
Submitted:
25 May 2025
Posted:
26 May 2025
You are already at the latest version
Abstract
Background: Irritable Bowel Syndrome (IBS) is a prevalent functional gastrointestinal disorder with diverse subtypes. Recent evidence suggests a link between vitamin D deficiency and IBS; however, the association between vitamin D levels, IBS subtypes, and hematological-biochemical parameters remains unclear. Methods: This retrospective study included 240 patients diagnosed with IBS according to the Rome IV criteria at XXX XXX Medical Faculty Hospital. The patients were classified as diarrhea-predominant (IBS-D), constipation-predominant (IBS-C), or mixed-type (IBS-M). Serum vitamin D levels and various hematological and biochemical parameters were evaluated at baseline and after vitamin D supplementation. Sex-related differences were assessed. Results: Baseline vitamin D levels were low in all IBS subtypes, with no significant differences between the groups. Vitamin D supplementation resulted in a significant increase in serum vitamin D levels across all subtypes (p=0.001). No significant correlations were identified between vitamin D levels and hematological or biochemical parameters. Sex differences in vitamin D levels were only significant in the IBS-M group, both at baseline and post-treatment (p< 0.05). Conclusion: Vitamin D deficiency is prevalent among all IBS subtypes and significantly improves with supplementation, independent of the subtype. Although no associations were found between vitamin D levels and laboratory parameters, the observed sex differences in patients with IBS-M highlight the need for further research into potential sex-related pathophysiological mechanisms, which underscores the importance of considering vitamin D assessment and supplementation in IBS management.
Keywords:
Irritable Bowel Syndrome
; Vitamin D
; IBS subtypes
; Gender differences
; Hematological parameters
; Biochemical parameters
1. Introduction
Recent findings have expanded the known health advantages of vitamin D beyond musculoskeletal well-being, highlighting its potential connection to systemic diseases such as colorectal cancer and inflammatory bowel disease [1]. Vitamin D serves two crucial roles in the body: it facilitates the absorption of calcium and phosphate, and controls the secretion of parathyroid hormone. Research indicates that vitamin D plays a vital role in regulating over 200 genes associated with the cell cycle, including proliferation, differentiation, and apoptosis (2). It is well established that the vitamin D receptor is expressed in a majority of tissues, including the gastrointestinal tract, nervous system, and immune cells [2]. Vitamin D receptors are found in the neurological system and the gastrointestinal tract, and their activation is linked to neurotransmitter levels, serotonin production, the permeability of the gastrointestinal epithelium, and gastrointestinal inflammation [3,4,5]. Vitamin D is believed to affect irritable bowel syndrome (IBS) by playing a part in inflammatory processes, regulating the immune system, and modulating gut microbiota. It might enhance the mucosal barrier and serve as an antimicrobial agent, which could help alleviate IBS symptoms [6,7,8].
IBS is a functional disorder of the gastrointestinal system characterized by recurring abdominal discomfort and changes in digestive habits [9]. The pathogenesis of IBS is multifaceted, involving the dysregulation of interactions between the brain and gut, along with various risk factors. This condition is a chronic disorder affecting the gastrointestinal tract, characterized by a cycle of symptoms that recur and remit and can be potentially disabling [10]. The Rome IV Diagnostic Criteria for functional bowel disorders currently serves as the "Gold Standard" for the diagnosis of IBS [11]. Although IBS is reported to affect 10%-22% of the adult population [12], epidemiological studies have demonstrated that its prevalence varies across different regions, countries, and even within the same country. This variability may be attributed to differences in the survey populations and methodologies. The prolonged nature of IBS demands significant medical resources, greatly impacting the quality of life of both patients and their families, and imposing a substantial societal burden [13,14]. Considering the significant burden of IBS [15], it is essential to deepen our understanding of its pathological mechanisms to develop effective treatment strategies. Vitamin D deficiency affects approximately 30%–50% of the global population and is similarly prevalent among individuals with gastrointestinal disorders [16]. Recent research has indicated that individuals with IBS have notably lower serum vitamin D levels than healthy individuals. Although vitamin D deficiency is prevalent among patients with IBS, the association between vitamin D levels and the severity of gastrointestinal symptoms in these patients remains unclear.
In this study we aimed to investigate the relationship between vitamin D and IBS, also we aimed to investigate the relationship between IBS subtypes and biochemical parameters such as ferritin levels, iron levels, calcium levels, magnesium levels, and vitamin B12 levels, and hematological parameters such as hemoglobin, white blood cell counts, platelet counts, and main corpuscular volume (MCV) of the patients.
2. Materials and Methods
Patients with IBS who were followed up and treated at the Van Yüzüncü Yıl University Faculty of Medicine Hospital between January 2020 and December 2024 were retrospectively screened for this study. The inclusion criteria were as follows: age between 18 and 85 years, not using medications that affect the metabolism of vitamin D such as seizure drugs or anti-tuberculosis drugs, not pregnant or lactating, and free of active infections. The exclusion criteria were as follows: age below 18 years, use of medications that affect vitamin D metabolism, pregnancy and/or breastfeeding, and active infections. The Rome IV diagnostic criteria were used to diagnose patients with IBS; these included recurrent abdominal pain on average at least 1day/week in the last 3 months, associated with two or more of the following criteria: 1-related to defecation, 2) associated with a change in the frequency of stool, and 3) associated with a change in the form (appearance) of stool. These criteria should be fulfilled in the last 3 months, with symptom onset at least 6 months before diagnosis. IBS patients were categorized into three subtypes: 1- constipation-predominant (IBS-C), 2- diarrhea-predominant (IBS-D) and 3- mixed-type (IBS-M) [11].
2.1. Ethical Approval
Ethical approval was obtained from the Ethics Committee of the Van Yüzüncü Yıl University Medical Faculty (decision date: 04.02.2025).; No. 2025/01-35). This study was conducted in accordance with the guidelines of the Declaration of Helsinki (revised in 2013). The requirement for informed consent was waived owing to the retrospective design of the study.
2.2. Statistical Analysis
Statistical analyses were performed using Analyze-it for Microsoft Excel (Analyze-it Software, Ltd., Leeds, UK). Quantitative variables are presented as mean standard deviation or median and percentiles (25-75%) depending on whether they showed a normal distribution. Data were tested for normality using the Shapiro-Wilk test. Chi-square suare test was used to examine the relationships between categorical data. Group comparisons were performed using a one-way ANOVA test for continuous data with a normal distribution. Group comparisons were performed using the Kruskal-Wallis test for continuous data without a normal distribution. A paired t-test was used to compare the differences between repeated measurements. Statistical significance was set than 0.05.
3. Results
A total of 750 IBS patients were screened retrospectively from their medical records. After applying the exclusion criteria, 240 patients were included in the study. The participant inclusion process is illustrated in Figure 1.
The median age was 44 (35-57) years in the IBS-D group, 46 (37-60) years in the IBS-C group, and 44 (30-61) years in the IBS-M group. Of all the patients, 47.5 % were female. According to the Rome IV criteria, of 240 patients with IBS, 22% had IBS-D, 45% had IBS-C, and 33% had IBS-M. The other demographic and biochemical characteristics are summarized in Table 1. In the comparison according to IBS subtypes, no significant difference was found between the groups in terms of sex distribution. Similarly, no statistically significant differences were observed between the groups in terms of hematological and biochemical parameters, such as age, hemoglobin level, white blood cell count, MCV, platelet count, and vitamin B12 level. When calcium, magnesium, iron, and ferritin levels were examined, no significant differences were found between the IBS subtypes. When vitamin D levels were evaluated both at the time of application and two months later, it was determined that these parameters did not show a significant difference between the groups. The findings showed no significant difference in basic biochemical parameters between the subtypes of IBS (Table 1).
The impact of treatment on serum vitamin D levels was assessed using both individual and summary visualizations. As shown in Figure 2A, most patient trajectories showed an upward trend, suggesting an overall increase in vitamin D levels after the intervention. This trend was reinforced by the box-and-whisker plot in Figure 2B, which displays a clear upward shift in the distribution of vitamin D concentrations. Specifically, the median serum vitamin D level increased from 12.0 ng/mL (25-75 % percentile: 8.42 to 20.0) before treatment to 32.0 ng/mL (25-75 % percentile: 20.0 to 39.0) after treatment. This change was statistically significant (p = 0.001), supporting a meaningful improvement in the vitamin D status among the study participants.
Together, these findings illustrate a consistent and significant elevation in vitamin D levels after treatment in IBS patients. When stratified by IBS subtype, all patient groups exhibited a significant increase in serum vitamin D levels after treatment. Among patients with IBS-D, the median vitamin D level rose from 12.0 ng/mL (interquartile range: 10–20) to 33.0 ng/mL (25–36), with a statistically significant difference (p = 0.001). Similarly, patients with IBS-C showed an increase from 13.0 ng/mL (9–22 ng/mL) before treatment to 32.0 ng/mL (20–40 ng/mL) after treatment (p = 0.001). In the IBS-M group, vitamin D levels improved from a median of 11.0 ng/mL (8–18) to 28.0 ng/mL (18–40), also reaching statistical significance (p = 0.001) (Table 2).
A correlation analysis was performed to explore the potential associations between baseline serum vitamin D levels and various hematological and biochemical parameters. As shown in Figure 3, no statistically significant correlation was observed between vitamin D levels and age, hemoglobin, white blood cell count, platelet count, MCV, or common micronutrients, such as calcium, magnesium, iron, or ferritin (all p>0.05). Correlation coefficients were generally weak and did not indicate any meaningful linear associations.
When stratified by both sex and IBS subtype, there was no statistically significant difference in serum vitamin D levels between female and male patients in the IBS-D and IBS-C groups either before or after treatment. However, in the IBS-M group, vitamin D levels differed significantly between sexes at both time points (Table 3).
4. Discussion
In this study, we evaluated the relationship between IBS subtypes and vitamin D level. Our findings showed no significant difference in vitamin D levels between the different IBS phenotypes at baseline or after treatment. However, vitamin D replacement therapy resulted in a statistically significant increase in serum levels in all IBS groups. Additionally, vitamin D levels were not significantly correlated with haematological and biochemical parameters such as age, hemoglobin, white blood cells, platelets, MCV, vitamin B12, calcium, magnesium, iron, and ferritin.
The impact of vitamin D deficiency on gastrointestinal function has been a subject of much debate. It has been suggested that vitamin D may play a role in the pathophysiology of IBS by regulating the immune system, controlling inflammation, and modulating gut microbiota [17]. Ali et al studied the correlation between vitamin D deficiency and IBS in 90 patients (45 healthy individuals vs 45 IBS patients). They found that vitamin D deficiency was higher in the IBS group (76.6% vs. 46.7%) (6). Similarly, in a study conducted by Husseiny et al., 56.06% of patients with IBS had vitamin D deficiency, while 39.65% had insufficient vitamin D levels [18]. A comparative case-control study revealed a notable correlation between vitamin D deficiency and IBS, showing that 82% of IBS patients have vitamin D deficiency compared with only 32% of healthy individuals [19]. In our study, vitamin D levels were found to be low at baseline in all IBS subtypes (diarrhea-predominant, constipation-predominant, and mixed-type), and increased significantly following replacement therapy. This increase was statistically significant in all the subgroups (p=0.001). The observation of similar improvement in all IBS subtypes following vitamin D replacement therapy suggests that this effect is realized via a general mechanism that is independent of the IBS subtype. Although numerous studies have reported positive correlations, some have not identified a notable difference in vitamin D levels between individuals with IBS and healthy individuals. For example, a study conducted by Matthews et al. reported no significant association between plasma vitamin D concentration and IBS symptoms in women. This study showed that in the IBS group, 40.3% were vitamin D-deficient and 33.9% were insufficient. The rates were similar in the healthy control group, with 41.4% deficient and 34.3% insufficient. This indicates no significant difference in vitamin D deficiency or insufficiency between the two groups [20]. Although there is much evidence suggesting a link between vitamin D deficiency and IBS, the exact nature of this relationship is not fully understood.
Typically, women have lower levels of vitamin D than men, which is attributed to a mix of biological, lifestyle, and environmental influences. Variations in body composition, hormonal differences, and cultural customs that influence sun exposure and eating patterns contribute to these distinctions [21,22]. A potential reason for the variation in outcomes across different experiments could be cultural differences in the lifestyles of men and women globally. A study of individuals aged 5–101 years who lived in urban areas of China found that women had lower levels of vitamin D. Based on these findings, the individuals with the highest risk of low levels, including significant deficiencies in plasma vitamin D, were females younger than 20 years and those older than 80 years [23]. Comparable results were found by researchers studying Brazilian children and adolescents aged between 12 and 17 years. Furthermore, 25(OH)D deficiency (defined as ≤20 ng/ml) was much more prevalent among girls and obese men [24]. Zhu et al. found that the rates of both body mass index and visceral obesity were significantly related to low serum 25 (OH) D concentrations in men [25]. The molecular mechanisms underlying the differences in serum 25 (OH) D concentrations between men and women remain unclear. Recent observations have shown that the use of estrogen-containing contraceptives leads to an increase in 25(OH)D levels [26]. Moreover, women exhibit a higher concentration of vitamin D-binding protein (DBP), which is associated with the estrogen-dependent production of DBP [27]. Certainly, sex hormones play a crucial role in influencing the gene expression levels related to vitamin D. However, this may not be the sole factor, as the findings from various studies show inconsistencies, suggesting that both males and females exhibit lower average levels of vitamin D, depending on the particular research. Therefore, alternative mechanisms may account for these differences. In our study, we observed that women generally had lower vitamin D levels both before and after treatment than men, although this difference was statistically significant only in the IBS-M group. The fact that this difference was only observed in IBS-M suggests that different subtypes may be associated with different pathophysiological mechanisms. There are few studies on this subject in the literature, so studies with larger samples addressing the interaction between sex and subtype are needed. However, vitamin D levels increased in both men and women with all IBS subtypes after the replacement therapy. This suggests that vitamin D deficiency is widespread among IBS patients, and that supplementation can effectively address this deficiency.
Various subtypes of IBS are reported to be the most common worldwide. The most common subtype was IBS-D, with a rate of 73.4% in the study by Elhosseiny et al. [28]. Similarly, Dorn et al. found that the most common IBS subtype was IBS-D (46%), followed by IBS-C (32%) and IBS-M (32%) [29]. Of the patients included in our study, 45% had IBS-C, which is the most common subtype of IBS. The reason for this difference may be the female predominance in the patients included in our study, because women are generally more affected by IBS, particularly IBS-C, while men are more likely to have IBS-D and IBS-M [30]. Our findings demonstrate that females had a higher propensity to experience IBS symptoms than males, specifically for constipation. However, this difference was not statistically significant. The lack of a statistically significant difference may be due to bias resulting from the retrospective design of the study. The higher prevalence of constipation-dominant IBS in women may be due to variations in intestinal motor and sensory functions, hormones, and microbiota between the sexes, associated with gut-brain interactions [31,32]. It is widely accepted that estrogen and progesterone play a role in reducing smooth muscle contractions, thereby affecting peristalsis and potentially leading to constipation [31]. Moreover, the influence of sex hormones on bacterial growth, expression, and metabolism can account for the observed differences between sexes [31].
Our study revealed no statistically significant differences in sex distribution; hematological parameters such as hemoglobin levels; white blood cell counts; mean corpuscular volume; platelet count; or biochemical markers such as levels of essential micronutrients including calcium, magnesium, iron, and ferritin among IBS subtypes. Ergenç et al. found significant relationships between vitamin D levels and several hematological parameters, including platelet count, monocyte count, MCV, neutrophil count, and calcium and vitamin B12 levels. Platelet and monocyte counts were significantly higher in the group with low vitamin D levels (<20ng/ml). However, the neutrophil count, MCV, calcium, and B12 levels were significantly lower in this group [33]. Mobarki et al investigated the prevalence of vitamin D deficiency among young adults and its correlation with various hematological and biochemical parameters. This study found no significant differences in hematological parameters (white blood cells, platelets, and red blood cells) among participants based on their vitamin D status [34].
In summary, this study revealed that vitamin D deficiency is common among patients with IBS, vitamin D replacement therapy is effective for all IBS subtypes, and that significant differences exist according to sex, particularly among patients with IBS-M. These findings are noteworthy for both clinical practice and future research.
Our study have some limitations. The retrospective design, selected patient population, and fact that the data were from a single center limits the generalizability of the study. In addition, failure to evaluate biomarkers potentially associated with vitamin D, such as inflammatory markers and microbiota analysis, is another limitation of our study. Finally, the symptom scores and quality of life measures were not assessed after vitamin D replacement. Therefore, the clinical implications of these biochemical improvements should be evaluated in future, prospective studies.
5. Conclusions
In conclusion, this study revealed that vitamin D replacement therapy significantly increased vitamin D levels in patients with IBS, but the relationship between vitamin D levels and haematological and biochemical parameters was weak. Such insights warrant further research to explore the underlying mechanisms by which vitamin D may influence IBS pathophysiology and evaluate the clinical implications of vitamin D supplementation in this patient population. Additionally, recognizing the potential variance in treatment responses across subgroups emphasizes the need for personalized approaches to IBS management. The identification of gender differences within the IBS-M group may introduce a new topic for discussion in the literature, warranting consideration for future research.
Author Contributions
Conceptualisation, N.D.O. and Y.Y.U.; methodology, H.H.A. and N.D.O; software, H.H.A.; validation, N.D.O., Y.Y.U. and H.H.A.; formal analysis, H.H.A. and N.D.O.; investigation, N.D.O. and Y.Y.U.; resources, N.D.O..; data curation, N.D.O. and Y.Y.U.; writing—original draft preparation, N.D.O and Y.Y.U.; writing—review and editing, N.D.O., H.H.A and Y.Y.U.; visualisation, N.D.O. and Y.Y.U.; supervision, Y.Y.U and H.H.A.; project administration, N.D.O., H.H.A. and Y.Y.U. All authors have read and agreed to the published version of the manuscript.
Funding
This reasearch received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Van Yüzüncü Yıl University Medical Faculty (decision date: 04.02.2025).; No. 2025/01-35).
Informed Consent Statement
Informed consent was waived owing to the retrospective design of the study.
Data Availability Statement
The original contributions presented in this study are included in the article; further inquiries can be directed to the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kulie, T.; Groff, A.; Redmer, J.; Hounshell, J.; Schrager, S. Vitamin D: An Evidence-Based Review. Journal of the American Board of Family Medicine 2009, 22, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Holick, M. F. Vitamin D Deficiency. The New England Journal of Medicine 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Patrick, R. P.; Ames, B. N. Vitamin D Hormone Regulates Serotonin Synthesis. Part 1: Relevance for Autism. The FASEB Journal 2014, 28, 2398–2413. [CrossRef]
- Kong, J.; Zhang, Z.; Musch, M. W.; Ning, G.; Sun, J.; Hart, J.; Bissonnette, M.; Li, Y. C. Novel Role of the Vitamin D Receptor in Maintaining the Integrity of the Intestinal Mucosal Barrier. American Journal of Physiology-gastrointestinal and Liver Physiology. [CrossRef]
- Li, Y. C.; Chen, Y.; Du, J. Critical Roles of Intestinal Epithelial Vitamin D Receptor Signaling in Controlling Gut Mucosal Inflammation. The Journal of Steroid Biochemistry and Molecular Biology 2015, 148, 179–183. [Google Scholar] [CrossRef]
- Ali, S.; Kamal Mohamed, I.; Zaki, Z. E.; Elsayed, A. S. Clinical Correlation between Serum Vitamin D Level and Irritable Bowel Syndrome. El-Minia Medical Bulletin, 2022; 33, 228–232. [Google Scholar] [CrossRef]
- Al-Shemery, M. K.; Al Kafhage, F. A.; Al-Masaoodi, R. A. Vitamin D3 And Irritable Bowel Syndrome: Review. The International Science of Health Journal 2024, 2, 117–127. [Google Scholar] [CrossRef]
- Yamamoto, E. A.; Jørgensen, T. N. Relationships Between Vitamin D, Gut Microbiome, and Systemic Autoimmunity. Frontiers in Immunology 2020, 10, 3141. [Google Scholar] [CrossRef]
- Lee, Y. J.; Park, K. S. Irritable Bowel Syndrome: Emerging Paradigm in Pathophysiology. World Journal of Gastroenterology 2014, 20, 2456–2469. [Google Scholar] [CrossRef]
- Mearin, F.; Lacy, B.; Chang, L.; Chey, W.; Lembo, A.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407. [Google Scholar] [CrossRef]
- Drossman, D. A.; Hasler, W. L. Rome IV—Functional GI Disorders: Disorders of Gut-Brain Interaction. Gastroenterology 2016, 150, 1257–1261. [Google Scholar] [CrossRef]
- Jang, A.; Hwang, S. K.; Padhye, N. S.; Meininger, J. C. Effects of Cognitive Behavior Therapy on Heart Rate Variability in Young Females with Constipation-Predominant Irritable Bowel Syndrome: A Parallel-Group Trial. Journal of Neurogastroenterology and Motility 2017, 23, 435–445. [Google Scholar] [CrossRef]
- Defrees, D. N.; Bailey, J. Irritable Bowel Syndrome: Epidemiology, Pathophysiology, Diagnosis, and Treatment. Primary Care 2017, 44, 655–671. [Google Scholar] [CrossRef]
- Black, C. J.; Ford, A. C. Global Burden of Irritable Bowel Syndrome: Trends, Predictions and Risk Factors. Nature Reviews Gastroenterology & Hepatology 2020, 17, 473–486. [Google Scholar] [CrossRef]
- Shorey, S.; Demutska, A.; Chan, V.; Siah, K. T. H. Adults Living with Irritable Bowel Syndrome (IBS): A Qualitative Systematic Review. Journal of Psychosomatic Research 2021, 140, 110289. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A. Nutritional Rickets around the World. The Journal of Steroid Biochemistry and Molecular Biology 2013, 136, 201–206. [Google Scholar] [CrossRef]
- Yu XL, Wu QQ, He LP, Zheng YF. Role of in Vitamin D in Irritable Bowel Syndrome. World Journal of Clinical Cases 2023, 11, 2677–2683. [Google Scholar] [CrossRef]
- Husseiny, A.; zamili, S.; Shala, H. Prevalence of IBS and Its Relationship to Vitamin D Deficiency in Al- Nasiriyah City, Iraq. Rawal Medical Journal 2023, 48, 630–634. [Google Scholar] [CrossRef]
- Khayyat, Y. M.; Attar, S. M. Vitamin D Deficiency in Patients with Irritable Bowel Syndrome: Does It Exist? Oman Medical Journal 2015, 30, 115–118. [Google Scholar] [CrossRef]
- Matthews, S. W.; Plantinga, A.; Burr, R. L.; Cain, K. C.; Savidge, T. C.; Kamp, K.; Heitkemper, M. M. Exploring the Role of Vitamin D and the Gut Microbiome: A Cross-Sectional Study of Individuals with Irritable Bowel Syndrome and Healthy Controls. Biological Research For Nursing 2023, 25, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicka, A. Sex Differences in Vitamin D Metabolism, Serum Levels and Action. British Journal of Nutrition 2022, 128, 2115–2130. [Google Scholar] [CrossRef]
- Al-Haddad, F.; Al-Mahroos, F.; Al-Sahlawi, H. S.; Al-Amer, E. A. The Impact of Dietary Intake and Sun Exposure on Vitamin D Deficiency among Couples. Bahrain medical bulletin 2014, 36, 33–37. [Google Scholar] [CrossRef]
- Ning, Z.; Song, S.; Miao, L.; Zhang, P.; Wang, X.; Liu, J.; Hu, Y.; Xu, Y.; Zhao, T.; Liang, Y.; Wang, Q.; Liu, L.; Zhang, J.; Hu, L.; Huo, M.; Zhou, Q. High Prevalence of Vitamin D Deficiency in Urban Health Checkup Population. Clinical Nutrition 2016, 35, 859–863. [Google Scholar] [CrossRef]
- Lacroix de Oliveira, C.; Vogt Cureau, F.; dos Santos Cople-Rodrigues, C.; Tavares Giannini, D.; Vergetti Bloch, K.; Caetano Kuschnir, M. C.; Baiocchi de Carvalho, K. M.; D’Agord Schaan, B. Prevalence and Factors Associated with Hypovitaminosis D in Adolescents from a Sunny Country: Findings from the ERICA Survey. The Journal of Steroid Biochemistry and Molecular Biology 2020, 199, 105609. [Google Scholar] [CrossRef]
- Zhu, X.; Chen, Z.; Li, Y.; Yang, P.; Liu, L.; Wu, L.; Wang, Y. Associations of Vitamin D with Novel and Traditional Anthropometric Indices According to Age and Sex: A Cross-Sectional Study in Central Southern China. Eating and Weight Disorders-studies on Anorexia Bulimia and Obesity 2020, 25, 1651–1661. [Google Scholar] [CrossRef] [PubMed]
- Harmon, Q. E.; Umbach, D. M.; Baird, D. D. Use of Estrogen-Containing Contraception Is Associated With Increased Concentrations of 25-Hydroxy Vitamin D. The Journal of Clinical Endocrinology and Metabolism 2016, 101, 3370–3377. [Google Scholar] [CrossRef]
- Lagunova, Z.; Porojnicu, A.; Lindberg, F. A.; Hexeberg, S.; Moan, J. E. The Dependency of Vitamin D Status on Body Mass Index, Gender, Age and Season. Anticancer Research 2009, 29, 3713–3720. [Google Scholar] [CrossRef]
- Elhosseiny, D.; Elfawy Mahmoud, N.; Manzour, A. F. Factors Associated with Irritable Bowel Syndrome among Medical Students at Ain Shams University. Journal of the Egyptian Public Health Association 2019, 94, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Dorn, S. D.; Morris, C. B.; Hu, Y.; Toner, B. B.; Diamant, N. E.; Whitehead, W. E.; Bangdiwala, S. I.; Drossman, D. A. Irritable Bowel Syndrome Subtypes Defined by Rome II and Rome III Criteria Are Similar. Journal of Clinical Gastroenterology 2009, 43, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Aslam, A. Irritable Bowel Syndrome in Western and Non-Western Populations: Prevalence, Psychological Comorbidities, Quality of Life and Role of Nutrition. Global Immunological & Infectious Diseases Review 2024, IX, 64–76. [Google Scholar] [CrossRef]
- Kim, Y. S.; Kim, N. Sex-Gender Differences in Irritable Bowel Syndrome. Journal of Neurogastroenterology and Motility 2018, 24, 544–558. [Google Scholar] [CrossRef]
- Chang, L.; Heitkemper, M. M. Gender Differences in Irritable Bowel Syndrome. Gastroenterology 2002, 123, 1686–1701. [Google Scholar] [CrossRef]
- Ergenc, Z.; Ergenç, H.; Yıldırım, İ.; Öztürk, A.; Usanmaz, M.; Karacaer, C.; Günay, S.; Kaya, G. Relationship between Vitamin D Levels and Hematological Parameters. Medical Science and Discovery 2023, 10, 1–7. [Google Scholar] [CrossRef]
- Mobarki, A. A.; Dobie, G.; Saboor, M.; Madkhali, A. M.; Habibullah, M.; Nahari, M. H.; Kamli, H.; Hakamy, A.; Hamali, H. A. Prevalence and Correlation of Vitamin D Levels with Hematological and Biochemical Parameters in Young Adults. Annals of Clinical and Laboratory Science 2022, 52, 815–824. [Google Scholar] [PubMed]
Figure 1.
Flow chart of the included patients.
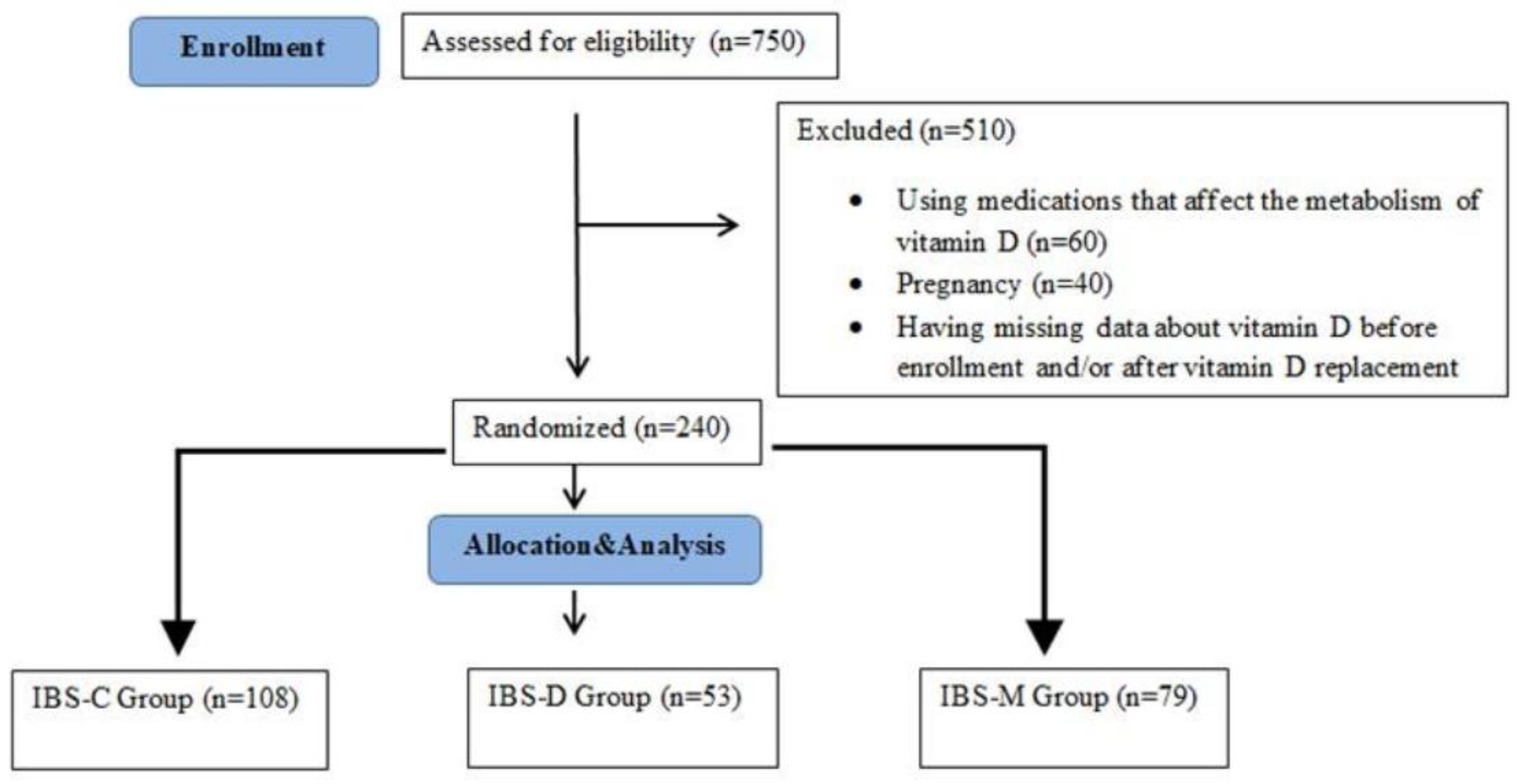
Figure 2.
Distribution of vitamin D levels in patients before and after vitamin D replacement therapy.
Figure 2.
Distribution of vitamin D levels in patients before and after vitamin D replacement therapy.
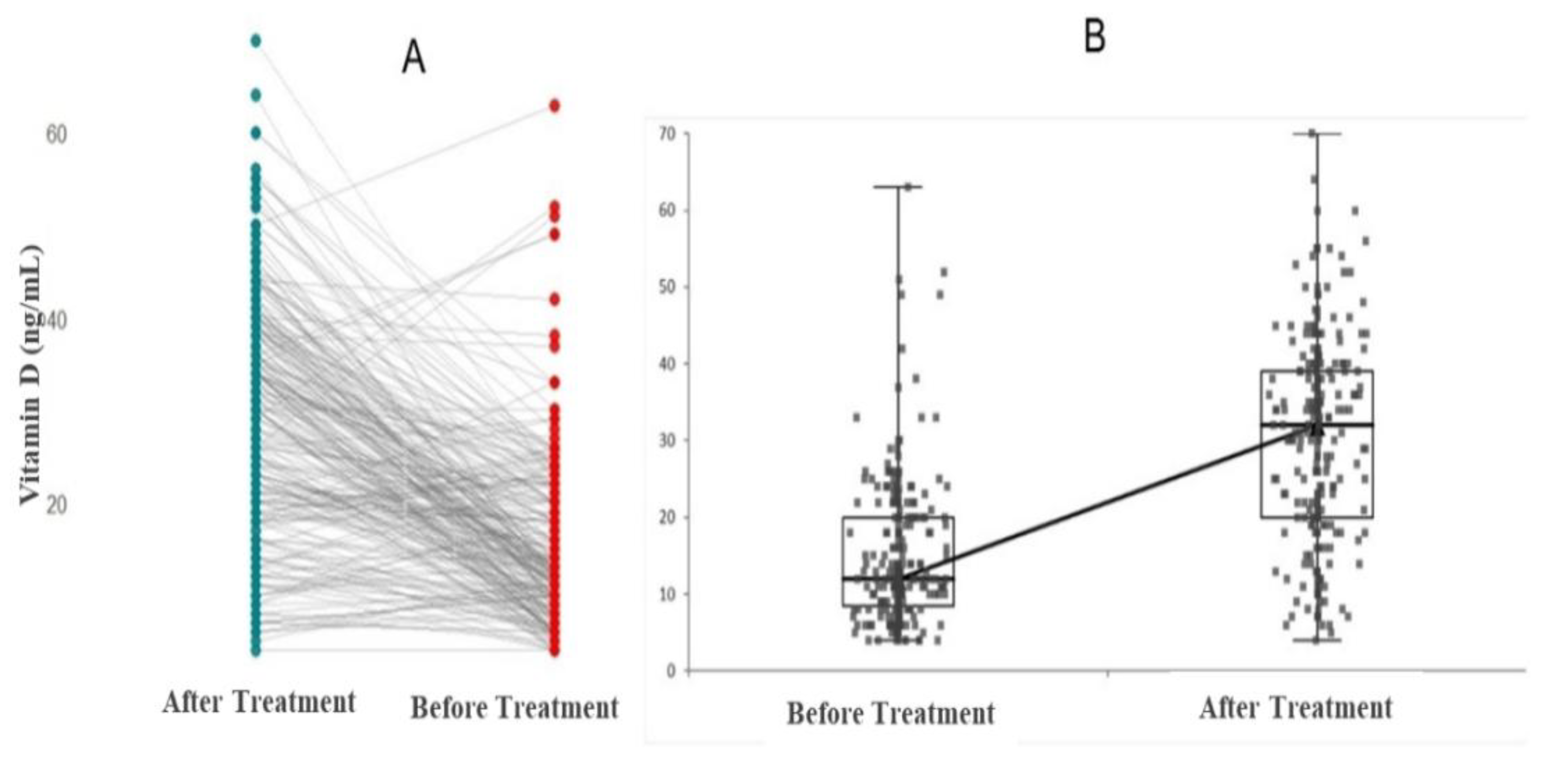
Figure 3.
Correlation analysis of vitamin D levels with age and haematological and biochemical parameters.
Figure 3.
Correlation analysis of vitamin D levels with age and haematological and biochemical parameters.
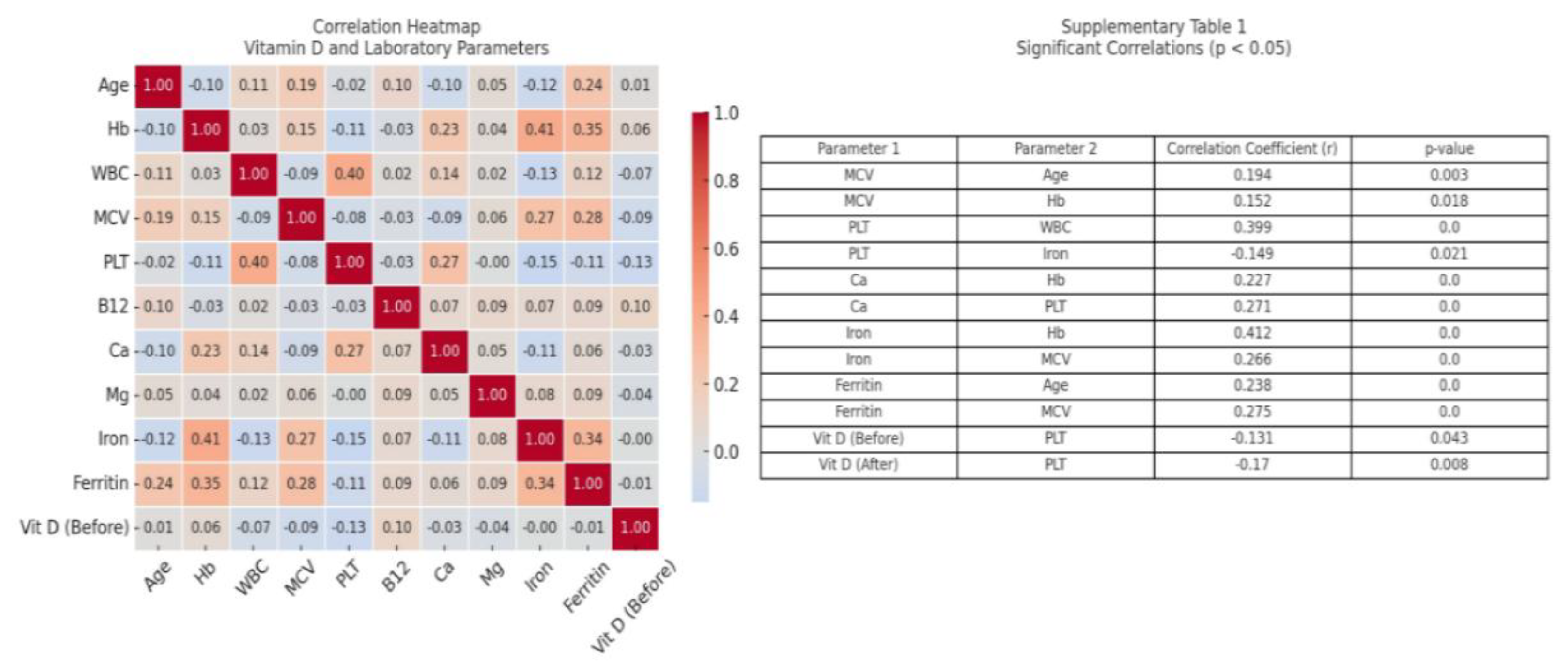

Table 1.
The descriptive data and comparison of the biochemical variables between irritabl bowel syndrome subgroups.
Table 1.
The descriptive data and comparison of the biochemical variables between irritabl bowel syndrome subgroups.
| Parameter | IBS-D Group (N=53) | IBS-C Group (N=108) | IBS-M Group (N=79) | P value |
|
Gender Female |
40 |
74 |
45 |
0.488 |
| Male | 13 | 34 | 34 | |
| Age | 44 (35-57) | 46 (37-60) | 44 (30-61) | 0.598 |
| Hemoglobin (g/dL) | 14.2 (13.1–15.9) | 14.4 (13.4–15.8) | 14.4 (13.2–15.7) | 0.728 |
| White blood cell (x103) | 8.0 (6.59–8.89) | 7.3 (6.2–8.7) | 7.3 (6.0–9.3) | 0.114 |
| Main corpuscular volume (fL) | 84.8 (81.6–88.0) | 84.9 (83.1–89.8) | 85.9 (83.1–88.0) | 0.357 |
| Platelet (x103) | 294 (235-336) | 274 (235-316) | 280 (237-327) | 0.579 |
| Vitamin B12 (pg/mL) | 277 (234-378) | 315 (241-389) | 280 (237-327) | 0.163 |
| Calcium (mg/dL) | 9.53 (9.21-8.91) | 9.56 (9.21–9.80) | 9.60 (9.20–9.90) | 0.498 |
| Magnesium (mg/dL) | 1.96 (1.84–2.11) | 1.95 (1.85–2.11) | 1.93 (1.80-2.08) | 0.609 |
| Iron (μg/dL) | 74.1 (51.6-94.1) | 78.3 (58.3-103) | 76.0 (52.0-96.6) | 0.659 |
| Ferritin (ng/mL) | 48.5 (18.8–85.3) | 50.6 (18.8–98.2) | 55.3 (23.0–121.8) | 0.082 |
| Vitamin D level at admission (ng/ml) | 12.0 (10.0-20.0) | 13.0 (9.01-22.0) | 11.0 (8.00-40) | 0.193 |
| Vitamin D level after 2 months (ng/ml) | 33.0 (26.0-36.0) | 32.0 (20.0-40.0) | 28.0 (18.0-40.0) | 0.652 |
* IBS-D: diarrhea-predominant IBS, IBS-C: constipation-predominant IBS, IBS-M: mixt-type IBS.
Table 2.
Comparison of serum vitamin D levels before and after treatment in IBS subgroups.
| IBS-D Group (N=53) | |||
| Before Treatment | After Treatment | P value | |
| Vitamin D (ng/mL) | 12 (10-20) | 33 (25-36) | 0.001 |
| IBS-C Group (N=108) | |||
| Vitamin D (ng/mL) | 13 (9-22) | 32 (20-40) | 0.001 |
| IBS-M Group (N=79) | |||
| Vitamin D (ng/mL) | 11 (8-18) | 28 (18-40) | 0.001 |
*IBS-D: diarrhea-predominant IBS, IBS-C: constipation-predominant IBS, IBS-M: mixt-type IBS.
Table 3.
Comparison of serum vitamin D levels between female and male patients in different IBS subtypes before and after treatment.
Table 3.
Comparison of serum vitamin D levels between female and male patients in different IBS subtypes before and after treatment.
| IBS-D Group (N=53) | P value | ||
| Female | Male | ||
| Before treatment Vitamin D (ng/mL) | 15 (10.2-20) | 11 (7.51-16.5) | 0.291 |
| After treatment Vitamin D (ng/mL) | 33 (21.2-33.7) | 34 (26.5-39.5) | 0.223 |
| IBS-C Group (N=108) | |||
| Before treatment Vitamin D (ng/mL) | 12 (8.75-20) | 16 (11-23.5) | 0.150 |
| After treatment Vitamin D (ng/mL) | 32 (19-40) | 32.5 (20-40.5) | 0.372 |
| IBS-M Group (N=79) | |||
| Before treatment Vitamin D (ng/mL) | 10 (7-13.5) | 13.5 (8-22.5) | 0.025 |
| After treatment Vitamin D (ng/mL) | 26 (16-39) | 34 (18.7-40.5) | 0.03 |
*IBS-D: diarrhea-predominant IBS, IBS-C: constipation-predominant IBS, IBS-M: mixt-type IBS.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



