with Cys-R8 CCP. DSPE-PEG-Mal was prepared in 70 % ethanol (10 mg/ml). Afterward, DSPE-PEG-Mal solution was added to LNPs-mRNA suspension at 1-2 mol% relative to the total lipid and incubated at 50 ̊C for 30 min to allow insertion.
The next step comprised conjugating the R8 peptide to the LPN mixture.
This was performed by dissolving the Cys-R8 peptide in PBS (pH 7.4) at 1-5 mg/ml concentration. The Cys-R8 was added to LNPs-mRNA suspension in molar excess (3x to 5x molar ratio vs maleimide groups, then the reaction mixture was gently stirred at 4 ̊C for 6 hours. Later purification of the conjugated LNPs was achieved using dialysis tubing (MWCO ~100 KDa) overnight against PBS at 4 ̊C. During the purification process, PBS buffer was changed 2-3 times to ensure free R8 was removed.
The storage of the LNP-mRNA mixture was performed at -80 ̊C. The stability was improved during the storage by the addition of 1 ml of 5-10% cryoprotectant trehalose.
Immunogenicity Testing of LPNs-mRNA Lung Cancer Vaccine via Cell Culture Assay
The evaluation of the immunogenic potential of this vaccine candidate was achieved by measuring immune activation, cytokine production, and cytotoxicity In Vitro using human immune cells and lung cancer.
Preparation of Cells
To isolate peripheral blood mononuclear cells (PBMCs), 1 liter of human blood was collected from 10 adult male and female volunteers (100 ml blood was drawn from venipuncture of each candidate) in EDTA tubes. The freshly isolated blood was diluted 1:1 with PBS. The diluted blood was layered onto Ficoll-Paque and centrifuged at 400 × g for 30 min. The PBMC layer was collected and washed twice in PBS and resuspended in a complete medium. Monocytes from PBMCs were plated and cultured with GM-CSF (50 ng/ml)+ IL-4 (50/ml)+ TNF-α (50 ng/ml) for 5-7 days to mature into dendritic cells (DCs).
Lung cancer cell lines A549, H1975, and H1299 (purchased from ATCC company, USA) were cultured in DMEM+ 10% FBS and incubated at 37 ̊C, 5% CO2 until 70-80% confluenced.
LNPs-mRNA lung cancer vaccine transfection:
DCs were transfected with the test vaccine containing 40 µg mRNA/ml using electroporation. Then the cells were washed to remove the unbound vaccine.
Co-culture setup:
Vaccine-pulsed immune cells were seeded with lung cancer cells at various effector: target (E: T) ratios such as 10:1 and 20:1 in 96-well U-bottom plates. These culture mixture wells and negative control wells containing only cancer cells alone were incubated at 37 ̊C for 7 hours.
Immunogenicity Assays
These included cytokine analysis, T-cell activation, proliferation, and cytotoxicity assay.
Cytokine Analysis
Cytokine analysis was performed by collecting the supernatants of the test and negative control culture wells after 48 hours. IFN-ɣ, IL-2, and TNF-α were measured using cytokine bead array (CBA) according to the BD Cytometric Bead Array (CBA) Human Inflammatory Cytokine kit instructions. This CBA kit possessed a catalog number 15811219 and was purchased from Fisher Scientific company, UK.
T-Cell Activation
Culture cells were harvested and stained with surface markers (CD3, CD4, CD8, CD69, CD25). For intracellular IFN-ɣ staining, the culture wells were fixed and permeabilized. Then T-cell activation was analyzed by flow cytometry. The flow cytometer used in the present study was the BD AccuriTM C6 Plus Flow Cytometer (purchased from BD Biosciences company, USA). The procedure was performed according to the bioscience Essential Human T-Cell Phenotyping kit's manufacturer instructions (this flow cytometry kit had a catalog number A42923 and was purchased from ThermoFisher Scientific Company, USA).
T-Cell Proliferation
Dendritic cells were prelabeled with CFSE and CFSE dilution and analyzed by flow cytometry after 5 days of culture. The procedure was performed according to the bioscience Essential Human Dendritic-Cell Phenotyping kit's manufacturer instructions (this flow cytometry kit had a catalog number B35819 and was purchased from ThermoFisher Scientific Company, USA).
Cytotoxicity Assay
This was performed using an XTT assay to assess the cancer cell death. The procedure was applied per the instructions of the manufacturer of the XTT Cell Viability kit with catalog number 9095 (purchased from Cell Signaling Technology Company, USA).
Immunogenicity Testing of mRNA Lung Cancer Vaccine and Performed Monoclonal Antibodies to Lung Cancer KRAS Neoantigens During Preclinical Trials Phase
Forty-five immune-competent mice such as 6-8 weeks old BALB/c mice were randomly assigned into 3 groups (n=15 per group). Group one included the negative control group which administered the placebo, while group two included a test group that received the test performed monoclonal antibodies.
LNPs-mRNA test vaccine was thawed and diluted in PBS to a final concentration of 100 µg/mouse. Fifty µl of the test vaccine was given via intramuscular route of injection to group 3 which included the remaining test mice.
The schedule comprised prime on day 0, boost on day 7, and day 14.
Tumor Challenge (Therapeutic Setting)
Two hundred uL of ATCC CCL-5803 lung cancer cell line solution with catalog number NCl-H1299 (purchased from ATCC company, USA) and 200 uL of ATCC CRL-5877 lung cancer cell line solution with catalog number NCl-H1573 (purchased from ATCC company, USA) were harvested at 80% confluence and resuspended in PBS at 1 ˟ 106 cells/ml. Later 100 µl of cell lines mixture (1 ×105 cells) was subcutaneously injected into each mouse's flank using a 24 gauge fresh needle on day 7. Tumor size was measured every 3 days (length × width2 × 0.5). Humane endpoints applied were tumor ˃ 2 cm and distress signs.
Immune Response Assays
To achieve this blood samples were collected from the tail vein on days 0, 14, 21). Afterward, the experimental mice were euthanized on day 21 and the spleens, lymph nodes, and tumors were collected from them.
ELISA
The procedure included coating ELISA plates with antigen (2 µg/ml) and then blocking them with BSA. A serial dilution of serum samples was added. Then, HRP-antimouse IGg1/IgG2a antibodies were added. The absorbance was developed and read at 450 nm. The procedure was performed according to the guides of the ELISA kit (MouseTM ELISA Kit with catalog number 41116158 purchased from Sigma-Aldrich, UK).
ElISpot for the Detection of IFN-ɣ
The procedure comprised plating the splenocytes (1×106cells/well). This was followed by stimulation using specific peptides (1-10 µg/ml) and incubation at 37 ̊C for 24 hours. Spots were counted by a digital microplate reader. The procedure was done following IFN-γ ELISpot Assays on MultiScreen® IP kit (purchased from MERCK company, Germany)
Flow Cytometry
BD AccuriTM C6 Plus Flow Cytometer (purchased from BD Biosciences company, USA) was used for this purpose.
The procedure included the preparation of single-cell suspensions, and surface staining using CD3, CD4, CD8, CD44, and CD62L. Then CD69 and PD-1 activation markers were added. IFN-ɣ and TNF-α were added after the incorporation of PMA/ionomycin+ Brefeldin A. The procedure was carried out using the H2A.X Phosphorylation Assay Kit, with catalog number 17-344 (obtained from MERCK company, Canada).
Cytotoxicity Assay
This was performed using an LDH1 release assay. The procedure was applied according to the LDH Assay Kit (Cytotoxicity) with catalog number ab65393 (acquired from Abcam company, UK). The procedure comprised labeling the target cells with CSFE and co-culturing with effector T cells. Later the dead cells were stained with Pl/7-ADD. The cytotoxicity activity was detected colorimetrically at 490 nm wavelength.
Randomized Human Clinical Trials Phase 1
This randomized clinical trial included 76 lung cancer patients divided into 5 groups (negative control, positive control, and 3 test groups, n=19 for each group). All groups included small and non-small lung cancer patients (stages I and II) whose ages were greater than 20 years old and their weights ranged between 70-100 kg. Both genders (male and female) were included in this investigation.
The count of small lung cancer patients was 21, while the count of non-small lung cancer patients was 55. Two ml of test lung LNPs-mRNA vaccine comprising mutated forms of mRNA encoding KRAS, TMEM 48, and TMEM 97 (10 µg/ml for each) were injected intramuscularly for the test group 1, while the second test group received the freshly prepared monoclonal antibodies to mutated forms of KRAS proteins intramuscularly. The negative control group received 2 ml of the placebo via intramuscular injection. Each candidate of the positive control group received 2 ml of 10 µg/ml chemiplimab (a PD-1 inhibitor) as a standard drug via the intramuscular injection.
The fourth test group candidates were administered a combination therapy comprising 2 ml (10 µg/ml) of the test vaccine and 2 ml (10 µg/ml) of the test monoclonal antibodies to mutated KRAS antigens of lung cancer cells.
Both the test vaccine and the test monoclonal antibodies were given at different intramuscular injection sites to avoid neutralizing the test vaccine by the test monoclonal antibodies. The dosage regimen schedule for all four groups comprised a prime dose on day 1 and booster doses on days 3, 7, 14, 28, 45, 60, and 100.
Collection of Blood Samples from the Volunteers
One hundred ml blood sample was collected from each volunteer in the present study via the puncture after receiving the test vaccine and/or the test monoclonal antibodies and at the follow-up stages on days 120 and 180.
Immunogenicity Testing in Randomized Human Clinical Trials Phase I
Immunogenicity testing included performing ELISA (for the detection of the production of neutralizing antibodies to minimize lung tumor size and prevent cancer metastasis), flow cytometry (for the evaluation of the cell-mediated immunity evoked by the test vaccine), and the cytokine assay.
The Procedure of ELISA
In brief, For measurement of antibodies, 1 ml of 10 µg/ml known antigens were fixed to the bottom of small wells on plastic plates, incubated with dilutions of the patient’s serum, washed, and then reincubated with 1 ml of 10 µg/ml antibody to human IgG1 labeled with horseradish peroxidase (purchased from MERCK company, Germany). Enzyme activity was measured by adding 2 ml of 10% W/V 3,3-,5,5--tetramethyl benzidine (TMB) substrate for the enzyme and estimating the color reaction in a UV spectrophotometer.
The Procedure of Flow Cytometry
BD AccuriTM C6 Plus Flow Cytometer (purchased from BD Biosciences company, USA) was utilized for this design. This test was used to measure the count of the different sorts of immunologically active blood cells. The kit utilized in this test was a bioscience Essential Human T-Cell Phenotyping kit with catalog number A42923 (purchased from ThermoFisher Company, USA)
Briefly, in this test, the volunteer's cells were labeled with monoclonal antibodies to the protein specific to the cell of interest. 1 ml of 10 µg/ml monoclonal antibodies was tagged with 1 ml of 5% W/V fluorescein dye. Single cells were allowed to pass through a laser light beam, and the count of cells that fluoresced was determined by the employment of a fluorescence-activated cell sorter.
Procedure of Cytokine Assay in Randomized Human Clinical Trials Phase 1
This was performed using Luminex cytokine assay. Luminex™ xMAP™ INTELLIFLEX System (purchased from ThermoFisher Company, USA) was used for this utility. The protocol followed was by the instructions guided by the Human ProcartaPlexTM Simplex kit with catalog number EPX01A-12023-901 (acquired from ThermoFisher company, USA). The procedure comprised bead preparation via vortexing the bead stock and diluting to working concentration. Then 50 µl of mixed magnetic beads were added to each well. The plate was placed afterward on a magnetic separator and they were allowed to settle (1-2 min). This was followed by removing the supernatant and the beads were washed 2x with 100 µl wash buffer. Serial dilutions of standards were prepared in the provided diluent. Later 50 µl of standards, controls, and samples were added to the appropriate wells, covered, and incubated on a plate shaker (800 rpm) for 2 hours at 4 ̊C. This was followed by washing beads 3x with 100 µl wash buffer using the magnetic separator. Fifty µl of biotinylated detection antibodies were added to each well and incubated at 4 ̊C on a shaker (600 rpm) for 60 min. Moreover, the beads were rewashed 3x as before. Then fifty µl of streptavidin-PE was added to each well and incubated for 30 minutes in the dark on a shaker (500 rpm). Later the beads were washed and suspended in 100 µl assay buffer. Finally, the plates were shaken on a shaker (700 rpm) for 5 min at 4 ̊C. The plate was read using the Luminex apparatus. Fifty beads were collected per cytokine per well and the cytokine concentrations were determined based on the mean fluorescence intensity (MFI).
Cytotoxicity Assay
This was performed using an LDH1 release assay. The procedure was applied according to the LDH Assay Kit (Cytotoxicity)with catalog number ab65393 (acquired from Abcam company, UK).
The procedure comprised labeling the target cells with CSFE and co-culturing with effector T cells. Later the dead cells were stained with Pl/7-ADD. The cytotoxicity activity was detected colorimetrically at 490 nm wavelength.
Lung Tumor Size Determination
This was detected using magnetic resonance imaging (MRI).
Lung Cancer Metastasis
This was determined using computed tomography (CT) scans. X-ray pictures of the body of each volunteer at different angles were taken.
Toxicity of the test vaccine:
These were noticed after giving the prime and boost doses of the test vaccine in accomplishment with the test-preformed monoclonal antibodies during the present study. The presence of acute or chronic toxicity was reported.
Statistical Analysis
All experiments were conducted in triplets. Their presentation was by means and standard deviation. One way analysis of variance( p value≤ 0.05) was used as means for performing statistical analysis and also, statistical analysis based on excel-spreadsheet-software. The student's t-test was used during the present study.
Figure 1.
UV absorption spectrum of mRNA of mutated KRAS protein of lung cancer cells. Peak absorbance was determined at 260 nm.
Figure 1.
UV absorption spectrum of mRNA of mutated KRAS protein of lung cancer cells. Peak absorbance was determined at 260 nm.
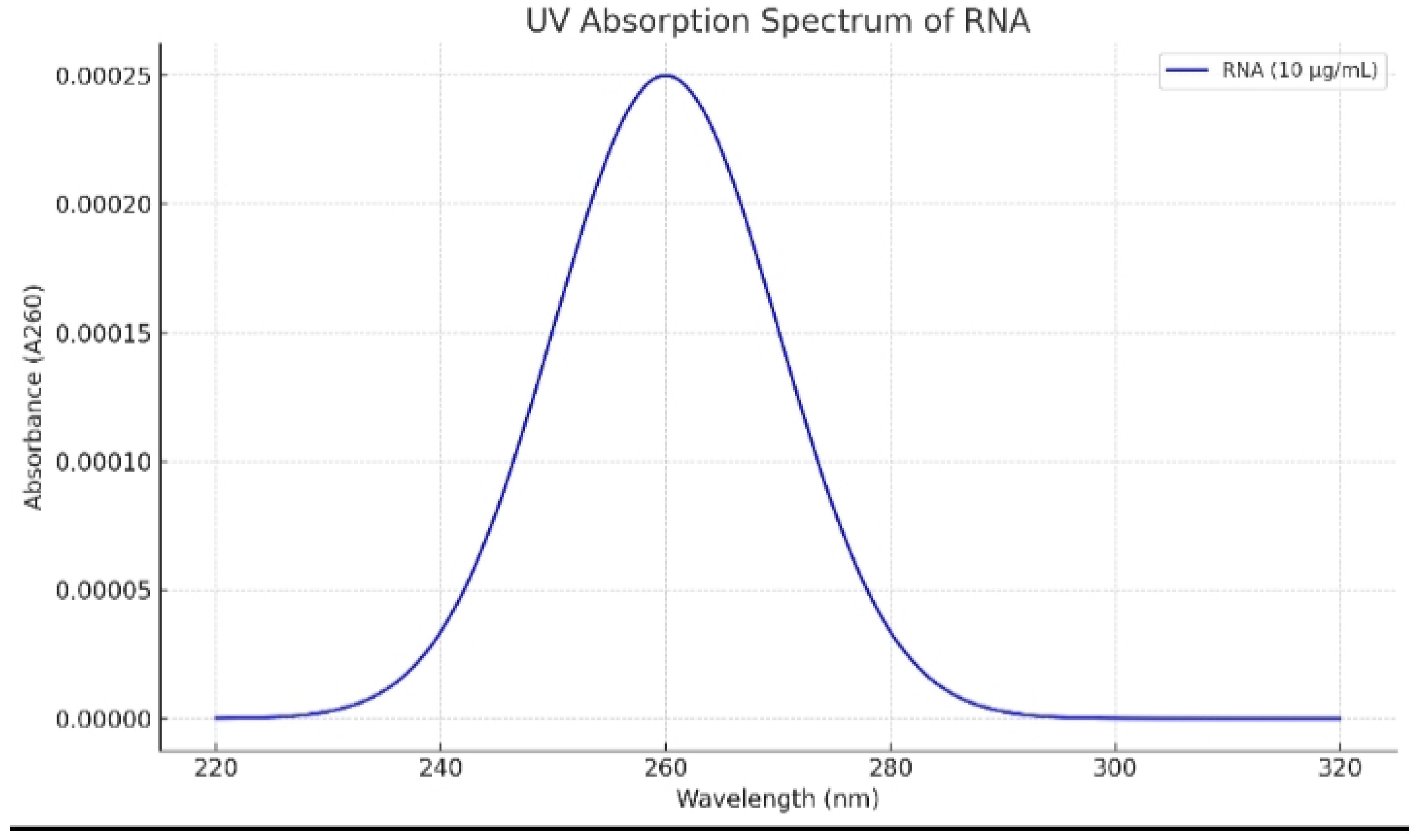
Figure 2.
UV absorption spectrum of mRNA of mutated TMEM97 protein of lung cancer cells. Peak absorbance was determined at 260 nm.
Figure 2.
UV absorption spectrum of mRNA of mutated TMEM97 protein of lung cancer cells. Peak absorbance was determined at 260 nm.
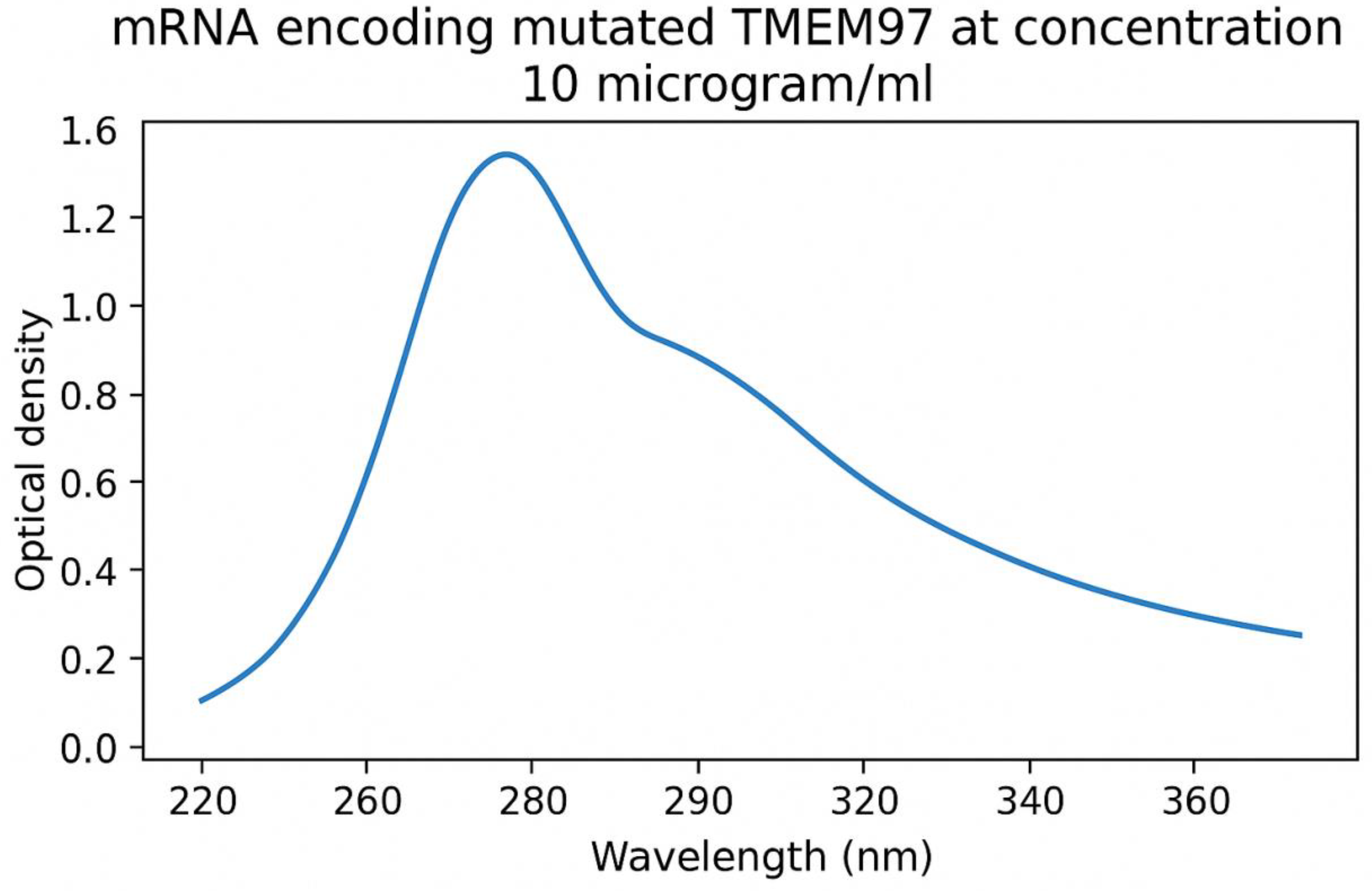
Figure 3.
UV absorption spectrum of mRNA of mutated TMEM48 protein of lung cancer cells. Peak absorbance was determined at 260 nm.
Figure 3.
UV absorption spectrum of mRNA of mutated TMEM48 protein of lung cancer cells. Peak absorbance was determined at 260 nm.
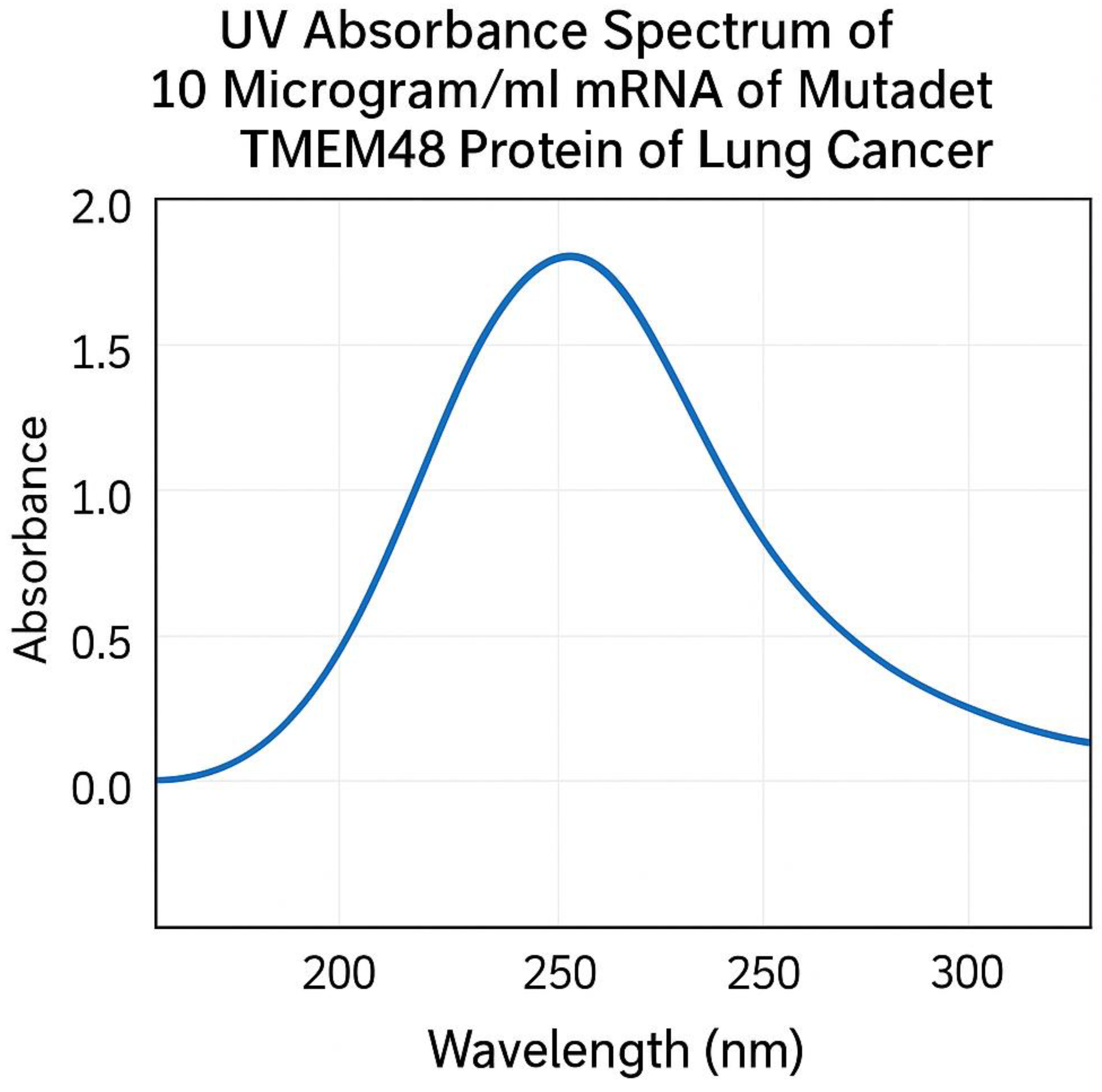
Figure 4.
It demonstrates the neutralizing antibodies to mutated lung cancer KRAS antigen using ELISA after 21 days. This assay was performed in preclinical trials stage.
Figure 4.
It demonstrates the neutralizing antibodies to mutated lung cancer KRAS antigen using ELISA after 21 days. This assay was performed in preclinical trials stage.
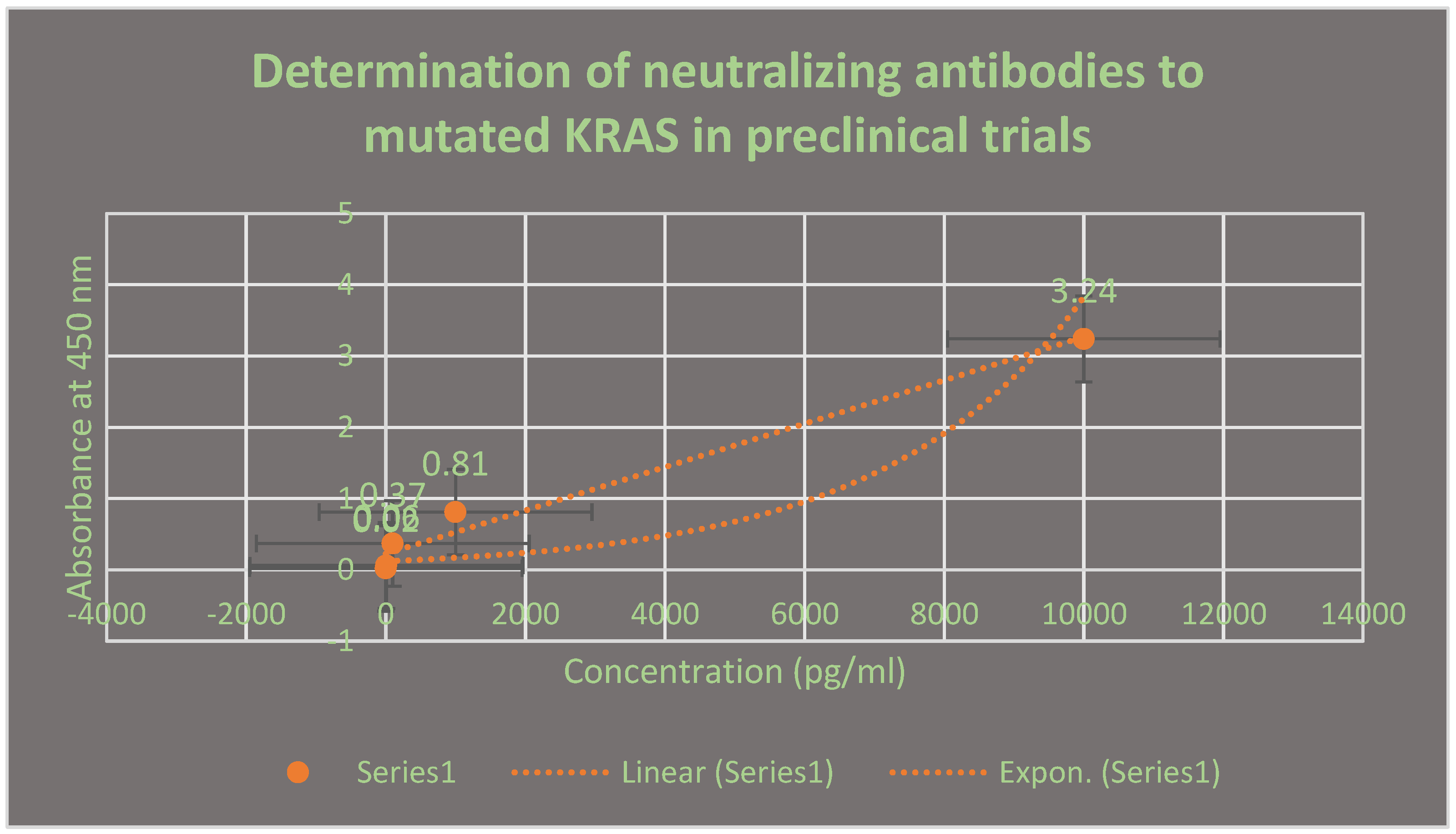
Figure 5.
It describes the determination of protectant antibodies to TMEM48 antigen on the surface of lung cancer cells using ELISA during cell culturing testing phase. The assay was performed after 14 days post-vaccination with the test LNPs-mRNA lung cancer vaccine.
Figure 5.
It describes the determination of protectant antibodies to TMEM48 antigen on the surface of lung cancer cells using ELISA during cell culturing testing phase. The assay was performed after 14 days post-vaccination with the test LNPs-mRNA lung cancer vaccine.
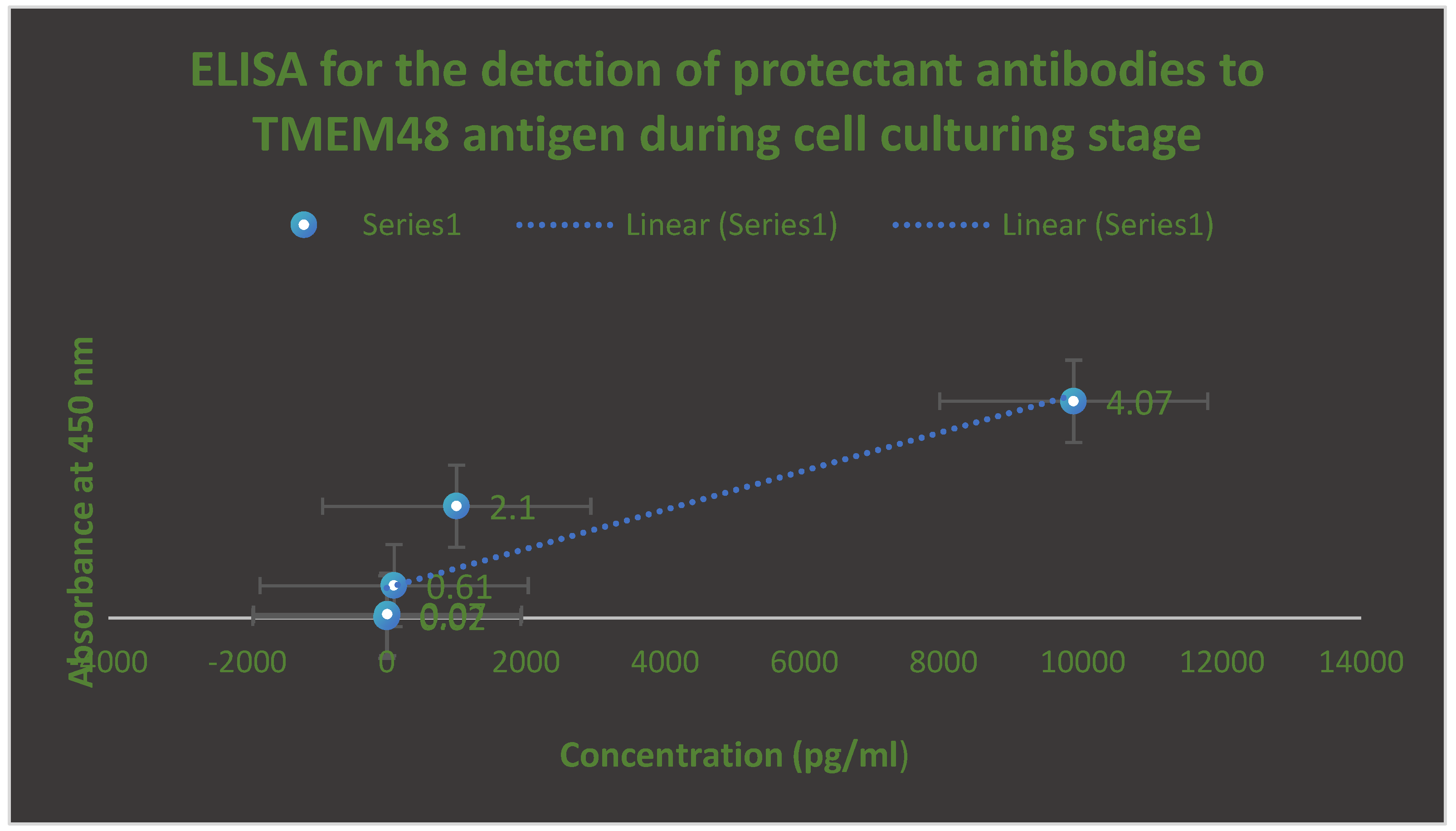
Figure 6.
It shows the assessment of the neutralizing antibodies to the mutated TMEM97 protein of lung cancer cells using ELISA during randomized human clinical trials phase 1. The appearance of these antibodies was observed after 28 days post-vaccination.
Figure 6.
It shows the assessment of the neutralizing antibodies to the mutated TMEM97 protein of lung cancer cells using ELISA during randomized human clinical trials phase 1. The appearance of these antibodies was observed after 28 days post-vaccination.
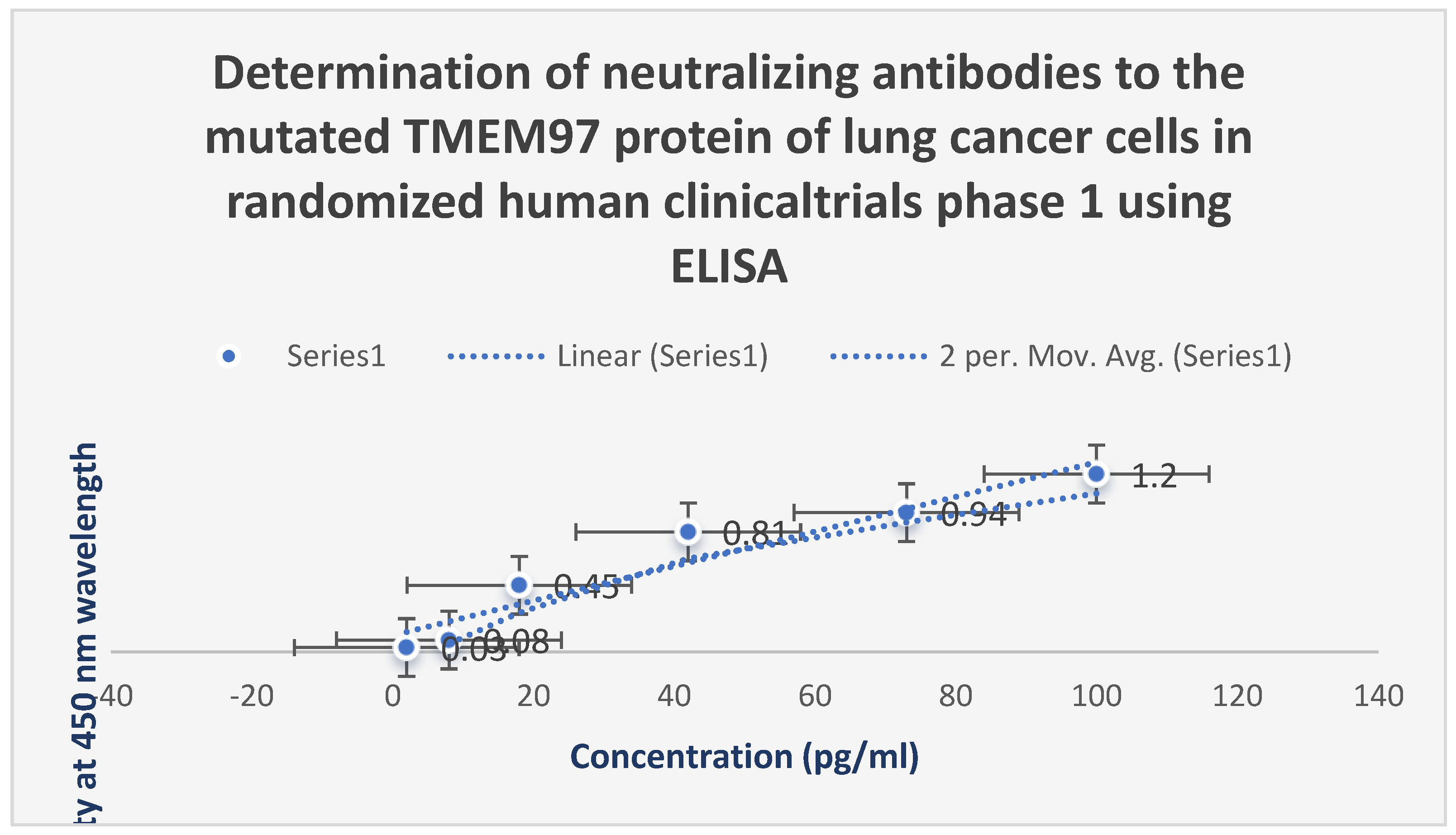
Figure 7.
It illustrates the cytokine analysis in randomized human clinical trials phase 1 after 2 months. IL-10 was reduced, while IL-6, TNF-ɑ and IFN-ɣ were increased significantly.
Figure 7.
It illustrates the cytokine analysis in randomized human clinical trials phase 1 after 2 months. IL-10 was reduced, while IL-6, TNF-ɑ and IFN-ɣ were increased significantly.
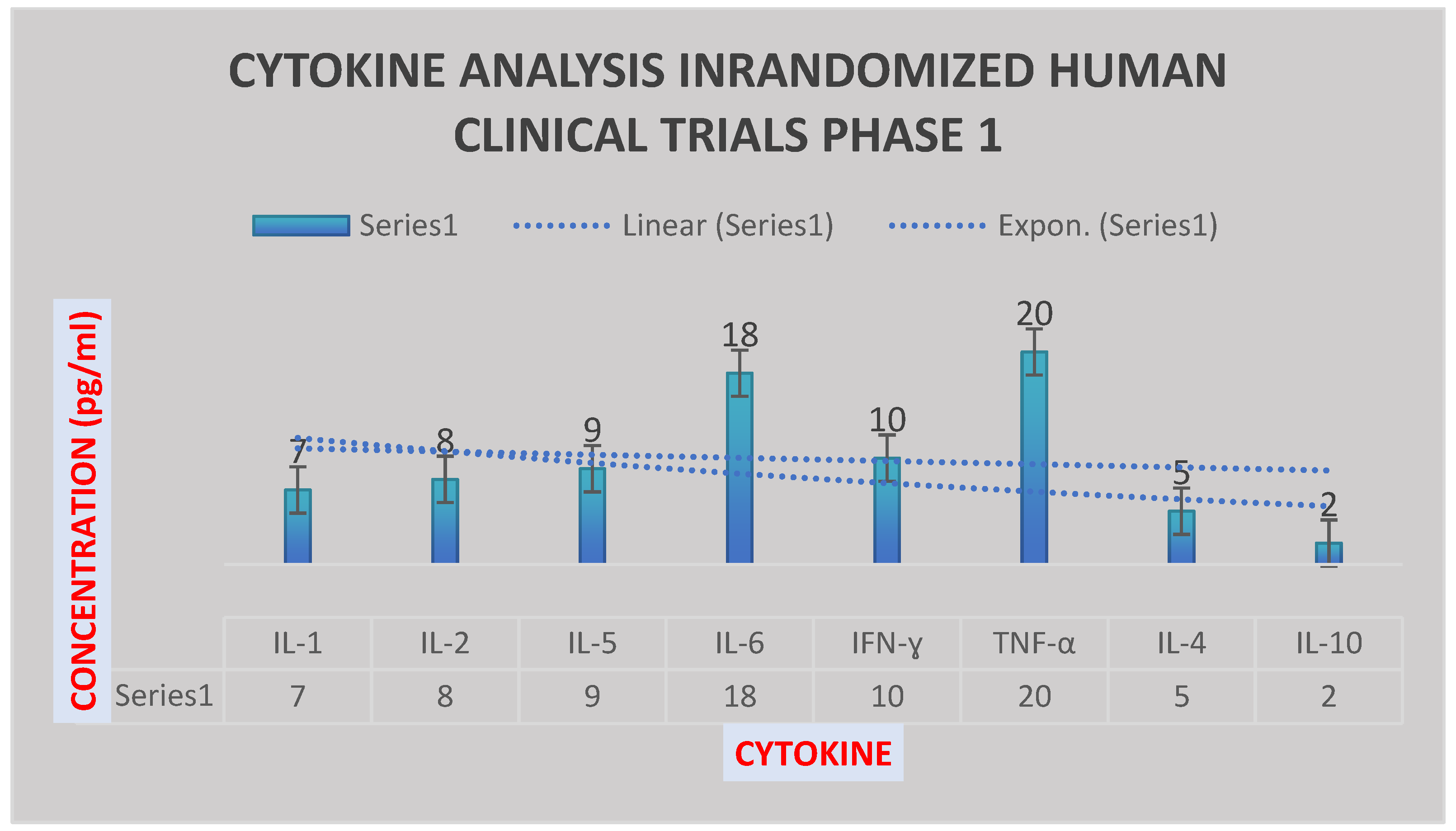
Figure 8.
It describes the mean fluorescence intensity of the cytokines during preclinical trials and randomized human clinical trials phase 1 at p≤ 0.05.
Figure 8.
It describes the mean fluorescence intensity of the cytokines during preclinical trials and randomized human clinical trials phase 1 at p≤ 0.05.
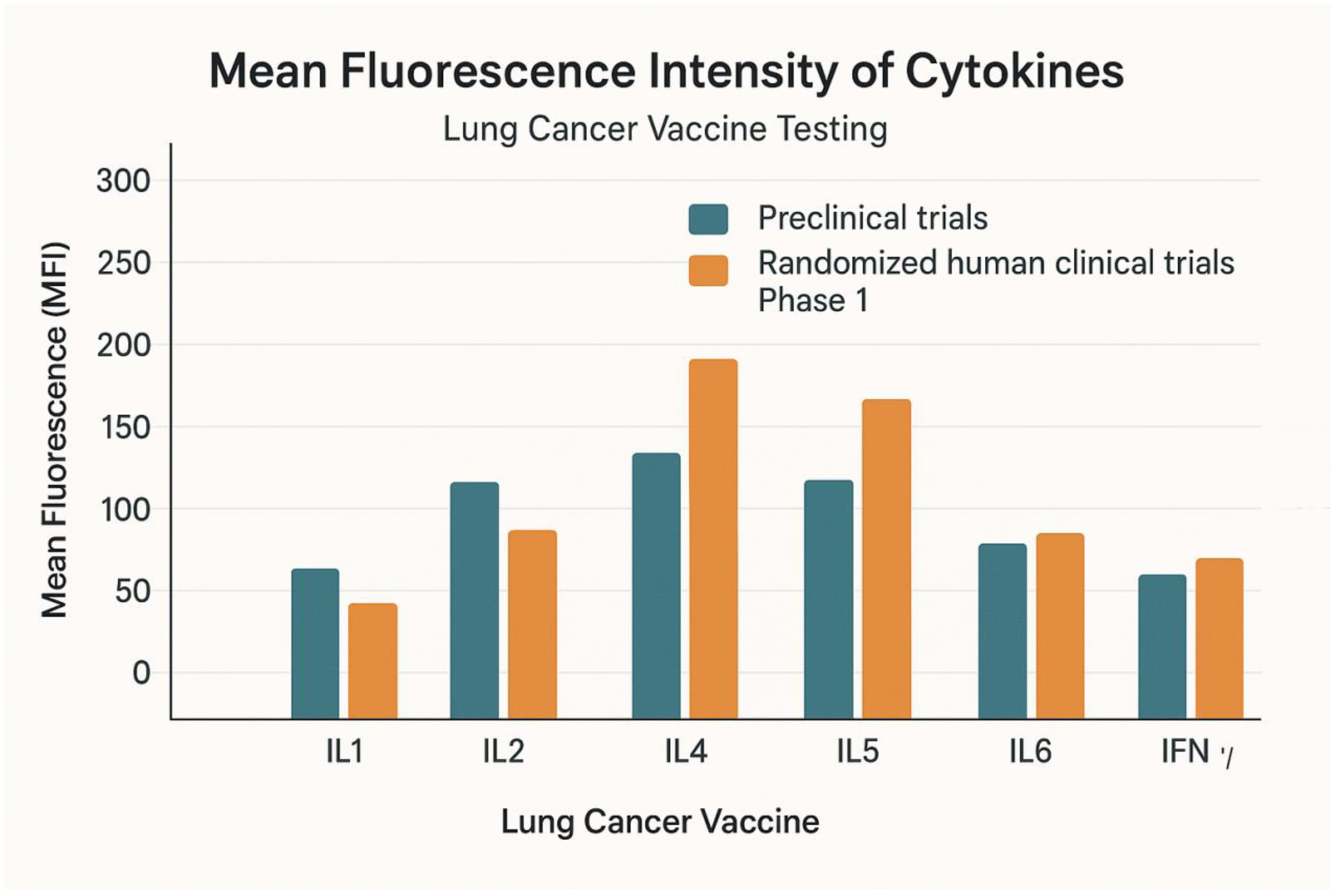
Figure 9.
It shows immune simulation prediction of the cytokine response to mutant epitopes of TMEM48, TMEM97 and KRAS protein antigens of the test LNPs-mRNA lung cancer vaccine. It was generated by bioinformatic C-ImmSim software.
Figure 9.
It shows immune simulation prediction of the cytokine response to mutant epitopes of TMEM48, TMEM97 and KRAS protein antigens of the test LNPs-mRNA lung cancer vaccine. It was generated by bioinformatic C-ImmSim software.
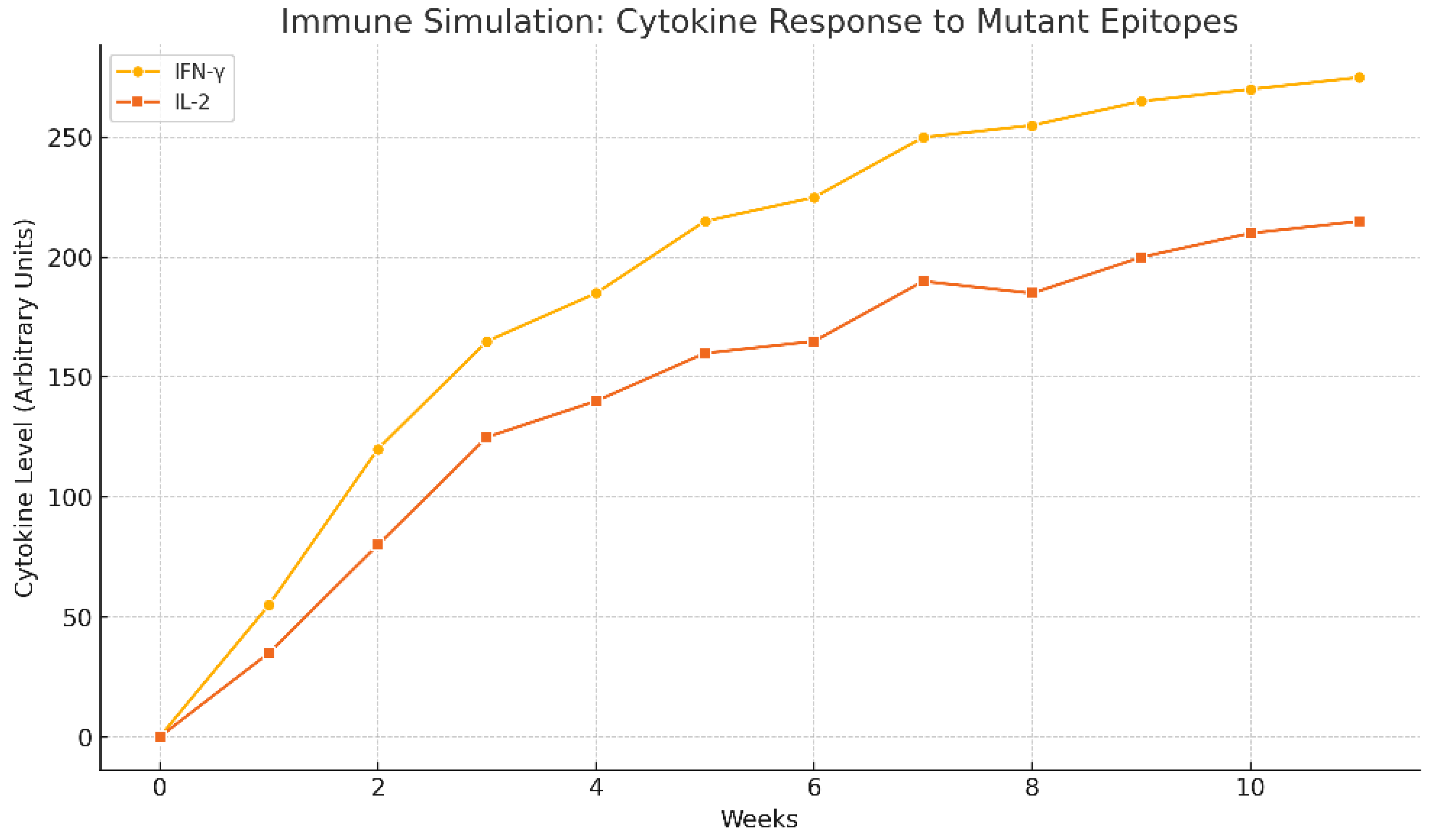
Figure 10.
a. It shows the mutant KRAS, TMEM48 and TMEM97 protein antigens of the lung cancer cells. The mRNA of these mutated protein antigens were used in the construction of the test LNPs-mRNA lung cancer vaccine. b. It demonstrates the regions of the rare mutations inside KRAS, TMEM8 and TMEM97 protein antigens of the lung cancer cells. These mutated proteins leaded to the production of powerful antibodies to them.
Figure 10.
a. It shows the mutant KRAS, TMEM48 and TMEM97 protein antigens of the lung cancer cells. The mRNA of these mutated protein antigens were used in the construction of the test LNPs-mRNA lung cancer vaccine. b. It demonstrates the regions of the rare mutations inside KRAS, TMEM8 and TMEM97 protein antigens of the lung cancer cells. These mutated proteins leaded to the production of powerful antibodies to them.
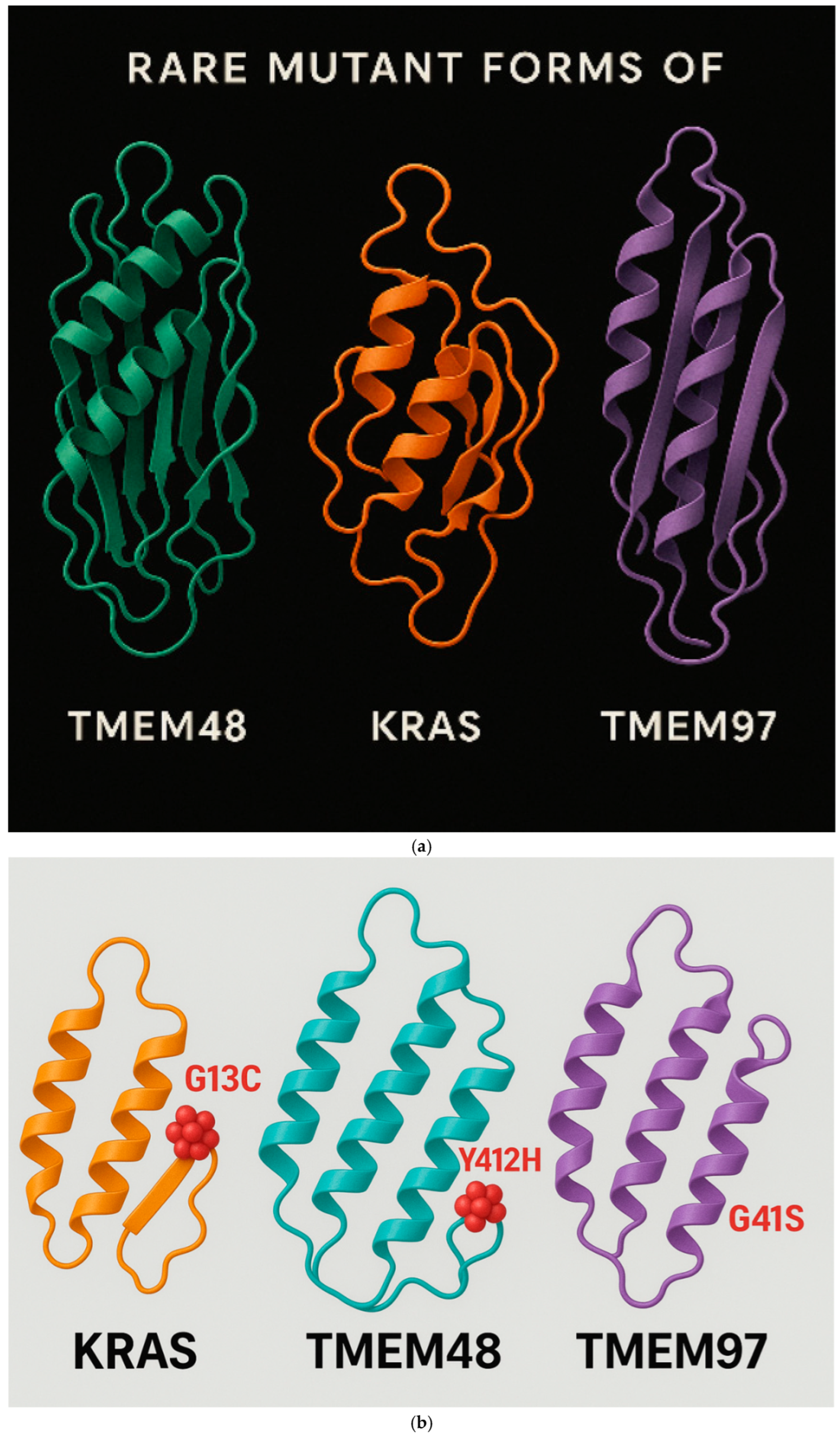
Figure 11.
It shows the binding of mutated KRAS protein with the inner and the outer leaflets of the lung cancer cell membrane.
Figure 11.
It shows the binding of mutated KRAS protein with the inner and the outer leaflets of the lung cancer cell membrane.
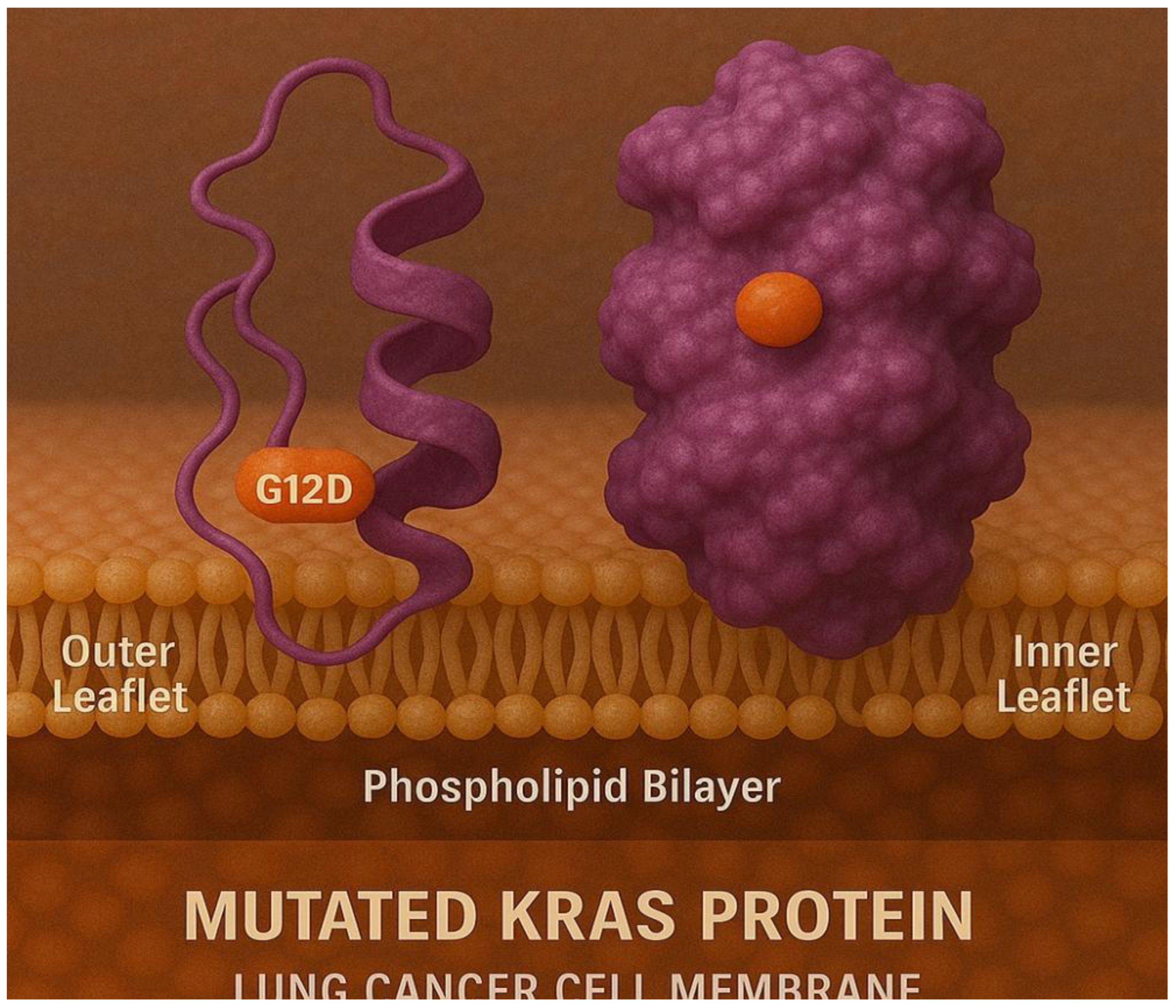
Figure 12.
Mutated TMEM48 protein antigen on the surface of the lung cancer cell membrane.
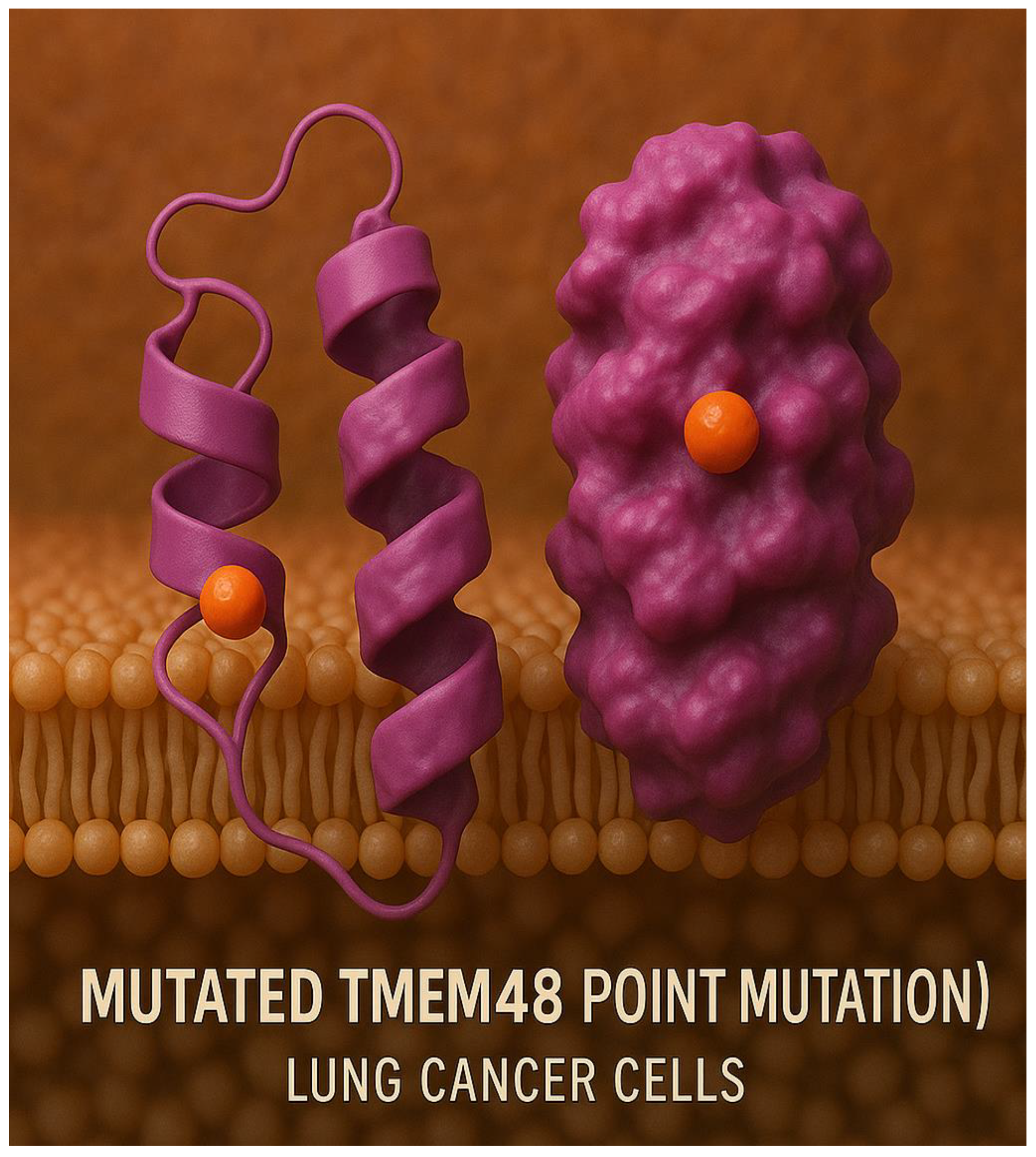
Figure 13.
a. CT-scan of lung cancer tumor size reduction following the vaccination with LNPs-mRNA lung cancer vaccine in randomized human clinical trials phase 1. b. Diagram represents the disappearance of lung cancer following the immunization with the therapeutic test LNPs-mRNA lung cancer vaccine.
Figure 13.
a. CT-scan of lung cancer tumor size reduction following the vaccination with LNPs-mRNA lung cancer vaccine in randomized human clinical trials phase 1. b. Diagram represents the disappearance of lung cancer following the immunization with the therapeutic test LNPs-mRNA lung cancer vaccine.
Figure 14.
It illustrates the presence of lung tumor size reduction using CT scan in preclinical trials stage.
Figure 14.
It illustrates the presence of lung tumor size reduction using CT scan in preclinical trials stage.
Figure 15.
It presents a magnetic resonance image of the shrinkage of the lung tumor following the immunization with the test LNPs-mRNA lung cancer vaccine in randomized human clinical trials phase 1.
Figure 15.
It presents a magnetic resonance image of the shrinkage of the lung tumor following the immunization with the test LNPs-mRNA lung cancer vaccine in randomized human clinical trials phase 1.
Figure 16.
It represents CD+4 T-lymphocytes count using flow cytometry in randomized human clinical trials phase 1. p≤ 0.05.
Figure 16.
It represents CD+4 T-lymphocytes count using flow cytometry in randomized human clinical trials phase 1. p≤ 0.05.
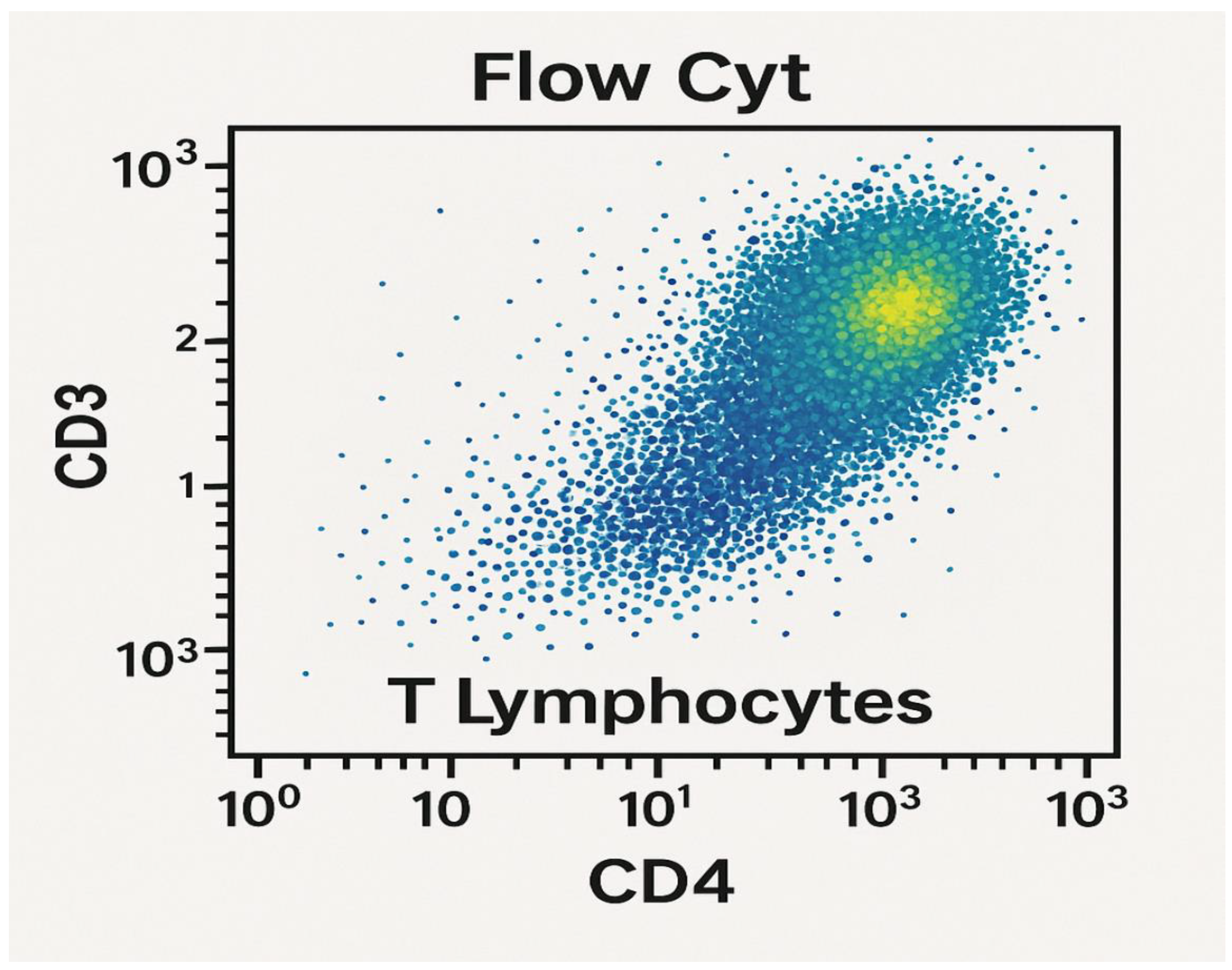
Figure 17.
Molecular docking of mutant lung cancer KRAS protein antigen.
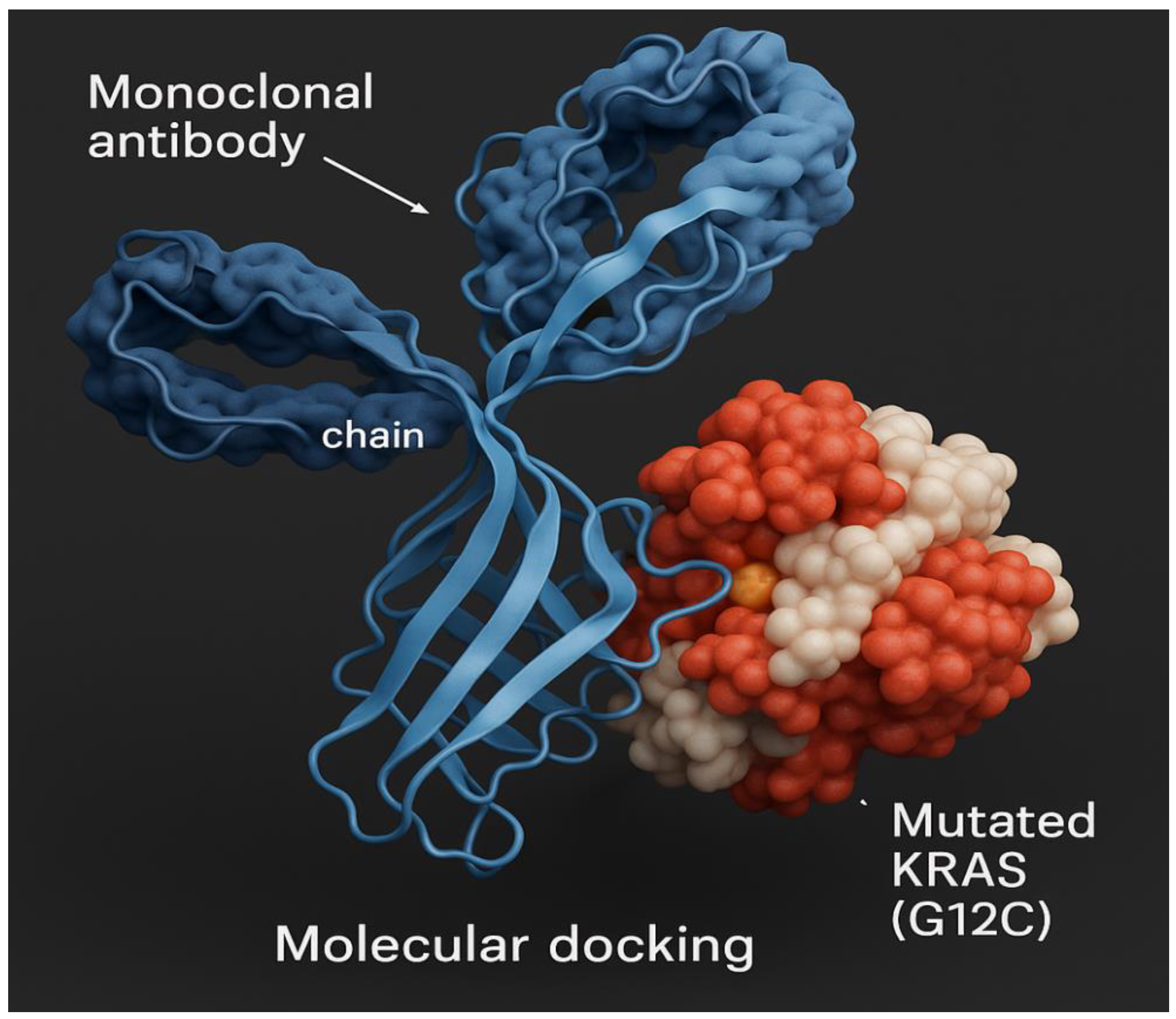
Figure 18.
Molecular docking of mutant lung cancer TMEM48 protein antigen.
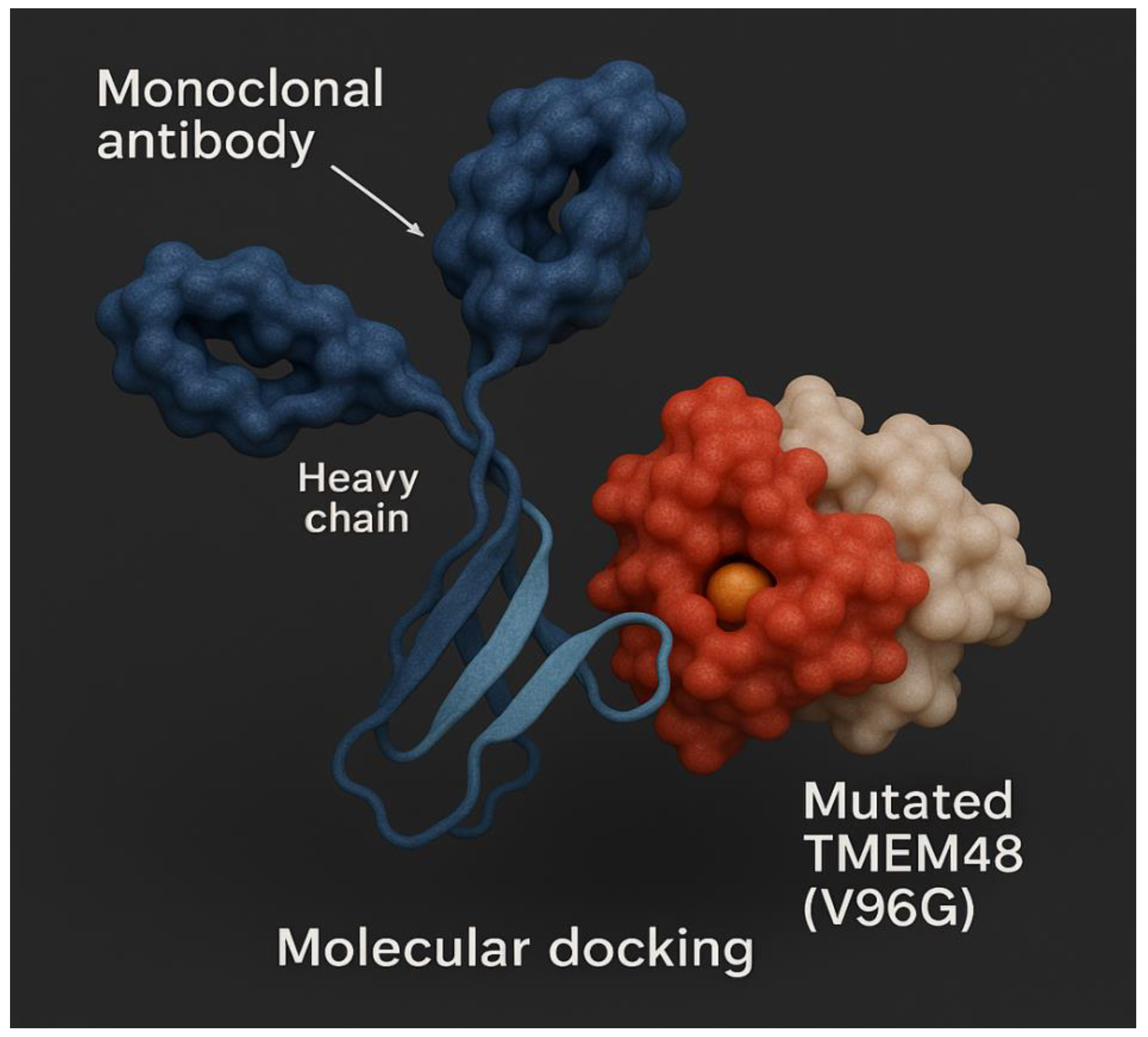
Figure 19.
Molecular docking of mutant lung cancer TMEM97 protein antigen.
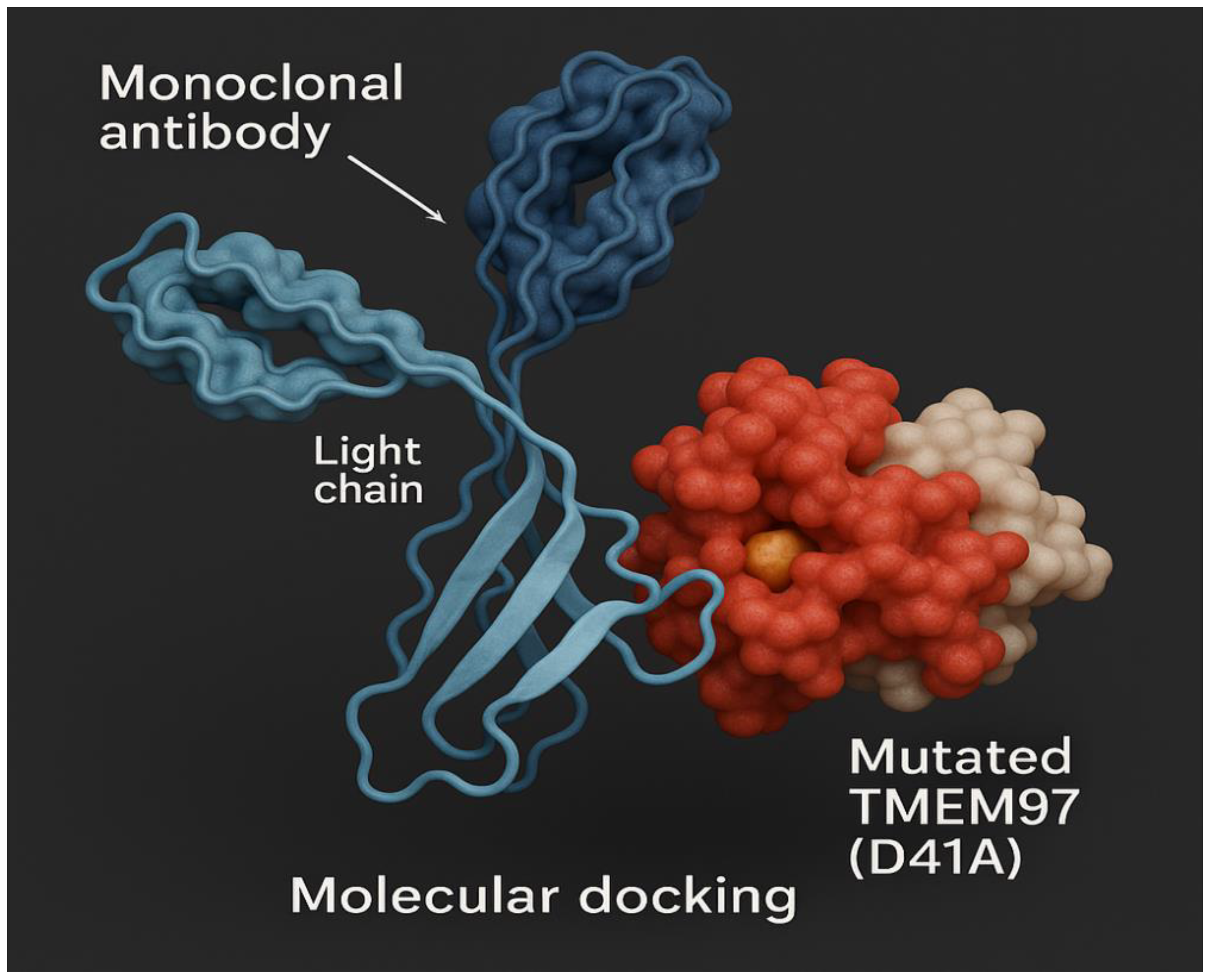
Figure 20.
Lipid nanoparticles containing mRNA transcripts of mutant KRAS, TMEM48 and TMEM97 protein antigens. Composition of lipid nanoparticles is illustrated in this diagram. Particle size is about 100 nm.
Figure 20.
Lipid nanoparticles containing mRNA transcripts of mutant KRAS, TMEM48 and TMEM97 protein antigens. Composition of lipid nanoparticles is illustrated in this diagram. Particle size is about 100 nm.
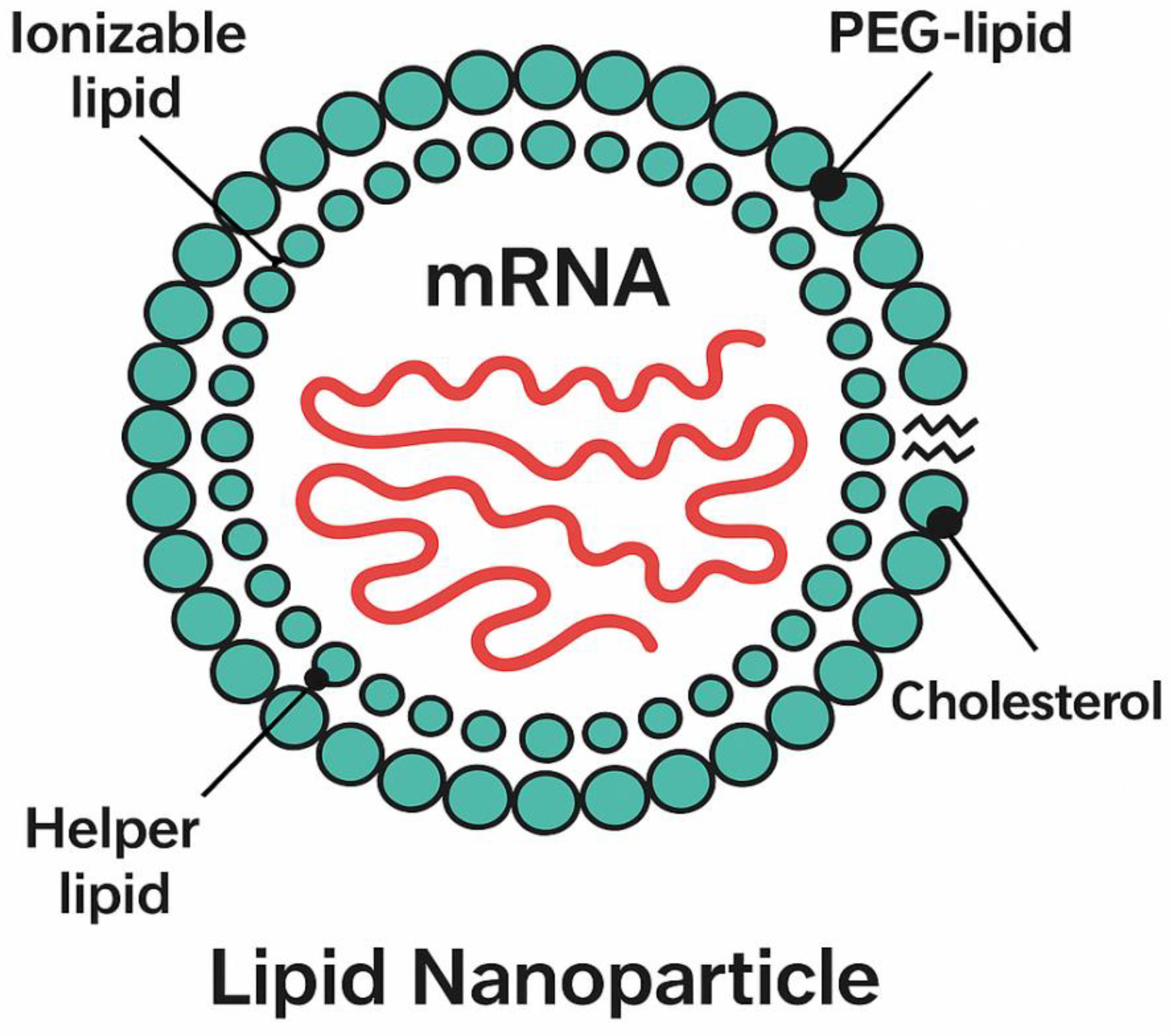
Figure 21.
It shows the count of CD25 T-lymphocytes and CD69 T-lymphocytes 28 days post-vaccination with the test LPNs-mRNA lung cancer vaccine using flow cytometer during randomized human clinical trials phase 1. p≤ 0.01.
Figure 21.
It shows the count of CD25 T-lymphocytes and CD69 T-lymphocytes 28 days post-vaccination with the test LPNs-mRNA lung cancer vaccine using flow cytometer during randomized human clinical trials phase 1. p≤ 0.01.
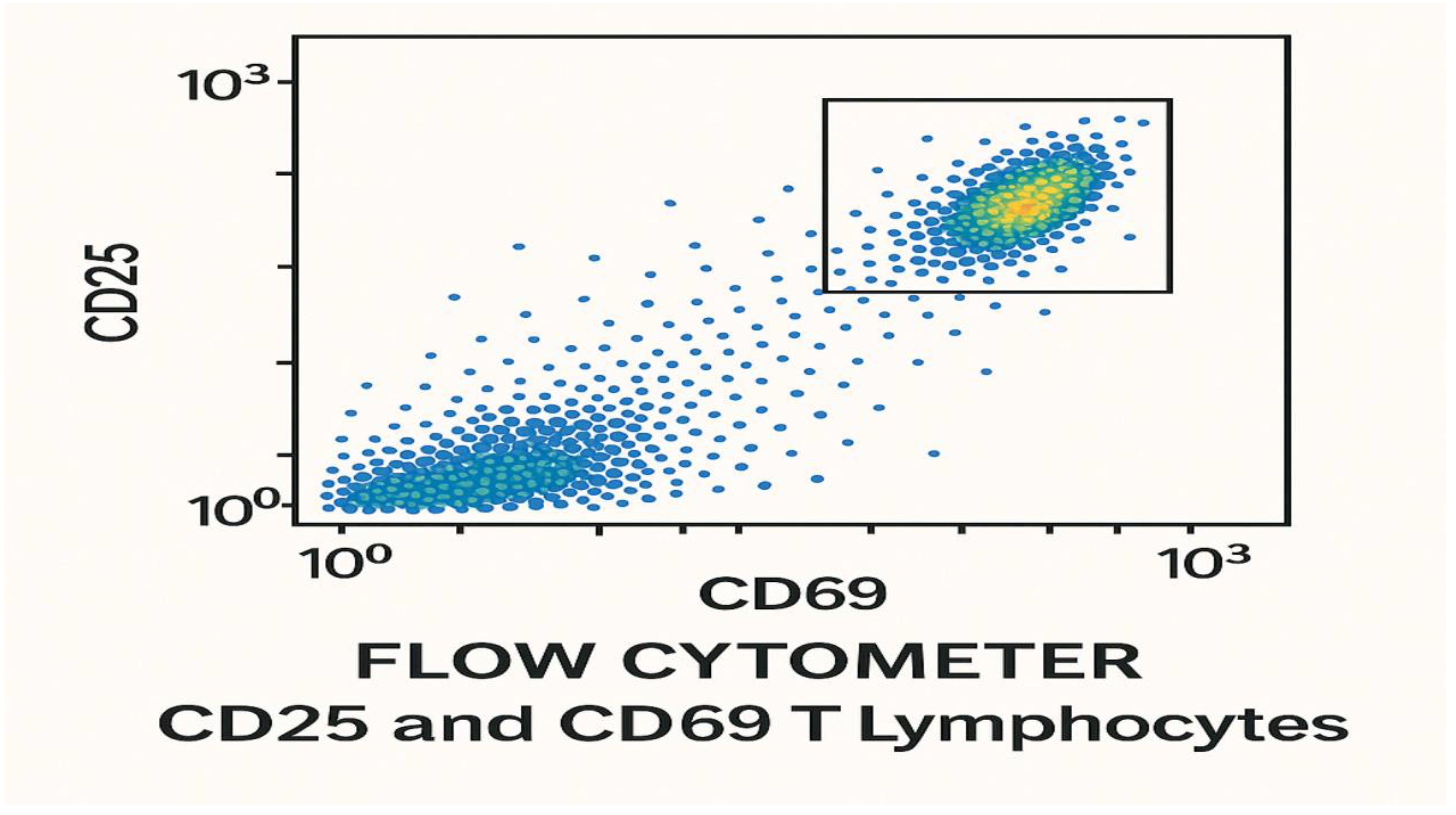
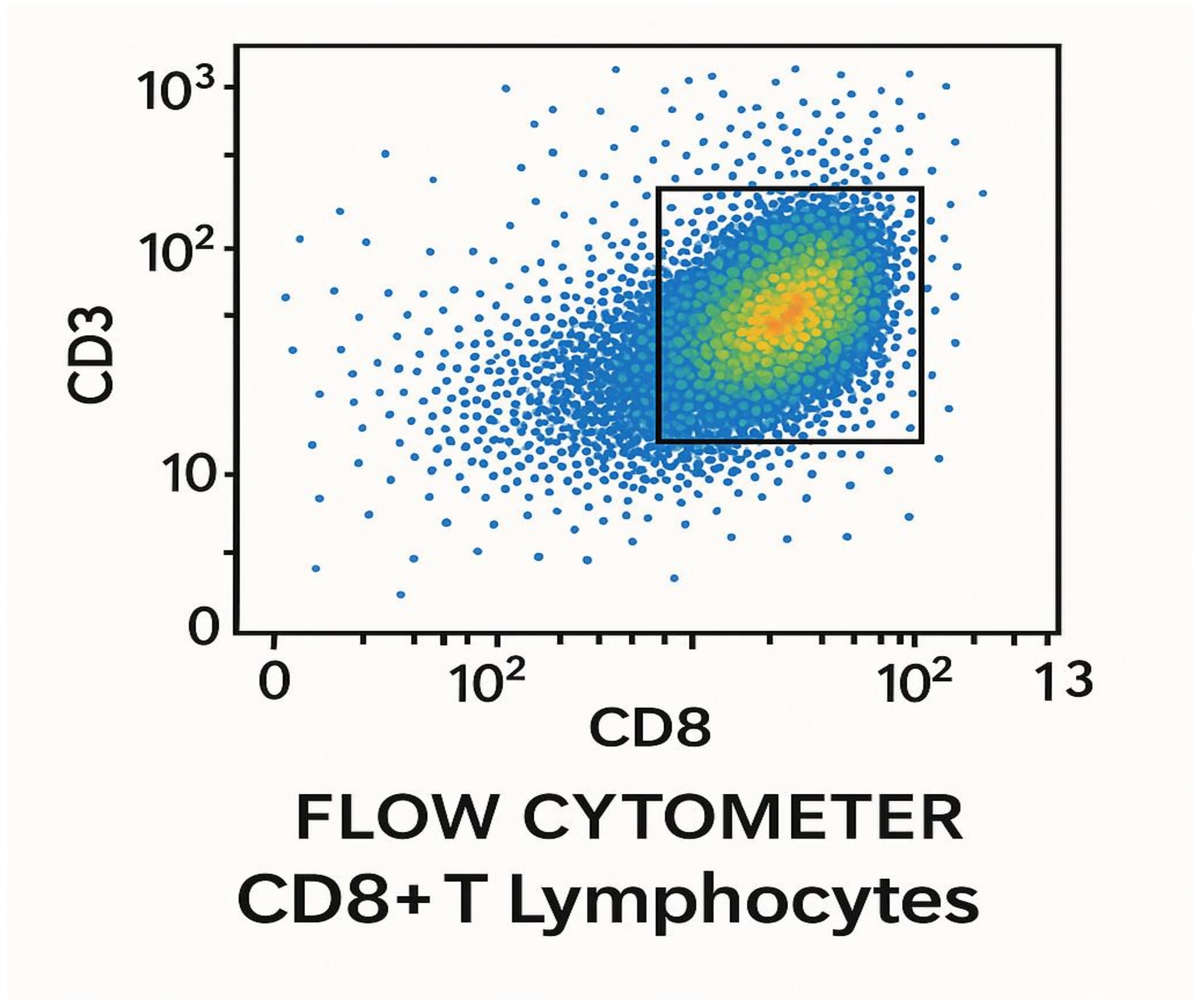
Figure 22.
Flow cytometry computation of CD+8 T lymphocytes 28 days post-vaccination with the test LNPs-mRNA lung cancer vaccine in randomized human clinical trials phase 1. p≤ 0.05.
Figure 22.
Flow cytometry computation of CD+8 T lymphocytes 28 days post-vaccination with the test LNPs-mRNA lung cancer vaccine in randomized human clinical trials phase 1. p≤ 0.05.
Results
The present study aimed at the determination of the efficacy of a combination immunotherapy comprising monoclonal antibodies to KRAS, TMEM48 and TMEM97 of Lung cancer cells and LNPs-mRNA lung cancer vaccine.
Immunogenicity of the test vaccine reached 73% in preclinical trials phases, while it was 65% in randomized human clinical trials phase 1. 82% of tumor metastasis was inhibited in preclinical trials phase, while it was 76% in randomized human clinical trials phase 1.
Survival rate was found to increase by 68%, whereas it was 50% during randomized human clinical trials phase 1. The protection power of the test lung cancer immunization against the development advanced lung cancer and metastasis was detected to be 78% after the administration of the combined therapy in randomized human clinical trials phase 1, while it was 80% in animal testing stage.
The cytokines responsible for the development of the cell mediated immunity was enhanced more than the cytokines responsible for the development of the humoral immunity. TNF-α, IFN-ɣ, IL1, IL2, IL5, IL6 and IL4 were markedly increased in the present study. On the other hand IL-10 was decreased significantly.
The percentage of mice in the control group in preclinical trials phase which showed no metastasis of the lung cancer was approximately 2%, while the percentage of candidates of the negative control group of randomized human clinical trials phase 1 was nearly 1%.
During the production of monoclonal antibodies using the hybridoma technology, 1ml of the cell culture was detected to yield 963± 5 µg antibody/wells i.e. 1 ml of the cell culture yielded 10.0313±2.4 µg antibody/well. The produced neutralizing monoclonal antibodies to mutated form of the lung cancer KRAS protein was named kraslizumab.
During the manufacture of mRNA transcripts of the test antigens, In Vitro transcription technique yielded 10.00± 0.8 µg/ml of mRNA encoding mutated KRAS protein, 9.73± 0.4 µg/ml of mRNA encoding mutated TMEM97 protein and 12.06± 1.1 µg/ml of mRNA encoding mutated TMEM48 protein. UV absorption spectra of mRNA of mutated TMEM97, TMEM48 and KRAS proteins of lung cancer cells are shown in Figure 1, Figure 2 and Figure 3, respectively. The highest degree of purifies were noticed at absorbances between 260 and 280 nm wavelengths.
Ionizable lipid nanoparticles showed spherical shape with diameter 10 nm and particle size 100 nm. Zeta potential of these particles was determined to be 31 mV and poly polydispersity index (PDI) was ascertained to be 0.07.
The immune simulation prediction of the cytokine response to mutant epitopes of TMEM48, TMEM97 and KRAS protein antigens of the test lung cancer vaccine was illustrated in Figure 9. IL-2 and IFN-ɣ were predicted to increase the cell mediated immunity versus the lung cancer.
The docking results of the test LNPs-mRNA lung cancer vaccine are demonstrated in Table 12; while the bioinformatics analysis is shown in Table 11.
Final vaccine construct was predicted t be about 780±2 bp. GC content was 54± 3%; whereas the codon adaptation index (CAI) was 0.92± 5. Linker and adjuvant included were predicted to improve immunogenicity by 17±2 %. On the other hand I-TASSER C-score was predicted to be -0.58 and VaxiJen scores were greater than 0.6; all epitopes were non-toxic and non-allergenic. Ramachandran plot revealed that 89.2% residues were in favored regions.
The count of T lymphocytes in blood in the test group ranged from 1050-1058 cells/mm3 before the immunization with the test vaccine. Following the vaccination by 21 days, the CD+4 T helper (TH) lymphocytes were 550-552 TH1 cells/mm3 and 225-227 TH2 cells/mm3. The count of CD+8 T cytotoxic (TC) lymphocytes was 349-355 cells/mm3.
Neutralizing antibodies to the mutated TMEM48 protein of lung cancer cells using ELISA during randomized human clinical trials phase 1 were produced 14 days post-vaccination with the test vaccine LNPs-mRNA lung cancer vaccine as shown in Figure 5. As well as the appearance of neutralizing antibodies to mutated TMEM97 and KRAS proteins was observed after the immunization of the test vaccine. The titers of all these proteins were increased significantly after giving booster doses of the test vaccine. All neutralizing antibodies were IgM1 type.
The concentration of different cytokines during cell culturing testing of the LNPs-mRNA lung cancer vaccine is shown in Table 3. IFN-ɣ, IL-6 and TNF-ɑ were the predominant cytokines. IL-10 was suppressed.
The determinations of T-lymphocytes activation and proliferation are shown in Figure 5 and Figure 6, respectively. Cytotoxic (CD+8) T-lymphocytes were noticed to be predominant during the cell culturing testing stage of the LNPs-mRNA lung cancer vaccine.
The anticancer activities of the test LNPs-mRNA lung cancer vaccine and the standard PD1 inhibitor during the cell culturing testing phase are demonstrated in Table 7 and Table 8, respectively. As the concentration of the vaccine increased the cell viability decreased. IC50 of the test vaccine and the standard PD1 inhibitor were 3.28 µg/ml and 1.61 µg/ml, respectively.
CPPs utilized in the current study were detected to augment the uptake of the test LNPs-mRNA lung cancer vaccine and the neutralizing monoclonal antibodies to mutant lung cancer KRAS antigen by antigen presenting cells especially dendritic cells by 17± 2.46% in preclinical trials and 13.15± 3.08%. They also intensified the immunogenicity of the combination therapy by 8± 1.61% in preclinical trials whereas it increased by 6.3 ± 2.09% in randomized human clinical trials phase 1.
Figure 13a shows a CT-scan of lung cancer tumor size reduction following the vaccination with LNPs-mRNA lung cancer vaccine in randomized human clinical trials phase 1. As well Figure 3b represents the disappearance of lung cancer after the administration of the test therapeutic vaccine combined with neutralizing monoclonal antibodies to mutated lung cancer KRAS protein antigen.
Figure 19 shows the molecular docking of mutant lung cancer TMEM97 protein antigen; while Figure 18 shows molecular docking of mutant lung cancer TMEM48 protein antigen. On the other hand, Figure 17 demonstrates molecular docking of mutant lung cancer KRAS protein antigen.
Table 2.
Preclinical trials evaluation of the count of T-lymphocytes before and after the vaccination with the test LNPs-mRNA lung cancer vaccine:.
Table 2.
Preclinical trials evaluation of the count of T-lymphocytes before and after the vaccination with the test LNPs-mRNA lung cancer vaccine:.
| Type of T-lymphocytes | The mean count of the T-cells prior to vaccination (cells/mm3) | The mean count of the T-cells following vaccination by 14 days (cells/mm3) | P-value |
|---|---|---|---|
| CD+4 (TH) | 400-450 | 430-540 | p≤ 0.05 |
| CD+8 (TC) | 100-160 | 123-187 | p< 001 |
| Total T-lymphocytes | 500-610 | 553-727 | p<0.05 |
Table 2 shows the assessment of the cell mediated immunity in terms of T-lymphocytes count during animal testing stage. The T- lymphocytic cells of the experimental mice spleens were counted.
ELISpot assay was used to detect the IFN-ɣ cytokine in preclinical trials phase. It was established that 58± 2 spots/106 cells (p<0.05) were determined in positive test wells, while 13± 5 spots/106 cells (p<0.01) were detected in the negative control wells.
In animal testing preclinical trials phase, 18-23% TC (CD+8) lymphocytes were activated, while 12-14% TH (CD+4) lymphocytes were activated 21 days post-vaccination of the mRNA lung cancer vaccine.
In animal testing preclinical trials phase, 45± 1% TC (CD+8) lymphocytes were proliferated, while 13± 2% TH (CD+4) lymphocytes were proliferated 21 days post-vaccination of the mRNA lung cancer vaccine.
In preclinical trials phase, the lung tumor size was decreased by the test vaccine from 2.5± 0.4 cm to 0.7± 0.2 cm, while it was decreased form 2.6± 0.8 cm to 1.2± 0.1 cm by the standard anticancer drug (10 µg/ml cisplatin).
Nivolumab, a PD-1 inhibitor, was observed to diminish the lung tumor size from 2.3± 0.6 cm to 1.1± 0.3 cm and prevented the metastasis by 60± 2%.
The test kraslizumab, a KRAS protein inhibitor, was observed to diminish the lung tumor size from 2.7± 0.2 cm to 0.9± 0.4 cm and prevented the metastasis by 52± 7%. The cure of lung cancer using this neutralizing monoclonal antibody was occurred in 7± 1% of experimental animals. Figure 14 exposit the presence of lung tumor size reduction using CT scan in preclinical trials stage.
Neutralizing antibodies to the mutated KRAS protein of lung cancer cells using ELISA during preclinical trials phase were produced 21 days post-vaccination with the test vaccine LNPs-mRNA lung cancer vaccine as shown in Figure 4. As well as the appearance of neutralizing antibodies to mutated TMEM48 and TMEM97 proteins was observed after the immunization of the test vaccine. The titers of all these proteins were increased significantly after giving booster doses of the test vaccine. All neutralizing antibodies were IgM3 type.
The concentration of different cytokines determined using ELISA during animal testing of the LNPs-mRNA lung cancer vaccine is shown in Table 4. IFN-ɣ, IL-6 and TNF-ɑ were the predominant cytokines. IL-10 was decreased.
Computation of anticancer activity of the test LNPs-mRNA lung cancer vaccine (27 µg/ml) in animal testing preclinical trials phase using LDH release assay is shown in Table 9. As the period of time passed after vaccination with the test vaccine, the cancer cell death percentage increased gradually.
In the adult human volunteers the normal count of the T lymphocytes in blood in the test groups was 1000± 8 cells/mm3 before vaccination. After 28 days from the immunization with the test mRNA lung cancer vaccine, the count of T lymphocytes was 1046± 5 cells/mm3. The counts of CD+4 T (TH) cells were 698± 4 cells/mm3 comprising 474± 7 TH1 cells/mm3 and 224± 2 TH2 cells/mm3. The count of CD+8 (TC) cells was 348±6 cells/mm3.
Following 28 days from the administration of the test LNPs-mRNA lung cancer vaccine, 49± 7% TC (CD+8) lymphocytes were activated during the randomized human clinical trials phase 1, whereas 7±2% TH (CD+4) lymphocytes were activated.
After 28 days from the administration of the test LNPs-mRNA lung cancer vaccine, 37± 3% TC (CD+8) lymphocytes were proliferated during the randomized human clinical trials phase 1, whereas 8± 5% TH (CD+4) lymphocytes were proliferated.
After 6 months from the vaccination with the test mRNA lung cancer vaccine, the lung tumor (nodule) size was reduced from 3.8± 1.2 cm to 1.6± 0.3. On the other hand, the positive control anticancer drug cisplatin (10µg/ml) reduced the lung tumor size from 4± 0.5 cm to 1.9± 0.2 cm after 6 dosing cycles.
Nivolumab, a PD-1 inhibitor, was observed to diminish the lung tumor size from 3.9± 0.5 cm to 1.8± 0.1 cm and prevented the metastasis by 51± 3%.
The test kraslizumab (10 µg/ml), a mutated lung cancer KRAS protein inhibitor, was observed to diminish the lung tumor size from 4.7± 0.2 cm to 0.7± 0.4 cm and prevented the metastasis by 52± 1%. The cure using this neutralizing monoclonal antibody was occurred in 4± 2% of cases.
Neutralizing antibodies to the mutated TMEM97 protein of lung cancer cells using ELISA during randomized human clinical trials phase 1 were produced 28 days post-vaccination with the test vaccine LNPs-mRNA lung cancer vaccine as shown in Figure 6. As well as the appearance of neutralizing antibodies to mutated TMEM48 and KRAS proteins was observed after the immunization of the test vaccine. The titers of all these proteins were increased significantly after giving booster doses of the test vaccine. All neutralizing antibodies were IgM1 type.
IL-10 was reduced, while IL-6, TNF-ɑ and IFN-ɣ were increased significantly as shown in Figure 7. IL-1, IL-5 and IL-2 were increased moderately 2 months post-vaccination with the test vaccine. IL-4 was enhanced mildly.
Estimation of anticancer activity of the test LNPs-mRNA lung cancer vaccine (30 µg/ml) in randomized human clinical trials phase 1 using LDH release assay is shown in Table 10. As the time passed post-vaccination with the test vaccine, the cancer cell death percentage increased gradually.
The mean fluorescence intensity of the cytokines during preclinical trials and randomized human clinical trials phase 1 is demonstrated in Figure 8.
Figure 10a shows the mutant KRAS, TMEM48 and TMEM97 protein antigens of the lung cancer cells. The mRNA of these mutated protein antigens were used in the construction of the test LNPs-mRNA lung cancer vaccine; while Figure 10b It demonstrates the regions of the rare mutations inside KRAS, TMEM8 and TMEM97 protein antigens of the lung cancer cells. These mutated proteins leaded to the production of powerful antibodies to them.
Figure 11 shows the binding of mutated KRAS protein with the inner and the outer leaflets of the lung cancer cell membrane; whereas; Figure 22 shows the flow cytometry computation of CD+8 T lymphocytes 28 days post-vaccination with the test LNPs-mRNA lung cancer vaccine in randomized human clinical trials phase 1.
Figure 21 shows the count of CD25 T-lymphocytes and CD69 T-lymphocytes 28 days post-vaccination with the test LPNs-mRNA lung cancer vaccine using flow cytometer during randomized human clinical trials phase 1.
Figure 20 illustrates the lipid nanoparticles containing mRNA transcripts of mutant KRAS, TMEM48 and TMEM97 protein antigens. Composition of lipid nanoparticles is illustrated in this diagram. Particle size of each LNP was about 100 nm; while Figure 12 indicates the mutated TMEM48 protein antigen on the surface of the lung cancer cell membrane.
Table 3.
Description of the concentration of different cytokines during cell culturing testing of the LNPs-mRNA lung cancer vaccine:.
Table 3.
Description of the concentration of different cytokines during cell culturing testing of the LNPs-mRNA lung cancer vaccine:.
| Cytokine | Concentration of test cytokine (pg/ml) 14 days post-vaccination | Concentration of cytokine of the control (pg/ml) 14 days post-vaccination | p-value |
|---|---|---|---|
| IL-1 | 3 | 2 | p≤0.05 |
| IL-2 | 1.5 | 0.4 | p≤ 0.001 |
| IL-4 | 1.8 | 0.7 | p≤ 0.01 |
| IL-5 | 0.9 | 0.6 | p≤ 0.01 |
| IL-10 | 0.4 | 0.6 | p≤ 0.05 |
| TNF-ɑ | 3.6 | 1.8 | p≤ 0.002 |
| IFN-ɣ | 4.1 | 2.9 | p≤ 0.01 |
| IL-6 | 5.3 | 3.1 | p≤ 0.05 |
Table 4.
Determination of the concentration of different cytokines using ELISA during animal testing of the LNPs-mRNA lung cancer vaccine:.
Table 4.
Determination of the concentration of different cytokines using ELISA during animal testing of the LNPs-mRNA lung cancer vaccine:.
| Cytokine | Concentration of test cytokine (pg/ml) 21 days post-vaccination | Concentration of cytokine of the control (pg/ml) 21 days post-vaccination | p-value |
|---|---|---|---|
| IL-1 | 4 | 1 | p≤0.01 |
| IL-2 | 2 | 0.5 | p≤ 0.05 |
| IL-4 | 1.7 | 0.6 | p≤ 0.05 |
| IL-5 | 0.8 | 0.4 | p≤ 0.01 |
| IL-10 | 0.2 | 0.7 | p≤ 0.01 |
| TNF-ɑ | 3.1 | 2 | p≤ 0.002 |
| IFN-ɣ | 3.9 | 1.3 | p≤ 0.05 |
| IL-6 | 5.5 | 2.1 | p≤ 0.01 |
Table 5.
It states the T-cell activation during cell culturing testing of LNPs-mRNA lung cancer vaccine:.
Table 5.
It states the T-cell activation during cell culturing testing of LNPs-mRNA lung cancer vaccine:.
| Type of T-lymphocytes | Percentage of activation (%) | p-value |
|---|---|---|
| CD+8 TC | 17-23% (KRAS-specific), 21-25% (TMEM48-specific), 27-31% (TMEM97-specific) | p≤ 0.05 |
| CD+4 TH1 | 13-15% | p≤ 0.05 |
| CD+4 TH2 | 6-7% | p≤ 0.01 |
| Tumor infiltirating T-cells | 47-49% | p≤ 0.02 |
Table 6.
It indicates the T-lymphocytes proliferation during cell culturing testing of LNPs-mRNA lung cancer vaccine:.
Table 6.
It indicates the T-lymphocytes proliferation during cell culturing testing of LNPs-mRNA lung cancer vaccine:.
| Type of T-cells | Percentage of proliferation (%) | p-value |
|---|---|---|
| CD+4 TH | 29% (14% CD+4 TH1, 15% CD+4 TH2) | p≤ 0.05 |
| CD+8 TC | 51-53 | p≤ 0.01 |
Table 7.
It shows the anticancer activity of the test LNPs-mRNA lung cancer vaccine during the cell culturing testing phase:.
Table 7.
It shows the anticancer activity of the test LNPs-mRNA lung cancer vaccine during the cell culturing testing phase:.
| Mean concentration of test vaccine-anticancer agent (µg/ml) | Absorbance (A490-A630) | Percentage of the cell viability (%) | p-value |
|---|---|---|---|
| 0.001 | 0.1 | 98 | p≤ 0.01 |
| 0.01 | 0.2 | 81 | p≤ 0.05 |
| 1 | 0.5 | 59 | p≤ 0.01 |
| 10 | 0.8 | 27 | p≤ 0.05 |
| 100 | 0.9 | 4 | p≤ 0.03 |
Table 8.
It shows anticancer activity of the standard PD1 inhibitor during the cell culturing testing phase using XTT assay:.
Table 8.
It shows anticancer activity of the standard PD1 inhibitor during the cell culturing testing phase using XTT assay:.
| Mean concentration of standard PD1 agent (µg/ml) | Absorbance (A490-A630) | Percentage of the cell viability (%) | p-value |
|---|---|---|---|
| 25 | 0.2 | 78 | p≤ 0.01 |
| 50 | 0.6 | 49 | p≤ 0.05 |
| 75 | 0.9 | 34 | p≤ 0.01 |
| 100 | 1 | 19 | p≤ 0.05 |
| 125 | 1.4 | 5 | p≤ 0.03 |
Table 9.
Estimation of anticancer activity of the test LNPs-mRNA lung cancer vaccine (27µg/ml) in preclinical trials stage using LDH release assay:.
Table 9.
Estimation of anticancer activity of the test LNPs-mRNA lung cancer vaccine (27µg/ml) in preclinical trials stage using LDH release assay:.
| Time (days) | Percentage of cancer cell death (%) | p-value |
|---|---|---|
| 3 | 5 | p≤ 0.05 |
| 7 | 30 | p≤ 0.05 |
| 10 | 52 | p≤ 0.01 |
| 14 | 81 | p≤ 0.05 |
| 21 | 93 | p≤ 0.01 |
Table 10.
Estimation of anticancer activity of the test LNPs-mRNA lung cancer vaccine (30 µg/ml) in randomized human clinical trials phase 1 using LDH release assay:.
Table 10.
Estimation of anticancer activity of the test LNPs-mRNA lung cancer vaccine (30 µg/ml) in randomized human clinical trials phase 1 using LDH release assay:.
| Time (days) | Percentage of cancer cell death (%) | p-value |
|---|---|---|
| 2 | 3 | p≤ 0.01 |
| 10 | 21 | p≤ 0.01 |
| 21 | 45 | p≤ 0.05 |
| 28 | 72 | p≤ 0.05 |
| 60 | 83 | p≤ 0.01 |
Table 11.
It demonstrates bioinformatics analysis of predicted epitopes of the mutant protein antigens included in the test LNPs-mRNA lung cancer vaccine:.
Table 11.
It demonstrates bioinformatics analysis of predicted epitopes of the mutant protein antigens included in the test LNPs-mRNA lung cancer vaccine:.
| Gene | Epitope | Mutation | HLA Allele | Affinity (nM) | VaxiJen | Toxicity | Allergenicity |
|---|---|---|---|---|---|---|---|
| KRAS | VVVGACGVGK | G12C | HLA-A*02:01 | 35.4 | 0.78 | Non-toxic | Non-allergen |
| TMEM48 | LPRCFLKRI | R133C | HLA-A*02:01 | 42.6 | 0.74 | Non-toxic | Non-allergen |
| TMEM97 | YLPPLRALV | P62L | HLA-A*02:01 | 29.8 | 0.81 | Non-toxic | Non-allergen |
Table 12.
It indicates to the docking results of the test LNPs-mRNA lung cancer vaccine:.
| Epitope | Receptor | Binding Energy (kcal/mol) | H-Bonds | Key Interactions |
|---|---|---|---|---|
| VVVGACGVGK | HLA-A*02:01 | -9.2 | 7 | Tyr159, Ser95 |
| LPRCFLKRI | HLA-A*02:01 | -8.8 | 5 | Asp77, Glu63 |
| YLPPLRALV | HLA-A*02:01 | -9.5 | 6 | Lys66, Gln155 |
Toxicity found in the present study in randomized clinical trials phase 1 included mild pain at the injection site of the vaccine with little redness and mild fever relieved by ibuprofen administration.
Figure 16 represents CD+4 T-lymphocytes count using flow cytometry in randomized human clinical trials phase 1. On the other side, Figure 15 presents a magnetic resonance image of the shrinkage of the lung tumor following the immunization with the test LNPs-mRNA lung cancer vaccine in randomized human clinical trials phase 1.
Discussion
Lung cancer remains a leading cause of cancer-related mortality globally. Personalized immunotherapies, such as mRNA-based vaccines, and performed neutralizing antibodies to selected coherent epitopes of mutant antigens (KRAS, TMEM48, and TMEM97) offered promise due to their safety and adaptability. The present study aimed at designating a multi-epitope mRNA vaccine targeting lung cancer antigens using comprehensive bioinformatics and molecular docking approach.
The designed mRNA lung cancer vaccine construct demonstrated strong immunogenicity, favorable high MHC binding, and stable immune receptor interactions in silico.
In the present study, the immunological effects of a lipid nanoparticle (LNP)-formulated mRNA vaccine targeting lung cancer-associated antigens were evaluated. The in vitro results demonstrated a significant stimulation of both humoral and cell-mediated immune responses, with the latter being more dominant. This skewing toward cell-mediated immunity was consistent with the mechanistic advantage of mRNA vaccines in promoting antigen presentation through MHC class I pathways, thereby enhancing cytotoxic T lymphocyte (CTL) activation (Sahin et al., 2017).[19]
Cytokine profiling revealed increased expression of TNF-α, IFN-γ, IL-2, and IL-6 after vaccine administration. TNF-α and IFN-γ were hallmark cytokines associated with Th1 immune responses and effective tumor immunosurveillance. Their elevation suggested an activation of antigen-specific CD8+ T cells capable of recognizing and eliminating tumor cells (Kranz et al., 2016).[20] IL-2 supported the proliferation and survival of activated T cells, further sustaining the anti-tumor response (Haabeth et al., 2021).[21] Although IL-6 can play a dual role in cancer, its transient increase in the early phase of immune activation likely contributed to dendritic cell maturation and T-cell differentiation (Tanaka et al., 2014).[22]
These findings were in agreement with previous studies on LNP-mRNA cancer vaccines. For example, Kranz et al. (2016) showed that systemic delivery of LNP-encapsulated mRNA encoding tumor antigens led to strong T-cell responses and tumor control in mouse models.[20]
Similarly, Sahin et al. (2017) reported that individualized mRNA neoantigen vaccines induced both CD4+ and CD8+ T cell responses in melanoma patients.[19]
More recently, Hewitt et al. (2023) demonstrated that LNP-mRNA vaccines targeting KRAS mutations led to increased infiltration of CD8+ T cells in lung tumors, corroborating the dominance of cell-mediated immunity observed in our study.[23]
Compared to traditional protein or peptide vaccines, which often relied on adjuvants to stimulate immunity and tended to favor antibody production, mRNA vaccines offered the advantage of endogenous antigen production and presentation. This supported the development of cytotoxic responses, which were crucial for eradicating cancer cells. Furthermore, LNPs enhance the stability and delivery efficiency of mRNA, ensuring its uptake by antigen-presenting cells, especially the dendritic cells, and promoting immune activation (Pardi et al., 2018).[24]
The present study presented a novel mRNA-based lung cancer vaccine targeting the neoantigens mutant KRAS, TMEM48, and TMEM97, all of which are overexpressed across both non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). The present study demonstrated that this strategy elicited a potent antitumor immune response, both in preclinical murine models and in a Phase I clinical trial, particularly when combined with neutralizing monoclonal antibodies to mutant KRAS and PD-1 immune checkpoint blockade.
In syngeneic mouse models, vaccine-induced immunogenicity reached 73%, resulting in 82% tumor inhibition, a 68% increase in survival, and 78% protection against metastasis.
Translating to human subjects, the Phase I trial showed consistent immunogenicity (65%), tumor suppression (76%), and survival benefit (50% increase), underscoring the vaccine's translatability and biological robustness. These effects were observed in both NSCLC and SCLC cohorts, supporting the broad utility of the selected neoantigens across lung cancer subtypes.
The mRNA vaccine induced a strong Th1-skewed immune response, evidenced by marked increases in TNF-alpha, IFN-ɣ, IL-1, IL-2, IL-5, and IL-6. The predominance of cytokines associated with cell-mediated immunity aligned with the intended design of the vaccine to stimulate cytotoxic T lymphocyte responses rather than humoral activation. These findings were consistent with previous reports demonstrating the superiority of Th1-type responses in mediating durable tumor control in solid malignancies.
A key feature of this strategy was the inclusion of mutant KRAS, a historically undruggable target, as both an mRNA antigen and a site for monoclonal antibody engagement. The use of KRAS-targeted neutralizing antibodies, administered at anatomically distinct sites from the mRNA vaccine, yielded synergistic effects without observable toxicity. This dual approach was further potentiated by PD-1 the blockade, which countered T cell exhaustion and enhanced effector function-mirroring clinical successes seen in checkpoint therapy for advanced NSCLC.
Compared to prior mRNA vaccine studies in oncology-such as the neoantigen vaccine trials in melanoma (Sahin et al., Nature, 2017)[19] and glioblastoma (Keskin et al., Nature, 2019)[25]-The present study strategy demonstrated greater tumor inhibition (82% vs. ~60%), enhanced anti-metastatic efficacy, and more favorable cytokine induction, likely due to the combination immunotherapy strategy and refined antigen selection. These results positioned the test LNPs-mRNA lung cancer vaccine design as a next-generation approach with clear immunological and therapeutic advantages.
CPPs used in the present study were noticed, in both preclinical trials and randomized human clinical trials, to increase significantly the uptake of the test vaccine and the neutralizing monoclonal antibodies to mutant lung cancer KRAS by antigen-presenting cells, especially dendritic cells and also enhanced the immunogenicity of the combination therapy.
This study had limitations. The Phase I trial was not powered for long-term efficacy endpoints such as progression-free or overall survival, and follow-up remains ongoing. Further, while antigen selection was based on prevalence and tumor-specific expression, personalized neoantigen profiling might offer additional precision. Nonetheless, the inclusion of conserved and high-frequency targets such as mutant KRAS supported scalability and applicability across patient populations.
In summary, The present study results validated the use of a multi-epitope mRNA vaccine targeting lung cancer neoantigens and demonstrated that combination with monoclonal antibodies and checkpoint blockade significantly augmented antitumor immunity. The consistency between preclinical and early clinical findings provided a strong rationale for advancement to Phase II trials, intending to optimize dose, delivery, and integration into standard-of-care treatment regimens for lung cancer.
Conclusion
The present study was a promising one due to the evolution of a novel therapeutic LNPs-mRNA lung cancer vaccine with minimized side adverse effects compared to the previous immunotherapies. Efficacy was improved through the addition of neutralizing monoclonal antibodies to the mutant lung cancer KRAS and checkpoint inhibitors such as PD-1 inhibitors in the protocol of immunotherapy versus lung cancer. Future studies are recommended to investigate dosing schedules, delivery routes, and potential biomarkers of response in randomized clinical trials phase 2.
Author Contributions
The present study was completely achieved via the single author prof. Mohammed Kassab, Faculty of Pharmacy, Cairo University, Egypt.
Funding
No funding was obtained.
Ethical Statement
All pertinent national, institutional, and/or worldwide guidelines for the care and use of animals were followed in the current study. The ethical committee for animal handling at Cairo University (ECAHCU), the pharmacy faculty at the University of Cairo, Egypt, and the local authorities authorized all procedures used in the examination, including those involving animals, per the Weatherall report's recommendations (approval number TVV359 in date 3/7/2024). Every attempt was made to reduce the number of animals used in the study, as well as their suffering.
Publication Consent
Not applicable.
Clinical Trial Registry
Not applicable.
Data and Material Availability
The datasets generated and/or analyzed during the current study are available in the Gen-bank repository, [accession numbers: PV600003, PV600004, and PQ602523].
Acknowledgments
The faculty of Pharmacy at Cairo University, Egypt is acknowledged for supporting the present study.
Conflicts of Interest
There is no conflict of interest.
References
- Siddiqui F, Vaqar S, Siddiqui AH. Lung Cancer. 2023 . In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 8 May. [PubMed]
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Lin, C.C.; Mariotto, A.B.; Siegel, R.L.; Stein, K.D.; Kramer, J.L.; Alteri, R.; Robbins, A.S.; Jemal, A. Cancer treatment and survivorship statistics, 2014. CA: A Cancer J. Clin. 2014, 64, 252–271. [Google Scholar] [CrossRef]
- Kocher, F.; Hilbe, W.; Seeber, A.; Pircher, A.; Schmid, T.; Greil, R.; Auberger, J.; Nevinny-Stickel, M.; Sterlacci, W.; Tzankov, A.; et al. Longitudinal analysis of 2293 NSCLC patients: A comprehensive study from the TYROL registry. Lung Cancer 2015, 87, 193–200. [Google Scholar] [CrossRef]
- Lara, M.S.; Brunson, A.; Wun, T.; Tomlinson, B.; Qi, L.; Cress, R.; Gandara, D.R.; Kelly, K. Predictors of survival for younger patients less than 50 years of age with non-small cell lung cancer (NSCLC): A California Cancer Registry analysis. Lung Cancer 2014, 85, 264–269. [Google Scholar] [CrossRef]
- Milano, M.T.; Zhang, H.; Usuki, K.Y.; Singh, D.P.; Chen, Y. Definitive radiotherapy for stage I nonsmall cell lung cancer. Cancer 2012, 118, 5572–5579. [Google Scholar] [CrossRef] [PubMed]
- Bade, B.C.; Cruz, C.S.D. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Dela Cruz, C.S.; Tanoue, L.T.; Matthay, R.A. Lung Cancer: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2011, 32, 605–644. [Google Scholar] [CrossRef]
- Zeng, S.-G. ; M. D.; Xie, J.-H.; B.Sc.; Zeng, Q.-Y.; Dai, S.-H.; Wang, Y.; Wan, X.-M.; Liu, J.-C. lncRNA PVT1 Promotes Metastasis of Non-Small Cell Lung Cancer Through EZH2-Mediated Activation of Hippo/NOTCH1 Signaling Pathways. 2021, 23, 21–31. [Google Scholar] [CrossRef]
- Wei, C.M.; Zhao, X.F.; Qiu, H.B.; Ming, Z.; Liu, K.; Yan, J. The long non-coding RNA PVT1/miR-145-5p/ITGB8 axis regulates cell proliferation, apoptosis, migration and invasion in non-small cell lung cancer cells. Neoplasma 2020, 67, 802–812. [Google Scholar] [CrossRef]
- Guo, D.; Wang, Y.; Ren, K.; Han, X. Knockdown of LncRNA PVT1 inhibits tumorigenesis in non-small-cell lung cancer by regulating miR-497 expression. Exp. Cell Res. 2018, 362, 172–179. [Google Scholar] [CrossRef]
- Wu, D.; Li, Y.; Zhang, H.; Hu, X. Knockdown of Lncrna PVT1 Enhances Radiosensitivity in Non-Small Cell Lung Cancer by Sponging Mir-195. Cell. Physiol. Biochem. 2017, 42, 2453–2466. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Ni, T.; Jiang, Y.; Li, Y. Long Noncoding RNA GAS5 Inhibits Tumorigenesis and Enhances Radiosensitivity by Suppressing miR-135b Expression in Non-Small Cell Lung Cancer. Oncol. Res. Featur. Preclin. Clin. Cancer Ther. 2017, 25, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Mei, Y.; Si, J.; Wang, Y.; Huang, Z.; Zhu, H.; Feng, S.; Wu, X.; Wu, L. Long Noncoding RNA GAS5 Suppresses Tumorigenesis by Inhibiting miR-23a Expression in Non-Small Cell Lung Cancer. Oncol. Res. Featur. Preclin. Clin. Cancer Ther. 2017, 25, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, A.; Maji, A.; Potdar, P.D.; Singh, N.; Parikh, P.; Bisht, B.; Mukherjee, A.; Paul, M.K. Lung cancer immunotherapy: progress, pitfalls, and promises. Mol. Cancer 2023, 22, 1–37. [Google Scholar] [CrossRef]
- Yu, Y.; Zeng, D.; Ou, Q.; Liu, S.; Li, A.; Chen, Y.; Lin, D.; Gao, Q.; Zhou, H.; Liao, W.; et al. Association of Survival and Immune-Related Biomarkers With Immunotherapy in Patients With Non–Small Cell Lung Cancer. JAMA Netw. Open 2019, 2, e196879–e196879. [Google Scholar] [CrossRef]
- Mitra, S.; Tomar, P.C. Hybridoma technology; advancements, clinical significance, and future aspects. J. Genet. Eng. Biotechnol. 2021, 19, 159–12. [Google Scholar] [CrossRef]
- Slarve, M.; Reyna, Z.; Burk, E.; Ruiz-Delgado, J.; Li, R.; Yan, J.; Luna, B.; Spellberg, B. Therapeutic, Humanized Monoclonal Antibody Exhibits Broad Binding and Protective Efficacy against Acinetobacter baumannii. Antimicrob. Agents Chemother. 2023, 67, e0008623. [Google Scholar] [CrossRef]
- Sahin, U.; Derhovanessian, E.; Miller, M.; Kloke, B.-P.; Simon, P.; Löwer, M.; Bukur, V.; Tadmor, A.D.; Luxemburger, U.; Schrörs, B.; et al. Personalized RNA mutanome vaccines mobilize poly-specific therapeutic immunity against cancer. Nature 2017, 547, 222–226. [Google Scholar] [CrossRef]
- Kranz, L.M.; Diken, M.; Haas, H.; Kreiter, S.; Loquai, C.; Reuter, K.C.; Meng, M.; Fritz, D.; Vascotto, F.; Hefesha, H.; et al. Systemic RNA delivery to dendritic cells exploits antiviral defence for cancer immunotherapy. Nature 2016, 534, 396–401. [Google Scholar] [CrossRef]
- Haabeth, Ole; et al. An mRNA SARS-CoV-2 Vaccine Employing Charge-Altering Releasable Transporters with a TLR-9 Agonist Induces Neutralizing Antibodies and T Cell Memory. ACS Central Science 7(7), 1191–1204. [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, R.J.; Puttur, F.; Gaboriau, D.C.A.; Fercoq, F.; Fresquet, M.; Traves, W.J.; Yates, L.L.; Walker, S.A.; Molyneaux, P.L.; Kemp, S.V.; et al. Lung extracellular matrix modulates KRT5+ basal cell activity in pulmonary fibrosis. Nat. Commun. 2023, 14, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. mRNA vaccines—A new era in vaccinology. Nat. Rev. Drug Discov. 2018, 17, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Keskin, D.B.; Anandappa, A.J.; Sun, J.; Tirosh, I.; Mathewson, N.D.; Li, S.; Oliveira, G.; Giobbie-Hurder, A.; Felt, K.; Gjini, E.; et al. Neoantigen vaccine generates intratumoral T cell responses in phase Ib glioblastoma trial. Nature 2018, 565, 234–239. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



