
Submitted:
30 May 2025
Posted:
30 May 2025
You are already at the latest version
Abstract
Background: The emergence and spread of urinary carbapenem-resistant organisms (CROs) is a major public health concern, particularly in Sri Lanka. We aimed to detect and genotypically characterize CROs in urinary tract infections (UTIs) and their clinical outcomes. Methods: Urinary CROs were collected from two hospitals in Sri Lanka from January to December, 2023. Among 7640 urine samples, 100 CROs were identified by disk diffusion method, and 99 were detected by BD PheonixTM automated system. The presence of eight carbapenemase genes; blaKPC, blaNDM, blaVIM, blaIMP, blaOXA-23, blaOXA-48, blaOXA-51, and blaOXA-58, among 97 CROs was detected by a multiplex PCR kit. Results: Out of 99 urinary CROs, K. pneumoniae (33/99, 33.3%) was the most common species. A single gene was detected in 35.05 % (34/97), whereas two or more genes co-occurred in 39.18% (38/97). The highest occurrence was blaOXA-51 (47.4%), followed by blaOXA-58 (41.2%). The education level of the patients was significantly associated with the presence of carbapenemase genes (p<0.05). The majority of the patients (95.74%; n=90/97) clinically improved within seven days of treatment. However, majority (74.20%; n=69/93) experienced one or more mild UTI episodes during the next three months. Four deaths (4/10, 40%) occurred during the hospital stay, and six deaths (6/10, 60%) during the follow-up period, but none were due to UTIs. Conclusion: K. pneumoniae, showed the highest carbapenemase gene diversity. Recurrent UTIs were observed during the follow-up period. Continuous surveillance and implementation of targeted infection control programs are needed to minimize further emergence and spread of carbapenemase genes.
Keywords:
Carbapenemase genes
; carbapenem resistance
; molecular characterization
; multiplex PCR
; Sri Lanka
; urinary tract infections (UTIs)
1. Introduction
Urinary tract infections (UTIs) cause a significant impact on health care systems worldwide. The treatment and management of affected patients are further complicated by the emergence of antibiotic-resistant bacteria such as, carbapenem-resistant organisms (CROs) [1]. An alarming trend of CROs was observed globally in recent years [2]. The World Health Organization (WHO) published their first list of “antibiotic-resistant priority pathogens”, including carbapenem-resistant Enterobacteriaceae (CRE), carbapenem-resistant Acinetobacter, and carbapenem-resistant Pseudomonas as the most critical groups [3]. In 2017, 13,100 infections in hospitalized patients were due to CRE, and 1,100 deaths were reported in the United States [4]. The mortality and morbidity associated with infections caused by CROs are relatively greater than those associated with infections caused by carbapenem-sensitive pathogens [5, 6]. The majority of CREs cause UTIs [7], of which patients with urinary catheters are at a great risk of CRE infections [4].
The major mechanism of resistance to carbapenem antibiotics is known to involve the production of carbapenemase enzymes [8]. These carbapenemases hydrolyse broad-spectrum β-lactam antibiotics including carbapenems, which are considered the last resort for the treatment of infections caused by multidrug-resistant (MDR) bacteria [7, 9, 10]. These carbapenemases are divided into different classes on the basis of their amino acid sequences. Ambler class A and D include serine β-lactamases, whereas class B includes metallo-β-lactamases. These classes were further divided considering carbapenemases within each class. The Ambler class A includes Klebsiella pneumoniae carbapenemase (blaKPC), whereas the class B includes Verona Integron encoding metallo-β-lactamase (blaVIM), New Delhi metallo-β-lactamase (blaNDM) and imipenemase (blaIMP). The Ambler class D includes oxacillinases such as blaOXA-23, blaOXA-48, blaOXA-181 etc. [7, 8, 10, 11]. Variations in the minimum inhibitory concentrations (MICs) of carbapenems occur depending on the type and expression of carbapenemase enzymes present, the type of CRO present, and the presence of other resistance mechanisms [11].
Many carbapenemases encoding genes were originated in India (i.e., blaNDM-1 and blaOXA-181), and India is considered a reservoir for most of the carbapenemase genes [12, 13]. The study by Tesfa et al. reported highest prevalence rate of carbapenem resistant K. pneumoniae from India, China, Egypt, Spain and USA ranging from 15% to 22%, and the lowest prevalence rate from Japan (0.13%). In addition, highest CRO colonization rate was observed in Asia, mainly in China and India (1.4%), followed by Europe (1.2%), America (0.3%), and Africa (0.07%) indicating that the CRO distribution is not uniform even within a single country [14, 15].
Since Sri Lanka is located at the southern tip of India, there is an increased risk of dissemination of carbapenemase genes to Sri Lanka through the frequent movement of people between the two countries [16]. Although, CROs are emerging as a global threat, Sri Lankan data on CRO prevalence is scarce. However, an increasing trend of CROs has been reported ranging from 8.3% in 2017 to 35.2% in 2022 among different CRO types isolated from different specimens, posing a substantial challenge in the management of patients [17 -21]. As Sri Lanka is a third world country with a free healthcare system, this alarming carbapenem resistance rate is a crucial concern for the economy [19]. Although, data on the epidemiology and characterization of carbapenemase genes were reported a few years ago from Sri Lanka [20, 21, 22], recent data on UTIs caused by CROs, their resistance mechanisms and clinical characteristics of these patients are lacking. Therefore, the objective of the present study was to detect carbapenemase genes present among urinary isolates that were initially resistant to carbapenem antibiotics by clinical laboratory standard institute (CLSI) disk diffusion method, and to assess the clinical characteristics of respective UTI patients over a period of three months.
2. Results
2.1. Demographic Characteristics
A total of 7640 urine samples were received to microbiology laboratories of two hospitals for routine urine culture and antibiotic susceptibility testing (ABST) during the sample collection period. Among the 5270 urine samples received to university hospital, Kotelawala Defence University (UHKDU), 53 were CROs. Following the exclusion of three isolates due to mixed growths, 50 isolates from the UHKDU were included in the study. Further, a total of 2370 urine samples were received to National cancer institute (NCI) and 65 cultures were positive for CROs. Of which 50/65 were included in our study following the exclusion of 15 isolates, due to the presence of mixed growth on the ABST plate and due to receiving of more than one urine sample from the same patient. Therefore, a total of 100 CROs were included. Most of the isolates were from adult patients between the ages of 61 and 70 years (21.1%). Whilst, the mean age of the study sample was 52.6±22.5 years and, a male predominance (54.5 %) was observed.
2.2. Organism Identification and Antibiotic Susceptibility Testing
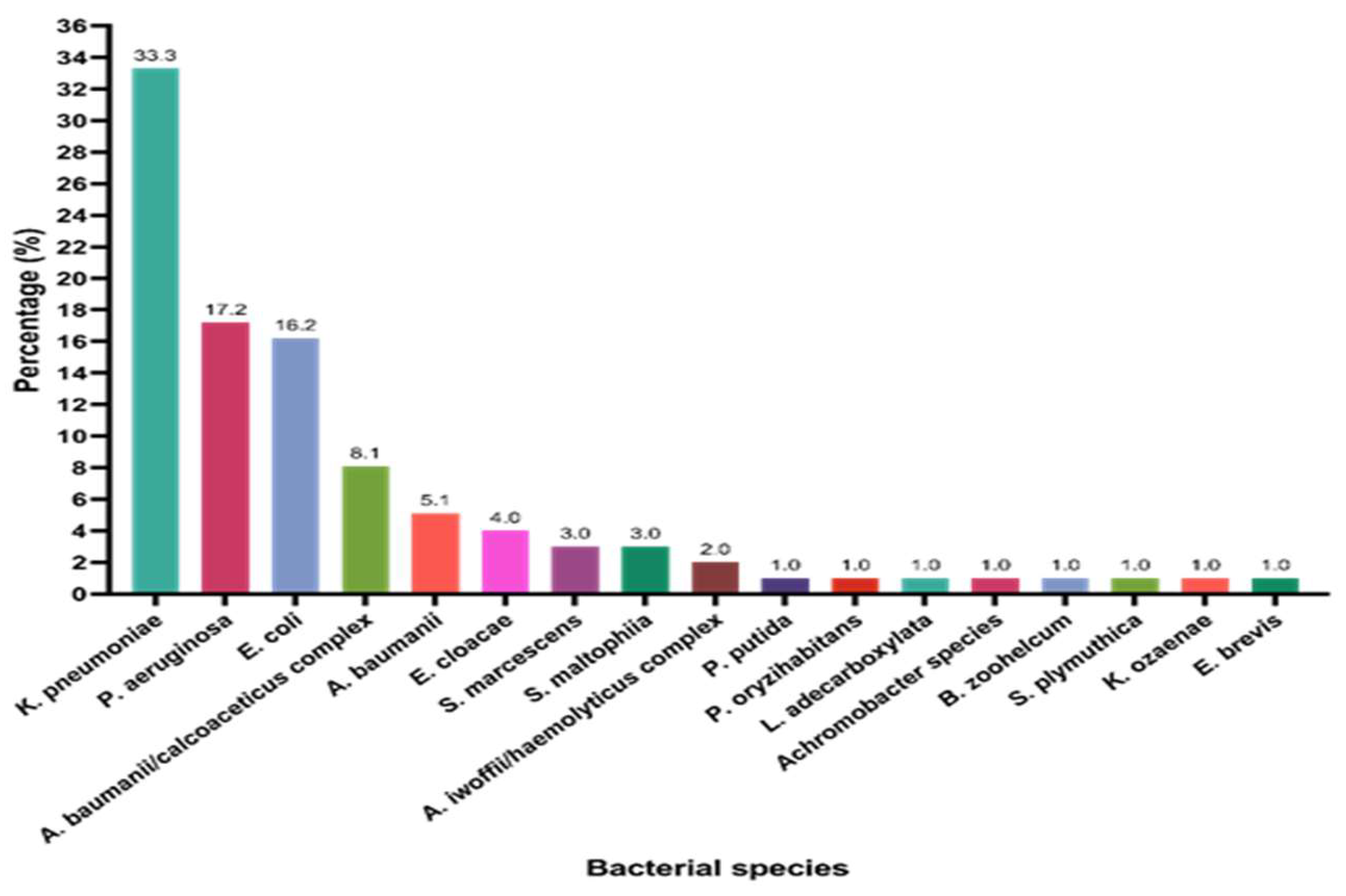
Among the 100 isolates, 99 were identified by the BD Phoenix automated system, due to the limitation of resources. The organism distribution among the study samples is shown in Figure 1. The majority were Klebsiella pneumoniae, accounting for 33.3% (n=33/99) of the study sample, followed by Pseudomonas aeruginosa (17.2%, n=17/99) and E. coli (16.2%, n=16/97). The resistance rates for imipenem and meropenem obtained by disk diffusion method were 87.6% (n=85/97) and 86.6% (n=84/97), respectively, whereas the resistance rates obtained by the automated method were equal for both the carbapenem antibiotics (88.7%, n=86/97).
2.1. Subsection
Figure 1.
Distribution of different carbapenem-resistant uropathogens isolated from patients with urinary tract infections in our study sample (n=99). The full names of the bacterial species used include; Klebsiella pneumoniae, Pseudomonas aeruginosa, Escherichia coli, Acinetobacter baumanii/calcoaceticus complex, Acinetobacter baumanii, Enterobacter cloaceae, Stenotrophomonas maltophilia, Acinetobacter iwoffii/haemolyticus, Pseudomonas putida, Pseudomonas oryzihabitans, Serratia marcescens, Leclercia adecarboxylata, Achromobacter species, Bergeyella zoohelcum, Serratia plymuthica, Empedobacter brevis, Klebsiella ozaenae.
Figure 1.
Distribution of different carbapenem-resistant uropathogens isolated from patients with urinary tract infections in our study sample (n=99). The full names of the bacterial species used include; Klebsiella pneumoniae, Pseudomonas aeruginosa, Escherichia coli, Acinetobacter baumanii/calcoaceticus complex, Acinetobacter baumanii, Enterobacter cloaceae, Stenotrophomonas maltophilia, Acinetobacter iwoffii/haemolyticus, Pseudomonas putida, Pseudomonas oryzihabitans, Serratia marcescens, Leclercia adecarboxylata, Achromobacter species, Bergeyella zoohelcum, Serratia plymuthica, Empedobacter brevis, Klebsiella ozaenae.
2.2. Distribution of Carbapenemase-Encoding Genes in the Study Sample
A total of 97 out of 99 isolates were tested for the determination of carbapenemase genes by a multiplex PCR kit, due to the limitation resources. Among these 97 isolates, 74.2% (n=72/97) were positive for the detected carbapenemase genes. A single gene was detected in 35.05% (n=34/97), whereas two or more genes co-occurred in 39.18% (n=38/97) of the isolates. When considering the overall carbapenemase gene distribution irrespective of its occurrence as combinations or as a single gene, the predominant gene was blaOXA-51 (47.4%, n= 46/97), and it was followed by blaOXA-58 (41.2%, n= 46/97), blaOXA-23 (23.7%, n= 23/97), blaVIM (17.5%, n= 17/97), blaOXA-48 (16.5%, n= 16/97), blaNDM (9.3%, n= 16/97), blaIMP (3.1%, n= 3/97), and blaKPC (1/97, n=1.0%). We detected blaVIM, blaOXA-23, blaOXA-48, blaOXA-51, and blaOXA-58 as single genes in different percentages. The distribution of different carbapenemase genes is shown in Figure 2. Among these genes, blaOXA-51 and blaOXA-58 showed the highest equal occurrence of 11.3% (n=11/97). The other carbapenemase genes; blaKPC, blaNDM, and blaVIM, were not detected as single genes. Two genes commonly co-occurred were, blaOXA-51+blaOXA-58 (7.2%, n=7/97). The predominant co-occurring gene combination among the three genes was blaOXA-51+blaOXA-58+blaVIM (5.2%, n=5/97). The maximum number of carbapenemase genes detected was four genes in the combination of blaNDM+blaIMP+blaOXA-48+blaOXA-51 (1.0%, n=1/97).
The most common genes detected in each CRO species irrespective of gene co-occurrences were blaOXA-51 (62.5%, n=5/8) in Acinetobacter baumannii; blaOXA-23 and blaOXA-51 (60.0%, n=3/5) in A. baumannii/calcoaceticus complex; blaOXA-51 and blaOXA-58 (53.33%, n=8/15) in E. coli; blaOXA-51 (35%, n=7/20) in other Gram-negative bacteria (GNB); blaOXA-48 (33.33%,n= 11/33) in K. pneumoniae; and blaVIM (25.0%, n=4/16) in P. aeruginosa. However, in A. baumannii/calcoaceticus complex, Achromobacter spp., Pseudomonas putida, Pseudomonas orizihabitans, Empedobacter brevis, Serratia plymuthica and Leclercia adecarboxylata, all the carbapenemase genes were presented as gene combinations.
When gene combinations were considered, blaOXA-51+blaOXA-23 was common in A. baumannii (60%, n=3/5) and the A. baumannii/ calcoaceticus complex (37.5%, n=3/8). In E. coli, blaOXA-51+blaOXA-58 was predominantly detected (13.3%, n=2/15). Among K. pneumoniae strains, blaVIM+blaOXA-48 was the most common gene combination (9.1%, n=3/33). The highest gene diversity was observed in K. pneumoniae, which included 11 gene combinations. Four coexisting carbapenemase genes (blaNDM+blaIMP+blaOXA-48+blaOXA-51, 3.0%) were also detected in an isolate of K. pneumoniae. It was isolated from a 73-year-old male patient admitted to the UHKDU. The Figure 3 shows the frequency distribution of carbapenemase genes among different carbapenem resistant uropathogenic species.
2.3. Demographic Characteristics Versus Carbapenemase Gene Presence
When the carbapenemase gene distribution among different age groups was considered, blaOXA-23 was common among the 41-50 years age group. The blaOXA-58 encoding genes were predominant among patients aged 51-60 years, whereas the blaOXA-51 encoding genes were predominant among patients aged 61-70 years and 71-80 years, as shown in Table 2. The predominant carbapenemase genes among males and females were blaOXA-58 and blaOXA-51, respectively. The blaKPC gene was not detected among females. A high frequency of coexisting genes was observed among males, as shown in Table 2. In terms of education level, the majority of the patients had a secondary education level (50/97, 51.54%) and were employed as skilled workers (46/97, 47.42%). The results of the univariate analysis are shown in Table 3. Only education level was significantly associated with the presence or absence of carbapenemase genes (p<0.05), and it was subjected to binary logistic regression. Among the four education levels considered, education only up to primary education significantly contributed to carbapenemase gene presence (p<0.05).
2.4. Clinical Characteristics Versus Carbapenemase Gene Presence
2.4.1. Type of Current UTI
When considering the type of UTI, the majority of the patients had uncomplicated cystitis (49/97, 50.5%), followed by complicated pyelonephritis (30/97, 30.9%). In addition, of the patients diagnosed with UTIs, the majority (72/97, 74.22%) were positive for one or more of the carabapenemase genes, without any statistically significant difference (p=0.415) with the presence of carbapenemase genes, as shown in Table 3.
2.4.2. Antibiotic Usage History
A total of 95.9% (n=95/97) of patients were treated with outpatient antibiotic medications prior to hospital admission within the last 3 months for UTIs and other infections. However, only 38.8% (n=34/95) were aware of the types of antibiotics used. Reasons for this were, poor knowledge of the patients on antibiotics and their names, and the absence of previous medical records with most of the patients. The antibiotics used to treat these patients included co-amoxiclav, ceftriaxone, ciprofloxacin, clarithromycin, nitrofurantoin, metronidazole, gentamicin, and meropenem. However, the majority of the patients were treated with co-amoxiclav (47.1%, n=16/34). Among the patients previously exposed to antibiotics, 73.7% were positive for carbapenemase genes. The only two patients who were not previously exposed to antibiotics were also positive for carbapenemase genes.
2.4.3. History of Episodes of UTIs in the Past Six Months
Overall, 19.6% (19/97) patients have not experienced UTIs during the past six months. In addition, 11.3% (11/97) had experienced one UTI, and an equal number of patients (13.4%, n=13/97) had previously experienced to two or three episodes of UTIs. A total of 42.3% (n=41/97) patients had experienced more than three previous episodes of UTIs during the past six months, and 68.3% (n=28/41) were positive for carbapenemase genes. Furthermore, out of the 19.6% (n=19/97) patients who had not experienced to previous UTI episodes, 78.9% (n=15/19) were positive for at least one carbapenemase-encoding gene tested. However, a statistically significant difference was not noted (p=0.593) between previous UTI episodes, and the presence or absence of carbapenemase genes, as shown in Table 3.

Table 3.
Univariate analysis of demographic and clinical outcome related factors with the presence or absence of carbapenemase genes among patients with urinary tract infections caused by carbapenem resistant organisms.
Table 3.
Univariate analysis of demographic and clinical outcome related factors with the presence or absence of carbapenemase genes among patients with urinary tract infections caused by carbapenem resistant organisms.
| Variables, n (%) | Total (n=97) | CRG present (n=72, %) | CRG absent (n=25, %) | p value | |||
| Demographic factors (n=97) | Age (mean ± SD, years=52.6 ± 22.5) |
0 – 10 | 7 | 6 (85.7 %) | 1 (14.3 %) | 0.634 | |
| 11 – 20 | 4 | 3 (75.0 %) | 1 (25.0 %) | ||||
| 21 – 30 | 6 | 5 (83.3 %) | 1 (16.7 %) | ||||
| 31 – 40 | 8 | 7 (97.5 %) | 1 (12.5 %) | ||||
| 41 – 50 | 11 | 6 (54.5 %) | 5 (45.5 %) | ||||
| 51 – 60 | 17 | 13 (76.5 %) | 4 (23.5 %) | ||||
| 61 - 70 | 21 | 13 (61.9 %) | 8 (38.1 %) | ||||
| 71 – 80 | 19 | 15 (78.94 %) | 4 (21.1 %) | ||||
| 81 – 90 | 3 | 3 (100 %) | 0 | ||||
| 91 - 100 | 1 | 1 (100 %) | 0 | ||||
| Gender | Male | 50 | 38 (76.0 %) | 12 (24.0 %) | 0.680 | ||
| Female | 47 | 34 (72.3 %) | 13 (27.7 %) | ||||
| Education level | Primary | 23 | 19 (82.6 %) | 4 (17.4 %) | 0.034* | ||
| Secondary | 50 | 31 (62.0 %) | 19 (38.0 %) | ||||
| Higher education | 21 | 19 (90.5 %) | 2 99.5 %) | ||||
| No schooling | 3 | 3 (100 %) | 0 | ||||
| Occupation | Unemployed | 25 | 19 (76.0 %) | 6 (24.0 %) | 0.680 | ||
| Retired | 4 | 2 (50.0 %) | 2 (50.0 %) | ||||
| Unskilled worker | 10 | 7 (70.0 %) | 3 (30.0 %) | ||||
| Skilled worker | 46 | 34 (73.9 %) | 12 (23.1 %) | ||||
| Professional or managerial | 7 | 5 (71.4 %) | 2 (28.6 %) | ||||
| Other | 5 | 5 (100 %) | 0 (0 %) | ||||
| Clinical presentation and history related factors (n=97) | Type of current urinary tract infection | Uncomplicated cystitis | 4 | 4 (100 %) | 0 (0 %) | 0.415 | |
| Complicated cystitis | 16 | 13 (81.3 %) | 3 (18.8 %) | ||||
| Uncomplicated pyelonephritis | 2 | 2 (100 %) | 0 | ||||
| Complicated pyelonephritis | 30 | 23 (76.7 %) | 7 (23.3 %) | ||||
| Other | 45 | 30 (66.7 %) | 15 (33.3 %) | ||||
| Outpatient antibiotic treatment prior to admission for the current illness | Yes | 95 | 70 (73.7 %) | 25 (26.3 %) | 0.400 | ||
| No | 2 | 2 (100 %) | 0 | ||||
| History of episodes of UTI in last 6 months | None | 19 | 15 (78.9 %) | 4 (21.1 %) | 0.593 | ||
| One | 11 | 10 (90.9 %) | 1 (9.1 %) | ||||
| Two | 13 | 10 (76.9 %) | 3 (23.1 %) | ||||
| Three | 13 | 9 (69.2 %) | 4 (30.7 %) | ||||
| More than three | 41 | 28 (68.3 %) | 13 (31.7 %) | ||||
| Clinical outcome assessment during hospital stay (n=97) | |||||||
| Clinical improvement during hospital stay | Clinical improvement at day 3 of treatment | Yes | 23 | 18 (78.3 %) | 5 (21.7 %) | 0.613 | |
| No | 74 | 54 (72.9 %) | 20 (27.0 %) | ||||
| Clinical improvement on day 5 treatment | Yes | 43 | 34 (79.1 %) | 9 (20.9 %) | 0.459 | ||
| No | 31 | 22 (70.9 %) | 11 (35.5 %) | ||||
| Clinical improvement at day 7 of treatment | Yes | 28 | 18 (64.3 %) | 10 (35.7 %) | 0.251 | ||
| No | 3 | 3 (50.0 %) | 0 | ||||
| Worsening after day 7 of treatment | Yes | 3 | 3 (100 %) | 0 | 0.402 | ||
| No | 90 | 68 (75.6 %) | 22 (24.4 %) | ||||
| Death | Death during hospital stay | Yes | Due to UTI | 0 | 0 | 0 | 0.971 |
| Due to other reasons | 4 | 3 (75.0 %) | 1 (25.0 0 %) | ||||
| No | 93 | 69 (74.2 %) | 24 (25.8 %) | ||||
| Clinical outcome assessment following hospital discharge (n=93) | |||||||
| UTI symptom recurrence following hospital discharge | UTI symptom recurrence within 30 days of infection | Yes | 33 | 25 (75.8 %) | 8 (24.2 %) | 0.761 | |
| No | 60 | 47 (78.3 %) | 13 (21.7 %) | ||||
| UTI symptom recurrence within 30-60 days of infection | Yes | 24 | 21 (87.5 %) | 3 (12.5 %) | 0.288 | ||
| No | 69 | 51 (73.9 %) | 18 (26.1 %) | ||||
| UTI symptom recurrence within 60-90 days of infection | Yes | 12 | 8 (66.7 %) | 4 (33.3 %) | 0.260 | ||
| No | 81 | 64 (79.0 %) | 17 (20.9 %) | ||||
| OPD treatment for UTI following hospital discharge | OPD treatment for UTI within 30 days of infection | Yes | 19 | 15 (78.9 %) | 4 (21.1 %) | 0.591 | |
| No | 74 | 57 (77.0 %) | 17 (22.9 %) | ||||
| OPD treatment for UTI with 30-60 days | Yes | 11 | 8 (72.2 %) | 3 (27.3 %) | 0.904 | ||
| No | 82 | 64 (78.1 %) | 18 (21.9 %) | ||||
| OPD treatment within 60-90 days for UTI infection | Yes | 6 | 3 (50.0 %) | 3 (50.0 %) | 0.161 | ||
| No | 87 | 69 (79.3 %) | 18 (20.7 %) | ||||
| Readmissions due to UTI during three months | Hospital admission due to UTIs within 30 days of infection | Yes | Ward admission | 26 | 19 (73.1 %) | 7 (26.9 %) | 0.699 |
| ICU admission | 0 | 0 | 0 | ||||
| No | 67 | 53 (79.1 %) | 14 (20.9 %) | ||||
| Hospital admission due to UTIs within 30-60 days of infection | Yes | Ward admission | 17 | 15 (88.2 %) | 2 (11.8 %) | 0.223 | |
| ICU admission | 0 | 0 | 0 | ||||
| No | 76 | 57 (75.0 %) | 19 (25.0 %) | ||||
| Hospital admission due to UTIs within 60-90 days of infection | Yes | Ward admission | 6 | 3 (50.0 %) | 3 (50.0 %) | 0.171 | |
| ICU admission | 0 | 0 | 0 | ||||
| No | 87 | 69 (79.3 %) | 18 (20.7 %) | ||||
| Outcome if readmitted due to UTI during three months | If admitted outcome within 30days | Complete recovery | 24 | 18 (75.0 %) | 6 (25.0 %) | 0.310 | |
| Complicated infection | 2 | 0 | 2 (100 %) | ||||
| No hospital admission | 67 | 53 (79.1 %) | 14 (20.9 %) | ||||
| If admitted outcome within 30 to 60 days of infection | Complete recovery | 16 | 14 (87.5 %) | 2 (12.5 %) | 0.525 | ||
| Complicated infection | 1 | 1 (100 %) | 0 | ||||
| No hospital admission | 76 | 57 (75.0 %) | 19 (25.0 %) | ||||
| If admitted outcome within 60-90 days of infection | Complete recovery | 6 | 4 (66. 7 %) | 2 (33.3 %) | 0.455 | ||
| Complicated infection | 0 | 0 | 0 | ||||
| No hospital admission | 87 | 72 (82.8 %) | 15 (17.2 %) | ||||
| Deaths occurred during three mo | Death within 30 days | Yes | Due to UTI | 0 | 0 | 0 | 0.265 |
| Due to other reasons | 4 | 2 (50.0 %) | 2 (50.0 %) | ||||
| No | 93 | 69 (74.2 %) | 24 (25.8 %) | ||||
| Death within 30-60 days | Yes | Due to UTI | 0 | 0 | 0 | 0.554 | |
| Due to other reasons | 1 | 1 (100 %) | 0 | ||||
| No | 96 | 71 (74.0 %) | 25 (26.0 %) | ||||
| Death within 60-90 nthsdays | Yes | Due to UTI | 0 | 0 | 0 | 0.554 | |
| Due to other reasons | 1 | 1 (100.0 %) | 0 | ||||
| No | 96 | 71 (74.0 %) | 25 (26.0 %) | ||||
*Statistically significant difference was noted, CRG-carbapenem resistance genes. OPD, outpatient department; ICU, intensive care unit
2.4.4. In-Hospital Clinical Improvement with the Presence Carbapenemase Genes
Among the study sample, clinical improvement was observed in 23.7% (n=23/97) patients by day three. Of these improved patients, 30.4% (n=7/23) harbored a single carbapenemase-encoding gene, while 47.8% (n=11/23) carried multiple carbapenemase-encoding genes. By day five of treatment, of 58.1% (n=43/74) patients demonstrated clinical improvement, an equal proportion (41.9%, n=18/43) harboring either single and multiple carbapenemase genes. At day seven, post-treatment with a sensitive antibiotic, 90.3% (n=28/31) of patients exhibited clinical improvement. Similar to the day five findings, an equal distribution of patients harbored single and multiple carbapenemase genes (32.1%, n=9/28). Accordingly, a progressive increase in clinical improvement was observed during the period of hospital stay. However, three patients were observed with worsening of their clinical condition following day seven of treatments, and all of them were found to carry multiple carbapenemases encoding genes. Moreover, a statistically significant difference was not noted (p>0.05) between the in-hospital clinical improvement and the presence of carbapenemase genes, as shown in Table 3.
2.4.5. Clinical Improvement Following Hospital Discharge with the Presence of Carbapenemase Genes
Overall, 71.1% (n=69/97) of the patients experienced UTI symptoms following hospital discharge, of whom 52.2% (n=36/69) were managed with outpatient department (OPD) medications. Out of which equal proportion (39.1%, n=27/69) harbored carbapenemases encoding genes. Additionally, 50.5% (n=49/97) of patients required readmission to general wards with no intensive care unit (ICU) admissions recorded. Among re-admitted patients, 30.6% (n=15/49) harbored single carbapenemases encoding genes, while 44.9% (n=22/49) harbored multiple genes. The majority (93.9%, n=46/49) were discharged following complete recovery. However, 6.1% (n=3/49) developed infectious complications, including one patient without detectable carbapenemase genes and two patients with multiple carbapenemases encoding genes. Furthermore, none of the considered clinical improvement-related factors were significantly associated with the presence of carbapenemase genes (p>0.05), as shown in Table 3.
2.4.6. Deaths Associated with the Presence of Carbapenemase Genes
Overall, 10.3 % (n=10/97) patients deceased during the study period, though mortality was attributed due to non-UTI related causes. As summarized in Table 4, the majority of the deceased patients were females (60.0%, n=6/10) and of advanced age. The most frequently observed CRO was K. pneumoniae. Notably, three of the deceased patients who deceased as shown in Table 4 did not harbor any carbapenemases encoding genes.
3. Discussion
UTIs represent a significant health concern worldwide with increasing resistance to common antibiotics, creating a substantial challenge in the management of patients [24]. Among the resistance mechanisms, production of carbapenemases by uropathogens is a threat, because of their ability to hydrolyse broad-spectrum β-lactam antibiotics, including carbapenems [25]. The global trends in CROs show alarming increase across multiple pathogens and regions. Particularly, the ATLAS surveillance program reported rising rates of CREs in Asia Pacific, Europe, Latin America, and Middle East Africa from 2018 to 2022, varying carbapenemase prevalence by region [26]. In the present study, we assessed molecular determinants of urinary CROs and their clinical characteristics. These isolates were recovered from hospitalized patients in two Sri Lankan hospitals, the UHKDU and the NCI, from January to December in 2023. Among the 7640 urine samples screened, 100 CROs were included in this study based on inclusion and exclusion criteria. Of which, 99/100 were identified to the species level via the BD Phoenix automated system. The genotypic analysis by a multiplex PCR kit was performed for 97/99 isolates and, 72/97 (74.2 %) were identified as carbapenemase producers.
In the present study, a high occurrence of CROs were observed among males, supporting previous findings [20, 27]. Although, UTIs are more common among females [1], the reason for this high CRO occurrence among males may be that older males have an increased risk of experiencing prostate-related infections such as, benign prostatic hyperplasia (BPH), which may cause urine incontinence and recurrent UTIs. In addition, due to prostate enlargement, urine catheterization is needed. When catheterized for a long period of time, biofilms are formed by antibiotic-resistant bacteria. As a result, repeated and chronic antibiotic treatments are needed, resulting in resistance. In addition, the highest occurrence of CROs was observed among elderly patients, supporting previous findings [28]. This may be due to the weakened immune system, recent hospitalizations, comorbidities, chronic diseases and frequent antibiotic usage with increasing age. In contrast, published studies reported a high rate of carbapenemase production among children aged less than one year in neonatal and pediatric wards [27].
Carbapenem resistance is particularly concerning in GNB such as; K. pneumoniae, P. aeruginosa and A. baumannii [29]. Our study detected a wide diversity of carbapenemase producers, with K. pneumoniae being the most common uropathogen (33.2%), which is in line with studies previously published in Sri Lanka [20-22] and elsewhere [27]. In contrast, different findings were also reported elsewhere [30]. K. pneumoniae was followed by P. aeruginosa, E. coli, the A. baumannii/calcoaceticus complex, A. baumannii and some other GNB, which is in line with previous findings [26, 30]. A. baumannii revealed high crabapenem resistance rates globally with an upward trend in 2020 to 2023 supporting our findings [31]. In addition, the isolation of some less frequent carbapenemase producers in our study is important, primarily due to their potential to disseminate carbapenemase genes and act as reservoirs for carbapenemases.
Genotypic analysis by PCR revealed that 74.2% (n=72/97) of the tested uropathogenic CROs were positive for carbapenemase-encoding genes. The tested eight carbapenemases encoding genes, i.e., blaNDM, blaKPC, blaIMP, blaVIM, blaOXA-51, blaOXA-23, blaOXA-48 and blaOXA-58, presented as single genes or in different combinations, indicating high carbapenem resistance variability in our study sample. In addition, the present study reported a high occurrence rate of gene combinations (39.18%) than single genes. Similar findings were reported in Egypt, with a substantial gene co-occurrence rate of 54.5%, which was higher than that of single-gene detection (45.5%), supporting our findings. The reason for this may be, as these genes are carried on mobile genetic elements and are transmissible easily within different hospital settings [32]. In addition, the diverse nature of blaNDM-1 and its capability to carry plasmids, retains the ability to harbor a high number of additional resistance genes, and these plasmids are considered as potential sources of MDR [34]. Furthermore, the observation of 25.77% (n=25/97) of carbapenem-resistant isolates detected by disk diffusion were PCR-negative for carbapenemase genes. This can be attributed to non-carbapenemase-mediated resistant mechanisms such as porin loss, over-expression of efflux pumps and alteration in penicillin-binding proteins [33]. This discrepancy underscore the importance of integrating phenotypic tests with genotypic methods to fully characterize resistance profiles.
Different carbapenemases producing genes, such as blaOXA-181 [14, 17], blaOXA-48-like [20] and blaNDM [21], have been reported previously from Sri Lanka. In addition, our study detected one E. coli isolate harboring blaKPC (1.0%) as a combination of blaKPC+blaOXA-51+blaOXA-58, and it was isolated from a 70 years old male patient, supporting the available local data [20-22]. In the present study, blaNDM did not occur as a single gene but, four combinations were noted. Higher blaNDM occurrence percentages than our study were reported locally and internationally [20, 35]. Moreover, blaNDM-1 and blaNDM-4-like variants have also been reported in Sri Lanka [14]. Although, previously only two combinations of blaNDM such as, blaNDM+blaOXA-48 and blaNDM+blaKPC+blaOXA-48, were reported in Sri Lanka, the present study reported four co-occurrences of blaNDM with blaOXA-48, blaOXA-23, blaOXA-51 and blaIMP in different combinations, supporting the findings of elsewhere [27, 36, 37]. Similar percentages to other carbapenemase genes such as, blaIMP, blaVIM, blaOXA-23, blaOXA-51 and blaOXA-58 were also reported in studies published in China [37], Thailand [38], Pakistan [39], etc. Interestingly, the blaOXA-23+blaOXA-51 combination was predominant among the A. baumanni (60%) and A. baumannii/calcoaceticus complex isolates (37.5%). To date, local studies reporting the occurrence of these blaIMP, blaVIM, blaOXA-23, blaOXA-51 and blaOXA-58 genes are scarce. This gap in data may be due to the lack of prior screening for carbapenemase-encoding genes in Sri Lankan clinical setting.
Univariate analysis revealed education level as the only factor that was significantly associated with the presence of carbapenemase genes, and of which education only up to primary grade was a significant predictor according to the binary logistic regression. Patients with low education levels are more likely to acquire UTIs caused by CROs, potentially due to less awareness of preventive measures and limited access to treatments supporting the available literature [40, 41]. None of the other clinical or demographic factors such as age, sex, occupation or type of UTI, were significantly associated with the presence of carbapenemase genes, highlighting the pivotal role of education level in predicting carbapenem resistance.
Previous episodes of UTIs and prior antibiotic treatments were not significantly associated with the presence of carbapenemase genes in our study. Although, the history of antibiotic use may contribute to the emergence of carbapenem resistance [42, 43]. However, the lack of statistically significant difference in our study could be due to diversified reasons such as, unawareness of patients about the medicines they are taking, limited sample size, and inclusion of immunocompromised patients with malignancies. In addition, the occurrence of potential carbapenem resistance in Sri Lanka was facilitated by inappropriate antibiotic prescriptions (22.6%), and redundant antibiotic therapy (17.1%) against local treatment guidelines [44]. This ultimately leads to high mortality and morbidity rates due to treatment failure, public health threats caused by outbreaks of antibiotic-resistant infections, and increased health care-associated costs [12]. In terms of clinical characteristics, neither clinical improvement during hospital stay nor clinical improvement after discharge from the hospital were significantly associated with the presence of carbapenemase genes.
Among the 97 enrolled patients, mortality was observed in 10 cases (10.3%), with four deaths occurring during hospitalization and 6 following discharge from hospitals. Of the post-discharge deaths, four occurred within 30 days, while the remaining two deaths were recorded within 30-60 days and 60-90 days post-discharge, respectively. Although, none of these fatalities were attributed due to UTIs. Demographic analysis revealed that mortality was more prevalent among female patients and older individuals. Notably, three deceased patients showed no detectable carbapenemase genes. These findings are in contrast with published literature demonstrating higher mortality rates due to infections among patients with CROs compared to those infected with carbapenem-susceptible organisms [45]. In addition, the clinical outcome may depend on the type of carbapenemase genes present. In particular, isolates encoding blaNDM-1 or blaNDM-1/ blaOXA-48 presented higher mortality rates than blaOXA-48 producers did. Notably, our findings demonstrate that the mere presence of carbapenemase genes does not independently predict mortality outcomes. The treatment of CROs associated UTIs should be decided on the basis of presence or absence of carbapenemase genes their mechanisms of resistance, and by careful clinical monitoring of patients’ response, especially when using carbapenems or colistin as therapeutic drugs. However, no statistically significant difference was documented in the mortality outcome of patients infected with CROs when treated with different antimicrobial agents, supporting our findings [46, 47, 48].
The present study reports the detection of eight carbapenemases encoding genes via a multiplex PCR kit to detect urinary CROs in Sri Lanka. This is the major strength of our study, which enabled the early identification of causative genetic mechanisms, and early initiation of appropriate antibiotic therapy, and preventive measures. Moreover, mortality associated with inappropriate, prolonged antibiotic prescriptions is limited by the use of multiplex PCR systems [49, 50]. Despite these strengths, there were several limitations as well. Although, this study included 100 patients from two hospitals, the BD Phoenix automated identification was performed for 99 isolates while, PCR testing was performed for only 97 isolates due to the limitation of resources. Further studies should be conducted including large sample sizes, in different geographical regions, with more resourced settings to detect carbapenemase genes circulating in the country. In addition, the broader epidemiology of CRO in the country may be identified by testing other clinical samples as well. In the present study, only carbapenemase production was tested, but the detection of other resistance mechanisms such as, efflux pumps, mutations in porins and penicillin-binding proteins, at least in PCR-negative isolates may contribute to the overall resistance profile.
Sri Lanka is the best-fitting and well-known country for the tourism industry and it plays a significant role in Sri Lanka’s economy. As a result of the high influx of foreign travelers from carbapenemase-encoding genes endemic countries such as India, there is an increased potential for the dissemination of these resistance genes, which poses a risk not only to local residents but, also to global health [34, 51]. Evidence-based public health policies, proper antibiotic stewardship programs, robust surveillance, and timely interventions play crucial roles in combating the threat of carbapenem resistance. Knowledge of resistance mechanisms is a cornerstone for reducing carbapenem resistance. Alternative β-lactamase inhibitor drug combinations such as, ceftazidime/avibactam, which are highly effective against blaOXA-48, and the addition of aztreonam are needed to treat blaNDM-1 [25]. In addition, the reuse of older forgotten antibiotics and, the development of new antibiotics would be beneficial in both local and global contexts.
4. Materials and Methods
A hospital-based prospective, cross-sectional study was conducted in two hospitals in the Western province of Sri Lanka; UHKDU, and NCI. The study duration was from January to December, in 2023. The urine culture samples received to respective microbiology laboratories were scrutinized on a daily basis to identify the eligible study population. Out of all the urine samples received, urinary isolates from UTI patients which showed ≥104 colony forming unite (CFU)/ml and demonstrated resistance and/ or intermediate resistance to meropenem and/ or imipenem according to CLSI disk diffusion method were included in the study. Patients who were not presenting with UTIs, isolates with mixed growths in urine cultures, and repeated isolates from same patient were excluded. Following the isolation of urinary CROs, further laboratory analysis, and clinical characteristics assessment were performed.
4.1. Screening for Carbapenem Resistance in Uropathogens by the Disk Diffusion Test
Zone diameters of meropenem and imipenem were interpreted according to 2023, CLSI guidelines [52]. Organisms that showed resistance or intermediate resistance to imipenem and/or meropenem antibiotic disks on Mueller‒Hinton agar plates were considered as possible CROs. Antimicrobial susceptibility testing was quality controlled with the Escherichia coli ATCC 25922 strain during the screening period, according to CLSI recommendations.
4.2. Organism Identification and Susceptibility Testing by the BD Phoenix Automated System
The BD PhoenixTM NMIC/ID-421 panel, which is specialized for the detection of carbapenemase-producing organisms, was used for urinary CRO identification and susceptibility testing of imipenem and meropenem in the BD Phoenix automated system. The tests were performed following the manufacturers’ instructions, and quality control was performed using the E. coli ATCC25922 strain.
4.3. Molecular Characterization of CROs
DNA extraction (HiPuraA® bacterial genomic extraction kit, catalogue no: MB505) and polymerase chain reaction (PCR) (Hi-PCR carbapenemase gene probe multiplex PCR kit, catalogue no: MBPCR132) were performed by commercially available, validated kits manufactured by Himedia laboratories in India, following the manufacturer’s instructions. A total of eight carbapenemases encoding genes were detected. The blaNDM, blaKPC, blaIMP, blaVIM, and blaOXA-48 were selected since they are the most clinically reported and wide spread carbapenemase genes across globe, particularly in South and South East Asia. Whilst, blaOXA-23, blaOXA-51, and blaOXA-58 were tested since they were commonly detected in A. baumannii, especially in South Asia which is a WHO priority pathogen, epidemiologically linked with healthcare associated outbreaks and limited evidence is available on Sri Lankan occurrence [3]. Each PCR run was quality controlled by positive and negative controls, that were available with the PCR kit.
4.4. Demographics, Clinical Factors and Clinical Outcome Assessment
A recently validated questionnaire by the same authors was used to collect demographic and clinical data from the selected group of patients, and the questionnaire was filled. Clinical outcome assessment during the hospital stay was assessed by visiting wards at three, five and seven days of intervals, subsequently urine cultures reports confirmed the presence of CROs. The parameters considered for in-ward clinical improvement assessment were; patients’ clinical response as indicated in the patients’ records, reduction in white blood cell (WBC) count, and C-reactive protein level. Data on these parameters were obtained by referring to patients’ medical records, inputs from treating medical officers and laboratory reports.
The clinical outcomes of patients following hospital discharge were collected by contacting patients/guardians over the phone. Written informed consent to participate in the study and contact over the phone were obtained from patients/guardians at the first ward visit. They were followed for up to three months, and contacted at day 30, 60 and 90 following hospital discharge. The patients/guardians were questioned regarding the recurrence of UTI symptoms such as, dysuria, increased urinary frequency, abdominal pain, fever, back pain, loin pain, nausea, vomiting, and confusion during this period. In addition, questions related to the type of medical treatment received for recurrent UTIs, such as outpatient department (OPD) treatment, ward treatment due to UTI recurrence, and mortality data during the 3 months, were also obtained.
4.5. Statistical Analysis
Data analysis was performed via SPSS software version 26. The means and standard deviations were used to summarize age. Frequencies and percentages are reported for categorical variables. Correlations between ordinal and non-normal continuous variables were analysed by the Spearman correlation coefficient, whereas Pearson’s chi-square test (or Fisher’s exact test for variables with <5 sample counts) was used to analyse the significance of categorical data. Associations of different genetic determinants with patient demographics and clinical outcomes were analysed by dividing the study sample into two groups as presence or absence of carbapenem resistance genes. Statistically significant demographic/clinical variables, with the presence or absence of carbapenem resistance genes identified by univariate logistic regression, were further subjected to binary logistic regression. A significance value (P) <0.05 was considered significant.
5. Conclusions
Carbapenem resistance is an increasing threat in Sri Lanka and globally. Understanding the local epidemiology and resistant mechanisms is important in therapeutic approaches. This study highlights the presence of diverse carbapenemases in UTI patients and their clinical characteristics in Sri Lanka. The detection of carbapenemases encoding genes as singles and co-occurrences emphasize the complex nature of treating infections caused by CRO associated UTIs. Consideration on mortality rate and determining causative factors are utmost important to improve patient care. Findings emphasize the need of continuous surveillance, infection control measures and antibiotic stewardship programs, to minimize further spread and future outbreaks of urinary CROs in clinical settings.
Author Contributions
Conceptualization, D.N., S.G. and T.S.; methodology, N.J. and U.K.; software, N.J. and U.K.; formal analysis, N.J. and T.S.; investigation, N.J. and U.K.; resources, N.J., D.N., D.D.S., S.G. and T.N; data curation, N.J.; writing—original draft preparation, N.J.; writing—review and editing, N.J., D.N., D.D.S., S.G. and T.S.; visualization, N.J. and U.K.; supervision, D.N. and T.S.; project administration, D.N., S.G. and T.S.; funding acquisition, T.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by General Sir John Kotelawala Defence University, grant number KGU/RG/2022/FAHS/005 and the study was conducted as a part of the MPhil research of N.J.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Faculty of Medicine, General Sir John Kotelawala Defence University (protocol code: RP/2022/30 and date of approval: 23.09.2022).
Informed Consent Statement
A detailed information sheet was distributed among potential participants, and the voluntary nature of the study was explained verbally. Then, the consent form was given, and written informed consent was obtained from individual participants/guardians to participate in this study as well as to contact participants three times over the phone, at 30-day intervals for three months after discharge from two hospitals. In addition, confidentiality and data protection of the participants were ensured throughout this study.
Data Availability Statement
All the data generated and analyzed during this study are included in this manuscript. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors want to acknowledge all the study participants and medical laboratory technologists at the UHKDU and NCIM for their support. In addition, the authors would like to express gratitude to General Sir John Kotelawala Defence University for funding this project.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ABST | Antibiotic susceptibility testing |
| BPH | Benign prostatic hyperplasia |
| CFU | Colony forming units |
| CRO | Carbapenem resistant organisms |
| CRE | Carbapenem resistant enterobacteriaceae |
| CLSI | Clinical laboratory standard institute |
| GNB | Gram negative bacteria |
| ICU | Intensive care unit |
| MDR | Multidrug-resistant |
| MIC | Minimum inhibitory concentration |
| NCI | National cancer institute |
| OPD | Out-patient depatment |
| PCR | Polymerase chain reaction |
| UHKDU | University hospital, Kotelawala Defence University |
| USA | United states of America |
| UTI | Urinary tract infection |
| WBC | White blood cells |
| WHO | World health organization |
| blaKPC | Klebsiella pneumoniae carbapenemase |
| blaIMP | Imipenemase |
| blaNDM | New Delhi metallo-β-lactamase |
| BlaOXA | Oxacillinase |
| blaVIM | Verona Integron encoding metallo-β-lactamase |
References
- Mancuso, G.; Midiri, A.; Gerace, E.; Marra, M.; Zummo, S.; Biondo, C. Urinary Tract Infections: The Current Scenario and Future Prospects. Pathogens. 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Elshamy, A.A.; Aboshanab, K.M. A review on bacterial resistance to carbapenems: Epidemiology, detection and treatment options. Futur Sci OA. 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. World Heal Organ. 2013, 43, 348–365. [Google Scholar]
- Centers for Diasease Control Prevention, C.D.C. Carbapenem-resistant Enterobacterals. Centers for Disease Control and prevention. 2024. 2024. Available online: https://www.cdc.gov/cre/about/index.html (accessed on 25 September 2023).
- Van, D.; Kaye, S.; Neuner, A.B. Carbapenem-resistant Enterobacteriaceae: a review of treatment and outcomes. J Neurochem. 2015, 4, 1–15. [Google Scholar]
- Nordmann, P.; Poirel, L. Epidemiology and Diagnostics of Carbapenem Resistance in gram-negative Bacteria. Clin Infect Dis. 2019, 69 (Suppl. 7), S521–S528. [Google Scholar] [CrossRef]
- Radu, V.D.; Costache, R.C.; Onofrei, P.; Miron, A.; Bandac, C.-A.; Arseni, D.; et al. Urinary Tract Infections with Carbapenem-Resistant Klebsiella pneumoniae in a Urology Clinic—A Case‒Control Study. Antibiotics. 2024, 13, 583. [Google Scholar] [CrossRef]
- Girija, S.A.; Priyadharsini, J.V.; Paramasivam, A. Prevalence of carbapenem-hydrolysing OXA-type β-lactamases among Acinetobacter baumannii in patients with severe urinary tract infection. Acta Microbiol Immunol Hung. 2020, 67, 49–55. [Google Scholar] [CrossRef]
- Rashedi, F.; Yazdanpour, Z.; Khademi, F.V.H. Prevalence of carbapenem-resistant Metallo-Beta-Lactamase-producing Escherichia coli. Med Lab J. 2023, 17, 19–22. [Google Scholar]
- Mancuso, G.; De Gaetano, S.; Midiri, A.; Zummo, S.; Biondo, C. The Challenge of Overcoming Antibiotic Resistance in Carbapenem-Resistant Gram-Negative Bacteria: “Attack on Titan”. Microorganisms. 2023, 11. [Google Scholar] [CrossRef]
- Caliskan-Aydogan, O.; Alocilja, E.C. A Review of Carbapenem Resistance in Enterobacterales and Its Detection Techniques. Microorganisms. 2023, 11, 1–26. [Google Scholar] [CrossRef]
- Castanheira, M.; Deshpande, L.M.; Mathai, D.; Bell, J.M.; Jones, R.N.; Mendes, R.E. Early dissemination of NDM-1- and OXA-181-producing Enterobacteriaceae in Indian hospitals: Report from the SENTRY Antimicrobial Surveillance Program, 2006-2007. Antimicrob Agents Chemother. 2011, 55, 1274–1278. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.M.; Corea, E.; Sanjeewani, A.H.D.; Inglis, T.J.J. Molecular mechanisms of β-lactam resistance in carbapenemase-producing Klebsiella pneumonia from Sri Lanka. J Med Microbiol. 2014, 63 Pt 8, 1087–1092. [Google Scholar] [CrossRef]
- Hammour, K.A.; Abu-Farha, R.; Itani, R.; Karout, S.; Allan, A.; Manaseer, Q.; et al. The prevalence of Carbapenem Resistance Gram negative pathogens in a Tertiary Teaching Hospital in Jordan. BMC Infect Dis. 2023, 23, 634. [Google Scholar] [CrossRef] [PubMed]
- Tesfa, T.; Mitiku, H.; Edae, M.; Assefa, N. Prevalence and incidence of carbapenem-resistant K. pneumoniae colonization: systematic review and meta-analysis. Sys Rev. 2022, 11, 1–15. [Google Scholar] [CrossRef]
- Zhu, C.; Liyanapathirana, V.; Li, C.; Pinto, V.; Hui, M.; Lo, N.; et al. Characterizing mobilized virulence factors and multidrug resistance genes in carbapenemase-producing Klebsiella pneumoniae in a Sri Lankan hospital. Front Microbiol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Tissera, K.; Liyanapathirana, V.; Dissanayake, N.; Pinto, V.; Ekanayake, A.; Tennakoon, M.; et al. Spread of resistant gram negatives in a Sri Lankan intensive care unit. BMC Infect Dis. 2017, 17. [Google Scholar] [CrossRef]
- Jayathilaka, S.H.; Jayatissa, A.H.; Chandrasiri, S.N.; Jayatilleke, K.; Kottahachchi, J. Detection of carbapenemase producing enterobacterales using the Modified Hodge Test from clinical isolates in Colombo South Teaching Hospital and Sri Jayewardenepura General Hospital, Sri Lanka in 2017. Sri Lankan J Infect Dis. 2024, 14, 1–7. [Google Scholar] [CrossRef]
- Fernando, M.M.P.S.C.; Luke, W.A.N.V.; Miththinda, J.K.N.D.; Wickramasinghe, R.D.S.S.; Sebastiampillai, B.S.; Gunathilake, M.P.M.L.; et al. Extended spectrum beta lactamase producing organisms causing urinary tract infections in Sri Lanka and their antibiotic susceptibility pattern –A hospital based cross sectional study. BMC Infect Dis. 2017, 17, 138. [Google Scholar] [CrossRef]
- Kumudunie, W.G.M.; Wijesooriya, L.I.; Namalie, K.D.; Sunil-Chandra, N.P.; Wijayasinghe, Y.S. Epidemiology of multidrug-resistant Enterobacteriaceae in Sri Lanka: First evidence of blaKPC harboring Klebsiella pneumoniae. J Infect Public Health. 2020, 13, 1330–1335. [Google Scholar] [CrossRef]
- Suranadee, Y.W.S.; Dissanayake, Y.; Dissanayake, B.M.B.T.; Jayalatharachchi, H.R.; Gamage, S.; Gunasekara, S.P. Gut colonization of carbapenem-resistant Enterobacteriaceae among patients with haematological malignancies in National Cancer Institute, Sri Lanka. JAC-Antimicrobial Resist. 2022, 4(Supplement_1). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8849380/.
- Suranadee, Y.W.S.; Jyalathacrachchi, H.R.; Gamage, S.G. Occurrence of blaKPC, blaNDM and bla OXA-48 genes among carbapenemase-producing Enterobacteriaceae (CRE) in National Cancer Institute, Sri Lanka. JAC-Antimicrobial Resist. 2022;4(Supplement-1):17–8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9040066/. [CrossRef]
- Pothoven, R. Management of urinary tract infections in the era of antimicrobial resistance. Drug Target Insights. 2023, 17, 126–137. [Google Scholar] [CrossRef] [PubMed]
- Thirapanmethee, K.; Srisiri-A-nun, T.; Houngsaitong, J.; Montakantikul, P.; Khuntayaporn, P.; Chomnawang, M.T. Prevalence of OXA-type β-lactamase genes among carbapenem-resistant Acinetobacter baumannii clinical isolates in Thailand. Antibiotics. 2020, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Radwan, E.; Al-dughmani, H.; Koura, B.; Bader, M.; Deen MAl Bueid, A.; et al. Molecular characterization of carbapenem resistant Enterobacterales in thirteen tertiary care hospitals in Saudi Arabia. Ann Saudi Med. 2021, 41, 63–70. [Google Scholar] [CrossRef]
- Wise, M.G.; Karlowsky, J.A.; Mohamed, N.; Hermsen, E.D.; Kamat, S.; Townsend, A.; et al. Global trends in carbapenem- and difficult-to-treat-resistance among World Health Organization priority bacterial pathogens: ATLAS surveillance program 2018–2022. J Glob Antimicrob Resist. 2024, 37, 168–175. [Google Scholar] [CrossRef]
- Elbadawi, H.S.; Elhag, K.M.; Mahgoub, E.; Altayb, H.N.; Ntoumi, F.; Elton, L.; et al. Detection and characterization of carbapenem resistant Gram-negative bacilli isolates recovered from hospitalized patients at Soba University Hospital, Sudan. BMC Microbiol. 2021, 21. [Google Scholar] [CrossRef]
- Chen, Y.C.; Tsai, I.T.; Lai, C.H.; Lin, K.H.; Hsu, Y.C. Risk Factors and Outcomes of Community-Acquired Carbapenem-Resistant Klebsiella pneumoniae Infection in Elderly Patients. Antibiotics. 2024, 13. [Google Scholar] [CrossRef]
- Codjoe, F.; Donkor, E. Carbapenem Resistance: A Review. Med Sci. 2017, 6, 1. [Google Scholar] [CrossRef]
- Probst, K.; Nurjadi, D.; Heeg, K.; Frede, A.; Dalpke, A.H.; Boutin, S. Molecular Detection of Carbapenemases in Enterobacterales : A Comparison of Real-Time Multiplex PCR and Whole-Genome Sequencing. Antibiotics 2021, 10, 726. [Google Scholar] [CrossRef]
- Beig, M.; Parvizi, E.; Navidifar, T.; Bostanghadiri, N.; Mofid, M.; Golab, N.; et al. Geographical mapping and temporal trends of Acinetobacter baumannii carbapenem resistance: A comprehensive meta-analysis. PLoS ONE. 2024, 19. [Google Scholar] [CrossRef]
- Abdelaziz, N.A. Phenotype-genotype correlations among carbapenem-resistant Enterobacterales recovered from four Egyptian hospitals with the report of SPM carbapenemase. Antimicrob Resist Infect Control. 2022, 11, 1–10. [Google Scholar] [CrossRef]
- Lee, Y.Q.; Sri La Sri Ponnampalavanar, S.; Chong, C.W.; Karunakaran, R.; Vellasamy, K.M.; Abdul Jabar, K.; et al. Characterization of non-carbapenemase-producing carbapenem-resistant Klebsiella pneumoniae based on their clinical and molecular profile in Malaysia. Antibiotics 2022, 11, 1670. [Google Scholar] [CrossRef] [PubMed]
- Kumarasamy, K.K.; Toleman, M.A.; Walsh, T.R.; Bagaria, J.; Butt, F.; Balakrishnan, R.; et al. Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: A molecular, biological, and epidemiological study. Lancet Infect Dis. 2010, 10, 597–602. [Google Scholar] [CrossRef]
- Ahmad, N.; Khalid, S.; Ali, S.M.; Khan, A.U. Occurrence of blaNDM variants among enterobacteriaceae from a neonatal intensive care unit in a Northern India hospital. Front Microbiol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, D.; Xu, G.; Huang, W.; Wang, X. Molecular epidemiology and drug-resistant mechanism in carbapenem-resistant Klebsiella pneumoniae isolated from paediatric patients in Shanghai, China. PLoS One. 2018, 13, 1–10. [Google Scholar]
- Li, C.; Chen, R.; Qiao, J.; Ge, H.; Fang, L.; Liu, R.; et al. Distribution and molecular characterization of carbapenemase - producing gram - negative bacteria in Henan, China. Sci Rep. 2024, 1–7. [Google Scholar] [CrossRef]
- Ali Albadery, A.; Shakir Mahdi Al-Amara, S.; Abd-Al-Ridha Al-Abdullah, A. Phenotyping and Genotyping Evaluation of E. coli Produces Carbapenemase Isolated from Cancer Patients in Al-Basrah, Iraq. Arch Razi Inst. 2023, 78, 823–829. [Google Scholar]
- Ehsan, B.; Haque, A.; Qasim, M.; Ali, A.; Sarwar, Y. High prevalence of extensively drug resistant and extended spectrum beta lactamases (ESBLs) producing uropathogenic Escherichia coli isolated from Faisalabad, Pakistan. World J Microbiol Biotechnol. 2023, 39, 1–13. [Google Scholar] [CrossRef]
- Allel, K.; García, P.; Labarca, J.; Munita, J.M.; Rendic, M.; Undurraga, E.A. Socioeconomic factors associated with antimicrobial resistance of Pseudomonas aeruginosa, Staphylococcus aureus, and Escherichia coli in Chilean hospitals (2008-2017). Rev Panam Salud Publica/Pan Am J Public Heal. 2020, 44, 1–11. [Google Scholar] [CrossRef]
- Thulasi, P.; Jamadarakhani, Siddappa; Rajani, KR.; Sujatha, M. Awareness Regarding the Disease and Its Prevention amongst Women with Recurrent Urinary Tract Infection: A Cohort Study. Kerala Surgica Journal 2024, 30, 57–62. [CrossRef]
- Otaigbe, I.I.; Elikwu, C.J. Drivers of inappropriate antibiotic use in low- and middle-income countries. JAC-Antimicrobial Resist. 2023, 5, 1–9. [Google Scholar] [CrossRef]
- Sihombing, B.; Bhatia, R.; Srivastava, R.; Aditama, T.Y.; Laxminarayan, R.; Rijal, S. Response to antimicrobial resistance in South‒East Asia Region. Lancet Reg Heal - Southeast Asia. 2023, 18, 100306. [Google Scholar] [CrossRef] [PubMed]
- Sheng, T.; Wijayaratne, G.B.; Dabrera, T.M.; Drew, R.J.; Nagahawatte, A.; Bodinayake, C.K.; et al. Point-prevalence study of antimicrobial use in public hospitals in southern Sri Lanka identifies opportunities for improving prescribing practices. Infect Control Hosp Epidemiol. 2019, 40, 224–227. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Simner, P.J. Phenotypic detection of carbapenemase-producing organisms from clinical isolates. J Clin Microbiol. 2018, 56. [Google Scholar] [CrossRef] [PubMed]
- Mathur, P.; Sagar, S.; Kumar, S.; Sharma, V.; Gupta, D.; Lalwani, S.; et al. Does the presence of Klebsiella pneumoniae carbapenemase and New Delhi metallo - β - lactamase - 1 genes in pathogens lead to fatal outcome ? Indian J Med Microbiol. 2016, 34, 495–499. [Google Scholar] [CrossRef]
- Chai, Y.; Fang, Y.; Mu, X.; Xiao, N.; Guo, J.; Wang, Z. Risk Factors for and Clinical Outcomes of Nosocomial Infections: A Retrospective Study in a Tertiary Hospital in Beijing, China. Infect Drug Resist. 2021, 14, 1393–1401. [Google Scholar] [CrossRef]
- Pudpong, K.; Pattharachayakul, S.; Santimaleeworagun, W.; Nwabor, O.F.; Laohaprertthisan, V.; Hortiwakul, T.; et al. Association Between Types of Carbapenemase and Clinical Outcomes of Infection Due to Carbapenem Resistance Enterobacterales. Infect Drug Resist. 2022, 15, 3025–3037. [Google Scholar] [CrossRef]
- Rule, R.; Paruk, F.; Becker, P.; Neuhoff, M.; Chausse, J.; Said, M. Clinical utility of the BioFire FilmArray Blood Culture Identification panel in the adjustment of empiric antimicrobial therapy in the critically ill septic patient. PLoS One. 2021, 16, 1–12. [Google Scholar] [CrossRef]
- Kakizaki, N.; Asai, K.; Kuroda, M.; Watanabe, R.; Kujiraoka, M.; Sekizuka, T.; et al. Rapid identification of bacteria using a multiplex polymerase chain reaction system for acute abdominal infections. Front Microbiol. 2023, 14, 1–9. [Google Scholar] [CrossRef]
- Doi, Y.; Paterson, D.L. Carbapenemase-producing Enterobacteriaceae. Semin Respir Crit Care Med. 2015, 36, 74–84. [Google Scholar]
- CLSI M100 for Antimicrobial Susceptibility Testing. 33rd ed. CLSI supplement M100. Vol. 40, Clinical and Laboratory Standards Institue. 2023. 32–41 p.
Figure 2.
Percentage distribution of carbapenem resistant genes as singles or combinations among the included carbapenem-resistant uropathogens (n=97).
Figure 2.
Percentage distribution of carbapenem resistant genes as singles or combinations among the included carbapenem-resistant uropathogens (n=97).
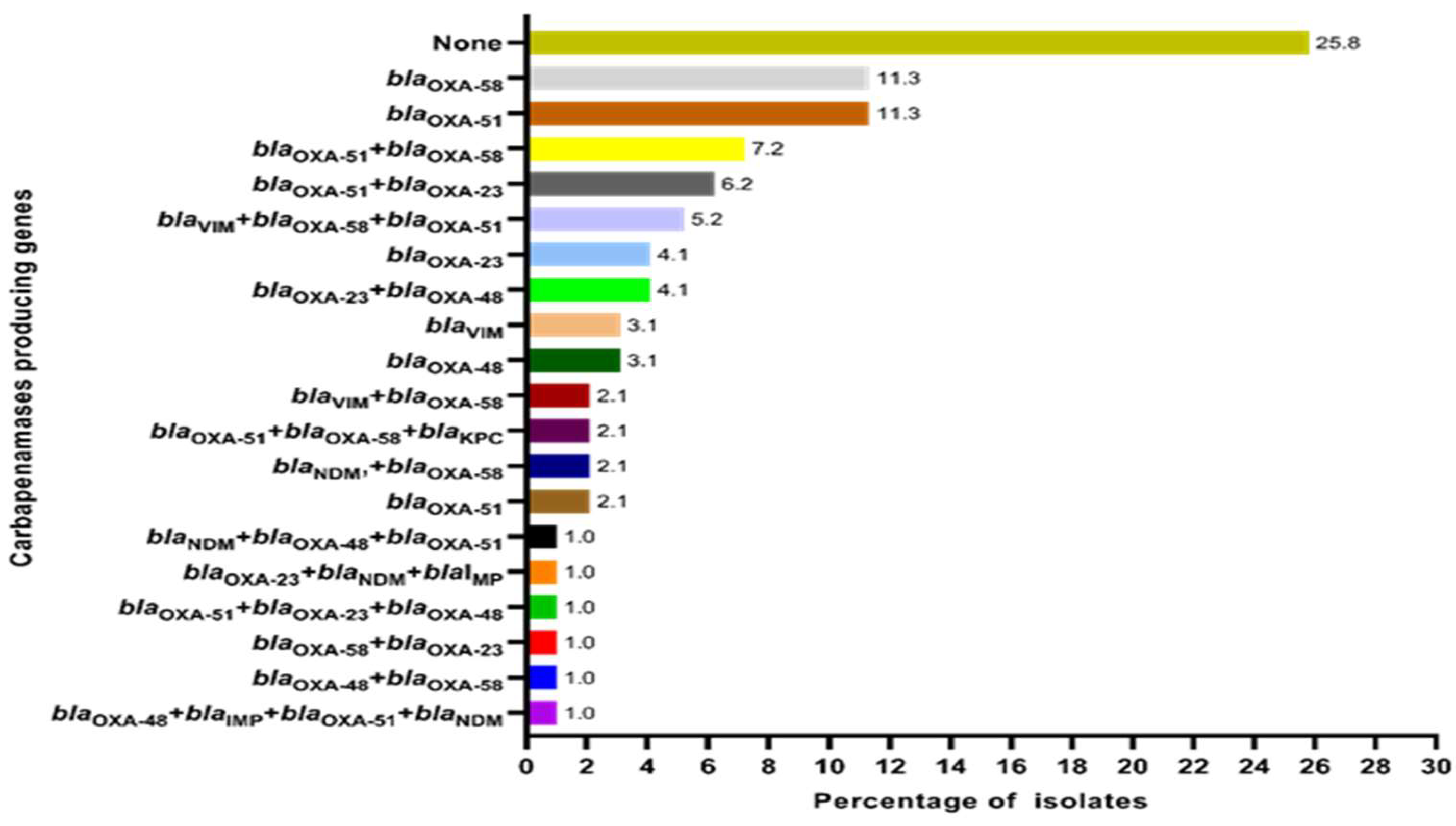
Figure 3.
Frequency distribution of carbapenemase genes among identified carbapenem-resistant uropathogenic species.
Figure 3.
Frequency distribution of carbapenemase genes among identified carbapenem-resistant uropathogenic species.
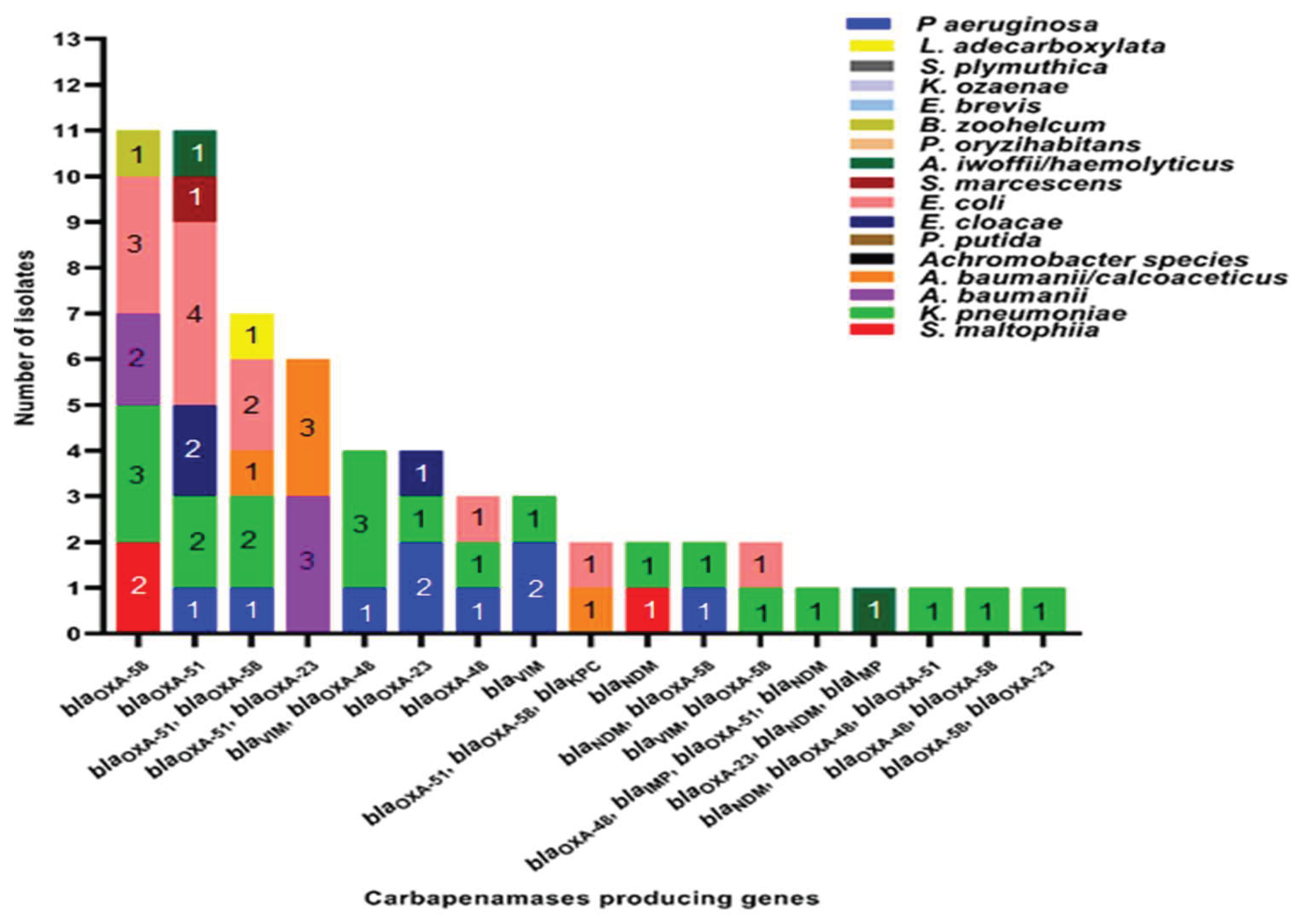
Table 2.
Distribution of carbapenemase genes among different age categories and genders within the study sample (n=97).
Table 2.
Distribution of carbapenemase genes among different age categories and genders within the study sample (n=97).
| Carbapenemases encoded by gene/s | Age categories in years | Gender | ||||||||||
| 0-10 | 11-20 | 21-30 | 31-40 | 41-50 | 51-60 | 61-70 | 71-80 | 81-90 | 91-100 | Males | Females | |
| blaNDM | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 2 |
| blaVIM | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 1 |
| blaOXA-51 | 0 | 0 | 2 | 0 | 1 | 2 | 2 | 3 | 1 | 0 | 3 | 8 |
| blaOXA-23 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 3 |
| blaOXA-48 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 0 | 0 | 0 | 1 | 2 |
| blaOXA-58 | 1 | 1 | 0 | 1 | 0 | 5 | 1 | 1 | 0 | 1 | 6 | 5 |
| blaNDM, blaOXA-58 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 |
| blaVIM, blaOXA-48 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 4 | 0 |
| blaVIM, blaOXA-58 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 |
| blaOXA-51, blaOXA-23 | 1 | 0 | 0 | 1 | 2 | 1 | 1 | 0 | 0 | 0 | 2 | 4 |
| blaOXA-51, blaOXA-58 | 1 | 1 | 1 | 0 | 0 | 0 | 2 | 2 | 0 | 0 | 4 | 3 |
| blaOXA-48, blaOXA-58 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 |
| blaOXA-48, blaOXA-23 | 0 | 0 | 0 | 0 | 2 | 1 | 0 | 1 | 0 | 0 | 2 | 2 |
| blaOXA-58, blaOXA-23 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 |
| blaOXA-51, blaOXA-23, blaOXA-48 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 |
| blaVIM, blaOXA-58, blaOXA-51 | 0 | 0 | 0 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 3 | 2 |
| blaOXA-51, blaOXA-58, blaKPC | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 0 |
| blaOXA-23, blaNDM, blaIMP | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| blaNDM, blaOXA-48, blaOXA-51 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 |
| blaOXA-48, blaOXA-51, blaIMP, blaNDM | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 |
| No carbapenemase encoding genes detected | 1 | 1 | 1 | 1 | 5 | 4 | 8 | 4 | 0 | 0 | 12 | 13 |
| Total | 7 | 4 | 6 | 8 | 11 | 17 | 21 | 19 | 3 | 1 | 50 | 47 |
Table 4.
Characteristics of death patients during the hospital stay and after discharged from the hospital.
Table 4.
Characteristics of death patients during the hospital stay and after discharged from the hospital.
| Period of death | Gender | Age (years) | Name of the CRO present | Carbapenemase genes present |
| During the hospital stay (n=4) | Female | 45 | K. pneumoniae | None |
| Male | 49 | A. baumannii | blaOXA-51+blaOXA-23 | |
| Female | 69 | K. pneumoniae | blaOXA-48 | |
| Female | 24 | K. pneumoniae | blaOXA-51 | |
| Within 30 days of discharge (n=4) |
Male | 65 | P. aeruginosa | None |
| Male | 79 | S. marcescens | blaOXA-51 | |
| Female | 80 | K. pneumoniae | None | |
| Female | 80 | K. pneumoniae | blaOXA-51 | |
| Within 30-60 days of discharge (n=1) | Male | 82 | A. baumannii/calcoaceticus complex | blaKPC+blaOXA-51+blaOXA-58 |
| Within 60-90 days of discharge (n=1) | Female | 70 | E. coli | blaOXA-51+blaOXA-58 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



